
Submitted:
26 July 2023
Posted:
27 July 2023
You are already at the latest version
Abstract
Background: Recently the role of nutraceutical compounds in the prevention of human diseases is rapidly increasing. Here, we aim to evaluate the beneficial effect of dietary supplementation with seven active principles, lycopene, sulphoraphane, silymarin, glutathione, escin, tryptophan, green tea catechins, on human health. Methods: An extensive search of PubMed and Medline database was performed with the following keywords: “silymarin”, “sulforaphane”, “lycopene”, “green tea catechins”, “tryptophan”, “glutathione” and “escin” accompanied by the keywords “supplement”, “supplementation”, “nutraceutics”. All pre-clinical and clinical trials have been considered for this review. Results: One-hundred and eighteen full-text articles were eligible for inclusion in this review. The papers examined presented considerable variability due to the wide heterogeneity of dosages administered, population involved and outcomes pursued. Conclusion: Nutritional supplementation with lycopene, sulphoraphane, silymarin, glutathione, escin, tryptophan and green tea catechins appears to exert a wide range of benefits on human health, ranging from mood and cognition to cardiovascular health, fertility, metabolism, antioxidant and anti-inflammatory capabilities, potential anti-cancer effects. Further studies are required to better define the potential synergic effect, optimal dosage, mechanism of action and tolerability profile of these substances.
Keywords:
sulphoraphane
; silymarin
; lycopene
; glutathione
; escin
; tryptophan
; green tea
; men health
; prevention
1. Introduction
Nowadays, dietary supplementation is a widespread practice which involves not only patients affected by actual diseases, but also healthy population. Over 50% of adults in the US regularly include some form of supplement intake in their daily routine [1]. Reasons for supplementation may range from a general intention to “stay healthy” and prevent diseases – cancer in particular – to addressing specific needs tied to known medical conditions or deficits [2]. Furthermore, the user almost always chooses the supplement as a “self-prescription”, rarely consulting a doctor before purchase [3].
There is an enormous amount of substances and actives of natural origin that are known for their purported health benefits, and the aim of this review is to narratively summarize the properties of seven particular principles which commonly recur in commercially available supplements and present some interest in the fields of not only urology and andrology, but also general well-being and prevention of oxidative-stress damage consequent to pollutants environmental exposure.
The chosen substances are: Sulforaphane, Lycopene, Escin, Silymarin, Glutathione, Green Tea and Tryptophan. There are multiple reasons for the choice of these seven particular substances. Firstly, they all have the common trait of having systemic wellness effects that could be useful for almost any patient regardless of age and comorbidity. Moreover, when used as supplements with adequate dosage, they have not shown relevant side-effects. Finally, their combined use in a single tablet could be possible due to their non-competitive and potentially synergistic mechanisms of action.
1.1. Research Questions
We put forth this research query:
Is dietary supplementation with silymarin, sulforaphane, lycopene, green tea catechins, tryptophan, glutathione and escin able to protect the human health, increase fertility and prevent aging disease?
In order to respond to these research questions, we performed a narrative review of all available studies performed with the aim to evaluate the efficacy of a dietary supplementation with silymarin, sulforaphane, lycopene, green tea catechins, tryptophan, glutathione and escin in the human health benefit.
2. Materials and Methods
2.1. Research Strategy and Literature Search
From January to March 2023, three independent reviewers (C.d.A., F.S., C.V.) performed the research in PubMed database, Cochrane CENTRAL and Scopus. All disagreements between the two reviewers were resolved by three experienced supervisors (F.P., T.C., A.P.). All references cited in relevant articles were also reviewed and analyzed. Considering the extent of the literature published on the subject in general and on each of the active substances in particular, the authors saw fit to present the results of this review in a narrative fashion. Systematic or meta-analytical comparison of so heterogeneous outcomes in measurements, population and methodology is beyond the scope of this work. The reaserch strategy includes the following keywords: “silymarin”, “sulforaphane”, “lycopene”, “green tea catechins”, “tryptophan”, “glutathione” and “escin” accompanied by the keywords “supplement”, “supplementation”, “nutraceutics”. Only papers in English language were included. Randomized controlled trials (RCTs), quasi-RCTs, non-randomized trials were included as priority, whereas prospective and retrospective cohort studies, case-control studies were included in case of significant results or population numbers. Case reports and case series were excluded. Pre-clinical and in-vitro evidence was examined and presented in the case of lack of significant clinical evidence for certain substances.
3. Results
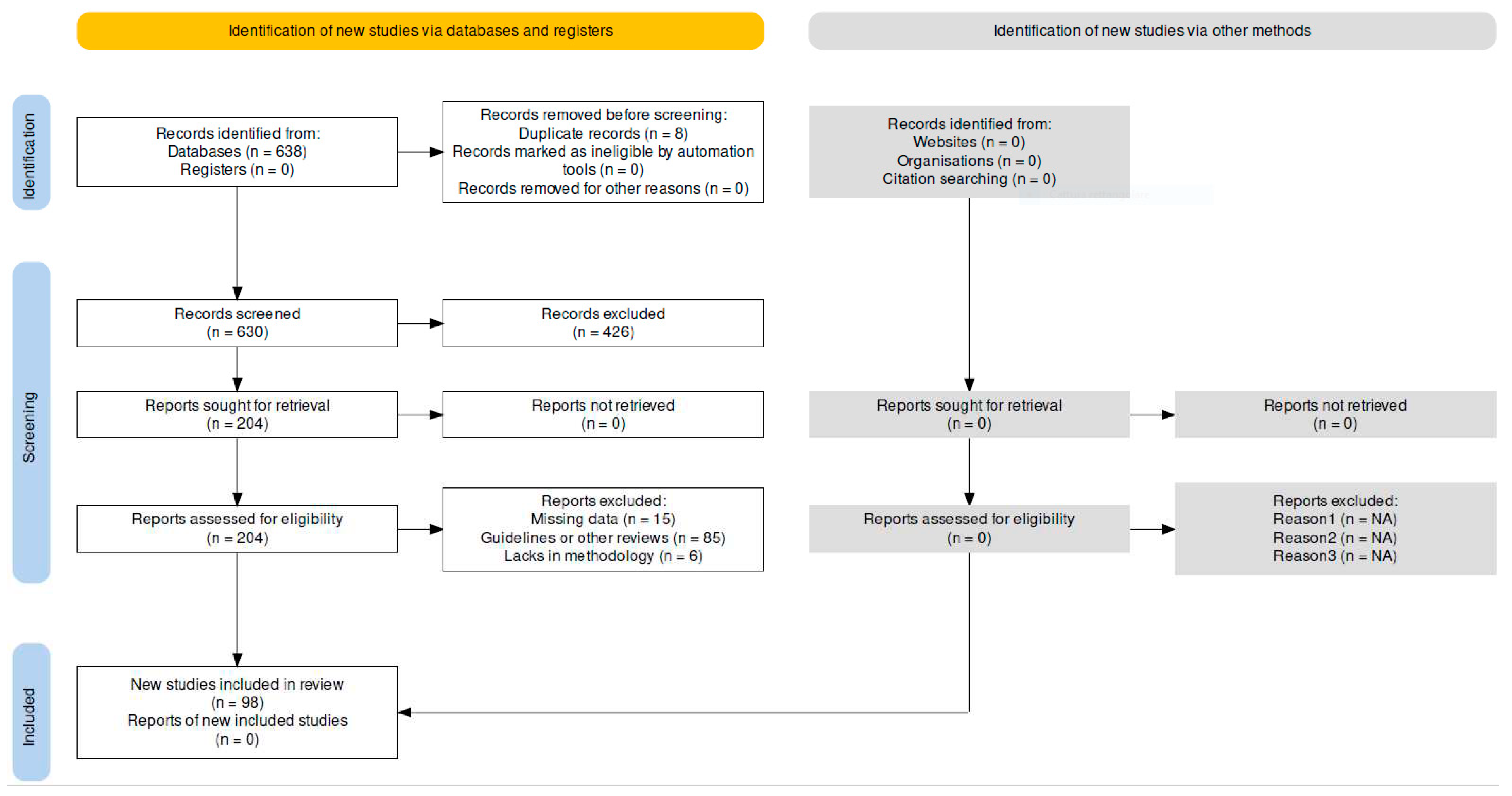
A total of 98 papers were included in this review: 7 for silymarin, 21 for sulforaphane, 9 for lycopene, 33 for green tea catechins, 12 for tryptophan, 4 for glutathione and 12 for escin. Of these, 39 were pre-clinical evidence papers and the remaining 59 were clinical trials. Amongst clinical trials papers, 50 were RCTs, 7 were non-RCTs and 2 were case-control studies.
Figure 1.
The figure shows the papers’ selection process according to PRISMA recommendations.
The Table 1 summarize the relevant findings according to the compounds.
| Substance | Reference | Specie |
Level of Evidence |
Dose & Duration |
Main Conclusions |
Clinical field of significance |
| Green tea | (47) | Human | RCT | 50 or 100 or 200 mg, single dose | Highest dose significantly increases excretion of cancerogen acrylamide | Antioxidant activity |
| (48) | Human | Non-RCT | 300 mg/day for 14 days | Slight decrease in plasma leukocyte count, significant increase in antioxidant status | ||
| (49) | Human | RCT | 1 cup single dose or 2 cups/day for 7 days | Increase in heme oxygenase-1 activity, decrease in lymphocytic DNA damage | ||
| (50) | Human | Non-RCT | 254 mg, single dose | Plasma PCOOH levels decreased with an inverse correlation to the increase in plasma EGCG levels | ||
| (51) | Human | RCT | 4 cups/day or 2 capsules/day for 8 weeks | Decrease in SAA levels | ||
| (52) | Human | RCT | 4 cups/day for 16 weeks | Decrease in urinary 8-OHdG levels in heavy smokers with mutations of glutathione-S-transferase | ||
| (53) | Human | RCT | 800 mg/day for 6 weeks | Beneficial period x treatment interaction in terms of body weight control in overweight subjects | Metabolism & cardiovascular health | |
| (54) | Human | RCT | 4 cups/day or 2 capsules/day for 8 weeks | Significant decrease in body weight and BMI | ||
| (55) | Human | RCT | 456 mg/day for 8 weeks | Mild changes in insulin level | ||
| (56) | Human | RCT | 630 mg/day for 14 weeks | Reduction in cholesterol levels | ||
| (57) | Human | RCT | 400 mg/day or 800 mg/day for 8 weeks | Reduction in LDL cholesterol and glucose-related markers | ||
| (58) | Human | RCT | 100 mg/day for 4 weeks | Improvements in insulin resistance | ||
| (59) | Human | RCT | 1450 mg, single dose | Reduction in some circulating catecholamines | ||
| (60) | Human | RCT | 1500 mg/day for 16 weeks | Within-group reduction in waist circumference, HOMA-IR index, insulin level; increase in ghrelin level | ||
| (61) | Human | RCT | 456 mg/day for 8 weeks | Reduction in HbA1c levels, borderline significant reduction in blood diastolic pressure | ||
| (62) | Human | RCT | 350 mg/day for 7 days | Reduction in insulin levels | ||
| (63) | Human | RCT | 800 mg/day for 8 weeks | Reduction in blood diastolic pressure | ||
| (64) | Human | RCT | 540 mg/day for 24 weeks | Improvements in skeletal muscle mass in sarcopenic subjects | Physical performance | |
| (65) | Human | RCT | 250 mg/day for 4 weeks | No negative effects on endurance-training adaptation | ||
| (66) | Human | RCT | 570 mg/day for 8 weeks | Improvements in aerobic capacity during training | ||
| (67) | Human | RCT | 1500 mg/day for 10 weeks | Improvements in metabolic and antioxidant status during physical exercise | ||
| (68) | Human | RCT | 900 mg/day for 52 weeks | Reduction in incidence of relapsing metachronous colorectal adenomas | Anti-cancer activity | |
| (69) | Human | Case-control | >2 cups/day for >20 years | Significant decrease in incidence of de novo myelodysplastic syndromes | ||
| (70) | Human | RCT | 600 mg/day for 24 weeks | No effect in preventing PCa incidence | ||
| (71) | Human | RCT | 600 mg/day for up to 20 weeks | No effect in preventing PCa incidence | ||
| (72) | Human | Non-RCT | 6000 mg/day for a median of 4 weeks | No anti-neoplastic activity in PCa patients | ||
| (73) | Human | RCT | 600 mg/day for 52 weeks | No effect in preventing PCa incidence in HGPIN patients | ||
| (74) | Human | RCT | 400 mg/day for 52 weeks | No effect in preventing PCa incidence in HGPIN and ASAP patients | ||
| (75) | Human | RCT | 843 mg/day for 52 weeks | Reduction of mammographic density in women aged 50-55 | ||
| (78) | Human | RCT | 800 mg/day for 16 weeks | Absence of recurrence in 1/3 of treated women with ovarian cancer | ||
| (79) | Human | RCT | 800 mg/day for 16 weeks | No protective effect on CIN | ||
| (76) | Human | RCT | 200 mg/day for up to 12 weeks | Lower recurrence of CIN | ||
| (80) | Human | RCT | N/A | Higher clinical response in uVIN | ||
| Sylmarin | (9) | Human | RCT | 160 mg 4 tablets/day for 10 weeks | The dietary supplement utilized in this study was shown to delay PSA progression after potentially curative treatment in a significant fashion | Anti-cancer activity |
| (10) | Human | RCT | 570 mg/day for 24 weeks | The combination of this study significantly reduced two markers of lipid metabolism known to be associated with PCa progression | ||
| (11) | Human | RCT | 570 mg daily for 24 weeks | Improvement of IPSS score, urodynamic parameters: maximal rate of urine flow (Qmax), average flow (Qave), V and RV, total PSA value | Antioxidant | |
| Sulforaphane | (29) | Human | RCT | Two tablets containing 10 mg sulforaphane each, three times/day for 24 weeks | Median log PSA slopes were consistently lower in sulforaphane-treated men | Anti-cancer activity |
| (30) | Human | RCT | Two 100-μmol/day taken 12 h apart. Mean intervention period was 4.4 wk | The supplement was associated with significant interactions in gene expression among some genes that are related to PCa development | ||
| (31) | Human | RCT | A weekly 300 mL portion of soup made from a standard broccoli or from an experimental broccoli genotypes with enhanced concentrations of glucoraphanin | Changes in gene expression and associated oncogenic pathways were attenuated in men on the glucoraphanin-rich broccoli soup in a dose-dependent manner. | ||
| Lycopene | (36) | Human | Non-RCT | 10 mg/day | A significant and maintained effect on PSA velocity over 1 year was demostrated | Anti-cancer activity |
| (38) | Human | RCT | 4 mg twice a day for 52 weeks | Lycopene delay or prevent HGPIN from developing into occult prostate cancer | ||
| (40) | Human | RCT | 30 mg/day for 3 weeks | Three weeks supplementation lowers PSA in patients with non-metastatic prostate cancer | ||
| Escine | (115) | Human | RCT | 10 days | Reduction in pain, decrease in the dilatation of the urinary tract, effective expulsion of the stone | Urolithiasis |
| (118) | Human | RCT | 60 mg/day for 2 months | Improvement in sperm density and in sperm motility | Male Infertility | |
| (121) | Human | RCT | 160 and 500 mg/day for 5 weeks | Decrease of pain, improvements regard to prostatic and urinary symptoms | CP/CPPS | |
| Reduced Glutathione | (102) | Human | RCT | N/A | Reduced glutathione reacts with lipid peroxides protecting germinal epithelium from ROS damage | Male Infertility |
| (106) | Human | Non-RCT | N/A | GSH can reactivate antioxidant enzymes stimulating increase in sperm count and decrease in morphological and motility changes | ||
| Tryptophan | (83) | Human | RCT | 200 mg/day for 7 days | Improvement of depressive mood in severe depression patients | Mood and cognition |
| (84) | RCT | 2000 or 4000 mg, single dose | Benefits on emotional function | |||
| (85) | Non-RCT | 25 mg/kg of body weight for 12 weeks | Mental state improvement on elderly subjects with mood disorders | |||
| (86) | RCT | 200 mg or 400 mg/day for 12 weeks | Improvements in social interaction | |||
| (87) | RCT | 800 mg, single dose | Promotion of charitable behaviour | |||
| (88) | RCT | 1000 mg for 19 days | Benefits on emotional and social function | |||
| (89) | Case-control | N/A | Higher intake of tryprophan is linked to reduced emotion-related impulsivity | |||
| (90) | RCT | 100 mg, single dose | Influence on attention-switching tasks | |||
| (91) | RCT | N/A | Reduction of chronic pain in fibromyalgia syndrome | Chronic pain | ||
| (92) | RCT | 280 mg/day for 16 weeks | Improvement in environmental enteropathy | Gastrointestinal health | ||
| (93) | RCT | N/A | Improvement in gastrointestinal symptoms in irritable bowel syndrome | |||
| (94) | Non-RCT | N/A | Decrease in fatigue perception during aerobic exercise | Physical performance |
4. Discussion
4.1. Silymarin
Silymarin is a flavonolignan complex derived from the seeds of milk thistle (Silybum marianum). It has been shown to have antioxidant, anti-inflammatory, anticancer, cancer protective and also hypocholesterolemic and hepatoprotective properties [4]. In a study on prostate cancer (PCa) cells, silymarin was able to inhibit cell growth and induce differentiation of these cells [5]. In different studies Silymarin has been shown to have anti-cancer effects particularly in preventing the growth of PCa cells [6,7,8]. In addition, silymarin may delay progression after a radical treatment for PCa [9,10].
In a randomized, double-blind, placebo-controlled crossover study 49 patients with a history of prostate cancer and rising PSA levels after radical prostatectomy (n = 34) or radiotherapy (n = 15) were enrolled. After 10 weeks of supplementation, 4- week washout period followed. Baseline parameters were homogeneous among the two groups.
Results showed that the slope of the PSA concentrations improved with the supplement. The median total PSA doubling time for the supplement periods was 1150 days and 445 days for the placebo periods [9].
In another RCT, 37 patients treated with radical prostatectomy were randomly allocated in supplementation (n = 19) or placebo group (n = 18) for six months. Both groups were homogenous. Physical examination, quality of life score, hematology, basic clinical chemistry and oxidative stress markers, testosterone levels and antioxidant status were evaluated at baseline and after 3 and 6 months. A statistically significant reduction of low-density lipoproteins and cholesterol was found. The authors conclude that the supplementation might be effective as these two markers are associated with PCa progression [10].
In addition, silymarin could be useful to treat BPH. In a RCT fifty-five patients were randomly allocated in treatment (n = 26) and placebo group (n = 29). Both groups were treated for 6 months. The following data were collected at baseline and after 6 months: the International Prostate Symptom Score (IPSS), bladder volume (BV), urinary flow rate, ultrasound estimated postvoid residual urine volume (PVR), serum PSA, testosterone, clinical biochemistry, hematology and oxidative stress parameters. The authors demonstrated statistically significant differences (p < 0.05) between treatment and placebo groups for the following parameters: IPSS score, maximal rate of urine flow (Qmax), average flow (Qave), BV and PVR and total PSA value [11].
The most common adverse effects reported are gastrointestinal symptoms. The frequency ranges from 2% to 10% in controlled trials and it is comparable to those of placebo. Other adverse effects are dermatological symptoms and headache, which are similar in frequency to placebo [12].
4.2. Sulforaphane
Sulforaphane is a sulphur-containing compound found in cruciferous vegetables such as broccoli, Brussels sprouts and cabbage. Sulforaphane has several health benefits, including antioxidant and anti-inflammatory effects, as well as the ability to inhibit the growth of cancer cells (13-35). Different studies showed a protective effect on different target in both in vitro [13,14,15,16,17] and in vivo models associated to oxidative stress damages [13,18,19,20,21].
Several researches highlighted the antiproliferative features of sulforaphane in bladder [22,23,24,25], prostate [26,27] and kidney cancer [28].
In a double-blinded, randomized, placebo-controlled multicenter trial 78 patients with rising PSA levels after radical prostatectomy were allocated in treatment group or control group, receiving daily oral administration of 60 mg of sulforaphane or placebo, respectively. The study was conducted for 6 months followed by 2 months without treatment. The primary endpoint was the slope of PSA. The secondary endpoints were the differences in adverse effects, PSA progression and the number of men with stabilized or increased PSA after 6 months. The primary end-point was not reached, while or secondary end-points, median PSA slopes were consistently lower in treated men, mean changes in PSA levels between first and sixth month were significantly lower in the treatment group (+0.099 ± 0.341 ng/ml) compared with placebo (+0.620 ± 1.417 ng/ml; p = 0.0433), PSA doubling time was 86% longer in the SF than in the placebo group (28.9 and 15.5 months, respectively) and PSA increases >20% after six months were significantly greater in the placebo group (71.8%) than in the treatment group (44.4%) [29].
A similar study was conducted on 98 men scheduled for prostate biopsy. Patients were allocated into either supplementation or placebo group in a double-blind, randomized controlled trial. The effects of supplementation on histone deacetylase activity, immunohistochemical biomarkers and prostate biopsy gene expression were evalueted. A significant difference in gene expression was observed among some genes that are related to PCa development [30].
In a 3- arm parallel randomized double-blinded intervention study forty-nine men on active surveillance were treated with a supplementation of broccoli soup for 12 months. The primary outcome was gene expression of prostate tissue obtained by transperineal biopsy before and after a dietary intervention while the secondary outcome was changes in metabolites The three groups were supplemented with a weekly 300 mL soup made from a standard broccoli (control group) or from 1 of 2 experimental broccoli genotypes with enhanced concentrations of glucoraphanin, delivering 3 and 7 times that of the control, respectively. The authors observed that changes in gene expression and associated oncogenic pathways were attenuated in men on the glucoraphanin rich broccoli soup in a dose-dependent trend [31].
4.3. Lycopene
Lycopene is a natural compound that belongs to the carotenoid family of phytochemicals, which are found in various fruits and vegetables. It is a bright red pigment that gives tomatoes its distinct colour [33]. Lycopene has been extensively studied over the past few decades for its ability to attenuate inflammation and oxidative stress [34]. In vitro and in vivo models also highlighted its suppressive ability against cancer cells growth [35,36].
Research suggests that it may have a large number of potential health benefits, particularly in the field of cancer prevention [37,38,39] and cardiovascular health promotion [33]. In a phase II clinical study 41 patients diagnosed with localized prostate cancer were enrolled and supplemented with 10 mg lycopene tablets per day. Of these patients 37 completed the study. Regression slopes of (log) PSA against time decreased in 26/37 (70%, 95% CI: 53–84%) and in eight cases (21%) the post-treatment slope was negative. On the other hand analysis of the PSA doubling time (pre- vs post-treatment PSA) showed a median increase after supplementation of 174 days; however, this was not statistically significant (p = 0.18) [36].
In a study on men with prostate cancer, 79 patients with prostate cancer were randomized to a nutritional intervention with either 1) tomato products containing 30 mg lycopene per day; 2) tomato products plus selenium, omega-3 fatty acids, soy isoflavones, grape/pomegranate juice, and green/black tea (tomato-plus); or 3) control diet for 3 weeks. Among patients with intermediate risk (n = 41) based on tumor classification and Gleason score post-surgery, revealed that median PSA decreased significantly in the tomato group as compared to controls (-2.9% and +6.5% respectively, p = 0.016) [40].
In another study a total of 40 patients diagnosed with HGPIN were randomized into 2 groups: the A group (n = 20) received 4 mg lycopene twice a day for one year, and the group B (n = 20) was periodically followed up. The serum PSA level in the treated group A decreased for a mean level of 6.07–3.5 ng/ml, while in the control group B, it increased from a mean value of 6.55 to 8.06 ng/ml[38].
Lycopene's anti-inflammatory and antioxidant properties are believed to contribute to its potential protective effects against prostate cancer [41].
In addition, lycopene may be a novel approach for the treatment of benign prostatic hyperplasia [42].
4.4. Green Tea
Green tea is a well-known common beverage obtained with the infusion of camellia sinensis leaves and buds, the daily consumption of which is particularly widespread in eastern countries. Its purported health benefits have been attributed to its rich content in plant polyphenols, especially epigallocatechin-3-gallate (EGCG), which is the most represented catechin in green tea and the most investigated one [43]. Experimental evidence on humans exists on a wide range of beneficial effects by either consumption of green tea as a beverage as well as supplementation with green tea extracts in the form or EGCG capsules or powder. The most reported health benefit of green tea polyphenols is, by far, its antioxidant activity. There is a wealth of studies investigating the mechanism and magnitude of this effect in human subjects. One such study investigated the antioxidant activity of tea polyphenols by attempting to measure their capacity to protect against the toxicity of probable human cancerogens such as acrylamide, which is commonly present in carbohydrate-rich heat-processed food. In a randomized single-blind trial, 78 adults were randomly assigned to receive corn starch capsules containing either placebo or 50 mg, 100 or 200 mg tea polyphenols after ingesting a bag of potato chips containing an estimated level of acrylamide. Blood samples were taken before, after 2 days and after 10 days, which showed that tea polyphenol supplementation with the highest dose (200 mg) significantly increased the excretion of acrylamide via its oxidative metabolism pathway [44]. More commonly, antioxidant activity of green tea has been investigated by measuring variations in the blood levels of cells or enzymes involved in antioxidant status. For instance, leukocyte activity and total plasma antioxidant status was measured by chemiluminescence methods measuring the capacity of plasma to scavenge superoxide in a recent study. Volunteers were asked to take 300 mg of green tea extract daily for 14 days; whole blood samples from participants were stimulated with a bacterial peptide. The intervention caused a slight but irrelevant decrease in circulating leukocytes count, but the total antioxidant status significantly increased (p=0.05) [45]. Antioxidant activity of green tea was also observed in a study on 16 subjects ingesting either a single dose of green tea, 7 days of 2-cups-per-day green tea, or water as control treatment. Both the single-dose and the 7-days group showed significant increase (p<0.0005) in the activity of human oxoguanine glycosilase 1 (hOGG1), a DNA repair enzyme, and in the activity of heme oxygenase-1, a protein with antioxidant and anti-inflammatory effects. Lymphocytic DNA damage was also significantly lower (p<0.001) in the intervention groups [46]. Furthermore, a trial in which 18 healthy male volunteers ingested green tea extract (254 mg of catechins) highlighted that plasma phosphatidylcholine hydroperoxide (PCOOH) levels decreased with an inverse correlation with the increase of epigallocatechin plasma levels, suggesting an effective antioxidant capability of the substance[47]. Supplementation of 4 cups per day of green tea, or 2 capsules per day of green tea extract, compared to placebo, were also associated in reduction of Serum Amyloid Alpha (SAA), an inflammation marker, in 35 obese subjects with metabolic syndrome during the course of an 8-week study [48]. Finally, a 4-month phase II randomized controlled three-arm trial studied the effect of drinking 4 cups daily of either green or black tea or water on oxidative DNA damage among a population of 133 heavy smokers by measurement of urinary 8-hydroxydeoxyguanosine (8-OHdG). This marker decreased significantly in green tea consumers after 4 months of the intervention in subjects with mutated genotypes of glutathione-S-transferase which are associated with many different types of tumors [49].
Abundant experimental literature exists on the purported effects of green tea catechins on metabolism and cardiovascular health. The general consensus seems to be that the regular intake of green tea and/or green tea extracts produces positive effects on body weight control, lipid and general hormonal metabolism, glucose level control and blood pressure control. However, those results do not always reach statistical significance. The main issue with evaluating this body of work comes from the extreme heterogeneity of outcomes investigated and methods used to express those outcomes. For instance, green tea consumption has been observed to either be protective against weight gain or be associated with body weight reduction in studies mostly conducted on overweight or obese individuals, even if some of these results were significant only when compared against the baseline and not against the placebo arm in some cases [50,51,52]. Lipid metabolism has been shown to be positively impacted by long-term green tea supplementation (12 to 14 weeks) in terms of lowering of LDL cholesterol in some studies [53,54], while one other study showed no acute benefit on total or LDL cholesterol after a single assumption of a high-dose EGCG supplement, even if a significant attenuation of postprandial triglycerides was observed [43]. Findings on blood glucose level control, insulin and insulin-resistance are mostly inconsistent between the various studies, with some showing positive effects, others concluding for either limited or no benefit [43,52,54,55,56,57,58,59,60]. In terms of blood pressure control, green tea supplementation has been associated with a positive lowering effect, but the results were significant against placebo only in a single study on 88 overweight or obese males, while another study showed only a within-group significance when comparing to baseline levels [52,60].
Green tea integration has also been investigated in terms of possible benefits on physical performance in the context of regular physical exercise or training programs. Improvements in muscle mass have been observed in sarcopenic elderly adults supplemented with green tea extract and essential amino acids during the course of 24 weeks [61]. Positive modifications in enzymes involved in physical endurance capacity have been found in previously untrained men and overweight women [62,63,64].
Green tea has a long history of having been associated with anti-cancer or at least chemo-preventive properties. While this seems to be confirmed by human experimentation on supplementation in relation to certain tumours, such as relapsing colorectal adenoma [65] or incidence of de novo myelodysplastic syndromes [66], evidence is not as solid for neoplasms of uro-andrological interest and no clear conclusions on safety were drawn [67,68,69,70,71]. Evidence for a clear benefit of green tea supplementation in human gynaecologic neoplasms is not totally conclusive either, despite very strong basic science, animal and human epidemiological evidence. EGCG supplementation for 12 months has been linked to a reduction of mammographic density (MD) – a measurement linked with breast cancer risk – in 1075 post-menopausal women, but only in the very selective group of women aged 50 to 55 years old [72]. Moreover, in a phase II clinical trial on ovarian cancer recurrence, less than one third of women treated with green tea supplementation presented absence of recurrence at 18 months [73,74,75]. Findings on Cervical Intraepithelial Neoplasia (CIN) and Vulvar Usual type of Intraepithelial Neoplasia (uVIN) were more encouraging, with significant benefits on clinical response or absence of progression in treatment arms. Of note, some of these studies included the application of catechin ointments with or without oral green tea supplements tested against placebo [73,76,77,79,80,81].
With regards to safety of green tea consumption, adverse effects ranging from gastrointestinal symptoms to liver toxicity have been reported with very high doses but to date, no real consensus on a recommended upper level of intake has been reached [78].
4.5. Tryptophan
Tryptophan (TRP) is an essential amino acid, thus it cannot be synthesized by human and must be obtained through dietary intake, usually by means of plant- and animal-based proteins and most commonly in the quantity or 3.5-5.0 mg per kilogram of body weight, or more depending on nutritional habits. Dietary supplementation with TRP has a long history because of the purported benefits on mood and nervous system health, it being a precursor of the neurotransmitter Serotonin or 5-hydroxytryptamine (5HT) which itself strongly modulates mood and sleep functions [79]. The effects of TRP on mood and nervous system health have been widely examined in interventional trials. Most commonly, improvements were found in depressive symptoms, stress management, sleep patterns, social-cognitive and emotional processing, attention and chronic pain. For instance, notable improvements in depression symptoms, mood and sleep patterns were highlighted in depressed young adults, healthy adult women undergoing a series of cognitive and emotional tests and elderly individuals with depression and sleep disorders when supplemented with TRP [80,81,82]. Increased recognition of positive emotions and consequent improvements in social interaction was observed in healthy middle-aged and older adults who underwent supplementation with TRP, suggesting a potential role of the substance in preventing age-related decline in social-cognitive processes [83]. Behavior can be positively influenced by TRP supplementation, as a shift towards inclination to charity, improvement in response patterns to negative words and emotion- and task-related impulsivity were observed in several studies [84,85,86,87]. Chronic pain seems also positively influenced by TRP supplementation, as observed in 60 females with fibromyalgia syndrome supplemented with a multi-nutraceutical compound [88]. There is also limited clinical evidence of TRP supplementation on gastrointestinal health, although in a few selected medical conditions. In particular, TRP, glutamine, leucine and micronutrient supplementation improved environmental enteropathy in affected Zambian adults [89] and a nutraceutical formulation with TRP and other actives significantly improved gastrointestinal symptoms in subjects with irritable bowel syndrome [90]. Another scarcely explored possible health benefit of TRP seems to pertain to physical exercise and performance. In fact, TRP supplementation has been observed to improve physical performance in aerobic exercise with supramaximal intercalated anaerobic bouts in 20 young healthy man, possibly because of serotoninergic modifications in neural drive [91]. When it comes to the safety of TRP supplementation, there are a few considerations to make. Unfortunately, in late 1989 a new syndrome named Eosinophilia Myalgia Syndrome (EMS) presenting with muscle pain and a high eosinophil blood count, appeared and was initially linked with inordinate or excessive intake of TRP supplements. Later investigation concluded that this syndrome was not TRP itself but the presence of contaminants in some of the supplements available. In fact, the incidence of EMS gradually returned to zero after the ban of certain products. Only excessive TRP consumption may actually induce side-effects when taken at very high doses (generally estimated in upwards of 70-200 mg/kg) which consist in tremor, nausea and dizziness. Of course, special caution must be exercised in individuals who are chronically treated with 5HT reuptake inhibitors, as TRP interactions with such drugs may cause Serotonin Syndrome, which manifests with delirium, seizure, fever and rarely coma. Although large-scale dose-related assessment remain to be found, it is nonetheless not likely that modest supplementation with TRP may cause more than mild and occasional side-effects [79].
4.6. Glutathione
Glutathione (GSH) is a tripeptide present in most tissues, especially in the liver, and plays an extremely important role in the protection of cells from damage caused by free radicals and from endogenous and exogenous toxicity [92]. Glutathione is known to have a strong antioxidant power which is expressed because of its intrinsic ability to alternate a reduced form (GSH), predominant and higher than 98%, with an oxidized form (GSSG), lower than 1%. It is distributed primarily in the cytosol and, to a lesser extent, in organelles such as the mitochondrion, nucleus, and endoplasmic reticulum where it participates in many cellular metabolic activities including ROS removal, DNA and protein synthesis, and signal transduction [93]. The anti-oxidant activity being its main distinctive character, glutathione has seen wide pre-clinical and clinical experimentation mainly in the fields of oxidation-reduction balance, cancer prevention and male infertility. It is known that reactive oxygen species (ROS) are essential for cellular metabolism and for various biochemical processes, but when in excess they can generate oxidative stress that can cause cell death. This is why cells possess several enzymes capable of maintaining a healthy balance between the synthesis and transformation of ROS into non-reactive forms. Glutathione is an essential part of a class of antioxidant enzymes called glutathione peroxidase. Glutathione peroxidase converts hydrogen peroxide (H¬¬¬¬2O2) into water with a mechanism that can be represented as follows:
2 G-SH + ROOH GSSG + ROH + H20
In this process, the reduced glutathione (GSH) is oxidized to GSSG by glutathione peroxidase and then regains its antioxidant capacity through the activity of another enzyme, glutathione reductase, which converts the macromolecule back into the reduced form with a NADPH-dependent process [92]. Glutathione has been investigated, mostly in the pre-clinical setting, because of its theorized anti-cancer activity. Cancer cells require high concentrations of ROS, higher than normal cells, and, therefore, need an equally effective antioxidant system to stem the resulting oxidative stress[92]. In fact, the reduction of GSH is implicated in the induction of various mechanisms of cell death (apoptosis, necrosis, autophagy) which the tumor cell inhibits, to the point that in many cancerous forms the increase in the level of GSH has been associated with resistance to chemotherapy [94]. Therefore, it is legitimate to hypothesize that the modulation of GSH concentration in the tumor population could be a valid therapeutic target to induce cell death by directly interfering with GSH synthesis, by inhibition of glutamate cysteine ligase (GCL) [95], or by exploiting the affinity that GSH shows towards various substrates such as isothiocyanates [94]. The latter are phytochemicals well represented in plant foods such as cruciferous vegetables and avidly bind the sulfhydryl group of the cysteine residue of GSH, demonstrating that they can play an important role in prevention of tumors such as prostate cancer [96]. Glutathione has also been of interest in the field of male infertility. The antioxidant property of reduced glutathione is essential for the development and protection of the germinal epithelium from ROS damage. In particular, reduced glutathione reacts with lipid peroxides which, if left active, can induce alterations in membrane permeability and potential, undermining the integrity of spermatozoa, whose cell membrane is rich in polyunsaturated fatty acids [97,98]. As evidence of this, the reduction of GSH, induced or pathological, can generate an oxidative stress such as to activate the autophagy mechanism in germ cells as an adaptive response [99]. From this it can be deduced that adequate levels of GSH can promote the survival and well-being of germ cells. Nonetheless, antioxidant therapy is commonly included as a means of treatment for male infertility. Spermatozoa are aerobic cells and, as such, are equipped with a wealth of different antioxidant enzymes for the various types of ROS to be modulated [100]. Indeed, ROS are natural products of sperm metabolism and are not always harmful. At low concentrations and carefully regulated, they lead to the genesis of the signals necessary for the fertilization processes. Conversely, at high concentrations, they trigger oxidative stress to which spermatozoa are particularly sensitive and which can cause damage to the DNA and the lipid and protein content of the cell [100]. Despite the high risk of incurring in injury due to oxidative stress, however, spermatozoa have a very low concentration (-0.3 mM) of reduced glutathione compared to somatic cells (10 mM), probably due to their inability to synthesize new proteins [100]. Yet in various studies it has been found that glutathione plays an important role in the reactivation of some antioxidant enzymes. In particular, in a study conducted on 112 patients between 28 and 38 years of age, it was possible to compare the concentration of phospholipid-hydroperoxide glutathione peroxidase, a selenoprotein belonging to the glutathione peroxidase family, both in a group of 75 men with infertility of various kinds (varicocele, unilateral orchidopexy, orchitis, testicular trauma, unknown) and in a group of 37 healthy donor men. The results showed that in the infertility group the enzyme activity (93.2 ± 60.1 mU/mg) was much lower than in the control group (187.5 ± 55.3 mU/mg), resulting in a decrease in sperm count (P < 0.01) and a percentage increase in morphological (P < 0.001) and motility (P < 0.001) changes [101]. There is also experimental evidence of the utility of glutathione for the treatment of other pathological conditions linked to male infertility. Leukocytospermia and Varicocele represent two different pathological conditions but both associated with oxidative stress resulting from inflammation [97]. Specifically, varicocele increases oxidant levels and decreases antioxidant levels [102]. In a study conducted on 53 patients, the concentrations of various antioxidant substances were evaluated, including GSH/GSSG ratio in three different groups: a first represented by patients with leukocytospermia, a second including patients with varicocele and a third control group with healthy patients. At the end of the study, it was possible to determine that the GSH/GSSH ratio was significantly higher in the control group than in the leukocytospermia group (P < 0.05) and in the varicocele group (P < 0.001) and, among the latter, it was higher in the leukocytospermia compared with the varicocele group (P < 0.05). Sperm concentration (P < 0.001), sperm motility (P < 0.001), and the percentage of sperm cells with normal morphology (P < 0.001) were also positively correlated with GSH/GSSG ratio [97].
4.7. Escin
Escin is a natural blend of triterpene saponins extracted from the seeds and shell of the seeds of Aesculus ippocastanum. It includes various isoforms of which the most exploitable clinically is β-escin. This form, although endowed with considerable clinical efficacy, is unfortunately impaired by a reduced bioavailability when administered orally, therefore requiring modifications aimed at increasing its water solubility. Nonetheless, from a pharmacological perspective, escin has been shown to possess different and perfectly usable beneficial activities although with not fully clarified mechanisms [103]. In fact, it is present in commercially available supplements and compounds for the management of varicose veins, hematomas, hemorrhoids and venous congestion, but presents potential utility also in the fields of urolithiasis, male infertility and varicocele, prostate and bladder cancer and chronic prostatitis. The purported anti-edema effect has actual mechanistic basis. In various preclinical models, it has been found that escin can inhibit the activity of hyaluronidases, hyaluronic acid degradation enzymes, favoring the reconstitution and strengthening of one of the essential components of the extravascular matrix of the capillaries and thus reducing the loss of plasma from the endothelium [103]. Escin may also be beneficial in protecting the endothelium from hypoxic damage. In various studies conducted on the endothelial cells of the umbilical vein incubated in hypoxic conditions, it was possible to appreciate the response of the escin capable of inhibiting the cascade of reactions causing tissue damage. In a study by Arnould et al. it was seen how, in hypoxia, the endothelial cells reduced the amount of ATP by 40% and increased the activity of phospholipase A2, an enzyme involved in the release of precursors of inflammatory mediators, as well as stimulating adhesiveness to neutrophils. In this setting, administration of escin (at a dose of 100-750 ng/mL) inhibited ATP loss, reduced phospholipase A2 activity by 57-72%, and been shown to prevent increased adhesion to neutrophils [104]. To confirm this ability, in another study conducted on the same model, attention was paid to the hypoxia-induced alterations in the expression of PECAM-1, a macromolecule important for the integrity of the junctions in the interendothelial adhesion sites and for the modulation of neutrophil transmigration. Escin, like adhesiveness, has been shown to be able to prevent PECAM-1 alterations as well [105]. Moreover, escin has been shown to prevent hypoxia-induced reorganization of the endothelial cytoskeleton, with consequent reduction of permeability and resolution of edema [103]. Effects of escin on vascular tone have also been investigated. In the in vitro study on a segment of the saphenous vein (obtained by saphenectomy and pretreated with norepinephrine), the administration of escin (at a dose of 5-10 µg/mL) induced an increase in venous tone which was maintained for more than 1 hour after application. This increase has been shown to be suppressed by incubating the segment with indomethacin or other NSAIDs. This suggests that the effect of escin on vascular tone may be dependent on prostaglandin F2α [106,107]. As described in a recent review, escin also seems to have an anti-inflammatory activity comparable to that of glucocorticoids, with the added advantage of triggering less adverse events. In fact, there are many similarities between escin and glucocorticoids, starting from the chemical structures, both belonging to the tetracyclic triterpenoids. Even more surprising are the similarities regarding pharmacological effects. Starting from an animal model, it would seem that escin can not only induce a down-regulation of inflammatory mediators by upregulating the expression of glucocorticoid receptor (GR) but can also inhibit the expression of NFkB and of AP-1. This follows, on the one hand, the marked anti-inflammatory activity of glucocorticoids and, on the other, recalls their anti-edema effect, with the inhibition of the pro-inflammatory pathways in the capillary endothelium which, by reducing permeability, solves consequently also edema. Escin, therefore, induces anti-inflammatory effects through transrepression (reduction of pro-inflammatory protein synthesis) and transactivation (increase of Ikb, lipocortin 1 and superoxide dismutase). Unlike glucocorticoids, however, it does not inhibit the physiological processes of tissue repair, does not increase the endogenous secretion of corticosterone and does not induce cellular apoptosis in the spleen or thymus of mice [108].
Benefits of escin in patients suffering from urolithiasis have been observed in clinical settings. Urolithiasis is a pathological condition characterized by the presence of solid agglomerates of various kinds (calcium, struvite, uric acid, cystine) present in the kidney and urinary tract. It is a very frequent pathology (it is estimated that 3 out of 20 men and 2 women out of 20 experience lithiasis at least once in their life) which can trigger even very intense symptoms with violent abdominal pain, restlessness, nausea, hematuria and dysuria [109]. In a prospective study, in particular, the effects of escin and prednisolone were compared on patients suffering from symptomatic ureteral calculi. A total of 360 patients were randomized into a first group treated with escin, a second group treated with glucocorticoid prednisolone and a third placebo control group. After 10 days of treatment, the reduction in pain, the decrease in the dilatation of the urinary tract, the rate of expulsion of the stones and any adverse events that occurred during the treatment were evaluated. The group treated with escin showed better outcomes than the placebo group (P < 0.00001) and superior efficacy compared to the prednisolone group (P < 0.05). Regarding stone expulsion, significant differences were found between the treatment groups and the control group (P < 0.05) but not between the escin group and the prednisolone group (P > 0.05), while adverse events were recorded only in the group taking prednisolone [110].
A promising role of escin can be found in the field of male infertility. A first potential mechanism might be in the anti-oxidant properties of this substance. As known, reactive oxygen species (ROS), although indispensable at low concentrations for fertilization processes, at high concentrations can damage the protein and lipid component and the DNA of spermatozoa [100]. In an animal model of a gastric ulcer induced by the administration of indomethacin, it was found that escin (at a dose of 0.45, 0.9 or 1.8 mg/Kg), in addition to reducing the concentration of malondialdehyde, TNF-alpha, P -selectin and VCAM-1, also promoted the activity of myeloperoxidases, superoxide dismutases, catalases and glutathione peroxidases, suggesting a relevant anti-oxidant effect [111]. Moreover, there are evidences of efficacy of escin in ameliorating seminal alterations linked with varicocele. In an animal model (rats), the pathological venous dilatation due to varicocele was reproduced with partial ligation of the left renal vein. After 4 weeks of daily administration of escin, the density of polymorphonuclear leukocytes, the number and motility of spermatozoa in the epididymis, the concentration of follicle-stimulating hormone, luteinizing hormone and testosterone were evaluated. It was seen that, in the group of rats treated with escin, the testicular blood flow was significantly reduced, the density of polymorphonuclear leukocytes underwent a significant decrease and, conversely, the sperm count increased [112]. Findings in human subjects were also encouranging. In a randomized placebo-controlled trial, three groups of patients with varicocele infertility were compared, including a control group, a group treated with surgery and one treated with orally administered escin at a dose of 60 mg/day continuously for 2 months. At the end of the treatment, compared to the control group, patients treated with surgery and escin showed an improvement both in sperm density (68.8% and 57.5% respectively compared to 38.5% in the control group) and in sperm motility (77.1% and 55.7% respectively versus 46.2% of the control group) [113].
Of note, escin is being investigated for potential cytotoxic effect and anti-tumor activity. In a recent study on both in vivo and in vitro models, the response of escin on castration-resistant cells of prostate cancer was evaluated. At the end of the treatment, it was found that escin can induce a cytotoxic effect in resistant cancer cells by inducing a chain mechanism. In fact, escin has been shown to be able to stimulate cell cycle arrest in G2/M leading to a marked reduction of cyclinβ1 expression and cyclin-dependent kinase 1 activation, with concomitant induction of p21 [114]. Potential cytotoxic properties were also investigated in bladder cancer cells. In the in vitro model, the ability of Escin to inhibit cell growth and induce the apoptosis seems to be mediated by modulation of the FAS receptor. Escin can also induce a cytotoxic effect also by reducing the mitochondrial membrane potential and increasing the activity of cytochrome C with consequent release of ROS [115].
Escin could also be of interest in the management of chronic prostatitis (CP) and chronic pelvic pain syndrome (CPPS). CP/CPPS is a pathological clinical condition characterized by pain in the perineum, pelvis, suprapubic area and external genitalia, urinary disturbances and ejaculation disorders, without evidence of bacterial infection. It is a condition that significantly reduces the quality of life of patients and which has been the subject of many studies. Among these, a recent study investigated the potential and efficacy of the combined treatment of extracorporeal shock wave therapy (ESWT) and administration of bromelain and escin. A total of 100 CP/CPPS patients were randomized into two groups, one treated with ESWT alone and another treated with ESWT plus bromelain and escin. Pain intensity, urinary and prostatitis symptoms and quality of life were assessed after 4, 12 and 24 weeks showing a significant reduction, and even disappearance, of pain in a significantly higher percentage of patients in the treated group with combined therapy compared to the group treated with ESWT alone, as well as slight improvements that were also found with regard to prostatic and urinary symptoms [116]. This can be explained by going back to the anti-inflammatory activity of both escin and bromelain (inhibition of mediators such as NF-kB, IL-1β, IL-6, TNF-α, PGE2), which inhibit different inflammatory pathways by cooperating with the ESWT in addressing the complex pathogenesis of CP/CPPS.
As for tolerability, escin has not yet produced drug interactions and is, in general, well tolerated. Even where it has produced adverse events, they have been mild and transient, commonly represented by gastrointestinal disorders (constipation, diarrhea, vomiting and nausea), headache, dizziness, hot flushes, itching and fatigue [117,118].
4.8. Limitations of the study
This narrative review was limited by the extreme heterogeneity of the studies included in terms of methodology, measurements and outcomes. Therefore, other than the classification of the effects and benefits of these substances, it was not possible to present statistical data significance. Further studies might be needed to provide confrontation between the significance of each trial performed for every single substance.
5. Conclusions
The evidence available on the substances investigated frame them as potential tools in the hands of the informed physician. Silymarin, sulforaphane, lycopene, green tea catechins, tryptophan, glutathione and escin, each demonstrated a potential benefit in offsetting the negative effects of oxidative stress and inflammation induced by environmental pollution on human health; an improvement ranging from mood and cognition to cardiovascular health and metabolism has also been observed. These substances have also shown a possible promising anti-aging and anti-cancer effect. Finally, a wide range of medical conditions, especially interesting for the urologist and andrologist, can be addressed by proper utilization of such supplements. Due to the different pathways involved in their mechanism of action, it is also unlikely for these substances to generate negative interactions in the case of simultaneous intake. Thus, further studies are required to better define the potential synergic effect, optimal dosage, mechanism of action and tolerability profile of these substances.
Author Contributions
Conceptualization, F.P., T.C. A.P.; methodology, F.P. and T.C.; software, C.d.A., F.S., C.V; formal analysis, C.d.A., F.S., C.V; data curation, C.d.A., F.S., C.V; writing—original draft preparation, C.d.A., F.S., C.V; writing—review and editing, F.P., T.C., L.G.; supervision, A.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Chen, F.; Du, M.; Blumberg, J.B.; Chui, K.K.H.; Ruan, M.; Rogers, G.; Shan, Z.; Zeng, L.; Zhang, F.F. Association Among Dietary Supplement Use, Nutrient Intake, and Mortality Among U.S. Adults: A Cohort Study. Ann. Intern. Med. 2019, 170, 604–613. [Google Scholar] [CrossRef] [PubMed]
- Wierzejska, R.E. Dietary Supplements-For Whom? The Current State of Knowledge about the Health Effects of Selected Supplement Use. Int. J. Environ. Res. Public Health 2021, 18. [Google Scholar] [CrossRef] [PubMed]
- Ronis, M.J.J.; Pedersen, K.B.; Watt, J. ADVERSE EFFECTS OF NUTRACEUTICALS AND DIETARY SUPPLEMENTS. Annu. Rev. Pharmacol. Toxicol. 2018, 58, 583. [Google Scholar] [CrossRef] [PubMed]
- Gazak, R.; Walterova, D.; Kren, V. Silybin and Silymarin - New and Emerging Applications in Medicine. Curr. Med. Chem. 2007, 14, 315–338. [Google Scholar] [CrossRef] [PubMed]
- Zi, X.; Agarwal, R. Silibinin Decreases Prostate-Specific Antigen with Cell Growth Inhibition via G1 Arrest, Leading to Differentiation of Prostate Carcinoma Cells: Implications for Prostate Cancer Intervention. Proc. Natl. Acad. Sci. U. S. A. 1999, 96, 7490–7495. [Google Scholar] [CrossRef] [PubMed]
- Singh, R.P.; Deep, G.; Blouin, M.J.; Pollak, M.N.; Agarwal, R. Silibinin Suppresses in Vivo Growth of Human Prostate Carcinoma PC-3 Tumor Xenograft. Carcinogenesis 2007, 28, 2567–2574. [Google Scholar] [CrossRef] [PubMed]
- Raina, K.; Blouin, M.-J.; Singh, R.P.; Majeed, N.; Deep, G.; Varghese, L.; Glodé, L.M.; Greenberg, N.M.; Hwang, D.; Cohen, P.; et al. Dietary Feeding of Silibinin Inhibits Prostate Tumor Growth and Progression in Transgenic Adenocarcinoma of the Mouse Prostate Model. Cancer Res. 2007, 67, 11083–11091. [Google Scholar] [CrossRef]
- Verschoyle, R.D.; Greaves, P.; Patel, K.; Marsden, D.A.; Brown, K.; Steward, W.P.; Gescher, A.J. Evaluation of the Cancer Chemopreventive Efficacy of Silibinin in Genetic Mouse Models of Prostate and Intestinal Carcinogenesis: Relationship with Silibinin Levels. Eur. J. Cancer 2008, 44, 898–906. [Google Scholar] [CrossRef]
- Schröder, F.H.; Roobol, M.J.; Boevé, E.R.; De Mutsert, R.; Zuijdgeest-Van Leeuwen, S.D.; Kersten, I.; Wildhagen, M.F.; Van Helvoort, A. Randomized, Double-Blind, Placebo-Controlled Crossover Study in Men with Prostate Cancer and Rising PSA: Effectiveness of a Dietary Supplement. Eur. Urol. 2005, 48, 922–931. [Google Scholar] [CrossRef]
- Vidlar, A.; Vostalova, J.; Ulrichova, J.; Student, V.; Krajicek, M.; Vrbkova, J.; Simanek, V. The Safety and Efficacy of a Silymarin and Selenium Combination in Men after Radical Prostatectomy - a Six Month Placebo-Controlled Double-Blind Clinical Trial. Biomed. Pap. Med. Fac. Univ. Palacky. Olomouc. Czech. Repub. 2010, 154, 239–244. [Google Scholar] [CrossRef]
- Vostalova, J.; Vidlar, A.; Ulrichova, J.; Vrbkova, J.; Simanek, V.; Student, V. Use of Selenium-Silymarin Mix Reduces Lower Urinary Tract Symptoms and Prostate Specific Antigen in Men. Phytomedicine 2013, 21, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, B.P.; Dennehy, C.; Ramirez, G.; Sapp, J.; Lawrence, V.A. Milk Thistle for the Treatment of Liver Disease: A Systematic Review and Meta-Analysis. Am. J. Med. 2002, 113, 506–515. [Google Scholar] [CrossRef] [PubMed]
- Yoon, H.-Y.; Kang, N.-I.; Lee, H.-K.; Jang, K.Y.; Park, J.-W.; Park, B.-H. Sulforaphane Protects Kidneys against Ischemia-Reperfusion Injury through Induction of the Nrf2-Dependent Phase 2 Enzyme. Biochem. Pharmacol. 2008, 75, 2214–2223. [Google Scholar] [CrossRef] [PubMed]
- Zhu, H.; Jia, Z.; Strobl, J.S.; Ehrich, M.; Misra, H.P.; Li, Y. Potent Induction of Total Cellular and Mitochondrial Antioxidants and Phase 2 Enzymes by Cruciferous Sulforaphane in Rat Aortic Smooth Muscle Cells: Cytoprotection against Oxidative and Electrophilic Stress. Cardiovasc. Toxicol. 2008, 8, 115–125. [Google Scholar] [CrossRef]
- Lii, C.-K.; Liu, K.-L.; Cheng, Y.-P.; Lin, A.-H.; Chen, H.-W.; Tsai, C.-W. Sulforaphane and Alpha-Lipoic Acid Upregulate the Expression of the Pi Class of Glutathione S-Transferase through c-Jun and Nrf2 Activation. J. Nutr. 2010, 140, 885–892. [Google Scholar] [CrossRef]
- Soane, L.; Li Dai, W.; Fiskum, G.; Bambrick, L.L. Sulforaphane Protects Immature Hippocampal Neurons against Death Caused by Exposure to Hemin or to Oxygen and Glucose Deprivation. J. Neurosci. Res. 2010, 88, 1355–1363. [Google Scholar] [CrossRef]
- Xue, M.; Qian, Q.; Adaikalakoteswari, A.; Rabbani, N.; Babaei-Jadidi, R.; Thornalley, P.J. Activation of NF-E2-Related Factor-2 Reverses Biochemical Dysfunction of Endothelial Cells Induced by Hyperglycemia Linked to Vascular Disease. Diabetes 2008, 57, 2809–2817. [Google Scholar] [CrossRef]
- Piao, C.S.; Gao, S.; Lee, G.-H.; Kim, D.S.; Park, B.-H.; Chae, S.W.; Chae, H.-J.; Kim, S.H. Sulforaphane Protects Ischemic Injury of Hearts through Antioxidant Pathway and Mitochondrial K(ATP) Channels. Pharmacol. Res. 2010, 61, 342–348. [Google Scholar] [CrossRef]
- Zhao, J.; Kobori, N.; Aronowski, J.; Dash, P.K. Sulforaphane Reduces Infarct Volume Following Focal Cerebral Ischemia in Rodents. Neurosci. Lett. 2006, 393, 108–112. [Google Scholar] [CrossRef]
- Baek, S.-H.; Park, M.; Suh, J.-H.; Choi, H.-S. Protective Effects of an Extract of Young Radish (Raphanus Sativus L) Cultivated with Sulfur (Sulfur-Radish Extract) and of Sulforaphane on Carbon Tetrachloride-Induced Hepatotoxicity. Biosci. Biotechnol. Biochem. 2008, 72, 1176–1182. [Google Scholar] [CrossRef]
- Song, M.-Y.; Kim, E.-K.; Moon, W.-S.; Park, J.-W.; Kim, H.-J.; So, H.-S.; Park, R.; Kwon, K.-B.; Park, B.-H. Sulforaphane Protects against Cytokine- and Streptozotocin-Induced Beta-Cell Damage by Suppressing the NF-KappaB Pathway. Toxicol. Appl. Pharmacol. 2009, 235, 57–67. [Google Scholar] [CrossRef] [PubMed]
- Xie, H.; Rutz, J.; Maxeiner, S.; Grein, T.; Thomas, A.; Juengel, E.; Chun, F.K.H.; Cinatl, J.; Haferkamp, A.; Tsaur, I.; et al. Plant-Derived Sulforaphane Suppresses Growth and Proliferation of Drug-Sensitive and Drug-Resistant Bladder Cancer Cell Lines In Vitro. Cancers (Basel). 2022, 14. [Google Scholar] [CrossRef] [PubMed]
- Jo, G.H.; Kim, G.Y.; Kim, W.J.; Park, K.Y.; Choi, Y.H. Sulforaphane Induces Apoptosis in T24 Human Urinary Bladder Cancer Cells through a Reactive Oxygen Species-Mediated Mitochondrial Pathway: The Involvement of Endoplasmic Reticulum Stress and the Nrf2 Signaling Pathway. Int. J. Oncol. 2014, 45, 1497–1506. [Google Scholar] [CrossRef] [PubMed]
- Xia, Y.; Kang, T.W.; Jung, Y. Do; Zhang, C.; Lian, S. Sulforaphane Inhibits Nonmuscle Invasive Bladder Cancer Cells Proliferation through Suppression of HIF-1α-Mediated Glycolysis in Hypoxia. J. Agric. Food Chem. 2019, 67, 7844–7854. [Google Scholar] [CrossRef]
- Park, H.S.; Han, M.H.; Kim, G.Y.; Moon, S.K.; Kim, W.J.; Hwang, H.J.; Park, K.Y.; Choi, Y.H. Sulforaphane Induces Reactive Oxygen Species-Mediated Mitotic Arrest and Subsequent Apoptosis in Human Bladder Cancer 5637 Cells. Food Chem. Toxicol. 2014, 64, 157–165. [Google Scholar] [CrossRef]
- Khurana, N.; Kim, H.; Chandra, P.K.; Talwar, S.; Sharma, P.; Abdel-Mageed, A.B.; Sikka, S.C.; Mondal, D. Multimodal Actions of the Phytochemical Sulforaphane Suppress Both AR and AR-V7 in 22Rv1 Cells: Advocating a Potent Pharmaceutical Combination against Castration-Resistant Prostate Cancer. Oncol. Rep. 2017, 38, 2774–2786. [Google Scholar] [CrossRef]
- Rutz, J.; Thaler, S.; Maxeiner, S.; Chun, F.K.H.; Blaheta, R.A. Sulforaphane Reduces Prostate Cancer Cell Growth and Proliferation In Vitro by Modulating the Cdk-Cyclin Axis and Expression of the CD44 Variants 4, 5, and 7. Int. J. Mol. Sci. 2020, 21, 1–14. [Google Scholar] [CrossRef]
- Juengel, E.; Maxeiner, S.; Rutz, J.; Justin, S.; Roos, F.; Khoder, W.; Tsaur, I.; Nelson, K.; Bechstein, W.O.; Haferkamp, A.; et al. Sulforaphane Inhibits Proliferation and Invasive Activity of Everolimus-Resistant Kidney Cancer Cells in Vitro. Oncotarget 2016, 7, 85208–85219. [Google Scholar] [CrossRef]
- Cipolla, B.G.; Mandron, E.; Lefort, J.M.; Coadou, Y.; Della Negra, E.; Corbel, L.; Le Scodan, R.; Azzouzi, A.R.; Mottet, N. Effect of Sulforaphane in Men with Biochemical Recurrence after Radical Prostatectomy. Cancer Prev. Res. (Phila). 2015, 8, 712–719. [Google Scholar] [CrossRef]
- Zhang, Z.; Garzotto, M.; Davis, E.W. 2nd; Mori, M.; Stoller, W.A.; Farris, P.E.; Wong, C.P.; Beaver, L.M.; Thomas, G. V; Williams, D.E.; et al. Sulforaphane Bioavailability and Chemopreventive Activity in Men Presenting for Biopsy of the Prostate Gland: A Randomized Controlled Trial. Nutr. Cancer 2020, 72, 74–87. [Google Scholar] [CrossRef]
- Traka, M.H.; Melchini, A.; Coode-Bate, J.; Al Kadhi, O.; Saha, S.; Defernez, M.; Troncoso-Rey, P.; Kibblewhite, H.; O’Neill, C.M.; Bernuzzi, F.; et al. Transcriptional Changes in Prostate of Men on Active Surveillance after a 12-Mo Glucoraphanin-Rich Broccoli Intervention-Results from the Effect of Sulforaphane on Prostate CAncer PrEvention (ESCAPE) Randomized Controlled Trial. Am. J. Clin. Nutr. 2019, 109, 1133–1144. [Google Scholar] [CrossRef] [PubMed]
- Bhamre, S.; Sahoo, D.; Tibshirani, R.; Dill, D.L.; Brooks, J.D. Temporal Changes in Gene Expression Induced by Sulforaphane in Human Prostate Cancer Cells. Prostate 2009, 69, 181–190. [Google Scholar] [CrossRef] [PubMed]
- Przybylska, S.; Tokarczyk, G. Lycopene in the Prevention of Cardiovascular Diseases. Int. J. Mol. Sci. 2022, 23. [Google Scholar] [CrossRef]
- Li, Y.; Zhu, J.; Zhao, X.; Sun, Y.; Xu, F.; Xu, S.; Shang, X. Oral Lycopene Administration Attenuates Inflammation and Oxidative Stress by Regulating Plasma Lipids in Rats with Lipopolysaccharide-Induced Epididymitis. J. Inflamm. Res. 2022, 15, 6517–6531. [Google Scholar] [CrossRef] [PubMed]
- Limpens, J.; Schröder, F.H.; De Ridder, C.M.A.; Bolder, C.A.; Wildhagen, M.F.; Obermüller-Jevic, U.C.; Krämer, K.; Van Weerden, W.M. Combined Lycopene and Vitamin E Treatment Suppresses the Growth of PC-346C Human Prostate Cancer Cells in Nude Mice. J. Nutr. 2006, 136, 1287–1293. [Google Scholar] [CrossRef]
- Barber, N.J.; Zhang, X.; Zhu, G.; Pramanik, R.; Barber, J.A.; Martin, F.L.; Morris, J.D.H.; Muir, G.H. Lycopene Inhibits DNA Synthesis in Primary Prostate Epithelial Cells in Vitro and Its Administration Is Associated with a Reduced Prostate-Specific Antigen Velocity in a Phase II Clinical Study. Prostate Cancer Prostatic Dis. 2006, 9, 407–413. [Google Scholar] [CrossRef]
- Konijeti, R.; Henning, S.; Moro, A.; Sheikh, A.; Elashoff, D.; Shapiro, A.; Ku, M.; Said, J.W.; Heber, D.; Cohen, P.; et al. Chemoprevention of Prostate Cancer with Lycopene in the TRAMP Model. Prostate 2010, 70, 1547–1554. [Google Scholar] [CrossRef]
- Mohanty, N.K.; Saxena, S.; Singh, U.P.; Goyal, N.K.; Arora, R.P. Lycopene as a Chemopreventive Agent in the Treatment of High-Grade Prostate Intraepithelial Neoplasia. Urol. Oncol. 2005, 23, 383–385. [Google Scholar] [CrossRef]
- van Poppel, H.; Tombal, B. Chemoprevention of Prostate Cancer with Nutrients and Supplements. Cancer Manag. Res. 2011, 3, 91–100. [Google Scholar] [CrossRef]
- Paur, I.; Lilleby, W.; Bøhn, S.K.; Hulander, E.; Klein, W.; Vlatkovic, L.; Axcrona, K.; Bolstad, N.; Bjøro, T.; Laake, P.; et al. Tomato-Based Randomized Controlled Trial in Prostate Cancer Patients: Effect on PSA. Clin. Nutr. 2017, 36, 672–679. [Google Scholar] [CrossRef]
- Jiang, L.N.; Liu, Y. Bin; Li, B.H. Lycopene Exerts Anti-Inflammatory Effect to Inhibit Prostate Cancer Progression. Asian J. Androl. 2018, 21, 80–85. [Google Scholar] [CrossRef] [PubMed]
- Minutoli, L.; Altavilla, D.; Marini, H.; Rinaldi, M.; Irrera, N.; Pizzino, G.; Bitto, A.; Arena, S.; Cimino, S.; Squadrito, F.; et al. Inhibitors of Apoptosis Proteins in Experimental Benign Prostatic Hyperplasia: Effects of Serenoa Repens, Selenium and Lycopene. J. Biomed. Sci. 2014, 21, 19. [Google Scholar] [CrossRef] [PubMed]
- de Morais Junior, A.C.; Schincaglia, R.M.; Passarelli, M.; Pimentel, G.D.; Mota, J.F. Acute Epigallocatechin-3-Gallate Supplementation Alters Postprandial Lipids after a Fast-Food Meal in Healthy Young Women: A Randomized, Double-Blind, Placebo-Controlled Crossover Study. Nutrients 2020, 12. [Google Scholar] [CrossRef] [PubMed]
- Wan, X.; Jia, W.; Wang, Q.; Chen, X.; Wang, A.; Zhu, L.; Liu, X.; Zhang, L.; Zhuang, P.; Jiao, J.; et al. Metabolomics Strategy Comprehensively Unveils the Effect of Catechins Intervention on the Biomarkers of Exposure to Acrylamide and Biomarkers of Cardiometabolic Risk. Environ. Int. 2022, 169, 107517. [Google Scholar] [CrossRef] [PubMed]
- Lowe, G.M.; Gana, K.; Rahman, K. Dietary Supplementation with Green Tea Extract Promotes Enhanced Human Leukocyte Activity. J. Complement. Integr. Med. 2015, 12, 277–282. [Google Scholar] [CrossRef]
- Ho, C.K.; Choi, S.; Siu, P.M.; Benzie, I.F.F. Effects of Single Dose and Regular Intake of Green Tea (Camellia Sinensis) on DNA Damage, DNA Repair, and Heme Oxygenase-1 Expression in a Randomized Controlled Human Supplementation Study. Mol. Nutr. Food Res. 2014, 58, 1379–1383. [Google Scholar] [CrossRef]
- Nakagawa, K.; Ninomiya, M.; Okubo, T.; Aoi, N.; Juneja, L.R.; Kim, M.; Yamanaka, K.; Miyazawa, T. Tea Catechin Supplementation Increases Antioxidant Capacity and Prevents Phospholipid Hydroperoxidation in Plasma of Humans. J. Agric. Food Chem. 1999, 47, 3967–3973. [Google Scholar] [CrossRef]
- Basu, A.; Du, M.; Sanchez, K.; Leyva, M.J.; Betts, N.M.; Blevins, S.; Wu, M.; Aston, C.E.; Lyons, T.J. Green Tea Minimally Affects Biomarkers of Inflammation in Obese Subjects with Metabolic Syndrome. Nutrition 2011, 27, 206–213. [Google Scholar] [CrossRef]
- Hakim, I.A.; Harris, R.B.; Chow, H.-H.S.; Dean, M.; Brown, S.; Ali, I.U. Effect of a 4-Month Tea Intervention on Oxidative DNA Damage among Heavy Smokers: Role of Glutathione S-Transferase Genotypes. Cancer Epidemiol. biomarkers Prev. a Publ. Am. Assoc. Cancer Res. cosponsored by Am. Soc. Prev. Oncol. 2004, 13, 242–249. [Google Scholar] [CrossRef]
- Brown, A.L.; Lane, J.; Holyoak, C.; Nicol, B.; Mayes, A.E.; Dadd, T. Health Effects of Green Tea Catechins in Overweight and Obese Men: A Randomised Controlled Cross-over Trial. Br. J. Nutr. 2011, 106, 1880–1889. [Google Scholar] [CrossRef]
- Basu, A.; Sanchez, K.; Leyva, M.J.; Wu, M.; Betts, N.M.; Aston, C.E.; Lyons, T.J. Green Tea Supplementation Affects Body Weight, Lipids, and Lipid Peroxidation in Obese Subjects with Metabolic Syndrome. J. Am. Coll. Nutr. 2010, 29, 31–40. [Google Scholar] [CrossRef] [PubMed]
- Fukino, Y.; Shimbo, M.; Aoki, N.; Okubo, T.; Iso, H. Randomized Controlled Trial for an Effect of Green Tea Consumption on Insulin Resistance and Inflammation Markers. J. Nutr. Sci. Vitaminol. (Tokyo). 2005, 51, 335–342. [Google Scholar] [CrossRef] [PubMed]
- Miyazaki, R.; Kotani, K.; Ayabe, M.; Tsuzaki, K.; Shimada, J.; Sakane, N.; Takase, H.; Ichikawa, H.; Yonei, Y.; Ishii, K. Minor Effects of Green Tea Catechin Supplementation on Cardiovascular Risk Markers in Active Older People: A Randomized Controlled Trial. Geriatr. Gerontol. Int. 2013, 13, 622–629. [Google Scholar] [CrossRef] [PubMed]
- Wu, A.H.; Spicer, D.; Stanczyk, F.Z.; Tseng, C.-C.; Yang, C.S.; Pike, M.C. Effect of 2-Month Controlled Green Tea Intervention on Lipoprotein Cholesterol, Glucose, and Hormone Levels in Healthy Postmenopausal Women. Cancer Prev. Res. (Phila). 2012, 5, 393–402. [Google Scholar] [CrossRef]
- Dower, J.I.; Geleijnse, J.M.; Gijsbers, L.; Zock, P.L.; Kromhout, D.; Hollman, P.C.H. Effects of the Pure Flavonoids Epicatechin and Quercetin on Vascular Function and Cardiometabolic Health: A Randomized, Double-Blind, Placebo-Controlled, Crossover Trial. Am. J. Clin. Nutr. 2015, 101, 914–921. [Google Scholar] [CrossRef]
- Churm, R.; Williams, L.M.; Dunseath, G.; Prior, S.L.; Bracken, R.M. The Polyphenol Epigallocatechin Gallate Lowers Circulating Catecholamine Concentrations and Alters Lipid Metabolism during Graded Exercise in Man: A Randomized Cross-over Study. Eur. J. Nutr. 2023, 62, 1517–1526. [Google Scholar] [CrossRef]
- Hsu, C.-H.; Liao, Y.-L.; Lin, S.-C.; Tsai, T.-H.; Huang, C.-J.; Chou, P. Does Supplementation with Green Tea Extract Improve Insulin Resistance in Obese Type 2 Diabetics? A Randomized, Double-Blind, and Placebo-Controlled Clinical Trial. Altern. Med. Rev. 2011, 16, 157–163. [Google Scholar]
- Fukino, Y.; Ikeda, A.; Maruyama, K.; Aoki, N.; Okubo, T.; Iso, H. Randomized Controlled Trial for an Effect of Green Tea-Extract Powder Supplementation on Glucose Abnormalities. Eur. J. Clin. Nutr. 2008, 62, 953–960. [Google Scholar] [CrossRef]
- Martin, B.J.; McGlory, C.; MacInnis, M.J.; Allison, M.K.; Phillips, S.M.; Gibala, M.J. Green Tea Extract Does Not Affect Exogenous Glucose Appearance but Reduces Insulinemia with Glucose Ingestion in Exercise Recovery. J. Appl. Physiol. 2016, 121, 1282–1289. [Google Scholar] [CrossRef]
- Brown, A.L.; Lane, J.; Coverly, J.; Stocks, J.; Jackson, S.; Stephen, A.; Bluck, L.; Coward, A.; Hendrickx, H. Effects of Dietary Supplementation with the Green Tea Polyphenol Epigallocatechin-3-Gallate on Insulin Resistance and Associated Metabolic Risk Factors: Randomized Controlled Trial. Br. J. Nutr. 2009, 101, 886–894. [Google Scholar] [CrossRef]
- Tokuda, Y.; Mori, H. Essential Amino Acid and Tea Catechin Supplementation after Resistance Exercise Improves Skeletal Muscle Mass in Older Adults with Sarcopenia: An Open-Label, Pilot, Randomized Controlled Trial. J. Am. Nutr. Assoc. 2023, 42, 255–262. [Google Scholar] [CrossRef] [PubMed]
- Kuo, Y.-C.; Lin, J.-C.; Bernard, J.R.; Liao, Y.-H. Green Tea Extract Supplementation Does Not Hamper Endurance-Training Adaptation but Improves Antioxidant Capacity in Sedentary Men. Appl. Physiol. Nutr. Metab. = Physiol. Appl. Nutr. Metab. 2015, 40, 990–996. [Google Scholar] [CrossRef] [PubMed]
- Ota, N.; Soga, S.; Shimotoyodome, A. Daily Consumption of Tea Catechins Improves Aerobic Capacity in Healthy Male Adults: A Randomized Double-Blind, Placebo-Controlled, Crossover Trial. Biosci. Biotechnol. Biochem. 2016, 80, 2412–2417. [Google Scholar] [CrossRef] [PubMed]
- Ghasemi, E.; Afzalpour, M.E.; Nayebifar, S. Combined High-Intensity Interval Training and Green Tea Supplementation Enhance Metabolic and Antioxidant Status in Response to Acute Exercise in Overweight Women. J. Physiol. Sci. 2020, 70, 31. [Google Scholar] [CrossRef] [PubMed]
- Shin, C.M.; Lee, D.H.; Seo, A.Y.; Lee, H.J.; Kim, S.B.; Son, W.-C.; Kim, Y.K.; Lee, S.J.; Park, S.-H.; Kim, N.; et al. Green Tea Extracts for the Prevention of Metachronous Colorectal Polyps among Patients Who Underwent Endoscopic Removal of Colorectal Adenomas: A Randomized Clinical Trial. Clin. Nutr. 2018, 37, 452–458. [Google Scholar] [CrossRef]
- Liu, P.; Zhang, M.; Jin, J.; Holman, C.D.J. Tea Consumption Reduces the Risk of de Novo Myelodysplastic Syndromes. Leuk. Res. 2015, 39, 164–169. [Google Scholar] [CrossRef]
- Gontero, P.; Marra, G.; Soria, F.; Oderda, M.; Zitella, A.; Baratta, F.; Chiorino, G.; Gregnanin, I.; Daniele, L.; Cattel, L.; et al. A Randomized Double-Blind Placebo Controlled Phase I-II Study on Clinical and Molecular Effects of Dietary Supplements in Men with Precancerous Prostatic Lesions. Chemoprevention or “Chemopromotion”? Prostate 2015, 75, 1177–1186. [Google Scholar] [CrossRef]
- Zhang, Z.; Garzotto, M.; Beer, T.M.; Thuillier, P.; Lieberman, S.; Mori, M.; Stoller, W.A.; Farris, P.E.; Shannon, J. Effects of ω-3 Fatty Acids and Catechins on Fatty Acid Synthase in the Prostate: A Randomized Controlled Trial. Nutr. Cancer 2016, 68, 1309–1319. [Google Scholar] [CrossRef]
- Jatoi, A.; Ellison, N.; Burch, P.A.; Sloan, J.A.; Dakhil, S.R.; Novotny, P.; Tan, W.; Fitch, T.R.; Rowland, K.M.; Young, C.Y.F.; et al. A Phase II Trial of Green Tea in the Treatment of Patients with Androgen Independent Metastatic Prostate Carcinoma. Cancer 2003, 97, 1442–1446. [Google Scholar] [CrossRef]
- Micali, S.; Territo, A.; Pirola, G.M.; Ferrari, N.; Sighinolfi, M.C.; Martorana, E.; Navarra, M.; Bianchi, G. Effect of Green Tea Catechins in Patients with High-Grade Prostatic Intraepithelial Neoplasia: Results of a Short-Term Double-Blind Placebo Controlled Phase II Clinical Trial. Arch. Ital. di Urol. Androl. organo Uff. [di] Soc. Ital. di Ecogr. Urol. e Nefrol. 2017, 89, 197–202. [Google Scholar] [CrossRef]
- Kumar, N.B.; Pow-Sang, J.; Egan, K.M.; Spiess, P.E.; Dickinson, S.; Salup, R.; Helal, M.; McLarty, J.; Williams, C.R.; Schreiber, F.; et al. Randomized, Placebo-Controlled Trial of Green Tea Catechins for Prostate Cancer Prevention. Cancer Prev. Res. (Phila). 2015, 8, 879–887. [Google Scholar] [CrossRef]
- Samavat, H.; Ursin, G.; Emory, T.H.; Lee, E.; Wang, R.; Torkelson, C.J.; Dostal, A.M.; Swenson, K.; Le, C.T.; Yang, C.S.; et al. A Randomized Controlled Trial of Green Tea Extract Supplementation and Mammographic Density in Postmenopausal Women at Increased Risk of Breast Cancer. Cancer Prev. Res. (Phila). 2017, 10, 710–718. [Google Scholar] [CrossRef]
- Garcia, F.A.R.; Cornelison, T.; Nuño, T.; Greenspan, D.L.; Byron, J.W.; Hsu, C.-H.; Alberts, D.S.; Chow, H.-H.S. Results of a Phase II Randomized, Double-Blind, Placebo-Controlled Trial of Polyphenon E in Women with Persistent High-Risk HPV Infection and Low-Grade Cervical Intraepithelial Neoplasia. Gynecol. Oncol. 2014, 132, 377–382. [Google Scholar] [CrossRef] [PubMed]
- Parish, M.; Massoud, G.; Hazimeh, D.; Segars, J.; Islam, M.S. Green Tea in Reproductive Cancers: Could Treatment Be as Simple? Cancers (Basel). 2023, 15. [Google Scholar] [CrossRef] [PubMed]
- Trudel, D.; Labbé, D.P.; Araya-Farias, M.; Doyen, A.; Bazinet, L.; Duchesne, T.; Plante, M.; Grégoire, J.; Renaud, M.-C.; Bachvarov, D.; et al. A Two-Stage, Single-Arm, Phase II Study of EGCG-Enriched Green Tea Drink as a Maintenance Therapy in Women with Advanced Stage Ovarian Cancer. Gynecol. Oncol. 2013, 131, 357–361. [Google Scholar] [CrossRef] [PubMed]
- Ahn, W.-S.; Yoo, J.; Huh, S.-W.; Kim, C.-K.; Lee, J.-M.; Namkoong, S.-E.; Bae, S.-M.; Lee, I.P. Protective Effects of Green Tea Extracts (Polyphenon E and EGCG) on Human Cervical Lesions. Eur. J. cancer Prev. Off. J. Eur. Cancer Prev. Organ. 2003, 12, 383–390. [Google Scholar] [CrossRef]
- Yap, J.; Slade, D.; Goddard, H.; Dawson, C.; Ganesan, R.; Velangi, S.; Sahu, B.; Kaur, B.; Hughes, A.; Luesley, D. Sinecatechins Ointment as a Potential Novel Treatment for Usual Type Vulval Intraepithelial Neoplasia: A Single-Centre Double-Blind Randomised Control Study. BJOG 2021, 128, 1047–1055. [Google Scholar] [CrossRef]
- Mah, E.; Chen, O.; Liska, D.J.; Blumberg, J.B. Dietary Supplements for Weight Management: A Narrative Review of Safety and Metabolic Health Benefits. Nutrients 2022, 14. [Google Scholar] [CrossRef]
- Fernstrom, J.D. Effects and Side Effects Associated with the Non-Nutritional Use of Tryptophan by Humans. J. Nutr. 2012, 142. [Google Scholar] [CrossRef]
- Tsujita, N.; Akamatsu, Y.; Nishida, M.M.; Hayashi, T.; Moritani, T. Effect of Tryptophan, Vitamin B6, and Nicotinamide-Containing Supplement Loading between Meals on Mood and Autonomic Nervous System Activity in Young Adults with Subclinical Depression: A Randomized, Double-Blind, and Placebo-Controlled Study. J. Nutr. Sci. Vitaminol. (Tokyo). 2019, 65, 507–514. [Google Scholar] [CrossRef]
- Gibson, E.L.; Vargas, K.; Hogan, E.; Holmes, A.; Rogers, P.J.; Wittwer, J.; Kloek, J.; Goralczyk, R.; Mohajeri, M.H. Effects of Acute Treatment with a Tryptophan-Rich Protein Hydrolysate on Plasma Amino Acids, Mood and Emotional Functioning in Older Women. Psychopharmacology (Berl). 2014, 231, 4595–4610. [Google Scholar] [CrossRef] [PubMed]
- Chojnacki, C.; Gąsiorowska, A.; Popławski, T.; Konrad, P.; Chojnacki, M.; Fila, M.; Blasiak, J. Beneficial Effect of Increased Tryptophan Intake on Its Metabolism and Mental State of the Elderly. Nutrients 2023, 15. [Google Scholar] [CrossRef]
- Suzuki, H.; Yamashiro, D.; Ogawa, S.; Kobayashi, M.; Cho, D.; Iizuka, A.; Tsukamoto-Yasui, M.; Takada, M.; Isokawa, M.; Nagao, K.; et al. Intake of Seven Essential Amino Acids Improves Cognitive Function and Psychological and Social Function in Middle-Aged and Older Adults: A Double-Blind, Randomized, Placebo-Controlled Trial. Front. Nutr. 2020, 7. [Google Scholar] [CrossRef] [PubMed]
- Steenbergen, L.; Sellaro, R.; Colzato, L.S. Tryptophan Promotes Charitable Donating. Front. Psychol. 2014, 5. [Google Scholar] [CrossRef]
- Mohajeri, M.H.; Wittwer, J.; Vargas, K.; Hogan, E.; Holmes, A.; Rogers, P.J.; Goralczyk, R.; Gibson, E.L. Chronic Treatment with a Tryptophan-Rich Protein Hydrolysate Improves Emotional Processing, Mental Energy Levels and Reaction Time in Middle-Aged Women. Br. J. Nutr. 2015, 113, 350–365. [Google Scholar] [CrossRef] [PubMed]
- Javelle, F.; Li, D.; Zimmer, P.; Johnson, S.L. Dietary Intake of Tryptophan Tied Emotion-Related Impulsivity in Humans. Int. J. Vitam. Nutr. Res. 2021, 91, 69–76. [Google Scholar] [CrossRef]
- Markus, C.R.; Jonkman, L.M. Attention Switching after Dietary Brain 5-HT Challenge in High Impulsive Subjects. J. Psychopharmacol. 2007, 21, 700–708. [Google Scholar] [CrossRef]
- Schweiger, V.; Secchettin, E.; Castellani, C.; Martini, A.; Mazzocchi, E.; Picelli, A.; Polati, E.; Donadello, K.; Valenti, M.T.; Carbonare, L.D. Comparison between Acupuncture and Nutraceutical Treatment with Migratens® in Patients with Fibromyalgia Syndrome: A Prospective Randomized Clinical Trial. Nutrients 2020, 12. [Google Scholar] [CrossRef]
- Louis-Auguste, J.; Besa, E.; Zyambo, K.; Munkombwe, D.; Banda, R.; Banda, T.; Watson, A.; Mayneris-Perxachs, J.; Swann, J.; Kelly, P. Tryptophan, Glutamine, Leucine, and Micronutrient Supplementation Improves Environmental Enteropathy in Zambian Adults: A Randomized Controlled Trial. Am. J. Clin. Nutr. 2019, 110, 1240–1252. [Google Scholar] [CrossRef]
- Fiorini, G.; Saracino, I.M.; Pavoni, M.; Nipote, B.; Colucci, R.; Capone, P.; Sannino, A.; Forte, F.; Vergori, E.D.E.; Brancaccio, M.; et al. Efficacy of a New Nutraceutical Formulation: L-Tryptophan, Probiotics, Charcoal, Chamomile, Mint, and Licorice (COLONIR®) in the Improvement of Gastrointestinal Symptoms in Subjects with Irritable Bowel Syndrome. Minerva Gastroenterol. 2023, 69, 123–127. [Google Scholar] [CrossRef]
- Javierre, C.; Segura, R.; Ventura, J.L.; Surez, A.; Rosés, J.M. L-Tryptophan Supplementation Can Decrease Fatigue Perception during an Aerobic Exercise with Supramaximal Intercalated Anaerobic Bouts in Young Healthy Men. Int. J. Neurosci. 2010, 120, 319–327. [Google Scholar] [CrossRef]
- Gupta, P.K. Biotransformation. Fundam. Toxicol. 2016, 73–85. [Google Scholar] [CrossRef]
- Lv, H.; Zhen, C.; Liu, J.; Yang, P.; Hu, L.; Shang, P. Unraveling the Potential Role of Glutathione in Multiple Forms of Cell Death in Cancer Therapy. Oxid. Med. Cell. Longev. 2019, 2019. [Google Scholar] [CrossRef] [PubMed]
- Kuo, M.T.; Chen, H.H.W. Role of Glutathione in the Regulation of Cisplatin Resistance in Cancer Chemotherapy. Met. Based. Drugs 2010, 2010. [Google Scholar] [CrossRef]
- Chen, Y.; Shertzer, H.G.; Schneider, S.N.; Nebert, D.W.; Dalton, T.P. Glutamate Cysteine Ligase Catalysis: Dependence on ATP and Modifier Subunit for Regulation of Tissue Glutathione Levels. J. Biol. Chem. 2005, 280, 33766–33774. [Google Scholar] [CrossRef]
- Amjad, A.I.; Parikh, R.A.; Appleman, L.J.; Hahm, E.R.; Singh, K.; Singh, S. V Broccoli-Derived Sulforaphane and Chemoprevention of Prostate Cancer: From Bench to Bedside. Curr. Pharmacol. reports 2015, 1, 382–390. [Google Scholar] [CrossRef]
- Moretti, E.; Micheli, L.; Noto, D.; Fiaschi, A.I.; Menchiari, A.; Cerretani, D. Resistin in Human Seminal Plasma: Relationship with Lipid Peroxidation, CAT Activity, GSH/GSSG Ratio, and Semen Parameters. Oxid. Med. Cell. Longev. 2019, 2019. [Google Scholar] [CrossRef] [PubMed]
- Bisht, S.; Dada, R. Oxidative Stress: Major Executioner in Disease Pathology, Role in Sperm DNA Damage and Preventive Strategies. Front. Biosci. (Schol. Ed). 2017, 9, 420–447. [Google Scholar] [CrossRef]
- Mancilla, H.; Maldonado, R.; Cereceda, K.; Villarroel-Espíndola, F.; Oca, M.M. De; Angulo, C.; Castro, M.A.; Slebe, J.C.; Vera, J.C.; Lavandero, S.; et al. Glutathione Depletion Induces Spermatogonial Cell Autophagy. J. Cell. Biochem. 2015, 116, 2283–2292. [Google Scholar] [CrossRef]
- O’Flaherty, C.; Scarlata, E. OXIDATIVE STRESS AND REPRODUCTIVE FUNCTION: The Protection of Mammalian Spermatozoa against Oxidative Stress. Reproduction 2022, 164, F67–F78. [Google Scholar] [CrossRef]
- Foresta, C.; Flohé, L.; Garolla, A.; Roveri, A.; Ursini, F.; Maiorino, M. Male Fertility Is Linked to the Selenoprotein Phospholipid Hydroperoxide Glutathione Peroxidase. Biol. Reprod. 2002, 67, 967–971. [Google Scholar] [CrossRef] [PubMed]
- Hassanin, A.M.; Ahmed, H.H.; Kaddah, A.N. A Global View of the Pathophysiology of Varicocele. Andrology 2018, 6, 654–661. [Google Scholar] [CrossRef] [PubMed]
- Gallelli, L. Escin: A Review of Its Anti-Edematous, Antiinflammatory, and Venotonic Properties. Drug Des. Devel. Ther. 2019, 13, 3425–3437. [Google Scholar] [CrossRef] [PubMed]
- Arnould, T.; Janssens, D.; Michiels, C. Effect of Aescine on Hypoxia-Induced Activation of Human Endothelial Cells. Eur. J. Pharmacol. 1996, 315, 227–233. [Google Scholar] [CrossRef] [PubMed]
- Montopoli, M.; Froldi, G.; Comelli, M.C.; Prosdocimi, M.; Caparrotta, L. Aescin Protection of Human Vascular Endothelial Cells Exposed to Cobalt Chloride Mimicked Hypoxia and Inflammatory Stimuli. Planta Med. 2007, 73, 285–288. [Google Scholar] [CrossRef] [PubMed]
- Annoni, F.; Mauri, A.; Marincola, F.; Resele, L.F. Venotonic Activity of Escin on the Human Saphenous Vein. Arzneimittelforschung. 1979, 29, 672–675. [Google Scholar]
- Longiave, D.; Omini, C.; Nicosia, S.; Berti, F. The Mode of Action of Aescin on Isolated Veins: Relationship with PGF2 Alpha. Pharmacol. Res. Commun. 1978, 10, 145–152. [Google Scholar] [CrossRef]
- Gallelli, L.; Cione, E.; Wang, T.; Zhang, L. Glucocorticoid-Like Activity of Escin: A New Mechanism for an Old Drug. Drug Des. Devel. Ther. 2021, 15, 699–704. [Google Scholar] [CrossRef]
- Calcoli Renali: Come Si Formano, Si Curano e Prevengono - ISSalute.
- Al-Azzawi, I.S. The Role of Aescin versus Prednisolone in the Management of Symptomatic Lower Ureteral Calculi: A Comparative Study. J. Pak. Med. Assoc. 2021, 71(Suppl 8, S77–S81. [Google Scholar]
- Wang, T.; Zhao, S.; Wang, Y.; Yang, Y.; Yao, L.; Chu, L.; Du, H.; Fu, F. Protective Effects of Escin against Indomethacin-Induced Gastric Ulcer in Mice. Toxicol. Mech. Methods 2014, 24, 560–566. [Google Scholar] [CrossRef]
- Tian, R.H.; Ma, M.; Zhu, Y.; Yang, S.; Wang, Z.Q.; Zhang, Z.S.; Wan, C.F.; Li, P.; Liu, Y.F.; Wang, J.L.; et al. Effects of Aescin on Testicular Repairment in Rats with Experimentally Induced Varicocele. Andrologia 2014, 46, 504–512. [Google Scholar] [CrossRef] [PubMed]
- Fang, Y.; Zhao, L.; Yan, F.; Xia, X.; Xu, D.; Cui, X. Escin Improves Sperm Quality in Male Patients with Varicocele-Associated Infertility. Phytomedicine 2010, 17, 192–196. [Google Scholar] [CrossRef]
- Piao, S.; Kang, M.; Lee, Y.J.; Choi, W.S.; Chun, Y.S.; Kwak, C.; Kim, H.H. Cytotoxic Effects of Escin on Human Castration-Resistant Prostate Cancer Cells through the Induction of Apoptosis and G2/M Cell Cycle Arrest. Urology 2014, 84, 982–e1. [Google Scholar] [CrossRef] [PubMed]
- Cheng, C.L.; Chao, W.T.; Li, Y.H.; Ou, Y.C.; Wang, S.S.; Chiu, K.Y.; Yuan, S.Y. Escin Induces Apoptosis in Human Bladder Cancer Cells: An in Vitro and in Vivo Study. Eur. J. Pharmacol. 2018, 840, 79–88. [Google Scholar] [CrossRef] [PubMed]
- Palmieri, A.; Cai, T.; Luise, L. Di; D’alterio, C.; CAVA, G.L.A.; Cirigliano, L.; Giovanni, A. Di; Gallelli, L.; Capece, M. Extracorporeal Shock Wave Therapy in Association with Bromelain and Escin for the Management of Patients Affected by Chronic Prostatitis/Chronic Pelvic Pain Syndrome. Biomed. reports 2022, 18. [Google Scholar] [CrossRef]
- Agenzia Europea per i Medicinali. Rapporto Di Valutazione Su Aesculus Hipocastanum L., Seme; 2009. Disponibile Da: Http://Www.Ema. Europa.Eu/Documents/Herbal-Report/Assessment-Report-Aesculus-Hippo Castanum-l-Semen_en.Pdf. Accesso Effettuato Il 30 Ot.
- Siebert, U.; Brach, M.; Sroczynski, G.; Überla, K. Efficacy, Routine Effectiveness, and Safety of Horsechestnut Seed Extract in the Treatment of Chronic Venous Insufficiency. A Meta-Analysis of Randomized Controlled Trials and Large Observational Studies. Int. Angiol. 2002, 21, 305–315. [Google Scholar]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



