Submitted:
08 November 2023
Posted:
08 November 2023
You are already at the latest version
Abstract
Background: Patients’ effective hand hygiene helps to reduce healthcare-associated infections, prevents the spread of nosocomial infections and communicable diseases, such as COVID-19. This study aimed to describe effective hand hygiene decisions based on the Health Action Process Ap-proach (HAPA) and whether this pattern is invariant for mental health.
Methods: Data were collected cross-sectionally from patients who had previously been admitted to a hospital (N=279; study 1) and longitudinally from psychosomatic rehabilitation patients (N=1,073; study 2). The fit of the HAPA framework and changes in hand hygiene decisions regarding com-pliance, as well as social-cognitive variables of the HAPA, and mental health status were examined.
Results: The trimmed HAPA framework fitted the data well (χ2=27.1, df=12, p<.01, CMIN/df=2.26, CFI=.97, RMSEA=.08). According to multi-group structural equation modeling, the HAPA model with hand hygiene behavior were found to be invariant with regard to mental health.
Conclusion: The trimmed HAPA framework revealed to be a generic framework in explaining so-cial-cognitive processes relating to hand hygiene decisions. Helping individuals to perform hand hygiene recommendation requires intention formation and bridging the intention-behavior gap. This can be done by promoting planning and self-efficacy. All processes appear generic to partic-ipants with and without mental health challenges.
Keywords:
Hand hygiene
; compliance
; health action process approach
; mental health
; depression
; generalized anxiety
1. Introduction
The prevention of communicable diseases and infections is key for overall population health and safety, especially in susceptible populations such as patients [1]. The prevention and containment of viruses and infections have been of elevated attention during the current COVID-19 pandemic [2]. Especially in hospital settings, many attempts were taken to ensure effective hand hygiene behavior of patients and healthcare professionals to reduce healthcare associated infections [3]. It was proven that hand hygiene behavior is a cost-effective way of reducing COVID-19 morbidity and accepted as crucial strategy to prevent the spread and transmission of COVID-19 in healthcare facilities such as hospitals [4,5]. Since still relatively little is known about patients’ hand hygiene behavior in hospitals, the aim of this study was to examine patients’ hand hygiene and its determinants [6,7]. This is especially important as many patients are oftentimes not sufficiently aware that they can actively participate in hand hygiene and thus protect themselves, and others, from infections. It is, however, crucial to understand barriers towards a good hand hygiene in hospitals in detail in order to effectively increase compliance [8].
In comparison to other preventative measures, especially hygiene behaviors, maintenance of hand hygiene behavior has been rather low, thus, calling for a better understanding of the reasons for the lack of performance and maintenance [9]. Even though individuals are often motivated to change their behavior, this initial motivation or intention does not always translate into an actual behavior change due to the intention-behavior gap [10]. Furthermore, it has been shown that even if a desired health behavior, such as hand hygiene behavior, is acquired, individuals may experience difficulties in maintaining this behavior over time and in face of difficulties. This may result in a relapse to old behavioral habits or patterns [11]. As the regulations to stop or prevent the spread and transmission of the COVID-19 virus have been introduced by the government, individuals were required to change or alter their behavior over a considerable time [12]. Several theories of social cognition have been used to provide an understanding of determinants of health-related behaviors such as hand hygiene behavior. The theory of planned behavior (TPB) as a classical and fundamental health behavior theory [13] and the Transtheoretical Model of Behavior Change (TTM) have widely been used to explain and predict health behaviors [14]. One of the main criticisms of those theories is, however, that they neglect or struggle to address the intention-behavior gap. Therefore, it has been suggested that those traditional models needed to be expanded to include a volitional phase in which individuals develop actions after having formed an intention. The Health Action Process Approach (HAPA) is an example of a theoretical behavior change model that includes both motivational and volitional phases. The HAPA has been known as a well-established theoretical framework that describes behavior changes by means of modelling social-cognitive determinants of behavior [15]. One important determinant is the intention to change, which is determined by positive and negative outcome expectancies, belief in one’s ability to perform the behavior (action self-efficacy) and acknowledgement of being at risk for not behaving in the healthy way (risk perception). If the intention is high, self-regulatory skills and planning on when, where, and how to perform the desired behavior as well as having the belief that the individual is able to engage in the desired behavior despite possible adversities (coping self-efficacy) determine action initiation. To maintain the health behavior, individuals need to be confident in their ability to sustain the behavior (maintenance self-efficacy) and need to monitor their behavior (action control) to prevent relapse [15,16,17].
The COVID-19 pandemic has increased the burden on the mental health of individuals. As a result, individuals have reported an increase in perceived distress, anxiety, and symptoms associated with depression or loneliness [18,19]. However, the questions as to whether those individuals have adapted their hygiene behaviors need further analyses. Literature has shown that mental health and compliance to recommended preventive behaviors were associated with one and another, thus creating a feedback loop [20,21]. Further, evidence examining anhedonic depression in the context of the COVID-19 pandemic has shown an association between depression and precautionary behaviors, i.e., that depressive symptoms can be a barrier of effective precautionary behaviors [22]. Furthermore, it has been shown that anhedonia has been frequently linked to poorer physical health outcomes, which may be explained by reduced self-care behaviors and self-regulatory strategies [23,24]. In addition, a decreased mental health status during the COVID-19 pandemic has been associated with more difficulties in adhering to health-related behaviors over a longer period of time [25]. Previous studies have shown that with regard to symptoms of depression, motivational deficits were associated with a reduced intention to engage in health behaviors [26]. Also, depressive symptoms have been associated with a decrease in self-efficacy and an increase in negative outcome expectations. Depressive individuals have also shown volitional deficits as they were less able to transform intentions into actions and showed reduced planning and maintenance self-efficacy capabilities [27]. According to these findings, it may be assumed that depressive patients may display reduced intentions to engage in effective hand hygiene decisions.
Despite the previous findings that mental health might be associated with deficits related to the social-cognitive variables, and consequently health behavior and outcomes, these associations have rather rarely been examined with regard to hand hygiene behavior. Thus, the present study will investigate whether hand hygiene decisions can be explained by a health behavior theory, namely the Health Action Process Approach (HAPA; [10,28]), and whether the pattern of the HAPA is invariant for mental health of the study participants.
Few studies such as the one by Gaube et al. [1] aimed to evaluate the hand hygiene behavior of patients, specifically by applying the HAPA model with inconclusive results. Self-efficacy, action control, and planning were not able to fully bridge the intention-behavior gap. Therefore, this study aims to validate previous studies on precautionary behaviors by examining the potentially important role of planning in overcoming the intention-behavior gap in hand hygiene. In addition, previous studies have not acknowledged the possible association between mental health and preventative measures (i.e., hand hygiene) in the context of the HAPA. Therefore, the current study will evaluate the HAPA determinants in the context of hand hygiene while acknowledging the role of symptoms of depression and anxiety, therefore examining invariance of the HAPA model for mental health.
In a first study, the fit of the HAPA model to hand hygiene data will be evaluated with mental health as a moderating covariate to see whether mental health will add additional variance to hand hygiene decisions beyond social-cognitive variables. In a second study, the role of mental health for the change of compliance in individuals with a pre-existing vulnerability (i.e., psychosomatic rehabilitation patients) will be evaluated in a longitudinal design. These vulnerable individuals have revealed motivational and adherence problems concerning health behaviors; thus, it is important to test whether the HAPA is robust for such potential differences. It is assumed that as psychosomatic rehabilitation patients receive behavior change interventions during their treatment, they will be more motivated to engage in hand hygiene behavior over time. Therefore, the following research questions will be tested in study 1: (a) Is the HAPA model applicable to hand hygiene decisions in patients? (b) Does a structural equation model, specified in terms of the social-cognitive variables of the HAPA, fit the data? (c) To what extend are hand hygiene decisions and its social-cognitive determinants invariant for mental health? Study 2 examined the research question: (d) Is mental health predictive of a change in hand hygiene compliance rates?
2. Materials and Methods
To test these hypotheses, two samples were recruited: people from the general population as a cross-sectional online sample (study 1) and patients from four psychosomatic rehabilitation clinics for the longitudinal analyses (study 2).
2.1. Study 1: Cross-sectional Study
2.1.1. Procedure and Participants
Participants (N=279) were recruited through press releases, social networks, and study homepages to answer an online survey. Only those indicating being admitted to a clinic during the last 60 months were included in the subsequent analyses. Data were collected anonymously between November 2019 and June 2020 in Germany in three waves before SARS-CoV-2 (n=97), during the first lockdown (n=85), and after lockdown measures were reduced (n=97)1 . All participants were informed about both the purpose of the survey and data security measures, and all were asked to indicate informed consent. The study was approved by the Ethics Committee at Jacobs University (now Constructor University; ClinicalTrials.gov Identifier: NCT04453475).
Participants who had previously (in the last 5 years)2 been admitted to a hospital as either an inpatient or an outpatient completed the online questionnaire (194 [69.5%] female, 16 [5.7%] missing). Age ranged from 18 to over 60 years. 206 (73.8%) participants revealed no depressive symptoms, while 42 (15.1%) participants showed depressive symptoms according to the threshold by Kroenke and colleagues [29]. 224 (80.3%) participants revealed no symptoms of generalized anxiety, whereas 33 (11.8%) revealed symptoms above the threshold according to Spitzer and colleagues [30].
2.1.2. Measures
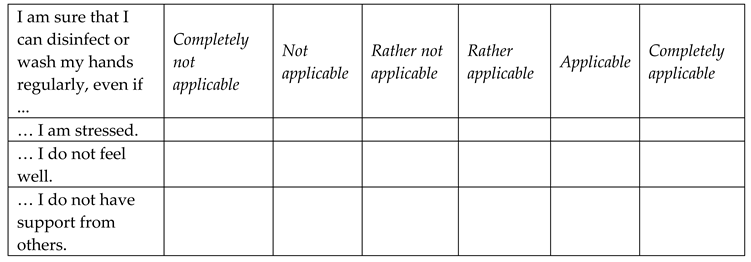
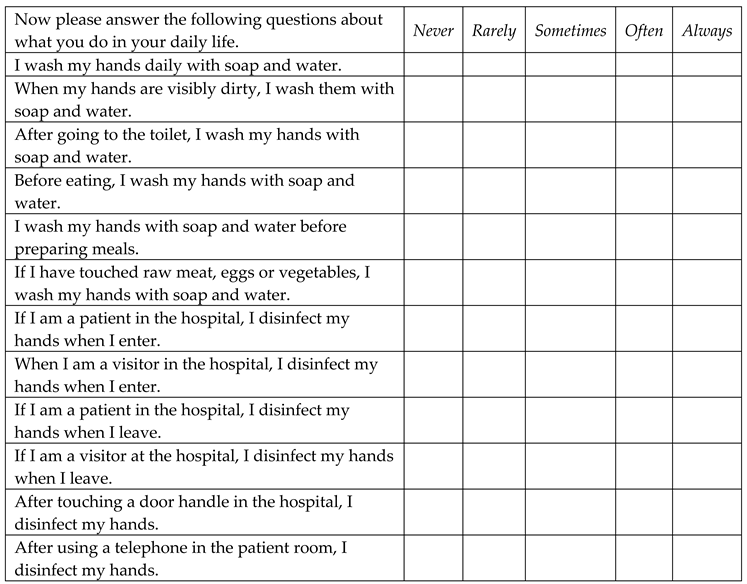
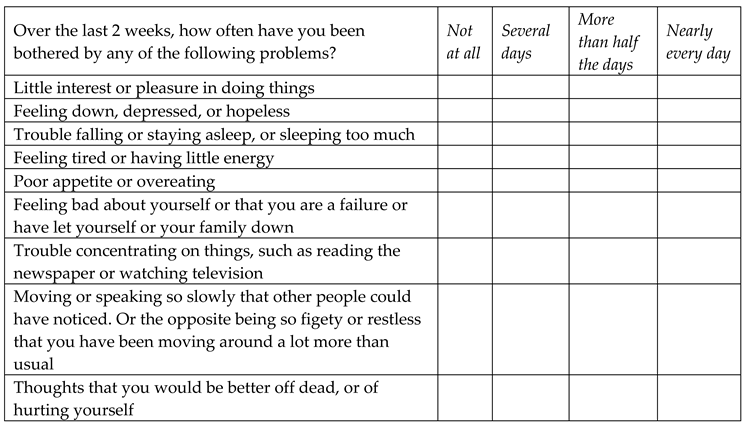
For an overview of all items used see Appendix A.
Socio-Demographic Information
Socio-demographic data included patients’ age and sex. Age was assessed in five categories (“younger than or 29 years old”, “30 to 39 years old”, “40 to 49 years old”, “50 to 59 years old” and “60 years and older”). Sex was categorized into two groups (“men” and “women”).
Hand Hygiene Decisions and HAPA Constructs
The questionnaire used to investigate social-cognitive variables of the HAPA model [31] was adapted for the purpose of hand hygiene behavior in primary healthcare settings. Risk perception was assessed using a single item on a seven-point Likert scale on which 1 indicated ‘Significantly below average’, and 7 indicated ‘Significantly above average’. Action self-efficacy (α=.87) was investigated by four items on a six-point Likert scale from 1 ‘Not at all’ to 6 ‘Completely’. Outcome expectancies (α=.83) were measured using five items on a six-point Likert scale from 1 ‘Not at all’ to 6 ‘Completely’.
Intention (α=.68) as well as action planning (α=.92) and coping planning (α=.78) were assessed using two questions each on a six-point Likert scale, where 1 indicated ‘Not at all’, and 6 indicated ‘Completely’. However, according to the literature, action and coping planning have frequently been combined as “planning”, increasing the content validity of the predictor. Hence, planning (α=.86) was used as a general construct for the following analysis [32,33]. Maintenance self-efficacy (α=.91) was assessed by three items on a six-point Likert scale from 1 ‘Not at all’ to 6 ‘Completely’. Means scores for all HAPA constructs were computed. Measures of hand hygiene decisions were adapted from the recommendations provided by the “Clean Hands Campaign”. Hand hygiene decisions were measured by twelve items on a five-point Likert scale (1-’Never’; 5-‘Always’; α=.87).. Hand hygiene decisions were measured retrospectively after discharge.
Mental Health Status
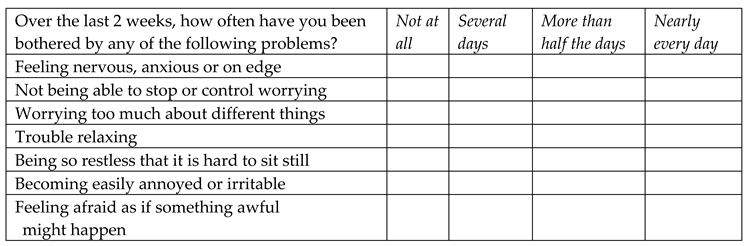
Symptoms of depression were assessed by the PHQ-9, which is the depression module of the Patient Health Questionnaire on a four-point Likert scale from 0 ‘Not at all’ to 3 ‘Nearly every day’ by asking patients to think about the past two weeks. For the analysis, composite mean scores were computed. A sum score of ≥10 depicts the cut-off value for symptom threshold. Cronbach’s alpha was .89 in primary care settings [29].
The GAD-7, a self-report measure of generalized anxiety disorder symptoms, was used to determine the symptom threshold of generalized anxiety. The seven items were measured on a 4-point Likert scale from 0 ‘Not at all’ to 3 ‘Nearly every day’. The questionnaire requires patients to think about the past two weeks. A sum score of ≥ 10 represents the cut-off value for the symptom threshold for symptoms of generalized anxiety. Primary validation estimated a Cronbach’s alpha of .86 [30].
2.1.3. Data Analysis
A bivariate correlation table (Table 1), including all HAPA variables, was used to examine correlations between the social-cognitive variables and hand hygiene decisions. Furthermore, structural equation modeling (SEM) with latent variables was performed to test whether the HAPA fitted the data, as well as to examine whether planning mediated the behavior-intention gap. For SEM fit indices including chi-square (χ²), degrees of freedom (df), chi-square to df ratio (CMIN/df), p-values for χ²-Test, Comparative Fit Index (CFI), and Root Mean Square Error of Approximation (RMSEA) were evaluated. A model is evaluated to have a good fit to the data if the following fit indices have been fulfilled: a CFI and TLI with values higher than .90 and a value of below .08 with regard to the RMSEA [34]. As the χ² statistic is considered to be dependent of the sample size, the χ²/df ratio was used as a goodness-of-fit criterion for the purposes of this paper. As suggested by [35], χ² should not be larger than 2-5 times of the degrees of freedom. The model with the best-fit indices was used for multi-group structural equation modeling to test for invariances across subsamples. Differences in the HAPA constructs and hand hygiene behavior between individuals below and above the symptom threshold for psychological symptoms were analyzed by latent means. Hence, mental health was treated as a moderating covariable.
Missing Data
The amount of missing data per item was below 5% for both samples. Participants with missing data on the social-cognitive variables were included in the analysis if they had at least one non-missing data point under the assumption of missing (completely) at random. Missing data were imputed via the full information likelihood method (FIML) in AMOS v. 28.
2.2. Study 2: Longitudinal Study
2.2.1. Procedure and Participants: Longitudinal Study
Participants (N=1,073) were recruited through four psychosomatic rehabilitation clinics from the Dr. Becker clinic group between July 2020 and August 2021. Data collection was performed longitudinally with two measurement timepoints. Data was collected from six weeks until the first day of the rehabilitation treatment and up to 12 weeks post-rehabilitation treatment. All participants were informed about the purpose of the study as well as associated data security measures on the clinic’s own study portal. Ethical approval for the study was obtained by Jacobs University at 17 September 2019 (protocol code 2020_09; date of approval: June 25, 2020; the Ethics Committee at Jacobs University (now Constructor University; ClinicalTrials.gov Identifier: NCT04453475). In total, N=1,073 participants took part in the study at both timepoints (before rehabilitation and after rehabilitation). Patients’ age, measured in categories, ranged from 18 to above 60 years. The most frequently reported age group was between 50 and 59 years (50.6%). 697 (65.4%) patients reported to be female.
2.2.2. Measures
Change in Hand Hygiene Decisions
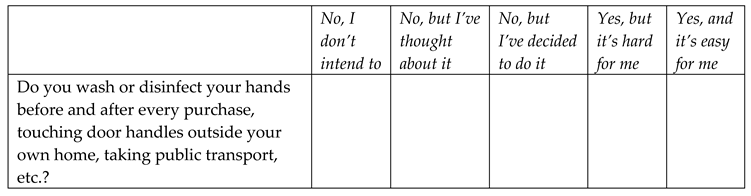
Measures for socio-demographic information were the same as in the cross-sectional study. Participants from the psychosomatic rehabilitation clinics (longitudinal study) were asked to answer a stage item assessing the intention to perform hand hygiene behavior on a 5-point Likert scale (1 = No, I do not intend to; 2 = No, but I have thought about it; 3 = No, but I have decided to do it; 4 = Yes, but it is hard for me; 5 = Yes, and it is easy for me). Answers were dichotomized as “non-compliant” (1-3) and “compliant” (4-5). For patients progressing from non-compliant at the first timepoint to compliant at the second timepoint, a ‘1’ was coded. Conversely, for patients regressing, a ‘-1’ was coded. With respect to patients who did not change in their compliance, a ‘0’ was coded.
Mental Health Symptoms
To measure depressive symptoms during the past, the PHQ-2 was administered which is part of the Patient Health Questionnaire-4 (PHQ-4) with two items [36] on a 4-point Likert scale from 0 ‘not at all’ to 3 ‘nearly every day’. A scale sum score of ≥3 (T1 Spearman’s rho=.83; T2 Spearman’s rho=.85) depicts the cut-off value between the normal range and a probable case of depression [37]. The PHQ-2 was used as a measure of symptom intensity.
In addition, the generalized anxiety index was examined via the GAD-2 which is a questionnaire part of the PHQ-4 [38]. The GAD-2 encompasses two items measuring symptoms of generalized anxiety during the past two weeks on a 4-point Likert scale from 0 ‘not at all’ to 3 ‘nearly every day’. A sum score of ≥3 [39] serves as the cut-off value between the normal range and a possible case of a generalized anxiety disorder (T1 Spearman’s rho=.80; T2 Spearman’s rho=.83). In contrast to the GAD-7, the GAD-2 was only used as a measure of symptoms intensity.
2.2.3. Data Analysis
To evaluate whether mental health (i.e. depression and generalized anxiety) played a role in changes in compliance with regard to hand hygiene decisions, the change was evaluated by a logistic regression analysis controlling for gender and age. Odds ratio with a 95% confidence interval was used to report the effect size estimate. Wald static was used as an indicator of the significance of each regression coefficient in the binary logistic regression. All of the analyses were conducted using IBM SPSS v.28 and AMOS v.28.
3. Results
3.1. Study 1
3.1.1. Scale Internal Consistency and Correlations between Constructs
Table 1 shows bivariate correlations between the social-cognitive variables for participants.
3.1.2. Structural Equation Modeling
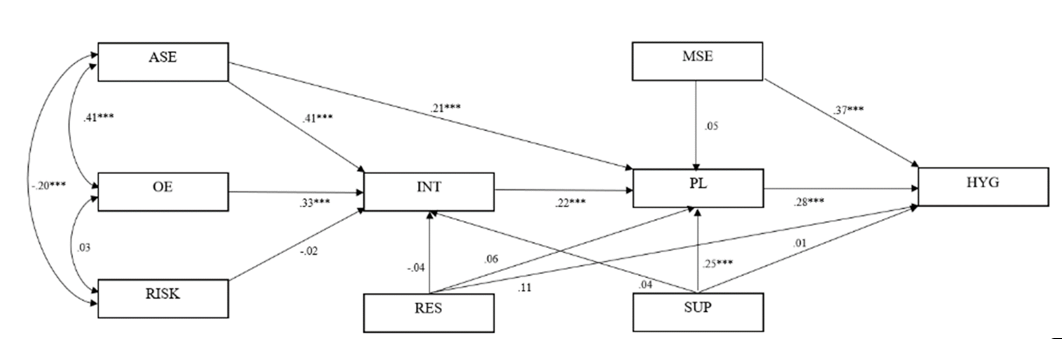
To examine links between HAPA variables, a structural equation modeling was run (see Figure 1). The hypothesized model had a poor fit with the proposed data according to literature [40,41]. Fit indices for the model were as follows: χ²=339.20, df=19; p<.001, CMIN/df=17.85, CFI=.53, RMSEA=.25. Standardized estimates for each path are reported in Figure 1.
Considering age and gender, as well as depressive and generalized anxiety symptoms as covariates, modifications proposed by AMOS lead to a final adaption of the HAPA framework with a reasonably good fit: χ²=27.1, df=12, p<.01, CMIN/df=2.26, CFI=.97, RMSEA=.08. The standardized estimates for each path in the trimmed HAPA framework are reported in Figure 2. All paths were significant at either p<.01 or p<.001 ranging between ß=-.20 and ß=.43. All covariates revealed to be non-significant except for symptoms of generalized anxiety which were associated with hand hygiene behavior, ß= -.16, p<.05. Adding mental health as a moderating covariate to the model increased variance from 38.1% to 39.3% of explained variance with regard to intention and from 21.8% to 23.5% for planning. All HAPA variables were able to explain 31.9% of variance in hand hygiene decisions and 33.2% when mental health was added as a moderating covariate to the model. However, the increase in variance revealed to be not significant.
3.1.3. Latent Mean Differences Across Mental Health Status
To test for potential differences in the HAPA constructs from the trimmed HAPA framework (Figure 2) between patients above and below the symptom threshold for generalized anxiety as well as for depression, a three-step multi-group analysis was conducted applying (1) an unrestricted model, (2) a semi-restricted model, and (3) a fully restricted model. All were subsequently compared with the χ² difference indices according to Yuan and Bentler [42].
With regard to depression, indices indicated a good fit for the unrestricted, semi-restricted, and full-restricted model (Table 2). Hence, χ²-difference tests between the unrestricted and semi-restricted model (χ²(12)=11.29, p=.501) and between the semi-restricted and fully restricted model (χ²(15)=11.38, p=.734) were performed and did not reach significance. Results confirmed measurement invariance and allowed for group comparison. This suggests structural equivalence [42], stating that, for patients above and below the symptom threshold for depression, the HAPA constructs were equivalent concerning their structural pattern and their magnitude. Therefore, no differences were detected concerning the symptomatology of depression in the pattern of relationships.
With regard to symptoms of anxiety, indices again indicated a good fit for the unrestricted, semi-restricted, and full-restricted model (Table 3). Hence, a χ²-difference test between the unrestricted and semi-restricted model (χ²(12)=10.884, p=.543) and between the semi-restricted and fully restricted model (χ²(15)=23.17, p=.082) was performed and did not reach significance. Results confirmed measurement invariance and allowed for group comparison. Hence, for patients above and below the symptom threshold for generalized anxiety, the HAPA constructs were equivalent concerning their structural pattern and magnitude. Therefore, no differences were detected concerning the symptomatology of generalized anxiety in the pattern of relationships.
With the results showing that factor loadings and covariances were invariant across individuals below and above the symptom threshold for depression as well as anxiety, the assumption for latent mean analysis was met. Therefore, it was analyzed to determine if the latent means of the HAPA constructs of the trimmed framework were different across individuals below and above the symptom threshold for depression and generalized anxiety. To estimate the latent mean differences between groups, the group below the symptom threshold for depression and generalized anxiety operated as a reference group. The latent mean was fixed to zero, against which the latent means of the other group were compared. The latent mean for the other group, above the symptom threshold for depression and generalized anxiety, was freely estimated.
Analysis of latent means of HAPA constructs revealed no significant differences between individuals below the symptom threshold and above the symptom threshold for depression and generalized anxiety (Table 4).
3.2. Study 2
3.2.1. Changes in compliance and its predictors
To analyze whether mental health was a predictor in changes regarding compliance or non-compliance in hand hygiene decisions, data from the longitudinal sample of psychosomatic rehabilitation patients was used. Table 5 shows the distribution and transitions of compliance with hand hygiene decisions from before to after rehabilitation.
Stages of compliance differed significantly regarding hand hygiene behavior, (F(1,1064)=2152.79, p<.01: those who were compliant had an average compliance score of 4.80 (SD=0.40) compared to non-compliant patients (M=2.11; SD=0.76).
The results of the binary logistic regression indicate that neither symptoms of depression nor generalized anxiety were significant predictors of change in compliance. Odds ratios, Wald statistics, and descriptive data are summarized in Table 6.
4. Discussion
The current study aimed to evaluate, as part of study 1, whether the theoretical structure of the HAPA model with its social-cognitive variables predicting health behavior can be fitted to hand hygiene decisions and whether the model is invariant for mental health (i.e., symptoms of depression and anxiety). Study 1 especially investigated whether planning was able to bridge the intention-behavior gap. Our results support the hypothesis evaluating interrelations between all HAPA variables and hand hygiene decisions: all variables (except for risk perception) were positively correlated with each other. Risk perception was negatively correlated with action self-efficacy, intention, maintenance self-efficacy, planning, and hand hygiene behavior as predicted.
With regard to whether the HAPA fitted the data well, the first attempt revealed a poor fit according to commonly accepted fit indices [43]. This, however, is not surprising as models with a good fit found in literature often are incomplete and do not include all of the HAPA constructs [28,44].
The final attempt to fit the HAPA model to the data after iterative changes revealed significant paths and acceptable fit indices. Still, the latest model needs to be treated with caution as the model fit was not strong according to the RMSEA [45]. However, like Kenny et al. [46] suggested, sample size and degrees of freedom also need to be looked at when interpreting RMSEA. Hence, models with small sample sizes and low degrees of freedom tend to display an elevated RMSEA. Therefore, taking all fit indices into consideration, we can assume that the proposed model fits our data. This is in line with the literature as the HAPA model has been used previously to explain healthcare workers’ hand hygiene as well as to inform successful interventions [47]. In a recent study, Gaube et al. found that the HAPA model could explain patients’ and visitors’ hand hygiene [1]. Hence, based on previous evidence, it seems that hand hygiene behavior is a health behavior developing in a dynamic process that is fairly similar between patients with limited or good mental health. Therefore, as expected, the process of performing hand hygiene along the HAPA may be described as follows: In the motivational phase, outcome expectancies and action self-efficacy were associated with intention.
These results indicate that improving beliefs about the beneficial effects of performing good hand hygiene might be promising when motivating patients to become more active concerning their hand hygiene. Contrary to the hypothesized structure of the HAPA, risk perception was not associated with intention. Risk perception does not seem to be significantly associated with the intention to practice good hand hygiene in the context of the HAPA model. This is in line with other studies in the area of physical activity [48,49]. These last findings have suggested that risk perception may not be sufficient to form an actual intention to change health behavior [15] and may instead be a distal predictor of hand hygiene behavior [33].
However, for effective maintenance and performance to occur, necessary self-regulatory strategies, such as planning, need to be developed and maintained in the volitional stage. It has been assumed that planning bridges the intention-behavior gap, thus ensuring maintenance of hand hygiene. Similar to the results by Gaube et al. [1], our results have shown a direct link between intention and the desired behavior. However, their study lacks results regarding the mediating effect of planning. Hence, the present study is the first to show that, for hand hygiene behavior of patients to be maintained, planning has the function to bridge the intention-behavior gap. Nevertheless, the present study did not include or acknowledge other self-regulatory skills, automatism, and action control as part of this study. Hence, integrating those variables should be regarded in future research.
Validating the HAPA as a generic framework in explaining social-cognitive processes of hand hygiene decisions invariant for mental health is in line with previous studies examining compliance to hand hygiene behavior in the general population, as well as in psychosomatic rehabilitation patients. Prior research indicates that both groups of participants display good hand hygiene behavior when either possessing greater fear of an infection or being more susceptible to anxiety [50,51]. In addition, the systematic review by Farholm and Sørensen [26] suggested no differences in motivational mechanisms between the normal population and individuals with mental illnesses.
Finally, as part of study 2, we aimed to investigate whether symptoms of depression and generalized anxiety were predictive of a change in compliance in hand hygiene decisions in psychosomatic rehabilitation patients. Our results indicated that neither symptoms of depression nor generalized anxiety were predictive of a change in compliance. Firstly, these findings confirm results from the general population that compliance with hand hygiene behavior is independent of mental health status [51]. However, previous researchers assumed that a reduced mental health status would be associated with a poorer compliance in hand hygiene behavior and that psychosomatic rehabilitation treatments would encourage health behavior change in patients. The present results do not support these assumptions. Possibly, hand hygiene is a rather stable construct irrespective of mental health status. For example, individuals who were compliant with hand hygiene behavior prior to the pandemic also were compliant during the pandemic and vice versa [52], which may also explain the absence of any differences based on the two data collection points (see Appendix B). Therefore, non-compliant individuals need to be encouraged to perform adequate hand hygiene. One way to do so may be to implement interventions that foster planning and self-efficacy measures, helping to overcome the intention-behavior gap where needed [47]).
The study was subjected to several limitations. All variables examining hand hygiene decisions within the general population were (retrospective) self-report measures collected at one point in time. This was done to validate previous research (e.g., [44]) and to assess data during the COVID-19 pandemic. However, recall bias and social desirability need to be considered when interpreting participants’ responses. To overcome this limitation, the handwashing behavior of patients should be observed by trained observers or tracked by technical devices. Still, even with testing for differences in time between hospitalization and participation in the survey (with regard to the self-reporting of hand hygiene behavior), no significant differences were found. This suggests that even though self-reporting biases and social desirability should be acknowledged, reported hand hygiene decisions have remained stable. Additionally, mental health was examined by a validated questionnaire but not via a diagnosis according to the International Classification of Disease (ICD-10) manual. Furthermore, mental health symptoms might have been exacerbated by the COVID-19 pandemic (e.g., through increasing uncertainty, reduced social contacts). Hence, the expression of depressive symptoms, or symptoms of generalized anxiety, may be confounded by the current situation and should be considered in future research.
A further methodological limitation may be that study 1 used data from a cross-sectional study to investigate hand hygiene processes in the general population. Using structural equation modeling on cross-sectional data does not reflect the dynamic nature of underlying processes over time and thus violates model assumptions. However, testing for differences in depression and generalized anxiety has shown no significant differences across the two timepoints of measurement, suggesting relatively stable constructs irrespective of situational context. It is recommended that future research should validate the results from the trimmed HAPA-model in the form of a prospective or experimental study (i.e., a randomized controlled trial) to determine causal effects conclusively. Prospective behavioral measures, especially of the main outcome of hand hygiene decisions, should be applied.
Another limitation is that only a few participants with symptoms of depression and generalized anxiety could be included in this study from the general population, thus, compromising the statistical power. Nevertheless, the findings of this cross-sectional study and longitudinal examination can contribute to the understanding of the current state of hand hygiene adherence of patients and provide a basis for designing interventions to improve psychological aspects related to hand hygiene.
Results indicate that encouragement for the patients, regardless of their mental health status, to create hand washing plans for specific situations should be considered when designing interventions. In this regard, digital tools could be employed to function as reminders of plans and past successes. The present results indicate that social-cognitive variables and self-regulatory processes are necessary determinants for effective hand hygiene behavior. Therefore, to make patients more aware of the necessity and to support them by reducing the need for self-regulatory processes, hospitals should be encouraged to promote hand hygiene behavior throughout the healthcare facilities with visible posters or dispensers at accessible and visible locations as shown in studies by Hobbs et al. [53].
To increase the intention to perform hand hygiene behavior, visual, auditory, and dynamic videos should be employed to encourage patients to clean their hands which has shown to be effective in other hospitals [54]. Furthermore, individuals should be better informed about the potential risks associated with reduced hand washing behavior and compliance. Literature has shown that, in general and irrespective of mental health status, individuals report more compliance if they are aware of the potential risks [51]. Hence, communication in the public media and in hospitals (i.e., on leaflets or posters) needs to be clearer and more objective while focusing on the risks.
5. Conclusions
In conclusion, the trimmed version of the HAPA model fitted hand hygiene data collected from the general public while highlighting significant associations between intention, planning and hand hygiene decisions. Furthermore, planning bridged the intention-behavior gap with regard to hand hygiene decisions. Irrespective of the mental health status of individuals, hand hygiene decisions could be explained by the social-cognitive variables of the HAPA model. In addition, the mental health status of the patients did not play a significant role in changes in compliance (i.e., from non-compliance to compliance or vice versa) with hand hygiene decisions. The present findings indicate that interventions should focus on social-cognitive predictors rather than on the role of mental health with regard to hand hygiene behavior. Drawing on the actual findings, it is feasible to help individuals to perform hand hygiene by intention formation and bridge the intention-behavior gap by planning and self-efficacy, regardless of mental health status.
Supplementary Materials
This paper includes results of the doctoral thesis entitled Understanding Patients and Mental Health during the COVID-19 Pandemic thru a Psychological Lens: Needs, Resources and Implications published by F.M.K. which can be downloaded at https://opus.constructor.university/frontdoor/index/index/docId/1105 or at https://portal.dnb.de/opac.htm?method=simpleSearch&cqlMode=true&query=idn%3D1265174520.
Author Contributions
Conceptualization, FK & SL; methodology, FK & SL; software, FK; validation, SL & AD; formal analysis, FM; investigation, FK & SL; resources, SL; data curation, FK; writing—original draft preparation, FK; writing—review and editing, AD & SL; visualization, FK; supervision, SL; project administration, FK; funding acquisition, SL & AD. All authors have read and agreed to the published version of the manuscript.
Funding
This research was partially funded by the Innovation Fund of the Federal Joint Committee, grant number 01VSF18023.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Ethics Committee of Jacobs University Bremen (protocol code 2020_09 and date of approval: 25 June 2020).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to confidential patient data being used.
Acknowledgments
This paper includes results of the doctoral thesis entitled Understanding Patients and Mental Health during the COVID-19 Pandemic thru a Psychological Lens: Needs, Resources and Implications published by F.M.K. at the faculty of Health Psychology and Behavioral Medicine at Jacobs University in 2022. We would like to thank Tran Ngoc Huong Quan for proofreading and editing the manuscript.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A. Questionnaire and items used
Risk perception – cross-sectional
| significantly below average | below average | rather below average | average | rather above average | above average | significantly above average | |
| Compared to an average person of my gender and age, my risk of getting an infection from poor hand hygiene is… |
Action self-efficacy – cross-sectional
| I am sure that I can regularly wash and disinfect my hands, even if... | Completely not applicable | Not applicable | Rather not applicable | Rather applicable | Applicable | Completely applicable |
| ... I have to force myself to do it. | ||||||
| ... it is time-consuming. | ||||||
| ... others do not wash their hands. | ||||||
| … even if my hands get dry. |
Outcome expectancies – cross-sectional
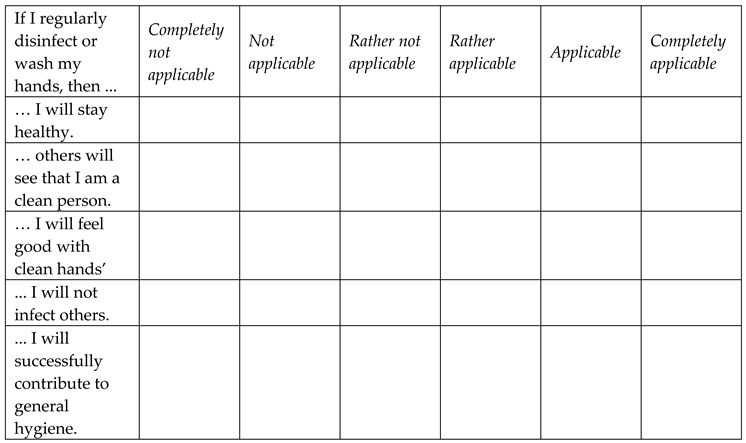 |
Intention – cross-sectional
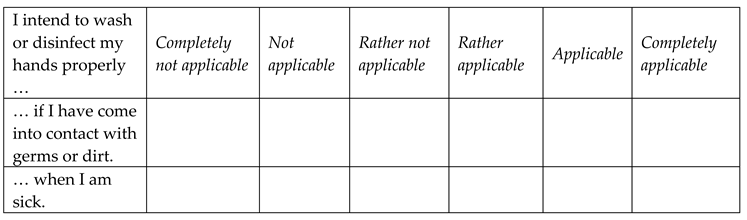 |
Action planning – cross-sectional
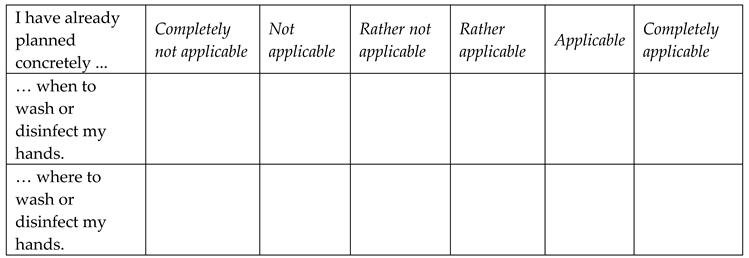 |
Coping planning – cross-sectional
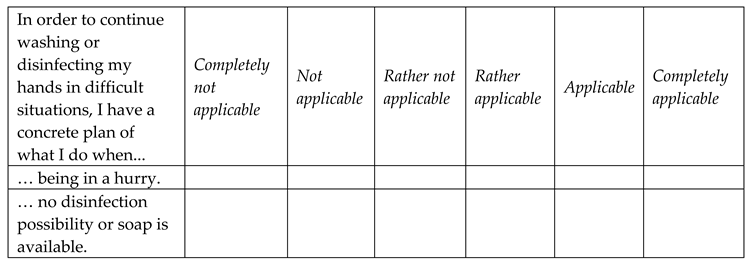 |
Maintenance self-efficacy – cross-sectional
 |
Hand hygiene behavior – cross-sectional
 |
PHQ-9 (Depression) – cross-sectional
 |
GAD-7 (Anxiety) – cross-sectional
 |
Hand hygiene behavior stage item – longitudinal
 |
PHQ-4 (Depression and Anxiety) – longitudinal
 |
Appendix B. Difference between participants from the three measurement waves
To examine differences in participants across the three measurement waves, chi-square analyses and analyses of variance were performed. The results showed no significant differences with respect to symptoms of depression χ²(2, n=248)=0.08 and for symptoms of generalized anxiety controlling for age and gender. In addition, no significant differences between the three waves were found with regard to the HAPA variables: outcome expectancies F(2, 266)=1.07, p=.34, ηp2=.02, risk perception F(2, 266)=1.75, p=.18, ηp2=.01, action self-efficacy F(2, 266)=2.76, p=.06, ηp2=.02, intention F(2, 278)=2.49, p=.07, ηp2=.02, maintenance self-efficacy F(2, 266)=1.79, p=.17, ηp2=.03, and planning F(2, 278)=3.00, p=.51, ηp2=.02 controlling for age and gender. In addition, no significant differences were found with regard to hand hygiene behavior between the three measurement waves F(2, 266) =0.45, p=.64, ηp2=.01.However, results revealed to be significant with regard to resources F(2, 266)=15.08, p<.01, ηp2=.10 and support F(2, 266)=13.67, p<.01, ηp2=.10 while controlling for the covariates age and gender.
Appendix C. Differences in variables with regard to time of hospital visit.
In order to control for time differences with regard to hospital visit as either an inpatient or an outpatient, variables related to the HAPA model as well as hand hygiene behavior and mental health related symptoms were examined for significant differences. No significant differences were revealed for the following variables: hand hygiene behavior, F(2, 266)=2.67, p=.07, ηp2=.02, action self-efficacy, F(2, 266)=2.37, p=.10, ηp2=.02, risk perception F(2, 266)=1.13, p=.32, ηp2=.01, outcome expectancies, F(2, 266)=0.29, p=.75, ηp2=.01, intention F(2, 266)=0.06, p=.94, ηp2=.01, maintenance self-efficacy, F(2, 266)=0.30, p=.74, ηp2=.01, planning, F(2, 266)=0.51, p=.60, ηp2=.01, resources, F(2, 266)=3.04, p=.54, ηp2=.02, and support F(2, 266)=.73, p=.48, ηp2=.01, symptoms of depression, F(2, 237)=0.49, p=.61, ηp2=.01, and symptoms of generalized anxiety, F(2, 246)=2.50, p=.08, ηp2=.02 controlling for age and gender.
| 1 | No significant differences were found for social-cognitive variables and mental health variables between the three measurement timepoints except for resources and support (see Appendix B). |
| 2 | No significant differences were found for social-cognitive variables and mental health symptoms (i.e. depression and anxiety) with regard to time between hospital visit and partaking in the survey (see Appendix C). |
References
- Gaube, S.; Fischer, P.; Lermer, E. Hand(y) Hygiene Insights: Applying Three Theoretical Models to Investigate Hospital Patients’ and Visitors’ Hand Hygiene Behavior. PLOS ONE 2021, 16, e0245543. [Google Scholar] [CrossRef] [PubMed]
- Abdelrahman, M. Personality Traits, Risk Perception, and Protective Behaviors of Arab Residents of Qatar During the COVID-19 Pandemic. Int. J. Ment. Health Addict. 2022, 20, 237–248. [Google Scholar] [CrossRef] [PubMed]
- Sickbert-Bennett, E.E.; DiBiase, L.M.; Willis, T.M.S.; Wolak, E.S.; Weber, D.J.; Rutala, W.A. Reduction of Healthcare-Associated Infections by Exceeding High Compliance with Hand Hygiene Practices. Emerg. Infect. Dis. 2016, 22, 1628–1630. [Google Scholar] [CrossRef] [PubMed]
- Juneau, C.-E.; Pueyo, T.; Bell, M.; Gee, G.; Collazzo, P.; Potvin, L. Lessons from Past Pandemics: A Systematic Review of Evidence-Based, Cost-Effective Interventions to Suppress COVID-19. Syst. Rev. 2022, 11, 90. [Google Scholar] [CrossRef] [PubMed]
- Lotfinejad, N.; Peters, A.; Pittet, D. Hand Hygiene and the Novel Coronavirus Pandemic: The Role of Healthcare Workers. J. Hosp. Infect. 2020, 105, 776–777. [Google Scholar] [CrossRef]
- Bellissimo-Rodrigues, F.; Pires, D.; Zingg, W.; Pittet, D. Role of Parents in the Promotion of Hand Hygiene in the Paediatric Setting: A Systematic Literature Review. J. Hosp. Infect. 2016, 93, 159–163. [Google Scholar] [CrossRef]
- Sande-Meijide, M.; Lorenzo-González, M.; Mori-Gamarra, F.; Cortés-Gago, I.; González-Vázquez, A.; Moure-Rodríguez, L.; Herranz-Urbasos, M. Perceptions and Attitudes of Patients and Health Care Workers toward Patient Empowerment in Promoting Hand Hygiene. Am. J. Infect. Control 2019, 47, 45–50. [Google Scholar] [CrossRef]
- Scheithauer, S.; Lemmen, S.W. How Can Compliance with Hand Hygiene Be Improved in Specialized Areas of a University Hospital? J. Hosp. Infect. 2013, 83 Suppl 1, S17–22. [Google Scholar] [CrossRef]
- Jabbari, P.; Taraghikhah, N.; Jabbari, F.; Ebrahimi, S.; Rezaei, N. Adherence of the General Public to Self-Protection Guidelines During the COVID-19 Pandemic. Disaster Med. Public Health Prep. 2022, 16, 871–874. [Google Scholar] [CrossRef]
- Schwarzer, R.; Luszczynska, A. How to Overcome Health-Compromising Behaviors: The Health Action Process Approach. Eur. Psychol. 2008, 13, 141–151. [Google Scholar] [CrossRef]
- Kwasnicka, D.; Dombrowski, S.U.; White, M.; Sniehotta, F. Theoretical Explanations for Maintenance of Behaviour Change: A Systematic Review of Behaviour Theories. Health Psychol. Rev. 2016, 10, 277–296. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, K.; Smith, S.R.; Keech, J.J.; Moyers, S.A.; Hagger, M.S. Application of the Health Action Process Approach to Social Distancing Behavior During COVID-19. Appl. Psychol. Health Well-Being 2020, 12, 1244–1269. [Google Scholar] [CrossRef] [PubMed]
- Sheeran, P.; Klein, W.M.P.; Rothman, A.J. Health Behavior Change: Moving from Observation to Intervention. Annu. Rev. Psychol. 2017, 68, 573–600. [Google Scholar] [CrossRef] [PubMed]
- Hashemzadeh, M.; Rahimi, A.; Zare-Farashbandi, F.; Alavi-Naeini, A.M.; Daei, A. Transtheoretical Model of Health Behavioral Change: A Systematic Review. Iran. J. Nurs. Midwifery Res. 2019, 24, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Schwarzer, R.; Lippke, S.; Luszczynska, A. Mechanisms of Health Behavior Change in Persons with Chronic Illness or Disability: The Health Action Process Approach (HAPA). Rehabil. Psychol. 2011, 56, 161–170. [Google Scholar] [CrossRef] [PubMed]
- Lao, C.K.; Li, X.; Zhao, N.; Gou, M.; Zhou, G. Using the Health Action Process Approach to Predict Facemask Use and Hand Washing in the Early Stages of the COVID-19 Pandemic in China. Curr. Psychol. N. B. NJ 2023, 42, 6484–6493. [Google Scholar] [CrossRef] [PubMed]
- Liang, W.; Duan, Y.; Li, F.; Rhodes, R.E.; Wang, X.; Peiris, D.L.I.H.K.; Zhou, L.; Shang, B.; Yang, Y.; Baker, J.S.; et al. Psychosocial Determinants of Hand Hygiene, Facemask Wearing, and Physical Distancing During the COVID-19 Pandemic: A Systematic Review and Meta-Analysis. Ann. Behav. Med. Publ. Soc. Behav. Med. 2022, 56, 1174–1187. [Google Scholar] [CrossRef] [PubMed]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The Psychological Impact of Quarantine and How to Reduce It: Rapid Review of the Evidence. Lancet Lond. Engl. 2020, 395, 912–920. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.A. Coronavirus Anxiety Scale: A Brief Mental Health Screener for COVID-19 Related Anxiety. Death Stud. 2020, 44, 393–401. [Google Scholar] [CrossRef]
- Cawcutt, K.A.; Starlin, R.; Rupp, M.E. Fighting Fear in Healthcare Workers during the COVID-19 Pandemic. Infect. Control Hosp. Epidemiol. 2020, 41, 1192–1193. [Google Scholar] [CrossRef]
- Ejeh, F.E.; Owoicho, S.; Saleh, A.S.; Madukaji, L.; Okon, K.O. Factors Associated with Preventive Behaviors, Anxiety among Healthcare Workers and Response Preparedness against COVID-19 Outbreak: A One Health Approach. Clin. Epidemiol. Glob. Health 2021, 10, 100671. [Google Scholar] [CrossRef] [PubMed]
- Denollet, J.; Pedersen, S.S.; Daemen, J.; de Jaegere, P.; Serruys, P.W.; van Domburg, R.T. Reduced Positive Affect (Anhedonia) Predicts Major Clinical Events Following Implantation of Coronary-Artery Stents. J. Intern. Med. 2008, 263, 203–211. [Google Scholar] [CrossRef] [PubMed]
- Kessing, D.; Pelle, A.J.; Kupper, N.; Szabó, B.M.; Denollet, J. Positive Affect, Anhedonia, and Compliance with Self-Care in Patients with Chronic Heart Failure. J. Psychosom. Res. 2014, 77, 296–301. [Google Scholar] [CrossRef]
- Leventhal, A.M. Relations Between Anhedonia and Physical Activity. Am. J. Health Behav. 2012, 36, 860–872. [Google Scholar] [CrossRef] [PubMed]
- Beeckman, M.; De Paepe, A.; Van Alboom, M.; Maes, S.; Wauters, A.; Baert, F.; Kissi, A.; Veirman, E.; Van Ryckeghem, D.M.L.; Poppe, L. Adherence to the Physical Distancing Measures during the COVID-19 Pandemic: A HAPA-Based Perspective. Appl. Psychol. Health Well-Being 2020, 12, 1224–1243. [Google Scholar] [CrossRef] [PubMed]
- Farholm, A.; Sørensen, M. Motivation for Physical Activity and Exercise in Severe Mental Illness: A Systematic Review of Cross-Sectional Studies. Int. J. Ment. Health Nurs. 2016, 25, 116–126. [Google Scholar] [CrossRef] [PubMed]
- Krämer, L.V.; Helmes, A.W.; Seelig, H.; Fuchs, R.; Bengel, J. Correlates of Reduced Exercise Behaviour in Depression: The Role of Motivational and Volitional Deficits. Psychol. Health 2014, 29, 1206–1225. [Google Scholar] [CrossRef] [PubMed]
- Lhakhang, P.; Lippke, S.; Knoll, N.; Schwarzer, R. Evaluating Brief Motivational and Self-Regulatory Hand Hygiene Interventions: A Cross-over Longitudinal Design. BMC Public Health 2015, 15, 79. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a Brief Depression Severity Measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Löwe, B. A Brief Measure for Assessing Generalized Anxiety Disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef]
- Gholami, M.; Schwarzer, R. Brief Scales for the Multilingual Assessment of HAPA Variables.
- Caudroit, J.; Stephan, Y.; Le Scanff, C. Social Cognitive Determinants of Physical Activity among Retired Older Individuals: An Application of the Health Action Process Approach. Br. J. Health Psychol. 2011, 16, 404–417. [Google Scholar] [CrossRef] [PubMed]
- Chiu, C.-Y.; Lynch, R.T.; Chan, F.; Berven, N.L. The Health Action Process Approach as a Motivational Model for Physical Activity Self-Management for People with Multiple Sclerosis: A Path Analysis. Rehabil. Psychol. 2011, 56, 171–181. [Google Scholar] [CrossRef]
- Tabachnick, B.G.; Fidell, L.S. Using Multivariate Statistics; Always learning; Seventh edition.; Pearson: New York, NY, 2019; ISBN 978-0-13-479054-1.
- Hoyle, R.H.; Gottfredson, N.C. Structural Equation Modeling with Latent Variables. In APA handbook of research methods in psychology: Research designs: Quantitative, qualitative, neuropsychological, and biological, Vol. 2, 2nd ed; APA Handbooks in Psychology®; American Psychological Association: Washington, DC, US, 2023; pp. 459–490. ISBN 978-1-4338-4133-0. [Google Scholar]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W. The Patient Health Questionnaire-2: Validity of a Two-Item Depression Screener. Med. Care 2003, 41, 1284–1292. [Google Scholar] [CrossRef] [PubMed]
- Löwe, B.; Kroenke, K.; Gräfe, K. Detecting and Monitoring Depression with a Two-Item Questionnaire (PHQ-2). J. Psychosom. Res. 2005, 58, 163–171. [Google Scholar] [CrossRef] [PubMed]
- Löwe, B.; Wahl, I.; Rose, M.; Spitzer, C.; Glaesmer, H.; Wingenfeld, K.; Schneider, A.; Brähler, E. A 4-Item Measure of Depression and Anxiety: Validation and Standardization of the Patient Health Questionnaire-4 (PHQ-4) in the General Population. J. Affect. Disord. 2010, 122, 86–95. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W.; Monahan, P.O.; Löwe, B. Anxiety Disorders in Primary Care: Prevalence, Impairment, Comorbidity, and Detection. Ann. Intern. Med. 2007, 146, 317–325. [Google Scholar] [CrossRef] [PubMed]
- Barrett, P. Structural Equation Modelling: Adjudging Model Fit. Personal. Individ. Differ. 2007, 42, 815–824. [Google Scholar] [CrossRef]
- Hu, L.; Bentler, P.M. Cutoff Criteria for Fit Indexes in Covariance Structure Analysis: Conventional Criteria versus New Alternatives. Struct. Equ. Model. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Yuan, K.-H.; Bentler, P.M. On Chi-Square Difference and z Tests in Mean and Covariance Structure Analysis When the Base Model Is Misspecified. Educ. Psychol. Meas. 2004, 64, 737–757. [Google Scholar] [CrossRef]
- Browne, M.W.; Cudeck, R. Alternative Ways of Assessing Model Fit. Sociol. Methods Res. 1992, 21, 230–258. [Google Scholar] [CrossRef]
- Reyes Fernández, B.; Knoll, N.; Hamilton, K.; Schwarzer, R. Social-Cognitive Antecedents of Hand Washing: Action Control Bridges the Planning-Behaviour Gap. Psychol. Health 2016, 31, 993–1004. [Google Scholar] [CrossRef] [PubMed]
- Shi, D.; Maydeu-Olivares, A.; Rosseel, Y. Assessing Fit in Ordinal Factor Analysis Models: SRMR vs. RMSEA. Struct. Equ. Model. Multidiscip. J. 2020, 27, 1–15. [Google Scholar] [CrossRef]
- Kenny, D.A.; Kaniskan, B.; McCoach, D.B. The Performance of RMSEA in Models with Small Degrees of Freedom. Sociol. Methods Res. 2015, 44, 486–507. [Google Scholar] [CrossRef]
- von Lengerke, T.; Ebadi, E.; Schock, B.; Krauth, C.; Lange, K.; Stahmeyer, J.T.; Chaberny, I.F. Impact of Psychologically Tailored Hand Hygiene Interventions on Nosocomial Infections with Multidrug-Resistant Organisms: Results of the Cluster-Randomized Controlled Trial PSYGIENE. Antimicrob. Resist. Infect. Control 2019, 8, 56. [Google Scholar] [CrossRef] [PubMed]
- Schwarzer, R.; Schuz, B.; Ziegelmann, J.P.; Lippke, S.; Luszczynska, A.; Scholz, U. Adoption and Maintenance of Four Health Behaviors: Theory-Guided Longitudinal Studies on Dental Flossing, Seat Belt Use, Dietary Behavior, and Physical Activity. Ann. Behav. Med. Publ. Soc. Behav. Med. 2007, 33, 156–166. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.-Q.; Zhang, R.; Schwarzer, R.; Hagger, M.S. A Meta-Analysis of the Health Action Process Approach. Health Psychol. Off. J. Div. Health Psychol. Am. Psychol. Assoc. 2019, 38, 623–637. [Google Scholar] [CrossRef] [PubMed]
- Dahmen, A.; Keller, F.; Kötting, L.; Derksen, C.; Lippke, S. Angst Vor Dem Coronavirus, Absicht Zum Befolgen Der AHA-Regeln Und Risikowahrnehmung Bezüglich Arztbesuchen: Querschnittsstudie Mit Psychisch Vorerkrankten Menschen. Gesundheitswesen Bundesverb. Arzte Offentlichen Gesundheitsdienstes Ger. 2021, 83, 274–281. [Google Scholar] [CrossRef] [PubMed]
- Lippke, S.; Keller, F.M.; Derksen, C.; Kötting, L.; Dahmen, A. Hygiene Behaviors and SARS-CoV-2-Preventive Behaviors in the Face of the COVID-19 Pandemic: Self-Reported Compliance and Associations with Fear, SARS-CoV-2 Risk, and Mental Health in a General Population vs. a Psychosomatic Patients Sample in Germany. Hygiene 2022, 2, 28–43. [Google Scholar] [CrossRef]
- Guzek, D.; Skolmowska, D.; Głąbska, D. Analysis of Gender-Dependent Personal Protective Behaviors in a National Sample: Polish Adolescents’ COVID-19 Experience (PLACE-19) Study. Int. J. Environ. Res. Public. Health 2020, 17, 5770. [Google Scholar] [CrossRef]
- Hobbs, M.A.; Robinson, S.; Neyens, D.M.; Steed, C. Visitor Characteristics and Alcohol-Based Hand Sanitizer Dispenser Locations at the Hospital Entrance: Effect on Visitor Use Rates. Am. J. Infect. Control 2016, 44, 258–262. [Google Scholar] [CrossRef]
- Gaube, S.; Tsivrikos, D.; Dollinger, D.; Lermer, E. How a Smiley Protects Health: A Pilot Intervention to Improve Hand Hygiene in Hospitals by Activating Injunctive Norms through Emoticons. PLOS ONE 2018, 13, e0197465. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Structural equation modeling of the full Health Action Process Approach. Note. HAPA variables: ASE=Action Self-Efficacy; OE=Outcome Expectancies, RISK=Risk Perception; INT=Intentions; MSE=Maintenance Self-Efficacy; PL=Planning, RES=Resources, SUP=Social Support, HYG=Hand Hygiene Decisions; N=279; Intention R²=39.5%; Planning R²=19.8%; Hand Hygiene R²=21.6%. The values reported represent the standardized estimates of each path in the model. Significant path at ***p<.001, **p<.01, *p<.05.
Figure 1.
Structural equation modeling of the full Health Action Process Approach. Note. HAPA variables: ASE=Action Self-Efficacy; OE=Outcome Expectancies, RISK=Risk Perception; INT=Intentions; MSE=Maintenance Self-Efficacy; PL=Planning, RES=Resources, SUP=Social Support, HYG=Hand Hygiene Decisions; N=279; Intention R²=39.5%; Planning R²=19.8%; Hand Hygiene R²=21.6%. The values reported represent the standardized estimates of each path in the model. Significant path at ***p<.001, **p<.01, *p<.05.
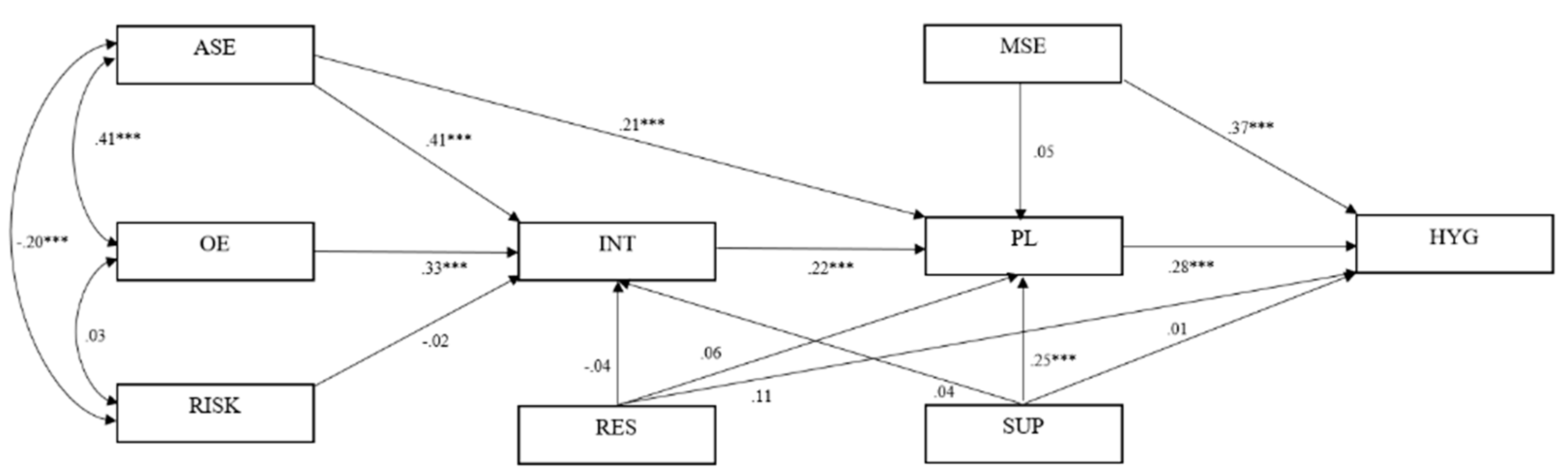
Figure 2.
Structural equation modeling of the trimmed Health Action Process Approach. Note. HAPA variables: ASE=Action Self-Efficacy; OE=Outcome Expectancies, RISK=Risk Perception; INT=Intentions; MSE=Maintenance Self-Efficacy; PL=Planning; HYG=Hand Hygiene Behavior; N=279; Intention R²=39.3%; Planning R²=23.5%; Hand Hygiene R²=33.2%. The values reported represent the standardized estimates of each path in the model. Age, gender, depressive symptoms, and symptoms of generalized anxiety were included as covariates. Significant path at ***p<.001, **p<.01, *p<.05. .
Figure 2.
Structural equation modeling of the trimmed Health Action Process Approach. Note. HAPA variables: ASE=Action Self-Efficacy; OE=Outcome Expectancies, RISK=Risk Perception; INT=Intentions; MSE=Maintenance Self-Efficacy; PL=Planning; HYG=Hand Hygiene Behavior; N=279; Intention R²=39.3%; Planning R²=23.5%; Hand Hygiene R²=33.2%. The values reported represent the standardized estimates of each path in the model. Age, gender, depressive symptoms, and symptoms of generalized anxiety were included as covariates. Significant path at ***p<.001, **p<.01, *p<.05. .
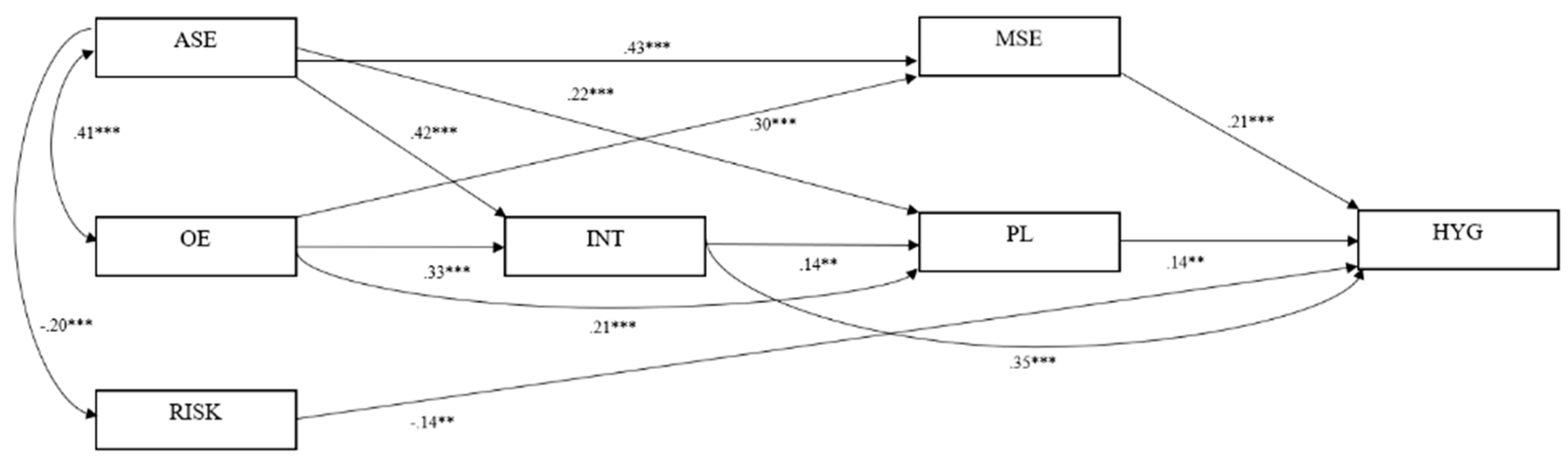

Table 1.
Correlations between Health Action Process Approach (HAPA) constructs, hand hygiene decisions, and mental health status of N=279 participants.
Table 1.
Correlations between Health Action Process Approach (HAPA) constructs, hand hygiene decisions, and mental health status of N=279 participants.
| α | M | SD | ASE | OE | RISK | INT | MSE | PL | RES | SUP | HYG | DEP | ANX | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ASE | .87 | 19.13 | 4.28 | - | ||||||||||
| OE | .83 | 24.61 | 3.83 | .41** | - | |||||||||
| RISK | -1 | 3.16 | 1.33 | -.20** | .03 | - | ||||||||
| INT | .68 | 10.04 | 1.87 | .55** | .50** | -.08 | - | |||||||
| MSE | .91 | 19.58 | 3.99 | .56** | .48** | -.08 | .55** | - | ||||||
| PL | .86 | 12.43 | 5.34 | .40** | .38** | -.14** | .40** | .28* | - | |||||
| RES | .81 | 20.28 | 5.03 | .27** | .34** | .03 | .21** | .26** | .16** | - | ||||
| SUP | .92 | 5.82 | 3.15 | .27** | .30** | .05 | .24* | .06 | .33** | .44** | - | |||
| HYG | .87 | 48.12 | 7.98 | .39** | .32** | -.20** | .52** | .44** | .36** | .22** | .12* | - | ||
| DEP | .86 | 5.89 | 4.75 | -.08 | -.03 | -.04 | .01 | -.03 | .01 | -.12 | -.07 | -.07 | - | |
| ANX | .85 | 4.70 | 3.82 | -.08 | -.03 | -.08 | .03 | -.10 | .01 | -.05 | -.10 | -.01 | -.48** | - |
Note. HAPA variables: ASE=Action Self-Efficacy, OE=Outcome Expectancies, RISK=Risk Perception (single-item), INT=Intentions, MSE=Maintenance Self-Efficacy, PL=Planning, RES=Resources, SUP=Social Support, HYG=Hand Hygiene Decisions, DEP=Depression, ANX=Anxiety; α=Cronbach’s alpha, *p<.05, **p<.01, M=Mean, SD=Standard deviation; 1Risk perception was examined via a single item. Therefore, no Cronbach’s alpha can be provided. N=279.
Table 2.
Model fit indices for the unrestricted model, the semi-restricted model, and the fully restricted model for the multi-group mental health status model for individuals below and above the symptom threshold for depression (N=279).
Table 2.
Model fit indices for the unrestricted model, the semi-restricted model, and the fully restricted model for the multi-group mental health status model for individuals below and above the symptom threshold for depression (N=279).
| Indices | Unrestricted model | Semi-restricted model | Fully restricted mode |
|---|---|---|---|
| χ2– Test of model fit | 40.49 | 51.77 | 63.15 |
| df | 16 | 12 | 27 |
| χ2 | p<.01 | p<.01 | p<.05 |
| CFI | .94 | .94 | .95 |
| TLI | .85 | .92 | .95 |
| Model 1 Delta TLI | - | -.07 | -.09 |
| RMSEA (90% CI) | .08 | .06 | .04 |
Note. df=degrees of freedom, χ²=Chi square, CFI=comparative fit index, TLI=Tucker-Lewis Index, RMSEA=root mean squared error of approximation.
Table 3.
Model fit indices for the unrestricted model, the semi-restricted model, and the fully restricted model for the multi-group model of individuals below and above the symptom threshold for generalized anxiety (N=279).
Table 3.
Model fit indices for the unrestricted model, the semi-restricted model, and the fully restricted model for the multi-group model of individuals below and above the symptom threshold for generalized anxiety (N=279).
| Indices | Unrestricted model | Semi-restricted model | Fully restricted model |
|---|---|---|---|
| χ2 – Test of model fit | 29.75 | 40.63 | 63.80 |
| df | 16 | 12 | 27 |
| χ2 | p=.020 | p=.062 | p=.013 |
| CFI | .97 | .97 | .97 |
| TLI | .92 | .95 | .95 |
| Model 1 Delta TLI | - | -.03 | -.03 |
| RMSEA (90% CI) | .06 | .04 | .04 |
Note. df=degrees of freedom, χ²=Chi square, CFI=comparative fit index, TLI=Tucker-Lewis Index, RMSEA=root mean squared error of approximation.
Table 4.
Latent Mean Analysis: Mean estimates, standard error, and critical ratio (N=279).
| ASE | OE | RISK | INT | MSE | PL | HYG | |
|---|---|---|---|---|---|---|---|
| With symptoms of depression in comparison to the reference group without depressive symptoms | |||||||
| Mean estimate (ME) | -0.194 | -0.090 | -0.137 | 0.049 | -0.239 | 0.050 | 0.016 |
| Standard error (SE) | 0.163 | 0.126 | 0.238 | 0.154 | 0.150 | 0.282 | 0.018 |
| Critical ratio (CR) | -1.252 | -0.715 | -0.576 | 0.320 | -1.159 | 0.177 | 0.907 |
| p | .233 | .475 | .565 | .749 | .110 | .859 | .365 |
| With symptoms of anxiety in comparison to the reference group without symptoms of anxiety | |||||||
| Mean estimate (ME) | -0.227 | -0.102 | -0.310 | 0.068 | -0.072 | 0.127 | -0.043 |
| Standard error (SE) | 0.212 | 0.136 | 0.242 | 0.176 | 0.168 | 0.294 | 0.029 |
| Critical ratio (CR) | -1.073 | -0.752 | -1.280 | 0.384 | -0.429 | 0.433 | -1.466 |
| p | .283 | .452 | .201 | .701 | .668 | .665 | .143 |
Note. HAPA variables: ASE=Action Self-Efficacy; OE=Outcome Expectancies, RISK=Risk Perception; INT=Intentions; MSE=Maintenance Self-Efficacy; PL=Planning; HYG=Hand Hygiene Behavior.
Table 5.
HAPA stage distributions and changes of the longitudinal sample (N=1,058).
| Time 2 (after rehabilitation) | ||||
|---|---|---|---|---|
| Non-compliance | Compliance | Total | ||
| Time 1 | Non-compliance | 25 (45.46) | 30 (54.54) | 55 (100) |
| Compliance | 47 (4.69) | 956 (95.31) | 1003 (100) | |
Note. Numbers in parentheses represent percentages of N=1058.
Table 6.
Summary of results from the binary logistic regression analysis and descriptive data for mental health variables and control variables predicting changes in compliance in hand hygiene decisions (n=71).
Table 6.
Summary of results from the binary logistic regression analysis and descriptive data for mental health variables and control variables predicting changes in compliance in hand hygiene decisions (n=71).
| Predictors | Wald | OR | 95% CIOR | p -Value | Remaining in baseline compliance | Change in compliance | ||
|---|---|---|---|---|---|---|---|---|
| M | SD | M | SD | |||||
| Change in compliance: remaining non-compliant (0) versus progression (1) | ||||||||
| Depression | 1.03 | 1.36 | 0.75-2.48 | .31 | 2.79 | 1.14 | 3.27 | 1.89 |
| Anxiety | 0.32 | 0.84 | 0.45-1.57 | .58 | 2.84 | 1.25 | 3.10 | 1.69 |
| Change in compliance: remaining compliant (0) versus regression (1) | ||||||||
| Depression | 1.14 | 1.15 | 0.89-1.48 | .29 | 3.45 | 1.66 | 3.83 | 1.61 |
| Anxiety | 0.05 | 0.97 | 0.75-1.26 | .84 | 3.61 | 1.67 | 3.82 | 1.35 |
Note. CI OR=95% confidence interval of the OR.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



