
Submitted:
06 November 2023
Posted:
07 November 2023
You are already at the latest version
Abstract
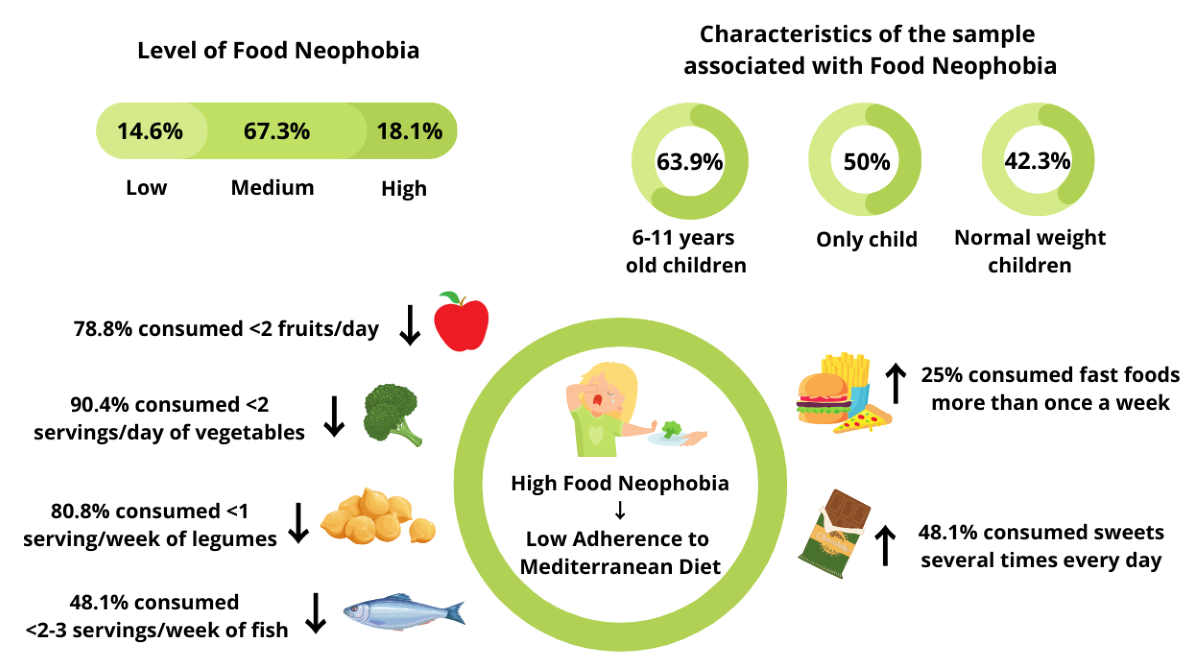
Food Neophobia (FN), defined as the reluctance to eat new or unfamiliar foods, mainly concerns fruit, vegetables, and legumes, typical of the Mediterranean Diet (MD). Considering these premises, this study aimed to clarify the relationship between FN and AMD in a sample of Italian children and their association with some socio-demographic factors and children's nutritional status. A sample of 288 children aged 3-11 years, participated to an assessment carried out with a questionnaire evaluating FN and AMD, respectively with Child Food Neophobia Scale (CFNS) and the KIDMED Test. Most of the sample showed an intermediate (67.3%) or high level of FN (18.1%) with high rates among 6-11 years old children (63.9%) and especially in only-child (50%). The AMD was mostly low (29.5%) or medium (54.8%) and reached lower levels among higher neophobic children (51.9%; p value < 0.05). Present results confirm the study hypothesis that FN is a driver of MD abandonment and show the positive effects on children's eating habits of having siblings. Finally, this study proves the relevance of adopting effective feeding strategies against FN to avoid its maintenance in adulthood and detrimental effects on future overall health and well-being.
Keywords:
Food Neophobia
; Adherence to Mediterranean Diet
; Sociodemographic Characteristics
; Children
; Italy
1. Introduction
Food preferences in children are linked to the exposure to high food diversity in the early years which improves dietary variety at the later developmental stages [1]. The reluctance to eat new or unknown foods is defined as Food Neophobia (FN) [2]. It is a normal developmental phase, occurring without distinction of gender, that typically peaks between 2 and 6 years of age and then gradually decreases into adulthood [2,3]. However, FN could have pervasive implications for food-related behaviors impacting the sensory perception of food in the sense that people having high levels of FN reported limited enjoyment of food [4].
Typical foods of the Mediterranean Diet (MD), such as fruit, vegetables, whole grains, and legumes are related to children's FN [1]. MD is negatively associated with the risk of non-communicable chronic diseases, such as diabetes, cardiovascular diseases, and all causes of mortality [5,6,7,8,9] when compared with Western Diet [10]. Hence, the nonadherence to MD in developmental ages was a behavior that needed to be corrected. Eating habits and behaviors are shaped in childhood and then maintained in adulthood [11] hence it is important to act early on neophobic behavior to ensure that it does not impact diet quality [12].
Over the last years in the Mediterranean Countries, a progressive abandoning of MD was observed either in children or adults [13]. Among children in Italy, several reports showed inadequate consumption of typical foods of MD such as fruit, vegetables, and legumes [14].
Among neophobic children it is common to find high consumption of foods rich in saturated fatty acids and sugars [15,16], typical of a Western-style diet [10]. Poor dietary variety and quality due to FN could be a predictor of childhood overweight/obesity, however to date, findings are not univocal [17,18,19,20].
FN is primarily a hereditary trait, in which the genetic determinants accounted for 78% [21]; however, several socio-environmental factors can influence its development [22,23]. Parent’s eating patterns and feeding strategies adopted are strongly associated with the development of FN in children [12,24]. During family mealtimes, due to the social facilitation mechanism [25], children can observe and acquire the eating habits of their parents and peers (e.g., siblings) [26,27,28].
Parents’ low consumption of fruit and vegetables is strongly associated with limited consumption of these foods by children [29] because of the transposition of parents’ food preferences on children. Consequences of this attitude could be the children’s restricted experience of learning about various types of food as well as a poor variety of dietary preferences [2,22,30]. Consistently, several studies demonstrated that the mother’s high level of neophobia is correlated with the highest neophobia in children [20,31,32]. Low parents’ educational level could be one of the causes of low Adherence to the Mediterranean Diet (AMD) and the high level of neophobia in children [33,34,35,36]. Moreover, parents’ insufficient nutritional knowledge about what foods are healthy for their children and how to offer them [15] could exacerbate either neophobia or low adherence to MD.
To the best of our knowledge, few studies have evaluated the relationship between FN and AMD in the pediatric population, mostly conducted in Spain [1,37]. For these reasons, the present study aimed to clarify the correlation between FN and AMD in children in an Italian sample. Specific purposes of the work were the analysis of the socio-demographic factors influencing AMD and FN as well as the relationship of AMD and FN with children's nutritional status.
The hypothesis basis of this work was that a high level of FN would correspond to worse adherence to MD. Consequently, the research questions this study would like to answer are: (i) FN could be a driver of AMD?; (ii) what children's behavior, in line or non-in line with MD, could be identified as most related to FN?; iii) what aspects characterizing the family would influence children’s neophobia?
2. Materials and Methods
2.1. Study Design
The present assessment is a cross-sectional study carried out on a sample of children aged 3–11 years, in the period between March 9 and May 11, 2022. The only inclusion criterion was the class of age.
The sample size was calculated according to Pourhoseingholi et al. [38], using the following formula: This is example 1 of an equation:
n = [Z2 ∗ P(1-P)]/[d2]
where n is the sample size, the Z value is 1.96 corresponding to a 95% level of confidence and P denotes the phenomenon to be measured. In this case, P is the prevalence of FN in children, which was estimated at 25% according to Predieri et al. [39], and expressed as a decimal. Finally, d is the precision level of 5%, expressed as a decimal. The resulting sample size was 288 subjects.
Most of the sample (227 subjects) resulted from direct data collection carried out by interviewing randomly selected parents of children attending schools and parks in Rome's fifth municipality and in the surrounding areas. The remaining sample (61 subjects) was obtained through an online administration of the questionnaire distributed through instant messaging apps (e.g., WhatsApp) and the social platforms Instagram and Facebook.
2.2. Data Collection Procedure
Following the European Commission General Data Protection Regulation (679/2016) those willing to participate signed a privacy policy and consent form concerning the collection and processing of socio-demographic data in advance. Before starting the data collection, participants were informed about the objective of the research, the consequent statistical analysis, and the intention to publish the results of the assessment in a scientific journal. Participation in the study was fully voluntary and anonymous and subjects could withdraw from the study at any time for any reason. This study was conducted according to the guidelines of the Declaration of Helsinki [40]. The present research is not considered either as medical experimentation, or a direct intervention on human subjects with diet changes or formulated food administration and did not involve any invasive procedures. In addition to that the Council for Research Economics and Agriculture (CREA) that performed the study is part of the National Statistical System (SISTAN) and guarantees individual data protection [41]. Hence an additional ethical committee review of the study protocol was considered unnecessary once informed consent was obtained.
2.3. The Questionnaire
The questionnaire was developed according to the objective of the study and was completed by an adult who acted as a caregiver of the assessed child. It consisted of three sections reported in the Supplementary Material (Table S1). The first section included questions on sociodemographic characteristics (gender, age, weight, and height of the child, ethnic group of the family, household income, number of workers in the family, and number of children in the family). Weight status identification was based on Body Mass Index (BMI) comparison with growth charts of the WHO and their cut-offs [42,43].
The second section investigated FN behavior in children with the Child Food Neophobia Scale (CFNS) developed by Pliner [44] and validated in Italy by Laureati et al. [45]. The CFNS consists of 10 items (five referring to neophiliac and five to neophobic attitude) evaluated with a 7-point scale ranging from 1 = “I strongly disagree” to 7 = “I strongly agree.”
The individual CFNS scores were computed according to Predieri et al. [39] as the sum of the scores of the 10 items, reversing the neophiliac items to have a univocal sense of all the responses. Therefore, the scores theoretically ranged from 10 to 70 with higher scores reflecting higher FN levels. Three groups of individuals were identified according to the following calculation: neutrals (score in the interval mean ± 1 SD), neophobic (score > mean + 1 SD), and neophiliac (score < mean – 1 SD) [16,46,47].
The third section of the questionnaire assessed the AMD in children with the “Mediterranean diet and quality index in children and adolescents KIDMED Test” [48], a questionnaire specifically developed to evaluate if children’s eating habits are based on principles of MD pattern. The test consists of 16 questions with closed answers (yes or no). The 14 questions denoting attitude in line with the MD principle were assigned a value of +1 (e.g., Uses olive oil at home); the 4 questions corresponding to attitude not in line with the MD principle were scored -1 (e.g., Skip breakfast). The KIDMED score ranges from 0 to 12, and the sums of the values from the administered test are classified into three levels of AMD: ≥8 indicates “optimal” AMD; 4-7 points indicates “average” AMD (improvement needed); ≤3 points indicate “very low” AMD.
2.4. Statical Analysis
Descriptive statistics of the data collected were produced. Single continuous and categorical variables were summarized as mean ± standard deviation and percentage (%). A contingency analysis was performed to check associations between variables. Specifically, double-entry tables were processed, and the Chi-square test of independence was applied, along with post-hoc tests to check pairwise comparisons, with Bonferroni corrections of the p-values. The test of independence on the mean was applied to compare continuous variables with categorical variables. Results were considered significant for p-value < 0.05. Statistical analysis was performed using Microsoft® Excel software.
3. Results
3.1. Characteristics of the Sample
Table 1 shows the sociodemographic characteristics of the sample. Females accounted for 42.7% and males 57.3%; a large part of the sample was Caucasians (79.8%) even a certain level of multi-ethnic origin was observed (12.9% Eurasians, 4.5% Africans, 1.4% Hispanics, and 1.4% Asiatic). The average age of the assessed children was 7.4 years (SD = 2.6) with most of them (71.2%) aged 6-11 years. Consistently, 65.6% of the sample attended primary school. In most cases, both parents were employed (87.8%). Consistently, household income for most families ranged between 25.000-40.000 euros (35.8%) and 10.000-25.000 euros (31.6%).
3.2. The Adherence to Mediterranean Diet Assessment (KIDMED Test)
The average overall AMD score was 4.9 (SD = 2.4). According to KIDMED scores categorization, 29.5% of respondents had low AMD, 54.8% showed average AMD and only 15.6% resulted in a high AMD (Figure 1). Inadequate consumption of fruit (<2 servings/day: 61.8%), vegetables (<2 servings/day: 73.3%), legumes (<1 serving/week: 53.8%), nuts (<2/3 servings/week: 74.7%), fish (<2/3 servings/week: 34.7%) was observed, on the other hand excessive consumption of sweets (>1 serving/day: 39.9%) and fast foods (>1 time/week: 18.8%) was reported. Among the habits in line with MD, it should be reported the occurrence of breakfast (88.2%), mainly with dairy products (91.7%) and commercially baked goods and pastries (81.6%). The consumption of cereals or grain (e.g., bread) for breakfast was less common (18.8%) (Supplementary Materials (Table S2)).
In males, AMD is more common than in females (65.2% vs 34.8% p-value <0.05). The occurrence of having both parents employed was associated with AMD in children (93% vs 7% p-value <0.05), while for the other sociodemographic characteristics, no significant association with AMD was found (age: dependency ratio on average 0.004; household income: p-value 0.5; ethnic group: p-value 0.2). Weight status was not significantly associated with AMD; however, higher levels of AMD were found in normal-weight children (42.2%) than in overweight (24.4%) or obese (24.4%) individuals (Table 2).
3.3. Food Neophobia Assessment
The average CFNS score was 42.2 (SD = 14.04) resulting in a large majority of the sample with an intermediate level of FN (67.3%) followed by a high (18.1%) and low (14.6%) level (Figure 2).
Having siblings influences the occurrence of FN in the sense that among neophiliac children a lower proportion of only-child was found with respect to the neophobic counterparts (16.7% vs 50%; p value <0.05). FN did not show significant associations with socio-demographic variables (gender: p value 0.7; age: dependency average of ratio 0.01; household income: p value 0.3; parental employment: 0.1; ethnic group: p value 0.6). The relationship between FN and weight status was also studied, resulting in a significant association. Higher rates of normal weight than overweight/obesity were found among respondents with lower levels of neophobia (61.9% vs 38.1%; p value < 0.05). However, even in higher neophobic individuals about half were normal weight (42.3%) (Table 3).
3.4. The Relationship between Adherence to the Mediterranean Diet and Food Neophobia
To test the study hypothesis that a high level of FN could be a driver of poor AMD, the association between these variables was assessed and significant results were observed (p-value <0.05). Specifically, almost half of children with a high level of FN (51.9%) showed poor AMD (Table 4).
To assess the intake of different food groups in both neophobic and neophiliac children, the association between FN and the items of the KIDMED Test was carried out. In lower neophobic children, adequate consumption of fruit (2 servings/day;76.2%), vegetables (2 servings/day;66.7%), and legumes (>1 serving/week; 92.9%) was found (p-value < 0.05). Otherwise, in higher neophobic respondents an insufficient consumption of fish (<2-3 servings/week; 48.1%; p-value <0.05) was observed. On the other hand, neophiliac children were less frequent consumers (< once a week) of fast foods than neophobic respondents (97.6% vs 75%; p value <0.05). Having breakfast did not show a significant association with FN (p-value 0.09), with almost all both neophiliac (95.2%) and neophobic (80.8%) children that did not skip breakfast. Concerning food choices, the consumption of milk (p-value 0.1) and commercially baked goods and pastries (p-value 0.7) was not related to FN, instead of cereals/grains for breakfast was higher in participants with a low level of FN than in those with a high level (31% vs 11.5%; p value 0.05) (Table 4).
Among higher neophobic children, the lowest daily Fruit and Vegetables (F&V) consumption frequencies were observed. In particular, 80.4% of the children with an intermediate level of FN and 65.4% with a high level of FN consumed only one fruit or fruit juice every day. Consumption of two servings per day was reported by 35% of children with intermediate FN and 21.5% of children with high FN. Similarly, 68% of the children with an intermediate level of FN and 46.1% with a high level of FN consumed fresh or cooked vegetables only once a day. These percentages reduced to 22.7% and 9.6% for two servings per day, respectively. A decreasing trend of weekly fish and legumes consumption between the different FN levels was also observed: among higher neophobic children only the 19.2% and 51.9% consumed, respectively, legumes more than once a week and fish at least 2-3 times per week, contrary to 92.9% and 71.4%, respectively for legumes and fish consumption, of neophiliac counterparts that showed an adequate intake (Figure 3).
Cronbach’s Alpha was calculated for the combined 26 items of CFNS and KIDMED resulting in a good (α = 0.80) internal consistency and a good reliability of the scale measured [49].
4. Discussion
The present work clarifies the relationship between FN and AMD in a sample of Italian children and describes the association with some socio-demographic factors and children's nutritional status.
The key finding in the current study highlights that a high level of FN significantly influences the lack of AMD in the assessed sample of Italian children. Notably, more than half of children with elevated FN demonstrated low AMD. The negative correlation between FN and AMD was reported in other studies carried out in the pediatric population [1,37] as well as in the adults [39]. FN in the present study was a significant barrier to a balanced and healthy diet and neophobic children resulted in a diet with lower nutritional quality than non-neophobic children.
FN was largely diffused in the present sample, since more than half of respondents showed an intermediate level of FN (67.3%), followed by a high level (18.1%), confirming rates observed in other Italian studies [19,47,50]. Children exhibiting a high level of FN are hesitant to experiment with a variety of foods, especially those they are unfamiliar with [51]. In the present sample, this results in children with limited eating variety with a dietary behavior far from the principles of MD that could have detrimental effects on future overall health and well-being. Conversely, children who were assessed as less neophobic resulted in general behaviors more in line with MD principles.
Foods commonly refused by neophobic children are fruit, vegetables, legumes, and fish, typical of MD [1]; on the other hand Western Diet characterizing foods such as highly palatable, ultra-processed foods, rich in salt and sugar and refined grains [10], are preferred by neophobic children [15,16]. Consequently, FN could be one of the many factors contributing to the shift toward a Western dietary pattern. Suboptimal children AMD was measured in this study (54.8% average and 29.5% very low), confirming trends of reducing AMD in the evolutive ages in Mediterranean areas as resulting in the meta-analysis conducted by Garcia-Cabrera et al. [13] (27% of low AMD among youths ≤12 years old).
The observed levels of AMD were related to two socio-demographic variables, namely gender and level of parental employment. Contrary to other studies [13,36], in this sample males followed more MD than females. Instead, a higher parental level of employment resulted in a negative factor for AMD as it was associated with higher rates of neophobia in children (93% vs 80%).
A more detailed examination of the data showed that a large proportion of the respondents did not achieve the recommendations for the consumption of fruit (61.8%), vegetables (73.3%), cereals or grain for breakfast (81.2%), legumes (53.8%) and fish (34.7%) and these included mainly children with an intermediate or high level of FN. Furthermore, F&V, legumes and fish consumption frequencies tended to decrease as the level of FN worsened. Overall, FN would seem to influence vegetable consumption more negatively than fruits. The sweet taste of fruit compared to the bitter taste of some vegetables could justify the difference found in this finding. However, the difference between fruit and vegetable consumption could be minor considering that the KIDMED item on fruit consumption also refers to fruit juices, normally preferred by children [52].
Regarding more palatable foods, the consumption of commercially baked goods and pastries for breakfast (81.6%), sweets (39.9%), and fast foods (18.8%), was frequent, especially among children with an intermediate or high level of FN. These findings are consistent with those obtained in studies conducted in other Mediterranean Countries that recognize FN as a driver in the abandonment of the MD [1,37]. On the other hand, also unhealthy home food environment and low parent AMD could be a predictor of maintenance of FN in children.
An interesting result that deserves attention is related to the fact that having siblings influences the occurrence of FN with a lower percentage of only children among neophiliac children compared to their neophobic counterparts (16.7% vs 50%) probably due to the influence of peers on children's eating habits [37,53].
The literature describes a peak of FN between 2 and 6 years of age with a decrease over [2,3]; in the present study, however, a high prevalence of FN was found in 6-11 years old children (63.9% of them with an intermediate level of FN). These results indicate the persistence of neophobic behavior during the child's growth and the possibility of its maintenance in adulthood. Adoption of coercive feeding strategies (e.g., pressure to eat, using food as a reward) could be one of the causes of FN persistence [23,24,54,55,56] considering that forcing attitude could have an immediate positive impact but a long-term negative effect on the development of preferences for healthy foods [57,58]. The prevalence of FN in adulthood in Italy has been confirmed by another study [39] that showed a strong negative association between FN and AMD and suggested that it could be a predictor of unhealthy dietary pattern adoption and greater metabolic risk. It is widely documented that FN limits the dietary variety and quality as it results in the rejection of healthy foods, both plant (e.g., fruit, vegetables, pulses) and animal (e.g., fish), and the preference for more palatable and high-calorie foods [15]. Considering these premises, it has been hypothesized that FN may contribute to childhood obesity [17].
Present results did not confirm the association between FN and childhood obesity. In fact, among the less neophobic children, a significantly higher percentage of normal weight was observed compared to overweight/obesity (61.9% vs 38.1%). However, even in higher neophobic respondents about half were normal weight (42.3%). The relationship between FN and weight status is an open question as it has been examined in a few studies that have produced conflicting results. Most of these found no association between the variables [18,19,59,60,61], while a smaller number found a positive relationship in the sense that neophobic children tend to be more overweight/obese [20,32]. Further research is needed to clarify this association, but we can speculate that it depends on the home food environment and the feeding practices adopted by parents: the abundance of calory-dense foods, rich in sugars or saturated fatty acids, and offering them to compensate for the rejection of healthy ones, could favor the development of overweight/obesity in neophobic children.
The strengths and limitations of the study can be mentioned. An important strength of this study is the fact that it addresses a research gap in Italy in which limited comprehensive assessments simultaneously investigate both FN and children's AMD. Understanding the interplay between FN and AMD is essential for promoting healthy eating habits among Italian children. Research in this area could reveal strategies to encourage a more balanced and nutritious diet in children, potentially reducing the impact of FN on their food choices. Another strength is the use of validated and largely employed questionnaires, the KIDMED test [48] and Neophobia scale [44], that have been designed to yield consistent and reproducible results. This allowed to place the findings in a broader context and make meaningful comparisons to existing research, enhancing the study's significance. Another strength of this work was that the sample size calculation fixed the level of precision of estimations ensuring the detection of meaningful effects and differences optimizing efforts and resources considering the difficulties of data collection in studies having children as the target group. This led to more robust statistical tests and analyses, increasing the study's ability to detect significant effects and relationships minimizing the risk of unnecessarily involving participants and collecting data that may not contribute significantly to the study's objectives.
This study has limitations. A significant weakness of this research lies in its cross-sectional examination of FN’s association with AMD, as well as the consumption of specific foods like fruits, vegetables, and weight outcomes. Consequently, the study design did not permit to establish a causal relationship. Nonetheless, the findings offer valuable groundwork for future investigations, which should explore causal connections between neophobia and diet quality during later stages of childhood. Another important limitation of the study is related to the fact that the assessment relied on respondent’s answers to the questionnaire. This methodology has the intrinsic limitation of the response bias consisting of the fact that respondents may provide inaccurate or socially desirable responses. Dietary intake evaluation is particularly influenced by social desirability bias with a tendency to provide consistent responses, which can potentially lead to less precise representations of actual food consumption [18]. In addition, the study relied on adults' assessments of neophobic behaviors that could be interpreted differently. All these aspects were partially overcome with the use of largely validated questionnaires. Another limitation of the study is related to the fact that the sample includes medium and high socioeconomic groups limiting the generalizability of results to the broader population that however was not an objective of the present study.
5. Conclusions
This study confirms the widespread prevalence of FN in pediatric age in Italy, especially in only child. Contrary to several studies describing a peak of FN between 2 and 6 years of age, present results showed the maintenance of neophobic behavior also in older children. Confirming the study hypothesis, FN is a driver of low AMD, negatively influencing the consumption of typical foods of MD such as fruit, vegetables, legumes, and nuts and contributing to the high intake of sweets and fast foods, characteristic of Western dietary patterns. An inadequate home food environment, unhealthy parents’ eating habits, and the adoption of ineffective feeding strategies could cause the maintenance of FN observed, predisposing to the occurrence of NCDs in adulthood. FN is a significant barrier to achieving a balanced and healthy diet, particularly among children. Neophobic children are at risk of consuming a diet with lower nutritional quality, which can impact their health and development. Encouraging neophobic individuals, especially children, to gradually expand their food choices can be a crucial step in promoting better dietary habits and overall well-being [62].
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Table S1: The Questionnaire; Table S2: Results of the KIDMED Test.
Author Contributions
S.P., U.S. and L.R. carried out the research questions, conceptualization, and design of the study. L.R. revised the methodology. A.D.N. and S.P. carried out the database compilation and data analysis. A.D.N. carried out the manuscript writing and original draft preparation. L.R. and US did the writing, review, and editing. All authors have read and agreed to the published version of the manuscript.
Funding
This paper did not receive any public funding or sponsorship.
Institutional Review Board Statement
The investigation was carried out following the rules of the 1975 Declaration of Helsinki (https://www.wma.net/what-we-do/medical-ethics/declaration-of-helsinki/, accessed on 29 September 2023), revised in 2013. Ethical review and approval were waived for this study because it did not involve any invasive procedure (e.g., fecal samples, voided urine, etc.), or laboratory assessment, or induced lifestyle changes, or dietary intake modifications.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The archived data and all the elaboration and analysis generated and used for the presentation of results in this study are fully available on request from the corresponding author.
Acknowledgments
Authors thank all the participants in the study that provided time for interviews. With their collaborative attitude, the respondents supported the fieldwork and contributed to the provision of high-quality results.
Conflicts of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
- Rodríguez-Tadeo, A.; Patiño-Villena, B.; González-Martínez-La-Cuesta, E.; Urquídez-Romero, R.; Ros-Berruezo, G. Food Neophobia, Mediterranean Diet Adherence and Acceptance of Healthy Foods Prepared in Gastronomic Workshops by Spanish Students. Nutrición Hospitalaria 2018, 35, 642–649. [CrossRef]
- Dovey, T.M.; Staples, P.A.; Gibson, E.L.; Halford, J.C.G. Food Neophobia and ‘Picky/Fussy’ Eating in Children: A Review. Appetite 2008, 50, 181–193. [CrossRef]
- Cole, N.C.; An, R.; Lee, S.-Y.; Donovan, S.M. Correlates of Picky Eating and Food Neophobia in Young Children: A Systematic Review and Meta-Analysis. Nutr Rev 2017, 75, 516–532. [CrossRef]
- Jaeger, S.R.; Prescott, J.; Worch, T. Food Neophobia Modulates Importance of Food Choice Motives: Replication, Extension, and Behavioural Validation. Food Quality and Preference 2022, 97, 104439. [CrossRef]
- Agnoli, C.; Krogh, V.; Grioni, S.; Sieri, S.; Palli, D.; Masala, G.; Sacerdote, C.; Vineis, P.; Tumino, R.; Frasca, G.; et al. A Priori-Defined Dietary Patterns Are Associated with Reduced Risk of Stroke in a Large Italian Cohort. J Nutr 2011, 141, 1552–1558. [CrossRef]
- Grosso, G.; Mistretta, A.; Frigiola, A.; Gruttadauria, S.; Biondi, A.; Basile, F.; Vitaglione, P.; D’Orazio, N.; Galvano, F. Mediterranean Diet and Cardiovascular Risk Factors: A Systematic Review. Critical Reviews in Food Science and Nutrition 2014, 54, 593–610. [CrossRef]
- Sofi, F.; Abbate, R.; Gensini, G.F.; Casini, A. Accruing Evidence on Benefits of Adherence to the Mediterranean Diet on Health: An Updated Systematic Review and Meta-Analysis12. The American Journal of Clinical Nutrition 2010, 92, 1189–1196. [CrossRef]
- Trichopoulou, A.; Martínez-González, M.A.; Tong, T.Y.; Forouhi, N.G.; Khandelwal, S.; Prabhakaran, D.; Mozaffarian, D.; de Lorgeril, M. Definitions and Potential Health Benefits of the Mediterranean Diet: Views from Experts around the World. BMC Med 2014, 12, 112. [CrossRef] [PubMed]
- Eleftheriou, D.; Benetou, V.; Trichopoulou, A.; Vecchia, C.L.; Bamia, C. Mediterranean Diet and Its Components in Relation to All-Cause Mortality: Meta-Analysis. British Journal of Nutrition 2018, 120, 1081–1097. [CrossRef]
- Azzam, A. Is the World Converging to a ‘Western Diet’? Public Health Nutr. 2021, 24, 309–317. [CrossRef]
- Montaño, Z.; Smith, J.D.; Dishion, T.J.; Shaw, D.S.; Wilson, M.N. Longitudinal Relations between Observed Parenting Behaviors and Dietary Quality of Meals from Ages 2 to 5. Appetite 2015, 87, 324–329. [CrossRef]
- Torres, T. de O.; Gomes, D.R.; Mattos, M.P. FACTORS ASSOCIATED WITH FOOD NEOPHOBIA IN CHILDREN: SYSTEMATIC REVIEW. Rev. paul. pediatr. 2021, 39, e2020089. [CrossRef] [PubMed]
- García Cabrera, S.; Herrera Fernández, N.; Rodríguez Hernández, C.; Nissensohn, M.; Román-Viñas, B.; Serra-Majem, L. KIDMED TEST; PREVALENCE OF LOW ADHERENCE TO THE MEDITERRANEAN DIET IN CHILDREN AND YOUNG; A SYSTEMATIC REVIEW. Nutr Hosp 2015, 32, 2390–2399. [CrossRef]
- EpiCentro Indagine nazionale 2019: i dati nazionali Available online: https://www.epicentro.iss.it/okkioallasalute/indagine-2019-dati (accessed on 29 July 2022).
- Russell, C.G.; Worsley, A. A Population-Based Study of Preschoolers’ Food Neophobia and Its Associations with Food Preferences. Journal of Nutrition Education and Behavior 2008, 40, 11–19. [CrossRef]
- Falciglia, G.A.; Couch, S.C.; Gribble, L.S.; Pabst, S.M.; Frank, R. Food Neophobia in Childhood Affects Dietary Variety. Journal of the American Dietetic Association 2000, 100, 1474–1481. [CrossRef]
- Brown, C.L.; Vander Schaaf, E.B.; Cohen, G.M.; Irby, M.B.; Skelton, J.A. Association of Picky Eating and Food Neophobia with Weight: A Systematic Review. Childhood Obesity 2016, 12, 247–262. [CrossRef]
- Perry, R.A.; Mallan, K.M.; Koo, J.; Mauch, C.E.; Daniels, L.A.; Magarey, A.M. Food Neophobia and Its Association with Diet Quality and Weight in Children Aged 24 Months: A Cross Sectional Study. Int J Behav Nutr Phys Act 2015, 12, 13. [CrossRef]
- Laureati, M.; Bertoli, S.; Bergamaschi, V.; Leone, A.; Lewandowski, L.; Giussani, B.; Battezzati, A.; Pagliarini, E. Food Neophobia and Liking for Fruits and Vegetables Are Not Related to Italian Children’s Overweight. Food Quality and Preference 2015, 40, 125–131. [CrossRef]
- Finistrella, V.; Manco, M.; Ferrara, A.; Rustico, C.; Presaghi, F.; Morino, G. Cross-Sectional Exploration of Maternal Reports of Food Neophobia and Pickiness in Preschooler-Mother Dyads. Journal of the American College of Nutrition 2012, 31, 152–159. [CrossRef]
- Cooke, L.J.; Haworth, C.M.; Wardle, J. Genetic and Environmental Influences on Children’s Food Neophobia. The American Journal of Clinical Nutrition 2007, 86, 428–433. [CrossRef]
- Lafraire, J.; Rioux, C.; Giboreau, A.; Picard, D. Food Rejections in Children: Cognitive and Social/Environmental Factors Involved in Food Neophobia and Picky/Fussy Eating Behavior. Appetite 2016, 96, 347–357. [CrossRef]
- Kutbi, H.A.; Alhatmi, A.A.; Alsulami, M.H.; Alghamdi, S.S.; Albagar, S.M.; Mumena, W.A.; Mosli, R.H. Food Neophobia and Pickiness among Children and Associations with Socioenvironmental and Cognitive Factors. Appetite 2019, 142, 104373. [CrossRef]
- Kaar, J.L.; Shapiro, A.L.B.; Fell, D.M.; Johnson, S.L. Parental Feeding Practices, Food Neophobia, and Child Food Preferences: What Combination of Factors Results in Children Eating a Variety of Foods? Food Quality and Preference 2016, 50, 57–64. [CrossRef]
- Clayton, D.A. Socially Facilitated Behavior. The Quarterly Review of Biology 1978, 53, 373–392. [CrossRef]
- Lumeng, J.C.; Cardinal, T.M.; Jankowski, M.; Kaciroti, N.; Gelman, S.A. Children’s Use of Adult Testimony to Guide Food Selection. Appetite 2008, 51, 302–310. [CrossRef]
- Bandura, A. Self-Efficacy: Toward a Unifying Theory of Behavioral Change. Psychological Review 1977, 84, 191–215. [CrossRef]
- Litterbach, E.V.; Campbell, K.J.; Spence, A.C. Family Meals with Young Children: An Online Study of Family Mealtime Characteristics, among Australian Families with Children Aged Six Months to Six Years. BMC Public Health 2017, 17, 111. [CrossRef]
- Goldman, R.L.; Radnitz, C.L.; McGrath, R.E. The Role of Family Variables in Fruit and Vegetable Consumption in Pre-School Children. J Public Health Res 2012, 1, 143–148. [CrossRef]
- Howard, A.J.; Mallan, K.M.; Byrne, R.; Magarey, A.; Daniels, L.A. Toddlers’ Food Preferences. The Impact of Novel Food Exposure, Maternal Preferences and Food Neophobia. Appetite 2012, 59, 818–825. [CrossRef]
- Kral, T.V.E.; Rauh, E.M. Eating Behaviors of Children in the Context of Their Family Environment. Physiol Behav 2010, 100, 567–573. [CrossRef]
- Faith, M.S.; Heo, M.; Keller, K.L.; Pietrobelli, A. Child Food Neophobia Is Heritable, Associated with Less Compliant Eating, and Moderates Familial Resemblance for BMI. Obesity (Silver Spring) 2013, 21, 1650–1655. [CrossRef]
- Kähkönen, K.; Rönkä, A.; Hujo, M.; Lyytikäinen, A.; Nuutinen, O. Sensory-Based Food Education in Early Childhood Education and Care, Willingness to Choose and Eat Fruit and Vegetables, and the Moderating Role of Maternal Education and Food Neophobia. Public Health Nutr 2018, 21, 2443–2453. [CrossRef]
- Scaglioni, S.; De Cosmi, V.; Ciappolino, V.; Parazzini, F.; Brambilla, P.; Agostoni, C. Factors Influencing Children’s Eating Behaviours. Nutrients 2018, 10, 706. [CrossRef]
- Wen, X.; Kong, K.L.; Eiden, R.D.; Sharma, N.N.; Xie, C. Sociodemographic Differences and Infant Dietary Patterns. Pediatrics 2014, 134, e1387-1398. [CrossRef]
- Iaccarino Idelson, P.; Scalfi, L.; Valerio, G. Adherence to the Mediterranean Diet in Children and Adolescents: A Systematic Review. Nutr Metab Cardiovasc Dis 2017, 27, 283–299. [CrossRef]
- Maiz, E.; Balluerka, N. Nutritional Status and Mediterranean Diet Quality among Spanish Children and Adolescents with Food Neophobia. Food Quality and Preference 2016, 52, 133–142. [CrossRef]
- Pourhoseingholi, M.A.; Vahedi, M.; Rahimzadeh, M. Sample Size Calculation in Medical Studies. Gastroenterol Hepatol Bed Bench 2013, 6, 14–17.
- Predieri, S.; Sinesio, F.; Monteleone, E.; Spinelli, S.; Cianciabella, M.; Daniele, G.M.; Dinnella, C.; Gasperi, F.; Endrizzi, I.; Torri, L.; et al. Gender, Age, Geographical Area, Food Neophobia and Their Relationships with the Adherence to the Mediterranean Diet: New Insights from a Large Population Cross-Sectional Study. Nutrients 2020, 12, 1778. [CrossRef] [PubMed]
- WMA - The World Medical Association-Declaration of Helsinki.
- Sette, S.; Le Donne, C.; Piccinelli, R.; Arcella, D.; Turrini, A.; Leclercq, C. The Third Italian National Food Consumption Survey, INRAN-SCAI 2005–06 – Part 1: Nutrient Intakes in Italy. Nutrition, Metabolism and Cardiovascular Diseases 2011, 21, 922–932. [CrossRef] [PubMed]
- WHO Multicentre Growth Reference Study Group WHO Child Growth Standards Based on Length/Height, Weight and Age. Acta Paediatr Suppl 2006, 450, 76–85. [CrossRef]
- de Onis, M. Development of a WHO Growth Reference for School-Aged Children and Adolescents. Bull World Health Organ 2007, 85, 660–667. [CrossRef] [PubMed]
- Pliner, P. Development of Measures of Food Neophobia in Children. Appetite 1994, 23, 147–163. [CrossRef] [PubMed]
- Laureati, M.; Spinelli, S.; Monteleone, E.; Dinnella, C.; Prescott, J.; Cattaneo, C.; Proserpio, C.; De Toffoli, A.; Gasperi, F.; Endrizzi, I.; et al. Associations between Food Neophobia and Responsiveness to “Warning” Chemosensory Sensations in Food Products in a Large Population Sample. Food Quality and Preference 2018, 68, 113–124. [CrossRef]
- Kozioł-Kozakowska, A.; Piórecka, B.; Schlegel-Zawadzka, M. Prevalence of Food Neophobia in Pre-School Children from Southern Poland and Its Association with Eating Habits, Dietary Intake and Anthropometric Parameters: A Cross-Sectional Study. Public Health Nutr. 2018, 21, 1106–1114. [CrossRef]
- Di Nucci, A.; Scognamiglio, U.; Grant, F.; Rossi, L. The Impact of COVID-19 Pandemic on Food Habits and Neophobia in Children in the Framework of the Family Context and Parents’ Behaviors: A Study in an Italian Central Region. Front Nutr 2022, 9, 1070388. [CrossRef]
- Serra-Majem, L.; Ribas, L.; Ngo, J.; Ortega, R.M.; García, A.; Pérez-Rodrigo, C.; Aranceta, J. Food, Youth and the Mediterranean Diet in Spain. Development of KIDMED, Mediterranean Diet Quality Index in Children and Adolescents. Public Health Nutrition 2004, 7, 931–935. [CrossRef]
- Hinton, P.; McMurray, I.; Brownlow, C. SPSS Explained; Routledge: London, 2004; ISBN 978-0-203-64259-7.
- Laureati, M.; Cattaneo, C.; Bergamaschi, V.; Proserpio, C.; Pagliarini, E. School Children Preferences for Fish Formulations: The Impact of Child and Parental Food Neophobia: L aureati et al . J Sens Stud 2016, 31, 408–415. [CrossRef]
- Białek-Dratwa, A.; Szczepańska, E.; Szymańska, D.; Grajek, M.; Krupa-Kotara, K.; Kowalski, O. Neophobia—A Natural Developmental Stage or Feeding Difficulties for Children? Nutrients 2022, 14, 1521. [CrossRef] [PubMed]
- Heyman, M.B.; Abrams, S.A.; SECTION ON GASTROENTEROLOGY, HEPATOLOGY, AND NUTRITION; COMMITTEE ON NUTRITION Fruit Juice in Infants, Children, and Adolescents: Current Recommendations. Pediatrics 2017, 139, e20170967. [CrossRef]
- Salvy, S.-J.; Kieffer, E.; Epstein, L.H. Effects of Social Context on Overweight and Normal-Weight Children’s Food Selection. Eat Behav 2008, 9, 190–196. [CrossRef]
- Cassells, E.L.; Magarey, A.M.; Daniels, L.A.; Mallan, K.M. The Influence of Maternal Infant Feeding Practices and Beliefs on the Expression of Food Neophobia in Toddlers. Appetite 2014, 82, 36–42. [CrossRef] [PubMed]
- Moding, K.J.; Stifter, C.A. Temperamental Approach/Withdrawal and Food Neophobia in Early Childhood: Concurrent and Longitudinal Associations. Appetite 2016, 107, 654–662. [CrossRef] [PubMed]
- Cooke, L.J.; Chambers, L.C.; Añez, E.V.; Wardle, J. Facilitating or Undermining? The Effect of Reward on Food Acceptance. A Narrative Review. Appetite 2011, 57, 493–497. [CrossRef]
- Bante, H.; Elliott, M.; Harrod, A.; Haire-Joshu, D. The Use of Inappropriate Feeding Practices by Rural Parents and Their Effect on Preschoolers’ Fruit and Vegetable Preferences and Intake. J Nutr Educ Behav 2008, 40, 28–33. [CrossRef] [PubMed]
- Galloway, A.T.; Fiorito, L.M.; Francis, L.A.; Birch, L.L. “Finish Your Soup”: Counterproductive Effects of Pressuring Children to Eat on Intake and Affect. Appetite 2006, 46, 318–323. [CrossRef] [PubMed]
- Tan, C.C.; Holub, S.C. Maternal Feeding Practices Associated with Food Neophobia. Appetite 2012, 59, 483–487. [CrossRef]
- Johnson, S.L.; Davies, P.L.; Boles, R.E.; Gavin, W.J.; Bellows, L.L. Young Children’s Food Neophobia Characteristics and Sensory Behaviors Are Related to Their Food Intake. J Nutr 2015, 145, 2610–2616. [CrossRef] [PubMed]
- Maternal Controlling Feeding Behaviours and Child Eating in Preschool-aged Children - MOROSHKO - 2013 - Nutrition & Dietetics - Wiley Online Library Available online: https://onlinelibrary.wiley.com/doi/abs/10.1111/j.1747-0080.2012.01631.x (accessed on 24 October 2023).
- Sarin, H.V.; Taba, N.; Fischer, K.; Esko, T.; Kanerva, N.; Moilanen, L.; Saltevo, J.; Joensuu, A.; Borodulin, K.; Männistö, S.; et al. Food Neophobia Associates with Poorer Dietary Quality, Metabolic Risk Factors, and Increased Disease Outcome Risk in Population-Based Cohorts in a Metabolomics Study. The American Journal of Clinical Nutrition 2019, 110, 233–245. [CrossRef]
Figure 1.
Adherence to the Mediterranean Diet (AMD) in the total sample, in males, and females.
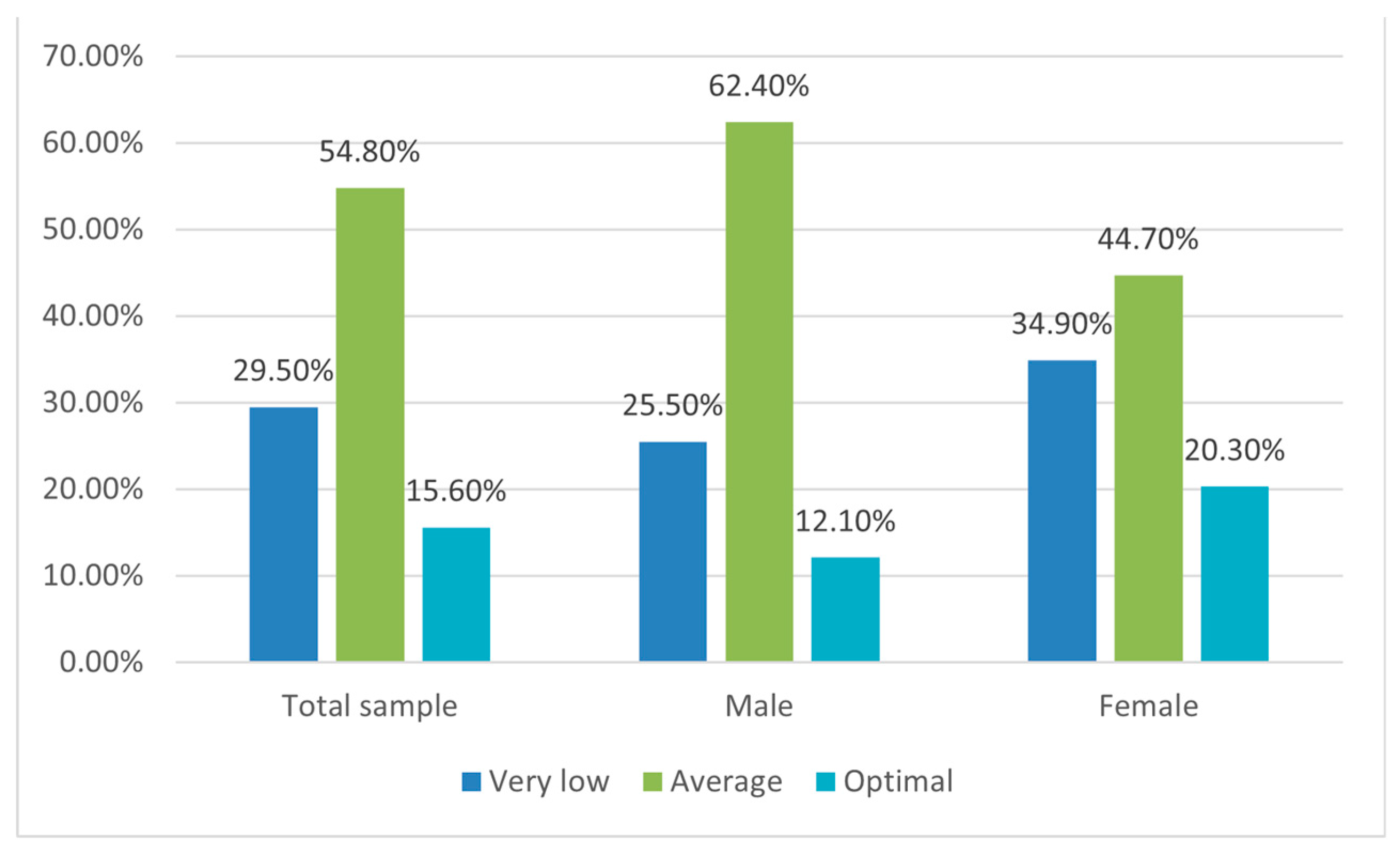
Figure 2.
Level of Food Neophobia (FN) in the total sample, in males, and females.
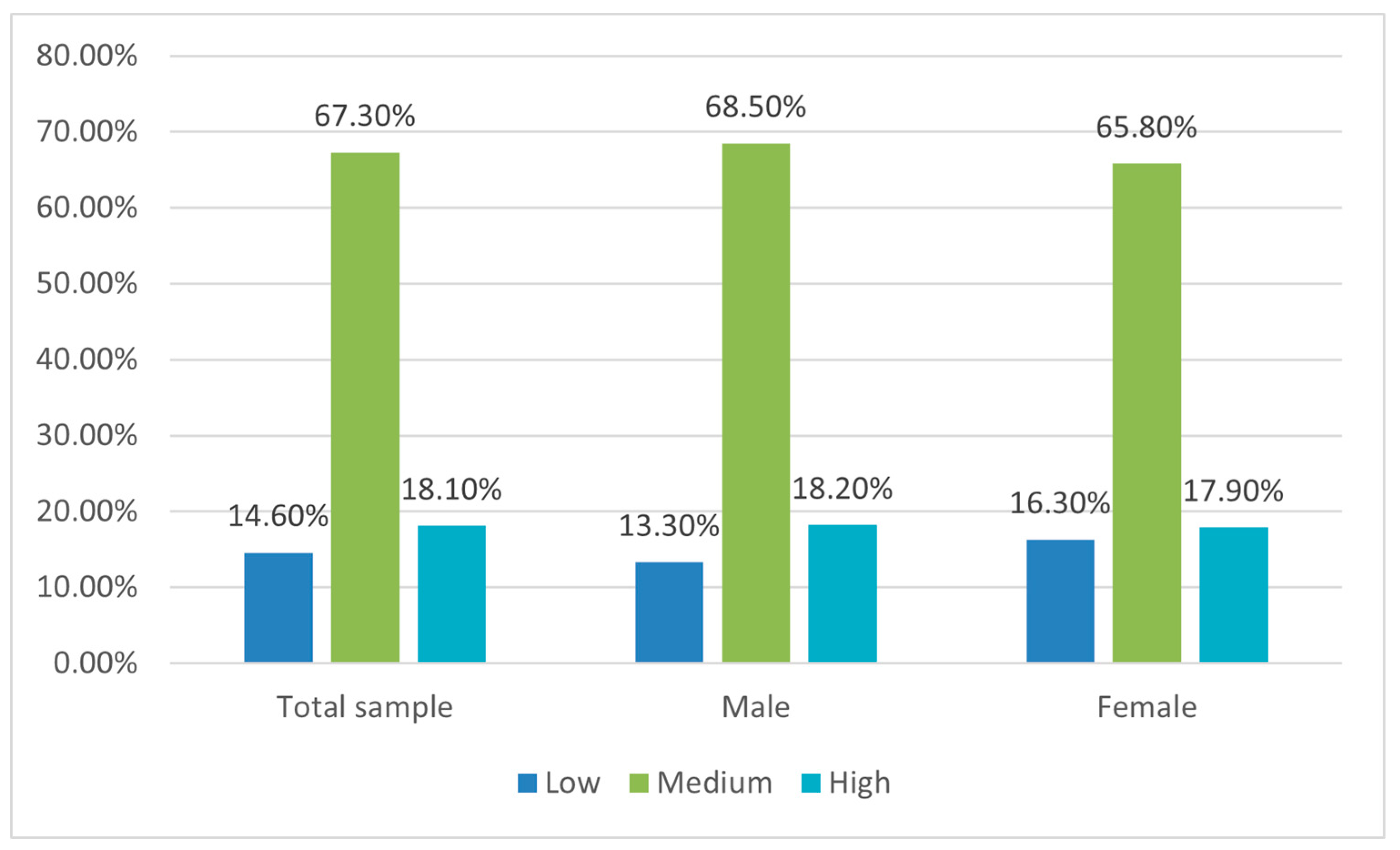
Figure 3.
Fruit, vegetables, legumes and fish consumption at different FN levels.
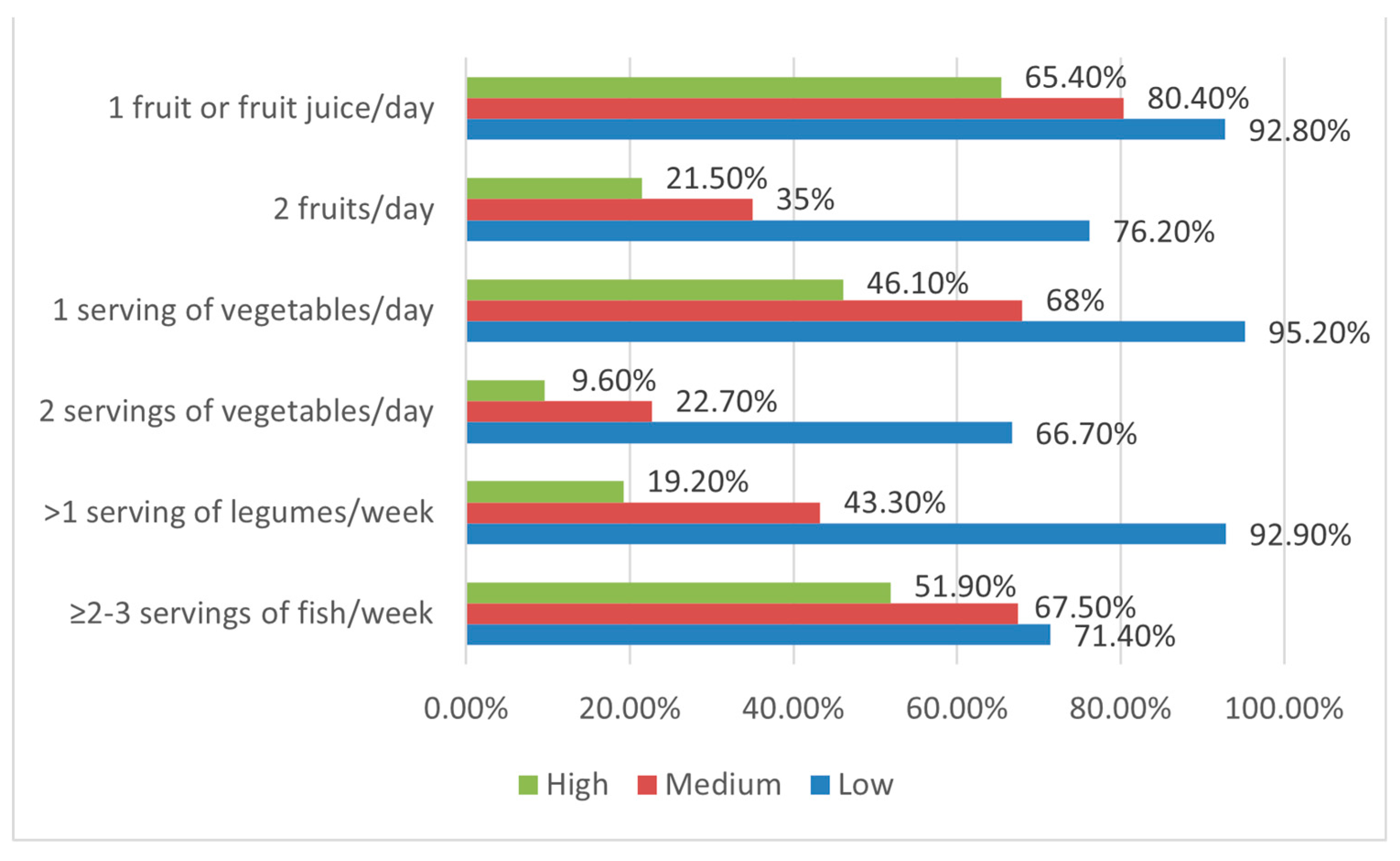

Table 1.
Characteristics of the sample (n=288).
| n | (%) | |
|---|---|---|
| Gender | ||
| Females | 123 | 42.7 |
| Males | 165 | 57.3 |
| Age | ||
| 3-5 years | 83 | 28.8 |
| 6-11 years | 205 | 71.2 |
| Ethnic group | ||
| African | 13 | 4.5 |
| Asiatic | 4 | 1.4 |
| Caucasian | 229 | 79.8 |
| Eurasian | 37 | 12.9 |
| Hispanic | 4 | 1.4 |
| Parents employment | ||
| Both parents employed | 253 | 87.8 |
| ≤1 parent employed | 35 | 12.2 |
| Household income | ||
| Up to 10.000 euros | 26 | 9 |
| Between 10.001 and 25.000 euros | 91 | 31.6 |
| Between 25.001-40.000 euros | 103 | 35.8 |
| Between 40.001 and more | 68 | 23.6 |
| Children per family | ||
| 1 | 108 | 37.5 |
| 2 | 145 | 50.3 |
| ≥2 | 35 | 12.2 |
| BMI | ||
| Underweight | 16 | 5.6 |
| Normal weight | 129 | 44.8 |
| Overweight | 60 | 20.8 |
| Obesity | 83 | 28.8 |
Table 2.
Association between socio-demographic characteristics of the sample, BMI, and Adherence to Mediterranean Diet (AMD) resulting from KIDMED test *p < 0.05.
Table 2.
Association between socio-demographic characteristics of the sample, BMI, and Adherence to Mediterranean Diet (AMD) resulting from KIDMED test *p < 0.05.
| AMD levels | Very low (≤3) | Average (4-7) | Optimal (≥8) | ||||
| n | % | n | % | n | % | ||
| Socio-demographic characteristics and BMI | |||||||
| Gender | Males | 42 | 49.4 | 103* | 65.2 | 20 | 44.4 |
| Females | 43 | 50.6 | 55 | 34.8 | 25 | 55.5 | |
| Household income | < 10.000€ | 9 | 10.6 | 11 | 6.9 | 6 | 13.3 |
| 10.000 - 25.000 € | 28 | 32.9 | 46 | 29.1 | 17 | 37.8 | |
| 25.000 - 40.000 € | 30 | 35.3 | 62 | 39.2 | 11 | 24.4 | |
| > 40.000 € | 18 | 21.2 | 39 | 24.7 | 11 | 24.4 | |
| Parents employment | Both parents employed | 68 | 80 | 147* | 93 | 38 | 84.4 |
| ≤1 parent employed | 17 | 20 | 11 | 7 | 7 | 15.6 | |
| Children per family | 1 | 35 | 41.2 | 65 | 41.1 | 8 | 17.8 |
| 2 | 40 | 47.1 | 73 | 46.2 | 32* | 71.1 | |
| > 2 | 10 | 11.8 | 20 | 10.8 | 5 | 11.1 | |
| Ethnic group | African | 1 | 1.2 | 9 | 5.7 | 3 | 6.7 |
| Asiatic | 2 | 2.3 | 1 | 0.6 | 1 | 2.2 | |
| Caucasian | 69 | 81.2 | 129 | 82.2 | 31 | 68.9 | |
| Eurasian | 11 | 13 | 16 | 10.2 | 10 | 22.2 | |
| Hispanic | 2 | 2.3 | 2 | 1.3 | 0 | 0 | |
| BMI | Underweight | 3 | 3.5 | 9 | 5.7 | 4 | 8.9 |
| Normal weight | 42 | 49.4 | 68 | 43 | 19 | 42.2 | |
| Overweight | 9 | 20 | 40 | 25.3 | 11 | 24.4 | |
| Obesity | 31 | 36.5 | 41 | 26 | 11 | 24.4 | |
Table 3.
Association between socio-demographic characteristics of the sample, BMI, and level of Food Neophobia (FN) resulting from Child Food Neophobia Scale (CFNS) *p < 0.05.
Table 3.
Association between socio-demographic characteristics of the sample, BMI, and level of Food Neophobia (FN) resulting from Child Food Neophobia Scale (CFNS) *p < 0.05.
| FN levels | Low | Medium | High | ||||
| n | % | n | % | n | % | ||
| Socio-demographic characteristics and BMI | |||||||
| Gender | Males | 22 | 52.4 | 113 | 58.2 | 30 | 57.7 |
| Females | 20 | 47.6 | 81 | 41.8 | 22 | 42.3 | |
| Household income | < 10.000€ | 2 | 4.8 | 19 | 9.8 | 5 | 9.6 |
| 10.000 - 25.000 € | 8 | 19 | 67 | 34.5 | 16 | 30.8 | |
| 25.000 - 40.000 € | 18 | 42.8 | 68 | 35.1 | 17 | 32.7 | |
| > 40.000 € | 14 | 33.3 | 40 | 20.6 | 14 | 26.9 | |
| Parents employment | Both parents employed | 40 | 95.2 | 170 | 87.6 | 43 | 82.7 |
| ≤1 parent employed | 2 | 4.8 | 24 | 12.4 | 9 | 17.3 | |
| Children per family | 1 | 7* | 16.7 | 75 | 38.7 | 26 | 50 |
| 2 | 25 | 59.5 | 98 | 50.5 | 22 | 42.3 | |
| > 2 | 10 | 23.8 | 21 | 10.8 | 4 | 7.7 | |
| Ethnic group | African | 2 | 4.8 | 10 | 5.2 | 1 | 1.9 |
| Asiatic | 0 | 0 | 4 | 2.1 | 0 | 0 | |
| Caucasian | 34 | 80.9 | 153 | 79.3 | 42 | 80.8 | |
| Eurasian | 6 | 14.3 | 22 | 11.4 | 9 | 17.3 | |
| Hispanic | 0 | 0 | 4 | 2.1 | 0 | 0 | |
| BMI | Underweight | 0 | 0 | 12 | 6.2 | 4 | 7.7 |
| Normal weight | 26 | 61.9 | 81 | 41.8 | 22 | 42.3 | |
| Overweight | 16 | 38.1 | 36 | 18.5 | 8 | 15.4 | |
| Obesity | 0* | 0 | 65 | 33.5 | 18 | 34.6 | |
Table 4.
Association between Adherence to Mediterranean Diet (KIDMED total score and component scores) and Food Neophobia *p < 0.05.
Table 4.
Association between Adherence to Mediterranean Diet (KIDMED total score and component scores) and Food Neophobia *p < 0.05.
| FN levels | Low | Medium | High | ||||
| n | % | n | % | n | % | ||
| KIDMED total score | Very low | 1 | 2.4 | 57 | 29.4 | 27* | 51.9 |
| Average | 26 | 61.9 | 109 | 56.2 | 23 | 44.2 | |
| Optimal | 15 | 35.7 | 28 | 14.4 | 2 | 3.8 | |
| KIDMED Test components | |||||||
| Fruit or fruit juice every day | Yes | 39 | 92.9 | 156 | 80.4 | 34 | 65.4 |
| No | 3 | 7.1 | 38 | 19.6 | 18* | 34.6 | |
| Second fruit every day | Yes | 32* | 76.2 | 67 | 34.5 | 11 | 21.2 |
| No | 10 | 23.8 | 127 | 65.5 | 41 | 78.8 | |
| Fresh or cooked vegetables regularly once a day | Yes | 40* | 95.2 | 132 | 68 | 24 | 46.2 |
| No | 2 | 4.8 | 62 | 32 | 28 | 53.8 | |
| Fresh or cooked vegetables more than once a day | Yes | 28* | 66.7 | 44 | 22.7 | 5 | 9.6 |
| No | 14 | 33.3 | 150 | 77.3 | 47 | 90.4 | |
| Fish at least 2-3 times per week | Yes | 30 | 71.4 | 131 | 67.5 | 27 | 51.9 |
| No | 12 | 28.6 | 63 | 32.5 | 25* | 48.1 | |
| Fast-food more than once a week | Yes | 1 | 2.4 | 40 | 20.6 | 13 | 25 |
| No | 41* | 97.6 | 154 | 79.4 | 39 | 75 | |
| Legumes more than once a week | Yes | 39* | 92.9 | 84 | 43.3 | 10 | 19.2 |
| No | 3 | 7.1 | 110 | 56.7 | 42 | 80.8 | |
| Cereals or grains (bread, etc.) for breakfast | Yes | 13* | 31 | 35 | 18 | 6 | 11.5 |
| No | 29 | 69 | 159 | 82 | 46 | 88.5 | |
| Nuts at least 2–3 times per week | Yes | 7 | 16.7 | 56 | 28.9 | 10 | 19.2 |
| No | 35 | 83.3 | 138 | 71.1 | 42 | 80.8 | |
| Skips breakfast | Yes | 2 | 4.8 | 22 | 11.3 | 10 | 19.2 |
| No | 40 | 95.2 | 172 | 88.7 | 42 | 80.8 | |
| Dairy product for breakfast (yoghurt, milk, etc.) | Yes | 40 | 95.2 | 180 | 92.8 | 44 | 84.6 |
| No | 2 | 4.8 | 14 | 7.2 | 8 | 15.4 | |
| Commercially baked goods or pastries for breakfast | Yes | 36 | 85.7 | 156 | 80.4 | 43 | 82.7 |
| No | 6 | 14.3 | 38 | 19.6 | 9 | 17.3 | |
| Sweets and candy several times every day | Yes | 11 | 26.2 | 79 | 40.7 | 25 | 48.1 |
| No | 31 | 73.8 | 115 | 59.3 | 27 | 51.9 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



