Submitted:
27 September 2023
Posted:
28 September 2023
You are already at the latest version
Abstract
This study uses explainable artificial intelligence to analyze major predictors of poor self-rated health, dementia and their comorbidity, which include various aspects of social support. Data came from the Korean Longitudinal Study of Ageing (2016-2018), with 5527 participants aged 56 or more. The dependent variables were: (1) poor self-rated health (SRH) with 5 categories (very good, good, middle, poor, very poor); (2) dementia (no, yes); and (3) their comorbidity with 4 categories (SRH very good, good or middle, dementia no; SRH very good, good or middle, dementia yes; SRH poor or very poor, dementia no; SRH poor or very poor, dementia yes). The 49 demographic, socioeconomic and health-related predictors were included. The accuracy and area under the receiver operating characteristic curve (AUC) were compared for logistic regression and the random forest. Logistic regression and the random forest registered similar AUCs with the range of 0.80-0.87. Based on random forest variable importance, 18 out of top-20 predictors were identical for SRH, dementia and their comorbidity: previous SRH, life satisfaction - health, age, body mass index, income, chronic diseases, life satisfaction - economic, life satisfaction - overall, grandchildren alive, friendship meeting, brothers/sisters alive, class identity, children alive, social activity - friendship, education, children in weekly contact, religion and drinker. However, some variations were found among the three dependent variables, i.e., previous SRH for comorbidity (1st) and SRH (1st) compared to dementia (11th), grandchildren alive for SRH (6th) and dementia (4th) compared to comorbidity (9th), chronic diseases for comorbidity (6th) compared to SRH (10th) and dementia (10th). In terms of Shapley Additive Explanation (SHAP) values, the probability of dementia is expected to decrease by 5.57% in case a predictor grandchildren alive is included to the model. This study highlights the importance of social support for the prediction of poor self-rated health, dementia and their comorbidity. Specifically, the promotion of family support and friendship activity for elders would be vital for the prevention and management of their self-rated health and dementia.
Keywords:
self-rated health
; dementia
; family support
; friendship activity
; artificial intelligence
1. Introduction
Dementia can be defined as “deterioration in cognitive function beyond usual consequences of biological ageing” [1]. It comes from various conditions having major or minor effects on the brain. Its prevalence is more than 55 million in the world now, whereas its new incidences are almost 10 million on the globe every year [1]. Its global prevalence is expected to reach 153 million for the year 2050, while its global female-to-male ratio is projected to stay stable between 1.69 in 2019 and 1.67 in 2050 [2]. This global trend agrees with its local counterpart in Korea. The prevalence of elders’ dementia in the nation registered a growth from 5.9% to 7.3% (588,000) during 2015-2019 [3]. The direct, indirect and total cost of dementia in the nation expanded by 56%, 36% and 46% during 2015-2019, i.e., 1400 to 2191, 1485 to 2026, and 2885 to 4218 USD million, respectively [3].
On the other hand, self-rated health can be conceptualized as “the overall perception of one’s own health” [4,5,6,7,8,9]. It is usually assessed in a single item, where participants rate their current health. It is considered to be an effective indicator of health status on its own right but it is expected to affect other health outcomes such as mortality based on a variety of indirect channels, e.g., socioeconomic conditions, biological, physical and mental functions, as well as health-related behaviors [4,5,6,7,8,9]. For example, a previous study on self-rated health in Japan and Korea [9] reported positive effects from socioeconomic status, daily activity and physical exercise, as well as negative impacts from chronic disease, overweight/obesity and smoking. In a similar context, existing literature confirms a strong association between poor self-rated health and the risk of dementia [10,11,12,13,14].
However, little study has been done on social support, dementia and self-rated health. A previous study [15] made a rare contribution for this line of research to use a machine learning model for testing: whether social determinants are major determinants of the association among cerebrovascular disease, hearing loss and cognitive impairment in a middle-aged or older population (hypothesis 1); and whether the association among the three diseases is very strong in the middle-aged or older population (hypothesis 2). Data came from the Korean Longitudinal Study of Aging (2014-2016), with 6060 participants aged ≥ 53 years. The findings of this study supported the two hypotheses, highlighting the importance of preventive measures, family support, socioeconomic status and friendship activity for managing the three diseases. But this study did not examine whether there exists a variation among different diseases regarding the importance of social support. In this vein, this study evaluates the following hypotheses based on machine learning models:
Hypothesis 1.
The predictors of social support are major predictors of dementia, poor self-rated health and their comorbidity in the middle-aged or old
Hypothesis 2.
There exist some variations among dementia, poor self-rated health and their comorbidity in the middle-aged or old in terms of the importance of social support
2. Methods
2.1. Participants and Variables
The data source of this study was the Korean Longitudinal Study of Ageing (KLoSA) (2016-2018). This study did not require either the approval of the ethics committee or the informed consent of human subjects given that (1) data were publicly available (https://survey.keis.or.kr/eng/klosa/klosa01.jsp) and (2) data were de-identified (patient anonymity was preserved). This study used the recoded version of data for immediate analysis (“light version”). But there were still missing values in some independent variables hence they were replaced with their median values (median imputation). The final sample of this study consisted of 5961 subjects aged 56 or more. The dependent variables were: (1) poor subjective or self-rated health (SRH) with 5 categories (very good, good, middle, poor, very poor); (2) dementia (no, yes); and (3) their comorbidity with 4 categories (SRH very good, good or middle, dementia no; SRH very good, good or middle, dementia yes; SRH poor or very poor, dementia no; SRH poor or very poor, dementia yes). The KLoSA questions on dementia and poor self-rated health in 2016 and 2018 were “Since the last survey, have you ever been diagnosed by a doctor dementia? 1. Yes. 5. No.” and “How do you evaluate your health condition? 1. Very Good. 2. Good. 3. Middle. 4. Poor. 5. Very Poor.”.
The independent variables were the following 49 predictors in 2016: (1) 5-category SRH (very good, good, middle, poor, very poor); (2) demographic information including age, gender, marital status (married, separated, divorced, widowed, unmarried); (3) socioeconomic conditions such as educational level (elementary school or below, junior high school, senior high school, college or above), income (monthly, normalized between 0 and 1), health insurance (Medicare, Medicaid), economic activity (employed, unemployed); (4) social support, that is, friendship meeting, social activities (religious, friendship, leisure, association), grandchildren (alive, raised, taken care), children (alive, cohabiting, meeting, contact, proximity), brothers/sisters (alive, cohabiting), parents (alive, cohabiting, meeting, contact, proximity); (5) health-related information, i.e., body mass index, smoker (non, former, current), drinker (non, former, current); and (6) other determinants including region (big urban, small urban, rural), religion (non, Protestant, Catholic, Buddhist, Won-Buddhist, other), residential type (apartment, other), subjective class (high-A, high-B, middle-A, middle-B, low-A, low-B), life satisfaction - health (0-100), life satisfaction - economic (0-100) and life satisfaction - overall (0-100).
2.2. Analysis
Logistic regression and the random forest were compared for the prediction of dementia, SRH and their comorbidity. For the random forest, the number of trees was 100, the criterion of split was GINI and the max of depth was not determined. Data on 5961 participants were divided into training and validation sets with a 75:25 ratio (4471 vs. 1490 observations). Criteria for validating the models trained were (1) accuracy, a ratio of correct predictions among 1490 observations, and (2) the area under the receiver-operating-characteristic curve (AUC), the plot of sensitivity over 1 - specificity. Here, the AUC measures how much sensitivity can be secured in case the threshold of sensitivity increases from 0 to 1 (that is, specificity increases from 0 to 1). Variable importance from the random forest, a GINI gap between a complete model and a model excluding a certain variable, was used for testing the two hypotheses of this study. The evaluation of Hypothesis 1 was based on whether the predictors of social support are top-20 predictors of dementia, SRH and their comorbidity across board. The evaluation of Hypothesis 2 was based on whether some variations are found among dementia, SRH and their comorbidity in terms of the variable importance ranking of social support. Finally, the Shapley Additive Explanation (SHAP) values were calculated to analyze the direction of association between a major predictor and its dependent variable in the model (random forest). The SHAP value of a particular predictor for a particular observation measures a difference between what the model (the random forest) predicts for the probability of the dependent variable for the observation with and without the predictor (https://github.com/shap/shap). Python 3.52 (Centrum voor Wiskunde en Informatica, Amsterdam, Netherlands) was employed for the analysis on January 2023.
3. Results
Descriptive statistics for participants’ categorical and continuous variables are shown in Table 1 and Table 2, respectively. The proportions of those with SRH poor/very poor and dementia in 2018 were 28.7% (1712) and 1.5% (89), respectively. The proportion of those with either or both disease in 2018 was 28.8% (1717). The proportion of those with SRH poor/very poor in 2016 was 26.8% (1598). The average numbers of family members or the average frequencies of social activity in a month were 4 (grandchildren alive), 3 (friendship meeting), 3 (brothers/sisters alive), 3 (children alive), 2 (social activity - friendship) and 2 (children in weekly contact). In the case of median imputation for missing values, logistic regression and the random forest registered similar AUCs with the range of 0.80-0.87 (Table 3). These performance measures were higher than those in the case of piece-wise deletion for missing values, i.e., 0.27-0.84.
Based on random forest variable importance (Table 4), 18 out of top-20 predictors were identical for SRH, dementia and their comorbidity: previous SRH, life satisfaction - health, age, body mass index, income, chronic diseases, life satisfaction - economic, life satisfaction - overall, grandchildren alive, friendship meeting, brothers/sisters alive, class identity, children alive, social activity - friendship, education, children in weekly contact, religion and drinker. This result supports Hypothesis 1: The predictors of social support are major predictors of dementia, poor self-rated health and their comorbidity in the middle-aged or old. However, some variations were found among the three dependent variables, i.e., previous SRH for comorbidity (1st) and SRH (1st) compared to dementia (11th), grandchildren alive for SRH (6th) and dementia (4th) compared to comorbidity (9th), chronic diseases for comorbidity (6th) compared to SRH (10th) and dementia (10th). This finding supports Hypothesis 2: There exist some variations among dementia, poor self-rated health and their comorbidity in the middle-aged or old in terms of the importance of social support. In terms of SHAP, the probability of dementia is expected to decrease by 21% in case a predictor grandchildren alive is included to the model (Table 5 and Figure 1). There exists a strong negative association between the predictor grandchildren alive and the dependent variable dementia.
4. Discussion
Existing literature reports inconsistent results on social support and dementia [16,17,18]. A retrospective cohort study adopted 355 elderly Americans and linear regression to find that a positive association exists between perceived emotional support and the Repeatable Battery for the Assessment of Neuropsychological Status score (cognitive function) in women only [16]. A retrospective cohort study, which employed 5852 elderly Koreans and Cox proportional hazard regression, reached a similar conclusion with its U.S. counterpart, i.e., emotional support has its protective effect on incident dementia among women only [17]. On the contrary, a prospective cohort study employed 14,088 elderly Japanese and Cox proportional hazard regression to discover that the protective effect of family support on incident dementia exists among men only [18]. The SHAP results in Table 5 of this study show that there exists, in general, a strong negative association between the predictor social support and the dependent variable dementia among all participants. In terms of SHAP, for example, the probability of dementia is expected to decrease by 21% in case a predictor grandchildren alive is included to the model. Artificial intelligence is a data-driven approach hence more examination is needed for more conclusive findings on social support and dementia.
On the other hand, existing literature reports that poor self-rated health results in the increased risk of mortality [19,20]. In a retrospective cross-sectional study with 2819 breast cancer patients in the United States, poor self-rated health was found to have a positive association with cancer mortality with the hazard ratio of 3.05 [19]. In a retrospective cohort study with 710 elderly men in Europe, poor self-rated health was also discovered to have a positive relationship with cancer mortality with the hazard ratio of 2.41 [20]. In other words, poor self-rated health requests due attention to its fatal role in the risks of mortality. Moreover, poor self-rated health in the previous period was the most important predictor for the comorbidity of dementia and poor self-rated health in the current period based on the findings of this study. Based on random forest variable importance (Table 4) in this study, 18 out of top-20 predictors were identical for SRH, dementia and their comorbidity, and six of these top predictors represented social support i.e., grandchildren alive, friendship meeting, brothers/sisters alive, children alive, social activity - friendship and children in weekly contact. Little literature is available and more investigation is needed on dynamic interactions among social support, poor self-rated health and dementia in a variety of study populations in different environments. The SHAP value can be considered to be the weighted average of all possible real-world scenarios [21] hence explainable artificial intelligence based on the SHAP including this study can be a very attractive option for this line research.
This study had some limitations. Firstly, this study had limited memory capacity and used a weak version of the longitudinal design with data in two waves. Poor self-rated health, dementia and their comorbidity in 2018 (Wave 7) served as the dependent variable of the models, while, the three diseases in 2016 (Wave 6) and the demographic, socioeconomic and health-related factors in 2016 (Wave 6) served as the independent variables of the models. Expanding memory capacity and employing a strong version of the longitudinal design with data in all seven waves would strengthen the performance of explainable artificial intelligence. Secondly, this study kept outliers to protect the sample size. Comparing different outlier management strategies would further the horizon of research on this topic. Finally, sub-group analysis would make a good contribution for this line of research, e.g., 55-64, 65-74 and 75+ in age.
In conclusion, this study highlights the importance of social support for the prediction of poor self-rated health, dementia and their comorbidity. Specifically, the promotion of family support and friendship activity for elders would be vital for the prevention and management of their self-rated health and dementia.
Author Contributions
H.G.J., C.-W.K., H.P. and K.-S.L. designed the study. H.G.J., C.-W.K., H.P. and K.-S.L. collected, analyzed, and interpreted the data. H.G.J., C.-W.K., H.P. and K.-S.L. wrote and reviewed the manuscript. All authors approved the final version of the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the Ministry of Health and Welfare of South Korea under Korea Health Industry Development Institute grants (No. HI21C1560; HI22C1302 (Korea Health Technology R&D Project)). The funder had no role in the design of the study, the collection, analysis and interpretation of the data and the writing of the manuscript.
Data Availability Statement
The data used for this study are available from the Korean Longitudinal Study of Ageing (KLoSA) (https://survey.keis.or.kr/eng/klosa/klosa01.jsp).
Conflicts of Interest
The authors declare no conflict of interest.
References
- World Health Organization. Dementia. https://www.who.int/news-room/fact-sheets/detail/dementia (Accessed 27 December 2022; Updated 20 September 2022).
- GBD 2019 Dementia Forecasting Collaborators. Estimation of the global prevalence of dementia in 2019 and forecasted prevalence in 2050: an analysis for the Global Burden of Disease Study 2019. Lancet Public Health 2022;7:e105-e125.
- Shon C, Yoon H. Health-economic burden of dementia in South Korea. BMC Geriatr 2021;21:549-558. [CrossRef]
- Jylh¨a M. What is self-rated health and why does it predict mortality? Towards a unified conceptual model. Soc Sci Med 2009;69;307-316.
- Mavaddat N, Valderas JM, van der Linde R, Khaw KT, Kinmonth AL. Association of self-rated health with multimorbidity, chronic disease and psychosocial factors in a large middle-aged and older cohort from general practice: a cross-sectional study. BMC Fam Pract 2014;15:185. [CrossRef]
- Sargent-Cox K, Cherbuin N, Morris L, Butterworth P, Anstey KJ. The effect of health behavior change on self-rated health across the adult life course: a longitudinal cohort study. Prev Med 2014;58:75-80. [CrossRef]
- Harris SE, Hagenaars SP, Davies G, David Hill W, Liewald DCM, Ritchie SJ, Marioni RE; METASTROKE Consortium, International Consortium for Blood Pressure Genome-Wide Association Studies; International Consortium for Blood Pressure Genome-Wide Association Studies; CHARGE Consortium Aging and Longevity Group; CHARGE Consortium Cognitive Group; Sudlow CLM, Wardlaw JM, McIntosh AM, Gale CR, Deary IJ. Molecular genetic contributions to self-rated health. Int J Epidemiol 2017;46:994-1009.
- Stephan Y, Sutin AR, Bayard S, Kriˇzan Z, Terracciano A. Personality and sleep quality: evidence from four prospective studies. Health Psychol 2018;37:271-281. [CrossRef]
- Park JH, Lee KS. Self-rated health and its determinants in Japan and South Korea. Public Health 2013;127:834-843. [CrossRef]
- Weisen SF, Frishman WH, Aronson MK, Wassertheil-Smoller S. Self-rated health assessment and development of both cardiovascular and dementing illnesses in an ambulatory elderly population: a report from the Bronx Longitudinal Aging Study. Heart Dis 1999;1:201-205.
- Yip AG, Brayne C, Matthews FE; MRC Cognitive Function and Ageing Study. Risk factors for incident dementia in England and Wales: The Medical Research Council Cognitive Function and Ageing Study. A population-based nested case-control study. Age Ageing 2006;35:154-160. [CrossRef]
- Montlahuc C, Soumar’e A, Dufouil C, Berr C, Dartigues JF, Poncet M, Tzourio C, Alp´erovitch A. Self-rated health and risk of incident dementia: a community based elderly cohort, the 3C study. Neurology 2011;77:1457-1464.
- St John P, Montgomery P. Does self-rated health predict dementia? J Geriatr Psychiatr Neurol 2013;26:41-50.
- Aschwanden D, Aichele S, Ghisletta P, Terracciano A, Kliegel M, Sutin AR, Brown J, Allemand M. Predicting cognitive impairment and dementia: a machine learning approach. J Alzheimers Dis 2020;75:717-728. [CrossRef]
- Lee KS, Park KW. Social determinants of the association among cerebrovascular disease, hearing loss and cognitive impairment in a middle-aged or older population: recurrent neural network analysis of the Korean Longitudinal Study of Aging (2014-2016). Geriatr Gerontol Int. 2019;19:711-716.
- Pillemer SC, Holtzer R. The differential relationships of dimensions of perceived social support with cognitive function among older adults. Aging Ment Health 2016;20:727-735. [CrossRef]
- Oh DJ, Yang HW, Kim TH, Kwak KP, Kim BJ, Kim SG, Kim JL, Moon SW, Park JH, Ryu SH, Youn JC, Lee DY, Lee DW, Lee SB, Lee JJ, Jhoo JH, Bae JB, Han JW, Kim KW. Association of low emotional and tangible support with risk of dementia among adults 60 years and older in South Korea. JAMA Netw Open 2022;5:e2226260. [CrossRef]
- Murata C, Saito T, Saito M, Kondo K. The Association between social support and incident dementia: a 10-year follow-up study in Japan. Int J Environ Res Public Health 2019;16:239. [CrossRef]
- Adeyemi OJ, Gill TL, Paul R, Huber LB. Evaluating the association of self-reported psychological distress and self-rated health on survival times among women with breast cancer in the U.S. PLoS One 2021;16:e0260481. [CrossRef]
- Giltay EJ, Vollaard AM, Kromhout D. Self-rated health and physician-rated health as independent predictors of mortality in elderly men. Age Ageing 2012;41:165-171. [CrossRef]
- Panda C, Mishra AK, Dash AK, Nawab H. Predicting and explaining severity of road incident using artificial intelligence, SHAP and feature analysis. International Journal of Crashworthiness 2022. [CrossRef]
Figure 1.
Random Forest SHAP Dependence Plots for Dementia. Legend: The SHAP value of a particular predictor for a particular observation measures a difference between what the model (the random forest) predicts for the probability of the dependent variable for the observation with and without the predictor. In terms of SHAP, for example, the probability of dementia is expected to decrease by 21% in case a predictor grandchildren alive is included to the model.
Figure 1.
Random Forest SHAP Dependence Plots for Dementia. Legend: The SHAP value of a particular predictor for a particular observation measures a difference between what the model (the random forest) predicts for the probability of the dependent variable for the observation with and without the predictor. In terms of SHAP, for example, the probability of dementia is expected to decrease by 21% in case a predictor grandchildren alive is included to the model.
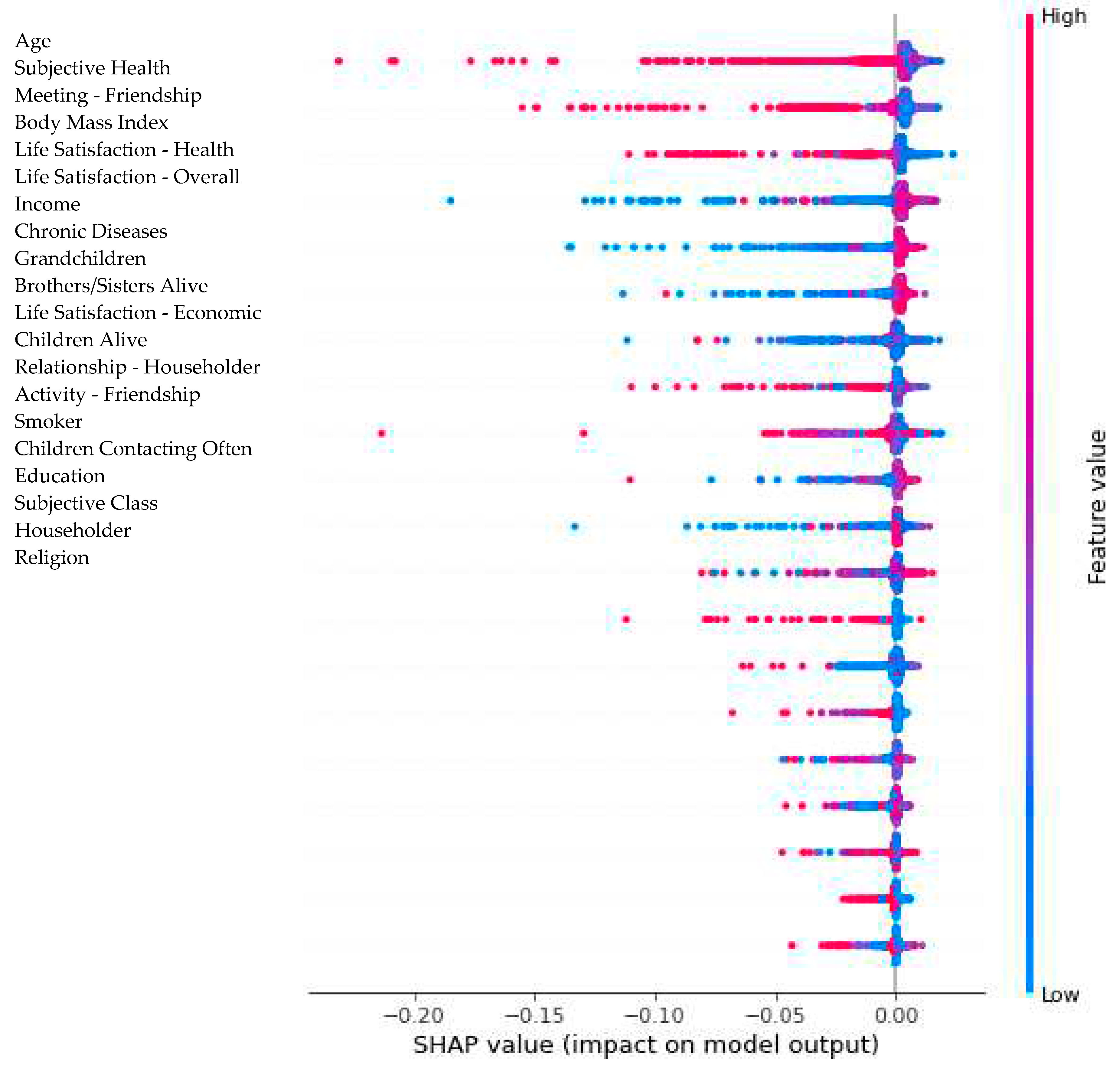

Table 1.
Descriptive Statistics for Participants’ Categorical Variables for Year 2018/2016.
| Variable | Count | Percentage (%) | ||
|---|---|---|---|---|
| Dependent Variables (in 2018) | ||||
| Comorbidity | ||||
| NNa | 4244 | 71.2 | ||
| YNb | 84 | 27.3 | ||
| NYc | 5 | 0.1 | ||
| YYd | 1628 | 1.4 | ||
| Subjective/Self-Rated Health | ||||
| Very Good | 81 | 1.4 | ||
| Good | 1471 | 24.7 | ||
| Middle (Neither Good nor Poor) | 2697 | 45.2 | ||
| Poor | 1332 | 22.3 | ||
| Very Poor | 380 | 6.4 | ||
| Dementia | ||||
| Yes | 89 | 1.5 | ||
| No | 5872 | 98.5 | ||
| Subjective/Self-Rated Health (in 2016 Hereafter) | ||||
| Very Good | 56 1587 |
0.9 | ||
| Good | 1587 | 26.2 | ||
| Middle (Neither Good nor Poor) | 2720 | 45.6 | ||
| Poor | 1307 | 21.9 | ||
| Very Poor | 291 | 4.9 | ||
| Householder | ||||
| Yes | 3378 | 56.7 | ||
| No | 2583 | 43.3 | ||
| Relationship - Householder | ||||
| Spouse | 5553 | 93.2 | ||
| Parents | 32 | 0.5 | ||
| Children not Married | 75 | 1.3 | ||
| Children Married | 276 | 4.6 | ||
| Brothers/Sisters | 9 | 0.2 | ||
| Grandchildren | 1 | 0 | ||
| Grandparents | 0 | 0 | ||
| Other | 15 | 0.3 | ||
| Gender | ||||
| Male | 2489 | 41.8 | ||
| Female | 3472 | 58.2 | ||
| Marriage | ||||
| Married | 4536 | 76.1 | ||
| Separated | 35 | 0.6 | ||
| Divorced | 121 | 2 | ||
| Widowed | 1228 | 20.6 | ||
| Unmarried | 41 | 0.7 | ||
| Grandchildren under Care, Aged Less than 10 | ||||
| Yes | 242 | 4.1 | ||
| No | 5719 | 95.9 | ||
| Grandchildren under Care, Aged Less than 10 (Last Year) | ||||
| Yes | 66 | 1.1 | ||
| No | 5895 | 98.9 | ||
| Parents Alive | ||||
| Father & Mother | 230 | 3.9 | ||
| Father | 93 | 1.6 | ||
| Mother | 886 | 14.9 | ||
| None | 4752 | 79.7 | ||
| Parents Cohabiting | ||||
| Yes | 170 | 2.9 | ||
| No | 5791 | 97.1 | ||
| Father Not Cohabiting | ||||
| Not Cohabiting with Other Children | 5921 | 99.3 | ||
| Cohabiting with Other Children | 38 | 0.6 | ||
| Other | 2 | 0 | ||
| Mother Not Cohabiting | ||||
| Not Cohabiting with Other Children | 5683 | 95.3 | ||
| Cohabiting with Other Children | 227 | 3.8 | ||
| Other | 51 | 0.9 | ||
| Health Insurance | ||||
| Health Insurance | 5673 | 95.2 | ||
| Medicare | 288 | 4.8 | ||
| Economic Activity | ||||
| Employed | 2210 | 37.1 | ||
| Unemployed | 3751 | 63 | ||
| Religion | ||||
| Non | 3412 | 57.2 | ||
| Protestant | 1011 | 17 | ||
| Catholic | 414 | 6.9 | ||
| Buddhist | 1082 | 18.2 | ||
| Won-Buddhist | 13 | 0.2 | ||
| Other | 29 | 0.5 | ||
| Drinker | ||||
| Current | 1931 | 32.4 | ||
| Former | 984 | 16.5 | ||
| Non | 3046 | 51.1 | ||
| Smoker | ||||
| Non | 4132 | 69.3 | ||
| Former | 1210 | 20.3 | ||
| Current | 619 | 10.4 | ||
| Education | ||||
| Elementary or Below | 2559 | 42.9 | ||
| Junior High | 1059 | 17.8 | ||
| Senior High | 1737 | 29.1 | ||
| College or Above | 606 | 10.2 | ||
| a | NN for | Subjective Health very good, good or middle | Dementia No | |
| b | YN for | Subjective Health poor or very poor | Dementia No | |
| c | NY for | Subjective Health very good, good or middle | Dementia Yes | |
| d | YY for | Subjective Health poor or very poor | Dementia Yes | |
Table 2.
Descriptive Statistics for Participants’ Continuous Variables for Year 2016.
| Variable | Mean | SD | Min | 25% | 50% | 75% | Max |
|---|---|---|---|---|---|---|---|
| Age | 69 | 9 | 55 | 61 | 68 | 76 | 100 |
| Meeting - Friendship | 3 | 3 | 0 | 1 | 3 | 4 | 10 |
| Activity - Religious | 1 | 3 | 0 | 0 | 0 | 0 | 16 |
| Activity - Friendship | 2 | 4 | 0 | 0 | 1 | 2 | 16 |
| Activity - Leisure | 0 | 2 | 0 | 0 | 0 | 0 | 16 |
| Activity - Association | 0 | 1 | 0 | 0 | 0 | 0 | 16 |
| Body Mass Index | 23 | 3 | 12 | 22 | 23 | 24 | 42 |
| # Chronic Diseases | 1 | 1 | 0 | 0 | 1 | 2 | 7 |
| # Children Alive | 3 | 1 | 0 | 2 | 3 | 4 | 9 |
| Income (Last Year) | 0 | 0 | 0 | 0 | 0 | 0 | 1 |
| # Children Cohabiting | 1 | 0 | 1 | 1 | 1 | 1 | 5 |
| # Children Cohabiting, Single | 1 | 0 | 1 | 1 | 1 | 1 | 4 |
| # Children Living Nearby* | 1 | 0 | 1 | 1 | 1 | 1 | 6 |
| # Children Meeting Often** | 1 | 0 | 1 | 1 | 1 | 1 | 6 |
| # Children Contacting Often** | 2 | 1 | 1 | 2 | 2 | 2 | 9 |
| # Grandchildren | 4 | 4 | 0 | 1 | 3 | 6 | 34 |
| # Grandchildren Under Care | 1 | 0 | 1 | 1 | 1 | 1 | 8 |
| # Grandchildren Under Care (Last Year) | 1 | 0 | 1 | 1 | 1 | 1 | 3 |
| # Brothers/Sisters Alive | 3 | 2 | 1 | 2 | 3 | 5 | 11 |
| # Brothers/Sisters Cohabiting | 1 | 0 | 1 | 1 | 1 | 1 | 5 |
| # Cohabiting Months with Father | 1 | 1 | 0 | 1 | 1 | 1 | 12 |
| # Cohabiting Months with Mother | 2 | 2 | 0 | 2 | 2 | 2 | 12 |
| Distance to Father*** | 3 | 0 | 1 | 3 | 3 | 3 | 4 |
| Monthly Frequency - Meeting Father | 7 | 0 | 1 | 7 | 7 | 7 | 9 |
| Monthly Frequency - Contacting Father | 4 | 0 | 1 | 4 | 4 | 4 | 8 |
| Distance to Mother*** | 3 | 0 | 1 | 3 | 3 | 3 | 4 |
| Monthly Frequency - Meeting Mother | 7 | 1 | 1 | 7 | 7 | 7 | 10 |
| Monthly Frequency - Contacting Mother | 4 | 1 | 1 | 4 | 4 | 4 | 10 |
| Life Satisfaction - Health | 59 | 19 | 0 | 50 | 60 | 70 | 100 |
| Life Satisfaction - Economic | 56 | 19 | 0 | 50 | 70 | 70 | 100 |
| Life Satisfaction - Overall | 63 | 16 | 0 | 50 | 70 | 70 | 100 |
| Subjective Class (1-6 Scale) | 4 | 1 | 1 | 4 | 4 | 5 | 6 |
Note: * Within 30-minute Distance by Public Transportation; ** Meeting Once or More Often a Week; *** Unit 30 Minutes: 1 30 Minutes, 2 60 Minutes, 3 90 Minutes, 4 120 Minutes.
Table 3.
Model Performance.
| Variable | Imputation | Deletion | ||||||
|---|---|---|---|---|---|---|---|---|
| Accuracy | AUC | Accuracy | AUC | |||||
| LR | RF | LR | RF | LR | RF | LR | RF | |
| Subjective Health | 0.55 | 0.58 | 0.82 | 0.80 | 0.56 | 0.58 | 0.82 | 0.80 |
| Dementia | 0.98 | 0.98 | 0.87 | 0.83 | 0.99 | 0.99 | 0.30 | 0.27 |
| Comorbidity | 0.79 | 0.80 | 0.87 | 0.87 | 0.79 | 0.8 | 0.83 | 0.84 |
Note: LR Logistic Regression, RF Random Forest, AUC Area under the Receiver-Operating-Characteristic Curve.
Table 4.
Random Forest Variable Importance.
| Comorbidity | Subjective Health | Dementia | |||
|---|---|---|---|---|---|
| Subjective Health - Previous Period | 0.1185 | Subjective Health - Previous Period | 0.0843 | Body Mass Index | 0.1013 |
| Life Satisfaction - Health | 0.0820 | Body Mass Index | 0.0738 | Age | 0.0903 |
| Age | 0.0746 | Income | 0.0732 | Income | 0.0847 |
| Body Mass Index | 0.0661 | Age | 0.0720 | # Grandchildren | 0.0646 |
| Income | 0.0645 | Life Satisfaction - Health | 0.0577 | Life Satisfaction - Health | 0.0490 |
| # Chronic Diseases | 0.0532 | # Grandchildren | 0.0456 | Life Satisfaction - Economic | 0.0484 |
| Life Satisfaction - Economic | 0.0497 | Life Satisfaction - Economic | 0.0454 | Meeting - Friendship | 0.0481 |
| Life Satisfaction - Overall | 0.0446 | Meeting - Friendship | 0.0416 | Life Satisfaction - Overall | 0.0469 |
| # Grandchildren | 0.0440 | # Brothers/Sisters Alive | 0.0409 | # Children Alive | 0.0461 |
| Meeting - Friendship | 0.0402 | # Chronic Diseases | 0.0403 | # Chronic Diseases | 0.0450 |
| # Brothers/Sisters Alive | 0.0334 | Life Satisfaction - Overall | 0.0388 | Subjective Health - Previous Period | 0.0433 |
| Subjective Class | 0.0316 | Subjective Class | 0.0327 | # Brothers/Sisters Alive | 0.0382 |
| # Children Alive | 0.0309 | # Children Alive | 0.0322 | # Children Contacting | 0.0299 |
| Activity - Friendship | 0.0282 | Activity - Friendship | 0.0315 | Subjective Class | 0.0280 |
| Education | 0.0264 | Education | 0.0265 | Religion | 0.0237 |
| # Children Contacting | 0.0233 | # Children Contacting | 0.0262 | Activity - Friendship | 0.0204 |
| Religion | 0.0206 | Religion | 0.0252 | Drinker | 0.0193 |
| Drinker | 0.0168 | Drinker | 0.0199 | Relationship - Householder | 0.0190 |
| Economic Activity | 0.0143 | Smoker | 0.0164 | Smoker | 0.0179 |
| Marriage | 0.0138 | Marriage | 0.0134 | Education | 0.0177 |
Table 5.
Random Forest Shapley Additive Explanation (SHAP) Values.
| Predictor/Dependent Variable | Comorbidity | Self-Rated Health | Dementia | |||
|---|---|---|---|---|---|---|
| Min | Max | Min | Max | Min | Max | |
| # Chronic Diseases | -0.0062 | 0.0024 | -0.1060 | 0.0811 | -0.0964 | 0.0107 |
| Subjective Health | -0.0079 | 0.0026 | -0.1788 | 0.2099 | -0.1336 | 0.0155 |
| Religion | -0.0008 | 0.0008 | -0.0172 | 0.0633 | -0.0297 | 0.0063 |
| Meeting - Friendship | -0.0017 | 0.0010 | -0.0646 | 0.0441 | -0.0966 | 0.0169 |
| Activity - Religious | -0.0005 | 0.0001 | -0.0320 | 0.0317 | -0.0468 | 0.0042 |
| Activity - Friendship | -0.0041 | 0.0017 | -0.0472 | 0.0910 | -0.0244 | 0.0077 |
| Activity - Leisure | -0.0003 | 0.0000 | -0.0278 | 0.0440 | -0.0105 | 0.0019 |
| Activity - Association | -0.0015 | 0.0031 | -0.0363 | 0.0961 | -0.1373 | 0.0014 |
| Householder | -0.0008 | 0.0011 | -0.0150 | 0.0148 | -0.0219 | 0.0063 |
| Relationship - Householder | -0.0006 | 0.0001 | -0.0239 | 0.0233 | -0.0509 | 0.0123 |
| # Children Alive | -0.0016 | 0.0039 | -0.0331 | 0.0378 | -0.0690 | 0.0100 |
| # Children Cohabiting | -0.0006 | 0.0001 | -0.0136 | 0.0254 | -0.0752 | 0.0031 |
| # Children Cohabiting, Single | 0.0000 | 0.0000 | -0.0071 | 0.0282 | -0.0094 | 0.0009 |
| # Children Living Nearby | -0.0014 | 0.0017 | -0.0214 | 0.0615 | -0.0295 | 0.0039 |
| # Children Meeting Often | -0.0008 | 0.0001 | -0.0103 | 0.0608 | -0.0440 | 0.0016 |
| # Children Contacting Often | -0.0008 | 0.0011 | -0.0435 | 0.0399 | -0.0382 | 0.0048 |
| # Grandchildren | -0.0011 | 0.0036 | -0.0478 | 0.0424 | -0.2100 | 0.0167 |
| Grandchildren Under Care | -0.0003 | 0.0000 | -0.0183 | 0.0180 | -0.0109 | 0.0013 |
| # Grandchildren Under Care | -0.0005 | 0.0000 | -0.0099 | 0.0056 | -0.0171 | 0.0020 |
| Grandchildren Under Care (Last Year) | 0.0000 | 0.0000 | -0.0099 | 0.0239 | -0.0003 | 0.0005 |
| # Grandchildren Under Care (Last Year) | 0.0000 | 0.0000 | -0.0006 | 0.0052 | -0.0002 | 0.0010 |
| # Brothers/Sisters Alive | -0.0008 | 0.0005 | -0.0271 | 0.0652 | -0.1114 | 0.0077 |
| # Brothers/Sisters Cohabiting | 0.0000 | 0.0000 | -0.0009 | 0.0031 | 0.0000 | 0.0000 |
| Parents Alive | -0.0002 | 0.0002 | -0.0248 | 0.0384 | -0.0024 | 0.0023 |
| # Cohabiting Months with Father | 0.0000 | 0.0000 | -0.0335 | 0.0129 | -0.0001 | 0.0001 |
| # Cohabiting Months with Mother | -0.0002 | 0.0001 | -0.0124 | 0.0284 | -0.0011 | 0.0010 |
| Parents Cohabiting | -0.0002 | 0.0000 | -0.0227 | 0.0183 | -0.0003 | 0.0003 |
| Father Cohabiting with Other Children | 0.0000 | 0.0000 | -0.0005 | 0.0137 | 0.0000 | 0.0002 |
| Distance to Father | 0.0000 | 0.0000 | -0.0180 | 0.0362 | 0.0000 | 0.0000 |
| Monthly Frequency - Meeting Father | 0.0000 | 0.0000 | -0.0257 | 0.0235 | 0.0000 | 0.0000 |
| Monthly Frequency - Contacting Father | 0.0000 | 0.0000 | -0.0254 | 0.0233 | -0.0001 | 0.0003 |
| Mother Cohabiting with Other Children | 0.0000 | 0.0000 | -0.0230 | 0.0204 | -0.0002 | 0.0008 |
| Distance to Mother | -0.0001 | 0.0001 | -0.0146 | 0.0330 | -0.0002 | 0.0002 |
| Monthly Frequency - Meeting Mother | -0.0002 | 0.0000 | -0.0151 | 0.0694 | -0.0006 | 0.0001 |
| Monthly Frequency - Contacting Mother | -0.0004 | 0.0001 | -0.0336 | 0.0501 | -0.0003 | 0.0003 |
| Education | -0.0022 | 0.0017 | -0.0416 | 0.0753 | -0.0463 | 0.0074 |
| Gender | -0.0011 | 0.0007 | -0.0130 | 0.0196 | -0.0108 | 0.0058 |
| Age | -0.0016 | 0.0028 | -0.1215 | 0.1101 | -0.2239 | 0.0176 |
| Marriage | -0.0034 | 0.0011 | -0.0434 | 0.0252 | -0.0166 | 0.0092 |
| Body Mass Index | -0.0015 | 0.0065 | -0.0510 | 0.0817 | -0.1325 | 0.0136 |
| Smoker | -0.0014 | 0.0014 | -0.0217 | 0.0376 | -0.0318 | 0.0042 |
| Drinker | -0.0010 | 0.0011 | -0.0146 | 0.0353 | -0.0321 | 0.0064 |
| Health Insurance | -0.0012 | 0.0000 | -0.0308 | 0.0224 | -0.0264 | 0.0022 |
| Economic Activity | -0.0018 | 0.0014 | -0.0159 | 0.0375 | -0.0101 | 0.0029 |
| Income | -0.0011 | 0.0018 | -0.0467 | 0.0961 | -0.0827 | 0.0162 |
| Life Satisfaction - Health | -0.0040 | 0.0017 | -0.0948 | 0.0935 | -0.0769 | 0.0101 |
| Life Satisfaction - Economic | -0.0029 | 0.0009 | -0.0699 | 0.0635 | -0.1263 | 0.0125 |
| Life Satisfaction - Overall | -0.0028 | 0.0042 | -0.0345 | 0.0558 | -0.0428 | 0.0074 |
| Subjective Class | -0.0019 | 0.0037 | -0.0636 | 0.0720 | -0.0389 | 0.0087 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



