Submitted:
02 August 2023
Posted:
04 August 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
We investigated humoral immune responses in 222 unvaccinated Japanese people after recovery from severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection in 2021. Anti-spike protein IgG antibody levels and neutralizing antibody titers were measured in serum samples obtained within 20–180 days after diagnosis. The geometric mean of antibody titers was 1555 ELU/mL (95% confidence interval [CI] = 1257-1923), and the neutralizing activities (50% inhibitory dilution) was 253 (95% CI = 204-313). The antibody titer and neutralizing activity both increased with increasing disease severity, and both values were approximately 4-fold higher for hospitalized patients than for non-hospitalized patients. However, these differences were smaller in older patients. The humoral immune response, which increased with increasing disease severity, gradually decreased over time after SARS-CoV-2 infection. Most patients with mild or moderate symptoms sustained neutralizing activity for up to 180 days after the infection, the decay of the neutralizing activity in the patients with asymptomatic was rather faster than other groups. 11.7% (26/222) of patients had very low neutralizing activity, and half of these were in the age of 20s. Our study results show the importance of measuring the neutralizing activity to confirm the immune status and also estimate the timing of vaccine.
Keywords:
COVID-19
; SARS-CoV-2
; Convalescent serum
; Neutralizing antibody
Introduction
Coronavirus disease 2019 (COVID-19) is an infectious disease caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), which was first identified in 2019 in Wuhan, China [1]. The outbreak of COVID-19 began with "pneumonia of unknown cause" in Wuhan City, Hubei Province in December 2019, followed by the international spread of the disease, mainly in China. The World Health Organization (WHO) declared a Public Health Emergency of International Concern (PHEIC) on January 30, 2020, and as of March 18, 2021, WHO reported 120,383,919 cases and 2,664,386 deaths worldwide, with 223 countries/regions with confirmed cases. Multiple coronavirus variants (alpha, beta, gamma, delta, and omicron) have been discovered to date, and they have spread globally (WHO).
It remained difficult to control SARS-CoV-2 transmission during pandemic waves because of the large number of people with asymptomatic infection, who have similar viral loads as symptomatic patients, as well as viral shedding in symptomatic patients before symptom onset. In Japan, seven SARS-CoV-2 epidemic waves were encountered through the middle of 2022. Each wave consisted of a sharp surge and subsequent decline in new infection cases. Some reports described the acquisition of humoral immune responses after recovery from SARS-CoV-2 infection in Japanese patients [2,3]; D614G mutation-carrying variants were the primary causes of COVID-19 [4].
Many important reports on the relationship between antibody production and patient background has been accumulated. In general, neutralizing antibody activities in patients with COVID-19 vary widely from patient to patient, peak neutralizing antibody activities, however, are known to increase in proportion to the severity of the disease [5]. However, the well-balanced and coordinated function of antibody-producing B cells, T cells is important for biological defense during acute infection with novel coronaviruses [6], and the importance of natural immune system has been pointed out, which contributes to an asymptomatically recovery despite the low production of antibodies [7]. Thus, a complex network of collaboration and communication among cells function to elimination virus should be considered, however, the information regarding antibody levels and activity analyzed by patient background and the decay of neutralizing activity still remains insufficient.
To manage the inoculation strategy for the available coronavirus vaccines, it is considered important for Japanese medical personnel to know the naturally acquired post–SARS-CoV-2 infection immunity status of patients and compare it with coronavirus vaccine-derived immunity. In this study, we evaluated the anti-spike and neutralizing antibody levels of patients infected with SARS-CoV-2 between January 2021 and September 2021. During this period, the alpha, delta, and D614G mutation-carrying variants were the primary causes of COVID-19 [4]. The objective of this study is to obtain the information for the development of new prophylactic vaccines and new treatments against COVID-19 in Japan.
Materials and Methods
Study Samples
Inclusion Criteria
Serum samples from non-hospitalized individuals or hospitalized individuals who had recuperated from previous SARS-CoV-2 infection, satisfying all of the following inclusion criteria, was selected in this observational study.
(1) Samples from study subjects from whom written voluntary informed consent to participate in this study has been obtained.
(2) Samples from study subjects who have given consent for the principal investigator, etc. to collect information on the diagnosis, treatment, etc. from the medical institution, health center, etc. where the SARS-CoV-2 infection was diagnosed/treated.
(3) Samples from study subjects aged 20 years or older at the time of informed consent.
(4) Samples from study subjects who have recuperated from infection after testing positive for SARS-CoV-2 diagnosed through nucleic acid detection or antigen testing and who tested negative in nucleic acid detection or antigen tests, or archival samples from individuals who have recuperated and are similar to those mentioned above.
(5) Samples from 20 to 180 days after testing positive for SARS-CoV-2.
Exclusion Criteria
Samples were excluded from the analysis if met any of the following criteria:
(1) Samples from individuals who have not recuperated from SARS-CoV-2 infection.
(2) Samples from recipients of prophylactic COVID-19 vaccines (including products in development).
(3) Samples for which there has been a request to withdraw consent.
(4) Samples considered ineligible by the principal investigator or sub-investigator.
Study Procedure
The SARS-CoV-2 infection was confirmed by nucleic acid detection or antigen testing. Samples from study subjects who recuperated from infection or archival samples from individuals who recuperated were transported to a testing facility in order to measure neutralizing activity against the pseudovirus of SARS-CoV-2 and SARS-CoV-2 spike (S) glycoprotein-specific antibody titers. For a sample collected from a study subject, a nucleic acid detection test or antigen test was performed again to confirm the SARS-CoV-2 infection status at the time of sample collection. If negative results are obtained, data was included in the analysis set of this study, and if positive results are obtained, data was excluded from the analysis set. Even if archival samples are used, data from samples with negative results was included in the analysis set.
The following information was entered into the case report form for each study subject: anonymized study ID, age, sex, onset date, date of definitive diagnosis, definitive diagnosis result (nucleic acid detection or antigen test), non-hospitalization/hospitalization, severity of SARS-CoV-2 infection, result of assessment of recuperation from infection (nucleic acid detection or antigen test), date of sample collection. The severity was classified into five levels as follows; asymptomatic, mild (no respiratory symptoms or cough only without dyspnea, SpO2 ≥ 96%, no evidence of pneumonia in any case), moderate I (no respiratory failure, pneumonia findings, or dyspnea, 93% < SpO2 < 96%), moderate II (respiratory failure requiring supplemental oxygen, SpO2 ≤ 93%), and severe (admitted to intensive care unit) or requiring a ventilator).
In this study, personal information was managed using an enrollment number unique to each study subject assigned for anonymization. A correspondence table of enrollment numbers was appropriately managed by the department in charge at the study institution providing biological samples. In addition, materials and correspondence tables containing other personal information collected in this study was managed appropriately in compliance with the management methods specified at the institution providing biological samples to protect personal information. If sharing study results with institutions providing biological samples, data was handled only with the anonymized study ID assigned for this study. The information to be provided to the collaborative research institution only was the anonymized study ID, measurement data, and information without personal identification and information that can identify a particular individual was not provided in order not to keep no possibility of risk or disadvantage associated with the leakage of information of study subjects.
Sample Analyses
SARS-CoV-2 anti-spike IgG concentrations were measured at Nexelis (Laval, Canada) using S-ELISA, and neutralizing activity (50% inhibitory dilution: ID50) was determined using PhenoSense SARS-CoV-2 neutralizing antibody assay (PNA) at Labcorp (Indianapolis, IN, USA). The analytical methods of S-ELISA and PNA were validated by Nexelis and Labcorp, respectively.
The SARS-CoV-2 Pre-Spike recombinant antigen is adsorbed onto the 96-well microplate. Following incubation, the microplate is washed to remove unbound SARS-CoV-2 Pre-Spike recombinant antigen and blocked to prevent non-specific binding. Standard, controls and sample dilutions are incubated in the coated microplate in which anti-SARS-CoV-2 Pre-Spike lgG specific antibodies (primary antibodies) bind to the coated antigen. Following incubation, the microplate is washed to remove unbound primary antibodies. Primary antibodies are detected with the addition of the anti-human lgG antibody (secondary antibody) conjugated to peroxidase. After incubation, the microplate is washed to remove unbound secondary antibodies. The peroxidase substrate solution, tetramethylbenzidine (TMB), is added to the microplate and a colored product is developed which is proportional to the amount of anti-SARS-CoV-2 Pre-Spike lgG antibodies present in the serum sample. 2N H2SO4 is then added to stop the colorimetric reaction. The absorbance of each well is measured using a microplate spectrophotometer reader at a specific wavelength (450/620 nm). Antibody concentrations are calculated for each control and sample dilution by interpolation of the OD values on the 4-parameter logistic (4-PL) standard curve and adjusted according to their corresponding dilution factor. The final concentration of controls and samples were then determined by calculating the geometric mean of all adjusted concentrations (for the given control or sample) obtained within the interpolation range of the standard curve. The mean absolute percentage of the relative error calculated from all standard points had to be 15.0% or less. Samples and controls concentrations are expressed as ELISA Laboratory Unit per milliliter (ELU/mL).
The measurement of neutralizing activity using PNA was performed by generating HIV-1 pseudovirions that express the SARS CoV-2 spike protein. The reporter pseudovirus is prepared by co-transfecting HEK293 producer cells with an HIV-1 genomic vector and a SARS CoV-2 envelope expression vector. Neutralizing antibody activity is measured by assessing the inhibition of luciferase activity in HEK293 target cells transiently expressing the ACE2 receptor following pre-incubation of the pseudovirions with the serum specimen. A serial dilution of test serum specimen is incubated with a reporter pseudovirus to generate an inhibition curve that enables the determination of an ID50 for each sample. Luminescence as an index of capability of inhibiting the virus from replicating and thereby prevent the luciferase by samples was measured as relative luminescent unit (RLU). Acceptable limit of intra-assay and inter-assay precision was set <30% ID50 CV.
Detection limit for ELISA titer (EUL/ml) and neutralizing activity (ID50) was 50 and 40, respectively. Accordingly, a value of 25 (half the minimum required dilution) for ELISA and a value of 20 (half the minimum required dilution) for PNA were assigned to samples below the cutoff point.
Statistical Analyses
Frequency table number of specimens, percentage were calculated from the categorical data. Continuous variables were expressed as the mean, median, minimum/maximum, and interquartile range. Antibody titers and neutralizing activity were stratified by age, sex, and disease severity. The geometric mean and 95% confidence interval were calculated for both S-ELISA and PNA data from eligible participants. Data analysis was performed by EPS Corporation (Tokyo, Japan), by using SAS® 9.4 (SAS Institute Inc., Cary, NC, USA.)
Sample Size
In a similar study overseas [8], the correlation between the severity of COVID-19 and neutralizing antibody activities is being evaluated using 32 samples from non-hospitalized individuals and 40 samples from hospitalized individuals. In this study, the sample size of at least 50 samples from non-hospitalized individuals and at least 50 samples from hospitalized individuals were set based on the number of individuals who have recuperated from previous SARS-CoV-2 infection that could be accrued by December 31, 2021, the end date of the study period, using this overseas study report as a reference.
Results
Clinical Characteristics
Two hundred twenty-two patients were eligible. Of these, 72 patients were hospitalized, and 136 patients (61.3%) were male. The gender balance was similar in the non-hospitalized and hospitalized groups. The mean age of the entire cohort was 40.0 years, and the mean ages of the non-hospitalized and hospitalized groups were 36.6 and 47.1 years, respectively, suggesting that older patients were more likely to require hospitalization. Concerning the severity of SARS-CoV-2 infection, 8 patients (3.6%) were asymptomatic, 146 patients (65.8%) had mild symptoms, 39 patients (17.6%) had moderate I symptoms, and 29 patients (13.1%) had moderate II symptoms. The majority of non-hospitalized patients had mild symptoms (94.0%), whereas most hospitalized patients had moderate I or moderate II severity (52.8% and 40.3%, respectively; Table 1).

Table 1.
Patient characteristics.
| Non-hospitalized N = 150 n (%) |
Hospitalized N = 72 n (%) |
Total N = 222 n (%) |
|
|---|---|---|---|
| Sex | |||
| Male | 92 (61.3) | 44 (61.1) | 136 (61.3) |
| Female | 58 (38.7) | 28 (38.9) | 86 (38.7) |
| Age (years) | |||
| n | 150 | 72 | 222 |
| Mean (SD) | 36.6 (13.1) | 47.1 (11.7) | 40.0 (13.5) |
| Median | 33.0 | 49.0 | 40.0 |
| Min, max | 20, 78 | 20, 79 | 20, 79 |
| 20 to <40* | 92 (61.3) | 17 (23.6) | 109 (49.1) |
| 40 to <60 | 52 (34.7) | 47 (65.3) | 99 (44.6) |
| ≥60 | 6 (4.0) | 8 (11.1) | 14 (6.3) |
| Severity of SARS-CoV-2 infection | |||
| Asymptomatic | 8 (5.3) | 0 | 8 (3.6) |
| Mild | 141 (94.0) | 5 (6.9) | 146 (65.8) |
| Moderate I | 1 (0.7) | 38 (52.8) | 39 (17.6) |
| Moderate II | 0 | 29 (40.3) | 29 (13.1) |
| Severe | 0 | 0 | 0 |
*Age of 20 to <30: Total N=64 (57; non-hospitalized, 7: hospitalized).
Immunogenicity Assessments
As S-ELISA result was deemed invalid for one patient, the numbers of test results for S-ELISA and PNA were 221 and 222, respectively.
The geometric mean of anti-spike antibody titer and neutralizing activity were 1555 ELU/mL and 253 ID50 (the reciprocal serum dilution corresponding to 50% neutralization), respectively, for eligible patients (Table 2). There were no differences in either parameter according to sex. Both the anti-spike antibody titer and neutralizing activity were approximately 4-fold higher in hospitalized patients than in non-hospitalized patients, excluding patients older than 60 years. Both anti-spike antibody titer and neutralizing activity in the age group of ≥30 to <40 years was larger than that of other two groups. No distinct difference in anti-spike antibody titer was observed between hospitalized versus non-hospitalized patients in the age group of >60 years, but older hospitalized patients displayed relatively lower neutralizing activity. Both anti-spike antibody titer and neutralizing activity increased with disease severity. (Table 2).
Table 2.
Antibody titer and neutralizing activity stratified by patient characteristics between non-hospitalized and hospitalized patients.
Table 2.
Antibody titer and neutralizing activity stratified by patient characteristics between non-hospitalized and hospitalized patients.
| Antibody titer (ELU/mL): S-ELISA | Neutralizing activity (ID50): PNA | ||||||
|---|---|---|---|---|---|---|---|
| Non-Hospitalized | Hospitalized | Total | Non-Hospitalized | Hospitalized | Total | ||
| All | 941 | 4391 | 1555 | 166 | 607 | 253 | |
| [753, 1176] | [3052, 6317] | [1257, 1923] | [132, 209] | [415, 888] | [204, 313] | ||
| N = 149 | N = 72 | N = 221 | N = 150 | N = 72 | N = 222 | ||
| Gender | Male | 977 | 4062 | 1549.55 | 182 | 638 | 273 |
| [727, 1312] | [2449, 6737] | [1172, 2047] | [133, 247] | [384, 1059] | [206, 361] | ||
| N = 92 | N = 44 | N = 136 | N = 92 | N = 44 | N = 136 | ||
| Female | 886 | 4963 | 1563 | 144 | 562 | 224 | |
| [627, 1253] | [2923, 8425] | [1119, 2183] | [101, 204] | [306, 1030] | [161, 312] | ||
| N = 58 | N = 28 | N = 85 | N = 58 | N = 28 | N = 86 | ||
| Age | 20 to <40 | 881 | 2932 | 1065 | 150 | 375 | 173 |
| (years) | [696, 1117] | [1376, 6245] | [837, 1356] | [111, 202] | [172, 817] | [131, 229] | |
| N = 91 | N = 17 | N = 108 | N = 92 | N = 17 | N = 109 | ||
| 40 to <60 | 1050 | 6209 | 2442 | 199 | 886 | 405 | |
| [667, 1652] | [4173, 9240] | [1725, 3456] | [134, 295] | [561, 1399] | [291, 563] | ||
| N = 52 | N = 47 | N = 99 | N = 52 | N = 47 | N = 99 | ||
| ≥60 | 983 | 1353 | 1180 | 159 | 183 | 172 | |
| [80, 12015] | [228, 8006] | [339, 4099] | [24, 1032] | [52, 636] | [70, 423] | ||
| N = 6 | N = 8 | N = 14 | N = 6 | N = 8 | N = 14 | ||
| Severity | Asymptomatic | 319 | - | 319 | 105 | - | 105 |
| [116, 877] | - | [116, 877] | [31, 353] | - | [31, 353] | ||
| N = 8 | N = 0 | N = 8 | N = 8 | N = 0 | N = 8 | ||
| Mild | 992 | 4221 | 1043 | 169 | 610 | 176 | |
| [790, 1246] | [77, 229822] | [819, 1327] | [133, 214] | [8, 43608] N = 5 |
[137, 227] | ||
| N = 140 | N = 5 | N = 145 | N = 141 | - | N = 146 | ||
| Moderate I | 3421 | 3241 | 3245 | 591 | 521 | 523 | |
| - | [1877, 5595] | [1908, 5521] | - | [302, 899] | [308, 888] | ||
| N = 1 | N = 38 | N = 39 | N = 1 | N = 38 | N = 39 | ||
| Moderate II | - | 6582 | 6582 | - | 741 | 741 | |
| - | [4840, 8950] | [4840, 8950] | - | [484, 1132] | [484, 1132] | ||
| N = 0 | N = 29 | N = 29 | N = 0 | N = 29 | N = 29 | ||
| Antibody titer and neutralizing activity were expressed as the geometric mean.The 95% confidence interval is presented within brackets.One patient was excluded from the analysis because of an invalid ELISA result. | |||||||
Distribution of anti-spike antibody titers by each patient is shown in Figure 1A. Seven patients (3.4%) had antibody titer lower than the detection limit (1.7; log ELISA titer), in all of which neutralizing activity was blow the detection limit (1.6; log ID50), although Covid-19 had been confirmed by polymerase chain reaction or antigen test. Including these 7 patients, anti-spike antibody titers were low in 8 patients (3.6 %) (2< log ELISA titer), low medium in 21 patients (9.5%) (2≤ log ELISA titer <2.5), medium in 69 patients (31.2%) (2.5≤ log ELISA titer <3), and high-medium in 49 patients (22.2 %) (3≤ log ELISA titer <3.5), and high in 51 (23.1%) (log ELISA titer 3.5≤). 23 patients developed extremely high antibody titer (log ELISA titer <4). The gender of these 23 patients was 17 males and 6 females. Two aged patients (≥60 years) included in this population.
Figure 1.
Distributions of anti-spike antibody titers (A) and neutralizing antibody activity (B) by each patient. 7 patients had anti-spike antibody titers below the detection limit (1.7; log ELISA titer) and 26 patients had neutralizing antibody activity below the detection limit (1.6; log ID50). For convenience, the following criteria were applied for the levels of antibody activity and neutralizing antibody activity: low (logID50 or ELISA titer <2), low-medium (2≤ logID50 or ELISA titer <2.5), medium (2.5≤ logID50 or ELISA titre <3), high-medium (3≤ logID50 or ELISA titer <3.5), and high (logID50 or ELISA titer: 3.5≤).
Figure 1.
Distributions of anti-spike antibody titers (A) and neutralizing antibody activity (B) by each patient. 7 patients had anti-spike antibody titers below the detection limit (1.7; log ELISA titer) and 26 patients had neutralizing antibody activity below the detection limit (1.6; log ID50). For convenience, the following criteria were applied for the levels of antibody activity and neutralizing antibody activity: low (logID50 or ELISA titer <2), low-medium (2≤ logID50 or ELISA titer <2.5), medium (2.5≤ logID50 or ELISA titre <3), high-medium (3≤ logID50 or ELISA titer <3.5), and high (logID50 or ELISA titer: 3.5≤).

Distribution of neutralizing activity by ascending order is shown in Figure 1B. 26 patients had neutralizing activity lower than the detection limit (1.6; log ID50). Of these 26 patients, 16 patients (61.5%) were between 20 and 39 years of age. When this age group was further divided into two groups, 13/16 were include in the 20-29 age group, and 3/16 were included in the 30-39 age group. 6 were included in the 40-59 age group, and 4 in the over 60 years group. By severity, 2 patients were asymptomatic, 22 mild, and 2 moderate I. Antibody titers in this population was low in 8 patients including 7 patients with below detection limit of ELISA titer, low-medium in 12 patients (2≤ log ELISA titer <2.5) and medium in 6 patients (2.5≤ log ELISA titer <3).
Neutralizing activities were low in 39 patients (17.6 %) (logID50: 2<), low-medium in 69 patients (31.1%) (2≤ logID50 <2.5), medium in 46 patients (20.7%) (2.5≤ logID50 <3), and high-medium in 28 patients (13%) (3≤ logID50 <3.5), and high in 9 patients (4.1%) (logID50: 3.5≤). 4 of 5 patients who developed extremely high neutralizing activity (log ID50: <4) were male.
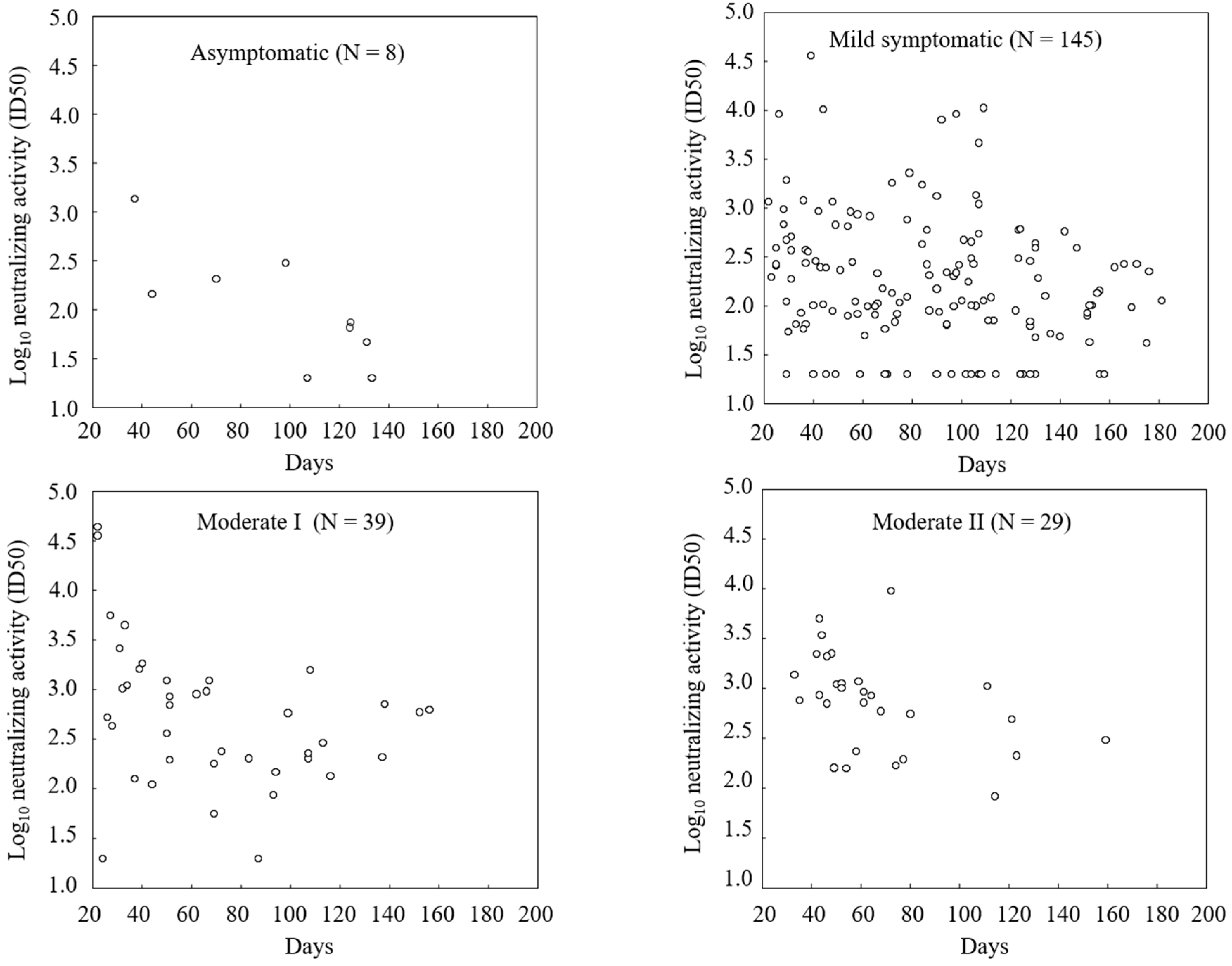
The anti-spike antibody titers and neutralizing activities displayed a good correlation in both the non-hospitalized and hospitalized groups, and correlation coefficient in all patients was 0.84 (Figure 2). Neutralizing activities gradually decreased over time after SARS-CoV-2 infection. In asymptomatic patients, serum neutralizing activity tended to disappear earlier, however there could not find clear relationship between severity of SARS-CoV-2 infection and the disappearance of antibody activities. Most patients with mild or moderate symptoms had sustained neutralizing activity up to 180 days after the SARS-CoV-2 infection (Figure 3).
Figure 2.
Relation between anti-spike antibody titer and neutralizing activity. Correlation coefficient was calculated excluding one patient with an invalid ELISA data.
Figure 2.
Relation between anti-spike antibody titer and neutralizing activity. Correlation coefficient was calculated excluding one patient with an invalid ELISA data.
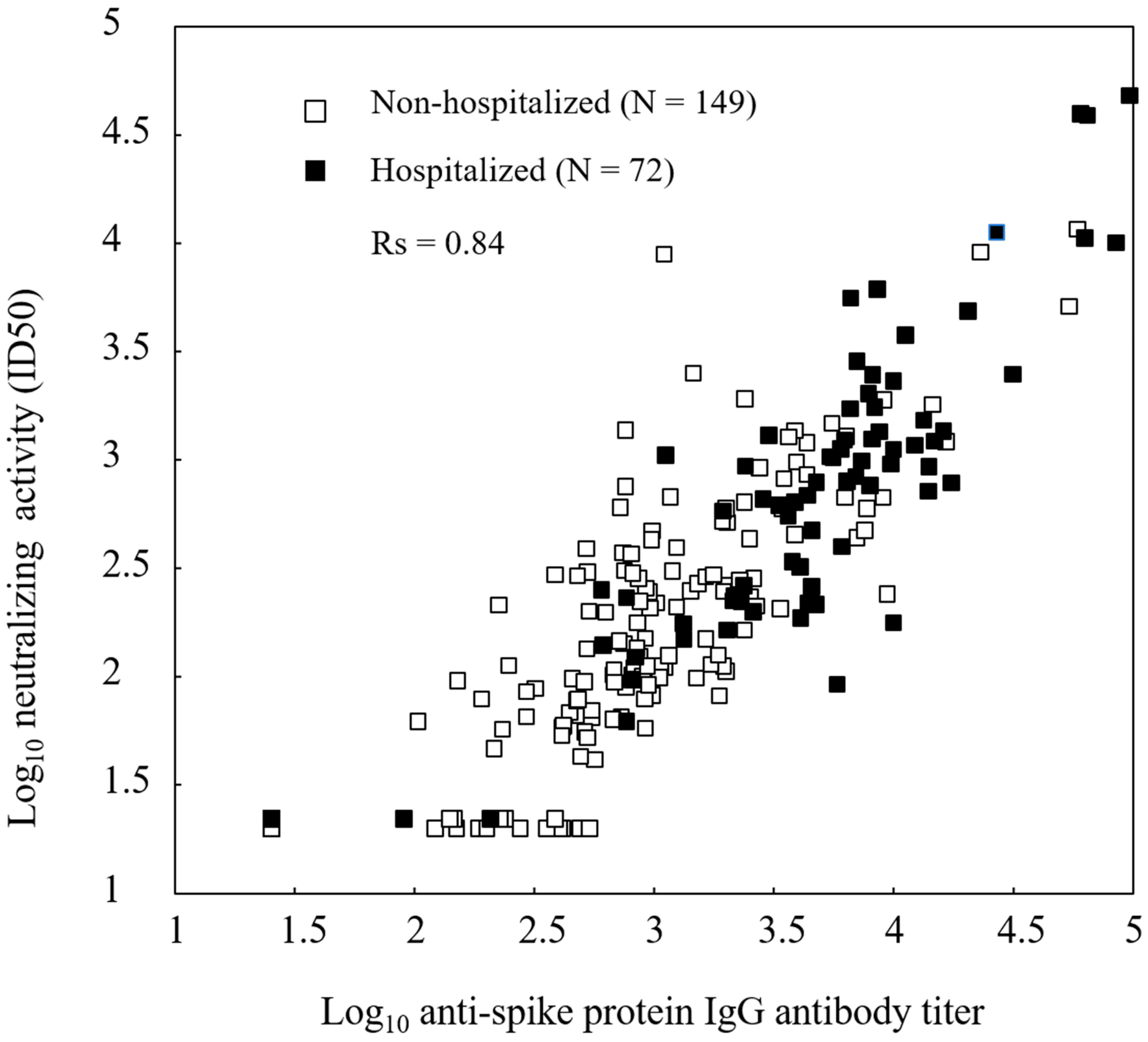
Figure 3.
Neutralizing activity at days after infection. X-axis: days after the diagnosis of Covid-19. Most patients with mild or moderate symptoms had sustained neutralizing activity up to 180 days after infection. There were 26 patients with neutralizing activity under detection limit, including 2 asymptomatic, 22 mild, and 2 moderate I cases.
Figure 3.
Neutralizing activity at days after infection. X-axis: days after the diagnosis of Covid-19. Most patients with mild or moderate symptoms had sustained neutralizing activity up to 180 days after infection. There were 26 patients with neutralizing activity under detection limit, including 2 asymptomatic, 22 mild, and 2 moderate I cases.
Discussion
In this cross-sectional study, we quantified anti-spike and neutralizing antibody levels in patients who contracted COVID-19 between January and September 2021. Accordingly, it is assumed that the dominant strains were the D614G variant from January to March, the alpha strain from April to June, and the delta strain from July to September [4]. In total, 96.5% (141 of 146) of patients with mild respiratory symptoms or high oxygen saturation did not require hospitalization, whereas 97% (38 of 39) of patients with moderate dyspnea or pneumonia required hospitalization, suggesting that medical care was provided appropriately during the pandemic in Japan.
It has been reported that male sex, older age, and hospitalization are associated with the anti-spike IgG response [9,10]. In the analysis stratified by age, antibody titers in our study were lower in patients aged 60 years and older, and antibody levels did not differ between hospitalized and non-hospitalized patients in this age group, illustrating that antibodies were not produced according to disease severity and suggesting that the insufficient immune response to new pathogens in older patients. Apart from this, age was identified as a negative independent variable for serum anti–SAR-CoV-2S antibody levels after immunization with mRNA-based COVID-19 vaccines based on data from more than 2000 people [11]. Anti-spike antibody titers and neutralizing activity did not differ according to sex in this study. This result was consistent with those reported by Trinite et al. [8], who found that the plateau of neutralizing activity was similar between men and women even though the maximum titer of neutralizing antibodies significantly differed. It is likely that there is not apparent gender difference in respect of antibody production [9,10]. However, Scully et al. is reporting that males are associated with a greater risk of more severe COVID-19 outcomes [12].
In this study, when patients with COVID-19 were classified by disease severity, antibody titers and neutralizing activity were low in asymptomatic and mildly ill patients, whereas they were high in patients with moderate disease severity. These results were consistent with those reports showing that the severely ill patients with COVID-19 have the higher anti-spike antibody levels, and the production of more potent neutralizing antibodies [8,13]. However, it is noteworthy that Trinité et. al., reported no correlation between neutralizing capacity and length of hospitalization, indicating the possibility that the presence of neutralizing antibodies is not a determinant for the disease resolution, i.e., a contradictory situation in which neutralizing activities are not associated with clinical benefit [8]. Furthermore, it is suggested that while antibody production plays an important role in the elimination of the SARS-CoV-2 virus, the well-balanced function of both CD4+ T cells essential for antibody production and memory B cell formation, and CD8+ T cells providing protection against antigens, is more important for preventing aggravation [6]
Our analysis illustrated that some patients have neutralizing activity of less than 1.6 log ID50 despite moderate antibody levels, suggestive of the production of non-neutralizing antibody as well as a risk of reinfection. The neutralizing activity of each IgG fraction and the amount of SARS-CoV-2–binding antibody in serum/plasma obtained at multiple time points were determined in 43 patients [14], and 16 patients with considerable antibody titers had no neutralizing activity during the observation periods. It is curious that the cohort with these characteristics mainly included patients with mild severity, and this finding was common to both studies. Further investigation regarding risk factors for the production of antibodies with insufficient activity is required in the future. Antibody level below the detection limit were observed in younger patients in our study. The reason why this type of patients was exclusively distributed in this group is uncertain. In general, if the innate immunity adequately and strongly functioned, in which in turn the virus could have been eliminated before production of antibody, and also functions for aggravation of infection. Moderbacher et al. proposed the important role of higher level of naïve T cells for eliminating virus in the young [6]. In addition, the importance of robust natural immune system has been pointed out, which may contribute to an asymptomatically recovery despite the low production of antibodies in children and youth [7,15].
Antibody titers in patients with moderate or severe disease persist for a relatively long period (up to 180 days). Previous reports in Japan also found that COVID-19 survivors had sustained neutralizing activity for approximately 6 or 12 months after infection [2,3]. How long the neutralizing activity of antibodies is maintained is important information for estimating the risk of re-infection. The antibody decay was analyzed by Khoury et al., and they extrapolated that the neutralizing activity would drop below the detection limit around 240 days after outbreak, and half-life was estimated to be approximately 90 days, of which the model assumed that the decay in neutralizing activity is the same regardless the initial starting antibody titers [16]. The data concerning the antibody titers and neutralizing activity necessary for preventing infection are are currently limited. However, after plasma antibodies from monkeys that had recovered from SARS-CoV-2 infection were transfused to other monkeys at various concentrations before challenge with SARS-CoV-2, the antibody titers required for protection, i.e., decreasing the amount of virus in the upper respiratory tract compared to that in the control group, was estimated at approximately 50 pseudovirus neutralizing antibody activity in blood before infection [17]. By utilizing the data from seven clinical trials for Covid-19 vaccine and one convalescent study, Khoury et al. is reporting the neutralizing activity which reduces half the chance of infection is equivalent to about 20% of the mean neutralizing activity of convalescent plasma based on a normally distributed model and about 30% by using a distribution-free approach [16].
The samples were cross-sectional, and the window of data collection was relatively tight. The sampled population is considered to represent a clinically diverse one, and its wide age range is representative of the blood donor population in a general clinical practice. However, this study had multiple limitations. Serum samples were not obtained from patients with severe symptoms in this study, and thus, we could not fully analyze the relationship between the levels and activity of antibodies or examine the time course of antibody activity across patients with COVID-19. The data released by the Japanese government from three different districts between January and February 2022 illustrated that the rate of severe disease among infected people with no history of vaccination remains low (less than 0.5% [145/34,136 patients]) [18]. This might partly support the plausibility of sampling bias in this analysis. In addition, this study contained fewer number of asymptomatic patients (n=8) as well as the elder patients (n=14). Furthermore, this study consisted of samples provided from the patients at a single and arbitrary point (pooled data), not from sequential sampling in each patient. In interpreting the results of this stratified analysis of antibody titers and neutralizing activities, it is important to note that time after infection, i.e., antibody decay, was not considered, therefore this could remain as a substantial bias. We could not also eliminate biases such as underlying factors, especially those affecting the immune system such as antibody production, as well as alternative confounding effects associated with the baseline characteristics used in this analysis and residual confounders.
Conclusions
Overall, this cross-sectional observational study revealed that the production of anti-spike antibody with neutralizing activity was sustained for more than 6 months in patients who were infected with SARS-CoV-2 variants such as the alpha and delta variants as well as variants carrying the D614G mutation, and also showed that there existed patients who had very low neutralizing activity particularly in young people, and those who had low neutralizing activity despite a certain level of antibody titers. The results of this analysis illustrate the importance of appropriately measuring neutralizing activity and provide useful information regarding management of COVID-19 vaccination.
Author Contributions
All authors meet the ICMJE criteria for authorship for this manuscript, take responsibility for the integrity of the work as a whole, and have given final approval for this version to be published. K Monzen, T Watanabe, T Okabe, and H Sekino contributed to the data acquisition and analysis. H Nakagami contributed to making manuscript. R Morishita contributed to the study design and protocol writing.
Funding
This study has been supported by a Project Promoting Support for Drug Discovery grant (JP21nf0101623h0002) from the Japan Agency for Medical Research and Development.
Acknowledgments
We thank Medical Grown Co., Ltd. for writing and editorial support.
Conflicts of interest
The authors declare no conflict of interest in conducting this project.
Ethics Statement
In the case study subjects visited the study institution for samples to be collected, written consent was obtained using the specified informed consent form. In the case archival samples retained at the study institution was used, the sample provider was notified through an opt-out procedure and, if an intention to withdraw consent was expressed, the samples was not utilized. The study was conducted according to the "Helsinki Declaration of the World Medical Congress". For this study, approval was obtained from the institutional review board of the representative study institution (Sekino Hospital, Tokyo), prior to the conduct of this study, and then an application for approval was submitted to the institutional review board of each study institution (approval No. and date: 20210618-22S372 at IRB No. 14000050 on July 16, 2001 and approval No. and date: 2102 at Sekino Hospital IRB on July 16, 2001). After approval is obtained at each study institution, this study was sequentially started. The outline of this study was registered into the public database (UMIN-CTR) established by the National University Hospital Council of Japan under the number UMIN000044638, and disclosed to the public prior to the start of conduct.
Abbreviations
| 50% inhibitory dilution | ID50 |
| Confidence interval | CI |
| Coronavirus disease 2019 | COVID-19 |
| PhenoSense SARS-CoV-2 neutralizing antibody assay | PNA |
| Severe acute respiratory syndrome coronavirus 2 | SARS-CoV-2 |
| SARS-COV-2 spike enzyme-linked immunosorbent assay | S-ELISA |
| University Hospital Medical Information Network | UMIN |
References
- Zhu N, Zhang D, Wang W, Li X, Yang B, Song J, Zhao X, Huang B, Shi W, Lu R, Niu P, Zhan F, Ma X, Wang D, Xu W, Wu G, Gao GF, Tan W; China Novel Coronavirus Investigating and Research Team. A novel coronavirus from patients with pneumonia in China, 2019. China novel coronavirus investigating and research team. N Engl J Med. 2020;382(8):727-733. doi: 10.1056/NEJMoa2001017. [CrossRef]
- Goto A, Go H, Miyakawa K, Yamaoka Y, Ohtake N, Kubo S, Jeremiah SS, Mihara T, Senuki K, Miyazaki T, Ikeda S, Ogura T, Kato H, Matsuba I, Sanno N, Miyakawa M, Ozaki H, Kikuoka M, Ohashi Y, Ryo A, Yamanaka T. Sustained neutralizing antibodies 6 months following infection in 376 Japanese COVID-19 survivors. Front Microbiol. 2021;12:661187. doi: 10.3389/fmicb.2021.661187. [CrossRef]
- Miyakawa K, Kubo S, Stanleyraj Jeremiah S, Go H, Yamaoka Y, Ohtake N, Kato H, Ikeda S, Mihara T, Matsuba I, Sanno N, Miyakawa M, Shinkai M, Miyazaki T, Ogura T, Ito S, Kaneko T, Yamamoto K, Goto A, Ryo A. Persistence of Robust Humoral Immune Response in Coronavirus Disease 2019 Convalescent Individuals Over 12 Months After Infection. Open Forum Infect Dis. 2021;9(2):ofab626. doi: 10.1093/ofid/ofab626. [CrossRef]
- Ode H, Nakata Y, Nagashima M, Hayashi M, Yamazaki T, Asakura H, Suzuki J, Kubota M, Matsuoka K, Matsuda M, Mori M, Sugimoto A, Imahashi M, Yokomaku Y, Sadamasu K, Iwatani Y. Molecular epidemiological features of SARS-CoV-2 in Japan, 2020-1. Virus Evol. 2022;8(1):veac034. doi: 10.1093/ve/veac034. [CrossRef]
- Seow J, Graham C, Merrick B, Acors S, Pickering S, Steel KJA, Hemmings O, O’Byrne A, Kouphou N, Galao RP, Betancor G, Wilson HD, Signell AW, Winstone H, Kerridge C, Huettner I, Jimenez-Guardeño JM, Lista MJ, Temperton N, Snell LB, Bisnauthsing K, Moore A, Green A, Martinez L, Stokes B, Honey J, Izquierdo-Barras A, Arbane G, Patel A, Tan MKI, O’Connell L, O’Hara G, MacMahon E, Douthwaite S, Nebbia G, Batra R, Martinez-Nunez R, Shankar-Hari M, Edgeworth JD, Neil SJD, Malim MH, Doores KJ. Longitudinal observation and decline of neutralizing antibody responses in the three months following SARS-CoV-2 infection in humans. Nat Microbiol. 2020 Dec;5(12):1598-1607. doi: 10.1038/s41564-020-00813-8. Epub 2020 Oct 26. PMID: 33106674; PMCID: PMC7610833. [CrossRef]
- Rydyznski Moderbacher C, Ramirez SI, Dan JM, Grifoni A, Hastie KM, Weiskopf D, et al. Antigen-specific adaptive immunity to SARS-CoV-2 in acute COVID-19 and associations with age and disease severity. Cell. 2020;183(4):996-1012.e19. doi: 10.1016/j.cell.2020.09.038. [CrossRef]
- Weisberg SP, Connors TJ, Zhu Y, Baldwin MR, Lin WH, Wontakal S, Szabo PA, Wells SB, Dogra P, Gray J, Idzikowski E, Stelitano D, Bovier FT, Davis-Porada J, Matsumoto R, Poon MML, Chait M, Mathieu C, Horvat B, Decimo D, Hudson KE, Zotti FD, Bitan ZC, La Carpia F, Ferrara SA, Mace E, Milner J, Moscona A, Hod E, Porotto M, Farber DL. Distinct antibody responses to SARS-CoV-2 in children and adults across the COVID-19 clinical spectrum. Nat Immunol. 2021 Jan;22(1):25-31. doi: 10.1038/s41590-020-00826-9. Epub 2020 Nov 5. PMID: 33154590; PMCID: PMC8136619. [CrossRef]
- Trinité B, Tarrés-Freixas F, Rodon J, Pradenas E, Urrea V, Marfil S, Rodríguez de la Concepción ML, Ávila-Nieto C, Aguilar-Gurrieri C, Barajas A, Ortiz R, Paredes R, Mateu L, Valencia A, Guallar V, Ruiz L, Grau E, Massanella M, Puig J, Chamorro A, Izquierdo-Useros N, Segalés J, Clotet B, Carrillo J, Vergara-Alert J, Blanco J. SARS-CoV-2 infection elicits a rapid neutralizing antibody response that correlates with disease severity. Sci Rep. 2021;11(1):2608. doi: 10.1038/s41598-021-81862-9. [CrossRef]
- Klein SL, Pekosz A, Park HS, Ursin RL, Shapiro JR, Benner SE, Littlefield K, Kumar S, Naik HM, Betenbaugh MJ, Shrestha R, Wu AA, Hughes RM, Burgess I, Caturegli P, Laeyendecker O, Quinn TC, Sullivan D, Shoham S, Redd AD, Bloch EM, Casadevall A, Tobian AA. Sex, age, and hospitalization drive antibody responses in a COVID-19 convalescent plasma donor population. Clin Invest. 2020;130(11):6141-6150. doi: 10.1172/JCI142004. [CrossRef]
- Mehew J, Johnson R, Roberts D, Harvala H. Convalescent plasma for COVID-19: male gender, older age and hospitalisation associated with high neutralising antibody levels, England. Euro Surveill. 2020;25(45):2001754. doi: 10.2807/1560-7917.ES.2020.25.45.2001754. [CrossRef]
- Kageyama T, Ikeda K, Tanaka S, Taniguchi T, Igari H, Onouchi Y, Kaneda A, Matsushita K, Hanaoka H, Nakada TA, Ohtori S, Yoshino I, Matsubara H, Nakayama T, Yokote K, Nakajima H. Antibody responses to BNT162b2 mRNA COVID-19 vaccine in 2,015 healthcare workers in a single tertiary referral hospital in Japan. Clin Microbiol Infect. 2021;27(12):1861.e1-1861.e5. doi: 10.1016/j.cmi.2021.07.042. [CrossRef]
- Scully EP, Haverfield J, Ursin RL, Tannenbaum C, Klein SL. Considering how biological sex impacts immune responses and COVID-19 outcomes. Nat Rev Immunol. 2020;20(7):442-447. doi: 10.1038/s41577-020-0348-8. [CrossRef]
- Garcia-Beltran WF, Lam EC, Astudillo MG, Yang D, Miller TE, Feldman J, Hauser BM, Caradonna TM, Clayton KL, Nitido AD, Murali MR, Alter G, Charles RC, Dighe A, Branda JA, Lennerz JK, Lingwood D, Schmidt AG, Iafrate AJ, Balazs AB. COVID-19-neutralizing antibodies predict disease severity and survival. Cell. 2021;184(2):476-488.e11. doi: 10.1016/j.cell.2020.12.015. [CrossRef]
- Maeda K, Higashi-Kuwata N, Kinoshita N, Kutsuna S, Tsuchiya K, Hattori SI, Matsuda K, Takamatsu Y, Gatanaga H, Oka S, Sugiyama H, Ohmagari N, Mitsuya H. Neutralization of SARS-CoV-2 with IgG from COVID-19-convalescent plasma. Sci Rep. 2021;11(1):5563. doi: 10.1038/s41598-021-84733-5. [CrossRef]
- Pierce CA, Preston-Hurlburt P, Dai Y, Aschner CB, Cheshenko N, Galen B, Garforth SJ, Herrera NG, Jangra RK, Morano NC, Orner E, Sy S, Chandran K, Dziura J, Almo SC, Ring A, Keller MJ, Herold KC, Herold BC. Immune responses to SARS-CoV-2 infection in hospitalized pediatric and adult patients. Sci Transl Med. 2020 Oct 7;12(564):eabd5487. doi: 10.1126/scitranslmed.abd5487. Epub 2020 Sep 21. PMID: 32958614; PMCID: PMC7658796. [CrossRef]
- Khoury DS, Cromer D, Reynaldi A, Schlub TE, Wheatley AK, Juno JA, Subbarao K, Kent SJ, Triccas JA, Davenport MP. Neutralizing antibody levels are highly predictive of immune protection from symptomatic SARS-CoV-2 infection. Nat Med. 2021 Jul;27(7):1205-1211. doi: 10.1038/s41591-021-01377-8. [CrossRef]
- McMahan K, Yu J, Mercado NB, Loos C, Tostanoski LH, Chandrashekar A, , Liu J, Peter L, Atyeo C, Zhu A, Bondzie EA, Dagotto G, Gebre MS, Jacob-Dolan C, Li Z, Nampanya F, Patel S, Pessaint L, Van Ry A, Blade K, Yalley-Ogunro J, Cabus M, Brown R, Cook A, Teow E, Andersen H, Lewis MG, Lauffenburger DA, Alter G, Barouch DH. Correlates of protection against SARS-CoV-2 in rhesus macaques. Nature. 2021;590(7847):630-634. doi: 10.1038/s41586-020-03041-6. [CrossRef]
- Preliminary data reported at the New Coronavirus Infectious Disease Control Advisory Board held at the Ministry of Health, Labor and Welfare on April 13, 2022 (in Japanese). Available from: https://www.mhlw.go.jp/content/10900000/000929082.pdf.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



