
Submitted:
30 August 2023
Posted:
31 August 2023
You are already at the latest version
Abstract
Sleep-disordered breathing is a significant problem affecting the pediatric population. These conditions can affect sleep quality and significantly affect children's overall health and well-being. Difficulties in social interaction, communication, and repetitive behavioral patterns characterize autism spectrum disorder. Sleep disturbances are common in children with ASD. This literature review aims to gather and analyze available studies on the relationship between SDB and children with autism spectrum disorder. We comprehensively searched the literature using major search engines (PubMed, Scopus, and Web of Science). After removing duplicates, we extracted a total of 96 records. We selected 19 studies for inclusion after a thorough title and abstract screening process. A total of 7 articles were ultimately included. This review has analyzed the relationship between autism spectrum disorder and sleep-disordered breathing, particularly Obstructive Sleep Apnea, highlighting an intriguing web of complex associations. Some studies involving children have demonstrated a significant association between autism spectrum disorder and the presence of Obstructive Sleep Apnea. Furthermore, a heightened risk of developing sleep disturbances, including sleep-disordered breathing, has emerged in children with autism. The risk and prevalence of obesity are increasing in pediatric subjects with autism spectrum disorder. Obesity has been identified as a predictive factor for Sleep-disordered breathing, and Body Mass Index can directly correlate with Obstructive Sleep Apnea in these children. Adenotonsillectomy has proven to be pivotal in improving behavioral issues in autism spectrum disorder children with obstructive Sleep Apnea. In conclusion, this review underscores the complexity of the interplay between autism spectrum disorder and sleep-disordered breathing, emphasizing the importance of further research to understand underlying mechanisms and develop optimal therapeutic and preventative approaches to enhance sleep quality and overall health in children with autism spectrum disorder.
Keywords:
autism spectrum disorder
; children
; sleep apnea
; sleep-disordered breathing
; sleep quality
1. Introduction
Sleep-disordered breathing (SDB) represents a significant issue affecting the pediatric population [1,2]. These conditions can have severe consequences on the health and well-being of children [1,3,4].
In the broader context, independent risk factors for Obstructive Sleep Apnea Syndrome (OSAS) encompass persistent snoring for ≥ 3 months, tonsillar and adenoid hypertrophy, and obesity (Xu et al., 2020). Moreover, the presence of frequent respiratory infections [5] may amplify the impact, particularly when coupled with factors such as tonsillar and adenoid hypertrophy or obesity. Muscle hypotonia in children with genetic comorbidities [6,7,8] may serve as concurrent catalysts exacerbating SDB. The intricate interplay of SDB can orchestrate disruptions in sleep patterns and intermittent hypoxia, exerting a discernible impact on the cognitive and behavioral faculties of children [9,10,11]. Consequently, delving into the long-term trajectories of these disorders and maintaining vigilant follow-up mechanisms becomes an imperative [1,12].
Neurodevelopmental disorders constitute a wide-ranging category of medical conditions that profoundly impact the intricate development of the nervous system, particularly during the critical phases of brain maturation. The delicate interplay of factors shaping proper nervous system development intertwines with the multifaceted complexities characterizing the manifestation of ASD during the crucial stages of childhood or infancy [13,14,15], explores the nuanced aspects of the condition. The resulting impact reverberates across a comprehensive spectrum of domains, encompassing the intricate threads of communication, the fabric of learning, the dance of social behavior, and the tapestry of motor skills. While ASD maintains its distinct identity with unique attributes, acknowledging the latent potential for multiple neurodevelopmental disorders to converge within the presentation of children remains of paramount significance [16,17,18].
Aims of the study
This study aims to explore the current understanding of the intricate relationship between ASD and SDB in children, the underlying mechanisms, and the importance of early detection and intervention for SDB in children with ASD. The study seeks to illuminate how early interventions can enhance sleep quality, address behavioral challenges, and improve the overall well-being of affected children.
2. Materials and Methods
We conducted a literature search using major search engines (PubMed, Scopus, and Web of Science; access date July 15, 2023), employing the relevant keywords listed below:
PubMed: (" autism spectrum disorders" OR " autism" OR "autistic" OR “Asperger” OR “Pervasive developmental disorder”) AND ("sleep-disordered breathing" OR "sleep apnea" OR "sleep apnoea" OR "sleep disorders breathing") AND ("Polysomnography" OR "Treatment outcomes" OR "Complications") AND ("Children" OR "Pediatric patients" OR "infant")
Scopus: (TITLE-ABS-KEY(" autism spectrum disorders") OR TITLE-ABS-KEY(" autism") OR TITLE-ABS-KEY("autistic") OR TITLE-ABS-KEY("Asperger") OR TITLE-ABS-KEY("Pervasive developmental disorder")) AND (TITLE-ABS-KEY("sleep disordered breathing") OR TITLE-ABS-KEY("sleep apnea") OR TITLE-ABS-KEY("sleep apnoea") OR TITLE-ABS-KEY("sleep disorders breathing")) AND (TITLE-ABS-KEY("polysomnography") OR TITLE-ABS-KEY("treatment outcomes") OR TITLE-ABS-KEY("complications")) AND (TITLE-ABS-KEY("children") OR TITLE-ABS-KEY("pediatric") OR TITLE-ABS-KEY("infant"))
WebOfScience: TS=(" autism spectrum disorders" OR " autism" OR "autistic" OR "Asperger" OR " Pervasive developmental disorder") AND TS=(“sleep-disordered breathing" OR "sleep apnea" OR "sleep apnoea" OR "sleep disorders breathing") AND TS=("Polysomnography" OR "Treatment outcomes" OR "Complications") AND TS=("Children" OR "Pediatric" OR “infant”).
Inclusion and exclusion criteria
The inclusion criteria comprised the pediatric age group, autism, autistic, pervasive, sleep apnea, SDB, OSA, and PSG. Exclusion criteria encompassed non-English articles, reviews, case reports, case series, or letters, studies focusing on adults (>18 years), studies lacking specific outcome reporting, and duplicate studies (i.e., those published multiple times or identified from different data sources).
3. Results
Ninety-six records were initially identified, accounting for duplicates. Through a meticulous screening of titles and abstracts, we narrowed our selection to 19 studies that aligned with our research objectives. Subsequently, we comprehensively evaluated these studies to ascertain their relevance and quality. Following this procedure, we ultimately incorporated 7 articles (Figure 1).
Four studies have examined SDB within the broader context of sleep disorders in children with ASD (Table 1). Youssef et al. investigated the relationship between ferritin levels, fragmented sleep, and joint movements in children [19]. Tudor et al. explored the correlation between pain and sleep problems [20]. Elrod et al. delved into the risk of sleep disorders associated with diagnostic/surgical procedures in children [21]. Johnson et al. explored the psychometric properties of the Sleep Subscale of the CSHQ [22]. Three studies (Table 1) specifically focused on OSA. Murata et al. examined behavioural changes following tonsillectomy and adenoidectomy interventions [23]. Tomkies et al. investigated predictors of OSA and severe OSA, along with demographic and clinical characteristics [24]. Additionally, a study compared OSA symptoms and the age of diagnosis [25].
Studies investigating the relationship between SDB and children with ASD have employed various methodologies and involved diverse subject groups. The survey conducted by Youssef et al. included a large population of children with ASD, analyzing participant data for ferritin levels and PSG data [19]. Tudor et al. evaluated parent-reported sleep habits using the CSHQ questionnaire. They examined correlations between pain and sleep disorders, including SDB, to understand the impact of pain on sleep quality [20]. Elrod et al. analyzed ASD data from a broad sample of children, comparing it to a control group. They assessed the risk rates of sleep disorders and SDB. Johnson et al. evaluated sleep habits and SDB using the CSHQ, and studied psychometric properties [21]. Murata et al. investigated OSA in children with and without ASD using PSG, assessing behavioural changes before and after treatment [23]. Tomkies et al. performed PSG on children, examining predictors of OSA and considering demographic and clinical variables [24]. Santapuram et al. reviewed clinical records, looking at diagnoses and treatments for SDB [25]. In summary, through diverse methodologies such as PSG analysis, the CSHQ questionnaire, ICD-9-CM data, and clinical assessments, these studies have delved into the intricate relationship between SDB and ASD, revealing crucial aspects of this dynamic.
SDB represents a complex study area for children with ASD and has brought forth several significant findings. In the first study by Youssef et al. ferritin levels and BMI were not significantly correlated with OSA. This lack of association suggested that different factors might contribute to the onset of SDB in this population [19]. On the other hand, the investigation by Tudor et al. revealed that sleep behaviours and vocalizations could influence scores on the SDB subscale of the CSHQ. This finding suggests that SDB might be associated with specific vocal behaviours and overall sleep quality [20]. Elrod et al. uncovered a higher risk of developing sleep disorders, including OSA, in children with ASD [21]. These results underscore the need for timely assessment and intervention to address such respiratory disorders. However, despite the association between ASD and SDB, loud snoring and other abnormal breathing behaviours were only rarely found in the children examined in Johnson et al.'s study [22]. This suggests that while sleep disorders are essential to consider, they might vary significantly in frequency and presentation. The findings from Murata et al. highlighted the effect of OSA on behaviours and overall well-being of children with ASD. OSA treatment emerged as a crucial element for improving behavioural issues [23]. Irrespective of obesity and age, the extent of the scope of OSA was further explored in the study by Tomkies et al., which revealed that OSA is common in children with ASD and can vary significantly in severity. Obesity emerged as a significant predictive factor, particularly for severe OSA [24]. Lastly, Santapuram et al. examined the association between autism severity, age at diagnosis, and factors like BMI in the context of OSA [25]. While the initial association between autism severity and age at OSA diagnosis did not prove statistically significant when accounting for other factors, both BMI and age at autism diagnosis appear to contribute to the age at OSA diagnosis independently.
In the final phase of the selection process, we also reviewed studies investigating the relationship between ASD and sleep disturbances, although not directly related to SDB (Table 2). These studies were excluded because they focused on distinct strategies to enhance sleep quality and treatments for insomnia associated with ASD, rather than respiratory conditions. Additionally, these studies explored general sleep difficulties and interventions to address them without specifically highlighting SDB.
Delemere and Dounavi investigated strategies to enhance sleep quality, concentrating on the effectiveness of 'bedtime fading' to improve sleep duration and latency [32]. In contrast, McCrae et al. showcased the effectiveness of cognitive-behavioural therapy in treating insomnia linked to autism [35]. Gender discrepancies in sleep disturbances within the autistic spectrum were examined by Estes et al., uncovering distinct sleep-related challenges encountered by females with ASD and revealing associations between heightened anxiety and sleep disturbances in males with ASD [36].
Miano and Ferri demonstrated that sleep issues in children with ASD mirror those found in typically developing children, albeit with higher frequency. These problems can be tackled through medication and behavioural approaches [26]. Notably, the utilization of melatonin as a potential solution has garnered attention. Wright et al. showcased melatonin's safe and influential role in enhancing insomnia and sleep duration [28]. Giannotti et al. identified sleep alterations in non-regressive autism with implications for managing insomnia [27]. Additionally, Silveira Cruz-Machado et al. delved into the intricate connection between sleep, immunity, and autism, proposing a potential role for melatonin [34]. The use of supplements, such as carnosine, as a possible treatment approach was also discussed by Mehrazad-Saber et al. [31].
Sleep disturbances pose a significant challenge for children with ASD, impacting their behaviours and overall well-being. Addressing these issues is essential to enhance their quality of life. Research has illuminated various strategies, including 'bedtime fading' and cognitive-behavioural therapy, to improve sleep in this population. Moreover, therapeutic interventions such as melatonin and supplements like carnosine offer promising avenues to manage sleep disturbances. With an advancing understanding of the complex interaction between sleep and ASD, further studies and personalized interventions will undoubtedly pave the way for improved sleep outcomes and enhanced overall well-being for individuals on the autism spectrum.
4. Discussion
Research on the effects of SDB or OSA in children with ASD has revealed significant insights (Figure 2). One study demonstrated that 34% of children with ASD (n=53, age 7.5 [4.8, 12.8] years) were diagnosed with OSA through PSG [19]. Another study reported that children with ASD (age 4.7±1.14 years) who snore occasionally account for 25.4%, and those who snore constantly are 5.1%. Children experiencing sleep apnea occasionally are 3.5%, and those experiencing it frequently are 0.6%, according to the CSHQ [22]. An elevated susceptibility to the development of sleep disorders, encompassing OSA, has been documented. The risk of sleep disorders in autistic children is increased by 96% compared to non-autistic children. Furthermore, children with ASD are also at a higher risk of undergoing PSG (increased by 274% compared to the control group) and ENT surgery (increased by 50% compared to the control group) [21]. Among 45 children with ASD (age 6.1±2.8 years), 58% had OSA diagnosed through PSG, and 33% were obese [24].
The incidence of obesity in children with ASD is at least as high as, or even higher than, the incidence in the general population of children. Risk factors for a high BMI have been identified as advanced child age, high maternal BMI, low physical activity, and an increased likelihood of food selectivity [38]. Obesity has been identified as a predictive factor for SDB (OR 1.04, 95% CI 1.0–1.08, P = 0.02), especially for severe OSA, in children with ASD [24]. Moreover, the risk and rate of obesity in pediatric individuals with ASD are elevated [39], with causes primarily attributed to sedentary lifestyles and improper dietary habits [40]. A study found that ferritin levels and BMI in children with ASD (n=53, age 7.5 [IQR 4.8, 12.8] years) were not significantly correlated with OSA, suggesting the presence of other influential factors [19]. Another study indicated that BMI and age of autism diagnosis could independently impact the generation of OSA diagnosis [25]. The treatment of OSA (diagnosed through PSG) with A&T has been crucial in improving behavioural issues, regardless of the child's obesity and age [23].
OSA negatively impacts behaviours and overall well-being in children with ASD [23]. A study found a correlation between the number of pain-related behaviours exhibited in the previous week. It increased overall sleep-related problems, specifically shorter sleep duration, parasomnias (sleepwalking or nightmares), and SDB [20]. Some researchers have concluded that children with ASD are more likely to receive a sleep disorder diagnosis, including SDB, and are more prone to undergo related diagnostic and surgical procedures than controls without ASD [21].
Investigations are currently in progress to delve into the potential connection between connective tissue irregularities and ASD; however, the precise nature of the relationship between these two factors remains incompletely understood. Altered connectivity can lead to phenomena of heightened sensitivity to environmental stimuli. Compared to healthy subjects, asthma and allergic rhinitis have a prevalence of 5:1 in ASD [41]. Frequent episodes of interstitial inflammation, immune-mediated forms of allergic asthma, bronchial hyperreactivity, nasal secretion, and nasal obstruction sensation have been observed following exposure to environmental allergens [42,43]. Nonetheless, a direct linear relationship between the extent of nasal obstruction and the intensity of SDB is absent. In most cases presenting moderate or severe OSA, nasal obstruction is not the primary underlying factor [44].
Hypermobility has quite a high prevalence in ASD, to the point that authors tend to include autism among hypermobility spectrum disorders (HSD) [43]. Recognizing the differences between muscle weakness (hypotonia), tendon laxity, and joint hypermobility is complex, especially when dealing with individuals with autism is an important issue [43,45]. However, hypotonia is also a recognizable marker of ASD [46]. Hypotonia is when children have very "soft" or flaccid muscle tone. The hypotonia observed was classified as mild to moderate and exhibited a widespread distribution across the entire body. Hypotonia was the most common motor symptom in a cohort of 154 children with ASD (51%), and it appears to improve over time. In the 2–6 year-old group, the prevalence of hypotonia was approximately 63% [45] at the age in which there is a high prevalence of SDB mainly due to adenotonsillar hypertrophy [47,48]. In general, the atonia of skeletal muscles present during REM sleep might be exacerbated by the underlying hypotonia in children [49], and in ASD might increase the risk of OSA. When muscles are not adequately toned, the airways can become more collapsible.
This review has analysed the relationship between ASD and SDB, particularly OSA, highlighting an intriguing landscape of complex correlations. Numerous research studies have established a notable correlation between ASD and the occurrence of OSA, with reported prevalence rates spanning from 34% to 58% [19,24]. Additionally, a higher risk of developing sleep disorders, including OSA, has been observed in children with ASD [21]. The risk and rate of obesity are increasing in pediatric individuals with ASD [24,39,40]. Obesity has been identified as a predictive factor for SDB, and BMI may be directly correlated with OSA in these children [19,25]. Surgical intervention via A&T has proven crucial in improving behavioural issues in children with ASD affected by OSA [23].
Children diagnosed with ASD might experience challenges in tolerating PSG [50,51] or discomfort sleeping in a different environment from their bed. However, some steps can help reduce anxiety during the PSG procedure, such as providing a detailed explanation of the procedure, identifying the child's strengths, using accessories that reflect the child's interests, and allowing family members to be present during the process to reduce anxiety, and paying close attention to the child's needs. It is important to note that if a child cannot undergo PSG due to their condition, there are alternative methods for assessing SDB for the development of an appropriate therapeutic plan [51,52,53].
5. Conclusions
In conclusion, this review has highlighted the complex interplay between ASD and SDB, underscoring the need for further research to understand the underlying mechanisms. The study's findings also emphasise the importance of early identification and treatment of SDB in children with ASD. SDB can significantly impact a child's physical and mental health, and early intervention can help improve sleep quality, reduce behavioural problems, and improve overall well-being.
Author Contributions
Conceptualization, M.Z. and L.Z.; methodology, M.Z.; validation, G.P., L.N. and L.Z.; formal analysis, M.Z.; investigation, M.Z.; writing—original draft preparation, M.Z. and L.Z.; writing—review and editing, G.P. and L.N..; visualization, L.N.; supervision, G.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data sharing not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Nosetti, L.; Zaffanello, M.; Katz, E.S.; Vitali, M.; Agosti, M.; Ferrante, G.; Cilluffo, G.; Piacentini, G.; La Grutta, S. Twenty-year follow-up of children with obstructive sleep apnea. J Clin Sleep Med 2022, 18, 1573–1581. [Google Scholar] [CrossRef]
- Nosetti, L.; Zaffanello, M.; De Bernardi, F.; Piacentini, G.; Roberto, G.; Salvatore, S.; Simoncini, D.; Pietrobelli, A.; Agosti, M. Age and Upper Airway Obstruction: A Challenge to the Clinical Approach in Pediatric Patients. Int J Environ Res Public Health 2020, 17. [Google Scholar] [CrossRef]
- Brockmann, P.E.; Gozal, D. Neurocognitive Consequences in Children with Sleep Disordered Breathing: Who Is at Risk? Children (Basel) 2022, 9. [Google Scholar] [CrossRef]
- Zaffanello, M.; Piacentini, G.; La Grutta, S. The cardiovascular risk in paediatrics: the paradigm of the obstructive sleep apnoea syndrome. Blood Transfus 2020, 1–9. [Google Scholar] [CrossRef]
- Nino, G.; Restrepo-Gualteros, S.M.; Gutierrez, M.J. Pediatric sleep apnea and viral respiratory infections: what do clinicians need to know? Expert Rev Respir Med 2022, 16, 253–255. [Google Scholar] [CrossRef] [PubMed]
- Khayat, A.; Bin-Hassan, S.; Al-Saleh, S. Polysomnographic findings in infants with Pierre Robin sequence. Ann Thorac Med 2017, 12, 25–29. [Google Scholar] [CrossRef]
- Schaefer, J.; Davey, M.J.; Nixon, G.M. Sleep-disordered breathing in school-aged children with Prader-Willi syndrome. J Clin Sleep Med 2022, 18, 1055–1061. [Google Scholar] [CrossRef]
- Hill, C.M.; Evans, H.J.; Elphick, H.; Farquhar, M.; Pickering, R.M.; Kingshott, R.; Martin, J.; Reynolds, J.; Joyce, A.; Rush, C.; et al. Prevalence and predictors of obstructive sleep apnoea in young children with Down syndrome. Sleep Med 2016, 27-28, 99–106. [Google Scholar] [CrossRef]
- Hunter, S.J.; Gozal, D.; Smith, D.L.; Philby, M.F.; Kaylegian, J.; Kheirandish-Gozal, L. Effect of Sleep-disordered Breathing Severity on Cognitive Performance Measures in a Large Community Cohort of Young School-aged Children. Am J Respir Crit Care Med 2016, 194, 739–747. [Google Scholar] [CrossRef]
- Menzies, B.; Teng, A.; Burns, M.; Lah, S. Neurocognitive outcomes of children with sleep disordered breathing: A systematic review with meta-analysis. Sleep Med Rev 2022, 63, 101629. [Google Scholar] [CrossRef]
- Zaffanello, M.; Ferrante, G.; Zoccante, L.; Ciceri, M.L.; Nosetti, L.; Tenero, L.; Piazza, M.; Piacentini, G. Predictive Power of Oxygen Desaturation Index (ODI) and Apnea-Hypopnea Index (AHI) in Detecting Long-Term Neurocognitive and Psychosocial Outcomes of Sleep-Disordered Breathing in Children: A Questionnaire-Based Study. J Clin Med 2023, 12. [Google Scholar] [CrossRef]
- Harris, V.C.; Links, A.R.; Kim, J.M.; Walsh, J.; Tunkel, D.E.; Boss, E.F. Follow-up and Time to Treatment in an Urban Cohort of Children with Sleep-Disordered Breathing. Otolaryngol Head Neck Surg 2018, 159, 371–378. [Google Scholar] [CrossRef]
- Zaffanello, M.; Zamboni, G.; Fontana, E.; Zoccante, L.; Tatò, L. A case of partial biotinidase deficiency associated with autism. Child Neuropsychol 2003, 9, 184–188. [Google Scholar] [CrossRef] [PubMed]
- Noto, A.; Fanos, V.; Barberini, L.; Grapov, D.; Fattuoni, C.; Zaffanello, M.; Casanova, A.; Fenu, G.; De Giacomo, A.; De Angelis, M.; et al. The urinary metabolomics profile of an Italian autistic children population and their unaffected siblings. J Matern Fetal Neonatal Med 2014, 27 Suppl 2, 46–52. [Google Scholar] [CrossRef]
- Hodges, H.; Fealko, C.; Soares, N. Autism spectrum disorder: definition, epidemiology, causes, and clinical evaluation. Transl Pediatr 2020, 9, S55–s65. [Google Scholar] [CrossRef]
- Morris-Rosendahl, D.J.; Crocq, M.A. Neurodevelopmental disorders-the history and future of a diagnostic concept. Dialogues Clin Neurosci 2020, 22, 65–72. [Google Scholar] [CrossRef]
- Posar, A.; Visconti, P. Sleep Problems in Children with Autism Spectrum Disorder. Pediatr Ann 2020, 49, e278–e282. [Google Scholar] [CrossRef]
- Schwichtenberg, A.J.; Janis, A.; Lindsay, A.; Desai, H.; Sahu, A.; Kellerman, A.; Chong, P.L.H.; Abel, E.A.; Yatcilla, J.K. Sleep in Children with Autism Spectrum Disorder: A Narrative Review and Systematic Update. Curr Sleep Med Rep 2022, 8, 51–61. [Google Scholar] [CrossRef]
- Youssef, J.; Singh, K.; Huntington, N.; Becker, R.; Kothare, S.V. Relationship of serum ferritin levels to sleep fragmentation and periodic limb movements of sleep on polysomnography in autism spectrum disorders. Pediatr Neurol 2013, 49, 274–278. [Google Scholar] [CrossRef] [PubMed]
- Tudor, M.E.; Walsh, C.E.; Mulder, E.C.; Lerner, M.D. Pain as a predictor of sleep problems in youth with autism spectrum disorders. Autism 2015, 19, 292–300. [Google Scholar] [CrossRef] [PubMed]
- Elrod, M.G.; Nylund, C.M.; Susi, A.L.; Gorman, G.H.; Hisle-Gorman, E.; Rogers, D.J.; Erdie-Lalena, C. Prevalence of Diagnosed Sleep Disorders and Related Diagnostic and Surgical Procedures in Children with Autism Spectrum Disorders. J Dev Behav Pediatr 2016, 37, 377–384. [Google Scholar] [CrossRef]
- Johnson, C.R.; DeMand, A.; Lecavalier, L.; Smith, T.; Aman, M.; Foldes, E.; Scahill, L. Psychometric properties of the children's sleep habits questionnaire in children with autism spectrum disorder. Sleep Med 2016, 20, 5–11. [Google Scholar] [CrossRef] [PubMed]
- Murata, E.; Mohri, I.; Kato-Nishimura, K.; Iimura, J.; Ogawa, M.; Tachibana, M.; Ohno, Y.; Taniike, M. Evaluation of behavioral change after adenotonsillectomy for obstructive sleep apnea in children with autism spectrum disorder. Res Dev Disabil 2017, 65, 127–139. [Google Scholar] [CrossRef]
- Tomkies, A.; Johnson, R.F.; Shah, G.; Caraballo, M.; Evans, P.; Mitchell, R.B. Obstructive Sleep Apnea in Children With Autism. J Clin Sleep Med 2019, 15, 1469–1476. [Google Scholar] [CrossRef] [PubMed]
- Santapuram, P.; Chen, H.; Weitlauf, A.S.; Ghani, M.O.A.; Whigham, A.S. Investigating differences in symptomatology and age at diagnosis of obstructive sleep apnea in children with and without autism. Int J Pediatr Otorhinolaryngol 2022, 158, 111191. [Google Scholar] [CrossRef]
- Miano, S.; Ferri, R. Epidemiology and management of insomnia in children with autistic spectrum disorders. Paediatr Drugs 2010, 12, 75–84. [Google Scholar] [CrossRef] [PubMed]
- Giannotti, F.; Cortesi, F.; Cerquiglini, A.; Vagnoni, C.; Valente, D. Sleep in children with autism with and without autistic regression. J Sleep Res 2011, 20, 338–347. [Google Scholar] [CrossRef]
- Wright, B.; Sims, D.; Smart, S.; Alwazeer, A.; Alderson-Day, B.; Allgar, V.; Whitton, C.; Tomlinson, H.; Bennett, S.; Jardine, J.; et al. Melatonin versus placebo in children with autism spectrum conditions and severe sleep problems not amenable to behaviour management strategies: a randomised controlled crossover trial. J Autism Dev Disord 2011, 41, 175–184. [Google Scholar] [CrossRef]
- Mazurek, M.O.; Sohl, K. Sleep and Behavioral Problems in Children with Autism Spectrum Disorder. J Autism Dev Disord 2016, 46, 1906–1915. [Google Scholar] [CrossRef]
- Aathira, R.; Gulati, S.; Tripathi, M.; Shukla, G.; Chakrabarty, B.; Sapra, S.; Dang, N.; Gupta, A.; Kabra, M.; Pandey, R.M. Prevalence of Sleep Abnormalities in Indian Children With Autism Spectrum Disorder: A Cross-Sectional Study. Pediatr Neurol 2017, 74, 62–67. [Google Scholar] [CrossRef]
- Mehrazad-Saber, Z.; Kheirouri, S.; Noorazar, S.G. Effects of l-Carnosine Supplementation on Sleep Disorders and Disease Severity in Autistic Children: A Randomized, Controlled Clinical Trial. Basic Clin Pharmacol Toxicol 2018, 123, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Delemere, E.; Dounavi, K. Parent-Implemented Bedtime Fading and Positive Routines for Children with Autism Spectrum Disorders. J Autism Dev Disord 2018, 48, 1002–1019. [Google Scholar] [CrossRef] [PubMed]
- Malhi, P.; Kaur, A.; Singhi, P.; Sankhyan, N. Sleep Dysfunction and Behavioral Daytime Problems in Children with Autism Spectrum Disorders: A Comparative Study. Indian J Pediatr 2019, 86, 12–17. [Google Scholar] [CrossRef]
- da Silveira Cruz-Machado, S.; Guissoni Campos, L.M.; Fadini, C.C.; Anderson, G.; Markus, R.P.; Pinato, L. Disrupted nocturnal melatonin in autism: Association with tumor necrosis factor and sleep disturbances. J Pineal Res 2021, 70, e12715. [Google Scholar] [CrossRef]
- McCrae, C.S.; Chan, W.S.; Curtis, A.F.; Nair, N.; Deroche, C.B.; Munoz, M.; Takamatsu, S.; McLean, D.; Davenport, M.; Muckerman, J.E.; et al. Telehealth cognitive behavioral therapy for insomnia in children with autism spectrum disorder: A pilot examining feasibility, satisfaction, and preliminary findings. Autism 2021, 25, 667–680. [Google Scholar] [CrossRef] [PubMed]
- Estes, A.; Munson, J.; St John, T.; Finlayson, R.; Pandey, J.; Gottlieb, B.; Herrington, J.; Schultz, R.T. Sleep problems in autism: Sex differences in the school-age population. Autism Res 2023, 16, 164–173. [Google Scholar] [CrossRef]
- Distefano, G.; Calderoni, S.; Apicella, F.; Cosenza, A.; Igliozzi, R.; Palermo, G.; Tancredi, R.; Tritto, G.; Craig, F.; Muratori, F.; et al. Impact of sleep disorders on behavioral issues in preschoolers with autism spectrum disorder. Front Psychiatry 2023, 14, 1181466. [Google Scholar] [CrossRef]
- Kamal Nor, N.; Ghozali, A.H.; Ismail, J. Prevalence of Overweight and Obesity Among Children and Adolescents With Autism Spectrum Disorder and Associated Risk Factors. Front Pediatr 2019, 7, 38. [Google Scholar] [CrossRef]
- Veronese, S.; Zoccante, L.; Smania, N.; Sbarbati, A. Stretch marks: a visible expression of connective's involvement in autism spectrum disorders. Front Psychiatry 2023, 14, 1155854. [Google Scholar] [CrossRef]
- Eow, S.Y.; Gan, W.Y.; Lim, P.Y.; Awang, H.; Mohd Shariff, Z. Parental Feeding Practices and Child-Related Factors are Associated with Overweight and Obesity in Children and Adolescents with Autism Spectrum Disorder. J Autism Dev Disord 2022, 52, 3655–3667. [Google Scholar] [CrossRef]
- Zerbo, O.; Leong, A.; Barcellos, L.; Bernal, P.; Fireman, B.; Croen, L.A. Immune mediated conditions in autism spectrum disorders. Brain Behav Immun 2015, 46, 232–236. [Google Scholar] [CrossRef]
- Tonacci, A.; Billeci, L.; Ruta, L.; Tartarisco, G.; Pioggia, G.; Gangemi, S. A systematic review of the association between allergic asthma and autism. Minerva Pediatr 2017, 69, 538–550. [Google Scholar] [CrossRef]
- Zoccante, L.; Ciceri, M.L.; Gozzi, L.A.; Gennaro, G.D.; Zerman, N. The "Connectivome Theory": A New Model to Understand Autism Spectrum Disorders. Front Psychiatry 2021, 12, 794516. [Google Scholar] [CrossRef]
- Georgalas, C. The role of the nose in snoring and obstructive sleep apnoea: an update. Eur Arch Otorhinolaryngol 2011, 268, 1365–1373. [Google Scholar] [CrossRef]
- Ming, X.; Brimacombe, M.; Wagner, G.C. Prevalence of motor impairment in autism spectrum disorders. Brain Dev 2007, 29, 565–570. [Google Scholar] [CrossRef]
- Gabis, L.V.; Shaham, M.; Leon Attia, O.; Shefer, S.; Rosenan, R.; Gabis, T.; Daloya, M. The Weak Link: Hypotonia in Infancy and Autism Early Identification. Front Neurol 2021, 12, 612674. [Google Scholar] [CrossRef] [PubMed]
- Nosetti, L.; Zaffanello, M.; De Bernardi di Valserra, F.; Simoncini, D.; Beretta, G.; Guacci, P.; Piacentini, G.; Agosti, M. Exploring the Intricate Links between Adenotonsillar Hypertrophy, Mouth Breathing, and Craniofacial Development in Children with Sleep-Disordered Breathing: Unraveling the Vicious Cycle. Children 2023, 10. [Google Scholar] [CrossRef]
- Kang, K.T.; Chou, C.H.; Weng, W.C.; Lee, P.L.; Hsu, W.C. Associations between adenotonsillar hypertrophy, age, and obesity in children with obstructive sleep apnea. PLoS One 2013, 8, e78666. [Google Scholar] [CrossRef] [PubMed]
- Strollo, P.J., Jr.; Rogers, R.M. Obstructive sleep apnea. N Engl J Med 1996, 334, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Asmika, A.; Oktafiani, L.D.A.; Kusworini, K.; Sujuti, H.; Andarini, S. Autistic Children Are More Responsive to Tactile Sensory Stimulus. Iran J Child Neurol 2018, 12, 37–44. [Google Scholar] [PubMed]
- Moore, M.; Evans, V.; Hanvey, G.; Johnson, C. Assessment of Sleep in Children with Autism Spectrum Disorder. Children (Basel) 2017, 4. [Google Scholar] [CrossRef] [PubMed]
- Villa, M.P.; Pietropaoli, N.; Supino, M.C.; Vitelli, O.; Rabasco, J.; Evangelisti, M.; Del Pozzo, M.; Kaditis, A.G. Diagnosis of Pediatric Obstructive Sleep Apnea Syndrome in Settings With Limited Resources. JAMA Otolaryngol Head Neck Surg 2015, 141, 990–996. [Google Scholar] [CrossRef] [PubMed]
- Chervin, R.D.; Weatherly, R.A.; Garetz, S.L.; Ruzicka, D.L.; Giordani, B.J.; Hodges, E.K.; Dillon, J.E.; Guire, K.E. Pediatric sleep questionnaire: prediction of sleep apnea and outcomes. Archives of Otolaryngology--Head & Neck Surgery 2007, 133, 216–222. [Google Scholar]
Figure 1.
The PRISMA flow diagram graphically illustrates the study selection process, indicating the number of studies incorporated at each phase (EXPORT DATE: 05 Jun 2023).
Figure 1.
The PRISMA flow diagram graphically illustrates the study selection process, indicating the number of studies incorporated at each phase (EXPORT DATE: 05 Jun 2023).
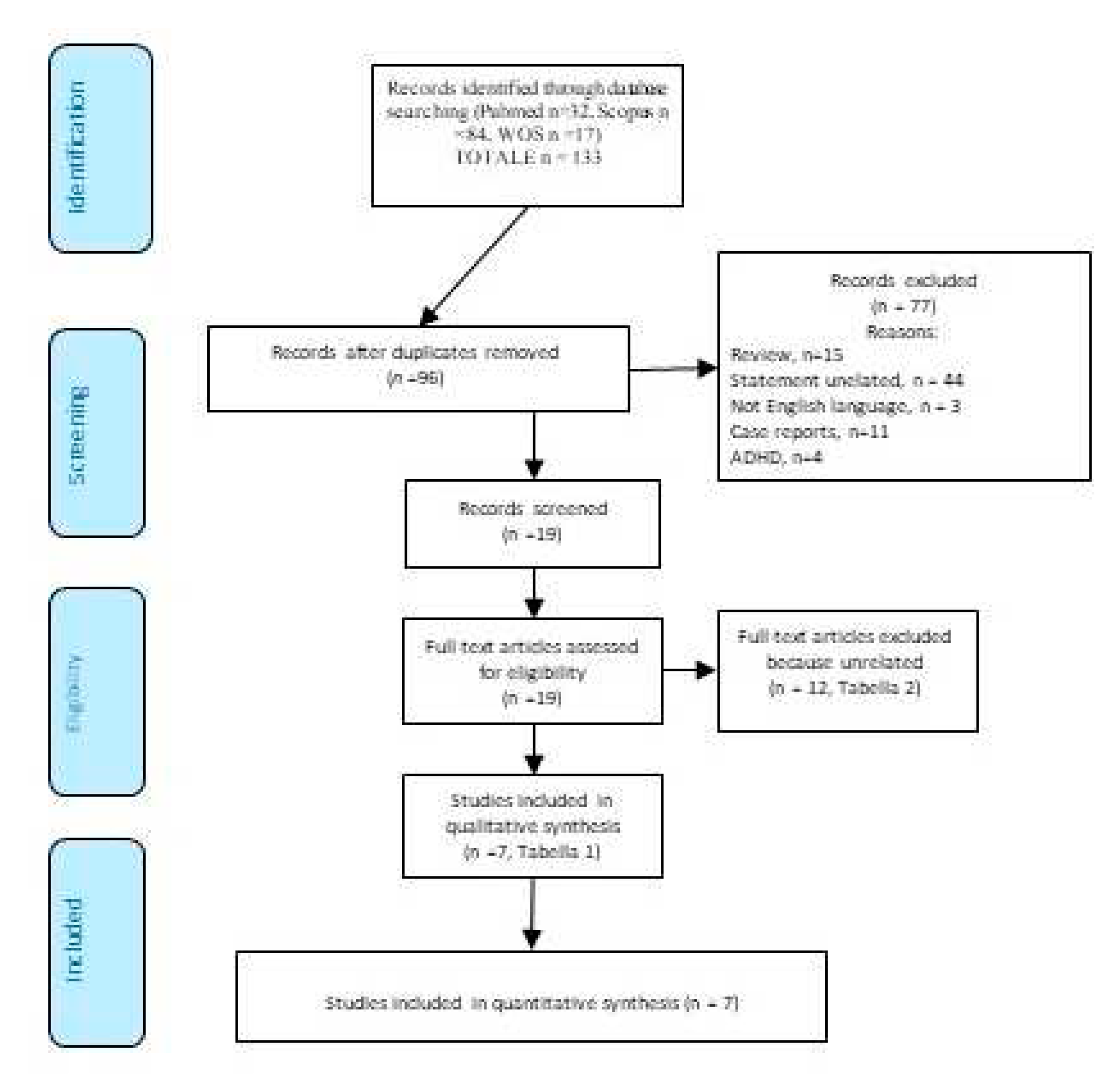
Figure 2.
The figure (AI image generator https://dream.ai/create) illustrates the association between autism and SDB in children. Key risk factors such as muscle hypotonia, obesity, and adenotonsillar hypertrophy are highlighted. Additionally, the figure underscores the importance of PSG in recognizing and treating SDB in autistic children. Lastly, the significance of otorhinolaryngological surgical intervention as an effective therapeutic option to alleviate symptoms of SDB and enhance the quality of life for children with autism is emphasized.
Figure 2.
The figure (AI image generator https://dream.ai/create) illustrates the association between autism and SDB in children. Key risk factors such as muscle hypotonia, obesity, and adenotonsillar hypertrophy are highlighted. Additionally, the figure underscores the importance of PSG in recognizing and treating SDB in autistic children. Lastly, the significance of otorhinolaryngological surgical intervention as an effective therapeutic option to alleviate symptoms of SDB and enhance the quality of life for children with autism is emphasized.

Table 1.
The table summarizes the key points of various scientific studies available on the relationship between Sleep Disordered Breathing (SDB) and autism spectrum disorder (ASD). Each column of the table provides specific information to enable an overall view of the characteristics and results of each study.
Table 1.
The table summarizes the key points of various scientific studies available on the relationship between Sleep Disordered Breathing (SDB) and autism spectrum disorder (ASD). Each column of the table provides specific information to enable an overall view of the characteristics and results of each study.
| Primo autore | Year of publication | Design | Aim | Subjects | Methods | Results | Conclusions |
|---|---|---|---|---|---|---|---|
| Youssef J et al. [19] | 2013 | Retrospective chart review (Massachusetts) | To investigate the relationship between ferritin levels, fragmented sleep disorders, and joint movements in children with ASD. | Out of the 9,791 identified ASD children, 511 had ferritin level data, 377 had PSG data, and 53 had both ferritin and PSG data. | Review of ASD children's records. PSG and ferritin analysis. Assessment of sleep fragmentation, limb movements. Comparison with the control group. |
37% had sleep apnea. There was no significant difference in BMI or ferritin levels between ASD patients with or without OSA (P > 0.1). Ferritin levels did not predict abnormal sleep outcomes (P > 0.1). | No correlation between apnea, ferritin, and BMI. |
| Tudor, M.E, et al. [20] | 2015 | - (USA) | Parental assessment. Correlation between pain and sleep issues. |
Individuals with ASD (N = 62), Child ages ranged from 3 to 18 yrs (9.39±4.19 yrs). | NCCPC-R and CSHQ. Correlations between pain and sleep, including duration, parasomnias, SDB. Impact of pain on sleep issues. | High scores in the SDB subscale were predicted by high scores in the Vocal subscale. SDB: mean subscale 3.99 ± 122; n.(%) scoring > 0.35 (56%). | Sleep behaviours and vocalizations influence duration, parasomnias, and SDB. |
| Elrod MG, et al. [21] | 2016 | Retrospective cohort study. (Bethesda) | Risk assessment between ASD and controls for sleep disorders and diagnostic/surgical procedures. | 48,762 children with ASD and controls (aged 2 to 18 yrs). | ASD (2000-2013). ASD matched 1:5 with controls for age, gender, and enrollment. Analysis of ICD-9-CM sleep disorders. RR and 95% CI were calculated using binary Poisson regression. |
ASD children have a higher risk of sleep disorders, including OSA (RR: 1.97 [95% CI, 1.91-2.02]). Higher risk of PSG (RR: 3.74 [95% CI, 3.56-3.93]) and related surgeries (RR: 1.50 [95% CI, 1.46-1.54]). |
Individuals with ASD have an elevated susceptibility to the emergence of sleep disorders, which includes OSA. They are more likely to have abnormal PSG results and undergo sleep-related surgeries than children without ASD. |
| Johnson CR et al. [22] | 2016 | Multisite RCT (Emory University, Indiana University, Ohio State University, University of Pittsburgh, University of Rochester, and Yale University) | Psychometric properties of the CSHQ in children with ASD. | 310 children with ASD (Age 4.7±1.14 yrs) | The CSHQ (8 subscales): Bedtime Resistance, Sleep Onset Delay, Sleep Duration, Sleep Anxiety, Night Wakings, Parasomnias, SDB, and Daytime Sleepiness. | Loud, persistent snoring (5.1%) and other abnormal breathing behaviours (frequent apnea 0.6%) during sleep are relatively infrequent. | Loud snoring and other abnormal breathing behaviours (apneas) during sleep are rare. |
| Murata E, et al. [23] | 2017 | Short-term retrospective study (Japan) | Behavioural changes after A&T for OSA in children with ASD. | 55 ASD children (30 with OSA). Mean age: 7 yrs and 3 months (SD = 2 years and 5 months, range: 5-14 yrs) in the OSA group, and 7 yrs and 5 months (SD = 2 years and 0 months, range: 5-13 yrs) in the control group. | Children with untreated OSA and ASD control without OSA. OSA diagnosis: PSG, cardiorespiratory monitoring, oximetry. CBCL before and after treatment. | Pre-A&T scores for externalizing (p < 0.01), somatic problems (p < 0.05), anxiety/depression (p < 0.05), social issues (p < 0.01), thought problems (p < 0.01), delinquent behaviour (p < 0.01), and aggressive behaviour (p < 0.05) are significantly higher in the improved group compared to the no-change/deterioration group. Sex, A&T age, obesity indices, and severity of OSA based on AHI/3% and ODI did not differ between the improved group and the no-change/deterioration group. |
OSA in children with ASD should be treated regardless of obesity and age, even in cases of mild OSA, especially when more severe behavioural problems are present. We need to be aware of OSA in children with ASD. |
| Tomkies A, et al. [24] | 2019 | Retrospective study (Texas) | Demographic and clinical characteristics, undergoing PSG, predictors of OSA and severe OSA. | 45 children (age range 2 - 18 yrs, mean age 6.1 yrs). | PSG on children (born between 2009 - Feb. 2015). Excluding severe comorbidities, tonsillectomy, and missing data. Collected age, sex, race, and clinical data. Analysis of OSA predictors. | The mean oAHI in children with OSA was 13.1 ± 18/hr. 58% had OSA (AHI >1). 33% were obese (BMI ≥ 95th percentile). Severe OSA is significantly associated with weight (OR 1.0, 95% CI 1.0-1.1, P = 0.05). The mean AHI is 7.7 /hour. 20% had severe OSA (AHI ≥ 10 /hr). There were no significant predictors for OSA except weight increase for severe OSA. | OSA is quite common in children, with considerable variability in severity. Obesity is associated with greater OSA severity. Weight appears to be a predictive factor for severe OSA. |
| Santapuram P, et al. [25] | 2022 | Retrospective cohort study (USA) | A study comparing symptoms and age of OSA diagnosis. Children with and without ASD. Assessment of symptoms and age of OSA diagnosis. Identification of differences between groups. |
Children with and without ASD. 166 children. The control group comprised 91 patients (54.9% male) with typical development and OSA. Age at OSA diagnosis: ASD 72.8 (45.6) months; Control 73.4 (47.4) months, p = 0.999. | Review of clinical records for OSA (2019-2021). Analysis of diagnosis and treatment. Included children with OSA and A&T. |
Less severity of autism was associated with a later age at OSA diagnosis (p < 0.001). Multivariate regression analysis did not reach statistical significance (p = 0.079). BMI and age at ASD diagnosis were independently associated with age at OSA diagnosis (p = 0.033 and p < 0.001, respectively). | Association between autism severity and age at OSA diagnosis. The association might not be significant when considering other factors simultaneously, such as BMI and age at ASD diagnosis. BMI and age at ASD diagnosis appear to have independent impacts on age at OSA diagnosis. |
Legend: AHI, apnea-hypopnea index; ASD, autism spectrum disorder; A&T, adenotonsillectomy; BMI, body mass index; CSHQ, Children's Sleep Habits Questionnaire; OSA, obstructive sleep apnea; PSG, polysomnography; SDB, sleep-disordered breathing; yrs, years.
Table 2.
The table summarizes the excluded articles from the review after careful evaluation and highlights the key points on Sleep Disturbances and Autism Spectrum Disorder (ASD). Each column in the table provides specific information to facilitate an overall understanding of the characteristics and outcomes of each study.
Table 2.
The table summarizes the excluded articles from the review after careful evaluation and highlights the key points on Sleep Disturbances and Autism Spectrum Disorder (ASD). Each column in the table provides specific information to facilitate an overall understanding of the characteristics and outcomes of each study.
| First author (yrs of publication) | Aim | Subjects | Methods | Results | Conclusions |
|---|---|---|---|---|---|
| Miano S, Ferri R. (2010) [26] | Analysis of Insomnia Epidemiology and Management in Children with ASD (Review) | ASD children | Causes of Insomnia in ASD: Neurochemical (Melatonin), Psychiatric (Anxiety), Behavioral (Sleep Habits). ASD-related Insomnia: Common, Difficulty Falling Asleep, Frequent Awakenings, Early Awakenings, Non-Restorative Sleep. Interventions: Behavioral Therapies (Routine, Relaxation, Anxiety), Medications (Melatonin), Multidisciplinary Approaches. | Sleep Issues in Children with ASD. Similar to typical ones, but more prevalent. Common Insomnia: onset, maintenance, restless, resistance, awakenings. PSG: less sleep, altered microstructure. Treatments: Medications, behavioural interventions, promising melatonin. |
Sleep in children with ASD presents issues similar to those in typical children but occurs more frequently. Insomnia, difficulty falling asleep, nighttime awakenings, restlessness, and resistance to sleep are typical. PSG analysis reveals reduced sleep duration and alterations in its structure. Medications, behavioural therapies, and melatonin appear promising for addressing these issues. |
| Giannotti, F., et al. (2011) [27] | Comparison of Sleep in Regressive Autism, Non-Regressive Autism, and Typical Development. NREM Analysis. Understanding Sleep in Autism Compared to Typical Development. |
Subjects with Non-Regressive Autism (22 participants) | 52 children (ages 5-10) - 22 with non-regressive autism, 18 with regressive autism (without comorbidities), 12 typically developing (TD). Instruments: PSG, CSHQ. | Higher CSHQ scores in TD. Regression: less efficient sleep, reduced total sleep time, prolonged REM, increased wakefulness after sleep onset. Lower CAP and A1 index in light sleep in regressive compared to TD and non-regressive. | TD children have higher CSHQ scores than non-regressive. Autism exhibits sleep changes: less sleep, prolonged REM, and wakefulness after sleep onset. These patterns provide insights into insomnia in non-regressives. |
| Wright, B., et al. (2011) [28] | Comparison of Melatonin vs. Placebo in Severe Sleep Disorders in ASD Unresponsive to Behavioral Management | 22 children with ASD, 17 children completed the study | Controlled crossover study: treated with melatonin/placebo for 3 months after behavioural therapies failed, assessment of sleep variables | Improvements with melatonin: Reduced sleep latency (47 minutes) and increased total sleep duration (52 minutes), but no effect on nighttime awakenings. Low and similar side effects between melatonin and placebo. | Melatonin improves sleep: sleep onset -47 min, duration +52 min. Minimal side effects enhance sleep safely and effectively. |
| Mazurek, M.O. & Sohl, K. (2016) [29] | The study examines relationships between sleep disturbances and behavioural issues in children with ASD | 81 children with ASD | Multivariate analysis to correlate sleep disturbances and behavioural problems in children with ASD. Assessment: Utilized Sleep Disturbance Scale and Aberrant Behavior Checklist. |
Sleep disturbances are linked to aggressiveness, attention, and hyperactivity. Analysis: Sleep explains 22-32% of the behavioural variance—nighttime awakenings linked to daytime issues, controlling for age and gender. | Sleep disturbances linked to behaviour: aggressiveness, attention, hyperactivity. Sleep explains 22-32% of behavioural variation—nighttime awakenings tied to daytime issues. Sleep impacts daytime behaviour. |
| Aathira, R. et al. (2017) [30] | Prevalence of Sleep Alterations in Indian Children with ASD | For children with ASD and controls, 109 children with ASD were screened, of which 71 fulfilled the inclusion criteria (age: 3-10 years). | Two-year Study. Sleep evaluated with Children's Sleep Habits Questionnaire. Additional assessments: PSG, Autism Scale, Behavioral Checklist, Developmental Profile 3. | Sleep prevalence: 77.5% in ASD, 29.2% in controls. PSG: Reduced efficiency, less REM, slow waves, desaturation in ASD. Checklist: A high score indicates poor sleepers—no correlation with autism scale or developmental profile 3. | The findings underscore the significance of addressing sleep disorders in ASD through tailored interventions aimed at enhancing overall well-being. |
| Mehrazad-Saber, Z., et al. (2018) [31] | Effects of l-Carnosine Supplementation on SDB and Severity of Core Autism Symptoms in ASD patients | Individuals with ASD (31 males and 12 females), ranging in age from 4 to 16 yrs old. | Double-masked study: carnosine (treatment), placebo (control). 2 months. Sleep assessment and symptoms using Gilliam Autism Rating Scale 2. Effects of carnosine on ASD sleep symptoms. | Carnosine supplement: Reduced sleep duration (p = 0.04). Reduced parasomnias (p = 0.02). Sleep disturbance score -7.59% vs. control (p = 0.006). |
Promising initial results: Carnosine may aid sleep—further research for confirmation, long-term effects, and mechanism of action. |
| Delemere E, Dounavi K (2018) [32] | Studying the effectiveness of stimulus control interventions (bedtime fading and positive routines) on sleep in children with ASD, using multiple designs | 6 children with ASD (2 and 7 yrs) | Two interventions related to stimulus control (bedtime fading and positive routines) were implemented. | Bedtime fading: Increased sleep duration, reduced latency. Positive routines: Mixed effects on sleep latency and duration in some participants. |
Bedtime fading aids sleep in some; positive routines vary—tailoring strategies for personalized adaptation for optimal outcomes. |
| Malhi, P. et al. (2019) [33] | Objective 1: Comparison of ASD sleep vs. controls. Objective 2: Association between sleep and behaviour in children with ASD. | 60 children with ASD (85% males). Mean age: 6.1 yrs (±2.4). Control group: 60 typically developing children, matched for age and socioeconomic status. |
Sleep: Assessed with CSHQ. Behaviour: Assessed with Child Psychopathology Measurement Tool. |
ASD: High prevalence of sleep problems. CSHQ, high resistance and duration. Sleep-related daytime behaviours. CSHQ and wakefulness explain behaviours. | Results: ASD and related sleep disturbances correlated; addressing them improves daytime behaviours and quality of life in ASD. |
| da Silveira Cruz-Machado, S., et al. (2021) [34] | To assess urinary aMT6s and salivary TNF, IL-6 in ASD. Correlation with sleep. |
40 participants: typical group (n = 20; mean age 10.2 yrs) and ASD group (n = 20; mean age 11.0 yrs). | Method: Urinary aMT6s, salivary TNF, IL-6 evaluated—correlation analysis with sleep disturbances. Sleep Disturbance Scale was used to assess sleep—correlation analysis with the same sleep disturbances. | Autism sleep results: 60% ASD: Increased nighttime aMT6s. ASD: Increased nighttime TNF, no change in IL-6. Sleep dysfunction (Scales) correlated with aMT6s. SDB: Decreased aMT6s; Increased TNF. |
Complex interaction between sleep, immunity, and autism, the possible role of melatonin. Further research is needed to understand mechanisms and clinical implications. |
| McCrae, C.S. et al. (2021) [35] | Common insomnia in ASD. CBT improves sleep and autism functioning. Parents benefit: their sleep improves with CBT. | Pilot study: CBT for insomnia via Telehealth. Participants: 17 children (6-12 yrs) with ASD and insomnia + parents. Evaluate the effectiveness of CBT for insomnia, and involve parents in ASD. | Telehealth delivery of eight-session cognitive behavioural treatment for childhood insomnia | High treatment fidelity. Parents satisfied with insomnia CBT. Telehealth: Sleep and functioning improvements. 1 month: Less inappropriate language, stable hyperactivity. | High treatment compliance and effective telehealth. CBT therapy is beneficial for insomnia in autism and improvements in parents and sleep, and some behaviours require further study. |
| Estes, A., et al. (2023) [36] | Evaluate gender differences in sleep problems in school-age autism. | Autistic children (n = 250); typically developing children (n = 114), 6–12 yrs of age | Title: Parent Sleep Problems (CSHQ) - Children 6-12 Years | Females with ASD: resistance, anxiety, drowsiness, reduced sleep. More sleep problems compared to males with ASD and typical children. Males with ASD: anxiety-sleep link. | Gender differences in ASD sleep disturbances: Females - resistance, anxiety, drowsiness; males - anxiety and sleep. Consider managing ASD sleep with gender differences in mind. |
| Distefano G, et al. 2023 [37] | Identifying sleep in preschool ASD, correlations with autism, development, comorbidities. | 163 preschool-age children diagnosed with ASD (43.37±12.56 months) | Applying CSHQ and standard tests to assess children's sleep, intelligence, repetitive behaviours, and psychiatric comorbidities (CBCL 11/2-5 and RBS-R). | Sleep disturbances linked to high scores on CSHQ and CBCL, with connections to anxiety symptoms for repetitive behaviours and CBCL syndromes. | Link between sleep and CSHQ and CBCL scores. Sleep problems are connected to behaviours and symptoms. Sleep treatment can improve well-being in children with behavioural and psychological symptoms. |
Legend: ASD, autism spectrum disorder; CBCL, Child Behavior Checklist; CBT, Cognitive behavioral treatment for childhood insomnia; CSHQ, Children's Sleep Habits Questionnaire; PSG, polysomnography; TD, typical development; yrs, years.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



