
Submitted:
08 August 2023
Posted:
09 August 2023
You are already at the latest version
Abstract
Background: The aim of this study was to design and analyze the content validity of an instrument to assess the risk of behaviors associated with the Chemsex phenomenon since there is currently no instrument with this objective. Method: Firstly, a bank of items identified from the literature was elaborated. Secondly, 50 experts with knowledge of the Chemsex phenomenon at the national level were contacted. A Delphi group was formed with them to carry out two rounds of item evaluation (comprehension and appropriateness) using a Likert scale of 1 to 5. To assess linguistic validity, the mean score of the item comprehension scores was used. The content validity index (CVI) and Aiken's V (VdA) were calculated for each item. A minimum value of CVI and VdA of 0.6 was established to include the items in the questionnaire. Results: In the first round of evaluation, 36 experts evaluated 114 items, of which 61 were selected. In a second round, 30 experts evaluated the 61 items selected, leaving the scale finally made up of 52 items. Conclusion: A questionnaire has been designed to assess the risk of behaviors associated with the Chemsex phenomenon. The items that make up the questionnaire have shown adequate content and linguistic validity, so this instrument can be considered valid. The Delphi method proved to be a useful technique for the proposed objective.
Keywords:
Delphi technique
; Expert consensus
; Validity
; Experts judgment
; psychometrics
1. Introduction
Chemsex understood as "the intentional use of stimulant drugs to have sex for a long period of time among gay, bisexual and other men who have sex with men" is a public health problem because of the increased incidence of cases [1,2] and because of the consequences on the physical and mental health of those who practice it [3,4,5,6]. According to Madrid's recent 2022-2026 Addictions Plan, care for people who practice chemsex has increased from 50 in 2017 to 351 in 2021, an increase of 602% in the number of people served in recent years [7].
It should also be noted that the increased use of geolocation applications has led to an increase in unprotected sexual encounters, which is associated with increased risk behaviors for sexually transmitted infections (STIs) [4,8]. Previous studies indicate association of chemsex with the priority consumption of substances such as mephredrone, methamphetamine, cocaine, GHB/GHL [9] and the search for achievement of emotions, pleasurable sensations, and management of negative symptoms [10]. Other studies indicate that individuals with substance use-related problems used in chemsex may have experienced early adverse events and may have an avoidant-insecure attachment style. In addition, those who have been diagnosed with HIV may show greater emotional dysregulation and worse self-care patterns. These variables should be routinely assessed in this population [11].
The assessment of mood disorders and addiction linked to the practice of chemsex is of interest given the psychoactive substances used [11]. The practice of chemsex has been linked to increased suicide sexually transmitted infections (STIs) [12,13,14,15] increase in psychosis [16] mental problems [9] and decreased adherence to pre-exposure prophylaxis treatment (PrEP) among others [17].
It is of interest to raise awareness of chemsex as a public health problem among gay, bisexual and men who have sex with men (GBMSM). Specific identification, education [18] and prevention programs need to be strengthened to reduce the incidence of the most undesirable implications of sexualized drug use (USD) among GBMSM [10].
The literature indicates the importance of self-monitoring for the reduction of harm from chemsex use [19] as well as the development of different programs that allow through computer applications [18] applications (app) [20,21] to support and inform participants, reduce the negative impacts associated with chemsex and encourage more reasoned participation. On the other hand, the lack of knowledge of professionals in our country [22] regarding a growing problem should be considered.
Thus, studies such as Nagington's in 2022, indicate that we suggest that medicalized forms of chemsex support could benefit from more rigorous and rapid forms of assessment for problematic chemsex, and provide infrastructure and training for peer support initiatives. We also suggest that medical services can learn from patients and their peers about support needs that professional services continue to miss and engage in collaborative approaches to practice development [23]. Early detection and knowledge of risk factors can contribute to the reinforcement of accessible, non-judgmental, and well-informed prevention and harm reduction activities to support MSM who engage in slamsex [24]. In addition, an equity-oriented approach should be adopted to facilitate unbiased care opportunities [25].
However, to date, the risk factors for chemsex have not been specifically addressed, nor is there currently any instrument available to assess them. All of the above can slow down the detection of these warning signs by the health professionals who work with them, who care for them and understand that the quality of life of these people is fundamental. Therefore, to improve their care and holistic well-being, it is necessary to know the predictive behaviors. To address and respond to the needs, the objective of this study was to design a questionnaire to detect risk factors for chemsex.
2. Materials and Methods
2.1. Desing
The study carried out was of the instrumental type, which, according to Montero and León (2005), is research that develops tests and devices, comprising both the design or adaptation and the study of their psychometric properties. The scale is literally translated from Spanish into English and will therefore be subject to validation in Spanish.
2.2. Item Bank Construction
The questionnaire was developed between July and August 2022. A literature search was conducted, and reference studies related to the research topic were analyzed, verifying the absence of instruments available for the study. The initial version of the questionnaire entitled "Chem-Sex Inventory" (CSI) was organized into six sections consisting of 114 items from various validated scales. The first block related to anxiety to 7 items (from 1-7) (GAD 7) [26]; the second block related to depression (PHQ-9) [27]; consisting of 9 items (from 8-16 items), the third block related to the risk of psycho (PQ-B) [28]; Scale of Corrigan [29]; and CAPE-15 scale [30]; consisting of 21 items (from 17-37), 14 ítems (from 88-99) and 15 ítems (from 100-114) respectively, the fourth block related to impulsivity (BIS-11) [31]; consisting of 30 items (from 38-67), the fifth block related to body perception (PHQ-15) [32]; consisting of 15 items (from 68-82) and finally the sixth block related to suicide risk and consisting of 5 items (from 83-87) (Paykel Scale) [33]. From the Corrigan Scale, the group of researchers initially eliminated two items associated with hospital admission.
Each member of the research committee, including all the authors of the study, collaborated in the development of the questionnaire, defining its structure and main characteristics, selecting the items and reviewing them.
2.3. Selection of Experts
Fifty experts on the subject were contacted, understanding as experts those professionals who had more than 5 years of experience in their field and professional trajectory and at least two years of experience in the management of users who practice Chemsex, had knowledge of the Chemsex phenomenon, were active specialists in their field and had a direct relationship with users who practice Chemsex. The 50 experts were made up of: 10 LGTBI+ individuals, 10 mental health professionals, 10 emergency and urgent care professionals, 10 primary care professionals and 10 professionals from infectious disease and/or sexually transmitted infection (STI) units.
The experts were invited to participate in the study directly by e-mail. Together with the e-mail, an information sheet was sent describing the objectives of the research, as well as the selection criteria, the confidentiality of the data and the voluntary nature of the study. The participation of this group of experts was carried out voluntarily, anonymously, and confidentially by means of a questionnaire through the Microsoft Forms platform. Before disseminating the first survey, the experts identified were asked to accept the Declaration of Consent if they were interested in participating in the study according to the Data Protection Law in force in Spain.
2.4. Delphi Method
The conventional Delphi method was used, through an iterative process in which experts are consulted in two rounds [34].; Linstone and Turoff (1975) consider that two rounds are sufficient to reach a consensus, which would allow adequate reflection on the group's responses [35].
This process was developed during the months of September and October through different phases. Each of the experts was asked to evaluate both the relevance and comprehensibility of each of the items using a Likert-type scale between 1 (strongly disagree) and 5 (strongly agree). A qualitative question on the relevance and clarity of the sections was also added. In addition to criteria of completeness, wording and structuring of each item. Secondly, the responses of the group of experts were received. Subsequently, the discussion group was held, where suggestions were taken into account. Finally, the experts' responses were collected, integrating the pertinent modifications, and the final version of the questionnaire was defined.
2.4.1. Round 1. Content Validity / Linguistic Validity and Loss of Experts are Evaluated.
The first round of consultation was used to evaluate both the content validity (appropriateness) and linguistic validity (comprehensibility) of each of the items. After this first round, the number of items to be evaluated in the second round was significantly reduced.
2.4.2. Round 2. Content Validity Assessed.
In the second round, the content validity of the items was evaluated (although in some cases there were still some items with adequate content validity but low scores in comprehensibility that were re-evaluated for comprehensibility).
2.5. Content Validity Analysis
The content validity of the questionnaire was analyzed by calculating the content validity index and Aiken's V value for each of the items. A minimum CVI and Aiken's V value of 0.6 was established to include the items in the questionnaire, this being the criterion used to select the items. Based on the experts' scores, the indicators were calculated. Following the methodology described by Polit and Beck [36]; and used by other authors [37,38,39]; the content validity index of each of the items (IVC and Aiken's V) was calculated individually, based on the ratings made by the group of experts, using the following equation:
CVI = number of experts who evaluated the item with 3 or 4 / Total of experts
The equation, algebraically modified by Penfield and Giacobbi (2004), is:
V=X−l k
X is the mean of the expert ratings in the sample, l is the lowest possible rating, and k is the range of possible values of the Likert scale used. For example, if l = 1 and k = 5, then k = 5 - 1= 4. The estimation of the confidence intervals for Aiken's V coefficient will use the score method [40].
The CVI and Aiken V indices were calculated with a database created in Excel 2013, using the assessments of the Expert Group and according to their respective formula.
2.6. Comprehensibility Analysis / Linguistic Validation
To obtain the validity of comprehension. The experts were asked to evaluate the degree of understanding of each of the items in the first round and whether they considered that any of the items in the questionnaire should be reformulated. It calculated the average score of such items. Items with scores above 4 were considered to be of high comprehensibility; those with scores between 3.5 and 4 were considered to be of medium comprehensibility; and those with scores below 3.5 were considered to be of low comprehensibility. The items that obtained lower scores in the first round and were selected for the second round because of their content validity were reformulated and their comprehensibility was re-evaluated in the second round.
3. Results
3.1. Characteristics of Experts
Of the 50 experts initially considered, 72% (36 experts) agreed to participate and completed the first round. The second and final round was completed by 30 experts (60%), 70% of whom were men and 30% women (Table 1). Other noteworthy characteristics of the group of experts are: eight mental health professionals, five emergency professionals, six primary care professionals, seven infectious disease professionals and four LGTBI+ professionals. They came from seven autonomous communities: Aragón (n=1); Extremadura (n=2); Canary Oslands (n=2); Catalonia (n=5); Valencian Community (n=1); La Rioja (n=3); Madrid (n=16). In relation to profession, 56.66% (n=17) were nurses, 33.33% (n=10) were physicians, 6.66 (n=2) were psychologists, and 3.33% (n=1) were social workers and sexologists.
3.2. Results of the Delphi Method
Figure 1 shows the questionnaire development process and the content validity index (I-CVI) of each of the 114 items from the Delphi rounds. Of these 114 items, 56 (49.1%) had an I-CVI >0.6 after the first round and 58 items that had an I-CVI <0.6 were eliminated. After the second round, 52 items (92.8%) were above the cutoff value, eliminating the remaining 4 items.
3.3. Content Validity Analysis
The criterion used to select the items that made up the final questionnaire was that the CVI value or the Aiken V test score was greater than 0.6.
The first round was completed by 36 experts. After review of the first round, those items that had obtained a minimum CVI and VdA value of 0.6 were selected. Of the 114 items that made up the questionnaire (Annex 1), 61 items met the criteria of permanence and relevance. Of these 61 items, we proceeded to the analysis of the experts' observations for reformulation and understanding of items 43, 44, 63, 65, 65, 73, 91, 92 and 97. The rest of the experts' suggestions were not taken into account because they were related to items that did not obtain a value higher than 0.6 and were therefore eliminated from the questionnaire. In addition, the group of experts considered that questions 11 and 81, 16 and 84, 10 and 82, 65 and 67, 9 and 83 (which, in principle, all met the criteria for permanence) were similar, so 5 of these 10 questions were eliminated, leaving 56 items finally selected after the first round.
The second round was completed by 30 experts out of the 36 who initially completed the first round. After review of the second round, the same criteria as in the first round were maintained, selecting those items that had obtained a minimum CVI and VdA value of 0.6. Of the 56 items in the questionnaire, the items that did not obtain a minimum CVI and VdA value of 0.6 were eliminated, leaving 54 items that met the criteria. According to the experts' observations, questions 11 "Have you had difficulty concentrating when doing everyday things, such as reading the newspaper or watching television?" and 26 "Are you a person who has difficulty concentrating?" were similar, so item 26 was eliminated because the question was less complete. Subsequently, after review by the research group, two similar items were observed, item 55 "Have you ever heard voices when you were alone?" and item 56 "Have you ever heard voices talking to each other when you were alone?" and the second item was removed. Finally, a questionnaire with 52 items was obtained.
When analyzing the content validity of the 52 items through the CVI and Aiken's V, the researchers eliminated 10 items for not being relevant to the topic even though they had values above 0.6. The values of CVI and Aiken's V for each of the items that make up the questionnaire are shown in Table A1 (Appendix A). Analyzing the CVI and Aiken's V for each item, we see that 97.6% of them reached the value of 0.6 considered acceptable. Only the following two items: "Have you ever seen things that other people cannot see?" and "Have you ever felt as if you were under the control of any external force or power?" scored below 0.6 in one of the two indicators but the other indicator was above 0.6. Finally, the questionnaire consisted of 42 items (Table 2).
3.4. Comprehensibility or Linguistic Validation Analysis
The reports on the items were minimal, some spelling and grammatical changes and syntax structure, for example, item 13 requested to reformulate the question "has felt bad about himself, that he has failed or has failed". The rest of the items were eliminated and were not reformulated. Items 2, 15, 40, 84, 93 and 95 were eliminated from the questionnaire because they presented a low level of comprehension with a value lower than 4. Item 13 was modified because it had values lower than 4 in comprehension; however, after its reformulation, it was considered important to keep it in the instrument.
All the active experts who participated responded that they understood, without difficulty, the content of the final questionnaire designed, the concepts and the answers to each of the items in terms of adequacy and comprehension. Finally, no expert detailed any doubts regarding the completion of the questionnaire.
4. Discussion
Given the importance regarding the increase in the prevalence and public health problem of Chemsex consumption, we proposed at the beginning of the work the design and validation of a scale entitled "Chem-Sex Inventory" (CSI) to reach a consensus on the content in the development of a questionnaire [42,43], based on the Delphi method and analyzing the content validity of the questionnaire to be able to know the behaviors that predict consumption, allowing a better approach to people who practice chemsex and an advance in research on this type of addictions [44].
As a strength of the study, this instrument will facilitate the development of future studies with the aim of analyzing and relating its construct to different variables such as substance use, impulsivity, altered body perception, risk of psychosis, risk of suicide, anxiety and depression. Its application will allow multidisciplinary teams of professionals to plan and develop a better approach to chemsex patients, as well as to know their behavior and conduct. In order to improve personal outcomes related to quality of life.
It used the Delphi method by being a relevant and useful method in the health area [45], characterized to get a reasoned opinion, consensual and individualized in relation to the analysis and reflection on a given research objective [46,47].
First, professionals who had practice-based knowledge and experience in the context of Chemsex and therefore could make valid contributions to the study were chosen as experts. Validation aims to ensure that the questionnaire documents what it is intended to measure and that its design and validation are of rigorous scientific quality. Such validation was carried out with experts to achieve an optimal level of validity, defined as the degree to which all representative indicators intended to be assessed are included in the questionnaire [44].
Furthermore, the group of experts consisted of a heterogeneous group and belonged to different regions and work services, which is fundamental because it allowed a different view from different points of view. Different studies indicate the strengths of using the modified Delphi technique as each round is conducted anonymously and independently, with the advantage of opportunity for participation in the study and reducing response bias that can appear in group settings [41]. Thus, all expert group participants had equal opportunity to participate in the study reducing the risk of response bias that can arise in group settings [41,48].
Secondly, the methodology used was the delphi technique, a consensus technique that allows quantitative estimators to be obtained through the degree of agreement among the participants. This is an effective method for building and creating consensus in a group without the group of experts having to meet in person [43], but rather contacting each of the group members via e-mail. With all of the above, it is necessary to have validated tools adapted to our environment that allow us to know the behavior and conduct of people who practice Chemsex.
Regarding the characteristics of the present study, we can assure that the content validity is high. As we have seen, the decision-making of the group of experts has become increasingly uniform in the different Delphi stages, which is reflected in the significant increase in the congruence index of the items included [44]. The group of experts considered that the 42 items of the “Chem-Sex Inventory” (CSI) questionnaire, having a high level of content validity, capture aspects related to the predictive behavior of Chemsex, and therefore present a high level of content validity [41]. Being a first version of the questionnaire, the research group eliminated second-round items with a CVI and Aiken's V higher than 0.6 as they were not relevant to assess the risk behaviors of Chemsex phenomenon, and kept items with a CVI and Aiken's V lower than 0.6 that were considered relevant to the study.
By means of the Delphi methodology, a high degree of agreement of the group of experts in the elaboration of the questionnaire was observed [44]. In the absence of content validation previously on the Chemsex phenomenon in the literature reviewed as in other situations (UPP, emergency department, etc.) and in the absence of tools to predict risk the development of new tools is necessary [49]. This study can be used in the future to inform other researchers in their own efforts to validate the content of behaviors predictive of the Chemsex phenomenon [43]. Following this it is planned to conduct a study of the LGTBI+ population that performs Chemsex in order to be able, after the resulting analysis, to assess additional aspects of its validity and reliability, and, based on the results, to perform item reduction, and subsequently establish a cut-off point to discriminate risk and allow for group stratification.
In this sense, the panel of experts made a quantitative and qualitative contribution that allowed improving the tool [50], obtaining very positive values in all dimensions and their assessment category, namely, the relevance of the reference question and its response category: Relevance to the object of research, clarity, adequacy and comprehension of the wording, structure and sequence of dimensions and questions. After content validation by experts, a final questionnaire was developed, which is in the process of validation of other psychometric properties.
For future studies, some limitations should be kept in mind; first, a diverse sample of experts working in different systems and in different autonomous communities was selected to obtain a broader perspective on the chemsex phenomenon. Although previous research identified snowball sampling as an effective method for identifying expert groups in Delphi studies [51], it was found that the application of this sampling method in the present study may have resulted in the inclusion of some non-experts in the sample.
This may indicate that those with less experience may have limited exposure to some aspects of chemsex practice. As this was a study based on expert opinion, and although the team of experts was sufficiently broad and knowledgeable about the phenomenon, there is always the possibility that not all aspects or dimensions of the phenomenon were addressed. Another of the limitations encountered is that the resulting questionnaire is relatively long in our opinion, which may lead to abandonment in the responses of users in future research. Since this is a first version of the "Chem-Sex Inventory" (CSI) questionnaire, it is the aim of the research team to shorten the questionnaire in successive versions while maintaining its properties. Por todo lo anterior, investigaciones futuras que utilicen muestras de expertos deben considerar hasta qué punto las experiencias de los participantes se ajustan a los objetivos de la investigación.
5. Conclusions
In conclusion, the results of the present study allow us to conclude that the questionnaire designed to determine the risk factors for the Chemsex phenomenon has a high level of content validity and can therefore be used in the different emergency departments, primary care, psychiatry and infectious disease departments for this purpose.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Table A1 can be downloaded at S1.
Author Contributions
Conceptualization, PDPH ; methodology, AMS and ECS; software, VGC.; validation, PJSD ; formal analysis, ECS ; investigation, CSO.; resources, CITG, JP ; data curation, MSB.; writing—original draft preparation, PDPH. RJV ; writing—review and editing, PDPH, AMS.; visualization, ; supervision, EBG RJV .; project administration, JP, ISA funding acquisition, ISA. All authors have read and agreed to the published version of the manuscript.”
Funding
The research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of the university of La Rioja
Informed Consent Statement
Informed Consent was not necessary.
Data Availability Statement
The data that support the finding of this study are available from the corresponding authors upon first author request.
Acknowledgments
We would like to thank all the members of the group of experts who have contributed to be part of it.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A

Table A1.
Index of content validity and comprehension of each item in the Delphi procedure in the first round.
Table A1.
Index of content validity and comprehension of each item in the Delphi procedure in the first round.
| Items | Relevant to the topic | Understanding for the topic | |
|---|---|---|---|
| CVI | Aiken´s V | Average Score | |
| 1. Have you ever felt nervous, anxious or very upset? | 0,946 | 0,903 | 4,39 |
| 2. Have you not been able to stop worrying? | 0,676 | 0,736 | 3,39 |
| 3. Have you worried too much about different things? | 0,622 | 0,681 | 3,56 |
| 4. Have you had difficulty relaxing? | 0,919 | 0,840 | 4,64 |
| 5. Have you ever felt so restless that you could not sit still? | 0,568 | 0,667 | 3,50 |
| 6. Have you been easily annoyed or irritated? | 0,919 | 0,903 | 4,61 |
| 7. Have you been afraid as if something terrible was going to happen? | 0,811 | 0,792 | 4,22 |
| 8. Have you had little interest or pleasure in doing things? | 0,838 | 0,847 | 4,39 |
| 9. Have you ever felt discouraged, depressed or hopeless? | 0,865 | 0,861 | 4,53 |
| 10. Have you had difficulty falling asleep, staying asleep, or sleeping too much? | 0,865 | 0,903 | 4,47 |
| 11. Have you ever felt tired or low on energy? | 0,865 | 0,840 | 4,47 |
| 12. Have you ever felt lacking in appetite or, on the contrary, have you eaten too much? | 0,703 | 0,757 | 4,19 |
| 13. Have you ever felt bad about yourself or that you are a failure or failing yourself? | 0,865 | 0,826 | 3,44 |
| 14. Have you had difficulty concentrating on doing things, such as reading the newspaper or watching television? | 0,784 | 0,799 | 4,17 |
| 15. Have you ever moved or talked so slowly that other people around you have noticed or, conversely, when you are nervous or restless do you move more than usual? | 0,595 | 0,681 | 3,39 |
| 16. Have you ever had thoughts that you might be better off dead or hurting yourself? | 0,919 | 0,889 | 4,28 |
| 17. Do familiar environments sometimes seem strange, confusing, threatening or unreal to you? | 0,784 | 0,792 | 4,25 |
| 18. Have you ever heard unusual sounds such as popping, popping, hissing, clapping, or ringing in your ears? | 0,676 | 0,729 | 4,06 |
| 19. Do the things you see seem different from the way they normally are (brighter or duller, bigger or smaller, or changed in some other way? | 0,649 | 0,701 | 4,00 |
| 20. Have you had any experiences of telepathy, seer or fortune teller powers? | 0,405 | 0,597 | 3,64 |
| 21. Have you ever felt as if you were not in control of your own thoughts or ideas? | 0,838 | 0,826 | 4,33 |
| 22. Have you had difficulty following your own topic because you ramble or lose track when you speak? | 0,892 | 0,819 | 3,78 |
| 23. Have you ever had a strong feeling or belief that you possess any kind of unusual gifts or talents, for example telepathy? | 0,514 | 0,604 | 3,81 |
| 24. Have you ever had the feeling that other people are watching you or talking about you? | 0,892 | 0,875 | 4,67 |
| 25. Have you ever noticed any sensation on or under the skin, such as bugs? | 0,757 | 0,806 | 4,19 |
| 26. have you ever felt suddenly distracted by distant sounds that you were not normally aware of? | 0,568 | 0,701 | 3,89 |
| 27. Have you ever had the feeling that there was a person or force around you, even though you could not see anyone? | 0,676 | 0,694 | 4,06 |
| 28. Have you ever worried that something might go wrong in your mind? | 0,865 | 0,861 | 4,28 |
| 29. Have you ever felt that you did not exist, that the world did not exist or that you were dead? | 0,568 | 0,653 | 3,83 |
| 30. Have you ever felt confused about whether something that happened to you was real or imaginary? | 0,811 | 0,806 | 4,31 |
| 31. Have you ever held beliefs that other people would find difficult to believe? | 0,649 | 0,708 | 3,75 |
| 32. Have you felt that parts of your body have changed in any way, or that parts of your body were functioning in a different way? | 0,622 | 0,715 | 3,92 |
| 33. Have you felt that your thoughts are sometimes so intense that you can almost hear them? | 0,676 | 0,722 | 4,14 |
| 34. Have you ever had feelings of distrust towards other people? | 0,811 | 0,840 | 4,47 |
| 35. Have you ever seen unusual things such as flashes, flames, glaring lights, or geometric shapes? | 0,757 | 0,736 | 4,17 |
| 36. Have you ever seen things that other people cannot see? | 0,757 | 0,764 | 4,08 |
| 37. Do people sometimes have a hard time understanding what you were saying? | 0,757 | 0,771 | 4,08 |
| 38. Have you planned your tasks carefully? | 0,459 | 0,590 | 3,69 |
| 39. Have you ever done things without thinking about them? | 0,595 | 0,694 | 4,17 |
| 40. Have you hardly ever taken things to heart or are you not easily disturbed? | 0,378 | 0,549 | 2,50 |
| 41. Have you ever had thoughts that your mind is going faster than normal? | 0,811 | 0,819 | 4,14 |
| 42. Do you consider yourself a person who plans your trips in advance? | 0,270 | 0,438 | 4,08 |
| 43. Do you consider yourself a person with self-control? | 0,811 | 0,785 | 4,25 |
| 44. Are you a person who is able to concentrate easily? | 0,730 | 0,715 | 4,39 |
| 45. Are you a person who saves regularly? | 0,514 | 0,604 | 4,42 |
| 46. Do you find it difficult to sit still for long periods of time? | 0,784 | 0,764 | 4,39 |
| 47. Do you think things through carefully? | 0,568 | 0,653 | 4,08 |
| 48. Do you plan to have a steady job or do you strive to ensure that you will have money to pay your expenses? | 0,514 | 0,625 | 3,86 |
| 49. Do you ever say things without thinking them through? | 0,595 | 0,681 | 4,19 |
| 50. Do you like to think about complicated problems? | 0,459 | 0,576 | 3,94 |
| 51. Do you change jobs frequently? | 0,514 | 0,660 | 4,28 |
| 52. Do you act impulsively? | 0,865 | 0,840 | 4,28 |
| 53. Do you get bored easily trying to solve problems in your mind? | 0,514 | 0,653 | 3,94 |
| 54. Do you visit the doctor and dentist frequently? | 0,514 | 0,632 | 4,00 |
| 55. Do you do things as they occur to you? | 0,595 | 0,681 | 4,06 |
| 56. Do you consider yourself a person who thinks without being distracted, that is, can you focus your mind on one thing for a long time? | 0,622 | 0,694 | 4,08 |
| 57. Do you change housing frequently, i.e., do you move frequently or do you dislike living in the same place for a long time? | 0,378 | 0,542 | 4,00 |
| 58. Do you buy things on impulse? | 0,595 | 0,694 | 4,25 |
| 59. Do you complete all the activities you start? | 0,622 | 0,688 | 4,33 |
| 60. Do you walk and move quickly? | 0,324 | 0,576 | 4,11 |
| 61. Do you solve problems by experimenting, i.e., do you solve problems by trying a possible solution and seeing if it works? | 0,541 | 0,667 | 3,83 |
| 62. Do you spend more in cash or credit than you earn? | 0,622 | 0,715 | 3,92 |
| 63. Have you noticed that you talk faster than usual? | 0,649 | 0,708 | 3,81 |
| 64. Have you ever had strange thoughts when you were thinking? | 0,676 | 0,736 | 3,61 |
| 65. Are you more interested in the present than in the future? | 0,622 | 0,688 | 4,33 |
| 66. Do you feel restless in classes or lectures if you have to listen to someone talk for a long period of time? | 0,595 | 0,667 | 4,17 |
| 67. Do you plan for the future, i.e., are you more interested in the future than in the present? | 0,595 | 0,632 | 4,00 |
| 68. Have you ever had stomach pain? | 0,459 | 0,576 | 4,50 |
| 69. Have you ever had back pain? | 0,351 | 0,528 | 4,44 |
| 70. Have you ever had pain in your arms, legs or joints (knees, hips)? | 0,432 | 0,563 | 4,28 |
| 71. Have you had menstrual cramps or other problems with your periods? | 0,297 | 0,458 | 3,97 |
| 72. Have you ever had headaches? | 0,541 | 0,646 | 4,58 |
| 73. Have you ever had chest pains? | 0,676 | 0,688 | 4,47 |
| 74. Have you ever had dizziness? | 0,703 | 0,701 | 4,39 |
| 75. Have you had any episodes of fainting? | 0,649 | 0,694 | 4,39 |
| 76. Have you ever felt that your heart was beating faster and faster? | 0,811 | 0,806 | 4,44 |
| 77. Have you ever felt short of breath? | 0,865 | 0,799 | 4,44 |
| 78. At any time have you experienced pain or problems during sexual penetration? | 0,649 | 0,708 | 4,28 |
| 79. Have you had episodes of constipation or diarrhea? | 0,514 | 0,632 | 4,47 |
| 80. Have you ever had nausea? | 0,622 | 0,681 | 4,50 |
| 81. Have you ever felt tired or low on energy? | 0,865 | 0,847 | 4,58 |
| 82. Have you had difficulty sleeping? | 0,946 | 0,903 | 4,75 |
| 83. Have you ever felt that life was not worth living? | 0,919 | 0,875 | 4,67 |
| 84. Have you ever wished you were dead or could sleep and wake up? | 0,784 | 0,771 | 3,08 |
| 85. Have you ever really had the idea of committing suicide? | 0,865 | 0,861 | 4,22 |
| 86. Have you thought about how you would do it? | 0,811 | 0,806 | 4,36 |
| 87. Have you ever tried to take your own life? | 0,811 | 0,847 | 4,61 |
| 88. Have you ever felt that you have difficulty maintaining your attention, are easily distracted, unable to concentrate? | 0,838 | 0,833 | 4,42 |
| 89. Have you ever felt that you are Impulsive, impatient, poorly tolerate pain or frustration? | 0,757 | 0,785 | 3,78 |
| 90. Do you ever feel uncooperative, uncaring, and demanding of yourself? | 0,541 | 0,694 | 3,69 |
| 91. Do you consider that you are violent or threatening to people? | 0,649 | 0,750 | 4,28 |
| 92. Do you consider yourself an explosive person or a person with anger attacks that are difficult to predict? | 0,757 | 0,785 | 4,39 |
| 93. Do you consider yourself a restless person, rubbing, moaning or other self-stimulating behavior? | 0,432 | 0,611 | 2,86 |
| 94. Do you consider yourself a restless person, come and go, and move around excessively? | 0,649 | 0,729 | 3,72 |
| 95. Do you consider yourself a person who exhibits repetitive, motor or verbal behaviors? | 0,541 | 0,688 | 3,44 |
| 96. Do you consider yourself a fast or excessive talker? | 0,595 | 0,722 | 4,17 |
| 97. Do you consider yourself a person who changes mood frequently? | 0,892 | 0,840 | 4,50 |
| 98. Do you consider yourself a person who cries or laughs easily and excessively? | 0,757 | 0,750 | 4,08 |
| 99. Do you consider yourself a person who insults or hurts others? | 0,541 | 0,667 | 3,69 |
| 100. Have you ever felt as if people were dropping hints or making double entendres? | 0,757 | 0,757 | 4,00 |
| 101. Have you ever felt as if some people are not what they appear to be? | 0,649 | 0,708 | 3,83 |
| 102. Have you ever felt that you are being persecuted in any way? | 0,730 | 0,771 | 4,25 |
| 103. Have you ever felt as if there was a conspiracy against you? | 0,703 | 0,764 | 4,19 |
| 104. Have you ever felt that people look at you strangely because of your appearance? | 0,811 | 0,771 | 4,33 |
| 105. Have you felt that certain electronic devices, such as computers, phones or tablets, can influence your thinking? | 0,676 | 0,715 | 4,19 |
| 106. Have you felt as if your thoughts were being pulled out of your head? | 0,676 | 0,708 | 3,94 |
| 107. Have you ever felt as if your thoughts were not your own? | 0,811 | 0,771 | 4,36 |
| 108. Have you ever had thoughts that were so intense that you were worried that others might hear them? | 0,595 | 0,688 | 4,22 |
| 109. Have you ever felt as if your thoughts were constantly repeating in your mind? | 0,811 | 0,778 | 4,39 |
| 110. Have you ever felt as if you were under the control of any external force or power? | 0,649 | 0,694 | 4,11 |
| 111. Have you ever felt as if a look-alike had impersonated a family member, friend or acquaintance? | 0,459 | 0,597 | 3,94 |
| 112. Have you ever heard voices when you were alone? | 0,784 | 0,778 | 4,42 |
| 113. Have you ever heard voices talking to each other when you were alone? | 0,703 | 0,722 | 3,89 |
| 114. Have you ever seen objects, people or animals that other people could not see? | 0,622 | 0,688 | 4,17 |
References
- Curto, J.; Dolengevich, H.; Soriano, R.; Belza, M.J. Documento técnico: abordaje de la salud mental del usuario con prácticas de Chemsex. MSD 2020. Available online: https://www.sanidad.gob.es/ciudadanos/enfLesiones/enfTransmisibles/sida/chemSex/docs/Abordaje_salud_mental_chemsex.pdf (accessed on 9 January 2023).
- Wang, H.; d'Abreu de Paulo, K.J.; Gültzow, T.; Zimmermann, H.M.; Jonas, K.J. Perceived Monkeypox Concern and Risk among Men Who Have Sex with Men: Evidence and Perspectives from The Netherlands. Trop Med Infect Dis. 2022, 10, 293. [Google Scholar] [CrossRef] [PubMed]
- Bolmont, M.; Tshikung, O.N.; Trellu, L.T. Chemsex, a Contemporary Challenge for Public Health. J Sex Med. 2022, 19, 1210–1213. [Google Scholar] [CrossRef]
- Maviglia, F.; Wickersham, J.A.; Azwa, I.; Copenhaver, N.; Kennedy, O.; Kern, M.; Khati, A.; Lim, S.H.; Gautam, K.; Shrestha, R. Engagement in Chemsex among Men Who Have Sex with Men (MSM) in Malaysia: Prevalence and Associated Factors from an Online National Survey. Int J Environ Res Public Health. 2022, 24, 294. [Google Scholar] [CrossRef] [PubMed]
- Guerras, J.M.; Hoyos, J.; Donat, M.; de la Fuente, L.; Palma Díaz, D.; Ayerdi, O.; García-Pérez, J.N.; García de Olalla, P.; Belza, M.J. Sexualized drug use among men who have sex with men in Madrid and Barcelona: The gateway to new drug use? Front Public Health. 2022, 15. [Google Scholar] [CrossRef]
- Chan, A.S.; Tang, P.M.; Yan, E. Chemsex and its risk factors associated with human immunodeficiency virus among men who have sex with men in Hong Kong. World J Virol. 2022, 25, 208–211. [Google Scholar] [CrossRef] [PubMed]
- Madrid Salud. Plan de Adicciones de la Ciudad de Madrid. 2021/2022. 2022. Available online: https://madridsalud.es/pdf/PLAN%20DE%20ADICCIONES%2022-26.pdf (accessed on 12 January 2023).
- Marqués-Sánchez, P.; Bermejo-Martínez, D.; Quiroga Sánchez, E.; Calvo-Ayuso, N.; Liébana-Presa, C.; Benítez-Andrades, J.A. Men who have sex with men: An approach to social network analysis. Public Health Nurs. 2023, 40, 73–79. [Google Scholar] [CrossRef]
- Amundsen, E.; Haugstvedt, Å.; Skogen, V.; Berg, R.C. Health characteristics associated with chemsex among men who have sex with men: Results from a cross-sectional clinic survey in Norway. PLoS One. 2022, 5. [Google Scholar] [CrossRef]
- Íncera-Fernández, D.; Román, F.J.; Moreno-Guillén, S.; Gámez-Guadix, M. Understanding Sexualized Drug Use: Substances, Reasons, Consequences, and Self-Perceptions among Men Who Have Sex with Other Men in Spain. Int. J. Environ. Res. Public Health 2023, 20, 2751. [Google Scholar] [CrossRef]
- González-Baeza, A.; Barrio-Fernández, P.; Curto-Ramos, J.; Ibarguchi, L.; Dolengevich-Segal, H.; Cano-Smith, J.; Rúa-Cebrián, G.; García-Carrillo de Albornoz, A.; Kessel, D. Understanding Attachment, Emotional Regulation, and Childhood Adversity and Their Link to Chemsex. Subst Use Misuse. 2023, 58, 94–102. [Google Scholar] [CrossRef]
- Strasser, M.; Halms, T.; Rüther, T.; Hasan, A.; Gertzen, M. Lethal Lust: Suicidal Behavior and Chemsex—A Narrative Review of the Literature. Brain Sci. 2023, 13, 174. [Google Scholar] [CrossRef]
- Huang, M. H.; Chen, G.J.; Sun, H.Y.; Chen, Y.T.; Su, L.H.; Ho, S.Y.; Chang, S.Y.; Huang, S.H.; Huang, Y.C.; Liu, W. D.; et al. Risky sexual practices and hepatitis C viremia among HIV-positive men who have sex with men in Taiwan. J microbiol Immunol Infectn. 2023, 56, 566–574. [Google Scholar] [CrossRef] [PubMed]
- Siddiq, M.; O'Flanagan, H.; Richardson, D.; Llewellyn, C.D. Factors associated with sexually transmitted shigella in men who have sex with men: a systematic review. Sex Transm Infect. 2023, 99, 58–63. [Google Scholar] [CrossRef] [PubMed]
- Devos, S.; Bonnet, F.; Hessamfar, M.; Neau, D.; Vareil, M.O.; Leleux, O.; Cazanave, C.; Rouanes, N.; Duffau, P.; Lazaro, E.; et al. Tobacco, alcohol, cannabis, and illicit drug use and their association with CD4/CD8 cell count ratio in people with controlled HIV: a cross-sectional study (ANRS CO3 AQUIVIH-NA-QuAliV). BMC Infect Dis. 2023, 9, 23. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Gámez, L.; Hernández-Huerta, D.; Lahera, G. Chemsex and Psychosis: A Systematic Review. Behav Sci (Basel). 2022, 15, 516. [Google Scholar] [CrossRef]
- Ugarte, A.; de la Mora, L.; García, D.; Martínez-Rebollar, M.; de-Lazzari, E.; Torres, B.; Inciarte, A.; Ambrosioni, J.; Chivite, I.; Solbes, E.; et al. Evolution of Risk Behaviors, Sexually Transmitted Infections and PrEP Care Continuum in a Hospital-Based PrEP Program in Barcelona, Spain: A Descriptive Study of the First 2 Years’ Experience. Infect Dis Ther 2023, 12, 425–442. [Google Scholar] [CrossRef]
- Choi, E.P.; Choi, K.W.; Wu, C.; Chau, P.H.; Kwok, J.Y.; Wong, W.C.; Chow, E.P. Web-Based Harm Reduction Intervention for Chemsex in Men Who Have Sex With Men: Randomized Controlled Trial. JMIR Public Health Surveill. 2023, 5, 9. [Google Scholar] [CrossRef]
- Platteau, T.; Herrijgers, C.; Kenyon, C.; Florence, E. Self-control for harm reduction in chemsex. Lancet HIV. 2023, 10, 1. [Google Scholar] [CrossRef]
- Herrijgers, C.; Platteau, T.; Vandebosch, H.; Poels, K.; Florence, E. Using Intervention Mapping to Develop an mHealth Intervention to Support Men Who Have Sex With Men Engaging in Chemsex (Budd): Development and Usability Study. JMIR Res Protoc. 2022, 21, 11. [Google Scholar] [CrossRef]
- Barmania, S. HERO-providing support for those engaged in chemsex. Lancet HIV. 2022, 9, 10. [Google Scholar] [CrossRef]
- Galicia, P.; Chuvieco, S.; Santos Larrégola, L.; Cuadros, J.; Ramos-Rincón, J.M.; Linares, M. Awareness of chemsex, pre-exposure prophylaxis, and sexual behavior in primary health care in Spain. Semergen. 2023, 49, 4. [Google Scholar]
- Nagington, M.; King, S. Support, care and peer support for gay and bi men engaging in chemsex. Health Soc Care Community. 2022, 30, 6. [Google Scholar] [CrossRef] [PubMed]
- Knoops, L.; van Amsterdam, J.; Albers, T.; Brunt, T.M.; van den Brink, W. Slamsex in The Netherlands among men who have sex with men (MSM): use patterns, motives, and adverse effects. Sex Health. 2022, 19, 566–573. [Google Scholar] [CrossRef]
- Abrahão, A.B.; Kortas, G.T.; Blaas, I.K.; Koch, G.; Leopoldo, K.; Malbergier, A.; Torales, J.; Ventriglio, A.; Castaldelli-Maia, J.M. The impact of discrimination on substance use disorders among sexual minorities. Int Rev Psychiatry. 2022, 34, 423–431. [Google Scholar] [CrossRef] [PubMed]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Löwe, B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001, 16, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Fonseca-Pedrero, E.; Gooding, D.C.; Ortuño-Sierra, J.; Paino, M. Assessing self-reported clinical high risk symptoms in community-derived adolescents: A psychometric evaluation of the Prodromal Questionnaire-Brief. Compr Psychiatry. 2016, 66, 201–208. [Google Scholar] [CrossRef]
- Garrote-Cámara, M.E.; Santolalla-Arnedo, I.; Ruiz de Viñaspre-Hernández, R.; Gea-Caballero, V.; Sufrate-Sorzano, T.; del Pozo-Herce, P.; Garrido-García, R.; Rubinat-Arnaldo, E.; Juárez Vela, R. Psychometric Characteristics and Sociodemographic Adaptation of the Corrigan Agitated Behavior Scale in Patients With Severe Mental Disorders. Front. Psychol. 2021, 12. [Google Scholar] [CrossRef]
- Capra, C.; Kavanagh, D.J.; Hides, L.; Scott, J.G. Current CAPE-15: a measure of recent psychotic-like experiences and associated distress. Early Interv Psychiatry. 2017, 11, 411–417. [Google Scholar] [CrossRef]
- Salvo, L.; Castro, A. Confiabilidad y validez de la escala de impulsividad de Barratt (BIS-11) en adolescentes. Rev. chil. neuro-psiquiatr. 2013, 51, 245–254. [Google Scholar] [CrossRef]
- Ros Montalbán, S.; Comas Vives, A.; Garcia-Garcia, M. Validation of the Spanish version of the PHQ-15 questionnaire for the evaluation of physical symptoms in patients with depression and/or anxiety disorders: DEPRE-SOMA study. Actas Esp Psiquiatr. 2010, 38, 345–57. [Google Scholar]
- Paykel, E.S.; Myers, J.K.; Lindenthal, J.J.; Tanner, J. Suicidal feelings in the general population: a prevalence study. Br J Psychiatry. 1974, 124, 460–469. [Google Scholar] [CrossRef]
- Hasson, F.; Keeney, S.; McKenna, H. Research guidelines for the Delphi survey technique. J Adv Nurs. 2000, 32, 1008–1015. [Google Scholar] [CrossRef]
- Mahajan, V.; Linstone, H.A.; Turoff, M. The Delphi Method: Techniques and Applications. Journal of Marketing Research. 1976, 13, 317. [Google Scholar] [CrossRef]
- Polit, D.F.; Beck, C.T. The content validity index: are you sure you know what's being reported? Critique and recommendations. Res Nurs Health. 2006, 29, 489–97. [Google Scholar] [CrossRef]
- Orts-Cortés, M.I.; Moreno-Casbas, T.; Squires, A.; Fuentelsaz-Gallego, C.; Maciá-Soler, L.; González-María, E. Content validity of the Spanish version of the Practice Environment Scale of the Nursing Work Index. Appl Nurs Res. 2013, 26, 5–9. [Google Scholar] [CrossRef]
- Squires, A.; Aiken, L.H.; van den Heede, K.; Sermeus, W.; Bruyneel, L.; Lindqvist, R.; Schoonhoven, L.; Stromseng, I.; Busse, R.; Brzostek, T.; et al. A systematic survey instrument translation process for multi-country, comparative health workforce studies. Int J Nurs Stud. 2013, 50, 264–273. [Google Scholar] [CrossRef]
- Chover-Sierra, E.; Martínez-Sabater, A.; Lapeña-Moñux, Y.R. An instrument to measure nurses' knowledge in palliative care: Validation of the Spanish version of Palliative Care Quiz for Nurses. PLoS One. 2017, 12, e0177000. [Google Scholar] [CrossRef]
- Randall, D.; Penfield & Peter, R.; Giacobbi, J.R. Applying a Score Confidence Interval to Aiken's Item Content-Relevance Index. Meas Phys Educ Exerc Sci. 2004, 8, 213–225. [CrossRef]
- Bull, C.; Crilly, J.; Latimer, S.; Gillespie, B.M. Establishing the content validity of a new emergency department patient-reported experience measure (ED PREM): a Delphi study. BMC Emerg Med. 2022, 9, 22. [Google Scholar] [CrossRef]
- McKenna, H.P. The Delphi technique: a worthwhile research approach for nursing? J Adv Nurs. 1994, 19, 1221–1225. [Google Scholar] [CrossRef]
- Varela-Ruiz, M.; Díaz-Bravo, L.; García-Durán, R. Descripción y usos del método Delphi en investigaciones del área de la salud. Investigación educ. médica. 2012, 1, 90–95. [Google Scholar]
- Gil, B.; Pascual-Ezama, D. La metodología Delphi como técnica de estudio de la validez de contenido. Annals of Psychology. 2012, 28, 1011–1020. [Google Scholar] [CrossRef]
- Okoli, C.; Pawlowski, S.D. The Delphi method as a research tool: an example, design considerations and applications. Information & Management. 2004, 42, 15–29. [Google Scholar] [CrossRef]
- Gilson, N.; Brown, W.J.; Faulkner, G.; McKenna, J.; Murphy, M.; Pringle, A.; Proper, K.; Puig-Ribera, A.; Stathi, A. The International Universities Walking Project: development of a framework for workplace intervention using the Delphi technique. J Phys Act Health. 2009, 6, 520–528. [Google Scholar] [CrossRef]
- Landeta, Jon. El método delphi: una técnica de previsión del futuro. Barcelona: Ariel, 2002. Print.
- Nyumba, Tobias.; Wilson, Kerrie.; Derrick, Christina.; Mukherjee, Nibedita. The use of focus group discussion methodology: Insights from two decades of application in conservation. Methods in Ecology and Evolution. 2018, 9, 20–32. [CrossRef]
- Kumar, A.; Rajinder, Mahal. Modified Delphi Technique: Content validity of the Pressure ulcer risk assessment tool. JoNSP. 2017, 7, 17.19.
- Keeney, S.; Hasson, F.; McKenna, H. Consulting the oracle: ten lessons from using the Delphi technique in nursing research. J Adv Nurs. 2006, 53, 205–212. [Google Scholar] [CrossRef]
- Skulmoski, G.; Hartman, F.; Krahn, J. The Delphi method for graduate research. J. Inf. Technol. 2007, 6, 1–21. [Google Scholar] [CrossRef]
Figure 1.
Final summary of the Delphi method. Own elaboration Adapted. [41].
Figure 1.
Final summary of the Delphi method. Own elaboration Adapted. [41].
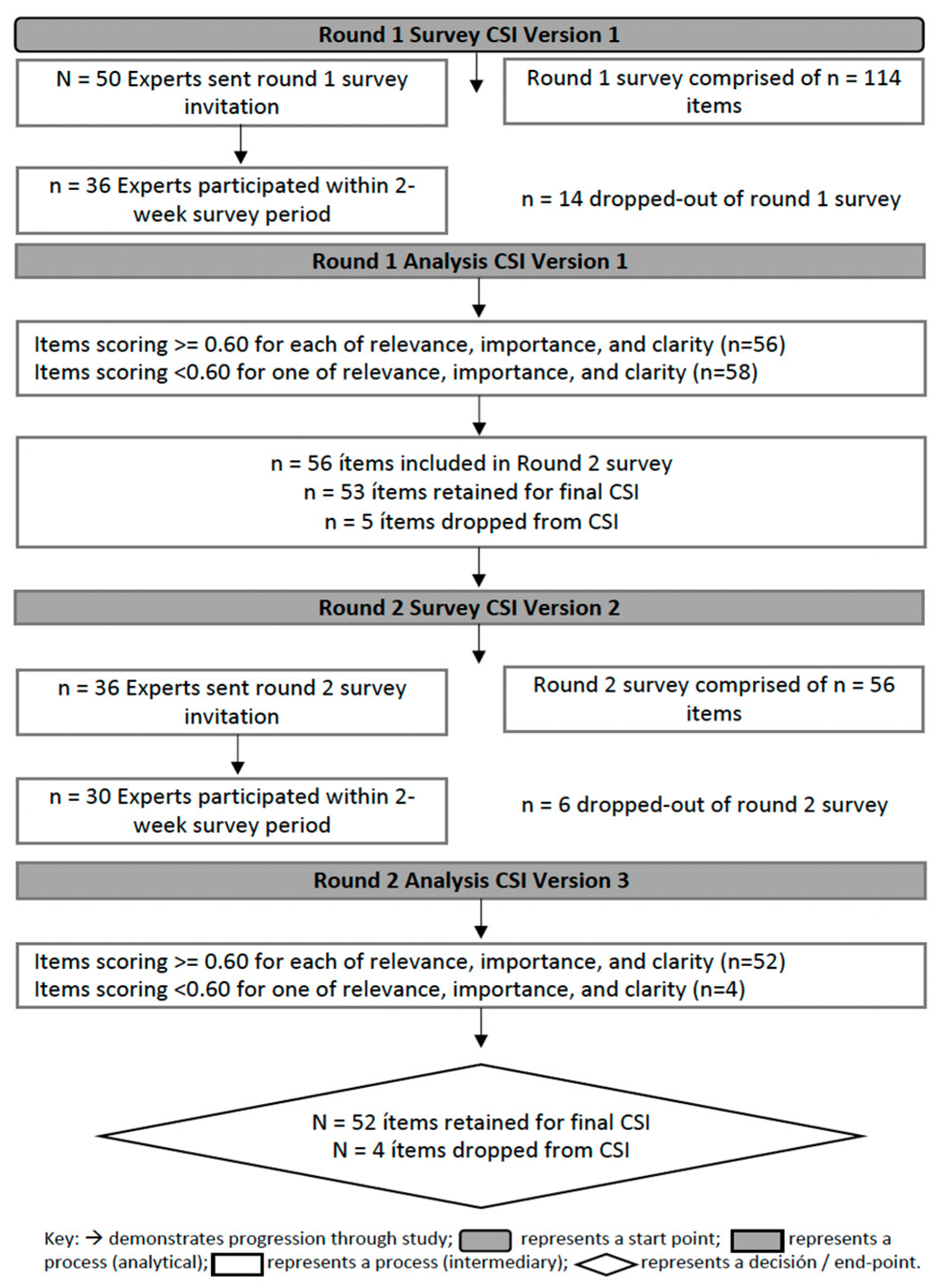
Table 1.
Demographic data of the panel of experts participating in the Delphi method.
| Characteristics | N | % |
|---|---|---|
| Gender | ||
| Male | 21 | (70) |
| Female | 9 | (30) |
| Position | ||
| LGTBI+ Collective | 4 | (13.33) |
| Psychiatry Service | 8 | (26.66) |
| Primary Care | 6 | (20) |
| Urgent Care / Emergency Service | 5 | (16.66) |
| Infectious Diseases Service / STIs Clinic 1 | 7 | (23.33) |
| Autonomous Community | ||
| Aragon | 1 | (3.33) |
| Extremadura | 2 | (6.66) |
| Canary Islands | 2 | (6.66) |
| Catalonia | 5 | (16.66) |
| Valencian Community | 1 | (3.33) |
| La Rioja | 3 | (10) |
| Madrid | 16 | (53.33) |
| Profession | ||
| Psysician | 10 | (33.33) |
| Nurse | 17 | (56.66) |
| Psychologist | 2 | (6.66) |
| Occupational Therapist / Sexologist | 1 | (3.33) |
1 STIs (Sexually Transmitted Infection).
Table 2.
Content validity index and Aiken's V for each of the items.
| Item number first round | Items | CVI | Aiken´s V |
|---|---|---|---|
| 1 | 1. Have you felt nervous, anxious or very upset? | 0,900 | 0,900 |
| 4 | 2. Have you ever had difficulty relaxing? | 0,900 | 0,850 |
| 6 | 3. Have you been easily annoyed or irritated? | 0,933 | 0,875 |
| 7 | 4. Have you been afraid as if something terrible was going to happen? | 0,733 | 0,767 |
| 8 | 5. Have you had little interest or pleasure in doing things? | 0,833 | 0,817 |
| 9 | 6. Have you ever felt discouraged, depressed or hopeless? | 0,867 | 0,867 |
| 11 | 7. Have you ever felt tired or low energy? | 0,733 | 0,783 |
| 12 | 8. Have you had no appetite or, on the contrary, have you eaten too much? | 0,667 | 0,725 |
| 13 | 9. Have you ever felt bad about yourself, felt that you are a failure or that you are failing yourself? | 0,800 | 0,817 |
| 14 | 10. Have you had difficulty concentrating on doing everyday things, such as reading the newspaper or watching television? | 0,867 | 0,800 |
| 16 | 11. Have you ever had thoughts that you would be better off dead or harming yourself? | 0,800 | 0,783 |
| 17 | 12. Do familiar environments sometimes seem strange, confusing, threatening or unreal to you? | 0,767 | 0,733 |
| 21 | 13. Have you ever felt as if you were not in control of your own thoughts or ideas? | 0,833 | 0,750 |
| 22 | 14. Have you ever had difficulty following your own conversation because you ramble or lose concentration too much when you talk? | 0,800 | 0,742 |
| 24 | 15. Have you ever had the feeling that other people are watching you or talking about you? | 0,800 | 0,767 |
| 25 | 16. Have you occasionally noticed any sensation on or under the skin, such as bugs? | 0,600 | 0,658 |
| 28 | 17.Have you ever worried that something might go wrong in your mind? | 0,667 | 0,717 |
| 30 | 18. Have you ever felt confused about whether something that happened to you was real or imaginary? | 0,733 | 0,725 |
| 34 | 19. Have you ever had feelings of distrust towards other people? | 0,800 | 0,758 |
| 35 | 20. Have you ever seen unusual things such as flashes, flames, glaring lights or geometric shapes? | 0,733 | 0,692 |
| 36 | 21. Have you ever seen things that other people cannot see? | 0,567 | 0,608 |
| 37 | 22. Do you have the feeling that people find it difficult to understand what you are saying? | 0,633 | 0,650 |
| 41 | 23. Have you ever had thoughts about your mind going faster than normal? | 0,700 | 0,733 |
| 52 | 26. In the last few days have you felt that you were acting impulsively? | 0,867 | 0,783 |
| 66 | 30. Do you feel restless in classes or lectures if you have to listen to someone talk for a long period of time? | 0,633 | 0,700 |
| 73 | 32. Have you ever had chest pains? | 0,700 | 0,708 |
| 76 | 34. Have you ever felt that your heart was beating faster than usual? | 0,800 | 0,800 |
| 77 | 35. Have you ever felt short of breath? | 0,767 | 0,775 |
| 82 | 36. Have you had difficulty sleeping? | 0,900 | 0,883 |
| 85 | 37. Have you ever really had the idea of committing suicide? | 0,833 | 0,792 |
| 86 | 38. Have you thought about how you would carry it out?. | 0,800 | 0,775 |
| 87 | 39. Have you ever tried to take your own life? | 0,700 | 0,700 |
| 88 | 40. Have you ever felt that you have difficulty maintaining your attention, that you are easily distracted, or that you are unable to concentrate? | 0,667 | 0,683 |
| 92 | 42. Do you consider yourself a person with anger attacks that are difficult to predict? | 0,867 | 0,783 |
| 97 | 43. At any time have you considered yourself to be a person who changes moods frequently? | 0,833 | 0,767 |
| 100 | 45. Have you ever felt as if people were dropping hints or saying things with a double meaning? | 0,667 | 0,675 |
| 104 | 46. Have you ever felt that people look at you strangely because of your appearance? | 0,633 | 0,650 |
| 106 | 47. Have you ever felt as if your thoughts were being pulled out of your head? | 0,600 | 0,617 |
| 107 | 48. Have you ever felt as if your thoughts were not your own? | 0,733 | 0,708 |
| 109 | 49. Have you ever felt as if your thoughts were constantly repeating in your mind? | 0,700 | 0,717 |
| 110 | 50. Have you ever felt as if you were under the control of any external force or power? | 0,600 | 0,592 |
| 112 | 51. Have you ever heard voices when you were alone? | 0,733 | 0,717 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



