
Submitted:
11 September 2023
Posted:
14 September 2023
You are already at the latest version
Abstract
Titanium middle ear prostheses are widely used in surgical practice due to their acoustic properties. However, they present a significant drawback shared by all synthetic materials currently in use for middle ear reconstruction: they can be rejected by the organism of the host. In this study, we aim to review the current literature on titanium TORP and PORP extrusion and dislocation. Eighty-one articles were analysed after full article review based on the inclusion and exclusion criteria. The most common indication for reconstruction was chronic otitis media with cholesteatoma. The average extrusion or dislocation rate was 5.1%, ranging from 0 to 35%. The average improvement in air-bone gap was 12.3 dB (1.6 dB to 25.1 dB) and 13.7 (-0,5 dB to 22.7 dB) for PORP ad TORP groups, respectively. The data reported on this topic are highly variable, demonstrating the functional outcomes are difficult to predict in clinical practice. We believe the current limitations could be overcome with technological developments, including bioengineering research focused on promoting the prothesis adaptation to the ME environment.
Keywords:
middle ear
; ossicular replacement prosthesis
; titanium
; extrusion
; dislocation
; complication
; hearing
1. Introduction
The restoration of hearing conduction entwined within the eradication of middle ear (ME) pathologies represent an outstanding goal of modern otosurgery. Indeed, with the demands of today’s fast paced society based on communication and rapid interactions, adequate social hearing is essential. As is well known, hearing loss leads to communication difficulties and social isolation. In addition to this, effortful listening increases energy required for processing and comprehending the auditory signal, thus diverting cognitive resources from other mental tasks[1]. Historically, the disadvantages of monaural compared with binaural hearing have not been stressed in audiological debate. Otherwise, current literature agrees hearing rehabilitation involves restoration of binaural stimulation. Indeed, central auditory pathway combine and compare the raw information from the two cochleae addressing complex tasks such as sound localization and speech perception in demanding listening environments[2]. While, since the 1990s to date technologies which bypass the ME sound-conducting mechanism have spread onto the market[3],[4], ossiculoplasty and passive ME implants continue to be widely used and studied. Several materials and techniques have been adopted over the years for ossicular reconstruction, with varying degrees of success. When available, autologous material refashioned to provide customized interposition is the prime source of repair[5]. In the last three decades, many alloplastic materials have been tested as suitable ossicular replacements, such as metals, ceramics, and plastics. Depending upon the defects to be reconstructed, synthetic prostheses are distinguished between Partial Ossicular Replacement Prostheses (PORP), mounted upon the intact stapes, and Total Ossicular Replacement Prostheses (TORP) for cases with no stapes superstructure[6]. At the present time, titanium is widely used for its physical properties, being lightweight with high stiffness and allowing easy individual adaptation to anatomical variations. In current literature numerous studies focus on hearing outcomes with titanium prostheses, demonstrating the reliably of this material in restoring conduction mechanism[7]. On the other hand, the rate of complications to be expected represent a notable aspect in presurgical counselling, regarding which the reported data are often conflicting. We aim to review the existing literature about complications of titanium prostheses ossicular reconstruction, with particular regard to extrusion and dislocation, and to discuss the current clinical perspectives.
2. Materials and Methods
A search of the literature was performed in the PUBMED database. The strategy used was based on the “Preferred Reporting Items for Systematic Reviews and Meta-analyses” (PRISMA) guidelines. The research was conducted using the following keywords: “((TORP) OR (PORP) OR (ossicular replacement) OR (ossiculoplasty)) AND titanium”. The population of interest was patients who had undergone ossiculoplasty with titanium PORP or TORP. There was no limitation in age, sex, or follow-up periods. The studies also had to include data about complications, namely prosthesis extrusion or dislocation focusing on cases not related to recurrence of cholesteatoma. Only articles in English were included. Review articles, letters, editorials and case reports were omitted. Exclusion criteria also applied to animal research and cadaver studies. In the included articles we considered the postoperative improvement in air-bone gap (ABG) as a secondary outcome.
3. Results
A PRISMA flow chart illustrating both the search numbers and included studies is schematically presented in Figure 1. A total of 311 records ware identified. However, after excluding articles written in languages other than English, editorials, letters to editors, case reports, and reviews, 243 studies were considered. A preliminary selection was based on titles and abstracts: 127 papers were evaluated for full text review, of which 41 did not meet the inclusion criteria and 5 additional records were excluded because the full text was unavailable. 81 articles were included in the review and were further analysed. The selected articles covered 7269 subjects and 7366 ME implants, including 3638 PORP and 3728 TORP. The demographic characteristics are displayed in Table 1. In 6 studies the average age was less than 18 years. The most common indication for reconstruction was chronic otitis media with cholesteatoma (CCOM, 34,1%), followed by chronic otitis media without cholesteatoma (COM, 16,2%). The indication was generically expressed as chronic otitis media in 2300 cases. Surgical details and functional outcomes are shown in Table 2. The average improvement in ABG for PORP was 12.3 dB, ranging from 1.6 dB to 25.1 dB. The average change in ABG for TORP was 13.7 (range from -0,5 dB to 22.7 dB). The average extrusion or dislocation rate was 5.1% (reported in 62 articles) ranging from 0 to 35%. Considering the six articles in which the average age was less than 18 years, the extrusion or dislocation rate in this limited cohort was 13.7%. The onset of complications is mentioned in only 16 articles, ranging from 2 months to 8 years. Their treatment is cited in 32 articles, in all cases except one the management consisted of surgical revision. The mean follow-up time was less than or equal to 12 months in 30 studies, among which the 25.4% of complications were reported.
4. Discussion
Considering the cognitive and psychosocial impact of hearing loss, its treatment is mandatory not only to restore the auditory perceptual skills but also to ameliorate the central management of cognitive resources[86]. In recent years, the interaction between hearing and cognitive processes has been studied through pupillometry. Indeed, pupil dilation response has demonstrated to be an indicator of mental processing load during listening effort[87]. Hence, the rehabilitation of hearing loss seems to be mandatory for optimization of the limited cognitive resource. Ossiculoplasty is a well-established surgical procedure intended to auditory rehabilitation, however its practical use still today collides with some technical issues. The ideal ossiculoplasty prosthesis should ensure hearing restoration as well as being safe and stably integrated into surrounding tissues. Titanium has demonstrated to be a reliable material in term of easy surgical manipulation and functional hearing results[26]. In a recent meta-analysis Kortebein et al. reported a rate of 70.7% of PORP and 57.1% of TORP patients with a postoperative ABG less than 20 dB[7]. Moreover, it is safe during magnetic resonance imaging both at 1.5 and 3 tesla, which could be necessary for the depiction of recuring cholesteatoma[88]. However, it is not free of postoperative complications such as dislocation or extrusion. To our knowledge, this is the first work that specifically analyses the existing literature about titanium TORP and PORP extrusion and dislocation rates. Kortebein and colleagues in their review have addressed this issue. However, they focused on articles presenting at least one audiometric outcome, with a 12-months minimum follow up, thus limiting the available data about complications[7]. On the other hand, with the present work we would provide a comprehensive overview about this topic. It can be argued the exclusion of extrusion or dislocation caused by cholesteatoma from the analysis to be a limit. However, we consider the presence of cholesteatoma in an operated ear a complication itself. Therefore, the decision was taken to avoid a possible misleading factor, focusing on the intrinsic issues of titanium prostheses. Moreover, we considered the rate of extrusion and dislocation for combined PORPs and TORPs because only few articles report complications separated for the two cohorts. Our literature review has demonstrated that the reported extrusion and dislocation rates vary greatly in literature, ranging from 0 to 35%, distributed over variable follow-up time. Interestingly, the 25.4% of the overall complications occurred in studies with mean follow-up time less than or equal to 12 months. The evaluation focused on the 6 paediatric studies has disclosed an increased complication rate in this cohort (13.7%) when compared to overall results (5.5%). We can speculate, as suggested by Michael and colleagues, a possible explanation to be the higher frequency of Eustachian tube dysfunction and of air way inflammation in pediatric population relative to adults[27]. Notably, the exiguity of details about the circumstances in which complications have occurred hampers a proper correlation with possible influencing factors, such as ME pathologies, surgical procedures or staging of treatment. Consistently, very few studies reported the onset time, thus allowing a limited discussion about this topic. The only remark which deserves to be underlined is the considerable variability of these findings, ranging from 2 months to 8 years. The information about extrusions and dislocations treatment are limited, however we found a trend in favour of a surgical revision attempt. Unfortunately, the available data do not allow to trace any cases eventually managed with other rehabilitation strategies, such as the active ME prostheses. In addition, in our analysis we considered the preoperative and postoperative ABG as a secondary outcome, despite the presence of these data was not among inclusion criteria. Our findings are in agreement with those of Kortebein et al., who reported an ABG improvement of 12.1 and 16.7 dB after titanium PORP and TORP placement, respectively[7]. We disclosed a high variability in the average ABG improvement among the studies included in the present review. It should be noted the data presented in literature are widely heterogeneous and thus difficult to compare, with respect to titanium prostheses models, underlying ME diseases, surgical hands and techniques, and follow-up strategies. The average ABG improvement was 12.3 dB, ranging from 1.6 dB to 25.1 dB, for PORP group, and 13.7 dB, from -0,5 dB to 22.7 dB, for TORP group. The functional results depend on many factors including status of the ME environment and Eustachian tube disfunction. According to our review, the most common indication for ossicular reconstruction is represented by chronic otitis media. Indeed, recurrence or progression of the ME pathology can affect the outcomes of ossiculoplasty. Moreover, host tissues are reported to interact with the surface of the ME prosthesis inducing a foreign body inflammation with a possible consequential dislocation and extrusion, thus compromising the initial functional results[89]. We strongly believe these considerations should be integral part of preoperatory counselling. Furthermore, the patients should be aware titanium PORP and TORP, despite their satisfying audiologic results, present the technical limitations shared by all passive ME prostheses. Namely, they aim to restore a normal coupling between the tympanic membrane and the inner ear, thus allowing a non-reinforced transmission of incident sound waves.[90] In fact, they entail certain anatomical and functional prerequisites that limit their use to selected situations.[6] Currently, the active ME prostheses, as well as percutaneous or transcutaneous bone conduction implants, have been designed to overcome the abovementioned issues[6],[3]. Otherwise, these solutions imply higher costs and the discomfort of an external component. All in all, current technological developments place us on the horns of a dilemma: to shelve the experience of the titanium prostheses or strive to overcome their ME adaptability and functional limits, maybe with bioengineering tools?
5. Conclusions
Here, we present a comprehensive literature review focused on titanium TORP and PORP extrusion and dislocation. We believe the variability in the reported complication rates demonstrates the factors involved in determining the prostheses adaptability in ME are highly changeable and difficult to predict. We advocate further research that using current technology could overcome the existing limits of titanium ME PORP and TORP to exploit their advantage in clinical practice.
Author Contributions
Conceptualization, P.C.; Methodology, E.C, L.B. and P.C.; Validation, M.M. and F.F; Formal Analysis, P.C. and E.C..; Investigation, E.C. D.M., C.C., I.O., M.M. and L.C.; Data Curation, E.C., C.C., I.O., D.M., F.L. and F.F.; Writing – Original Draft Preparation, E.C.; Writing – Review & Editing, P.C.; Visualization, L.B.; Supervision, S.B and M.B.; Project Administration, P.C.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest
References
- Slade, K.; Plack, C.J.; Nuttall, H.E. The effects of age-related hearing loss on the brain and cognitive function. Trends Neurosci 2020, 43, 810–821. [Google Scholar] [CrossRef] [PubMed]
- Avan, P.; Giraudet, F.; Büki, B. Importance of binaural hearing. Audiol Neurootol 2015, 20 Suppl 1, 3–6. [Google Scholar] [CrossRef]
- Canzi, P.; Avato, I.; Beltrame, M.; Bianchin, G.; Perotti, M.; Tribi, L.; Gioia, B.; et al. Retrosigmoidal placement of an active transcutaneous bone conduction implant: surgical and audiological perspectives in a multicentre study. Acta Otorhinolaryngol Ital 2021, 41, 91–99. [Google Scholar] [CrossRef] [PubMed]
- Canzi, P.; Berrettini, S.; Albera, A.; Barbara, M.; Bruschini, L.; Canale, A.; Carlotto, E.; et al. Current trends on subtotal petrosectomy with cochlear implantation in recalcitrant chronic middle ear disorders. Acta Otorhinolaryngol Ital 2023, 43, S67–S75. [Google Scholar] [CrossRef] [PubMed]
- Potsangbam, D.S.; Akoijam, B.A. Endoscopic transcanal autologous cartilage ossiculoplasty. Indian J Otolaryngol Head Neck Surg 2019, 71, 54–59. [Google Scholar] [CrossRef] [PubMed]
- Beutner, D.; Hüttenbrink, K.B. Passive and active middle ear implants. GMS Curr Top Otorhinolaryngol Head Neck Surg 2009, 8, Doc09. [Google Scholar] [PubMed]
- Kortebein, S.; Russomando, A.C.; Greda, D.; Cooper, M.; Ledbetter, L.; Kaylie, D. Ossicular chain reconstruction with titanium prostheses: a systematic review and meta-analysis. Otol Neurotol 2023, 44, 107–114. [Google Scholar] [CrossRef]
- Wang, X.; Song, J.; Wang, H. Results of tympanoplasty with titanium prostheses. Otolaryngol Head Neck Surg 1999, 121, 606–609. [Google Scholar] [CrossRef]
- Dalchow, C.V.; Grün, D.; Stupp, H.F. Reconstruction of the ossicular chain with titanium implants. Otolaryngol Head Neck Surg 2001, 125, 628–630. [Google Scholar] [CrossRef]
- Krueger, W.W.; Feghali, J.G.; Shelton, C.; Green, J.D.; Beatty, C.W.; Wilson, D.F.; Thedinger, B.S.; Barrs, D.M.; McElveen, J.T. Preliminary ossiculoplasty results using the Kurz titanium prostheses. Otol Neurotol 2002, 23, 836–839. [Google Scholar] [CrossRef]
- Hillman, T.A.; Shelton, C. Ossicular chain reconstruction: titanium versus plastipore. Laryngoscope 2003, 113, 1731–1735. [Google Scholar] [CrossRef] [PubMed]
- Ho, S.Y.; Battista, R.A.; Wiet, R.J. Early results with titanium ossicular implants. Otol Neurotol 2003, 24, 149–152. [Google Scholar] [CrossRef]
- Neff, B.A.; Rizer, F.M.; Schuring, A.G.; Lippy, W.H. Tympano-ossiculoplasty utilizing the Spiggle and Theis titanium total ossicular replacement prosthesis. Laryngoscope 2003, 113, 1525–1529. [Google Scholar] [CrossRef] [PubMed]
- Neumann, A.; Schultz-Coulon, H.J.; Jahnke, K. Type III tympanoplasty applying the palisade cartilage technique: A study of 61 cases. Otol Neurotol 2003, 24, 33–37. [Google Scholar] [CrossRef]
- Fisch, U.; May, J.; Linder, T.; Naumann, I.C. A new L-shaped titanium prosthesis for total reconstruction of the ossicular chain. Otol Neurotol 2004, 25, 891–902. [Google Scholar] [CrossRef]
- Gardner, E.K.; Jackson, C.G.; Kaylie, D.M. Results with titanium ossicular reconstruction prostheses. Laryngoscope 2004, 114, 65–70. [Google Scholar] [CrossRef]
- Martin, A.D.; Harner, S.G. Ossicular reconstruction with titanium prosthesis. Laryngoscope 2004, 114, 61–64. [Google Scholar] [CrossRef]
- Menéndez-Colino, L.M.; Bernal-Sprekelsen, M.; Alobid, I.; Traserra-Coderch, J. Preliminary functional results of tympanoplasty with titanium prostheses. Otolaryngol Head Neck Surg 2004, 131, 17–19. [Google Scholar] [CrossRef]
- Lehnerdt, G.; Van Delden, A.; Lautermann, J. Management of an “Ear Camp” for children in Namibia. Int J Pediatr Otorhinolaryngol 2005, 69, 663–668. [Google Scholar] [CrossRef]
- De Vos, C.; Gersdorff, M.; Gérard, J.M. Prognostic factors in ossiculoplasty. Otol Neurotol 2006, 28, 61–67. [Google Scholar] [CrossRef]
- Vassbotn, F.S.; Møller, P.; Silvola, J. Short-term results using Kurz titanium ossicular implants. Eur Arch Otorhinolaryngol 2007, 264, 21–25. [Google Scholar] [CrossRef] [PubMed]
- Schmerber, S.; Troussier, J.; Dumas, G.; Lavieille, J.P.; Nguyen, D.Q. Hearing results with the titanium ossicular replacement prostheses. Eur Arch Otorhinolaryngol 2006, 263, 347–354. [Google Scholar] [CrossRef] [PubMed]
- Hales, N.W.; Shakir, F.A.; Saunders, J.E. Titanium middle ear prostheses in staged ossiculoplasty: does mass really matter? Am J Otolaryngol 2007, 28, 164–167. [Google Scholar] [CrossRef]
- Siddiq, M.A.; Raut, V.V. Early results of titanium ossiculoplasty using the Kurz titanium prosthesis - A UK perspective. J Laryngol Otol 2007, 121, 539–544. [Google Scholar] [CrossRef] [PubMed]
- Truy, E.; Naiman, A.N.; Pavillon, C.; Abedipour, D.; Lina-Granade, G.; Rabilloud, M. Hydroxyapatite versus titanium ossiculoplasty. Otol Neurotol 2007, 28, 492–498. [Google Scholar] [CrossRef]
- Coffey CS, Lee F, Lambert PR. Titanium versus nontitanium prostheses in ossiculoplasty. Laryngoscope 2008, 118, 1650–1658. [Google Scholar] [CrossRef]
- Michael, P.; Fong, J.; Raut, V. Kurz titanium prostheses in paediatric ossiculoplasty- short term results. Int J Pediatr Otorhinolaryngol 2008, 72, 1329–1333. [Google Scholar] [CrossRef]
- Redaelli De Zinis, L.O. Titanium vs hydroxyapatite ossiculoplasty in canal wall down mastoidectomy. Arch Otolaryngol Head Neck Surg 2008, 134, 1283–1287. [Google Scholar] [CrossRef]
- Alaani, A.; Raut, V.V. Alaani A, Raut V V. Kurz titanium prosthesis ossiculoplasty — Follow-up statistical analysis of factors affecting one year hearing results. Auris Nasus Larynx 2010, 37, 150–154. [Google Scholar] [CrossRef]
- Colletti, V.; Carner, M.; Colletti, L. TORP vs round window implant for hearing restoration of patients with extensive ossicular chain defect. Acta Otolaryngol 2009, 129, 449–452. [Google Scholar] [CrossRef]
- Roth, J.A.; Pandit, S.R.; Soma, M.; Kertesz, T.R. Ossicular chain reconstruction with a titanium prosthesis. J Laryngol Otol 2009, 123, 1082–1086. [Google Scholar] [CrossRef]
- Woods, O.; Fata, E.l.; Saliba, I. Ossicular reconstruction: incus versus universal titanium prosthesis. Auris Nasus Larynx 2009, 36, 387–392. [Google Scholar] [CrossRef] [PubMed]
- Fong, J.C.; Michael, P.; Raut, V. Titanium versus autograft ossiculoplasty. Acta Otolaryngol 2010, 130, 554–558. [Google Scholar] [CrossRef]
- Iñiguez-Cuadra, R.; Alobid, I.; Borés-Domenech, A.; Menéndez-Colino, L.M.; Caballero-Borrego, M.; Bernal-Sprekelsen, M. Type III tympanoplasty with titanium total ossicular replacement prosthesis: anatomic and functional results. Otol Neurotol 2010, 31, 409–414. [Google Scholar] [CrossRef] [PubMed]
- Luers, J.C.; Huttenbrink, K.B.; Mickenhagen, A.; Beutner, D. A modified prosthesis head for middle ear titanium implants- experimental and first clinical results. Otol Neurotol 2010, 31, 624–629. [Google Scholar] [CrossRef]
- Praetorius, M.; Kirchenbauer, S.S.; Buss, S.; Klingmann, C.; Plinkert, P.K.; Baumann, I. First experiences with a new adjustable length titanium ossicular prosthesis (ALTO). Acta Otolaryngol 2010, 130, 1237–1241. [Google Scholar] [CrossRef] [PubMed]
- Quesnel, S.; Teissier, N.; Viala, P.; Couloigner, V.; Van Den Abbeele, T. Long term results of ossiculoplasties with partial and total titanium Vario Kurz prostheses in children. Int J Pediatr Otorhinolaryngol 2010, 74, 1226–1229. [Google Scholar] [CrossRef] [PubMed]
- Yung, M.; Smith, P. Titanium versus nontitanium ossicular prostheses-a randomized controlled study of the medium-term outcome. Otol Neurotol 2010, 31, 752–758. [Google Scholar] [CrossRef]
- Babighian, G.; Albu, S. Stabilising total ossicular replacement prosthesis for ossiculoplasty with an absent malleus in canal wall down tympanomastoidectomy - a randomised controlled study. Clin Otolaryngol 2011, 36, 543–549. [Google Scholar] [CrossRef]
- Mardassi, A.; Deveze, A.; Sanjuan, M.; Mancini, J.; Parikh, B.; Elbedeiwy, A.; Magnan, J.; Lavieille, J.P. Titanium ossicular chain replacement prostheses: prognostic factors and preliminary functional results. Eur Ann Otorhinolaryngol Head Neck Dis 2011, 128, 53–58. [Google Scholar] [CrossRef]
- Nevoux, J.; Moya-Plana, A.; Chauvin, P.; Denoyelle, F.; Garabedian, E.N. Total ossiculoplasty in children: predictive factors and long-term follow-up. Arch Otolaryngol Head Neck Surg 2011, 137, 1240–1246. [Google Scholar] [CrossRef] [PubMed]
- Berenholz, L.P.; Burkey, J.M.; Lippy, W.H. Short- and long-term results of ossicular reconstruction using partial and total plastipore prostheses. Otol Neurotol 2013, 34, 884–889. [Google Scholar] [CrossRef]
- Gostian, A.O.; Pazen, D.; Luers, J.C.; Huttenbrink, K.B.; Beutner, D. Titanium ball joint total ossicular replacement prosthesis - Experimental evaluation and midterm clinical results. Hear Res 2013, 301, 100–104. [Google Scholar] [CrossRef] [PubMed]
- Hess-Erga, J.; Møller, P.; Vassbotn, F.S. Long-term hearing result using Kurz titanium ossicular implants. Eur Arch Oto-Rhino-Laryngology 2013, 270, 1817–1821. [Google Scholar] [CrossRef]
- Meulemans, J.; Wuyts, F.L.; Forton, G.E. Middle ear reconstruction using the titanium Kurz Variac partial ossicular replacement prosthesis: functional results. JAMA Otolaryngol Head Neck Surg 2013, 139, 1017–1025. [Google Scholar] [CrossRef]
- Shah, K.D.; Bradoo, R.A.; Joshi, A.A.; Sapkale, D.D. The efficiency of titanium middle ear prosthesis in ossicular chain reconstruction: our experience. Indian J Otolaryngol Head Neck Surg 2013, 65, 298–301. [Google Scholar] [CrossRef] [PubMed]
- Birk, S.; Brase, C.; Hornung, J. Experience with the use of a partial ossicular replacement prosthesis with a ball-and-socket joint between the plate and the shaft. Otol Neurotol 2014, 35, 1248–1250. [Google Scholar] [CrossRef] [PubMed]
- Fayad, J.N.; Ursick, J.; Brackmann, D.E.; Friedman, R.A. Total ossiculoplasty: short- and long- term results using a titanium prosthesis with footplate shoe. Otol Neurotol 2014, 35, 108–113. [Google Scholar] [CrossRef]
- Órfão, T.; Júlio, S.; Ramos, J.F.; Dias, C.C.; Silveira, H.; Santos, M. Audiometric outcome comparison between titanium prosthesis and molded autologous material. Otolaryngol Head Neck Surg 2014, 151, 315–320. [Google Scholar] [CrossRef]
- Pringle, M.B.; Sunkaraneni, V.S.; Tann, N. Is cartilage interposition required for ossiculoplasty with titanium prostheses? Otol Neurotol 2014, 35, 482–488. [Google Scholar] [CrossRef]
- Baker, A.B.; O’Connell, B.P.; Nguyen, S.A.; Lambert, P.R. Ossiculoplasty with titanium prostheses in patients with intact stapes: comparison of TORP versus PORP. Otol Neurotol 2015, 36, 1676–1682. [Google Scholar] [CrossRef]
- Boleas-Aguirre, M.S.; Ruiz de Erenchun-Lasa, I.; Bulnes-Plano, M.D. Audiological results after total ossicular reconstruction for stapes fixation. Eur Arch Otorhinolaryngol 2015, 272, 3123–3130. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.I.; Yoo, S.H.; Lee, C.W.; Song, C.l.; Yoo, M.H.; Park, H.J. Short-term hearing results using ossicular replacement prostheses of hydroxyapatite versus titanium. Eur Arch Otorhinolaryngol 2015, 272, 2731–2735. [Google Scholar] [CrossRef] [PubMed]
- Ocak, E.; Beton, S.; Meço, C.; Dursun, G. Titanium versus Hydroxyapatite prostheses: comparison of hearing and anatomical outcomes after ossicular chain reconstruction. Turk Arch Otorhinolaryngol 2015, 53, 15–18. [Google Scholar] [CrossRef]
- Roux, A.; Bakhos, D.; Villeneuve, A.; Hermann, R.; Suy, P.; Lescanne, E.; Truy, E. Does checking the placement of ossicular prostheses via the posterior tympanotomy improve hearing results after cholesteatoma surgery? Otol Neurotol 2015, 36, 1499–1503. [Google Scholar] [CrossRef]
- Wolter, N.E.; Holler, T.; Cushing, S.L.; Chadha, N.K.; Gordon, K.A.; James, A.L.; Papsin, B.C. Pediatric ossiculoplasty with titanium total ossicular replacement prosthesis. Laryngoscope 2015, 125, 740–745. [Google Scholar] [CrossRef]
- Faramarzi M, Jahangiri R, Roosta S. Comparison of Titanium vs. Polycel total ossicular replacement prosthesis. Iran J Otorhinolaryngol. 2016, 28(2), 89–97.
- Gostian, A.O.; Kouame, J.M.; Bremke, M.; Ortmann, M.; Hüttenbrink, K.B.; Beutner, D. Long term results of the titanium clip prosthesis. Eur Arch Otorhinolaryngol 2016, 273, 4257–4266. [Google Scholar] [CrossRef] [PubMed]
- Gostian, A.O.; Kouamé, J.M.; Bremke, M.; Ortmann, M.; Hüttenbrink, K.B.; Beutner, D. Long-term results of the cartilage shoe technique to anchor a titanium total ossicular replacement prosthesis on the stapes footplate after type III tympanoplasty. JAMA Otolaryngol Head Neck Surg 2016, 142, 1094–1099. [Google Scholar] [CrossRef]
- O’Connell, B.P.; Rizk, H.G.; Hutchinson, T.; Nguyen, S.A.; Lambert, P.R. Long-term outcomes of titanium ossiculoplasty in chronic otitis media. Otolaryngol Head Neck Surg 2016, 154, 1084–1092. [Google Scholar] [CrossRef]
- Amith N, RS M. Autologous incus versus titanium partial ossicular replacement prosthesis in reconstruction of Austin type A ossicular defects: A prospective randomised clinical trial. J Laryngol Otol 2017, 131, 391–398. [Google Scholar] [CrossRef] [PubMed]
- Govil, N.; Kaffenberger, T.M.; Shaffer, A.D.; Chi, D.H. Factors influencing hearing outcomes in pediatric patients undergoing ossicular chain reconstruction. Int J Pediatr Otorhinolaryngol 2017, 99, 60–65. [Google Scholar] [CrossRef] [PubMed]
- McMullen, K.P.; Harris, M.S.; Dodson, E.E. Use of 2-Octyl cyanoacrylate in cartilage Interposition adherence during ossiculoplasty. Laryngoscope 2017, 127, 731–734. [Google Scholar] [CrossRef]
- Mulazimoglu, S.; Saxby, A.; Schlegel, C.; Linder, T. Titanium incus interposition ossiculoplasty: audiological outcomes and extrusion rates. Eur Arch Otorhinolaryngol 2017, 274, 3303–3310. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.S.; Shin, S.O. Results of hearing outcome according to the alloplastic ossicular prosthesis materials. Indian J Otolaryngol Head Neck Surg 2018, 70, 184–187. [Google Scholar] [CrossRef] [PubMed]
- Kahue, C.N.; O’Connnell, B.P.; Dedmon, M.M.; Haynes, D.S.; Rivas, A. Short and Long-Term Outcomes of Titanium Clip Ossiculoplasty. Otol Neurotol 2018, 39, e453–e460. [Google Scholar] [CrossRef]
- Kong, J.; Jeong, C.; Shim, M.; Kim, W.; Yeo, S.; Park, S. Comparative study of new autologous material, bone-cartilage composite graft, for ossiculoplasty with Polycel® and Titanium. Clin Otolaryngol 2018, 43, 434–439. [Google Scholar] [CrossRef]
- Kumar, S.; Yadav, K.; Ojha, T.; Sharma, A.; Singhal, A.; Gakhar, S. To evaluate and compare the result of ossiculoplasty using different types of graft materials and prosthesis in cases of ossicular discontinuity in chronic suppurative otitis media cases. Indian J Otolaryngol Head Neck Surg 2018, 70, 15–21. [Google Scholar] [CrossRef]
- Lahlou, G.; Sonji, G.; De Seta, D.; Mosnier, I.; Russo, F.Y.; Sterkers, O.; Bernardeschi, D. Anatomical and functional results of ossiculoplasty using titanium prosthesis. Acta Otorhinolaryngol Ital 2018, 38, 377–383. [Google Scholar] [CrossRef]
- Saliba I, Sabbah V, Poirier JB. Total ossicular replacement prosthesis: a new fat interposition technique. Clin Med Insights Ear Nose Throat 2018, 11, 117955061774961. [Google Scholar] [CrossRef]
- Gu, F.M.; Chi, F.L. Titanium ossicular chain reconstruction in single stage canal wall down tympanoplasty for chronic otitis media with mucosa defect. Am J Otolaryngol 2019, 40, 205–208. [Google Scholar] [CrossRef] [PubMed]
- Haidar, H; Abu Rajab Altamimi, Z. ; Larem, A.; Aslam, W.; Elsaadi, A.; Abdulkarim, H.; Al Duhirat, E.; et al. The benefit of trans-attic endoscopic control of ossicular prosthesis after cholesteatoma surgery. Laryngoscope 2019, 129, 2754–2759. [Google Scholar] [CrossRef]
- Wood, C.B. , Yawn, R.; Lowery, A.S.; O’Connell, B.P.; Haynes, D.; Wanna, G.B. Long-term hearing outcomes following total ossicular reconstruction with titanium prostheses. Otolaryngol Head Neck Surg 2019, 161, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Mantsopoulos, K.; Thimsen. V.; Taha, L.; Eisenhut, F.; Müller, S.K.; Sievert, M.; Iro, H.; Hornung, J. Comparative analysis of titanium clip prostheses for partial ossiculoplasty. Am J Otolaryngol 2021, 42, 103062. [Google Scholar] [CrossRef] [PubMed]
- Baazil AHA, Ebbens FA, Van Spronsen E, De Wolf MJF, Dikkers FG. Comparison of long-term microscopic and endoscopic audiologic results after total ossicular replacement prosthesis surgery. Otol Neurotol 2022, 43, 1189–1195. [Google Scholar] [CrossRef]
- Bahmad F, Perdigão AG. Titanium prostheses versus stapes columella type 3 tympanoplasty: a comparative prospective study. Braz J Otorhinolaryngol 2022, 88, 562–569. [Google Scholar] [CrossRef]
- Kraus, E.M.; Russell, G.B.; Allen, S.J.; Pearson, S.A. Long-term hearing results of endoskeletal ossicular reconstruction in chronic ears using titanium prostheses having a helical coil: Part 1 - Kraus K-Helix Crown, incus to stapes. Otol Neurotol 2022, 43, 1056–1064. [Google Scholar] [CrossRef]
- Park, S.; Lim, K.H.; Lim, S.J.; Park, D.H.; Rah, Y.C.; Choi, J. Functional outcomes of single-stage ossiculoplasty in chronic otitis media with or without cholesteatoma. J Int Adv Otol 2022, 18, 415–419. [Google Scholar] [CrossRef]
- Plichta, L.; Dabkowska, A.; Wawszczyk-Frohlich, S.; Skarzynski, H.; Skarzynski, P.H. Titanium prostheses for treating posttraumatic ossicular chain disruption. J Int Adv Otol 2022, 18, 411–414. [Google Scholar] [CrossRef]
- Van Hoolst, A.; Wuyts, F.L.; Forton, G.E.J. Total ossicular chain reconstruction using a titanium prosthesis: functional results. Eur Arch Otorhinolaryngol 2022, 279, 5615–5621. [Google Scholar] [CrossRef]
- Chien, C.; Tai, S.; Chan, L.P.; Wang, H.M.; Chang, N.C.; Wang, L.F.; Ho, K.Y.; Li, K.H. Predictive factors and audiometric outcome comparison between titanium prosthesis and autologous incus in traumatic ossicular injury. Ann Otol Rhinol Laryngol 2023, 34894231181746, Epub ahead of print. [Google Scholar] [CrossRef]
- Faramarzi, M.; Roosta, S.; Faramarzi, A.; Kherad, M. Comparison of partial vs. total ossicular chain reconstruction using titanium prosthesis: a retrospective cohort study. Eur Arch Otorhinolaryngol 2023, 280, 3567–3575. [Google Scholar] [CrossRef] [PubMed]
- Gülşen S, Çıkrıkcı S. A novel technique in treatment of advanced tympanosclerosis: results of malleus replacement and loop prostheses combination; pure endoscopic transcanal approach. Eur Arch Otorhinolaryngol 2023, 280, 3601–3608. [Google Scholar] [CrossRef] [PubMed]
- Kálmán, J.; Horváth, T.; Dános, K.; Tamás, L.; Polony, G. Primary ossiculoplasties provide better hearing results than revisions: a retrospective cohort study. Eur Arch Otorhinolaryngol 2023, 280, 3177–3185. [Google Scholar] [CrossRef]
- Kim, H.; Ha, J.; Choo, O.S.; Park, H.; Choung, Y.H. Which is better for ossiculoplasty following tympanomastoidectomy: Polycel® or Titanium? Ann Otol Rhinol Laryngol 2023, 23, 34894231159969, Epub ahead of print. [Google Scholar] [CrossRef]
- Castiglione, A.; Benatti, A.; Velardita, C.; Favaro, D.; Padoan, E.; Severi, D.; Pagliaro, M.; et al. Aging, cognitive decline and hearing loss: effects of auditory rehabilitation and training with hearing aids and cochlear implants on cognitive function and depression among older adults. Audiol Neurootol 2016, 21 Suppl 1, 21–28. [Google Scholar] [CrossRef]
- Bönitz, H.; Lunner, T.; Finke, M.; Fiedler, L.; Lyxell, B.; Riis, S.K.; Ng, E.; et al. How do we allocate our resources when listening and memorizing speech in noise? A pupillometry study. Ear Hear 2021, 42, 846–859. [Google Scholar] [CrossRef]
- Martin, A.D.; Driscoll, C.L.W.; Wood, C.P.; Felmlee, J.P. Safety evaluation of titanium middle ear prostheses at 3.0 tesla. Otolaryngol Head Neck Surg 2005, 132, 537–542. [Google Scholar] [CrossRef]
- Danti, S.; Stefanini, C.; D’Alessandro, D.; Moscato, S.; Pietrabissa, A.; Petrini, M.; Berrettini, S. Novel biological/biohybrid prostheses for the ossicular chain: fabrication feasibility and preliminary functional characterization. Biomed Microdevices 2009, 11, 783–793. [Google Scholar] [CrossRef]
- Sanna, M.; Hiroshi, S.; Mancini, F.; Russo, A.; Taibah, A.; Falcioni, M. Middle ear and mastoid microsurgery; Thieme: Stuttgart, Germany, 2018; pp. 187–244. [Google Scholar]
Figure 1.
PRISMA 2020 based flow-diagram showing review search.
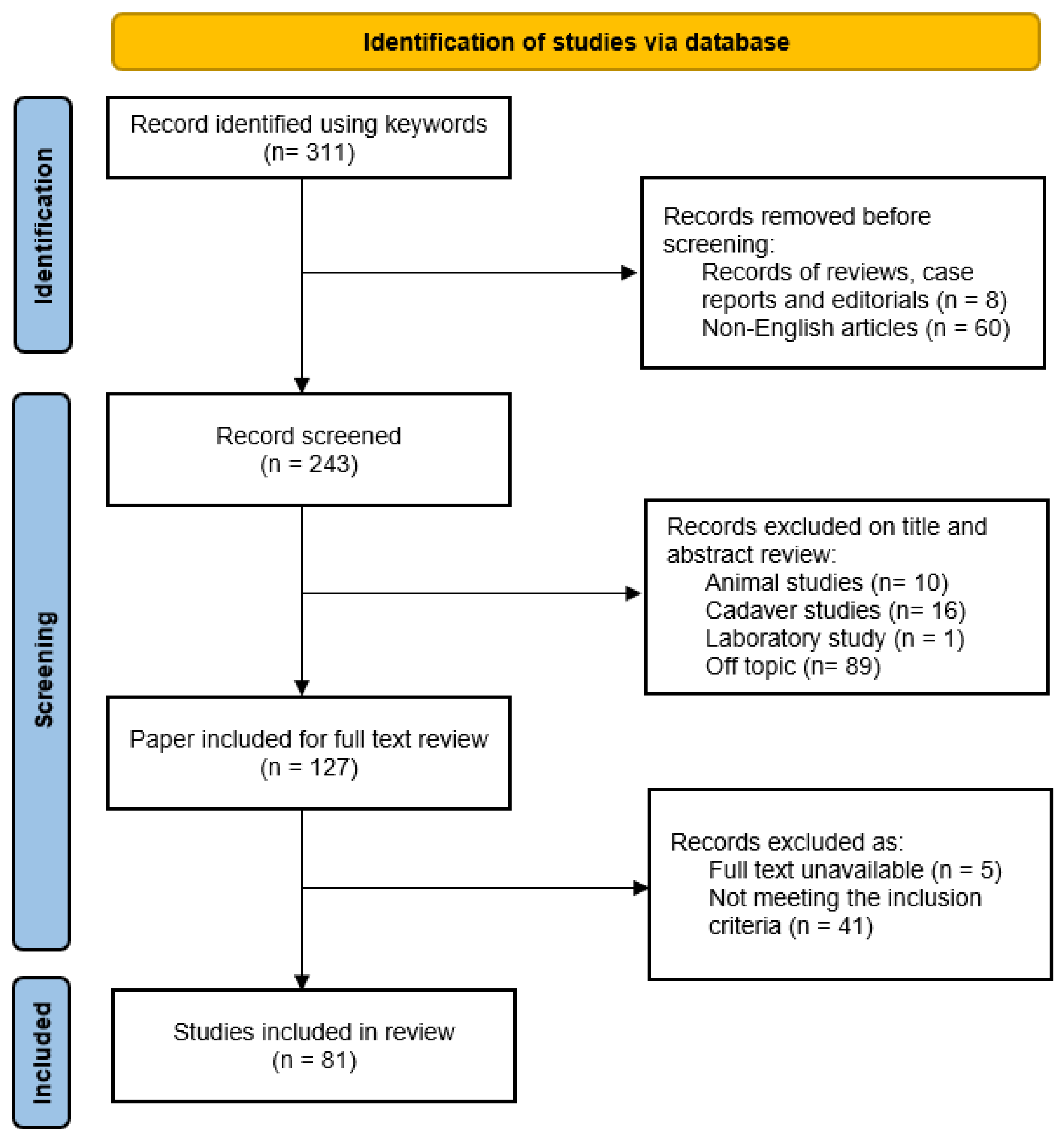

Table 1.
Demographics and clinical data.
| Authors, year | Pts | Ears | PORP | TORP | Age at surgery (range) | Middle ear disorder |
|---|---|---|---|---|---|---|
| Wang et al. 1999[8] | 113 | 124 | 86 | 38 | n.a. | 59 CCOM, 54 COM, 2 CA, 9 TS |
| Dalchow et al. 2001[9] | 1304 | 1304 | 647 | 657 | 5- 82y | 1304 COM + CCOM |
| Krueger et al. 2002[10] | 31 | 31 | 16 | 15 | n.a. | 31 CCOM + COM |
| Hillman and Shelton. 2003[11] | 53 | 53 | 30 | 23 | 34.8y | n.a. |
| Ho et al. 2003[12] | 25 | 25 | 14 | 11 | 45y (14–74) | 15 CCOM, 6 COM, 4 CA |
| Neff et al. 2003[13] | 18 | 18 | 0 | 18 | 37y (8 - 80) | 11 CCOM, 7 COM+TS |
| Neumann et al. 2003[14] | 59 | 61 | 27 | 34 | 36y (7-81) | 32 CCOM, 11 COM, 16 AT, 2 TS |
| Fisch et al. 2004[15] | 46 | 46 | 0 | 46 | 44.8y (22-65) | 19 CCOM, 20 COM, 7 CA + TR |
| Gardner et al. 2004[16] | 149 | 149 | 111 | 38 | 32.5 y (3-75) | 77 CCOM, 40 COM, 32 n.a. |
| Martin et al. 2004[17] | 68 | 68 | 30 | 38 | 39y (6-74) | 68 CCOM+ COM |
| Menéndez-Colino et al. 2004[18] | 23 | 23 | 0 | 23 | 37y (8-65) | 17 CCOM, 3 COM, 1 AT, 2 CA |
| Lehnerdt et al. 2005[19] | 15 | 15 | 14 | 1 | 12y (n.a.) | 15 CCOM + COM |
| De Vos et al. 2006[20] | 129 | 140 | 65 | 75 | 37y (3-73) | 72 CCOM, 12 COM, 17 AT, 16 TS, 23 n.a. |
| Vassbotn et al. 2006[21] | 71 | 73 | 38 | 35 | 31.5 y | 40 CCOM, 4 COM. 29 CA |
| Schmerber et al. 2006[22] | 111 | 111 | 61 | 50 | 38.4 y (7 – 76) | 82 CCOM, 16 COM, 4 AT, 5 CA, 1 OTO, 3 TR |
| Hales et al. 2007[23] | 34 | 34 | 24 | 10 | 26y (4-59) | 29 CCOM, 5 n.a. |
| Siddiq and Raut. 2007[24] | 33 | 33 | 20 | 13 | 35.9 y (7 - 64) | 15 CCOM, 18 COM |
| Truy et al. 2007[25] | 62 | 62 | 27 | 35 | 37.5y (n.a.) | 38 CCOM, 24 n.a. |
| Coffey et al. 2008[26] | 80 | 80 | 29 | 51 | 28.8y (n.a.) | 35 CCOM, 36 COM, 3 CA, 4 OTO, 2 TR |
| Michael et al. 2008[27] | 14 | 14 | 9 | 5 | 11y (7-14) | 6 CCOM, 4 COM, 3 AT, 1 n.a. |
| Redaelli de Zinis. 2008[28] | 26 | 26 | 12. | 14. | 49y (17-78) | 26 CCOM |
| Alaani and Raut. 2009[29] | 97 | 97 | 65 | 32 | 39.6 y (5 –75) | 40 CCOM, 10 COM, 38 AT, 9 n.a. |
| Colletti et al. 2009[30] | 19 | 19 | 0 | 19 | 50 y (19 - 76) | 19 COM |
| Roth et al. 2009[31] | 54 | 54 | 32 | 22 | 34y (6-74) | 36 CCOM, 9 COM, 4 CA, 5 TR |
| Woods et al. 2009[32] | 70 | 70 | 40 | 30 | 34.1y (11-76) | 33 CCOM, 12 COM, 10 AT, 15 n.a. |
| Fong et al. 2010[33] | 51 | 51 | 34 | 17 | 38 y (7 – 69) | 20 CCOM, 31 COM |
| Inũiguez-Cuadra et al. 2010[34] | 85 | 94 | 0 | 94 | n.a. | n.a. |
| Luers et al. 2010[35] | 70 | 70 | 0 | 70 | 43.6y (6-66) | 40 CCOM, 30 COM |
| Praetorius et al. 2010[36] | 14 | 14 | 14 | 0 | 50.4y (13–74) | 14 CCOM |
| Quesnel et al. 2010[37] | 74 | 74 | 27 | 47 | 11.3y (n.a.) | n.a. |
| Yung and Smith. 2010[38] | 49 | 49 | 19 | 30 | 44y (n.a.) | 14 CCOM, 35 COM |
| Babighian and Albu. 2011[39] | 125 | 125 | 0 | 125 | 43.7 (n.a.) | 125 CCOM |
| Beutner et al. 2011[6] | 18 | 18 | 18 | 0 | 44.4y (8-69) | 12 CCOM, 6 COM |
| Quaranta et al. 2011[37] | 57 | 57 | 19 | 38 | 38 y (6 – 67) | 57 CCOM |
| Mardassi et al. 2011[40] | 70 | 70 | 37 | 33 | 43y (5-77) | 47 CCOM, 23 COM |
| Nevoux et al. 2011[41] | 114 | 116 | 0 | 116 | 9.8y (n.a) | 116 CCOM |
| Berenholz et al. 2013[42] | 152 | 152 | 84 | 68 | 47.3y (n.a.) | 92 CCOM, 56 COM, 4 n.a. |
| Gostian et al. 2013[43] | 12 | 12 | 0 | 12 | 42y (9 - 73) | 8 CCOM, 4 COM |
| Hess-Erga et al. 2013[44] | 76 | 76 | 44 | 32 | 33y (6-78) | 40 CCOM, 5 COM, 31 TR |
| Meulemans et al 2013[45] | 83 | 89 | 89 | 0 | n.a. (7-85) | 51 CCOM, 21 COM, 17 n.a. |
| Shah et al. 2013[46] | 19 | 19 | 15 | 4 | 14–50y (n.a.) | 19 CCOM + COM |
| Birk et al. 2014[47] | 60 | 62 | 62 | 0 | 38y (4 - 83) | n.a. |
| Fayad et al. 2014[48] | 62 | 62 | 0 | 62 | 38.4y (3 - 82) | 60 COM, 2 n.a. |
| Órfão et al. 2014[49] | 43 | 43 | 26 | 17 | 39y (7- 70) | 14 CCOM, 17 COM, 12 n.a. |
| Pringle et al. 2014[50] | 73 | 73 | 36 | 37 | 32.9y (6 - 64) | n.a. |
| Baker et al. 2015[51] | 79 | 83 | 56 | 27 | 37.3y (6–79) | 74 CCOM+ COM, 9 n.a. |
| Boleas-Aguirre et al. 2015[52] | 16 | 16 | 0 | 16 | 56y (57–40) | 8 CCOM+COM, 5 TS, 3 OTO |
| Lee et al. 2015[53] | 27 | 27 | 18 | 9 | 54y (14 - 76) | 17 CCOM, 10 COM |
| Ocak et al. 2015[54] | 18 | 18 | 8 | 10 | 35.2y (13 - 57) | 18 CCOM+ COM |
| Roux et al. 2015[55] | 68 | 68 | 32 | 36 | 34.5y (13-56) | 68 CCOM |
| Wolter et al. 2015[56] | 71 | 75 | 0 | 75 | 14.3 y (7 - 18) | 66 CCOM, 2 CA, 7 n.a. |
| Faramarzi et al. 2016[57] | 45 | 45 | 0 | 45 | n.a. | 10 CCOM, 3 COM, 11 TS, 21 n.a. |
| Gostian et al. 2016[58] | 47 | 47 | 47 | 0 | 43y (7–73) | 17 CCOM, 30 COM |
| Gostian et al. 2016[59] | 42 | 42 | 0 | 42 | 42.8y (6-78) | 26 CCOM, 16 COM |
| O’Connell et al. 2016[60] | 149 | 149 | 56 | 93 | 30.1y (n.a.) | 80 CCOM, 69 COM |
| Amith and Rs. 2017[61] | 20 | 20 | 20 | 0 | 25 y (12 - 52) | 10 CCOM, 10 COM |
| Govil et al. 2017[62] | 101 | 101 | 47 | 54 | 9.8y (3.4-17.3) | n.a. |
| McMullen et al. 2017[63] | 71 | 71 | 23 | 48 | 26y (6-73) | n.a. |
| Mulazimoglu et al. 2017[64] | 126 | 126 | 126 | 0 | 37 y (7 –72) | 86 CCOM, 11 COM, 13 CHL, 11 TR, 3 TS, 2 TU |
| Choi and Shin. 2018[65] | 45 | 45 | 20 | 25 | n.a. | 45 CCOM + COM |
| Kahue et al. 2018[66] | 130 | 130 | 130 | 0 | 36 y (n.a.) | 121 COM, 9 TR |
| Kong et al. 2017[67] | 20 | 20 | 9 | 11 | 49 y (n.a.) | n.a. |
| Kumar et al. 2017[68] | 37 | 37 | 31 | 6 | 31.6 y (13-48) | 37 CCOM+ COM |
| Lahlou et al. 2018[69] | 256 | 280 | 163 | 117 | 44y (17 - 74) | 125 CCOM, 85 COM, 40 AT, 4 CA, 11 OTO, 12 TR, 3 TU |
| Saliba et al. 2018[70] | 158 | 158 | 0 | 158 | 29.7y (n.a.) | 103 CCOM, 25 COM, 19 CA, 11 n.a. |
| Gu and Chi. 2019[71] | 206 | 206 | 134 | 72 | 46y (12-70) | 206 CCOM + COM |
| Haidar et al. 2019[72] | 129 | 133 | 88 | 45 | 33 y (7 – 74) | 34 COM, 10 AT, 24 GR, 65 n.a. |
| Potsangbam and Akoijam. 2019[5] | 20 | 20 | 14 | 6 | 30y (8 - 64) | 20 CCOM |
| Wood et al. 2019[73] | 153 | 153 | 0 | 153 | 40y (6-89) | 120 CCOM, 10 COM, 23 n.a. |
| Mantsopoulos et al. 2021[74] | 274 | 274 | 274 | 0 | 38 y (6 – 67) | 168 CCOM, 62 COM, 37 TS, 6 TR, 1 TU |
| Baazil et al. 2022[75] | 106 | 106 | 0 | 106 | 35y (6.6–75.3) | 105 CCOM+ COM, 1 CA |
| Bahmad and Perdigão. 2022[76] | 13 | 13 | 0 | 13 | 44y (n.a.) | 7 CCOM, 6 COM |
| Kraus et al. 2022[77] | 36 | 38 | 38 | 0 | 40.4y (6-81) | 18 CCOM, 20 COM |
| Park et al. 2022[78] | 135 | 135 | 86 | 49 | n.a. | 94 CCOM, 41 COM |
| Plichta et al. 2022[79] | 24 | 24 | 12 | 12 | 38.33 y (4-62) | 24 TR |
| Van Hoolst et al. 2022[80] | 99 | 113 | 0 | 113 | n.a. (8 - 87) | 74 CCOM, 15 COM, 24 CA |
| Chien et al. 2023[81] | 8 | 8 | 8 | 0 | n.a. (27-48) | 8 TR |
| Faramarzi et al. 2023[82] | 248 | 248 | 115 | 133 | 33 y (n.a.) | 248 CCOM+COM+TS |
| Gülşen and Çıkrıkcı. 2023[83] | 21 | 21 | 0 | 21 | n.a. (28-44) | 21 TS |
| Kálmán et al. 2023[84] | 130 | 130 | 84 | 46 | n.a. | 130 CCOM+ COM |
| Kim et al. 2023[85] | 130 | 130 | 78 | 52 | 49.2y (n.a.) | 71 CCOM, 59 COM |
Number of patients (pts): when not specified is assumed to be the same number of ears, years (y), not available (n.a.), chronic otitis media with cholesteatoma (CCOM), chronic otitis media without cholesteatoma (COM), atelectasis (AT), tympanosclerosis (TS), traumatic injuries (TR), otosclerosis (OTO), congenital abnormalities (CA).
Table 2.
Surgical details and functional outcomes.
| Authors, year | Surgery | Staging | Pre-op ABG | Post-op ABG | Extrusions and dislocations/ears (%) | Onset | Treatment | Follow-up | ||
| PORP | TORP | PORP | TORP | |||||||
| Wang et al. 1999[8] | 11 CWD, 48 CWU, 65 OPL | 0 | n.a. | n.a. | n.a. | n.a. | 2/124 (1.6%) | n.a. | n.a. | 12-46 mo |
| Dalchow et al. 2001[9] | n.a. | 1100 | n.a. | n.a. | 14 | 15 | 29/1304 (2.2%) | n.a. | n.a. | 6-72 mo |
| Krueger et al. 2002[10] | n.a. | n.a. | n.a. | n.a. | 14.1 | n.a. | 0/31 (0%) | / | / | 16 mo - 2 y |
| Hillman and Shelton. 2003[11] | n.a. | n.a. | n.a. | n.a. | n.a. | n.a. | 2/53 (3.8%) | 12 mo | surgical | 3mo- n.a. |
| Ho et al. 2003[12] | 9 CDW, 15 CWU, 1 OPL | 20 | 38.7 | 42.8 | 18.1 | 21.5 | 1/25 (4%) | n.a. | surgical | 6 mo |
| Neff et al. 2003[13] | 16 OPL, 2 n.a. | 6 | n.a. | 33.9 | n.a. | 16.9 | 0/ 18 (0%) | / | / | 8 mo |
| Neumann et al. 2003[14] | n.a. | 0 | n.a. | n.a. | n.a. | n.a. | 0/61 (0%) | / | / | 38 mo |
| Fisch et al. 2004[15] | 21 CWD, 25 CWU | 46 | / | 41.9 | / | 20.7 | 0/46 (0%) | / | / | 1-7 y |
| Gardner et al. 2004[16] | 13 CWD,68 CWU, 21 OPL, 47 n.a. | 13 | 26 | 40 | 18.8 | 21.7 | 1/149 (0.7%) | n.a. | n.a. | 1.5y |
| Martin et al. 2004[17] | 14 CWD, 7 CWU, 47 OPL | 4 | 34 | 34 | 17 | 25 | 1/68 (1.5%) | n.a. | surgical | 3 mo- 2.5y |
| Menéndez-Colino et al. 2004[18] | 16 CWD, 7 CWU | 0 | / | n.a. | / | n.a. | 0/23 (0%) | / | / | 18 mo |
| Lehnerdt et al. 2005[19] | n.a. | 0 | n.a. | n.a. | n.a. | n.a. | 1/15 (6.6%) | n.a. | n.a. | 6 mo |
| De Vos et al. 2006[20] | 8 CWD, 65 CWU, 67 OPL | 24 | 32.7 | 42.5 | 18.1 | 19.8 | 11/140 (7.9%) | 22 mo | surgical | 11.8 mo |
| Vassbotn et al. 2006[21] | 20 CWD, 53 CWU | 0 | 28 | 38 | 9 | 19 | 4/73 (5.5%) | n.a. | 2 surgical, 2 n.a. | 14.2 mo |
| Schmerber et al. 2006[22] | 18 CWD, 93 CWU | 65 | n.a. | n.a. | 15 | 26.5 | 14/111 (12.6%) | 1: 17 mo, 1: 20 mo, 12 n.a. | 13 surgical, 1 refused | 20.5 mo |
| Hales et al. 2007[23] | 4 CWD, 30 CWU | 34 | n.a. | n.a. | n.a. | n.a. | 2/34 (5.9%) | n.a. | n.a. | 19 mo |
| Siddiq and Raut. 2007[24] | 5 CWD, 14 CWU, 14 n.a. | n.a. | 25.1 | 23.3 | 15.3 | 13.4 | 0/33 (0%) | / | / | 6 - 18 mo |
| Truy et al. 2007[25] | n.a. | n.a. | 30.9 | 28 | 19.4 | 18.3 | 2/62 (3.2%) | 2 mo | surgical | 12 mo |
| Coffey et al. 2008[26] | 22 CDW, 22 CWU, 30 OPL | 34 | n.a. | n.a. | 14.3 | 16.0 | 3/80 (3.8%) | n.a. | n.a. | 14.9 mo |
| Michael et al. 2008[27] | 7 CWD, 3 CWU, 4 OPL | 7 | n.a. | n.a. | n.a. | n.a. | 0/7 (0%) | / | / | 12 mo |
| Redaelli de Zinis. 2008[28] | 26 CWD | 0 | n.a. | n.a. | n.a. | n.a. | 0/ 14 (0%) | / | / | 12 mo |
| Alaani and Raut. 2009[29] | 57 CWD, 40 CWU+ OPL | 29 | 26.3 | 32.1 | 10.6 | 14.8 | 2/97 (2.1%) | 1 y | 1 surgical, 1 n.a. | 1 y |
| Colletti et al. 2009[30] | 19 CWU | n.a. | / | 40.7 | / | 21.5 | 3/19 (15.8%) | n.a. | 2 surgical, 1 n.a. | 36 mo |
| Roth et al. 2009[31] | 11 CWD, 27 CWU, 16 OPL | 29 | 31.0 | 38.2 | 13.3 | 16.4 | 1/54 (1.8%) | / | surgical | 1-5 y |
| Woods et al. 2009[32] | n.a. | 3 | 32.2 | 39.2 | 26.9 | 29.2 | 11/70 (15.7%) | n.a. | n.a. | 6 mo |
| Fong et al. 2010[33] | 4 CWD, 47 CWU | n.a. | n.a. | n.a. | n.a. | n.a. | 1/51 (2%) | n.a. | n.a. | 12 mo |
| Inũiguez-Cuadra et al. 2010[34] | 56 CWD, 38 CWU | n.a. | / | 23.8 | / | 15.4 | 8/94 (8.5%) | n.a. | n.a. | 38 mo |
| Luers et al. 2010[35] | 33 CWD, 37 CWU | 0 | / | 33.9 | / | 19.7 | 0/70 (0%) | / | / | 2 mo |
| Praetorius et al. 2010[36] | n.a. | n.a. | 26.6 | / | 15.2 | / | 0/14 (0%) | / | / | 8 mo |
| Quesnel et al. 2010[37] | n.a. | 49 | 30.2 | 36.6 | 20.8 | 22 | 5/74 (6.8%) | n.a. | n.a. | 33 mo |
| Yung and Smith. 2010[38] | n.a. | 7 | 29.2 | 32.5 | 16.2 | 20.7 | 8/49 (16.3%) | n.a. | n.a. | 2y |
| Babighian and Albu. 2011[39] | 125 CWD | 125 | / | 44.9 | / | 22.3 | 2/125 (1.6%) | n.a. | n.a. | 12 mo |
| Beutner et al. 2011[6] | 11 CWD, 7 CWU | 0 | 26.8 | / | 18.2 | / | 0/18 (0%) | / | / | 6 mo |
| Quaranta et al. 2011[37] | 57 CWU | 57 | 36.7 | 45.3 | 24.1 | 27.2 | 6/57 (10.5%) | n.a. | surgical | 24 mo |
| Mardassi et al. 2011[40] | 70 CWU+ OPL | 24 | 27.2 | 32.8 | 15 | 19.5 | 4/70 (5.7%) | n.a. | surgical | 9.8 mo |
| Nevoux et al. 2011[41] | 116 CWU | 116 | / | 41 | / | 22.4 | 17/116 (14.7%) | 2: 1y, 6: 2 y, 5: 5y, 1: >5y, 3: n.a. | surgical | 34 mo |
| Berenholz et al. 2013[42] | 15 CWD, 50 CWU, 87 n.a. | 16 | 32.5 | 30.6 | 11.9 | 15.8 | 10/152 (6.6%) | n.a. | surgical | 4.3 y |
| Gostian et al. 2013[43] | 1 CWD, 11 CWU | n.a. | / | 26.6 | / | 18.8 | 0/12 (0%) | / | / | 32 mo |
| Hess-Erga et al. 2013[44] | 31 OPL, 40 n.a. | n.a. | 28 | 37 | 15 | 20 | 4/76 (5%) | <1y | 2 surgical | 5.2y |
| Meulemans et al 2013[45] | 7 CWD, 65 CWU, 17 OPL | 0 | 26.2 | / | 15.6 | / | 3/89 (3.4%) | / | surgical | 13 mo |
| Shah et al. 2013[46] | 19 CWU | 0 | n.a. | n.a. | n.a. | n.a. | 0/19 (0%) | / | / | 11.1y |
| Birk et al. 2014[47] | n.a. | n.a. | 26.9 | / | 15.4 | / | 1/62 (1.6%) | n.a. | n.a. | 7 mo |
| Fayad et al. 2014[48] | 8 CWD, 21 CWU, 30 OPL, 3 n.a. | 23 | / | 35.1 | / | 18 | 1/62 (1.6%) | 1 y | n.a. | 21.7 mo |
| Órfão et al. 2014[49] | 1 CWD, 11 CWU, 31 OPL | 0 | 32.8 | 37.1 | 21.9 | 25.7 | 1/43 (2%) | n.a. | n.a. | 20 mo |
| Pringle et al. 2014[50] | 9 CWD, 47 CWU, 17 OPL | 52 | n.a. | n.a. | n.a. | n.a. | 5/73 (6.8%) | n.a. | surgical | 6 - 96 mo |
| Baker et al. 2015[51] | n.a. | 38 | 28.2 | 30.3 | 16.5 | 20.6 | 5/ 83 (6.0%) | n.a. | surgical | 41.8 mo |
| Boleas-Aguirre et al. 2015[52] | 2 CWD, 2 CWU, 12 OPL | n.a. | / | 34 | / | 16.4 | 0/ 16 (0%) | / | / | 12 mo |
| Lee et al. 2015[53] | 15 CWD, 11 CWU, 1 OPL | n.a. | 23 | 28 | 12 | 15 | 0/27 (0%) | / | / | 6 mo |
| Ocak et al. 2015[54] | 15 CWU, 3 OPL | n.a. | 33.7 | 38 | 8.6 | 19 | 1/18 (5.5%) | 12 mo | n.a. | 38.5 mo |
| Roux et al. 2015[55] | 68 CWU | 19 | 23.5 | 31 | 19.5 | 26 | 0/68 (0%) | / | / | 23 mo |
| Wolter et al. 2015[56] | n.a. | n.a. | / | 44 | / | 30 | 1/75 (1.3%) | 3.9 y | surgical | 2.7 y |
| Faramarzi et al. 2016[57] | 45 OPL | 45 | / | 36 | / | 24.7 | 2/45 (4.4%) | n.a. | n.a. | 6-12 mo |
| Gostian et al. 2016[58] | 15 CWD, 32 CWU | n.a. | 25.7 | n.a. | 16.8 | n.a. | 1/47 (2%) | / | / | 6.5y |
| Gostian et al. 2016[59] | 18 CWD, 24 CWU | 0 | / | 33 | / | 22 | 2/42 (4.8%) | 6 mo | surgical | 6.8y |
| O’Connell et al. 2016[60] | n.a. | 77 | 30.9 | 37.9 | 17.6 | 21.8 | 5/149 (3.2%) | n.a. | surgical | 51.6 mo |
| Amith and Rs. 2017[61] | 3 OPL, 17 n.a. | 3 | 44.4 | / | 31.3 | / | 3/20 (15%) | n.a. | n.a. | 12 mo |
| Govil et al. 2017[62] | n.a. | n.a. | n.a. | n.a. | n.a. | n.a. | 29/101 (29%) | 1.3 y | surgical | 2.2y |
| McMullen et al. 2017[63] | n.a. | 50 | n.a. | n.a. | n.a. | n.a. | 1/71 (1.4%) | 8 mo | conservative | 10.2 mo |
| Mulazimoglu et al. 2017[64] | 33 OPL, 93 n.a. | 33 | / | 28.2 | / | 22.3 | 30/126 (23.8%) | 26 mo | 12 surgical, 18 n.a. | 4.5 y |
| Choi and Shin. 2018[65] | n.a. | 8 | n.a. | n.a. | n.a. | n.a. | 2/45 (4.4%) | / | / | 12 mo |
| Kahue et al. 2018[66] | 5 CWD, 77 CWU, 48 OPL | 10 | 29 | / | 18 | / | 3/130 (2.3%) | 25 mo | surgical | 37 mo |
| Kong et al. 2017[67] | n.a. | n.a. | 27.6 | 28.5 | 26 | 29 | 4/20 (20%) | n.a. | n.a. | 27 mo |
| Kumar et al. 2017[68] | n.a. | 0 | 32.1 | 37.5 | 26.3 | 21.6 | 1/37 (2.7%) | n.a. | n.a. | 6 mo |
| Lahlou et al. 2018[69] | 46 CWD, 74 CWU, 160 OPL | 0 | 26 | 30 | 15 | 20 | 17/280 (6.1%) | n.a. | surgical | 12 mo |
| Saliba et al. 2018[70] | 36 CWD, 122 CWU | 62 | / | 38 | / | 26.3 | 24/158 (15%) | n.a. | surgical | 18 mo |
| Gu and Chi. 2019[71] | 206 CWD | 0 | 27.8 | 28 | 16.4 | 18.4 | 2/206 (1.0%) | / | / | 30 mo |
| Haidar et al. 2019[72] | 133 CWU | 8 | 29.6 | 33.3 | 12.9 | 18.7 | 5/133 (2.3%) | n.a. | n.a. | 6 mo |
| Potsangbam and Akoijam. 2019[5] | 20 OPL | 20 | 37.1 | 40.3 | 17.6 | 22.5 | 7/20 (35%) | 4- 8y | n.a. | 3y |
| Wood et al. 2019[73] | 24 CWD, 114 CWU, 15 OPL | 14 | / | 37.5 | / | 24.9 | 1/153 (0.6%) | n.a. | surgical | 44 mo |
| Mantsopoulos et al. 2021[74] | n.a. | n.a. | 22.7 | / | 15.7 | / | 8/274 (2.9%) | n.a. | n.a. | 4 mo |
| Baazil et al. 2022[75] | 3 CWD, 33 CWU, 70 OPL | 74 | / | 38.1 | / | 27.6 | 8/106 (7.5%) | n.a. | n.a. | 11.7 mo |
| Bahmad and Perdigão. 2022[76] | 13 CWD | n.a. | / | 35.1 | / | 20.7 | 0/13 (0%) | / | / | 6 mo |
| Kraus et al. 2022[77] | n.a. | 0 | 21.8 | / | 10.5 | / | 2/38 (5.3%) | n.a. | n.a. | 1-9 y |
| Park et al. 2022[78] | 113 CWD, 22 CWU | 0 | 28.1 | 28.1 | 18.4 | 23.5 | 1/135 (0.7%) | n.a. | n.a. | 8.1 mo |
| Plichta et al. 2022[79] | 24 OPL | n.a. | n.a. | n.a. | n.a. | n.a. | 1/24 (4.1%) | n.a. | surgical | 24 mo |
| Van Hoolst et al. 2022[80] | 28 CWD, 23 OPL, 62 n.a. | n.a. | / | 32.7 | / | 21.7 | 17/113 (15.0%) | n.a. | surgical | 39 mo |
| Chien et al. 2023[81] | 8 OPL | 0 | 25.9 | / | 10.8 | / | 0/8 (0%) | / | / | 3.58 mo |
| Faramarzi et al. 2023[82] | 248 OPL | 248 | 34 | 37.6 | 21.2 | 24.6 | 7/248 (2.8%) | n.a. | n.a. | 12.5 mo |
| Gülşen and Çıkrıkcı. 2023[83] | 21 OPL | 0 | / | 37.1 | / | 14.5 | 1/21 (4.8%) | n.a. | surgical | 12 mo |
| Kálmán et al. 2023[84] | n.a. | n.a. | n.a. | n.a. | n.a. | n.a. | 11/130 (8.5%) | n.a. | surgical | 8.8 mo |
| Kim et al. 2023[85] | 130 OPL | 130 | n.a. | n.a. | n.a. | n.a. | 10/130 (7.7%) | n.a. | n.a. | 22.7 mo |
Canal wall down (CWD), canal wall up (CWU), ossiculoplasty (OPL), years (y), months (mo), not available (n.a.). Data included in column “surgery” refer to the procedure performed at the time of ME implant positioning regardless of any previous surgery. In column “staging” we reported, when available, the number of ossicular reconstruction performed in a second stage procedure. In the columns preoperative ABG (pre-op ABG) and postoperative ABG (post-op ABG) n.a. indicates this outcome is not mentioned or audiometric results differentiated between PORP and TORP group are not available. “Extrusions and dislocations/ears (%)”: we excluded extrusions and dislocations caused by cholesteatomas. The data included in the columns “Onset” and “Treatment” refer to the time of appearance and management of complications. “Follow-up” indicates the average follow-up or, when not available, its range.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



