
Submitted:
19 September 2023
Posted:
21 September 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Because of ambiguous and widely debated observations concerning incidence trend and management of TC, we performed this analysis. We drew attention to some events, such as “cancer screening activity,” introduction of noninvasive follicular neoplasm with papillary-like nuclear features (NIFTP) to TC types, possibility of papillary thyroid microcarcinoma (PTMC) active surveillance (AS), occurrence of personalized medicine in TC management and finally COVID-19 pandemic time. Because of the opinion that all changes have been made mostly by PTC, we compared it to the rest of types of TC in terms of incidence, clinical and pathological characteristics and treatment. The prevalence of TC significantly increased from 5.15% in 2008 to 13.84% in 2015 and then significantly decreased to 1.33% in 2022 when the pandemic lasted (p<0.0001). A similar trend was observed for PTC, when the incidence significantly increased to 13.99% in 2015 and then decreased to 1.38% in 2022 (p<0.0001). At that time, the NIFTP category was introduced, and observation of PTMC began. The prevalence of FTC and MTC also increased until 2015 and then decreased. Significant differences in age, types of surgery, necessity of reoperation, pTNM, between PTCs and other types of TCs were observed. The average age was significantly lower in PTC patients than in patients with the remaining types of TC (p<0.0001). Four milestones, including NIFTP introduction, the possibility of PTMC AS, personalized cancer medicine and the COVID-19 pandemic, may have influenced the general statistics of TC.
Keywords:
thyroid cancer management
; incidence trends
; NIFTP
; PTC
; personalized medicine
; COVID-19
; cancer screening activity
1. Introduction
The rapid increase in the detection rate of thyroid cancer (TC) over recent years has caused many changes in the management of these malignancies. TC accounts for 3.4% of all cancers diagnosed annually worldwide [1]. Some data suggest that TC is increasing globally much faster than other malignant lesions [2,3]. It might be a consequence of widespread use of ultrasonography (US) examination and ultrasound guided fine needle aspiration biopsy (UG-FNAB) procedures. Generally, this observation led to the globally highlighted discussion about the causes of such a situation. Some authors say that the higher incidence of TC is due to overdiagnosis [3]. Others believe that various additional factors may play a role in this observation, such as obesity and increased exposure to ionizing radiation [4]. However, the fast increase in the occurrence of TC was observed to evolve to a point of slowing down and even reversing, which might be due to certain worldwide events. Some of them might be the introduction of noninvasive follicular neoplasm with papillary-like nuclear features (NIFTP) as a TC type, the possibility of papillary thyroid microcarcinoma (PTMC) active surveillance (AS), the occurrence of personalized medicine in TC management and finally the COVID-19 pandemic time. This phenomenon of TC occurrence is still debated and worthy of further investigation. When we start from TC with the most favorable prognosis, we have papillary TC (PTC) and follicular TC (FTC). Both of them are known as well-differentiated TC (WDTC). Next, we have medullary TC (MTC), which is the only type that arises from C cells of the thyroid gland, poorly differentiated TC (PDTC), and anaplastic TC (ATC). ATC is the most aggressive and unfavorable form (1-3). These five main forms of TC present tremendous variability in clinical course, histopathology, biological presentation, and, of course, prognosis. Four of them arise from thyroid follicular cells (PTC, FTC, PDTC, ATC). It is obvious that the heterogeneity of these four types of TC comes not only from histological diversity but also from genetic and epigenetic alterations, interactions between tumor cells and surrounding tissues forming specific microenvironments, and interhuman differences [1]. Even in ultrasound scans, many PTCs present irregular borders and infiltration of the surrounding thyroid physiological tissues. However, as a tumor assigned to the WDTC category, PTC very often contains a capsule, which makes it similar to noninvasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP). The introduction of NIFTP to thyroid tumor types might have had some influence on TC occurrence and surgical management.
Generally, WDTCs are indolent tumors characterized by an excellent prognosis. Almost all of them present a good response to standard therapeutic treatment. The 10-year survival rate is estimated to be 90% [2,3]. However, unfortunately, 10% of all patients with WDTC die because of this tumor [1].
The rapidly increasing number of TCs observed worldwide has forced scientists to debate whether it is a TC epidemic time or whether it is caused by the availability of better, more accessible diagnostic tools [2]. Moreover, the high diagnostic sensitivity of thyroid nodule stratification and its important role in the identification, management and monitoring of these lesions was not limiting. This observation brought clinicians and scientists to the introduction of personalized cancer medicine in clinical practice. Although the majority of TCs are derived from one type of cell, these malignancies represent a very heterogeneous group of tumors.
The next important event, which might influence TC management, was the possibility of TC AS in clinical practice. Currently, AS might be a potential option for the management of patients with PTMC. Nevertheless, the decision to treat the patients in this way should be made with information that reliably indicates that there is a low-risk tumor.
Because of these four important events, i.e., NIFTP introduction, possibility of PTMC AS, appearance of personalized medicine in clinical practice and finally COVID-19 pandemic time, we decided to analyze the changes in the occurrence and management of TC during the last 14 years.
2. Materials and Methods
We retrospectively analyzed 5806 medical records of patients admitted and surgically treated in the Department and Clinic of General, Minimally Invasive and Endocrine Surgery due to thyroid nodules (TNs) between January 2008 and December 2022. The selection of the study group is presented as a flow diagram (Figure 1).
The study protocol was approved by the Institutional Review Board and Ethics Committee of Wroclaw Medical University, Wroclaw, Poland (No: KB 783/2023). All our patients provided admission informed consent, which stipulated that the results may be used for research purposes. The data were analyzed retrospectively and anonymously from established medical records. The authors did not have access to identifying patient information or direct access to the study participants.
From a retrospective series of the thyroid surgical specimens archived in one center, 678 (11.7%) malignant thyroid tumors were obtained. All of the patients with malignant thyroid tumor resection had a minimum of one UG-FNAB performed before surgery. All cytological specimens were evaluated according to The Bethesda System for Reporting Thyroid Cytopathology (TBSRTC) introduced in 2009 [5] and reclassified in 2017 [6,7]. In all of the neoplasms, pTNM parameters were analyzed. All of the patients were evaluated, and the following parameters were recorded: sex, age, tumor size, tumor shape, echogenicity, microcalcifications, vascularity, and type of tumor (solitary, multifocal, bilateral).
We drew attention to some events, such as NIFTP introduction to thyroid tumor types, the possibility of PTMC observation in TC management, personalized medicine dissemination in recent years and the COVID-19 pandemic. We checked whether “cancer screening activity” was depressed by the mentioned world events. We analyzed whether these events may have influenced the diagnostics, approach and management of TC. Because of the opinion that all changes in the field of TC have been made mostly because of PTC, we also compared the most common type of TC, i.e., PTC, to the reemaining types of TC in terms of incidence, clinical and pathological characteristics and treatment.
2.1. Statistical Analysis
Data analysis was conducted using Ms Excel and Statistica 13.3 software (Tibco Software Inc., Palo Alto, CA, USA). The Kolmogorov‒Smirnov test was employed to evaluate the data distribution. Descriptive data are presented as the number of observations (percent) or mean ± standard deviation (mean ± SD). The Chi-square test or Fisher’s exact test was used to analyze qualitative data. Student’s t test was employed to compare quantitative data between two independent study groups. All values of p<0.05 were considered statistically significant.
3. Results
Overall, 678 out of 5806 (11.7%) were recruited as malignant tumors due to satisfying all required diagnostic criteria. Therefore, the study consisted of a group of PTC, FTC, MTC, undifferentiated TC (UTC), sarcoma, lymphoma, squamous cell carcinoma, myeloma and secondary tumors in a 14-year-long period (2008-2022). Table 1 presents the demographics and clinical and tumor characteristics of the TC group and two subgroups of TC: PTC and the remaining types of TC (Table 1).
There were 581 (85.69%) female patients and 97 (14.30%) males in the TC group. The average age at diagnosis was 51.66 ± 15.98 years old (range 18-81 years). The largest subgroups of TC patients were PTC—579 patients (85.39%), FTC—31 (4.57%) and MTC—24 (3.53%). Significant differences in age, types of surgery, necessity of reoperation, pTNM, pT, pN and pM were observed between PTC and patients with other types of TC (Table 1). The average age was significantly lower in PTC patients than in patients with the remaining types of TC (p<0.0001). Total thyroid resection was performed significantly more often in PTC patients than in patients with other types of TC (p<0.0001). Patients with other types of TC significantly more often required reoperation (p=0.002). In the PTC subgroup, significantly higher rates of pTNM stage I were observed, and in other types of TC, the prevalence of pTNM stage IV was significantly higher than that in PTC (p<0.0001). Among the subgroup of patients with other types of TC, the rates of pT4b, pN1b and pM1 were significantly higher in comparison to PTC patients (p<0.0001 for all).
The UG-FNAB results were available in all cases (100%). The selected ultrasound features in the total group of TC, PTC and other types of cancer are presented in Table 2. A significantly higher rate of tumor size above 5 mm, irregular tumor shape, hypoechogenicity, presence of microcalcifications and high vascularity was observed in the subgroup of patients with other types of TC than in patients with PTC (p<0.05 for all).
The prevalence rates of benign thyroid tumors and thyroid cancers (TCs) from 2008 to 2022 are shown in Table 3 and Figure 2. The prevalence of TC significantly increased from 5.15% in 2008 to 13.84% in 2015, and then the incidence of TC significantly decreased to 1.33% in 2021 and 2022 (p<0.0001).
A similar trend was observed for PTC, where the incidence of cases significantly increased to 13.99% in 2015 and then significantly decreased to 1.38% in 2021-2022 (p<0.0001) (Table 4 and Figure 2). The prevalence of FTC and MTC also increased until 2015, and then a decrease in the rate of cases of these types of TC was observed.
In Figure 4, we present the incidence of malignant thyroid tumors, i.e., all TC patients and PTC patients with respect to the sex of individuals in 2008-2022 (Figure 4).
In Figure 5 and Figure 6, we present the incidence of malignant thyroid tumors, i.e., all TC patients and PTC patients with respect to age (<55 years old vs. >55 years old) and the incidence of PTC patients with respect to tumor size (<5 mm vs. >5 mm) in 2008-2022 (Figure 5 and Figure 6, respectively).
4. Discussion
In recent years, the number of TCs has increased; however, almost 60-70% of them are low-risk PTMCs [8,9,10,11]. However, heterogeneity, even in such a homogenous group of tumors, can also be observed [9,10,11]. First, there might be multiple lesions. Multifocal unilateral or bilateral PTC is also not very rare [12]. This feature of PTC is not always connected with heterogeneity at the molecular and gene levels; however, some authors confirm the high rate of molecular variation within one tumor [13,14,15]. In our study, the majority of TCs in recent years were PTCs below 1 cm in dimension (PTMC, pT1a). The next largest group of TCs was also PTC but in lesions sizes of above 1 cm to 2 cm in diameter (pT1b). We did not observe it in the remaining TC types. In this group of patients, the smallest tumors (pT1a) constituted the smallest group. Therefore, we confirmed in our analysis that in recent years, the majority of TCs are still small tumors, mostly less than 1 cm in diameter.
As mentioned previously, WDTCs are generally indolent tumors characterized by an excellent prognosis, although some authors observe a high rate of WDTC recurrence worldwide [16,17]. A completely different situation occurs in the case of PDTC and ATC. Both of these tumors present a dramatically poor prognosis. One of the reasons for this situation is resistance to radioiodine therapy. In our analysis, among PTC patients, the largest group comprised patients who did not require surgery after the first surgical intervention. This might be because of the previously mentioned characteristic that many of them were diagnosed in the very low stage of disease. Unfortunately, we did not observe such a situation in the case of other TCs. In this group of neoplasms, many individuals required reoperation due to nonradical primary treatment or tumor recurrence.
The majority of PTC cases are associated with additional TC foci localized in the same or second lobe of the thyroid gland. This characteristic pathological feature of PTC is estimated for 18-87% of all PTCs [1,18,19]. For many years, the debate might be observed regarding whether such PTC features come from autonomous multiple independent tumors or are a consequence of intrathyroidal spread of the primary PTC focus. Currently, on the basis of many studies, both theories of PTC multiplicity are still valid [20,21]. However, some authors emphasize that while the BRAF V600E mutation is observed in the primary tumor, it is very often not observed in LNM and coexisting lesions [22]. In our opinion, there might also be a situation in which the ipsilateral or contralateral PTC additional foci without the BRAF V600E mutation metastasize to the lymph nodes, so they are not presented in the cancer genetic profile. However, we can also suggest that this mutation can develop de novo in metastatic PTC cells. However, we estimated that the multifocality of neoplasms is not characteristic of PTC only. We observed the same characteristic in the remaining TCs. A different situation exists regarding bilaterality. This histopathological feature remains characteristic of PTC.
A rapidly increasing number of TCs has been observed worldwide [2,16,23]. Currently, we notice widespread application of neck ultrasound examination and, consequently, a large number of UG-FNABs of thyroid nodules [24]. This observation occurs despite the proposal and introduction of the American Thyroid Association (ATA) Guidelines in 2016 [25,26]. In one of our previous studies, we called this phenomenon “cancer screening activity” [24]. Indeed, in our analysis, we observed this phenomenon in our study population up to 2016. At that point, new cases, especially small PTCs, were diagnosed. After that year, some new world events appeared. They probably influenced this phenomenon and changed the TC number tendency.
Currently, the treatment of TC patients depends on the characteristics of histopathological samples obtained from tumors after surgery. Such a clinical approach applies to all forms of TC, especially follicular types, and all forms of WDTCs. AS is one of the potential options for the management of patients with PTMC. Generally, PTMC grows slowly and has indolent biological behavior. The rate of local recurrence is estimated as 2-6%, and distant metastasis is extremely rare and is observed in 1-2% of cases [27,28]. Some authors suggest that even when local or regional metastases and disease progression appear, such a clinical situation does not worsen the prognosis [29]. It is obvious that delayed surgery is mandatory. On the basis of many studies, AS was introduced in some countries, such as the United States, Korea and Japan, as a potential management strategy for low-risk PTMC and as an alternative to immediate surgery [25,30,31,32,33,34]. However, in fact, in many countries, immediate surgery is the first-line and routine treatment in many cases of PTMC [25,35]. The authors highlight some advantages of this option, such as simple removal of the malignant tumor, feasible and easier follow-up, decreased risk of secondary surgeries and, perhaps the most valuable for many patients, elimination of the inherent anxiety connected with awareness of having a malignant tumor. On the other hand, we must remember some potential complications that might occur after surgical treatment [36,37,38]. There is an open question or unsolved dilemma regarding which quality of life is lower, living with potential complications after surgery or living with awareness of malignant tumors inside. However, the main question stands—not about tumor progression or local or regional metastasis, because it has been estimated that delayed surgery guarantees favorable outcomes; rather, the main question relates to the risk of potential distant metastasis in the AS period and whether the prognosis in such a clinical situation is worse. Some autopsy studies revealed the high prevalence of small, subclinical TC, particularly PTMC [39]. Hugen et al. [40] showed in a national Dutch autopsy study that distant metastases were revealed in 8.9% of cases with PTC and in 19% of individuals with FTC in whom TC was first diagnosed on autopsy. In our analysis, distant metastases were observed much less frequently in the PTC group than in the remaining TC patients (3.45% vs. 26.53%). Therefore, this observation confirms that AS might be a good therapeutic option for some PTMC patients. In Poland, the discussion about AS as a potential therapeutic option for some individuals harboring PTMC started in 2016 [24]. Therefore, after this point in time, a slight decrease in the number of new TC cases was observed. Thyroid gland US examination enables the detection of even small TCs. At the time of this diagnosis, the main question appears whether to observe or excise the tumor. This is the crucial question addressed by surgeons at this time in PTMC management. Ito and Tuttle stated that AS is a safe alternative to immediate surgery but only for selected patients [41,42]. Therefore, the question is which patients? How do we select the patients in routine clinical practice and possibly do so without increasing costs? The second question is whether patient selection is effective. Many younger individuals prefer AS over immediate surgery; however, according to some authors, younger age is associated with a higher rate of TC growth [29,42]. Heterogeneity of thyroid cells applies to tumor and stromal tissues. Tumor cells may exhibit follicular differentiation, perifollicular differentiation, or both types of differentiation or dedifferentiation. Due to the two main hypotheses of carcinogenesis, we can form some clinically pragmatic observations. The first is that tumor growth is a consequence of genome instability of somatic cells, which may lead to the selection of more aggressive clones and thus more aggressive TC types [43,44]. This is known as a multistep carcinogenesis model [1,43,44]. The second hypothesis is that in the primary tumor, there are small populations of stem cells, which, after certain mutations or genetic and epigenetic transformations, may produce phenotypically totally different cells of TC, very often more aggressive ones. This second theory, known as the cancer stem cell model, was first presented by Mitsutake et al. [45] in 2007. On the basis of these two theories, we can assume that PDTC and ATC may come from WDTCs, and consequently, when we treat patients with WDTC, some of them might be patients with early-stage PDTC or ATC. We are aware that this is a controversial question; however, in our clinical practice, there is some evidence to draw attention to this issue. PDTC is characterized by expansive growth, an incomplete capsule, an increased number of tumor-associated macrophages, and low lymphocyte and dendritic cell infiltration compared to PTC [46,47]. Additionally, the BRAF V600E mutation is also frequently observed in PDTC connected with PTC nuclear features or even PTC foci. Currently, ATC is considered the most heterogeneous TC. Moreover, it is still an extremely invasive thyroid neoplasm with extensive infiltration of the lymph nodes and surrounding soft neck tissues and organs. One “optimistic” feature, if we can express it in this way, is that similar to encapsulated PDTC, encapsulated types of ATC sometimes might present a slightly better prognosis with an overall survival time up to 57 months [48,49]. In our group of ATC patients, we noticed that a well-defined, nonruptured ATC capsule was a good prognostic factor of ATC regardless of some other ultrasound and pathologic features.
In 2017, the WHO established a new classification for endocrine tumors [50,51,52]. It elaborated and published the criteria for a new endocrine tumor, which was named noninvasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP). Unfortunately, NIFTP can be described only on the basis of the surgical specimens, and its final histological diagnosis is possible after surgery. Its great utility and usefulness of this new classification, especially in clinical practice, is well established. In our study, according to the ATA classification, after 2017, we excluded all NIFTP entities from the TC group and included them in the benign tumor group. This might be the next reason for the decrease in TC number after 2016. As clinicians, we should know that NIFTP has to exhibit a well-defined capsule, a sharply separated nodule mass from the thyroid tissue and no infiltration. The pattern of architecture of this nodule is follicular but with nuclear characteristics, which are similar to those of classical PTC. Despite a precise description of NIFTP and its great clinical utility, there are some fundamental questions that still do not have accurate answers. For example, the minimal and maximal sizes of NIFTPs are not specified; however, many scholars describe these tumors as lesions with dimensions of 1 cm or more [53,54,55]. Interestingly, NIFTP is currently recognized as a benign tumor; however, it is still very often treated as TC. Generally, these tumors present an indolent course and do not present a genetic profile characteristic of malignant entities. Therefore, in our patients, all of those who harbored NIFTP underwent molecular testing according to BRAF 600 mutation to exclude TC diagnosis. This test is performed in an oncological center, in which all patients with NIFTP are reconsulted and potentially treated.
In the analyzed period, we noticed a fast increase in TC incidence up to 2015/2016. We observed that the occurrence slowed down and even reversed after this point in time—especially in small entities of PTC, in likely response to some clinical, histopathological, sociological and epidemiological events. At the very beginning of our observation period, high-resolution imaging techniques were introduced to detect even small TNs. Because of widespread US and UG-FNAB, an increased detection rate of PTC was observed. However, it was not connected with any benefits, such as reduced mortality risk [56]. Given such observation, ATA guidelines did not recommend biopsy of small nodules, especially below 5.0 mm in diameter [25]. However, in our patients, we did not observe important differences after this time in the PTC group or in the remaining TCs.
Despite the indolent nature of some PTCs and the majority of PTMCs, the words “cancer” or “carcinoma” included in their names cause unnecessary fear and anxiety in patients. Moreover, these terms very often force surgeons to perform aggressive procedures such as total thyroidectomy with lymphadenectomy of the central and even lateral compartments. However, currently, the treatment of some benign tumors, such as NIFTP, is still controversial. Some authors recommend total thyroidectomy in cases of NIFTP because, in their opinion, this tumor is often multifocal or bilateral with lymph node metastases [57]. Nevertheless, others say that PTC and NIFTP, with diameters of 1-4 cm, surgically treatment by thyroidectomy or lobectomy with lymphadenectomy would provide comparable oncologic outcomes [58]. In cases of larger tumors, i.e., more than 4 cm in diameter, the main question is whether only surgical treatment is sufficient or whether complete radioiodine therapy with TSH suppression should also be added. ATA guidelines recommend two-step therapy options, i.e., surgery with radioiodine therapy completion [25]. However, there are also authors who do not accept this approach and say that even larger tumors may be treated less aggressively [59]. Generally, the majority of NIFTP tumors, even those with dimensions greater than 4 cm, are treated as indolent nodules, and radioiodine therapy or suppressive doses of levothyroxine are avoided. In our group of patients with NIFTP diagnosis, surgery was provided for everyone as the only target therapy. During the observation time, we did not observe any recurrence or metastases. However, our observation time may be too short to form any conclusions. In any event, our observations are in accordance with some other authors, who also followed up patients with multifocal or bilateral NIFTP [60]. Others emphasize that because of these clinical and pathological characteristics of NIFTP, patients should be strictly observed after lobectomy [61]. We absolutely agree with these authors, and we practice according to these recommendations.
PTC very often exists as an accompanying lesion, i.e., one tumor diagnosed presurgically as PTC is found microscopically after surgery to be composed of a minimum of two subtypes of PTC. Even homogenous types, such as the classical variant of PTC (CVPTC), are very often accompanied by the follicular variant of PTC (FVPTC) [1]. It is extremely important to diagnose all of the components of PTC nodules if one of them represents a more aggressive type. Some authors emphasize that such uneventful characteristics, such as metastasis or recurrence, are just produced by its aggressive part [62]. LiVolsi [62] noticed that a worse prognosis of PTC is made by the higher percentage of coexistence of tall-cell variant PTC (TCVPTC). However, as some authors say, it is not established what minimal percentage of the component of TCVPTC is required to diagnose the cancer as TCVPTC, and they say approximately 10-70% of cells are reported [63]. According to the latest data, a minimum of 50% of TCVPTC in PTC nodules should be diagnosed as TCVPTC [62]. Of course, there might be some tumors that include two or more subtypes or variants of PTC, and more interestingly, both might be on the same level of clinical importance. Baloch et al. [64] described a patient with a malignant tumor consisting of TCVPTC and Hurthle cell cancer. It had clinical consequences because TCVPTC metastasized to regional lymph nodes, but Hurthle cell cancer metastases were observed in the lungs [64]. Several years ago, we performed studies in which we analyzed many cases of PTC and PTMC with completely different clinical courses and prognoses [15,65]. However, we did not have accurate and detailed histopathological descriptions of every single microcarcinoma. Currently, it is well established that the different clinical courses, potential metastasis and recurrence depend on histological subtypes and variants. In our group of patients with a very unfavorable clinical course, after some specimen reclassification, we diagnosed three cases of hobnail variant PTC (HVPTC) in heterogeneous PTC cases along with TCVPTC and anaplastic thyroid cancer. Baloch et al. [66] assessed that HVPTC may account for approximately 30% of all PTC subtypes. Moreover, approximately 50% of HVPTC lesions represents distant metastases to the brain, lungs, liver and bones [66]. Other authors proved that HVPTC was significantly associated with lymph node metastasis (LNM) [67].
It was estimated that appropriate individuals for AS are patients with characteristics as follows: well-defined solitary nodules equal to or less than 1-1.5 cm in dimension, diagnosed with PTC with at least 2 mm of noninfiltrated thyroid tissue surrounding the tumor, without pathological lymph nodes, and older age [68,69]. The molecular profile of TC is currently not mandatory and is considered additional information in AS and patient selection [70]. Tuttle et al. [68] estimated that patients with PTC and multiple driver events, such as BRAF V600E+TERT and RAS+TERT, were not appropriate candidates for AS. Regarding some clinical and ultrasound features, Sakai et al. [71] noticed that high vascularity and calcifications predispose tumors to faster growth, which makes them inappropriate for AS.
In our opinion, AS is one of the most responsible methods of PTC patient management. It requires many ultrasound examination skills on the part of the attending physicians. The patient has to agree to long-term observation methods, so a high level of understanding of PTC behavior is absolutely needed. Such a clinical approach to PTC patients is called personalized medicine, which in Poland has been widely promoted since 2017 [24].
The next clinical dilemma connected with patients with small PTC, which is currently also under debate, is the extent of surgery. As far as recommendations, for small PTC, i.e., equal to or below 1.0 cm in diameter, guidelines are clearly established. Larger tumors are treated more variably. During the last fourteen years of observation, the approach to diagnosis and treatment of patients with thyroid cancer has changed based on better diagnosis and faster detection. Although thyroid surgery, radioactive iodine therapy, and TSH suppression continue to be the mainstay of treatment, current knowledge has allowed the treatment of people with low-risk differentiated thyroid cancer to be de-escalated. Treatment options for patients with aggressive thyroid tumors have also been expanded. In addition, over the past 14 years, advances in knowledge of the molecular aspects of thyroid cancer have improved the diagnosis of TC and enabled individualized treatment options for selected patients with the most aggressive form of the disease. The guidelines of many societies around the world reflect these changes and include a focus on adopting a more individualized approach to clinical management. Some management aspects of TC treatment, which were impossible some years ago, such as AS of selected small TCs or monitoring small TNs without UG-FNAB, are currently implemented and are even clinical routine in some departments. Regarding the surgical treatment of TC, there is more acceptance of hemithyroidectomy for low-risk TC. However, we must remember the challenges resulting from these new approaches to TC management, such as long-term follow-up costs, patient and clinician anxiety and uncertainty in thyroglobulin (Tg) monitoring after nonradical treatment. However, personalized medicine in the management of TC is currently well established, and it will probably remain for a long time.
Our study has some limitations. First, it is a retrospective study, so some inaccuracies typical of such studies were unfortunately present. Second, the work was performed at a single institution. Third, the number of patients was not very high. Fourth, one of the inclusion criteria of this study was obtaining histopathology results, so the study included selection bias because we evaluated only patients with malignant tumors who underwent surgery. However, the histopathology results of all patients were mandatory for this study to form any conclusions. Fifth, the analyzed patients did not undergo molecular tests, so no correlation to pathological diagnosis was estimated. We are aware that this information would be the most valuable, especially in patients in whom AS and personalized medicine approaches were taken into consideration.
In conclusion, during the time when “cancer screening activity” was widely observed, four world events, i.e., the possibility of PTMC AS in clinical practice, NIFTP introduction to TNs and exclusion from TC types, personalized medicine occurrence in the field of TC approach and COVID-19 pandemic time, were observed. They may have influenced the general statistics of TC, including the number of new cases and trends in clinical management.
Author Contributions
Conceptualisation, KK; methodology, KK and DD; software, KK and DD; validation, KK and DD; formal analysis, KK and DD; investigation, KK, MM, KJ, MK, SM, AD, SB, ML, BL, KSS, MS, PD, KS and BW; resources, KK, DD, MM, KJ, MK, SM, AD, SB, ML, BL, KSS, MS, PD, KS and BW; data curation, KK, DD, MM, KJ, MK, SM, AD, SB, ML, BL, KSS, MS, PD, KS and BW; writing - original draft preparation, KK and DD; writing—review and editing, KK; visualization, KK; supervision, KK, DD and BW; project administration, KK; funding acquisition KK. All authors have read and agreed to the published version of the manuscript.
Funding
This study was supported by the Internal Grant for Science Development of Wroclaw Medical University in Poland (Grant Number SUBZ.A440.23.009).
Institutional Review Board Statement
All procedures were conducted in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. Our study protocol was approved by the Bioethics Committee of Wroclaw Medical University, Poland (Signature number: KB-231/2023).
Informed Consent Statement
All our patients provided admission informed consent, which stipulated that results may be used for research purposes. This procedure was approved by the Bioethics Committee. The data were analyzed retrospectively and anonymously from established medical records. The authors did not have access to identifying patient information or direct access to the study participants.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Acknowledgments
The authors are grateful to all the staff and the patients at the study center who contributed to this work.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Chmielik, E.; Rusinek, D.; Oczko-Wojciechowska, M.; Jarzab, M.; Krajewska, J.; Czarniecka, A.; Jarzab, B. Heterogeneity of thyroid cancer. Pathobiology 2018, 85, 117–129. [Google Scholar] [CrossRef]
- Lim, H.; Devesa, S.S.; Sosa, J.A.; Check, D.; Kitahara, C.M. Trends in thyroid cancer incidence and mortality in the United States, 1974-2013. JAMA 2017, 317, 1338–1348. [Google Scholar] [CrossRef] [PubMed]
- Haymart, M.R.; Banerjee, M.; Reyes-Gastelum, D.; Caoili, E.; Norton, E.C. Thyroid ultrasound and the increase in diagnosis of low-risk thyroid cancer. J. Clin. Endocrinol. Metab. 2019, 104, 785–792. [Google Scholar] [CrossRef] [PubMed]
- Albi, E.; Cataldi, S.; Lazzarini, A.; Codini, M.; Beccari, T.; Ambesi-Impiombato, F.; Curcio, F. Radiation and thyroid cancer. Int. J. Mol. Sci. 2017, 18, 911. [Google Scholar] [CrossRef] [PubMed]
- Cibas, E.S.; Ali, S.Z. The Bethesda system for reporting thyroid cytopathology. Am. J. Clin. Pathol. 2009, 132, 658–665. [Google Scholar] [CrossRef]
- Cibas, E.S.; Ali, S.Z. The 2017 Bethesda system for reporting thyroid cytopathology. J. Am. Soc. Cytopathol. 2017, 6, 217–222. [Google Scholar] [CrossRef]
- Krane, J.F.; Nayar, R.; Renshaw, A.A. ypia of undetermined significance/follicular lesion of undetermined significance. In The Bethesda System for Reporting Thyroid Cytopathology: Definitions, criteria, and explanatory notes, 2nd ed.; Ali, S.Z., Cibas, E.S., Eds.; Springer Nature: Switzerland, 2017; pp. 49–70. [Google Scholar]
- Liu, C.; Liu, Y.; Zhang, L.; Dong, Y.; Hu, S.; Xia, Y.; Zhang, B.; Cao, Y.; Liu, Z.; Chen, G.; et al. Risk factors for high-volume lymph node metastases in cN0 papillary thyroid microcarcinoma. Gland Surg. 2019, 8, 550–556. [Google Scholar] [CrossRef]
- Liu, C.; Zhang, L.; Liu, Y.; Xia, Y.; Cao, Y.; Liu, Z.; Chen, G.; Liu, N.; Shang, Z.; Yang, J.; et al. Ultrasonography for the prediction of high-volume lymph node metastases in papillary thyroid carcinoma: Should surgeons believe ultrasound results? World J. Surg. 2020, 44, 4142–4148. [Google Scholar] [CrossRef]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Pizzato, M.; Li, M.; Vignat, J.; Laversanne, M.; Singh, D.; La Vecchia, C.; Vaccarella, S. The epidemiological landscape of thyroid cancer worldwide: GLOBOCAN estimates for incidence and mortality rates in 2020. Lancet Diabetes Endocrinol. 2022, 10, 264–272. [Google Scholar] [CrossRef]
- Kaliszewski, K.; Diakowska, D.; Wojtczak, B.; Migoń, J.; Kasprzyk, A.; Rudnicki, J. The occurrence of and predictive factors for multifocality and bilaterality in patients with papillary thyroid microcarcinoma. Medicine 2019, 98, e15609. [Google Scholar] [CrossRef] [PubMed]
- Schopper, H.K.; Stence, A.; Ma, D.; Pagedar, N.A.; Robinson, R.A. Single thyroid tumour showing multiple differentiated morphological patterns and intramorphological molecular genetic heterogeneity. J. Clin. Pathol. 2017, 70, 116–119. [Google Scholar] [CrossRef] [PubMed]
- Gospodarowicz, M.; Mackillop, W.; O'Sullivan, B.; Sobin, L.; Henson, D.; Hutter, R.V.; Wittekind, C. Prognostic factors in clinical decision making. Cancer 2001, 91, 1688–1695. [Google Scholar] [CrossRef]
- Kaliszewski, K. Does every classical type of well-differentiated thyroid cancer have excellent prognosis? A case series and literature review. Cancer Manag. Res. 2019, 11, 2441–2448. [Google Scholar] [CrossRef] [PubMed]
- Eustatia-Rutten, C.F.A.; Corssmit, E.P.M.; Biermasz, N.R.; Pereira, A.M.; Romijn, J.A.; Smit, J.W. Survival and death causes in differentiated thyroid carcinoma. J. Clin. Endocrinol. Metab. 2006, 91, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Mazzaferri, E.L.; Kloos, R.T. Clinical review 128: Current approaches to primary therapy for papillary and follicular thyroid cancer. J. Clin. Endocrinol. Metab. 2001, 86, 1447–1463. [Google Scholar] [CrossRef] [PubMed]
- Katoh, R.; Sasaki, J.; Kurihara, H.; Suzuki, K.; Iida, Y.; Kawaoi, A. Multiple thyroid involvement (intraglandular metastasis) in papillary thyroid carcinoma. A clinicopathologic study of 105 consecutive patients. Cancer 1992, 70, 1585–1590. [Google Scholar] [CrossRef]
- Kuhn, E.; Teller, L.; Piana, S.; Rosai, J.; Merino, M.J. Different clonal origin of bilateral papillary thyroid carcinoma, with a review of the literature. Endocr. Pathol. 2012, 23, 101–107. [Google Scholar] [CrossRef]
- Wang, W.; Wang, H.; Teng, X.; Wang, H.; Mao, C.; Teng, R.; Zhao, W.; Cao, J.; Fahey, T.J.; Teng, L. Clonal analysis of bilateral, recurrent, and metastatic papillary thyroid carcinomas. Hum. Pathol. 2010, 41, 1299–1309. [Google Scholar] [CrossRef]
- Shattuck, T.M.; Westra, W.H.; Ladenson, P.W.; Arnold, A. Independent clonal origins of distinct tumor foci in multifocal papillary thyroid carcinoma. N. Engl. J. Med. 2005, 352, 2406–2412. [Google Scholar] [CrossRef]
- Vasko, V.; Hu, S.; Wu, G.; Xing, J.C.; Larin, A.; Savchenko, V.; Trink, B.; Xing, M. High prevalence and possible de novo formation of BRAF mutation in metastasized papillary thyroid cancer in lymph nodes. J. Clin. Endocrinol. Metab. 2005, 90, 5265–5269. [Google Scholar] [CrossRef] [PubMed]
- National Cancer Institute. Surveillance, epidemiology, and end results program. Available online: https://seer.cancer.gov/statfacts/html/thyro.html.
- Kaliszewski, K.; Diakowska, D.; Wojtczak, B.; Rudnicki, J. Cancer screening activity results in overdiagnosis and overtreatment of papillary thyroid cancer: A 10-year experience at a single institution. PLoS One 2020, 15, e0236257. [Google Scholar] [CrossRef]
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M.; et al. 2015 American thyroid association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: The American thyroid association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid 2016, 26, 1–133. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.B.; Xu, H.X.; Zhang, Y.F.; Guo, L.H.; Xu, S.H.; Zhao, C.K.; Liu, B.J. Comparisons of ACR TI-RADS, ATA guidelines, Kwak TI-RADS, and KTA/KSThR guidelines in malignancy risk stratification of thyroid nodules. Clin. Hemorheol. Microcirc. 2020, 75, 219–232. [Google Scholar] [CrossRef] [PubMed]
- Londero, S.C.; Krogdahl, A.; Bastholt, L.; Overgaard, J.; Pedersen, H.B.; Hahn, C.H.; Bentzen, J.; Schytte, S.; Christiansen, P.; Gerke, O.; et al. Papillary thyroid carcinoma in Denmark, 1996–2008: Outcome and evaluation of established prognostic scoring systems in a prospective national cohort. Thyroid 2015, 25, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Leboulleux, S.; Tuttle, R.M.; Pacini, F.; Schlumberger, M. Papillary thyroid microcarcinoma: Time to shift from surgery to active surveillance? Lancet Diabetes Endocrinol. 2016, 4, 933–942. [Google Scholar] [CrossRef] [PubMed]
- Ito, Y.; Miyauchi, A.; Kihara, M.; Higashiyama, T.; Kobayashi, K.; Miya, A. Patient age is significantly related to the progression of papillary microcarcinoma of the thyroid under observation. Thyroid 2014, 24, 27–34. [Google Scholar] [CrossRef]
- Ito, Y.; Miyauchi, A. Active surveillance as first-line management of papillary microcarcinoma. Annu. Rev. Med. 2019, 70, 369–379. [Google Scholar] [CrossRef]
- Ito, Y.; Miyauchi, A.; Kudo, T.; Oda, H.; Yamamoto, M.; Sasai, H.; Masuoka, H.; Fukushima, M.; Higashiyama, T.; Kihara, M.; et al. Trends in the implementation of active surveillance for low-risk papillary thyroid microcarcinomas at Kuma hospital: Gradual increase and heterogeneity in the acceptance of this new management option. Thyroid 2018, 28, 488–495. [Google Scholar] [CrossRef]
- Kwon, H.; Oh, H.-S.; Kim, M.; Park, S.; Jeon, M.J.; Kim, W.G.; Kim, W.B.; Shong, Y.K.; Song, D.E.; Baek, J.H.; et al. Active surveillance for patients with papillary thyroid microcarcinoma: A single center’s experience in Korea. J. Clin. Endocrinol. Metab. 2017, 102, 1917–1925. [Google Scholar] [CrossRef]
- Molinaro, E.; Campopiano, M.C.; Pieruzzi, L.; Matrone, A.; Agate, L.; Bottici, V.; Viola, D.; Cappagli, V.; Valerio, L.; Giani, C.; et al. Active surveillance in papillary thyroid microcarcinomas is feasible and safe: Experience at a single Italian center. J. Clin. Endocrinol. Metab. 2020, 105, e172–e180. [Google Scholar] [CrossRef] [PubMed]
- Saravana-Bawan, B.; Bajwa, A.; Paterson, J.; McMullen, T. Active surveillance of low-risk papillary thyroid cancer: A meta-analysis. Surgery 2020, 167, 46–55. [Google Scholar] [CrossRef] [PubMed]
- Russ, G.; Bonnema, Steen J. ; Erdogan, Murat F.; Durante, C.; Ngu, R.; Leenhardt, L. European thyroid association guidelines for ultrasound malignancy risk stratification of thyroid nodules in adults: The EU-TIRADS. Eur. Thyroid J. 2017, 6, 225–237. [Google Scholar] [CrossRef]
- Caulley, L.; Johnson-Obaseki, S.; Luo, L.; Javidnia, H. Risk factors for postoperative complications in total thyroidectomy. Medicine 2017, 96, e5752. [Google Scholar] [CrossRef]
- Christou, N.; Mathonnet, M. Complications after total thyroidectomy. J. Visc. Surg. 2013, 150, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Chahardahmasumi, E.; Salehidoost, R.; Amini, M.; Aminorroaya, A.; Rezvanian, H.; Kachooei, A.; Iraj, B.; Nazem, M.; Kolahdoozan, M. Assessment of the early and late complication after thyroidectomy. Adv. Biomed. Res. 2019, 8, 14. [Google Scholar] [CrossRef]
- Furuya-Kanamori, L.; Bell, K.J.L.; Clark, J.; Glasziou, P.; Doi, S.A.R. Prevalence of differentiated thyroid cancer in autopsy studies over six decades: A meta-analysis. J. Clin. Oncol. 2016, 34, 3672–3679. [Google Scholar] [CrossRef]
- Hugen, N.; Sloot, Y.J.E.; Netea-Maier, R.T.; van de Water, C.; Smit, J.W.A.; Nagtegaal, I.D.; van Engen-van Grunsven, I.C.H. Divergent metastatic patterns between subtypes of thyroid carcinoma results from the nationwide dutch pathology registry. J. Clin. Endocrinol. Metab. 2020, 105, e299–e306. [Google Scholar] [CrossRef]
- Ito, Y.; Miyauchi, A.; Oda, H. Low-risk papillary microcarcinoma of the thyroid: A review of active surveillance trials. Eur. J. Surg. Oncol. 2018, 44, 307–315. [Google Scholar] [CrossRef]
- Tuttle, R.M.; Fagin, J.A.; Minkowitz, G.; Wong, R.J.; Roman, B.; Patel, S.; Untch, B.; Ganly, I.; Shaha, A.R.; Shah, J.P.; et al. Natural history and tumor volume kinetics of papillary thyroid cancers during active surveillance. JAMA Otolaryngol. Head Neck Surg. 2017, 143, 1015–1020. [Google Scholar] [CrossRef]
- Takano, T. Fetal cell carcinogenesis of the thyroid: A modified theory based on recent evidence. Endocr. J. 2014, 61, 311–320. [Google Scholar] [CrossRef]
- Gerashchenko, T.S.; Denisov, E.V.; Litviakov, N.V.; Zavyalova, M.V.; Vtorushin, S.V.; Tsyganov, M.M.; Perelmuter, V.M.; Cherdyntseva, N.V. Intratumor heterogeneity: Nature and biological significance. Biochemistry (Moscow) 2013, 78, 1201–1215. [Google Scholar] [CrossRef] [PubMed]
- Mitsutake, N.; Iwao, A.; Nagai, K.; Namba, H.; Ohtsuru, A.; Saenko, V.; Yamashita, S. Characterization of side population in thyroid cancer cell lines: Cancer stem-like cells are enriched partly but not exclusively. Endocrinology 2007, 148, 1797–1803. [Google Scholar] [CrossRef] [PubMed]
- Ugolini, C.; Basolo, F.; Proietti, A.; Vitti, P.; Elisei, R.; Miccoli, P.; Toniolo, A. Lymphocyte and immature dendritic cell infiltrates in differentiated, poorly differentiated, and undifferentiated thyroid carcinoma. Thyroid 2007, 17, 389–393. [Google Scholar] [CrossRef] [PubMed]
- Ryder, M.; Ghossein, R.A.; Ricarte-Filho, J.C.M.; Knauf, J.A.; Fagin, J.A. Increased density of tumor-associated macrophages is associated with decreased survival in advanced thyroid cancer. Endocr. Relat. Cancer 2008, 15, 1069–1074. [Google Scholar] [CrossRef]
- Ito, Y.; Matsuzuka, F.; Yoshida, H.; Morita, S.; Nakano, K.; Kobayashi, K.; Yokozawa, T.; Hirai, K.; Kakudo, K.; Kuma, K.; et al. Encapsulated anaplastic thyroid carcinoma without invasive phenotype with favorable prognosis: Report of a case. Surg. Today 2003, 33, 277–281. [Google Scholar] [CrossRef]
- Dibelius, G.; Mehra, S.; Clain, J.B.; Urken, M.L.; Wenig, B.M. Noninvasive anaplastic thyroid carcinoma: Report of a case and literature review. Thyroid 2014, 24, 1319–1324. [Google Scholar] [CrossRef]
- Lloyd, R.V.; Osamura, R.Y.; Kioppel, G.; Rosai, J. International Agency for Research on Cancer. WHO Classification of Tumours of Endocrine Organs; IARC Who Classification of Tumours: Lyon, 2017. [Google Scholar]
- Nikiforov, Y.E.; Seethala, R.R.; Tallini, G.; Baloch, Z.W.; Basolo, F.; Thompson, L.D.; Barletta, J.A.; Wenig, B.M.; Al Ghuzlan, A.; Kakudo, K.; et al. Nomenclature revision for encapsulated follicular variant of papillary thyroid carcinoma: A paradigm shift to reduce overtreatment of indolent tumors. JAMA Oncol. 2016, 2, 1023–1029. [Google Scholar] [CrossRef] [PubMed]
- Canini, V.; Leni, D.; Pincelli, A.I.; Scardilli, M.; Garancini, M.; Villa, C.; Di Bella, C.; Capitoli, G.; Cimini, R.; Leone, B.E.; et al. Clinical-pathological issues in thyroid pathology: Study on the routine application of NIFTP diagnostic criteria. Sci. Rep. 2019, 9, 13179. [Google Scholar] [CrossRef] [PubMed]
- Tallini, G.; Tuttle, R.M.; Ghossein, R.A. The history of the follicular variant of papillary thyroid carcinoma. J. Clin. Endocrinol. Metab. 2017, 102, 15–22. [Google Scholar] [CrossRef]
- Hung, Y.P.; Barletta, J.A. A user's guide to non-invasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP). Histopathology 2017, 72, 53–69. [Google Scholar] [CrossRef] [PubMed]
- Seethala, R.R.; Baloch, Z.W.; Barletta, J.A.; Khanafshar, E.; Mete, O.; Sadow, P.M.; LiVolsi, V.A.; Nikiforov, Y.E.; Tallini, G.; Thompson, L.D.R. Noninvasive follicular thyroid neoplasm with papillary-like nuclear features: A review for pathologists. Mod. Pathol. 2018, 31, 39–55. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Maso, L.D.; Vaccarella, S. Global trends in thyroid cancer incidence and the impact of overdiagnosis. Lancet Diabetes Endocrinol. 2020, 8, 468–470. [Google Scholar] [CrossRef] [PubMed]
- Pigac, B.; Masic, S.; Hutinec, Z.; Masic, V. Rare occurrence of incidental finding of noninvasive follicular thyroid neoplasm with papillary-like nuclear features in hurthle cell adenoma. Med. Arch. 2018, 72, 367–370. [Google Scholar] [CrossRef] [PubMed]
- Gartland, R.M.; Lubitz, C.C. Reply to “impact of noninvasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP) on the outcomes of lobectomy”. Ann. Surg. Oncol. 2019, 26, 307–308. [Google Scholar] [CrossRef]
- Rosario, P.W. Long-term outcomes of patients with noninvasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP) ≥4 cm treated without radioactive iodine. Endocr. Pathol. 2017, 28, 367–368. [Google Scholar] [CrossRef]
- Thompson, L.D.R. Ninety-four cases of encapsulated follicular variant of papillary thyroid carcinoma: A name change to Noninvasive Follicular Thyroid Neoplasm with Papillary-like Nuclear Features would help prevent overtreatment. Mod. Pathol. 2016, 29, 698–707. [Google Scholar] [CrossRef]
- Canberk, S.; Montezuma, D.; Taştekin, E.; Grangeia, D.; Demirhas, M.P.; Akbas, M.; Tokat, F.; Ince, U.; Soares, P.; Schmitt, F. “The other side of the coin”: Understanding noninvasive follicular tumor with papillary-like nuclear features in unifocal and multifocal settings. Hum. Pathol. 2019, 86, 136–142. [Google Scholar] [CrossRef]
- LiVolsi, V.A. Papillary carcinoma tall cell variant (TCV): A review. Endocr. Pathol. 2010, 21, 12–15. [Google Scholar] [CrossRef]
- Akslen, L.A.; LiVolsi, V.A. Prognostic significance of histologic grading compared with subclassification of papillary thyroid carcinoma. Cancer 2000, 88, 1902–1908. [Google Scholar] [CrossRef]
- Baloch, Z.W.; Mandel, S.; LiVolsi, V.A. Combined tall cell carcinoma and hürthle cell carcinoma (collision tumor) of the thyroid. Arch. Pathol. Lab. Med. 2001, 125, 541–543. [Google Scholar] [CrossRef] [PubMed]
- Kaliszewski, K.; Diakowska, D.; Wojtczak, B.; Forkasiewicz, Z.; Pupka, D.; Nowak, Ł.; Rudnicki, J. Which papillary thyroid microcarcinoma should be treated as “true cancer” and which as “precancer”? World J. Surg. Oncol. 2019, 17, 91. [Google Scholar] [CrossRef] [PubMed]
- Baloch, Z.; LiVolsi, V.A.; Tondon, R. Aggressive variants of follicular cell derived thyroid carcinoma; the so called ‘Real Thyroid Carcinomas’. J. Clin. Pathol. 2013, 66, 733–743. [Google Scholar] [CrossRef] [PubMed]
- Chung, Y.J.; Lee, J.S.; Park, S.Y.; Park, H.J.; Cho, B.Y.; Park, S.J.; Lee, S.Y.; Kang, K.-H.; Ryu, H.S. Histomorphological factors in the risk prediction of lymph node metastasis in papillary thyroid carcinoma. Histopathology 2013, 62, 578–588. [Google Scholar] [CrossRef]
- Tuttle, R.M.; Zhang, L.; Shaha, A. A clinical framework to facilitate selection of patients with differentiated thyroid cancer for active surveillance or less aggressive initial surgical management. Expert Rev. Endocrinol. Metab. 2018, 13, 77–85. [Google Scholar] [CrossRef]
- Zanocco, K.A.; Hershman, J.M.; Leung, A.M. Active surveillance of low-risk thyroid cancer. JAMA 2019, 321, 2020–2021. [Google Scholar] [CrossRef]
- Kim, K.J.; Kim, S.G.; Tan, J.; Shen, X.; Viola, D.; Elisei, R.; Puxeddu, E.; Fugazzola, L.; Colombo, C.; Jarzab, B.; et al. BRAF V600E status may facilitate decision-making on active surveillance of low-risk papillary thyroid microcarcinoma. Eur. J. Cancer 2020, 124, 161–169. [Google Scholar] [CrossRef]
- Sakai, T.; Sugitani, I.; Ebina, A.; Fukuoka, O.; Toda, K.; Mitani, H.; Yamada, K. Active surveillance for T1bN0M0 papillary thyroid carcinoma. Thyroid 2019, 29, 59–63. [Google Scholar] [CrossRef]
Figure 1.
Selection of the study group from 5821 individuals referred for surgery from 2008 to 2022. All participants underwent a minimum of one UG-FNAB. All evaluated patients underwent surgery, and histopathology results were obtained in all cases. 678 patients with malignant tumor were included and analyzed.
Figure 1.
Selection of the study group from 5821 individuals referred for surgery from 2008 to 2022. All participants underwent a minimum of one UG-FNAB. All evaluated patients underwent surgery, and histopathology results were obtained in all cases. 678 patients with malignant tumor were included and analyzed.
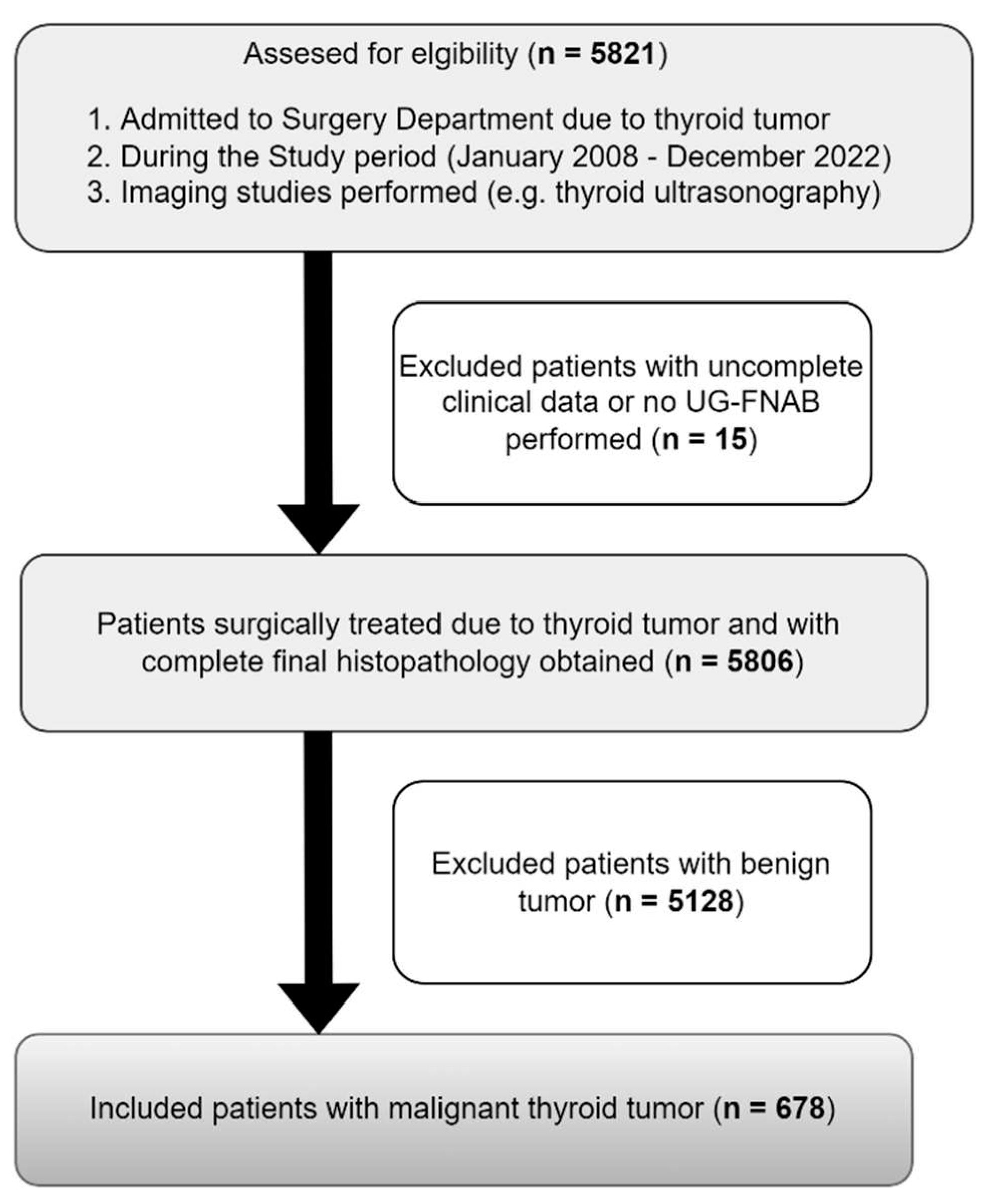
Figure 2.
The incidence rate of thyroid tumors: benign, TC and PTC in years 2008-2022. Rates were calculated as number of cases per number of all patients in study year. * apogee of “cancer screening activity” time, ** possibility of PTMC AS in clinical practice, *** NIFTP excluded from TC types, **** personalized medicine recommended, ***** Covid-19 pandemic time. .
Figure 2.
The incidence rate of thyroid tumors: benign, TC and PTC in years 2008-2022. Rates were calculated as number of cases per number of all patients in study year. * apogee of “cancer screening activity” time, ** possibility of PTMC AS in clinical practice, *** NIFTP excluded from TC types, **** personalized medicine recommended, ***** Covid-19 pandemic time. .
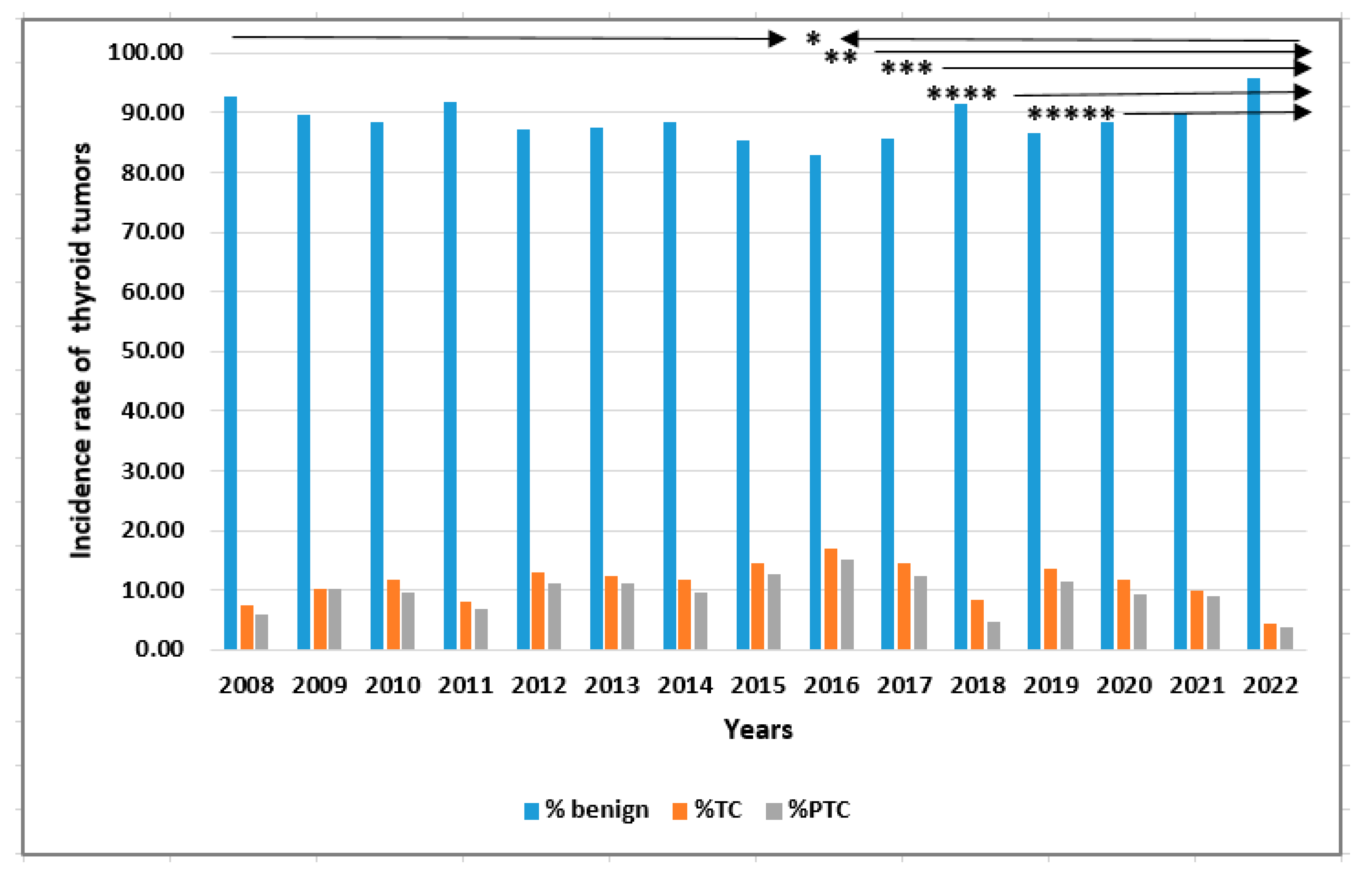
Figure 3.
The incidence of benign thyroid tumors with respect to the sex of patients in 2008-2022 Rates were calculated as the number of cases per number of all patients in the study year.
Figure 3.
The incidence of benign thyroid tumors with respect to the sex of patients in 2008-2022 Rates were calculated as the number of cases per number of all patients in the study year.
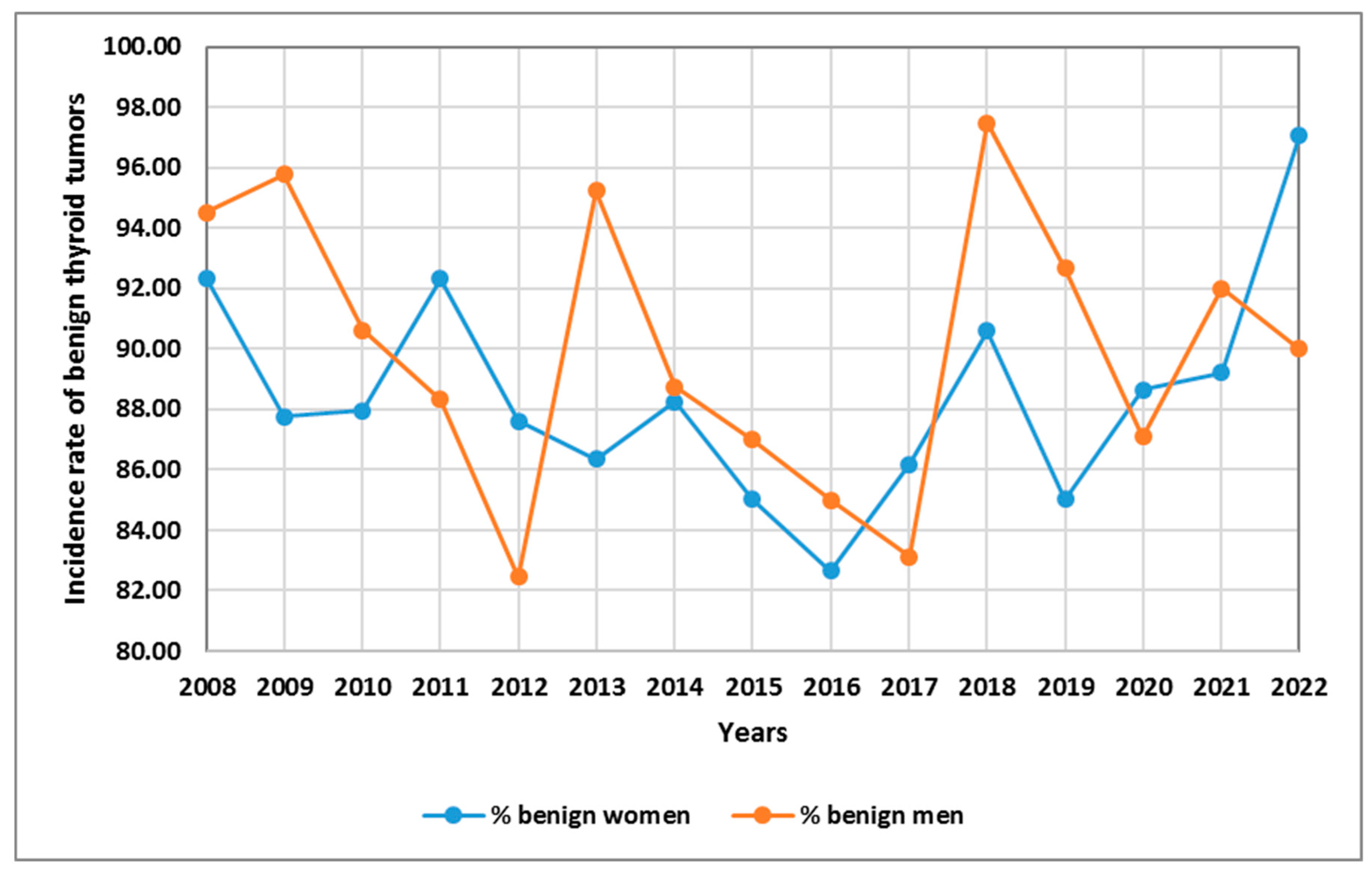
Figure 4.
The incidence of malignant thyroid tumors: TC and PTC with respect to the sex of patients in the years 2008-2022. Rates were calculated as the number of cases per number of all patients in the study year.
Figure 4.
The incidence of malignant thyroid tumors: TC and PTC with respect to the sex of patients in the years 2008-2022. Rates were calculated as the number of cases per number of all patients in the study year.
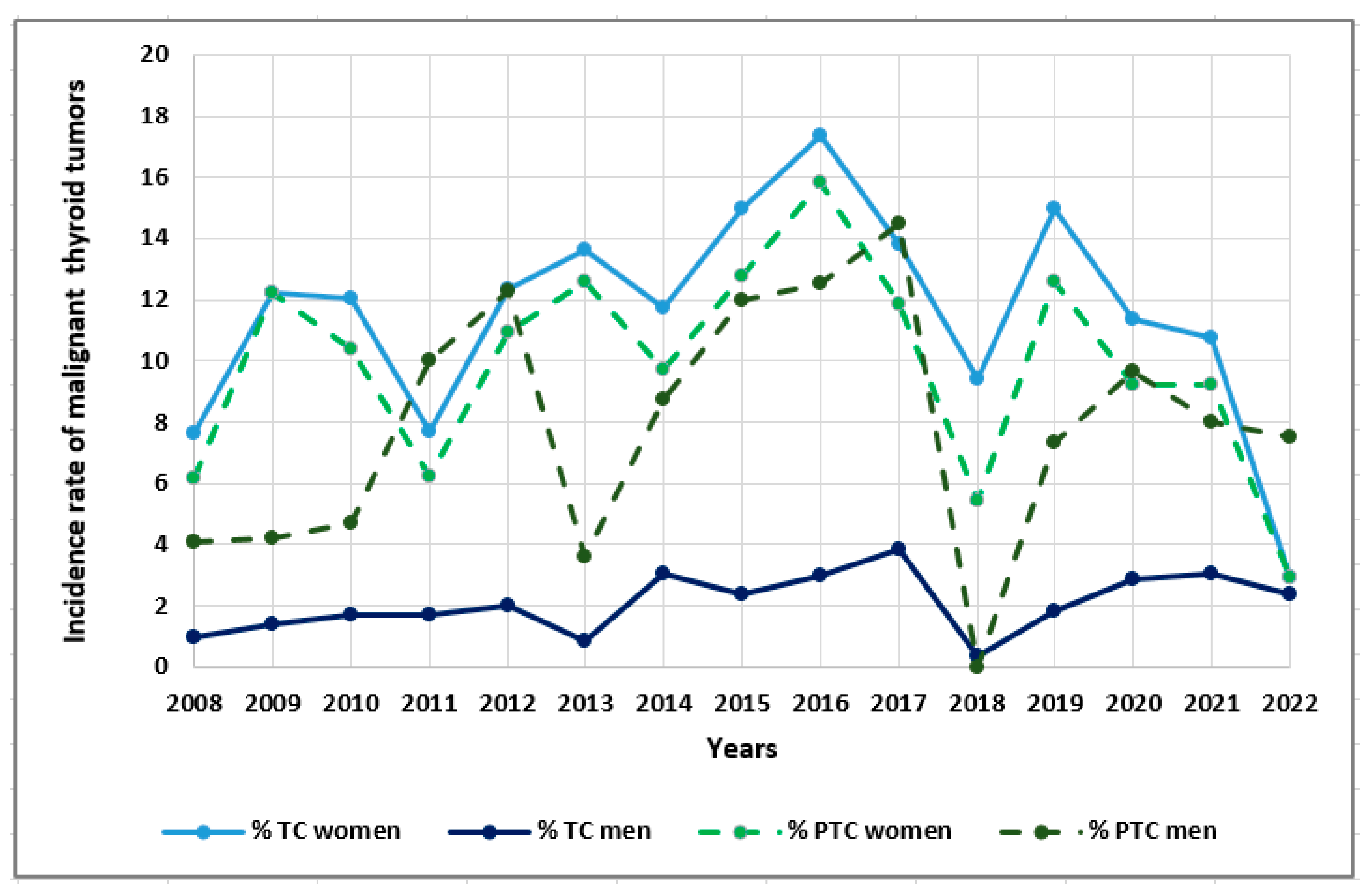
Figure 5.
The incidence of malignant thyroid tumors: TC and PTC with respect to age (<55 years old vs. >55 years old) in 2008-2022. Rates were calculated as the number of cases per number of all patients in the study year.
Figure 5.
The incidence of malignant thyroid tumors: TC and PTC with respect to age (<55 years old vs. >55 years old) in 2008-2022. Rates were calculated as the number of cases per number of all patients in the study year.
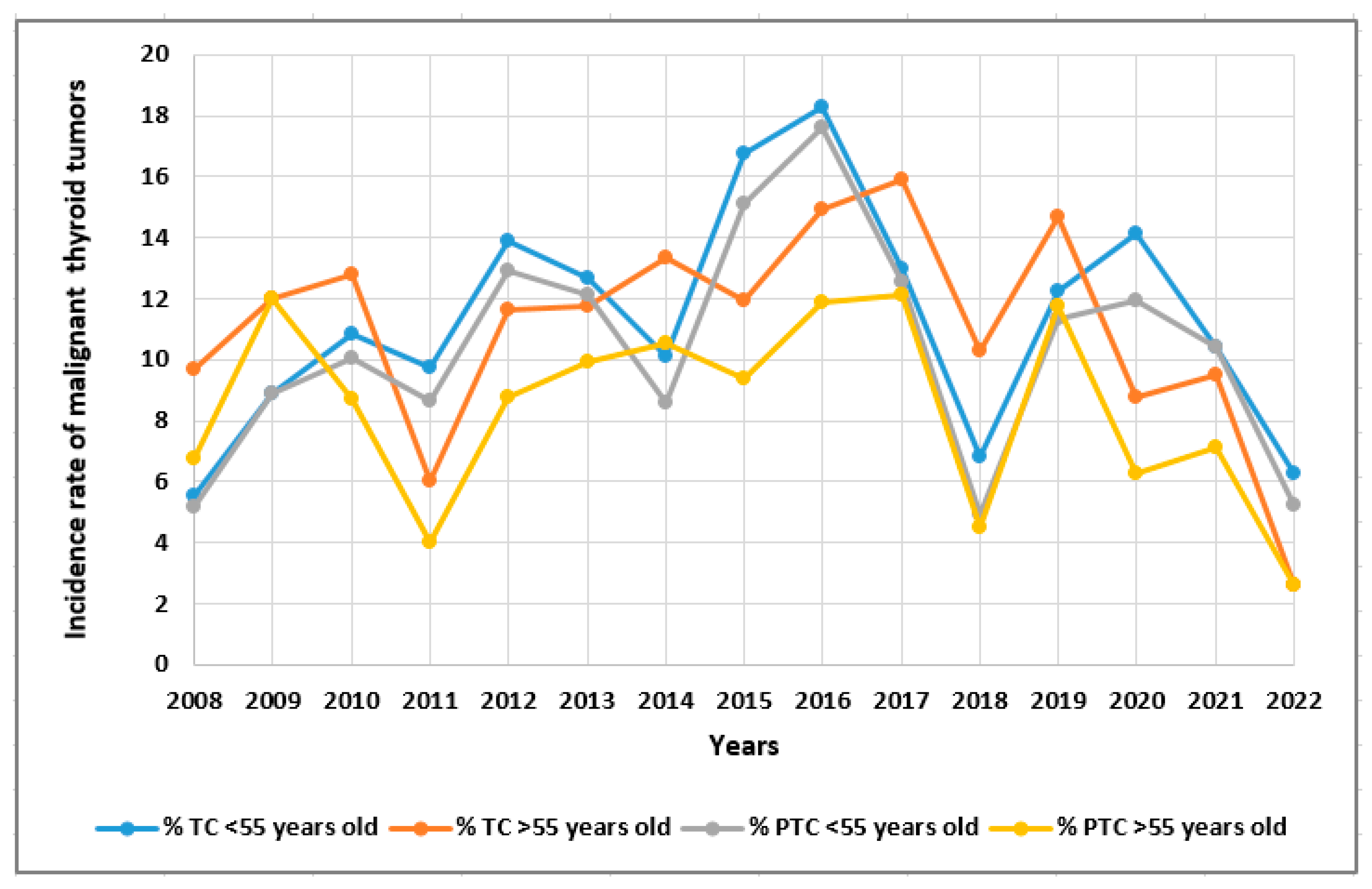
Figure 6.
The incidence of PTC with respect to tumor size (<5 mm vs. >5 mm) from 2008-2022. Rates were calculated as the number of PCT cases per number of TC patients in the study year.
Figure 6.
The incidence of PTC with respect to tumor size (<5 mm vs. >5 mm) from 2008-2022. Rates were calculated as the number of PCT cases per number of TC patients in the study year.
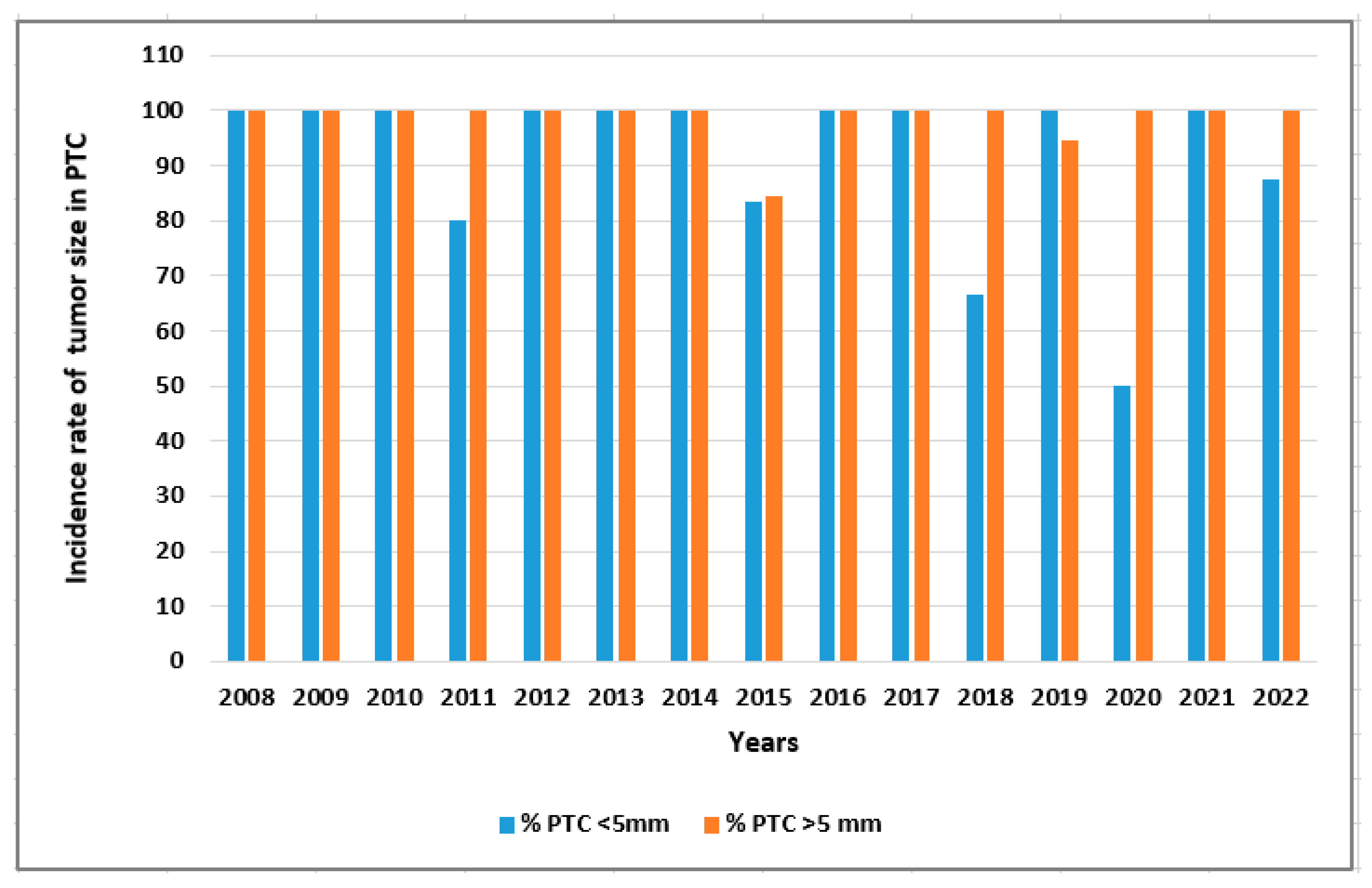
Figure 7.
The incidence of PTC and other TC with respect to pTNM (stage I vs. stage II-IV) in 2008-2022. Rates were calculated as the number of PCT cases/other TC cases per number of TC patients in the study year.
Figure 7.
The incidence of PTC and other TC with respect to pTNM (stage I vs. stage II-IV) in 2008-2022. Rates were calculated as the number of PCT cases/other TC cases per number of TC patients in the study year.
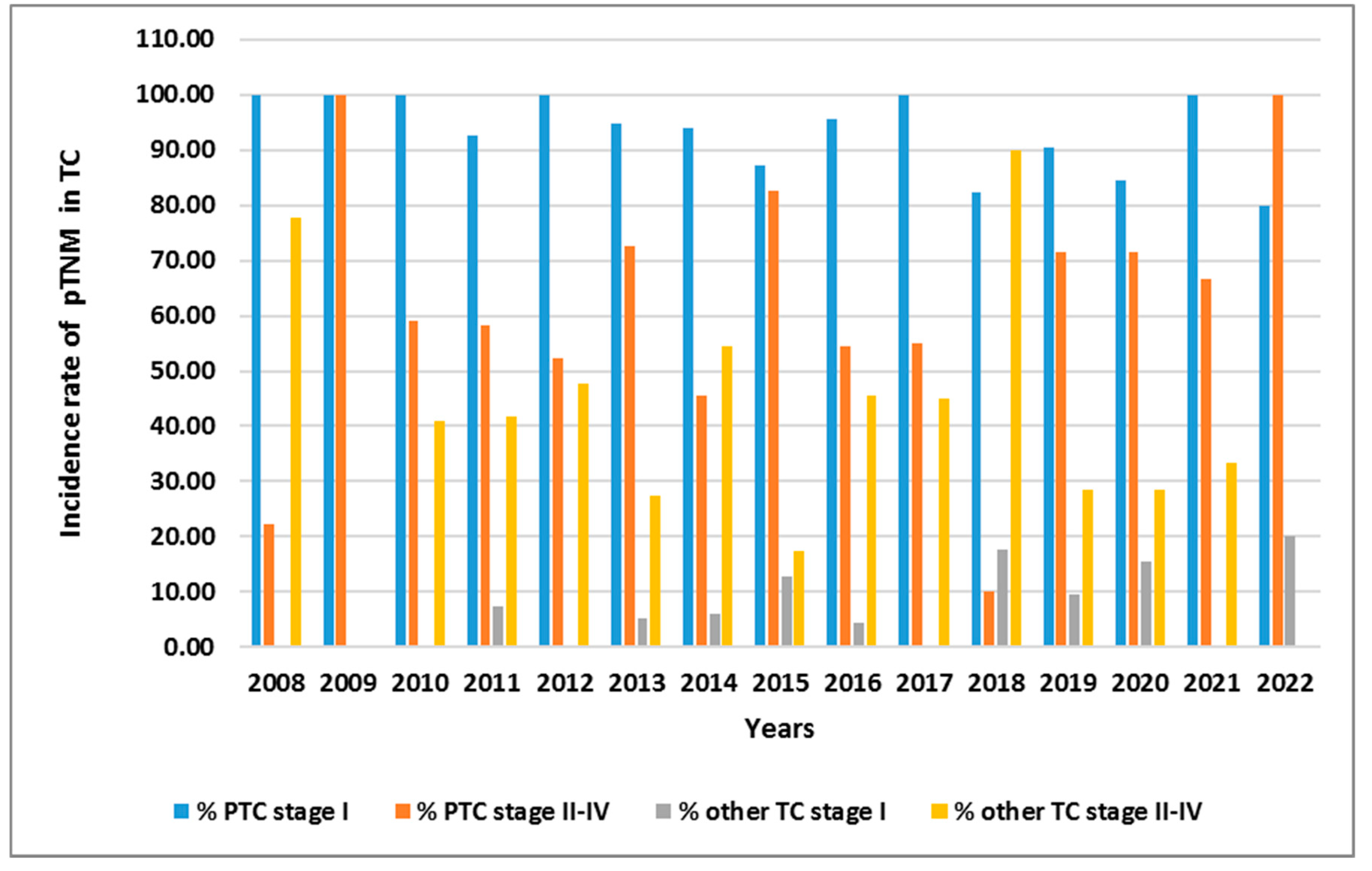

Table 1.
Demographic, clinical and tumor characteristics of all patients with TC, papillary thyroid cancer (PTC) and other types of cancer.
Table 1.
Demographic, clinical and tumor characteristics of all patients with TC, papillary thyroid cancer (PTC) and other types of cancer.
| Parameters | Total TC patients (n=678) |
PTC patients (n=579) |
Other types of TC (n=99) |
P value |
|---|---|---|---|---|
| N (%) or mean + SD |
N (%) or mean + SD |
N (%) or mean + SD |
||
| Sex Female Male |
581 (85.69) 97 (14.30) |
501 (86.53) 78 (13.47) |
80 (80.81) 19 (19.19) |
0.133 |
| Age (years) |
51.66 + 15.98 | 50.25 + 15.20 | 59.92 + 17.95 | <0.0001* |
| Age: <55 years old >55 years old |
385 (56.78) 293 (43.21) |
355 (61.31) 224 (38.69) |
30 (30.30) 69 (69.70) |
<0.0001* |
| Type of surgery: Total No total |
474 (69.91) 204 (30.09) |
426 (73.58) 153 (26.42) |
48 (48.48) 51 (51.52) |
<0.0001* |
| Reoperation needed: No Yes |
503 (74.04) 176 (25.95) |
441 (76.17) 138 (23.83) |
61 (61.62) 38 (38.38) |
0.002* |
| Histological type of cancer: Papillary (PTC) Follicular (FTC) Medullary (MTC) Undifferentiated Sarcoma Secondary Lymphoma Squamous cell carcinoma Myeloma |
579 (85.39) 31 (4.57) 24 (3.53) 14 (2.06) 3 (0.44) 10 (1.47) 12 (1.76) 4 (0.58) 1 (0.14) |
579 (100.00) |
- 31 (31.31) 24 (24.24) 14 (14.14) 3 (3.03) 10 (10.10) 12 (12.12) 4 (4.04) 1 (1.01) |
- |
| pTNM: I II III IV |
501 (73.89) 90 (13.27) 42 (6.19) 45 (6.63) |
473 (81.69) 74 (12.78) 24 (4.15) 8 (1.38) |
27 (27.55) 16 (16.33) 18 (18.37) 37 (37.76) |
<0.0001* |
| pT: pT1a pT1b pT2 pT3 pT4a pT4b pTm |
256 (37.75) 276 (40.70) 78 (11.50) 24 (3.54) 16 (2.36) 26 (3.83) 2 (0.29) |
245 (42.76) 245 (42.76) 61 (10.65) 13 (2.27) 3 (0.52) 5 (0.87) 1 (0.17) |
9 (9.09) 29 (29.29) 15 (15.15) 11 (11.11) 13 (13.13) 21 (21.21) 1 (1.01) |
<0.0001* |
| pN: pN0 pN1a pN1b pNx |
427 (62.97) 184 (27.14) 35 (5.16) 32 (4.72) |
386 (66.67) 158 (27.29) 13 (2.25) 22 (3.80) |
41 (41.41) 26 (26.26) 22 (22.22) 10 (10.10) |
<0.0001* |
| pM: pM0 pM1 pMx |
568 (83.78) 46 (6.78) 64 (9.43) |
506 (87.39) 20 (3.45) 53 (9.15) |
61 (62.24) 26 (26.53) 11 (11.22) |
<0.0001* |
TC: thyroid cancer, PTC: papillary thyroid cancer, FTC: follicular thyroid cancer, MTC: medullary thyroid cancer, *: statistically significant.
Table 2.
Selected ultrasound features of all TCs, papillary thyroid cancer (PTC) and other types of cancer.
Table 2.
Selected ultrasound features of all TCs, papillary thyroid cancer (PTC) and other types of cancer.
| Parameters | Total TC patients (n=678) |
PTC patients (n=579) |
Other types of TC (n=99) |
P value |
|---|---|---|---|---|
| N (%) | N (%) | N (%) |
||
| Tumor size: <5 mm >5 mm |
294 (43.36) 384 (56.64) |
225 (38.89) 354 (61.11) |
69 (70.00) 30 (30.00) |
0.049* |
| Tumor shape: Regular Irregular |
294 (43.36) 384 (56.61) |
284 (49.13) 295 (50.87) |
10 (10.20) 89 (89.80) |
<0.0001* |
| Echogenicity: Hyperechoic Hypoechoic |
120 (17.69) 557 (82.15) |
116 (20.03) 463 (79.97) |
4 (4.08) 95 (95.92) |
0.0001* |
| Microcalcifications: No Yes |
275 (40.56) 403 (59.43) |
259 (44.73) 320 (55.27) |
16 (16.16) 83 (83.84) |
<0.0001* |
| Vascularity: Low High |
307 (45.28) 371 (54.71) |
295 (51.04) 283 (48.96) |
12 (12.24) 87 (87.76) |
<0.0001* |
| Type of tumor: Solitary Multifocal |
488 (71.96) 190 (28.02) |
423 (73.01) 156 (26.99) |
65 (65.66) 34 (34.34) |
0.132 |
| Bilateral: No Yes |
626 (92.32) 52 (7.67) |
529 (91.52) 49 (8.48) |
96 (96.97) 3 (3.03) |
0.060 |
TC: thyroid cancer, PTC: papillary thyroid cancer, *: statistically significant.
Table 3.
The prevalence of benign thyroid tumors and thyroid cancers (TCs) in 2008-2022. Descriptive data are presented as the number of observations (percent).
Table 3.
The prevalence of benign thyroid tumors and thyroid cancers (TCs) in 2008-2022. Descriptive data are presented as the number of observations (percent).
| Year | Benign tumors | Thyroid cancers | All patients |
|---|---|---|---|
| 2008 | 443 (8.64) | 35 (5.15) | 478 (8.23) |
| 2009 | 342 (6.67) | 39 (5.74) | 381 (6.56) |
| 2010 | 372 (7.26) | 49 (7.22) | 421 (7.25) |
| 2011 | 438 (8.54) | 39 (5.74) | 477 (8.22) |
| 2012 | 479 (9.34) | 71 (10.46) | 549 (9.46) |
| 2013 | 491 (9.58) | 69 (10.16) | 560 (9.65) |
| 2014 | 334 (6.50) | 44 (6.63) | 378 (6.51) |
| 2015 | 547 (10.67) | 94 (13.84) | 641 (11.04) |
| 2016 | 397 (7.74) | 81 (11.93) | 478 (8.23) |
| 2017 | 381 (7.43) | 64 (9.43) | 445 (7.67) |
| 2018 | 290 (5.66) | 27 (3.98) | 317 (5.46) |
| 2019 | 180 (3.51) | 28 (4.12) | 208 (3.58) |
| 2020 | 152 (2.96) | 20 (2.95) | 172 (2.96) |
| 2021 | 81 (1.58) | 9 (1.33) | 90 (1.55) |
| 2022 | 201 (3.92) | 9 (1.33) | 210 (3.62) |
| N (%) for groups | 5128 (100.00) | 678 (100.00) | 5806 (100.00) |
| N (%) for total | 5128 (88.32) | 678 (11.68) | 5806 (100.00) |
Table 4.
The prevalence of types of TC in years 2008-2022. Descriptive data are presented as the number of observations (percent).
Table 4.
The prevalence of types of TC in years 2008-2022. Descriptive data are presented as the number of observations (percent).
| Year | PTC | FTC | MTC | Undifferentiated | Sarcoma | Secondary TC | Lymphoma | SCC | Myeloma | All |
|---|---|---|---|---|---|---|---|---|---|---|
| 2008 | 28 (4.84) | 1 (3.23) | 1 (4.17) | 1 (7.14) | 1 (33.33) | 1 (10.00) | 2 (16.67) | - | - | 35 (5.16) |
| 2009 | 39 (6.74 | - | - | - | - | - | - | - | - | 39 (5.75) |
| 2010 | 40 (6.91) | 2 (6.45) | 2 (8.33) | 4 (28.57) | - | - | 1 (8.33) | - | - | 49 (7.23) |
| 2011 | 32 (5.53) | 3 (9.68) | 2 (8.33) | 1 (7.14) | - | 1 (10.00) | - | - | - | 39 (5.75) |
| 2012 | 61 (10.54) | 4 (12.90) | 1 (4.17) | 1 (7.14) | 1 (33.33) | 2 (20.00) | 1 (8.33) | - | - | 71 (10.47) |
| 2013 | 63 (10.88) | 3 (9.68) | - | 1 (7.14) | - | 2 (20.00) | - | - | - | 69 (10.18) |
| 2014 | 36 (6.22) | 2 (6.45) | 2 (8.33) | - | 1 (33.33) | 1 (10.00) | 2 (16.67) | - | - | 44 (6.49) |
| 2015 | 81 (13.99) | 5 (16.13) | 7 (29.17) | - | - | - | 1 (8.33) | - | - | 94 (13.86) |
| 2016 | 73 (12.61) | - | 3 (12.50) | 2 (14.29) | - | 3 (30.00) | - | - | - | 81 (11.95) |
| 2017 | 55 (9.50) | - | 1 (4.17) | 1 (7.14) | - | - | 3 (25.00) | 3 (75.00) | 1 (100.00) | 64 (9.44) |
| 2018 | 15 (2.59) | 6 (19.35) | 2 (8.33) | 2 (14.29) | - | - | 1 (8.33) | 1 (25.00) | - | 27 (3.98) |
| 2019 | 24 (4.15) | 1 (3.23) | 2 (8.33) | 1 (7.14) | - | - | - | - | - | 28 (4.13) |
| 2020 | 16 (2.76) | 4 (12.90) | - | - | - | - | - | - | - | 20 (2.95) |
| 2021 | 8 (1.38) | - | - | - | - | - | 1 (8.33) | - | - | 9 (1.33) |
| 2022 | 8 (1.38) | - | 1 (4.17) | - | - | - | 0 (0.00) | - | - | 9 (1.33) |
| N (%) for subgroups | 579 (100.00) | 31(100.00) | 24(100.00) | 14(100.00) | 3(100.00) | 10(100.00) | 12(100.00) | 4(100.00) | 1(100.00) | 678 (100.00) |
| N (%) for total | 579 (85.40) | 31(4.57) | 24(3.54) | 14(2.06) | 3(0.44) | 10(1.47) | 12(1.77) | 4(0.59) | 1(0.15) | 678 (100.00) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



