
Submitted:
29 July 2023
Posted:
01 August 2023
You are already at the latest version
Abstract
Encephalitis is a condition with a variety of etiologies, clinical presentations and degrees of severity. The causes of these disorders include both neuroinfections and autoimmune diseases in which host antibodies are pathologically directed against self antigens. In autoimmune encephalitis, autoantibodies are expressed in the central nervous system. The incidence of this disease is approximately 4% of all reported cases of encephalitis. Autoimmune encephalitis can be induced by antibodies against neuronal surface antigens such as N-methyl-D-aspartate-activated glutamate receptors (NMDAR), ⍺-amino-3-hydroxy-5-methyl-4-isoxazole propionate receptors (AMPAR) or gangliosides GQ1b, DPPX, CASPR2, LGI1, as well as by antibodies against neuronal intracellular antigens. The paper presents a number of both mental and neurological symptoms of autoimmune encephalitis. Moreover, the coexistence of psychoses, neoplastic diseases and the methods of diagnosing autoimmune encephalitis are discussed. Attention was also drawn to the fact that early diagnosis, as well as early initiation of targeted treatment, increases the chance of a successful course of the therapeutic process.
Keywords:
autoimmune inflamation with antibodies
; anti-NMDAR antibodies
; anti-AMPAR antibodies
; anti-GQ1b antibodies
; anti-DPPX antibodies
; anti-CASPR2 antibodies
; anti-LGI1 antibodies
; encephalitis
; psychoses
Strategy and methodology
The articles on which the following paper was based were searched using search engines such as PubMed and Medline. Considering that anti-NMDAR antibodies were first described in 2007, the articles were from 2007 -2023. The selection of papers was done by entering the phrases "autoimmune encephalitis and psychosis/paraneplastic syndromes or cancer". The total number of articles that could be searched was 747, of which 100 items were selected, being the most recent reports illustrating the presented topic. 34 of them were rejected, in connection with case reports or papers that could not be accessed.
1. Introduction
Encephalitis is a severe disorder with many possible causes with varying clinical presentations and degrees of severity. The causes of these disorders include both neuroinfections and autoimmune diseases [1,2]. There are reports indicating that various inflammatory conditions may outnumber infectious diseases in the central nervous system [3].
Autoimmune encephalitis is a heterogeneous group of inflammatory diseases of the central nervous system of various etiologies, requiring complex differential diagnosis. It is a severe clinical condition in which there is a misdirected immune response and directing autoantibodies against self-antigens, with expression taking place in the central nervous system [3,4]. Autoimmune encephalitis is a heterogeneous group of diseases with central nervous system inflamation, characterized by a wide range of symptoms, both neurological and psychiatric. They can occur at any age, and it is characteristic that they develop as a rapidly progressive encephalopathy (usually in less than 6 weeks) caused by encephalitis [5, 6]. According to Zuliani et al. [7], autoimmune encephalitis describes several types of different diseases with different pathophysiology, the understanding of which is necessary in the selection of appropriate therapy. In turn, this understanding requires diagnosis based on the identification of autoantibodies associated with this neurological disorder.
Autoimmune encephalitis is not uncommon these days. Initially, the incidence of this disease was a small proportion of all reported cases of encephalitis. However, the last two decades have seen a significant increase in the incidence of autoimmune encephalitis. This is related to the development of diagnostic methods and the discovery over this time of numerous autoantibodies directed against the extracellular domains of neuroglial proteins. Advances in autoimmune encephalitis research have led to the identification of new biomarkers that have allowed for an extended diagnostic approach to these disorders. Thus, there was a significant increase in the number of reported cases of autoimmune encephalitis. Due to the multitude of symptoms of autoimmune encephalitis, this disease is still underestimated. This makes it impossible to unequivocally determine the percentage of morbidity among the general population. Recent epidemiological studies even suggest that autoimmune encephalitis is probably as common as infectious encephalitis, with a prevalence estimated at 13.7/100,000 [5, 6, 7].
The factor that makes it difficult to make a diagnosis in the diagnosis of autoimmune encephalitis is the time from the onset of the first symptoms. In the majority of reported cases, the median time to CSF antibody response ranges from a few days to a few weeks, with a peak frequency around the third week. However, the literature on the subject describes chronic cases, even from one to five years. Therefore, diagnostics based on differential tests of autoantibodies in the patient's blood have become so important [8, 9].
The paper presents a number of both mental and neurological symptoms of autoimmune encephalitis. Moreover, the coexistence of psychoses, neoplastic diseases and the methods of diagnosing autoimmune encephalitis are discussed. Attention was also drawn to the fact that early diagnosis, as well as early initiation of targeted treatment, increase the chance of a successful course of the therapeutic process.
2. Antibodies in the course of autoimmune encephalitis
One of the essential elements of the diagnosis of autoimmune encephalitis is the detection and identification of specific antineuronal antibodies. This disease can be induced by antibodies directed against neuronal surface antigens, such as glutamate receptors activated by N-methyl-D-aspartate (NMDAR), ⍺-amino-3-hydroxy-5-methyl-4-isoxazole propionate receptors (AMPAR) and gangliosides GQ1b, DPPX, CASPR2, LGI1, as well as by antibodies directed against intracellular antigens of neurons. Identification of these antibodies determines the initiation of specific therapeutic actions [8, 9, 10].
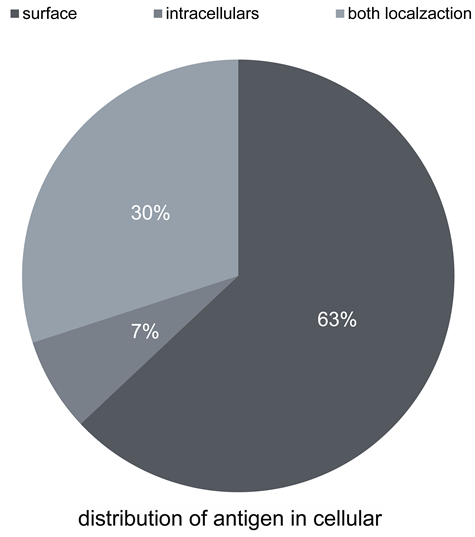
Currently, numerous antibodies inducing the described autoimmune disease are distinguished. According to Wandinger et al. [10], newly identified forms of autoimmune encephalitis are often associated with antineuronal antibodies directed not only against intracellular antigens, but above all against surface antigens. According to these authors, in as many as 63% of cases of diagnosed autoimmune encephalitis we deal with antibodies against surface antigens, in 30% of cases we deal with antibodies against intracellular antigens, and only in 7% of patients we encounter both types of antibodies. Wandinger et al. [10] estimated the frequency of individual antibodies in their work.
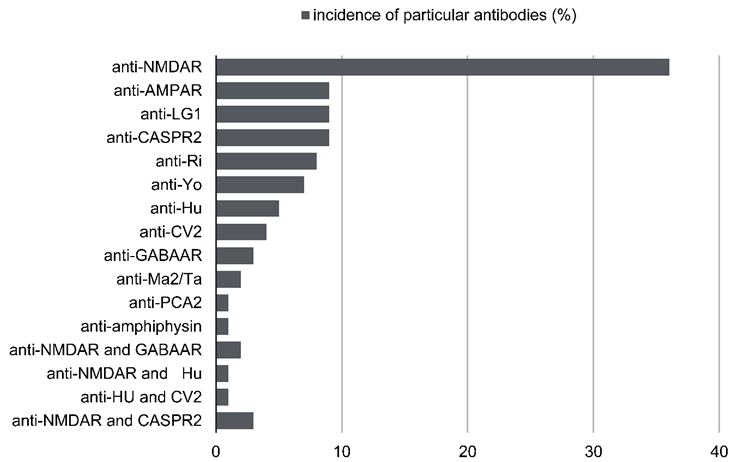
As reported, with the highest frequency of 36%, a single anti-neuronal antibody directed against NMDAR antigens is identified. At the level of 9%, a single anti-neuronal antibody directed against AMPAR antigens is identified. At the level of 9%, a single antineuronal antibody directed against LGI1 antigens is identified. At the level of 9%, a single antineuronal antibody directed against CASPR2 antigens is identified. At the level of 8%, a single antineuronal antibody directed against Ri antigens is identified. At the level of 7%, a single antineuronal antibody directed against Yo antigens is identified. At the level of 5%, a single antineuronal antibody directed against Hu antigens is identified. At the level of 4%, a single anti-neuronal antibody directed against CV2 antigens is identified. At the level of 3%, a single antineuronal antibody directed against GABABR antigens is identified. At the 2% level, a single antineuronal antibody directed against the Ma2/Ta antigens is identified. At the 1% level, a single anti-neuronal antibody directed against PCA-2 antigens is identified. At the 1% level, a single anti-neuronal antibody directed against amphiphysin antigens is identified. These authors, in their work, also determined the frequency of coexistence of individual antineuronal antibodies in the course of autoimmune encephalitis at the level of: 3% for antibodies directed against NMDAR and CASPR2 antigens, 2% for antibodies directed against NMDAR and GABABR antigens, 1% for antibodies directed against antigens NMDAR and Hu and 1% for antibodies directed against Hu and CV2 antigens [8, 9, 10, 11, 12].
Due to the frequency of occurrence, particular attention should be paid to antibodies against glutamate receptors induced by N-methyl-D-aspartate (NMDAR), antibodies to ⍺-amino-3-hydroxy-5-methyl-4-isoxazole propionate (AMPAR) receptors and antibodies against gangliosides CASPR2, LGI1, as well as recently described GQ1b and DPPX [8, 9].
2.1. Autoimmune encephalitis with anti-NMDAR antibodies
Autoimmune encephalitis caused by antibodies directed against the NMDA (N-methyl-D-aspartate) receptor subtype was first described in 2007. It has since entered the mainstream of interest in neurology and psychiatry. Some patients with rapidly progressive psychiatric symptoms or cognitive impairment, seizures, abnormal movements, or coma of unknown cause have been observed to have previously undiagnosed autoimmune disease.
Anti-NMDAR encephalitis is the most common form of autoimmune antibody-associated encephalitis. The prevalence of the disease was initially estimated at approximately 4% of all reported cases of encephalitis. In the study, the aim of which was to determine the cause of the first psychotic episode, in less than 4% of participants the background was defined as non-psychiatric, of which anti-NMDAR antibodies were detected in as many as 75% [11, 12]. The condition can affect people of all ages, but the highest incidence rates are in children and young adults. More than 37% of patients are under the age of 18 at the onset of the disease. The disease affects women more often than men. As many as 80% of patients are women, with an average age of onset of 21 years [12]. In more than half of cases, the disease is associated with cancer and responds to treatment, but may recur. Ovarian teratoma was observed in 58% of women over 18 years of age. In addition to age, the presence of the tumor also depends on gender and ethnicity, being slightly more common in black women than in white women. Patients treated with tumor resection and immunotherapy (corticosteroids, intravenous immunoglobulins, or plasma exchange) respond more quickly to treatment and are less likely to require second-line immunotherapy (cyclophosphamide or rituximab or both) than patients without a tumor who receive similar initial immunotherapy. In over 75% of all patients, a significant recovery occurs, which occurs in the reverse order of the development of symptoms and is associated with a decrease in antibody titer [13].
In this disease, autoantibodies serve as a diagnostic marker and alter NMDAR-related synaptic transmission. N-methyl-d-aspartate receptor antibodies belong to the immunoglobulin G1 subclass and are capable of activating complement on human embryonic kidney cells expressing the N-methyl-d-aspartate receptor. Patients' antibodies cause a titer-dependent, reversible decrease in synaptic NMDAR through a mechanism of cross-linking and internalization. Based on models of pharmacological or genetic disruption of NMDARs, these antibody effects reveal a probable pathogenic link between receptor depletion and the clinical features of anti-NMDAR encephalitis [10]. The pathogenesis of autoimmune encephalitis with anti-NMDAR antibodies most likely has its origin in neoplastic lesions as well as in virus-infected neurons. They release antigens for NMDA receptors (NMDARs), which are taken up by antigen-presenting cells (APCs) after apoptosis. APCs migrate to local lymph nodes, where, as a result of cooperation with CD4+ T lymphocytes, naive B lymphocytes differentiate into plasma cells and memory cells. The anti-NMDAR antibodies produced by these plasma cells are transported with the blood to the regions of the brain and synaptic connections, where they compete with the GluN1 and RphB2 subunits and lead to neurotransmitter dysregulation. Thus, they become the cause of psychotic symptoms [13].
At the onset of symptoms, distinguishing autoimmune encephalitis from a primary psychiatric disorder is difficult. Autoimmune encephalitis with anti-NMDAR antibodies may begin with non-specific flu-like symptoms followed by fairly rapid (within days to six weeks) development of neuropsychiatric symptoms. The disease presents as a rapidly progressing encephalopathy with acute or subacute onset. The main symptom, which occurs in 90% of patients, is psychiatric disorders, usually of acute onset. The coexistence of a number of symptoms is significant, which is not characteristic of any mental illness. Most patients with anti-NMDAR encephalitis develop a multi-stage disease that progresses from psychosis and seizures to an unresponsive state with catatonic features often associated with autonomic and respiratory instability. In the cognitive sphere, abnormalities such as disorientation, confabulation, confusion or memory deficits can be observed. The clinical picture is complemented by pathology noted in the motor sphere. Symptoms such as facial and tongue dyskinesia, chorea, stereotypia, athetosis and dystonia as well as epileptic seizures (mainly tonic-clonic morphology, focal seizures and absence seizures) are not uncommon. The severity of symptoms often requires intensive care. Other than clinical evaluation, there are no specific prognostic biomarkers. The disease is characterized by an acute and aggressive course, however, in the case of correct diagnosis and promptly implemented treatment, most patients achieve permanent remission. Correctly defined criteria of diagnosis determine the period of occurrence of symptoms as not longer than 3 months. In addition to obtaining a positive result of anti-NMDAR antibodies, additional tests such as EEG or MRI should be performed to confirm symptoms associated with autoimmune encephalitis with anti-NMDAR antibodies, such as: EEG or MRI [1, 8, 14, 15, 16, 17].
2.2. Autoimmune encephalitis with anti-AMPAR antibodies
Autoimmune encephalitis can be induced by antibodies directed against ⍺-amino-3-hydroxy-5-methyl-4-isoxazole propionate receptors (AMPAR), which are neuronal surface antigens. The disease is a rare type of autoimmune encephalitis, which was first described by Lai et al. [18]. ⍺-Amino-3-hydroxy-5-methyl-4-isoxazole propionate receptors are expressed throughout the central nervous system, particularly in the hippocampus and other limbic regions. Anti-AMPAR antibodies are directed against extracellular epitopes of the GluA1 or GluA2 subunits of this receptor. Anti-AMPAR encephalitis is most common in middle-aged women, and most patients had an acute or subacute onset. As with anti-NMDAR autoimmune encephalitis, suspected anti-AMPAR autoimmune encephalitis often shows inflammatory changes in the cerebrospinal fluid in laboratory tests. Therefore, it can be expected that in patients with anti-NMDAR and anti-AMPAR encephalitis, tests will show inflammatory changes in the cerebrospinal fluid in most cases. This is important in the diagnosis of this autoimmune disease, as it allows for making appropriate and quick therapeutic decisions. Encephalitis caused by anti-AMPAR antibodies is a neurological disease that is often accompanied by the presence of tumors, and therefore may cover the entire spectrum of paraneoplastic syndrome [8, 18].
The thymus is the central organ of the immune system and it is believed that tumors of the thymus may be the initiators of many neurological disorders. Recently, there is increasing evidence that thymomas are associated with autoimmune encephalitis. Omi et al. [19] were the first to describe a case of encephalitis directed against the α-amino-3-hydroxy-5-methyl-4-isoxazole propionic acid receptor, whose clinical recurrence coincided with thymoma recurrence. Clinical recurrence of anti-AMPAR encephalitis after recurrence of the initially detected tumor has not been previously reported. The patient had been in remission for 34 months and showed clinical relapse 3 months after the thymoma recurrence was detected. This case highlights the pathogenic importance of specific tumor antigens as a trigger for anti-AMPAR antibody production and disease induction. In turn, Song et al. [20] tracked data from January 1, 2011 to October 1, 2021 from PubMed, Web of Science, Ovid and CNKI platforms to analyze general demographic characteristics, frequency of symptoms and associations, and prognosis results treatment of 68 patients with naty-AMPAR autoimmune encephalitis in combination with thymoma. Clinical manifestations were mainly cognitive changes (70.6%), psychiatric disorders (57.4%) and epilepsy (50.0%). Treatment included immunotherapy and thymoma therapy, with 79.7% of patients improving post-treatment. While 20.3% of patients had a poor prognosis. Relapse occurred in 14.8% of patients. According to these authors, thymoma-associated autoimmune encephalitis is a disease entity that absolutely requires long-term follow-up of chest CT results. Zhang et al. [21] report that inflammation of the limbic system of the brain is very often accompanied by antibodies against AMPAR receptors. Autoimmune encephalitis in this form is clinically characterized by a subacute disorder consisting of short-term memory loss, confusion, abnormal behavior and seizures. According to these authors, most patients with anti-AMPAR encephalitis had malignant complications such as thymoma, small cell lung cancer, breast cancer, and ovarian cancer. Most patients with anti-AMPAR encephalitis showed a partial neurological response to immunotherapy. McCombe et al. [22] confirmed the occurrence of thymoma as the most common tumor accompanying autoimmune encephalitis with anti-AMPAR antibodies. In addition, these authors report that in anti-AMPAR encephalitis, the concomitant antibodies predict a different clinical picture than encephalitis and thymoma. In isolated cases, anti-AMPAR autoimmune encephalitis is accompanied by unexpected disease entities. Despite not fully understood connections between its co-diagnosis with thymoma and myasthenia gravis, Li et al. [23] were the first to describe the autoimmune profile and clinical picture of a patient with α-amino-3-hydroxy-5-methyl- 4-isoxazole propionic acid and myasthenia gravis. This points to the extraordinary complexity of thymoma-associated autoimmune networks. Joubert et al. (24) report that the clinical picture of autoimmune encephalitis with anti-AMPAR antibodies is variable. Most patients present with symptoms suggestive of autoimmune limbic encephalitis. They may also show no symptoms or may manifest as severe encephalitis that evolves to a state of minimal consciousness and diffuse cerebral atrophy. Contrary to other reports, in the group of seven patients analyzed, these authors observed only one patient with epileptic seizures and only two patients with cancer - one lung cancer and one thymus cancer. These authors clearly emphasize that due to poorly understood clinical features, patients with suspected autoimmune encephalitis associated with the presence of antibodies to the α-amino-3-hydroxy-5-methyl-4-isoxazole propionic acid receptor should be screened for presence of anti-AMPR antibodies both in the serum and in the cerebrospinal fluid [18, 19, 20, 21, 22, 23, 24, 25].
2.3. Autoimmune encephalitis with anti-GQ1b, anti-DPPX, anti-CASPR2 and anti-LGI1 antibodies
Autoimmune encephalitis can also be induced by antibodies directed against gangliosides GQ1b, DPPX, CASPR2, LGI1 [8, 26, 27, 28, 29, 30].
In the 1950s, Bickerstaff and Fisher independently reported cases with the unique symptom of ophthalmoplegia and ataxia. Neurological symptoms were usually preceded by a previous infection, and most patients recovered spontaneously. However, both authors saw some similarities with Guillain-Barré syndrome, such as the presence of peripheral neuropathy and albuminocytological dissociation of the cerebrospinal fluid. The discovery of anti-GQ1b antibodies in patients with Fisher's syndrome and later Bickerstaff's encephalitis was crucial in providing the necessary evidence to conclude that both conditions were in fact part of the same spectrum of diseases due to their common clinical and immunological characteristics. The occurrence of anti-GQ-1b antibodies is associated with a variety of disorders. According to Yoshikawa et al. [27], confirmation of the presence of anti-GQ1b antibodies may affect vision disorders. Only recently have these antibodies been associated with autoimmune encephalitis [26, 27].
Autoimmune encephalitis caused by autoantibodies directed against dipeptidyl peptidase-like protein (DPPX), a potassium channel subunit, is rare. In autoimmune encephalitis with antibodies against DPPX receptors, the cerebrospinal fluid is often characterized by inflammation. The disease is typically characterized by a triad of symptoms that include weight loss, central nervous system hyperactivity, and cognitive deficits. However, recent reports suggest that the clinical picture may be more heterogeneous. Although blood and cerebrospinal fluid analyzes often show normal cell counts, high titers of DPPX antibodies in the blood and cerebrospinal fluid confirm autoimmune encephalitis with anti-DPPX antibodies. Piepgras et al. [28] confirmed the pathogenic role of anti-DPPX antibodies in anti-DPPX encephalitis in studies on the hyperexcitability of neurons of the enteric nervous system and the reduction of the level of DPPX from the membranes of hippocampal neurons. Xiao et al. [29] conducted a retrospective analysis of nine patients with anti-DPPX encephalitis to expand the clinical and imaging phenotypes of anti-DPPX encephalitis. Nine patients (median age 51 years; range 14-65 years) were identified with symptoms of prodromal fever, diarrhea, or weight loss, followed by rapidly progressive encephalopathy characterized by cognitive impairment. They described three patients with anti-DPPX encephalitis who had sleep disturbance with abnormal sleep behavior with rapid eye movements, limb paralysis, and severe pleocytosis. One patient who received methylprednisolone therapy and a trial of tacrolimus showed significant improvement and had no recurrence during the 6-month follow-up. However, these authors emphasize that further research is warranted to explain the entire clinical spectrum of anti-DPPX encephalitis, its pathogenic mechanisms and prognosis in the case of long-term immunosuppressive therapy [28, 29, 30].
CASPR2 and LGI1 are proteins that are part of a complex of proteins related to the voltage-gated potassium channel VGKC (VGKC). Autoantibodies against extracellular proteins LGI1 and Caspr2 were first described in 2010. This has significantly changed the view on the clinical relevance of antibodies associated with the voltage-gated potassium channel. Autoimmune encephalitis with autoantibodies to inactivated leucine-rich glioma 1 (LGI1) accounts for the diagnosis of anti-LGI1 autoimmune encephalitis. In turn, the diagnosis of antibodies directed against contacttin-like protein 2 (CASPR2) is responsible for anti-CASPR2 encephalitis. Encephalitis associated with antibodies to CASPR2 is a rare autoimmune disease. The main clinical manifestations are believed to be convulsions, memory loss, psychiatric symptoms, dizziness and sleep disturbances. The most common clinical symptoms in both of these subtypes are epileptic seizures, memory deficits, mental disorders and disturbances of consciousness. Currently, all of these antibodies are classified as VGKC complex antibodies and are generally considered to be of similar clinical value. However, research over the last few years shows that the immune responses mediated by these antibodies have different clinical relevance. Antibodies against LGI1 and Caspr2 are associated with different but well-defined neurological syndromes. Both share common and distinct clinical features mediated by autoantibodies directed against different proteins complexed with voltage-gated potassium channels.
Limbic encephalitis is an etiologically heterogeneous disease, because it can occur both as a paraneoplastic disease and in patients without oncological disease. Various neuronal autoantibodies have been found in patients with this type of encephalitis. According to previous studies, antibodies against the VGKC complex are most often present, and among the proteins included in this complex, antibodies against the LGI1 protein, a protein that plays an important role in synaptic transmission by participating in the formation of pre- and post-synaptic protein complexes.
Anti-CASPR2 and anti-LGI1 encephalitis is the most common subtype in the elderly, with the majority of CSF findings normal. As a result, in patients with encephalitis with anti-NMDAR, anti-AMPAR and anti-DPPX antibodies, in most cases the tests will show inflammatory changes in the cerebrospinal fluid supporting the diagnosis of an autoimmune disease. Unfortunately, this will not be the case for most patients with anti-LGI1 and anti-CASPR2 antibodies. However, in the case of suspected autoimmune encephalitis with anti-LGI1 and anti-CASPR2 antibodies in the elderly, the results of these tests should not lead to a decision to abandon the serum antineuronal antibody test [31, 32, 33, 34].
3. Autoimmune encephalitis and psychosis
Schizophrenia is a disease resulting from functional and structural changes in the brain. Psychopathological symptoms indicating a diagnosis of schizophrenia include disturbances in the course and content of thinking. They are characterized by the occurrence of delusions: of reference, of persecution, of influence. Commenting voices or echoes of thought often co-occur as well. Another characteristic symptom of the disease are negative symptoms. The risk of occurrence in the general population is 1-1.5%. [1,2]. However, single psychotic episodes (psychotic like expirience – PLE) may affect as many as 5-8% of the population [3].
Psychosis is a mental disorder in which the patient experiences disturbances in perceiving reality, and sometimes also consciousness, as a result of which he is unable to maintain a critical attitude towards realism. Psychosis can manifest itself in primary psychotic disorders, neurological diseases and disease states [4]. Thus, the positive symptoms presented by the patient are not always the first manifestation of schizophrenia. Autoimmune encephalitis is an example of diseases in which psychotic symptoms are not uncommon. The first-time symptoms of autoimmune encephalitis with anti-NMDAR antibodies include: delirium, amnesia and epileptic seizures. Symptoms from the spectrum of psychopathology are also characteristic, such as: mood disorders, behavioral disorders, psychosis or catatonia.
Psychosis is a serious mental disorder that is characterized by frequent delusions and hallucinations. Its special feature is defective or completely lost contact with reality, which is associated with a completely different interpretation and perception of reality than in the case of healthy people. Loss of contact with reality is manifested in psychosis by hallucinations and delusions as well as disorganization in the way of expressing emotions, behavior, thinking and communicating. In the course of autoimmune encephalitis with anti-NMDAR antibodies, the mental status of the patient changes depending on the severity of the inflammatory changes and the duration of the disorder. In the initial period, only non-specific prodromal symptoms are observed, indicating the onset of the disease, before specific symptoms occur, which appear as early as 1-2 weeks after diagnosis and intensification of inflammation. The emerging psychosis is characterized by a number of psychiatric symptoms, among which the most common are delusions, hallucinations, mania, anxiety, speech disorders, catatonia, abulia, anhedonia, insomnia and frequent epileptic seizures. As neurological complications, movement disorders, dysautonomia (fluctuations in blood pressure and heart rate), hypoventilation and seizures may occur simultaneously. These symptoms prove that emerging psychosis does not have to be a symptom of schizophrenia, depression, dementia, bipolar affective disorder or addiction to psychoactive substances, and may be the result of Autoimmune Encephalitis [35, 36].
4. Relationship between autoimmune encephalitis and neoplastic diseases and paraneoplastic syndromes
Malignancies, usually ovarian teratoma and herpetic encephalitis, are known triggers of NMDAR autoimmunity. The humoral response, which is the basis of the pathophysiology of autoimmune encephalitis, leading to the production of antineuronal antibodies by plasma cells directed against their surface antigens, e.g. NMDAR, is important not only in the diagnosis of these neurological disorders, but also allows to estimate the risk of cancer. Thus, anti-neuronal antibodies make it possible to assess the risk of cancer in the course of autoimmune encephalitis, and some of them have a significant relationship with specific cancers. The presence of specific antibodies in Autoimmune Encephalitis may indicate a specific type of tumor and may lead to improvement or stabilization of symptoms related to its treatment. On the other hand, in the case of the paraneoplastic nature of the disease, diagnosis based on antineuronal antibodies facilitates the targeting of the cancer search.
Clinically, paraneoplastic encephalitis may not be distinct from non-paraneoplastic encephalitis. For this reason, when a patient is diagnosed with autoimmune encephalitis, targeted oncology diagnostics should be performed. Autoimmune encephalitis may be paraneoplastic or, in a small number of cases, be unrelated to cancer. In adults, the presence of an antibody against anti-Hu intracellular antigens is almost always associated with an existing tumor. In addition to it, anti-neuronal antibodies with a high risk of cancer include: anti-Ri, anti-Yo, anti-Ma2/Ta, anti-CV2, anti-amphiphysin. According to Gultekin et al. [37], the most common types of cancer associated with the course of autoimmune encephalitis include:
- Lung cancer, with an incidence of 50% of patients with autoimmune encephalitis, of which 40% are Small Cell Lung Cancer, 10% are Non-Small Cell Lung Cancer
- Testicular tumors, with an incidence of 20% of patients with autoimmune encephalitis
- Breast cancer, with an incidence of 8% of patients with autoimmune encephalitis
- Ovarian teratoma, with an incidence of 4% of patients with autoimmune encephalitis
- Hodgkin's disease, with an incidence of 4% of patients with autoimmune encephalitis
- Thymus, with an incidence of 2% of patients with autoimmune encephalitis
- Other cancers, with an incidence of 8% of patients with autoimmune encephalitis
According to the same authors, only 4% of patients who are found to have any anti-neuronal antibodies, thus confirming Autoimmune Encephalitis, are not affected by any type of cancer.
Antibodies directed against intracellular antigens, apart from the targeted diagnosis of autoimmune encephalitis, also allow to estimate the occurrence of classic paraneoplastic disorders. In turn, other most common antibodies against surface antigens, such as anti-LGI1 or anti-CASPR2, are associated with typical non-paraneoplastic forms of limbic encephalitis [38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50].
Also worth mentioning is the encephalopathy associated with Hashimoto's disease. This is a controversial and poorly understood disease entity with a still unclear etiology. The incidence is estimated at 2.1/100,000, with a significant predisposition among adults between the fourth and sixth decades of life, with a definite predominance among women (4:1) than men [51]. The substrate of the disease is most likely based on autoimmune processes. Basic laboratory tests usually show no significant abnormalities. TSH levels are within normal limits, and only about 30% of patients have hypothyroidism. Nevertheless, elevated serum anti-TPO and/or anti-TGAb levels are noted in every patient [52,53]. Moreover, in about 62-75% of patients, antibodies, characteristic of autoimmune encephalitis, such as anti-NMDAR, anti-GABAAR, anti-Caspr2, anti-LGi1 or anti-AMPAR, are found in the cerebrospinal fluid [54,55].
5. Diagnostics of autoimmune encephalitis in adults and children
According to the latest recommendations from 2021 [56], when autoimmune encephalitis is clinically suspected, the procedure begins with brain imaging and cerebrospinal fluid (CSF) analysis. One of the key elements of diagnostics is testing for the presence of antineuronal antibodies, not only in the cerebrospinal fluid, but above all in the blood serum. Although there is a marked intrathecal synthesis of anti-N-methyl-d-aspartate receptor antibodies, absolute levels of anti-N-methyl-d-aspartate receptor antibodies are generally higher in serum than in cerebrospinal fluid.
However, the diagnostic procedure is different in children and adults.
The diagnostic algorithm for autoimmune encephalitis in adults first involves confirming focal or multifocal brain pathology suggestive of autoimmune encephalitis [56]. For this purpose, an MRI examination with or without contrast is performed. If the MRI result is negative, or if the patient has encephalopathy or has frequent seizures, an EEG is then performed. If the result of the MRI test is negative and the diagnosis after the initial tests is still unclear, the FDG-PET test is performed in turn. In the next stage of the diagnostic procedure, the inflammatory etiology should be confirmed and other diagnoses excluded. For this purpose, we perform a CSF test including anti-neuronal antibody testing and a blood test that includes anti-neuronal antibody testing. If the diagnosis is still unclear, a brain biopsy is needed. The final step in the diagnostic procedure is cancer screening. For this purpose, we perform a CT scan of the chest, abdomen and pelvis, mammography/MRI of the breast and ultrasound examination of the pelvis or testicles. In the event of negative results, we perform the FDG-PET test.
Pediatric encephalitis should be diagnosed based on the clinical picture and additional tests, including anti-neuronal antibodies [57, 58]. Thus, the diagnostic algorithm for autoimmune encephalitis in children first includes the verification of the results of basic tests, imaging and anti-neuronal antibodies in order to determine their relationship with autoimmune encephalitis. In the case of negative results, there is a need to consider other causes of symptoms in a pediatric patient with a primary suspicion of symptoms of autoimmune encephalitis. In case of positive results, it should be verified whether the present antibodies are related to pediatric autoimmune encephalitis: anti-NMDAR, anti-MOG, anti-GAD65, anti-GABAA/BR, anti-GlyR, anti-m-GluR5, anti- dopamine receptor. Negative results are likely to be non-antibody pediatric encephalitis. If the result is positive, pediatric antibody-associated encephalitis is certain.
In the diagnosis of anti-neuronal antibodies when autoimmune encephalitis is suspected, the gold standard is an indirect immunofluorescence test (IIFT) or an immunohistochemical method using animal tissues as a substrate, and then performing highly specific tests to confirm - immunoblot for most antibodies against intracellular antigens or cellular tests, so-called cell-based assay (CBA), for antibodies directed against surface or synaptic antigens. Currently, the CBA test, which is a modification of the indirect immunofluorescence method, is quite commonly used. In this assay, cells transfected with selected target antigens for anti-neuronal antibodies are used as a substrate. The positive reaction is the characteristic fluorescence of cells transfected with primary specific human autoantibodies and fluorescein-labeled secondary anti-human antibodies, which allows differentiation from non-specific reactions and obtaining highly reliable results.
In the study and differentiation of the pathophysiology of autoimmune encephalitis, comprehensive panel studies of antineuronal antibodies are recommended, taking into account the importance of antineuronal antibodies of the IgG class only. This diagnosis is based on qualitative indirect immunofluorescence (IFA) tests for the detection of anti-NMDAR IgG. High levels of these antibodies correlate with disease severity and variable response to treatment. The study of antineuronal autoantibodies in suspected autoimmune encephalitis is of unquestionable importance. It allows to identify the subtype of autoimmune encephalitis, is a prognostic factor regarding the prognosis and success of therapy, enabling its monitoring. Currently, it is recommended to perform antineuronal antibody tests with a high clinical suspicion of Autoimmune Encephalitis, even in the case of normal results of the basic CSF test. According to the recommendations, the sensitivity and specificity of the analysis in serum or cerebrospinal fluid differ depending on the tested antineuronal antibodies, therefore it is recommended to perform the test in both samples [59]: "In the case of suspected autoimmune or paraneoplastic encephalitis associated with the presence of antibodies on the surface of neurons, CSF screening should be mandatory” [1, 61, 62, 63, 64, 65, 66].
6. Summary
In recent years, autoimmune encephalitis is increasingly recognized as one of the causes of epilepsy, especially drug-resistant epilepsy. The cause of this disorder are autoantibodies directed against antigens, which are ion channels, receptors and other synaptic proteins involved in neuronal transmission and brain plasticity, sometimes also in cytotoxic processes. Autoimmune encephalitis with the antibodies listed in the article can manifest itself in many ways. It is not uncommon for many different symptoms, both neurological and psychiatric, to occur. The clinical picture of autoimmune encephalitis with the presence of antibodies varies depending on their subtype and individual factors.
In the last decade, significant progress has been made in the diagnosis of autoimmune encephalitis. With effective differential diagnosis, levels of evidence of autoimmune encephalitis (possible, probable or certain) with a specific antibody subtype are obtained, which can lead to the implementation of rapid immunotherapy. Early diagnosis and early initiation of targeted treatment increases the chance of a successful therapeutic process and may help patients achieve a good prognosis. However, in order to improve the diagnosis and treatment of autoimmune encephalitis, further research is needed to develop more sensitive diagnostic tools, identify prognostic biomarkers and implement new treatments that significantly accelerate recovery.
List of abbreviations used
| MRI | magnetic resonance imaging |
| EEG | electroencephalography |
| FDG-PET | fluorodeoxyglucose-positron emission tomography |
| CT | computed tomography |
References
- Gałecki P., Szulc A., Psychiatry, Edra Urban & Partner, Wroclaw, 2018, s. 159.
- Gałecki P., Mental state examination, ICD-11 Criteria, Edra Urban & Partner, Wroclaw, 2022, s. 63-88.
- Granerod J., Ambrose H.E., Davies N.W. i wsp.: Causes of encephalitis and differences in their clinical presentations in England: a multicentre, population-based prospective study. Lancet In- fect. Dis. 2010; 10: 835–844. [CrossRef]
- Alloza C., Blesa-Cábez M., Bastin M.E., Madole J.W., Buchanan C.R., Janssen J., Gibson J., Deary I.J., Tucker-Drob E.M., Whalley H.C., Arango C., McIntosh A.M., Cox S.R., Larie S.M., Psychotic-like experiences, polygenic risk scores for schizophrenia, and structural properties of the salience, default mode, and central-executive networks in healthy participants from UK Biobank, Transl Psychiatry, 2020 Apr 27;10(1):122. [CrossRef]
- Julayanont P, Suryadevara U. Psychosis. Continuum (Minneap Minn). 2021 Dec 1;27(6):1682-1711. [CrossRef]
- Dalmau J., Graus F.: Antibody-Mediated encephalitis. N. Engl. J. Med. 2018; 378: 840–851. [CrossRef]
- Zuliani L. et al. Central nervous system neuronal surface antibody associated syndromes: review and guidelines for recognition. Journal of Neurology, Neurosurgery & Psychiatry 83.6 (2012): 638–645. [CrossRef]
- Newman M.P., Blum S., Wong R.C. i wsp.: Autoimmune encephalitis. Intern. Med. J. 2016; 46(2): 148–157. [CrossRef]
- Ramanathan S., Al-Diwani A., Waters P. i wsp.: The autoantibody-mediated encephalitides: from clinical observations to molecular pathogenesis. J. Neurol. 2021; 268: 1689–1707. [CrossRef]
- Wandinger K.P. et al. Multiparametric serological testing in autoimmune encephalitis using recombinant immunofluorescence cell substrates and EUROTIDE technology. Scientific presentation at the 10th Dresden Symposium on Autoantibodies. Dresden 2011.
- Graus F., Titulaer M.J., Balu R. i wsp.: A clinical approach to diagnosis of autoimmune encephalitis. Lancet Neurol. 2016; 15: 391–404. [CrossRef]
- Dalmau J, Tüzün E, Wu Hy, et al. Paraneoplastic anti-N-methyl-D-aspartate receptor encepha- litis associated with ovarian teratoma. Ann Neurol. 2007; 61(1): 25–36, indexed in Pubmed: 17262855. [CrossRef]
- Dalmau J, Lancaster E, Martinez-Hernandez E, et al. Clinical experience and laboratory investigations in patients with anti-NMDAR encephalitis. Lancet Neurol. 2011; 10(1): 63–74, indexed in Pubmed: 21163445. [CrossRef]
- Lai M., Hughes E.G., Peng X. i wsp.: AMPA receptor antibodies in limbic encephalitis alter synaptic receptor location. Ann. Neurol. 2009; 65: 424–434. [CrossRef]
- Huang Q, Xie Y, Hu Z, Tang X. Anti-N-methyl-D-aspartate receptor encephalitis: A review of pathogenic mechanisms, treatment, prognosis. Brain Res. 2020 Jan. [CrossRef]
- Al-Diwani A., Handel A., Townsend L. i wsp.: The psychopathology of NMDAR-antibody encephalitis in adults: a systematic review and phenotypic analysis of individual patient data. Lan- cet Psychiatry 2019; 6: 235–246. [CrossRef]
- Varley J.A., Andersson M., Grant E. i wsp.: Absence of neuronal autoantibodies in neuropsychiatric systemic lupus erythematosus. Ann. Neurol. 2020; 88: 1244–1250. [CrossRef]
- Lai M, Hughes EG, Peng X, Zhou L, Gleichman AJ, Shu H i wsp. AMPA receptor antibodies in limbic encephalitis alter synaptic receptor location. Ann Neurol 2009;65: 424-34. [CrossRef]
- Omi T, Kinoshita M, Nishikawa A, Tomioka T, Ohmori K, Fukada K, Matsunaga H. Clinical Relapse of Anti-AMPAR Encephalitis Associated with Recurrence of Thymoma. Intern Med. 2018 Apr 1;57(7):1011-1013. [CrossRef]
- Song W, Li K, Li J, Liu X, Wu X, Xu X, Xiong K, Chen X, Zhang Y. Thymoma-associated autoimmune encephalitis: Analysis of factors determining prognosis. CNS Neurosci Ther. 2023 May;29(5):1213-1221. [CrossRef]
- Zhang TY, Cai MT, Zheng Y, Lai QL, Shen CH, Qiao S, Zhang YX. Anti-Alpha-Amino-3-Hydroxy-5-Methyl-4-Isoxazolepropionic Acid Receptor Encephalitis: A Review. Front Immunol. 2021 May 21;12:652820. 21 May. [CrossRef]
- McCombe JA, Zivelonghi C, Vorasoot N, Majed M, Flanagan EP, Dubey D, Pittock SJ, McKeon A, Zekeridou A. AMPAR autoimmunity: Neurological and oncological accompaniments and co-existing neural autoantibodies. J Neuroimmunol. 2023 Feb 15;375:578012. [CrossRef]
- Li X, Mao YT, Wu JJ, Li LX, Chen XJ. Anti-AMPA receptor encephalitis associated with thymomatous myasthenia gravis. J Neuroimmunol. 2015 Apr 15;281:35-7. [CrossRef]
- Joubert B, Kerschen P, Zekeridou A, Desestret V, Rogemond V, Chaffois MO, Ducray F, Larrue V, Daubail B, Idbaih A, Psimaras D, Antoine JC, Delattre JY, Honnorat J. Clinical Spectrum of Encephalitis Associated With Antibodies Against the α-Amino-3-Hydroxy-5-Methyl-4-Isoxazolepropionic Acid Receptor: Case Series and Review of the Literature. JAMA Neurol. 2015 Oct;72(10):1163-9. [CrossRef]
- Spatola M, Stojanova V, Prior JO, Dalmau J, Rossetti AO. Serial brain ¹⁸FDG-PET in anti-AMPA receptor limbic encephalitis. J. Neuroimmunol 2014;271(1-2):53-5. [CrossRef]
- Shahrizaila N, Yuki N. Bickerstaff brainstem encephalitis and Fisher syndrome: anti-GQ1b antibody syndrome. J Neurol Neurosurg Psychiatry. 2013 May;84(5):576-83. [CrossRef]
- Yoshikawa K, Kuwahara M, Morikawa M, Kusunoki S. Bickerstaff brainstem encephalitis with or without anti-GQ1b antibody. Neurol Neuroimmunol Neuroinflamm. 2020 Sep 15;7(6):e889. [CrossRef]
- Piepgras J, Höltje M, Michel K, Li Q, Otto C, Drenckhahn C, Probst C, Schemann M, Jarius S, Stöcker W, Balint B, Meinck HM, Buchert R, Dalmau J, Ahnert-Hilger G, Ruprecht K. Anti-DPPX encephalitis: pathogenic effects of antibodies on gut and brain neurons. Neurology. 2015 Sep 8;85(10):890-7. [CrossRef]
- Xiao J, Fu PC, Li ZJ. Clinical and imaging analysis to evaluate the response of patients with anti-DPPX encephalitis to immunotherapy. BMC Neurol. 2022 Apr 5;22(1):129. [CrossRef]
- Seery N, Butzkueven H, O'Brien TJ, Monif M. Rare antibody-mediated and seronegative autoimmune encephalitis: An update. Autoimmun Rev. 2022 Jul;21(7):103118. [CrossRef]
- Seery N, Butzkueven H, O'Brien TJ, Monif M. Contemporary advances in antibody-mediated encephalitis: anti-LGI1 and anti-Caspr2 antibody (Ab)-mediated encephalitides. Autoimmun Rev. 2022 May;21(5):103074. [CrossRef]
- Ghimire P, Khanal UP, Gajurel BP, Karn R, Rajbhandari R, Paudel S, Gautam N, Ojha R. Anti-LGI1, anti-GABABR, and Anti-CASPR2 encephalitides in Asia: A systematic review. Brain Behav. 2020 Oct;10(10):e01793. [CrossRef]
- Guo YP, Li XY, Liu HF, Zhang M, Shi L, Zhao XJ, Li JZ, Liu XY, Cui J. [Clinical analysis of 7 cases with anti-Caspr2 antibody-associated autoimmune encephalitis]. Zhonghua Yi Xue Za Zhi. 2020 Feb 25;100(7):513-515.
- van Sonderen A, Petit-Pedrol M, Dalmau J, Titulaer MJ. The value of LGI1, Caspr2 and voltage-gated potassium channel antibodies in encephalitis. Nat Rev Neurol. 2017 May;13(5):290-301. [CrossRef]
- Endres D, Leypoldt F, Bechter K, Hasan A, Steiner J, Domschke K, Wandinger KP, Falkai P, Arolt V, Stich O, Rauer S, Prüss H, van Elst LT. Autoimmune encephalitis as a differential diagnosis of schizophreniform psychosis: clinical symptomatology, pathophysiology, dignostic ap- proach, and therapeutic considerations. Eur Arch Psychiatry Clin Neurosci. 2020 Oct;270(7):803- 818. [CrossRef]
- Beattie M, Goodfellow J, Oto M, Krishnadas R. Anti-NMDAR encephalitis for psychiatrists: the essentials. BJPsych Bull. 2021 Jun 2;46(4):1-7. [CrossRef]
- Gultekin S.H., et.al. Paraneoplastic limbic encephalitis: neurological symptoms, immunological findings and tumour association in 50 patients. Brain 123 (2000): 1481–1494. [CrossRef]
- Dalmau J, Tüzün E, Wu HY, Masjuan J, Rossi JE, Voloschin A, Baehring JM, Shimazaki H, Koide R, King D, Mason W, Sansing LH, Dichter MA, Rosenfeld MR, Lynch DR. Paraneoplastic anti-N-methyl-D-aspartate receptor encephalitis associated with ovarian teratoma. Ann Neurol. 2007 Jan;61(1):25-36. [CrossRef]
- Titulaer MJ, McCracken L, Gabilondo I, Armangué T, Glaser C, Iizuka T, Honig LS, Benseler SM, Kawachi I, Martinez-Hernandez E, Aguilar E, Gresa-Arribas N, Ryan-Florance N, Torrents A, Saiz A, Rosenfeld MR, Balice-Gordon R, Graus F, Dalmau J. Treatment and prognostic factors for long-term outcome in patients with anti-NMDA receptor encephalitis: an observational cohort study. Lancet Neurol. 2013 Feb;12(2):157-65. [CrossRef]
- Dalmau J, Gleichman AJ, Hughes EG, Rossi JE, Peng X, Lai M, Dessain SK, Rosenfeld MR, Balice-Gordon R, Lynch DR. Anti-NMDA-receptor encephalitis: case series and analysis of the effects of antibodies. Lancet Neurol. 2008 Dec;7(12):1091-1098. [CrossRef]
- Kayser MS, Dalmau J. Anti-NMDA Receptor Encephalitis in Psychiatry. Curr Psychiatry Rev. 2011;7(3):189-193. [CrossRef]
- Hughes EG, Peng X, Gleichman AJ, Lai M, Zhou L, Tsou R, Parsons TD, Lynch DR, Dalmau J, Balice-Gordon RJ. Cellular and synaptic mechanisms of anti-NMDA receptor encephalitis. J Neurosci. 2010 Apr 28;30(17):5866-5875. [CrossRef]
- Kayser MS, Titulaer MJ, Gresa-Arribas N, Dalmau J. Frequency and characteristics of isolated psychiatric episodes in anti–N-methyl-d-aspartate receptor encephalitis. JAMA Neurol. 2013 Sep 1;70(9):1133-9. [CrossRef]
- Lejuste F, Thomas L, Picard G, Desestret V, Ducray F, Rogemond V, Psimaras D, Antoine JC, Delattre JY, Groc L, Leboyer M, Honnorat J. Neuroleptic intolerance in patients with anti-NMDAR encephalitis. Neurol Neuroimmunol Neuroinflamm. 2016 Aug 29;3(5):e280. [CrossRef]
- de Bruijn MAAM, van Sonderen A, van Coevorden-Hameete MH, Bastiaansen AEM, Schreurs MWJ, Rouhl RPW, van Donselaar CA, Majoie MHJM, Neuteboom RF, Sillevis Smitt PAE, Thijs RD, Titulaer MJ. Evaluation of seizure treatment in anti-LGI1, anti-NMDAR, and anti-GABABR encephalitis. Neurology. 2019 May 7;92(19):e2185-e2196. 7 May.
- Sansing LH, Tüzün E, Ko MW, Baccon J, Lynch DR, Dalmau J. A patient with encephalitis associated with NMDA receptor antibodies. Nat Clin Pract Neurol. 2007 May;3(5):291-296. [CrossRef]
- Martinez-Hernandez E, Horvath J, Shiloh-Malawsky Y, Sangha N, Martinez-Lage M, Dalmau J. Analysis of complement and plasma cells in the brain of patients with anti-NMDAR encephalitis. Neurology. 2011 Aug 9;77(6):589-593. [CrossRef]
- Dalmau J., Lancaster E., Martinez-Hernandez E., Rosenfeld M.R., Balice-Gordon R. Clinical experience and laboratory investigations in patients with anti-NMDAR encephalitis.. The Lancet Neurology, 10 (1),2011: 63-74. [CrossRef]
- Irani SR, Bera K, Waters P, Zuliani L, Maxwell S, Zandi MS, Friese MA, Galea I, Kullmann DM, Beeson D, Lang B, Bien CG, Vincent A. N-methyl-D-aspartate antibody encephalitis: temporal progression of clinical and paraclinical observations in a predominantly non-paraneoplastic disorder of both sexes. Brain. 2010 Jun;133(Pt 6):1655-1667. [CrossRef]
- Iizuka T, Yoshii S, Kan S, Hamada J, Dalmau J, Sakai F, Mochizuki H. Reversible brain atrophy in anti-NMDA receptor encephalitis: a long-term observational study. J Neurol. 2010 Oct;257(10):1686-91. [CrossRef]
- Mocellin R., Walterfang M., Velakoulis D. Hashimoto’s encephalopathy: Epidemiology, pathogenesis and management. CNS Drugs. 2007;21:799–811. [CrossRef]
- Weetman, A.P. An update on the pathogenesis of Hashimoto’s thyroiditis. J. Endocrinol. Invest. 2021;44:883–890. [CrossRef]
- Tzakas P., Sit S.W. Progressive impairment of cognition and motor function: Hashimoto encephalopathy. CMAJ. 2011;183:E495–E497. [CrossRef]
- Kishitani T., Matsunaga A., Ikawa M., Hayashi K., Yamamura O., Hamano T., Watanabe O., Watanabe O., Nakamoto Y., Yoneda M. Limbic encephalitis associated with anti-NH2-terminal of α-enolase antibodies: A clinical subtype of Hashimoto encephalopathy. Medicine. 2017. [CrossRef]
- Waliszewska-Prosół M, Ejma M. Hashimoto Encephalopathy-Still More Questions than Answers. Cells. 2022 Sep 14;11(18):2873. [CrossRef]
- Abboud, H. Autoimmune encephalitis: proposed best practice recommendations for diagnosis and acute management. Journal of Neurology, Neurosurgery & Psychiatry 92(7)2021: 757–768. [CrossRef]
- Cellucci, T. Clinical approach to the diagnosis of autoimmune encephalitis in the pediatric patient. Neurology – Neuroimmunology Neuroinflammation 7(2), 2020. [CrossRef]
- Knurowska A., Zawadzka M., Anuszkiewicz K., Stogowski P., Mazurkiewicz-Beldzińska M. Autoimmune encephalitis with anti-NMDA antibodies in the pediatric population - literature review and case report. Pol. Przegl. Neurol 2020;16(4):239-243.
- Graus, F. et al. Updated Diagnostic Criteria for Paraneoplastic Neurologic Syndromes. Neurology – Neuroimmunology Neuroinflammation, 8(4), 2021. [CrossRef]
- Bacchi S, Franke K, Wewegama D, Needham E, Patel S, Menon D. Magnetic resonance imaging and positron emission tomography in anti-NMDA receptor encephalitis: A systematic review. J Clin Neurosci. 2018 Jun;52:54-59. [CrossRef]
- Suh-Lailam BB, Haven TR, Copple SS, Knapp D, Jaskowski TD, Tebo AE. Anti-NMDA-receptor antibody encephalitis: performance evaluation and laboratory experience with the anti-NMDA-receptor IgG assay. Clin Chim Acta. 2013 Jun 5;421:1-6. [CrossRef]
- Armangue T, Leypoldt F, Málaga I, Raspall-Chaure M, Marti I, Nichter C, Pugh J, Vicente-Rasoamalala M, Lafuente-Hidalgo M, Macaya A, Ke M, Titulaer MJ, Höftberger R, Sheriff H, Glaser C, Dalmau J. Herpes simplex virus encephalitis is a trigger of brain autoimmunity. Ann Neurol. 2014 Feb;75(2):317-323. [CrossRef]
- Graus F., Titulaer M.J., Balu R., Benseler S., Bien C.G., Cellucci, T. A clinical approach to diagnosis of autoimmune encephalitis. The Lancet Neurology, 15 (4),2016: 391-404. [CrossRef]
- Scheibe F, Prüss H, Mengel AM, Kohler S, Nümann A, Köhnlein M, Ruprecht K, Alexander T, Hiepe F, Meisel A. Bortezomib for treatment of therapy-refractory anti-NMDA receptor encephalitis. Neurology. 2017 Jan 24;88(4):366-370. [CrossRef]
- Gable MS, Sheriff H, Dalmau J, Tilley DH, Glaser CA. The frequency of autoimmune N-methyl-D-aspartate receptor encephalitis surpasses that of individual viral etiologies in young individuals enrolled in the California Encephalitis Project. Clin Infect Dis. 2012 Apr;54(7):899-904. [CrossRef]
- Dalmau J, Armangué T, Planagumà J, Radosevic M, Mannara F, Leypoldt F, Geis C, Lancaster E, Titulaer MJ, Rosenfeld MR, Graus F. An update on anti-NMDA receptor encephalitis for neurologists and psychiatrists: mechanisms and models. Lancet Neurol. 2019 Nov;18(11):1045-1057. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



