
Submitted:
09 October 2023
Posted:
10 October 2023
You are already at the latest version
Abstract
(1) Background: Newer generation ophthalmologists practicing in the developed world are not very familiar with some tropical ocular diseases due to the absence of reports in the ophthalmic literature over the past thirty years. Because of world globalization or due to influx of immigrants from Sub Saharan Africa, exotic retinal diseases are being encountered more often in ophthalmology clinics; (2) Methods: Case series of chorioretinitis or optic neuritis with obscure etiology; (3) Results: 4 cases qualified with the diagnosis of ocular onchocerciasis based on their residence near fast rivers in endemic areas, multimodal imaging, long term follow-up showing progressive disease and negative workup for other diseases. Characteristic findings include peripapillary choroiditis with optic neuritis or atrophy, subretinal tracts of the microfilaria, progressive RPE atrophy around heavily pigmented multifocal chorioretinal lesions of varying shapes and subretinal white or crystalline dots. Typical skin findings are often absent in eyes with chorioretinitis rendering the diagnosis more challenging; (4) Conclusions: Familiarity with the myriad ocular findings of onchocerciasis, and a high degree of suspicion in subjects residing in endemic areas can help in the correct diagnosis and implementation of appropriate chemotherapy. Onchocercid chorioretinitis is a slow insiduous progressive and prolonged polymorphous disease.
Keywords:
blackfly
; blindness
; chorioretinitis
; ivermectin
; microfilaria
; onchocerciasis
; optic atrophy
; optic neuritis
; river blindness
; tropical disease
; uveitis.
1. Introduction
Onchocerciasis, also called river blindness, is a vector-borne disease under the neglected tropical diseases caused by the tissue nematode Onchocerca volvulus (O. volvulus). It is highly prevalent in areas where there is an abundance of fast flowing rivers and vegetation. Most of the disease exists in sub-Saharan Africa where it is endemic, with few foci in Yemen and Latin America [1,2]. It is estimated that around 21 million O. volvulus infections exist worldwide with 14.6 million having stigmatizing skin disease (severe itching and disfiguring skin conditions), 1.15 million suffering from visual disability, and 100,00 cases experiencing epilepsy (Nodding syndrome or tonic-clonic) [3,4]. Onchocerciasis is transmitted through repeated bites of infected black flies belonging to the genus Simulium. Despite the preventive community-directed ivermectin treatment via mass drug administration coverage of around 80%, onchocerciasis transmission in many districts remains persistent in many districts [2,5].
Inside the human host, female blackflies release around a thousand microfilariae daily over a life span of 9-13 years. These microfilariae, or embryonic larvae, that travel to the skin, eyes, and other organs. The microfilariae that are consumed by a female blackfly after biting an infected person grow inside the blackfly and are subsequently passed to the next human host during consecutive bites. Microfilariae measure 300 µm in length and 8 µm in cross section with one year lifespan. Inside blood vessels, the filariae hardly ever trigger an immunological reaction. Inflammation in the host is brought on by the parasite's decomposition. The microfilariae and Wolbachia bacteria coexist in a mutualistic relationship. These bacteria appear necessary for filarial growth and survival [6]. The development of inflammatory diseases is also greatly influenced by these endosymbionts, explaining the use of antibiotics like doxycycline (or azithromycin) which delivers a macrofilaricidal activity and modulates inflammatory processes [6,7]. Diethylcarbamazine, ivermectin, and albendazole were prescribed as medical treatments for microfilariae. Opoku et al. [7] compared the outcomes of 1500 individuals with O volvulus skin infection that were treated with single doses of either of the 2 macrocyclic lactones ivermectin (half-life 1 day) or moxidectin (half-life 1 month) [8]. After one year of therapy, the percentage of participants without detectable cutaneous microfilariae was 2.5-fold in the moxidectin group (38.4%) than in the ivermectin group (15%) [7,8]. Despite many rounds of sustainable ivermectin mass drug administration (Mectizan®, donated by Merck) with 80% therapeutic coverage, onchocerciasis persists in adults in many African villages, with more time needed to reach elimination of the disease [9-14].
Onchocerciasis is the second-most common infectious cause of blindness in the world, causing vision loss in 1.15 million individuals [1]. Despite these epidemiologic statistics [15-24], little has been written about onchocerciasis in the recent retina and uveitis literatures [25-48]. This renders young ophthalmologists esp. in the developed world unfamiliar with the clinical features. With increasing international travel or hunger and poverty driven mass global population immigration, clinicians in nonendemic countries must be familiar with imported neglected tropical diseases.
The risk of visual impairment increases, in part, with rising infection prevalence and intensity in a population [5]. Partially correlated with rising infection prevalence and intensity in a community, visual impairment chances increased [5]. In some villages, the prevalence of infection can range from 80 to 100 percent by the age of 20, with blindness reaching its peak between 40 and 50 years of age. Before the implementation of control measures, hyperendemic areas were commonly abandoned due to high incidence of blindness. WHO programmes shifted from control to elimination in the American continent. WHO advises ivermectin chemotherapy at least twice a year for more than 10 years, but so far there is limited success in the African continent.
Due to tourism or migration in recent years, parasitic diseases, which cause major ocular morbidity in certain areas, have been moving from endemic areas to other regions of the world [10,44,45]. Our aim is to present a case series of chorioretinitis related to onchocerciasis with the diagnosis delayed due to its rarity in the developed world and its polymorphic appearance. The two largest retina image banks totaling more than 66,000 multimodal images (Retina Image Bank from American Society of Retina Specialists and Retina Rocks Retina Image and Reference Library from Retina World Congress) had no photographs related to onchocerciasis.
2. Materials and Methods
Case series of chorioretinitis cases seen in different parts of the developed world where diagnosis was missed for a long time. All subjects gave their informed consent for inclusion in this study. The study was conducted in accordance with the Declaration of Helsinki. National legislation indicated that ethics approval is not required for this type of retrospective anonymized noninterventional study.
3. Results
3.1. Case 1
This 46-year-old White man worked in Abidjan (Côte D’Ivoire, Africa) for the past 23 years. He developed painful red swelling of the eyes in 1998 one year after initial visits to the neighboring river. Ten years later (2008), he developed blurry vision bilaterally. Fluorescein angiography (FA) revealed disc staining that was interpreted as drusen of the optic nerve head. No retinal scars were detected except for peripapillary subretinal tracts (Figure 1, Figure 2 and Figure 3). Subsequently several specialists in Côte D’Ivoire diagnosed papillitis and 5 consecutive yearly MR brain imaging were performed, and all were negative. In 2012 and 2013, multiple chorioretinal scars were evident at the equator with large area of peripapillary atrophy. In 2016, extensive uveitis workup (normal CBC-no eosinophilia; PPD skin test; VDRL; Chest radiograph), failed to reveal positive tests except for toxoplasmosis (IgM 0.66IU/ml- negative <0.8; IgG 418 IU/ml- positive>3). Intraocular dexamethasone implants were given to quiet the uveitis in the left eye with the working diagnosis of toxoplasma chorioretinitis. In June 2018, he presented with 20/40 vision right eye and finger counting 20cm left eye. He had severe flare in the anterior chamber and dense nuclear sclerosis in the left eye. Our initial impression was river blindness (Figure 4, Figure 5). He was given azithromycin 1 tablet for 12 days to be followed by a single dose of moxidectin 8mg. Inability to procure moxidectin lead to the use of ivermectin. Subsequently he underwent uneventful cataract surgery elsewhere and had relapse of the uveitis, as per recent contact 25 years after his first eye symptoms developed. The serial fundus photographs, autofluorescence, fluorescein angiography and SD-OCT were collated and shown in chronological order over 18-year period (Figure 1, 2).
3.2. Case 2
This 71-year-old White man is the cousin of Case 1 and lived together in the same household in Africa. He also visited frequently the nearby river. He had no visual symptoms. Similar blood workup to Case 1 was negative. Visual acuity was 20/20 in both eyes. Large deep chorioretinal scars were noted temporally with adjacent zone of RPE alterations in both eyes (Figure 6).
3.3. Case 3
This 67-year-old Black African woman was referred for decreased vision after cataract surgery. Best corrected visual acuity was 20/125 right eye and 20/50 left eye with posterior chamber intraocular implant and dense nuclear sclerosis left eye. Posterior vitreous detachment was noted bilaterally without vitritis. The right fundus had crystalline deposits noted by funduscopy and as hyperreflective mid retinal foci by SD-OCT (Figure 7). Diffuse patchy loss of the ellipsoid in the posterior pole of the right eye (Figure 7). Supertemporal linear subretinal fibrosis tracks in the right eye (Figure 7) were initially interpreted as spontaneous reattachment of a detached retina. The inferior retina revealed perivascular sheathing along the inferotemporal arcade and inferonasal perivascular pigmentary deposits (Figure 6). She reported decrease in vision in the right eye since age 30. Systemic history was positive for hypertension well controlled on beta-blocker. The patient immigrated from Sierra Leonne where she lived by the riverside. She reports heavy consumption of Kola nuts. Blood workup (including CBC, hemoglobin electrophoresis (for sickle cell disease), RPR, FTA-ABS, angiotensin converting enzyme, and lysozyme) and chest radiograph were all negative. The preliminary differential diagnosis was uveitic crystalline maculopathy, West African crystalline retinopathy and resolved retinal detachment.
3.4. Case 4
This 49-year-old White man had lived for 3 decades near swamps connected to the Wouri river in Cameroon. Upon presentation, best corrected vision was 20/600 right eye and 20/80 left eye. Optic atrophy was impressive bilaterally (Figure 9). Fine retinal tracts were noted in the left eye. Systemic and uveitis workup (including absence of eosinophilia, MR Brain, ANA, malaria, etc.) and coagulation screen (Factor V Leiden, VIII, antithrombin III) were negative. A tropical disease was suspected, and all documented ocular history was requested. 14.5 years ago, A large juxtafoveal temporal patch of stippled retina had outer retinal thinning by OCT. Subsequently 15 months ago, he developed uveitis of the left eye and left papillophebitis with macular detachment that was well controlled by oral corticosteroids. 100 days later, the right eye had papillophlebitis with cystoid macular edema that was interpreted as central retinal vein occlusion. He received oral corticosteroid and intravitreal bevacizumab.
- 1.1.2009 Initial OCT scan: outer retinal thinning left macula with pigment stippling.
- 24.5.2022 Left papillophlebitis 13.5 years after initial presentation.
- 17.7.7.2022 Left papillophlebitis resolved after oral corticosteroids.
- 9.9.2022 Right papillophlebitis 100 days after left papillophlebitis.
- 19.10.2022 Disc edema right eye.
- 29.12.2022 Resolved papillophlebitis after intravitreal bevacizumab and oral corticosteroids. Peripapillary fibrosis is noted superiorly.
- 22.5.2023 last follow-up 14.5 years after presentation revealed bilateral optic atrophy and subtle subretinal tracts (arrows). Peripapillary fibrosis is noted.
Little is known about multimodal findings in the setting of river blindness and most reports detail short follow-up without fundus documentation. Over the past thirty years, most of the publications appeared in epidemiologic or infection or tropical disease literature with no fundus photograph familiarizing the disease in the ophthalmic or retina or uveitis literatures. We present a long-term follow-up of a case series where the clinical diagnosis was obscure and showing progressive disease with myriad of findings captured by multimodal imaging, with unique fundus findings that help in the diagnosis of the disease.
The ocular findings in onchocerciasis are very varied (Table 1). Our aim is to refresh these findings and add multimodal findings plus long-term photographic documentation of this progressive pleomorphic disease. All the presented cases had an indefinite diagnosis for a prolonged time. Diagnosing this disease is time costly and a great challenge to the ophthalmologist as most infected individuals manifested no disease symptoms. Without skin findings, the gold standard diagnostic test (i.e., the skin snip) could not be applied.
The road to diagnosis of onchocerciasis chorioretinitis: 1-search for travel or residency in endemic areas; 2-access past fundus photographs to assess progression; 3-exclude all known causes of uveitis or optic neuritis (complete work-up).
Onchocercal choroiditis is a condition that has been studied more than 3 decades ago experimentally [26, 45], observationally [15], and epidemiologically [16, 17]. First, after injecting 100,000 live Onchocerca volvulus microfilariae intravitreally, the retinal pigment epithelium gradually became atrophic in patches along with inflammation and thinning of the outer retina. Second, little was known about the evolution of choroidal lesions over the long term. It was Semba et al [15] that tried in 57 patients to track the evolution of onchocercal chorioretinitis over a period of 1 to 3 years: In fresh cases, live retinal microfilariae, retinal hemorrhages, and fine retinal pigment epithelium (RPE) alterations are noted; Subsequently there is growth of the depigmentation zone (200 microns yearly) at the borders of the chorioretinal scars regardless of treatment. Third, the epidemiology of onchocerciasis in rain forest regions in Africa and South America provided deep insight into the disease severity. This first epidemiological investigation involved 800 inhabitants of a rubber plantation amidst a hyperendemic region of the Liberian rain forest: 84% had the infection; of these, 29% had intraocular microfilariae, and 2.4% were blind in one or both eyes. All cases of bilateral blindness and one-third of visual impairment were caused by onchocerciasis. Chorioretinitis was detected in three-quarters of the participants and was the direct cause for half of the visual impairment. The presence of retinitis, subretinal fibrosis, and optic neuropathy was found to be strongly correlated with uveitis. In this second epidemiologic study from Ecuador's rain forest onchocerciasis focus, Cooper et al. [33] examined 785 infected people all with a positive skin snip: Onchocerciasis caused 0.4% of blindness, 8.2% of visual impairment, 5.1% of optic atrophy, and 28.0% of chorioretinopathy. Of great importance is early detection and treatment as chorioretinitis becomes irreversible when treated late or inadequately [24].
Our case series establish 1- peripapillary atrophy; 2- subretinal tracts showing trajectory of the microfilariae; temporal chorioretinal lesions of varying sizes [29]: dot size, coin size, round lesions or torpedo lesions or any form; chorioretinal atrophy adjacent to toxoplasma like deep chorioretinal scars; retinitis and vitritis attacks; optic neuritis attacks; optic atrophy; retinal vasculitis; retinal venous engorgement or central retinal vein occlusion-like accompanied by papillophlebitis. Serial exams allowed us to witness the changing face of onchocerciasis with follow-up beyond ten years documented photographically. FA demonstrated retinal vasculitis and disc leakage as well as cystoid macular edema. OCT documented outer retinal atrophy around peripapillary choroiditis, disc edema in optic neuritis, crystalline deposits in macula and cystoid macular edema. Future OCT studies may further document microfilaria in the conjunctiva, cornea, anterior chamber, or retina in heavily infected eyes in mesoendemic regions during the acute phases. No such photographic documentation exists to date. OCT was instrumental in detecting disc swelling in “normal-appearing” discs and this can complement visual fields testing which was shown to detect severe changes in apparently normal discs [Thylefors]. Moreover, optic neuritis or atrophy accompanied by temporal retinal mottling or OCT signs of outer retinal atrophy appears to be characteristic of onchocerciasis [Thylefors].
More than half of the ocular fluids from individuals with ocular onchocerciasis contained autoimmune antibodies that were directed against the outer region of the photoreceptor and were unrelated to either the interphotoreceptor retinoid binding protein or the retinal S-antigen (S-Ag) [40, 41]. These anti-retinal antibodies could contribute to the retinal degeneration brought on by onchocerciasis [40]. According to several investigations, posterior segment disorders may be exacerbated by cross-reactive antibodies produced in response to the antigens of O. volvulus (Ov39) and the retinal pigment epithelial (RPE) antigen (hr44). [18,19]. It is unclear if the persistence of microfilariae or their byproducts in the posterior segment or autoimmune reactions are to blame for these progressive ocular alterations.
The diagnosis of infection in a person has varied, with the classical clinical presentations varying from being obvious in heavily infected cases (e.g., observation of microfilaria in the cornea or anterior chamber, detecting the parasites in skin-snip biopsy, or finding a palpable subcutaneous adult worm) to being relatively insensitive in patients carrying lower loads of the parasite. The incubation period can be prolonged up to 15 months. Onchodermatitis resembles eczema with varying degrees of papular, lichenoid, atrophic, and pigmentary alterations [50]. Eosinophilia is not a sensitive indicator of Onchocerca volvulus, according to recent clinical investigations, with one-third of patients having a normal eosinophil count. The currently recommended epidemiological diagnostic method entails the measurement of an antibody response to the parasite antigen Ov16 with 20% false negative results [46].
More recent research suggests that it is largely the Wolbachia bacteria (which are endosymbionts), which cause the immunogenic response [46]. It appears that there are two main strains of O. volvulus: the savanna strain that causes ocular disease, even with moderate parasite burdens, and the rainforest strain, that does not lead to blindness despite high parasite burdens. This predilection for ocular disease seems related to higher quantities of Wolbachia.
Ivermectin binds to the inhibitory neurotransmitter GABA on neurons and muscles leading to activation of a chloride influx, hyperpolarization of the membrane, resulting in paralysis and death of microfilariae. The life span of microfilariae is 1-2 years while the clearance of microfilariae has been studied extensively [38, 39]. Skin microfilariae are reduced by half in 24 hours, 94% in one week, and 98% by 4 weeks following a single dose of ivermectin with the clearance from the anterior chamber lagging by several months. Microfilariae repopulate the eye several months after a single dose of ivermectin from the continuous production of microfilariae by the adult worm. This explains the WHO recommendation of biannual ivermectin to be administered over a span of 10 to 15 years [38]. Even children as early as 4 years should be included in the massive drug administration (dose 150 μg/kg) according to a recent metaanalysis [37, 39]. Note that there is ample evidence that moxidectin appears to offer better control than ivermectin [38, 39].
One major challenge facing elimination of O. volvulus transmission following mass chemotherapy administration in sub-Saharan Africa is the very variable response of adult worms to the embryostatic effect of ivermectin as well as the variable number of adult worms per person [55]. Moreover, recent literature has suggested the appearance of strains of O. volvulus resistant to ivermectin. Therefore, other treatments have been tried with varying levels of success include azithromycin and rifampin. Opoku et al [7] compared the 18 months results of single doses of ivermectin and moxidectin, on around 1500 subjects infected with O volvulus microfilariae. The proportion of subjects with undetectable skin microfilariae at one year post treatment was 38·4% in the moxidectin compared with only 1·5% in the ivermectin group [8]. This longer lasting effect of moxidectin related to the long half-life (moxidectin 20–43 days, ivermectin <1 day) [8]. Ophthalmologists would like to extrapolate the results of the skin effect to the choroid in the hope of curing this cause of blindness. Cousens et al. [35] in his field study in mesoendemic communities in Nigeria concluded that annual delivery of ivermectin in a sustained fashion could halt onchocercal blindness from optic atrophy. These findings were confirmed by different investigators [18, 36, 48].
In Case 4 where venous impedance followed disc edema, treating the disc edema can lead to prompt return of normal retinal venous pattern. In the first eye, systemic corticosteroid and intravitreal anti-vascular endothelial growth factor achieved good control of the disc edema and cystoid macular edema, while intravitreal dexamethasone implant in the fellow eye achieved similar response. It is well known that when early central retinal vein occlusion or venous stasis is deemed secondary to optic nerve swelling or neuritis, corticosteroid whether systemic or local, alleviate optic nerve swelling, thereby relieving compartment obstruction at the level of the lamina cribrosa, and improving venous outflow [47].
Ocular lesions in river blindness are not specific including corneal scars, uveitis, cataract and chorioretinitis. Differential diagnosis of ocular onchocerciasis chorioretinitis [56-60] include toxoplasmosis, sarcoidosis, tuberculosis, larva migrans, syphilis, diffuse unilateral subacute neuroretinitis from various nematodes (Toxocara canis, Ancylostoma caninum, Strongyloides stercoralis, Ascaris lumbricoides, and Baylisascaris procyonis), schistosomiasis [57], cestodes [58] and other microfilaria (including Marsonella perstans, Loa loa, Onchocerca gutturosa, or Dracunculus medinensis). Oculocutaneous tropical disease differential includes: tuberculosis, leprosy, Chagas disease (also known as American trypanosomiasis), sporotrichosis (also known as “rose gardener's disease”) [59], coccidioidomycosis (also known as San Joaquin Valley fever) [60], leishmaniasis [56], giardiasis [56] and infection by other microfilaria (Onchocerca gutturosa, Loa loa, Dracunculus medinensis, Marsonella perstans).
Drawback of the paper is absence of superficial skin lesions that can offer a chance for snip biopsies as well as lack of adjuvant tests like PCR and serology. Historical evidence (living near rivers in endemic areas), negative workup for other etiologies, long-term followup and characteristic clinical findings are the four cornerstones for the current diagnosis.
Conclusions
Live microfilariae caused little or no inflammation. The immune reaction to degenerating dead worms resulted in intraocular inflammation (uveitis, keratitis, chorioretinitis, optic neuritis) with progressive visual loss. Peripapillary chorioretinitis, retinal tracks, papillophlebitis, retinal vasculitis, and polymorphic chorioretinitis characterize the disease. Experimental and clinical data indicated a cardinal role of the endosymbiotic Wolbachia bacteria in the pathogenesis of blindness. Besides ivermectin chemotherapy, oral administration of doxycycline resulted in significant decrease in Wolbachia bacterial load, altered filarial embryogenesis and ultimately a reduced ocular inflammatory response.
Ocular onchocerciasis should be suspected in subjects residing near sub-Saharan rivers, subjects with disfiguring skin disease or seizures. With the recent influx of African immigrants, ocular onchocerciasis may be seen more often in clinics in temperate climates in immigrants and travelers from endemic regions. Familiarity of ophthalmologists with the various ocular signs corneal scar, evolving chorioretinitis, optic neuropathy would help recognize the entity. Blindness caused by O. volvulus results in significant morbidity, long-term disability, reduced economic productivity and life expectancy. Clinicians should have high suspicion for imported onchocerciasis which is in the rise among people residing in endemic areas with vision changes, subcutaneous nodules, or itchy skin rashes. The parasite that gained historical notoriety as “African river blindness” needs to be revived in our retina and uveitis clinics.
Author Contributions
Conceptualization, AM; methodology, AM; software, AM.; validation, AM, LR, HM, MY, MBP; formal analysis, AM, LR, HM, MY, MBP; investigation, AM, LR, HM, MY, MBP.; resources, AM, LR, HM, MY, MBP; data curation, AM, LR, HM, MY, MBP; writing—original draft preparation, AM.; writing—review and editing, AM, LR, HM, MY, MBP; visualization, HM; supervision, HM; project administration, HM.; funding acquisition, AMM. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, Ethical review and approval were waived for this study due to its anonymized noninterventional retrospective case series.
Informed Consent Statement
Written informed consent has been obtained from the patients to publish this paper.
Data Availability Statement
No new data were created.
Acknowledgments
In this section, you can acknowledge any support given which is not covered by the author contribution or funding sections. This may include administrative and technical support, or donations in kind (e.g., materials used for experiments).
Conflicts of Interest
The authors declare no conflict of interest.
References
- Meribo, K.; Kebede, B.; Feleke, S.M.; Mengistu, B.; Mulugeta, A.; Sileshi, M.; Samuel, A.; Deribe, K.; Tadesse, Z. Review of Ethiopian Onchocerciasis Elimination Programme. Ethiop Med J. 2017, 55, 55–63. [Google Scholar]
- Basánez, M-G. ; Pion, S.D.S.; Churcher, T.S.; Breitling LP, Little MP, Boussinesq M. River Blindness: A Success Story under Threat? PLoS Med. 2006, 3, e37. [Google Scholar]
- Hadermann A, Amaral LJ, Van Cutsem G, Siewe Fodjo JN, Colebunders R. Onchocerciasis-associated epilepsy: an update and future perspectives. Trends Parasitol. 2023, 39, 126–138. [CrossRef]
- Vinkeles Melchers, N.V.S. , Mollenkopf, S., Colebunders, R. et al. Burden of onchocerciasis-associated epilepsy: first estimates and research priorities. Infect Dis Poverty 2018, 7, 101. [Google Scholar] [CrossRef]
- Gebremedhin Gebrezgabiher G, Mekonnen Z, Yewhalaw D, Hailu A. Status of parasitological indicators and morbidity burden of onchocerciasis after years of successive implementation of mass distribution of ivermectin in selected communities of Yeki and Asosa districts, Ethiopia. BMC Public Health 2020, 20, 1233. [Google Scholar]
- McGillan P, Berry NG, Nixon GL, Leung SC, Webborn PJH, Wenlock MC, Kavanagh S, Cassidy A, Clare RH, Cook DA, Johnston KL, Ford L, Ward SA, Taylor MJ, Hong WD, O'Neill PM. Development of Pyrazolopyrimidine Anti-Wolbachia Agents for the Treatment of Filariasis. ACS Med Chem Lett. 2021, 12, 1421–1426. [CrossRef]
- Opoku NO, Bakajika DK, Kanza EM, et al. Single dose moxidectin versus ivermectin for Onchocerca volvulus infection in Ghana, Liberia, and the Democratic Republic of the Congo: A randomized, controlled, double-blind phase 3 trial. Lancet 2018. [CrossRef]
- Boussinesq, M. A new powerful drug to combat river blindness. Lancet 2018. [CrossRef]
- Ekpo UF, Eneanya OA, Nwankwo EN, Soneye IY, Weil GJ, Fischer PU, Nwaorgu OC. Persistence of onchocerciasis in villages in Enugu and Ogun states in Nigeria following many rounds of mass distribution of ivermectin. BMC Infect Dis. 2022, 22, 832. [CrossRef]
- Doğan, N. Globalisation and Ocular Parasitic Infections: A Review of Recent Studies. Turkiye Parazitol Derg 2020, 44, 239–257. [Google Scholar] [CrossRef]
- Olliaro PL, Kuesel AC, Halleux CM, Sullivan M, Reeder JC. Creative use of the priority review voucher by public and not-for-profit actors delivers the first new FDA-approved treatment for river blindness in 20 years. PLoS Negl Trop Dis 2018; 12: e0006837.
- Nicholls RS, Duque S, Olaya LA, López MC, Sánchez SB, Morales AL, et al. Elimination of onchocerciasis from Colombia: first proof of concept of river blindness elimination in the world. Parasit Vectors 2018; 11.
- Colebunders R, Basáñez MG, Siling K, Post RJ, Rotsaert A, Mmbando B, et al. From river blindness control to elimination: bridge over troubled water. Infect Dis Poverty 2018; 7: 21.
- Komlan K, Vossberg PS, Gantin RG, Solim T, Korbmacher F, Banla M, et al. Onchocerca volvulus infection and serological prevalence, ocular onchocerciasis and parasite transmission in northern and central Togo after decades of Simulium damnosum s.l. vector control and mass drug administration of ivermectin. PLoS Negl Trop Dis 2018; 12: e0006312.
- Semba RD, Murphy RP, Newland HS, et al. Longitudinal study of lesions of the posterior segment in onchocerciasis. Ophthalmology. 1990, 97, 1334–41. [CrossRef]
- Newland HS, White AT, Greene BM, Murphy RP, Taylor HR. Ocular manifestations of onchocerciasis in a rain forest area of west Africa. Brit J Ophthalmol. 1991, 75, 163–169. [Google Scholar] [CrossRef]
- Cooper PJ, Proaño R, Beltran C, Anselmi M, Guderian RH. Onchocerciasis in Ecuador: ocular findings in Onchocerca volvulus infected individuals. Brit J Ophthalmol. 1995, 79, 157–162. [Google Scholar] [CrossRef]
- Abiose A, Murdoch I, Babalola O, Cousens S, Liman I, Onyema J, Evans J, Gregory W, Jones B. Distribution and aetiology of blindness and visual impairment in mesoendemic onchocercal communities, Kaduna State, Nigeria. Kaduna Collaboration for Research on Onchocerciasis. Br J Ophthalmol. 1994, 78, 8–13. [Google Scholar] [CrossRef]
- 19. Anderson J, Fuglsang H, Marshall TF. Studies on onchocerciasis in the United Cameroon Republic. III. A four-year follow-up of 6 rain-forest and 6 Sudan-savanna villages. Trans R Soc Trop Med Hyg. 1976;70(5-6):362–373.
- Rolland A, Thylefors B, Pairault C. Evolution sur neuf ans de l'onchocercose oculaire dans une communauté villageoise d'Afrique occidentale. Bull World Health Organ. 1978, 56, 805–810. [Google Scholar]
- Dadzie KY, Remme J, Rolland A, Thylefors B. The effect of 7-8 years of vector control on the evolution of ocular onchocerciasis in West African savanna. Trop Med Parasitol. 1986, 37, 263–270. [Google Scholar]
- Anderson J, Fuglsang H, Marshall TF, Radolowicz A, Vaughan JP. Studies on onchocerciasis in the United Cameroon Republic. IV. A four-year follow-up of six rain-forest and six savanna villages. The incidence of ocular lesions. Trans R Soc Trop Med Hyg. 1978, 72, 513–515. [Google Scholar] [CrossRef]
- Budden, FH. The natural history of ocular onchocerciasis over a period of 14-15 years and the effect on this of a single course of suramin therapy. Trans R Soc Trop Med Hyg. 1976, 70, 484–491. [Google Scholar] [CrossRef]
- Banla M, Tchalim S, Karabou PK, Gantin RG, Agba AI, Kére-Banla A, Helling-Giese G, Heuschkel C, Schulz-Key H, Soboslay PT. Sustainable control of onchocerciasis: ocular pathology in onchocerciasis patients treated annually with ivermectin for 23 years: a cohort study. PLoS One. 2014, 9, e98411.
- Cooper PJ, Proaño R, Beltran C, Anselmi M, Guderian RH. Onchocerciasis in Ecuador: evolution of chorioretinopathy after amocarzine treatment. Br J Ophthalmol. 1996, 80, 337–342. [CrossRef]
- Semba RD, Donnelly JJ, Young E, Green WR, Scott AL, Taylor HR. IV. Chorioretinitis elicited by Onchocerca volvulus microfilariae. Invest Ophthalmol Vis Sci. 1991, 32, 1499–507.
- Paul, E.V. , Zimmerman, LE. Some observations on the ocular pathology of onchocerciasis. Human Pathology 1970, 1, 581–594. [Google Scholar] [CrossRef]
- Rodger, FC. The pathogenesis and pathology of ocular onchocerciasis. Part IV. The pathology. Am J Ophthalmol. 1960, 49, 560–594. [Google Scholar] [CrossRef]
- Bird AC, el-Sheikh H, Anderson J, Fuglsang H. Changes in visual function and in the posterior segment of the eye during treatment of onchocerciasis with diethylcarbamazine citrate. Br J Ophthalmol. 1980, 64, 191–200. [Google Scholar] [CrossRef]
- Neumann E, Gunders AE.Pathogenesis of the posterior segment lesion of ocular onchocerciasis. Am J Ophthalmol. 1973, 75, 82–89. [CrossRef]
- Kayembe DL, Kasonga DL, Kayembe PK, Mwanza JC, Boussinesq M. Profile of eye lesions and vision loss: a cross-sectional study in Lusambo, a forest-savanna area hyperendemic for onchocerciasis in the Democratic Republic of Congo. Trop Med Int Health. 2003, 8, 83–89. [CrossRef]
- Shivalingaiah PR, Veerabhadraiah P, et al. Onchocerciasis in the Orbital Region: An Unexpected Guest From Tropics. Int J Head Neck Surg 2018, 9, 137–139. [CrossRef]
- Cooper PJ, Guderian RH, Proaño R, Taylor DW. The pathogenesis of chorioretinal disease in onchocerciasis. Parasitology Today 1997, 13, 94–98. [CrossRef]
- Thylefors B, Tønjum AM. Visual field defects in onchocerciasis. Br J Ophthalmol. 1978, 62, 462–467. [CrossRef]
- Cousens SN, Yahaya H, Murdoch I, Samaila E, Evans J, Babalola OE, Zakari M, Abiose A, Jones BR. Risk factors for optic nerve disease in communities mesoendemic for savannah onchocerciasis, Kaduna State, Nigeria. Trop Med Int Health. 1997 Jan;2(1):89-98. [CrossRef]
- Abiose A, Jones BR, Cousens SN, Murdoch I, Cassels-Brown A, Babalola OE, Alexander ND, Nuhu I, Evans J, Ibrahim UF, et al. Reduction in incidence of optic nerve disease with annual ivermectin to control onchocerciasis. Lancet. 1993 Jan 16;341(8838):130-4. [CrossRef]
- Jittamala P, Monteiro W, Smit MR, Pedrique B, Specht S, Chaccour CJ, Dard C, Del Giudice P, Khieu V, Maruani A, Failoc-Rojas VE, Sáez-de-Ocariz M, Soriano-Arandes A, Piquero-Casals J, Faisant A, Brenier-Pinchart MP, Wimmersberger D, Coulibaly JT, Keiser J, Boralevi F, Sokana O, Marks M, Engelman D, Romani L, Steer AC, von Seidlein L, White NJ, Harriss E, Stepniewska K, Humphreys GS, Kennon K, Guerin PJ, Kobylinski KC. A systematic review and an individual patient data meta-analysis of ivermectin use in children weighing less than fifteen kilograms: Is it time to reconsider the current contraindication? PLoS Negl Trop Dis. 2021 Mar 17;15(3):e0009144. [CrossRef]
- Bakajika D, Kanza EM, Opoku NO, Howard HM, Mambandu GL, Nyathirombo A, Nigo MM, Kennedy KK, Masembe SL, Mumbere M, Kataliko K, Bolay KM, Attah SK, Olipoh G, Asare S, Vaillant M, Halleux CM, Kuesel AC. Effect of a single dose of 8 mg moxidectin or 150 μg/kg ivermectin on O. volvulus skin microfilariae in a randomized trial: Differences between areas in the Democratic Republic of the Congo, Liberia and Ghana and impact of intensity of infection. PLoS Negl Trop Dis. 2022 Apr 27;16(4):e0010079. [CrossRef]
- Kura K, Milton P, Hamley JID, Walker M, Bakajika DK, Kanza EM, Opoku NO, Howard H, Nigo MM, Asare S, Olipoh G, Attah SK, Mambandu GL, Kennedy KK, Kataliko K, Mumbere M, Halleux CM, Hopkins A, Kuesel AC, Kinrade S, Basáñez MG. Can mass drug administration of moxidectin accelerate onchocerciasis elimination in Africa? Philos Trans R Soc Lond B Biol Sci. 2023 Oct 9;378(1887):20220277. [CrossRef]
- Chan CC, Nussenblatt RB, Kim MK, Palestine AG, Awadzi K, Ottesen EA. Immunopathology of ocular onchocerciasis. 2. Anti-retinal autoantibodies in serum and ocular fluids. Ophthalmology. 1987, 94, 439–43. [CrossRef]
- Van der Lelij A, Rothova A, Stilma JS, Hoekzema R, Kijlstra A. Cell-mediated immunity against human retinal extract, S-antigen, and interphotoreceptor retinoid binding protein in onchocercal chorioretinopathy. Invest Ophthalmol Vis Sci. 1990, 31, 2031–6.
- Braun G, McKechnie NM, Connor V, Gilbert CE, Engelbrecht F, Whitworth JA, Taylor DW. Immunological crossreactivity between a cloned antigen of Onchocerca volvulus and a component of the retinal pigment epithelium. J Exp Med. 1991, 174, 169–177. [CrossRef]
- McGillan P, Berry NG, Nixon GL, Leung SC, Webborn PJH, Wenlock MC, Kavanagh S, Cassidy A, Clare RH, Cook DA, Johnston KL, Ford L, Ward SA, Taylor MJ, Hong WD, O'Neill PM. Development of Pyrazolopyrimidine Anti-Wolbachia Agents for the Treatment of Filariasis. ACS Med Chem Lett. 2021, 12, 1421–1426. [CrossRef]
- Saint André AV, Blackwell NM, Hall LR, Hoerauf A, Brattig NW, Volkmann L, Taylor MJ, Ford L, Hise AG, Lass JH, Diaconu E, Pearlman E. The role of endosymbiotic Wolbachia bacteria in the pathogenesis of river blindness. Science. 2002, 295, 1892–1895.
- Semba RD, Donnelly JJ, Rockey JH, Lok JB, Sakla AA, Taylor HR. Experimental ocular onchocerciasis in cynomolgus monkeys. II. Chorioretinitis elicited by intravitreal Onchocerca lienalis microfilariae. Invest Ophthalmol Vis Sci. 1988, 29, 1642–1651.
- Gyasi ME, Okonkwo ON, Tripathy K. Onchocerciasis. 2023 Feb 22. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan–. [PubMed]
- Cho YJ, Lee DH, Kang HM, Kim M, Koh HJ. Reversal of early central retinal vein occlusion by alleviating optic nerve edema with an intravitreal dexamethasone implant. Korean J Ophthalmol. 2014, 28, 192–193. [CrossRef]
- Murdoch I, Abiose A, Babalola O et al. Ivermectin and onchocercal optic neuritis: Short-term effects. Eye 1994, 8, 456–461. [CrossRef]
- Showler AJ, Nutman TB. Imported onchocerciasis in migrants and travelers. Curr Opin Infect Dis. 2018, 31, 393–398. [CrossRef]
- Schwartz RA, Al-Qubati Y, Zieleniewski Ł, Shah R, Kapila R. Onchocerciasis (river blindness): larva-induced eczema (onchodermatitis) from an important oculocutaneous tropical disease spilling over into North America and Europe. Int J Dermatol. 2020, 59, 1065–1070. [CrossRef]
- 51. Aziz MA, Diallo S, Diop IM, Lariviere M, Porta M. Efficacy and tolerance of ivermectin in human onchocerciasis. Lancet, 1982; 2: 171–173.
- Brattig, N.W.; Cheke, R.A.; Garms, R. Onchocerciasis (river blindness) – more than a century of research and control. Acta Tropica 2021, 218, 105677. [Google Scholar] [CrossRef]
- Korten, S.; Badusche, M.; Büttner, D.W.; et al. Natural death of adult Onchocerca volvulus and filaricidal effects of doxycycline induce local FOXP3+/CD4+ regulatory T cells and granzyme expression. Microbes Infect. 2008, 10, 313–324. [Google Scholar] [CrossRef]
- Mackenzie, C.D. A Much-Needed Advance in the Diagnosis of River Blindness. J Infect Dis. 2020, 221, 1746–1748. [Google Scholar] [CrossRef]
- Hedtke, S.M.; Choi, Y.J.; Kode, A.; Chalasani, G.C.; Sirwani N, Jada SR, Hotterbeekx A, Mandro M, Siewe Fodjo JN, Amambo GN, Abong RA, Wanji S, Kuesel AC, Colebunders R, Mitreva M, Grant WN. Assessing Onchocerca volvulus Intensity of Infection and Genetic Diversity Using Mitochondrial Genome Sequencing of Single Microfilariae Obtained before and after Ivermectin Treatment. Pathogens. 2023, 12, 971. [Google Scholar] [CrossRef]
- El-Sayed, N.M.; Elmeya Hassan Safar, E.H. Characterization of the parasite-induced lesions in the posterior segment of the eye. Indian J Ophthalmol. 2015, 63, 881–887. [Google Scholar] [CrossRef]
- Pizem, H.; Ben-Arie-Weintrob, Y.; Naaman, E. Neuroretinitis with secondary retinal venous stasis in a patient with Schistosomiasis. Am J Ophthalmol Case Rep. 2022, 25, 101355. [Google Scholar] [CrossRef]
- Agarwal, M.; Jha, V.; Chaudhary, S.P.; Singh, A.K. Multifocal cysticercosis with optical coherence tomography findings in a child. Middle p East Afr J Ophthalmol. 2012, 19, 240–242. [Google Scholar] [CrossRef]
- Ramírez-Soto, M.C.; Tirado-Sánchez. A.; Bonifaz, A. Ocular Sporotrichosis. J Fungi (Basel). 2021, 7, 951. [Google Scholar] [CrossRef]
- Glasgow, B.J. , Brown, H.H., Foos, R.Y. Miliary retinitis in coccidioidomycosis. Am J Ophthalmol. 1987, 104, 24–27. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual authors and contributors and not of MDPI and/or the editors. MDPI and/or the editors disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
Figure 1.
Subretinal tracts of microfilaria of right eye in Case 1 (white dots and blue stars on fluorescein angiography (FA) and right eye of Case 2 (white arrows on fundus photography).
Figure 1.
Subretinal tracts of microfilaria of right eye in Case 1 (white dots and blue stars on fluorescein angiography (FA) and right eye of Case 2 (white arrows on fundus photography).
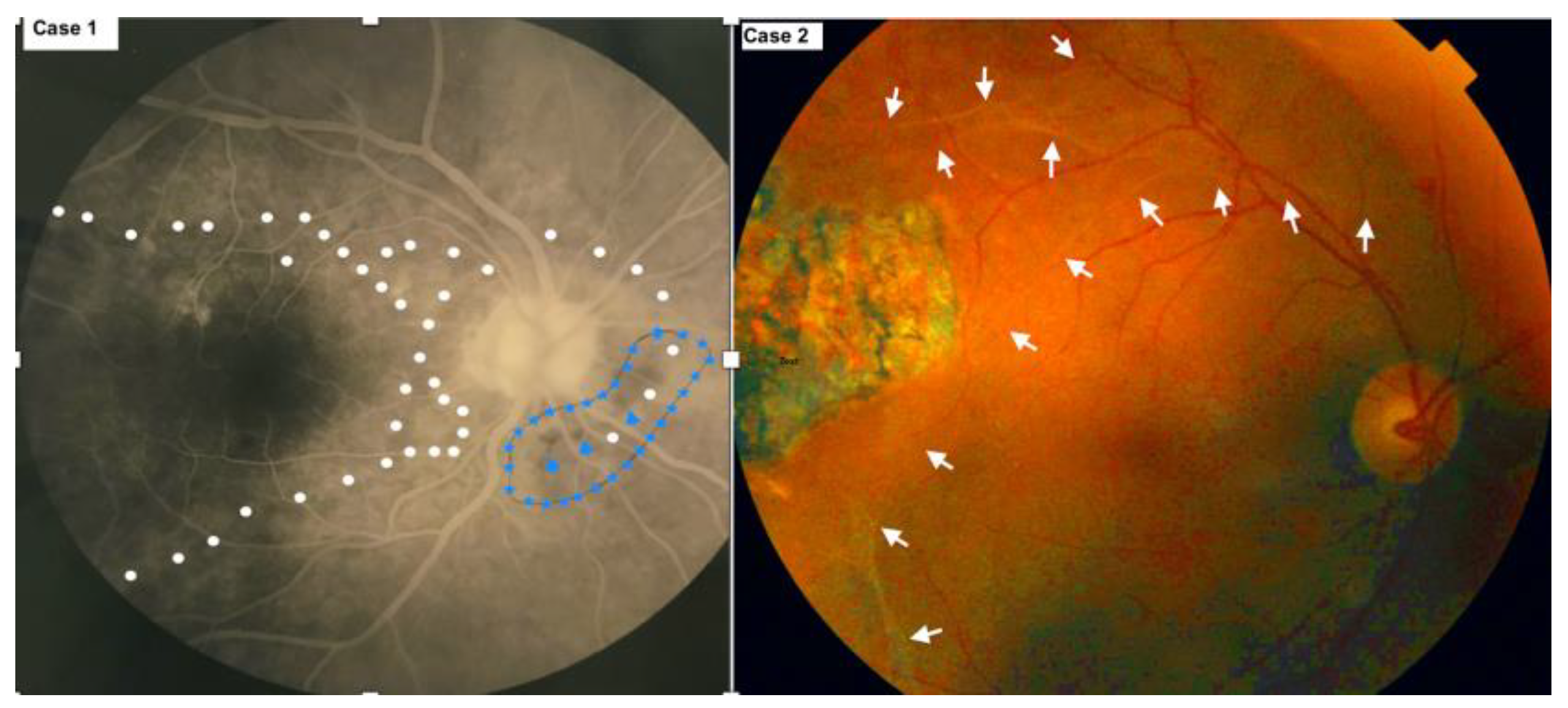
Figure 2.
(Case 1; right FA). 12 year followup showing the new onset of peripapillary atrophy.
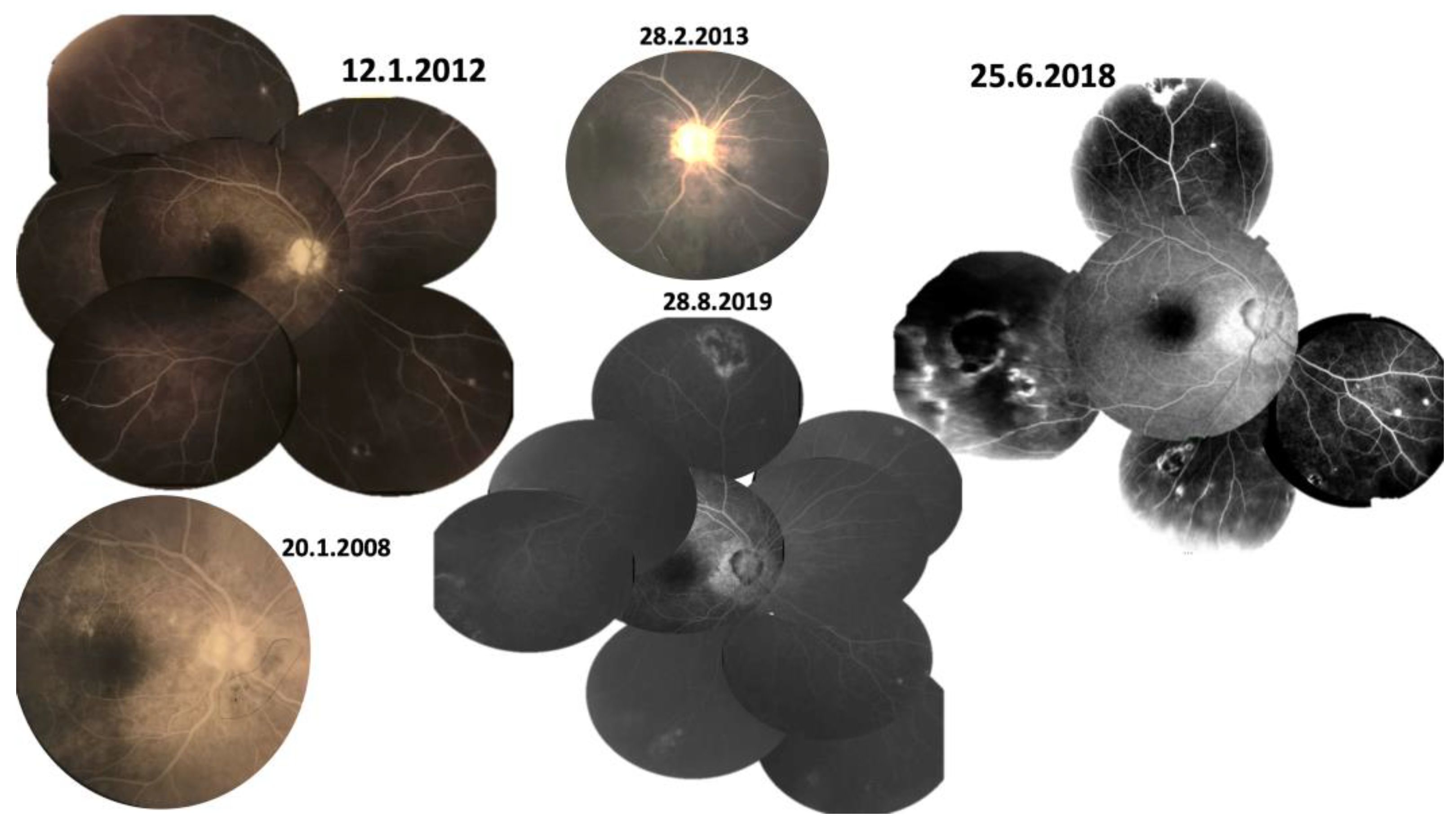
Figure 3.
(Case 1; left FA). 12 year followup showing active vitritis at 12 year followup with optic nerve and peripapillary inflammation with one new focus of retinitis superiorly (arrowhead). Torpedo or round lesions are noted at the equator with central blocking fluorescence and a surround with fluorescein staining.
Figure 3.
(Case 1; left FA). 12 year followup showing active vitritis at 12 year followup with optic nerve and peripapillary inflammation with one new focus of retinitis superiorly (arrowhead). Torpedo or round lesions are noted at the equator with central blocking fluorescence and a surround with fluorescein staining.
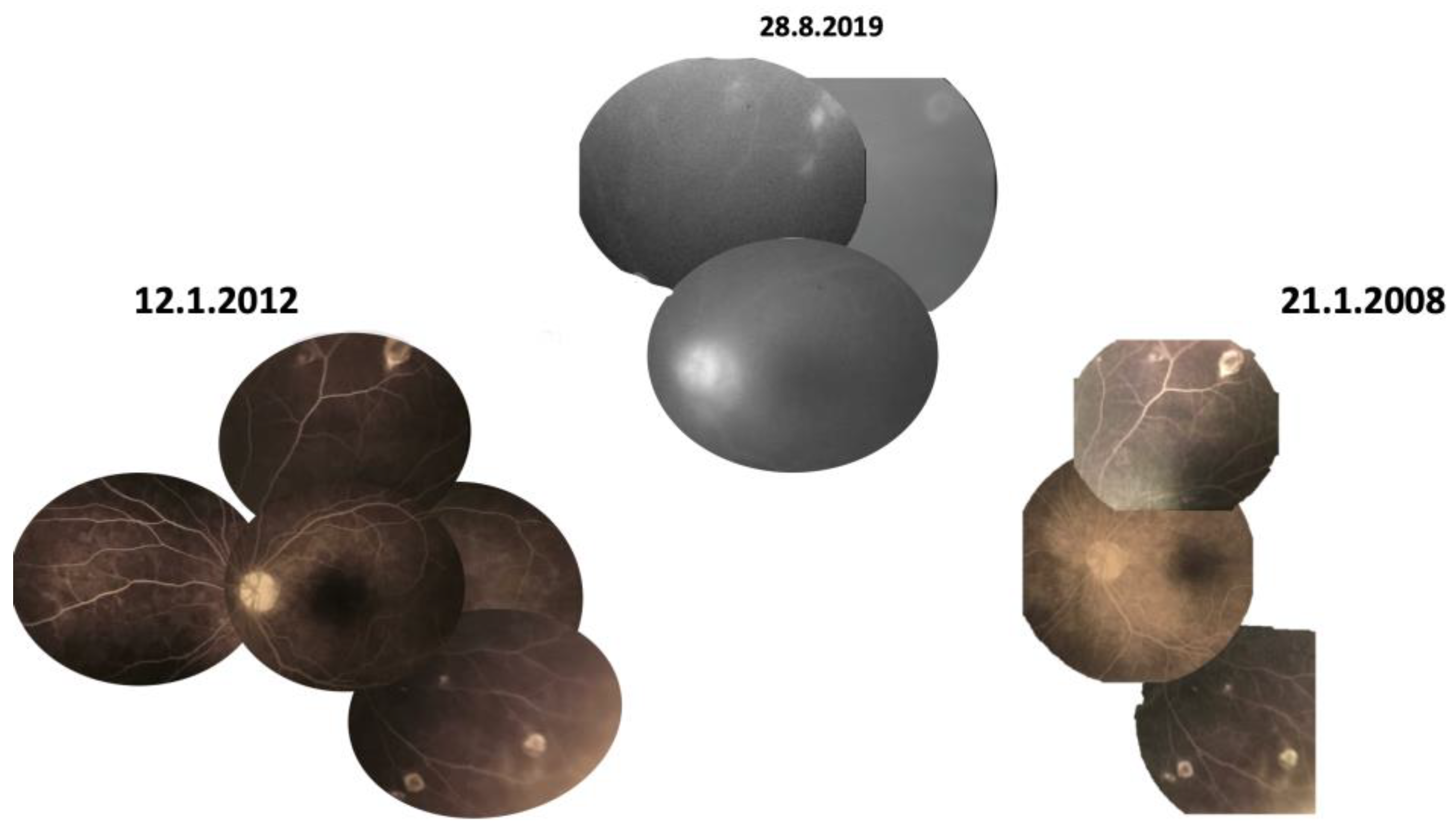
Figure 4.
(Case 1). Montage of the right fundus on 7.10.2020. Noted are the following: Optic pallor, One disc diameter of peripapillary atrophy with pigment stipling; Retinal arterial attenuation; Small yellowish pinpoint or coin shaped lesions at the equator; Multifocal pigment-centered lesions with yellow surround or yellow-centered lesions with pigment surround.
Figure 4.
(Case 1). Montage of the right fundus on 7.10.2020. Noted are the following: Optic pallor, One disc diameter of peripapillary atrophy with pigment stipling; Retinal arterial attenuation; Small yellowish pinpoint or coin shaped lesions at the equator; Multifocal pigment-centered lesions with yellow surround or yellow-centered lesions with pigment surround.
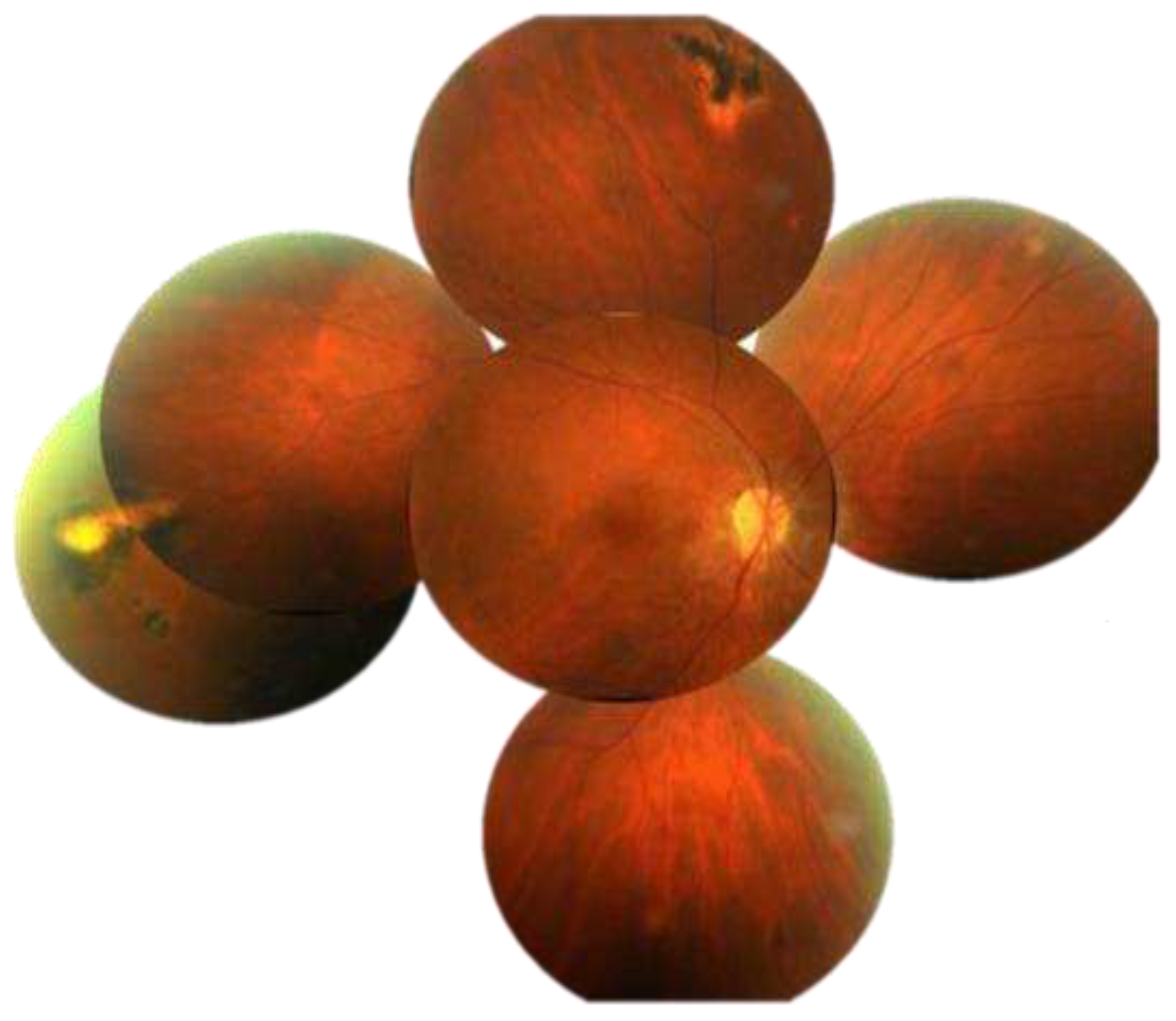
Figure 5.
OCT macula, optic disc and fundus autofluorescence on 25.6.2028. Disorganization of nasal macula with atrophy of superficial retina and dissolution of the outer peripapillary retina. Subclinical disc swelling is well noted by SD-OCT. Peripapillary ring of hypo-autofluorescence is characteristic of onchocerciasis chorioretinitis. .
Figure 5.
OCT macula, optic disc and fundus autofluorescence on 25.6.2028. Disorganization of nasal macula with atrophy of superficial retina and dissolution of the outer peripapillary retina. Subclinical disc swelling is well noted by SD-OCT. Peripapillary ring of hypo-autofluorescence is characteristic of onchocerciasis chorioretinitis. .
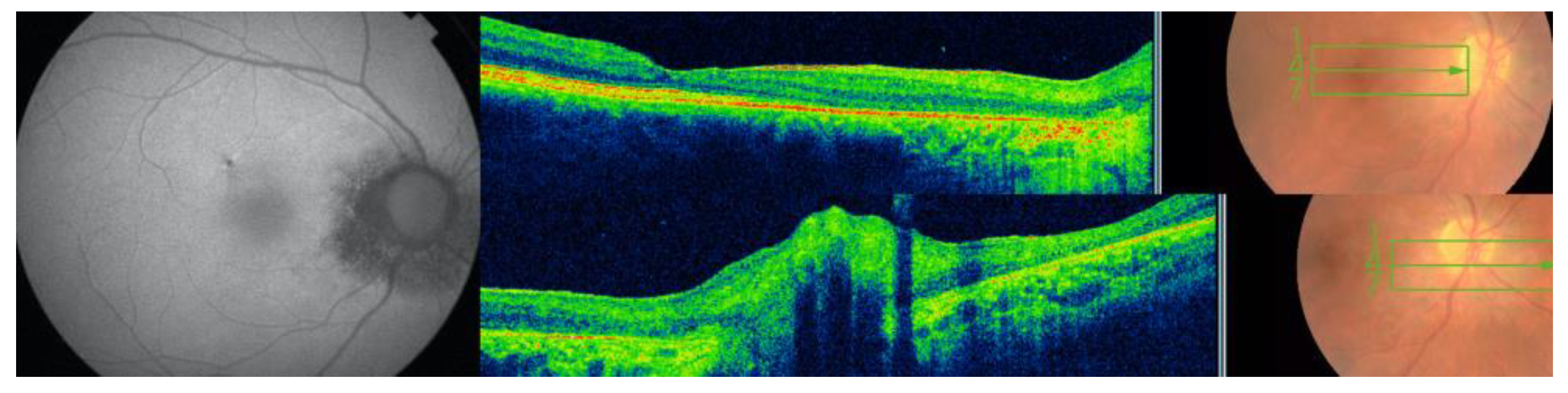
Figure 6.
(Case 2). Montage of fundus photograph and fundus autofluorescence of both eyes show small lesion beside large geographic lesions temporal to the fovea right eye and superior to the fovea left eye.
Figure 6.
(Case 2). Montage of fundus photograph and fundus autofluorescence of both eyes show small lesion beside large geographic lesions temporal to the fovea right eye and superior to the fovea left eye.
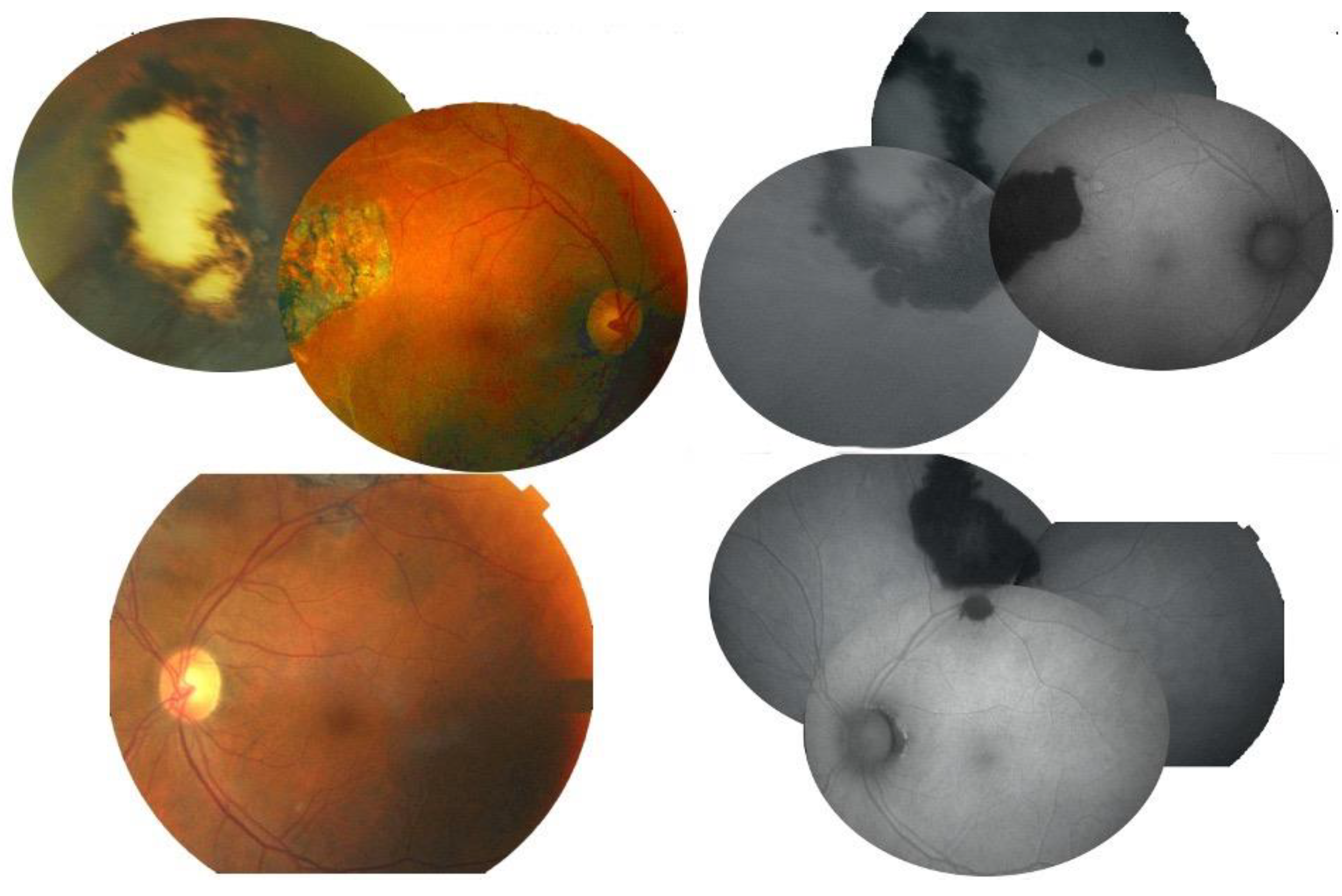
Figure 8.
(Case 3). The right eye had microfilaria tract superotemporally, crystalline deposit in fovea, patchy ellipsoid zone disruption, vasculitis with perivascular pigmentary deposit.
Figure 8.
(Case 3). The right eye had microfilaria tract superotemporally, crystalline deposit in fovea, patchy ellipsoid zone disruption, vasculitis with perivascular pigmentary deposit.
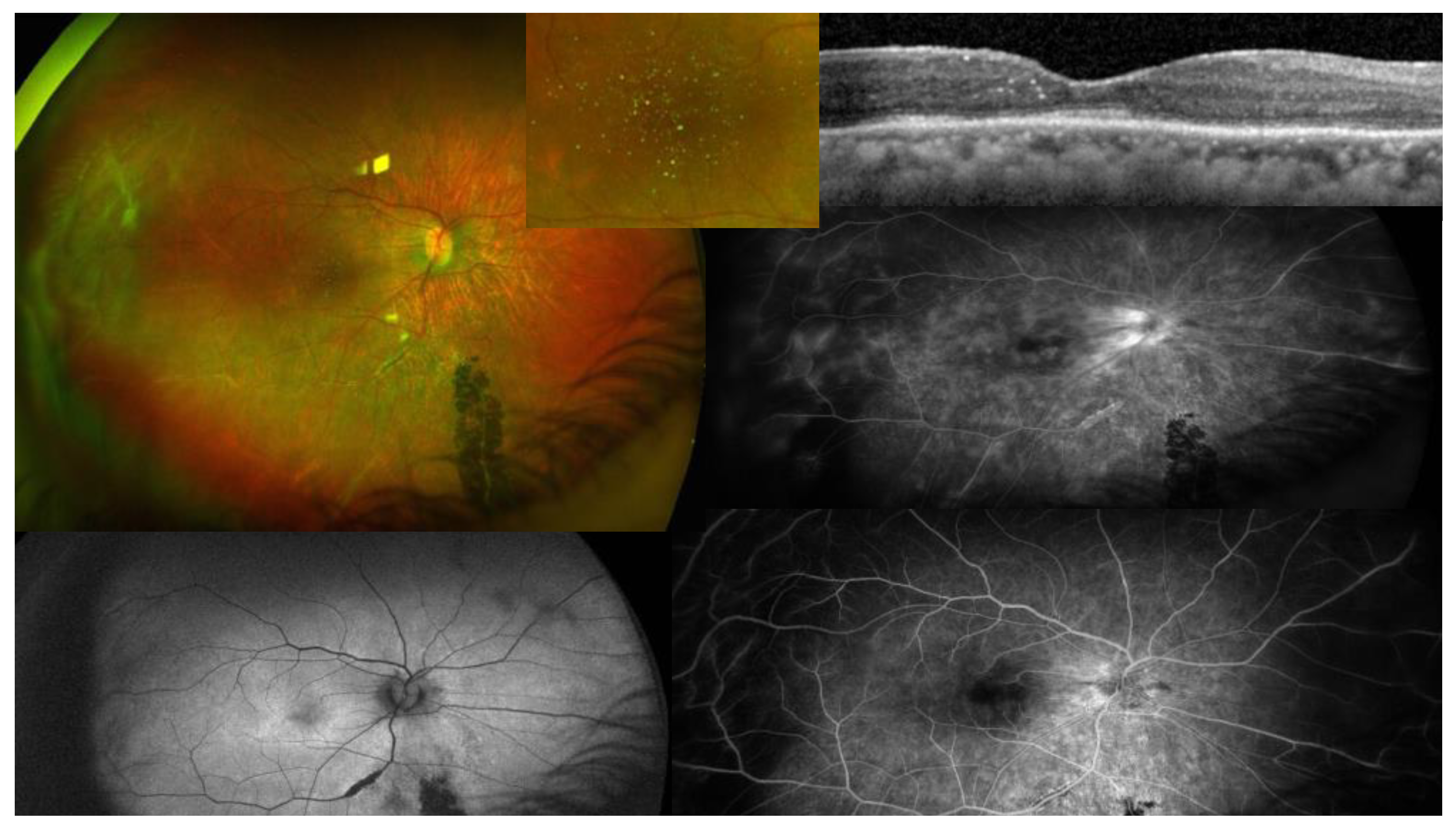
Figure 9.
Case 4 composite of fundus photographs, FA, auto fluorescence and OCT.

Table 1.
Ocular findings in onchocerciasis.
| Site | Findings | Frequency | References |
|---|---|---|---|
| Adnexa | Adnexal nodule | Rare | 32 |
| Conjunctiva | conjunctivitis | common | |
| phlyctenule | common | ||
| microfilaria | common | ||
| Cornea | motile microfilaria | 13.8%-95.7% | 7, 29, 31 |
| punctate keratitis (snowflake) | 13.80% | 16, 31 | |
| sclerosing keratitis | 5% | 16 | |
| neovascularization | rare | ||
| Sclera | microfilaria | rare | 27 |
| Anterior chamber | motile microfilaria | 13,6%-40% | 7, 16 |
| glaucoma | 1.60% | 16 | |
| iridocyclitis | 8% | 31 | |
| Lens | Cataract | infrequent | |
| Vitreous | microfilariae | infrequent | 27 |
| Optic disc | optic neuritis | 1%-5.5% | 16 |
| optic atrophy | 5.1%-57% | 16, 28, 35 | |
| microfilariae | rare | 28 | |
| epipapillary fibrosis | uncommon | 29 | |
| Retina-choroid | chorioretinitis | 38%-75% | 15, 29 |
| peripapillary atrophy | 9%-25% | 28, 29 | |
| mottled fundus | common | 29 | |
| retinal vasculitis | 1% | 16 | |
| retina tracts | 10% | 16 | |
| white intraretinal deposit | 21.40% | 16 | |
| microfilaria | rare | 27 |
N.B. Results vary according to cross sectional vs longitudinal design, degree of fly infestation, length of follow-up, study design (field vs. clinic exam), age and gender of participants.
Table 2.
Comparison between experimental [26, 45] and human onchocerciasis [15, 46].
| Model | Monkey | Human |
|---|---|---|
| Uveitis | Common | Common |
| RPE changes | ||
| Common | Common | |
| Disc edema/Atrophy | ||
| Common | Common | |
| Retinal vasculitis | Common | Infrequent |
| Venous engorgement | Frequent | Uncommon |
| Retinal hemorrhages | Common | Uncommon |
| Histopathology | Eosinophilic choroiditis | Eosinophilic choroiditis [27, 28] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



