Submitted:
27 July 2023
Posted:
28 July 2023
You are already at the latest version
Abstract
This study analyzes the effect of economic growth and income distribution on health inequality using data from the Organization for Economic Cooperation and Development (OECD). A panel analysis was conducted by combining 21 years of data (from 2000 to 2020) from 38 OECD countries. Life expectancy and avoidable mortality were set as the dependent variables; gross domestic product and poverty gap were set as the independent variables; body mass index, consumption, smoking rate, healthcare personnel, number of beds in health service facilities, national medical expenses, and unemployment were set as control variables. First, economic growth and poverty gap significantly affect life expectancy and avoidable mortality. It has been confirmed that to resolve health inequality, growth during growth and distribution must be prioritized. Second, it has been confirmed that as the poverty gap increases, life expectancy increases and the avoidable mortality rate decreases. A mechanism different from the existence of a medical security system targeting the lowest class or an increase in the welfare of society worked. In conclusion, as a policy proposal to alleviate health inequality, this study suggests that policy intervention is necessary to block or alleviate the negative impact of income inequality in health care policies.
Keywords:
Inequality of Health
; Health Disparity
; National Welfare
; Panel Analysis
; Fixed Effect Model
1. Introduction
Gross domestic product (GDP), which is confined to national income, has been used as an indicator of the quality of life of people in combination with two conditions—namely, the empirical assumption that income exerts an absolute impact on the quality of life and the practical environment for improving living standards after World War II. Level of income is the primary material basis for improving the level of happiness. Economists consider individual happiness as a function of income. That is, the opinion of economists on happiness is that the happiness of individuals, households, and the country increases as income increases, improving the capability to fulfill demands.
However, new approaches for the correlation between income and happiness have emerged, such as a study showing that an increase in the absolute amount of income does not correlate with an increase in happiness [1] and the Esterlin paradox that the increase in happiness proceeds slightly when the increase in income reaches a certain level.
What is the relationship between income and health? Differences in the level of health are as diverse and unequal as those in the level of income. Humans do not have the same features, the way of becoming ill, or even the way to die. In addition to genetic factors, differences in the level of health depend on the social and economic status of parents, which continues to influence people’s lives. The level of income differs according to educational background, resulting in differences in the qualitative and quantitative capabilities of medical services.
This study conducted a conceptual review of the differences in health and health levels. Consequently, describing the concept of health as an absolute unified theory or explanation that transcends time and space is difficult. That is, it should be considered a relative concept that is flexible within the interests of an individual or group by reflecting the generation.
The factors influencing health remain controversial with respect to whether the cause of health is a personal and behavioral result or a social and structural problem [2]. Examining the perspectives of reformism and historical materialism is vital. Reformism emphasizes the importance of social and environmental factors. This approach argues for the need for social and environmental improvements, such as lifestyle and nutrition management, for groups that could develop diseases, as the causes of various diseases interact. Therefore, a reformist position exists within the medical paradigm in a large framework, and health and disease are attributed to individual eating habits and health behaviors such as exercise. Conversely, the historical materialistic perspective emphasizes factors such as social structural inequality, poverty, and poor living conditions, rather than individual behavior. Some view the results of capitalist economic development as a health gap [3,4]. The other point of the historical materialistic view argues that industrialization caused health risk factors, not capitalism itself, which improved the diet, nutrition, and environment of living [5]. Reformism and historical materialistic perspectives have significant relevance to the “cause-related debate” on health responsibility. For example, although reformists include social factors by emphasizing diet, health behavior, and hygiene, they tend to ignore socioeconomic factors such as income and wealth distribution. However, this position perpetuates the notion that premature death is a personal—rather than a social—responsibility [6].
However, to understand health, it is important to understand the relationship between health and the environment, including factors related to individuals, communities, and the macro and political levels. McKeown argued that changes in the socioeconomic environment are more relevant than the quality of medical care [7]. Both the Black Report and Acheson Report, which deal with health inequality in the UK, emphasize that living conditions have a significant influence on health than the quality of medical technology or medical services. Both reports emphasize that socioeconomic, cultural, and environmental conditions, housing or working conditions, and community influences are as important as income distribution [8,9]. Furthermore, the relationship between health and income inequality is controversial, although empirical studies on the relationship between the two variables have been conducted in recent years.
Income influences on health in two conditions. One is the lack of the absolute income necessary to maintain proper health conditions, such as poverty, and the other is the case wherein an intensive income gap causes various social side effects that negatively affect health. The relationship between per capita income and health is mainly addressed in the absolute income hypothesis, while the relationship between income inequality is addressed in the relative income hypothesis. Both hypotheses explain the relationship between income inequality and health, but each has a different explanation.
The absolute income hypothesis (AIH) refers that the effect of income on health refers a diminishing return as income increases [10]. As income increases, the slope of life expectancy and mortality gradually increases. Preston (1976) argued that when economic growth reaches a certain level, life expectancy increases slightly, even if national income increases. Wilkinson (1996) mentioned the level of gross national product per capita as a threshold. Based on this, the AIH refers that the health of individuals is affected by an individual income, not by the condition of income distribution [11]. Moreover, it refers to the effect of income inequality on national health as a compositional effect caused by the presence of lower-income individuals in society. Conversely, the relative income hypothesis (RIH) refers that income inequality affects health, irrespective of the absolute income level of individuals. That is, it is possible to worsen health conditions through income inequality, even when individuals have the same income level. The factor that explains an individual’s health level is personal characteristics and the influence of the group or region to which he belongs, that is, the contextual effect. According to the RIH, a person’s health can be affected by incomes of other people.
The RIH, or the contextual effects on health, is as follows:
Macinko presented a new materialism perspective whereby income deficiencies, such as poverty, influence health because the number of the poor increases as income inequality intensifies[12]. However, this perspective is consistent with the AIH described previously, and the following perspectives can be seen as appropriate contextual effects. Second, the reduction of social investment refers to income inequality, causing under-investment in human capital [13]. They tend to have a lower proportion of the total budget in the medical and educational sectors in intensified income inequality regions than those that do not. This suggests that regions with intensified income inequality have lower HDI indicators on human development index. The more intense the income inequality, the lower the social expenditure, the more inequality prevails, and the different interests of the rich and middle class differ [14]. That is, there is a possibility of a lower supply of public goods, such as public health services, as societies under intensified inequality have become more polarized [15]. Third, from the social psychology perspective, income inequality weakens social cohesion and adversely affects social capital and mutual [16]. That is, residents in regions with intensified income inequality tend to distrust each other, have lower rates of civic group membership, and have less social interaction, which increases crime rates and is strongly correlated with mortality. Income inequality weakens social ties and adversely affects the public health. Finally, from the perspective of "social status" in social psychology, the deterioration of income inequality affects individual social status inequality, which can lead to the deterioration of health. This is because the higher the income inequality, the more likely individuals with lower social status are to be under severe stress and the greater the health impact of low income.

Table 1.
Influence of Income Inequality on Public Health.
| Theory | Social Psychology | New Materialism | |
|---|---|---|---|
| Analytic Level | |||
| Individual |
Social Status: Inequality causes chronic stress in low-income families, which is detrimental to health |
Individual Income: Low-income levels have fewer material conditions to avoid diseases and risks, which is detrimental to health |
|
| Social |
Social Cohesion: Inequality undermines social ties, which leads to low confidence and increased crime rates, which are detrimental to health |
Social Disinvestment: Inequality causes a decline in investment in social and environmental conditions necessary to promote health for low-income people, which is detrimental to health |
|
In conclusion, although many empirical studies have examined the relationship between income inequality and health, income inequality tends to negatively affect health and major values in the public sphere, such as trust and fairness [15,16,19].
As a representative empirical study on the relationship between income and health, Rodgers [17] analyzed the significant correlation between income level and life expectancy and revealed that countries with equal income distribution differ in average life expectancy by up to 10 years compared to countries with unequal income distribution. Willkinson [18] proved this correlation by analyzing the relationship between the Gini coefficient and life expectancy in 11 Organization for Economic Cooperation and Development (OECD) countries. According to the analysis, income distribution has a significant effect on health inequality than GDP. While the effect of the GDP on life expectancy is less than 10%, the income share of low-income families accounts for approximately 75% of life expectancy [20]. Le Grand [21] also revealed that the mortality rate is closely related to income redistribution. In a study of 17 countries, Le Grand found that the relationship between the income of the lower 20% of the poor and the proportion of the country’s total income is important. Kaplan [13] studied the relationship between the proportion of income and total mortality accounted for by the bottom 50% of the total income in 50 states in the United States; they found that income distribution and age-standardized mortality were significantly correlated. This effect appears to be a universal phenomenon, regardless of sex or race.[22]
In this regard, this study conducts a panel analysis with OECD statistics data for 21 years to analyze how economic growth and distribution levels have significant relevance to health inequality.
2. Materials and Methods
2.1. Data Collection
This study applied OECD statistical data to verify health inequalities in OECD countries. The OECD provides health and healthcare data and data from various fields such as employment, social policy, family, and pension per year, thus facilitating the analysis of socioeconomic factors and income inequality. For the analysis, pooled data were combined in a time series of 21 years from 2000 to 2020. Thirty-eight countries (Australia, Austria, Belgium, Canada, Chile, Colombia, Costa Rica, Czech Republic, Denmark, Estonia, Finland, France, Germany, Greece, Hungary, Iceland, Ireland, Israel, Italy, Japan, Korea, Latvia, Lithuania, Luxembourg, Mexico, the Netherlands, New Zealand, Norway, Poland, Portugal, Slovakia, Spain, Switzerland, Turkey, the United Kingdom, and the United States) are subject to analysis.
2.2. Setting Variables
This study empirically analyzes the factors that influence the growth and distribution of health inequality using OECD statistics. Life expectancy (tax) and avoidable mortality (% per 100,000 people) were applied as the dependent variables for health inequality. This is because the patterns of each dependent variable may refer to various conditions depending on economic growth and distribution, unemployment, and poverty. It is reasonable to apply various variables as proxy variables rather than applying a single variable to measure health inequality. Life expectancy is the average age expected to survive in the future of the population aged 40, 60, 65, and 80 years, based on OECD analysis, and an indicator of the overall health status of the people of each country is applied. The avoidable mortality rate is the sum of the preventable mortality rate before accidents and diseases occur and the treatable mortality rate that can be secondarily prevented through examination and treatment after accidents and diseases. It is calculated as the mortality rate per 100,000 people according to OECD population standards.
Proxy indicators of growth and distribution were used as independent variables. GDP, which measures the basic income of a country, is measured as per capita GDP for each country and is based on the US dollar (USD) used as the key currency. In the case of GDP per capita, the deviation between countries is relatively large, and the unit difference is larger than that of the other variables, indicating that the related problem has been solved through log conversion. In the case of distribution, a poverty gap utilizing the concept of relative poverty was applied. Relative poverty is an arbitrary concept in which the meaning of absolute poverty itself is relative [22], and was introduced by Heo et al. [23] as having the possibility of arbitrary or relative judgment being involved in setting standards that are essential for minimum needs. Even in countries with the same relative poverty rate, the poverty gap has been applied as a variable of distribution because it may differ depending on the relative size of poverty, that is, the average income of the lower-income class. The poverty gap is calculated and reflected after taxes and the transfer of income based on 50% of the poverty line.
Additionally, to verify the pure statistical effect of the independent variables, diverse variables that may affect the level of health inequality were controlled. First, the effects of drinking, smoking, and obesity were controlled as health-risk variables. Drinking means consumption per person of the population aged 15 or older, and smoking means smoking rate among the population aged 15 or older, and it was measured as %. Overweight or obesity was presented as the percentage of people with a body mass index (BMI) of 25 or more out of the total population of each country, based on the International Health Organization's BMI index.
Simultaneously, the representative variable, which indirectly measures healthcare resources, was controlled. First, the number of health care personnel and beds was calculated as "health care personnel per 1000 people" and "the number of beds per 1000 people." Health and medical expenses were measured as %, and national medical expenses were controlled for. This study controls for the share of government and compulsory schemes in national medical expenses related to GDP.
Finally, unemployment rate (%) is also a major variable influencing health inequality. Economic activity is directly related to an individual's income [24], and it has been reported that unemployment increases the mortality rate regardless of other variables and affects risk variables related to death [25]. Therefore, in this study, the ratio of the unemployed to the economic population aged 15 years or older was controlled for by OECD standards.
2.3. Analytical Method
The data for the analysis of this study are arranged by combining two spatially different cases (N) and chronologically different cases (T). The combination of these space and time (N×T) data has the advantage of analyzing cross-sectional area fluctuations and temporal fluctuations simultaneously as well as the effect of increasing the degree of freedom. It also enables research on variables that cannot be analyzed using simple cross-sectional data or time-series data because there is little or no volatility in time and space, and enables systematic comparison of causal factors that change spatially or in time. Panel analysis is estimated using generalized Ordinary Least Square (OLS); however, OLS could violate the basic assumptions of several estimates. First, combined data tend to exhibit autocorrelation, which is a correlation between different time points, owing to the characteristics of interdependent observation values over time. Second, there is a heteroscedastic characteristic in which the dispersion of errors varies depending on the unit of time [25,26]. Third, the errors tended to show contemporaneous correlations across spatial units at certain points in time. Fourth, the errors included both time and unit effects [25]. Because OLS has biased, inefficient, or inconsistent estimation problems, this study considers the applicability of OLS.
The analysis procedure was as follows: First, the average and standard deviation of the variables were reviewed using descriptive statistics of the major variables. Second, the Lagrange multiplier test proposed by Breusch and Pagan [27] was conducted to confirm the simultaneous correlation and determine the appropriate model between the pooled OLS and random effects models. Third, through an F-test, an appropriate model was identified between the pooled OLS model and the fixed-effect model. Fourth, to compare the suitability of the fixed effects and pooled OLS models, a Hausman test was conducted to determine a valid model, and the factors influencing health inequality were verified through the final model.
3. Results
3.1. Descriptive Statistics of Variables
3.1.1. Results of Cross-sectional Data Analysis
This section may be divided by subheadings. It should provide a concise and precise description of the experimental results, their interpretation, as well as the experimental conclusions that can be drawn.
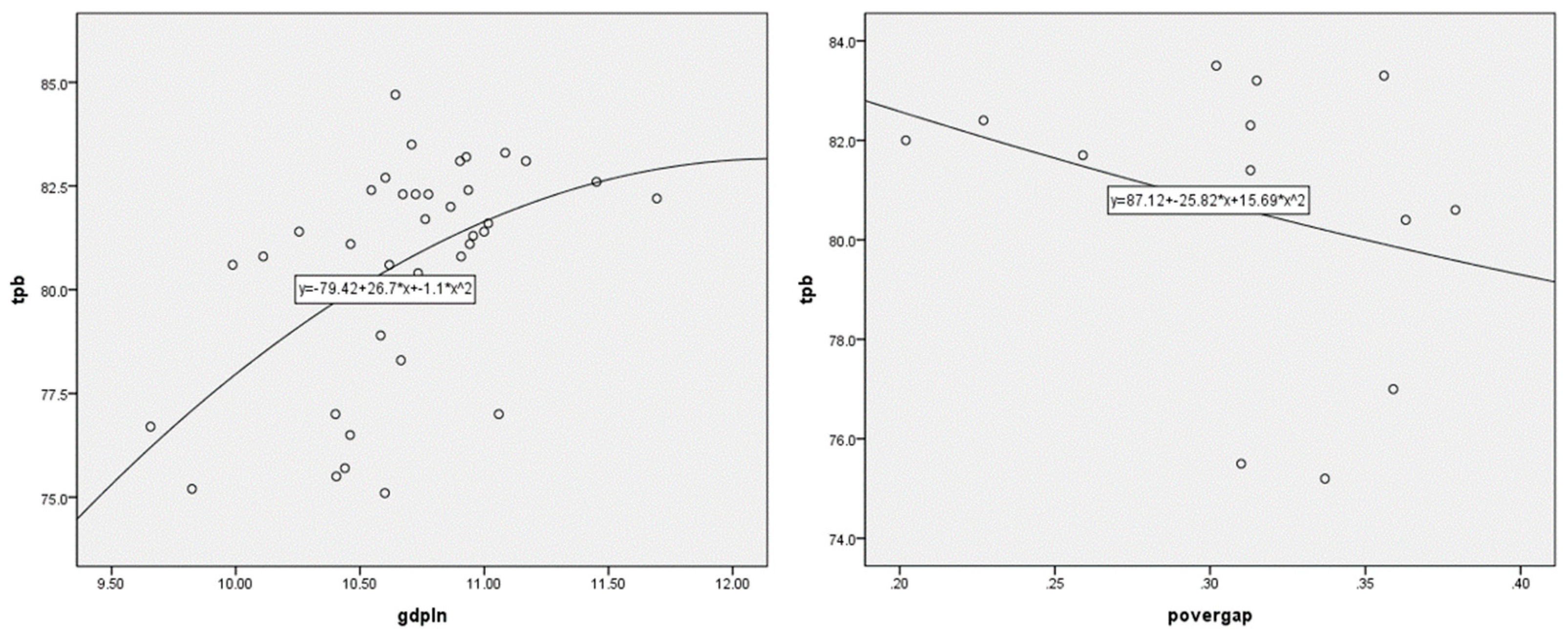
Figure 1.
Relationship between economic growth, poverty gap, and life expectancy (2020 data); The circle refers to individual countries; gdpln logs GDP per capita; puffgap indicates poverty gap; tpb indicates life expectancy.
Figure 1.
Relationship between economic growth, poverty gap, and life expectancy (2020 data); The circle refers to individual countries; gdpln logs GDP per capita; puffgap indicates poverty gap; tpb indicates life expectancy.
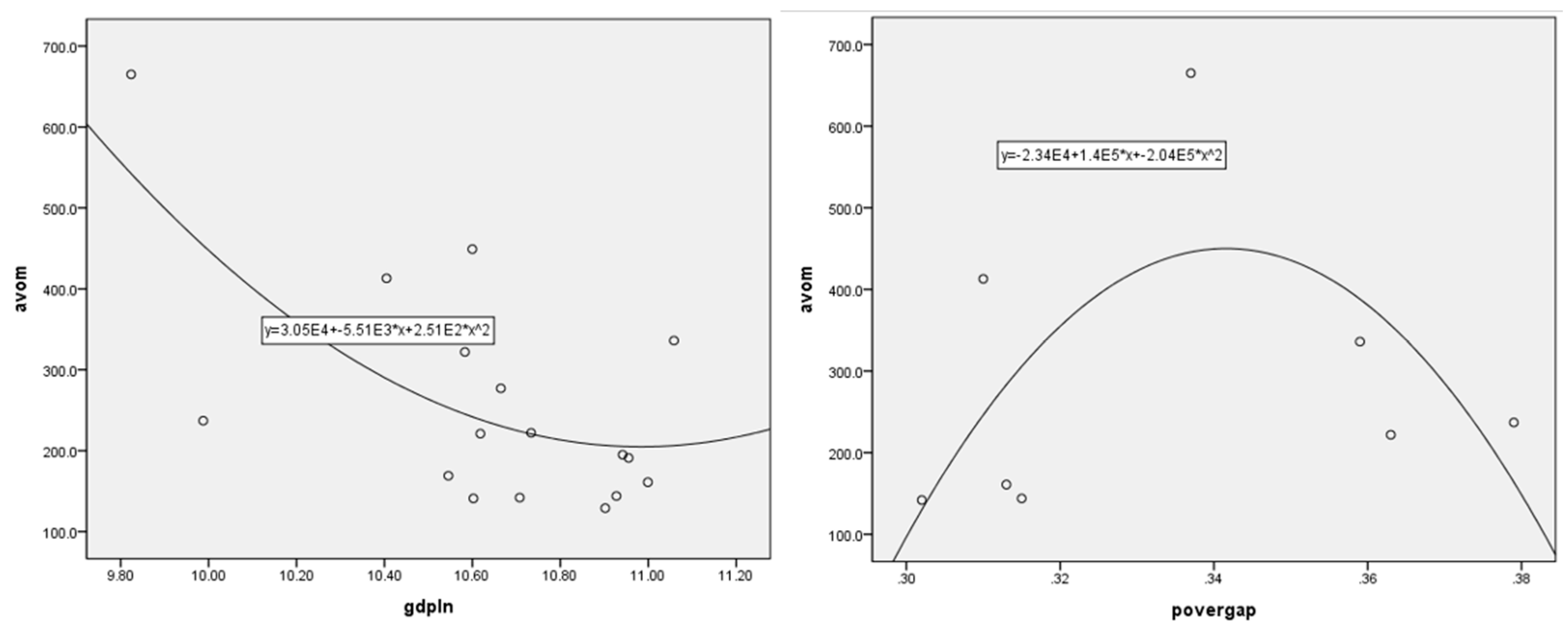
Second is the relationship between economic growth, the poverty gap, and avoidable deaths. When GDP per capita increased, the avoidable death rate of a country continued to decrease. Similar to life expectancy, it was confirmed that if a country's income reached a certain level or higher, a flat section of avoidable deaths appeared, even if income increased.
However, the poverty gap does not intuitively reveal a relationship with avoidable mortality rate. As the poverty gap increases, the avoidable mortality rate increases and then decreases when it reaches a certain level; however, this is not statistically significant. As a result of conducting a regression analysis based on cross-sectional data, both economic growth (β = -.676, t = -1.929, p = .112) and poverty gap (β = -.056, t = -.161, p = .879) could not confirm statistical significance in the avoidable mortality rate.
Figure 2.
Relationship between economic growth, poverty gap, and avoidable death (2020 data) (2020 data); The circle is an individual country, gdpln is the log of GDP per capita, popgap is the poverty gap, and avom is avoidable mortality.
Figure 2.
Relationship between economic growth, poverty gap, and avoidable death (2020 data) (2020 data); The circle is an individual country, gdpln is the log of GDP per capita, popgap is the poverty gap, and avom is avoidable mortality.
In conclusion, the results of the analysis using cross-sectional data have variables that provide intuitive implications; however, most cases do not. Individual-level data were verified based on the statistical data for each country. This is because it is possible to secure far more samples than when using these data. However, in this case, it becomes difficult to compare or control the level of social security, healthcare fiscal expenditure, and influence of medical indicators in individual countries. Therefore, when analyzing country-specific data, a panel analysis that combines space and time data can provide more realistic and practical implications.
3.1.2. Tendency in Key Variables by Country
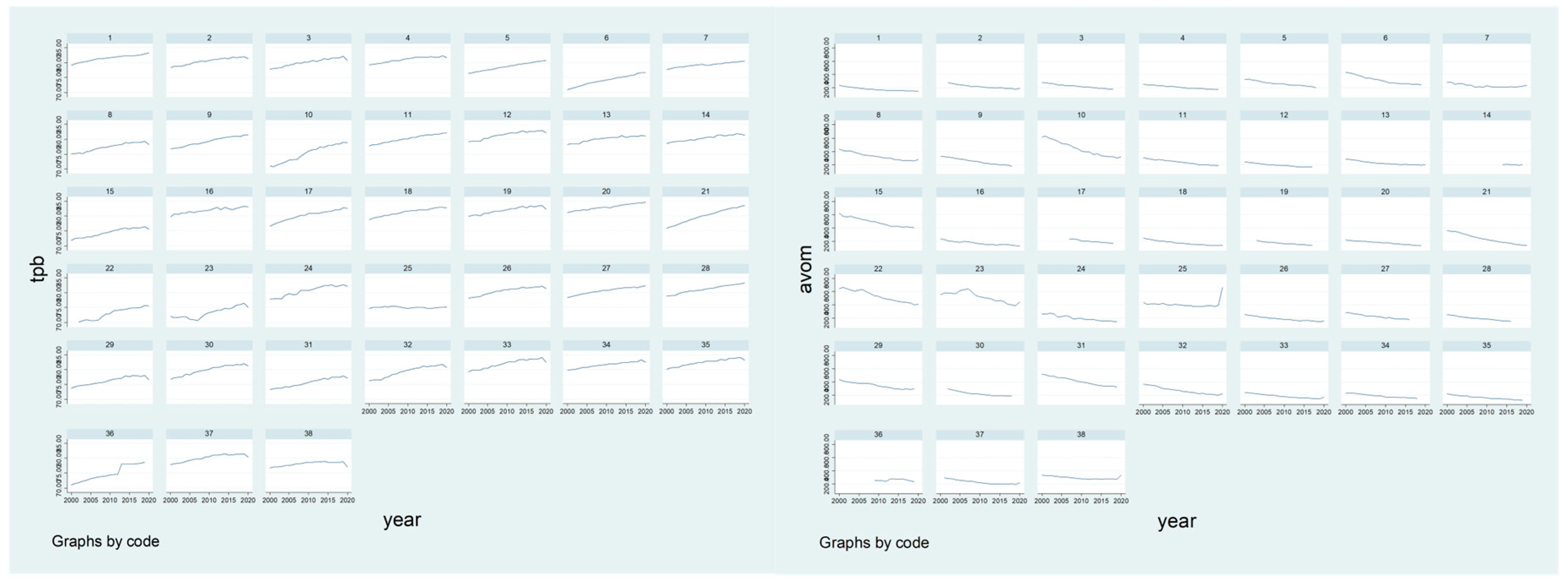
The graph below depicts trends in life expectancy and avoidable fantasy rate in individual countries. First, for life expectancy, there is deviation in each country; however, it has been confirmed that life expectancy continues to increase. This tendency is thought to reflect factors such as economic growth and improvements in medical services. Simultaneously, even in the case of avoidable mortality rate, a relatively decreasing tendency was confirmed. This can also be interpreted because of improvements in living standards, changes in the value of life, and improvements in the quality and quantity of medical services.
Figure 3.
Trends in life expectancy and avoidable mortality.
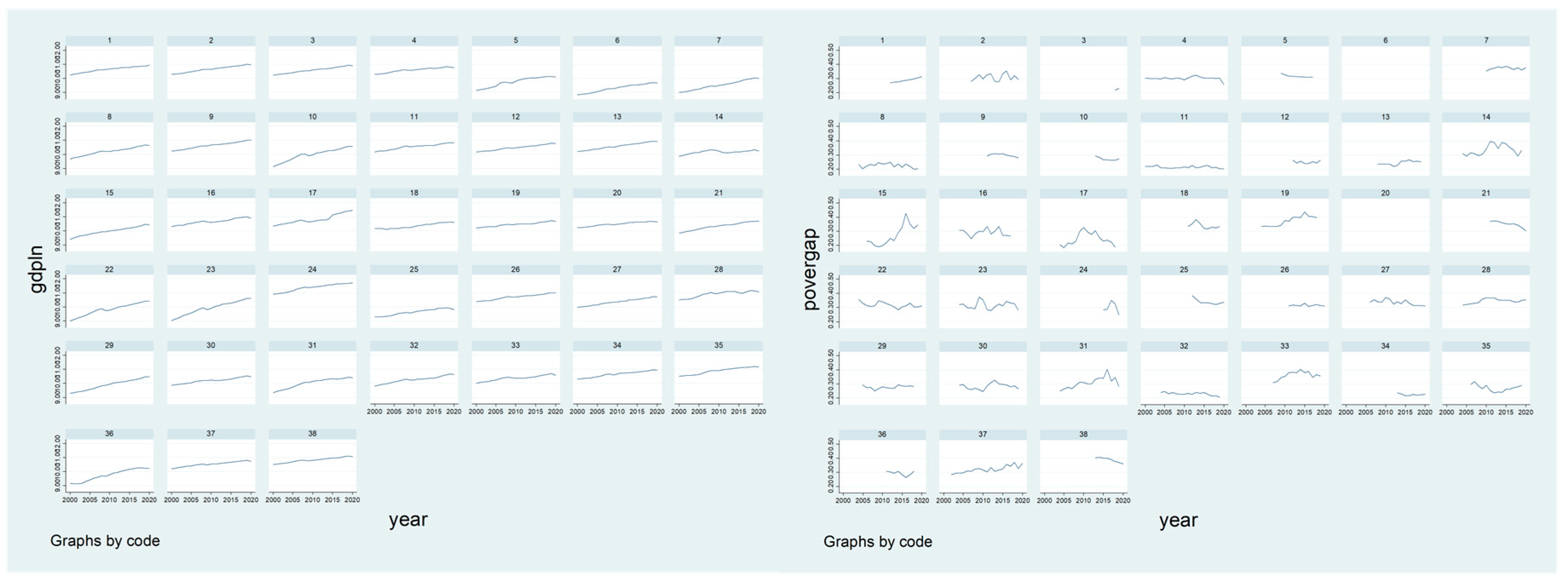
From 2000 to 2020, the per capita GDP of individual countries continued to increase. However, it is difficult to determine the tendencies of the countries uniformly. In general, the poverty gap represents how much income people in the lower-income class must earn to escape poverty, and the degree of insufficient income. Therefore, the lower the average income of the lower-income class, the greater the poverty gap. It is difficult to confirm a tendency of increase or decrease in most countries. The reason for this tendency is evidence that individual countries have prioritized economic growth in the direction of state affairs or have not implemented policies that are advantageous to the lower class, even if various social security systems and redistribution policies exist.
Figure 4.
GDP per capita; trends in poverty gap.
3.1.3. Descriptive Statistics for Panel Data
This study applied 38 countries as the panel group for the analysis, and the total number of observations was 798. Descriptive statistics of the major variables are as follows:
First, for dependent variables, the average life expectancy is 79.14 years, the minimum life expectancy is 70.2 years (2002 in Latvia), and the maximum life expectancy is 84.7 years (2020 in Japan). The average avoidable mortality rate was 267.23%, with a minimum mortality rate of 124.0% (Switzerland in 2019) and a maximum mortality rate of 667.0% (Latvia in 2021).
Among the independent variables, the average per-capita GDP was $34,735, with the minimum value of $6,886 (2000 Colombia) and a maximum value of $119,883 (2020 Luxembourg). The average poverty gap was 0.29%, the minimum value was 0.18% (Ireland, 2005), and the maximum value was 0.44% (Italy, 2015).
The Table 2 refers to the descriptive statistics of the health risks. A review of the proportion of people with a BMI of 25 or higher in individual countries showed that the average was 52.41%, the minimum was 23.7% (Japan in 2012), and the maximum was 75.2% (Mexico in 2018). The average consumption of alcohol per person aged 15 and older was 9.03 l, with the minimum consumption country being 1.2 l per person (2006, 2020 in Turkey), and the maximum consumption being 14.8 l (2007 in Estonia). Among the population aged 15 years and over, the average smoking rate was 26.67%, the minimum smoking rate was 7.3% (2020 Iceland), and the maximum smoking rate was 40.0% (2006 Greece).
Table 2.
Setting Variables.
| Section | Variables | Measurement | |
|---|---|---|---|
| Dependent Variables |
Life Expectancy | Year | |
| Avoidable Mortality |
%, per 100,000 | ||
| Independent Variables |
GDP per capita | GDP per capita (USD), log conversion | |
| Poverty Gap | %, based on 50% of the poverty line | ||
| Controlled Variables | Health Risk | BMI | %, BMI> 25 and more |
| Alcohol Consumption |
Litre, per person of the population aged 15 or older | ||
| Smoking Rate | %, per person of the population aged 15 or older | ||
| Health Care Resources | Health Care Personnel |
per 1000 | |
| The Number of Beds in Health Care Facil-ities |
per 1000 | ||
| Employment | The National Medical Expenses |
%, the share of government and compulsory scheme in national medical expenses to GDP | |
| Unemployment | % | ||
The average number of healthcare personnel per 1000 people who can indirectly measure healthcare resources in OECD countries was 45.41, the minimum number of people was 8.1 (2010 in Turkey), and the maximum number was 110.9 (2019 in Norway). The average number of bed hospitals per 1000 people was 4.89, and the distribution of 0.95 (2019 Mexico) to 14.69 (2000 in Japan) was confirmed. In terms of health and medical costs in OECD countries, the ratio of national medical expenses to GDP is in the range of 8.33%, at least 3.89% (2000 in Korea), and up to 18.81% (2020 in the United States). The average unemployment rate was 7.57%, ranging from 2.01% (2019, Czech Republic) to 27.46% (2013 Greece).
Table 3.
Descriptive statistics of variables.
| Variables | N | Min | Max | Mean | S.D |
|---|---|---|---|---|---|
| Life Expectancy | 795 | 70.2 | 84.7 | 79.14 | 3.08 |
| Avoidable Mortality | 712 | 124.0 | 667.0 | 267.23 | 113.71 |
| GDP per Capita (log conversion) |
798 | 6,886.4 (8.84) |
119,883.0 (11.69) |
34,735.09 (10.34) |
16,982.44 (0.56) |
| Poverty Gap | 436 | 0.18 | 0.44 | 0.29 | 0.05 |
| BMI | 127 | 23.7 | 75.2 | 52.41 | 16.37 |
| Alcohol Consumption | 785 | 1.2 | 14.8 | 9.03 | 2.91 |
| Smoking Rate | 435 | 7.3 | 40.0 | 19.71 | 5.89 |
| Health Care Personnel | 727 | 8.1 | 110.9 | 45.41 | 23.01 |
| The Number of Beds in Health Care Facilities | 744 | 0.95 | 14.69 | 4.89 | 2.60 |
| The National Medical Expenses |
798 | 3.89 | 18.81 | 8.33 | 2.17 |
| Unemployment | 747 | 2.01 | 27.46 | 7.57 | 4.01 |
3.2. Determination of a Panel Analysis Model
3.2.1. Lagrange Multiplier Test
It is necessary to determine which model to use in the panel analysis. Therefore, using the Lagrange multiplier test for the two dependent variables, we determined which model was more suitable: the random effects model or the pooled OLS model.
First, when the dependent variable was life expectancy, the null hypothesis was rejected at the 1% significance level because the p-value (.0006) of the analysis was less than .01. Therefore, it was concluded that a probability effect model should be estimated by considering the individual characteristics of the panel rather than estimating the pooled OLS model. For the avoidable mortality rate as the dependent variable, the p-value (.0363) was less than .05; therefore, it was rejected at the 5% significance level.
3.2.2. F-Test
An F-test was performed on 798 observations and 38 panel groups (countries) to confirm that the estimated coefficients are all close to zero. The p-value of the F-test is less than .01, and the null hypothesis was rejected at the 1% significance level. Therefore, the fixed-effects model, which considers the individual characteristics of the panel, is more appropriate than the pooled OLS model.
3.2.3. Hausman Test
Using the Lagrange multiplier test and F-test, this research model shows that the pooled OLS model is unsuitable. Therefore, the Hausman test determines which of the fixed- and random-effect models are more suitable. If the null hypothesis is rejected, the fixed effects model is valid; the random effects model is valid if the null hypothesis is not rejected.
In this study, the Stata command 'sigmamore was used to increase the robustness of the test. The Hausmann test results are as follows:
First, because of the test, the null hypothesis was rejected at the 5% significance level because the prob>chi2 value (.0190) is less than .05. That is, the fixed-effects model may be determined to be more appropriate than the random effects model. As a result of the test, the prob>chi2 value of the avoidable mortality rate is .0209, and the null hypothesis was adopted. Therefore, the fixed-effects model was judged to be a more appropriate analytical model. As a result of the test, the null hypothesis was rejected at the 1% significance level because the prob>chi2 value (.0002) is less than .01. That is, the fixed effects model was more appropriate than the random effects model.
Therefore, the final model of this study was estimated as a fixed effects model, as shown in <Equation 1>, where i denotes the number of cross-sectional data, t is the number of time-series data, and k is the number of independent and control variables. β1yit-1 is the input of a parallax dependent variable into an independent variable to remove autocorrelation.
3.3. Results of Panel Analysis
By analyzing the effect of growth and distribution on health inequality, the impact on life expectancy was analyzed using a fixed-effects model. By controlling for variables that can affect life expectancy inequality, we found that per capita GDP has a statistically significant effect on life expectancy (β = 3.943, p < .01). That is, life expectancy improved as the GDP per capita increased. Simultaneously, the poverty gap was statistically significant for life expectancy (β = 5.711, p < .01). These results may appear somewhat contrary to social norms. This is contrary to previous studies [13,17,18,21] that if income inequality intensifies, the life expectancy of people gradually decreases. However, unlike the Gini coefficient, the method for measuring income inequality may be interpreted from a different perspective if it is measured as a poverty gap. The Gini coefficient, a representative inequality index, represents the income imbalance of society as a whole. However, the poverty gap focuses on the average income of the lower classes. Therefore, an increase in the Gini coefficient does not necessarily indicate an increase in the poverty gap. However, even if the country's economic growth improves living conditions and quantitative and qualitative access to medical services, this can be interpreted as a lack of appropriate redistribution policies (specifically for the lower class) or social security policies that have not helped the lowest class. This is because, as confirmed in the above longitudinal graph, the phenomenon of a decreasing poverty gap has not been confirmed despite the national redistribution policy and social security system. The variables that have a significant effect on the control variables are reviewed below. Generally, a country's health and medical resources include hospital facilities (total hospital beds), health and medical personnel (number of doctors and nurses), medical equipment, and medical technology (CT scanners and MRI equipment). Among them, health and medical personnel (β = .089, p < .05) has a significant effect on the increase in life expectancy, and the unemployment rate (β = .183, p < .01) has a statistically significant effect on life expectancy. However, the higher the unemployment rate, the higher the life expectancy of individuals, resulting in results different from those of previous studies.
Moreover, the results of identifying variables affecting the avoidable mortality rate, similar to life expectancy, confirmed that per capita GDP, poverty gap, and control variables, such as healthcare personnel and unemployment, had a statistically significant effect. That is, as the economy grew and the number of health and medical personnel increased, the socially preventable mortality rate decreased. However, the avoidance mortality rate decreased as the poverty gap and unemployment rates increased.
Table 4.
Analysis Results.
| Life Expectancy | Avoidable Mortality | |||||
|---|---|---|---|---|---|---|
| variables | Coef. | Std.Err | T | Coef. | Std.Err | t |
| GDP per capita | 3.943 | .939 | 4.20** | -137.647 | 28.664 | -4.80** |
| Poverty Gap | 5.711 | 1.825 | 3.16** | -120.890 | 53.288 | -2.27** |
| BMI | .012 | .018 | .67 | .391 | .531 | .74 |
| Alcohol Consumption |
.004 | .079 | .05 | .280 | 2.188 | .13 |
| Smoking Rate | .009 | .031 | .29 | -.640 | .893 | -.72 |
| Health Care Personnel |
.089 | .026 | 3.38** | -2.430 | .766 | -3.17** |
| The Number of Beds in Health Care Facilities | -.030 | .051 | -.59 | 1.682 | 1.420 | 1.18 |
| The National Medical $Expenses | .095 | .112 | .85 | .097 | 3.381 | .03 |
| Unemployment | .183 | .046 | 3.98** | -5.238 | 1.300 | -4.03** |
| A Constant | 29.978 | 9.677 | 3.10** | 1844.684 | 286.219 | 6.45** |
*p<0.05, **p<0.01.
4. Discussion and Conclusion
This study analyzed how a country’s growth and distribution are significantly correlated with health inequality. A panel analysis was conducted using 21 years of time-series data for 38 OECD countries. The analysis results are summarized as follows:
First, the influence of independent variables that could not be confirmed in cross-sectional analysis was statistically significant as a result of panel analysis. In the case of cross-analysis of OECD data, the number of small samples (number of countries) may cause distortion of the analysis results. At the same time, it is difficult to compare or control the level of social security, the level of health care fiscal expenditure, and the level of impact of medical indicators in individual countries in the case of using statistics by country in individual. Therefore, panel analysis that combines space and time data could derive more practical implications as in this study.
Second, it was confirmed that economic growth (GDP per capita) influences on life expectancy and avoidable mortality as a result of panel analysis.
Economic growth and income distribution affect life expectancy and avoidable mortality rates. In particular, an increase in GDP per capita increases life expectancy and decreases avoidable mortality rate. Economic growth affects individual countries in various ways, including changes in living standards, diversification of individual values, development and accessibility of medical services, and development of medical technology, increasing life expectancy and decreasing preventable deaths.
Third, it has been confirmed that as the poverty gap increases, life expectancy increases and the avoidable mortality rate decreases.
Generally, income inequality is known to negatively affect health inequality; however, the results of this study are conflicting. In this regard, unlike the Gini coefficient, the poverty gap does not represent income distribution in society. That is, the poverty gap focuses on the average income of the lower class rather than on the Gini coefficient. Thus, an improvement in the Gini coefficient does not necessarily indicate an improvement in the poverty gap. Therefore, it provides the meaning that health inequality can improve even if the average income of the lower class does not improve. Perhaps, each country has a separate specialized medical system for the lowest class (i.e., Korea has a medical benefit system); thus, if the poverty gap increases, it is likely to be included in the related medical security system. In other words, it has possibility that a new medical security system for the poor will be established or coverage of the existing medical security system will be expanded in the case of growing poverty gap. Therefore, as in this study, income inequality cannot necessarily be judged to have a negative effect on health inequality. That is, it should be noted that an increase in the poverty gap causes medical intervention and expansion of social security for the lowest class, resulting in improvement of health inequality. These analysis results are difficult to confirm in cross-sectional analysis, and it is derived through panel analysis. Furthermore, there is a discussion that when income inequality in society as whole increases, relative deprivation affects various paths of health inequality through socio-psychological factors and awareness of inequality. However, even before the lowest class recognized relative deprivation, social-structural inequality existed. That is, social and psychological factors such as deprivation can occur depending on the proportion of all members of society; however, if limited to the lower class, social and psychological factors can have less influence. In addition, the increase in quality of life or satisfaction of the second-highest class may have had a greater impact on the overall welfare of society.
Considering the impact of economic growth and income inequality on health, it is necessary to pay attention to income inequality and lower-class healthcare policies in the future. Preceding literatures have empirically proven the causal effects of social protection systems and regime on health [28,29]. Thus, it is necessary to strengthen the potential role of social protection and to strengthen the comprehensive medical service system and poverty policy. Policy interventions are required to block or alleviate the negative effects of income inequality [30]. According to Sen [31], health is a key element in the ability to properly enjoy and claim basic rights and opportunities for political and economic participation in democracy. As physical and mental health status is related to basic energy in daily life, such as economic, cultural, and political activities [32], the deterioration of health owing to income inequality has side effects that undermine the overall capacity of life. Simultaneously, if income inequality leads to health deterioration through various non-health paths, support for the vulnerable needs to be strengthened through non-health policies such as education, housing welfare, transportation, and improvement of the working environment [33]. Policy support in the non-medical sector should be provided along with health support in various forms to enhance the capabilities of poor or vulnerable groups sensitive to the negative effects of income inequality. Furthermore, efforts are required to design health policies that reduce social gaps and promote equity, along with policies that can macroscopically reduce income inequality.
Supplementary Materials
The following supporting information can be downloaded at: Preprints.org.
Author Contributions
Han conducted all procedure of this study.
Funding
This research received no external funding
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
All data and material are available through the website of OECD. Stat (OECD Statistics) Portal.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Dusenberry, J. Income, Saving and the Theory of Consumer Behaviors; Harvard University Press: Cambridge, 1949. [Google Scholar]
- Doyal, L.; Pennell, I. The Political Economy of Health; Pluto Press: London, UK, 1979. [Google Scholar]
- Navarro, V. Class, Struggle, the State and Medicine; Martin Robertson: London, UK, 1978. [Google Scholar]
- Townsend, P. Individual or Social Responsibility for Premature Death? Current Controversies in the British Debate about Health. International Journal of Health Services 1990, 20, 373–392. [Google Scholar] [CrossRef]
- Hart, N. Is Capitalism Bad for Your Health? British Journal of Sociology 1982, 33, 435–443. [Google Scholar] [CrossRef]
- Townsend, P. Individual or Social Responsibility for Premature Death? Current Controversies in the British Debate about Health. International Journal of Health Services 1990, 20, 373–392. [Google Scholar] [CrossRef] [PubMed]
- Marmot, M.G. Improvement of Social Environment to Improve Health. The Lancet 1998, 351, 57–60. [Google Scholar] [CrossRef] [PubMed]
- Whitehead, M. Tackling Inequalities a Review of Policy Initiatives. In Tackling Inequalities in Health: An agenda for action; Benzeval, M., Judge, Whitehead, K. M., Eds.; Kings Fund: London, UK, 1995. [Google Scholar]
- Hertzman, C.; Frank, J.; Evans, R. G. Heterogeneities in Health Status and the Determinants of Population Health. In Why are some people healthy and others not? The determinants of the health of population; Evans, R. G., Barer, M., Mormor, L. T. R., Eds.; de Gruyter: New York, US 1994. [Google Scholar]
- Berkman, L. F.; Kawachi, I. Social Epidemiology; Oxford University: Oxford, UK, 2000. [Google Scholar]
- Wagstaff, A.; Doorslaer, E. van. Income Inequality and Health: What does the Literature Tell Us? Annual Review of Public Health 2000, 21, 543–567. [Google Scholar] [CrossRef] [PubMed]
- Karlsson, M.; Nilsson, T.; Lyttkens, C.; Leeson, G. Income inequality and health: importance of a cross country perspective. Social Science & Medicine 2010, 70, 875–885. [Google Scholar]
- Kaplan, G.A.; Pamuk, E.R.; Lynch, J.W.; Cohen, R.D.; Balfour, J.L. Inequality in income and mortality in United State: Analysis of mortality and potential pathways. BMJ. 1996, 312, 999–1003. [Google Scholar] [CrossRef] [PubMed]
- Krugman, P. The spiral of inequality. Mother Jones 1996, 21, 44–49. [Google Scholar]
- Kawachi, I.; Kennedy, B. P.; Lochner, K.; Prothrow-Smith. ,D. Social Capital, Income Inequality, and Mortality. American Journal of Public Health 1997, 87, 1491–1498. [Google Scholar] [CrossRef] [PubMed]
- Asthana, S.; Halliday, D.J. What works in tackling health inequalities? Pathways, policies, and practice through the life course; The Policy Press: Bristol, UK, 2006. [Google Scholar]
- Rodgers, G.B. Income and inequality as determinants of mortality: An international cross-section analysis. Popul Stud 1979, 33, 343–51. [Google Scholar] [CrossRef]
- Willkinson, R.G. Income and mortality. In Class and Health Research and longitudinal data; Willkinson, R., Ed.; Tavistock Publications: London, UK, 1986. [Google Scholar]
- Wilkinson, Richard G. "Income and mortality. In Class and health; Willkinson, R., Ed.; Routledge: London, UK, 2022; pp. 88–114. [Google Scholar]
- Wilkinson, R.G. Income distribution and life expectancy. Br Med J 1992, 304, 165–168. [Google Scholar] [CrossRef] [PubMed]
- Le Grand, J. Inequalities in health: Some international comparisons. Eur Econ Rev 1987, 31, 182–191. [Google Scholar] [CrossRef]
- Townsend, P. Poverty in the United Kingdom; Penguin: London, UK, 1979. [Google Scholar]
- Heo, J.H.; Cho, Y.T.; Kwon, S.M. The effect of socioeconomic deprivations on health. Korea J Sociol. 2010, 44, 93–120. [Google Scholar]
- Stronks, K.; Van de Mheen, H.; Van den Bos, J.; Mackenbach, J.P. The interrelationship between income, health and employment status. International Journal Epidemiology 1997, 26, 592–600. [Google Scholar] [CrossRef] [PubMed]
- Hicks, A.M.; Janoski, T. The comparative political economy of the welfare state; Cambridge University Press: Cambridge, 1994. [Google Scholar]
- Beck, N.; Katz, J.N. What to do (and not to do) with Time Series Cross Section Models. American Political Science Review 1995, 89, 634–647. [Google Scholar] [CrossRef]
- Breusch, T.S.; Pagan, A.R. The Lagrange multiplier test and its applications to model specification in econometrics. The review of economic studies 1980, 47, 239–253. [Google Scholar] [CrossRef]
- Chung, H. , Muyntaner, C., Welfare state matters: a typological multilevel analysis of wealthy countries. Healthy Policy 2007, 80, 328–338. [Google Scholar] [CrossRef] [PubMed]
- Avendano, M.; Glymour, M. Unemployment insurance policies and the effects of life-course income, wealth, and employment status on late life health: disentangling causal effects, Harvard Center for Population and Development Studies, 2011.
- Kang, Y.J.; Jung, K.H. An empirical study on the inequality of income and health in Korean Society. Korean Public Administration Review 2012, 46, 265–291. [Google Scholar]
- Sen, A.K. Development as freedom; Oxford University Press: Oxford, UK, 1999. [Google Scholar]
- Loehr, J.; Schwartz, T. The power of full engagement: Managing energy, not time, is the key to high performance and personal renewal; The Free Press: Los Angeles, US, 2003. [Google Scholar]
- Kim, C.Y. The way to understand the inequality of health. Health and Welfare Policy Forum 2009, 3, 2–3. [Google Scholar]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



