
Submitted:
14 August 2023
Posted:
14 August 2023
Read the latest preprint version here
Abstract
Pancreatic neuroendocrine tumor (P-NET) is a rare neoplasm originating in the neuroendocrine system. Carcinoid syndrome occurs in approximately 19% of patients with functional P-NETs, typically when liver metastases occur. NETs diagnosis is frequently late, along with symptoms related to hormone hypersecretion. We described the case of a patient with a low-grade non-functional P-NET, but with a typical clinical presentation of a carcinoid syndrome; moreover, we reviewed the literature regarding this topic. An 81-year-old male was admitted to our Department of Internal Medicine at Cannizzaro Hospital (Catania, Italy) because of the onset of abdominal pain with nausea, loose stools and episodic flushing. Firstly, an abdominal contrast-enhanced CT scan showed a small pancreatic hypervascular mass; then a gallium-68 DOTATOC integrated PET/CT revealed an elevated expression of SSTR receptors. Serum Chromogranin A and urinary 5-HIAA measurements resulted negative. Given the small size of the lesion (8 mm), we preferred to perform an endoscopic ultrasonography (EUS) with fine-needle biopsy (EUS-FNB), allowing the diagnosis of low-grade (G1) non-functional P-NET (NF-P-NET). Surgery was waived, while a follow-up strategy was chosen. Early recognition of P-NETs, although rare, is necessary to improve patient’s survival. EUS-FNB should be the protocol of choice for an early characterization of these tumors.
Keywords:
Neuroendocrine tumors
; NETs
; pancreatic neuroendocrine tumors
; P-NETs
; endoscopic ultrasonography
; EUS-FNA
; EUS-FNB
1. Introduction
Neuroendocrine neoplasms (NENs) are enigmatic malignancies with an increasing incidence and prevalence[1-3]. Given the common morphological and immunophenotypical features, all these tumors arise from cells of the diffuse endocrine system.
NENs range from asymptomatic well-differentiated neuroendocrine tumors (NETs) to aggressive neuroendocrine carcinomas (NECs). In fact, nearly 80%-90% of NENs are NETs, while the remaining 10%-20% are carcinomas[4].
NETs can develop in any tissue of the body. Gastrointestinal tract and pancreas are the most common sites of origin, accounting for approximately 60% of the primary sites[5], followed by lungs and other sites.
About 40% of NETs can release hormones responsible for symptoms, depending on the secreted hormone. Carcinoid syndrome is a paraneoplastic syndrome characterized by episodic flushing and diarrhea, due to various vasoactive substances (serotonin, histamine, and other amines.) released into the systemic circulation[6].
Non-functional NETs may often present with subtle and sporadic symptoms, sometimes with gastrointestinal bleeding, abdominal pain, bowel obstruction or unexplained weight loss[7].
Treatment and prognosis depend on the grade and stage of the tumor. NETs diagnosis is frequently late, along with symptoms related to hormone hypersecretion, often after NETs have metastasized to the liver, where bioactive substances fail to be inactivated. Early diagnosis and recognition are necessary to improve patient’s survival, that did not significantly change over the last 30 years[8].
In this paper, we presented a case of a pauci-symptomatic pancreatic neuroendocrine tumor in a patient with unspecific clinical presentation (abdominal pain) and mild additional symptoms (nausea and loose stools). This was the occasion for a narrative review of the literature on the diagnosis and the management of pancreatic neuroendocrine tumors (P-NETs).
2. Case-report
In May 2023, an 81-year-old man was admitted to our Department of Internal Medicine at Cannizzaro Hospital (Catania, Italy) because of the onset of abdominal pain, especially in the lower abdominal quadrants, with nausea and loose stools (<3 times/day).
The patient’s past medical history included arterial hypertension, type 2 diabetes mellitus, peripheral artery disease (PAD), obesity, hypothyroidism and depressive syndrome. In the past six months he complained of abdominal distension and changes in bowel habits (loose stools). No relevant family history. He was taking levothyroxine, insulin according to HGT, lansoprazole, acarbose, ezetimibe/simvastatin and furosemide. He denied anamnestic consumption of uncooked meat, or fish, or unpasteurized dairy products.
On admission, no fever, arterial hypertension (177/76 mmHg), normal heart rate (86 bpm), glycemia 102 mg/dL and normal SaO2 on room air (98%); no sensorium alterations. Physical examination revealed abdominal distension, with colic pain on deep palpation and hypoactive abdomen sounds. Mucous membranes were normally hydrated. Bedside FAST (Focused Assessment with Sonography in Trauma) scan did not detect peritoneal fluid. Digital rectal examination showed blood traces.
Laboratory tests were performed, showing an increase in serum CRP (17.9 mg/dL), moderate leukocytosis, moderate renal dysfunction (Cr: 1,33 mg/dL, eGFR: 54 ml/min/1.73 m2), normal serum potassium (3.6 mEq/L), sodium (139 mEq/L) and chloride (100 mEq/L), mild metabolic acidosis (pH: 7.33, HCO3: 21 mmol/L, pCO2: 42 mmHg) and serum procalcitonin <0.2 ng/mL. Infectious causes of diarrhea were excluded by microbiological and chemical fecal examinations. An abdomen X-ray excluded bowel obstruction or perforation. Moderate intravenous fluid repletion was given.
After a few hours from admission, the patient experienced transient states of agitation, with uncontrolled crying spells and temper tantrums. Due to his past medical history of untreated depression, anxiolytic and antipsychotic therapy was prescribed, but with poor efficacy. During this altered emotional status, a flushing episode was observed in the face and the neck.
A contrast-enhanced abdominal CT scan revealed a pancreatic hypervascular small mass (8 mm) (Figure 1).
On the fifth day of admission, given the suspicion of a pancreatic neuroendocrine tumor (P-NET), a gallium-68 DOTATOC integrated PET/CT was performed (Figure 2), showing a lesion between head and body of pancreas, with elevated expression of SSTR2/5 somatostatin receptors. No other sites of disease were detected.
Serum chromogranin A (CgA) measurement resulted within the normal range (98.0 ng/ml, normal values <101.9 ng/ml), as well as did a urine 5-HIAA - test (urinary 5-HIAA: 1.6 mg/24 h; normal values: 1.0 – 8.2 mg/24 h).
A progressive recovery was observed, with no further abdominal pain. In accordance with the remission of symptoms and the normal laboratory values, the patient was discharged with the prescription to undergo an endoscopic ultrasonography with fine-needle biopsy (EUS-FNB), for a targeted diagnostic and treatment management.
In June 2023, EUS-FNB visualized the presence of an oval hypo-echogenic mass with a major axis of 8.9 mm (Figure 3), which was sampled for cyto-histological examination.
Histological and immunohistochemical examination confirmed the suspicion of P-NET (stage WHO G1, well-differentiated, synaptophysin positive, CgA positive, Ki67 1%,) (Figure 4).
In accordance with the current guidelines, this finding allowed us to make diagnosis of low-grade (G1) non-functional pancreatic neuroendocrine tumor (NF-P-NET) (well-differentiated neoplasm, absence of mythosis, Ki67 ≤2%)[9].
After the evaluation of stage, grading, symptoms and comorbidities, a conservative approach of watchful waiting was chosen by the surgeon, with a radiological follow-up after one year. We scheduled a clinical follow-up in order to keep symptoms under observation.
3. Review of the Literature
Neuroendocrine neoplasms (NENs) are heterogenous neoplasms arising in secretory cells of the diffuse neuroendocrine system, the so called APUD (Amine Precursor Uptake and Decarboxylation) System. Characterized by amine and neuropeptide hormone production with dense vesicles, these neuroendocrine cells are specialized to receive neuronal inputs and consequentially release message peptides into circulation for regulation and modulation of cell proliferation, growth, and development. NENs are distinguished from pheochromocytomas and paragangliomas (neuroendocrine non-epithelial neoplasms) by the expression of keratin in the former ones, given their epithelial origin[10].
Neuroendocrine tumors (NETs) represent only 0.5% of all malignant conditions and 2% of all malignant tumors of the gastrointestinal tract[11]. Given the continued update in classification of NENs, these epidemiological data are continuously evolving. The prevalence of NETs ranges between 2.5 and 8.35 cases per 10,000, with a recent increase in their incidence rates[1-3,12-15], probably due to imaging improvement, leading to an earlier and more frequent diagnosis of the disease[5].
In the 2019 WHO classification of tumors of the digestive system[16], NENs are divided into well-differentiated neuroendocrine tumors (NETs) and poorly differentiated neuroendocrine carcinomas (NECs), based on their molecular differences. In addition, “mixed neuroendocrine-non-neuroendocrine neoplasms” (MiNENs) were better characterized, according to the simultaneous presence of both neuroendocrine and non-neuroendocrine components, typically poorly differentiated (Table 1).
The most frequent primary sites are gastrointestinal tract (61%), lung (25%), and about 14% remains of unknown origin[17]. Twelve to 22% percent of patients are metastatic at presentation[5].
The 2019 WHO classification[16] provided an improved system for determining prognosis and treatment, appliable to all NENs, replacing previous classification based on cell embryologic origin (foregut, midgut, hindgut)[18]. In contrast to 2017 WHO classification of tumors of endocrine organs[19], last classification included pancreatic tumors in gastroenteropancreatic NENs (GEP-NENs)[16].
Gastroenteropancreatic tumors (GEP-NETs) are most commonly located in the gastric mucosa, the small intestine, the rectum, and the pancreas[20]. While a subset of NENs is functional (40%), presenting with characteristic endocrine-related symptoms, the majority of them are non-functional and do not present with symptoms until later stages.
Up to 90% of P-NETs are hormonally silent, a behavior affecting the prognosis as compared with functioning neoplasms, probably because of late diagnosis[21].
P-NETs may produce a large variety of hormones, such as insulin, gastrin, glucagon, vasoactive intestinal peptide (VIP), serotonin, somatostatin, and others[22]. By contrast, non-functional P-NETs, without hormones overproduction, may present with unspecific symptoms, such as abdominal pain, weight loss, diarrhea and gastrointestinal bleeding[7,23]. Most P-NENs are sporadic, whereas a minority are inherited, associated with Type 1 multiple endocrine neoplasia (MEN-1), von Hippel-Lindau syndrome (VHL), tuberous sclerosis or neurofibromatosis.
Functional pancreatic neuroendocrine tumors that are associated with a variety of clinical syndromes include[24]:
- Insulinomas, the commonest functional P-NETs, which may appear as a part of MEN1, are associated with overproduction of insulin leading to Whipple’s triad (symptoms of hypoglycemia, plasma glucose levels <40 mg/dL, and relief of symptoms with glucose administration for diagnosis).
- Gastrinomas, or Zollinger Ellison syndrome, are responsible of symptoms of gastric acid hypersecretion, such as abdominal pain, diarrhea, esophageal symptoms. Twenty-five percent of gastrinomas are associated with MEN-1 syndrome. Nearly 70% of gastrinomas occurs in duodenum, nearly 25% in pancreas, nearly 5% in other sites.
- Pancreatic polypeptide-secreting tumors are not characterized by a clinical syndrome, but are associated with weight loss, jaundice, and abdominal pain.
- VIPomas, or Verner-Morrison syndrome, are responsible of large volume watery diarrhea, hypokalemia and reduced gastric acid secretion, with or without facial flushing.
- Glucagonomas are exclusively pancreatic NENs, overproducing the counterregulatory hormone glucagon. Patients with glucagonomas typically present with necrolytic migratory erythema, weight loss, new onset diabetes mellitus, anemia, thromboembolism and depression.
- Somatostatinomas are the least common NETs, primarily located in the pancreas and duodenum. Most symptoms are nonspecific, such as abdominal pain, weight loss and achlorhydria. Few patients may present with somatostatinomas syndrome, characterized by diabetes mellitus, steatorrhea and cholelithiasis.
Carcinoid syndrome is a paraneoplastic syndrome occurring because of the release of bio-active substances, predominantly serotonin (5-HT), but also histamine, bradykinin, prostaglandins E and F, and tachykinins[25]. Recently, Halperin et al.[26] demonstrated, in a population-based analysis carried out on the American “Surveillance, Epidemiology, and End Results-Medicare” database, that 19% of patients with NETs had carcinoid syndrome. Typical symptoms are flushing and diarrhea. Wheezing, palpitations, breathlessness, abdominal pain, telangiectasias and neuropsychiatric symptoms could be also associated to carcinoid syndrome[25,27]. In the majority of cases, tumors are slow-growing and can produce hormonal substances such as serotonin, bradykinins, tachykinins and prostaglandins, with minimal clinical symptoms. When the tumor metastasizes to liver, bioactive substances are no longer inactivated because of the presence of hepatic metastases, therefore reaching systemic circulation. Usually, serotonin is physiologically metabolized by monoamine oxidases in the liver, lungs, and brain to 5-hydroxyindoleacetic acid (5-HIAA)[25,28]. However gastrointestinal NENs, with extensive retroperitoneal nodal involvement, can cause carcinoid syndrome even without hepatic metastases[29]. Recently, long-term complications from carcinoid syndrome, such as mesenteric and/or retroperitoneal fibrosis and carcinoid heart disease (CHD), have been well described[27,30,31]. In particular, CHD is characterized by right heart failure, due to deposition of plaques of fibrotic tissue on the right-side heart valves, caused by vaso-active substances secreted by the tumors (5-HT, histamine, prostaglandins)[32]. The left side of the heart is preserved by the inactivation of bioactive substances in the lung[33]. Otherwise, psychiatric symptoms, such as depression and acute psychosis, have been associated with metastatic carcinoid disease[34,35]. Depressive syndrome could be explained by the reduced levels of tryptophane, due to peripheral consumption by serotonin overproducing NETs[36].
The diagnosis of GEP-NENs is made on the basis of tissue histological examination. Radiological and functional imaging is used to evaluate disease extension (staging) and assess response to therapy, as well as to localize the primary site. Laboratory tests play a diagnostic role only for carcinoid syndrome and hormone-specific syndromes (gastrinomas, insulinomas, glucagonomas).
The current WHO classification emphasized the role of histological examination in surgically removed neoplasms, in order to establish the morphological characteristics and grading[16]. Three grades (G1, G2, G3) are described for GEP-NETs, based on the proliferation activity assessed by mitotic rate and Ki67 proliferation index[37,38]. NECs are no longer graded, as they are known as high grade by definition, because poorly differentiated. The mitotic rates are expressed as the number of mitoses/2 mm2, which is assessed by counting in 50 fields of 0.2 mm2. To determine the Ki-67 proliferation index, at least 500 cells in the regions of highest labeling, known as “hotspots,” are counted[19,39,40]. For a specific pathological diagnosis, together with morphology and grading, immunohistochemical staining for chromogranin A (CgA) and synaptophysin should be assessed, as biomarkers of neuroendocrine tumors. Recently, insulinoma-associated protein 1 (INSM1) has been proposed as a novel sensitive immunostaining for NETs[41]. All NETs express INSM1, synaptophysin, and chromogranin; the majority expresses chromogranin A, that is the most widely used biomarker. INSM1 seemed to be more sensitive in the detection of NENs, probably because it is a transcription factor with a nuclear expression easily interpretable, at variance of other cytoplasmatic markers[42,43].
Although WHO histological classifications are specifically intended for surgically removed NENs[9,16], recent studies have investigated the role of endoscopic ultrasound-guided fine-needle aspiration (EUS-FNA) and fine-needle biopsy (EUS-FNB) for the pre-operative evaluation and management of pancreatic NETs (P-NETs)[44-53]. Despite data about grading concordance between EUS-FNA and surgical specimens highlighted a significant rate of under- or over-grading[48-54], the recent introduction of needles for EUS-guided fine-needle biopsy (EUS-FNB) has changed the scenario[48,49]. EUS-FNB, in fact, allows to obtain tissue samples on which easily performing immunohistochemical examination to evaluate Ki67 proliferation index[50-56]. As a matter of fact, in patients with less than 2 cm P-NETs, management is still controversial, especially for asymptomatic and non-functional P-NETs[57-60]. Endoscopy with biopsy is already the gold standard for diagnosing NENs of the stomach, duodenum and colorectum[61,62]. In the diagnosis of pancreatic NENs, EUS is particularly useful in detecting small lesions. The introduction of EUS-FNB could overcome the interpretative limits of EUS-FNA, permitting an early characterization of tumors in which surgery would be destructive of heathy tissue [51,52].
Tumor-nodes-metastasis (TNM)-based staging of GEP-NENs follows the 2017 Union for International Cancer Control (UICC) classification of malignant tumors[63]. European Neuroendocrine Tumor Society (ENETS) proposed a similar staging system, depending on tumor size and the extent of invasion, with a different classification of gastric, appendiceal and pancreatic tumors[64]. Recent studies suggested the use of ENETS staging for pancreatic NENs, since it seemed superior to UICC scheme, especially for prognostic relevance[9,65].
To investigate NENs, several imaging methods are available, including computed tomography (CT), magnetic resonance (MRI), ultrasonography and functional imaging with scintigraphy and positron emission tomography (PET). The optimal choice of imaging modality depends on the location of primary and metastatic lesions[66].
In order to establish the global burden of the disease, contrast-enhanced CT of the neck-thorax-abdomen and pelvis is the first choice[9,67]. In primary P-NETs, contrast-enhanced CT scans are highly accurate in detecting tumors larger than 2 cm and have a sensitivity range of 63%–82%, and specificity range of 83%–100%[67]. CT sensitivity for NET liver metastases is higher, ranging from 75 to 100%, with a specificity of 83-100%[67].
MRI is advantageous in the assessment of location and extent of small tumor of the pancreas and liver metastases[68,69]. Mean sensitivity for P-NETs is 79% (range 54-100%), with a specificity of 100%[67].
Endoscopic ultrasonography (EUS) has become a very useful technique to evaluate pancreatic lesions. On EUS, P-NETs typically appear as well-defined, round, hypoechoic, homogenous vascular lesions[70]. EUS allows the accurate localization of P-NETs, which would be crucial for surgical interventions. As mentioned before, EUS allows cyto-histological confirmation of neuroendocrine tumors, through guided tissue acquisition for histological procedures[44-53].
Functional imaging of GEP-NENs is based on the typical expression of somatostatin receptors (SSTR) by neuroendocrine cells[71]. In the past, functional studies were performed with 111indium pentetreotide scintigraphy (Octreoscan®); in recent years, PET/CT with somatostatin analogs tracked with gallium-68 (68Ga-SSA PET/CT) has become the modality of choice for SSTR imaging[9,67,72,73]. Functional imaging is indicated for staging, localization of the unknown primary tumor in patients with established neuroendocrine metastases, in vivo demonstration of SSTR expression on neuroendocrine cells (for therapeutic planning), as well as the extent of disease after treatment. The most commonly somatostatin analogs used in the clinical practice are 68Ga-DOTA-Tyr3-octreotide (68Ga-DOTA-TOC), 68Ga-DOTA-Tyr3-octreotate (68Ga-DOTA-TATE) and 68Ga-DOTA-Nal3-octreotide (68Ga-DOTA-NOC). Mean sensitivity of 68Ga-DOTA-SSA PET/CT for the diagnosis of P-NETs was 92%, while specificity was 83%[67,74,75]. In advanced fast-growing G2 and G3 NENs, especially if receptor negativity is demonstrated at 68Ga-SSA PET/CT, 18FDG-PET/CT may be considered in the diagnostic approach[60,67,76].
Nowadays, biochemical diagnosis of NENs has been downsized, due to the high proportion of non-functioning NENs. Considering the high rates of false positive and the heterogeneous serum determinations, Chromogranin A (CgA) should be used in patients with an already documented diagnosis of NEN, in order to establish the treatment response or during the follow-up[77,78], although it results less sensitive for primary diagnosis. On the other hand, Neuron-specific enolase (NSE) is considered an unreliable diagnostic biomarker for NETs, due to low sensitivity and specificity, while no evidence is available regarding its role in follow-up[79].
Laboratory tests for specific biomarkers (gastrin, insulin, glucagon, VIP, 5-HIAA) play an important role in certain clinical syndromes. Elevated gastrin levels (>10-fold) combined with low gastric pH (<2), after discontinuation of PPis for at least one week, are required to establish the diagnosis of Zollinger Ellison Syndrome; a greater diagnostic accuracy is obtained dosing gastrin levels after secretin stimulus. The gold-standard for the biochemical diagnosis of insulinoma is the 72-h fasting test, based on the lack of physiological suppression of insulin during hypoglycemia. A patient suffering from insulinoma in fact exhibits autonomous insulin secretion and fails to suppress insulin secretion, despite the presence of hypoglycemia. An insulinoma is diagnosed in the presence of hypoglycemia (<55 mg/dL) along with inappropriately increased insulin levels (≥ 3 μU/L) and low β-hydroxybutyrate levels (≤ 2.7 mmol/L)[80]. Elevated glucagon levels, usually above 500 pg/mL are observed in glucagon producing P-NETs (glucagonomas)[79]. Elevated vaso-active intestinal peptide (VIP) levels in the presence of typical clinical presentation are considered diagnostic for a Vipoma[81]. 5-hydroxyindoleacetic acid (5-HIAA), detected in 24-hour urine collection using optimal conditions for assay, is the specific tumor marker of carcinoid syndrome. 5-HIAA has demonstrated a diagnostic sensitivity of 70%, with a specificity of 90%[82]. It is not recommended to use 5-HIAA as a screening test in the presence of diarrhea. Instead, it should be used in patients diagnosed with NEN, to confirm carcinoid syndrome and assess its response to therapy[9,82].
Circulating tumor cells, circulating tumor DNA, circulating micro-RNAs, and NETest (simultaneous measurement of 51 neuroendocrine-specific marker genes in the peripheral blood) are novel biomarkers under validation for NENs. NETest has high sensitivity (85%-98%) and specificity (93%-97%) for the detection of GEP-NENs, irrespective of stage and grade of the disease and the use of PPIs and SSAs. It has 93% accuracy in establishing the diagnosis and can be used for monitoring the response to therapy, to detect recurrence and for assessing the prognosis. However, this test is not widely available, and needs further validation[83].
4. Discussion
Our case report describes an old patient with an extremely rare pancreatic neuroendocrine tumor (P-NET), diagnosed in presence of unspecific gastrointestinal symptoms and skin flushing. This observation is even much rarer in old people. Despite symptoms suggesting carcinoid syndrome, tumor was well-differentiated and localized in the pancreas without liver metastases. This presentation is extremely rare, with only a few cases reported in the literature[84-86]. Biochemical testing for serum CgA and urinary 5-HIAA resulted negative. As emphasized before, laboratory biomarkers have been recently downsized, due to the high rates of false positivity and their pharmacological interference, leading to low sensitivity and specificity[77,78,82].
We confirmed the P-NETs diagnosis through contrast-enhanced CT, followed by functional imaging with a gallium-68 DOTATOC integrated PET/CT. Given the small size of tumor (8 mm), we decided to perform an EUS-FNB, in order to make grading and completing the P-NET management and treatment. EUS-FNB confirmed the diagnosis of well-differentiated, low grade (G1) P-NET (CgA +, Synaptophysin +, Ki67 1%).
The association of NETs and carcinoid syndrome occurs in approximately 19% of patients[26], especially in case of liver metastases[25,28]. However, some patients with carcinoid tumor show symptoms of flushing with low or normal levels of 5-HIAA[87,88]. In our case, patient experienced carcinoid symptoms (diarrhea, flushing, unresponsive depression) in absence of documented liver metastases and with negative serum CgA and normal urinary 5-HIAA.
Therefore, imaging and histological examination, remain the major tools in the diagnostic process of NETs with symptoms of carcinoid syndrome. As we reported, performing an EUS-FNB and assessing cyto-histological features could be the protocol of choice in patients with small, low grade, pauci-symptomatic P-NETs in order to avoid or delay surgical treatment. Of note, we would again underscore the concept that P-NET occurrence without metastases in old patients is really very rare.
Author Contributions
Conceptualization, M.R. and L.M.; methodology, M.R. and L.M.; investigation, M.R., N.C., C.S., M.C., A.L., F.M., S.M., S.P., M.I., G.T.; data curation, M.R., N.C., C.S.; writing—original draft preparation, M.R., N.C., C.S., F.M.; writing—review and editing, M.R., L.M.; visualization, M.R.; supervision, L.M., M.I. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki. Ethical review and approval were waived due to the type of the study that is a case report.
Informed Consent Statement
The patient provided written informed consent to publish this manuscript and for material sampling.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
List of Acronyms
| APUD | Amine Precursor Uptake and Decarboxylation |
| CgA | Chromogranin A |
| CHD | Carcinoid heart disease |
| Cr | Creatinine |
| CT | Computed tomography |
| CRP | C-reactive protein |
| eGFR | Estimated glomerular filtration rate |
| ENETS | European Neuroendocrine Tumor Society |
| EUS-FNA | Endoscopic ultrasound with fine-needle aspiration |
| EUS-FNB | Endoscopic ultrasound with fine-needle biopsy |
| FAST | Focused Assessment with Sonography in Trauma |
| 68Ga-DOTA-NOC | gallium-68-DOTA-Nal3-octreotide |
| 68Ga-DOTA-TATE | gallium-68-DOTA-Tyr3-octreotate |
| 68Ga-DOTA-TOC | gallium-68-DOTA-Tyr3-octreotide |
| GEP-NEN | Gastroenteropancreatic neuroendocrine neoplasm |
| GEP-NET | Gastroenteropancreatic neuroendocrine tumor |
| HGT | Hemo Glucose Test |
| 5-HIAA | 5-hydroxyindoleacetic acid |
| 5-HT | serotonin |
| INSM1 | insulinoma-associated protein 1 |
| MEN-1 | Multiple endocrine neoplasia 1 |
| MiNEN | Mixed neuroendocrine-non-neuroendocrine neoplasm |
| MRI | Magnetic resonance imaging |
| NF-P-NET | Non-functional pancreatic neuroendocrine tumor |
| NEC | Neuroendocrine carcinoma |
| NEN | Neuroendocrine neoplasm |
| NET | Neuroendocrine tumor |
| NSE | Neuron-specific enolase |
| P-NET | Pancreatic neuroendocrine tumor |
| PAD | Peripheral artery disease |
| PET | Positive emission tomography |
| PPi | Proton pomp inhibitor |
| SaO2 | Oxygen saturation |
| SSA | Somatostatin analogue |
| SSTR | Somatostatin receptor |
| TNM | Tumor-nodes-metastasis-based staging |
| UICC | 2017 Union for International Cancer Control |
| VHL | von Hippel-Lindau syndrome |
| VIP | Vaso-active intestinal peptide |
| WHO | World health organization |
References
- Yao, J. C.; Hassan, M.; Phan, A.; Dagohoy, C.; Leary, C.; Mares, J. E.; Abdalla, E. K.; Fleming, J. B.; Vauthey, J. N.; Rashid, A.; Evans, D. B. One hundred years after "carcinoid": epidemiology of and prognostic factors for neuroendocrine tumors in 35,825 cases in the United States. Journal of clinical oncology : official journal of the American Society of Clinical Oncology 2008, 26(18), 3063–3072. [Google Scholar] [CrossRef]
- Das, S.; Dasari, A. Epidemiology, Incidence, and Prevalence of Neuroendocrine Neoplasms: Are There Global Differences? Current oncology reports 2021, 23(4), 43. [Google Scholar] [CrossRef]
- Leoncini, E.; Boffetta, P.; Shafir, M.; Aleksovska, K.; Boccia, S.; & Rindi, G. Increased incidence trend of lowgrade and high-grade neuroendocrine neoplasms 2017 Endocrine, 58(2), 368–379. [CrossRef]
- Pavel, M.; Öberg, K.; Falconi, M.; Krenning, E. P.; Sundin, A.; Perren, A.; Berruti, A.; ESMO Guidelines Committee. Gastroenteropancreatic neuroendocrine neoplasms: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Annals of oncology : official journal of the European Society for Medical Oncology 2020 31(7), 844–860. [CrossRef]
- Dasari, A.; Shen, C.; Halperin, D.; Zhao, B.; Zhou, S.; Xu, Y.; Shih, T.; Yao, J. C. Trends in the Incidence, Prevalence, and Survival Outcomes in Patients With Neuroendocrine Tumors in the United States. JAMA oncology, 2017 3(10), 1335–1342. [CrossRef]
- Clement, D.; Ramage, J.; Srirajaskanthan, R. Update on Pathophysiology, Treatment, and Complications of Carcinoid Syndrome. Journal of oncology 2020, 8341426. [Google Scholar] [CrossRef]
- Metz, D. C.; Jensen, R. T. Gastrointestinal neuroendocrine tumors: pancreatic endocrine tumors. Gastroenterology 2008, 135(5), 1469–1492. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Carbonero, R.; Capdevila, J.; Crespo-Herrero, G.; Díaz-Pérez, J. A.; Martínez Del Prado, M. P.; Alonso Orduña, V.; Sevilla-García, I.; Villabona-Artero, C.; Beguiristain-Gómez, A.; Llanos-Muñoz, M. et al. Incidence, patterns of care and prognostic factors for outcome of gastroenteropancreatic neuroendocrine tumors (GEP-NETs): results from the National Cancer Registry of Spain (RGETNE). Annals of oncology : official journal of the European Society for Medical Oncology 2010 21(9), 1794–1803. [CrossRef]
- AIOM for Neuroendocrine Tumors Guide Line 2020. Accessed 15 July 2023 https://www.aiom.it/wp-content/uploads/2020/10/2020_LG_AIOM_Neuroendocrini.pdf.
- Ordóñez, N. G. Broad-spectrum immunohistochemical epithelial markers: a review. Human pathology 2013, 44(7), 1195–1215. [Google Scholar] [CrossRef] [PubMed]
- Moertel, C. G. Karnofsky memorial lecture. An odyssey in the land of small tumors. Journal of Clinical Oncology 1987, 5(10), 1502–1522. [Google Scholar] [CrossRef] [PubMed]
- Ito, T.; Igarashi, H.; Nakamura, K.; Sasano, H.; Okusaka, T.; Takano, K.; Komoto, I.; Tanaka, M.; Imamura, M.; Jensen, R. T.; Takayanagi, R.; Shimatsu, A. Epidemiological trends of pancreatic and gastrointestinal neuroendocrine tumors in Japan: a nationwide survey analysis. Journal of gastroenterology 2015, 50(1), 58–64. [Google Scholar] [CrossRef]
- Cho, M. Y.; Kim, J. M.; Sohn, J. H.; Kim, M. J.; Kim, K. M.; Kim, W. H.; Kim, H.; Kook, M. C.; Park, D. Y.; Lee, J. H.; et al. Current Trends of the Incidence and Pathological Diagnosis of Gastroenteropancreatic Neuroendocrine Tumors (GEP-NETs) in Korea 2000-2009: Multicenter Study. Cancer research and treatment 2012, 44(3), 157–165. [Google Scholar] [CrossRef]
- Scherübl, H.; Streller, B.; Stabenow, R.; Herbst, H.; Höpfner, M.; Schwertner, C.; Steinberg, J.; Eick, J.; Ring, W.; Tiwari, K.; et al. Clinically detected gastroenteropancreatic neuroendocrine tumors are on the rise: epidemiological changes in Germany. World journal of gastroenterology 2013, 19(47), 9012–9019. [Google Scholar] [CrossRef]
- White, B. E.; Rous, B.; Chandrakumaran, K.; Wong, K.; Bouvier, C.; Van Hemelrijck, M.; George, G.; Russell, B.; Srirajaskanthan, R.; Ramage, J. K. Incidence and survival of neuroendocrine neoplasia in England 1995-2018: A retrospective, population-based study. The Lancet regional health. Europe 2022, 23, 100510. [Google Scholar] [CrossRef]
- Nagtegaal, I. D.; Odze, R. D.; Klimstra, D.; Paradis, V.; Rugge, M.; Schirmacher, P.; Washington, K. M.; Carneiro, F.; Cree, I. A.; WHO Classification of Tumours Editorial Board. The 2019 WHO classification of tumours of the digestive system. Histopathology 2020, 76(2), 182–188. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, C. J.; Agarwal, M.; Pottakkat, B.; Haroon, N. N.; George, A. S; Pappachan, J. M. Gastroenteropancreatic neuroendocrine neoplasms: A clinical snapshot. World journal of gastrointestinal surgery 2021, 13(3), 231–255. [Google Scholar] [CrossRef] [PubMed]
- Klöppel, G.; Perren, A.; Heitz, P. U. The gastroenteropancreatic neuroendocrine cell system and its tumors: the WHO classification. Annals of the New York Academy of Sciences 2004, 1014, 13–27. [Google Scholar] [CrossRef] [PubMed]
- Lloyd, R.V.; Osamura, R.Y.; Klöppel, G.; Rosai, J. WHO classification of tumours of endocrine organs, 2017 vol. 10. 4th ed. Lyon: International Agency for Research on Cancer.
- Modlin, I. M.; Lye, K. D.; Kidd, M. A 5-decade analysis of 13,715 carcinoid tumors. Cancer 2003, 97(4), 934–959. [Google Scholar] [CrossRef]
- Cives, M.; Strosberg, J. R. Gastroenteropancreatic neuroendocrine tumors. CA: a cancer journal for clinicians 2018 68(6), 471-487. [CrossRef]
- Turaga, K.K.; Kvols, L.K. Recent progress in the understanding, diagnosis, and treatment of gastroenteropancreatic neuroendocrine tumors. CA Cancer J Clin. 2011, 61(2), 113–32. [Google Scholar] [CrossRef]
- Zerbi, A.; Falconi, M.; Rindi, G.; Delle Fave, G.; Tomassetti, P.; Pasquali, C.; Capitanio, V.; Boninsegna, L.; Di Carlo, V.; AISP-Network Study Group. Clinicopathological features of pancreatic endocrine tumors: a prospective multicenter study in Italy of 297 sporadic cases. The American journal of gastroenterology 2010 105(6), 1421–1429. [CrossRef]
- Jensen, R. T.; Cadiot, G.; Brandi, M. L.; de Herder, W. W.; Kaltsas, G.; Komminoth, P.; Scoazec, J. Y.; Salazar, R.; Sauvanet, A.; Kianmanesh, R.; Barcelona Consensus Conference participants. ENETS Consensus Guidelines for the management of patients with digestive neuroendocrine neoplasms: functional pancreatic endocrine tumor syndromes. Neuroendocrinology 2012 95(2), 98–119. [CrossRef]
- Gade, A. K.; Olariu, E.; Douthit, N. T. Carcinoid Syndrome: A Review. Cureus 2020, 12(3), e7186. [Google Scholar] [CrossRef]
- Halperin, D. M.; Shen, C.; Dasari, A.; Xu, Y.; Chu, Y.; Zhou, S.; Shih, Y. T.; Yao, J. C. Frequency of carcinoid syndrome at neuroendocrine tumour diagnosis: a population-based study. The Lancet. Oncology 2017, 18(4), 525–534. [Google Scholar] [CrossRef]
- Mota, J. M.; Sousa, L. G.; Riechelmann, R. P. Complications from carcinoid syndrome: review of the current evidence. Ecancermedicalscience 2016, 10, 662. [Google Scholar] [CrossRef]
- Kvols L., K. Metastatic carcinoid tumors and the malignant carcinoid syndrome. Annals of the New York Academy of Sciences 1994, 733, 464–470. [Google Scholar] [CrossRef]
- Ahmed, M. Gastrointestinal neuroendocrine tumors in 2020. World journal of gastrointestinal oncology 2020, 12(8), 791–807. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharyya, S.; Davar, J.; Dreyfus, G.; Caplin, M. E. Carcinoid heart disease. Circulation 2007, 116(24), 2860–2865. [Google Scholar] [CrossRef] [PubMed]
- Druce, M.; Rockall, A.; Grossman, A. B. Fibrosis and carcinoid syndrome: from causation to future therapy. Nature reviews. Endocrinology 2009, 5(5), 276–283. [Google Scholar] [CrossRef] [PubMed]
- Dobson, R.; Burgess, M. I.; Pritchard, D. M.; Cuthbertson, D. J. The clinical presentation and management of carcinoid heart disease. International journal of cardiology 2014, 173(1), 29–32. [Google Scholar] [CrossRef] [PubMed]
- Rubin de Celis Ferrari, A. C.; Glasberg, J.; Riechelmann, R. P. Carcinoid syndrome: update on the pathophysiology and treatment. Clinics (Sao Paulo, Brazil) 2018 73(suppl 1), e490s. [CrossRef]
- Russo, S.; Boon, J. C.; Kema, I. P.; Willemse, P. H.; den Boer, J. A.; Korf, J.; de Vries, E. G. Patients with carcinoid syndrome exhibit symptoms of aggressive impulse dysregulation. Psychosomatic medicine 2004, 66(3), 422–425. [Google Scholar] [CrossRef] [PubMed]
- Kohen, I.; Arbouet, S. Neuroendocrine carcinoid cancer associated with psychosis. Psychiatry (Edgmont (Pa. : Township)) 2008 5(6), 29–30.
- Nobels, A.; Geboes, K.; Lemmens, G. M. May depressed and anxious patients with carcinoid syndrome benefit from treatment with selective serotonin reuptake inhibitors (SSRIs)?: findings from a case report. Acta oncologica (Stockholm, Sweden) 2016 55(11), 1370–1372. [CrossRef]
- Tatsumoto, S.; Kodama, Y.; Sakurai, Y.; Shinohara, T.; Katanuma, A.; Maguchi, H. Pancreatic neuroendocrine neoplasm: correlation between computed tomography enhancement patterns and prognostic factors of surgical and endoscopic ultrasound-guided fine-needle aspiration biopsy specimens. Abdominal imaging 2013, 38(2), 358–366. [Google Scholar] [CrossRef] [PubMed]
- Grillo, F.; Albertelli, M.; Brisigotti, M. P.; Borra, T.; Boschetti, M.; Fiocca, R.; Ferone, D.; Mastracci, L. Grade Increases in Gastroenteropancreatic Neuroendocrine Tumor Metastases Compared to the Primary Tumor. Neuroendocrinology 2016, 103(5), 452–459. [Google Scholar] [CrossRef]
- Cree, I. A.; Tan, P. H.; Travis, W. D.; Wesseling, P.; Yagi, Y.; White, V. A.; Lokuhetty, D.; Scolyer, R. A. Counting mitoses: SI(ze) matters!. Modern pathology : an official journal of the United States and Canadian Academy of Pathology, Inc 2021 34(9), 1651–1657. [CrossRef]
- Huang, W.; Nebiolo, C.; Esbona, K.; Hu, R.; Lloyd, R. Ki67 index and mitotic count: Correlation and variables affecting the accuracy of the quantification in endocrine/neuroendocrine tumors. Annals of diagnostic pathology 2020, 48, 151586. [Google Scholar] [CrossRef]
- Rindi, G.; Mete, O.; Uccella, S.; Basturk, O.; La Rosa, S.; Brosens, L. A. A.; Ezzat, S.; de Herder, W. W.; Klimstra, D. S.; Papotti, M.; et al. Overview of the 2022 WHO Classification of Neuroendocrine Neoplasms. Endocrine pathology 2022, 33(1), 115–154. [Google Scholar] [CrossRef]
- Rosenbaum, J. N.; Guo, Z.; Baus, R. M.; Werner, H.; Rehrauer, W. M.; Lloyd, R. V. INSM1: A Novel Immunohistochemical and Molecular Marker for Neuroendocrine and Neuroepithelial Neoplasms. American journal of clinical pathology 2015, 144(4), 579–591. [Google Scholar] [CrossRef]
- Maleki, Z.; Nadella, A.; Nadella, M.; Patel, G.; Patel, S.; Kholová, I. INSM1, a Novel Biomarker for Detection of Neuroendocrine Neoplasms: Cytopathologists' View. Diagnostics (Basel, Switzerland) 2021 11(12), 2172. [CrossRef]
- Atiq, M.; Bhutani, M. S.; Bektas, M.; Lee, J. E.; Gong, Y.; Tamm, E. P.; Shah, C. P.; Ross, W. A.; Yao, J.; Raju, G. S.; et al. EUS-FNA for pancreatic neuroendocrine tumors: a tertiary cancer center experience. Digestive diseases and sciences 2012, 57(3), 791–800. [Google Scholar] [CrossRef] [PubMed]
- Larghi, A.; Capurso, G.; Carnuccio, A.; Ricci, R.; Alfieri, S.; Galasso, D.; Lugli, F.; Bianchi, A.; Panzuto, F.; De Marinis, L.; et al. Ki-67 grading of nonfunctioning pancreatic neuroendocrine tumors on histologic samples obtained by EUS-guided fine-needle tissue acquisition: a prospective study. Gastrointestinal endoscopy 2012, 76(3), 570–577. [Google Scholar] [CrossRef]
- Unno, J.; Kanno, A.; Masamune, A.; Kasajima, A.; Fujishima, F.; Ishida, K.; Hamada, S.; Kume, K.; Kikuta, K.; Hirota, M. et al. The usefulness of endoscopic ultrasound-guided fine-needle aspiration for the diagnosis of pancreatic neuroendocrine tumors based on the World Health Organization classification. Scandinavian journal of gastroenterology 2014 49(11), 1367–1374. [CrossRef]
- Paiella, S.; Landoni, L.; Rota, R.; Valenti, M.; Elio, G.; Crinò, S. F.; Manfrin, E.; Parisi, A.; Cingarlini, S; D'Onofrio, M. et al. Endoscopic ultrasound-guided fine-needle aspiration for the diagnosis and grading of pancreatic neuroendocrine tumors: a retrospective analysis of 110 cases. Endoscopy 2020 52(11), 988–994. [CrossRef]
- Crinò, S. F.; Ammendola, S.; Meneghetti, A.; Bernardoni, L.; Conti Bellocchi, M. C.; Gabbrielli, A.; Landoni, L.; Paiella, S.; Pin, F.; Parisi, A. et al. Comparison between EUS-guided fine-needle aspiration cytology and EUS-guided fine-needle biopsy histology for the evaluation of pancreatic neuroendocrine tumors. Pancreatology 2021 21(2), 443–450. [CrossRef]
- Rimbaş, M.; Crino, S. F.; Gasbarrini, A.; Costamagna, G.; Scarpa, A.; Larghi, A. EUS-guided fine-needle tissue acquisition for solid pancreatic lesions: Finally moving from fine-needle aspiration to fine-needle biopsy? Endoscopic ultrasound 2018, 7(3), 137–140. [Google Scholar] [CrossRef]
- Eusebi, L. H.; Thorburn, D.; Toumpanakis, C.; Frazzoni, L.; Johnson, G.; Vessal, S.; Luong, T. V.; Caplin, M.; Pereira, S. P. Endoscopic ultrasound-guided fine-needle aspiration vs fine-needle biopsy for the diagnosis of pancreatic neuroendocrine tumors. Endoscopy international open 2019, 7(11), E1393–E1399. [Google Scholar] [CrossRef] [PubMed]
- Di Leo, M.; Poliani, L.; Rahal, D.; Auriemma, F.; Anderloni, A.; Ridolfi, C.; Spaggiari, P.; Capretti, G.; Di Tommaso, L.; Preatoni, P. et al. Pancreatic Neuroendocrine Tumours: The Role of Endoscopic Ultrasound Biopsy in Diagnosis and Grading Based on the WHO 2017 Classification. Digestive diseases (Basel, Switzerland) 2019 37(4), 325–333. [CrossRef]
- Leeds, J. S.; Nayar, M. K.; Bekkali, N. L. H.; Wilson, C. H.; Johnson, S. J.; Haugk, B.; Darne, A.; Oppong, K. W. Endoscopic ultrasound-guided fine-needle biopsy is superior to fine-needle aspiration in assessing pancreatic neuroendocrine tumors. Endoscopy international open 2019, 7(10), E1281–E1287. [Google Scholar] [CrossRef]
- Melita, G.; Pallio, S.; Tortora, A.; Crinò, S. F.; Macrì, A.; Dionigi, G. Diagnostic and Interventional Role of Endoscopic Ultrasonography for the Management of Pancreatic Neuroendocrine Neoplasms. Journal of clinical medicine 2021, 10(12), 2638. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, J.; Ustun, B.; Alomari, A.; Bao, F.; Aslanian, H. R.; Siddiqui, U.; Chhieng, D.; Cai, G. Performance of endoscopic ultrasound-guided fine needle aspiration in diagnosing pancreatic neuroendocrine tumors. CytoJournal 2013, 10, 10. [Google Scholar] [CrossRef]
- Boutsen, L.; Jouret-Mourin, A.; Borbath, I.; van Maanen, A.; Weynand, B. Accuracy of Pancreatic Neuroendocrine Tumour Grading by Endoscopic Ultrasound-Guided Fine Needle Aspiration: Analysis of a Large Cohort and Perspectives for Improvement. Neuroendocrinology 2018, 106(2), 158–166. [Google Scholar] [CrossRef]
- Heidsma, C. M.; Tsilimigras, D. I.; Rocha, F.; Abbott, D. E.; Fields, R.; Smith, P. M.; Poultsides, G. A.; Cho, C.; van Eijck, C.; van Dijkum, E. N. et al. Clinical relevance of performing endoscopic ultrasound-guided fine-needle biopsy for pancreatic neuroendocrine tumors less than 2 cm. Journal of surgical oncology 2020 122(7), 1393–1400. [CrossRef]
- Gratian, L.; Pura, J.; Dinan, M.; Roman, S.; Reed, S.; Sosa, J. A. Impact of extent of surgery on survival in patients with small nonfunctional pancreatic neuroendocrine tumors in the United States. Annals of surgical oncology 2014, 21(11), 3515–3521. [Google Scholar] [CrossRef]
- Sharpe, S. M.; In, H.; Winchester, D. J.; Talamonti, M. S.; Baker, M. S. Surgical resection provides an overall survival benefit for patients with small pancreatic neuroendocrine tumors. Journal of gastrointestinal surgery 19(1), 117–123. [CrossRef]
- Sallinen, V.; Haglund, C.; Seppänen, H. Outcomes of resected nonfunctional pancreatic neuroendocrine tumors: Do size and symptoms matter? Surgery 2015, 158(6), 1556–1563. [Google Scholar] [CrossRef] [PubMed]
- Falconi, M.; Eriksson, B.; Kaltsas, G.; Bartsch, D. K.; Capdevila, J.; Caplin, M.; Kos-Kudla, B.; Kwekkeboom, D.; Rindi, G.; Klöppel, G. et al. ENETS Consensus Guidelines Update for the Management of Patients with Functional Pancreatic Neuroendocrine Tumors and Non-Functional Pancreatic Neuroendocrine Tumors. Neuroendocrinology 2016 103(2), 153–171. [CrossRef]
- Delle Fave, G.; O'Toole, D.; Sundin, A.; Taal, B.; Ferolla, P.; Ramage, J. K.; Ferone, D.; Ito, T.; Weber, W.; Zheng-Pei, Z.; et al. ENETS Consensus Guidelines Update for Gastroduodenal Neuroendocrine Neoplasms. Neuroendocrinology 2016, 103(2), 119–124. [Google Scholar] [CrossRef] [PubMed]
- Ramage, J. K.; De Herder, W. W.; Delle Fave, G.; Ferolla, P.; Ferone, D.; Ito, T.; Ruszniewski, P.; Sundin, A.; Weber, W.; Zheng-Pei, Z.; et al. ENETS Consensus Guidelines Update for Colorectal Neuroendocrine Neoplasms. Neuroendocrinology 2016, 103(2), 139–143. [Google Scholar] [CrossRef] [PubMed]
- Bertero, L.; Massa, F.; Metovic, J.; Zanetti, R.; Castellano, I.; Ricardi, U.; Papotti, M.; Cassoni, P. Eighth Edition of the UICC Classification of Malignant Tumours: an overview of the changes in the pathological TNM classification criteria-What has changed and why?. Virchows Archiv : an international journal of pathology 2018 472(4), 519–531. [CrossRef]
- Rindi, G.; Klöppel, G.; Alhman, H.; Caplin, M.; Couvelard, A.; de Herder, W. W.; Erikssson, B.; Falchetti, A.; Falconi, M.; Komminoth, P. et al. TNM staging of foregut (neuro)endocrine tumors: a consensus proposal including a grading system. Virchows Archiv : an international journal of pathology 2006 449(4), 395–401. [CrossRef]
- Yang, M.; Ke, N. W.; Zhang, Y.; Tan, C. L.; Tian, B. L.; Liu, X. B.; Huang, W.; Nunes, Q.; Sutton, R. Functional and non-functional pancreatic neuroendocrine tumours: ENETS or AJCC TNM staging system? Oncotarget 2017, 8(47), 82784–82795. [Google Scholar] [CrossRef] [PubMed]
- Morse, B.; Al-Toubah, T.; Montilla-Soler, J. Anatomic and functional imaging of neuroendocrine tumors. Current treatment options in oncology 2020, 21(9), 75. [Google Scholar] [CrossRef] [PubMed]
- Sundin, A.; Arnold, R.; Baudin, E.; Cwikla, J. B.; Eriksson, B.; Fanti, S.; Fazio, N.; Giammarile, F.; Hicks, R. J.; Kjaer, A. et al. ENETS Consensus Guidelines for the Standards of Care in Neuroendocrine Tumors: Radiological, Nuclear Medicine & Hybrid Imaging. Neuroendocrinology 2017 105(3), 212–244. [CrossRef]
- Caramella, C.; Dromain, C.; De Baere, T.; Boulet, B.; Schlumberger, M.; Ducreux, M.; Baudin, E. Endocrine pancreatic tumours: which are the most useful MRI sequences? European radiology 2010, 20(11), 2618–2627. [Google Scholar] [CrossRef]
- Dromain, C.; de Baere, T.; Lumbroso, J.; Caillet, H.; Laplanche, A.; Boige, V.; Ducreux, M.; Duvillard, P.; Elias, D. et al. Detection of liver metastases from endocrine tumors: a prospective comparison of somatostatin receptor scintigraphy, computed tomography, and magnetic resonance imaging. Journal of clinical oncology 2005 23(1), 70–78. [CrossRef]
- Lee, D. W.; Kim, M. K.; Kim, H. G. Diagnosis of Pancreatic Neuroendocrine Tumors. Clinical endoscopy 2017, 50(6), 537–545. [Google Scholar] [CrossRef]
- Rust, E.; Hubele, F.; Marzano, E.; Goichot, B.; Pessaux, P.; Kurtz, J. E.; Imperiale, A. Nuclear medicine imaging of gastro-entero-pancreatic neuroendocrine tumors. The key role of cellular differentiation and tumor grade: from theory to clinical practice. Cancer imaging 2012 12(1), 173–184. [CrossRef]
- Buchmann, I.; Henze, M.; Engelbrecht, S.; Eisenhut, M.; Runz, A.; Schäfer, M.; Schilling, T.; Haufe, S.; Herrmann, T.; Haberkorn, U. Comparison of 68Ga-DOTATOC PET and 111In-DTPAOC (Octreoscan) SPECT in patients with neuroendocrine tumours. European journal of nuclear medicine and molecular imaging 2007, 34(10), 1617–1626. [Google Scholar] [CrossRef]
- Van Binnebeek, S.; Vanbilloen, B.; Baete, K.; Terwinghe, C.; Koole, M.; Mottaghy, F. M.; Clement, P. M.; Mortelmans, L.; Bogaerts, K.; Haustermans, K. et al. Comparison of diagnostic accuracy of (111)In-pentetreotide SPECT and (68)Ga-DOTATOC PET/CT: A lesion-by-lesion analysis in patients with metastatic neuroendocrine tumours. European radiology 2016 26(3), 900–909. [CrossRef]
- Treglia, G.; Castaldi, P.; Rindi, G.; Giordano, A.; Rufini, V. Diagnostic performance of Gallium-68 somatostatin receptor PET and PET/CT in patients with thoracic and gastroenteropancreatic neuroendocrine tumours: a meta-analysis. Endocrine, 42(1) 2012 80–87. [CrossRef]
- Bozkurt, M. F.; Virgolini, I.; Balogova, S.; Beheshti, M.; Rubello, D.; Decristoforo, C.; Ambrosini, V.; Kjaer, A.; Delgado-Bolton, R.; Kunikowska, J. et al. Guideline for PET/CT imaging of neuroendocrine neoplasms with 68Ga-DOTA-conjugated somatostatin receptor targeting peptides and 18F-DOPA. European journal of nuclear medicine and molecular imaging 2017 44(9), 1588–1601. [CrossRef]
- Binderup, T.; Knigge, U.; Loft, A.; Federspiel, B.; Kjaer, A. 18F-fluorodeoxyglucose positron emission tomography predicts survival of patients with neuroendocrine tumors. Clinical cancer research 2010, 16(3), 978–985. [Google Scholar] [CrossRef]
- Leon, A.; Torta, M.; Dittadi, R.; degli Uberti, E.; Ambrosio, M. R.; Delle Fave, G.; De Braud, F.; Tomassetti, P.; Gion, M.; Dogliotti, L. Comparison between two methods in the determination of circulating chromogranin A in neuroendocrine tumors (NETs): results of a prospective multicenter observational study. The International journal of biological markers 2005, 20(3), 156–168. [Google Scholar] [CrossRef]
- Welin, S.; Stridsberg, M.; Cunningham, J.; Granberg, D.; Skogseid, B.; Oberg, K.; Eriksson, B.; Janson, E. T. Elevated plasma chromogranin A is the first indication of recurrence in radically operated midgut carcinoid tumors. Neuroendocrinology 2009, 89(3), 302–307. [Google Scholar] [CrossRef]
- Sansone, A.; Lauretta, R.; Vottari, S.; Chiefari, A.; Barnabei, A.; Romanelli, F.; Appetecchia, M. Specific and Non-Specific Biomarkers in Neuroendocrine Gastroenteropancreatic Tumors. Cancers 2019, 11, 1113. [Google Scholar] [CrossRef]
- Cryer, P. E.; Axelrod, L.; Grossman, A. B.; Heller, S. R.; Montori, V. M.; Seaquist, E. R.; Service, F. J. ; Endocrine Society Evaluation and management of adult hypoglycemic disorders: an Endocrine Society Clinical Practice Guideline. The Journal of clinical endocrinology and metabolism 2009, 94(3), 709–728. [Google Scholar] [CrossRef] [PubMed]
- Bloom S., R. Vasoactive intestinal peptide, the major mediator of the WDHA (pancreatic cholera) syndrome: value of measurement in diagnosis and treatment. The American journal of digestive diseases 1978, 23(4), 373–376. [Google Scholar] [CrossRef] [PubMed]
- Oberg, K.; Couvelard, A.; Delle Fave, G.; Gross, D.; Grossman, A.; Jensen, R. T.; Pape, U. F.; Perren, A.; Rindi, G.; Ruszniewski, P. et al. ENETS Consensus Guidelines for Standard of Care in Neuroendocrine Tumours: Biochemical Markers. Neuroendocrinology 2017 105(3), 201–211. [CrossRef]
- Ma, Z. Y.; Gong, Y. F.; Zhuang, H. K.; Zhou, Z. X.; Huang, S. Z.; Zou, Y. P.; Huang, B. W.; Sun, Z. H.; Zhang, C. Z. et al. Pancreatic neuroendocrine tumors: A review of serum biomarkers, staging, and management. World journal of gastroenterology 2020 26(19), 2305–2322. [CrossRef]
- Feldman, J. M.; Jones, R. S. Carcinoid syndrome from gastrointestinal carcinoids without liver metastasis. Annals of surgery 1982, 196(1), 33–37. [Google Scholar] [CrossRef] [PubMed]
- Zavras, N.; Schizas, D.; Machairas, N.; Damaskou, V.; Economopoulos, N.; Machairas, A. Carcinoid syndrome from a carcinoid tumor of the pancreas without liver metastases: A case report and literature review. Oncology letters 2017, 13(4), 2373–2376. [Google Scholar] [CrossRef] [PubMed]
- Famerée, L.; Van Lier, C.; Borbath, I.; Yildiz, H.; Lemaire, J.; Baeck, M. Misleading clinical presentation of carcinoid syndrome. Acta gastro-enterologica Belgica 2021 84(3), 501–503. [CrossRef]
- Oberg, K.; Janson, E. T.; Eriksson, B. Tumour markers in neuroendocrine tumours. Italian journal of gastroenterology and hepatology 1999, 31 Suppl 2, S160–S162. [Google Scholar]
- Eriksson, B. , Oberg, K., & Stridsberg, M. (2000). Tumor markers in neuroendocrine tumors. Digestion 62 Suppl 1, 33–38. [CrossRef]
Figure 1.
Contrast-enhanced abdominal CT scan: axial section showing a homogeneous and hypervascular mass of 8 mm (red arrow) on arterial phase.
Figure 1.
Contrast-enhanced abdominal CT scan: axial section showing a homogeneous and hypervascular mass of 8 mm (red arrow) on arterial phase.
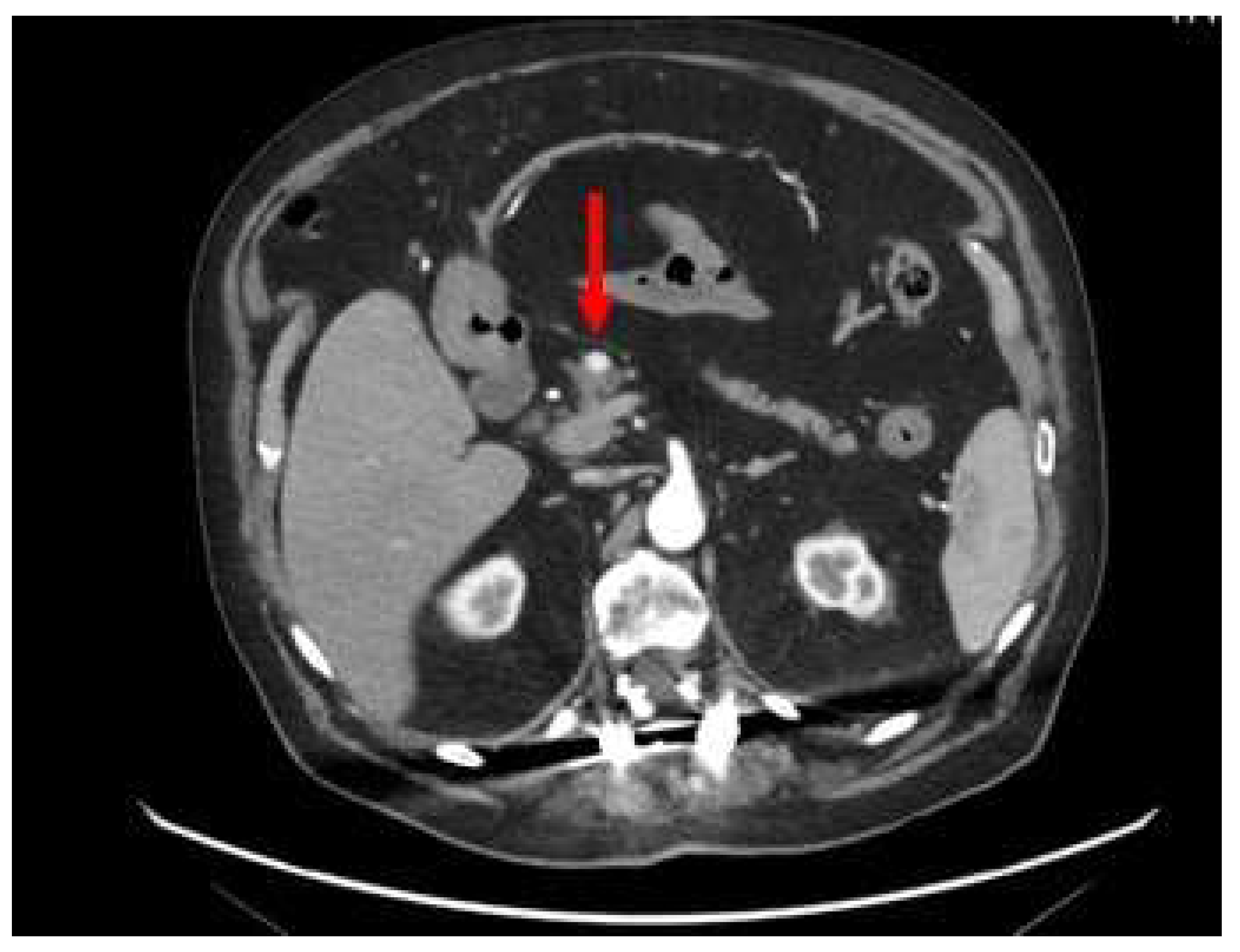
Figure 2.
68Ga-DOTA-TOC integrated PET/CT, transaxial (A) and MIP (B), shows focal and intense uptake in the primary pancreatic lesion (red arrows), with elevated expression of SSTR2/5 somatostatin receptors.
Figure 2.
68Ga-DOTA-TOC integrated PET/CT, transaxial (A) and MIP (B), shows focal and intense uptake in the primary pancreatic lesion (red arrows), with elevated expression of SSTR2/5 somatostatin receptors.
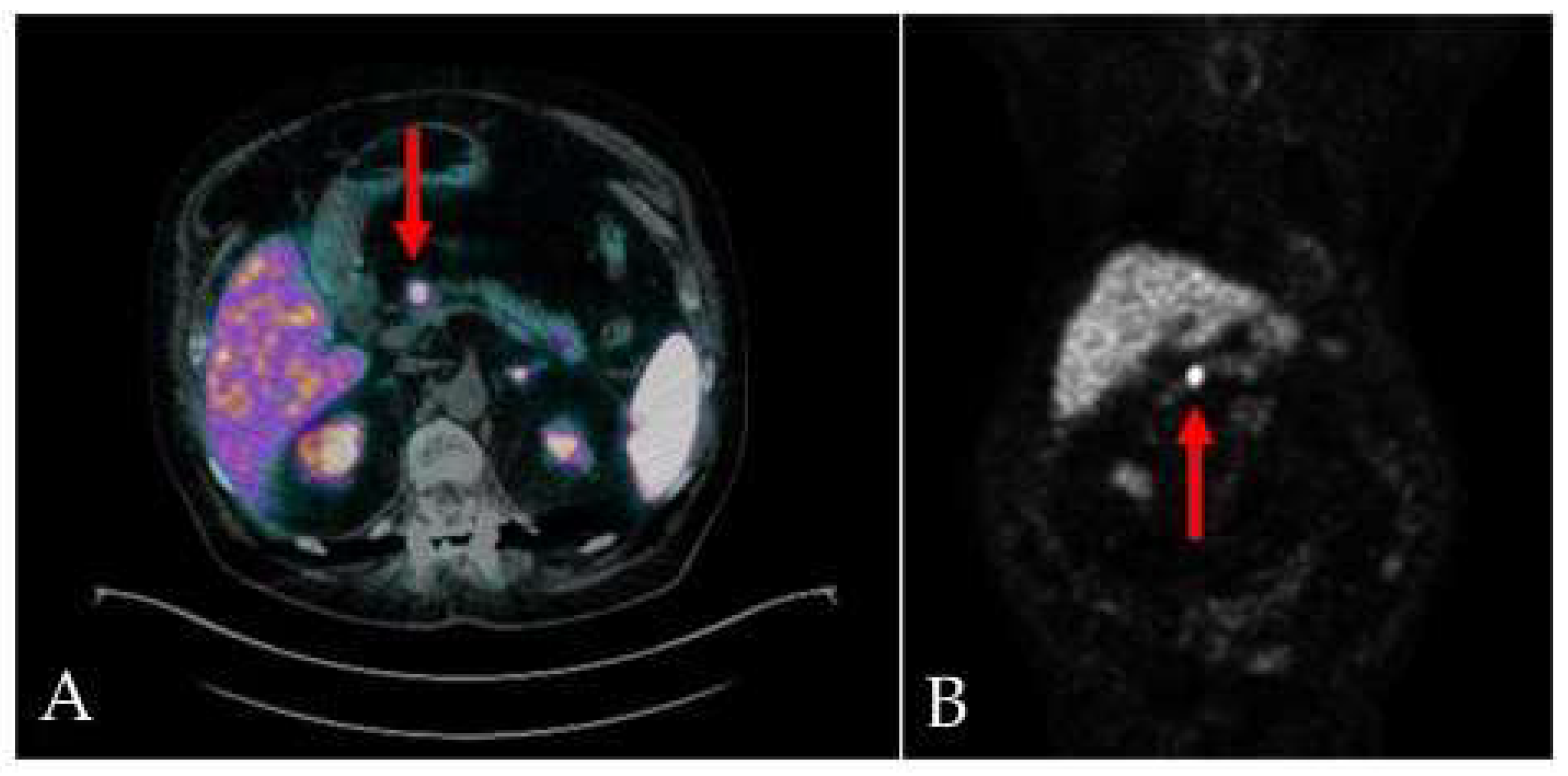
Figure 3.
Endoscopic ultrasound (EUS) image (red arrow) of a small, well rounded, hypo-echogenic lesion with regular margin and a major axis of 8.9 mm.
Figure 3.
Endoscopic ultrasound (EUS) image (red arrow) of a small, well rounded, hypo-echogenic lesion with regular margin and a major axis of 8.9 mm.
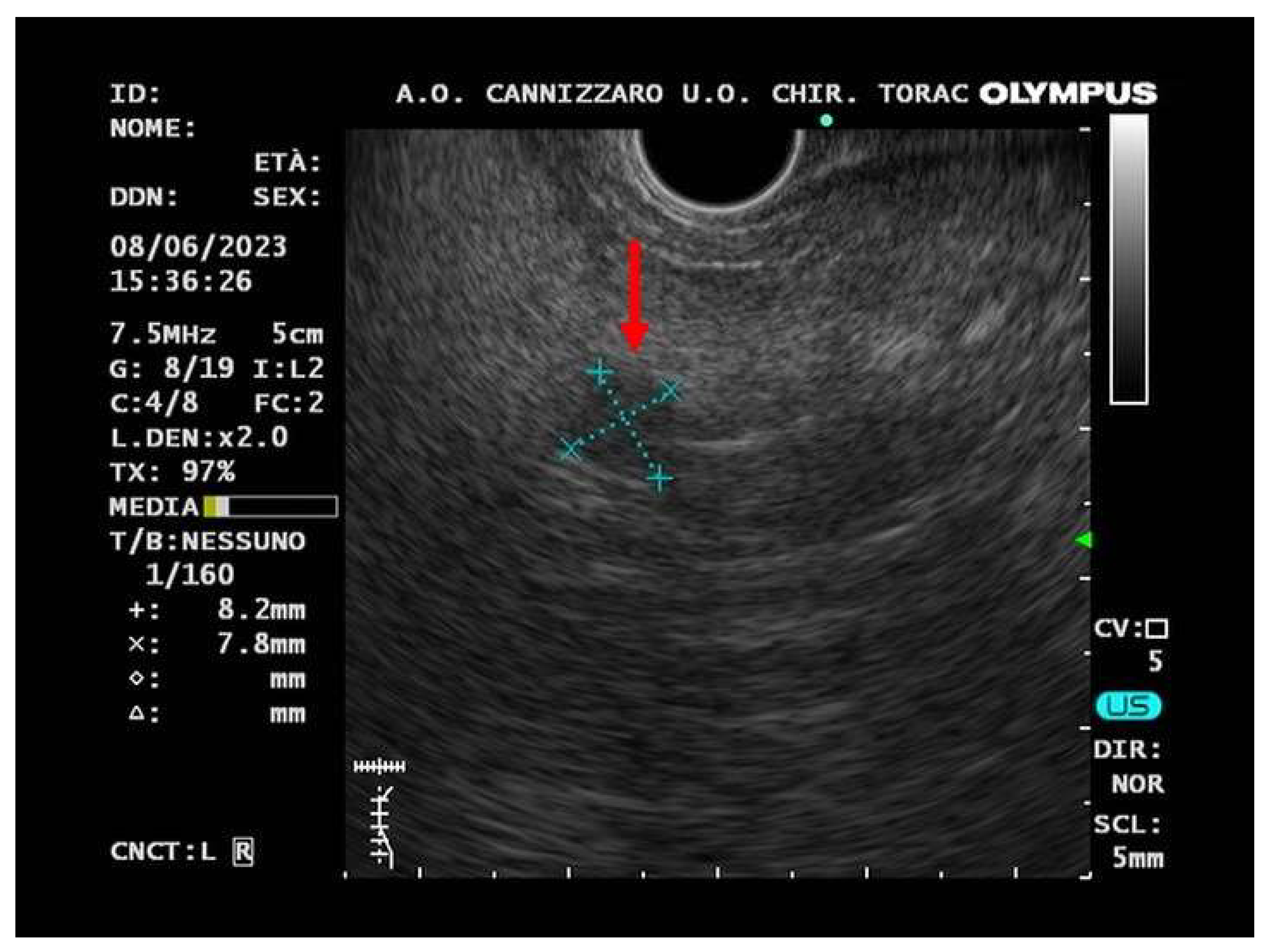
Figure 4.
(A) Fine needle biopsy allows to obtain microcores of sample tissue; then, using pipette, microcores were picked up to be treated as traditional biopsy. (B) Microcores were composed by abundant blood and entrapped epithelial elements of pancreatic tissue. (C) A monomorphic population of epithelial cells, in solid sheets or small nodules, with granular cytoplasm and nuclei with dense chromatin, was observed. Immunohistochemistry reveals positivity for neuroendocrine markers, such as Chromogranin A (D) and Synaptophysin (E); the absence of mitosis and necrosis together with low Ki 67 index (F), allow the diagnosis of low grade neuroendocrine neoplasm.
Figure 4.
(A) Fine needle biopsy allows to obtain microcores of sample tissue; then, using pipette, microcores were picked up to be treated as traditional biopsy. (B) Microcores were composed by abundant blood and entrapped epithelial elements of pancreatic tissue. (C) A monomorphic population of epithelial cells, in solid sheets or small nodules, with granular cytoplasm and nuclei with dense chromatin, was observed. Immunohistochemistry reveals positivity for neuroendocrine markers, such as Chromogranin A (D) and Synaptophysin (E); the absence of mitosis and necrosis together with low Ki 67 index (F), allow the diagnosis of low grade neuroendocrine neoplasm.
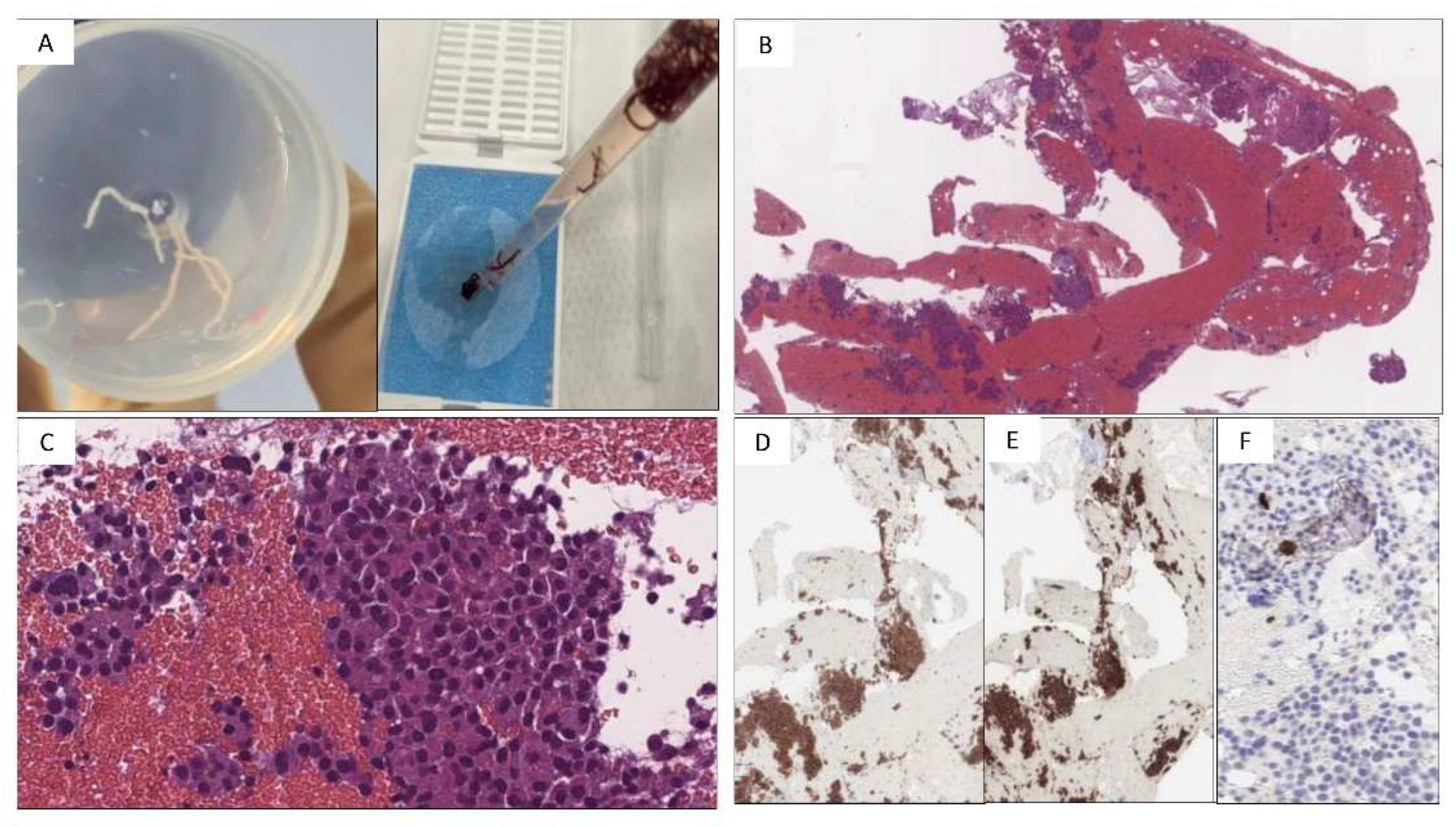

Table 1.
2019 WHO classification and grading criteria for gastroenteropancreatic neuroendocrine neoplasms (GEP-NENs)[16].
Table 1.
2019 WHO classification and grading criteria for gastroenteropancreatic neuroendocrine neoplasms (GEP-NENs)[16].
| Differentiation | Grade | Mitotic rate (mitoses/2 mm2) | Ki-67 index | |
| NET, G1 | Well differentiated | Low | <2 | <3% |
| NET, G2 | Intermediate | 2-20 | 3-20% | |
| NET, G3 | High | >20 | >20% | |
| NEC, small-cell type | Poorly differentiated | High | >20 | >20% |
| NEC, large-cell type | >20 | >20% | ||
| MiNEN | Well or poorly differentiated | Variable | Variable | Variable |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



