
Submitted:
26 July 2023
Posted:
28 July 2023
You are already at the latest version
Abstract
Background: This study assessed the nephrotoxicity of oral BRAF inhibitors (BRAFi), regorafenib (REG) and encorafenib (ENC), in metastatic colorectal cancer (mCRC), through an analysis of re-ports from the US Food and Drug Administration's Adverse Event Reporting System (FAERS) da-tabase.
Methods: A descriptive and disproportional analyses were performed for all reports with ENC and REG as the primary suspect.
Results: A total of 379 reports had at least one renal ADR, mainly related to REG (93.1%). Potential safety signals for REG particularly included chromaturia (n = 44; ROR = 12.00, CI 95% = 8.92-16.16; IC = 2.36, IC025-IC075 = 2.06-2.66), hydronephrosis (10; 8.70, 4.67-16.19; 1.85, 1.23-2.47), nephrotic syn-drome (7; 5.73, 2.73-12.03; 1.47, 0.73-2.21), renal impairment (53; 4.16, 3.17-5.45; 1.39, 1.12-1.66), dys-uria (19; 3.06, 1.95-4.81; 1.06, 0.61-1.52), renal failure (38; 1.66, 1.20-2.28; 0.49, 0.17-0.81), and acute kidney injury (AKI) (43; 1.46, 1.08-1.97; 0.37, 0.07-0.67). For ENC, consistent disproportionalities were observed for AKI (n = 11; ROR = 3.79, CI 95% = 2.09-6.90; IC = 1.32, IC025-IC075 = 0.72-1.91) and dysuria (4; 6.50, 2.43-17.39; 1.86, 0.88-2.85).
Conclusions: These findings highlighted some not extensively reported renal ADRs that required further investigations to better characterize the safety profile of BRAFi in patients with mCRC.
Keywords:
Colorectal cancer
; pharmacovigilance
; BRAF inhibitors
; regorafenib
; encorafenib
; adverse drug reactions
; renal disorders
1. Introduction
Colorectal cancer (CRC) is considered the third most common cancer after lung and breast carcinoma, and the second leading cause of death worldwide after lung cancer. In the United States (US) alone, more than 150,000 new cases and over 52,000 deaths were reported in 2022 [1,2]. Around 20% of new diagnoses confirm metastatic CRC (mCRC), while approximately 40% reveal localized cancer that later develops metastases [3,4]. From a molecular pathophysiology standpoint, CRC is characterized by specific molecular and mutational alterations. Approximately 40% of CRC patients have KRAS mutations, while 6% have NRAS mutations [5,6]. These mutations lead to the constitutive activation of the Ras-Raf-mitogen-activated protein kinase (MAPK) signaling pathway downstream of the epidermal growth factor receptor (EGFR). As a result, CRC exhibits resistance to anti-EGFR therapies, making the MAPK pathway the primary target [7,8]. Notably, mutations in the BRAF gene, a potent modulator of the MAPK pathway, are observed in approximately 8-12% of CRC patients, with BRAF-V600E accounting for over 95% of these mutations [9,10].
The identification of BRAF mutations has led to the development of specific oral targeted agents, which are currently used for the treatment of mCRC patients harboring these alterations. These therapies offer several advantages over injectable formulations, including flexibility, convenience, cost-effectiveness in some cases, and improved compliance [11,12]. Currently, two types of oral BRAF inhibitors (BRAFi) with mCRC indication are available: regorafenib (REG) since 2012 and encorafenib (ENC) [13,14]. ENC is approved for use in combination with cetuximab (CET) for the treatment of mCRC in 2020.
Although the introduction of REG and ENC has improved survival in patients with mCRC, their use is not exempt from adverse events (AEs). In premarketing studies, almost 91% of patients treated with REG experienced at least one AE, including serious ones, with fatigue (46%), hand-foot skin reaction (HFSR) (42%), and hypertension (30%) being the most common [15]. Gastrointestinal disorders are primarily reported for ENC, along with fatigue (33%) and dermatitis acneiform (30%) [16]. Due to the clinical relevance of some AEs that have not been fully characterized yet, it may be beneficial to use real-word data from the spontaneous reporting system (SRS) databases. Renal adverse drug reactions (ADRs) have been identified in several studies, suggesting that nephrotoxicity may be a common class effect of BRAFi [16,17,18]. However, the specific mechanisms underlying kidney-related ADRs are not fully understood. Additionally, only proteinuria is reported as a renal and urinary disorder in the label of REG [13].
Currently, only a few studies have been conducted on REG [19,20,21], and there are no studies directly comparing the safety profiles of REG and ENC plus CET. The SRS databases play a crucial role in identifying new ADRs and may, therefore, contribute to improving the quality of life (QoL) and overall clinical outcomes of treatment. For this reason, the aim of the study was to evaluate and characterize the safety profile of oral BRAFi for mCRC, with a specific focus on renal and urinary disorders. This was achieved by conducting an analysis of the US Food and Drug Administration's Adverse Event Reporting System (FAERS).
2. Materials and Methods
2.1. Data Source and Case Definition
An observational retrospective pharmacovigilance study was conducted based on reports of suspected ADRs collected in the FAERS database. FAERS is one of the widely used publicly available databases, gathering more than 20 million reports from patients, healthcare professionals, and pharmaceutical companies in the US, Europe, and Asia. The reported information includes identification number, dates of receipt and events, reporting country, qualifications of primary sources, patient characteristics (e.g., gender, age, and weight), suspected and concomitant drugs with their indications, ADRs, and their seriousness. All ADRs are coded using the Medical Dictionary for Regulatory Activities (MedDRA®) [22] in terms of the involved organ or system and corresponding signs/symptoms, referred to as System Organ Class (SOC) and Preferred Term (PT), respectively.
All the zipped ASCII FAERS quarterly data extract files from Q4 2012 to Q4 2022 (https://fis.fda.gov/extensions/FPD-QDE-FAERS/FPD-QDE-FAERS.html, accessed on 30th January 2023), have been downloaded and processed to remove duplicates. Duplicate reports were identified by overlapping information in key fields, including AE, event date, gender, age, body weight, reporting country, and suspected active substances. Reports with a unique Case ID related to REG and ENC (primary suspect), having CRC as the indication, and collected from October 2012 (the date of REG's first approval for the treatment of mCRC) to December 2022 were included.
Reports that contain at least one ADR belonging to the SOC “Renal and urinary disorders” were selected as “cases” while the remaining reports were identified as “non-cases”. The selection process at the case level was based on the identification number, ensuring that reports with multiple renal ADRs were counted only once.
2.2. Data Analyses
A descriptive statistical analysis was conducted to assess the demographic and clinical characteristics of the FAERS reports related to renal disorders. Specifically, patient characteristics (gender and age), primary source of information, year of reporting, reporting country, and ADR characteristics, including seriousness, outcome, and time to onset (TTO) were described. The TTO is based on the duration between drug administration and the onset of the ADR, and it was expressed as a median with interquartile range (Q1-Q3). Continuous variables were presented as medians (Q1-Q3), while categorical variables were reported as absolute (percentage) values. To compare the reports with at least one renal ADR to all other FAERS reports, differences in categorical variables were evaluated using Pearson’s chi-square test on a 2x2 contingency table with Yates’ continuity correction. Differences in continuous variables were assessed using the Mann-Whitney U test.
An exploratory disproportionality analysis using a case/non-case methodology was performed to identify new, previously undetected renal ADRs by PTs. The Reporting Odds Ratio (ROR) with the corresponding 95% confidence interval (CI) was calculated for this analysis. The statistical baseline was determined based on the lower limit of the 95% of the ROR being >1, with a minimum of 3 reports for each drug-event pair. ADRs that were not reported in the FDA Full Prescribing Information at the time of the study were considered unexpected. To minimize the risk of detecting false associations and to evaluate the strength of association between REG or ENC and the onset of renal ADRs, the Bayesian Information Component (IC) was calculated. The lower limit of a 95% credibility interval > 0 (IC025> 0) was indicative of a connection between the drug and the ADR [23,24].
A statistically significant threshold was set at a p value of <0.05 for all analyses. All statistical analyses were performed using SPSS version 23.0 (IBM Corp., SPSS Statistics).
3. Results
3.1. Descriptive Analysis
From October 2012 to December 2022, a total of 14,323 reports referring to REG and ENC were recorded in the FAERS database. After excluding premarketing reports supported by literature (n = 524), reports related to other indications (n = 7,768), reports with another drug as the primary suspect (n = 1,022), and duplicates (n = 25), a total of 4,984 reports were included in the analysis. Among these, the majority of reports were related to REG (n = 4,496; 90.2%), followed by ENC (n = 488; 9.8%). Reports containing at least one renal ADR (cases) were 379 (7.6%) (Figure 1).
Renal ADR reports were more frequently related to males compared to all other reports (60.7 % vs. 51.8%, p = 0.006). However, there was no statistically significant difference in the distribution of cases between the adult and elderly population. Consumers were the primary reporters of cases compared to non-cases (48.5% vs. 42.1%, p = 0.025), particularly in the years 2016 and 2018 (10.8% vs. 6.9%, p = 0.006 and 13.2% vs. 9.0%, p = 0.010, respectively). Renal ADRs were more likely to be classified as serious compared to all other reports (97.6% vs. 89.5%, p < 0.001) and had a higher frequency of hospitalization and life-threatening outcomes (39.6% vs. 27.6%, p < 0.001 and 4.0% vs. 2.1%, p = 0.028, respectively). REG was predominantly involved in renal ADRs compared to other reports (93.1% vs. 90.0%, p = 0.046) (Table 1).
The median (Q1-Q3) TTO of renal ADRs was higher with ENC compared to REG [14 (5-34) vs. 7 (0-21) days, p = 0.037] (Figure 2).
Renal and urinary disorders primarily involved renal impairment (n = 56; 14.8%) followed by acute kidney injury (AKI) (n = 54; 14.3%), chromaturia (n = 44; 11.6%), and renal failure (n = 40; 10.6%). Among these disorders, renal impairment, chromaturia, and renal failure were mostly reported for REG (in order n = 53; 15.0%, n = 44; 12.7%, and n = 38; 10.8%), while AKI was more commonly associated with ENC (n = 11; 42.3%).
3.2. Disproportionality Analysis
Relevant disproportionality signals of ADRs related to REG and belonging to the SOC renal and urinary disorders were already known and mentioned in the FDA Full Prescribing Information, including proteinuria, haematuria, and haemorrhage of the urinary tract. However, this analysis also revealed consistent new potential safety signals for REG, specifically: prerenal failure (n = 4; ROR = 22.13, CI 95% = 8.29-59.11; IC = 1.89, IC025-IC075 = 0.91-2.87), chromaturia (44; 12.00, 8.92-16.16; 2.36, 2.06-2.66), urinary tract obstruction (5; 9.16, 3.81-22.04; 1.66, 0.78-2.54), hydronephrosis (10; 8.70, 4.67-16.19; 1.85, 1.23-2.47), micturition disorder (3; 5.78, 1.86-17.95; 1.23, 0.10-2.37), nephrotic syndrome (7; 5.73, 2.73-12.03; 1.47, 0.73-2.21), renal pain (6; 4.08, 1.83-9.10; 1.19, 0.39-1.99), urinary retention (27; 4.99, 3.42-7.28; 1.53, 1.15-1.91), urine odour abnormal (4; 4.61, 1.73-12.28; 1.19, 0.21-2.17), renal impairment (53; 4.16, 3.17-5.45; 1.39, 1.12-1.66), anuria (6; 3.48, 1.56-7.76; 1.07, 0.27-1.87), nocturia (6; 3.39, 1.52-7.55; 1.05, 0.25-1.85), oliguria (5; 3.25, 1.35-7.81; 0.99, 0.11-1.87), dysuria (19; 3.06, 1.95-4.81; 1.06, 0.61-1.52), renal disorder (19; 2.72, 1.73-4.26; 0.95, 0.50-1.40), urinary incontinence (13; 2.46, 1.43-4.24; 0.85, 0.30-1.39), renal failure (38; 1.66, 1.20-2.28; 0.49, 0.17-0.81), and AKI (43; 1.46, 1.08-1.97; 0.37, 0.07-0.67) (Table 2).
For ENC, the analysis showed consistent disproportionality signals for renal ADRs that were not reported in the FDA Full Prescribing Information, specifically, AKI (n = 11; ROR = 3.79, CI 95% = 2.09-6.90; IC = 1.32, IC025-IC075 = 0.72-1.91) and dysuria (4; 6.50, 2.43-17.39; 1.86, 0.88-2.85) (Table 2).
4. Discussion
This study, focusing on renal disorders associated with oral BRAFi in patients with mCRC using the FAERS database, can be considered the first of its kind. Renal disorders accounted for approximately 8% of all the reports analyzed. The findings of this analysis revealed a higher association of renal ADRs with males with an equal distribution between the adult and elderly population, compared to other cases. Previous studies have indicated that men may have a higher risk of developing renal impairment with targeted therapies compared to women [25,26]. This could be attributed to testosterone which has been implicated in the progression of chronic kidney disease (CKD) and the worsening of kidney function in men [27]. The onset of renal ADRs in both adult and elderly patients could be related to the early screening of mCRC in adults [2], as well as the presence of comorbidities commonly found in elderly patients diagnosed with cancer, such as hypertension or diabetes mellitus, along with pre-existing kidney dysfunction. These factors can substantially contribute to the development of nephrotoxicity [28]. Notably, two case reports have confirmed instances of renal impairment in two patients aged 62 and 70, respectively, who received REG treatment for mCRC [29,30].
Renal ADRs were predominantly classified as serious compared to other reported ADRs, as evidenced by literature data on TKIs where a significant proportion (79%) of renal reports were serious [26]. In contrast to the previous pharmacovigilance study, a clinical trial reported serious renal disorders of grade 3 in only 10% of the patients [31]. This suggests that the occurrence of severe renal complications associated with the treatment may vary between real-life studies and clinical trials, underscoring the importance of pharmacovigilance in safety investigations. The higher frequency of renal ADRs requiring hospitalization can be explained by the complexity of patients, particularly older adults, who are often on polytherapy and may have multi-organ damage that poses a risk to their own life [32,33].
The median TTO for renal ADRs was found to be higher with ENC compared to REG. In the literature, the median TTO for all TKIs varied significantly, ranging from 26 days to 684 days for renal disorders [26,34]. This greater difference could be attributed to the fact that different TKIs, including ENC and REG, may have distinct renal effects and toxicity profiles, leading to variations in the occurrence of serious renal disorders. However, a previous study reported a similar median TTO of 27 days for AKI in patients treated with ENC, which aligns with our findings [35]. Furthermore, three case series have indicated the presence of two types of kidney injury associated with BRAFi. One type manifested shortly after the initiation of drug treatment, typically within 1-2 weeks. The other type of kidney injury had a more gradual onset and became apparent within 1-2 months [18].
Despite extensive explanations reported in the literature regarding the occurrence of renal disorders with REG and ENC, several relevant disproportionality signals related to REG and ENC in the SOC renal and urinary disorders have not been mentioned in the FDA Full Prescribing Information. One possible explanation is that REG functions as a multikinase inhibitor, affecting molecules, such as the vascular-endothelial growth factor (VEGF), that play a crucial role in the glomerular filtration barrier. This can result in increased proteinuria and the development of thrombotic microangiopathy (TMA) [29,36,37]. Additionally, REG, like other well-documented anti-angiogenetic agents, may exhibit dose-dependent nephrotoxicity [38]. Moreover, renal impairment has been associated with BRAFi, including ENC. This finding aligns with kidney biopsy results observed in patients treated with other BRAFi, such as vemurafenib, which showed signs of acute and chronic tubular injury [39]. However, the underlying mechanisms of nephrotoxicity in relation to BRAFi are not yet fully understood. One possible mechanism is the interaction of BRAFi with tubular creatinine secretion, which may induce acute tubular necrosis (ATN) [40]. Furthermore, the potential involvement of ENC in association with CET cannot exclude the role of CET itself in the development of renal disorders. This can be explained by the role of EGFR in cell regeneration following ATN. The use of anti-EGFR therapies, such as CET, may potentially hinder the re-epithelialization of tubules and impede the recovery process [41]. Additionally, in the European Medicines Agency (EMA)’s Summary of Product Characteristics (SmPC), renal failure is reported as an ADR associated with ENC [42].
Considering all the disproportionality analyses, potential safety signals were identified for REG, including prerenal failure, renal failure, and AKI. These ADRs could also be associated with other potential safety signals such as renal impairment, renal disorders, and renal pain. Prerenal failure and AKI typically occur as a result of extrarenal diseases that lead to a decrease in the glomerular filtration rate [43]. TKIs may induce AKI through two mechanisms: toxic injury to the renal tubules and the occurrence of tumor lysis syndrome [44]. Furthermore, TKIs have the potential to cause injury to podocytes by inducing tyrosine phosphorylation of nephrin, which is a critical protein in maintaining the integrity of the filtration barrier. The loss of normal podocyte fenestration can lead to various complications, including microvascular injury, capillary thrombosis, and the development of renal glomeruli sclerotic lesions, ultimately resulting in renal failure [45].
Regarding the potential signal related to nephrotic syndrome, a previous study has assessed that the known side effect of REG, proteinuria, could lead to minimal change nephrotic syndrome and TMA [46]. Interestingly, TMA has been found to occur more frequently in anti-VEGF therapies, such as bevacizumab, while nephrotic syndrome has been associated with other TKIs, including dasatinib [47]. It is worth noting that instances of nephrotic syndrome, with or without TMA characteristics, as severe side effects of TKIs in adult cancer patients, have been infrequently reported in the literature [30,48].
The disproportionality analysis revealed a significant association between REG and various urinary ADRs, including micturition disorder, urinary retention, urinary tract obstruction, urinary incontinence, anuria, nocturia, dysuria, oliguria, hydronephrosis, chromaturia, and urine odour abnormal. In the REG FDA Full Prescribing Information, burning or painful urination is reported as a symptom associated with infections [13]. It is possible that the presence of an infection itself can lead to difficulties or discomfort during urination, which encompasses all the potential signals mentioned above. Furthermore, urinary disorders including chromaturia, may be associated with other ADRs, such as severe bleeding and liver problems. According to the FDA Full Prescribing Information, pink or brown urine may indicate severe bleeding, while dark "tea-colored" urine may suggest liver problems [13]. Additionally, an abnormal urine odour could potentially indicate the development of CRC. Unusual changes in the smell of urine may serve as a notable symptom that should prompt further investigation or medical evaluation to assess the possibility of underlying CRC [49]. Moreover, dysuria was identified as a potential safety signal for ENC as well. A previous premarketing study demonstrated the occurrence of urinary tract infection in approximately 8% of patients receiving ENC plus CET [16]. Urinary tract infection is one of the most common causes of dysuria [50]. Therefore, the onset of dysuria could be a consequence of the onset of this infection.
Strengths and Limitations
The risk/benefit profile of oral BRAFi appears to be well characterized. However, renal ADRs are not fully mentioned in the FDA Full Prescribing Information for REG and ENC. The strength of this study lies in the large number of reports analyzed, which contribute to the cumulative knowledge about the nephrotoxicity of BRAFi. The use of a global database and the combination of a disproportionality approach with case/non-case evaluation has been documented in the literature [23,51]. One of the main advantages of using the SRS database is its ability to generate new potential safety signals for ADRs that may result undetected during the premarketing phase [52]. Patients with cancer often experience a lower health-related QoL, which can be influenced by the use of chemotherapeutic agents, including second- and third-line therapies as observed previously [53,54]. Notably, the increased use of BRAFi as second-line therapy in patients with mCRC following prior treatment with nephrotoxic chemotherapeutic agents may impact QoL [28,38,55,56]. Moreover, renal disorders can worsen over the duration of the tumor course and the progression of metastases. In this context, it would be interesting to analyze, in a real-world setting, whether the patterns of metastatic disease in CRC (e.g. bone metastasis, which can be associated with hypercalcemia and hypercalciuria) could influence the development of renal ADRs. Therefore, timely detection of ADRs can assist oncologists in the best treatment choices for patients affected by mCRC.
However, the FAERS database may not always provide comprehensive information on potential confounding factors. Details such as a patient's past medical history, concomitant treatments, and precise dosing and frequency of drug administration may not always be available, which limits the ability to fully assess the impact of these factors on kidney toxicity. Various factors, including gender differences [27] and underlying conditions associated with mCRC such as diarrhea, dehydration, bone marrow suppression, and infections, could also contribute to kidney toxicity [34]. The absence of drug users as a denominator, underreporting or overreporting phenomena, as well as the lack of specific data in the FAERS database, can pose challenges in establishing a clear causal relationship between the use of BRAFi and the occurrence of renal ADRs. Although disproportionality analysis is a validated method used in drug safety research and surveillance to identify potential signals of ADRs, it is crucial to acknowledge that disproportionality analysis alone should be considered an exploratory approach to generate signals rather than providing definitive confirmation of causality [57].
5. Conclusions
In recent years, the use of oral BRAFi as second-line treatment for mCRC has brought improvements in medical treatment and patient compliance. The case/non-case analysis has highlighted some ADRs that have not been extensively reported in the literature but are worth discussing, such as AKI, renal failure, nephrotic syndrome, and urinary conditions associated with REG and ENC. These renal ADRs can have a significant impact on patient's QoL and treatment outcomes.
Encouraging collaboration and mutual learning between oncologists and nephrologists is essential for improving patient care, managing clinical symptoms, and minimizing the onset of nephrotoxicity with BRAFi. It is crucial to expand the knowledge of renal ADRs and their impact on the well-being of patients affected by mCRC through further pharmacovigilance studies. Such studies will contribute to a better understanding of nephrotoxicity and enable the development of strategies to enhance patient well-being and treatment management.
Author Contributions
Conceptualization, G.R., M.A.B., and E.E.S.; methodology, M.A.B.; validation, N.S. and E.S.: formal analysis, M.A.B. and E.E.S.; writing—original draft preparation, G.R. and M.A.B.; writing—review and editing, M.A.B., T.F., and M.S.; visualization, G.R., M.A.B., E.E.S., G.C., T.F., M.S., N.S., and E.S.; supervision, N.S. and E.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was approved by the Ethics Committee of University Hospital of Messina (n. 40/23 of 28 February 2023).
Data Availability Statement
The datasets analyzed during the current study are available in the following resource available in the public domain: https://fis.fda.gov/extensions/FPD-QDE-FAERS/FPD-QDE-FAERS.html (accessed on 30th January 2023).
Conflicts of Interest
The authors declare no conflict of interest.
References
- Biller, L.H.; Schrag, D. Diagnosis and treatment of metastatic colorectal cancer: A review. JAMA - J. Am. Med. Assoc. 2021, 325, 669–685. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer statistics, 2022. CA. Cancer J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, R.; Guo, F.; Heisser, T.; Hackl, M.; Ihle, P.; De Schutter, H.; Van Damme, N.; Valerianova, Z.; Atanasov, T.; Májek, O.; et al. Colorectal cancer incidence, mortality, and stage distribution in European countries in the colorectal cancer screening era: an international population-based study. Lancet Oncol. 2021, 22, 1002–1013. [Google Scholar] [CrossRef] [PubMed]
- Howlader, N.; Noone, A.; Krapcho, M.; Miller, D.; Brest, A.; Yu, M.; Ruhl, J.; Tatalovich, Z.; Mariotto, A.; Lewis, D.R.; et al. SEER Cancer Statistics Review, 1975-2017; National Cancer Institute: Bethesda, MD. Available online: https://seer.cancer.gov/Csr/1975_2017/ (accessed on 30 January 2023).
- Bylsma, L.C.; Gillezeau, C.; Garawin, T.A.; Kelsh, M.A.; Fryzek, J.P.; Sangaré, L.; Lowe, K.A. Prevalence of RAS and BRAF mutations in metastatic colorectal cancer patients by tumor sidedness: A systematic review and meta-analysis. Cancer Med. 2020, 9, 1044–1057. [Google Scholar] [CrossRef]
- Chang, Y.-Y.; Lin, P.-C.; Lin, H.-H.; Lin, J.-K.; Chen, W.-S.; Jiang, J.-K.; Yang, S.-H.; Liang, W.-Y.; Chang, S.-C. Mutation spectra of RAS gene family in colorectal cancer. Am. J. Surg. 2016, 212, 537–544.e3. [Google Scholar] [CrossRef]
- Sepulveda, A.R.; Hamilton, S.R.; Allegra, C.J.; Grody, W.; Cushman-Vokoun, A.M.; Funkhouser, W.K.; Kopetz, S.E.; Lieu, C.; Lindor, N.M.; Minsky, B.D.; et al. Molecular Biomarkers for the Evaluation of Colorectal Cancer: Guideline From the American Society for Clinical Pathology, College of American Pathologists, Association for Molecular Pathology, and American Society of Clinical Oncology. Arch. Pathol. Lab. Med. 2017, 141, 625–657. [Google Scholar] [CrossRef]
- Zarkavelis, G. Current and future biomarkers in colorectal cancer. Ann. Gastroenterol. 2017, 30, 613–621. [Google Scholar] [CrossRef]
- Caputo; Santini; Bardasi; Cerma; Casadei-Gardini; Spallanzani; Andrikou; Cascinu; Gelsomino BRAF-Mutated Colorectal Cancer: Clinical and Molecular Insights. Int. J. Mol. Sci. 2019, 20, 5369. [CrossRef]
- Hummel, M.; Hegewisch-Becker, S.; Neumann, J.H.L.; Vogel, A. BRAF testing in metastatic colorectal carcinoma and novel, chemotherapy-free therapeutic options. Pathologe 2021, 42, 98–109. [Google Scholar] [CrossRef]
- García-Alfonso, P.; Muñoz Martín, A.J.; Ortega Morán, L.; Soto Alsar, J.; Torres Pérez-Solero, G.; Blanco Codesido, M.; Calvo Ferrandiz, P.A.; Grasso Cicala, S. Oral drugs in the treatment of metastatic colorectal cancer. Ther. Adv. Med. Oncol. 2021, 13, 175883592110090. [Google Scholar] [CrossRef]
- Piawah, S.; Venook, A.P. Targeted therapy for colorectal cancer metastases: A review of current methods of molecularly targeted therapy and the use of tumor biomarkers in the treatment of metastatic colorectal cancer. Cancer 2019, 125, 4139–4147. [Google Scholar] [CrossRef] [PubMed]
- US Food and Drug Administration Full Prescribing Information Stivarga®. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2012/203085lbl.pdf (accessed on Jan 30, 2023).
- US Food and Drug Administration Full prescribing information Braftovi®. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2020/210496s006lbl.pdf (accessed on Jan 30, 2023).
- Van Cutsem, E.; Martinelli, E.; Cascinu, S.; Sobrero, A.; Banzi, M.; Seitz, J.-F.; Barone, C.; Ychou, M.; Peeters, M.; Brenner, B.; et al. Regorafenib for Patients with Metastatic Colorectal Cancer Who Progressed After Standard Therapy: Results of the Large, Single-Arm, Open-Label Phase IIIb CONSIGN Study. Oncologist 2019, 24, 185–192. [Google Scholar] [CrossRef] [PubMed]
- Tabernero, J.; Velez, L.; Trevino, T.L.; Grothey, A.; Yaeger, R.; Van Cutsem, E.; Wasan, H.; Desai, J.; Ciardiello, F.; Yoshino, T.; et al. Management of adverse events from the treatment of encorafenib plus cetuximab for patients with BRAF V600E-mutant metastatic colorectal cancer: insights from the BEACON CRC study. ESMO Open 2021, 6, 100328. [Google Scholar] [CrossRef] [PubMed]
- Stammler, R.; Gallois, C.; Taieb, J.; Duong, J.-P.; Karras, A.; Thervet, E.; Lazareth, H. Acute renal failure under encorafenib, binimetinib and cetuximab for BRAF V600E–mutated colorectal cancer. Eur. J. Cancer 2021, 147, 60–62. [Google Scholar] [CrossRef]
- Wanchoo, R.; Jhaveri, K.D.; Deray, G.; Launay-Vacher, V. Renal effects of BRAF inhibitors: a systematic review by the Cancer and the Kidney International Network. Clin. Kidney J. 2016, 9, 245–251. [Google Scholar] [CrossRef] [PubMed]
- Guha, A.; Jain, P.; Fradley, M.G.; Lenihan, D.; Gutierrez, J.M.; Jain, C.; Lima, M.; Barnholtz-Sloan, J.S.; Oliveira, G.H.; Dowlati, A.; et al. Cardiovascular adverse events associated with BRAF versus BRAF/MEK inhibitor: Cross-sectional and longitudinal analysis using two large national registries. Cancer Med. 2021, 10, 3862–3872. [Google Scholar] [CrossRef] [PubMed]
- Meirson, T.; Asher, N.; Bomze, D.; Markel, G. Safety of BRAF+MEK Inhibitor Combinations: Severe Adverse Event Evaluation. Cancers (Basel). 2020, 12, 1650. [Google Scholar] [CrossRef]
- Sasaoka, S.; Matsui, T.; Abe, J.; Umetsu, R.; Kato, Y.; Ueda, N.; Hane, Y.; Motooka, Y.; Hatahira, H.; Kinosada, Y.; et al. Evaluation of the Association of Hand-Foot Syndrome with Anticancer Drugs Using the US Food and Drug Administration Adverse Event Reporting System (FAERS) and Japanese Adverse Drug Event Report (JADER) Databases. YAKUGAKU ZASSHI 2016, 136, 507–515. [Google Scholar] [CrossRef] [PubMed]
- Food and Drug Administration FDA Adverse Event Reporting System (FAERS) Public Dashboard. Available online: https://fis.fda.gov/sense/app/95239e26-e0be-42d9-a960-9a5f7f1c25ee/sheet/8eef7d83-7945-4091-b349-e5c41ed49f99/state/analysis (accessed on Jan 24, 2023).
- Harpaz, R.; DuMouchel, W.; LePendu, P.; Bauer-Mehren, A.; Ryan, P.; Shah, N.H. Performance of Pharmacovigilance Signal-Detection Algorithms for the FDA Adverse Event Reporting System. Clin. Pharmacol. Ther. 2013, 93, 539–546. [Google Scholar] [CrossRef]
- Norén, G.N.; Hopstadius, J.; Bate, A. Shrinkage observed-to-expected ratios for robust and transparent large-scale pattern discovery. Stat. Methods Med. Res. 2013, 22, 57–69. [Google Scholar] [CrossRef]
- Jhaveri, K.D.; Wanchoo, R.; Sakhiya, V.; Ross, D.W.; Fishbane, S. Adverse Renal Effects of Novel Molecular Oncologic Targeted Therapies: A Narrative Review. Kidney Int. Reports 2017, 2, 108–123. [Google Scholar] [CrossRef] [PubMed]
- Cellier, M.; Bourneau-Martin, D.; Abbara, C.; Crosnier, A.; Lagarce, L.; Garnier, A.-S.; Briet, M. Renal Safety Profile of BCR-ABL Tyrosine Kinase Inhibitors in a Real-Life Setting: A Study Based on Vigibase®, the WHO Pharmacovigilance Database. Cancers (Basel). 2023, 15, 2041. [Google Scholar] [CrossRef]
- Filler, G.; Ramsaroop, A.; Stein, R.; Grant, C.; Marants, R.; So, A.; McIntyre, C. Is Testosterone Detrimental to Renal Function? Kidney Int. Reports 2016, 1, 306–310. [Google Scholar] [CrossRef]
- García-Carro, C.; Draibe, J.; Soler, M.J. Onconephrology: Update in Anticancer Drug-Related Nephrotoxicity. Nephron 2023, 147, 65–77. [Google Scholar] [CrossRef] [PubMed]
- Yin, Q.; Guo, N.; Zhou, X.; Xu, H.; Lei, S.; Fu, P.; Zhong, H. Regorafenib-induced renal-limited thrombotic microangiopathy: a case report and review of literatures. BMC Nephrol. 2022, 23, 112. [Google Scholar] [CrossRef]
- Strasma, A.; Coke, H.; Mamlouk, O.; Tchakarov, A.; Mandayam, S. Lupus-Like Glomerulonephritis Associated With Regorafenib, a Multikinase Inhibitor. Kidney Med. 2021, 3, 294–298. [Google Scholar] [CrossRef] [PubMed]
- Eisen, T.; Joensuu, H.; Nathan, P.D.; Harper, P.G.; Wojtukiewicz, M.Z.; Nicholson, S.; Bahl, A.; Tomczak, P.; Pyrhonen, S.; Fife, K.; et al. Regorafenib for patients with previously untreated metastatic or unresectable renal-cell carcinoma: a single-group phase 2 trial. Lancet Oncol. 2012, 13, 1055–1062. [Google Scholar] [CrossRef] [PubMed]
- Arcoraci, V.; Barbieri, M.A.; Rottura, M.; Nobili, A.; Natoli, G.; Argano, C.; Squadrito, G.; Squadrito, F. Kidney Disease Management in the Hospital Setting : A Focus on Inappropriate Drug Prescriptions in Older Patients. 2021, 12, 1–10. [Google Scholar] [CrossRef]
- Barbieri, M.A.; Rottura, M.; Cicala, G.; Mandraffino, R.; Marino, S.; Irrera, N.; Mannucci, C.; Santoro, D.; Squadrito, F.; Arcoraci, V. Chronic Kidney Disease Management in General Practice: A Focus on Inappropriate Drugs Prescriptions. J. Clin. Med. 2020, 9, 1346. [Google Scholar] [CrossRef] [PubMed]
- Taieb, J.; Lonardi, S.; Desai, J.; Folprecht, G.; Gallois, C.; Marques, E.P.; Khan, S.; Castagné, C.; Wasan, H. Adverse Events Associated with Encorafenib Plus Cetuximab in Patients with BRAFV600E-mutant Metastatic Colorectal Cancer: An in-depth Analysis of the BEACON CRC Study. Clin. Colorectal Cancer 2023, 22, 59–66. [Google Scholar] [CrossRef]
- Seethapathy, H.; Bates, H.; Chute, D.F.; Strohbehn, I.; Strohbehn, S.; Fadden, R.M.; Reynolds, K.L.; Cohen, J. V.; Sullivan, R.J.; Sise, M.E. Acute Kidney Injury Following Encorafenib and Binimetinib for Metastatic Melanoma. Kidney Med. 2020, 2, 373–375. [Google Scholar] [CrossRef]
- Pfister, F.; Amann, K.; Daniel, C.; Klewer, M.; Büttner, A.; Büttner-Herold, M. Characteristic morphological changes in anti-VEGF therapy-induced glomerular microangiopathy. Histopathology 2018, 73, 990–1001. [Google Scholar] [CrossRef] [PubMed]
- Izzedine, H.; Mangier, M.; Ory, V.; Zhang, S.-Y.; Sendeyo, K.; Bouachi, K.; Audard, V.; Péchoux, C.; Soria, J.C.; Massard, C.; et al. Expression patterns of RelA and c-mip are associated with different glomerular diseases following anti-VEGF therapy. Kidney Int. 2014, 85, 457–470. [Google Scholar] [CrossRef] [PubMed]
- Kala, J.; Salman, L.A.; Geara, A.S.; Izzedine, H. Nephrotoxicity From Molecularly Targeted Chemotherapeutic Agents. Adv. Chronic Kidney Dis. 2021, 28, 415–428.e1. [Google Scholar] [CrossRef] [PubMed]
- Teuma, C.; Perier-Muzet, M.; Pelletier, S.; Nouvier, M.; Amini-Adl, M.; Dijoud, F.; Duru, G.; Thomas, L.; Fouque, D.; Laville, M.; et al. New insights into renal toxicity of the B-RAF inhibitor, vemurafenib, in patients with metastatic melanoma. Cancer Chemother. Pharmacol. 2016, 78, 419–426. [Google Scholar] [CrossRef] [PubMed]
- Hurabielle, C.; Pillebout, E.; Stehlé, T.; Pagès, C.; Roux, J.; Schneider, P.; Chevret, S.; Chaffaut, C.; Boutten, A.; Mourah, S.; et al. Mechanisms Underpinning Increased Plasma Creatinine Levels in Patients Receiving Vemurafenib for Advanced Melanoma. PLoS One 2016, 11, e0149873. [Google Scholar] [CrossRef]
- Rayego-Mateos, S.; Rodrigues-Diez, R.; Morgado-Pascual, J.L.; Valentijn, F.; Valdivielso, J.M.; Goldschmeding, R.; Ruiz-Ortega, M. Role of Epidermal Growth Factor Receptor (EGFR) and Its Ligands in Kidney Inflammation and Damage. Mediators Inflamm. 2018, 2018, 1–22. [Google Scholar] [CrossRef] [PubMed]
- European Medicines Agency Braftovi®, Summary of Product Characteristics. Available online: https://www.ema.europa.eu/en/documents/product-information/braftovi-epar-product-information_en.pdf (accessed on Jul 5, 2023).
- Makris, K.; Spanou, L. Acute Kidney Injury: Definition, Pathophysiology and Clinical Phenotypes. Clin. Biochem. Rev. 2016, 37, 85–98. [Google Scholar]
- Mielczarek, Ł.; Brodziak, A.; Sobczuk, P.; Kawecki, M.; Cudnoch-Jędrzejewska, A.; Czarnecka, A.M. Renal toxicity of targeted therapies for renal cell carcinoma in patients with normal and impaired kidney function. Cancer Chemother. Pharmacol. 2021, 87, 723–742. [Google Scholar] [CrossRef]
- Simons, M.; Schwarz, K.; Kriz, W.; Miettinen, A.; Reiser, J.; Mundel, P.; Holthöfer, H. Involvement of Lipid Rafts in Nephrin Phosphorylation and Organization of the Glomerular Slit Diaphragm. Am. J. Pathol. 2001, 159, 1069–1077. [Google Scholar] [CrossRef]
- Izzedine, H.; Escudier, B.; Lhomme, C.; Pautier, P.; Rouvier, P.; Gueutin, V.; Baumelou, A.; Derosa, L.; Bahleda, R.; Hollebecque, A.; et al. Kidney Diseases Associated With Anti-Vascular Endothelial Growth Factor (VEGF). Medicine (Baltimore). 2014, 93, 333–339. [Google Scholar] [CrossRef] [PubMed]
- Ollero, M.; Sahali, D. Inhibition of the VEGF signalling pathway and glomerular disorders. Nephrol. Dial. Transplant. 2015, 30, 1449–1455. [Google Scholar] [CrossRef]
- Vankalakunti, M.; Siddini, V.; Bonu, R.; Prakash, G.; Babu, K.; Ballal, H.; Jha, P. Sunitinib induced nephrotic syndrome and thrombotic microangiopathy. Indian J. Nephrol. 2013, 23, 67. [Google Scholar] [CrossRef] [PubMed]
- Bax; Lotesoriere; Sironi; Capelli Review and Comparison of Cancer Biomarker Trends in Urine as a Basis for New Diagnostic Pathways. Cancers (Basel). 2019, 11, 1244. [CrossRef]
- Mehta, P.; Leslie, S.; Reddivari, A. Dysuria. Available online: https://www.ncbi.nlm.nih.gov/books/NBK549918/ (accessed on Jul 5, 2023).
- Barbieri, M.A.; Sorbara, E.E.; Russo, G.; Cicala, G.; Franchina, T.; Santarpia, M.; Silvestris, N.; Spina, E. Neuropsychiatric Adverse Drug Reactions with Tyrosine Kinase Inhibitors in Gastrointestinal Stromal Tumors: An Analysis from the European Spontaneous Adverse Event Reporting System. Cancers (Basel). 2023, 15, 1851. [Google Scholar] [CrossRef] [PubMed]
- Raschi, E.; Moretti, U.; Salvo, F.; Pariente, A.; Cosimo Antonazzo, I.; De Ponti, F.; Poluzzi, E. Evolving Roles of Spontaneous Reporting Systems to Assess and Monitor Drug Safety . Available online: http://dx.doi.org/10.5772/intechopen.79986 (accessed on 10 January 2023).
- Barbieri, M.A.; Sorbara, E.E.; Cicala, G.; Santoro, V.; Cutroneo, P.M.; Franchina, T.; Spina, E. Adverse Drug Reactions with HER2-Positive Breast Cancer Treatment: An Analysis from the Italian Pharmacovigilance Database. Drugs - Real World Outcomes 2022, 9, 91–107. [Google Scholar] [CrossRef]
- Barbieri, M.A.; Sorbara, E.E.; Cicala, G.; Santoro, V.; Cutroneo, P.M.; Franchina, T.; Santarpia, M.; Silvestris, N.; Spina, E. Safety profile of tyrosine kinase inhibitors used in non-small-cell lung cancer: An analysis from the Italian pharmacovigilance database. Front. Oncol. 2022, 12, 1005626. [Google Scholar] [CrossRef]
- Jagieła, J.; Bartnicki, P.; Rysz, J. Nephrotoxicity as a complication of chemotherapy and immunotherapy in the treatment of colorectal cancer, melanoma and non-small cell lung cancer. Int. J. Mol. Sci. 2021, 22, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Van Wynsberghe, M.; Flejeo, J.; Sakhi, H.; Ollero, M.; Sahali, D.; Izzedine, H.; Henique, C. Nephrotoxicity of Anti-Angiogenic Therapies. Diagnostics 2021, 11, 640. [Google Scholar] [CrossRef] [PubMed]
- Palleria, C.; Leporini, C.; Chimirri, S.; Marrazzo, G.; Sacchetta, S.; Bruno, L.; Lista, R.; Staltari, O.; Scuteri, A.; Scicchitano, F.; et al. Limitations and obstacles of the spontaneous adverse drugs reactions reporting: Two “challenging” case reports. J. Pharmacol. Pharmacother. 2013, 4, S66–S72. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Flowchart of reports selection process. Abbreviations: FAERS= US Food and Drug Administration's Adverse Event Reporting System (FAERS) database; mCRC= metastatic colorectal cancer; REG= regorafenib; ENC= encorafenib; CET= cetuximab.
Figure 1.
Flowchart of reports selection process. Abbreviations: FAERS= US Food and Drug Administration's Adverse Event Reporting System (FAERS) database; mCRC= metastatic colorectal cancer; REG= regorafenib; ENC= encorafenib; CET= cetuximab.
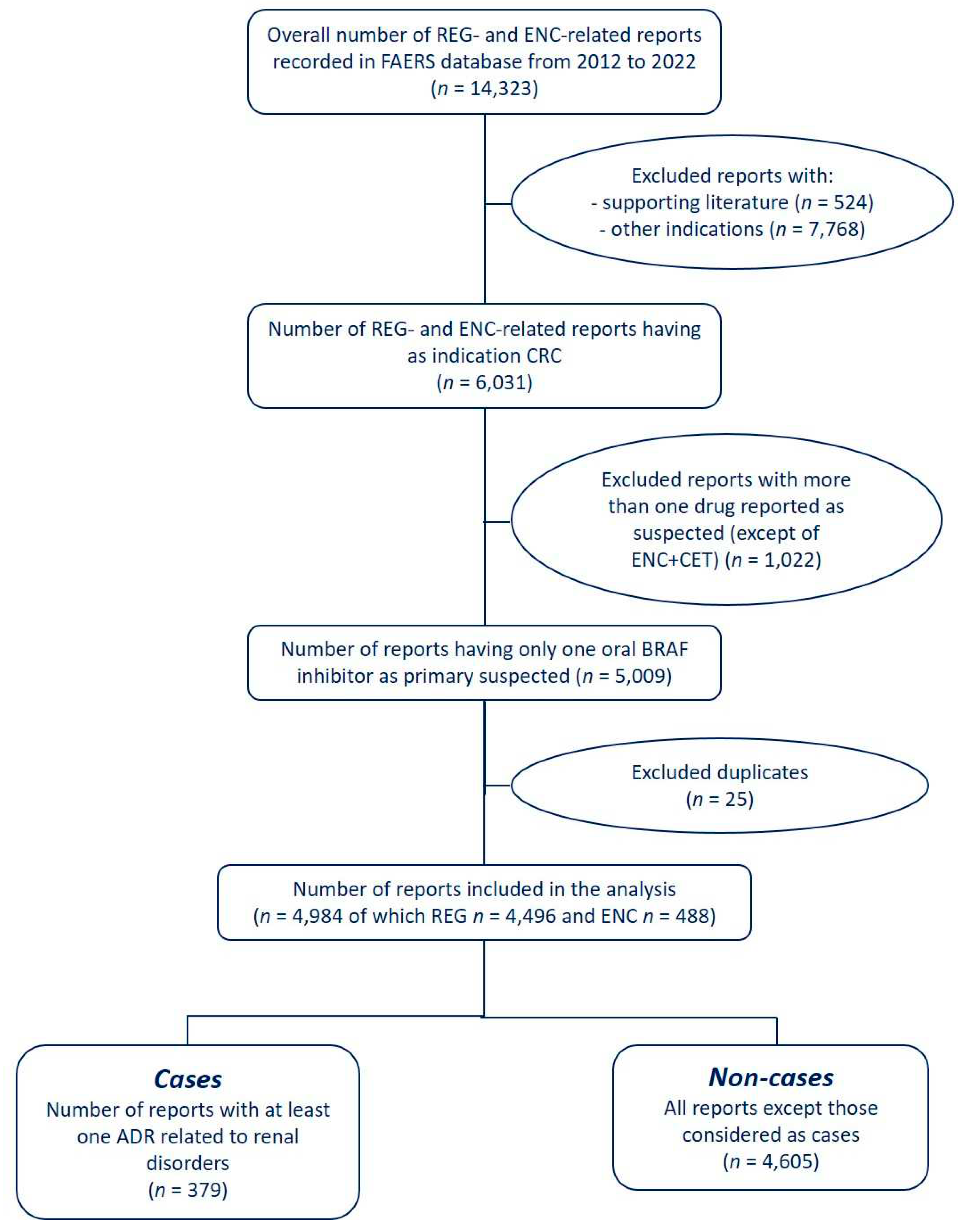
Figure 2.
Time to onset of renal ADRs. Data are reported as box plot with the box drawing from Q1 to Q3 and the horizontal line drawing in the middle to denote the median. Abbreviations: REG= regorafenib; ENC= encorafenib.
Figure 2.
Time to onset of renal ADRs. Data are reported as box plot with the box drawing from Q1 to Q3 and the horizontal line drawing in the middle to denote the median. Abbreviations: REG= regorafenib; ENC= encorafenib.
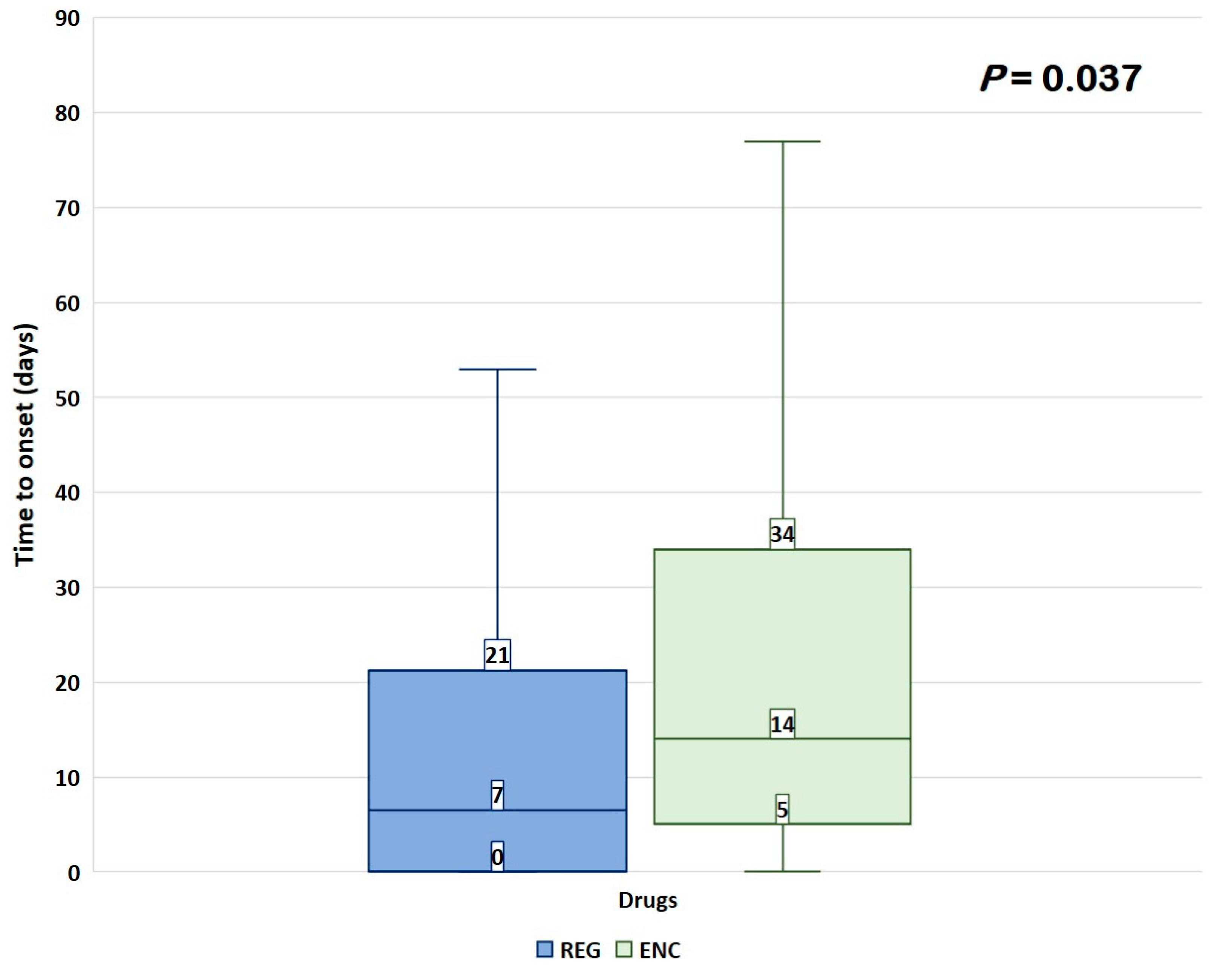

Table 1.
Characteristics of reports with renal disorders related to regorafenib or encorafenib.
| Characteristic | Renal cases (n = 379) |
Other reports (n = 4,605) |
P value | Total (n = 4,984) |
|---|---|---|---|---|
| Gender, n (%) | ||||
| Male | 230 (60.7) | 2,384 (51.8) | 0.006 | 2,614 (52.4) |
| Female | 141 (37.2) | 1,991 (43.2) | 2,132 (42.8) | |
| Not specified | 8 (2.1) | 230 (5.0) | 238 (4.8) | |
| Median age (Q1-Q3), years | 65 (55-71) | 64 (56-71) | 0.886 | 64 (56-71) |
| Age group, n (%) | ||||
| Adult | 170 (44.9) | 1,990 (43.3) | 0.494 | 2,160 (43.3) |
| 18-29 years | 0 (0.0) | 26 (0.6) | 0.197 | 26 (0.5) |
| 30-49 years | 40 (10.6) | 399 (8.7) | 439 (8.8) | |
| 50-64 years | 130 (34.3) | 1,565 (34.0) | 1,695 (34.0) | |
| Elderly | 170 (44.9) | 1,830 (39.8) | 2000 (40.1) | |
| 65-75 years | 125 (33.0) | 1,283 (27.9) | 0.449 | 1,408 (28.3) |
| 76-85 years | 42 (11.1) | 487 (10.6) | 529 (10.6) | |
| >85 years | 3 (0.8) | 60 (1.3) | 63 (1.3) | |
| Missing | 39 (10.3) | 785 (17.0) | 824 (16.5) | |
| Reporter type, n (%) | ||||
| Consumer | 184 (48.5) | 1,941 (42.1) | 0.025 | 2,125 (42.6) |
| Healthcare professional | 194 (51.2) | 2,617 (56.8) | 2,811 (56.4) | |
| Not specified | 1 (0.3) | 47 (1.0) | 48 (1.0) | |
| Reporter Country, n (%) | ||||
| Africa | 1 (0.3) | 34 (0.7) | 0.457 | 35 (0.7) |
| Asia | 98 (25.9) | 1,063 (23.1) | 0.244 | 1,161 (23.3) |
| Europe | 75 (19.8) | 783 (17.0) | 0.190 | 858 (17.2) |
| North America | 177 (46.7) | 2,199 (47.8) | 0.734 | 2,376 (47.7) |
| Oceania | 4 (1.1) | 49 (1.1) | 0.987 | 53 (1.1) |
| South America | 12 (3.2) | 141 (3.1) | 0.910 | 153 (3.1) |
| Not specified | 12 (3.2) | 336 (7.3) | - | 348 (7.0) |
| Serious, n (%) | 370 (97.6) | 4,122 (89.5) | <0.001 | 4,492 (90.1) |
| Outcome, n (%) | ||||
| Died | 78 (20.6) | 970 (21.1) | 0.876 | 1,048 (21.0) |
| Disabled | 5 (1.3) | 53 (1.2) | 0.964 | 58 (1.2) |
| Hospitalized | 150 (39.6) | 1,273 (27.6) | <0.001 | 1,423 (28.6) |
| Life threatening | 15 (4.0) | 96 (2.1) | 0.028 | 111 (2.2) |
| Non-serious | 9 (2.4) | 483 (10.5) | <0.001 | 492 (9.9) |
| Other outcomes | 122 (32.2) | 1,727 (37.5) | 0.045 | 1,849 (37.1) |
| Required intervention | 0 (0.0) | 3 (0.1) | - | 3 (0.1) |
| Year of reporting, n (%) | ||||
| 2012 | 6 (1.6) | 75 (1.6) | 0.946 | 81 (1.6) |
| 2013 | 40 (10.6) | 619 (13.4) | 0.129 | 659 (13.2) |
| 2014 | 33 (8.7) | 477 (10.4) | 0.352 | 510 (10.2) |
| 2015 | 47 (12.4) | 491 (10.7) | 0.336 | 538 (10.8) |
| 2016 | 41 (10.8) | 316 (6.9) | 0.006 | 537 (7.2) |
| 2017 | 38 (10.0) | 437 (9.5) | 0.802 | 475 (9.5) |
| 2018 | 50 (13.2) | 416 (9.0) | 0.010 | 466 (9.3) |
| 2019 | 34 (9.0) | 366 (7.9) | 0.544 | 400 (8.0) |
| 2020 | 25 (6.6) | 458 (9.9) | 0.043 | 483 (9.7) |
| 2021 | 34 (9.0) | 515 (11.2) | 0.216 | 549 (11.0) |
| 2022 | 31 (8.2) | 435 (9.4) | 0.470 | 466 (9.3) |
| Primary suspect drug | ||||
| ENC | 26 (6.9) | 462 (10.0) | 0.046 | 488 (9.8) |
| REG | 353 (93.1) | 4,143 (90.0) | 4,496 (90.2) |
ENC = encorafenib; Q1= quartile 1; Q3= quartile 3; REG = regorafenib. * Calculated Adults vs. Elderly
Table 2.
Disproportionality analyses, included ROR and IC, and notoriety based on FDA label for renal and urinary ADRs related to ENC and REG.
Table 2.
Disproportionality analyses, included ROR and IC, and notoriety based on FDA label for renal and urinary ADRs related to ENC and REG.
| Preferred Term | ENC | REG | Total | ||||||
|---|---|---|---|---|---|---|---|---|---|
| N | ROR (95% CI) | IC (IC025-IC075) | Unexpected | N | ROR (95% CI) | IC (IC025-IC075) | Unexpected | ||
| Renal Impairment | 3 | 2.35 (0.75-7.31) | 53 | 4.16 (3.17-5.45) | 1.39 (1.12-1.66) | Yes | 56 | ||
| AKI | 11 | 3.79 (2.09-6.90) | 1.32 (0.72-1.91) | Yes | 43 | 1.46 (1.08-1.97) | 0.37 (0.07-0.67) | Yes | 54 |
| Chromaturia | 44 | 12.00 (8.92-16.16) | 2.36 (2.06-2.66) | Yes | 44 | ||||
| Renal Failure | 2 | NA | 38 | 1.66 (1.20-2.28) | 0.49 (0.17-0.81) | Yes | 40 | ||
| Proteinuria | 29 | 11.01 (7.64-15.86) | 2.24 (1.87-2.60) | No | 29 | ||||
| Urinary Retention | 27 | 4.99 (3.42-7.28) | 1.53 (1.15-1.91) | Yes | 27 | ||||
| Dysuria | 4 | 6.50 (2.43-17.39) | 1.86 (0.88-2.85) | Yes | 19 | 3.06 (1.95-4.81) | 1.06 (0.61-1.52) | Yes | 23 |
| Haematuria | 22 | 3.29 (2.16-5.00) | 1.14 (0.72-1.56) | No | 22 | ||||
| Renal Disorder | 1 | NA | 19 | 2.72 (1.73-4.26) | 0.95 (0.50-1.40) | Yes | 20 | ||
| Urinary Incontinence | 13 | 2.46 (1.43-4.24) | 0.85 (0.30-1.39) | Yes | 13 | ||||
| Hydronephrosis | 1 | NA | 10 | 8.70 (4.67-16.19) | 1.85 (1.23-2.47) | Yes | 11 | ||
| Pollakiuria | 2 | NA | 8 | 1.18 (0.59-2.36) | 10 | ||||
| Renal Pain | 2 | NA | 6 | 4.08 (1.83-9.10) | 1.19 (0.39-1.99) | No | 8 | ||
| Nephrolithiasis | 1 | NA | 6 | 0.95 (0.43-2.11) | 7 | ||||
| Nephrotic Syndrome | 7 | 5.73 (2.73-12.03) | 1.47 (0.73-2.21) | No | 7 | ||||
| Anuria | 6 | 3.48 (1.56-7.76) | 1.07 (0.27-1.87) | Yes | 6 | ||||
| Nocturia | 6 | 3.39 (1.52-7.55) | 1.05 (0.25-1.85) | Yes | 6 | ||||
| Oliguria | 5 | 3.25 (1.35-7.81) | 0.99 (0.11-1.87) | Yes | 5 | ||||
| Urinary Tract Obstruction | 5 | 9.16 (3.81-22.04) | 1.66 (0.78-2.54) | Yes | 5 | ||||
| Haemorrhage Urinary Tract | 4 | 11.23 (4.21-29.96) | 1.66 (0.68-2.64) | No | 4 | ||||
| Micturition Urgency | 4 | 2.28 (0.86-6.08) | 4 | ||||||
| Prerenal Failure | 4 | 22.13 (8.29-59.11) | 1.89 (0.91-2.87) | Yes | 4 | ||||
| Urine Odour Abnormal | 4 | 4.61 (1.73-12.28) | 1.19 (0.21-2.17) | Yes | 4 | ||||
| Bladder Disorder | 3 | 1.96 (0.63-6.09) | 3 | ||||||
| CKD | 3 | 0.23 (0.07-0.72) | 3 | ||||||
| Micturition Disorder | 3 | 5.78 (1.86-17.95) | 1.23 (0.10-2.37) | Yes | 3 | ||||
Significant RORs are in bold type. NA= not available because there were fewer than three reports. AKI = acute kidney injury; CI = confidence interval; CKD = chronic kidney disease; ENC = encorafenib; NA = not applicable; IC = information component; PT = preferred term; REG = regorafenib; ROR = Reporting Odds Ratio.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



