Submitted:
19 July 2023
Posted:
19 July 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
The COVID-19 pandemic caused by the SARS-CoV-2 virus has led to significant global health implications. Although the respiratory manifestations of COVID-19 are widely recognized, emerging evidence suggests that the disease may also significantly affect the gut microbiota, the intricate community of bacteria that lives within the gastrointestinal system. This extensive article intends to investigate the impact of COVID-19 on the gut microbiota, examining the underlying mechanisms, clinical implications, and potential therapeutic interventions. Understanding the complex interactions between COVID-19 and the gut microbiota will help us to gain valuable insights into the broader consequences of this viral infection on human health.
Keywords:
COVID-19
; Gut Microbiota
; Microbiome
; Dysbiosis
Introduction:
The COVID-19 pandemic is a global health crisis caused by severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2), a single-stranded enveloped positive-sense RNA virus with an average diameter of 75–150 nm that originated in Wuhan, China, at the end of 2019 and spread worldwide [1]. On March 11, 2020, the World Health Organization (WHO) declared COVID-19 a global pandemic [2], and to date, almost 7 million people have died from COVID-19 [3]. The virus predominantly affects the respiratory system, inducing a spectrum of symptoms that can range from mild to severe respiratory impairment, with several symptoms such as pyrexia, respiratory distress, pharyngitis, exhaustion, and myalgia [4]. In more severe cases, COVID-19 infection may lead to the development of pneumonia and acute respiratory distress syndrome (ARDS), may require mechanical ventilation, and lead to a significant risk of mortality [5].
In addition to respiratory manifestations, the pathogenesis of COVID-19 may result in systemic consequences such as the failure of multiple organs and physiological systems throughout the body [6]. COVID-19 manifests as inflammation of the cardiac muscle (myocarditis) [7] and vascular organs (endotheliitis), which increases the risk of blood clots, leading to pulmonary embolism and deep vein thrombosis [8]. Several reports have suggested that COVID-19 is associated with arrhythmia [9] and myocardial infarction [10]. A group of neurological manifestations has been observed in patients with COVID-19, including loss of taste and smell [11], generalized headache[12], dizziness with vertigo [13], seizures [14], encephalitis [15], and Guillain-Barré syndrome [16]. However, the exact mechanism underlying these effects is still under the laboratory bench. Several digestive system symptoms such as nausea, vomiting, diarrhea, and acute abdominal tenderness have been observed in some COVID-19 patients [17]. Renal impairment with acute renal injury is found in COVID-19 patients as a result of an inflammatory reaction by the body or a direct viral invasion of the kidneys [18].
The human gastrointestinal tract (GIT) is densely populated by the microbiota. The gut microbiota, a collection of bacteria, viruses, and fungi that live in the gastrointestinal tract, not only maintains mucosal immunity but also regulates the host's systemic immune response [19]. Gut microbiota plays an important role in a broad range of physiological processes, from the digestion of complex polysaccharides to the regulation of neuronal signaling. In recent decades, it’s getting more and more attention because of its association with a wide variety of diseases, ranging from metabolic disorders (e.g. diabetes and its complications) [20,21,22,23,24,25] to autoimmune diseases (such as rheumatoid arthritis, inflammatory bowel disease, and type 1 diabetes), Obesity [26], cancer [27], reproductive health [28,29,30], sexual disorders [31,32] even neurodevelopmental disorders (e.g. autism) and neurodegenerative diseases (e.g. Alzheimer). Furthermore, modifying the microbiota in the human body may be a key factor for the treatment of disease. According to recent research on various respiratory disorders, gut microbiota may influence immunity and inflammation in the lungs [33]. Several studies observed an association between gut microbiota and SARS-CoV-2. In this review, we summarize the information that is currently available on the interaction between the gut microbiome and the host's immune response to SARS-CoV-2. We continue to explore the relevance of the diversity of the gut microbiome and the variations in its composition as diagnostic indicators as well as the possibility of the gut microbiome as an interventional target in influencing COVID-19 results.
Understanding the composition and diversity of the gut microbiota
Around 100 trillion microorganisms (bacteria, fungi, viruses, protozoa, and viruses) are found in the human gut. The human genome is made up of 23 thousand genes, while the microbiome encodes over 3 million genes producing more than thousands of metabolites, impacting human health [34]. The composition and metabolism of the adult gut microbial communities are affected by a combination of factors including diet, demographics, use of medication, health status, and environmental components shaping the gut environment [35,36,37]. Humans can be herbivorous, carnivorous, and all that, depending on the culture, the food supply, and so on. The diversity of the distinctive microbes of each habitat varies considerably, even in healthy individuals, with a high specialization of niches within and between individuals. According to the Human Microbiome Project Consortium, the overall fecal microbiota richness was estimated to be 226 bacterial genera among 208 donors [38]. The microbiota of the human gut is dominated by two major phyla, Bacteroidetes and Firmicutes [39,40].
Roles of gut microbiota in digestion, nutrient metabolism, and immune regulation:
The gut microbiota provides essential capabilities to digest non-digestible substrates like dietary fibers by fermentation, complex carbohydrates, and very few amounts of fats. This fermentation gives rise to specific gut microbes which produce different types of metabolites including short-chain fatty acids (SCFAs) and alcohols; ammonia, branched-chain fatty acid; glycerol, and choline [41]. Acetate, propionate, and butyrate are the three major SCFAs. Both Butyrate and propionate control gut hormones and decrease food intake and appetite[41,42]. Butyrate is also used as a main energy source of human colonocytes, increases apoptosis in cancer cells, and can induce gluconeogenesis in the intestine. Gut microbes producing propionate regulate satiety by interacting with the gut fatty acid receptors and also control hepatic gluconeogenesis [43]. Acetate is used in cholesterol metabolism and lipogenesis in the peripheral tissues [44]. Microbial enzymes produced in gut microbes help bile acid metabolism by producing un-conjugated and secondary bile acids that influence essential signaling and metabolic pathways in humans [45].
Factors influencing gut microbiota composition, including diet, lifestyle, and medications:
The intestinal microbiota is part and parcel of the human halobionts. Past studies have shown that various factors, such as diet and drugs, play an important role in the composition and diversity of the intestinal microbiome [34,46,47]. Dietary patterns, as well as individual foods, can directly influence the diversity of the microbiome. Artificial sweeteners (Sucralose, aspartame, saccharin) significantly increased Bacteroides, Clostridia, and other aerobic bacteria in the gut. Food additives like emulsifiers in processed food reduced microbial diversity and increased inflammation promoting Proteobacteria [48,49]. Popular food-restrictive diets (vegan, raw food, gluten-free diets) can also impact gut microbial diversity. Some studies have shown the advantages of a vegan diet over an omnivorous diet, but others have not succeeded to prove this theory [50]. Apart from food, drugs are also a key factor in the gut microbiota composition. Drugs such as proton pump inhibitors have a significant impact on microbial composition, which could explain the higher levels of gastrointestinal infection in people taking these drugs. Antibiotics are impacting the intestinal microbiome [51]. Earlier observational human studies have shown an obesogenic effect in humans, even at low doses of antibiotics on food [52].
Gut Microbiota Alterations in COVID-19 Patients:
Several research investigations have explored alterations in gut microbiota in COVID-19 patients illuminating the possible involvement of the gut microbiome in relation to the illness. The aforementioned investigation insights into the association between COVID-19 and gut microbiota dysbiosis, as well as its potential implications for the severity and treatment of the disease. A study conducted by Zuo et al., (2020) examined the gut microbiota composition in COVID-19 patients. The researchers observed a substantial reduction of beneficial commensal bacteria such as Bifidobacterium and Lactobacillus and along with a corresponding increase in opportunistic pathogens, such as Clostridium hathewayi [53]. Another study done by Gu and colleagues in 2020, reported that the alteration of gut microbiota decreased the amount of butyrate-producing bacterial species which are well known for their potential anti-inflammatory effects.
Furthermore, investigations observed that patient with COVID-19 exhibits a reduction of microbial diversity. A study by Zuo et al. (2021) showed a reduction in the prevalence of bacterial species linked to elevated microbial diversity in COVID-19 cases, in comparison with subjects without any underlying health conditions. The connection between a decline in microbial diversity and higher vulnerability to inflammatory illnesses and infections implies that it may be involved in the development of COVID-19 [54]. Interestingly, modifications in the gut microbiota have also been correlated with the severity of COVID-19 disease. According to Yeoh and colleagues' investigation conducted in 2021, it was identified that severe cases of COVID-19 were distinguished by a condition of gut dysbiosis, resulting in a decline in the presence of beneficial bacteria while allowing for an overgrowth of potential pathogens [55]. Another investigation conducted by Gu et al. In the year 2020, it was observed that patients with more severe symptoms have a discernible variation in the composition of their gut microbiota in relation to those experiencing milder symptoms [56]. These studies suggest a possible association between dysbiosis and the severity of symptoms associated with COVID-19.
Dysbiosis in the gut microbiota can lead to impaired regulation of the immune response, elevated systemic inflammation, and increased susceptibility to respiratory infections. Several studies have indicated that dysbiosis of gut microbiota may play a role in the pro-inflammatory conditions witnessed in severe cases of COVID-19. Dhar and Mohanty (2021) reported that the alteration of pro-inflammatory cytokine levels observed in COVID-19 patients, accompanied by evidence of gut dysbiosis, suggests a potential mechanism by which the gut microbiota influences the variability in disease outcomes [57].
The gut microbiota has recently been identified as a promising diagnostic and prognostic indicator for COVID-19. Researchers have identified specific microbial indicators that enable differentiation between individuals afflicted with COVID-19 from healthy individuals. Qin Liu and colleagues, developed a diagnostic model based on gut microbiota demonstrating high efficacy in discerning patients with COVID-19 from those without the infection. Moreover, specific microbial profiles have demonstrated a correlation with the severity of diseases, proposing that gut microbiota analysis could serve as a promising prognostic tool [58].
It is important to consider that the treatment of COVID-19 has a significant effect on gut microbiota. The administration of antibiotics and antiviral agents has been reported to potentially disturb microbial equilibrium, which may ultimately worsen dysbiosis. A study by Lucie et al. reported in 2022, that COVID-19 patients receiving antibiotics had greater dysbiosis compared to those not receiving antibiotics, suggesting the need for prudent administration of antimicrobial agents to ameliorate the potential adverse effects on the gut microbiota [59]. Yeoh and colleagues observed correlations between specific gut microbial taxa and inflammatory markers such as C-reactive protein (CRP) and cytokines with pro-inflammatory properties [55].
Research investigating gut microbiota alterations in COVID-19 patients has elucidated the phenomenon of dysbiosis, a decline in microbial diversity, and potential associations with the severity of the illness. The role of gut microbiota in modulating the immune response and impact of systemic inflammation emphasizes its significance in the pathogenesis of COVID-19.
Mechanisms of Gut Microbiota Dysbiosis in COVID-19
The complex and multifaceted causes of gut microbiota in COVID-19 are difficult to exclude. Although we are still improving our knowledge, several likely explanations have been suggested, according to existing research (Figure 1).
The infiltration of viruses and disruption of the intestinal barrier:
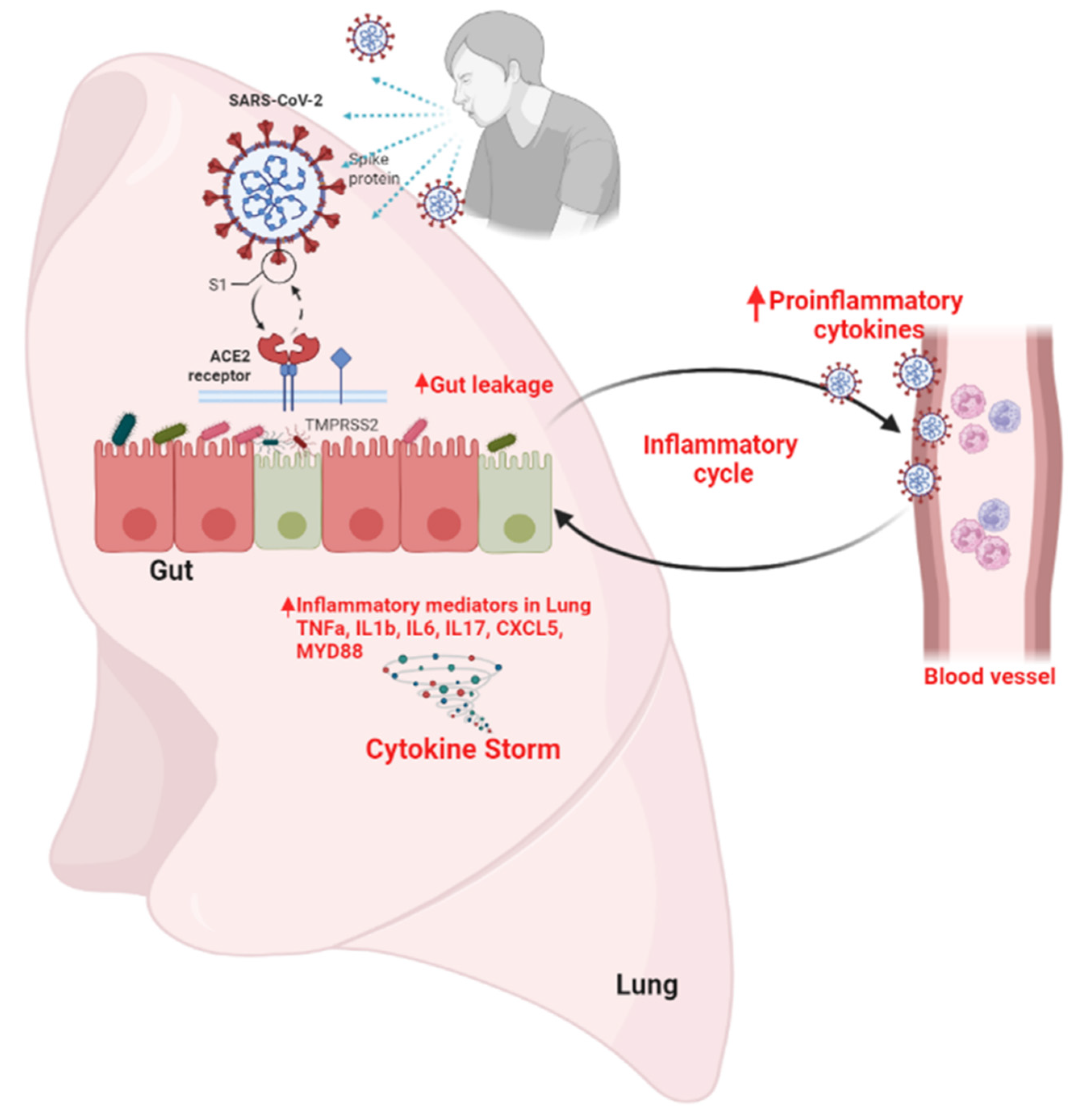
The infiltration of viruses and disruption of the intestinal barrier, SARS-CoV-2, the virus responsible for COVID-19, has been detected in the gastrointestinal tract, suggesting the possibility of direct viral invasion in the gut, suggesting the possibility of direct viral invasion within the gut. This invasion can disrupt the intestinal barrier by compromising its integrity which results increase gut permeability [60,61] As a result, deleterious microbial constituents and toxins possess the capacity to migrate across the bloodstream, eliciting an inflammatory reaction and dysbiosis [62].
Dysregulation of the immune system:
COVID-19 leads to cytokine storm- a hyperactive immune response characterized by the release of interferons, interleukins, tumor necrosis factors, chemokines, and several other mediators which causes injury to host cells. Systemic inflammation as a result of cytokine storm is very obvious [63]. These hyperinflammatory conditions disrupt the balance of the gut microbiota by eliminating both beneficial and harmful bacteria which leads to dysbiosis. Gut microbial metabolites short-chain fatty acids (SCFAs) such as butyric acid and acetic acid are pioneers for an immune response [64]. SCFAs can also act as inhibitors of histone deacetylase (HDAC) which results from a reduction of inflammatory responses by enhancing the amount and activity of T helper cells, regulatory T cells, and Th17 effector cells [65,66,67,68]. High Lipopolysaccharide (LPS) levels were observed in the circulation in severe and fatal lung injury cases [69]. Dysbiosis of gut microbiota facilitates the translocation of LPS into the portal circulation which stimulates the hepatic kuffer cell to activate the NF-κB pathway and secretion of TNF-α and IFN-β [53]. This can cause hepatic inflammation as well as systemic inflammation [70].
Effects of antibiotic treatments:
A group of investigations has been done previously which implies that the use of antibiotics can impact gut microbiota. Antibiotics such as amoxicillin [71], ciprofloxacin [72], and cefprozil [73] have been found to have short and long time alterations of the taxonomic, genomic, and functional capacity of gut microbiota. Reduction of bacterial diversity has been observed by using broad-spectrum antibiotics [74] which causes the expanding and collapsing of the membership of specific indigenous taxa [75]. Antibiotics are widely used during COVID-19 management to reduce bacterial co-infections [76] which disrupts the gut microbiota by eliminating both beneficial and harmful microbiota [77]. This phenomenon has the potential to induce dysbiosis, which may further aggravate the vulnerability to secondary infections.
Dietary Modifications and Nutritional Alterations:
Patients suffering from COVID-19 with severe symptoms experience altered dietary habits. These alterations, such as reduced intake of dietary fibers can impact the gut microbiome. Individuals consuming diets low in fiber tend to have reduced microbial diversity [78]. Several studies show dietary fiber replaced with animal protein and fat can alter microbial populations in the mortal gastrointestinal tract as dietary fiber is the main source of energy for the microbiome [79,80,81,82,83].
Hospitalization and stress:
COVID-19 patients undergo several stressful events due to the new unexperienced disease condition, Isolation as well as hospitalization. Several studies show stressful events induced depression, and anxiety, and disrupted the gut microbiome. This gut dysbiosis persisted for at least 6 months [84].
The Gut-Lung Axis:
A very interesting finding was observed in 1998, Lyte and colleagues observed Anxiety-like behavior in rats after subclinical dosages of a single, unique bacterium (Campylobacter jejuni) were administered to them orally [85]. Later studies supported this finding, showing that mice exposed to introducing C jejuni displayed anxiety-like behavior along with the activation of brain areas depending on signals ingested from the gut via the vagus nerve [86]. This is the first study to understand the gut-brain axis. However, a recent study discusses the gut lung axis, a bidirectional communication pathway between the gastrointestinal tract (the gut) and the lungs. Despite being technically separate, the gut-lung axis (GLA), along with possible anatomic interactions and intricate pathways involving their respective bacteria, has been proven to exist. Recent research has demonstrated the connection between dysbiosis and a number of lung-related conditions, including allergies, cystic fibrosis, asthma, and chronic obstructive pulmonary disease [87,88]. Due to the breakdown of the intestinal barrier brought on by dysbiotic circumstances, the inflammatory cascade in non-intestinal organs was mediated by the transfer of bacteria or microbial metabolites to the lungs [89,90]. In contrast to healthy people, the presence of the gut permeability marker fatty acid binding protein-2, as well as the gut microbial antigens peptidoglycan and lipopolysaccharides, was significantly higher in patients with COVID-19 [91].
Figure 2.
Schematic illustration of the involvement of the gut-lung axis in managing COVID-19 disease with dysbiosis of the gut microbiota. Because the gut-lung axis is bidirectional, lung inflammation affects the level of gut microbiota while compounds originating from gut bacteria have an impact on the lung through blood.
Figure 2.
Schematic illustration of the involvement of the gut-lung axis in managing COVID-19 disease with dysbiosis of the gut microbiota. Because the gut-lung axis is bidirectional, lung inflammation affects the level of gut microbiota while compounds originating from gut bacteria have an impact on the lung through blood.
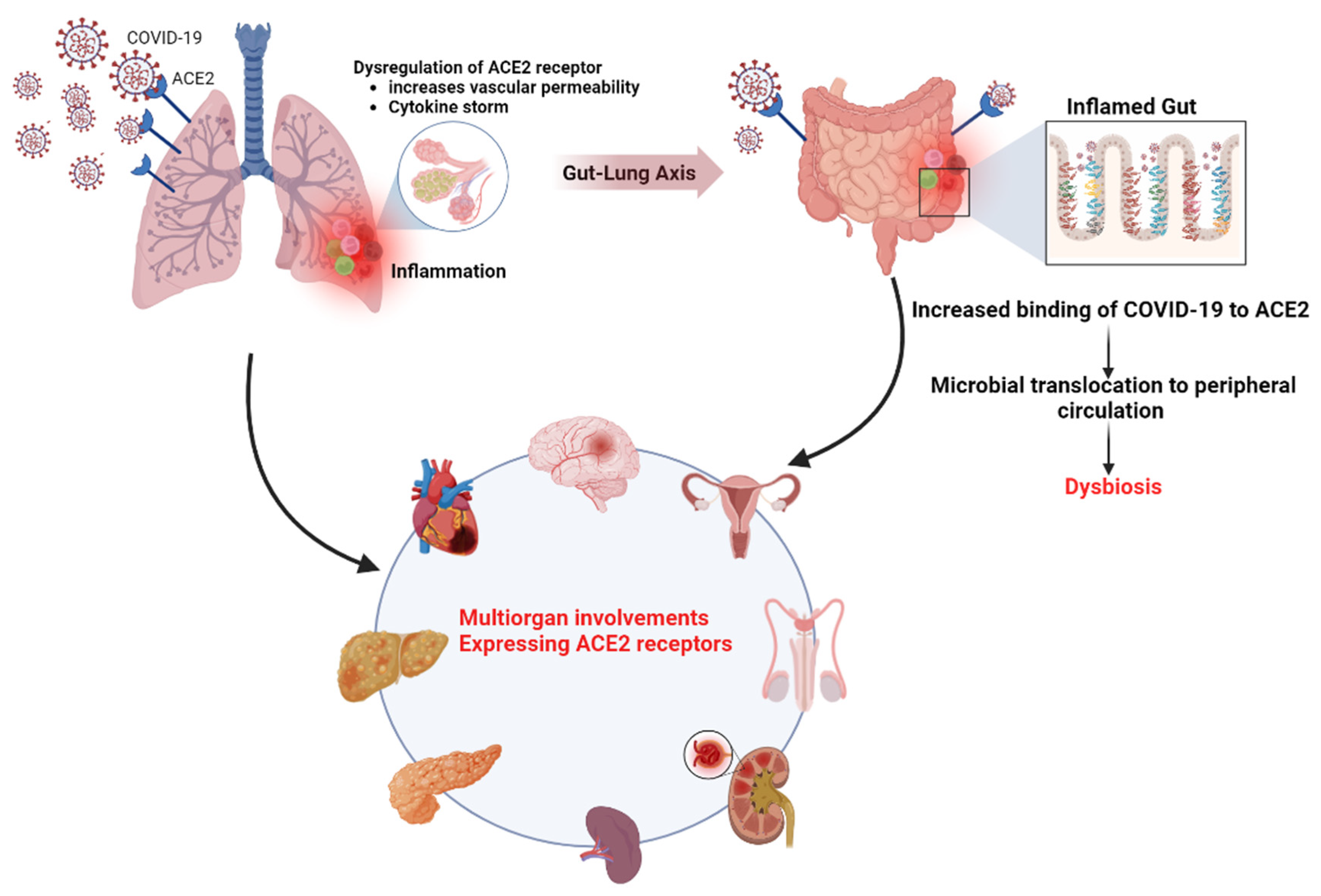
The role of the ACE2 receptor in SARS-CoV-2 infection and gut microbiota dysbiosis
A homolog of Angiotensin-Converting Enzyme (ACE) called ACE2, has been reported as a negative regulator of the Renin-Angiotensin System (RAS), reducing the harmful effects caused by Ang II signaling through Ang II receptor type 1 (AT1R) [92]. ACE2 receptor plays a vital role in the infection process of the SARS-CoV-2 virus which is responsible for COVID-19 [93]. ACE2 is present on the surface of numerous cells throughout the human body, including those in the digestive system, respiratory tract, lungs, heart, and kidneys [93].
SARS-CoV-2 enters host cells by interacting with ACE2 receptors on the cell surface. The virus's spike protein interacts with ACE2 to help the virus enter the cell. Once the virus has entered the host cell, it replicates and spreads, leading to COVID-19 symptoms. In the respiratory tract, the ACE2 receptor is highly expressed, which results from respiratory symptoms associated with COVID-19 [94].
ACE2 receptors are also highly expressed in gut, particularly in the epithelial cells of the small intestine. Yifei and his colleagues found the presence of SARS-CoV-2 RNA in the feces of COVID-19 patients. SARS CoV2 RNA was detected in stool samples from 28 out of 42 (66.67%) laboratory-confirmed COVID-19 patients, and this finding was unrelated to gastrointestinal symptoms or the severity of the illness [95]. Another study by Qun et al, observed SARS-CoV-2 had already replicated in the patient's rectum during the incubation period, with no obvious intestinal pathological damage. In this case, the patient developed a dry cough and fever in the early stage after the operation [96].
ACE2 plays a key role in controlling the effects of amino acid deficiency on microbial ecology and intestinal inflammation [97,98]. The gut microbiome of COVID-19 patients was significantly altered, with the opportunistic pathogen (such as Clostridium hathewayi and Clostridium ramosum) and an inverse correlation between probiotic bacteria (such as Lactobacillus and Bifidobacterium) and anti-inflammatory bacteria (such as Faecalibacterium prausnitzii) [54,99]. Furthermore, the immunological response elicited by the SARS-CoV-2 infection may contribute to intestinal dysbiosis [100].
SARS-CoV-2 infection-related dysbiosis may have systemic effects beyond the gut. Inflammatory bowel diseases (IBD) such as Crohn's disease (CD) and ulcerative colitis (UC) are the most common. Several evidence shows that intestinal microbial dysbiosis has a role in the pathogenesis of IBD [101]. Dysbiosis in systemic disease involves metabolic disorders metabolic diseases such as obesity or T2D [102], immune disorders [103], and mental health disorders [84].
Intestinal Inflammation and Gut Microbiota:
Several gastrointestinal symptoms have been observed in a significant number of COVID-19 patients. A study by Tian et al. from March 2020 found that anorexia was the most often reported gastrointestinal symptoms in adults, occurring in between 39.9% and 50% of confirmed cases. Diarrhea was the second most typical symptom, with 2% to 49.5% of patients reporting it. In adults who tested positive for COVID-19, the prevalence of nausea and vomiting varied between 1% and 29.4%. The prevalence of abdominal pain in individuals with confirmed COVID-19 ranges from 2.2% to 6% in the literature [104]. The prevalence of abdominal pain among patients with confirmed COVID-19 ranges from 2.2% to 6% less frequently described in the literature. In a study by Lei et al, Among the 190 patients in our sample, 138 (69%) had at least 1 gastrointestinal symptom at the time of diagnosis; if hypoxia/anorexia were excluded, 93 patients (48.9%) had at least 1 gastrointestinal symptom. Diarrhea was one gastrointestinal symptom that was linked to a reduced mortality rate. Diarrhea was verified as an independent predictor of decreased mortality after multivariate analysis [105].
George Cholankeril and his group from Stanford University School of Medicine analyzed data collected from 116 patients who tested positive for the coronavirus at Stanford Health Care from March 4-24, 2020. 31.9% of the patients complained of gastrointestinal problems. The majority of those polled described their symptoms as minor. According to the study, 22% had a loss of appetite, 22% had nausea and vomiting, and 12% had diarrhea [106]. A group of researchers from New York Presbyterian Columbia University Medical Centre conducted a study on 147 patients. The most prevalent GI symptoms for COVID-19 in 147 patients without pre-existing GI conditions had diarrhea (23%), nausea/vomiting (21%), and abdominal pain (6.1%) at the time of hospitalization. At a median follow-up time of 106 days, the most prevalent GI symptoms were abdominal pain (7.5%), constipation (6.8%), diarrhea (4.1%), and vomiting (4.1%), with 16% reporting at least one GI symptom (95% confidence interval from 11 to 23%) [107].
Consequences of intestinal inflammation on gut barrier function and bacterial translocation:
Consequences of intestinal inflammation in gut barrier function and bacterial translocation: The gut barrier, a selectively permeable structure, is widely recognized as an essential factor in the maintenance of intestinal homeostasis as it permits complex crosstalk between commensal intestinal microbes. Gut microbial dysbiosis due to both genetic and environmental factors can imbalance such equilibrium and may lead to intestinal inflammation which ultimately triggers pathogenic microbe invasion and different pathogenic conditions such as inflammatory bowel diseases (IBD), Crohn's disease, irritable bowel syndrome, colorectal cancer, obesity and type-1 diabetes [35]. Inflammation can be triggered by components of the invading bacterium that can lead to a series of inflammatory pathways involving interleukins and other cytokines. In the same way, by-products of metabolic processes in bacteria, including some short-chain fatty acids, may play a role in inhibiting inflammatory processes. Persistently high levels of inflammatory mediators, such as lipopolysaccharides & interleukins, can initiate pathological processes that can lead to multiple chronic disorders [108,109,110].
Understanding the interplay between the gut microbiota and the immune system:
There are two immune systems: the innate immune system and the adaptive immune system. The gut microbiota plays a crucial role in the development and maturation of the immune system, especially throughout childhood [111]. The immune system is trained to recognize and respond to pathogens while maintaining tolerance to harmless antigens. Through various mechanisms through various mechanisms [112]. Microbial molecules and metabolites interact directly with immune cells to activate, proliferate, and differentiate. These interactions play a role in the regulation of immune responses and homeostasis[113]. The gut microbiota helps to maintain the integrity of the intestinal barrier. Microbes help to improve the gut barrier by increasing mucus production and maintaining the structure of the intestinal epithelial cell layer. A good gut barrier stops harmful bacteria and toxins from entering your body, which can trigger your immune system [114]. Immune system dysfunction caused by COVID-19 may contribute to intestinal barrier dysfunction. Disruption of the intestinal barrier allows microbial components such as lipopolysaccharides (LPS) to escape from the gut into the bloodstream. This translocation induces an immune response and systemic inflammation, which can further affect the composition and function of the gut microbiota [108].
Impact on Short-Chain Fatty Acids (SCFAs):
Through the anaerobic fermentation of dietary fiber, the gut microbiota creates short-chain fatty acids (SCFAs). SCFAs, such as butyrate, propionate, and acetate, have important immunomodulatory effects and contribute to gut health [115]. SCFAs can affect the lung's immunological milieu and the severity of allergic inflammation [116]. The generation of SCFAs may be impacted by immunological dysregulation in COVID-19, altering immune responses and gut microbiota composition [117]. Fen Zhang and colleagues performed shotgun metagenomic sequencing on fecal samples from 66 antibiotics-naïve patients with COVID-19 and 70 non-COVID-19 controls. They observed Impaired SCFAs biosynthesis in the gut microbiome persisted beyond 30 days after recovery in patients with COVID-19 [118].
Long-Term Health Consequences of Gut Microbiota Alterations
Gut microbiota alterations, such as dysbiosis or imbalances in the composition and function of the gut microbial community, can have serious long-term health effects. Studies have revealed a connection between obesity and metabolic disorders like insulin resistance and type 2 diabetes, and changes in the composition of the gut microbiota, such as a decline in microbial diversity [119,120]. Imbalances in gut bacteria can affect energy extraction from the diet, influence fat storage, and impact metabolic processes [121]. Inflammatory bowel illnesses including Crohn's disease and ulcerative colitis have been linked to imbalances in the gut microbiota that contribute to their onset and progression [122]. The progression of these disorders can be aided by disruptions in the delicate balance of gut bacteria, which can result in persistent inflammation of the intestinal lining [82,123]. An association between changes in the gut microbiota and the emergence of allergies and autoimmune illnesses is being supported by more and more research [124,125]. These disorders may be triggered or made worse by dysbiosis, an imbalance of gut bacteria, which may affect the immune system's regulation [126,127]. Emerging research indicates a potential link between gut microbiota and mental health issues like anxiety, depression, and even neurodevelopmental abnormalities like autism spectrum disorders [128]. These relationships may be influenced by the gut-brain axis, a bidirectional communication link between the gut and the central neurological system [129]. Some studies suggest that imbalances in gut microbiota composition may influence cardiovascular health by affecting lipid metabolism, blood pressure regulation, and systemic inflammation [130]. It has been shown that the gut microbiota changes as people age, and that changes in the gut's bacterial composition may be a factor in the development of age-related disorders like frailty, cognitive decline, and chronic inflammation [131]. However, the causal relationship and underlying mechanisms require further investigation.
Therapeutic Strategies and Interventions:
Prebiotics and synbiotics on COVID-19-related gut dysbiosis is currently emerging. However, several therapies have been studied in the context of general gut health and immune support, which may have implications for COVID-19 and its impact on gut microbiota.
Probiotics have been explored for their immune-modulating properties and potential to support respiratory and gastrointestinal health. While there is limited direct data on their influence on COVID-19-related gut microbiota disease, probiotics could potentially help restore gut microbiota balance and improve gut health [132]. They play an important role to supporting immune response, reducing inflammation, and maintaining intestinal barrier integrity. However, further research is needed to establish their specific benefits in the context of COVID-19 [133].
Prebiotics, like the ones that have been mentioned above, give nourishment to good gut microbes and encourage their growth. Prebiotics maybe helpful by supporting the growth of beneficial bacteria and restoring gut microbiota balance, which is relevant to COVID-19 related gut dysbiosis. Prebiotics can contribute to a healthy gut barrier and immune function. Prebiotic-rich food such as fruits, vegetables, whole grains beneficial for overall gut health [134,135,136,137].
Mesenchymal stem cell therapy [138] and Fecal microbiota transplantation (FMT) is an approved therapy for recurrent clostridium difficile infection. The donor's stool shall be reconstituted from a range of solutions, including homogenization, filtering or strain and the following is administered after centrifugation either via Lower and upper GI tract or as gelatin capsules [139]. Bacteria (Escherichia coli, Bifidobacterium, Lactobacilli, and Faecalibacterium prausnitzii), viruses (Anelloviruses, Microviridae, and Siphoviridae), archaea and fungus (Candida albicans), human colonocytes, and metabolites are among the fecal components that can be transported by FMT [140]. In order to prevent or cure
Conclusion:
The clinical effects of COVID-19 are catastrophic, and the GI tract's contribution is greatly underappreciated. Observational studies have shed light on the function of dysbiosis in acute and post-acute COVID-19 situations as well as their connection to the severity of the illness. To uncover potential causal relationships between the human microbiome and COVID-19, a whole scenario investigation still not done. It is obvious that the microbiota has a significant role in how the host immune system reacts to different illnesses, including COVID-19. Given that the COVID-19 pandemic is still severe in some areas of the world, this study area should get top priority.
Funding
This research received no external funding.
Acknowledgments
We want to thanks Svaksha V Shukla, Arpita Barua, Mrs. Jyothi for their continuous support.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Frontiers | SARS-CoV-2: Structure, Biology, and Structure-Based Therapeutics Development. 2023. [CrossRef]
- Aubert O, Y.D. , Zielinski D, Cozzi E, et all. COVID-19 pandemic and worldwide organ transplantation: a population-based study. The Lancet. Public health 2021, 6. [Google Scholar] [CrossRef] [PubMed]
- @sprinklr. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.
- J, M.; T, M. Recent Developments on Therapeutic and Diagnostic Approaches for COVID-19. The AAPS journal 2021, 23. [Google Scholar] [CrossRef]
- Aslan, A.; Aslan, C.; Zolbanin, N.M.; Jafari, R. Acute respiratory distress syndrome in COVID-19: possible mechanisms and therapeutic management. Pneumonia 2021, 13, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Frontiers | Mechanism of Multi-Organ Injury in Experimental COVID-19 and Its Inhibition by a Small Molecule Peptide. 2023. [CrossRef]
- Davis, M.G.; Bobba, A.; Chourasia, P.; Gangu, K.; Shuja, H.; Dandachi, D.; Farooq, A.; Avula, S.R.; Shekhar, R.; Sheikh, A.B. COVID-19 Associated Myocarditis Clinical Outcomes among Hospitalized Patients in the United States: A Propensity Matched Analysis of National Inpatient Sample. Viruses 2022, 14, 2791. [Google Scholar] [CrossRef] [PubMed]
- Xu, S.-w.; Ilyas, I.; Weng, J.-p. Endothelial dysfunction in COVID-19: an overview of evidence, biomarkers, mechanisms and potential therapies. Acta Pharmacologica Sinica 2022, 44, 695–709. [Google Scholar] [CrossRef] [PubMed]
- Mohammad, M.; Emin, M.; Bhutta, A.; Gul, E.H.; Voorhees, E.; Afzal, M.R. Cardiac arrhythmias associated with COVID-19 infection: state of the art review. [CrossRef]
- Increased risk of acute myocardial infarction after COVID-19 recovery: A systematic review and meta-analysis - International Journal of Cardiology. 2023. [CrossRef]
- Javed, N.; Ijaz, Z.; Khair, A.H.; Dar, A.A.; Lopez, E.D.; Abbas, R.; Sheikh, A.B. COVID-19 loss of taste and smell: potential psychological repercussions. The Pan African Medical Journal 2022, 43. [Google Scholar] [CrossRef]
- Tana, C.; Bentivegna, E.; Cho, S.-J.; Harriott, A.M.; García-Azorín, D.; Labastida-Ramirez, A.; Ornello, R.; Raffaelli, B.; Beltrán, E.R.; Ruscheweyh, R.; et al. Long COVID headache. The Journal of Headache and Pain 2022, 23, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Korres, G.; Kitsos, D.K.; Kaski, D.; Tsogka, A.; Giannopoulos, S.; Giannopapas, V.; Sideris, G.; Tyrellis, G.; Voumvourakis, K. The Prevalence of Dizziness and Vertigo in COVID-19 Patients: A Systematic Review. Brain Sciences 2022, 12, 948. [Google Scholar] [CrossRef]
- How does the COVID-19 cause seizure and epilepsy in patients? The potential mechanisms - Multiple Sclerosis and Related Disorders. 2023. [CrossRef]
- Encephalitis as a neurological complication of COVID-19: A systematic review and meta-analysis of incidence, outcomes, and predictors. 2023. [CrossRef]
- COVID-19-associated Guillain-Barre syndrome: Postinfectious alone or neuroinvasive too? 2023. [CrossRef]
- Groff, A.; Kavanaugh, M.; Ramgobin, D.; McClafferty, B.; Aggarwal, C.S.; Golamari, R.; Jain, R. Gastrointestinal Manifestations of COVID-19: A Review of What We Know. 2021. [CrossRef]
- Faour, W.H.; Choaib, A.; Issa, E.; Choueiry, F.E.; Shbaklo, K.; Alhajj, M.; Sawaya, R.T.; Harhous, Z.; Alefishat, E.; Nader, M. Mechanisms of COVID-19-induced kidney injury and current pharmacotherapies. Inflammation Research 2021, 71, 39–56. [Google Scholar] [CrossRef] [PubMed]
- MB, A. Could the menagerie of the gut microbiome really cure cancer? Hope or hype. Journal for immunotherapy of cancer 2019, 7. [Google Scholar] [CrossRef]
- MS, M.; T, H.; R, I.; E, M.-Y.; Y, Y.; H, N.-S.; S, A.; M, K.; M, M.; M, K.; et al. Glucagon-Like Peptide-1 Receptor Agonist Protects Dorsal Root Ganglion Neurons against Oxidative Insult. Journal of diabetes research 2019, 2019. [Google Scholar] [CrossRef]
- Mohabbulla Mohib, M.; Fazla Rabby, S.M.; Paran, T.Z.; Mehedee Hasan, M.; Ahmed, I.; Hasan, N.; Abu Taher Sagor, M.; Mohiuddin, S. Protective role of green tea on diabetic nephropathy—A review. Cogent Biology 2016, 2, 1248166. [Google Scholar] [CrossRef]
- MS, M.; T, H.; Y, Y.; Y, M.; M, K.; S, T.; Y, K.; J, N.; H, K. Glucagon Prevents Cytotoxicity Induced by Methylglyoxal in a Rat Neuronal Cell Line Model. Biomolecules 2021, 11. [Google Scholar] [CrossRef]
- S, T.; FM, A.; Y, H.; R, Y.; I, A.; MS, M.; MM, K.; D, G.; MA, M. Antenatal depression among women with gestational diabetes mellitus: a pilot study. Reproductive health 2022, 19. [Google Scholar] [CrossRef]
- M, M.; T, H.; H, N.-S.; R, I.; N, O.; Y, H.; S, S.; MS, M.; E, A.-H.; M, K.; et al. Deficiency of glucagon gene-derived peptides induces peripheral polyneuropathy in mice. Biochemical and biophysical research communications 2020, 532. [Google Scholar] [CrossRef]
- M, C.; A, R.; A, K. Adiponectin/AdipoRs signaling as a key player in testicular aging and associated metabolic disorders. Vitamins and hormones 2021, 115. [Google Scholar] [CrossRef]
- W, D.; M, C.; S, P.; HA, S.; L, O. Adipocyte CAMK2 deficiency improves obesity-associated glucose intolerance. Molecular metabolism 2021, 53. [Google Scholar] [CrossRef]
- Barua, R.; Mizuno, K.; Tashima, Y.; Ogawa, M.; Takeuchi, H.; Taguchi, A.; Okajima, T. Bioinformatics and Functional Analyses Implicate Potential Roles for EOGT and L-fringe in Pancreatic Cancers. Molecules 2021, 26, 882. [Google Scholar] [CrossRef]
- Choubey, M. Growth Hormone and Insulin-like Growth Factor-I: Novel Insights into the Male Reproductive Health. Available online: https://scholar.google.com/citations?
- Ranjan, A.; Choubey, M.; Yada, T.; Krishna, A. Nesfatin-1 ameliorates type-2 diabetes-associated reproductive dysfunction in male mice. Journal of Endocrinological Investigation 2019, 43, 515–528. [Google Scholar] [CrossRef] [PubMed]
- M, C.; A, R.; PS, B.; A, K. Protective role of adiponectin against testicular impairment in high-fat diet/streptozotocin-induced type 2 diabetic mice. Biochimie 2020, 168. [Google Scholar] [CrossRef]
- Ranjan, A.; Choubey, M.; Yada, T.; Krishna, A. Immunohistochemical localization and possible functions of nesfatin-1 in the testis of mice during pubertal development and sexual maturation. Journal of Molecular Histology 2019, 50, 533–549. [Google Scholar] [CrossRef] [PubMed]
- M, C.; A, R.; PS, B.; F, B.; A, K. Direct actions of adiponectin on changes in reproductive, metabolic, and anti-oxidative enzymes status in the testis of adult mice. General and comparative endocrinology 2019, 279. [Google Scholar] [CrossRef]
- AT, D.; BJ, M. Microbes, metabolites, and the gut-lung axis. Mucosal immunology 2019, 12. [Google Scholar] [CrossRef]
- Structure, function and diversity of the healthy human microbiome. Nature 2012, 486, 207–214. [CrossRef] [PubMed]
- OC, T.-C.; J, M.; A, G. Colonization and impact of disease and other factors on intestinal microbiota. Digestive diseases and sciences 2007, 52. [Google Scholar] [CrossRef]
- C, L.; K, F.; J, R.; JJ, F.; DN, F.; J, Z.; JI, G.; R, K. Identifying genomic and metabolic features that can underlie early successional and opportunistic lifestyles of human gut symbionts. Genome research 2012, 22. [Google Scholar] [CrossRef]
- MJ, C.; Department of Microbiology, U.C.C. , Ireland.; IB, J.; S, C.; SE, P.; EM, O.C.; S, C.; HM, H.; M, C.; B, L.; et al. Gut microbiota composition correlates with diet and health in the elderly. Nature 2023, 488, 178–184. [Google Scholar] [CrossRef]
- Analyses of the Stability and Core Taxonomic Memberships of the Human Microbiome | PLOS ONE. 2023. [CrossRef]
- Ley, R.E.; Bäckhed, F.; Turnbaugh, P.; Lozupone, C.A.; Knight, R.D.; Gordon, J.I. Obesity alters gut microbial ecology. 2005. [CrossRef]
- Ley, R.E.; Turnbaugh, P.J.; Klein, S.; Gordon, J.I. Human gut microbes associated with obesity. Nature 2006, 444, 1022–1023. [Google Scholar] [CrossRef] [PubMed]
- Oliphant, K.; Allen-Vercoe, E. Macronutrient metabolism by the human gut microbiome: major fermentation by-products and their impact on host health. Microbiome 2019, 7, 1–15. [Google Scholar] [CrossRef]
- HV, L.; A, F.; EJ, K.; AR, N.; MM, L.; JR, K.; JA, H.; D, S.; X, Y.; G, F.; et al. Butyrate and propionate protect against diet-induced obesity and regulate gut hormones via free fatty acid receptor 3-independent mechanisms. PloS one 2012, 7. [Google Scholar] [CrossRef]
- Microbiota-Generated Metabolites Promote Metabolic Benefits via Gut-Brain Neural Circuits: Cell. 2023. [CrossRef]
- Frost, G.; Sleeth, M.L.; Sahuri-Arisoylu, M.; Lizarbe, B.; Cerdan, S.; Brody, L.; Anastasovska, J.; Ghourab, S.; Hankir, M.; Zhang, S.; et al. The short-chain fatty acid acetate reduces appetite via a central homeostatic mechanism. Nature Communications 2014, 5, 1–11. [Google Scholar] [CrossRef]
- SL, L.; CGM, G.; SA, J. Interactions between gut bacteria and bile in health and disease. Molecular aspects of medicine 2017, 56. [Google Scholar] [CrossRef]
- D, R.; O, W.; E, B.; A, K.; T, K.; D, Z.; PI, C.; A, G.; IN, K.; N, B.; et al. Environment dominates over host genetics in shaping human gut microbiota. Nature 2018, 555. [Google Scholar] [CrossRef]
- Gacesa, R.; Kurilshikov, A.; Vich Vila, A.; Sinha, T.; Klaassen, M.A.Y.; Bolte, L.A.; Andreu-Sánchez, S.; Chen, L.; Collij, V.; Hu, S.; et al. Environmental factors shaping the gut microbiome in a Dutch population. Nature 2022, 604, 732–739. [Google Scholar] [CrossRef] [PubMed]
- Frontiers | Is It Time to Begin a Public Campaign Concerning Frailty and Pre-frailty? A Review Article. 2023. [CrossRef]
- B, C.; O, K.; JK, G.; AC, P.; S, S.; RE, L.; AT, G. Dietary emulsifiers impact the mouse gut microbiota promoting colitis and metabolic syndrome. Nature 2015, 519. [Google Scholar] [CrossRef]
- Wu, G.D.; Compher, C.; Chen, E.Z.; Smith, S.A.; Shah, R.D.; Bittinger, K.; Chehoud, C.; Albenberg, L.G.; Nessel, L.; Gilroy, E.; et al. Comparative metabolomics in vegans and omnivores reveal constraints on diet-dependent gut microbiota metabolite production. 2016. [CrossRef]
- Jackson, M.A.; Goodrich, J.K.; Maxan, M.-E.; Freedberg, D.E.; Abrams, J.A.; Poole, A.C.; Sutter, J.L.; Welter, D.; Ley, R.E.; Bell, J.T.; et al. Proton pump inhibitors alter the composition of the gut microbiota. 2016. [CrossRef]
- MJ, B. Antibiotic use and its consequences for the normal microbiome. Science (New York, N.Y.) 2016, 352. [Google Scholar] [CrossRef]
- T, Z.; F, Z.; GCY, L.; YK, Y.; AYL, L.; H, Z.; Y, W.; ACK, C.; CP, C.; N, C.; et al. Alterations in Gut Microbiota of Patients With COVID-19 During Time of Hospitalization. Gastroenterology 2020, 159. [Google Scholar] [CrossRef]
- T, Z.; Q, L.; F, Z.; GC, L.; EY, T.; YK, Y.; Z, C.; SS, B.; FK, C.; PK, C.; et al. Depicting SARS-CoV-2 faecal viral activity in association with gut microbiota composition in patients with COVID-19. Gut 2021, 70. [Google Scholar] [CrossRef]
- Yeoh, Y.K.; Zuo, T.; Lui, G.C.-Y.; Zhang, F.; Liu, Q.; Li, A.Y.; Chung, A.C.; Cheung, C.P.; Tso, E.Y.; Fung, K.S.; et al. Gut microbiota composition reflects disease severity and dysfunctional immune responses in patients with COVID-19. 2021. [CrossRef]
- S, G.; Y, C.; Z, W.; Y, C.; H, G.; L, L.; F, G.; X, Z.; R, L.; C, H.; et al. Alterations of the Gut Microbiota in Patients With Coronavirus Disease 2019 or H1N1 Influenza. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America 2020, 71. [Google Scholar] [CrossRef]
- D, D.; A, M. Gut microbiota and Covid-19- possible link and implications. Virus research 2020, 285. [Google Scholar] [CrossRef]
- Liu, Q.; Su, Q.; Zhang, F.; Tun, H.M.; Mak, J.W.Y.; Lui, G.C.-Y.; Ng, S.S.S.; Ching, J.Y.L.; Li, A.; Lu, W.; et al. Multi-kingdom gut microbiota analyses define COVID-19 severity and post-acute COVID-19 syndrome. Nature Communications 2022, 13, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Bernard-Raichon, L.; Venzon, M.; Klein, J.; Axelrad, J.E.; Zhang, C.; Sullivan, A.P.; Hussey, G.A.; Casanovas-Massana, A.; Noval, M.G.; Valero-Jimenez, A.M.; et al. Gut microbiome dysbiosis in antibiotic-treated COVID-19 patients is associated with microbial translocation and bacteremia. Nature Communications 2022, 13, 1–13. [Google Scholar] [CrossRef]
- Tsounis, E.P.; Triantos, C.; Konstantakis, C.; Marangos, M.; Assimakopoulos, S.F. Intestinal barrier dysfunction as a key driver of severe COVID-19. http://www.wjgnet.com/. [CrossRef]
- Sun, Z.; Song, Z.-G.; Liu, C.; Tan, S.; Lin, S.; Zhu, J.; Dai, F.-H.; Gao, J.; She, J.-L.; Mei, Z.; et al. Gut microbiome alterations and gut barrier dysfunction are associated with host immune homeostasis in COVID-19 patients. BMC Medicine 2022, 20, 1–13. [Google Scholar] [CrossRef]
- Z, S.; ZG, S.; C, L.; S, T.; S, L.; J, Z.; FH, D.; J, G.; JL, S.; Z, M.; et al. Gut microbiome alterations and gut barrier dysfunction are associated with host immune homeostasis in COVID-19 patients. BMC medicine 2022, 20. [Google Scholar] [CrossRef]
- Frontiers | The COVID-19 Cytokine Storm; What We Know So Far. 2023. [CrossRef]
- Gonçalves, P.; Innate Immunity Unit, I.P. , Paris, France; Institut National de la Santé et de la Recherche Médicale (INSERM) U1223, P., France; Araújo, J.R.; Molecular Microbial Pathogenesis Unit, I.P., Paris, France; Institut National de la Santé et de la Recherche Médicale (INSERM) U1202, P., France; Di Santo, J.P.; Institut National de la Santé et de la Recherche Médicale (INSERM) U1223, P., France. A Cross-Talk Between Microbiota-Derived Short-Chain Fatty Acids and the Host Mucosal Immune System Regulates Intestinal Homeostasis and Inflammatory Bowel Disease. Inflammatory Bowel Diseases 2023, 24, 558–572. [Google Scholar] [CrossRef]
- J, T.; C, M.; M, P.; AN, T.; CR, M.; L, M. The role of short-chain fatty acids in health and disease. Advances in immunology 2014, 121. [Google Scholar] [CrossRef]
- EE, H.; MR, M.; KJ, L. HDAC Inhibitors as Epigenetic Regulators of the Immune System: Impacts on Cancer Therapy and Inflammatory Diseases. BioMed research international 2016, 2016. [Google Scholar] [CrossRef]
- AS, H.; M, T.; O, R.; SA, H.; TW, S. GPCR-Mediated Signaling of Metabolites. Cell metabolism 2017, 25. [Google Scholar] [CrossRef]
- M, L.; BCAM, v.E.; GTM, W.; J, G.; G, F.; PAJ, H. Pro- and anti-inflammatory effects of short chain fatty acids on immune and endothelial cells. European journal of pharmacology 2018, 831. [Google Scholar] [CrossRef]
- Y, L.; Z, Z.; Y, L.; W, H.; M, Z.; X, Z.; W, J. Angiotensin-converting enzyme inhibition attenuates lipopolysaccharide-induced lung injury by regulating the balance between angiotensin-converting enzyme and angiotensin-converting enzyme 2 and inhibiting mitogen-activated protein kinase activation. Shock (Augusta, Ga.) 2015, 43. [Google Scholar] [CrossRef]
- Pro-Inflammatory Activated Kupffer Cells by Lipids Induce Hepatic NKT Cells Deficiency through Activation-Induced Cell Death | PLOS ONE. 2023. [CrossRef]
- MF, D.L.C.; T, D.; P, L.; A, B.; JP, G.; J, D. Resilience of the dominant human fecal microbiota upon short-course antibiotic challenge. Journal of clinical microbiology 2005, 43. [Google Scholar] [CrossRef]
- L, D.; S, H.; ML, S.; DA, R. The pervasive effects of an antibiotic on the human gut microbiota, as revealed by deep 16S rRNA sequencing. PLoS biology 2008, 6. [Google Scholar] [CrossRef]
- F, R.; AA, O.; M, D.; N, I.; H, G.; B, D.; P, L.; PL, P.; R, G.; È, B.; et al. The initial state of the human gut microbiome determines its reshaping by antibiotics. The ISME journal 2016, 10. [Google Scholar] [CrossRef]
- G, D.; JC, L.; C, R.; F, A.; P, H.; S, M.; N, D.; NP, D.; A, P.; J, A.; et al. Culturomics and pyrosequencing evidence of the reduction in gut microbiota diversity in patients with broad-spectrum antibiotics. International journal of antimicrobial agents 2014, 44. [Google Scholar] [CrossRef]
- Modi, S.R.; Collins, J.J.; Relman, D.A. Antibiotics and the gut microbiota. 2014. [CrossRef]
- Global antibiotic use during the COVID-19 pandemic: analysis of pharmaceutical sales data from 71 countries, 2020–2022 - eClinicalMedicine. 2023. [CrossRef]
- de Nies, L.; Galata, V.; Martin-Gallausiaux, C.; Despotovic, M.; Busi, S.B.; Snoeck, C.J.; Delacour, L.; Budagavi, D.P.; Laczny, C.C.; Habier, J.; et al. Altered infective competence of the human gut microbiome in COVID-19. Microbiome 2023, 11, 1–16. [Google Scholar] [CrossRef]
- J, W. Murine gut microbiota-diet trumps genes. Cell host & microbe 2015, 17. [Google Scholar] [CrossRef]
- C, D.F.; D, C.; M, D.P.; M, R.; JB, P.; S, M.; S, C.; G, P.; P, L. Impact of diet in shaping gut microbiota revealed by a comparative study in children from Europe and rural Africa. Proceedings of the National Academy of Sciences of the United States of America 2010, 107. [Google Scholar] [CrossRef]
- T, Y.; FE, R.; MJ, M.; I, T.; MG, D.-B.; M, C.; M, M.; G, H.; RN, B.; AP, A.; et al. Human gut microbiome viewed across age and geography. Nature 2012, 486. [Google Scholar] [CrossRef]
- J, O.; F, C.; EG, Z.; JP, D.; M, W.; K, N.; HR, G.; SJ, O.K. Diet, microbiota, and microbial metabolites in colon cancer risk in rural Africans and African Americans. The American journal of clinical nutrition 2013, 98. [Google Scholar] [CrossRef]
- LA, D.; CF, M.; RN, C.; DB, G.; JE, B.; BE, W.; AV, L.; AS, D.; Y, V.; MA, F.; et al. Diet rapidly and reproducibly alters the human gut microbiome. Nature 2014, 505. [Google Scholar] [CrossRef]
- ED, S.; JL, S. Starving our microbial self: the deleterious consequences of a diet deficient in microbiota-accessible carbohydrates. Cell metabolism 2014, 20. [Google Scholar] [CrossRef]
- Dhar, D. Frontiers | Impending Mental Health Issues During Coronavirus Disease 2019 – Time for Personalized Nutrition Based on the Gut Microbiota to Tide Over the Crisis? 2023. [CrossRef]
- M, L.; JJ, V.; MT, B. Anxiogenic effect of subclinical bacterial infection in mice in the absence of overt immune activation. Physiology & behavior 1998, 65. [Google Scholar] [CrossRef]
- LE, G.; RP, G.; N, O.; R, R.; N, B.; M, L. Activation in vagal afferents and central autonomic pathways: early responses to intestinal infection with Campylobacter jejuni. Brain, behavior, and immunity 2005, 19. [Google Scholar] [CrossRef]
- EPA, R.; K, L.; WA, B.; EFM, W. Disturbed intestinal integrity in patients with COPD: effects of activities of daily living. Chest 2014, 145. [Google Scholar] [CrossRef]
- Frontiers | Diet, Microbiota and Gut-Lung Connection. 2023. [CrossRef]
- CY, S.; CH, Y.; WY, Y.; HZ, Y. Gut-Lung Microbiota in Chronic Pulmonary Diseases: Evolution, Pathogenesis, and Therapeutics. The Canadian journal of infectious diseases & medical microbiology = Journal canadien des maladies infectieuses et de la microbiologie medicale 2021, 2021. [CrossRef]
- Schuijt, T.J.; Lankelma, J.M.; Scicluna, B.P.; Melo, F.d.S.e.; Roelofs, J.J.T.H.; Boer, J.D.d.; Hoogendijk, A.J.; Beer, R.d.; Vos, A.d.; Belzer, C.; et al. The gut microbiota plays a protective role in the host defence against pneumococcal pneumonia. 2016. [CrossRef]
- R, P.; MJ, P.; JL, F.; CP, V.; S, F.; M, D.; A, H.; CS, J.; J, W.; R, L.; et al. Plasma microbiome in COVID-19 subjects: an indicator of gut barrier defects and dysbiosis. bioRxiv : the preprint server for biology. [CrossRef]
- K, K.; Y, I.; JM, P. Multiple functions of angiotensin-converting enzyme 2 and its relevance in cardiovascular diseases. Circulation journal : official journal of the Japanese Circulation Society 2013, 77. [Google Scholar] [CrossRef]
- Frontiers | Body Localization of ACE-2: On the Trail of the Keyhole of SARS-CoV-2. 2023. [CrossRef]
- Jackson, C.B.; Farzan, M.; Chen, B.; Choe, H. Mechanisms of SARS-CoV-2 entry into cells. Nature Reviews Molecular Cell Biology 2021, 23, 3–20. [Google Scholar] [CrossRef]
- The presence of SARS-CoV-2 RNA in the feces of COVID-19 patients - Chen - 2020 - Journal of Medical Virology - Wiley Online Library. 2023. [CrossRef]
- Qian, Q.; Department of Colorectal and Anal Surgery, Z.H.o.W.U. , Wuhan, China; Clinical Center of Intestinal and Colorectal Diseases of Hubei Province, W., China; Hubei Key Laboratory of Intestinal and Colorectal Diseases (Zhongnan Hospital of Wuhan University), W., China; Colorectal and Anal Disease Research Center of Medical School (Zhongnan Hospital of Wuhan University), W., China; Quality Control Center of Colorectal and Anal Surgery of Health Commission of Hubei Province, W., China; Fan, L.; Department of Pathology, H.C.H., Wuhan, China; Liu, W.; Department of Colorectal and Anal Surgery, Z.H.o.W.U., Wuhan, China; et al. Direct Evidence of Active SARS-CoV-2 Replication in the Intestine. Clinical Infectious Diseases 2023, 73, 361–366. [Google Scholar] [CrossRef]
- T, H.; T, P.; A, R.; J, T.; H, I.; M, P.; V, S.; T, H.; R, H.; S, L.; et al. ACE2 links amino acid malnutrition to microbial ecology and intestinal inflammation. Nature 2012, 487. [Google Scholar] [CrossRef]
- Wang, J.; Zhao, S.; Liu, M.; Zhao, Z.; Xu, Y.; Wang, P.; Lin, M.; Xu, Y.; Huang, B.; Zuo, X.; et al. ACE2 expression by colonic epithelial cells is associated with viral infection, immunity and energy metabolism. 2020. [CrossRef]
- Alterations in Gut Microbiota of Patients With COVID-19 During Time of Hospitalization - Gastroenterology. 2023. [CrossRef]
- Ferreira, C.; Viana, S.D.; Reis, F. Gut Microbiota Dysbiosis–Immune Hyperresponse–Inflammation Triad in Coronavirus Disease 2019 (COVID-19): Impact of Pharmacological and Nutraceutical Approaches. Microorganisms 2020, 8, 1514. [Google Scholar] [CrossRef]
- DC, B.; SR, C. Inflammatory bowel disease: cause and immunobiology. Lancet (London, England) 2007, 369. [Google Scholar] [CrossRef]
- Zhang, H.; DiBaise, J.K.; Zuccolo, A.; Kudrna, D.; Braidotti, M.; Yu, Y.; Parameswaran, P.; Crowell, M.D.; Wing, R.; Rittmann, B.E.; et al. Human gut microbiota in obesity and after gastric bypass. 2009. [CrossRef]
- Kim, Y.; Division of Gastroenterology and Hepatology, D.o.I.M., University of Michigan; Kamada, N.; Division of Gastroenterology and Hepatology, D.o.I.M., University of Michigan; Laboratory of Microbiology and Immunology, W.I.F.R.C. , Osaka University, Suita, Osaka 565-0871, Japan. The role of the microbiota in myelopoiesis during homeostasis and inflammation. International Immunology 2023, 35, 267–274. [Google Scholar] [CrossRef] [PubMed]
- Y, T.; L, R.; W, N.; Y, H. Review article: gastrointestinal features in COVID-19 and the possibility of faecal transmission. Alimentary pharmacology & therapeutics 2020, 51. [Google Scholar] [CrossRef]
- Pan, L.M., PhD1; Mu, M.M., 4; Yang, P.M.; Sun, Y.M.; Wang, R.M.; Yan, J.M.; Li, P.M.; Hu, B.M., PhD10; Wang, J.M.; Hu, C.M.; et al. Clinical Characteristics of COVID-19 Patients With Digestive... : Official journal of the American College of Gastroenterology | ACG. 2023. [CrossRef]
- G, C.; A, P.; VI, A.; B, T.; EA, P.; SP, S.; D, K.; A, H.; A, A. High Prevalence of Concurrent Gastrointestinal Manifestations in Patients With Severe Acute Respiratory Syndrome Coronavirus 2: Early Experience From California. Gastroenterology 2020, 159. [Google Scholar] [CrossRef]
- JW, B.; J, L.; D, J.; DE, F. Prevalence and risk factors for gastrointestinal symptoms after recovery from COVID-19. Neurogastroenterology and motility : the official journal of the European Gastrointestinal Motility Society 2022, 34. [Google Scholar] [CrossRef]
- Ghosh, S.S.; Department of Internal Medicine, V.M.C., Richmond; Wang, J.; Department of Internal Medicine, V.M.C., Richmond; Yannie, P.J.; Hunter Homes McGuire VA Medical Center, R., Virginia; Ghosh, S.; Department of Internal Medicine, V.M.C., Richmond; Hunter Homes McGuire VA Medical Center, R. , Virginia. Intestinal Barrier Dysfunction, LPS Translocation, and Disease Development. Journal of the Endocrine Society 2023, 4. [Google Scholar] [CrossRef]
- Gionchetti, P.; Lammers, K.M.; Rizzello, F.; Campieri, M. Probiotics and barrier function in colitis. 2005. [CrossRef]
- Bander, Z.A.; Nitert, M.D.; Mousa, A.; Naderpoor, N. The Gut Microbiota and Inflammation: An Overview. International Journal of Environmental Research and Public Health 2020, 17, 7618. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.-J.; Wu, E. The role of gut microbiota in immune homeostasis and autoimmunity. https://doi.org/10.4161/gmic.19320. [CrossRef]
- Zheng, D.; Liwinski, T.; Elinav, E. Interaction between microbiota and immunity in health and disease. Cell Research 2020, 30, 492–506. [Google Scholar] [CrossRef]
- Lu, Y.; Yuan, X.; Wang, M.; He, Z.; Li, H.; Wang, J.; Li, Q. Gut microbiota influence immunotherapy responses: mechanisms and therapeutic strategies. Journal of Hematology & Oncology 2022, 15, 1–20. [Google Scholar] [CrossRef]
- Takiishi, T.; Fenero, C.I.M.; Câmara, N.O.S. Intestinal barrier and gut microbiota: Shaping our immune responses throughout life. https://doi.org/10.1080/21688370.2017.1373208. [CrossRef]
- YP, S.; A, B.; RL, F. The Role of Short-Chain Fatty Acids From Gut Microbiota in Gut-Brain Communication. Frontiers in endocrinology 2020, 11. [Google Scholar] [CrossRef]
- Trompette, A.; Gollwitzer, E.S.; Yadava, K.; Sichelstiel, A.K.; Sprenger, N.; Ngom-Bru, C.; Blanchard, C.; Junt, T.; Nicod, L.P.; Harris, N.L.; et al. Gut microbiota metabolism of dietary fiber influences allergic airway disease and hematopoiesis. Nature Medicine 2014, 20, 159–166. [Google Scholar] [CrossRef]
- Chakraborty, C.; Sharma, A.R.; Bhattacharya, M.; Dhama, K.; Lee, S.-S. Altered gut microbiota patterns in COVID-19: Markers for inflammation and disease severity. http://www.wjgnet.com/. [CrossRef]
- F, Z.; Y, W.; T, Z.; YK, Y.; Q, L.; L, Z.; H, Z.; W, L.; W, X.; GCY, L.; et al. Prolonged Impairment of Short-Chain Fatty Acid and L-Isoleucine Biosynthesis in Gut Microbiome in Patients With COVID-19. Gastroenterology 2022, 162. [Google Scholar] [CrossRef]
- Iatcu, C.O.; Steen, A.; Covasa, M. Gut Microbiota and Complications of Type-2 Diabetes. Nutrients 2021, 14, 166. [Google Scholar] [CrossRef] [PubMed]
- Boulangé, C.L.; Neves, A.L.; Chilloux, J.; Nicholson, J.K.; Dumas, M.-E. Impact of the gut microbiota on inflammation, obesity, and metabolic disease. Genome Medicine 2016, 8, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Richard, W. Stephens, L.A., Mihai Covasa. Gut Microbiota: From Microorganisms to Metabolic Organ Influencing Obesity - Stephens - 2018 - Obesity - Wiley Online Library. 2023. [CrossRef]
- Khan, I.; Ullah, N.; Zha, L.; Bai, Y.; Khan, A.; Zhao, T.; Che, T.; Zhang, C. Alteration of Gut Microbiota in Inflammatory Bowel Disease (IBD): Cause or Consequence? IBD Treatment Targeting the Gut Microbiome. Pathogens 2019, 8, 126. [Google Scholar] [CrossRef]
- Haneishi, Y.; Furuya, Y.; Hasegawa, M.; Picarelli, A.; Rossi, M.; Miyamoto, J. Inflammatory Bowel Diseases and Gut Microbiota. International Journal of Molecular Sciences 2023, 24, 3817. [Google Scholar] [CrossRef] [PubMed]
- Colucci, R.; Moretti, S. Implication of Human Bacterial Gut Microbiota on Immune-Mediated and Autoimmune Dermatological Diseases and Their Comorbidities: A Narrative Review. Dermatology and Therapy 2021, 11, 363–384. [Google Scholar] [CrossRef] [PubMed]
- Vijay, A.; Valdes, A.M. Role of the gut microbiome in chronic diseases: a narrative review. European Journal of Clinical Nutrition 2021, 76, 489–501. [Google Scholar] [CrossRef]
- Lee, K.H.; Song, Y.; Wu, W.; Yu, K.; Zhang, G. The gut microbiota, environmental factors, and links to the development of food allergy. Clinical and Molecular Allergy 2020, 18, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Plunkett, C.H.; Department of Pathology, T.U.o.C. , Chicago, IL 60637; and; Nagler, C.R.; Department of Pathology, T.U.o.C., Chicago, IL 60637; and; Committee on Immunology, T.U.o.C., Chicago, IL 60637. The Influence of the Microbiome on Allergic Sensitization to Food. The Journal of Immunology 2023, 198, 581–589. [Google Scholar] [CrossRef]
- Mangiola, F.; Ianiro, G.; Franceschi, F.; Fagiuoli, S.; Gasbarrini, G.; Gasbarrini, A. Gut microbiota in autism and mood disorders. http://www.wjgnet.com/. [CrossRef]
- Ma, Q.; Xing, C.; Long, W.; Wang, H.Y.; Liu, Q.; Wang, R.-F. Impact of microbiota on central nervous system and neurological diseases: the gut-brain axis. Journal of Neuroinflammation 2019, 16, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Almeida, C.P. , ∗; Barata, P.P., MD,; Fernandes, R.P. The influence of gut microbiota in cardiovascular diseases—a... : Porto Biomedical Journal. 2023. [CrossRef]
- Buford, T.W. (Dis)Trust your gut: the gut microbiome in age-related inflammation, health, and disease. Microbiome 2017, 5, 1–11. [Google Scholar] [CrossRef]
- McFarland, L.V. Use of probiotics to correct dysbiosis of normal microbiota following disease or disruptive events: a systematic review. 2014. [CrossRef]
- AC, C.; TJ, F.; HH, H.; JF, C.; YW, K.; YY, H.; SY, T.; SF, W.; HC, L.; YT, Y. A multi-strain probiotic blend reshaped obesity-related gut dysbiosis and improved lipid metabolism in obese children. Frontiers in nutrition 2022, 9. [Google Scholar] [CrossRef]
- Tsai, Y.-L.; Lin, T.-L.; Chang, C.-J.; Wu, T.-R.; Lai, W.-F.; Lu, C.-C.; Lai, H.-C. Probiotics, prebiotics and amelioration of diseases. Journal of Biomedical Science 2019, 26, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Md. Ehsan Uddin Talukder, F.M. Md. Ehsan Uddin Talukder, F.M., Rashu Barua, Samsad Sultana, Farhana Yesmin, Mohammad Sayedul Islam, Robiul Hasan Bhuiyan. In vitro Assessment of Cytotoxic Activity of Hybrid Variety of Momordica charantia (Bitter Gourd). 2023. [CrossRef]
- Barua, R.; Department of Biochemistry and Molecular Biology, U.o.C. , Chittagong-4331, Bangladesh.; Sultana, S.; Department of Biochemistry and Molecular Biology, U.o.C., Chittagong-4331, Bangladesh.; Talukder, M.E.U.; Department of Biochemistry and Molecular Biology, U.o.C., Chittagong-4331, Bangladesh.; Chakma, K.; Department of Biochemistry and Molecular Biology, U.o.C., Chittagong-4331, Bangladesh abd Tohoku University Graduate School of Medicine, Sendai 980-8575, Japan; Hasan, C.M.M.; Department of Biochemistry and Molecular Biology, U.o.C., Chittagong-4331, Bangladesh.; et al. Antioxidant and Cytotoxic Activity of Crude Flavonoid Fraction from the Fruits of Hybrid Variety of Momordica charantia (Bitter Gourd). Journal of Pharmaceutical Research International. [CrossRef]
- Rashu Barua, M.E.U.T. , Mohammad Sayedul Islam, Farhana Yesmin, Kanchan Chakma, Md Golam Kabir, Robiul Hasan Bhuiyan. Nutritional Analysis and Phytochemical Evaluation of Bitter Gourd (Momordica Charantia) from Bangladesh. 2020. [CrossRef]
- Akter, S.; Choubey, M.; Mohib, M.M.; Arbee, S.; Sagor, M.A.T.; Mohiuddin, M.S. Stem Cell Therapy in Diabetic Polyneuropathy: Recent Advancements and Future Directions. Brain Sciences 2023, 13, 255. [Google Scholar] [CrossRef]
- CR, K.; S, K.; P, K.; L, L.; D, R.; A, A.; T, M.; G, W. Update on Fecal Microbiota Transplantation 2015: Indications, Methodologies, Mechanisms, and Outlook. Gastroenterology 2015, 149. [Google Scholar] [CrossRef]
- Diana, P. Bojanova, S.R.B. Fecal Transplants: What Is Being Transferred? 2023. [CrossRef]
Figure 1.
Possible mechanism of cytokine storm and subsequent pathogen infections resulting from lung microbiota dysbiosis in COVID-19 patients.
Figure 1.
Possible mechanism of cytokine storm and subsequent pathogen infections resulting from lung microbiota dysbiosis in COVID-19 patients.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



