
Submitted:
31 August 2023
Posted:
05 September 2023
You are already at the latest version
Abstract
Background: Mood disorders, especially depression, and emotional difficulties such as anxiety are very common problems among patients with spinal cord injury (SCI). The loss of physical training may deteriorate their mental state, which in turn has a significant impact on the improvement of functioning. The aim of the present study was to examine the influence of innovative rehabilitation approaches involving robotic assisted gait therapy (RAGT) on mood and anxiety symptoms in pa-tients with SCI.
Methods: To this single-centre, single-blinded, single-arm, prospective study, 110 participants with subacute SCI were enrolled; patients were divided into experimental (robotic assisted gait therapy -RAGT) and control (conventional gait therapy with dynamic parapodium - DPT) groups. They received five training sessions per week over 7- weeks. The severity of de-pression was assessed by Depression Assessment Questionnaire (KPD) and anxiety symptoms by State - Trait Anxiety Inventory (STAI X-1) on the beginning and end of therapy.
Results: SCI patients experienced significantly lower levels of anxiety and depression-related symptoms after completing the seven-week rehabilitation program (KPD: Z=6.35; p<0.001; r=0.43; STAI X-1: Z=-6.20; p<0.001; r=0.42) in both group of patients. In the RAGT group, post-rehabilitation measurements also indicated an improvement in psychological functioning, i.e., a decrease in depression and anxiety, and an increase in self-regulation. Significant results were noted for each variable (STAI X-1: Z = -4.93; KPD: Z = -5.26; SR: Z = -3.21). In the control group, there was also a decrease in the effect on the depression, anxiety-state and an increase in self-regulation ability (STAI X-1: Z=-4.01; KPD: Z=-3.65; SR: Z=-2.83). Rehabilitation modality did not appear to have a statistically significant relationship with the magnitude of improvement in KPD (including SR) and STAI scores. However, there were some significant differences when comparing the groups by extent and depth of injury and type of paralysis. The study also did not find a significant rela-tionship between improvements in physical aspects and changes in psychological factors.
Conclusion: Subjects in RAGD and DPT groups experienced a decrease in anxiety and depres-sion after a 7-week rehabilitation program. However, the rehabilitation modality (DPT vs. RAGT) did not differentiate patients with SCI in terms of the magnitude of this change. Our results may suggest that individuals with severe neurological condition and complete spinal cord injury (AIS A) may experience more benefit in terms of change in psychological parameters after rehabilitation with RAGT.
Keywords:
spinal cord injury
; robotic rehabilitation
; coordinative rehabilitation
; depression
; mood
; anxiety
1. Introduction
There are approximately 10.5 new cases of traumatic spinal cord injury (SCI) diagnoses per 100.000 people worldwide each year [1]. Based on epidemiological data in Poland, the majority of people in this population are men (the sex ratio is 2.5 to 6), average age is > 40 years and the most common cause of injury is traffic accidents [2,3]. Spinal cord injuries directly lead to loss or limitation of motor and sensory function at the level of injury and below. Secondary symptoms are usually sphincter dysfunction, chronic neuropathic pain, autonomic dysreflexia, respiratory failure, sexual dysfunction, digestive disorders and respiratory failure [4]. Direct and secondary somatic symptoms after SCI, as well as the loss of independence, the need to reorganize functioning in family, social and professional life can affect the deterioration of: psychological well-being of these patients, quality of life, body image and its perception (concerning attitudes toward the body at the level of thoughts, emotions and behavior), self-confidence and belief in one's abilities and the perception of one's social attractiveness [5,6,7,8,9]. The most common symptoms described in the literature within psychological functioning are feelings of anxiety and lowered mood often in clinical form (depression). Anxiety disorder, including generalized anxiety disorder (GAD) and post-traumatic stress disorder (PTSD), is the second most commonly described mental disorder in studies. It is estimated to affect approximately 15% to 32% of people with SCI, depending on the measure used [10]. The risk rate for depression among SCI patients undergoing inpatient treatment ranges between 20 and 43%, and the average of the results obtained from different studies is 30% [11]. A measure of the prevalence of anxiety and depression among people with spinal cord injury is therefore higher than in the general population.
Rehabilitation and other regular exercise and physical activity are significantly related to lower levels of stress and depression-related symptoms, social participation and quality of life. They may also have a preventive effect against a decline in quality of life after a spinal injury, mainly through their effect on reducing pain levels, as well as increasing sense of control and mastery, improved fitness and performance [12,13]. Due to the breadth and diversity of health problems after SCI, early, intensive but, above all, multispecialty assistance is essential. An early coordinated rehabilitation program makes it possible to anticipate its implications in terms of somatic and psychological health in the form of reduced anxiety and depression [14,15,16].
One of the most important and desirable goals of rehabilitation after SCI (regardless of the level, depth of injury, time since the injury, and age of the patient) is to achieve the ability to maintain an upright position and regain gait function [17,18]. The upright position not only has a beneficial effect on secondary physical symptoms, but is also related to improved quality of life, a sense of independence and self-confidence [19,20]. Rehabilitation robots are increasingly being used during gait re-education. Robotic-assisted gait training (RAGT) uses stationary devices such as the Lokomat machine and exoskeletons. The Locomat system is mostly conducted for lower extremities and a body-weight support treadmill training. It offers a number of advantages, including the ability to start therapy early after an injury, therapy for people with significant lower limb paralysis. In addition, it will allow adjustment of parameters such as speed, weight-bearing relief (intensity) and length of the training session to suit the patient's current capabilities, and it allows accurate monitoring of the patient's progress. It is a device well tolerated by patients [21,22,23,24]. The U.S. Food and Drug Administration defines a powered exoskeleton as: "(...) is a prescription device that is composed of an external, powered, motorized orthosis that is placed over a person's paralyzed or weakened lower extremity limb(s) for medical purposes” [25]. There are two groups of exoskeletons: assistive exoskeletons and rehabilitation exoskeletons. A rehabilitation exoskeleton is a device that provides support for the patient's total body weight [26]. It is an equally promising, safe and well-tolerated method of therapy for patients with neurological disorders including post SCI patients [27,28,29,30]. Modern multifaceted rehabilitation using RAGT has a beneficial effect not only on improving sensorimotor, kinematic and autonomic functions, also give a greater sense of control over one's own body and independence thus contributing to an improvement in psychological functioning and subjective assessment of quality of life [5,31,32,33,34].
There are few studies describing rehabilitation using RAGT that include psychological variables. Most of them also focus on quality of life rather than emotional difficulties or affective disorders, or include people with other neurological disorders such as multiple sclerosis or stroke [35,36,37,38,39,40,41]. The results of these trials are often inconclusive. Some studies suggest an association between RAGT and a reduction in depressive symptoms and an increase in quality of life, while others have found no such association. Others emphasize its relevance and equivalence with biological and social factors [30,42,43,44,45]. Relatively few studies have been done on the efficacy of rehabilitation with RAGT conducted on a group of patients with SCI and the analyses conducted so far are promising especially for patients with significant hemiparesis [17,22,38,40,46,47,48,49,50,51,52]. The researchers emphasize that RAGT should not replace conventional rehabilitation, but complement it [42,43,53,54,55]. The rehabilitation procedures have also not been delineated in terms of duration, frequency and intensity of training, among others [56].
Based on previous available knowledge, we hypothesized that SCI patients would experience less anxiety and lower levels of depression-related symptoms after both forms of therapy but with RAGT favor [5,12,13,14,15,34,48,57]. The main objective of our study was to analyze the association of rehabilitation with RAGT with symptoms related to depression and anxiety and clinical status. In addition, we sought to answer the questions of whether the level and extent of injury and type of paralysis affect the magnitude of change in the level of symptoms of depression and anxiety - the condition after the 7-week rehabilitation program, and whether the change in these parameters is related to improvements in medical parameters (i.e., functional independence and mobility and the extent of recovery of gait function).
In the study we assumed the following hypothesis:
- Both the rehabilitation group with DPT used (S0) and GAIT used (S1) show significant improvement in the severity of symptoms related to depression and state anxiety.
- Patients in the experimental group (S1) will achieve greater improvements in psychological indicators (severity of depression-related symptoms and state anxiety) compared to those in the control group (S0).
- The improvement in psychological parameters (i.e., the decrease in symptoms related to depression and anxiety - state) is observed to have a significant relationship with the improvement in gait function and functional independence after SCI.
In addition, we set out to see if patients with paraplegia present different levels of anxiety and depression than patients with tetraplegia in patients from the experimental and control groups. Simultaneously, the type of rehabilitation is significant in terms of changes in the symptoms of depression and anxiety-state in patients with different degrees of injury on the AIS scale (AIS A vs AIS B, C, D). Patients with spinal cord injury differ significantly in their neurological status, which has a major impact on their potential abilities and functional status [58,59,60]. In this study, we decided to divided patients into separate groups according to the AIS classification (AIS A with complete injury and AIS B,C,D with incomplete injury), and the type of paralysis (tetraplegia and paraplegia).
2. Materials and Methods
2.1. Study Protocol
The present study was a single-blinded, prospective, clinical study. The following study has been authorized by the ethical committee and conducted accordingly to the Helsinki declaration committee. The project obtained approval from the Ethical Board of the District Medical Chamber in Szczecin (Poland) (Nr OIL-Sz/MF/KB/452/05/07/2018; Nr OIL-SZ/MF/KB/450/UKP/10/2018). All participants before being accepted to the study have been through thorough Medical examinations conducted by Physicians specialized in neurology physical rehabilitation medicine doctor physiotherapist and psychologist.
Medical inclusion criteria included: time since injury ranging from 3 months to 2 years; general condition of the patient defined as conscious, able to cooperate with the physiotherapist, and adapted to upright position; complete and incomplete SCI (cervical, thoracic or lumbar) with preserved flexion and extension function at the elbow and wrist; with surgical stabilization of the spine being in the phase of completed bone fusion; no contraindications to rehabilitation arising from, among other things; among others, from venous thrombosis, pulmonary embolism, orthostatic hypotension, epilepsy and infection; body weight not exceeding 120 kg, height between 150 and 190 cm. Exclusion criteria included: high and complete tetraplegia and very low lumbar spine injury; lack of completion of bone fusion after established spinal stabilization; lack of completed bone fusion after spine surgery; having respiratory insufficiency, circulatory insufficiency III and IV New York Heart Association (NYHA) grade; osteoporosis; lower limb shortening of more than 2 cm; the presence of decubitus ulcers, deep abrasions or skin lesions that could be exacerbated by the robotic system used; intensive spasticity (4 points on the Ashworth scale) and having muscle contractures making it impossible to conduct robotic rehabilitation; past or present neurological disorders, i.e. traumatic spinal stroke, multiple sclerosis, childhood cerebral palsy; having symptoms of recurrent autonomic dysreflexia. In psychological studies, additional exclusion criteria were the finding of a reduced general level of intellectual functioning preventing questionnaire tests and the age below 16 (no normalization of the psychological tools used for this age group).
All patients underwent two physiotherapeutic, medical and psychological assessments by professionals unfamiliar with the purpose of the study, at the beginning and at the end of the 7-week treatment program. Research tools with proven validity and reliability were used to verify the research hypotheses. The research procedure followed scheme No.1 each time. Medical physical and neurological examination including medical history, questionnaire tests using: Spinal Cord Independence Measure, version III (SCIM-III), Walking Index for Spinal Cord Injury, version II (WISCI-II). Carry out the test procedure using The American Spinal Cord Injury Association (ASIA) Impairment Scale (AIS). The psychological examination included a structured interview, conducting surveys using questionnaires (including Depression Assessment Questionnaire, KPD) and anxiety - state by The State-Trait Anxiety Inventory (STAI, X-1). To standardize the research procedure, the psychologist read the questionnaire questions and marked the answer. This was necessary due to the motor difficulties of some patients, i.e. the problem of marking answers and turning the pages of the sheet.
2.2. Physiotherapy and psychological intervention
The rehabilitation program consisted of two phases lasting three weeks each, with a one-week break in between. Rehabilitation interventions took place six days a week. Psychological activities were held once a week and included individual sessions (targeting patients' needs and difficulties based on their resources) and group therapy.
Patients were enrolled into two groups by coin toss: a control group (S0) subjected to conventional gait therapy with a dynamic parapodium therapy (DPT), and an experimental group subjected to rehabilitation using RAGT. The mentioned therapies lasted 30-minutes. Patients enrolled to the experimental group (S1) received RAGT sessions using the EKSO-GT exoskeleton (model EKSO 1 by Ekso Bionics, year of manufacture 2014) or Locomat Pro (model LO218 by Hocoma AG, year of manufacture 2014) in addition to the general standard physiotherapy training program based on proprioceptive neuromuscular facilitation. All participants from the Locomat group with incomplete SCI started with 60% body weight support and an initial treadmill speed of 1.5 km/h. Patients with complete SCI started with 100-90% body weight support. In patients with EKSO-GT, a minimum of 100 steps were required per session. All patients in both the S0 and S1 groups received psychological support; meetings were held three times during the cycle of the seven-week rehabilitation program 50-minute individual sessions based on cognitive-behavioral therapy (CBT) techniques were held at least once a week (at least eight times during the course of the camp). In general, CBT therapy is aimed at changing maladaptive patterns of thinking and behavior. The program and purpose of the meetings were tailored to each patient's needs and problems, and were closely coordinated with the patient. In addition to individual meetings, weekly 90-minute group therapy meetings were conducted based on the CBT, therapy method, Rational Behavior Therapy, using Motivational Interviewing and Mindfulness-Based Cognitive Therapy. The group therapy was aimed at the general difficulties faced by people after SCI, and was also aimed at exchanging information, supporting each other's patients and receiving feedback from them.
2.3. Participants
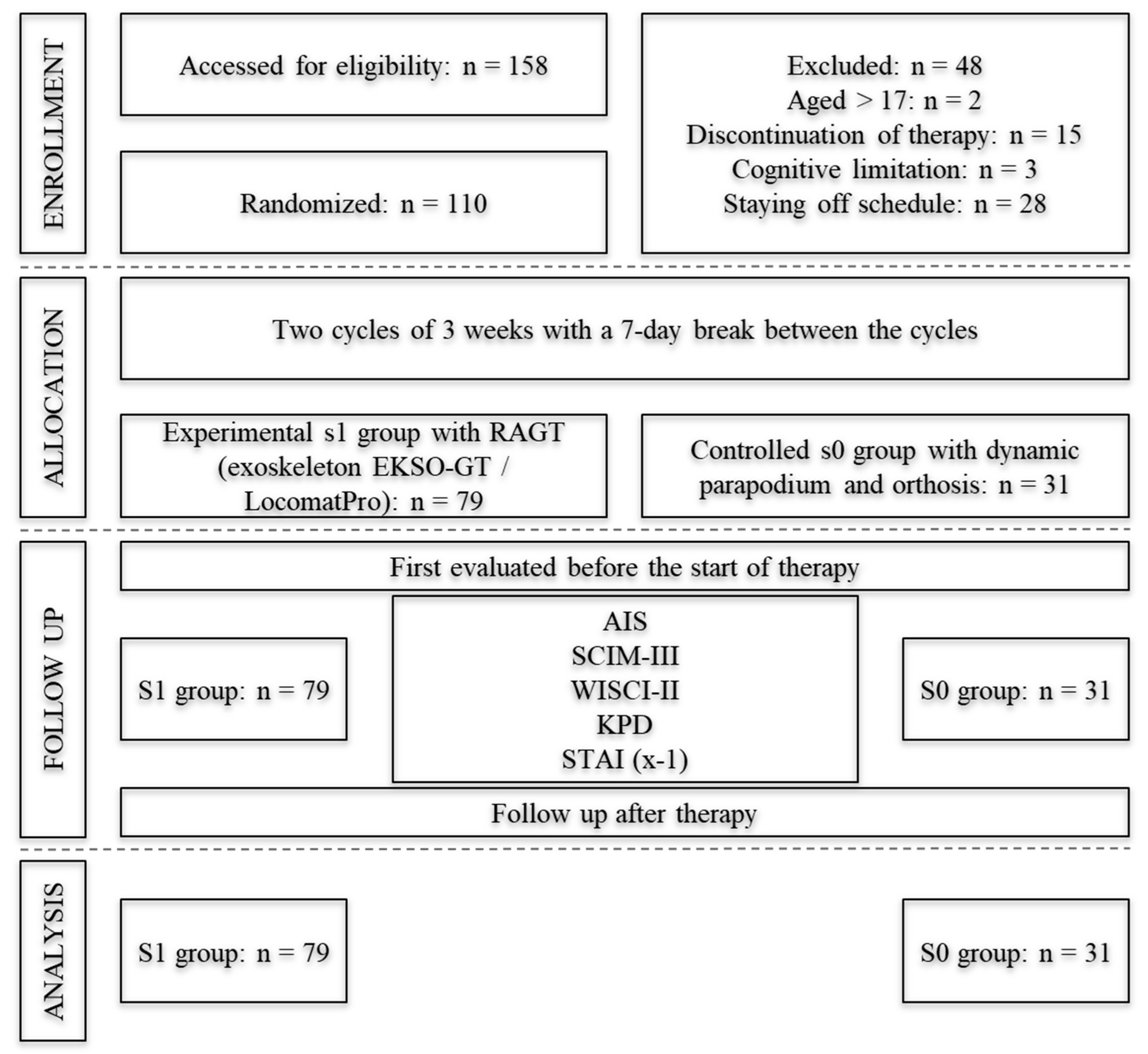
Patients self-reported from all over the country to participate in the study. They agreed to participate and signed an informed consent form before the study. Based on the criteria, three patients did not qualify for psychological testing. One of the subjects had moderate intellectual disabilities and two of them were under the age of 16 (scheme no.2).
A simple randomization method was used to assign patients to comparison groups. Random assignment to groups was done by an unaware of the study's purpose (a blinded investigator) medical staff member. The medical team, paramedical team and psychologist were unaware of the purpose of the study when performing treatment and therapeutic measures (single blinding).
The 110 patients completed the study; (79) of them were assigned to the S1 group participating in rehabilitation with RAGT including 62 men and 17 women and 31 to S0 group including 27 men and 4 women. The disproportion in the number of patients assigned to the control group was related to the fact that patients were quitting when they found out they had drawn a group without RAGT. Also, the situation caused by the COVID-19 pandemic folded that 11 patients in the S0 group did not complete the rehabilitation cycle. All patients had neurological impairment after SCI. Neurological impairment at the cervical level was possessed by 25% of patients in the S0 group and 20.3% in S1; at the thoracic level, 48.4 and 53.2%, respectively, and at the lumbar level, 25.8 and 26.6%.
Comparisons of the S0 and S1 groups with sociodemographic variables and other characteristic variables showed that there were no differences between the groups at the initial level. In both groups, the majority were men and people with higher education, in a formal relationship. The largest group was made up of respondents living in large cities. The most common cause of injury was a fall from a height of more than 1 meter. The main level of neurological damage was Th. The median age was 37 (S0) and 36 (S1), and for time since the accident, respectively: 13 and 12 months.
The Materials and Methods should be described with sufficient details to allow others to replicate and build on the published results. Please note that the publication of your manuscript implicates that you must make all materials, data, computer code, and protocols associated with the publication available to readers. Please disclose at the submission stage any restrictions on the availability of materials or information. New methods and protocols should be described in detail while well-established methods can be briefly described and appropriately cited.
Research manuscripts reporting large datasets that are deposited in a publicly available database should specify where the data have been deposited and provide the relevant accession numbers. If the accession numbers have not yet been obtained at the time of submission, please state that they will be provided during review. They must be provided prior to publication.
Interventionary studies involving animals or humans, and other studies that require ethical approval, must list the authority that provided approval and the corresponding ethical approval code.

Table 1.
Characteristics of the study group.
| Group | S0 (N = 31; 28.2%) | S1 (N = 79; 71.8%) | p-Value |
|---|---|---|---|
| Sex | |||
| Women | 4 (12.9%) | 17 (21.5%) | 0.301 |
| Men | 27 (87.1%) | 62 (78.5%) | |
| Education | |||
| In the course of education | 2 (6.5%) | 4 (5.1%) | 0.554* |
| Elementary | 0 (0.0%) | 2 (2.5%) | |
| Vocational | 6 (19.4%) | 7 (8.9%) | |
| Secondary | 6 (19.4%) | 19 (24.1%) | |
| Higher | 17 (54.8%) | 47 (59.5%) | |
| Accommodation | |||
| Countryside | 8 (25.8%) | 22 (28.6%) | 0.912 |
| Small town | 7 (22.6%) | 20 (26.0%) | |
| Medium-size town | 6 (19.4%) | 11 (14.3%) | |
| Big city | 10 (32.3%) | 24 (31.2%) | |
| Marital status | |||
| Lack of partner | 5 (16.1%) | 22 (27.8%) | 0.338 |
| Informal relationship | 5 (16.1%) | 15 (19%) | |
| Formal relationship | 21 (67.7%) | 42 (53.2%) | |
| Cause of injury | |||
| Vehicle accident | 12 (38.7%) | 24 (30.8%) | 0.089* |
| Fall < 1 m | 2 (6.5%) | 5 (6.4%) | |
| Fall > 1 m | 8 (25.8%) | 29 (37.2%) | |
| Dive | 2 (6.5%) | 2 (2.6%) | |
| Violence-related trauma | 0 (0.0%) | 1 (1.3%) | |
| Body crushing | 4 (12.9%) | 1 (1.3%) | |
| Others | 3 (9.7%) | 16 (20.5%) | |
| Level of neurological impairment | |||
| Cervical | 8 (25.8%) | 16 (20.3%) | 0.811 |
| Thoracic | 15 (48.4%) | 42 (53.2%) | |
| Lumbar | 8 (25.8%) | 21 (26.6%) | |
| Age | |||
| Median (IQR) | 37.0 (22) | 36 (23) | 0.666 |
| Time from accident (months) | |||
| Median (IQR) | 13 (13) | 12 (11) | 0.433 |
* – Fisher’s exact test.
The study flowchart is shown in Figure 1.
Figure 3.
The details flowchart of patients’ recruitment.
2.4. Outcome measures
2.4.1. Primary outcome measures
In the present analysis, the primary outcome measures were the overall depression severity scores and the anxiety severity-status measure, while the second-order indicators were the individual depression symptom severity scores and the scores for the level of functional independence and mobility of people after SCI and the gait function measure.
To estimate the severity of depression symptoms, the Depression Assessment Questionnaire (KPD) by E. Łojek, J. Stańczak, A. Wójcik was used. KPD measures the severity of depression and its individual symptoms and includes an additional scale to assess the subjects' self-regulatory abilities. Its theoretical basis is based on data on symptoms and mechanisms of depression in accordance with international diagnostic criteria. The Overall Score (WO) of the KPD indicates the general severity of depression. Possible scores range from 60 (no depression) to 240 (severe depression). A WO of 130 points is the cutoff between normal and a score suggestive of depressive disorders [61].
To measure anxiety as a state STAI - X1, by C.D. Spielberger, R.L. Gorsuch, R.E. Lushene was used. Anxiety - state understood as tension related to the current situation. Possible scores range from 20 (low anxiety) to 80 (high anxiety) [62].
2.4.2. Secondary outcome measures
Additional scales of the KPD were used to measure the severity of individual depressive symptoms. KPD consists of five scales, i.e. DPUE- Cognitive deficits and energy loss (it refers to symptoms associated with decreased learning performance, impaired attention and memory performance, as well as deterioration of psychomotor functions and loss of energy, the range of scores is from 19-76 points); MSPA - Thinking about death, pessimism and alienation (refers to the measurement of the severity of loss of meaning in life, social withdrawal and emotions with a negative sign, the lowest possible raw score is 15 and the highest is 60, indicating a very high severity of the described symptoms), PWNL - Guilt and anxiety tension (measures the severity of fear, anxiety and related emotional tension, the tendency to blame oneself for various situations, behaviors and thoughts, also allows to estimate the level of self-esteem and sense of social attractiveness, the score range is from 16 to 64), OPSZ- Psychosomatic symptoms and decline in interest (refers to the subjective assessment of one's somatic and mental health, also allows to determine the decrease in previous interests, anhedonia, the range of raw scores is from 10-40), SR- Self-regulation (is an additional scale used to measure the emotional and cognitive resources of the subjects protecting them from depression, the minimum number of points possible is 15 and the maximum is 60), the sum of the scores of the first four scales affects the overall score of the severity of symptoms associated with depression (WO) [61].
In order to diagnose and assess the neurological and functional status tests were conducted using: The AIS was used to assess motor and sensory functions; we divided patients according to AIS to A, B, C, D or E subgroups; where AIS A meant complete and AIS B, C and D incomplete SCI [63]. Walking Index for Spinal Cord Injury (WISCI-II) was used for measuring improvement in gait function of our patients after SCI. It is the most sensitive measure in terms of change in gait ability compared to other leading measurement scales [54]. The index provides an assessment of the level of gait function. A level of 0 indicates the inability to stand and participate in walking, and a level of 21 indicates the ability to walk without the use of aids, orthoses, and assistance from others [65]. The Spinal Cord Independence Measure, version III (SCIM-III) was used for functional assessment, because it is a reliable and accurate scale for assessing skills in daily functioning of patients with spinal cord injury, with proven adequacy in group studies [66], is the only comprehensive scale for assessing patients' performance in the ability to perform basic daily activities. Version III contains 19 tasks divided into three areas, i.e.: Self-care; Breathing and sphincter control; Mobility. The total score ranges from 0 (indicating total dependence) to 100 (indicating total independence) [67].
2.5. Statistical analyses
Initially, distributions were checked and descriptive statistics of quantitative variables were calculated. Normality of the distribution was tested with the Shapiro-Wilk test, but values of skewness and kurtosis were also considered. Due to violation of the assumptions of normal distribution and numerous outlier observations exceeding the third standard deviation, analyses were based on non-parametric tests.
Firstly, we checked the differences in anxiety-state and depression indicators between pre-rehabilitation vs post-rehabilitation measurements. Similarly, this analysis was conducted with the division into groups (S0 vs S1). In the next step, we were made between group comparison to the investigated and control group. Also checked differences in functional indices were tested as follows: WISCI-II and SCIM-III separately in the S0 and S1 groups, and for the change within these indices between the groups. As additions to previous analyses, comparisons were made between measurements of anxiety and depression before and after rehabilitation, as well as changes in anxiety and depression when divided into S0 and S1 groups, but also when divided into spinal cord injury classifications. In the analyses, the classification was merged into two groups: AIS A vs AIS B, C, D. In a further step, the differences between subjects with two types of paralysis: tetraplegia vs paraplegia, were checked for anxiety and depression. Not only the type of rehabilitation but also the classification of spinal cord injury was taken into account, hence four groups were compared: S0 AIS A, S0 AIS B,C,D, S1 AIS A, S1 AIS B, C, D. In the last section, we tested whether there were relationships between the change that occurred between measurements in functional indicators (WISCI-II, SCIM-III) and changes in mental health (STAI X-1, KPD). Within-group comparisons of quantitative variables were based on the Wilcoxon rank-sum sign test, while between-group comparisons were based on the Mann-Whitney-U test. Comparisons of nominal and ordinal variables for group characteristics were based on chi-square tests of independence along with Fisher's exact test. In addition, correlation analyses with Spearman's rho coefficient were performed to check the relationship between variables. The analyses were performed using the IBM SPSS Statistics package version 25.
3. Results
3.1. Severity of anxiety-state and depression after 7-weeks rehabilitation program.
The results provided in Table 2, the severity of the anxiety-state (Z = -6.20, p<0.001) and general depression symptoms (Z = 6.35, p<0.001) and all depression factors (DPUE, MSPA, PWLN, OPSZ) were significantly decreased, after the 7-week rehabilitation program, compared to the first measurement, regardless of the type of rehabilitation. The ability to self-regulate has also increased significantly. The moderate effect size of rehabilitation was obtained in both severity of depression (r = 0.42) and anxiety-state (r = 0.43). Similarly, a moderate effect size in PWLN depression factor and a weak effect size of rehabilitation in DPUE, MSPA, OPSZ and SR was obtained.
3.1.1. Differences in anxiety-state, depression and functionality in comparison to the type of rehabilitation.
The results in Table 3 showed a significant increase in all general depression symptoms, depression factors and anxiety-state after 7-weeks of rehabilitation in both the experimental and control group. In the RAGT group, the effect size of rehabilitation was moderate for anxiety and all KPD subscales except PWLN and SR. For PWLN and SR the weak effect size of RAGT rehabilitation was obtained.
Table 3 also showed the differences of results in functional scales tested as follows: WISCI-II and SCIM-III separately in the S0 and S1 subgroups. There was an improvement in clinical functioning tests in the S0 group in second measurement compared to the first. In the S1 group, there was also a significant improvement in patients' clinical functioning after RAGT rehabilitation, but with a greater effect in the WISCI-II scale (Z = -5.17; p < 0.001; ), as well as in SCIM-III scale (Z = 6.99; p < 0.001). The effect size of RAGT rehabilitation in the WISCI-II (r = 0.41) and SCIM-III (r = 0.56) scales were moderate. Intergroup comparisons (S0 vs. S1) in terms of functional impairment showed a greater improvement in the S1 group, but only for in WISCI-II scale. The effect size of RAGT rehabilitation was weak. There were no statistically significant differences for SCIM-III between S0 and S1 groups (Z = -0.69; p = 0.487).
3.1.2. Functional and mental status correlation
Table 4 showed relationships between the change that occurred between measurements in functional indicators (WISCI-II, SCIM-III) and changes in mental health (STAI X-1, KPD). There was no significant relationship between somatic and mental functioning changes.
3.2. Severity of anxiety-state and depression according to neurological impairment (AIS).
The anxiety and depression comparisons before and after rehabilitation, in all patients and subgroups according to AIS classification in Table 5 is provided. The results indicate a significant increase in self-regulation, and a decrease in anxiety and depression in both the experimental and control groups.
In the group of patients S0 and AIS A, there was a significant decrease in anxiety-state after rehabilitation with strong effect size (Z=-3.07; p=0.002; r=0.60). However, there were no significant differences between the measurements of general depressive symptoms (Z=-1.45; p=0.147). Among patients in the S0 group and AIS B, C, D the effects size of DPT for general depression score and MSPA subscale were strong. The impact of DPT on other depression factors (DPUE, PWLN, OPSZ and SR) was moderate. In the S1 and AIS A and S1 and AIS B, C, D groups, significant decreases were also observed at each depression and anxiety-state measurement. In the S1 group with AIS A, the effect size was weak for self-regulation (r = 0.26). The effect size of RAGT rehabilitation was moderate strength for the other KPD subscales (DPUE, MSPA, PWLN, OPSZ) and STAI -X. The S1 group and AIS B, C, D also showed statistically significant decreased in depression and anxiety symptoms between two measures and an increase in SR.
In addition, Table 5 presented a comparison of the groups AIS (AIS A vs AIS B, C, D) and depression and anxiety indicators separately in the S0 and S1 groups. It turns out, in the S0 group, a greater reduction for MSPA in AIS B, C, D than in AIS A, was observed (Z = -2.46; p = 0.014). The effect size of DPT is moderate (r = 0.45). There were no significant differences between the two groups in other KPD subscales (DPUE, PWLN, OPSZ, SR). In contrast, the comparison between the RAGT groups (AIS A vs. AIS B, C, D) showed that the severity of changes in anxiety and depression were quite similar. The groups did not differ in self-regulation.
3.3. Severity of anxiety-state and depression according to the type of paralysis.
In Table 6, the differences between subjects with two types of paralysis (tetraplegia vs paraplegia) for anxiety and depression indicators were checked..
The results indicated a significant decrease in the level of anxiety-state (Z = -5.40; p < 0.001; r = 0.40) and depression (Z = -5.59; p < 0.001; r = 0.42), including an increase in self-regulation ( Z = -2.95, p = 0.003, r = 0.22) among people with paraplegia. The effect size on SR is weak, while the effect on the other subscales of the KPD and STAI-X were moderate.
In patients with tetraplegia, there was a significant decrease in anxiety-state, and general depression indicators and MSPA, PWLN, OPSZ, and SR subscales. Only on the MSPA subscale, there were no significant differences between the two measurements. An increase in self-regulation after the rehabilitation program was obtained (Z = -3.48; p < 0.001). Among those with tetraplegia, there was also a decrease in the severity of symptoms related to depression and anxiety-state and an increase in self-regulatory capacity. The effect size was strong for SR, but moderate for the other KPD and STAI subscales. People with tetraplegia also showed a decrease in anxiety (Z = -3.08; p = 0.002) and in the total score for depression (Z = -3.07; p = 0.002) and other subscales, except for the DPUE index. In this group of patients, there was also an increase in self-regulation (Z = -3.48; p < 0.001) after rehabilitation. The effect was strong for SR, but moderate for other significant differences (i.e., general KPD scores, MSPA, PWLN, and OPSZ subscales) and for STAI X-1.
In the Table 6 the differences in anxiety and depression in groups with different types of paralysis is provided. The results indicate that subjects with paraplegia were characterized by a smaller increase in self-regulation compared to subjects with tetraplegia. The significant difference between groups were obtained with low size effect. No differences between groups were observed for the other KPD subscales (DPUE, MSPA, PWLN, OPSZ) and for anxiety - state.
4. Discussion
4.1. The impact of 7-weeks rehabilitation programme on severity of depression, anxiety-state and functionality
Our study showed a significant decrease in anxiety-state and symptoms of depression and an increase in self-regulation in patients in both groups (S0 and S1) after a 7-week rehabilitation program. However, no significant difference was observed between the groups according to the type of rehabilitation (RAGT vs. DPT). Although no differences were found between the types of rehabilitation (RAGT vs. DPT) in reducing the severity of anxiety-state and symptoms of depression, it can be speculated from the results that robotic rehabilitation may be particularly important for patients with complete spinal cord injury (AIS A). After robotic rehabilitation, a decrease in the severity of the anxiety - state and a decrease in the level of perceived symptoms of depression were observed in both patients with complete and incomplete SCI patients. In addition, we also noted no significant statistical association between functional independence and psychological factors. A statistically significant difference was observed only for the WISCI-II scale. Patients in the rehabilitation group with RAGT achieved greater improvement in gait function. We analyzed the association of medical parameters with psychological variables. We found the improvements in gait function (WISCI II) and functional independence (SCIM-III) were unrelated to improvements in depression (KPD), anxiety-state as a condition (STAI, X-1) and self-regulation (KPD) scores.
Both rehabilitation using RAGT and conventional rehabilitation using DPT appeared to have a similar relationship with the reduction of anxiety - state and symptoms of depression. The mechanism for reducing depression and anxiety symptoms could be related to general fitness and performance improvement after rehabilitation. SCI patients were recovered independence in everyday activities which improved the mood and reduced the severity of anxiety. In addition, rehabilitation and other regular exercise and physical activity are significantly associated with lower levels of stress and depressive symptoms, social participation and quality of life. They may also have a preventive effect on the decline in quality of life after spinal cord injury, primarily through their effect on reducing pain levels, as well as increasing feelings of control and mastery, improving fitness and performance [12,13]. It can also be assumed that improvement of anxiety-state and symptoms of depression is a natural process of recovery and adaptation to disability [68]. In addition, time since injury and adaptation to new living conditions through the introduction of practical training, such as independent use of a handicapped accessible car, improving wheelchair mobility, etc., may have a positive impact on the emotional and affective state of spinal cord injury patients.
The present study did not show an association between improvements in gait function and functional independence after SCI and anxiety and symptoms of depression. These aspects are not correlated, which may be partly explained by the patient's subjective assessment of their health. Perception of health and objective physical condition functional assess were not the same in SCI participations.
The results of a review and meta-analysis by den Brave, M., et.al. (2023) indicate that in randomized control trials, improvements in depression-related outcomes were observed after RAGT training [57]. Our result also differs from those obtained by Shahin et.al. (2017), who noted a statistically significant difference between subjects rehabilitated with RAGT and those rehabilitated using conventional methods with DPT. This discrepancy may be due to the use of a different measurement tool and the size of the study group [69]. The referenced study was conducted on a group of forty people (N=40) and depression was measured using the Beck Depression Inventory. Other meta-analyses and retrospective studies, however, indicate that there is insufficient evidence of an association between robotic rehabilitation and reductions in depression or improvements in quality of life [38]. However, our results are largely consistent with other reports indicating that all rehabilitation interactions have a beneficial effect on psychological well-being, emotional state and mood, lowering depressive symptoms. Many researchers emphasize that the most optimal results in re-educating gait and improving the overall functioning of patients with SCI are obtained in combination with conventional rehabilitation and the coordinated interaction of multiple specialists [57,69]. This is due, among other things, to the peculiarities of neurological disorders, the physical effects of which are multi-systemic, translating into psycho-sociological aspects.
4.2. Anxiety-state and depression status and neurological impairment, depth of injury and type of paralysis
Patients who participated in rehabilitation with the dynamic parapodium (S0) showed a statistically significant reduction only in the level of anxiety - state, while no improvement in symptoms of depression was observed in patients with complete SCI (AIS-A). As we emphasized above, patients rehabilitated with RAGT with complete SCI (AIS A) and incomplete impairment (AIS B,C,D) experienced a reduction in both anxiety-state and symptoms of depression, in contrast to patients with complete impairment (AIS A) who reported only a reduction in anxiety-state. It can be assumed that rehabilitation with RAGT allows patients with such a severe neurological condition to maintain an upright natural posture and to move their lower limbs for a longer period of time.
In the present study, there was also a significantly greater decrease in symptoms related to Thinking About Death and Feeling Alienated (moderate effect) in the control group among patients with incomplete spinal cord injury according to ASIA classification compared to those with complete injury (AIS A). Perhaps this can be explained by an improved neurological condition, which is important for greater mobility and independence. This allows patients to participate more in social life, and influences a higher level of satisfaction with life, hope, and plans for the future.
Additionally, we observed no significant differences between the groups by type of paralysis (paraplegia vs tetraplegia) in the reduction of anxiety - state and symptoms of depression. The only difference was in the increase in self-regulation when comparing improvement by type of paralysis, i.e. paraplegia vs. tetraplegia. The results showed a greater increase in self-regulation in people with tetraplegia. The higher increase in self-regulation abilities of people with tetraplegia can perhaps be explained by the initial low expectations of being able to change their condition resulting from the diagnosis received and low confidence in achieving rehabilitation goals. Medical and paramedical staff are geared to provide positive reinforcement, jointly setting motivating, satisfactory but realistic rehabilitation goals and giving hope of achieving them positively influences the growth of self-confidence, self-control and on the subjective belief of self-efficacy in coping [64]. Hopes for the coordinated rehabilitation program allow us to anticipate its implications in the psychological dimension in the form of a reduction in anxiety-state and depression, i.e. common symptoms co-occurring with spinal cord injury [16]. Psychological support and assistance is, according to many researchers, as important as rehabilitation in the quest to improve the quality of life of people with spinal cord injury [71].
4.3. General discussion
Our study showed that all study patients experienced less anxiety and depression-related symptoms after the 7-week rehabilitation program. However, we did not observe significant differences between the groups (DPT vs. RAGT). The data obtained allows us to assume that RAGT can be recommended to patients with severe neurological conditions and total spinal cord injury in the context of their emotional and affective state. Our research may also suggest that the perception of one's own health and the actual physical health may not be the same. We can also assume that psychological support during rehabilitation is an essential part of the process.
There are several limitations to this study. First and foremost are: 1) Patients for the study were self-recruited, which may have influenced the falsified representativeness of this group among the general population of people with spinal cord injury 2) disproportion of patients between the experimental and control groups, and those with complete and incomplete SCI injury; 3) lack of qualitative control and quantitative measurement of patient-reported fear of falling that they experienced during exoskeleton rehabilitation.
Future research should pay attention to the adaptation of the tools measure mental health status, tailored to special needs and difficulties of SCI patients or consider the validation of existing instruments in this group of patients. Very important research issues related to people with spinal cord injury that should be considered in future studies are: sexual problems, chronic pain, spastic tension vs. neuroticism and anxiety, the relationship of motivation level on the outcomes of rehabilitation progress, anxiety and depression among caregivers and families of people with SCI, social adaptation and socioeconomic functioning of patients after the end of institutional rehabilitation.
5. Conclusions
In conclusion, both types of rehabilitation (RAGT vs. DPT) appeared to be associated with a reduction in anxiety and depression-related symptoms. However, it can be assumed that rehabilitation with RAGT can be particularly useful for people with complete spinal cord injury (AIS A) and a serious neurological condition. Rehabilitation with RAGT contributes to strengthening the self-regulation ability of patients with tetraplegia.
Based on these preliminary results, RAGT can be recommended as additional rehabilitation method, especially for people with total spinal cord injury and severe neurological condition in order to improve their affect and mood (AIS-A).
Author Contributions
Conceptualization, A.W.S. and B.T.; methodology, A.W.S, B.T, B.K; software, A.W.S.; formal analysis, A.W.S; investigation, A.W.S; B.T; B.K.; data curation, A.W.S; B.T; B.K; writing—A.W.S; B.T; J.W draft preparation, A.W.S; B.T; J.W; writing—review and editing, B.T; J.W.; visualization, A.W.S.; supervision, B.T; J.W.; project administration, B.T; B.K.
Funding
This study was supported by a grant from the National Center for Research and Development, Poland (Nr POIR.01.01.01–00–0848/17–00).
Institutional Review Board Statement
Institutional Review Board Statement: The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of the District Medical Chamber in Szczecin (Poland) (Nr OIL-Sz/MF/KB/452/05/07/2018; Nr OIL-SZ/MF/KB/450/UKP/10/2018).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data sharing not applicable.
References
- Kumar, R., Lim, L., Mekary, R.A., Rattani, A., Dewan, M.C., Sharif, Y.S., Osorio-Fonseca, E., Park, K.B. (2018).Traumatic Spinal Injury: Global Epidemiology and Worldwide Volume. World Neurosurgery, 113: 345-363. [CrossRef]
- Tederko, P., Jagodziński, R., Krasuski, M., Tarnacka, B. (2017). People with Spinal Cord Injury in Poland, Country Report. American Journal of Physical Medicine & Rehabilitation, 96(2): 102–105.
- Wysocka, B.; Ślusarz, R., Haor, B. (2012). Epidemiology of spinal cord injury in the own material of the Emergency Room in Włocławek: A retrospective study. Neurological and Neurological Nursing [online], 1(3): 109-118.
- Holanda, L.J., Silva, P.M.M., Amorim, T.C., Lacerda, M.O., Simão, C.R., Morya, E.(2017). Robotic assisted gait as a tool for rehabilitation of individuals with spinal cord injury: a systematic review. Journal of NeuroEngineering and Rehabilitation, 14:126.
- Maggio, M.G., Naro, A., De Luca, R., Latella, D., Balletta, T., Caccamo, L., Pioggia, G., Bruschetta, D., Calabrò, R.S. (2022). Body Representation in Patients with Severe Spinal Cord Injury: A Pilot Study on the Promising Role of Powered Exoskeleton for Gait Training. Journal of Personalized Medicine, 12(4): 619. [CrossRef]
- Van Diemen, T., van Leeuwen, C., van Nes, I., Geertzen, J., Post M. (2017).Body Image in Patients with Spinal Cord Injury during Inpatient Rehabilitation. Archives of Physical Medicine and Rehabilitation, 98:1126–1131. [CrossRef]
- Craig, A., Tran, Y., Wijesuriya, N., Middleton, J. (2012). Fatigue and tiredness in people with spinal cord injury. Journal of Psychosomatic Research, 73(3):205-210. [CrossRef]
- Kalpakjian, C.Z., Toussaint, L.T., Albright, K.J., Bombardier, Ch.H., Krause, J.K., Tate, D.G. (2009). Patient health Questionnaire-9 in spinal cord injury: an examination of factor structure as related to gender. The Journal of Spinal Cord Medicine, 32(2):147-56. [CrossRef]
- Anderson, K.D. (2004). Targeting Recovery: Priorities of the Spinal Cord-Injured Population. Journal of Neurotrauma, 21(10): 1371-1383. [CrossRef]
- Le, J., Dorstyn, D. (2016). Anxiety prevalence following spinal cord injury: a meta-analysis. Spinal Cord, 54(8): 570–578. [CrossRef]
- Craig, A., Tran, Y., Middleton, J., (2009). Psychological morbidity and spinal cord injury: a systematic review. Spinal Cord, 47(2):108–114.
- Hicks, A.L., Martin, K.A., Ditor, D.S., Latimer, A.E., Craven, C., Bugaresti, J., McCartney, N. (2003). Long-term exercise training in persons with spinal cord injury: effects on strength, arm ergometry performance and psychological well-being. Spinal Cord, 41(1): 34 – 43.
- Swank, Ch., Holden, A., McDonald, L., Driver, S., Callender, L., Bennett, M., Sikka, S. (2022). Foundational ingredients of robotic gait training for people with incomplete spinal cord injury during inpatient rehabilitation (FIRST): A randomized controlled trial protocol. PLOS One,10;17(5):0267013. [CrossRef]
- Ong, B., Wilson, J.R., Henzel, M.K. (2020). Management of the Patient with Chronic Spinal Cord Injury. Medical Clinics of North America, 104(2):263-278. [CrossRef]
- Alizo, G., Sciarretta, J. D., Gibson, S., Muertos, K., Holmes, S., Denittis, F., Cheatle J., Davis J., Pepe, A. (2018). Multidisciplinary team approach to traumatic spinal cord injuries: a single institution’s quality improvement project. European Journal of Trauma and Emergency Surgery, 44(2), 245–250. [CrossRef]
- Craig, A., Perry K.N., Guest R., Tran Y., Dezarnaulds A., Hales A., Ephraums C., Middleton J. (2015). Prospective Study of the Occurrence of Psychological Disorders and Comorbidities After Spinal Cord Injury. Physical Medicine and rehabilitation, 96(8):1426-1434. [CrossRef]
- Fleerkotte, B. M., Koopman, B., Buurke, J. H., van Asseldonk, E. H. F., van der Kooij, H., & Rietman, J. S. (2014). The effect of impedance-controlled robotic gait training on walking ability and quality in individuals with chronic incomplete spinal cord injury: an explorative study. Journal of NeuroEngineering and Rehabilitation, 11(1):26. [CrossRef]
- Ditunno, P. L., Patrick, M., Stineman, M., & Ditunno, J. F. (2008). Who wants to walk? Preferences for recovery after SCI: a longitudinal and cross-sectional study. Spinal Cord, 46(7): 500–506. [CrossRef]
- Daunoraviciene, K., Adomaviciene, A., Svirskis, D., Griškevičius, J., Juocevicius, A. (2018). Necessity of early-stage verticalization in patients with brain and spinal cord injuries: Preliminary study. Technology and Health Care, 26(S2): 613–623. [CrossRef]
- Nordström, B., Nyberg, L., Ekenberg, L., Näslund, A. (2014). The psychosocial impact on standing devices. Disability and Rehabilitation: Assistive Technology, 9(4): 299–306. [CrossRef]
- Mirbagheri, M. M., Kindig, M., Xun Niu, Varoqui, D., Conaway, P. (2013). Robotic-locomotor training as a tool to reduce neuromuscular abnormality in spinal cord injury: The application of system identification and advanced longitudinal modeling. 2013 IEEE 13th International Conference on Rehabilitation Robotics (ICORR). [CrossRef]
- Moll, F., Kessel, A., Bonetto, A., Stresow, J., Herten, M., Dudda, M., Adermann, J. (2022). Use of Robot-Assisted Gait Training in Pediatric Patients with Cerebral Palsy in an Inpatient Setting—A Randomized Controlled Trial. Sensors, 22(24): 9946. [CrossRef]
- Ustinova, K., Chernikova, L., Bilimenko, A., Telenkov, A., Epstein, N.(2011). 85Effect of robotic locomotor training in an individual with Parkinson’s disease: a case report. Disability and Rehabilitation: Assistive Technology, 6(1): 77– 85. [CrossRef]
- Raigoso, D., Céspedes, N., Cifuentes, C.A., del-Ama, A.J., Múnera1, M. (2021). A Survey on Socially Assistive Robotics: Clinicians’ and Patients’ Perception of a Social Robot within Gait Rehabilitation Therapies. Brain Sciences., 11(6): 738. [CrossRef]
- https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfPCD/classification.cfm?ID=PHL; 02 june 2023.
- Duddy, D., Doherty, R.,Connolly,J., Loughrey,J., Condell,J., Hassan,D.,Faulkner, M. (2022). The Cardiorespiratory Demands of Treadmill Walking with and without the Use of Ekso GT™ within Able-Bodied Participants: A Feasibility Study. International Journal of Environmental Research and Public Health, 19(10): 6176. [CrossRef]
- Høyer, E., Opheim, A., & Jørgensen, V. (2020). Implementing the exoskeleton Ekso GTTM for gait rehabilitation in a stroke unit – feasibility, functional benefits and patient experiences. Disability and Rehabilitation: Assistive Technology, 17(4):1–7. [CrossRef]
- Swank, Ch., Sikka, S., Driver, S., Bennett, M., Callender, L. (2020). Feasibility of integrating robotic exoskeleton gait training in inpatient rehabilitation. Disabil Rehabil Assist Technol, 15(4):409-417. [CrossRef]
- Toderita, A., Vlase, S. (2020). Reliability Study on PUR Injection Machine. Procedia Manufacturing, 46: 885–890. [CrossRef]
- Federici, S., Meloni, F., Bracalenti, M., De Filippis, M. L. (2015). The effectiveness of powered, active lower limb exoskeletons in neurorehabilitation: A systematic review. NeuroRehabilitation, 37(3): 321–340. [CrossRef]
- Donati, A.R.C, Shokur, S., Morya, E., Campos, D.S.F., Moioli, R.C., Gitti, C.M., Augusto, P.B., Tripodi, S., Pires, C.G., Pereira, G.A., Brasil, F.L., Gallo, S., Lin, A.A., Takigami, A.K., Aratanha, M.A., Joshi, S., Bleuler, H., Cheng, G., Rudolph A., Nicolelis, M.A.L. (2016). Long-term training with a brain-machine Interface-based gait protocol induces partial neurological recovery in paraplegic patients. Scientific Reports, 6(1): 30383. [CrossRef]
- Hartigan, C., Kandilakis, C., Dalley, S., Clausen, M., Wilson, E., Morrison, S., Etheridge, S., Farris, R. (2015). Mobility Outcomes Following Five Training Sessions with a Powered Exoskeleton. Top Spinal Cord Inj Rehabil, 21(2):93-99. [CrossRef]
- Juszczak, M., Gallo, E., Bushnik, T. (2018). Examining the Effects of a Powered Exoskeleton on Quality of Life and Secondary Impairments in People Living With Spinal Cord Injury. Top Spinal Cord Inj Rehabil, 24(4): 336–342. [CrossRef]
- Rodríguez-Fernández, A., Lobo-Prat, J., & Font-Llagunes, J. M. (2021). Systematic review on wearable lower-limb exoskeletons for gait training in neuromuscular impairments. Journal of NeuroEngineering and Rehabilitation, 18(1):22. [CrossRef]
- Bragoni, M., Broccoli, M., Iosa, M., Morone, G., De Angelis, D., Venturiero, V., Coiro, P., Pratesi, L., Mezzetti, G., Fusco, A., Paolucci, S. (2013). Influence of psychologic features on rehabilitation outcomes in patients with subacute stroke trained with robotic-aided walking therapy. American Journal of Physical Medicine & Rehabilitation, 92(10):16 - 25. 10.1097/phm.0b013e3182a20a34.
- Kozlowski, A.J., Fabian, M., Lad, D., Delgado, A.D.. (2017). Feasibility and Safety of a Powered Exoskeleton for Assisted Walking for Persons With Multiple Sclerosis: A Single-Group Preliminary Study. Archives of Physical Medicine and Rehabilitation, 98(7):1300-1307. [CrossRef]
- Ozsoy-Unubol, T., Ata, E., Cavlak, M., Demir, S., Candan, Z., Yilmaz, F. (2021). Effects of Robot-Assisted Gait Training in Patients With Multiple Sclerosis: A Single-Blinded Randomized Controlled Study. Am J Phys Med Rehabi. 101(8):768-774. [CrossRef]
- Alashram, A. R., Annino, G., & Padua, E. (2021). Robot-assisted gait training in individuals with spinal cord injury: A systematic review for the clinical effectiveness of Lokomat. Journal of Clinical Neuroscience, 91: 260–269. [CrossRef]
- Straudi, S., Fanciullacci, Ch., Martinuzzi, C., Pavarelli, C., Rossi, B., Chisari, C., Basaglia, N. (2016). The effects of robot-assisted gait training in progressive multiple sclerosis: A randomized controlled trial. Mult Scler, 22(3):373-84. [CrossRef]
- Wier, L.M., Hatcher, M.S., Triche, E.W., Lo, A.C. (2011). Effect of Robot-Assisted Versus Conventional Body-Weight-Supported Treadmill Training on Quality of Life for People With Multiple Sclerosis. J. Rehabil. Res. Dev.48(4):483-92. [CrossRef]
- Middleton, J., Tran, Y., Craig, A. (2007). Relationship between quality of life and self-efficacy in persons with spinal cord injuries. Archives of Physical Medicine and Rehabilitation, 88(12):1643-8. [CrossRef]
- Shin, J. C., Kim, J. Y., Park, H. K., & Kim, N. Y. (2014). Effect of Robotic-Assisted Gait Training in Patients With Incomplete Spinal Cord Injury. Annals of Rehabilitation Medicine, 38(6): 719. [CrossRef]
- Ma, D.-N., Zhang, X.-Q., Ying, J., Chen, Z.-J., Li, L.-X. (2017). Efficacy and safety of 9 nonoperative regimens for the treatment of spinal cord injury. Medicine, 96(47): 8679. [CrossRef]
- Çinar, Ç., Yildirim, M.A., Öneş, K., Gökşenoğlu. G. (2021). Effect of robotic-assisted gait training on functional status, walking and quality of life in complete spinal cord injury. International Journal of Rehabilitation Research, 44(3): 262-268. [CrossRef]
- Mustafaoglu, R., Erhan, B., Yeldan, I., Gunduz, B., & Tarakci, E. (2020). Does robot-assisted gait training improve mobility, activities of daily living and quality of life in stroke? A single-blinded, randomized controlled trial. Acta Neurologica Belgica. 120(2):335-344. [CrossRef]
- Calabrò, R. S., Billeri, L., Ciappina, F., Balletta, T., Porcari, B., Cannavò, A., Pignolo, L., Manuli, A., Naro, A. (2022). Toward improving functional recovery in spinal cord injury using robotics: a pilot study focusing on ankle rehabilitation. Expert Review of Medical Devices, 19(1):83-95. [CrossRef]
- Miller, L., Zimmermann, A., & Herbert, W. (2016). Clinical effectiveness and safety of powered exoskeleton-assisted walking in patients with spinal cord injury: systematic review with meta-analysis. Medical Devices: Evidence and Research, 22(9):455-66. [CrossRef]
- Nam, K. Y., Kim, H. J., Kwon, B. S., Park, J.-W., Lee, H. J., & Yoo, A. (2017). Robot-assisted gait training (Lokomat) improves walking function and activity in people with spinal cord injury: a systematic review. Journal of NeuroEngineering and Rehabilitation, 14(1):24. [CrossRef]
- Schwartz, I., Meiner, Z. (2015). Robotic-Assisted Gait Training in Neurological Patients: Who May Benefit? Annals of Biomedical Engineering, 43(5): 1260–1269. [CrossRef]
- Stampacchia, G., Olivieri, M., Rustici, A., D’Avino, C., Gerini, A., Mazzoleni, S. (2020). Gait rehabilitation in persons with spinal cord injury using innovative technologies: an observational study. Spinal Cord, 58(9):988-997. [CrossRef]
- Zhang, L., Lin, F., Sun, L., Chen, Ch.(2022). Comparison of Efficacy of Lokomat and Wearable Exoskeleton-Assisted Gait Training in People With Spinal Cord Injury: A Systematic Review and Network Meta-Analysis. Front Neurol.13: 772660. [CrossRef]
- Calabrò, R.S., Reitano, S., Leo, A., De Luca, R., Melegari, C., PT, Bramanti, P. (2014). Can robot-assisted movement training (Lokomat) improve functional recovery and psychological well-being in chronic stroke? Promising findings from a case study. Functional Neurology, 29(2): 139–141.
- Hayes, S. C., James Wilcox, C. R., Forbes White, H. S., Vanicek, N. (2018). The effects of robot assisted gait training on temporal-spatial characteristics of people with spinal cord injuries: A systematic review. The Journal of Spinal Cord Medicine, 41(5): 529–543. [CrossRef]
- Mıdık, M., Paker, N., Buğdaycı, D., Mıdık, A.C. (2020). Effects of robot-assisted gait training on lower extremity strength, functional independence, and walking function in men with incomplete traumatic spinal cord injury. Turk J Phys Med Rehabil, 66(1):54-59. [CrossRef]
- Wan, Ch., Huang, S., Wang, X., Ge, P., Wang, Z., Zhang, Y., Li, Y., Su, B. (2023). Effects of robot-assisted gait training on cardiopulmonary function and lower extremity strength in individuals with spinal cord injury: A systematic review and meta-analysis. J Spinal Cord Med., 27:1-9. [CrossRef]
- Contreras-Vidal, J. L., A Bhagat, N., Brantley, J., Cruz-Garza, J. G., He, Y., Manley, Q., Nakagome Sh., Nathan K., Tan S.H., Zhu F., Pons, J. L. (2016). Powered exoskeletons for bipedal locomotion after spinal cord injury. Journal of Neural Engineering, 13(3): 031001. [CrossRef]
- den Brave, M., Beaudart, Ch., de Noordhout, B.M., Gillot, V., Kaux J-F. (2023). Effect of robot-assisted gait training on quality of life and depression in neurological impairment: A systematic review and meta-analysis. Clinical Rehabilitation, 37(7):876-890. [CrossRef]
- Rosado-Rivera, D., Radulovic, M., Handrakis, J. P., Cirnigliaro, C. M., Jensen, A. M., Kirshblum, S., Bauman, W.A., Wecht, J. M. (2011). Comparison of 24-hour cardiovascular and autonomic function in paraplegia, tetraplegia, and control groups: Implications for cardiovascular risk. The Journal of Spinal Cord Medicine, 34(4): 395–403. [CrossRef]
- Goulet, J., Richard-Denis, A., Thompson, C., Mac-Thiong, J.-M. (2018). Relationships between Specific Functional Abilities and Health-Related Quality of Life in Chronic Traumatic Spinal Cord Injury. American Journal of Physical Medicine & Rehabilitation, 98(1):14-19. [CrossRef]
- O’Shea, T. M., Burda, J. E., Sofroniew, M. V. (2017). Cell biology of spinal cord injury and repair. Journal of Clinical Investigation, 127(9): 3259–3270. [CrossRef]
- Łojek, E, Stańczak, J, Wójcik, A. The Depression Assessment Questionarie. Manual. Labolatory of Psychological Testing of the Polish Psychological Association: Warsaw, Poland, 2015.
- Wrześniewski, K., Jaworska, A., Sosnowski, T., Fecenec, D. State- Trait Anxiety Inventory. Polish adaptation of STAI. Manual. 4th.Laboratory of Psychological Testing of the Polish Psychological Association: Warsaw, Poland, 2011.
- Bell, W., Meyer, P.R., Edelstein, D. American Spinal Injury Association (ASIA). (1984). Paraplegia, 22 (1): 45-54. [CrossRef]
- Opera, J., Mehlich, K., Bielecki, A. Zastosowanie Indeksu Chodu po Urazie Rdzenia Kregowego- WISCI. Ortopedia. Traumatologia. Rehabilitacja, 9(2): 122-127.
- Lam, T., Noonan, V.K., Eng, J.J.A systematic review of functional ambulation outcome measures in spinal cord injury. (2008). Spinal Cord, 46(4):246–254. [CrossRef]
- Itzkovich, M., Shefler, H., Front, L., Gur-Pollack, R., Elkayam, K., Bluvshtein, V., Gelernter, I., Catz, A. (2018). SCIM III (Spinal Cord Independence Measure version III): reliability of assessment by interview and comparison with assessment by observation. Spinal Cord, 56(1): 46–51. [CrossRef]
- Itzkovich, M., Gelernter, I., Biering-Sorensen, F., Weeks, C., Laramee, M.T., Craven, B.C., Tonack, M., Hitzig, S.L., Glaser, E., Zeilig, G., Aito, S., Scivoletto, G., Mecci, M., Chadwick, R.J., El Masry, W.S., Osman, A., Glass, C.A., Silva, P., Soni, B.M., Gardner, B.P., Savic, G., Bergström, E.M., Bluvshtein, V., Ronen, J., Catz, A. (2007). The Spinal Cord Independence Measure (SCIM) version III: reliability and validity in a multi-center international study. Disability and Rehabilitation, 29(24):1926-33. [CrossRef]
- Wrona-Polanska, H. Psychological aspects of informing patients about illness. in. Kubacka-Jasiecka, D., Ostrowski, T. M. Psychological dimensions of health, crisis and disease, Jagiellonian University Publishing House, Edition I, Cracow, Polad, 2005.
- Shahin, A.A, Shawky, Sh.A., Rady, H.M., Effat, D.A., Abdelrahman, Sh.K., Mohamed, e., Awad, R. (2017). Effect of Robotic Assisted Gait Training on functional and psychological improvement in patients with Incomplete Spinal Cord Injury. Journal of Novel Physiotherapy and Physical Rehabilitation, 4(3):83-86. [CrossRef]
- Sin, N.L., Lyubomirsky, S. (2009). Enhancing well-being and alleviating depressive symptoms with positive psychology interventions: a practice-friendly meta-analysis. Journal of Clinical Psychology, 65(5):467-87. [CrossRef]
Table 2.
Changes in anxiety-state and depression across the study sample.
| Variables | The whole group | ||
|---|---|---|---|
| Baseline, Median (IQR) |
Final Median (IQR) |
size effect |
|
| STAI X-1 | 35.00 (13.00) | 31.00 (8.50) | 0.42*** |
| KPD | 89.00 (34.00) | 80.50 (29.50) | 0.43*** |
| DPUE | 29.00 (10.00) | 26.50 (7.50) | 0.35*** |
| MSPA | 19.00 (8.00) | 17.00 (5.50) | 0.35*** |
| PWLN | 27.00 (8.00) | 24.50 (10.00) | 0.43*** |
| OPSZ | 16.00 (7.00) | 13.00 (6.50) | 0.32*** |
| SR | 46.00 (8.00) | 49.00 (10.00) | 0.29*** |
Abbreviations: IQR – interquartile range; size effect: r. *** – p < 0.001; ** – p < 0.01; * p – < 0.05.
Table 3.
Changes in anxiety-state and depression accordingly and changes in functioning rates by type of rehabilitation.
Table 3.
Changes in anxiety-state and depression accordingly and changes in functioning rates by type of rehabilitation.
| Variables | S0 (n = 30) | S1 (n = 79) | S0 (n = 30) | S1 (n = 79) | size effect |
||||
|---|---|---|---|---|---|---|---|---|---|
| Baseline, Median (IQR) |
Final Median (IQR) |
size effect |
Baseline, Median (IQR) |
Final Median (IQR) |
size effect |
Change Median (IQR) |
Change Median (IQR) |
||
| STAI X-1 | 35.00 (13.00) | 31.00 (8.50) | 0.52*** | 32.00 (13.00) | 26.00 (5.00) | 0.39*** | 5.00 (0.00) | 4.00 (9.00) | 0.05 |
| KPD | 89.00 (34.00) | 80.50 (29.50) | 0.47*** | 85.00 (30.00) | 78.00 (26.00) | 0.42*** | 5.50 (12.00) | 6.00 (11.00) | 0.04 |
| DPUE | 29.00 (10.00) | 26.50 (7.50) | 0.42** | 27.00 (10.00) | 26.00 (8.00) | 0.32*** | 2.50 (5.00) | 2.00 (5.00) | 0.09 |
| MSPA | 19.00 (8.00) | 17.00 (5.50) | 0.38** | 19.00 (5.00) | 17.00 (4.00) | 0.34*** | 2.00 (3.75) | 1.00 (2.00) | 0.07 |
| PWLN | 27.00 (8.00) | 24.50 (10.00) | 0.40** | 25.00 (9.00) | 21.00 (8.00) | 0.45*** | 11.00 (8.25) | 10.00 (5.00) | 0.14 |
| OPSZ | 16.00 (7.00) | 13.00 (6.50) | 0.40** | 15.00 (6.00) | 14.00 (5.00) | 0.28*** | 1.50 (4.00) | 1.00 (4.00) | 0.12 |
| SR | 46.00 (8.00) | 49.00 (10.00) | 0.37** | 46.00 (7.00) | 47.00 (8.00) | 0.26** | 3.00 (4.25) | 2.00 (4.00) | 0.11 |
| WISCI | 0.00 (4.00) | 0.50 (5.75) | 0.26* | 2.00 (11.00) | 6.00 (15.00) | 0.41*** | 0.00 (0.00) | 0.00 (3.00) | 0.24* |
| SCIM | 63.50 (27.25) | 66.50 (22.25) | 0.50*** | 64.00 (20.00) | 70.00 (24.00) | 0.56*** | 4.00 (8.25) | 5.00 (7.00) | 0.07 |
Abbreviations: S0: control group; S1: experimental group; IQR - interquartile range. The change for SR was based on the P2-P1 difference, and P1-P2 for the others. Size effect: r. *** - p < 0.001; ** - p < 0.01; * p - < 0.05.
Table 4.
Correlations of functional change (SCIM and WISCI) with changes in mental health (STAI X-1 and KPD).
Table 4.
Correlations of functional change (SCIM and WISCI) with changes in mental health (STAI X-1 and KPD).
| S0 (n = 30) | S1 (n = 79) | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Change | |||||||||
| Change, STAI X-1 |
Change, KPD |
Change, STAI X-1 |
Change, KPD |
||||||
| rs | p | rs | p | rs | p | rs | p | ||
| SCIM | -0.29 | 0.152 | -0.16 | 0.422 | 0.17 | 0.233 | 0.08 | 0.573 | |
| WISCI | 0.03 | 0.902 | 0.04 | 0.841 | -0.02 | 0.870 | -0.15 | 0.281 | |
Table 5.
Changes in anxiety-state and depression according to rehabilitation type and spinal cord injury classification.
Table 5.
Changes in anxiety-state and depression according to rehabilitation type and spinal cord injury classification.
| S0 | ASIA-A (n = 13) | ASIA-B, C, D (n = 17) | ASIA-A | ASIA-B, C, D | ||||||
|
Baseline, Median (IQR) |
Final Median (IQR) |
size effect |
Baseline, Median (IQR) |
Final Median (IQR) |
size effect |
Change, Median (IQR) |
Change, Median (IQR) |
size effect |
||
| STAI X-1 | 32.00 (7.50) | 27.00 (7.50) | 0.60** | 38.00 (8.50) | 33.00 (11.50) | 0.48** | 5.00 (0.00) | 5.00 (6.50) | 0.07 | |
| KPD | 78.00 (20.50) | 78.00 (24.00) | 0.28 | 97.00 (38.50) | 84.00 (40.00) | 0.59*** | 4.00 (10.00) | 10.00 (16.50) | 0.34 | |
| DPUE | 27.50 (8.75) | 24.00 (9.00) | 0.37 | 35.00 (13.50) | 28.00 (13.50) | 0.47** | 2.00 (3.50) | 4.00 (7.50) | 0.25 | |
| MSPA | 16.00 (5.50) | 17.00 (3.50) | 0.07 | 21.00 (13.00) | 18.00 (10.50) | 0.56** | 0.00 (3.50) | 2.00 (4.00) | 0.45* | |
| PWLN | 23.50 (5.75) | 24.00 (8.50) | 0.37 | 28.00 (6.50) | 25.00 (11.50) | 0.44* | 11.00 (7.00) | 15.00 (9.50) | 0.16 | |
| OPSZ | 15.00 (4.50) | 13.00 (5.00) | 0.34 | 19.00 (8.50) | 12.00 (9.00) | 0.43* | 1.00 (5.00) | 2.00 (4.50) | 0.05 | |
| SR | 47.50 (5.25) | 49.00 (9.00) | 0.34 | 45.00 (11.50) | 48.00 (12.50) | 0.38* | 2.00 (4.50) | 3.00 (7.50) | 0.14 | |
| ASIA-A (n = 30) | ASIA-B, C, D (n = 49) | ASIA-A | ASIA-B, C, D | |||||||
| S1 | ||||||||||
|
Baseline, Median (IQR) |
Final Median (IQR) |
size effect |
Baseline, Median (IQR) |
Final Median (IQR) |
size effect |
Change, Median (IQR) |
Change, Median (IQR) |
size effect |
||
| STAI X-1 | 31.50 (11.50) | 26.00 (2.75) | 0.41** | 33.00 (12.00) | 26.00 (6.00) | 0.38*** | 4.00 (0.00) | 3.00 (8.50) | <0.01 | |
| KPD | 80.50 (33.75) | 75.50 (23.50) | 0.44** | 86.00 (27.00) | 79.00 (31.00) | 0.40*** | 6.00 (12.25) | 6.00 (10.00) | <0.01 | |
| DPUE | 26.50 (10.25) | 26.00 (5.75) | 0.30** | 28.00 (10.50) | 26.00 (10.50) | 0.33** | 2.00 (5.50) | 2.00 (4.00) | 0.04 | |
| MSPA | 17.00 (5.00) | 16.00 (4.00) | 0.39** | 19.00 (5.50) | 18.00 (4.50) | 0.32** | 1.00 (2.00) | 1.00 (2.00) | <0.01 | |
| PWLN | 24.50 (7.50) | 19.00 (7.50) | 0.44** | 26.00 (10.00) | 22.00 (10.00) | 0.44*** | 9.50 (6.00) | 11.00 (4.50) | 0.11 | |
| OPSZ | 14.00 (7.50) | 14.00 (5.25) | 0.30** | 15.00 (5.50) | 14.00 (5.50) | 0.27** | 1.00 (4.00) | 1.00 (4.00) | 0.02 | |
| SR | 47.00 (6.00) | 47.50 (9.00) | 0.26* | 44.00 (8.00) | 46.00 (9.50) | 0.25* | 1.50 (4.25) | 2.00 (4.50) | 0.04 | |
Abbreviations: S0: control group; S1: experimental group; IQR – interquartile range. The change for SR was based on the P2-P1 difference, and for the others P1-P2. Size effect: r. *** – p < 0.001; ** – p < 0.01; * p – < 0.05.
Table 6.
Changes in anxiety-state and depression depending on the type of paralysis.
| Variables | Paraplegia (n = 89) | Tetraplegia (n = 20) | Paraplegia (n = 89) | Tetraplegia (n = 20) | size effect |
||||
|---|---|---|---|---|---|---|---|---|---|
| Baseline, Median (IQR) |
Final Median (IQR) |
size effect |
Baseline, Median (IQR) |
Final Median (IQR) |
size effect |
Change Median (IQR) |
Change Median (IQR) |
||
| STAI X-1 | 33.00 (13.00) | 26.00 (7.00) | 0.40*** | 35.00 (13.50) | 28.00 (6.75) | 0.49** | 4.00 (0.00) | 3.50 (8.75) | <0.01 |
| KPD | 86.00 (29.00) | 79.00 (25.50) | 0.42*** | 92.00 (35.50) | 81.50 (31.00) | 0.49** | 6.00 (13.00) | 7.00 (8.50) | <0.01 |
| DPUE | 28.00 (9.50) | 26.00 (7.00) | 0.36*** | 27.00 (13.00) | 25.00 (13.50) | 0.28 | 2.00 (4.50) | 1.50 (5.50) | 0.06 |
| MSPA | 19.00 (5.50) | 17.00 (4.00) | 0.35*** | 18.00 (6.50) | 18.00 (4.00) | 0.32* | 1.00 (2.00) | 0.50 (3.50) | 0.06 |
| PWLN | 26.00 (8.50) | 22.00 (8.50) | 0.43*** | 25.00 (11.00) | 23.00 (10.75) | 0.47** | 10.00 (6.00) | 10.50 (7.00) | 0.03 |
| OPSZ | 15.00 (6.50) | 13.00 (5.00) | 0.30*** | 16.00 (7.50) | 14.00 (5.50) | 0.41** | 1.00 (4.00) | 2.00 (3.75) | 0.11 |
| SR | 46.00 (9.00) | 47.00 (10.00) | 0.22** | 46.00 (7.00) | 49.00 (8.75) | 0.55*** | 1.00 (4.00) | 3.00 (5.50) | 0.20* |
Abbreviations: S0: control group; S1: experimental group; IQR - interquartile range. The change for SR was based on the P2-P1 difference, and P1-P2 for the others. Size effect: r. *** - p < 0.001; ** - p < 0.01; * p - < 0.05.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



