
Submitted:
28 September 2023
Posted:
03 October 2023
You are already at the latest version
Abstract
The climate crisis is developing to a life-changing event on a global level. Health promotion with the aim to increase the health status of individuals, independent from the present health status has been developed on scientific basis at least for the last eight decades and follows. There are some basic principles, which are prerequisites for both, health promotion and climate protection. Those principles include (1) sustainability, (2) orientation on determinants, and (3) requirement of in-dividual as well as community approaches. People are generally aiming to protect their lifestyle habits (e.g. traveling, consumer habits) and personal properties (e.g. car, house) by easy solution with as little effort as possible, and this can affect both, health and climate. To reduce the emission of greenhouse gases and to protect our environment, changes towards a sustainable lifestyle have to be embed into everybody’s mind. Examples for domains, that need to be addressed in health promotion as well as in climate protection include education/ knowledge/ (health) literacy, physical activity, nutrition and dietary habits, mental health, and social capital. If health promo-tion fails to tackle those domains, this will continue to drive climate crisis. And climate change, in turn, will affect health. On the other hand, developing and promoting health resources in the domains mentioned could again help to mitigate the health-damaging effects of climate change.
Keywords:
one health
; health promotion
; climate change
; exercise
; nutrition
; health literacy
; climate literacy
; sustainability
; social determinants
1. Introduction
The impact of climate change on health has recently been acknowledged in various international publications and calls for urgent action issued by COP26 [1], WHO [2, 3] and the Lancet commission [4], among many others. The link was also made explicit in the UN’s Sustainable Development Goals (SDGs) [5], especially goals 2, 3, 6, 13, and 15.
WHO now calls climate change the single biggest health threat facing humanity with environmental factors taking the lives of around 13 million people annually. Over 90% of people are exposed to unhealthy levels of air pollution, largely resulting from burning fossil fuels, which in turn further drives climate change. In 2018, air pollution from fossil fuels caused USD 2.9 trillion in health and economic costs, about USD 8 billion a day. The direct damage costs to health is estimated to be between USD 2-4 billion per year by 2030. [6] The impact of droughts and the subsequent damages to agriculture will increase considerably, with an estimated 40% of the global population living in areas under severe water stress by 2050, and approximately five million more deaths will be attributable to climate change [7]. Increasingly it is also acknowledged that rising temperatures will have a real impact on productivity and job performance. The International Labour Organisation [8] forecasts that the equivalent productivity of 80 million full-time jobs will be lost by 2030 due to heat-related stress. These are only some of the examples of how climate change now impacts every aspect of individual and community health. Given these multi-faceted and multi-layered effects of climate change on the health and wellbeing of individuals and communities, it becomes ever more urgent to think about ways in which synergies can be found to build resilient individuals, communities and systems, which can enable a climate protective and health promotive lifestyle.
The connection between health promotion and climate protection has most recently been brought together by WHO in its global framework for integrating well-being into public health utilizing a health promotion approach [9]. The global framework gives guidance to policymakers on how to implement the 6 strategic directions, first defined by the Geneva Charter in 2021 [3]. This charter in itself updated the principles of health promotion set out by the WHO Ottawa Charter [10] and aligned them with the SDGs [5] and the concept of planetary health [7]. The 6 strategic directions outlined in the global strategy address the need to adopt a planetary health approach to foster healthy environments, to continue the efforts of implementing universal health coverage by strengthening primary health care, health promotion and community empowerment, and ensure sustainable change through a rigorous approach to measuring and monitoring progress.
2. Breaking down the complexity – three principles to protect the climate and promote health
There are some basic concepts, which are prerequisites for both, health promotion and climate protection. The need to promote sustainable change on all levels, from the individual to the system, necessitates participatory approaches, which involve individuals and communities in co-designing and implementing solutions. A clear understanding of the determinants for health, wellbeing and climate protection strengthen these solutions.
(1) Sustainability
Both, climate protection and health promotion can only be successful, when actions, initiatives, campaigns and policies are geared towards long-term, sustainable change in habits, behaviours and lifestyles. In its groundbreaking “Special report on climate change and health: the health argument for climate action”, COP26 summarised the evidence on how health promoting policies and lifestyles can benefit a healthy climate as well [1]. For example, policies and actions to facilitate walking and cycling as climate-friendly means of transport improves health through increased physical activity, resulting in reductions in respiratory diseases, cardiovascular diseases, some cancers, diabetes mellitus and obesity [11]. Similarly, the promotion of urban green spaces reduces exposure to air pollution, generates local cooling effects, helps to relief stress, and increases recreational space for social interaction and physical activity [12, 13]. A shift to more nutritious plant-based diets in line with WHO recommendations could reduce global emissions significantly, ensure a more resilient food system, and avoid up to 5.1 million diet-related deaths a year by 2050 [14]. But all of these actions require sustainable changes from individuals and communities.
In connection with climate protection, the definition of sustainability as drawn up by the World Commission on Environment and Development (Brundtland Commission) is used very frequently. This definition is, “meeting the needs of the present without compromising the ability of future generations to meet their own needs” [15]. In relation to health, many different definitions of sustainability are used in the scientific literature. Most of these definitions revolve around the fact that measures are still taken after a certain period of time, that changed lifestyle habits are maintained for a longer period of time, or that health effects can still be proven after a certain period of time [16]. There is a certain tradition in health promotion of organizing and financing this in projects with a defined beginning and a defined end. However, sustainability can only be guaranteed in non-terminated programmes, which is why there has been a long debate about health promotion in projects. A large number of factors have been identified that either support or hinder the sustainability of health promotion programmes [17]. Many models have been introduced to support long-term lifestyle changes and maintain behaviour modification, one of the best known being the Trans-Theoretical Model which describes the different stages of change [18]. The strength of this model lies in the fact that it allows not only for progress, but also relapses into old habits, which are not depicted as failures, but as a natural occurrence in individual change behaviour: sustainable change is not achieved through linear progress, but through a start, maintain, fail, and try again process, which can spiral upwards or downwards. Similar approaches need to be developed for behavior changes for climate protection, and the lessons learned from decades of health promotion should be taken into account.
Using the obvious synergies of programmes to promote healthier lifestyles and at the same time help protect the climate, may also widen the audience of individuals and communities, which can be reached. A comparison of the Social Ecological Model of Health [19] with the SDGs [5] illustrates this interrelationship and strengthens the argument for concerted efforts in the area of health promotion and climate protection (see Figure 1).
(2) Focus on determinants
The Social Ecological Model of Health (SEM) [19] describes the multi-faceted determinants of health on all levels, from the individual to the system. It builds on the realisation that 90% of one’s health outcomes are influenced by other factors than access to clinical care [20, 21]. Similarily, the Sustainable Development Goals (SDGs) are an evolution of the Millenium Development Goals (MDGs) recognising that health, economic and social development, as well as our natural environment are inextricably intertwined. Table 1 highlights the alignment between the determinants of health as defined by the SEM and the SDGs, but it is best captured in the Ottawa Charter’s statement that "Health is created and lived by people within the settings of their everyday life; where they learn, work, play, and love." [10]
Social determinants of health (SDH) are among the best researched and verified factors that facilitate or hinder the development of health [22]. Social capital for example represents the relationships between people and their community and these resources are associated with the ability and motivation of individuals for adaptations towards specific topics as well as their overall well-being [23]. Increasing individual social capital and increasing social cohesion on a community level is an important part of individual and public health promotion. It is also part of SDGs 11 and 16.
Likewise, climate protection is dependent on social determinants and projects worldwide have shown that social cohesion in society favours changes towards a sustainable and climate-friendly economy. Data of rural households in Ethiopia were investigated to identify correlations between social capital and climate change adaptation [24]. Similar results of high social capital and climate change adaptation in the agricultural sector were published by investigating data of Indonesian farmers, which had to deal with an increasing risk of pest attacks. A strong sense of solidarity and belonging to the community engaged 70% of the farmers to contribute to adaptation processes to solve issues responsible for crop failures [25].
The SEM and SDH concepts and evidence of their validity has been around for decades, and so has their description of the influence of the living environment on health. Still, the impact of the environment and climate on health has only emerged as a priority area for action through the recent discussions on climate change itself, the SDGs and recent publications from WHO [6]. Again, this is an example where research and practice on climate protection can learn a lot from the research on health promotion and the climate aspect on the determinants of health should be strengthened. The example of the WHO Healthy Cities network already illustrates how the two concepts are interlinked with the overall aims of a Healthy City including the creation of a health-supportive environment and the provision of basic sanitation and hygiene needs (https://www.who.int/activities/creating-healthy-cities).
(3) Individual as well as community approaches
While health promotion is often seen as taking individual action, climate protection is perceived as a collective and global challenge. However, for sustainable and positive change to happen, both for health promotion as well as for climate protection a combination of individual and community approaches is necessary. Individual approaches include for example sustainable behaviour changes towards a healthier lifestyle and the reduction of the CO2 footprint by switching to more sustainable modes of transport, like cycling or public transport. Another key element is for people to be aware how daily choices influence the environment and can contribute towards climate protection, just as their lifestyle choices effect their health. Health literacy forms one pillar of WHO’s definition of health promotion [26], and in parallel, climate literacy needs to be established as a key element of climate protection.
Individual and community approaches therefore need to apply participatory strategies, which enable and support people to actively co-design, decide and implement solutions fitting into their context and life. Change is always difficult, and will only be sustainable if people understand why it is necessary, how it will affect them and how it will fit into their living environment and daily life. This is true for both health promotion [9, 19] and climate protection measures. A key term used in both arenas is empowerment. In health, empowerment refers to “the process by which people develop their intrinsic capabilities to increase control over the factors, decisions and actions that affect their health and care and the process of gaining power externally over them.” [27] Tools to implement empowerment exist on the individual as well as on the community level, and include strengthening health literacy, enabling informed choice and co-production of solutions. There is a plethora of examples on how individuals can be more actively involved in their health and care, and these are usually linked to the concept of person-centred health systems [28, 29]. In addition to the involvement and empowerment of individuals, the health arena is increasingly working together with communities to create healthy environments and contextualise service delivery according to the needs of the local population. Concepts like population health management emphasise the importance of proactive health promotion and prevention over reactive treatment and management of diseases [30, 31]. Similar principles are used in health promotion, for which the key strategies of health promotion are Advocacy, Mediation and Empowerment [10, 26]. This again reflects the need to recognise and enforce the rights and responsibilities of individuals and communities, to collaborate across sectors and interest groups and to ensure recognise communities as equal partners in the design and implementation of solutions. In parallel, the Action for Climate Empowerment (ACE) adopted by the UN Framework Convention on Climate Change wants to empower all members of society to engage in climate action, through the six ACE elements - climate change education and public awareness, training, public participation, public access to information, and international cooperation on these issues (https://unfccc.int/ace#Article-6-of-the-Convention).
While health promotion recognizes the need to use both individual as well as community approaches [10, 19, 26], in the Paris Agreement the call for action is issued mainly to institutions and systems, including governments, cities, regions, businesses and investors. The lack of individual and community involvement or empowerment in the official climate policies and strategies has found its counterpart in the direct action by global movements like Fridays for Future or the Last Generation. It would strengthen climate action if similar individual and community approaches were used to harness the power and expertise of local communities.
3. Examples for common domains of health promotion and climate protection
There is a multitude of domains, which affect both, health and the climate. Examples discussed here are (1) literacy, (2) physical activity, (3) and nutrition and dietary habits. Some of them will be challenged by the burden of climate conditions (e.g. physical activity, diet and food supply) others will be more important than before (e.g. training and education of the public, as well as health professionals, or fostering social cohesion and building social capital). If health promotion fails to tackle those domains, these will drive the climate crisis and consequently yield into a variety of health issues. On the other hand, developing and promoting health resources in the mentioned domains could again help to mitigate the health-damaging effects of climate change) [32].
(1) Literacy
According to an OECD definition, literacy refers to reading and writing skills in a broader sense. It is the ability to recognize, understand, interpret, create, communicate and evaluate written materials in different contexts. According to this definition, literacy enables persons to achieve their goals, develop their knowledge and potential and to fully participate in society [33].
The WHO defines health literacy as the achievement of “a level of knowledge, personal skills and confidence to take action to improve personal and community health by changing personal lifestyles and living conditions.” [34] This definition implies that health literacy means more than the ability to get access to, read and understand health information (functional health literacy). It also creates the foundation on which persons are empowered to play an active role in improving their own health by critically evaluate the value of health information (critical health literacy), to apply the information and be an equal player in the healthcare system (interactive health literacy), and to lobbying for better health conditions in the society. Health literacy is, more and more understood as a social determinant of health [35], and improving health literacy in the community needs both, interventions aimed at individuals and interventions that create the conditions for this at the population level [36].
Climate literacy can be understood as the ability to know and understand the principles of climate, impacts of climate change, and approaches to adaptation or mitigation [37]. By analogy with the definitions of literacy and health literacy, climate literacy would mean more than just reading and understanding. Individuals should be able to critically evaluate and apply the information, and challenge decision makers and lobby for sustainable policies and changes at the societal level. The basic principles of salutogenesis, as defined by Antonovsky as dimensions of the sense of coherence [38], can also be applied to the genesis of climate protection. Comprehensibility, a trust that that connections with regard to climate change are understandable and that future climate developments are predictable is an important prerequisite. Manageability means the trust that climate protection measures can not only be actually be implemented, but also do not necessarily mean significant economic and personal rights-cutting losses. Meaningfulness means the trust that things in life like climate protection are interesting, worthwhile, and a source of satisfaction. It also means ta ability to see measures of climate protection in a larger context, also beyond the borders of one's own generation and the present time.
To create literacy, both, health and climate literacy, need campaigns and trainings by local, national and global stakeholders (e.g. policy, public health, etc.) and a framework for education (e.g. health and climate literacy in schools, climate change curriculum in medical and health professional education, and health aspects in ecological education curricula). [39, 40] Limaye et al. summarized results of 72 peer-reviewed articles on climate change, human health, and education or training and thereby established a framework for climate and health literacy [40]. They grouped the identified elements into three categories: (1) functional literacy, including knowledge about causalities and mechanisms, how factors worsen both, climate crisis and human health, and how climate change effects human health; (2) intermediate literacy, including understanding of determinants and intertwining of environment and human health, implications of climate changes and the possible impact of interventions towards climate protection; (3) advanced literacy, including understanding the evidence derived from different types of data and models as well as understanding the complexity and variations over space and time. [40] Clear parallels can be discerned with the Action for Climate Engagement (ACE).
(2) Physical activity
Physical activity (PA) is widely used for the prevention, therapy and rehabilitation of chronic diseases. Also, PA increases well-being and quality of life, and therefore is a well-established tool in health promotion [41]. PA increases physical fitness, and thereby creates resilience against many non-communicable diseases including health burdens as consequences of the climate change-related heat episode, like heat strokes and circulatory problems [42, 43]. This connection is contrasted by the fact that older and vulnerable groups in particular might experience a possible negative health impact, if PA is carried out in the heat. However, these dangers can be mitigated if special safety measures are followed on hot days.
Changing and maintaining the lifestyle towards more PA is a major challenge. In order to reach sustainability in this regard, orientation towards the determinants, including the social determinants, of PA behavior is a basic requirement. In addition, sustainable implementation of this health behavior requires individual measures aimed at improved health literacy and the acquisition of skills to carry out health enhancing PA and physical training, as well as societal, public, and community-based measures that create the conditions for this, such as a change towards a culture in which PA is considered socially desirable, and creating physical, environmental, structural and legislative requirements for safe PA.
PA not only has positive consequences for health, but also for the climate. Especially transport related PA (e.g. walking, running, cycling, riding an e-bike, riding a scooter) to cover daily distances and thereby replace motorized vehicles that consume fossil fuels are discussed to be associated with a lower production of greenhouse gases and therefore contribute towards climate protection.
Green spaces are important areas for climate protection due to their CO2 binding capacity. Additionally, parks and green spaces play an important role to avoid so called urban heat islands [12, 13, 44]. Furthermore, green spaces are prerequisites and important determinants of PA behaviour. In fact, a study in Austria has shown a strong correlation between green spaces and the perceived accessability of green spaces with the amount of PA on a local level [45].
PA is expected to change because of climate change. Climate change influences the weather towards higher temperatures, more heat days, a higher humidity, and more extreme weather events. This is expected to influence physical activity behavior. The amount of PA is reduced at both, cold and hot temperatures, as well as on precipitation days [46]. As hot days become more frequent due to climate change, it is to be expected that PA will decrease in many countries for a longer period of time in the summer. Another aspect of climate change is the decreased duration and accumulation of snowfall, especially in mountainous areas. This affects winter sports, and as a consequence decreases the amount of PA activity in winter. In fact, a study from an alpine Austrian region showed that the intention to participate in recreational winter sports activities decreased due to the climate change [47]. People with a higher socio-economic position might find it easier to regularly participate in PA, disregarding the weather outside. The geographical region is also important, since in colder regions climate change might increase the amount of PA and in wormer regions climate change might decrease the amount of PA.
According to the World Health Organization´s Global Action Plan on Physical Activity (GAPPA) from 2018 - 2030, there are five domains related to PA, which are influenced by climate change. These are infrastructures, green spaces, exercise programs, mass communication and mass participation events as well as training of professionals. These domains are connected with climate policy, demonstrating clearly the link of strategies for physical activity promotion and the reduction of greenhouse gas emissions. To reach their goals, the GAPPA mainly focuses on four strategic objectives (active societies; active environments; active people; active systems) and 20 policy actions and emphasizes changes in PA policy making, proposing among other facts health economic assessments of health and climate & environmental benefits in the areas of active transport and urban design [48].
(3) Nutrition and dietary habits
The growing understanding of how our dietary choices impact not only our health but also the environment has led to a realization that sustainable dietary practices can be a powerful tool for addressing both climate change and public health concerns. It must be acknowledged that not all climate-friendly foods are considered healthy and not all healthy foods are climate-neutral at the same time. However, plant-based diets, rich in fruits, vegetables, legumes, nuts, and whole grains, are components of a healthy dietary pattern, and they have the potential to have lower carbon footprints compared to diets high in animal products. In the last decades researchers provided data and evidence that a sustainable nutrition in the frame of a sustainable lifestyle is beneficial for the environment as well as for the overall health and well-being of humans [49 – 51]. The One Health dietary approach, developed by the Food and Agriculture Organization of the United Nations [52] can contribute to both, climate protection and health promotion.
Healthy diets are often associated with reduced risk factors for chronic diseases such as obesity, diabetes mellitus, cardiovascular diseases, and cancer. A shift towards plant-based diets can lead to lower saturated fat intake, reduced cholesterol levels, and improved weight management. Plant-based diets are rich in fiber, vitamins, and antioxidants which are linked to various health benefits [53 -55].
Modern food systems, characterized by extensive livestock production, energy-intensive processing, and long supply chains, contribute significantly to greenhouse gas emissions, deforestation, and biodiversity loss. In fact, diets and food quality have been identified to be responsible for 25% of global greenhouse-gas emissions. Adopting sustainable diet patterns can mitigate these impacts. [56-58]
Various determinants influence dietary choices, encompassing individual, cultural, economic, and social factors. Education, knowledge and finally literacy play a vital role in promoting sustainable and healthy dietary behaviours. Furthermore, economic factors, such as the affordability and accessibility of healthy and sustainable foods, are crucial determinants. Not only individual choices, but also policies that support sustainable agriculture, subsidize nutrient-rich foods, and encourage local food production can create an enabling environment for healthier and more sustainable diets. [59]
Climate change, vice versa, also affects food production. Agricultural productivity might decrease due to environmental degradation, desertification, soul depletion, overgrazing, rising sea levels, urban development, increase of roads and industrial use. Adverse weather events like flooding, landslides and erosion, storms, hurricanes and droughts will further damage crops. Those mechanisms together with other like transport related problems, spoilage and bacterial damage, and increased necessity for pesticide use will worsen nutritional problems associated with climate change [60]. All those factors contribute towards a loss of food diversity and a reduced supply of fresh foods such as vegetables and fruit, and subsequently to an increase in the price of fresh and healthy food.
4. From policy to practice
There now exists a long list of publications, which provide evidence on the impact of climate change on health and wellbeing, and an equally long list of international policies, frameworks and strategies of how to tackle these challenges. What is still missing is to use the collective experience in the health promotion and climate action arenas, to create synergies and co-design and implement viable solutions with local communities and individuals to move towards true planetary health. Taking up the call of the WHO global framework [9] for whole of government and whole of society approaches “to generate health benefits for the populations and the planet” these should be extended to include climate protection as a vehicle for health promotion and vice versa. Similar to the Health-in-all-policies approach a climate-in-all-policies approach could foster holistic solutions to complex challenges. Health and other experts need to be fully involved in climate decision-making processes at all levels, to ensure health and equity considerations are well understood and accounted for when developing climate policies [1-4, 9].
In Table 2 the synergies between health promotion and climate protection in the three mentioned examples are summarized, with a focus on the prerequisite for both, sustainability, determinants orientation, and individual and community approaches.
5. Conclusions
Health promotion and climate protection do not overlap 100%, but they share many concepts and tools, which help to create synergies in tackling the challenges faced by societies and governments. Summarising these in three key principles of sustainability, focus on determinants, and a combination of individual and public approaches organizes the increasing evidence and the existing policies to outline clear areas for joint action.
Author Contributions
Conceptualization, investigation, writing, K.V.S. and T.E.D. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- World Health Organization. COP26 special report on climate change and health: the health argument for climate action. Geneva: World Health Organization 2021. Licence: CC BY-NC-SA 3.0 IGO.
- Prüss-Ustün, A.; Wolf, J.; Corvalán, C.; Bos, R.; Neira, M. Preventing disease through healthy environments: a global assessment of the burden of disease from environmental risks. Geneva: World Health Organization 2016. Available online: https://www.who.int/publications/i/item/9789241565196 (accessed on 25 09 2023).
- World Health Organization. Geneva Charter for Well-Being. Geneva: World Health Organization 2021. Available online: https://www.who.int/publications/m/item/the-geneva-charter-for-well-being (accessed on 25 09 2023).
- Romanello, M.; Di Napoli, C.; Drummond, P.C.; et al. The 2022 report of the Lancet Countdown on health and climate change: health at the mercy of fossil fuels. Lancet 2021, 397, 129–170.
- United Nations. Transforming our World: The 2030 Agenda for Sustainable Development. New York: United Nations 2015. Available online: https://sdgs.un.org/publications/transforming-our-world-2030-agenda-sustainable-development-17981 (accessed on 25 09 2023).
- World Health Organization. Fast Facts on Climate Change and Health. Technical Document, Geneva: World Health Organization, 8 Sep 2021. Available online: https://www.who.int/publications/m/item/fast-facts-on-climate-change-and-health (accessed on 25 09 2023).
- Whitmee, S.; Haines, A.; Beyrer, C.; Boltz, F.; Capon, A.G.; de Souza Dias, B.F.; Ezeh, A.; Frumkin, H.; Gong, P.; Head, P.; et al. Safeguarding human health in the Anthropocene epoch: Report of The Rockefeller Foundation—Lancet Commission on planetary health. Lancet 2015, 386, 1973–2028. [CrossRef]
- International Labour Organization. Working on a warmer planet. The impact of heat stress on labour productivity and decent work. Geneva: International Labour Organization. Available online: https://www.ilo.org/wcmsp5/groups/public/---dgreports/---dcomm/---publ/documents/publication/wcms_711919.pdf (accessed on 25 09 2023).
- World Health Organization. Achieving well-being. A global framework for integrating well-being into public health utilizing a health promotion approach. WHA 76, Geneva: World Health Organization 2023. Available online: https://www.who.int/publications/m/item/wha-76---achieving-well-being--a-global-framework-for-integrating-well-being-into-public-health-utilizing-a-health-promotion-approach (accessed on 25 09 2023).
- World Health Organization. The Ottawa charter for health promotion. Geneva: World Health Organization 1987. Available online: https://www.who.int/publications/i/item/WH-1987 (accessed on 25 09 2023).
- Lee, I.M.; Shiroma, E.J.; Lobelo, F.; Puska, P.; Blair, S.N.; Katzmarzyk, P.T.; Lancet Physical Activity Series Working Group. Effect of physical inactivity on major non-communicable diseases worldwide: An analysis of burden of disease and life expectancy. Lancet 2012, 380, 219–229. [CrossRef]
- Kardan, O.; Gozdyra, P.; Misic, B.; Moola, F.; Palmer, L.J.; Paus, T.; Berman, M.G. Neighborhood greenspace and health in a large urban center. Sci. Rep. 2015, 5, 11610. [CrossRef]
- Gascon, M.; Triguero-Mas, M.; Martínez, D.; Dadvand, P.; Rojas-Rueda, D.; Plasència, A.; Nieuwenhuijsen, M.J. Residential green spaces and mortality: A systematic review. Environ. Int. 2016, 86, 60–67. [CrossRef]
- Springmann, M.; Godfray, H.C.J.; Rayner, M.; Scarborough, P. Analysis and valuation of the health and climate change cobenefits of dietary change. Proc Natl Acad Sci U S A 2016, 113, 4146–4151. [CrossRef]
- Borowy, I. Defining Sustainable Development: the World Commission on Environment and Development (Brundtland Commission). London: Routledge, 2013.
- Moore, J.E.; Mascarenhas, A.; Bain, J.; Straus, S.E. Developing a comprehensive definition of sustainability. Implement. Sci. 2017, 12, 1–8. [CrossRef]
- Bodkin, A.; Hakimi, S. Sustainable by design: a systematic review of factors for health promotion program sustainability. BMC Public Heal. 2020, 20, 1–16. [CrossRef]
- Prochaska, J.O.; DiClemente, C.C. Transtheoretical therapy: Toward a more integrative model of change.. Psychotherapy 1982, 19, 276–288. [CrossRef]
- Dahlgren, G.; Whitehead, M. Policies and Strategies to Promote Social Equity in Health. Stockholm, Sweden: Institute for Futures Studies, 1991.
- Gnadinger, T. Health policy brief: The relative contribution of multiple determinants to health outcomes. Health Affairs Blog, 22 August 2014, Accessible at: https://www.healthaffairs.org/do/10.1377/hblog20140822.040952/full/ (accessed on 25 09 2023).
- Hood, C.M.; Gennuso, K.P.; Swain, G. R.; Catlin, B.B. County health rankings: Relationships between determinant factors and health outcomes. Am J Prev Med. 2016 50, 129–135. [CrossRef]
- Marmot, M.; Allen, J.; Bell, R.; Bloomer, E.; Goldblatt, P.; Consortium for the European Review of Social Determinants of Health and the Health Divide. WHO European review of social determinants of health and the health divide. Lancet 2012, 380, 1011-1029. [CrossRef]
- Wolf, J.; Adger, W.N.; Lorenzoni, I.; Abrahamson, V.; Raine, R. Social capital, individual responses to heat waves and climate change adaptation: An empirical study of two UK cities. Glob. Environ. Chang. 2010, 20, 44–52. [CrossRef]
- Belay, D.; Fekadu, G. Influence of social capital in adopting climate change adaptation strategies: empirical evidence from rural areas of Ambo district in Ethiopia. Clim. Dev. 2021, 13, 857–868. [CrossRef]
- Saptutyningsih, E.; Diswandi, D.; Jaung, W. Does social capital matter in climate change adaptation? A lesson from agricultural sector in Yogyakarta, Indonesia. Land Use Policy 2019, 95, 104189. [CrossRef]
- World Health Organization. The Shanghai declaration on promoting health in the 2030 Agenda for Sustainable Development. Ninth Global Conference on Health Promotion, Shanghai, 21–24 November 2016. Geneva: World Health Organization 2016. Available at: https://www.who.int/publications/i/item/WHO-NMH-PND-17.5 (accessed on 25 09 2023).
- Ferrer, L. Engaging patients, carers and communities for the provision of coordinated/integrated health services: Strategies and tools. Working Document. Copenhagen: WHO Regional Office for Europe 2015.
- Stein, K.V.; Amelung, V.E. Refocussing Care - What Does People-Centredness Mean? In Handbook Integrated Care. Amelung, V.E.; Stein, K.V.; Suter, E.; Goodwin, N.; Nolte, E.; Balicer, R., Eds.; Springer Nature, 2021.
- World Health Organization. Framework on integrated, people-centred health services. Report by the Secretariat, 69th World Health Assembly. Geneva: World Health Organisation 2016.
- van Ede, A.F.T.M.; Minderhout, R.N.; Stein, K.V.; Bruijnzeels, M.A. How to successfully implement population health management: a scoping review. BMC Heal. Serv. Res. 2023, 23, 1–10. [CrossRef]
- Steenkamer, B.M.; Drewes, H.W.; Heijink, R.; Baan, C.A.; Struijs, J.N.; Msc; D, P.; Slabaugh, S.L.; Shah, M.; Zack, M.; et al. Defining Population Health Management: A Scoping Review of the Literature. Popul. Heal. Manag. 2017, 20, 74–85. [CrossRef]
- Chastonay, P.; Zybach, U.; Simos, J.; Mattig, T. Climate change: an opportunity for health promotion practitioners? Int J Public Health. 2015, 60, 763-764. [CrossRef]
- OECD. Adult health literacy. Available at: https://www.oecd.org/education/innovation-education/adultliteracy.htm (accessed on 25 09 2023).
- Nutbeam, D.; Muscat, D.M. Health Promotion Glossary 2021. Heal. Promot. Int. 2021, 36, 1578–1598. [CrossRef]
- Nutbeam, D.; Lloyd, J.E. Understanding and Responding to Health Literacy as a Social Determinant of Health. Annu. Rev. Public Health 2021, 42, 159–173. [CrossRef]
- Nutbeam, D.; McGill, B.; Premkumar, P. Improving health literacy in community populations: A review of progress. Health Promot. Int. 2018, 33, 901–911. [CrossRef]
- U.S. Global Change Research Program. Climate Literacy: The Essential Principles of Climate Science. Washigton DC 2009. Available at: https://downloads.globalchange.gov/Literacy/climate_literacy_highres_english.pdf (accessed on 25 09 2023).
- Antonovsky, A. Unraveling The Mystery of Health - How People Manage Stress and Stay Well. San Francisco: Jossey-Bass Publishers, 1987.
- Frumkin, H.; Hess, J.; Luber, G.; Malilay, J.; McGeehin, M. Climate Change: The Public Health Response. Am. J. Public Heal. 2008, 98, 435–445. [CrossRef]
- Limaye, V.S.; Grabow, M.L.; Stull, V.J.; Patz, J.A. Developing A Definition Of Climate And Health Literacy: Study seeks to develop a definition of climate and health literacy. Health Aff (Millwood). 2020, 39, 2182-2188. [CrossRef]
- U.S. Department of health and Human Services. 2018 Physical Activity Guidelines Advisory Committee. 2018 Physical Activity Guidelines Advisory Committee Scientific Report. https://health.gov/sites/default/files/2019-09/PAG_Advisory_Committee_Report.pdf (accessed on 25 09 2023).
- Leyk, D. Health Risks and Interventions in Exertional Heat Stress. Dtsch. Aerzteblatt Online 2019, 116, 537–+. [CrossRef]
- Gardner, J.W.; Kark, J.A.; Karnei, K.; Sanborn, J.S.; Gastaldo, E.; Burr, P.; Wenger, C.B. Risk factors predicting exertional heat illness in male Marine Corps recruits. Med. Sci. Sports Exerc. 1996, 28, 939–944. [CrossRef]
- Reis, C.; Lopes, A. Evaluating the Cooling Potential of Urban Green Spaces to Tackle Urban Climate Change in Lisbon. Sustainability 2019, 11, 2480. [CrossRef]
- Dorner, T.E.; Haider, S.; Lackinger, C.; Kapan, A.; Titze, S. Determinants of Exercise, Fulfilling the Recommendations for Aerobic Physical Activity and Health Status: Results of a Correlation Study in the Federal States of Austria. Gesundheitswesen 2020, 82, S207-S216.. [CrossRef]
- Obradovich, N.; Fowler, J.H. Climate change may alter human physical activity patterns. Nat. Hum. Behav. 2017, 1. [CrossRef]
- Frühauf, A.; Niedermeier, M.; Kopp, M. Intention to Engage in Winter Sport in Climate Change Affected Environments. Front. Public Heal. 2020, 8. [CrossRef]
- Abu-Omar, K.; Gelius, P.; Messing, S. Physical activity promotion in the age of climate change. F1000Res. 2020, 9, 349. [CrossRef]
- Tilman, D.; Clark, M. Global diets link environmental sustainability and human health. Nature 2014, 515, 518–522. [CrossRef]
- Poore, J.; Nemecek, T. Reducing food’s environmental impacts through producers and consumers. Science 2018, 360, 987–992. [CrossRef]
- Hayek, M.N.; Harwatt, H.; Ripple, W.J.; Mueller, N.D. The carbon opportunity cost of animal-sourced food production on land. Nat. Sustain. 2020, 4, 21–24. [CrossRef]
- FAO. One health. Available at: https://www.fao.org/one-health/en (accessed on 25 09 2023).
- Wallace, T.C.; Bailey, R.L.; Blumberg, J.B.; Burton-Freeman, B.; Chen, C.-Y.O.; Crowe-White, K.M.; Drewnowski, A.; Hooshmand, S.; Johnson, E.; Lewis, R.; et al. Fruits, vegetables, and health: A comprehensive narrative, umbrella review of the science and recommendations for enhanced public policy to improve intake. Crit. Rev. Food Sci. Nutr. 2020, 60, 2174–2211. [CrossRef]
- Angelino, D.; Godos, J.; Ghelfi, F.; Tieri, M.; Titta, L.; Lafranconi, A.; Marventano, S.; Alonzo, E.; Gambera, A.; Sciacca, S.; et al. Fruit and vegetable consumption and health outcomes: an umbrella review of observational studies. Int. J. Food Sci. Nutr. 2019, 70, 652–667. [CrossRef]
- Fanzo, J.; Rudie, C.; Sigman, I.; Grinspoon, S.; Benton, T. G.; Brown, M.E.; Covic, N.; Fitch, K.; Golden, C.D.; Grace, D.; Hivert, M.F.; Huybers, P.; Jaacks, L.M.; Masters, W.A.; Nisbett, N.; Richardson, R.A.; Singleton, C.R.; Webb, P.; Willett, W.C. Sustainable food systems and nutrition in the 21st century: a report from the 22nd annual Harvard Nutrition Obesity Symposium. Am J Clin Nutr. 2022, 115, 18-33. [CrossRef]
- Vermeulen, S.J.; Campbell, B.M.; Ingram, J.S.I. Climate Change and Food Systems. Annu. Rev. Environ. Resour. 2012, 37, 195–222. [CrossRef]
- Duchin, F. Sustainable Consumption of Food: A Framework for Analyzing Scenarios about Changes in Diets. J. Ind. Ecol. 2005, 9, 99–114. [CrossRef]
- Stehfest, E. Food choices for health and planet. Nature 2014, 515, 501–502. [CrossRef]
- Salm, L.; Nisbett, N.; Cramer, L.; Gillespie, S.; Thornton, P. How climate change interacts with inequity to affect nutrition. WIREs Clim. Chang. 2020, 12. [CrossRef]
- Binns, C.W.; Lee, M.K.; Maycock, B.; Torheim, L.E.; Nanishi, K.; Duong, D.T.T. Climate Change, Food Supply, and Dietary Guidelines. Annu Rev Public Health. 2021, 42, 233-255. [CrossRef]
Figure 1.
Social Ecological Model of Health and the Sustainable Development Goals.
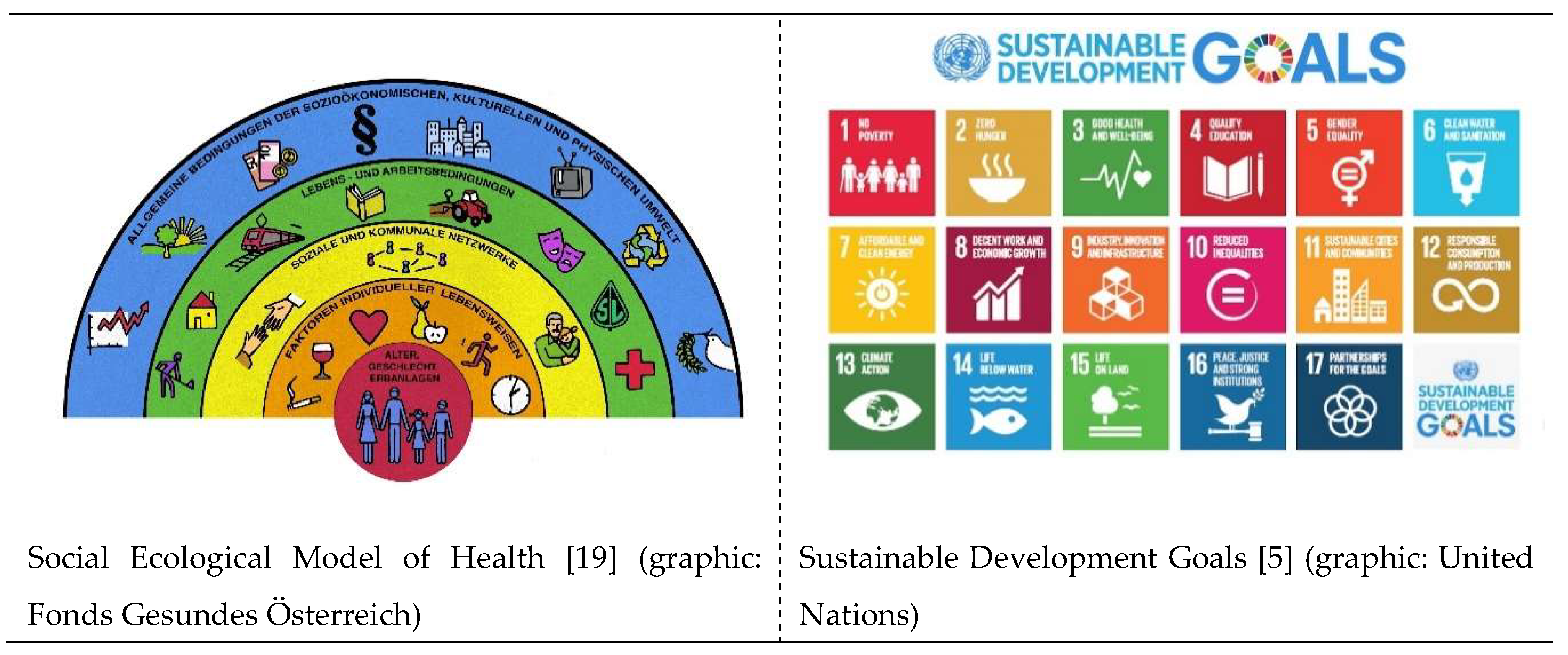

Table 1.
Alignment of the determinants of health with the SDGs.
| SEM1 | SDG2 |
|---|---|
| Environmental conditions | Affordable and clean energy (7), sustainable cities and communities (11), climate action (13), life below water (14), life on land (15) |
| Agriculture and food production | Zero hunger (2), responsible consumption and production (12) |
| Education | Quality education (4) |
| Work environment | Decent work and economic growth (8) |
| Unemployment | No poverty (1) |
| Water and sanitation | Clean water and sanitation (6) |
| Health care services | Good health and wellbeing (3) |
| Social and community networks | Social and community networks |
| Sex | Gender equality (5) |
| Conditional factors | Industry innovation and infrastructure (9), reduced inequalities (10), peace, justice and strong institutions (16) |
1 Social Ecological Model; 2 Sustainable Development Goals (number of the respective SDG in brackets).
Table 2.
Recommendations for actions to use the synergies of health promotion and climate protection.
Table 2.
Recommendations for actions to use the synergies of health promotion and climate protection.
| Sustainability | Determinants | Individual and community approaches |
|
|---|---|---|---|
| Literacy | Adaptation of the dimensions of the sense of coherence, as a prerequisite for salutogenesis (comprehensibility, manageability, and meaningfulness) can also be seen as a prerequisite for sustainability in the genesis of climate protection. | Social determinants, especially education play a key part in the levels of health and climate literacy. Easy access to evidence-based information in lay language is another important determinant. Facilitating these levers through active policies in education and health and climate promotion can mitigate negative impact of determinants. | Address individuals, patients, health professionals and the whole society to increase health literacy and climate literacy. Furthermore, the people, patients and the public must be seen as important and equal partners for health promotion and climate protection. Including comprehensive education on health and climate from kindergarden, continuing to geriatric care, would establish a baseline understanding across society. |
| Physical activity | Bottom-up instead of top-down approaches and orientation on individual stages of change can promote a change in physical activity behavior towards sustainable, active mobility. | The orientation of policies and strategies towards social, economic, cultural, individual and health and fitness-related determinants is an important prerequisite for the promotion of active mobility. |
Encourage individuals towards physically active transportation as alternative for daily distances and create the conditions for it like green spaces and a traffic system, which is safe and inviting for physically active transportation. |
| Nutrition and dietary habits | A sustainable change and maintenance of healthy eating habits is very difficult for many people. The best results can be achieved by considering all established pillars of health promotion (empowerment, participation, orientation towards determinants, personal needs and believes, and stages of change, etc.). | Social, economic, individual and cultural determinants of eating habits must be taken into account for a healthy and climate-friendly change in diet. | Develop sustainable nutrition guidelines for healthy nutrition with focus on local, organic, and plant-based food and communicate them to individuals, to stakeholders and the public. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



