
Submitted:
31 July 2023
Posted:
01 August 2023
You are already at the latest version
Abstract
With an increasing aging population worldwide, the concept of multimorbidity has attracted growing interest over recent years, especially in frailty, which leads to progressive multisystem decline and increased adverse clinical outcomes. The relative contribution of multiple disorders to overall frailty index in older populations has not been established so far. This study aimed to assess the association between the Vulnerable Elders Survey-13 (VES-13) score, which is acknowledged to be one of the most widely used measures of frailty, and the most common ac-companying diseases among hospitalized adults aged 60 years old and more. 2860 participants with an average age of 83 years were included in this study. Multiple logistic regression with adjustment for age and nutritional status was used to assess the independent impact of every particular disease on vulnerability. Diabetes mellitus type 2, coronary artery disease, atrial fibrillation, heart failure, chronic kidney disease, osteoarthritis, fractures, eyes disorders, depression, dementia, pres-sure ulcers, and urinary incontinence were associated with higher scores of VES-13. Hospital admission of older subjects with those conditions should primarily draw attention to the risk of functional decline and while qualifying older patients for further treatment, particularly in surgery and oncology. At the same time, lipid disorders, gastrointestinal diseases, higher body mass index and albumins level were related to lower risk of being vulnerable, what may be attributed to younger age and better nu-tritional status of those patients.
Keywords:
VES-13
; frailty
; multimorbidity
; cardiovascular diseases
; diabetes
1. Introduction
The global population is aging, and this demographic shift poses a significant challenge for healthcare systems worldwide. Older adults are more likely to develop multiple chronic conditions which can increase their risk of functional decline and death.
To address this challenge, healthcare professionals need accurate tools to predict the risk of functional decline and death in older patients. One of the tools is the Vulnerable Elders Survey-13 (VES-13) which is a brief, self-administered questionnaire. It assesses various domains of health, including activities of daily living, physical function, self-rated health, and it is one of the most widely used measures of frailty [1,2].
Research shows that VES-13 is a useful tool for identifying older adults with limited life expectancy [3]. Nevertheless, though VES-13 was developed for 2-year estimation of functional decline and mortality risks, it might be useful in 5-year prediction period as well [4]. High scores of VES-13 are associated with lower quality of life. Silva et al. reported that VES-13 shows 84% sensitivity and 98.2% negative predictive value while testing the quality of life in older individuals. Also, according to this study, VES-13 might help to determine which patients require comprehensive geriatric assessment [5].
There are many publications of VES-13 usage in oncology. VES-13 scale showed prominent level of reliability and operability in patients with advanced castration-resistant prostate cancer [6], gastrointestinal cancer [7], and gynecological malignancies [8]. Recent research reported that vulnerability predicts mortality better than a diagnosis of prostate cancer among older men [9]. Besides that, VES-13 might be useful to assess older oncological patients who are at risk of chemotherapy toxicity and help with choosing a method of treatment [8,10].
An interesting study showed that VES-13 might be useful in the preoperative identification of frailty and vulnerability and in assistance with perioperative decision-making in geriatric patients. VES-13 scores were correlated to hospital length of stay, post-anesthesia care unit stay, altered mental status, and morbidity [11]. In older adults with traumatic injury, each additional VES-13 point was associated with greater risk of complication or death [12]. In patients 60 years and older who were hospitalized with COVID-19 infection, VES-13 was performed to estimate the risks of in-hospital mortality and need for invasive mechanical ventilation. According to research, patients classified as extremely vulnerable (8-10 points in VES-13 score), and male sex were strongly and independently associated with a higher relative risk of those outcomes [13].
Cardiometabolic diseases remain in the leading position in causes of death and disabilities, especially in older adults [14]. Coronary artery disease (CAD) and stroke hold the first two positions in the structure of mortality, and second and third place as causes of disability. Diabetes mellitus type 2 (DM2) is in the rank of the first ten causes both in mortality and disability structure. A prospective observational cohort study was performed in patients hospitalized with acute coronary syndrome and/or decompensated heart failure (HF). High prevalence of vulnerable patients was found (54%) and vulnerability was associated with increased use of healthcare services, including a greater number of clinic visits, emergency room visits and hospitalizations [15]. Another research found that 44.4% of the patients aged 65 years old or more that were hospitalized for acute coronary syndromes and/or acute decompensated HF were vulnerable at baseline and 34.4% were vulnerable at 90 days after hospital discharge [16].
Interestingly, there is a relative paucity of data on how cardiometabolic disorders may contribute to frailty, preceding subsequent disability, institutionalization and death. Identifying the diseases that are most strongly connected with frailty is important for healthcare professionals as it can develop targeted interventions to improve patients’ outcomes. Although VES-13 has been validated as a useful tool for predicting mortality and functional decline, it is not entirely clear on how each disease impacts vulnerability. While some data was found in fields of oncology and surgery, there is a gap of knowledge in the cardiometabolic diseases’ impact on VES-13 and frailty. Therefore, in the present study, we tried to identify which chronic disorders of geriatric population are associated with vulnerability assessed by VES-13, focusing on cardiometabolic diseases.
2. Materials and Methods
2.1 Patients
For this study, patients were recruited from January 2012 to December 2019 at Central Veterans Hospital in Lodz, Poland. During 2020-2022 the department served partially as a Covid-19 ward. All 3382 older patients that were admitted to the Geriatric department during 2012-2019 were screened. The total number of individuals was selected with the following inclusion criteria: admission into the department, age of 60 years old or more and filling out the VES-13 scale. After screening, 2860 patients (2036 women and 824 men) met the inclusion criteria and were enrolled in the analysis.
2.2 Anamnesis
The presence of arterial hypertension (HT), DM2, lipid disorders, current or previous stroke, CAD, current or previous myocardial infarction (MI), atrial fibrillation (AF), chronic HF, chronic kidney disease (CKD), obstructive lung diseases (chronic obstructive pulmonary disease (COPD) and asthma), osteoarthritis (OA), osteoporosis, current or previous fractures, gastrointestinal diseases (chronic gastritis, gastrointestinal ulcer), neoplastic diseases, eyes disorders (glaucoma, cataract), depression, dementia, pressure ulcers (PU), and urinary incontinence (UI) was scrutinized from the patients’ medical histories.
2.3 Measurements
VES-13 scale in the Polish version [17] was completed with all patients. The score ranges from 0 to 10, with higher scores indicating a higher risk of functional decline and death. According to research [1] score of more than 3 points was associated with four times higher risk of death or functional decline when compared to elders scoring 3 or less. Taking that into consideration, cutoff point of 3 points was suggested by authors.
Body mass index (BMI) was calculated by dividing the weight (in kilograms) by height squared (in meters). CKD was defined as a glomerular filtration rate (GFR) lower than 60 mL/min/1.73m2 according to BIS1 formula [18]. The presence of depression was assessed using the Geriatric Depression Scale [19], where a score of 5 or higher indicates the presence of depression. Dementia was diagnosed based on the results of the Mini-Mental State Examination, where a score of less than 24 points indicates the presence of dementia [20]. Albumins concentration was measured in g/l, using a 5-Diff Sysmex XS-1000i hematological analyzer (Sysmex, Kobe, Japan).
2.3 Statistical analysis
The normality of distribution was verified using the Shapiro-Wilk test. As several variables were not normally distributed, data have been presented both as mean ± standard deviation and median (interquartile differences from the first (25%) to the third (75%)). The qualitative variables such as sex and presence of disease were presented as raw numbers and percent of the group. Qualitative variables were compared using Chi-square test, quantitative variables - with the Mann-Whitney U-test. Pearson correlation coefficients were used to calculate the relationship between variables. After dichotomization of VES-13 with cutoff point set at 3 points, the multivariate logistic regression was performed. Statistical significance was set at p≤0.05. Statistical analysis was performed using Statistica 13.1.
2.4 Ethical consideration
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Ethics Committee of the Medical University of Lodz (approval number: RNN/68/23/KE; date of approval: 18.04.2023).
3. Results
The median age was 83 (77-87) years for both sexes. Table 1 shows the characteristics of 2860 patients according to sex. There was no significant difference between men and women in age, BMI, the prevalence of HT, stroke, CAD, HF, CKD, gastrointestinal, neoplastic diseases, eyes disorders, dementia, and PU. Men had higher body mass and the prevalence of DM2, MI, AF, and obstructive lung diseases. At the same time, women had significantly higher levels of albumins, more points in VES-13 scale, higher prevalence of lipid disorders, OA, osteoporosis, fractures, depression, and UI.
The comparison of VES-13 results between participants with and without particular disease is presented in Table 2. For obstructive lung diseases, osteoarthritis and eyes disorders, there were no significant differences in VES-13 scores among patients with and without those conditions. Women with HT, DM2 and MI, and men with UI had higher scores of VES-13 as compared to their peers without the disease.
For stroke, CAD, AF, HF, CKD, fractures, depression, dementia, and PU, presence of disease was associated with significantly higher scores of VES-13 in both sexes. At the same time, patients with lipid disorders or gastrointestinal diseases in both sexes, and women with osteoporosis or neoplastic diseases had lower VES-13 results compared to patients without those conditions.
Linear correlation was performed for age and VES-13 with R=0.587 (p<0.0001), BMI and VES-13 with R=-0.11 (p<0.0001), albumins and VES-13 with inverse correlation, R=-0.37 (p<0.0001).
Additional bivariate analyses were performed between the presence of diseases and age (Table 3). The patients presenting with diseases such as HT (women), stroke (women), CAD, MI, AF, HF, CKD, osteoporosis (men), fractures, eyes disorders (men), dementia and PU were significantly older, whereas the patients with DM2 (men), lipid disorders, osteoporosis (women) and gastrointestinal diseases (women) were significantly younger in comparison to those without disease.
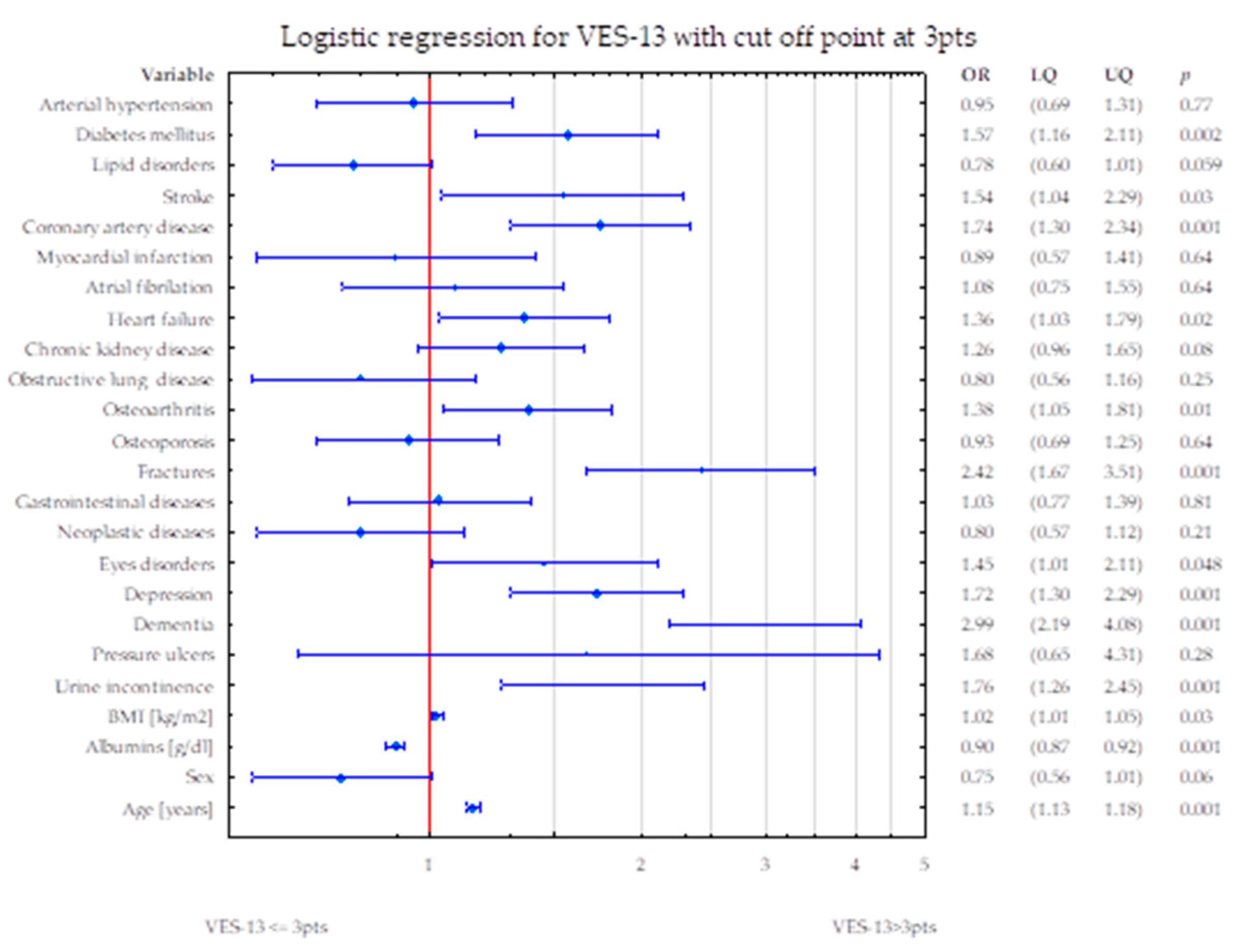
To assess the potential influence of diseases on VES-13 simultaneously, two statistical models were constructed. Firstly, with sex and BMI and secondly, with age and albumins level. In the first model, DM2, CAD, AF, HF, CKD, OA, fractures, eyes disorders, depression, dementia, PU, and UI were related to higher values of VES-13 (increased odds ratio for risk of death and disability). Lipid disorders, gastrointestinal diseases and higher BMI were related to lower values of VES-13 (Figure 1).
In the second model, DM2, stroke, CAD, HF, CKD, OA, fractures, eyes disorders, depression, dementia, UI and age were related to higher values of VES-13 (increased odds ratio for risk of death and disability). Higher albumins level was related to lower values of VES-13.
Figure 2.
shows the simultaneous statistical impact of concomitant diseases, BMI, sex, age and albumins level on VES-13 scores. DM2, stroke, CAD, HF, CKD, OA, fractures, eyes disorders, depression, dementia, and UI were related to higher values of VES-13 (increased odds ratio for risk of death and disability). Higher albumins level was related to lower values of VES-13.
Figure 2.
shows the simultaneous statistical impact of concomitant diseases, BMI, sex, age and albumins level on VES-13 scores. DM2, stroke, CAD, HF, CKD, OA, fractures, eyes disorders, depression, dementia, and UI were related to higher values of VES-13 (increased odds ratio for risk of death and disability). Higher albumins level was related to lower values of VES-13.
4. Discussion
To the best of our knowledge, this is the first paper presenting the association between a wide range of the most common chronic disorders and vulnerability assessed by VES-13 in a large, hospitalized geriatric population. Simultaneous assessment of all major concomitant disorders with sex and BMI, revealed some diseases independently related to vulnerability: several cardiometabolic conditions, CKD, OA, fractures, eyes disorders, depression, dementia, PU and UI. Interestingly, lipid disorders, gastrointestinal diseases and higher BMI were related to lower vulnerability – this may be attributed to lower age of patients presenting these conditions. In a fully adjusted model, after inclusion of age and albumins representing nutritional state, the statistical impact of several conditions became not evident. Nevertheless, DM2, current or past stroke, CAD, HF, OA, fractures, eyes disorders, depression, dementia, and UI remained associated with vulnerability status of the patients.
Cardiometabolic disorders
The majority of cardiometabolic conditions were related to higher vulnerability. DM2, current or past stroke, CAD and HF retained their contribution to vulnerability in fully adjusted model.
Our results are consistent with the data showing that hypertensive patients were more often frail compared to robust [21], although abovementioned study did not use VES-13 but the FRAIL scale. There are also recommendations discussing the perspective of treatment for vulnerable subjects with HT [22,23,24]. While there is not a large body of research examining the relationship between HT, gender, and VES-13, we may find some evidence suggesting that hypertensive women may be at greater risk for functional decline than men [25]. Likewise, we found that women with HT had higher VES-13 score than women without HT. At the same time, there were no significant differences in VES-13 results in men with or without HT.
In the presently available literature, there are no studies that have examined the association between VES-13 scores and history of stroke. However, frailty increases the risk of stroke and mortality in patients with AF [26], promotes increased stroke complications, poorer recovery, and weaker response to treatment [15,27]. In our group, patients with current or previous stroke had significantly higher VES-13 results also in fully adjusted multivariate model.
According to our data, patients with CAD had significantly higher results in VES-13 scores in both sexes. When using CAD and MI in multiple regression, only CAD was selected as a factor associated with VES-13. Systematic review reported the bidirectional association between frailty and cardiovascular disease [28]. The study of Purser et al. demonstrates that frailty, measured by the gait speed test, was the strongest predictor of mortality in a population with CAD [29].
AF is strongly related to HT and stroke. Our data show that AF is related to vulnerability in both bivariate association and multivariate model. Frailty deteriorates clinical management of AF and increases the risk of adverse outcomes, such as stroke or bleeding [30,31]. Frail AF patients have increased risk of death, ischemic stroke, and bleeding, and thus demand holistic and person-tailored approach to their care [32].
Previous research reported that HF is independently associated with increased vulnerability. Both conditions are inseparably related to sarcopenia, inflammation, global dysfunction and independently increase the risk of each other [15,33]. It is consistent with our data - patients with HF presented an almost doubled risk of increased VES-13 scores. In available literature, there is some information about the sex-heterogeneous pattern of frailty occurrence, especially in coexistence with other disorders like HF [34], stroke, DM2, CKD, dementia or OA [35]. These sex differences are also visible in our data.
DM2 is associated with an accelerated aging process that manifests as the premature onset of geriatric syndromes, also frailty. Progressive muscle and nerve dysfunction, deterioration of cardiometabolic status and physical function loss caused by diabetes mellitus inevitably led to the development of frailty [36,37,38]. This conform with our finding that DM2 is an independent predictor of higher values of VES-13, also in adjusted multivariate models. Pre-frailty and frailty are linked to increased morbidity and mortality, as well as higher healthcare utilization, in individuals with DM2 [39].
Unlike other cardiometabolic conditions, lipid disorders were related to lower levels of VES-13. According to logistic regression, the risk of elevated VES-13 is 42% lower among hyperlipidemic subjects. No research comparing VES-13 scale with lipid disorders was found in available literature. The above-mentioned relation may be the effect of two factors. Our subjects with lipid disorders were significantly younger. On the other hand, frailty is inseparably linked with malnutrition, which is in strong reverse relation with lipid disorders.
Similar interpretation may be put forward for BMI association to VES-13. It is consistent with the study, where normal- or underweight frail older participants have a poorer 3-year survival rate [40]. Jayanama et al. have found that being overweight is a protective factor against mortality in moderately/severely frail people and obesity grade 1 may be protective for mortality for people with at least mild level of frailty [41]. The abovementioned papers are in line with our results that higher BMI may be an independent protective factor for low results of VES-13. On the other hand, some studies did not find a relationship between BMI and frailty [42].
Osteoarthritis, osteoporosis and fractures
Subjects with rheumatoid arthritis and OA are more likely to have or develop frailty [43]. Frailty may hinder the self-repair of joint structure [44], reversely, presence of OA leads to functional capacity decline [45]. In addition to that, chronic pain caused by OA affects the degree of frailty [46]. Currently available literature does not provide any records referring to OA and VES-13. Our data revealed that there are no statistically significant differences observed in the levels of VES-13 among individuals with OA and those without. However, logistic regression indicates that presence of OA is linked with 53% and 38% (fully adjusted model) higher risk of elevated results of VES-13.
Our data shows no association between VES-13 and osteoporosis in multivariate logistic regression. A prospective cohort study by Sternberg et al. indicated that frailty status as defined by the VES-13 predicts a decrease in bone mineral density (BMD) after 1 year of follow-up [47]. In research with 6 years follow-up, the difference in calcaneal BMD of 1.4 T-score units between subjects with highest and lowest frailty scores corresponded to 2-3 times higher risk of fracture, even after adjusting for age, weight, sex, and race [48].
With the growing number of older subjects in society, the complication associated with fractures will continue to increase [49]. In our study, the presence of current or previous fracture was significantly associated with elevated VES-13 (OR 2.15) which is concordant with previous reports. According to Min et al., in hospitalized older patients with traumatic injury, each additional VES-13 point was associated with increased risk of complications or death [12]. Among traumatic patients, increased frailty scores were independently connected with increased mortality [50], risk of complications and prolonged hospitalizations [51].
Depression, dementia, pressure ulcers and urinary incontinence
All these conditions are inter-related and closely associated with advanced age. Vulnerability is strongly associated with the presence of depressive symptoms [52]. Furthermore, some scientists indicate a reciprocal interaction between depression and frailty [53,54]. It is consistent with our findings that patients with depression had significantly worse scores of VES-13, also after full adjustment in multivariate model.
Dementia is inseparably connected with frailty [55]. Each additional point of the VES-13 refers to a worse outcome in patients with dementia [4]. Our results are fully in line with the abovementioned papers. Elderly with dementia had significantly higher scores of VES-13. In logistic regression, dementia influenced the level of VES-13 the most out of all studied disorders with OR = 4.96. Accordingly, cognitive frailty becomes a newly acknowledged dimension of this geriatric syndrome [56,57].
Age-related skin changes, comorbidities, polypharmacy, reduced mobility, inadequate nutrition and hydration, and continence issues strictly lead to development of PU [58]. This increased vulnerability is present particularly among the physically limited or bedridden older subjects [59]. In our study, PU were significantly associated with worse VES-13 with OR of 2.51.
UI is twice as common in older people with frailty in comparison to those without [60]. UI is also a predictor of higher mortality rates, particularly in the geriatric population [61]. Currently available literature does not provide the works investigating the association between VES-13 scores and UI. In our study, a multivariate analysis showed a 79% higher risk of increased VES-13 scores among patients with UI, being concordant with available knowledge in that field.
Other chronic conditions
According to the systematic review referring to CKD and frailty [62] the incidence of frailty increases with reduced GFR. It is consistent with our analyses, that patients with GFR below 60 ml/min/m2 had 2.69-fold higher risk of increased score of VES-13. Frailty is highly prevalent and connected with adverse outcomes of CKD mortality and end-stage kidney disease [31].
So far, no study has initiated discussion on obstructive lung diseases and VES-13. Frailty, defined by the Fried criteria, was associated with higher severity of airflow limitation, dyspnea, and more frequent exacerbations in the group of 2.142 participants [63]. Another work has presented that frailty phenotype is associated with an increased risk of non-COPD hospitalizations [64,65], prolongation of hospital stays, worse in-hospital mortality, and decreased activity of daily living at discharge. [66]. Yet, our research showed no significant difference in VES-13 levels in patients with COPD. This may relate to lower prevalence of this chronic disorder in comparison with other diseases.
In older adults with gastrointestinal diseases undergoing abdominal surgery, preoperative frailty was associated with postoperative complication incidence and longer hospital stays [67]. It stands in contradiction with our data. Our patients with gastrointestinal diseases had significantly better results in VES-13 scale. Gastrointestinal disorders are linked with malnutrition and indirectly with frailty. This contradiction may be at least partially explained by the fact that our hospitalized women with this type of disorders were significantly younger.
The presently available literature about VES-13 in the majority refers to neoplastic diseases. According to some researchers, VES-13 is a feasible tool for predicting survival and qualifying for oncological treatment [10,64,65,68,69]. In our results, neoplastic diseases had no impact on VES-13 in multivariate design. This contradiction may be explained by the relatively low prevalence of those disorders in our population and by the fact that we enrolled both past and present oncological problems. Subjects successfully treated from neoplasms often present greater health awareness and better functional outcomes.
Our initial analysis did not reveal any significant differences in VES-13 scores between patients with and without eyes disorders. However, a subsequent logistic regression analysis demonstrated a significant association between the presence of eyes disorders and higher VES-13 scores, with an odds ratio of 1.61. We did not find any publications connected with VES-13 and eyes disorders. However, according to some works, frailty itself is associated with vision impairment [70,71,72].
According to previous research, scores of two widely used nutritional scales (Nutrition Risk Screening 2002 and Subjective Global Assessment Form) were positively associated with the results of VES-13 [73]. That means that worse nutritional status was associated with vulnerability. Albumins are well known biomarker of malnutrition [74]. Therefore, it is consistent with our results: patients with higher level of albumins had lower risk of vulnerability.
There are several limitations in this study that could be addressed in future research. It is a cross-sectional analysis, and monitoring the vulnerability status after the hospitalization would probably bring new information. This study focused on older inpatients in central Poland. Multiple medical problems were reported but probably not all the concomitant disorders were scrutinized. Larger multicenter studies in different populations would enable to draw more general conclusions. The relationship between vulnerability and concomitant diseases may also be different in community or long-term institutional environment. We only used one short vulnerability screening test - VES-13. Other frailty assessment tools might have performed differently. Nevertheless, the strengths of our research are the large sample size and the inclusion of multiple diseases with their separate impact estimation.
5. Conclusion
VES-13 is often used to qualify patients for further comprehensive geriatric assessment. Our results can help to identify in which accompanying conditions in older hospitalized adults this assessment will be most necessary. According to our data, DM2, CAD, AF, HF, CKD, OA, fractures, eyes disorders, depression, dementia, PU and UI were associated with higher scores of VES-13. At the same time, lipid disorders, gastrointestinal diseases, higher BMI and albumins level were related to lower risk of being vulnerable.
Considering the importance of VES-13 for predicting negative clinical outcomes in older patients and qualifying them for further treatment, particularly in surgery and oncology, paying attention to conditions associated with higher VES-13 scores may be useful for clinicians.
Author Contributions
Conceptualization, G.K., T.K., B.K.S; Methodology, G.K., T.K., B.K.S; Software, G.K., T.K., B.K.S.; Validation, G.K., T.K., B.K.S.; Formal Analysis, T.K., B.K.S.; Investigation, G.K., R.K-B., S.S.S., T.K., B.K.S.; Resources, T.K.; Data Curation, G.K., R.K-B., S.S.S., B.K.S.; Writing—Original Draft Preparation, Writing—Review and Editing, G.K., R.K-B., S.S.S., T.K., B.K.S.; Visualization, B.K.S.; Supervision, T.K.; Project Administration, T.K., B.K.S.; Funding Acquisition, T.K. All authors have read and agreed to the published version of the manuscript.
Funding
The authors were supported by the grant from the Medical University of Lodz, Poland (503/6-077-01/503-61-001-19-00).
Institutional Review Board Statement
This study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board or Ethics Committee of Medical University of Lodz, Poland (protocol code RNN/68/23/KE).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The statistical data used to support the presented findings may be obtained upon request to corresponding author.
Acknowledgments
Special thanks to Łukasz Kroc, Edyta Piechocka-Wochniak and Elizaveta Fife for their support in collecting research material.
Conflicts of Interest
There is no conflict of interest to be declared.
References
- Saliba, D., et al., The Vulnerable Elders Survey: a tool for identifying vulnerable older people in the community. J Am Geriatr Soc, 2001. 49(12): p. 1691-9. [CrossRef]
- Kenig, J., et al., Six screening instruments for frailty in older patients qualified for emergency abdominal surgery. Arch Gerontol Geriatr, 2015. 61(3): p. 437-42. [CrossRef]
- Assis, D.L., et al., The role of VES-13 to identify limited life expectancy in older adults in primary healthcare settings. Rev Esc Enferm USP, 2021. 55: p. e03743. [CrossRef]
- Min, L., et al., The vulnerable elders-13 survey predicts 5-year functional decline and mortality outcomes in older ambulatory care patients. J Am Geriatr Soc, 2009. 57(11): p. 2070-6. [CrossRef]
- Silva, S.M., et al., VES-13 and WHOQOL-bref cutoff points to detect quality of life in older adults in primary health care. Rev Saude Publica, 2019. 53: p. 26. [CrossRef]
- Feng, J., et al., Reliability and validity test of VES-13 and analysis of influencing factors for the vulnerable condition of patients with advanced castration-resistant prostate cancer. Pak J Med Sci, 2021. 37(1): p. 137-141. [CrossRef]
- Carneiro, F., et al., Vulnerability in elderly patients with gastrointestinal cancer--translation, cultural adaptation and validation of the European Portuguese version of the Vulnerable Elders Survey (VES-13). BMC Cancer, 2015. 15: p. 723. [CrossRef]
- Ferrero, A., et al., Can Vulnerable Elders Survey-13 predict the impact of frailty on chemotherapy in elderly patients with gynaecological malignancies? Medicine (Baltimore), 2018. 97(39): p. e12298.
- Lowenstein, L.M., et al., Which better predicts mortality among older men, a prostate cancer (PCa) diagnosis or vulnerability on the Vulnerable Elders Survey (VES-13)? A retrospective cohort study. J Geriatr Oncol, 2016. 7(6): p. 437-443. [CrossRef]
- Luciani, A., et al., Estimating the risk of chemotherapy toxicity in older patients with cancer: The role of the Vulnerable Elders Survey-13 (VES-13). J Geriatr Oncol, 2015. 6(4): p. 272-9. [CrossRef]
- Vernon, T.L., 3rd, et al., Implementation of Vulnerable Elders Survey-13 Frailty Tool to Identify At-Risk Geriatric Surgical Patients. J Perianesth Nurs, 2019. 34(5): p. 911-918.e2.
- Min, L., et al., The vulnerable elders survey-13 predicts hospital complications and mortality in older adults with traumatic injury: a pilot study. J Am Geriatr Soc, 2011. 59(8): p. 1471-6. [CrossRef]
- Assis, F.C., et al., Association of health vulnerability with adverse outcomes in older people with COVID-19: a prospective cohort study. Clinics (Sao Paulo), 2021. 76: p. e3369.
- Balakumar, P., U.K. Maung, and G. Jagadeesh, Prevalence and prevention of cardiovascular disease and diabetes mellitus. Pharmacol Res, 2016. 113(Pt A): p. 600-609. [CrossRef]
- Bell, S.P., et al., Development of a multivariable model to predict vulnerability in older American patients hospitalised with cardiovascular disease. BMJ Open, 2015. 5(8): p. e008122. [CrossRef]
- Wang, J., et al., Changes in vulnerability among older patients with cardiovascular disease in the first 90 days after hospital discharge: A secondary analysis of a cohort study. BMJ Open, 2019. 9(1): p. e024766. [CrossRef]
- Kroc, Ł., et al., Validation of the Vulnerable Elders Survey-13 (VES-13) in hospitalized older patients. European Geriatric Medicine, 2016. 7(5): p. 449-453. [CrossRef]
- Oscanoa, T.J., et al., Estimation of the glomerular filtration rate in older individuals with serum creatinine-based equations: A systematic comparison between CKD-EPI and BIS1. Arch Gerontol Geriatr, 2018. 75: p. 139-145. [CrossRef]
- Yesavage, J.A., et al., Development and validation of a geriatric depression screening scale: a preliminary report. J Psychiatr Res, 1982. 17(1): p. 37-49. [CrossRef]
- Folstein, M.F., S.E. Folstein, and P.R. McHugh, "Mini-mental state". A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res, 1975. 12(3): p. 189-98. [CrossRef]
- Aprahamian, I., et al., Hypertension and frailty in older adults. J Clin Hypertens (Greenwich), 2018. 20(1): p. 186-192. [CrossRef]
- Richter, D., et al., Frailty in cardiology: definition, assessment and clinical implications for general cardiology. A consensus document of the Council for Cardiology Practice (CCP), Association for Acute Cardio Vascular Care (ACVC), Association of Cardiovascular Nursing and Allied Professions (ACNAP), European Association of Preventive Cardiology (EAPC), European Heart Rhythm Association (EHRA), Council on Valvular Heart Diseases (VHD), Council on Hypertension (CHT), Council of Cardio-Oncology (CCO), Working Group (WG) Aorta and Peripheral Vascular Diseases, WG e-Cardiology, WG Thrombosis, of the European Society of Cardiology, European Primary Care Cardiology Society (EPCCS). Eur J Prev Cardiol, 2022. 29(1): p. 216-227. [CrossRef]
- Benetos, A., M. Petrovic, and T. Strandberg, Hypertension Management in Older and Frail Older Patients. Circ Res, 2019. 124(7): p. 1045-1060. [CrossRef]
- Oliveros, E., et al., Hypertension in older adults: Assessment, management, and challenges. Clin Cardiol, 2020. 43(2): p. 99-107. [CrossRef]
- Odden, M.C., et al., Rethinking the association of high blood pressure with mortality in elderly adults: the impact of frailty. Arch Intern Med, 2012. 172(15): p. 1162-8.
- Guo, Q., X. Du, and C.S. Ma, Atrial fibrillation and frailty. J Geriatr Cardiol, 2020. 17(2): p. 105-109. [CrossRef]
- Evans, N.R., et al., Frailty and cerebrovascular disease: Concepts and clinical implications for stroke medicine. Int J Stroke, 2022. 17(3): p. 251-259.
- Afilalo, J., et al., Role of Frailty in Patients With Cardiovascular Disease. American Journal of Cardiology, 2009. 103(11): p. 1616-1621. [CrossRef]
- Purser, J.L., et al., Identifying frailty in hospitalized older adults with significant coronary artery disease. J Am Geriatr Soc, 2006. 54(11): p. 1674-81. [CrossRef]
- Proietti, M., et al., Epidemiology and impact of frailty in patients with atrial fibrillation in Europe. Age Ageing, 2022. 51(8). [CrossRef]
- Wilkinson, C., et al., Management of atrial fibrillation for older people with frailty: a systematic review and meta-analysis. Age Ageing, 2019. 48(2): p. 196-203. [CrossRef]
- Proietti, M., et al., Frailty prevalence and impact on outcomes in patients with atrial fibrillation: A systematic review and meta-analysis of 1,187,000 patients. Ageing Res Rev, 2022. 79: p. 101652. [CrossRef]
- Pandey, A., D. Kitzman, and G. Reeves, Frailty Is Intertwined With Heart Failure: Mechanisms, Prevalence, Prognosis, Assessment, and Management. JACC Heart Fail, 2019. 7(12): p. 1001-1011.
- Davis, M.R., et al., Gender differences in the prevalence of frailty in heart failure: A systematic review and meta-analysis. Int J Cardiol, 2021. 333: p. 133-140. [CrossRef]
- Mielke, N., et al., Gender differences in frailty transition and its prediction in community-dwelling old adults. Sci Rep, 2022. 12(1): p. 7341. [CrossRef]
- Yanase, T., et al., Frailty in elderly diabetes patients. Endocr J, 2018. 65(1): p. 1-11. [CrossRef]
- Assar, M.E., O. Laosa, and L. Rodríguez Mañas, Diabetes and frailty. Curr Opin Clin Nutr Metab Care, 2019. 22(1): p. 52-57.
- Umegaki, H., Sarcopenia and frailty in older patients with diabetes mellitus. Geriatr Gerontol Int, 2016. 16(3): p. 293-9. [CrossRef]
- Chao, C.T., J. Wang, and K.L. Chien, Both pre-frailty and frailty increase healthcare utilization and adverse health outcomes in patients with type 2 diabetes mellitus. Cardiovasc Diabetol, 2018. 17(1): p. 130. [CrossRef]
- Lee, Y., et al., Frailty and body mass index as predictors of 3-year mortality in older adults living in the community. Gerontology, 2014. 60(6): p. 475-82. [CrossRef]
- Jayanama, K., et al., Relationship of body mass index with frailty and all-cause mortality among middle-aged and older adults. BMC Med, 2022. 20(1): p. 404. [CrossRef]
- Bhardwaj, P.V., et al., The Association Between Body Mass Index, Frailty and Long-Term Clinical Outcomes in Hospitalized Older Adults. Am J Med Sci, 2021. 362(3): p. 268-275. [CrossRef]
- Cook, M.J., et al., Increased Frailty in Individuals With Osteoarthritis and Rheumatoid Arthritis and the Influence of Comorbidity: An Analysis of the UK Biobank Cohort. Arthritis Care Res (Hoboken), 2022. 74(12): p. 1989-1996. [CrossRef]
- O'Brien, M.S. and J.J. McDougall, Age and frailty as risk factors for the development of osteoarthritis. Mech Ageing Dev, 2019. 180: p. 21-28. [CrossRef]
- Salaffi, F., S. Farah, and M. Di Carlo, Frailty syndrome in rheumatoid arthritis and symptomatic osteoarthritis: an emerging concept in rheumatology. Acta Biomed, 2020. 91(2): p. 274-296. [CrossRef]
- Ardoino, I., et al., Pain and Frailty in Hospitalized Older Adults. Pain Ther, 2020. 9(2): p. 727-740. [CrossRef]
- Sternberg, S.A., et al., Frailty and osteoporosis in older women--a prospective study. Osteoporos Int, 2014. 25(2): p. 763-8. [CrossRef]
- Ma, S.L., et al., Self-reported frailty is associated with low calcaneal bone mineral density in a multiracial population of community-dwelling elderly. Osteoporos Int, 2009. 20(11): p. 1837-46. [CrossRef]
- Court-Brown, C.M. and M.M. McQueen, Global Forum: Fractures in the Elderly. J Bone Joint Surg Am, 2016. 98(9): p. e36. [CrossRef]
- Curtis, E., et al., Frailty score on admission predicts mortality and discharge disposition in elderly trauma patients over the age of 65 y. J Surg Res, 2018. 230: p. 13-19. [CrossRef]
- Yan, B., et al., Prognostic significance of frailty in older patients with hip fracture: a systematic review and meta-analysis. Int Orthop, 2022. 46(12): p. 2939-2952. [CrossRef]
- Cabral, J.F., et al., Vulnerability and associated factors among older people using the Family Health Strategy. Cien Saude Colet, 2018. 24(9): p. 3227-3236.
- Soysal, P., et al., Relationship between depression and frailty in older adults: A systematic review and meta-analysis. Ageing Res Rev, 2017. 36: p. 78-87. [CrossRef]
- Vaughan, L., A.L. Corbin, and J.S. Goveas, Depression and frailty in later life: a systematic review. Clin Interv Aging, 2015. 10: p. 1947-58. [CrossRef]
- Waite, S.J., et al., Sarcopenia and frailty in individuals with dementia: A systematic review. Arch Gerontol Geriatr, 2021. 92: p. 104268. [CrossRef]
- Arai, H., S. Satake, and K. Kozaki, Cognitive Frailty in Geriatrics. Clin Geriatr Med, 2018. 34(4): p. 667-675. [CrossRef]
- Sugimoto, T., H. Arai, and T. Sakurai, An update on cognitive frailty: Its definition, impact, associated factors and underlying mechanisms, and interventions. Geriatr Gerontol Int, 2022. 22(2): p. 99-109. [CrossRef]
- Cornish, L., Prevention of pressure ulcers in older people with frailty. Nurs Older People, 2022. [CrossRef]
- Jaul, E., Assessment and management of pressure ulcers in the elderly: current strategies. Drugs Aging, 2010. 27(4): p. 311-25.
- Veronese, N., et al., Association between urinary incontinence and frailty: a systematic review and meta-analysis. Eur Geriatr Med, 2018. 9(5): p. 571-578. [CrossRef]
- John, G., et al., Urinary Incontinence as a Predictor of Death: A Systematic Review and Meta-Analysis. PLoS One, 2016. 11(7): p. e0158992. [CrossRef]
- Chowdhury, R., et al., Frailty and chronic kidney disease: A systematic review. Arch Gerontol Geriatr, 2017. 68: p. 135-142. [CrossRef]
- Lahousse, L., et al., Risk of Frailty in Elderly With COPD: A Population-Based Study. J Gerontol A Biol Sci Med Sci, 2016. 71(5): p. 689-95. [CrossRef]
- Yee, N., et al., Frailty in Chronic Obstructive Pulmonary Disease and Risk of Exacerbations and Hospitalizations. Int J Chron Obstruct Pulmon Dis, 2020. 15: p. 1967-1976. [CrossRef]
- Bandidwattanawong, C. and G. Kerkarchachai, The benefits of G8 and VES-13 geriatric screening tools for older patients with advanced lung cancer. J Geriatr Oncol, 2022. 13(8): p. 1256-1259. [CrossRef]
- Ushida, K., et al., Hospital Frailty Risk Score Predicts Outcomes in Chronic Obstructive Pulmonary Disease Exacerbations. Arch Gerontol Geriatr, 2022. 100: p. 104658. [CrossRef]
- Kameyama, H., et al., Efficacy of preoperative frailty assessment in patients with gastrointestinal disease. Geriatr Gerontol Int, 2021. 21(3): p. 327-330. [CrossRef]
- Augschoell, J., et al., PPT and VES-13 in elderly patients with cancer: evaluation in multidimensional geriatric assessment and prediction of survival. J Geriatr Oncol, 2014. 5(4): p. 415-21. [CrossRef]
- Cavdar, E., et al., Prospective comparison of the value of CARG, G8, and VES-13 toxicity tools in predicting chemotherapy-related toxicity in older Turkish patients with cancer. J Geriatr Oncol, 2022. 13(6): p. 821-827. [CrossRef]
- Shang, X., et al., Associations of vision impairment and eye diseases with frailty in community-dwelling older adults: a nationwide longitudinal study in China. Br J Ophthalmol, 2022. [CrossRef]
- Varadaraj, V., et al., Near Vision Impairment and Frailty: Evidence of an Association. Am J Ophthalmol, 2019. 208: p. 234-241. [CrossRef]
- Zhao, Y., et al., Combined Vision and Hearing Impairment is Associated with Frailty in Older Adults: Results from the West China Health and Aging Trend Study. Clin Interv Aging, 2022. 17: p. 675-683. [CrossRef]
- Kroc, Ł., et al., Comparison of Nutrition Risk Screening 2002 and Subjective Global Assessment Form as Short Nutrition Assessment Tools in Older Hospitalized Adults. Nutrients, 2021. 13(1). [CrossRef]
- Zhang, Z., et al., Evaluation of Blood Biomarkers Associated with Risk of Malnutrition in Older Adults: A Systematic Review and Meta-Analysis. Nutrients, 2017. 9(8). [CrossRef]
Figure 1.
shows the simultaneous statistical impact of concomitant diseases, BMI and sex on VES-13 scores. DM2, CAD, AF, HF, CKD, OA, fractures, eyes disorders, depression, dementia, PU, and UI were related to higher values of VES-13 (increased odds ratio for risk of death and disability). Lipid disorders, gastrointestinal diseases and higher BMI were related to lower values of VES-13.
Figure 1.
shows the simultaneous statistical impact of concomitant diseases, BMI and sex on VES-13 scores. DM2, CAD, AF, HF, CKD, OA, fractures, eyes disorders, depression, dementia, PU, and UI were related to higher values of VES-13 (increased odds ratio for risk of death and disability). Lipid disorders, gastrointestinal diseases and higher BMI were related to lower values of VES-13.
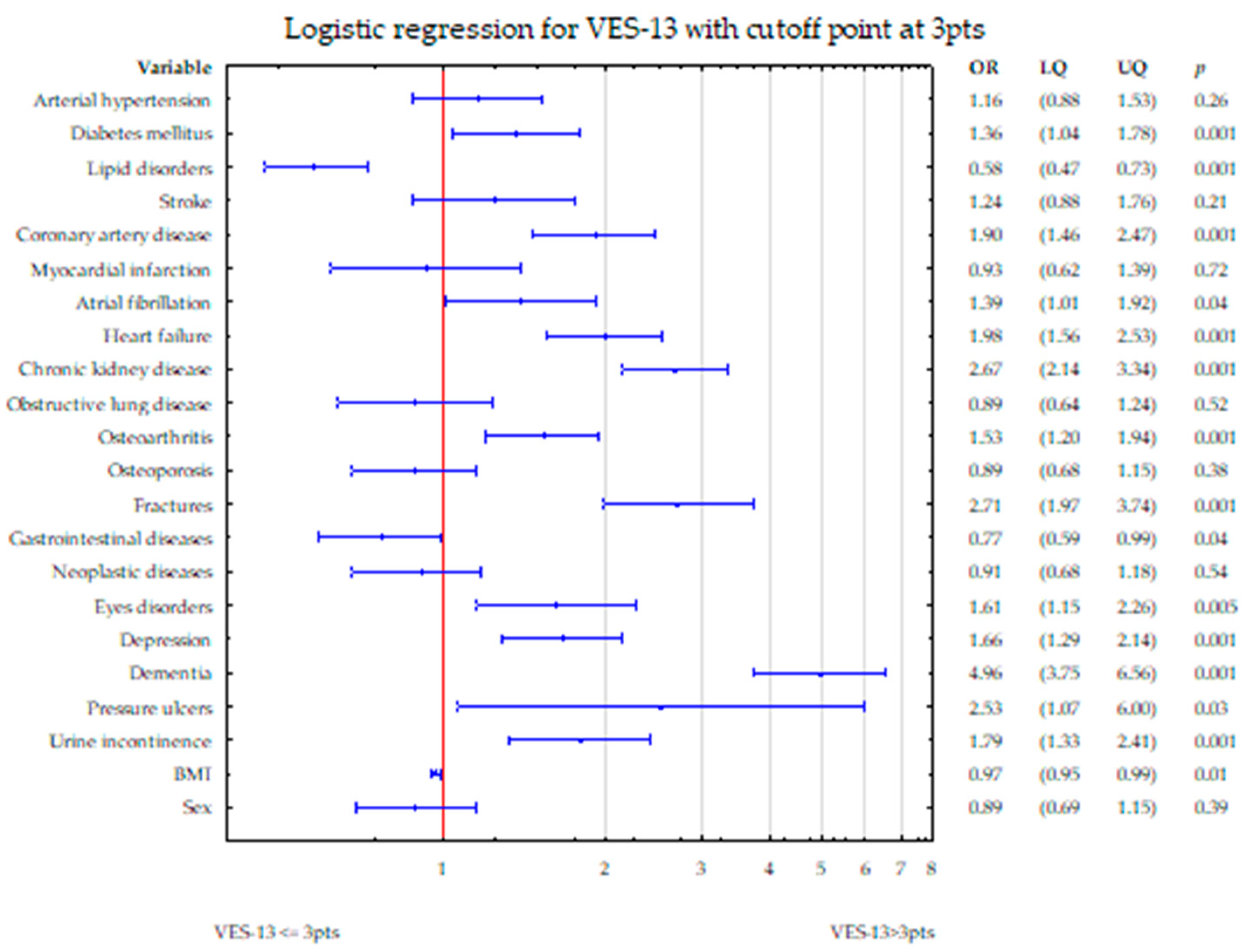

Table 1.
General characteristics of the study population (n=2860) according to sex.
| Parameter/disease | Women n=2036 |
Men n=824 |
p-value |
|---|---|---|---|
| Age (mean±SD, median (quartiles)) | 81.7±7.9 83 (77-87) |
81.8±8.3 83 (76-88) |
p=0.4(U) |
| BMI, m/kg² (mean±SD, median (quartiles)) | 26.2±5.4 25.4 (22.3-29.2) |
26.0±4.6 25.5 (23.0-28.1) |
p=0.92(U) |
| Body mass, kg (mean±SD, median (quartiles)) | 64.4±14.3 63 (54.5-72) |
74.8±14.5 73 (65-81) |
p<0.0001(U) |
| Albumins, g/l (mean±SD, median (quartiles)) | 39.7±5.7 41 (36.9-43.7) |
39±6.2 40.3 (35.9-43.2) |
p=0.002 (U) |
| VES-13, points (mean±SD, median (quartiles)) | 6.78±2.8 8 (4-10) |
6.4±2.9 7 (4-9) |
p=0.002(U) |
| Arterial hypertension, n, % | 1618 (79.5%) | 633 (76.8%) | p=0.117(chi2) |
| Diabetes mellitus, n, % | 507 (24.9%) | 248 (30.1%) | p=0.004(chi2) |
| Lipid disorders, n, % | 919 (45.1%) | 284 (34.5%) | p<0.0001(chi2) |
| Stroke, n, % | 322 (15.8%) | 141 (17.1%) | p=0.4(chi2) |
| Coronary artery disease, n, % | 766 (37.6%) | 335 (40.7%) | p=0.13(chi2) |
| Myocardial infarction, n, % | 186 (9.1%) | 128 (15.5%) | p<0.0001(chi2) |
| Atrial fibrillation, n, % | 385 (18.9%) | 212 (25.7%) | p<0.0001(chi2) |
| Heart failure, n, % | 964 (47.4%) | 397 (48.2%) | p=0.69(chi2) |
| Chronic kidney disease, n, % | 1331 (66.1%) | 519 (63.6%) | p=0.22(chi2) |
| Obstructive lung diseases, n, % | 250 (12.3%) | 119 (14.4%) | p<0.0001(chi2) |
| Osteoarthritis, n, % | 767 (37.7%) | 212 (25.7%) | p<0.0001(chi2) |
| Osteoporosis, n, % | 667 (32.8%) | 93 (11.3%) | p<0.0001(chi2) |
| Fractures, n, % | 464 (22.8%) | 109 (13.2%) | p<0.0001(chi2) |
| Gastrointestinal diseases, n, % | 439 (21.5%) | 183 (22.2%) | p=0.83(chi2) |
| Neoplastic diseases, n, % | 293 (14.4%) | 153 (18.6%) | p=0.06(chi2) |
| Eyes disorders, n, % | 302 (14.8%) | 101 (12.3%) | p=0.2(chi2) |
| Depression, n, % | 678 (33.3%) | 187 (22.7%) | p<0.0001(chi2) |
| Dementia, n, % | 866 (42.5%) | 313 (38%) | p=0.3(chi2) |
| Pressure ulcers, n, % | 118 (5.8%) | 54 (6.6%) | p=0.96(chi2) |
| Urinary incontinence, n, % | 443 (21.7%) | 114 (13.8%) | p<0.0001(chi2) |
SD: standard deviation, BMI: body mass index, (U): U Mann-Whitney test, (chi2): chi-square test.
Table 2.
VES-13 according to the presence of the most common chronic diseases.
| Disease | Gender | VES-13 | p value | |||
| in patients with the presence of particular disease | in patients without particular disease | |||||
| mean±SD | median (quartiles) | mean±SD | median (quartiles) | |||
| Arterial hypertension | Women | 6.9±2.8 | 8.0 (4.0-10.0) | 6.2±2.9 | 7.0 (3.0-8.0) | p<0.0001(U) |
| Men | 6.4±2.8 | 7.0 (3.0-9.0) | 6.6±3.0 | 7.0 (4.0-10.0) | p=0.17(U) | |
| Diabetes mellitus | Women | 7.1±2.7 | 8.0 (4.0-10.0) | 6.7±2.9 | 7.0 (4.0-10.0) | p=0.01(U) |
| Men | 6.5±2.8 | 7.0 (4.0-9.0) | 6.4±2.9 | 7.0 (3.0-9.0) | p=0.44(U) | |
| Lipid disorders | Women | 6.1±2.9 | 6.0 (3.0-8.0) | 7.3±2.7 | 8.0 (5.0-10.0) | p<0.0001(U) |
| Men | 5.6±2.9 | 5.5 (3.0-8.0) | 6.8±2.8 | 7.0 (4.0-10.0) | p<0.0001(U) | |
| Stroke | Women | 7.4±2.5 | 8.0 (6.0-10.0) | 6.6±2.9 | 7.0 (4.0-10.0) | p<0.0001(U) |
| Men | 6.9±2.6 | 7.0 (4.0-9.0) | 6.3±2.9 | 7.0 (3.0-9.0) | p=0.04(U) | |
| Coronary artery disease | Women | 7.4±2.6 | 8.0 (6.0-10.0) | 6.4±2.9 | 7.0 (3.0-9.0) | p<0.0001(U) |
| Men | 6.8±2.8 | 7.0 (4.0-10.0) | 6.1±2.9 | 7.0 (3.0-8.0) | p=0.0003(U) | |
| Myocardial infarction | Women | 7.3±2.7 | 8.0 (5.0-10.0) | 6.7±2.9 | 7.0 (4.0-10.0) | p=0.014(U) |
| Men | 6.7±2.8 | 7.0 (4.0-9.5) | 6.4±2.9 | 7.0 (3.0-9.0) | p=0.3(U) | |
| Atrial fibrillation | Women | 7.6±2.6 | 8.0 (6.0-10.0) | 6.6±2.9 | 7.0 (4.0-9.0) | p<0.0001(U) |
| Men | 7.2±2.8 | 8.0 (5.0-10.0) | 6.1±2.8 | 7.0 (3.0-8.0) | p<0.0001(U) | |
| Heart failure | Women | 7.4±2.6 | 8.0 (5.0-10.0) | 6.2±2.9 | 7.0 (3.0-9.0) | p<0.0001(U) |
| Men | 7.1±2.7 | 8.0 (5.0-10.0) | 5.8±2.9 | 6.0 (3.0-8.0) | p<0.0001(U) | |
| Chronic kidney disease | Women | 7.2±2.7 | 7.0 (4.0-10.0) | 6.0±3.0 | 7.0 (3.0-8.0) | p<0.0001(U) |
| Men | 6.8±2.8 | 7.0 (4.0-10.0) | 5.7±2.9 | 6.0 (3.0-8.0) | p<0.0001(U) | |
| Obstructive lung diseases | Women | 7.0±2.7 | 8.0 (4.0-10.0) | 6.7±2.9 | 8.0 (4.0-10.0) | p=0.24(U) |
| Men | 6.6±2.8 | 7.0 (4.0-9.0) | 6.4±2.9 | 7.0 (4.0-9.0) | p=0.58(U) | |
| Osteoarthritis | Women | 6.8±2.7 | 8.0 (4.0-10.0) | 6.7±2.9 | 8.0 (4.0-10.0) | p=0.68(U) |
| Men | 6.5±2.8 | 7.0 (4.0-9.0) | 6.4±2.9 | 7.0 (3.5-9.0) | p=0.57(U) | |
| Osteoporosis | Women | 6.4±2.9 | 7.0 (4.0-9.0) | 7.0±2.8 | 8.0 (4.0-10.0) | p=0.00002(U) |
| Men | 6.8±2.8 | 8.0 (4.0-10.0) | 6.4±2.9 | 7.0 (3.0-9.0) | p=0.15(U) | |
| Fractures | Women | 7.3±2.7 | 8.0 (4.0-10.0) | 6.6±2.9 | 7.0(4.0-10.0) | p<0.0001(U) |
| Men | 7.2±2.6 | 8.0 (5.0-10.0) | 6.3±2.9 | 7.0(3.0-9.0) | p=0.0017(U) | |
| Gastrointestinal diseases | Women | 6.4±2.8 | 7.0 (3.0-9.0) | 6.9±2.8 | 8.0 (4.0-10.0) | p=0.0004(U) |
| Men | 6.0±2.8 | 6.0 (3.0-8.0) | 6.5±2.9 | 7.0 (4.0-9.0) | p=0.04(U) | |
| Neoplastic diseases | Women | 6.4±2.9 | 7.0 (4.0-9.0) | 6.8±2.8 | 8.0 (4.0-10.0) | p=0.04(U) |
| Men | 6.8±2.8 | 8.0 (4.0-9.0) | 6.3±2.9 | 7.0 (3.0-9.0) | p=0.07(U) | |
| Eyes disorders | Women | 7.0±2.7 | 8.0 (4.0-10.0) | 6.7±2.9 | 8.0 (4.0-10.0) | p=0.14(U) |
| Men | 7.0±2.6 | 7.0 (5.0-9.0) | 6.3±2.9 | 7.0 (3.0-9.0) | p=0.37(U) | |
| Depression | Women | 7.2±2.6 | 8.0 (6.0-10.0) | 6.5±2.9 | 7.0 (4.0-10.0) | p<0.0001(U) |
| Men | 7.0±2.7 | 8.0 (4.0-9.0) | 6.2±2.9 | 7.0 (3.0-9.0) | p=0.002(U) | |
| Dementia | Women | 8.0±2.3 | 8.0 (7.0-10.0) | 5.9±2.9 | 6.0 (3.0-8.0) | p<0.0001(U) |
| Men | 7.7±2.5 | 8.0 (7.0-10.0) | 5.6±2.8 | 5.0 (3.0-8.0) | p<0.0001(U) | |
| Pressure ulcers | Women | 8.5±2.0 | 9.0 (8.0-10.0) | 6.7±2.8 | 7.0 (4.0-10.0) | p<0.0001(U) |
| Men | 8.4±1.8 | 8.5 (7.0-10.0) | 6.3±2.9 | 7.0 (3.0-9.0) | p<0.0001(U) | |
| Urinary incontinence | Women | 6.9±2.6 | 8.0 (4.0-9.0) | 7.0±2.9 | 8.0 (4.0-10.0) | p=0.53(U) |
| Men | 7.0±2.4 | 7.0 (5.0-9.0) | 6.3±3.0 | 7.0 (3.0-9.0) | p=0.033(U) | |
SD: standard deviation, (U): U Mann-Whitney test.
Table 3.
Age of patients according to the presence of particular disease.
| Disease | Gender | Age | p value | |||
| in patients with the presence of particular disease | in patients without particular disease | |||||
| mean±SD | median (quartiles) | mean±SD | median (quartiles) | |||
| Arterial hypertension | Women | 82.3±7.5 | 83 (78-87) | 79.3±8.8 | 80 (72-86) | p<0.0001 (U) |
| Men | 81.8±8.2 | 83 (76-88) | 81.8±8.5 | 83 (76-88) | p=0.81 (U) | |
| Diabetes mellitus | Women | 81.9±7.4 | 83 (77-87) | 81.6±8.1 | 83 (77-87) | p=0.9 (U) |
| Men | 80.8±8.2 | 82 (74-87) | 82.3±8.3 | 84 (78-88) | p=0.03 (U) | |
| Lipid disorders | Women | 79.9±7.9 | 81 (74-86) | 83.2±7.6 | 84 (79-88) | p<0.0001 (U) |
| Men | 80.1±8.6 | 82 (74-86) | 82.8±8.0 | 84 (79-88) | p<0.0001 (U) | |
| Stroke | Women | 82.7±7.5 | 84 (79-88) | 81.5±7.9 | 83 (77-87) | P=0.02 (U) |
| Men | 81.1±8.3 | 83 (75-88) | 82.0±8.3 | 83 (77-88) | p=0.3 (U) | |
| Coronary artery disease | Women | 83.4±6.8 | 84 (79-88) | 80.7±8.3 | 82 (75-87) | p<0.0001 (U) |
| Men | 83.7±7.7 | 85 (80-89) | 80.6±8.4 | 82 (75-87) | p<0.0001 (U) | |
| Myocardial infarction | Women | 83.1±7.3 | 85 (79-88) | 81.6±7.9 | 83 (77-87) | p=0.007 (U) |
| Men | 83.5±7.3 | 85 (79.5-88) | 81.5±8.4 | 83 (76-88) | p=0.02 (U) | |
| Atrial fibrillation | Women | 84.2±6.6 | 85 (80-89) | 81.1±8.1 | 82 (76-87) | p<0.0001 (U) |
| Men | 84.2±7.6 | 86 (81-89) | 81.0±8.4 | 82 (75-87) | p<0.0001 (U) | |
| Heart failure | Women | 83.8±6.9 | 85 (80-88) | 79.8±8.3 | 81 (74-86) | p<0.0001 (U) |
| Men | 83.6±7.8 | 85 (80-89) | 80.1±8.3 | 81 (74-86) | p<0.0001 (U) | |
| Chronic kidney disease | Women | 83.8±6.7 | 84 (80-88) | 77.6±8.4 | 78 (71-84) | p<0.0001 (U) |
| Men | 84.5±6.6 | 85 (81-89) | 77.3±9.0 | 78 (70-84) | p<0.0001 (U) | |
| Obstructive lung diseases | Women | 81.9±7.0 | 82.5 (78-87) | 81.7±8.0 | 83 (77-87) | p=0.9 (U) |
| Men | 82.2±7.5 | 83 (78-87) | 81.8±8.4 | 83 (76-88) | p=0.9 (U) | |
| Osteoarthritis | Women | 81.9±7.4 | 83 (78-87) | 81.6±8.2 | 83 (76-88) | p=0.68 (U) |
| Men | 82.0±8.4 | 84 (78-88) | 81.8±8.2 | 83 (76-88) | p=0.9 (U) | |
| Osteoporosis | Women | 80.9±7.9 | 82 (76-87) | 82.1±7.9 | 83 (77-88) | p=0.001 (U) |
| Men | 83.5±7.3 | 84 (79-89) | 81.6±8.4 | 83 (76-88) | p=0.06 (U) | |
| Fractures | Women | 82.6±7.3 | 84 (78-88) | 81.4±8.0 | 83 (76.5-87) | p=0.009 (U) |
| Men | 83.3±9.6 | 84 (78-91) | 81.6±8.1 | 83 (76-88) | p=0.02 (U) | |
| Gastrointestinal diseases | Women | 79.8±8.4 | 81 (74-86) | 82.2±7.7 | 83 (78-88) | p<0.0001 (U) |
| Men | 81.5±7.6 | 83 (77-87) | 81.9±8.5 | 83 (76-88) | p=0.5 (U) | |
| Neoplastic diseases | Women | 81.0±8.0 | 82 (76-87) | 81.8±7.9 | 83 (77-87) | p=0.07 (U) |
| Men | 83.0±7.9 | 84 (80-88) | 81.6±8.4 | 83 (76-88) | p=0.06 (U) | |
| Eyes disorders | Women | 82.6±7.3 | 83 (79-88) | 81.6±8.0 | 83 (77-87) | p=0.2 (U) |
| Men | 83.7±7.4 | 85 (81-89) | 81.6±8.4 | 83 (76-88) | p=0.01 (U) | |
| Depression | Women | 81.8±7.3 | 83 (78-87) | 81.7±8.2 | 83 (77-88) | p=0.7 (U) |
| Men | 81.9±7.6 | 83 (78-87) | 81.8±8.5 | 83 (76-88) | p=0.8 (U) | |
| Dementia | Women | 84.6±6.4 | 85 (81-89) | 79.5±8.2 | 81 (73-86) | p<0.0001 (U) |
| Men | 84.1±7.2 | 85 (80-89) | 80.4±8.6 | 82 (74-87) | p<0.0001 (U) | |
| Pressure ulcers | Women | 84.4±7.9 | 85 (80-90) | 81.5±7.9 | 83 (77-87) | p=0.0002 (U) |
| Men | 83.7±6.9 | 85 (82-88) | 81.7±8.4 | 83 (76-88) | p=0.07 (U) | |
| Urinary incontinence | Women | 81.8±7.6 | 83 (77-87) | 81.6±8.0 | 83 (77-87) | p=0.9 (U) |
| Men | 82.5±7.8 | 84 (78-88) | 81.7±8.3 | 83 (76-88) | p=0.3 (U) | |
SD: standard deviation, (U): U Mann-Whitney test.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



