
Submitted:
04 August 2023
Posted:
08 August 2023
You are already at the latest version
Abstract
Insufficient physical activity (PA) is associated with low cardiorespiratory fitness, which favors cardiovascular and other non-communicable diseases. Besides, it evidentially affects mental health. Considering the WHO PA guidelines, CrossFit® represents a versatile exercise program, combining aerobic and resistance training with mobility and could help lowering disease incidences among sedentary people. Yet, long-term CrossFit research is sparse. We conducted a nine-months intervention (≥ 2 CrossFit workouts/week) in sixteen beginners (14 males, 35 6.8 years, 180 8.6 cm, 85. 5 19.1 kg). As primary endpoint, VO2max was assessed at baseline, after four, and nine months. A repeated-measures ANOVA and pearson correlation were conducted. Well-being was investigated by WHO-5-index pre- and post-intervention. For exploratory purpose, body composition was tracked. Main outcome was an 11.5 % VO2max improvement with large effect (p < .01, η_p^2 = .27). Strong negative correlations between baseline VO2max and its progression after nine months (p = .006, r = -.654) were found. Well-being increased by 8.7 % (p = .024, d = .51). Body composition improved without statistical significance. Resting metabolic rate increased by 2.2 % (p = .042). This study reveals the potential of CrossFit to enhance physiological and psychological health in beginners. For more robust results, bigger sample sizes with higher proportion of women are needed.
Keywords:
CrossFit
; functional fitness training
; group training
; cardiorespiratory fitness
; VO2max
; well-being
; body composition
; sitting hours
1. Introduction
Despite the well-known adverse effects of sedentary behavior, regular engagement in physical activity (PA) decreases among populations worldwide. Especially in western high-income countries, the number of people lacking regular PA grew from 30.9% in 2001 to 36.8% in 2016 [1]. Half of the employed men and women in Germany reported to be mostly sitting during their daily work in 2018 [2]. The Covid-19 pandemic supposedly worsened the situation, as it required social distancing and changes in daily activities. Recent studies reported negative effects of the pandemic on PA levels, hours spent sitting, and eating habits [3,4].
Health implications of sedentary behavior include increased risk of all-cause mortality, cardiovascular disease (CVD), adiposity, type-2-diabetes, cancer, musculoskeletal disorders, as well as diverse mental and psychological illnesses [5,6,7,8]. CVD must be mentioned in particular, as they account for almost one third of all global deaths. Cardiorespiratory fitness (CRF), commonly measured as VO2max, is an important clinical parameter to assess CVD-risk. Low CRF is associated with reduced survival and higher incidences of CVD and other comorbidities [9]. It can be improved by a variety of endurance but also resistance training [10]. Evidence suggests that already 5–10 minutes of running per day can reduce CVD-risk and -mortality [11]. Benefits of resistance training on CRF were also proven across different age groups [12].
The WHO guidelines for PA among adults recommend both regular aerobic physical exercise as well as muscle-strengthening exercises [5]. A sport that targets this combination of stimuli in a time-efficient manner is CrossFit® (CF) (CrossFit® Inc., Washington, USA). What is special about CF is the combination of routines from gymnastics, bodyweight exercises and Olympic weightlifting in a group-based setting. It prepares athletes for diverse and random physical challenges [13] and was initially invented to cover the physical demands of people working in military, police, or firefighting. For the general public, CF is still a new exercise modality, and the physiological mechanisms that it triggers have yet to be scientifically investigated.
Previously reported effects of CF training on CRF are contradictory. McKenzie et al. found no significant VO2max improvement in females after four weeks intervention [14]. Inconsistent with this, Cosgrove et al. indicated that only female novices significantly improved throughout six-month intervention, while males did not [15]. Likewise, Murawska-Cialowicz and colleagues stated a significant VO2max increase in women but not men [16]. Among studies investigating CF and body composition, the same ambiguity is found. Some report beneficial effects [16,17] whereas others found no effect [18]. One previous study investigated prolonged CF practice and overall well-being with no significant improvements [19].
Yet, several points are striking about to-date CF literature. Few CF studies show high level of evidence and low risk of bias combined [20]. Many investigated short-term interventions or single CF training sessions. Moreover, most studies included predominantly male subjects with CF experience. Beneficial health outcomes could however be especially prominent in sedentary individuals without CF experience. Therefore, this target group needs further investigation. Exclusively one six-month interventional study included male and female inactive employees. They identified beneficial outcomes on mobility and strength [19]. Following up on this, we aimed to fill the gap on continuous CF training and CRF in a sedentary population of CF beginners.
To the best of our knowledge, this is the first study to test effects of a nine-months intervention in male and female working-age beginners with less than six months CF experience. This should control for interference with any previously existing CF-related fitness. Next to changes in aerobic capacity (VO2max) and well-being, we investigated body composition on multiple occasions. We anticipated that the high intensity and power output of CF training would provide a great stimulus for CRF and body composition improvement. Further, frequent group workouts were thought to positively influence overall well-being.
2. Materials and Methods
This pre-post, single group, interventional study was conducted from August 2018 to September 2020. Participants engaged in regular CF training for nine months. We investigated CRF, well-being, and body composition during five screening visits at the laboratory. Three “big” measurements including cardiopulmonary exercise testing (CPET) and anthropometric measures were conducted after recruitment (t0), in month 3–4 (t2) and in month 8–9 (t4). In-between, two “small” measurements (t1, t3) tracked the anthropometric measures. Pre- and post-intervention (t0, t4), participants filled in the WHO-5-index for well-being. A study timeline is displayed in Figure 1.
Subjects provided health-related information (smoker/non-smoker, diet, history of disease and injuries, activity level at occupation) and reported their present and past participation in sports (CF and others).
This study was conducted in accordance with the 1975 Declaration of Helsinki and approved by the Ethics Committee of the University of the Bundeswehr Munich, Germany (06/04/2018). All participants provided informed consent before study participation. The trial was registered on ClinicalTrials.gov (trial number: DRKS00027059, on 11/04/2021).
Subjects
Recruitment was conducted by use of advertising posters in nine CF affiliates in Munich (Aug. 2018 – Oct. 2019). We included participants that were 1) aged 18 or older, 2) CF beginners (< 6 months experience), 3) willing to perform ≥ 2 CF workouts/week for nine months, 4) willing to attend five screening visits. Pregnancy and chronic or acute health issues (severe cardiovascular, respiratory, musculoskeletal, or metabolic diseases, osteoporosis, intervertebral disc damage, joint replacements, fresh scars, and hypertension) were defined as exclusion criteria. 46 participants were initially recruited for baseline screening (Table A1, supplement). Participants who missed screening visits were excluded from the analysis. All were informed about potential risks and advised to consult their physician before study participation. Afterwards, all provided written, informed consent.
Procedures
CF workouts combine multiple domains: Aerobic exercises (like running, cycling, or rowing), gymnastics and bodyweight movements (like hand stands and pull-ups), and weightlifting routines (like squats, deadlifts, clean, snatch, and overhead press). A classical CF workout comprises 60 minutes, starting with a warm-up and a skill development part. Afterwards, the “Workout of the day” (WOD) of about 10-20 minutes follows. The workout is summed up by a cool down. The StartXFit protocol scheduled participation in ≥ 2 CF sessions per week for nine months. Both exercising with a coach and self-organized exercise (“open gym”) in line with the CF concept were possible. Information on frequency and kind of CF participation was provided by the subjects in a questionnaire.
Endpoints
The primary endpoint was defined as change in maximum oxygen uptake (VO2max, in ml/min/kg) assessed by cardiopulmonary exercise testing (CPET). It was screened on three occasions, t0, t2 and t4. Statistical power analysis was based on the measurement of our primary endpoint. Development of psychological well-being was screened as secondary endpoint with a questionnaire (t0 and t4). Body composition was assessed for exploratory purpose at t0–t4.
Cardiopulmonary Exercise Testing (CPET)
For CPET measures, participants were instructed not to engage in vigorous exercise and avoid alcohol or massive caffeine consumption 24 hours prior to testing. They were advised to eat well three hours before and ensure adequate fluid intake. Maximum oxygen uptake (VO2max, ml/min/kg) was assessed with a mobile breath-by-breath spiroergometry system (dynostics, Sicada GmbH, Bad Wörishofen, Germany). Subjects performed an incremental step test on an electronically braked cycle ergometer (motion cycle 800, emotion fitness GmbH & Co. KG, Speyer, Germany). The test was initiated with a load of 75/50 watts for males and females, respectively. A power increment of 25 watts/20 watts was applied every two minutes. Participants should pedal at 60–80 rpm. The test was conducted until maximal exertion, defined as fulfilling one or more of the following: RER of > 1.1, VO2 plateau, heart rate within 10 bpm of age-predicted max. VO2max was captured by averaging the VO2 (ml/min/kg) of the last thirty seconds at individual peak performance. Heart rate was continuously tracked by use of a Bluetooth heart rate belt (Polar H9, Polar AG, Kempele, Finland).
Well-Being
The German version of the WHO-5-Index was used to test well-being. It is a well-respected method to assess psychological well-being, showing high validity and reliability [21]. The questionnaire comprises five simple statements on current mental health within the last two weeks. Participants rated their accordance with the statements on a 0–5-point scale. All scores were summed up and multiplied by four. The resulting well-being score was given as a percentage, whereby 100 % was achieved by rating all five statements with five points.
Body Composition
Anthropometric measures comprised height (cm), weight (kg), BMI (kg/m2), muscle mass (%), body fat (%), and resting metabolic rate (kcal). Body composition analysis was conducted by bioelectrical impedance analysis on a Tanita scale (Tanita SC-240 MA, Tanita Europe BV, Amsterdam, Netherlands). We advised participants to avoid changes in their nutritional habits 48 hours prior to testing and ensure adequate hydration status.
Statistical Analysis
The change in VO2max between t0, t2, and t4 should display the effects of the CF intervention. We therefore conducted a one-way repeated measures ANOVA. To determine the most prominent change, post hoc Bonferroni-adjusted pairwise comparisons were subsequently performed. ANOVA results are shown as mean and 95 % confidence interval (CI). Effects sizes are given as partial eta2 () and interpreted as follows: small effect (> .01), medium effect (> .06) and large effect (> .14). We performed a pearson product-moment correlation between VO2max at baseline (t0) and after nine-months (t4) (ΔVO2max ml/min/kg %). For this purpose, we divided the sample into three different groups (non-responder, responder+, and responder++). For exploratory purpose, we assessed changes in body composition from t0 to t4 by means of a one-way repeated measures ANOVA. A t-test for dependent samples was used to assess changes in well-being (t0–t4). Cohen’s d is indicated for the effect size and interpreted as follows: small effect (= .2), medium effect (= .5) and large effect (= .8) [22]. All data were priorly analyzed for normality by Shapiro-Wilk Test. In case of violations of normality (p < .05), we analyzed by Friedman Test in addition to the parametric test. In case of violations of sphericity, tested by Mauchly-test, a Greenhouse-Geisser adjustment was used. Statistical significance was set at p ≤ .05. Descriptive statistics are presented as mean ± standard deviation (SD). All data analysis was performed in SPSS 28® (IBM SPSS, Armonk, NY, USA).
3. Results
Four of the 46 initially recruited participants were excluded (> six months of CF experience). Of the remaining 42 subjects, 16 completed the study protocol and provided enough data for inclusion into our analysis. This results in a dropout of 65.2 %. Figure 2 displays the flow of participants throughout the study.
3.1. Descriptive Statistics
Baseline (t0) statistics of all subjects who completed the intervention are listed in Table 1. Age ranged between 23–55 years. Two subjects were former smokers.
Exercising behavior changed throughout the study. At t0, CF was performed on 2.3 ± 0.6 days a week for 1 ± 0.3 hours per session. At t4, average CF sessions per week increased significantly to 3.6 ± 1.6 days for 1.2 ± 0.3 hours per session (t(13) = -3.41, p = .002). Next to CF, 75 % (n = 12) practised other sports on 1 ± 1.4 days per week at t0. Endurance sports was the most frequently mentioned additional sport in 56.3 % (n = 9) of the cases. At t4, the participation in other sports slightly decreased to 62.5 % (n = 10). Still, 43.8 % (n = 7) mentioned endurance sports as the additional workout of the week.
87.5 % (n = 14) have played sports in their childhood and adolescence, on 3.6 ± 1.3 days per week (Table A2, supplement).
3.2. Primary Endpoint VO2max
VO2max significantly increased (F (2, 30) = 5.617, p < .01, = .27) (Table 2) with the most prominent increase between t0 and t4 (Mdiff = 4.97, [0.12, 9.73]). VO2 data were not normally distributed (p < .05). Additional analysis by Friedman test confirmed significant increase in VO2max (χ2(2) = 7.63, p = .022) (Table A3, supplement).
To get a deeper understanding on the effect of CF training on VO2max, the percentual changes from t0 to t4 were categorized for all subjects. In the category “non-responders” (n = 6) subjects either decreased their VO2max during the intervention or showed a negligible effect (-14.3–1.0 %). N = 5 participants fell into the category “responders+”, with an increase of 7.4–16.8 %. At last, the “responders++”, (n = 5) raised their individual VO2max by 23–62.5 %. Comparing the VO2max at t4 among the three categories shows, that all achieved similar values of 49.73 ml/min/kg, 47.25 ml/min/kg and 47.58 ml/min/kg, respectively. This was regardless of the fact that at baseline, VO2max clearly differed between the three categories (Figure 3). A pearson product-moment correlation revealed a strong negative correlation between VO2max at baseline (t0) and its progression in % at t4 (Δ VO2max ml/min/kg %) (r = -.654, p = .006, n = 16) (Figure 3).
3.3. Secondary Endpoint Well-Being
Psychological well-being was assessed by WHO-5-Index pre- and post-intervention (t0 and t4). A significant increase of 8.7 % was found (t (11) = -2.24, p = .005, d = .59) (Table 2).
3.4. Exploratory
Resting metabolic rate changed significantly (F (2.3, 25.5) = 3.43, p = .042, = .24) (Table 3). As some data were not normally distributed, analysis by Friedman test approved the non-significant development of all anthropometric measures but resting metabolic rate (χ2(2) = 13.64, p = .009) (Table A4, supplement).
4. Discussion
The main outcome of the StartXFit trial was a significant 11,5 % effect of time for aerobic capacity (VO2max, ml/min/kg). Especially subjects with low baseline VO2max improved. Further, psychological well-being significantly increased by 8.7 %. Resting metabolic rate significantly increased by 2.2 %, while other anthropometric measures followed a positive but non-significant trend. To the best of our knowledge, this was the first study to look at long-term effects on cardiopulmonary fitness in CF beginners as a primary endpoint.
Primary Endpoint - VO2max
All subjects reported to be predominantly sitting at work. Considering the growing body of evidence for the association between time spent sitting and CVD risk [23,24], CRF was chosen as primary endpoint in this study. CRF is an important clinical measure to asses individual CVD-risk and is often indicated as VO2max (ml/min/kg). After nine months of CF intervention (≤ 2 CF workouts/week), participants improved their VO2max by an average of 11.5 % with high statistical significance (p < .01) and a large effect ( = .27). According to Lee et al., a 1-MET VO2max improvement (3.5 ml/min/kg) is already associated with 19 % lower risk of CVD mortality [11]. The mean achievement of 5 ml/min/kg observed in our subjects therefore indicates the potential of regular CF training to improve individual aerobic fitness, cardiopulmonary health, and lower the risk for CVD. Increased VO2max is a product of enhanced oxygen uptake, transportation, and utilization at cellular level. We assume that the 11.5 % improvement mainly resulted from the characteristic WOD part of a CF workout, which combines resistance training, anaerobic and aerobic exercises at high intensity. A recent study from Meier et al. supports this assumption. They specified, that especially the WOD imposes intense cardiorespiratory stimuli, with heart rate (HR) values of ≥ 91 % of HRmax [25]. In line with that, Helgerud et al. investigated superior VO2max improvement through short, high-intensity running intervals at 90–95 % HRmax in comparison to training at lower intensities at lactate threshold or 70 % HRmax [26]. Previous studies investigating effects of CF on CRF appeared to be contradictory. McKenzie et al. found no significant VO2max improvement in young females after four weeks intervention, while specific strength parameters improved [14]. On the contrary, Murawska-Cialowicz and colleagues reported a significant VO2max increase in women but not in men after three months of CF participation [16]. Similarly, Cosgrove et al. tested VO2max with the Cooper test pre and post six months of intervention [15]. Female CF beginners (0–6 months experience) improved significantly, while those with > 6 months experience did not. In men, they found no significant effect on aerobic performance. At last, Crawford et al. failed to indicate any significant change in VO2max in both sexes after a six-weeks HIFT intervention [27]. Our results add to the literature, that it took nine months of CF intervention to achieve a significant 11.5 % change in VO2max. At screening visit t2 (after 3–4 months) aerobic capacity improved by 8.8 %, which was non-significant. However, it must be considered, that we exclusively included CF beginners, whereas other studies tested participants with mixed experience levels. This complicates the comparison of results. Further, as our sample only includes two females, an analysis based on gender is difficult.
Another finding in our study was the strong negative correlation between individual VO2max at baseline and its change (in %) after nine-months. Therefore, the better the VO2max of a participant was at t0, the less this parameter improved in percentage at t4. Hence, especially sedentary, and unfit individuals can benefit from regular CF participation and achieve great effects on cardiovascular fitness. Previously, Cosgrove et al. reported similar results when comparing effects of CF training in experienced and non-experienced subjects [15]. Women with 0–6 months CF experience showed greater improvement on their 1.5 mile run than those with 7+ months experience. Further, Ozaki et al. described comparable findings in their study on resistance training effects on VO2max. They found a significant negative correlation between individual VO2max measures at baseline and the resistance-training-induced changes at study end [12]. These findings suggest the dependence of training-induced VO2max changes upon baseline VO2max.
Secondary Endpoint - Well-Being
Our intervention resulted in 8.7 % greater well-being with a significant, medium effect (d = .59). This highlights the positive impact of CF training on mental health. Previously, only Brandt et al. investigated well-being before and after a six-month CF intervention in sedentary employees. Strikingly, they found no significant improvement. In comparison, our subjects reported greater well-being at baseline (60.5 % to 54,4 %) and study end (69.2 % to 61.6 %) [19].
Prior to the intervention, as much as 87.5 % of our subjects already practiced some kind of sport. We therefore cannot argue that the improvement in well-being observed here solely resulted from being physically active. We however assume, that particularly CF as a sport influenced individual well-being. Possibly, it brought a new athletic challenge to the subject’s workaday life, yielding physiological but also psychological effects. This assumption is supported by the increase of weekly CF sessions reported by the participants along study duration. The study protocol prescribed a minimum of two weekly sessions. At t0, the average was 2.3 sessions/week, which significantly increased to 3.6 sessions/week at t4. A possible explanation can be found in the philosophy of CF: To many athletes, CF does not solely encompass the physical training concept but a whole lifestyle with certain philosophies on exercise, recovery, nutrition, and even fashion [13]. Moreover, the group-based character of CF should not be underestimated. Working out in a group can enhance adherence and generate a social atmosphere [28]. Whiteman-Sandland et al. demonstrated a greater “sense of community” and belonginess among members of CF affiliates in comparison to those exercising in traditional gyms [29]. Altogether, this could explain the positive effect on well-being observed here.
Exploratory
Occupational sitting hours are associated with adverse effects on body weight and fat mass [24,30,31,32]. Body composition was therefore screened for exploratory purpose. Improved body composition through CF training was earlier reported, even after shorter intervention periods [16,33]. Unlike our assumptions, body weight (-1.6 kg, 1.9 %) and body fat (-1.2 %) showed a negative trend and muscle mass increased by 1.2 %, however these changes were non-significant. Only resting metabolic rate significantly rose by 42.4 kcal/day (2.2 %), even though mean body weight decreased. Despite no significant improvements in body weight, fat mass, and muscle mass, the positive trend among all parameters still holds a clinical value for overall health status. In line with this, Sobrero et al reported no improvement of body composition after ten weeks of CF intervention in sedentary women. They proposed increased appetite due to increased physical exercise as a possible reason [18]. We did not control for a change in diet or collect data on nutritional habits during the intervention, which makes assumptions difficult. Cavedon et al. found, that a high weekly training load (> 10 h) yielded superior changes in muscle mass, lean body mass, and fat mass when compared to less or no CF training [17].
Per definition, mean BMI at baseline (26.1 kg/m2) and at intervention end (25.7 kg/m2) were categorized as slightly overweight [34]. The average BMI of the sample fell into the range (24.5–36.4 kg/m2) previously reported by other CF studies (15,19,33,35). To reveal the underlying body composition, average fat (t0: 21.1 %) and muscle mass (t0: 75 %) were also tracked. Contextualizing these measures with previous CF studies suggests a high baseline fitness of our sample. Smith et al for example reported a BMI of 28.1 kg/m2 for men and 25.1 for women, with a fat mass of 22.2 % and 26.6 %, respectively (33). Brisebois et al. tested physically inactive adults with a BMI of 36.4 kg/m2 for male and 26.5 kg/m2 for female participants and an average fat percentage of 38 % [35].
It is however striking, that an average of 3.3 weekly trainings (2.3 days CF, 1 day additional sport) did not result in reduction of weigth or bodyfat, nor did muscle mass increase significantly in our participants. A potential explanation will be discussed below.
For the implication of both VO2max and body composition outcomes, some important facts have to be discussed. Firstly, in the questionnaire at t0 and t4, 75 % of participants reported to engage in other sports next to the intervention. 56.3 % of them did at least one weekly endurance training at t0. At t4, the number decreased to 43.8 %. Further, most subjects (87.5 %) engaged in sports since their childhood and used to do as much as 3.6 weekly workouts. As stated before, this suggests a high baseline fitness, even though our subjects were CF beginners with low activity level at work. The baseline VO2max measures, especially those of the non-responder group (51.8 ml/min/kg, Figure 3), suggest a high fitness level compared to up-to-date measures in a northern European population [36]. The low average fat percentage (21.1 %) underscores this notion. Under this baseline circumstances, the question raises what additional improvement in aerobic capacity and body composition through the intervention could be expected in this sample.
Even though two weekly CF workouts were obligatory for study participation, some subjects completed as many as six per week. Yet, neither a significant dose-response relationship between weekly hours of CF and VO2max improvement nor a correlation between VO2max improvement and engagement in endurance training next to CF could be indicated. These aspects need further investigation.
Dropout and limitations
The dropout rate of 65.2 % was unexpectedly high. Previous CF interventional studies with durations of >10 weeks reported dropouts of 29 % [19] and 20 % [33], whereas many did not clarify their dropouts. A mean drop-out of 45 % for physical activity interventional studies in general was earlier reported by Marcus et al. [37]. Different reasons may explain the prior termination of 26 participants in our study. Firs, our nine-month intervention was longer than any other CF interventional study yet reported. It comprised two mandatory workouts/week and a total of five laboratory screenings. This time-consuming design asked for a lot of commitment and engagement. Further, only CF beginners were included, which involved the risk of subjects trying out CF but then terminating their participation priorly. On top of that, the Covid-19 pandemic provided additional barriers to working out in groups and affiliates.
A clear limitation of our study is the uneven distribution of the sexes. We lost 15 of initially 17 female participants. Another constraint is the missing information on training load, type of training, and well-being at timepoint t2. To set the collected VO2max and body composition measures at t2 into a context, this information would be of value. Therefore, the questionnaire should have been collected at t2 as well. Further, details on diet and eating habits could add important information to the analysis of body composition, especially to control if the subject’s appetite was increased by the training intervention. Besides, even though the sample was standardized in terms of CF experience level, the baseline fitness level differed among the participants (VO2max range of 25.1–73.8 ml/min/kg, body fat range of 11.2–35.9 %). Lastly, our definition of a CF beginner (< 6 months experience) still allows a potential difference of 6 months in experience between the participants. This complicates the interpretation of physiological measures and body composition as discussed above.
A major strength of our trial was the long-term intervention period. For the first time, CF athletes were tracked over more than 6 months duration. Further, our intervention did not stick to a certain CF routine or protocol. We investigated participation in regular CF training as it happens in a genuine CF affiliate. This increases the value for practical implication.
5. Conclusions
What stands out about this study is the significant improvement (11.5 %) in VO2max after nine months of ≥ 2 CF workouts/week in adult beginners. Another major finding was the significant increase (8.7 %) in overall well-being. Also, resting metabolic rate increased significantly (2.2 %). A non-significant positive trend on body weight, fat mass, and muscle mass could be registered. These findings reveal the health and fitness promoting effects of regular CF training, especially on cardiorespiratory parameters. The benefits were particularly promising for subjects with low baseline fitness. Due to the group-based, versatile, and time-efficient design, CF is a suitable training program, even for people with low intrinsic motivation.
Author Contributions
Conceptualization, A.S.; methodology, J.S. and T.B.; formal analysis, J.S., T.B. and A.S.; investigation, J.S. and T.B.; resources, A.S; writing—original draft preparation, J.S..; writing—review and editing, T.B. and A.S.; supervision, A.S.; funding acquisition, J.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding. The costs for open Access publication were funded internally by the library of the University of the Bundeswehr Munich (Universitäsbibliothek, OpenAccess Fund) grant number UID DE811246937.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of the University of the Bundeswehr Munich (6th of April, 2018).” for studies involving humans. The trial was registered on ClinicalTrials.gov (DRKS00027059; 11/04/2021).
Informed Consent Statement
Written, informed consent for participation in the study as well as for publication of this paper was obtained from all subjects involved in the study.
Data Availability Statement
Anonymized data have been made publicly available at the Open Science Framework (osf.io) and can be accessed at: https://osf.io/h7fjq/?view_only=d03a82fe6a394f1dbd857a7c3a189620.
Acknowledgments
The authors would like to thank all participants for volunteering and engaging in the intervention. Further, we would like to thank CrossFit Wuid in Munich for providing the accommodation for all tests.
Conflicts of Interest
The authors declare no financial or non-financial conflict of interest.
Appendix A
CrossFit
The exercise program CF combines multiple domains: Aerobic exercises (like running, cycling, or rowing), gymnastics and bodyweight movements (like hand stands and pull-ups), and weightlifting routines (like squats, deadlifts, clean, snatch, and overhead press). The movements range from being rudimentary to very complex and should always involve multiple joints. Exercises are either completed based on time, on repetitions, a specific distance covered, or a specific weight lifted [15]. A classical CF workout comprises 60 minutes, starting with a warm-up and a skill development part. Afterwards, the “Workout of the day” (WOD) of about 10-20 minutes follows. Every day, it focuses on alternating exercises, muscle groups and skills. As an example, the workout “Kelly” comprises 5 rounds of: 400 m run, 30 box jumps, and 30 wall balls that should be completed as fast as possible. Which WOD will appear on the agenda is unknown to the athletes in advance. The workout is summed up by a cool down which focusses on extensive stretching.
Statistical power
Our intervention focused on CF beginners with less than six months experience. Therefore, large effects in CRF were expected, which is in line with other studies in CF athletes of mixed fitness levels, who found significant improvements in VO2max 16,33. To achieve a statistical power of at least 85 % with an alpha level of .05 (two-sided), we calculated the need for at least 18 participants using the G*Power software (version 3.1.9.6; Heinrich Heine Universität Düsseldorf, Germany). Because of the time-consuming study design, a drop-out of about 50 % was expected 37. Therefore, 46 participants were initially recruited.
Appendix B

Table A1.
Anthropometry and demographics of initially recruited participants at baseline (t0).
| All participants (n = 46) |
Males (n = 29) |
Females (n = 17) |
|
| Male (%) | 63 | ||
| Female (%) | 36 | ||
| Age (y) | 33.8±8.1 | 35.1±7.3 | 31.5±9 |
| Height (cm) | 177.2±9.2 | 182.1±7.2 | 168.8±5.4 |
| Weight (kg) | 80.1±17.8 | 89.1±15.6 | 64.8±8.5 |
| Body fat (%) | 23.1±7.2 | 20.8±6.5 | 27.0±6.8 |
| Muscle mass (%) | 73.0±6.9 | 75.3±6.2 | 69.2±6.4 |
| Resting metabolic rate (kcal) | 1819.1±378.9 | 2056.3±260.4 | 1414.4±95.6 |
| Current smoker (%) | 6.5(n=3) | ||
| Sedentary occupation (%) | 93.5(n=43) |
Values are mean ± SD; age: at beginning of intervention; sedentary occupation: predominantly sitting at work.
Table A2.
CrossFit and other sports behavior of participants at baseline (t0) and at end of intervention (t4).
Table A2.
CrossFit and other sports behavior of participants at baseline (t0) and at end of intervention (t4).
| t0 (n = 16) |
t4 (n = 14) |
p | |
|---|---|---|---|
| CrossFit: sessions/week | 2.3 ± 0.6 | 3.6 ± 1.6 | .002 |
| Hours per CrossFit session (h) | 1 ± 0.3 | 1.2 ± 0.3 | .168 |
| Practicing other sport (%) | 75 (n = 12) | 62.5 (n = 10) | |
| Practicing endurance sports (%) | 56.3 (n = 9) | 43.8 (n = 7) | |
| Other sports: sessions/week | 1 ± 1.4 | 0.7 ± 1.1 | |
| Hours per other training session (h) | 0.8 ± 1.3 | 1.6 ± 1.1 | |
| Practiced sports as child/adolescent (%) | 87.5 (n = 14) | ||
| Childhood sports sessions/week | 3.6 ± 1.3 |
Values are mean ± SD; p < 0.05*.
Table A3.
Non-parametric Friedman test for primary outcome VO2max (ml/min/kg).
| n | Chi-Square | p | |
|---|---|---|---|
| VO2max (ml/min/kg) | 16 | 7.63 | .022* |
Maximum oxygen uptake (VO2max) in ml/min/kg; *p < .05.
Table A4.
Non-parametric Friedman test for exploratory endpoints.
| df | Chi-Square | p | |
|---|---|---|---|
| Weight (kg) | 16 | 2.41 | .662 |
| Body fat (%) | 16 | 2.20 | .699 |
| Muscle mass (%) | 16 | 2.33 | .675 |
| Basal metabolism (kcal) | 12 | 13.64 | .009* |
| Resting heart rate (bpm) | 16 | 0.61 | .962 |
bpm = beats per minute; *p < .05.
References
- Guthold R, Stevens GA, Riley LM, Bull FC. Worldwide trends in insufficient physical activity from 2001 to 2016: A pooled analysis of 358 population-based surveys with 1·9 million participants. Lancet Glob Health. 2018, 6, e1077–e1086. [CrossRef]
- Finger JD, Mensink G, Lange C, Manz Kristin. Arbeitsbezogene körperliche Aktivität bei Erwachsenen in Deutschland Journal of Health Monitoring Arbeitsbezogene körperliche Aktivität bei Erwachsenen in Deutschland. Robert Koch Institut [Internet]. 2017; Available from: www.geda-studie.de.
- Brach M, Trabelsi K, Chtourou H, Boukhris O, Masmoudi L, Bouaziz B; et al. Effects of COVID-19 home confinement on physical activity and eating behaviour Preliminary results of the ECLB-COVID19 international online-survey. [CrossRef]
- Cheval B, Sivaramakrishnan H, Maltagliati S, Fessler L, Forester C, Sarrazin P; et al. Relationships Between Changes in Self-Reported Physical Activity and Sedentary Behaviours and Health During the Coronavirus (COVID-19) Pandemic in France and Switzerland. Journal of Sports Science. 2021, 39, 699–704. [CrossRef]
- World Health Organization. WHO Guidelines on physical activity and sedentary behaviour [Internet]. 2020 [cited 2023 Jan 30]. Available from: https://www.who.int/publications/i/item/9789240015128.
- Bize R, Johnson JA, Plotnikoff RC. Physical activity level and health-related quality of life in the general adult population: A systematic review. Prev Med (Baltim). 2007, 45, 401–415. [CrossRef]
- Cerin E, Leslie E, Sugiyama T, Owen N. Associations of multiple physical activity domains with mental well-being. Ment Health Phys Act. 2009, 2, 55–64. [CrossRef]
- Mason P, Kearns A. Physical activity and mental wellbeing in deprived neighbourhoods. Ment Health Phys Act. 2013, 6, 111–117. [CrossRef]
- Al-Mallah MH, Sakr S, Al-Qunaibet A. Cardiorespiratory Fitness and Cardiovascular Disease Prevention: An Update. Vol. 20, Current Atherosclerosis Reports. Current Medicine Group LLC 1; 2018. [CrossRef]
- Ross R, Blair SN, Arena R, Church TS, Després JP, Franklin BA; et al. Importance of Assessing Cardiorespiratory Fitness in Clinical Practice: A Case for Fitness as a Clinical Vital Sign: A Scientific Statement From the American Heart Association. Circulation 2016, 134. [CrossRef]
- Lee D chul, Pate RR, Lavie CJ, Sui X, Church TS, Blair SN. Leisure-Time Running Reduces All-Cause and Cardiovascular Mortality Risk. J Am Coll Cardiol. 2014, 64, 472–481.
- Ozaki H, Loenneke JP, Thiebaud RS, Abe T. Resistance training induced increase in VO2max in young and older subjects. European Review of Aging and Physical Activity. 2013, 10, 107–116. [CrossRef]
- Glassmann, G. Level 1 Training Guide - CrossFit Training. 2020 [cited 2023 Jan 30]; Available from: http://library.crossfit.com/free/pdf/CFJ_English_Level1_TrainingGuide.pdf.
- McKenzie, MJ. Crossfit Improves Measures Of Muscular Strength And Power In Active Young Females. Med Sci Sports Exerc. 2015, 47, 797. [Google Scholar] [CrossRef]
- Cosgrove SJ, Crawford DA, Heinrich KM. Multiple fitness improvements found after 6-months of high intensity functional training. Sports 2019, 7. [CrossRef]
- Murawska-Cialowicz E, Wojna J, Zuwala-Jagiello. J. Crossfit training changes brain-derived neurotrophic factor and irisin levels at rest, after Wingate and progressive tests, and improves aerobic capacity and body composition of young physically active men and women. Journal of Physiology and Pharmacology. 2015, 66, 811–821.
- Cavedon V, Milanese C, Marchi A, Zancanaro C. Different amount of training affects body composition and performance in High-Intensity Functional Training participants. PLoS ONE 2020, 15, e0237887. [Google Scholar] [CrossRef]
- Sobrero GL, Inman C, Stone W, Zagdsuren B, Arnett SW, Shafer MA; et al. Crossfit Vs. Circuit-trained Individuals. Med Sci Sports Exerc. 2015, 47, 800.
- Brandt T, Schmidt A, Schinköthe T, Heinz E, Klaaßen Y, Limbara S; et al. MedXFit—Effects of 6 months CrossFit® in sedentary and inactive employees: A prospective, controlled, longitudinal, intervention study. Health Sci Rep. 2022, 5.
- Claudino JG, Gabbett TJ, Bourgeois F, Souza H de S, Miranda RC, Mezêncio B; et al. CrossFit Overview: Systematic Review and Meta-analysis. Vol. 4, Sports Medicine - Open. Springer; 2018. [CrossRef]
- Topp CW, Østergaard SD, Søndergaard S, Bech P. The WHO-5 Well-Being Index: A Systematic Review of the Literature. Psychother Psychosom. 2015, 84, 167–176.
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences. Routledge; 2013.
- Henschel B, Gorczyca AM, Chomistek AK. Time Spent Sitting as an Independent Risk Factor for Cardiovascular Disease. Am J Lifestyle Med. 2020, 14, 204–215. [CrossRef]
- Straker L, Coenen P, Dunstan D, Gilson N, Healy G. Sedentary Work – Evidence on an Emergent Work Health and Safety Issue – Final Report. Safe Work Australia [Internet]. 2016 [cited 2023 Feb 2]; Available from: https://www.safeworkaustralia.gov.au/sites/default/files/2022-03/literature-review-of-the-hazards-of-sedentary-work%202.pdf.
- Meier N, Sietmann D, Schmidt A. Comparison of Cardiovascular Parameters and Internal Training Load of Different 1-h Training Sessions in Non-elite CrossFit® Athletes. Journal of Science in Sport and Exercise. 2022 Jun 22; [CrossRef]
- Helgerud J, HØydal K, Wang E, Karlsen T, Berg P, BJERKAAS M; et al. Aerobic High-Intensity Intervals Improve V˙O2max More Than Moderate Training. Med Sci Sports Exerc. 2007, 39, 665–671. [CrossRef]
- Crawford D, Drake N, Carper M, DeBlauw J, Heinrich K. Are Changes in Physical Work Capacity Induced by High-Intensity Functional Training Related to Changes in Associated Physiologic Measures? Sports. 2018, 6, 26.
- Heinrich KM, Patel PM, O’Neal JL, Heinrich BS. High-intensity compared to moderate-intensity training for exercise initiation, enjoyment, adherence, and intentions: An intervention study. BMC Public Health 2014, 14. [CrossRef]
- Whiteman-Sandland J, Hawkins J, Clayton D. The role of social capital and community belongingness for exercise adherence: An exploratory study of the CrossFit gym model. J Health Psychol. 2018, 23, 1545–1556. [CrossRef]
- Straker LM (Leon M, Coenen P, Dunstan DW, Gilson N, Healy G, Safe Work Australia. Sedentary work : Evidence on an emergent work health and safety issue. 61 p.
- Biddle SJH, Bengoechea García E, Pedisic Z, Bennie J, Vergeer I, Wiesner G. Screen Time, Other Sedentary Behaviours, and Obesity Risk in Adults: A Review of Reviews. Curr Obes Rep. 2017, 6, 134–147. [CrossRef]
- Lin T chi, Courtney TK, Lombardi DA, Verma SK. Association Between Sedentary Work and BMI in a U.S. National Longitudinal Survey. Am J Prev Med. 2015, 49, e117–23.
- Smith MM, Sommer AJ, Starkoff BE, Devor ST. Crossfit-Based High-Intensity Power Training Improves Maximal Aerobic Fitness and Body Composition [RETRACTED]. J Strength Cond Res. 2013, 27, 3159–3172. [CrossRef]
- U.S. Department of Health & Human Services. Defining Adult Overweight and Obesity. 2022 [cited 2023 Feb 2]; Available from: https://www.cdc.gov/obesity/basics/adult-defining.html.
- Brisebois M, Rigby B, Nichols D. Physiological and Fitness Adaptations after Eight Weeks of High-Intensity Functional Training in Physically Inactive Adults. Sports. 2018, 6, 146. [CrossRef]
- van der Steeg GE, Takken T. Reference values for maximum oxygen uptake relative to body mass in Dutch/Flemish subjects aged 6–65 years: The LowLands Fitness Registry. Eur J Appl Physiol. 2021, 121, 1189–1196. [CrossRef]
- Marcus BH, Williams DM, Dubbert PM, Sallis JF, King AC, Yancey AK; et al. Physical Activity Intervention Studies. Circulation. 2006, 114, 2739–2752.
Figure 1.
Study protocol with five screening visits (t0–t4) along the 9-months intervention timeline.
Figure 1.
Study protocol with five screening visits (t0–t4) along the 9-months intervention timeline.

Figure 2.
Flowchart of participants from recruitment to analysis.
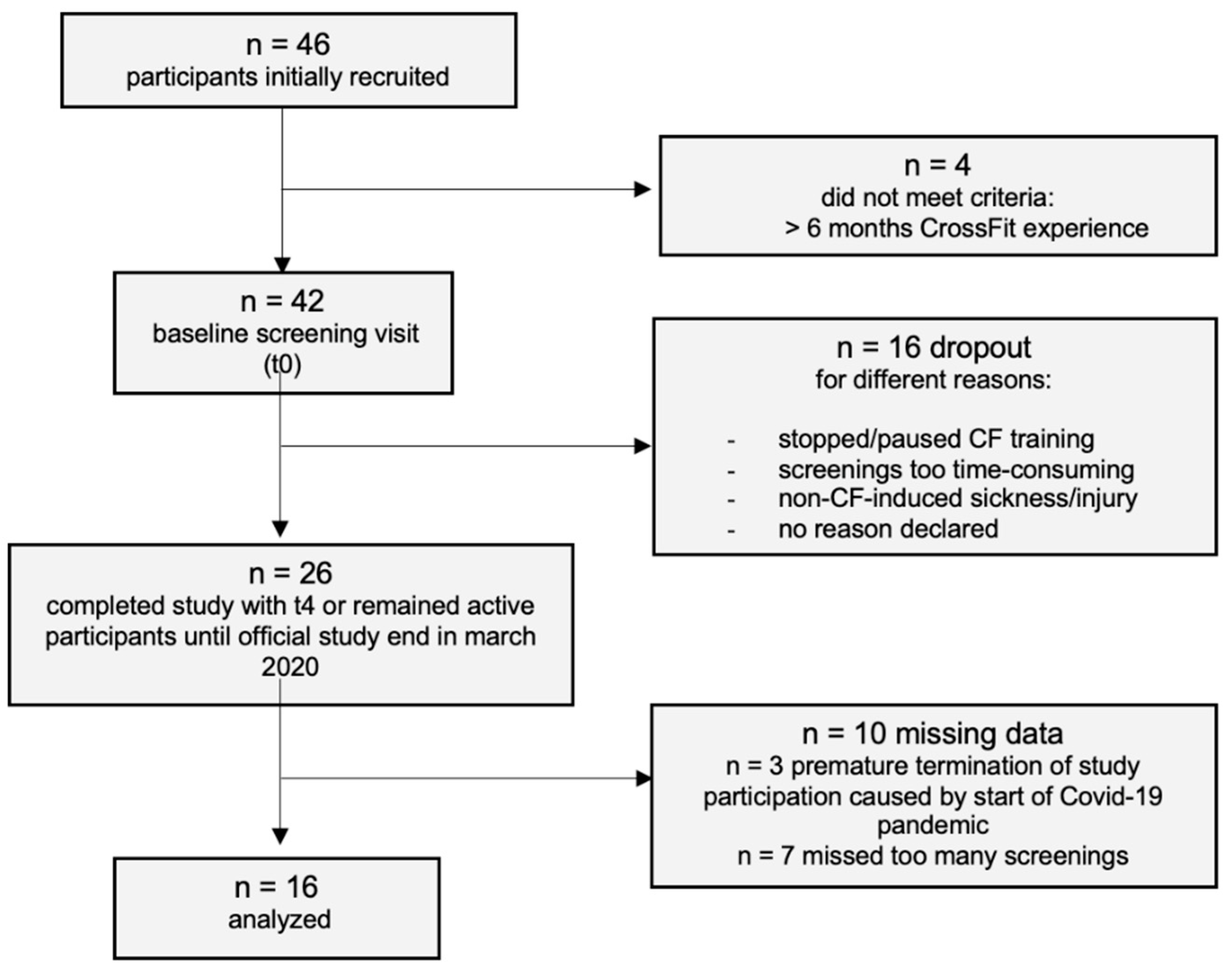
Figure 3.
VO2max (ml/min/kg) improvement (t0–t4) by category (“non-responders”, n = 6, -14.3–1.0 %; “responders+”, n = 5, 7.4–16.8 %; “responders++, n = 5, 23–62.5 %) and for total sample. Values shown as mean and 95 % CI.
Figure 3.
VO2max (ml/min/kg) improvement (t0–t4) by category (“non-responders”, n = 6, -14.3–1.0 %; “responders+”, n = 5, 7.4–16.8 %; “responders++, n = 5, 23–62.5 %) and for total sample. Values shown as mean and 95 % CI.
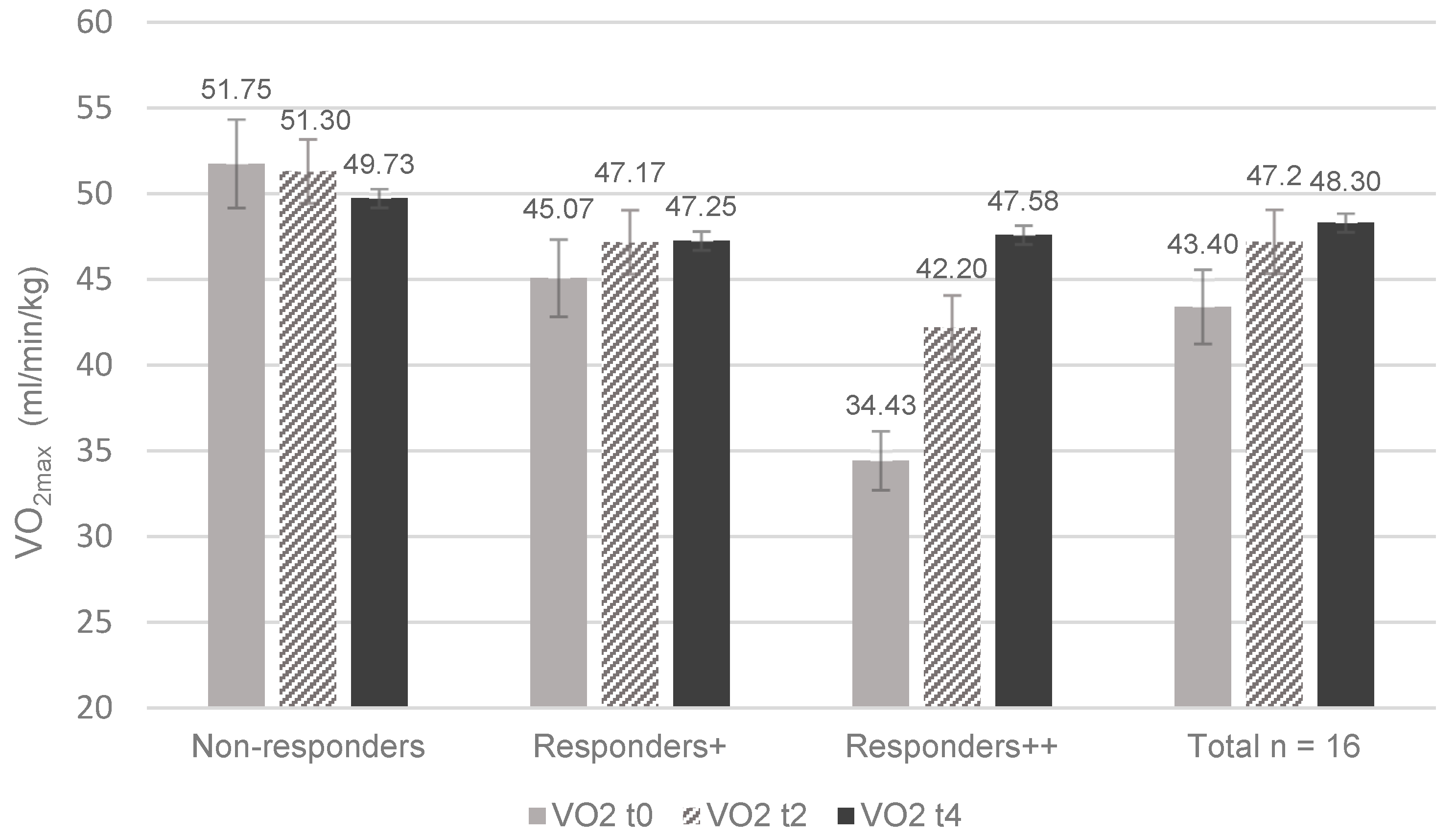
Table 1.
Anthropometry and demographics of the final n = 16 participants at baseline (t0).
| All participants (n = 16) |
Males (n = 14) |
Females (n = 2) |
|
| Male (%) | 87.5 | ||
| Female (%) | 12.5 | ||
| Age (y) | 35 ± 6.8 | 36 ± 6.4 | 28 ± 7.1 |
| Height (cm) | 180.6 ± 8.6 | 182.9 ± 5.9 | 164.0 ± 5.7 |
| Weight (kg) | 85.5 ± 19.1 | 88.6 ± 18.3 | 66.1 ± 4.5 |
| BMI (kg/m2) | 26.1 ± 4.6 | 26.3 ± 4.8 | 24.7 ± 3.3 |
| Body fat (%) | 21.1 ± 7.2 | 20.4 ± 7.4 | 26.3 ± 0.4 |
| Muscle mass (%) | 75.0 ± 6.8 | 75.7 ± 7 | 69.9 ± 0.3 |
| Resting metabolic rate (kcal) | 1962.3 ± 321.1 | 2032.7 ± 274.3 | 1469.0 ± 110.3 |
| Resting heart rate (bpm) | 65.9 ± 9.6 | ||
| Current smoker (%) | 6.3 (n = 1) | ||
| Sedentary occupation (%) | 100 (n = 16) |
Values expressed as mean ± SD; BMI: body mass index; bpm: beats per minute; sedentary occupation: mostly sitting at work.
Table 2.
Characteristics of VO2max and well-being throughout the intervention.
| n | t0 | t2 | t4 | Difference | ANOVA | ||
| M [95 % CI] |
M [95 % CI] |
M [95 % CI] |
t0–t4 | p | |||
| VO2max (ml/min/kg) | 16 | 43.3 [37.6, 49.1] |
47.2 [42.2, 52.1] |
48.3 [43.9, 52.7] |
5 [-4, 1.9] |
.008* | .27 |
| n | t0 | t4 | Difference | t-test | |||
| M [95 % CI] | M [95 % CI] | t0-t4 | p | d | |||
| Well-being (%) | 16 | 60.5 [52.2, 67.9] |
69.2 [61.1, 76.9] |
8.7 [2.4, 15] |
.005* | .59 | |
Inner-subject effects of time presented as mean and [95 % confidence interval]; Maximum oxygen uptake (VO2max in ml/min/kg) from t0-t4; *p < .05; effect size as η2p; Well-being in % at t0 and t4, effect size presented as Cohens’ d.
Table 3.
Characteristics of anthropological parameters from t0 to t4.
| t0 | t1 | t2 | t3 | t4 | Difference | ANOVA | ||
|---|---|---|---|---|---|---|---|---|
| M [95 % CI] | M [95 % CI] | M [95 % CI] | M [95 % CI] | M [95 % CI] | t0-t4 | p | ||
| Weight (kg) | 85.5 [75.3, 95.7] |
85.9 [76, 95.8] |
85.2 [75.7, 94.7] |
85.3 [76.2, 94.5] |
83.9 [76.8, 91.1] |
-1.6 [-8.4, 11.6] |
.617 | .02 |
| BMI (kg/m2) | 26.1 [23.6, 28.5] |
26.2 [23.8, 28.7] |
26 [23.7, 28.4] |
26 [23.8, 28.2] |
25.8 [24.2, 27.4] |
-.3 [-1.4, 1.9] |
.729 | .01 |
| Body fat (%) | 21.1 [17.3, 24.9] |
21.5 [17.4, 25.6] |
21.7 [17.6; 25.9] |
20.9 [17.2, 24.6] |
19.9 [16.2, 23.5] |
-1.2 [-1.7, 4.2] |
.296 | .08 |
| Muscle mass (%) | 75.0 [71.3, 78.6] |
74.6 [70.7, 78.5] |
74.3 [70.4, 78.3] |
75.2 [71.7, 78.6] |
76.2 [72.7, 79.7] |
1.2 [-4.1, 1.6] |
.282 | .08 |
|
RMR (kcal) |
1935.3 [1732, 2139] |
1934.7 [1737, 2133] |
1905.3 [1723, 2088] |
1942.1 [1756, 2128] |
1977.8 [1776, 2179] |
42.4 [-143.3, 58.4] |
.042* | .24 |
Inner-subject effects of time; *p < .05; effect size presented as η2p; RMR: resting metabolic rate.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



