
Submitted:
18 September 2023
Posted:
19 September 2023
You are already at the latest version
Abstract
Cardiac resynchronization therapy (CRT) via biventricular pacing (BiVP-CRT) is considered a mainstay treatment for symptomatic heart failure patients with reduced ejection fraction and wide QRS. However, up to one third of patients receiving BiVP-CRT are considered non-responders to the therapy. Multiples strategies have been proposed to maximize the percentage of CRT responders including two new physiological pacing modalities that have emerged during the lasts years: His bundle pacing (HBP) and left bundle branch area pacing (LBBAP). Both pacing techniques aim at restoring the normal electrical activation of the ventricles through the native conduction system in opposition to the cell-to-cell activation of conventional right ventricular myocardial pacing. Conduction system pacing (CSP), including both HBP and LBBAP appears to be a promising pacing modality for delivering CRT and has proven to be safe and feasible in this particular setting. This article will review the current state of the art of CSP-based CRT, its limitations and future directions.
Keywords:
cardiac resynchronization therapy
; His bundle pacing
; Left bundle branch area pacing
; conduction system pacing
Introduction
Cardiac resynchronization therapy (CRT) is an established treatment for patients with heart failure (HF), wide QRS and impaired LV systolic function despite optimal medical treatment1. It was first described by Cazeau et al.2 in 1994 who used four chamber pacing (biauricular and biventricular pacing [BiVP]) for the treatment of a patient with advanced HF and left bundle branch block (LBBB) assuming that the electromechanical dyssynchrony induced by the LBBB could be counteracted by this new pacing modality. The standard CRT technique was thereafter refined and consisted in the transvenous implantation of a right atrial lead, a RV lead and a left ventricular (LV) lead implanted in a tributary branch of the coronary sinus (CS) in order to obtain BiVP. Since the initial description, the technique rapidly evolved and multiple observational non-randomized studies first showed significant acute hemodynamic improvements3-6. Subsequently, the firsts randomized trials demonstrated BiVP-CRT benefits in terms of functional capacity, peak oxygen consumption, LV ejection fraction (LVEF) improvement and reduction of HF hospitalizations7-13. Finally, over the next decade, multiple large randomized controlled trials showed that CRT delivered through BiVP significantly decreased mortality and HF hospitalizations14-25. As a result, current guidelines consider BiVP-CRT as a mainstay therapy for patients with symptomatic HF with reduced ejection fraction and wide QRS in spite of optimal medical therapy (Figure 1).
However, approximately one third of patients implanted with a BiVP-CRT device show no clinical or echocardiographic improvement and are considered non-responders to the therapy. Moreover, and in spite of the improvement of implant tools and device technology, there is still a small percentage of patients in which either the implant of a CS lead is not successful or once implanted optimal resynchronization is hampered by a high pacing threshold or by the presence of phrenic nerve stimulation26-28. As a result, different strategies have emerged in order to reduce the percentage of BiVP-CRT non-responders including the use of quadripolar LV leads and the optimization of AV and VV intervals among many others29.
Concomitantly, during the last years a renewed interest on His-bundle pacing (HBP) has emerged30-32. This physiological pacing modality aims for the restoration of the normal electrical cardiac activation sequence through the intrinsic conduction system and has been used for patients with bradycardia pacing indications30-34. Different studies have shown that HBP is able to correct intraventricular conduction disturbances including right and left bundle branch block (LBBB). In the same manner, but more recently, left bundle branch area pacing (LBBAP) has been described as a second conduction system pacing modality (CSP)35-38, and both techniques have been proposed as potential alternative methods for delivering CRT. This article will review the state of the art on CSP-based CRT.
Physiopathology associated with asynchronous LV activation
The pathophysiological fundamentals of CRT effectiveness are based on the presence of electromechanical dyssynchrony induced by intraventricular conduction disturbances such as LBBB or the abnormal ventricular activation associated with conventional right ventricular (RV) myocardial pacing39-43. In patients with normal QRS, the myocardium is activated uniformly and the electrical waveform rapidly spreads through the His-Purkinje system and the bundle branches resulting in a synchronized depolarization of the ventricles. However, in the presence of a LBBB, the ventricular activation pattern changes starting in the RV as the right bundle branch (RBB) function is preserved. Then, the activation waveform travels through the interventricular septum from the RV endocardium to the LV endocardium finally propagating to the endocardium of the posterolateral LV and completing a significantly slower LV ventricular activation as the electrical waveform travels through myocardial fibers not using the rapidly conducting Purkinje system.
Preclinical studies have shown that both LBBB and RV myocardial pacing are associated with poorer acute hemodynamic parameters in comparison with the normal activation observed with narrow QRS as a result of the mechanical dis-coordination leading to a structural, electrical and contractile remodeling39-40. At the cellular level, the dyssynchronous heart typically shows an increase in the apoptosis markers (tumour necrosis factor alpha [TNFα], caspases, DNA fragmentation), with development of fibrosis (increasing expression of collagen, matrix metalloproteases [MMPs], transforming growth factor beta [TGFβ], connective tissue growth factor [CTGF] and osteopontin [OPN]) and hypertrophy (increased levels of B-type natriuretic peptide [BNP], myosin heavy chain alpha [MHCα] and CTGF with reduction of miR133)44-45. As a result, LBBB is associated with cardiac adverse remodeling, worsening of systolic and diastolic function and progressive HF. BiVP plays a key role in correcting the LBBB-induced asynchrony by reducing the interventricular and intraventricular dyssynchrony.
In patients with permanent conventional RV myocardial pacing, a specific entity called “pacemaker induced cardiomyopathy” (PICM) has also been defined to describe the detrimental effects of the asynchronous activation of the LV due to chronic RV pacing42-43,46. PICM has a variable incidence ranging between 10-30% depending on the series and during the last 20 years different pacing strategies aiming for physiological pacing have emerged including algorithms to reduce unnecessary RV pacing in patients with preserved intrinsic conduction. However, these strategies are not useful in patients who need permanent RV pacing and BiVP or CSP-based CRT could play a role in this particular scenario47-48.
The potential role of CSP in CRT candidates
HBP is a physiological pacing modality first described in 1999 by Deshmunk et al.49 The objective of this pacing modality is to place a pacing lead in the His bundle area in order to capture the conduction system and restore the physiological activation of the ventricles through the specific conduction system and not in a cell-to-cell fashion as with conventional myocardial RV pacing. HBP was initially evaluated in patients with chronic atrial fibrillation undergoing atrioventricular (AV) node ablation and thus requiring permanent RV pacing. Subsequently, safety and feasibility of HBP has also been demonstrated in other conduction disturbances including supra-Hisian and infra-Hisian AV block, and has also shown the capacity of correcting both RBBB and LBBB in a variable percentage of patients30-34. For this reason, HBP has been proposed as an alternative or complementary technique for CRT.
More recently, a second physiological pacing modality has been described, namely left bundle branch area pacing (LBBAP), which includes both left bundle branch pacing (LBBP) and left ventricular septal pacing (LVSP). LBBP was first described by Huang et al. in 201750 and since this initial description observational studies have demonstrated its safety and feasibility in different scenarios including conventional bradycardia pacing indications35-38. Interestingly, LBBAP has been also tested in patients with wide QRS demonstrating a high percentage of bundle branch correction with higher implantation success (85-95%) and lower complication rates when compared with HBP. Moreover, acute and mid-term electrical parameters are also superior to those previously described with HBP including lower pacing thresholds and higher R wave sensing amplitudes. As a result, LBBAP has also been investigated as an alternative or complementary technique for CRT.
Using non-invasive epicardial electrocardiographic imaging Arnold et al.51 identified CRT candidates in which HBP shortened left ventricular activation time (LVAT) (18/23, 78%) and then compared the hemodynamic effects of both HBP and conventional BiVP in those patients showing that HBP was associated with greater reduction in QRS duration, LVAT and left ventricular dyssynchrony index, also with a better hemodynamic response than conventional BiVP. In the same way, Sussenbek and colleagues have recently used ultra-high-frequency electrocardiography (UHF-ECG) to compare ventricular activation patterns during BiVP and LBBAP in patients with baseline LBBB and CRT indication using 2 principal parameters: e-DYS (time difference between the first and last activation in V1–V8 leads) and Vdmean (average of V1–V8 local depolarization durations)52. LBBAP was associated with shorter e-DYS and shorter Vdmean than BiVP in spite of a comparable paced QRS duration in both groups pointing towards a more physiological ventricular activation with LBBAP in comparison with BiVP.
key concepts and definitions for CSP-based CRT
HBP implies the capture of the proximal or distal His bundle resulting in a normal ventricular activation in the presence of a normal conduction through the right and left bundle branches. When no adjacent myocardium is captured, selective HB pacing is defined (S-HBP) while non-selective HBP (NS-HBP) implies capture of both the HB and part of the surrounding myocardium53. Both capture patterns have been associated with comparable benefits in terms of electromechanical resynchronization. However, in patients with CRT indications, a baseline wide QRS is usually present due to intraventricular conduction disturbances, typically LBBB. In this particular scenario, it is not enough to have HB capture (either selective or non-selective) but is mandatory to obtain correction of the bundle branch block with subsequent QRS narrowing in order to be able to restore electrical synchrony (Figure 2). Thus, during HBP-CRT, up to 5 different capture patterns can be described including S- and NS-HBP, both with or without bundle branch correction, as well as myocardial only capture. Every HBP-CRT capture pattern will be associated with a particular pacing threshold that should be clearly detailed in order to facilitate adequate device programming and follow-up as only bundle branch correction thresholds (either selective or non-selective) are useful to obtain cardiac resynchronization.
On the other hand, LBBP is defined by the direct capture of the LBB or any of its fascicles together with a variable amount of the surrounding myocardium whereas LVSP is characterized by the capture of the LV septal subendocardium with subsequently rapid engagement of the left conduction system54. Both concepts are included under the term LBBAP and require the intraseptal implantation of a pacing lead reaching the subendocardium of the left ventricular septum. As the conduction system is captured distally to the right bundle branch during LBBAP, a delay in RV activation is typically seen with this pacing modality expressed by the characteristic r prime wave present in lead V1 (Figure 3). As both the distal and proximal dipoles of the LBBAP lead are usually within the interventricular septum, bipolar pacing may result in anodal capture which implies that the right side of the septum is being also captured during pacing resulting in a faster activation of the RV with this particular pacing configuration and thus a potential benefit in terms of QRS narrowing and better electrical resynchronization. Finally, the RV activation delay induced by LBBAP-CRT can be also compensated by fusing the intact intrinsic conduction through the right bundle branch present in patients with baseline LBBB with the LBBAP wavefront adjusting the device programmed AV interval.
Clinical evidence of HBP-CRT
HBP is theoretically the most physiological pacing modality as it can restore the normal electrical activation pattern of the ventricles. In CRT candidates with a typical LBBB, HBP with bundle branch correction would eliminate the asynchronous activation associated with the intraventricular conduction defect. In 2013 Barba et al.55 described the first series of 16 patients with CRT indication who underwent HBP after a failed CS lead implantation attempt. In this series, LBBB correction was temporally obtained in 81% of the cases, but permanent LBBB correction was finally achieved only in 56% due to difficulties in HBP lead fixation. Mean LBBB correction threshold at implant was high (3.09V± 0.44) and tended to increase at last follow-up (3.7V±0.54) with no cases of lead dislodgment. LV diameters and LVEF significantly improved during a follow-up of 31.33±21.45 months. Subsequently, different mostly observational studies have evaluated the potential utility of HBP for CRT56-63 (Table 1). Sharma et al.57 published the largest multicenter, observational and retrospective study of HBP in patients with different indications for CRT (primary CRT strategy, previous failed CS lead implantation, non-responders to conventional CRT) including 106 patients with a successful implant in 95 (90%). The mean BBB correction threshold was 2±1.2V at 1ms. During a mean follow-up of 14 months there was a significant improvement in LVEF and functional class with a 6.6% of lead related complications. In patients with a baseline LVEF<35%, mean LVEF went from 25% at baseline to 40% at last follow-up (p=0.0001) and the NYHA functional class significantly increased from 2.8 ± 0.5 to 1.8 ± 0.6 (p=0.0001). Other small, observational, single-center studies have shown similar results with significant improvement of LVEF and NYHA class58-59.
To date, only 4 randomized studies have directly compared conventional BiVP-CRT with HBP-CRT56,60-62. Lutsgarten et al.56 conducted a randomized, crossover study including 29 patients with wide QRS (>130 ms) and CRT indication who received both a LV and a HB lead and were randomized after 1 month to HBP or BiVP during 6 months and then crossover to the alternative pacing mode for 6 additional months. The HBP implant success rate was 72% and 12 patients completed the entire protocol showing significant and comparable improvements in LVEF, NYHA class, 6-minute walking test distance and quality of live (QoL) between HBP and BiVP. The His-SYNC pilot was a multicenter, prospective, randomized controlled trial comparing BiVP-CRT with HBP-CRT in patients with conventional CRT indications60. A total of 41 patients were enrolled in the study with 21 randomized to HBP-CRT and 20 to BiVP-CRT. In the treatment-received analysis, patients who received HBP-CRT showed a significantly greater QRS narrowing in comparison to BiVP-CRT (125±22 ms vs 164±25ms, p=0.001). After a mean follow-up duration of 12.2 months, the echocardiographic response, defined by a LVEF improvement ≥5%, tended to be higher with HBP-CRT but did not reach statistical significance. Of note, up to 48% of patients allocated to HBP-CRT crossed over to BiVP-CRT while 26% of patients initially randomized to BiVP-CRT were finally implanted with HBP-CRT. The presence of non-specific intraventricular conduction disturbance (IVCD) was the principal reason to crossover from HBP-CRT to BiVP-CRT.
In the His-Alternative trial, Vinther et al.61 randomized 50 patients with symptomatic HF, LVEF ≤ 35% and LBBB according to Strauss criteria, to HBP-CRT or BiVP-CRT in a 1:1 ratio and were followed during 6 months. LBBB correction was achieved in up to 72% of patients in the HBP-CRT group at implant. In the per-protocol analysis there were no differences in the LVEF improvement at 6-months between the 2 groups and HBP thresholds were significantly higher than CS lead thresholds both at implant and at follow-up. However, 7 patients crossed over from HBP-CRT group to BiVP-CRT group at implant while only 1 patient crossed over from BiV CRT to HBP CRT. In the treatment-received analysis, LVEF was significantly higher (48±8% vs. 42±8%, p<0.05) and the LV end-systolic volume (LVESV) was lower (65±22 ml vs. 83±27ml, p<0.05) in the HBP-CRT group in comparison with the BiVP-CRT group.
HBP-CRT has been also compared to BiV-CRT in patients with atrial fibrillation and LVEF<40% undergoing AV node ablation62. Using a crossover design, patients received both a CS lead and a HBP lead and were randomized to either HBP-CRT or BiVP-CRT during the first 9 months and then, switched to the alternative pacing mode during another 9 months. Fifty patients were enrolled but only 38 patients completed the 2 phases of the study and were included in the final analysis. HBP-CRT was associated with a significant improvement in LVEF in comparison to BiVP-CRT. In both groups, LVEDD, NYHA class and B-type natriuretic peptide levels significantly improved.
In summary, HBP has been evaluated in lieu of CRT in small, observational and mainly single-center studies with limited follow-up data. To date, only 125 patients have been allocated to HBP in randomized controlled trials and compared to BiVP in patients with conventional CRT indications. Two principal concerns arise when observing the currently published data in this particular setting. The first one is that the BBB correction rate with HBP is limited and highly variable ranging from 52 to 93% in patients included in randomized studies with baseline wide QRS. The second one is that this HBP-BBB correction rate is achieved with high pacing thresholds and with a relatively high incidence of lead related complications (up to 10.3%) including loss of HB capture or significant increase in BBB correction threshold during follow-up. Finally, it should be taken into consideration that all these data come from highly specialized centers with huge experience in CSP so the replication of these results may not be possible in other centers.
Clinical evidence of LBBAP-CRT
The first description of LBBP by Huang et al. in 2017 was in a patient with dilated cardiomyopathy, HF and LBBB in which both CS lead implantation and HBP lead implantation failed50. Posterior development of the technique, with the addition of left ventricular septal pacing (LVSP) under the term LBBAP, revealed that this new physiological pacing modality appeared to be technically easier than HBP, with higher implant success rates and was associated with lower pacing thresholds at implant and during follow-up. Thus, taking into account these findings, LBBAP was considered a potential alternative for CRT (Figure 4).
Li and colleagues published the first multicenter observational study evaluating LBBAP as a primary or rescue strategy after failed CS lead implantation in patients with conventional indications for CRT64 (Table 2). They attempted LBBAP in 37 patients with successful implantation in 30 including 3 patients who received both a LBBAP lead and a CS lead, and compared the outcomes with 54 matched controls retrospectively recruited who had been previously treated with conventional BiVP-CRT. LBBAP-CRT resulted in significantly narrower paced QRS, greater increase in LVEF and greater echocardiographic response and super-response in comparison with conventional BiVP-CRT. A larger observational and retrospective series was published by Vijayaraman et al.65 in 2021 including 325 patients with conventional indications for CRT who underwent LBBAP showing similar results: implant success rate of 85%, optimal and stable electrical parameters, and significant reduction in paced QRS duration, significant improvement of LVEF and NYHA class during a mean follow-up of 6 months. Other studies have consistently shown similar data in terms of significant reduction in the paced QRS duration, optimal and stable electrical parameters during follow-up and low lead-related complication rates associated with LBBAP-CRT66-67.
The first multicentre, randomized controlled study comparing LBBAP-CRT with conventional BiV-CRT was published in 2022 by Wang et al.68 A total of 40 patients with non-ischaemic cardiomyopathy, LVEF ≤ 35% and LBBB were randomized in a 1:1 fashion to LBBAP-CRT or BiVP-CRT. Two patients crossed-over from LBBAP-CRT to BiVP-CRT whereas 4 patients randomized to BiVP-CRT finally underwent LBBAP-CRT. In the intention to treat analysis and after a follow-up of 6 months, LBBAP-CRT resulted in higher LVEF improvement, greater LVESV reduction and greater reduction in NT-proBNP levels when compared with BiVP-CRT. However, rates of CRT response, paced QRS duration, changes in NYHA class and 6-minute walking test distance were comparable between LBBAP-CRT and BiVP-CRT. In the LEVEL-AT trial69 70 patients were randomized to BiVP-CRT (n=35) or CSP-CRT (n=35, 4 patients to HBP and 31 to LBBAP) showing a similar decrease in LVAT, LVESV and similar rates of mortality and HF hospitalization at 6 months follow-up between the 2 groups in the intention-to-treat analysis.
Data on clinical outcomes comparing BiVP and LBBAP have begun to arise during the last year, principally from observational, non-randomized studies but constantly pointing towards a significant reduction in HF hospitalization with LBBAP-CRT when compared with BiVP-CRT, with no differences in overall mortality70-73. The largest multicenter, observational and retrospective study published so far comparing LBBAP-CRT with BiVP-CRT included 1778 patients, 797 receiving LBBAP-CRT and 981 BiVP-CRT and provided data on clinical outcomes73. During a mean follow-up of 33±16 months both LBBAP-CRT and BiVP-CRT were associated with a significant increase in LVEF, but LBBAP-CRT showed a greater change in LVEF from baseline than BiVP-CRT (+13±12% vs. +10±12%, p<0.001). The primary outcome of the study was a combined endpoint of time to death from any cause or the first episode of HF hospitalization, and was significantly reduced with LBBAP-CRT compared to BiVP-CRT (20.8% vs 28%; HR: 1.495; 95% CI: 1.213-1.842; p < 0.001). Secondary outcomes showed that mortality was comparable between the two groups but there was a significant reduction in HF hospitalizations in the LBBAP-CRT group (HR: 1.494; 95% CI: 1.159-1.927; p=0.002).
In summary, both HBP-CRT and LBBAP-CRT are currently available techniques for delivering CRT and have demonstrated to be safe and feasible. When directly compared to BiVP and HBP-CRT, LBBAP-CRT appears to be technically easier, with better electrical parameters and with a low rate of lead-related complications74-76 (Table 3). LBBAP-CRT and HBP-CRT are associated with a better acute hemodynamic response and with a significantly greater improvement in LVEF than BiVP during follow-up when compared to BiVP-CRT. However, these direct comparisons arise from observational studies and should be taken cautiously. Data from randomized controlled trials is still required to draw definitive conclusions.
Combination of CSP with CS lead pacing-CRT
There is a subset of patients in which CSP is not able to completely correct the baseline abnormal electrical activation of the ventricles. This can be explained by the presence of a normal His-Purkinje activation even in the presence of a wide QRS that reflects a primary myocardial disease and not an electrical disease. Upadhyay et al.77 showed that among patients with LBBB patterns according to current guidelines78 intact Purkinje activation was present in up to 36% of patients and no QRS narrowing could be obtained in this subset of patient even with demonstrated HB capture. In this scenario, and when CSP in patients with baseline wide QRS is not able to obtain a significant QRS narrowing, the combination of a CS lead with either HBP (His-optimized cardiac resynchronization therapy [HOT-CRT] or LBBAP (left bundle branch-optimized cardiac resynchronization therapy [LOT-CRT] may have beneficial effects in terms of electrical resynchronization79-83 (Figure 5).
Vijayaraman et al.79 attempted HOT-CRT in 27 patients with CRT indication and different baseline conduction disease (LBBB in 17, intraventricular conduction defect in 5 and RV pacing in 5 patients) in an observational, multicentre and retrospective study. HOT-CRT was successful in 93% and the paced QRS was further reduced with HOT-CRT (120 ± 16 ms) in comparison with BiVP (162 ± 17 ms) or HBP alone (151 ± 24 ms), p<0.0001. Moreover, LVEF and NYHA class significantly improved during a mean follow-up of 14 ± 10 months with clinical and echocardiographic response obtained in 84% and 92%, respectively.
LOT-CRT has been also evaluated in 112 CRT candidates in another observational study reporting an implant success rate of 81%82. LOT-CRT resulted in a significantly greater reduction in QRS duration (144 ± 22 ms) when compared with BiVP-CRT (170 ± 30 ms) and LBBAP-CRT (162 ± 23 ms), p<0.0001. With a mean follow-up of 7.8 ± 2.3 months there was a significant improvement in LVEF and a significant reduction of NT-proBNP levels. Echocardiographic response was obtained in 62.8% and clinical response in 76% of patients.
Results from randomized controlled trials currently on-going such as the HIS-Purkinje Conduction System Pacing Optimized Trial of Cardiac Resynchronization Therapy (HOT-CRT) (NCT04561778) or the Conduction System Pacing Optimized Therapy (CSPOT) study (NCT04905290) are expected to give additional light to the potential utility of both HOT and LOT-CRT.
CSP-based CRT in other clinical scenarios
CSP-based CRT in patients with non-LBBB
Current guidelines recommend CRT for patients with symptomatic HF in spite of optimal medical treatment, LVEF ≤ 35% and non-LBBB morphology wide QRS with a lesser degree of recommendation with respect to patients with baseline LBBB (IIa if QRS ≥ 150 ms or IIb if QRS 130-149 ms according to the ESC Guidelines1). However, in the MADIT-CRT trial84, no clinical benefit was observed in patients with non-LBBB (RBBB or intraventricular conduction disturbance [IVCD]) and the echocardiographic improvements were significantly higher in patients with LBBB. The prevalence of RBBB among HF patients has been estimated around 6.1% with a non-negligible 1-year all-cause mortality rate of 11.9% so there is still a significant number of HF patients with non-LBBB who could be potential targets for pacing therapy according to guidelines but with limited support in terms of clinical benefit from currently published data85.
HBP-CRT has been evaluated in patients with baseline RBBB and CRT indications in a multicentre observational study including 39 patients (implant success rate 95%) showing acceptable bundle branch correction pacing thresholds (1.4 ± 0.7 V at 1 ms), a significant QRS narrowing (from 158±24 ms to 127±17 ms, p=0.0001) and a significant improvement in LVEF (from 31±10% to 39±13%, p=0.004) and NYHA class (from 2.8±0.6 to 2±0.7, p=0.0001) during a mean follow-up of 15 ± 23 months86. The utility of LBBAP-CRT has also been tested in an observational study including 121 patients with standard CRT indications and RBBB84. Implant success rate was 88% and LBBAP-CRT resulted in a significant narrowing of the QRS (from 150 ± 20 ms at baseline to 150 ± 24 ms, p=0.01) and a significant LVEF improvement (from 35 ± 9% to 43 ± 12, p<0.01). Clinical and echocardiographic response was seen in 60% and 61%, respectively. Females and those patients with a greater reduction in QRS duration with pacing (≥10 ms) obtained the maximum benefit from LBBAP-CRT in this particular setting.
In contradistinction to HBP, QRS duration reduction with LBBAP in the presence of a RBBB is challenging as the activation of the left conduction system is inevitably inducing delay on RV activation so most of the QRS duration narrowing observed during LBBAP in patients with baseline RBBB is due to the septal myocardial capture obtained during non-selective LBBAP. Using a bipolar pacing configuration, anodal capture, which implies simultaneous capture from the distal and proximal poles of the pacing lead tip both located within the interventricular septum, may enhance RV septal myocardial capture and thus reduce RV delayed activation. However, anodal capture thresholds are usually high (>3V in 52% of patients in the Vijayaraman et al.87 series) so cannot be used systematically in order to reduce QRS duration in patients with RBBB undergoing LBBAP-CRT.
CSP-based CRT in patients with HF undergoing AV node ablation
Patients with atrial fibrillation, HF and impaired LVEF are candidates for AV node ablation and CRT 62,88-91. In this setting CSP-based CRT is a new available pacing modality. In the ALTERNATIVE-AF62, HBP-CRT showed significant improvement of LVEF in comparison with BiVP with similar benefits in terms of NYHA class and BNP levels between both pacing modalities.
BiBP, HBP and LBBAP have been recently compared in an observational, retrospective study including 50 patients with refractory AF, symptomatic HF, impaired LVEF and narrow QRS who underwent AV node ablation and implantation of a pacing device91. HBP (n=25) and LBBAP (n=10) were associated with a significant improvement in NYHA class and LVEF whereas no significant change in both parameters was registered with BiVP (n=13).
CSP-based CRT in coronary venous lead failure or non-responders to BiVP-CRT
Both HBP and LBBAP-CRT have shown to be suitable and effective alternatives for patients with CRT indications and previous CS lead failure implant. But one step forward is to consider the potential utility of CSP-based CRT for conventional BiVP-CRT non-responders. In a multicenter, observational study, Vijayaraman et al.92 included 44 non-responders to previous BiVP-CRT patients who underwent LBBAP or LOT-CRT by adding a pacing lead in the LBB area. LVEF and volumes significantly improved with LBBAP/LOT-CRT. In this unfavorable scenario, LBBAP/LOT-CRT was able to obtain an echocardiographic response in 40%, superresponse in 9% and clinical response in 45% of these previously non-responder patients. The utility of this strategy to potentially increase CRT response and the evaluation of the risks associated with an added intervention should be tested in large randomized controlled trials.
Current recommendations and future directions
CSP-based CRT is a stablished technique with demonstrated safety and feasibility and widely accepted as an alternative for patients with CRT indications and a failed CS lead implantation in everyday clinical practice. Although HBP-CRT is theoretically the most physiological pacing modality, the difficulties in lead fixation, unreliable lead stability, limited rate of bundle branch correction and frequently high pacing thresholds are currently hindering the spread use of this physiological pacing modality in patients with CRT indications. On the contrary, LBBAP-CRT has the advantage of better lead stability, with lower pacing thresholds and higher implant success rate compared to HBP and, in spite of introducing some amount RV activation delay, has been consolidated as the preferred CSP modality for patients requiring CRT. There are still important evidence gaps regarding CSP-based CRT including the lack of long-term performance, safety and complications data as well as significant concerns about LBBAP lead extractability in the future. The development of a better and wider range of implant tools, with improvements in lead design, batteries and introduction of specific algorithms for CSP-based CRT by the manufacturers are also a critical aspect of the evolution of this technique and will surely result in patient’s benefit.
Meanwhile, current guidelines have prudently introduced CSP-based CRT into their recommendations1,93. The ESC Guidelines only consider HBP-CRT as an alternative to conventional BiVP-CRT after unsuccessful CS lead implantation or as an alternative to BiVP in patients with AF and HF undergoing AVN ablation. More recently, the 2023 HRS/APHRS/LAHRS guideline on cardiac physiologic pacing and mitigation of HF have widely introduced both HBP and LBBAP as an alternative to BiVP-CRT in multiple scenarios (Table 4).
Anyway, the bulk of evidence about CRT benefits still favors conventional BiVP-CRT as shown in figure with up to 10000 patients included in randomized controlled trials reporting data on hard clinical endpoints such as mortality and HF hospitalizations (Figure 6). On the other side, CSP-based CRT is a relatively new and promising technique and data from randomized studies is still scarce but is rapidly growing, especially with LBBAP-CRT. Large multicentre observational studies are consistently showing that LBBAP-CRT is associated with a greater LVEF improvement and significantly higher reduction of HF hospitalizations in comparison to BiVP-CRT. Multiple on-going randomized clinical trials are expected to provide more evidence in the following years to underpin CSP-based CRT as an alternative to conventional BiVP-CRT.
Conclusions
HBP and LBBAP are new physiologic pacing modalities that are able to provide effective CRT. Initial observational studies have shown that both techniques are safe and feasible and, in comparison to conventional BiVP-CRT, may be associated with a significant reduction in HF hospitalizations in patients with CRT indications. On-going randomized controlled studies should elucidate if CSP-based CRT is non-inferior or even superior to conventional BiVP-CRT.
Funding
non.
Conflicts of Interest
Dr. Cano has received consultant fees from Biotronik, Boston Scientific, Medtronic and Microport. All other authors have nothing to disclose.
References
- Glikson M, Nielsen JC, Kronborg MB, Michowitz Y, Auricchio A, Barbash IM, Barrabés JA, Boriani G, Braunschweig F, Brignole M, Burri H, Coats AJS, Deharo JC, Delgado V, Diller GP, Israel CW, Keren A, Knops RE, Kotecha D, Leclercq C, Merkely B, Starck C, Thylén I, Tolosana JM; ESC Scientific Document Group. 2021 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy. Eur Heart J. 2021 Sep 14;42(35):3427-3520. Erratum in: Eur Heart J. 2022 May 1;43(17):1651. [CrossRef]
- Cazeau S, Ritter P, Bakdach S, Lazarus A, Limousin M, Henao L, Mundler O, Daubert JC, Mugica J. Four chamber pacing in dilated cardiomyopathy. Pacing Clin Electrophysiol. 1994 Nov;17(11 Pt 2):1974-9. [CrossRef] [PubMed]
- Cazeau S, Ritter P, Lazarus A, Gras D, Backdach H, Mundler O, Mugica J. Multisite pacing for end-stage heart failure: early experience. Pacing Clin Electrophysiol. 1996 Nov;19(11 Pt 2):1748-57. [CrossRef] [PubMed]
- Leclercq C, Cazeau S, Le Breton H, Ritter P, Mabo P, Gras D, Pavin D, Lazarus A, Daubert JC. Acute hemodynamic effects of biventricular DDD pacing in patients with end-stage heart failure. J Am Coll Cardiol. 1998 Dec;32(7):1825-31. [CrossRef] [PubMed]
- Blanc JJ, Etienne Y, Gilard M, Mansourati J, Munier S, Boschat J, Benditt DG, Lurie KG. Evaluation of different ventricular pacing sites in patients with severe heart failure: results of an acute hemodynamic study. Circulation. 1997 Nov 18;96(10):3273-7. [CrossRef] [PubMed]
- Butter C, Auricchio A, Stellbrink C, Fleck E, Ding J, Yu Y, Huvelle E, Spinelli J; Pacing Therapy for Chronic Heart Failure II Study Group. Effect of resynchronization therapy stimulation site on the systolic function of heart failure patients. Circulation. 2001 Dec 18;104(25):3026-9. [CrossRef] [PubMed]
- Cazeau S, Leclercq C, Lavergne T, Walker S, Varma C, Linde C, Garrigue S, Kappenberger L, Haywood GA, Santini M, Bailleul C, Daubert JC; Multisite Stimulation in Cardiomyopathies (MUSTIC) Study Investigators. Effects of multisite biventricular pacing in patients with heart failure and intraventricular conduction delay. N Engl J Med. 2001 Mar 22;344(12):873-80. [CrossRef] [PubMed]
- Linde C, Leclercq C, Rex S, Garrigue S, Lavergne T, Cazeau S, McKenna W, Fitzgerald M, Deharo JC, Alonso C, Walker S, Braunschweig F, Bailleul C, Daubert JC. Long-term benefits of biventricular pacing in congestive heart failure: results from the MUltisite STimulation in cardiomyopathy (MUSTIC) study. J Am Coll Cardiol. 2002 Jul 3;40(1):111-8. [CrossRef] [PubMed]
- Auricchio A, Stellbrink C, Sack S, Block M, Vogt J, Bakker P, Huth C, Schöndube F, Wolfhard U, Böcker D, Krahnefeld O, Kirkels H; Pacing Therapies in Congestive Heart Failure (PATH-CHF) Study Group. Long-term clinical effect of hemodynamically optimized cardiac resynchronization therapy in patients with heart failure and ventricular conduction delay. J Am Coll Cardiol. 2002 Jun 19;39(12):2026-33. [CrossRef] [PubMed]
- Abraham WT, Fisher WG, Smith AL, Delurgio DB, Leon AR, Loh E, Kocovic DZ, Packer M, Clavell AL, Hayes DL, Ellestad M, Trupp RJ, Underwood J, Pickering F, Truex C, McAtee P, Messenger J; MIRACLE Study Group. Multicenter InSync Randomized Clinical Evaluation. Cardiac resynchronization in chronic heart failure. N Engl J Med. 2002 Jun 13;346(24):1845-53. [CrossRef] [PubMed]
- Young JB, Abraham WT, Smith AL, Leon AR, Lieberman R, Wilkoff B, Canby RC, Schroeder JS, Liem LB, Hall S, Wheelan K; Multicenter InSync ICD Randomized Clinical Evaluation (MIRACLE ICD) Trial Investigators. Combined cardiac resynchronization and implantable cardioversion defibrillation in advanced chronic heart failure: the MIRACLE ICD Trial. JAMA. 2003 ;289(20):2685-94. 28 May. [CrossRef] [PubMed]
- Higgins SL, Hummel JD, Niazi IK, Giudici MC, Worley SJ, Saxon LA, Boehmer JP, Higginbotham MB, De Marco T, Foster E, Yong PG. Cardiac resynchronization therapy for the treatment of heart failure in patients with intraventricular conduction delay and malignant ventricular tachyarrhythmias. J Am Coll Cardiol. 2003 Oct 15;42(8):1454-9. [CrossRef] [PubMed]
- Abraham WT, Young JB, León AR, Adler S, Bank AJ, Hall SA, Lieberman R, Liem LB, O'Connell JB, Schroeder JS, Wheelan KR; Multicenter InSync ICD II Study Group. Effects of cardiac resynchronization on disease progression in patients with left ventricular systolic dysfunction, an indication for an implantable cardioverter-defibrillator, and mildly symptomatic chronic heart failure. Circulation. 2004 Nov 2;110(18):2864-8. [CrossRef]
- Bristow MR, Saxon LA, Boehmer J, Krueger S, Kass DA, De Marco T, Carson P, DiCarlo L, DeMets D, White BG, DeVries DW, Feldman AM; Comparison of Medical Therapy, Pacing, and Defibrillation in Heart Failure (COMPANION) Investigators. Cardiac-resynchronization therapy with or without an implantable defibrillator in advanced chronic heart failure. N Engl J Med. 2004 ;350(21):2140-50. 20 May. [CrossRef] [PubMed]
- Cleland JG, Daubert JC, Erdmann E, Freemantle N, Gras D, Kappenberger L, Tavazzi L; Cardiac Resynchronization-Heart Failure (CARE-HF) Study Investigators. The effect of cardiac resynchronization on morbidity and mortality in heart failure. N Engl J Med. 2005 Apr 14;352(15):1539-49. [CrossRef]
- Cleland JG, Daubert JC, Erdmann E, Freemantle N, Gras D, Kappenberger L, Tavazzi L. Longer-term effects of cardiac resynchronization therapy on mortality in heart failure [the CArdiac REsynchronization-Heart Failure (CARE-HF) trial extension phase]. Eur Heart J. 2006 Aug;27(16):1928-32. [CrossRef]
- Kindermann M, Hennen B, Jung J, Geisel J, Böhm M, Fröhlig G. Biventricular versus conventional right ventricular stimulation for patients with standard pacing indication and left ventricular dysfunction: the Homburg Biventricular Pacing Evaluation (HOBIPACE). J Am Coll Cardiol. 2006 ;47(10):1927-37. 16 May. [CrossRef]
- Beshai JF, Grimm RA, Nagueh SF, Baker JH 2nd, Beau SL, Greenberg SM, Pires LA, Tchou PJ; RethinQ Study Investigators. Cardiac-resynchronization therapy in heart failure with narrow QRS complexes. N Engl J Med. 2007 Dec 13;357(24):2461-71. [CrossRef]
- Chung ES, Leon AR, Tavazzi L, Sun JP, Nihoyannopoulos P, Merlino J, Abraham WT, Ghio S, Leclercq C, Bax JJ, Yu CM, Gorcsan J 3rd, St John Sutton M, De Sutter J, Murillo J. Results of the Predictors of Response to CRT (PROSPECT) trial. Circulation. 2008 ;117(20):2608-16. 20 May. [CrossRef]
- Linde C, Gold MR, Abraham WT, St John Sutton M, Ghio S, Cerkvenik J, Daubert C; REsynchronization reVErses Remodeling in Systolic left vEntricular dysfunction Study Group. Long-term impact of cardiac resynchronization therapy in mild heart failure: 5-year results from the REsynchronization reVErses Remodeling in Systolic left vEntricular dysfunction (REVERSE) study. Eur Heart J. 2013 Sep;34(33):2592-9. [CrossRef]
- Moss AJ, Hall WJ, Cannom DS, Klein H, Brown MW, Daubert JP, Estes NA 3rd, Foster E, Greenberg H, Higgins SL, Pfeffer MA, Solomon SD, Wilber D, Zareba W; MADIT-CRT Trial Investigators. Cardiac-resynchronization therapy for the prevention of heart-failure events. N Engl J Med. 2009 Oct 1;361(14):1329-38. [CrossRef]
- Tang AS, Wells GA, Talajic M, Arnold MO, Sheldon R, Connolly S, Hohnloser SH, Nichol G, Birnie DH, Sapp JL, Yee R, Healey JS, Rouleau JL; Resynchronization-Defibrillation for Ambulatory Heart Failure Trial Investigators. Cardiac-resynchronization therapy for mild-to-moderate heart failure. N Engl J Med. 2010 Dec 16;363(25):2385-95. [CrossRef]
- Curtis AB, Worley SJ, Adamson PB, Chung ES, Niazi I, Sherfesee L, Shinn T, Sutton MS; Biventricular versus Right Ventricular Pacing in Heart Failure Patients with Atrioventricular Block (BLOCK HF) Trial Investigators. Biventricular pacing for atrioventricular block and systolic dysfunction. N Engl J Med. 2013 Apr 25;368(17):1585-93. [CrossRef] [PubMed]
- Ruschitzka F, Abraham WT, Singh JP, Bax JJ, Borer JS, Brugada J, Dickstein K, Ford I, Gorcsan J 3rd, Gras D, Krum H, Sogaard P, Holzmeister J; EchoCRT Study Group. Cardiac-resynchronization therapy in heart failure with a narrow QRS complex. N Engl J Med. 2013 Oct 10;369(15):1395-405. [CrossRef]
- Thibault B, Harel F, Ducharme A, White M, Ellenbogen KA, Frasure-Smith N, Roy D, Philippon F, Dorian P, Talajic M, Dubuc M, Guerra PG, Macle L, Rivard L, Andrade J, Khairy P; LESSER-EARTH Investigators. Cardiac resynchronization therapy in patients with heart failure and a QRS complex. [CrossRef]
- Gamble JHP, Herring N, Ginks M, Rajappan K, Bashir Y, Betts TR. Procedural Success of Left Ventricular Lead Placement for Cardiac Resynchronization Therapy: A Meta-Analysis. JACC Clin Electrophysiol. 2016 Feb;2(1):69-77.
- Moubarak G, Bouzeman A, Ollitrault J, Anselme F, Cazeau S. Phrenic nerve stimulation in cardiac resynchronization therapy. J Interv Card Electrophysiol. 2014 Oct;41(1):15-21. [CrossRef] [PubMed]
- Biffi M, Exner DV, Crossley GH, Ramza B, Coutu B, Tomassoni G, Kranig W, Li S, Kristiansen N, Voss F. Occurrence of phrenic nerve stimulation in cardiac resynchronization therapy patients: the role of left ventricular lead type and placement site. Europace. 2013 Jan;15(1):77-82. [CrossRef] [PubMed]
- Auricchio A, Heggermont WA. Technology Advances to Improve Response to Cardiac Resynchronization Therapy: What Clinicians Should Know. Rev Esp Cardiol (Engl Ed). 2018 Jun;71(6):477-484. English, Spanish. [CrossRef] [PubMed]
- Abdelrahman M, Subzposh FA, Beer D, Durr B, Naperkowski A, Sun H, Oren JW, Dandamudi G, Vijayaraman P. Clinical Outcomes of His Bundle Pacing Compared to Right Ventricular Pacing. J Am Coll Cardiol. 2018 ;71(20):2319-2330. 22 May. [CrossRef] [PubMed]
- Zanon F, Abdelrahman M, Marcantoni L, Naperkowski A, Subzposh FA, Pastore G, Baracca E, Boaretto G, Raffagnato P, Tiribello A, Dandamudi G, Vijayaraman P. Long term performance and safety of His bundle pacing: A multicenter experience. J Cardiovasc Electrophysiol. 2019 Sep;30(9):1594-1601. [CrossRef] [PubMed]
- Keene D, Arnold AD, Jastrzębski M, Burri H, Zweibel S, Crespo E, Chandrasekaran B, Bassi S, Joghetaei N, Swift M, Moskal P, Francis DP, Foley P, Shun-Shin MJ, Whinnett ZI. His bundle pacing, learning curve, procedure characteristics, safety, and feasibility: Insights from a large international observational study. J Cardiovasc Electrophysiol. 2019 Oct;30(10):1984-1993. [CrossRef] [PubMed]
- Shan P, Su L, Zhou X, Wu S, Xu L, Xiao F, Zhou X, Ellenbogen KA, Huang W. Beneficial effects of upgrading to His bundle pacing in chronically paced patients with left ventricular ejection fraction. [CrossRef] [PubMed]
- Vijayaraman P, Herweg B, Dandamudi G, Mittal S, Bhatt AG, Marcantoni L, Naperkowski A, Sharma PS, Zanon F. Outcomes of His-bundle pacing upgrade after long-term right ventricular pacing and/or pacing-induced cardiomyopathy: Insights into disease progression. Heart Rhythm. 2019 Oct;16(10):1554-1561. [CrossRef] [PubMed]
- Huang W, Chen X, Su L, Wu S, Xia X, Vijayaraman P. A beginner's guide to permanent left bundle branch pacing. Heart Rhythm. 2019 Dec;16(12):1791-1796. [CrossRef] [PubMed]
- Vijayaraman P, Subzposh FA, Naperkowski A, Panikkath R, John K, Mascarenhas V, Bauch TD, Huang W. Prospective evaluation of feasibility and electrophysiologic and echocardiographic characteristics of left bundle branch area pacing. Heart Rhythm. 2019 Dec;16(12):1774-1782. [CrossRef] [PubMed]
- Su L, Wang S, Wu S, Xu L, Huang Z, Chen X, Zheng R, Jiang L, Ellenbogen KA, Whinnett ZI, Huang W. Long-Term Safety and Feasibility of Left Bundle Branch Pacing in a Large Single-Center Study. Circ Arrhythm Electrophysiol. 2021 Feb;14(2):e009261. [CrossRef] [PubMed]
- Sharma PS, Patel NR, Ravi V, Zalavadia DV, Dommaraju S, Garg V, Larsen TR, Naperkowski AM, Wasserlauf J, Krishnan K, Young W, Pokharel P, Oren JW, Storm RH, Trohman RG, Huang HD, Subzposh FA, Vijayaraman P. Clinical outcomes of left bundle branch area pacing compared to right ventricular pacing: Results from the Geisinger-Rush Conduction System Pacing Registry. Heart Rhythm. 2022 Jan;19(1):3-11. Erratum in: Heart Rhythm. 2023 Jul;20(7):1100. [CrossRef] [PubMed]
- Vecera J, Penicka M, Eriksen M, Russell K, Bartunek J, Vanderheyden M, Smiseth OA. Wasted septal work in left ventricular dyssynchrony: a novel principle to predict response to cardiac resynchronization therapy. Eur Heart J Cardiovasc Imaging. 2016 Jun;17(6):624-32. [CrossRef] [PubMed]
- Spragg DD, Leclercq C, Loghmani M, Faris OP, Tunin RS, DiSilvestre D, McVeigh ER, Tomaselli GF, Kass DA. Regional alterations in protein expression in the dyssynchronous failing heart. Circulation. 2003 Aug 26;108(8):929-32. [CrossRef] [PubMed]
- Tan NY, Witt CM, Oh JK, Cha YM. Left Bundle Branch Block: Current and Future Perspectives. Circ Arrhythm Electrophysiol. 2020 Apr;13(4):e008239. [CrossRef] [PubMed]
- Sweeney MO, Hellkamp AS, Ellenbogen KA, Greenspon AJ, Freedman RA, Lee KL, Lamas GA; MOde Selection Trial Investigators. Adverse effect of ventricular pacing on heart failure and atrial fibrillation among patients with normal baseline QRS duration in a clinical trial of pacemaker therapy for sinus node dysfunction. Circulation. 2003 Jun 17;107(23):2932-7. [CrossRef] [PubMed]
- Wilkoff BL, Cook JR, Epstein AE, Greene HL, Hallstrom AP, Hsia H, Kutalek SP, Sharma A; Dual Chamber and VVI Implantable Defibrillator Trial Investigators. Dual-chamber pacing or ventricular backup pacing in patients with an implantable defibrillator: the Dual Chamber and VVI Implantable Defibrillator (DAVID) Trial. JAMA. 2002 Dec 25;288(24):3115-23. [CrossRef] [PubMed]
- Kirk JA, Kass DA. Cellular and Molecular Aspects of Dyssynchrony and Resynchronization. Card Electrophysiol Clin. 2015 Dec;7(4):585-97. [CrossRef] [PubMed]
- Nguyên UC, Verzaal NJ, van Nieuwenhoven FA, Vernooy K, Prinzen FW. Pathobiology of cardiac dyssynchrony and resynchronization therapy. Europace. 2018 Dec 1;20(12):1898-1909. [CrossRef] [PubMed]
- Merchant FM, Mittal S. Pacing induced cardiomyopathy. J Cardiovasc Electrophysiol. 2020 Jan;31(1):286-292. [CrossRef] [PubMed]
- Khurshid S, Obeng-Gyimah E, Supple GE, Schaller R, Lin D, Owens AT, Epstein AE, Dixit S, Marchlinski FE, Frankel DS. Reversal of Pacing-Induced Cardiomyopathy Following Cardiac Resynchronization Therapy. JACC Clin Electrophysiol. 2018 Feb;4(2):168-177. [CrossRef] [PubMed]
- Lu W, Lin J, Dai Y, Chen K, Zhang S. The therapeutic effects of upgrade to cardiac resynchronization therapy in pacing-induced cardiomyopathy or chronic right ventricular pacing patients: a meta-analysis. Heart Fail Rev. 2022 Mar;27(2):507-516. [CrossRef] [PubMed]
- Deshmukh P, Casavant DA, Romanyshyn M, Anderson K. Permanent, direct His-bundle pacing: a novel approach to cardiac pacing in patients with normal His-Purkinje activation. Circulation. 2000 Feb 29;101(8):869-77. [CrossRef] [PubMed]
- Huang W, Su L, Wu S, Xu L, Xiao F, Zhou X, Ellenbogen KA. A Novel Pacing Strategy With Low and Stable Output: Pacing the Left Bundle Branch Immediately Beyond the Conduction Block. Can J Cardiol. 2017 Dec;33(12):1736.e1-1736.e3. [CrossRef] [PubMed]
- Arnold AD, Shun-Shin MJ, Keene D, Howard JP, Sohaib SMA, Wright IJ, Cole GD, Qureshi NA, Lefroy DC, Koa-Wing M, Linton NWF, Lim PB, Peters NS, Davies DW, Muthumala A, Tanner M, Ellenbogen KA, Kanagaratnam P, Francis DP, Whinnett ZI. His Resynchronization Versus Biventricular Pacing in Patients With Heart Failure and Left Bundle Branch Block. J Am Coll Cardiol. 2018 Dec 18;72(24):3112-3122. [CrossRef] [PubMed]
- Sussenbek O, Rademakers L, Waldauf P, Jurak P, Smisek R, Stros P, Poviser L, Vesela J, Plesinger F, Halamek J, Leinveber P, Herman D, Osmancik P, Curila K. Left bundle branch area pacing results in more physiological ventricular activation than biventricular pacing in patients with left bundle branch block heart failure. Eur Heart J Suppl. 2023 ;25(Suppl E):E17-E24. 24 May. [CrossRef] [PubMed]
- Vijayaraman P, Dandamudi G, Zanon F, Sharma PS, Tung R, Huang W, Koneru J, Tada H, Ellenbogen KA, Lustgarten DL. Permanent His bundle pacing: Recommendations from a Multicenter His Bundle Pacing Collaborative Working Group for standardization of definitions, implant measurements, and follow-up. Heart Rhythm. 2018 Mar;15(3):460-468. [CrossRef] [PubMed]
- Burri H, Jastrzebski M, Cano Ó, Čurila K, de Pooter J, Huang W, Israel C, Joza J, Romero J, Vernooy K, Vijayaraman P, Whinnett Z, Zanon F. EHRA clinical consensus statement on conduction system pacing implantation: executive summary. Endorsed by the Asia-Pacific Heart Rhythm Society (APHRS), Canadian Heart Rhythm Society (CHRS) and Latin-American Heart Rhythm Society (LAHRS). Europace. 2023 Apr 15;25(4):1237-1248. [CrossRef] [PubMed]
- Barba-Pichardo R, Manovel Sánchez A, Fernández-Gómez JM, Moriña-Vázquez P, Venegas-Gamero J, Herrera-Carranza M. Ventricular resynchronization therapy by direct His-bundle pacing using an internal cardioverter defibrillator. Europace. 2013 Jan;15(1):83-8. [CrossRef] [PubMed]
- Lustgarten DL, Crespo EM, Arkhipova-Jenkins I, Lobel R, Winget J, Koehler J, Liberman E, Sheldon T. His-bundle pacing versus biventricular pacing in cardiac resynchronization therapy patients: A crossover design comparison. Heart Rhythm. 2015 Jul;12(7):1548-57. [CrossRef] [PubMed]
- Sharma PS, Dandamudi G, Herweg B, Wilson D, Singh R, Naperkowski A, Koneru JN, Ellenbogen KA, Vijayaraman P. Permanent His-bundle pacing as an alternative to biventricular pacing for cardiac resynchronization therapy: A multicenter experience. Heart Rhythm. 2018 Mar;15(3):413-420. [CrossRef] [PubMed]
- Huang W, Su L, Wu S, Xu L, Xiao F, Zhou X, Mao G, Vijayaraman P, Ellenbogen KA. Long-term outcomes of His bundle pacing in patients with heart failure with left bundle branch block. Heart. 2019 Jan;105(2):137-143. [CrossRef] [PubMed]
- Moriña-Vázquez P, Moraleda-Salas MT, Manovel-Sánchez AJ, Fernández-Gómez JM, Arce-Léon Á, Venegas-Gamero J, Barba-Pichardo R. Early improvement of left ventricular ejection fraction by cardiac resynchronization through His bundle pacing in patients with heart failure. Europace. 2020 Jan 1;22(1):125-132. [CrossRef] [PubMed]
- Upadhyay GA, Vijayaraman P, Nayak HM, Verma N, Dandamudi G, Sharma PS, Saleem M, Mandrola J, Genovese D, Oren JW, Subzposh FA, Aziz Z, Beaser A, Shatz D, Besser S, Lang RM, Trohman RG, Knight BP, Tung R; His-SYNC Investigators. On-treatment comparison between corrective His bundle pacing and biventricular pacing for cardiac resynchronization: A secondary analysis of the His-SYNC Pilot Trial. Heart Rhythm. 2019 Dec;16(12):1797-1807. [CrossRef] [PubMed]
- Vinther M, Risum N, Svendsen JH, Møgelvang R, Philbert BT. A Randomized Trial of His Pacing Versus Biventricular Pacing in Symptomatic HF Patients With Left Bundle Branch Block (His-Alternative). JACC Clin Electrophysiol. 2021 Nov;7(11):1422-1432. [CrossRef] [PubMed]
- Huang W, Wang S, Su L, Fu G, Su Y, Chen K, Zou J, Han H, Wu S, Sheng X, Chen X, Fan X, Xu L, Zhou X, Mao G, Ellenbogen KA, Whinnett ZI. His-bundle pacing vs biventricular pacing following atrioventricular nodal ablation in patients with atrial fibrillation and reduced ejection fraction: A multicenter, randomized, crossover study-The ALTERNATIVE-AF trial. Heart Rhythm. 2022 Dec;19(12):1948-1955. [CrossRef] [PubMed]
- Whinnett ZI, Shun-Shin MJ, Tanner M, Foley P, Chandrasekaran B, Moore P, Adhya S, Qureshi N, Muthumala A, Lane R, Rinaldi A, Agarwal S, Leyva F, Behar J, Bassi S, Ng A, Scott P, Prasad R, Swinburn J, Tomson J, Sethi A, Shah J, Lim PB, Kyriacou A, Thomas D, Chuen J, Kamdar R, Kanagaratnam P, Mariveles M, Burden L, March K, Howard JP, Arnold A, Vijayaraman P, Stegemann B, Johnson N, Falaschetti E, Francis DP, Cleland JGF, Keene D. Effects of haemodynamically atrio-ventricular optimized His bundle pacing on heart failure symptoms and exercise capacity: the His Optimized Pacing Evaluated for Heart Failure (HOPE-HF) randomized, double-blind, cross-over trial. Eur J Heart Fail. 2023 Feb;25(2):274-283. [CrossRef] [PubMed]
- Li X, Qiu C, Xie R, Ma W, Wang Z, Li H, Wang H, Hua W, Zhang S, Yao Y, Fan X. Left bundle branch area pacing delivery of cardiac resynchronization therapy and comparison with biventricular pacing. ESC Heart Fail. 2020 Aug;7(4):1711-1722. [CrossRef] [PubMed]
- Vijayaraman P, Ponnusamy S, Cano Ó, Sharma PS, Naperkowski A, Subsposh FA, Moskal P, Bednarek A, Dal Forno AR, Young W, Nanda S, Beer D, Herweg B, Jastrzebski M. Left Bundle Branch Area Pacing for Cardiac Resynchronization Therapy: Results From the International LBBAP Collaborative Study Group. JACC Clin Electrophysiol. 2021 Feb;7(2):135-147. [CrossRef] [PubMed]
- Jastrzębski M, Kiełbasa G, Cano O, Curila K, Heckman L, De Pooter J, Chovanec M, Rademakers L, Huybrechts W, Grieco D, Whinnett ZI, Timmer SAJ, Elvan A, Stros P, Moskal P, Burri H, Zanon F, Vernooy K. Left bundle branch area pacing outcomes: the multicentre European MELOS study. Eur Heart J. 2022 Oct 21;43(40):4161-4173. [CrossRef] [PubMed]
- Chen X, Ye Y, Wang Z, Jin Q, Qiu Z, Wang J, Qin S, Bai J, Wang W, Liang Y, Chen H, Sheng X, Gao F, Zhao X, Fu G, Ellenbogen KA, Su Y, Ge J. Cardiac resynchronization therapy via left bundle branch pacing vs. optimized biventricular pacing with adaptive algorithm in heart failure with left bundle branch block: a prospective, multi-centre, observational study. Europace. 2022 ;24(5):807-816. 3 May. [CrossRef] [PubMed]
- Wang Y, Zhu H, Hou X, Wang Z, Zou F, Qian Z, Wei Y, Wang X, Zhang L, Li X, Liu Z, Xue S, Qin C, Zeng J, Li H, Wu H, Ma H, Ellenbogen KA, Gold MR, Fan X, Zou J; LBBP-RESYNC Investigators. Randomized Trial of Left Bundle Branch vs Biventricular Pacing for Cardiac Resynchronization Therapy. J Am Coll Cardiol. 2022 Sep 27;80(13):1205-1216. [CrossRef] [PubMed]
- Pujol-Lopez M, Jiménez-Arjona R, Garre P, Guasch E, Borràs R, Doltra A, Ferró E, García-Ribas C, Niebla M, Carro E, Puente JL, Vázquez-Calvo S, Invers-Rubio E, Roca-Luque I, Castel MÁ, Arbelo E, Sitges M, Brugada J, Tolosana JM, Mont L. Conduction System Pacing vs Biventricular Pacing in Heart Failure and Wide QRS Patients: LEVEL-AT Trial. JACC Clin Electrophysiol. 2022 Nov;8(11):1431-1445. [CrossRef] [PubMed]
- Vijayaraman P, Zalavadia D, Haseeb A, Dye C, Madan N, Skeete JR, Vipparthy SC, Young W, Ravi V, Rajakumar C, Pokharel P, Larsen T, Huang HD, Storm RH, Oren JW, Batul SA, Trohman RG, Subzposh FA, Sharma PS. Clinical outcomes of conduction system pacing compared to biventricular pacing in patients requiring cardiac resynchronization therapy. Heart Rhythm. 2022 Aug;19(8):1263-1271. [CrossRef] [PubMed]
- Ezzeddine FM, Pistiolis SM, Pujol-Lopez M, Lavelle M, Wan EY, Patton KK, Robinson M, Lador A, Tamirisa K, Karim S, Linde C, Parkash R, Birgersdotter-Green U, Russo AM, Chung M, Cha YM. Outcomes of conduction system pacing for cardiac resynchronization therapy in patients with heart failure: A multicenter experience. Heart Rhythm. 2023 Jun;20(6):863-871. [CrossRef] [PubMed]
- Diaz JC, Sauer WH, Duque M, Koplan BA, Braunstein ED, Marín JE, Aristizabal J, Niño CD, Bastidas O, Martinez JM, Hoyos C, Matos CD, Lopez-Cabanillas N, Steiger NA, Kapur S, Tadros TM, Martin DT, Zei PC, Tedrow UB, Romero JE. Left Bundle Branch Area Pacing Versus Biventricular Pacing as Initial Strategy for Cardiac Resynchronization. JACC Clin Electrophysiol. 2023 Aug;9(8 Pt 2):1568-1581. [CrossRef] [PubMed]
- Vijayaraman P, Sharma PS, Cano Ó, Ponnusamy SS, Herweg B, Zanon F, Jastrzebski M, Zou J, Chelu MG, Vernooy K, Whinnett ZI, Nair GM, Molina-Lerma M, Curila K, Zalavadia D, Haseeb A, Dye C, Vipparthy SC, Brunetti R, Moskal P, Ross A, van Stipdonk A, George J, Qadeer YK, Mumtaz M, Kolominsky J, Zahra SA, Golian M, Marcantoni L, Subzposh FA, Ellenbogen KA. Comparison of Left Bundle Branch Area Pacing and Biventricular Pacing in Candidates for Resynchronization Therapy. J Am Coll Cardiol. 2023 Jul 18;82(3):228-241. [CrossRef] [PubMed]
- Mariani MV, Piro A, Forleo GB, Della Rocca DG, Natale A, Miraldi F, Vizza CD, Lavalle C. Clinical, procedural and lead outcomes associated with different pacing techniques: a network meta-analysis. Int J Cardiol. 2023;377:52–9. [CrossRef] [PubMed]
- Ali N, Arnold AD, Miyazawa AA, Keene D, Chow JJ, Little I, Peters NS, Kanagaratnam P, Qureshi N, Ng FS, Linton NWF, Lefroy DC, Francis DP, Phang Boon L, Tanner MA, Muthumala A, Shun-Shin MJ, Cole GD, Whinnett ZI. Comparison of methods for delivering cardiac resynchronization therapy: an acute electrical and haemodynamic within- patient comparison of left bundle branch area, His bundle, and biventricular pacing. Europace. 2023;25(3):1060–7. [CrossRef] [PubMed]
- Hua J, Wang C, Kong Q, Zhang Y, Wang Q, Xiong Z, Hu J, Li J, Chen Q, Hong K. Comparative effects of left bundle branch area pacing, His bundle pacing, biventricular pacing in patients requiring cardiac resynchronization therapy: a network meta-analysis. Clin Cardiol. 2022;45(2):214–223. [CrossRef] [PubMed]
- Upadhyay GA, Cherian T, Shatz DY, Beaser AD, Aziz Z, Ozcan C, Broman MT, Nayak HM, Tung R. Intracardiac Delineation of Septal Conduction in Left Bundle-Branch Block Patterns. Circulation. 2019 Apr 16;139(16):1876-1888. [CrossRef] [PubMed]
- Surawicz B, Childers R, Deal BJ, Gettes LS. AHA/ACCF/HRS recommendations for the standardization and interpretation of the electrocardiogram, part III: intraventricular conduction disturbances: a scientific statement from the American Heart Association Electrocardiography and Arrhythmias Committee, Council on Clinical Cardiology; the American College of Cardiology Foundation; and the Heart Rhythm Society: endorsed by the International Society for Computerized Electrocardiology. Circulation. 2009;119:e235–e240. [CrossRef]
- Vijayaraman P, Herweg B, Ellenbogen KA, Gajek J. His-Optimized Cardiac Resynchronization Therapy to Maximize Electrical Resynchronization: A Feasibility Study. Circ Arrhythm Electrophysiol. 2019 Feb;12(2):e006934. [CrossRef] [PubMed]
- Zweerink A, Zubarev S, Bakelants E, Potyagaylo D, Stettler C, Chmelevsky M, Lozeron ED, Hachulla AL, Vallée JP, Burri H. His-Optimized Cardiac Resynchronization Therapy With Ventricular Fusion Pacing for Electrical Resynchronization in Heart Failure. JACC Clin Electrophysiol. 2021 Jul;7(7):881-892. [CrossRef] [PubMed]
- Deshmukh A, Sattur S, Bechtol T, Heckman LIB, Prinzen FW, Deshmukh P. Sequential His bundle and left ventricular pacing for cardiac resynchronization. J Cardiovasc Electrophysiol. 2020 Sep;31(9):2448-2454. [CrossRef] [PubMed]
- Jastrzębski M, Moskal P, Huybrechts W, Curila K, Sreekumar P, Rademakers LM, Ponnusamy SS, Herweg B, Sharma PS, Bednarek A, Rajzer M, Vijayaraman P. Left bundle branch-optimized cardiac resynchronization therapy (LOT-CRT): Results from an international LBBAP collaborative study group. Heart Rhythm. 2022 Jan;19(1):13-21. [CrossRef] [PubMed]
- Feng XF, Yang LC, Zhao Y, Yu YC, Liu B, Li YG. Effects of adaptive left bundle branch-optimized cardiac resynchronization therapy: a single centre experience. BMC Cardiovasc Disord. 2022 Aug 6;22(1):360. Erratum in: BMC Cardiovasc Disord. 2022 Dec 22;22(1):558. [CrossRef] [PubMed]
- Zareba W, Klein H, Cygankiewicz I, Hall WJ, McNitt S, Brown M, Cannom D, Daubert JP, Eldar M, Gold MR, Goldberger JJ, Goldenberg I, Lichstein E, Pitschner H, Rashtian M, Solomon S, Viskin S, Wang P, Moss AJ; MADIT-CRT Investigators. Effectiveness of Cardiac Resynchronization Therapy by QRS Morphology in the Multicenter Automatic Defibrillator Implantation Trial-Cardiac Resynchronization Therapy (MADIT-CRT). Circulation. 2011 Mar 15;123(10):1061-72. [CrossRef] [PubMed]
- Baldasseroni S, Opasich C, Gorini M, Lucci D, Marchionni N, Marini M, Campana C, Perini G, Deorsola A, Masotti G, Tavazzi L, Maggioni AP; Italian Network on Congestive Heart Failure Investigators. Left bundle-branch block is associated with increased 1-year sudden and total mortality rate in 5517 outpatients with congestive heart failure: a report from the Italian network on congestive heart failure. Am Heart J. 2002 Mar;143(3):398-405. [CrossRef] [PubMed]
- Sharma PS, Naperkowski A, Bauch TD, Chan JYS, Arnold AD, Whinnett ZI, Ellenbogen KA, Vijayaraman P. Permanent His Bundle Pacing for Cardiac Resynchronization Therapy in Patients With Heart Failure and Right Bundle Branch Block. Circ Arrhythm Electrophysiol. 2018 Sep;11(9):e006613. [CrossRef] [PubMed]
- Vijayaraman P, Cano O, Ponnusamy SS, Molina-Lerma M, Chan JYS, Padala SK, Sharma PS, Whinnett ZI, Herweg B, Upadhyay GA, Subzposh FA, Patel NR, Beer DA, Bednarek A, Kielbasa G, Tung R, Ellenbogen KA, Jastrzebski M. Left bundle branch area pacing in patients with heart failure and right bundle branch block: Results from International LBBAP Collaborative-Study Group. Heart Rhythm O2. 2022 ;3(4):358-367. 14 May. [CrossRef] [PubMed]
- Koniari I, Gerakaris A, Kounis N, Velissaris D, Rao A, Ainslie M, Adlan A, Plotas P, Ikonomidis I, Mplani V, Hung MY, de Gregorio C, Kolettis T, Gupta D. Outcomes of Atrioventricular Node Ablation and Pacing in Patients with Heart Failure and Atrial Fibrillation: From Cardiac Resynchronization Therapy to His Bundle Pacing. J Cardiovasc Dev Dis. 2023 Jun 26;10(7):272. [CrossRef] [PubMed]
- Huang W, Su L, Wu S, Xu L, Xiao F, Zhou X, Ellenbogen KA. Benefits of Permanent His Bundle Pacing Combined With Atrioventricular Node Ablation in Atrial Fibrillation Patients With Heart Failure With Both Preserved and Reduced Left Ventricular Ejection Fraction. J Am Heart Assoc. 2017 Apr 1;6(4):e005309. [CrossRef] [PubMed]
- Su L, Cai M, Wu S, Wang S, Xu T, Vijayaraman P, Huang W. Long-term performance and risk factors analysis after permanent His-bundle pacing and atrioventricular node ablation in patients with atrial fibrillation and heart failure. Europace. 2020 Dec 26;22(Suppl_2):ii19-ii26. [CrossRef] [PubMed]
- Ivanovski M, Mrak M, Mežnar AZ, Žižek D. Biventricular versus Conduction System Pacing after Atrioventricular Node Ablation in Heart Failure Patients with Atrial Fibrillation. J Cardiovasc Dev Dis. 2022 Jul 1;9(7):209. [CrossRef] [PubMed]
- Vijayaraman P, Herweg B, Verma A, Sharma PS, Batul SA, Ponnusamy SS, Schaller RD, Cano O, Molina-Lerma M, Curila K, Huybrechts W, Wilson DR, Rademakers LM, Sreekumar P, Upadhyay G, Vernooy K, Subzposh FA, Huang W, Jastrzebski M, Ellenbogen KA. Rescue left bundle branch area pacing in coronary venous lead failure or nonresponse to biventricular pacing: Results from International LBBAP Collaborative Study Group. Heart Rhythm. 2022 Aug;19(8):1272-1280. [CrossRef] [PubMed]
- Chung MK, Patton KK, Lau CP, Dal Forno ARJ, Al-Khatib SM, Arora V, Birgersdotter-Green UM, Cha YM, Chung EH, Cronin EM, Curtis AB, Cygankiewicz I, Dandamudi G, Dubin AM, Ensch DP, Glotzer TV, Gold MR, Goldberger ZD, Gopinathannair R, Gorodeski EZ, Gutierrez A, Guzman JC, Huang W, Imrey PB, Indik JH, Karim S, Karpawich PP, Khaykin Y, Kiehl EL, Kron J, Kutyifa V, Link MS, Marine JE, Mullens W, Park SJ, Parkash R, Patete MF, Pathak RK, Perona CA, Rickard J, Schoenfeld MH, Seow SC, Shen WK, Shoda M, Singh JP, Slotwiner DJ, Sridhar ARM, Srivatsa UN, Stecker EC, Tanawuttiwat T, Tang WHW, Tapias CA, Tracy CM, Upadhyay GA, Varma N, Vernooy K, Vijayaraman P, Worsnick SA, Zareba W, Zeitler EP. 2023 HRS/APHRS/LAHRS guideline on cardiac physiologic pacing for the avoidance and mitigation of heart failure. Heart Rhythm. 2023 Sep;20(9):e17-e91. [CrossRef] [PubMed]
Figure 1.
Conventional BiVP-CRT using a quadripolar CS lead in a patient with ischaemic cardiomyopathy. Panel A shows the baseline QRS with LBBB; panel B shows the final paced QRS obtained with BiVP; panel C and D show the final lead position in the 30º LAO and RAO views, respectively. CS: coronary sinus; DF: defibrillation; LAO: left anterior oblique view; RAO: right anterior oblique view. ECG sweep speed 25 mm/s.
Figure 1.
Conventional BiVP-CRT using a quadripolar CS lead in a patient with ischaemic cardiomyopathy. Panel A shows the baseline QRS with LBBB; panel B shows the final paced QRS obtained with BiVP; panel C and D show the final lead position in the 30º LAO and RAO views, respectively. CS: coronary sinus; DF: defibrillation; LAO: left anterior oblique view; RAO: right anterior oblique view. ECG sweep speed 25 mm/s.
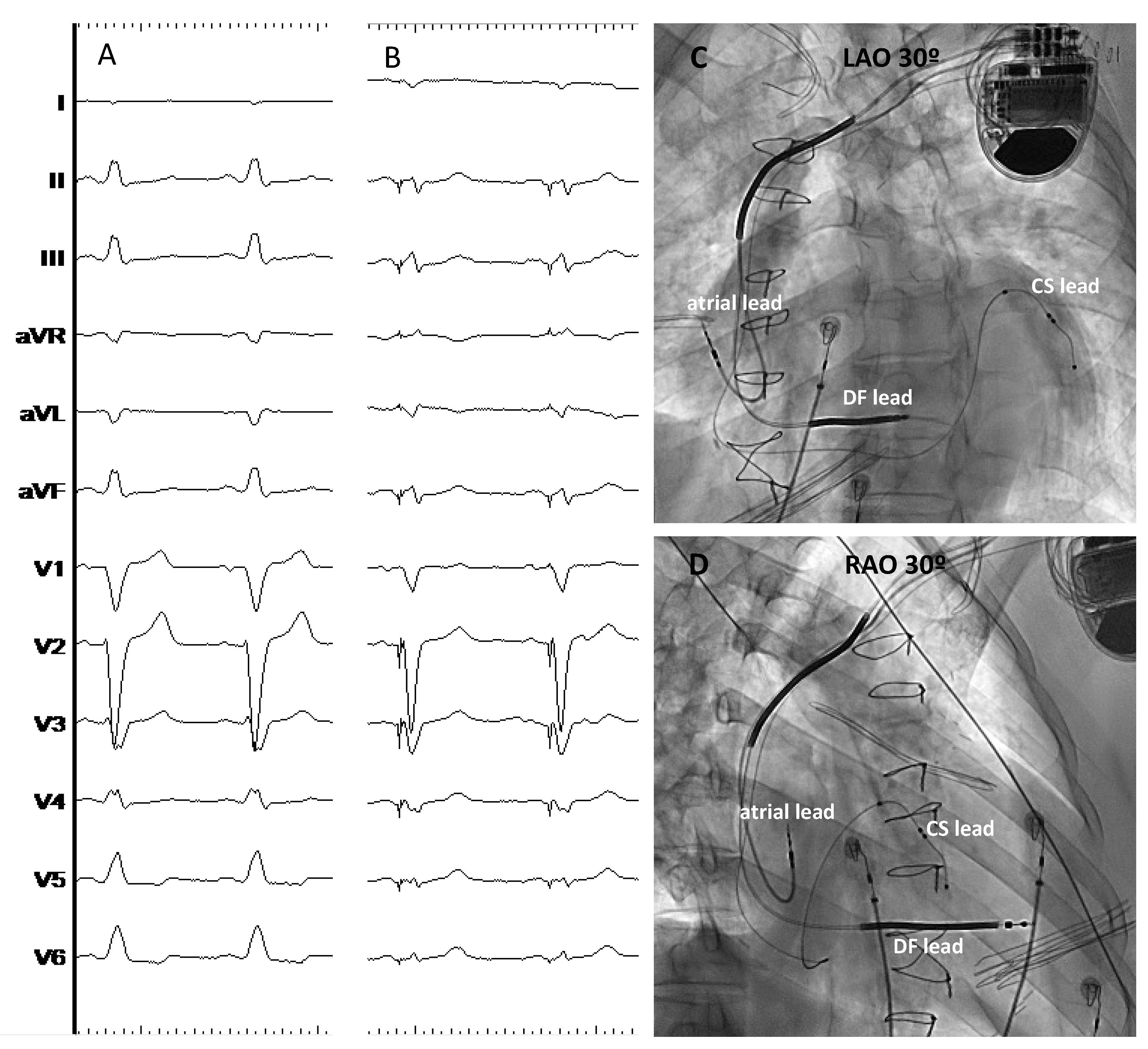
Figure 2.
Different capture patterns during HBP-CRT. On the left side of the figure a patient with baseline LBBB (panel A); HBP results in LBBB correction at high outputs (panel B), partial LBBB correction at intermediate output and selective HB capture but without LBBB correction at lower output (panel D). On the right side, a patient with baseline RBBB (panel E) shows complete RBBB correction at high output (panel F), partial correction at intermediate outputs (panel G) and selective HB capture without RBBB correction at lower outputs (panel H). HBED: His bundle electrogram (distal); HBEP: His bundle electrogram (proximal). Sweep speed 100 mm/s.
Figure 2.
Different capture patterns during HBP-CRT. On the left side of the figure a patient with baseline LBBB (panel A); HBP results in LBBB correction at high outputs (panel B), partial LBBB correction at intermediate output and selective HB capture but without LBBB correction at lower output (panel D). On the right side, a patient with baseline RBBB (panel E) shows complete RBBB correction at high output (panel F), partial correction at intermediate outputs (panel G) and selective HB capture without RBBB correction at lower outputs (panel H). HBED: His bundle electrogram (distal); HBEP: His bundle electrogram (proximal). Sweep speed 100 mm/s.
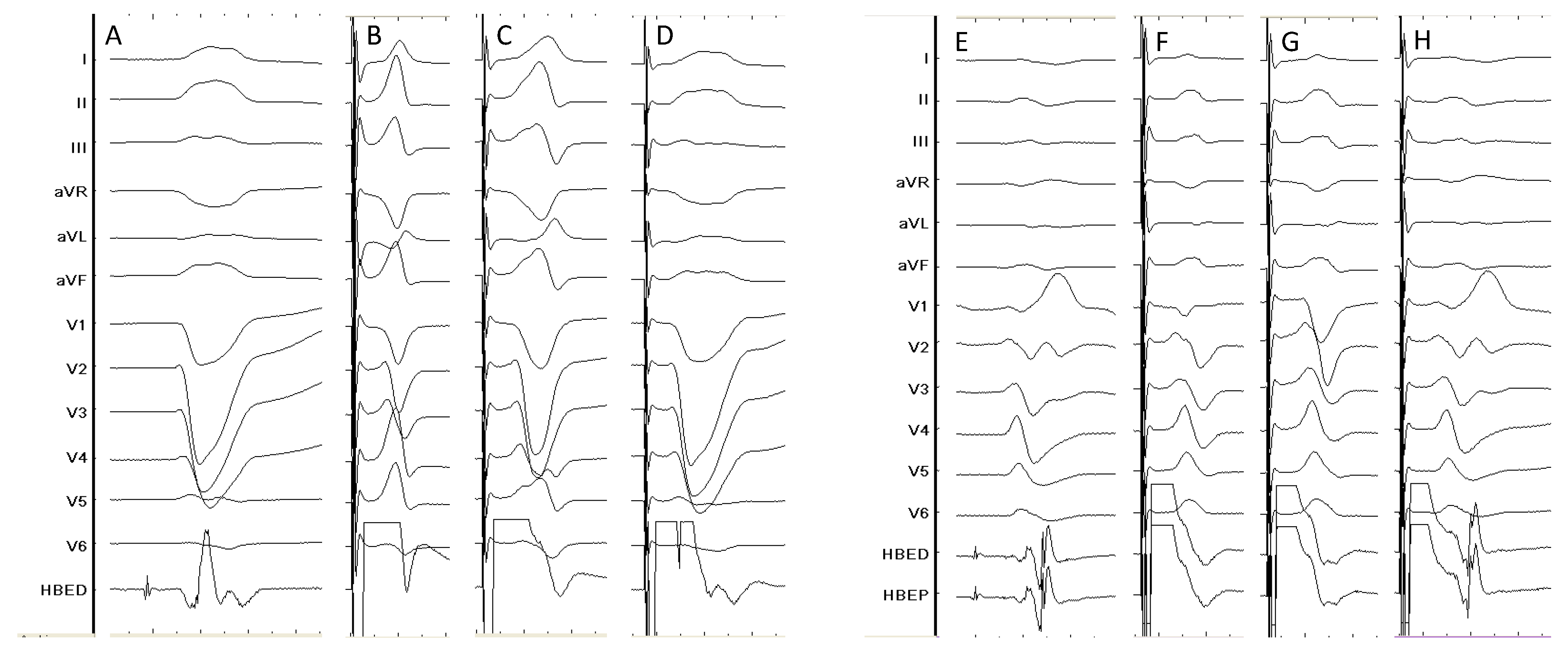
Figure 3.
Different capture patterns during LBBAP-CRT in a patient with non-ischaemic cardiomyopathy and baseline wide QRS (panel A). During the procedure LVSP (panel B), NS-LBBP and S-LBBP (D) could be observed during unipolar pacing at different outputs. Bipolar pacing with AV Interval adjusting to favor intrinsic conduction through the RBB resulted in further QRS narrowing (E). Panels F and G show the final lead position in the LAO (40º) and RAO (35º) projections, respectively. COI: current of injury; DF: defibrillation; LB: left bundle; LVSP: left ventricular septal pacing; NS-LBBP: non-selective left bundle branch pacing; S-LBBP: selective left bundle branch pacing. Sweep speed 100 mm/s.
Figure 3.
Different capture patterns during LBBAP-CRT in a patient with non-ischaemic cardiomyopathy and baseline wide QRS (panel A). During the procedure LVSP (panel B), NS-LBBP and S-LBBP (D) could be observed during unipolar pacing at different outputs. Bipolar pacing with AV Interval adjusting to favor intrinsic conduction through the RBB resulted in further QRS narrowing (E). Panels F and G show the final lead position in the LAO (40º) and RAO (35º) projections, respectively. COI: current of injury; DF: defibrillation; LB: left bundle; LVSP: left ventricular septal pacing; NS-LBBP: non-selective left bundle branch pacing; S-LBBP: selective left bundle branch pacing. Sweep speed 100 mm/s.

Figure 4.
Patient with dilated cardiomyopathy undergoing LBBAP-CRT. Panel A shows the baseline QRS (188 ms); panel B shows NS-LBBP and panel C shows S-LBBP; panel D shows the final paced QRS after adjusting the programmed AV delay in the device to allow intrinsic conduction through the intact patient’s RBB resulting in further QRS narrowing; panels E and F show the RAO and LAO 30º view of the final lead location; panel G shows a 4-chamber echocardiographic view with the LBBAP lead tip in the subendocardium of the left ventricular septum. COI: current of injury; DF: defibrillation; LAO: left anterior oblique view; LB: left bundle; LBBAP: left bundle branch area pacing; RAO: right anterior oblique view; RBB: right bundle branch. Sweep speed 100 mm/s.
Figure 4.
Patient with dilated cardiomyopathy undergoing LBBAP-CRT. Panel A shows the baseline QRS (188 ms); panel B shows NS-LBBP and panel C shows S-LBBP; panel D shows the final paced QRS after adjusting the programmed AV delay in the device to allow intrinsic conduction through the intact patient’s RBB resulting in further QRS narrowing; panels E and F show the RAO and LAO 30º view of the final lead location; panel G shows a 4-chamber echocardiographic view with the LBBAP lead tip in the subendocardium of the left ventricular septum. COI: current of injury; DF: defibrillation; LAO: left anterior oblique view; LB: left bundle; LBBAP: left bundle branch area pacing; RAO: right anterior oblique view; RBB: right bundle branch. Sweep speed 100 mm/s.
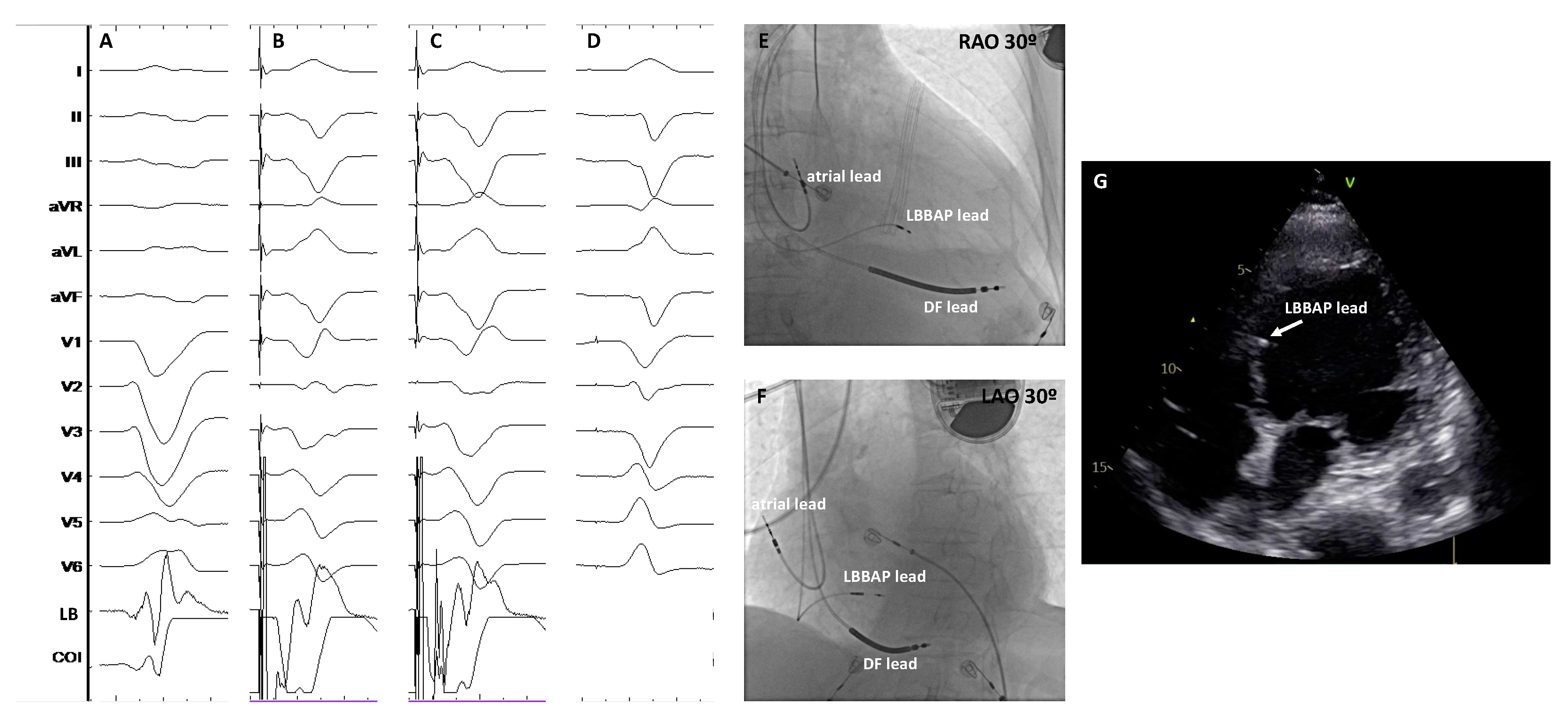
Figure 5.
Patient with non-ischaemic cardiomyopathy undergoing HOT-CRT. Baseline LBBB (panel A) could be only partially corrected with HBP (panel B). S-HBP without bundle branch correction could be seen at low outputs (panel C). Adding a CS lead and pacing from the His lead 20 ms earlier than from the CS lead, a further reduction in QRS duration could be obtained (panel E). Panel D shows the paced QRS morphology from the CS lead only. Panel F and G show the final lead locations in the LAO and RAO views, respectively. CS: coronary sinus; HBED: His bundle electrogram (distal). HOT-CRT: His-Optimized cardiac resynchronization therapy. Sweep speed 25 mm/s.
Figure 5.
Patient with non-ischaemic cardiomyopathy undergoing HOT-CRT. Baseline LBBB (panel A) could be only partially corrected with HBP (panel B). S-HBP without bundle branch correction could be seen at low outputs (panel C). Adding a CS lead and pacing from the His lead 20 ms earlier than from the CS lead, a further reduction in QRS duration could be obtained (panel E). Panel D shows the paced QRS morphology from the CS lead only. Panel F and G show the final lead locations in the LAO and RAO views, respectively. CS: coronary sinus; HBED: His bundle electrogram (distal). HOT-CRT: His-Optimized cardiac resynchronization therapy. Sweep speed 25 mm/s.
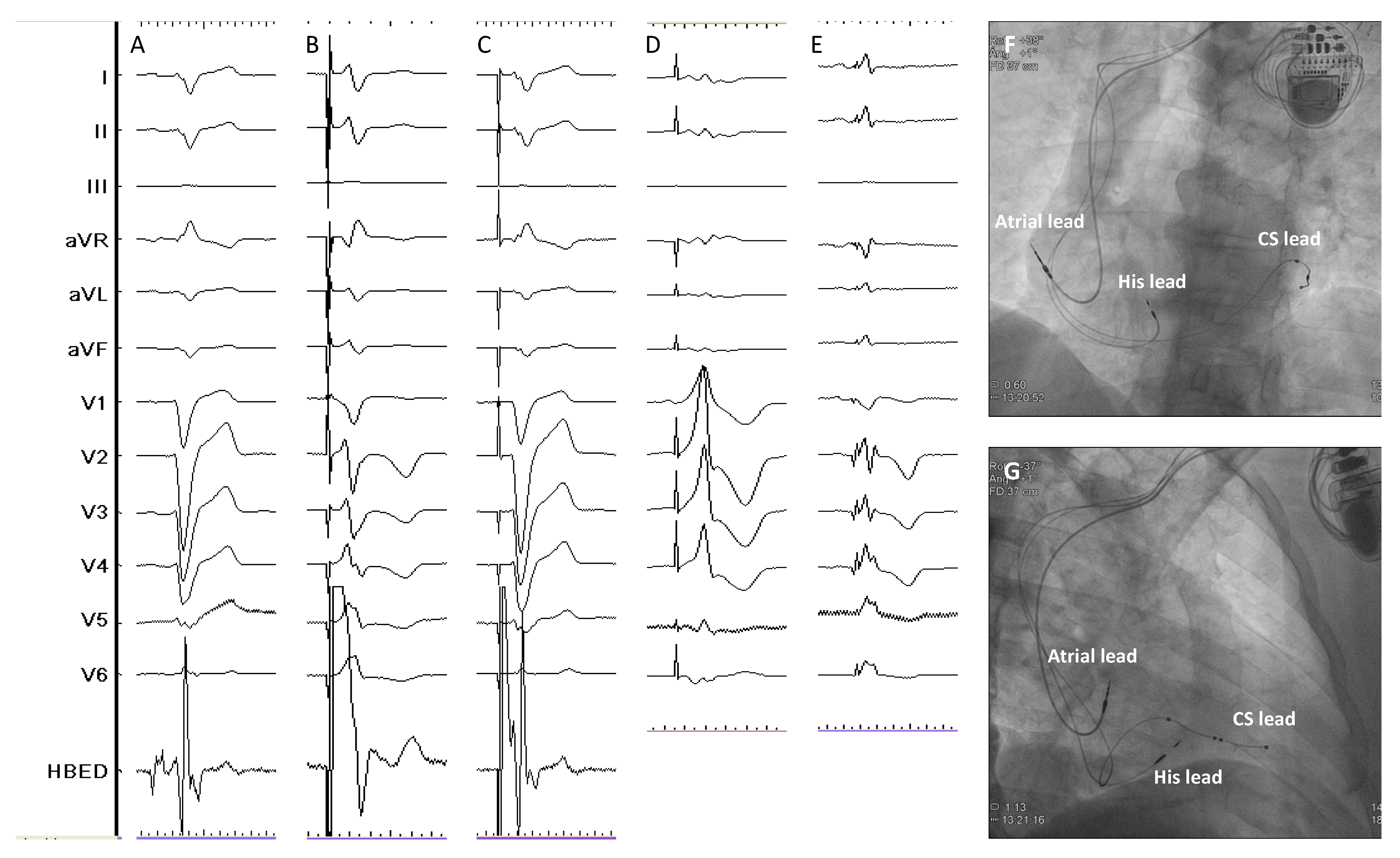
Figure 6.
Principal studies reporting data about BiVP-CRT, HBP-CRT and LBBAP-CRT with the total number of patients included. Asteriks indicate randomized studies.
Figure 6.
Principal studies reporting data about BiVP-CRT, HBP-CRT and LBBAP-CRT with the total number of patients included. Asteriks indicate randomized studies.
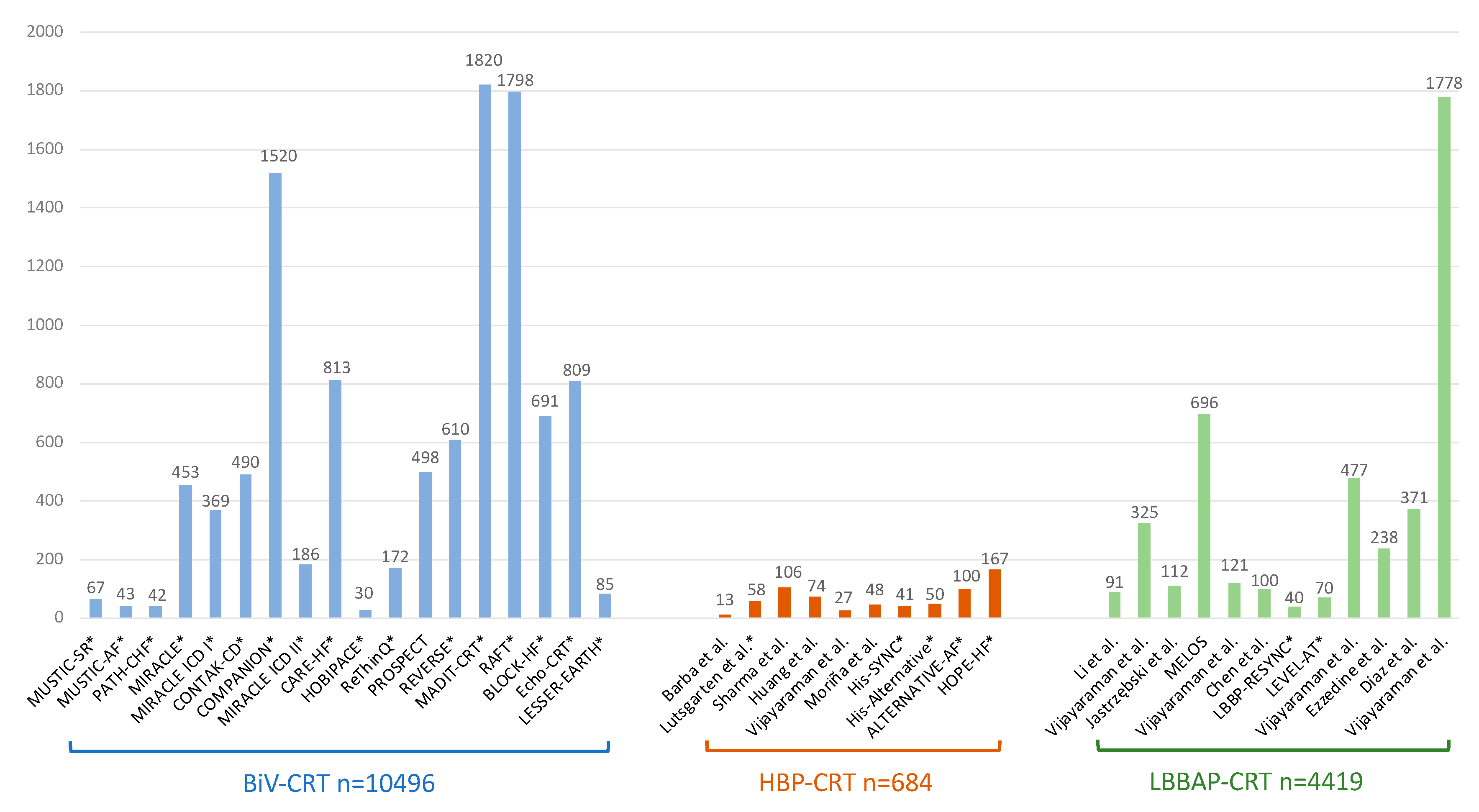

Table 1.
Principal studies reporting data about HBP-CRT.
| Study | Design | Patients’ allocation | BBB correction rate | HBP threshold at implant (V)* | HBP threshold at follow-up (V)* | Mean follow-up (months) | Outcomes# | HBP lead related complications (%)# |
|---|---|---|---|---|---|---|---|---|
| Barba et al.55 Europace, 2013 | observational, retrospective, single-centre |
HBP: 16 | 81% temporarily 56% permanently |
3.1 ± 0.4 | 3.7 ± 0.5 | 31 | QRS narrowing, LVEF improvement and reduction of LVEDD and LVESD | 0 |
| Lutsgarten et al.56 Heart Rhythm, 2015 | randomized, crossover, multicentre | HBP: 29 BiVP: 29 |
72% | 1.3 ± 2.2 | 2.4 ± 4.5 | 12 | LVEF, NYHA class, 6MWT and QoL significantly improved with both HBP and BiVP | 10.3 |
| Sharma et al.57 Heart Rhythm, 2018 | observational, retrospective, multicentre |
HBP: 106 | 90% | 1.4 ± 0.9 | 2.0 ± 1.2 | 14 | QRS narrowing, LVEF and NYHA class improvement | 6.6 |
| Huang et al.58 Heart, 2019 | observational, prospective, single-centre | HBP: 74 | 97% temporarily 76% permanently |
1.9 ± 1.1 | 2.3 ± 0.9 | 37 | QRS narrowing, LVEF and NYHA class improvement | 0 |
| Moriña-Vázquez et al.59 Europace, 2020 | observational, prospective, single-centre |
HBP: 48 | 81% | 1.6 (0.9-1.9) | 0.9 (0.7-2) | 6 | QRS narrowing, LVEF and dyssynchrony parameters improvement | 0 |
| Upadhyay et al.60 Heart Rhythm, 2019 | randomized, prospective, multicentre | HBP: 21 BiVP: 20 |
52% | 2.75 (1.3-3.4) | 2 (1-3.3) | 12 | QRS narrowing, trend towards higher echo response with HBP vs BiVP | 0 |
| Vinther et al.61 JACC EP, 2021 | randomized, prospective, single-centre | HBP: 25 BiVP: 25 |
72% | 2.2 ± 1.2 | 2.4 ± 1.6 | 6 | LVEF significantly higher and LVESV significantly lower in HBP group at 6 months | 5.3 |
| Huang et al.62 Heart Rhythm, 2022 |
randomized, prospective, multicentre, crossover |
HBP: 50 BiVP: 50 |
N/A, patients with baseline narrow QRS undergoing AV node ablation | 0.9 ± 0.6 | 0.9 ± 0.6b | 9 | significant improvement in LVEF with HBP vs BiVP | 0 |
| Whinnet et al.63 Eur J Heart Fail, 2023 | randomized, crossover, multicentre | HBP: 167 | 93% | N/A | N/A | 6 | HBP did not increased peak O2 uptake but significantly improved QoL | 5.6 |
* HBP threshold refers to the BBB correction threshold. Note that HB pacing thresholds were measured at different pulse widths depending on the study. #In randomized studies, outcomes and HBP lead related complications are reported as per-protocol analyses. BBB: bundle branch block; BiVP: biventricular pacing; HBP: His bundle pacing; LVEDD: left ventricular end-dyastolic diameter; LVEF: left ventricular ejection fraction; LVESD: left ventricular end-systolic diameter; LVESV: left ventricular end-systolic volume; NYHA: New York Heart Association; QoL: quality of life; 6MWT: 6-minutes walking test.
Table 2.
Principal studies reporting data on LBBAP-CRT.
| Study | Design | Patients’ allocation | Implant success rate | Pacing threshold at implant (V) | Pacing threshold at follow-up (V) | Mean follow-up (months) | Outcomes# | LBBAP/CS lead related complications (%)# |
|---|---|---|---|---|---|---|---|---|
| Li et al.64 ESC Heart Failure, 2020 | observational, prospective, multicentre | LBBAP: 37 BiVP: 54 |
LBBAP: 81% BiVP: N/A |
LBBAP: 0.81 ± 0.30a BiVP: 1.22 ± 0.62 |
LBBAP: 0.75 ± 0.31b BiVP: 1.43 ± 0.74 |
6 | narrower QRS, greater LVEF improvement, greater echocardiographic response and higher rate of super-responders with LBBAP vs BiVP | LBBAP: 0 BiVP: N/A |
| Vijayaraman et al.65 JACC EP, 2021 | observational, retrospective, multicentre | LBBAP: 325 | 85% | 0.6 ± 0.3 | 0.7 ± 0.3 | 6 | QRS narrowing, LVEF and NYHA class improvement | 2.5 |
| Jastrzębski et al.66 Eur Heart J, 2022 | observational, retrospective, multicentre | LBBAP: 696 | 82% | N/A | N/A | 6.4 | N/A | N/A |
| Chen X et al.67 Europace, 2022 | observational, prospective, multicentre | LBBAP: 49 BiVP: 51 |
LBBAP: 98% BiVP: 91% |
LBBAP: 0.92 ± 0.20 BiVP: 1.45 ± 0.39 |
LBBAP: 0.66 ± 0.17 BiVP: 1.42 ± 0.33 |
12 | narrower QRS, greater LVEF improvement and higher rate of super-responders with LBBAP vs BiVP | LBBAP: 0 BiVP: 1.8 |
| Wang Y et al.68 JACC EP, 2022 | randomized, prospective, multicentre | LBBAP: 20 BiVP: 20 |
LBBAP: 90% BiVP: 80% |
LBBAP: 0.69 ± 0.26 BiVP: 0.92 ± 0.40 |
LBBAP: 0.82 ± 0.20 BiVP: 1.12 ± 0.67 |
6 | higher LVEF improvement and greater reduction in LVESV and NT-proBNP with LBBAP | LBBAP: 0 BiVP: 5 |
| Pujol-López et al.69 JACC EP, 2022 | randomized, prospective, single-centre | LBBAP*: 35 BiVP: 35 |
LBBAP: 77% BiVP: 94% |
LBBAP: 1.0 ± 0.4 BiVP: 1.2 ± 0.5 |
LBBAP: 0.8 ± 0.4 BiVP: 1.0 ± 0.3 |
6 | similar decrease in LVAT and LVESV; similar rates of mortality and HF hospitalization | LBBAP: 0 BiVP: 5 |
| Vijayaraman et al.70 Heart Rhythm, 2022 | observational, retrospective, multicentre | HBP: 87 LBBAP: 171 BiVP: 219 |
CSP: 86% BiVP: 75% |
HBP: 1.1 ± 0.7 LBBAP: 0.8 ± 0.4 BiVP: 1.3 ± 0.6 |
HBP: 1.1 ± 0.7 LBBAP: 0.9 ± 0.5 BiVP: 1.4 ± 0.7 |
27 | greater improvement of LVEF with CS; combined outcome of death or HF hospitalization lower with CSP vs BiVP | HBP: 2.3 LBBAP: 0.6 BiBP: 0.5 |
| Ezzedine et al.71 Heart Rhythm, 2023 | observational, retrospective, multicentre | HBP: 69 LBBAP: 50 BiVP: 119 |
N/A | HBP: 1.29 ± 1 LBBAP: 0.92 ± 0.54 BiVP: N/A |
HBP: 1.46 ± 1.14 LBBAP: 0.86 ± 0.5 BiVP: N/A |
9 | greater proportion of CRT responders in CSP groups vs BiVP. No differences in overall survival or time to first HF hospitalization | HBP: 11.1 LBBAP: 2.1 BiVP: 2.5 |
| Díaz et al.72 JACC EP, 2023 | observational, prospective, multicentre | LBBAP: 128 BiVP: 243 |
LBBAP: 84.4% BiVP: 94.7% |
N/A | N/A | 11 | higher LVEF improvement with LBBAP; significant reduction of all-cause mortality or HF hospitalization with LBBAP | LBBAP: 7 BiVP: 6.2 |
| Vijayaraman et al.73 JACC, 2023 | observational, retrospective, multicentre | LBBAP: 797 BiVP: 981 |
N/A | LBBAP: 0.72 ± 0.4 BiVP: 1.15 ± 0.7 |
LBBAP: 0.74 ± 0.3 BiVP: 1.31 ± 0.7 |
33 | higher LVEF improvement with LBBAP and higher proportion of patients with NYHA class improvement; significant reduction of time to death or HF hospitalization with LBBAP | LBAP: 1.3 BiVP: 2.5 |
* this study included 4 patients with HBP-CRT. #In randomized studies, pacing thresholds, outcomes and HBP lead related complications are reported as per-protocol analyses. BBB: bundle branch block; BiVP: biventricular pacing; CS: coronary sinus; HBP: His bundle pacing; LBBAP: left bundle branch area pacing; LVEF: left ventricular ejection fraction; LVESV: left ventricular end-systolic volume; NYHA: New York Heart Association.
Table 3.
Comparison of procedural and follow-up outcomes with the different CRT techniques. Estimation of the effect of the different pacing modalities has been obtained from pooled from the references.
Table 3.
Comparison of procedural and follow-up outcomes with the different CRT techniques. Estimation of the effect of the different pacing modalities has been obtained from pooled from the references.
| BiVP-CRT | HBP-CRT | LBBAP-CRT | Ref. | |
|---|---|---|---|---|
| Procedural time | lower than HBP higher than LBBAP |
higher than BiVP higher than LBBAP |
lower than BiVP lower than HBP |
60,61,63, 65,68-70,72-73 |
| Fluoroscopy time | higher than HBP higher than LBBAP |
lower than BiVP comparable to LBBAP |
lower than BiVP comparable to HBP |
55,59,61,64,67-70,72,73 |
| Acute CS/CSP lead threshold | lower than HBP higher than LBBAP |
higher than BiVP higher than LBBAP | lower than BiVP lower than HBP |
55-62,64-65,67-71,73 |
| Acute haemodynamic effects | worst than HBP worst than LBBAP |
better than BiVP comparable to LBBAP |
better than BiVP comparable to HBP |
75 |
| Paced QRS duration | wider than HBP wider than LBBAP |
narrower than BiVP comparable to LBBAP |
narrower than BiVP comparable to HBP |
74-76 |
| Change in LVEF | lower than HBP lower than LBBAP |
greater than BiVP comparable to LBBAP |
greater than BiVP comparable to HBP |
74-76 |
| Follow-up CS/CSP lead threshold | lower than HBP higher than LBBAP |
higher than BiVP higher than LBBAP | lower than BiVP lower than HBP |
55-62,64-65,67-71,73 |
| CS/CSP lead-related complications | lower than HBP comparable to LBBAP |
higher than BiVP higher than LBBAP |
comparable to BiVP lower than HBP |
55-65,67-73 |
BiVP-CRT: biventricular pacing cardiac resynchronization therapy; CS: coronary sinus; CSP: conduction system pacing; HBP-CRT: His bundle pacing cardiac resynchronization therapy; LBBAP-CRT: left bundle branch area pacing cardiac resynchronization therapy; LVEF: left ventricular ejection fraction.
Table 4.
Current CRT recommendations from the 2021 ESC guideline on cardiac pacing and CRT and the 2023 HRS/APHRS/LAHRS guideline on cardiac physiologic pacing for the avoidance and mitigation of heart failure.
Table 4.
Current CRT recommendations from the 2021 ESC guideline on cardiac pacing and CRT and the 2023 HRS/APHRS/LAHRS guideline on cardiac physiologic pacing for the avoidance and mitigation of heart failure.
| Clinical scenarios | 2021 ESC Guideline on Cardiac Pacing and CRT1 | Clinical scenarios | 2023 HRS/APHRS/LAHRS Guideline on Cardiac Physiologic Pacing93 |
|---|---|---|---|
| HF, SR, LVEF ≤35%, LBBB, QRS ≥150 ms | BiVP-CRT (I-A) HBP if unsuccessful CS lead implantation (IIa-B) |
HF, LBBB, LVEF ≤30%, NYHA class I | BiVP-CRT (2b, B-R) |
| HF, SR, LVEF ≤35%, LBBB, QRS 130-149 ms | BiVP-CRT (IIa-B) HBP if unsuccessful CS lead implantation (IIa-B) |
HF, LBBB, QRS ≥150 ms, LVEF ≤35%, NYHA class II-IV | BiVP-CRT (1, A) HBP or LBBAP if BiVP-CRT cannot be achieved (2a, C-LD) |
| HF, SR, LVEF ≤35%, non-LBBB, QRS ≥150 ms | BiVP-CRT (IIa-B) HBP if unsuccessful CS lead implantation (IIa-B) |
HF, LBBB, QRS 120-149 ms, LVEF ≤35%, NYHA class II-IV | BiVP-CRT (1, A) if female sex BiVP-CRT (2a, B-R) for the rest |
| HF, SR, LVEF ≤35%, non-LBBB, QRS 130-149 ms | BiVP-CRT (IIb-B) HBP if unsuccessful CS lead implantation (IIa-B) |
HF, LBBB, QRS ≥150 ms, LVEF 36-50%, NYHA class II-IV | BiVP-CRT (2b, C-LD) HBP or LBBAP (2b, C-LD) |
| HF, AF, LVEF ≤35%, LBBB, QRS ≥130 ms, NYHA class III-IV | BiVP-CRT (IIa-C) HBP if unsuccessful CS lead implantation (IIa-B) |
HF, non-LBBB, LVEF ≤35%, QRS 120-149 ms, NYHA class III-IV | BiVP-CRT (2b, B-NR) HBP or LBBAP (2b, C-LD) |
| HF, LVEF ≤35%, previous PM/ICD with high VP burden | BiVP-CRT (IIa-B) HBP if unsuccessful CS lead implantation (IIa-B) |
HF, non-LBBB, LVEF ≤35%, QRS ≥150 ms, NYHA class II | BiVP-CRT (2b, B-R) HBP or LBBAP (2b, C-LD) |
| Symptomatic AF, LVEF<40% candidates for AVN ablation | BiVP-CRT (I-B) HBP if unsuccessful CS lead implantation (IIa-B) HBP (IIb-C) |
HF, non-LBBB, LVEF ≤35%, QRS ≥150 ms, NYHA class III-IV | BiVP-CRT (2a, A) HBP or LBBAP if BiVP-CRT cannot be achieved (2b, C-LD) |
| Symptomatic AF, LVEF 40-49% candidates for AVN ablation | BiVP-CRT (IIa-C) HBP if unsuccessful CS lead implantation (IIa-B) HBP (IIb-C) |
Pacemaker indication, LVEF 36-50% and anticipated high VP burden | BiVP-CRT (2a, B-R) HBP or LBBAP (2a, B-NR) |
| Symptomatic AF, LVEF ≥50% candidates for AVN ablation | BiVP-CRT (IIb-C) HBP if unsuccessful CS lead implantation (IIa-B) HBP (IIb-C) |
Pacemaker indication, LVEF 36-50%, LBBB and anticipated low VP burden | BiVP-CRT (2b, C-LD) HBP or LBBAP (2b, C-LD) |
| SR or AF, pacing indication for high degree AV block and LVEF<40% | BiVP-CRT (I-A) HBP if unsuccessful CS lead implantation (IIa-B) |
PICM with HF and high burden RVP | BiVP-CRT (1, B-NR) HBP or LBBAP (2b, C-LD) |
| AF + AVN ablation + LVEF ≤50% | BiVP-CRT (2a, B-R) |
AF: atrial fibrillation; AVN: atrioventricular node; BiVP-CRT: biventricular pacing cardiac resynchronization therapy; HBP: His bundle pacing; HF: heart failure: SR: sinus rhythm; LVEF: left ventricular ejection fraction; LBBAP: left bundle branch area pacing; LBBB: left bundle branch block; NYHA: New York Heart Association; PICM: pacemaker induced cardiomyopathy; RVP: right ventricular pacing; VP: ventricular pacing.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



