
Submitted:
08 October 2023
Posted:
09 October 2023
You are already at the latest version
Abstract
Introduction and Problem: With conventional mechanical rotation measurement of joints, only static measurements are possible with the patient at rest. In the future, however, it would be interesting to carry out dynamic rotation measurements, for example when walking or doing sports. Therefore, a measurement method with an elastic capacitive measuring system was developed and validated. Material and Methods: The measurement system consists of a capacitive strain gauge connected to a flexible printed circuit board. The electronics on the printed circuit board are used for data acquisition and transmission. When the sensor strip is stretched, the distance between the fingers of the strain gauge changes and with it the capacitance. Consequently, the strain can be measured via the change in capacitance. The measurement system is taped to the knee with the sensor on the skin in the direction of the anterolateral ligament (ALL). The bottom of the sensor (silicone) and the bottom of the circuit board are in contact with the knee surface. The sensor must be attached to the knee without pre-stretching The system is validated with an in vivo test on 11 patients. For this purpose, the internal rotational laxity of the knee was tested on healthy volunteers and the results compared with the measurements on the static measuring device (Laxitester). The subjects are placed in the supine position. First the left and then the right leg is clinically examined one after the other and documented using an examination form. Exclusion criteria are the presence of a pathological ligament findings in the area of the collateral/cruciate ligaments, previous knee operations or limitations in the range of motion. The distal thigh rests on a support bench on which a knee joint flexion of 30° is set by height adjustment. The femoral condyles are secured against rotation in the positioning aid by posts. This also prevents internal rotation and displacement of the thigh. The foot is strapped into the holding device without shoes. The second toe beam is centered using an adjustable side clamp on the medial and lateral edge of the foot. Dorsiflexion is set at 2 Nm with a torque meter, in accordance with previous studies, to rule out rotational laxity in the ankle. The strain gauge sensor is taped to Gerdii’s tubercle in the course of the antero-lateral ligament below the lateral epicondyle of the thigh. Then, in three repeated measurements, the internal rotation of the foot and thus the lower leg is measured with a torque of 2 Nm. The change in length of the stretch mark is compared with the measured internal rotation angle in the static measuring device (Laxitester). Results: A significant difference between the sexes was found in the internal rotation range of the knee (p=0.003). The range of rotation was greater for female participants than for male participants. Regarding the measured length change values, the measurements presented showed an individual result for each participant, which tended to decrease with increasing internal rotation angle, with no age or gender differences being observed. The stiffness of the strain gauge was in the linear range for all measurements, within the first 20% strain of the sensor. The differences determined do not result from a different stretching of the sensor, but from individual differences between the test persons. The comparison between length change and internal rotation angle of the knee showed a strong positive correlation (r=1, p<0.01). Conclusion: Elastic capacitive strain gauges can be used to reliably measure the internal rotation angle of the knee joint. This will allow dynamic measurements in the future.
Keywords:
laxitx measuremenrt knee
; straingauges
; anterolateral ligament knee
; elastic capacitive measuring system
1. Introduction
The increase in recreational sports activities such as jogging and running over the past decade has also led to a corresponding increase in knee injuries. Among these, one of the most common knee injuries is a tear of the anterior cruciate ligament (ACL), which accounts for 20% of all knee injuries [1]. In Germany, 76,935 arthroscopic and 3192 open surgical ligamentoplasties were performed on the knee joint in 2022 [2]. This compares with 43,360 cases in 2012 [3]. In the United States, 78 cases per 100,000 population were reported for 2022, for a total of 256,000 injuries in 328 million people [4] and 6.5 cases per 100,000 people in 2012 [5]. Therefore, in recent decades, the importance of devices and methods for measuring knee laxity caused by ACL rupture has been increased. Currently, there are several examination methods for diagnosing ACL ruptures caused by internal rotation of the tibia: the physical examination and instrumental measurement methods. The physical examination includes the Lachman test, the pivot shift test, and the anterior drawer test. These methods measure the range of motion between the stationary (upper) and mobile (lower) knee to analyze the degree of laxity [6]. These physical examination methods are standardized in principle, but results often vary and depend on examiners. A well-known technical instrument for measuring rotational laxity of the knee is the KT-1000 arthrometer, developed in the 1980s by MEDmetric Corp. The instrument is strapped to the leg, and the examiner uses a handle to pull the tibia forward with different forces. The instrument is used to measure the rotational laxity of the knee. However, many studies have reported poor reproducibility [7] and results that differ from clinical findings [8]. The conventional mechanical rotation measurement of joints were only static measurements, that are possible when the patient is at rest. However, these measurements for measuring knee laxity are not repeatable [9,10,11] and are strongly influenced by the experience of the physician performing the measurement [12,13,14]. In the future, however, it would be interesting to perform dynamic rotational measurements, for example during walking or sports. Therefore, a measurement method with an elastic-capacitive measurement system was developed and validated.
2. Materials and Methods
2.1. Materials
The polymer-based sensor is fabricated using carbon black polydimethylsiloxane (C-PDMS) on the sensing part and pure PDMS as the substrate. PDMS, obtained from the blend of two base materials, was used for the substrate. Two silicones, Neukasil® RTV-23 and RTV-17 (both from Altropol Kunststoff GmbH, Stockelsdorf, Germany), were mixed in a weight ratio of 10:4 and degassed to release all the air bubbles. For the conductive layer, an electrically conductive PDMS blend, called here C-PDMS (Carbon black-PDMS), was obtained by further mixing this silicone blend with 10.6 wt% carbon black powder ENSACO® 250 P (TIMCAL Ltd., Bodio, Switzerland).
2.2. Methods
The production of the polymer-based capacitive strain gauge as well as the printed circuit board was carried out as already described by us [15]. The C-PDMS and PDMS were stirred for 10 minutes with a blade mixer at 1200 rpm. The mixture obtained was highly viscous, which caused the material to distribute unevenly in the mold. Therefore, the viscosity of this mixture was reduced by adding 2.04 g of n-heptane. Neukasil silicone was used to fabricate the sensor. A mushroom-shaped aluminum pin was embedded for electrical contact. Molds with holes are used for the fabrication process (10 holes with a diameter of 1.05 mm and a depth of 1.40 mm) to accommodate rigid electrical contacts during molding of a C-PDMS layer. The rigid electronic contacts are manufactured from aluminum using a CNC machine. They have a mushroom-like shape with small holes in their apex to ensure good mechanical fixation and electrical connection during embedding in the C-PDMS layer. To ensure a stable connection with the C-PDMS even during sensor extension, the contact pads are coated with a primer (NuSil SP-120, Silicon Primer, Songhan Plastic Technology Co., Ltd., Shanghai, China). While the slim base of the contact is placed in the holes in the mold, the crown protrudes into the mold cavity to be surrounded by C-PDMS from all sides and through its holes.
The measurement system consists of a polymer-based capacitive strain gauge connected to a flexible printed circuit board. The electronics on the printed circuit board were used for data acquisition and transmission. When the sensor strip is stretched, the distance between the fingers of the strain gauge changes and with it the capacitance. Consequently, the strain can be measured via the change in capacitance as described previously [15]. The measurement system was taped to the knee with the sensor on the skin in the direction of the anterolateral ligament (ALL). The bottom of the sensor (silicone) and the bottom of the circuit board were in contact with the knee surface. The sensor must be attached to the knee without pre-stretching (please see Figure 1).
The system was validated with an in vivo test on 10 subjects (5 females/5 males). For this purpose, the internal rotational laxity of the knee was tested on healthy volunteers and the results compared with the measurements on the static measuring device (Laxitester). The subjects were placed in the supine position. First the left and then the right leg was clinically examined one after the other and documented using an examination form. Exclusion criteria were the presence of a pathological ligament findings in the area of the collateral/cruciate ligaments, previous knee operations or limitations in the range of motion. The distal thigh rests on a support bench on which a knee joint flexion of 30° was set by height adjustment. The femoral condyles were secured against rotation in the positioning aid by posts. This also prevents internal rotation and displacement of the thigh. The foot was strapped into the holding device without shoes (see Figure 2). The second toe beam was centered using an adjustable side clamp on the medial and lateral edge of the foot. Dorsiflexion is set at 2 Nm with a torque meter, in accordance with previous studies [16,17], to rule out rotational laxity in the ankle. The polymer-based strain gauge sensor was taped to the Gerdii´s tubercle in the course of the antero-lateral ligament below the lateral epicondyle of the thigh. Then, in three repeated measurements, the internal rotation of the foot and thus the lower leg was measured with a torque of 2 Nm. The change in length of the stretch mark was compared with the measured internal rotation angle in the static measuring device (Laxitester) (please see Figure 2).
The actual measurement was performed stepwise in 5°, with at least 20 seconds being spent in the position after each step before the next 5° step was taken until the maximum knee rotation of the respective subject was reached. Using calibration curves as already described in a previous work [15,18], the conversion of the clock-ticks into length change [mm] was carried out.
3. Results
The measurements showed a highly significant correlation between the purely mechanical measurement under maximum force and the digital measurement during dynamic examination with strain gauges (see Figure 3). Furthermore, a significant difference in laxity was found between men and women (Table 1).
If we look at the results in Table 1, we see clear differences between the genders. The internal knee rotation of the women allows up to 45° in some cases, whereas only 25° is possible for most of the men. In addition, different values for the change in length were found for the same angle of rotation. The reason for this was the different sizes of the test subjects. When analyzing the data, it became apparent, that it was necessary to mathematically correct the changes in length recorded using the polymer-based capacitive strain gauges depending by the leg circumference of the person examined (see Figure 4). This means that in order to convert the change in length to an angle measure, this correction factor must be taken into account.
4. Discussion
The Laxitester can only be used to measure the dorsiflexion when applying the maximum force (2 Nm) - other statements cannot be made. The advantage of digital measurement using polymer-based capacitive strain gauges compared to mechanical internal rotation measurement with a fixed internal rotation force is that a linear measurement of internal rotation laxity is possible without applying a maximum force [10,19]. In addition, the measurements were reproducible [9,10,11] and independent of the investigator [12,13,14], one of the main points of criticism in the previous knee laxity measurements. The only dependence of the values is the size of the subject, which could be corrected by the correction factor (knee circumference). After calibration has been performed for each patient, the strain gauges can also be used for other dynamic measurements such as walking, running or stair climbing.
5. Conclusions
In the current study, the method using polymer-based capacitive strain gauges demonstrated high validity in measuring the dynamic internal rotation laxity of the knee joint. The measurements were reproducible and independent of the investigator. To compensate for individual differences between subjects, a correction factor (knee circumference) was included.
Author Contributions
Conceptualization, H.O.M and M.S.; methodology: H.O.M and M.S., software: K.S.P. and L.C.; validation: H.O.M and M.S.; formal analysis: H.O.M and M.S.; investigation: N.R. and K.S.P.; resources: H.O.M and M.S.; data curation: K.S.P, H.O.M and M.S.; writing—original draft preparation: H.O.M and M.S.; writing—review and editing: H.O.M and M.S.; visualization: H.S.; supervision: P.W.; project administration: H.S.; funding acquisition: H.O.M and P.W.; All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the German Science Foundation (DFG), grant number 222567169 and The APC was funded by the Baden-Wuerttemberg Ministry of Science, Research and Art and the University of Freiburg in the funding program Open Access Publishing.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of the Albert-Ludwigs-University Freiburg (approval number 487/16).
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Boden, B.P.; Sheehan, F.T. Mechanism of non-contact acl injury: Oref clinical research award 2021. 2022, 40, 531–540. [CrossRef]
- destatis. Fallpauschalenbezogene krankenhausstatistik (drg-statistik) operationen und prozeduren der vollstationären patientinnen und patienten in krankenhäusern (4-steller) für 2021. Office, G.F.S., Ed. Wiesbaden, 2022.
- destatis. Fallpauschalenbezogene krankenhausstatistik (drg-statistik) diagnosen, prozeduren, fallpauschalen und case mix der vollstationären patientinnen und patienten in krankenhäusen für 2012. Wiesbaden, 2013.
- Evans, J.; Nielson, J.I. Anterior cruciate ligament knee injury. [updated 2022 may 5]. In: Statpearls [internet]. Treasure island (fl): Statpearls publishing; 2023 jan-. Available from: Https://www.Ncbi.Nlm.Nih.Gov/books/nbk499848/. https://www.ncbi.nlm.nih.gov/books/NBK499848/ (09-26).
- Joseph, A.M.; Collins, C.L.; Henke, N.M.; Yard, E.E.; Fields, S.K.; Comstock, R.D. A multisport epidemiologic comparison of anterior cruciate ligament injuries in high school athletics. Journal of athletic training 2013, 48, 810–817. [Google Scholar] [CrossRef]
- Imhoff, A.; Linke, R.; Baumgartner, R. Checkliste orthopädie. Thieme: Stuttgart, Germany, 2021; Vol. 4. [CrossRef]
- Lam, M.H.; Fong, D.T.; Yung, P.; Ho, E.P.; Chan, W.Y.; Chan, K.M. Knee stability assessment on anterior cruciate ligament injury: Clinical and biomechanical approaches. Sports medicine, arthroscopy, rehabilitation, therapy & technology : SMARTT 2009, 1, 20. [Google Scholar] [CrossRef]
- Wiertsema, S.H.; van Hooff, H.J.; Migchelsen, L.A.; Steultjens, M.P. Reliability of the kt1000 arthrometer and the lachman test in patients with an acl rupture. Knee 2008, 15, 107–110. [Google Scholar] [CrossRef]
- Ahldén, M.; Samuelsson, K.; Fu, F.H.; Musahl, V.; Karlsson, J. Rotatory knee laxity. Clinics in sports medicine 2013, 32, 37–46. [Google Scholar] [CrossRef]
- Zens, M.; Niemeyer, P.; Bernstein, A.; Feucht, M.J.; Kühle, J.; Südkamp, N.P.; Woias, P.; Mayr, H.O. Novel approach to dynamic knee laxity measurement using capacitive strain gauges. Knee Surgery, Sports Traumatology, Arthroscopy 2015, 23, 2868–2875. [Google Scholar] [CrossRef]
- Mayr, H.O.; Stöhr, A. [current status of instrumental measurement of knee laxity]. Arthroskopie 2010, 23, 56–61. [Google Scholar] [CrossRef]
- Lange, T.; Freiberg, A.; Dröge, P.; Lützner, J.; Schmitt, J.; Kopkow, C. The reliability of physical examination tests for the diagnosis of anterior cruciate ligament rupture – a systematic review. Manual Therapy 2015, 20, 402–411. [Google Scholar] [CrossRef]
- Kuroda, R.; Hoshino, Y.; Kubo, S.; Araki, D.; Oka, S.; Nagamune, K.; Kurosaka, M. Similarities and differences of diagnostic manual tests for anterior cruciate ligament insufficiency:A global survey and kinematics assessment. 2012, 40, 91–99. [CrossRef]
- Branch, T.P.; Mayr, H.O.; Browne, J.E.; Campbell, J.C.; Stoehr, A.; Jacobs, C.A. Instrumented examination of anterior cruciate ligament injuries: Minimizing flaws of the manual clinical examination. Arthroscopy: The Journal of Arthroscopic & Related Surgery 2010, 26, 997–1004. [Google Scholar] [CrossRef]
- Sheeja Prakash, K.; Mayr, H.O.; Agrawal, P.; Agarwal, P.; Seidenstuecker, M.; Rosenstiel, N.; Woias, P.; Comella, L.M. Batch fabrication of a polydimethlysiloxane based stretchable capacitive strain gauge sensor for orthopedics. Polymers 2022, 14, 2326. [Google Scholar] [CrossRef]
- Mayr, H.O.; Hoell, A.; Bernstein, A.; Hube, R.; Zeiler, C.; Kalteis, T.; Suedkamp, N.P.; Stoehr, A. Validation of a measurement device for instrumented quantification of anterior translation and rotational assessment of the knee. Arthroscopy: The Journal of Arthroscopic & Related Surgery 2011, 27, 1096–1104. [Google Scholar] [CrossRef]
- Mayr, H.O.; Hellbruegge, G.; Haasters, F.; Ipach, B.; Schmal, H.; Prall, W.C. Laxity measurement of internal knee rotation after primary anterior cruciate ligament rupture versus rerupture. Archives of Orthopaedic and Trauma Surgery 2022, 142, 2839–2847. [Google Scholar] [CrossRef] [PubMed]
- Sheeja Prakash, K.; Andersen, E.; von Einem, V.C.; Muthalagu, S.K.; Agarwal, P.; Mayr, H.O.; Seidenstuecker, M.; Rosenstiel, N.; Roundy, S.; Woias, P. , et al. Design and implementation of a wearable system based on a flexible capacitive sensor, monitoring knee laxity. Advanced Sensor Research 2023, n/a, 2300058. [Google Scholar] [CrossRef]
- Zens, M.; Niemeyer, P.; Ruhhammer, J.; Bernstein, A.; Woias, P.; Mayr, H.O.; Südkamp, N.P.; Feucht, M.J. Length changes of the anterolateral ligament during passive knee motion: A human cadaveric study. The American Journal of Sports Medicine 2015, 43, 2545–2552. [Google Scholar] [CrossRef]
Figure 1.
Positioning of the sensor on the knee during measurements.
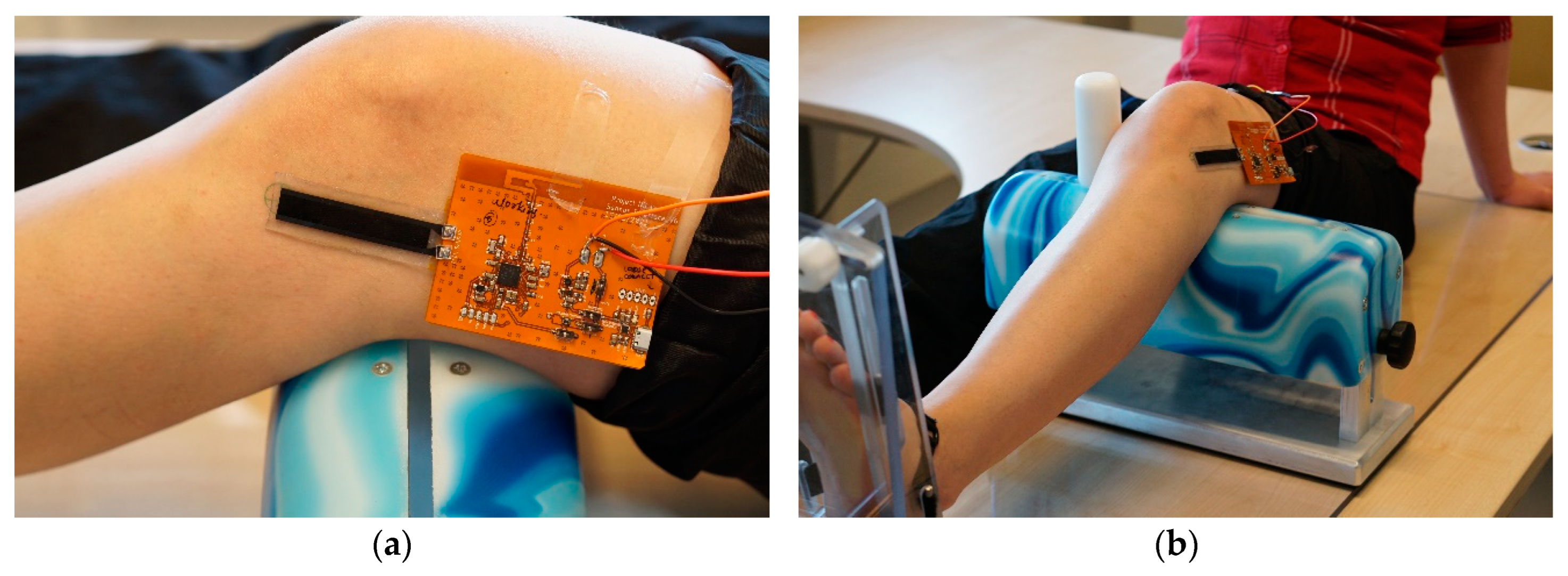
Figure 2.
Measurement of knee laxity on the laxity tester.
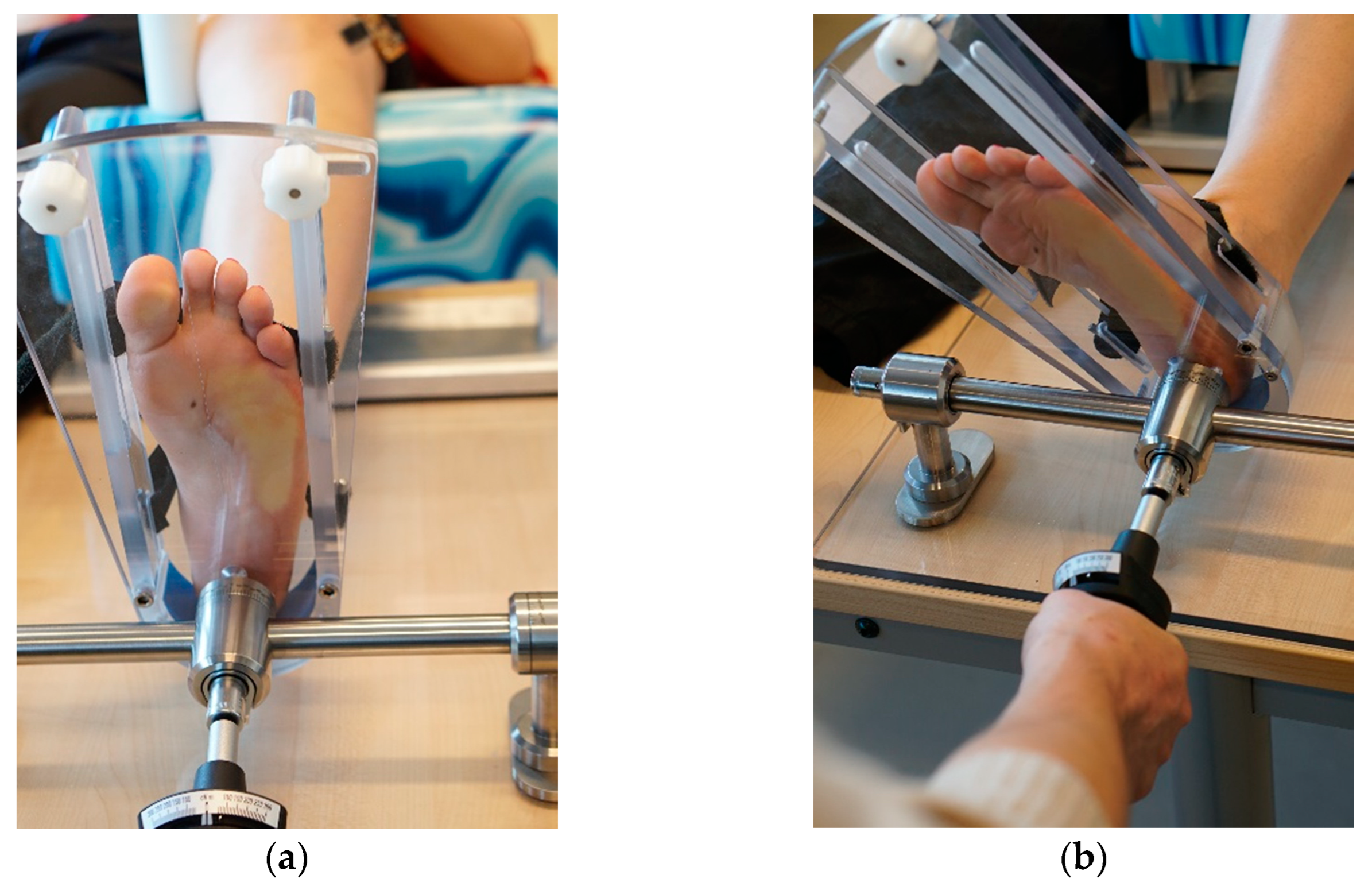
Figure 3.
comparison of the length change of the polymer-based capacitive strain gauge as a function of the internal knee rotation for all participants.
Figure 3.
comparison of the length change of the polymer-based capacitive strain gauge as a function of the internal knee rotation for all participants.
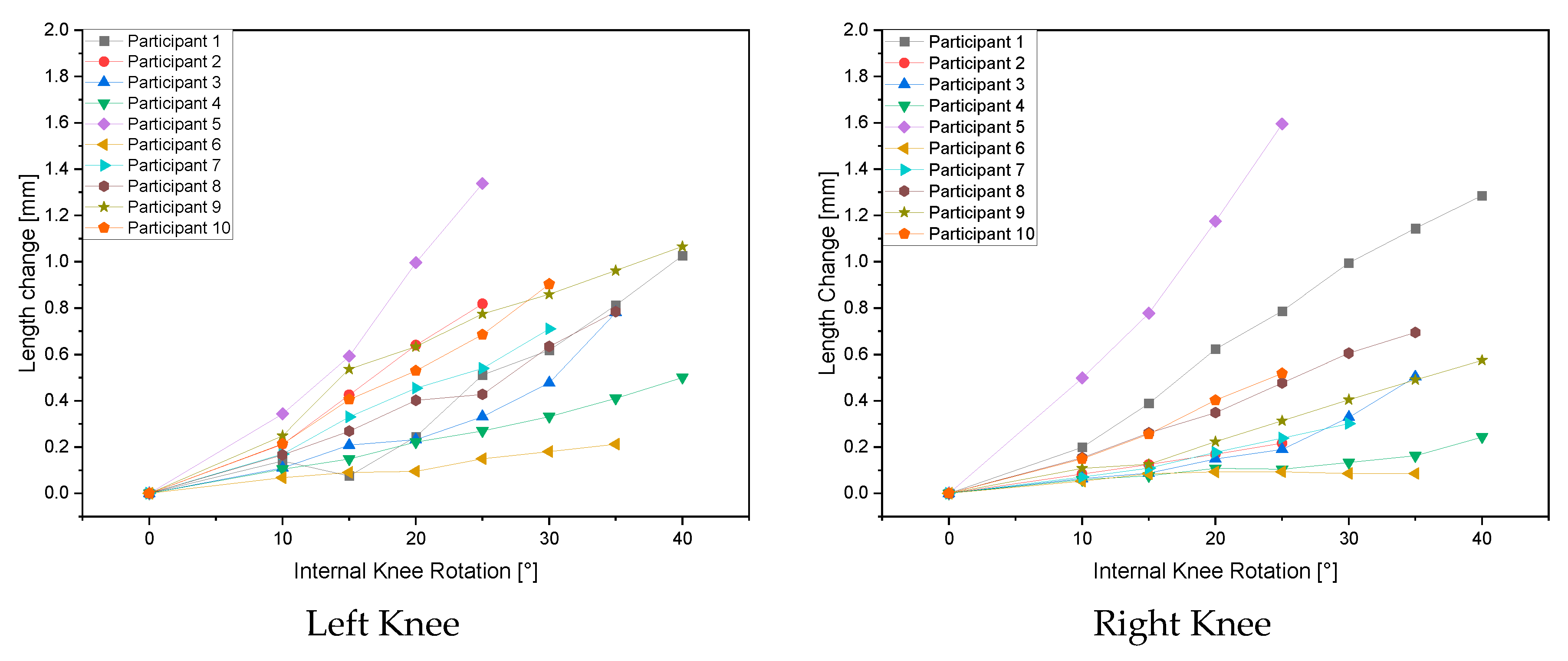
Figure 4.
Circumference corrected length change as function of internal knee rotation.
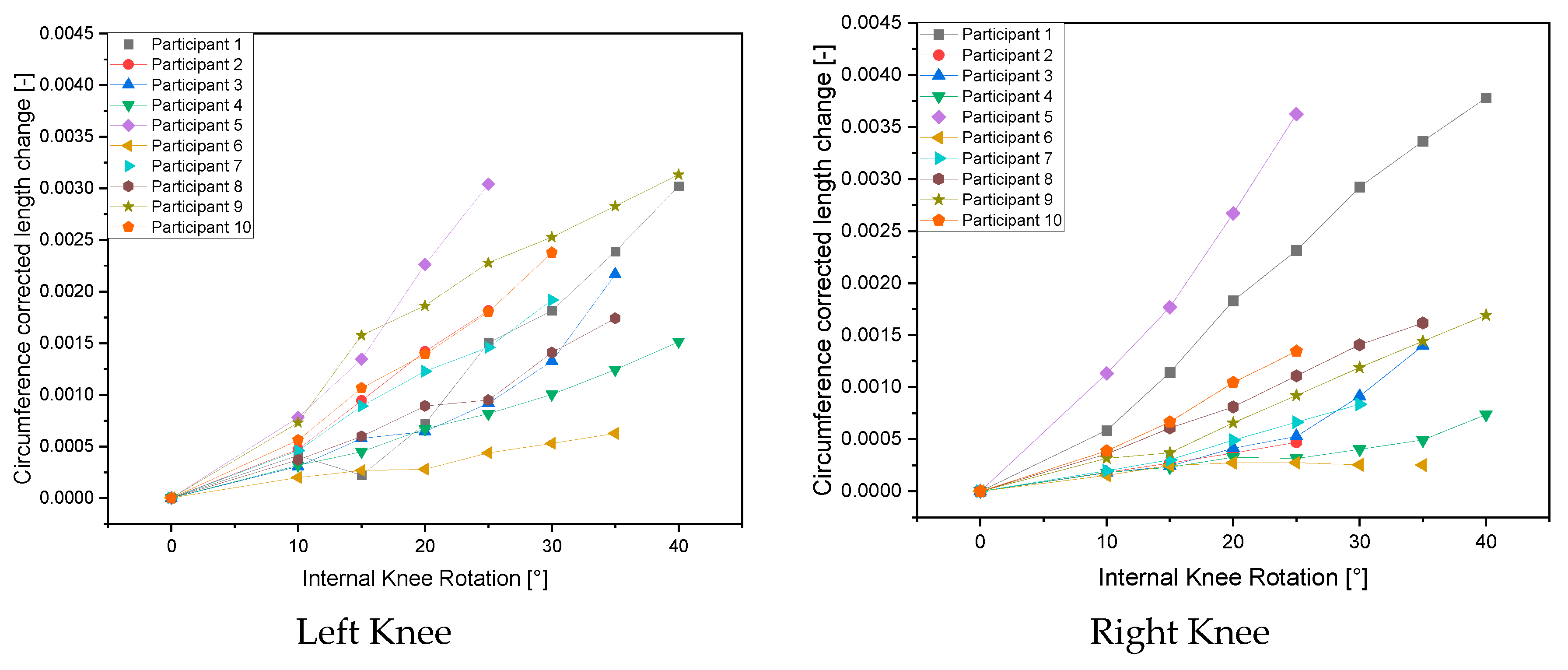

Table 1.
Length change of the polymer-based capacitive strain gauge as a function of knee internal rotation: comparison of women and men for the left and right knee.
Table 1.
Length change of the polymer-based capacitive strain gauge as a function of knee internal rotation: comparison of women and men for the left and right knee.
| Length Change [mm] | ||||||||
| Internal Knee Rotation | 0° | 10° | 15° | 20° | 25° | 30° | 35° | 40° |
| Left Knee Females | ||||||||
| Female 1 | 0 | 0.140 | 0.076 | 0.245 | 0.512 | 0.618 | 0.813 | 1.028 |
| Female 2 | 0 | 0.110 | 0.208 | 0.232 | 0.331 | 0.478 | 0.781 | |
| Female 3 | 0 | 0.104 | 0.148 | 0.222 | 0.270 | 0.332 | 0.410 | 0.500 |
| Female 4 | 0 | 0.166 | 0.269 | 0.402 | 0.428 | 0.635 | 0.784 | |
| Female 5 | 0 | 0.249 | 0.536 | 0.634 | 0.775 | 0.859 | 0.961 | 1.066 |
| Left Knee Males | ||||||||
| Male 1 | 0 | 0.212 | 0.426 | 0.640 | 0.818 | |||
| Male 2 | 0 | 0.344 | 0.592 | 0.996 | 1.338 | |||
| Male 3 | 0 | 0.068 | 0.091 | 0.095 | 0.149 | 0.180 | 0.213 | |
| Male 4 | 0 | 0.170 | 0.330 | 0.454 | 0.540 | 0.710 | ||
| Male 5 | 0 | 0.213 | 0.405 | 0.530 | 0.686 | 0.904 | ||
| Right Knee Females | ||||||||
| Female 1 | 0.000 | 0.199 | 0.388 | 0.623 | 0.787 | 0.994 | 1.144 | 1.285 |
| Female 2 | 0.000 | 0.064 | 0.087 | 0.149 | 0.190 | 0.329 | 0.503 | |
| Female 3 | 0.000 | 0.059 | 0.076 | 0.108 | 0.104 | 0.133 | 0.163 | 0.244 |
| Female 4 | 0.000 | 0.154 | 0.261 | 0.349 | 0.477 | 0.605 | 0.695 | |
| Female 5 | 0.000 | 0.108 | 0.126 | 0.223 | 0.313 | 0.404 | 0.490 | 0.575 |
| Right Knee Males | ||||||||
| Male 1 | 0 | 0.084 | 0.124 | 0.169 | 0.217 | |||
| Male 2 | 0 | 0.499 | 0.778 | 1.175 | 1.594 | |||
| Male 3 | 0 | 0.052 | 0.084 | 0.093 | 0.093 | 0.086 | 0.085 | |
| Male 4 | 0 | 0.071 | 0.109 | 0.177 | 0.239 | 0.301 | ||
| Male 5 | 0 | 0.149 | 0.256 | 0.402 | 0.518 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



