
Submitted:
15 July 2023
Posted:
18 July 2023
You are already at the latest version
Abstract
Abstract: Objective: This study aimed to estimate adherence to methotrexate in patients with rheumatoid arthritis and identify specific nonadherence risk factors. Methods: A cross-sectional study included 111 patients (age mean 56.2±10.6 years, 78.4% female, and disease duration mean 6 (3-13) years). Three adherence self-assessment questionnaires were used: the Compli-ance-Questionnaire-Rheumatology (CQR19), the Medication Adherence Reports Scale (MARS-5), and the Visual Analogue Scale (VAS). We also collected demographic data, disease and treatment characteristics, and anxiety/depression estimation results (Hospital Anxiety and Depression Scale- HADS). Results: Adherence was identified in 48.6% of patients (COR19), 70.3% (MARS-5), and 82.9% of patients in the VAS questionnaire. All three questionnaires displayed a significant positive mutual correlation: CQR19 with MARS-5 and VAS (r =0.364, r=0.329 respectively, p<0.001 for both), between VAS and MARS-5 score (r=0.496, p<0.001). A significant positive prediction was shown for urban residence (0.347 (0.134-0.901), p=0.030), using the MARS-5 scale, female sex (0.264 (0.095-0.730), p=0.010) according to CQR19 and for a dose of methotrexate (0.881 (0.783-0.992), p=0.036) in VAS scale, while negative prediction were shown for comorbidity number (3.062 (1.057-8.874), p=0.039), and depression (1.142 (1.010-1.293), p=0.035) using MARS-5 scale and for older age (1.041 (1.003-1.081), p=0.034) according to CQR19. The use of steroids was a significant positive predictor in all three questionnaires and remained an independent predictor for metho-trexate adherence in multivariant logistic regression. Conclusion: We showed nonadherence to methotrexate in a significant number of patients using all three questionnaires. Concomitant steroid therapy emerged as an independent positive predictor for adherence.
Keywords:
prediction
; adherence
; methotrexate
; self-report questionnaires
; rheumatoid arthritis
1. Introduction
Rheumatoid arthritis (RA) is a chronic inflammatory autoimmune disease characterized by symmetric peripheral polyarthritis and progressive joint damage. Disease-modifying antirheumatic drugs (DMARD) reduce disease activity and radiologic progression, ameliorating long-term functional status in RA patients [1]. To achieve this aim, patients need to take medication regularly.
Methotrexate (MTX) is a synthetic DMARD recommended as the first-line treatment in the patient with RA [2,3], due to its safety and efficacy, different ways of application (parenteral and oral), and drug dose titration possibility [4,5]. It can be used as a monotherapy or combined with other synthetic or biological DMARD [6]. Nevertheless, not all patients display a good response to MTX, which can be partially attributed to therapy noncompliance [7,8]. Optimal utilization of MTX requires starting therapy immediately, and adherence to a prescribed dose and regimen until a satisfactory response is obtained, followed by complying with a maintenance dose.
Nonadherence is defined as the avoidance of therapy onset, intentional or unintentional disregard for the physician’s recommendations, or non-persistence with treatment [9]. Several studies have been conducted concerning adherence to MTX in RA patients. The results were inconstant due to different criteria for establishing adherence, vast heterogeneity of participants’ samples, employment of different types of measurements, and follow-up length. Literature analysis revealed a large variation in adherence, with its’ rate range spanning from 59% to 107%, where MTX excessive use was also considered an adherence problem [10,11]. In previous studies, the association of certain demographic and disease characteristics, socio-economic status, mental health, and patient’s beliefs regarding medication with adherence to MTX was found [12,13]. Hope et al. concluded that the mild course of the disease, depression absence, patients’ confidence in the efficacy and necessity of the therapy, as well as MTX monotherapy are potential predictors of adherence to MTX [10]. According to the literature, more than 200 variables have an influence on adherence, but none of them showed correlative consistency in different studies [14], indicating that no uniform nonadherence profile could be made [15].
In order to enhance adherence, the priority is to identify individuals displaying nonadherent behavior [16]. Along with the substantial subjective and objective measurement approaches, no strategy is rated as optimal. A multi-method that combines self-assessment and reasonable objective measurements is currently the most adequate procedure to estimate adherent behavior. Still, the most feasible manner of detecting nonadherent patients in clinical practice is a self-reporting method.
Besides the need for better education of patients, there are still numerous issues in adherence improvement [17,18]. Considering the existence of a still significant number of nonadherent patients, innovative interventions to optimize the use of MTX are needed to improve the disease’s final outcome [19]. Therefore, this research aimed to estimate adherence to MTX and identify specific socio-demographic, clinical, and psychological risk factors for nonadherence.
2. Materials and Methods
Study Patients
This cross-sectional study included patients treated in the Rheumatology Clinic of the Military Medical Academy in Belgrade, during 2016 and 2017, who met the following requirements: RA diagnosis was based on the classification criteria ACR/EULAR2010 [20], age ≥18 years, prescribed MTX with minimum two months’ continuance. Exclusion criteria were: the presence of another connective tissue systemic disease, psychiatric disorders, and antidepressant therapy within the last month, as well as recent infections and surgical procedures.
This is a single-center study approved by the institutional ethics committee and conformed to the Declaration of Helsinki. All participants have signed informed consent.
Literature-based questionnaires were used to collect data about patients and disease characteristics. One part of the questionnaire was related to sociodemographic characteristics (sex, age, place of residence, education, employment, and smoking status), and the other to clinical aspects of the disease (disease duration, current MTX dose, maximal MTX dose, therapy side effects, concomitant use of steroids, other DMARD or biologics, comorbidity presence, frequency of blood laboratory analysis and the annual number of physician visits).
The following inflammatory markers were analyzed: erythrocyte sedimentation rate according to Westergreenum (mm/h), C reactive protein (CRP) using nephelometry (range 0-5mg/l) and IL-6 serum level engaging Enzyme-linked immunosorbent assay (ELISA, Bionova) according to the manufacturer instructions (range 0-5.9 pg/ml).
RA activity was assessed by Disease Activity Score 28-joint count (DAS28-SE) [21], and Clinical Disease Activity Index (CDAI) [22,23,24]. Disease activity was defined as remission (DAS28 < 2.6, CDAI ≤ 2.8), low disease activity (DAS28 2.6-3.2, CDAI 2.8-10), moderate disease activity (DAS28 3.2-5.1, CDAI 10-22), and high disease activity for DAS28 over 5.1 and CDAI over 22. The functional ability was estimated using a questionnaire for assessing patients’ health status Health Assessment Questionnaire (HAQ), more accurately disability index HAQ-DI [25]. The HAQ score from 0-1 represents mild to moderate difficulties, 1-2 moderate to heavy disabilities, and 2-3 severely heavy disabilities.
Adherence Assessment
Adherence to MTX therapy was conveyed employing three literature-based questionnaires: the Compliance Questionnaire for Rheumatology (CQR19), the Medication adherence rating scale (MARS-5), and freely estimated adherence on Visual Analogue Scale (VAS) ranging from 0 to 10 cm.
The CQR19 questionnaire [28,29] is composed of 19 statement questions regarding specific barriers in taking prescribed medication, and patient grades the level of agreement according to a Likert scale from 1 to 4 (1 point=strongly disagree, 2 points= disagree, 3 points=agree and 4 points=strongly agree). Six of the 19 questions were formulated in negation (numbered questions 4, 8, 9, 11, 12, and 19), and therefore reverse scoring had to be applied. The overall score is obtained by adding up all points and subtracting value 19 from the total sum. The new calculated value is divided by 0.57. This ensures that the complete CQR19 result can vary from 0 (no adherence) to 100 (perfect adherence) [26,27,28]. In agreement with published data, a less than 80% score represents low adherence.
MARS-5 is an adherence questionnaire developed for patients with different chronic diseases [29]. The questionnaire is composed of 5 questions regarding certain aspects of nonadherent behavior. Each question has multiple-choice answers: 1= always, 2= often, 3= sometimes, 4= rarely, and 5= never. The total MARS-5 score can take values from 5 to 25, with a higher rating indicating elevated adherence levels. Different studies suggest that in the majority of measuring scales, a score above 80% is considered satisfactory. Therefore, in this study, patients with MARS-5 scores above 23 were qualified as adherents [30].
Visual analog scale (VAS) ranged from 0% to 100%. On a scale span from 0 cm to 10 cm, a patient solely determines the level of adherence by marking a number or position that most adequately suits his subjective estimation of compliance to therapy. Values beyond 80% were considered a high level of therapy adherence.
Mental health Assessment
Mental health assessment was conveyed by The Hospital Anxiety and Depression Scale (HADS) questionnaire, recommended by The National Institute for Health and Care Excellence (NICE) in order to diagnose depression and anxiety [31]. The questionnaire was comprised of 14 questions, with half of them (7) related to anxiety and the other half (7 related) to depression. Each question is answered according to a Likert scale with 4 possible answers (0-3). The overall score for each scale was ranging from 0 to 21 and was categorized as: 0-7 = normal finding, 8-10 = borderline anxiety/depression, and 11-21 = abnormal, presence of anxiety/depression [32,33]. The specificity of these scores is 0.78 and 0.79 for anxiety and depression, respectively, while score sensitivity corresponding orderly to anxiety and depression is 0.9 and 0.83 [34].
Statistical Data Analysis
Statistical analysis was performed using IBM SPSS version 26.0. Descriptive values were presented as average values with standard deviation or as median with an interquartile range (25-75th percentile). Distribution was verified by the Kolmogorov-Smirnov test. Attribute variables were presented in the form of frequencies of individual categories. Statistical significance was estimated by the Chi-square test or Fisher’s exact test for attributive variables. Continuous variables were tested using a Student’s t-test for (in) dependent samples or nonparametric alternative Mann-Whitney test and Wilcoxon test. The correlation was estimated by Pearson correlation. Predictive value exploration for the chosen variables in the assessment of adherence to MTX in the group of patients with RA was conveyed by univariant and multivariant logistic regression analysis. A p-value less than 0.05 was considered statistically significant.
3. Results
Our study included 111 RA patients with an age average of 56.2±10.6 years. Females made up the majority of the survey sample (78.4%), almost half of the patients (48.6%) were non-smokers, and 35.1% were employed. The majority of respondents lived in the city (79.3%) and the largest number had a high school education (68.5%) (Table 1).
Comorbidities were marked in 74 (66.7%) patients, and 23 (20.7%) of them had three or more conditions. The median disease duration in our sample population from the establishment of diagnosis was 6 years (IQR: 3-13.5). The number of annual visits to a rheumatologist in our patients was 4 (IQR: 3-6), while the average underwent laboratory analysis was 4 times a year.
In combined therapy adjacent to MTX, 96 patients (86.5%) were taking steroids, the median dose was 6 mg. Antimalarials were used by 33 (29.7%) patients, and 34 study participants (30.6%) were on biological therapy. The third of the subjects has some side effects: gastrointestinal tract discomforts (13.5%), leukopenia, and elevated liver enzymes (10.8%).
According to the CDAI index low disease activity was detected in 29.7% of patients, moderate was observed in 32.4%, and high in 33.3%. Similar results were obtained by DAS28 scoring: 36.9% of study participants had high, and 34.2% moderate disease activity. The average HAQ scale score was 0.89 ± 0.48.
Mental health analysis revealed that 18% of patients had elevated scores on the HADS scale for depression, while 10.8% of study participants had increased scores on the HADS scale for anxiety. About a quarter of patients accomplished borderline score HADS for depression and anxiety.
Adherence to MTX measured by three scales (CQR19, MARS-5, and VAS) was represented as a dichotomous variable. (Table 2) The average score for adherence to MTX on the CQR19 scale was 76.9 ± 13.5, while a non-adherence level to MTX was detected in 56 (50.5%) patients. According to the MARS-5 scale criteria, a non-adherence level was found in 32 study partakers (28.8%) (average score 22.63 ± 2.58). On a VAS scale ranging from 0 to 100 mm, patients graded self-reported adherence to MTX with 87.44 ± 16.49. Non-adherence to MTX (<80%) according to the VAS scale was detected in 19 of the study participants (17.1%) (Table 2).
Analysis of all three scores used to measure adherence showed a statistically significant positive correlation of CQR19 score with MARS-5 score (r=0.364, p<0.001) and VAS score (r=0.329, p<0.001). An even stronger positive correlation was observed between VAS and MARS-5 score (r=0.496, p<0.001). (Figure 1).
An analysis of adherence indicators CQR19, MARS-5, and VAS score identified a significant difference in adherence to MTX regarding sex, age, and urban residence. Also, prominent dissimilarity was observed with respect to the number of present chronic diseases, number of annual physician visits, MTX dose, and comedication with steroids. Patients on corticosteroid therapy had markedly enhanced adherence expressed with VAS (p=0.049) and CQR19 score (p=0.022) (Table 1).
In univariate logistic regression, statistical significance for non-adherence measured by the VAS scale was obtained for MTX dose (0.881 (0.783-0.992), p=0,036) and concomitant steroid use (0.273 (0.078-0.956), p=0.042). Patients who used a lower dose of MTX and those without concomitant steroid therapy had a higher degree of non-adherence (Table 3).
Using the MARS 5 scale, statistical significance for nonadherence was obtained for the place of residence (0.347 (0.134-0.901), p=0.030), where a higher degree of nonadherence was obtained for those living in rural areas.
Statistical significance was also obtained for the number of comorbidities (3.062 (1.057-8.874), p=0.039), where patients with a higher number of comorbidities are more non-adherent. Additionally, the presence of depression (1.142 (1.010-1.293), p=0.035) leads to a higher degree of non-adherence. As observed in the previous questionnaire, a statistically significant parameter for non-adherence was the concomitant use of steroids (0.306 (0.094-0.998). p=0.050). It follows that patients who were without steroids had a higher degree of non-adherence. (Table 3)
In multivariate logistic regression, it was found that a statistically significant independent predictor for non-adherence was the concomitant use of steroids. (Table 4) Concomitant use of corticosteroids reduces the chance of poor nonadherence by 4.4 times.
For non-adherence measured by the CQR scale by univariate regression, statistical significance was obtained for sex (0.264 (0.095-0.730), p=0.010), where males have a higher degree of non-adherence. Statistical significance was both detected for age (1.041 (1.003-1.081), p=0.034), meaning older patients were more non-adherent, as well as for the concomitant use of steroids (0.157 (0.033-0.746), p=0.020.
Multivariate logistic regression identified gender and concomitant use of steroids as statistically significant independent predictors of non-adherence (Table 5). Concomitant use of corticosteroids diminishes the odds of non-adherence by 5.1 times, while the female gender reduces this chance by approximately 3.9.
4. Discussion
In this study, the employment of three self-assessment questionnaires showed that 48.6% (CQR19), 70.3% (MARS-5), and 82.9% (VAS) patients were adherent. Logistic regression showed that concomitant use of corticosteroids is an independent predictor of adherence to MTX in all three questionnaires. Current studies exhibit significant variation in the degree of adherence using different measuring instruments. The latest research on adherence assessment by CQR questionnaire found that 78% and 85.7% of patients were adherent [13,35]. De Cuyper et al. demonstrated that only 24.2% of patients were adherent when the MARS-5 questionnaire estimation tool was used, while the VAS score delivered more promising results showing adherent behavior in 94% of the subjects. This observation can be explained by the absence of an existing standard for adherence measuring and the probability of overestimation in the self-reporting approach. The CQR questionnaire was chosen as the only validated questionnaire in the rheumatology field. For the MARS-5 questionnaire, the latest studies did not use the same cut-off point for the dichotomisation of the MARS-5 scale, limiting the possibility of data comparison.
The statistical difference was detected between adherent and nonadherent patients in terms of gender, age, place of residence, number of annual visits to a physician, MTX dose, and steroid co-medication. In our cohort, younger patients had a higher degree of adherence, which is consistent with the data from van den Bemt et al. [15].
This could be clarified by the association of older age with comorbidities, and therefore polypharmacy, increasing the probability of side effect incidence. However, other research groups report opposing results that show adherence in the elderly patient population [36,37,38] succeeding to the conclusion that age can affect adherence differentially. Female gender impact on better adherence was previously observed [39,40,41], still, other authors report inconsistency [16,35].
The positive influence of comorbidities on non-adherence is in accordance with published research [35,40], where two or more comorbidities represent a predictor of non-adherence. When multiple comorbidities are present, complexity and the extent of therapy carry a risk of forgetfulness and unintentional nonadherence [42]. In our study, patients who had a higher number of annual visits to a physician were more adherent. This is understandable since doctor-patient relations have a big effect on the efficacy of therapeutic regimens. Occasionally, nonadherence can occur due to a lack of consciousness in patients, regarding medication necessity [43]. Educating patients about their condition and therapy, as well as a doctor-patient confidence level, can diversly affect adherence [44].
In univariate logistic regression following the VAS scale, the current MTX dose was a significant predictor of non-adherence, while the MARS-5 questionnaire showed a marked prediction of adherence for depression and comorbidities, and for gender and age in the CQR-19 questionnaire.
The concomitant use of steroids was a statistically significant predictor of non-adherence, according to the results of all three questionnaires. The majority of the studies didn’t find an association between the dose of MTX and adherence, only one study highlighted a connection between the higher dose of MTX with improved adherence [45], but the supportive validation from other research groups is missing [35,46].
The negative association between worse mental health with adequate adherence has also been shown in studies by other authors [13,47], which is consistent with our research. Patients suffering from depression have a 2-3 times higher rate of nonadherence, compared to ones without this disorder [44].
In our study, the multivariant analysis revealed that concomitant use of steroids is an independent positive predictor of adherence, measured by MARS-5 and CQR19 questionnaires. According to our knowledge, the influence of concomitant use of steroids on MTX adherence was analyzed in only a few studies and the results are inconsistent [48,49,50]. For example, H. Bliddal et al. did not find any influence of prednisolone therapy on MTX adherence [49], while the negative impact of concomitant steroid use was shown by Alrubaye et al. [50]. On the other hand, Hoekstra M et al. showed that concomitant use of prednisolone remained significantly related to MTX therapy in multivariate analysis which is consistent with our results [48].
This result may be a consequence of the fact that our patients had more frequent relapses of the disease, which required the use of steroids and thus affects the patient’s belief in the necessity of MTX therapy. Perhaps, the large number of patients who received steroids in comparison with other studies where this number was significantly smaller, influenced this result.
Several research showed that the lack of comprehension related to MTX’s slow-acting effects can impact adherence [50]. Presumably, steroid administration with rapid and efficient action could have altered adherence. Treharna et al., have found that adherence is better in the group of patients with steroids because the absence of therapy can lead to a significant worsening of symptoms in the active form of the disease [51]. These results could also be an explanation for the better adherence to MTX in our group of patients on steroids, where steroids enhance the importance of MTX itself in the treatment of RA. On the other hand, the side effects of steroids cause concern in patients and could be diminished with MTX as a steroid-sparing drug.
The main limitations of this study are cross-sectional design and monocentric character. Cross-sectional design enables adherence-related variable identification but with inconclusive results. An additional problem is a bias selection since all included subjects were recruited from the same institution and had an opportunity for more frequent controls, which could have diminished the inclusion of nonadherent patients. Also, a small patient sample size does not have enough statistical power to determine the influence of examined variables on adherence. The utilization of the MARS-5 questionnaire without a clearly defined cut-off point for the separation of adherent and nonadherent study participants may result differentially. Commonly, the use of scale dichotomization and cutoff points can lead to the loss of important information due to the simplification of examined characteristics. Also, employing self-assessment scales can yield an overestimation of adherence due to social desirability and giving adjusted answers. The research did not convey a follow-up over time, and it is known that adherence is a dynamic process it can be influenced by several factors, and the patient’s behavior can change over time.
This study’s strength is using three measuring scales that exhibited significant mutual correlation, especially the one observed between the VAS and MARS-5 scales. To our knowledge, DeCuyper et al. were the only authors until now that use three self-reported questionnaires assessing adherence to MTX and show similar results. In accordance with the research of these authors, this would indicate the importance of VAS application in everyday use for rapid assessment of adherence to MTX in patients with RA [13].
5. Conclusions
Our study showed that a significant percentage of patients with RA are non-adherent and also an extensive variation in the level of adherence can be observed depending on the measuring tool. A curious fact is that concomitant use of steroids was singled out as an independent predictor of non-adherence. Since adherence to MTX in patients with RA is still suboptimal, and measurements are not standardized, they are nevertheless necessary for daily clinical practice. Given the above facts, further research is needed to discover non-adherent patients and the reasons for non-adherence as well as to develop adapted and possibly highly personalized interventions to improve adherence. Authors should discuss the results and how they can be interpreted from the perspective of previous studies and of the working hypotheses. The findings and their implications should be discussed in the broadest context possible. Future research directions may also be highlighted.
Author Contributions
Conceptualization, J.C., D.K.T. and G.R.; methodology, J.C. and G.R.; software, M.C., N.R. and M.M.; validation, J.C.; formal analysis, M.C., M.M. and N.R.; investigation, M.P., J.C., M.C. and J.C.; resources, J.C.; data curation, J.C.; writing—original draft preparation, all authors; writing—review and editing, G.R. and N.R.; visualization, J.C.; supervision, G.R. and D.K.T.; project administration, J.C.; funding acquisition, J.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of the University of Belgrade, Serbia (protocol code 29/III-16, Date: March 13, 2017) for studies involving humans.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patient(s) to publish this paper.
Data Availability Statement
The data sets used and/or analyzed in the present study are available from the corresponding author on reasonable request.
Acknowledgments
NA.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Jones, G.; Halbert, J.; Crotty, M.; Shanahan, E.M.; Batterham, M.; Ahern, M. The effect of treatment on radiological progression in rheumatoid arthritis: a systematic review of randomized placebo-controlled trials. Rheumatology. 2003, 42, 6–13. [Google Scholar] [CrossRef]
- Combe, B.; Landewe, R.; Daien, C.I.; Hua, C.; Aletaha, D.; Álvaro-Gracia, J.M.; et al. 2016 update of the EULAR recommendations for the management of early arthritis. Ann Rheum Dis. 2017, 76, 948–959. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Care Excellence. The management of rheumatoid arthritis in adults. Nice: National Institute for Health and Care Excellence 2018.
- Taylor, P.C.; Balsa Criado, A.; Mongey, A.B.; Avouac, J.; Marotte, H.; Mueller, R.B. How to get the most from methotrexate (MTX) treatment for your rheumatoid arthritis patient? -MTX in the treat-to-target strategy. J Clin Med. 2019, 8, 515. [Google Scholar] [PubMed]
- Krüger, K.; Wollenhaupt, J.; Albrecht, K.; Alten, R.; Backhaus, M.; Baerwald, C.; et al. European League of Associations for Rheumatology (EULAR). S1-Leitlinie der DGRh zur sequenziellen medikamentösen Therapie der rheumatoiden Arthritis 2012. Adaptierte EULAR-Empfehlungen und aktualisierter Therapiealgorithmus [German 2012 guidelines for the sequential medical treatment of rheumatoid arthritis. Adapted EULAR recommendations and updated treatment algorithm]. Z Rheumatol. 2012, 71, 592–603. [Google Scholar]
- O’Dell, J.R.; Curtis, J.R.; Mikuls, T.R.; Cofield, S.S.; Bridges, S.L. Jr; Ranganath, V.K.; et al. ; TEAR Trial Investigators. Validation of the methotrexate-first strategy in patients with early, poor-prognosis rheumatoid arthritis: results from a two-year randomized, double-blind trial. Arthritis Rheum. 2013, 65, 1985–1994. [Google Scholar] [PubMed]
- Choy, E.H.; Smith, C.M.; Farewell, V.; Walker, D.; Hassell, A.; Chau, L.; et al. CARDERA (Combination Anti-Rheumatic Drugs in Early Rheumatoid Arthritis) Trial Group. Factorial randomised controlled trial of glucocorticoids and combination disease modifying drugs in early rheumatoid arthritis. Ann Rheum Dis. 2008, 67, 656–663. [Google Scholar] [PubMed]
- Hider, S.L.; Silman, A.; Bunn, D.; Manning, S.; Symmons, D.; Lunt, M. Comparing the long-term clinical outcome of treatment with methotrexate or sulfasalazine prescribed as the first disease-modifying antirheumatic drug in patients with inflammatory polyarthritis. Ann Rheum Dis. 2006, 65, 1449–1455. [Google Scholar] [CrossRef]
- Brodtkorb, E.; Samsonsen, C.; Sund, J.K.; Bråthen, G.; Helde, G.; Reimers, A. Treatment non-adherence in pseudo-refractory epilepsy. Epilepsy Res. 2016, 122, 1–6. [Google Scholar] [CrossRef]
- Hope, H.F. ; Bluett, J; Barton, A. ; Hyrich, K.L.; Cordingley, L.; Verstappen, S.M. Psychological factors predict adherence to methotrexate in rheumatoid arthritis; findings from a systematic review of rates, predictors and associations with patient-reported and clinical outcomes. RMD Open. 2016, 2, e000171. [Google Scholar]
- Curtis, J.R.; Bykerk, V.P.; Aassi, M.; Schiff, M. Adherence and Persistence with Methotrexate in Rheumatoid Arthritis: A Systematic Review. J Rheumatol. 2016, 43, 1997–2009. [Google Scholar] [CrossRef]
- Cannon, G.W.; Mikuls, T.R.; Hayden, C.L.; Ying, J.; Curtis, J.R.; Reimold, A.M.; Caplan, L.; Kerr, G.S.; Richards, J.S.; Johnson, D.S.; Sauer, B.C. Merging Veterans Affairs rheumatoid arthritis registry and pharmacy data to assess methotrexate adherence and disease activity in clinical practice. Arthritis Care Res (Hoboken). 2011, 63, 1680–1690. [Google Scholar] [CrossRef] [PubMed]
- De Cuyper, E.; De Gucht, V.; Maes, S.; Van Camp, Y.; De Clerck, L.S. Determinants of methotrexate adherence in rheumatoid arthritis patients. Clin Rheumatol. 2016, 35, 1335–1339. [Google Scholar] [CrossRef] [PubMed]
- de Klerk, E; van der Heijde; D. ; Landewé, R.; van der Tempel, H.; Urquhart, J.; van der Linden, S. Patient compliance in rheumatoid arthritis, polymyalgia rheumatica, and gout. J Rheumatol 2003, 30, 44–54.
- van den Bemt, B.J.; Zwikker, H.E.; van den Ende, C.H. Medication adherence in patients with rheumatoid arthritis: a critical appraisal of the existing literature. Expert Rev Clin Immunol. 2012, 8, 337–351. [Google Scholar] [CrossRef] [PubMed]
- Horne, R.; Weinman, J. Patients’ beliefs about prescribed medicines and their role in adherence to treatment in chronic physical illness. J Psychosom Res. 1999, 47, 555–567. [Google Scholar] [CrossRef]
- Zangi, H.A.; Ndosi, M.; Adams, J.; Andersen, L.; Bode, C.; Boström, C.; et al. European League Against Rheumatism (EULAR). EULAR recommendations for patient education for people with inflammatory arthritis. Ann Rheum Dis. 2015, 74, 954–962. [Google Scholar]
- Sowden, E.; Hassan, W.; Gooden, A.; Jepson, B.; Kausor, T.; Shafait, I.; et al. Limited end-user knowledge of methotrexate despite patient education: an assessment of rheumatologic preventive practice and effectiveness. J Clin Rheumatol. 2012, 18, 130–133. [Google Scholar] [CrossRef]
- Horne, R. Compliance, adherence, and concordance. In: Taylor K, Harding G, eds. Pharmacy practice. London: Taylor & Francis, 2001, 148–167.
- Aletaha, D.; Neogi, T.; Silman, A.J.; Funovits, J.; Felson, D.T.; Bingham, C.O. 3rd; et al. 2010 Rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum. 2010, 62, 2569–2581. [Google Scholar]
- Prevoo, M.L.; van ‘t Hof, M.A.; Kuper, H.H.; van Leeuwen, M.A.; van de Putte, L.B.; van Riel, P.L. Modified disease activity scores that include twenty-eight joint counts. Development and validation in a prospective longitudinal study of patients with rheumatoid arthritis. Arthritis Rheum. 1995, 38, 44–48. [Google Scholar]
- Smolen, J.S.; Aletaha, D. Scores for all seasons: SDAI and CDAI. Clin Exp Rheumatol. 2014, 32(5 Suppl 85), S-75–S-79. [Google Scholar]
- Aletaha, D.; Smolen, J. The Simplified Disease Activity Index (SDAI) and the Clinical Disease Activity Index (CDAI): a review of their usefulness and validity in rheumatoid arthritis. Clin Exp Rheumatol. 2005, 23(5 Suppl 39), S100–108. [Google Scholar]
- Smolen, J.S.; Breedveld, F.C.; Schiff, M.H.; Kalden, J.R.; Emery, P.; Eberl, G.; van Riel, P.L.; Tugwell, P. A simplified disease activity index for rheumatoid arthritis for use in clinical practice. Rheumatology (Oxford). 2003, 42, 244–257. [Google Scholar] [CrossRef] [PubMed]
- Bruce, B.; Fries, J.F. The Stanford Health Assessment Questionnaire: dimensions and practical applications. Health Qual Life Outcomes. 2003, 1, 20. [Google Scholar] [CrossRef]
- de Klerk, E.; van der Heijde, D.; van der Tempel, H.; van der Linden, S. Development of a questionnaire to investigate patient compliance with antirheumatic drug therapy. J Rheumatol. 1999, 26, 2635–2641. [Google Scholar]
- de Klerk, E.; van der Heijde, D.; Landewé, R.; van der Tempel, H.; van der Linden, S. The compliance-questionnaire-rheumatology compared with electronic medication event monitoring: a validation study. J Rheumatol. 2003, 30, 2469–2475. [Google Scholar] [PubMed]
- Cinar, F.I.; Cinar, M.; Yilmaz, S.; Acikel, C.; Erdem, H. ; Pay, S; et al. Cross-Cultural Adaptation, Reliability, and Validity of the Turkish Version of the Compliance Questionnaire on Rheumatology in Patients With Behçet’s Disease. J Transcult Nurs. 2016, 27, 480–486. [Google Scholar]
- Salt, E.; Hall, L.; Peden, A.R.; Home, R. Psychometric properties of three medication adherence scales in patients with rheumatoid arthritis. J Nurs Meas. 2012, 20, 59–72. [Google Scholar] [CrossRef]
- Garfield, S.; Clifford, S.; Eliasson, L.; Barber, N.; Willson, A. Suitability of measures of self-reported medication adherence for routine clinical use: a systematic review. BMC Med Res Methodol. 2011, 11, 149. [Google Scholar] [CrossRef] [PubMed]
- National Collaborating Centre for Mental Health. Common Mental Health Disorders: The NICE Guideline on Identification and Pathways to Care. National Clinical Guideline Number 123. http://www.nice.org.uk/nicemedia/live/13476/54604/54604.pdf.
- Katchamart, W.; Narongroeknawin, P.; Chanapai, W.; Thaweeratthakul, P.; Srisomnuek, A. Prevalence of and factors associated with depression and anxiety in patients with rheumatoid arthritis: A multicenter prospective cross-sectional study. Int J Rheum Dis. 2020, 23, 302–308. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef]
- Bjelland. , I; Dahl, A.A.; Haug, T.T.; Neckelmann, D. The validity of the Hospital Anxiety and Depression Scale. An updated literature review. J Psychosom Res. 2002, 52, 69–77.
- de Thurah, A.; Nørgaard, M.; Johansen, M.B.; Stengaard-Pedersen, K. Methotrexate compliance among patients with rheumatoid arthritis: the influence of disease activity, disease duration, and co-morbidity in a 10-year longitudinal study. Scand J Rheumatol. 2010, 39, 197–205. [Google Scholar] [CrossRef] [PubMed]
- Viller, F.; Guillemin, F.; Briançon, S.; Moum, T.; Suurmeijer, T.; van den Heuvel, W. Compliance to drug treatment of patients with rheumatoid arthritis: a 3 year longitudinal study. J Rheumatol. 1999, 26, 2114–2122. [Google Scholar] [PubMed]
- Park, D.C.; Hertzog, C.; Leventhal, H.; Morrell, R.W.; Leventhal, E.; Birchmore, D.; Martin, M.; Bennett, J. Medication adherence in rheumatoid arthritis patients: older is wiser. J Am Geriatr Soc. 1999, 47, 172–183. [Google Scholar] [CrossRef] [PubMed]
- Yajima, N.; Kawaguchi, T.; Takahashi, R.; Nishiwaki, H.; Toyoshima, Y.; Oh, K.; et al. Adherence to methotrexate and associated factors considering social desirability in patients with rheumatoid arthritis: a multicenter cross-sectional study. BMC Rheumatol. 2022, 6, 75. [Google Scholar] [CrossRef] [PubMed]
- Hurkmans, E.J.; Maes, S.; de Gucht, V.; Knittle, K.; Peeters, A.J.; Ronday, H.K.; Vlieland, T.P. Motivation as a determinant of physical activity in patients with rheumatoid arthritis. Arthritis Care Res (Hoboken). 2010, 62, 371–377. [Google Scholar] [CrossRef] [PubMed]
- Borah, B.J.; Huang, X.; Zarotsky, V.; Globe, D. Trends in RA patients’ adherence to subcutaneous anti-TNF therapies and costs. Curr Med Res Opin. 2009, 25, 1365–1377. [Google Scholar] [CrossRef]
- Berner, C.; Erlacher, L.; Fenzl, K.H.; Dorner, T.E. Medication Adherence and Coping Strategies in Patients with Rheumatoid Arthritis: A Cross-Sectional Study. Int J Rheumatol. 2019, 2019, 4709645. [Google Scholar] [CrossRef]
- Choudhry, N.K.; Fischer, M.A.; Avorn, J.; Liberman, J.N.; Schneeweiss, S.; Pakes, J.; Brennan, T.A.; Shrank, W.H. The implications of therapeutic complexity on adherence to cardiovascular medications. Arch Intern Med. 2011, 171, 814–822. [Google Scholar] [CrossRef]
- Katchamart, W.; Narongroeknawin, P.; Sukprasert, N.; Chanapai, W.; Srisomnuek, A. Rate and causes of noncompliance with disease-modifying antirheumatic drug regimens in patients with rheumatoid arthritis. Clin Rheumatol. 2021, 40, 1291–1298. [Google Scholar] [CrossRef]
- Goh, H.; Kwan, Y.H.; Seah, Y.; Low, L.L.; Fong, W.; Thumboo, J. A systematic review of the barriers affecting medication adherence in patients with rheumatic diseases. Rheumatol Int. 2017, 37, 1619–1628. [Google Scholar] [CrossRef]
- Aletaha, D.; Smolen, J.S. Effectiveness profiles and dose dependent retention of traditional disease modifying antirheumatic drugs for rheumatoid arthritis. An observational study. J Rheumatol. 2002, 29, 1631–1638. [Google Scholar] [PubMed]
- Ideguchi, H.; Ohno, S.; Ishigatsubo, Y. Risk factors associated with the cumulative survival of low-dose methotrexate in 273 Japanese patients with rheumatoid arthritis. J Clin Rheumatol. 2007, 13, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Cabrera-Marroquín, R.; Contreras-Yáñez, I.; Alcocer-Castillejos, N.; Pascual-Ramos, V. Major depressive episodes are associated with poor concordance with therapy in rheumatoid arthritis patients: the impact on disease outcomes. Clin Exp Rheumatol. 2014, 32, 904–913. [Google Scholar]
- Hoekstra, M.; van de Laar, M.A.; Bernelot Moens, H.J.; Kruijsen, M.W.; Haagsma, C.J. Longterm observational study of methotrexate use in a Dutch cohort of 1022 patients with rheumatoid arthritis. J Rheumatol. 2003, 30, 2325–2329. [Google Scholar] [PubMed]
- Smolen, J.S.; Landewé, R.B.M.; Bijlsma, J.W.J.; Burmester, G.R.; Dougados, M.; Kerschbaumer, A.; et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2019 update. Ann Rheum Dis. 2020, 79, 685–699. [Google Scholar] [CrossRef] [PubMed]
- Yasir, S.J. Alrubaye; Mohammed, B.M. Al-Juboori; Ameer, K. Al-Humairi. The Causes of Non-Adherence to Methotrexate in Patients with Rheumatoid Arthritis. Research J. Pharm. and Tech. 2021, 14, 769–774. [Google Scholar]
- Treharne, G.; Lyons, A.; Kitas, G. Medication adherence in Rheumatoid arthritis: effects of psychosocial factors. Psychology, Health & Medicine. 2004, 9, 337–349. [Google Scholar]
Figure 1.
Correlation between three questionnaires of quality of life in the patients with rheumatoid arthritis.
Figure 1.
Correlation between three questionnaires of quality of life in the patients with rheumatoid arthritis.
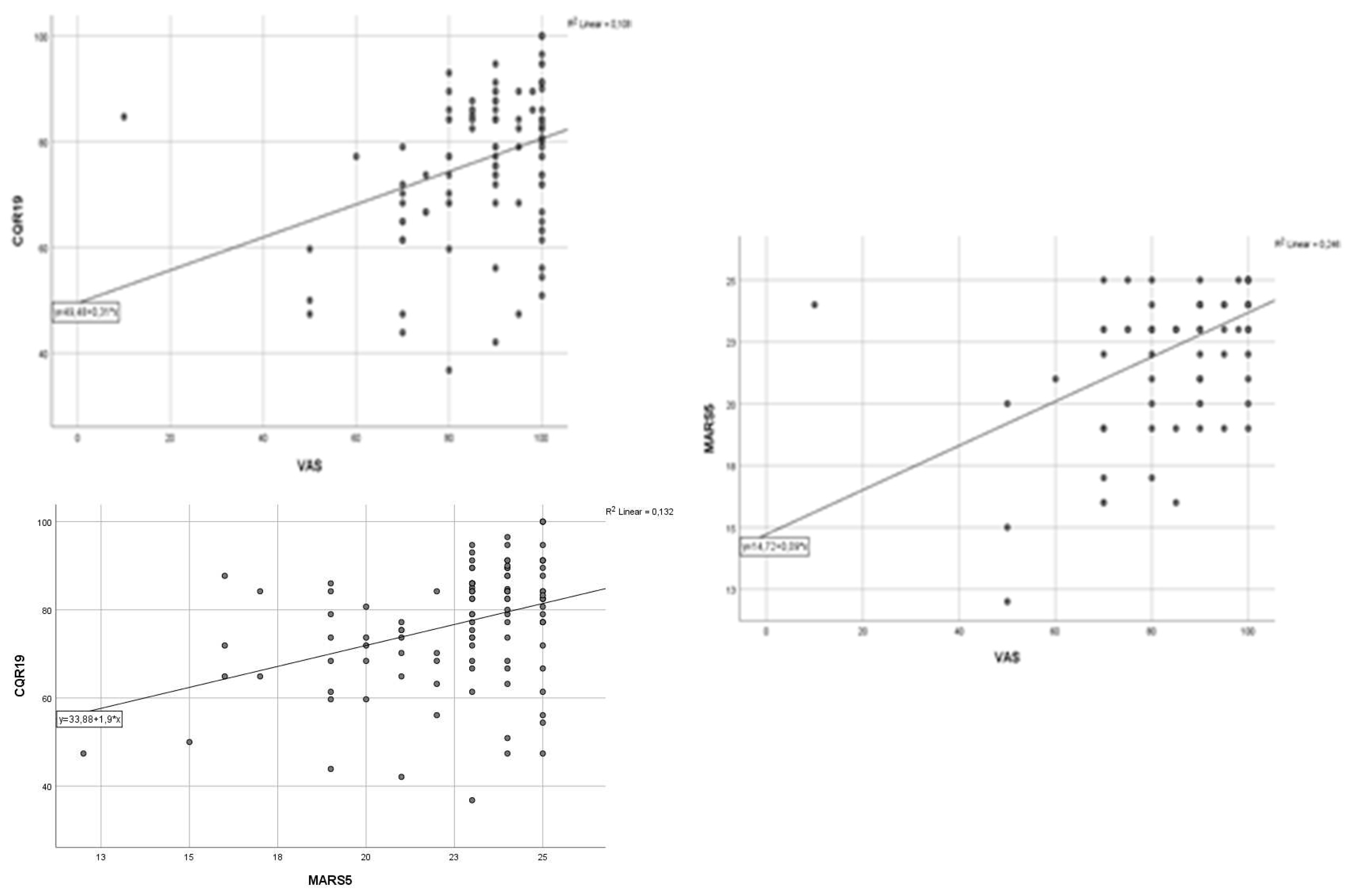

Table 1.
Participant characteristics and comparison between demographic, clinical, and psycho-logical features of adherent and non-adherent patients.
Table 1.
Participant characteristics and comparison between demographic, clinical, and psycho-logical features of adherent and non-adherent patients.
| All (n=111) | VAS | MARS-5 | CQR19 | |||||||
| Variable | Adherent | Nonadherent | p | Adherent | Nonadherent | p | Adherent | Nonadherent | p | |
| Female n (%) | 87 (78,4) | 72 (78.3) | 15 (78.9) | 1 | 64 (82.1) | 22 (68.8) | 0.201 | 48 (88.9) | 38 (67.9) | 0.015 |
| Male n (%) | 24 (21.6) | 20 (21.7) | 4 (21.1) | 14 (17.9) | 10 (31.3) | 6 (11.1) | 18 (32.1) | |||
| Age (yrs) | 56.2±10.6 | 56.0±9.9 | 57.1±13.8 | 0.708 | 56.3±10.5 | 56.5±10.9 | 0.927 | 54.2±10.1 | 58.5±10.6 | 0.031 |
| Living city, n (%) | 88 (79.3) | 73 (79.3) | 15 (78.9) | 1 | 66 (84.6) | 21 (65.6) | 0.049 | 43 (79.6) | 44 (78.6) | 1 |
| Living countryside, n (%) | 23 (20.7) | 19 (20.7) | 4 (21.1) | 12 (15.4) | 11 (34.4) | 11 (20.4) | 12 (21.4) | |||
| Employment status | ||||||||||
| Unemployed n (%) | 31 (27.9) | 27 (29.3) | 4 (21.1) | 0.564 | 23 (29.5) | 8 (25.0) | 0.861 | 18 (33.3) | 13 (23.3) | 0.24 |
| Employed n (%) | 39 (35.1) | 33 (35.9) | 6 (31.6) | 27 (34.6) | 11 (34.4) | 20 (37.0) | 18 (32.1) | |||
| Retiree n (%) | 41 (36.9) | 32 (34.8) | 9 (47.7) | 28 (35.9) | 13 (40.6) | 16 (29.6) | 25 (44.6) | |||
| Education | ||||||||||
| Primary n (%) | 9 (8.1) | 7 (7.6) | 2 (10.5) | 0.896 | 5 (6.4) | 4 (12.5) | 0.528 | 3 (5.6) | 6 (10.7) | 0.539 |
| Secondary n (%) | 76 (68.5) | 63 (68.5) | 13 (68.4) | 55 (70.5) | 20 (62.5) | 39 (72.2) | 36 (64.3) | |||
| Higher n (%) | 26 (23.4) | 22 (23.9) | 4 (21.1) | 18 (23.1) | 8 (25.0) | 12 (22.2) | 14 (25.0) | |||
| Nonsmoker n (%) | 54 (48.6) | 44 (47.8) | 10 (52.6) | 0.742 | 38 (48.7) | 15 (46.9) | 0.936 | 22 (40.7) | 31 (55.4) | 0.308 |
| Ex-smoker n (%) | 25 (22.5) | 22 (23.9) | 3 (15.8) | 17 (21.8) | 8 (25.0) | 14 (25.9) | 11 (19.6) | |||
| Smoker n (%) | 32 (28.8) | 26 (28.3) | 6 (31.6) | 23 (29.5) | 9 (28.1) | 18 (33.3) | 14 (25.0) | |||
| Comorbidities: n (%) | ||||||||||
| 0 | 37 (33.3) | 32 (34.8) | 5 (26.3) | 0.373 | 28 (35.9) | 8 (25.0) | 0.039 | 22 (40.7) | 14 (25.0) | 0.243 |
| 1 | 30 (27.0) | 22 (23.9) | 8 (42.1) | 16 (20.5) | 14 (43.8) | 12 (22.2) | 18 (32.1) | |||
| 2 | 21 (18.9) | 19 (20.7) | 2 (10.5) | 14 (17.9) | 7 (21.9) | 8 (14.8) | 13 (23.2) | |||
| ≥ 3 | 23 (20.7) | 19 (20.7) | 4 (21.1) | 20 (26.6) | 3 (9.4) | 12 (22.2) | 11 (19.6) | |||
| Disease duration (yrs) | 6 (3-13.5) | 6 (3-13) | 7 (4-17) | 0.452 | 6 (3-13.8) | 6 (3.3-13.5) | 1 | 6 (3.8-14.3) | 6 (3-10.3) | 0.37 |
| Physician visits (per year) | 4 (3-6) | 4 (3-6) | 3 (2-4) | 0.036 | 4 (3-6) | 3 (3-7.5) | 0.285 | 4 (3-6) | 4 (3-5.8) | 0.812 |
| Tender joint count (n) | 5 (1-10) | 5 (1-10) | 4 (0-12) | 0.488 | 6 (1-10) | 4 (0-9.5) | 0.298 | 4.5 (1-10) | 5 (1-11) | 0.797 |
| Swollen joint count (n) | 0 (0-3) | 0 (0-2.5) | 0 (0-4) | 0.635 | 1 (0-2) | 0 (0-3.8) | 0.629 | 0.5 (0-2.8) | 0 (0-3) | 0.869 |
| SE (mm/h) | 26 (14-52) | 26 (14-51) | 39 (20-63) | 0.187 | 26 (12-51) | 28 (17.5-72.75) | 0.293 | 24 (13-47.5) | 28 (14.75-62.25) | 0.154 |
| CRP (mg/l) | 3.89 (1.28-14.99) | 3.42 (1.00-13.96) | 4.75 (2.98-18.3) | 0.197 | 3.05 (0.92-10.03) | 6.5 (2.39-15.73) | 0.062 | 2.87 (0.87-9.53) | 5.21 (2-19) | 0.042 |
| IL-6 (pg/ml) | 12.7 (3.59-42.26) | 14.34 (3.23-13.96) | 5.38 (4.43-42.2) | 0.599 | 12.08 (2.89-42.26) | 14.2 (4.03-41.75) | 0.832 | 16.68 (7.76-43.24) | 4.7 (2-40.34) | 0.059 |
| Dosage MTX (mg) | 15(10-17.5) | 15 (10-17.5) | 12.5 (10-15) | 0.03 | 15 (10-17.5) | 12.5 (10-15) | 0.22 | 15 (10-17.5) | 15 (10-17.5) | 0.506 |
| Side effects of MTX, n (%) | 31 (28.2) | 23 (25.0) | 8 (42.1) | 0.218 | 20 (25.6) | 11 (34.4) | 0.489 | 12 (22.2) | 19 (33.9) | 0.249 |
| Concomitant steroids, n (%) | 96 (86.5) | 82 (91.1) | 14 (73.7) | 0.049 | 70 (92.1) | 25 (78.1) | 0.086 | 51 (96.2) | 44 (80.0) | 0.022 |
| Dosage of corticosteroids (mg) | 6.0(5-9.5) | 5.5 (5-8.5) | 7.5 (5-10) | 0.64 | 5 (5-8.5) | 7.5 (5-10) | 0.473 | 6 (5-10) | 5.5 (5-9.5) | 0.659 |
| sDMARD n (%) | 44 (39.6) | 35 (38.0) | 9 (47.4) | 0.618 | 26 (33.3) | 17 (53.1) | 0.086 | 17 (31.5) | 26 (46.4) | 0.158 |
| bDMARD n (%) | 34 (30.6) | 30 (32.6) | 4 (21.1) | 0.471 | 24 (30.8) | 10 (31.2) | 1,000 | 16 (29.6) | 18 (32.1) | 0.937 |
| CDAI | 17.7±12.4 | 17.8±12.8 | 17.3±10.3 | 0.894 | 17.9±12.7 | 16.97±11.8 | 0.732 | 16.4±11.5 | 18.7±13.2 | 0.347 |
| DAS28-ESR | 4.31±1.7 | 4.28±1.8 | 4.4±1.5 | 0.761 | 4.3±1.7 | 4.3±1.8 | 0.871 | 4.2±1.7 | 4.4±1.7 | 0.628 |
| HAQ | 0.9±0.5 | 0.9±0.5 | 0.9±0.4 | 0.881 | 0.9±0.5 | 0.9±0.4 | 0.935 | 0.9±0.5 | 0.9±0.5 | 0.694 |
| HADS depression | 7.6±3.5 | 7.4±3.5 | 9.0±3.7 | 0.072 | 7.1±3.5 | 8.8±3.3 | 0.03 | 7.2±3.4 | 7.9±3.7 | 0.246 |
| HADS anxiety | 6.1±3.8 | 5.8±3.7 | 7.6±4.0 | 0.07 | 6.0±4.0 | 6.2±3.1 | 0.776 | 6.6±4.1 | 5.6±3.4 | 0.204 |
Results are expressed as mean value ± standard deviation, median (25st; 75rd percentile), or number (percentage). Chi-square test or Fisher’s Exact test; Mann-Whitney test; Independent Samples t-test.
Table 2.
The medication adherence rate to methotrexate.
| Scale | Adherence | N (%) | |
|---|---|---|---|
| CQR19 | 76.92 ± 13.47 | Nonadherent | 56 (50.5) |
| Adherent | 54 (48.6) | ||
| MARS-5 | 22.63 ± 2.58 | Nonadherent | 32 (28.8) |
| Adherent | 78 (70.3) | ||
| VAS | 87.44 ± 16.49 | Nonadherent | 19 (17.1) |
| Adherent | 92 (82.9) |
Results are expressed as mean value ± standard deviation or number (percentage); Adherence is expressed as a dichotomous variable.
Table 3.
Univariant logistic regression-prediction of nonadherent behavior.
| Baseline predictor | VAS | MARS-5 | CQR19 | |||
|---|---|---|---|---|---|---|
| OR (95%CI) | p | OR (95%CI) | p | OR (95%CI) | p | |
| Gender | 1.042 (0.311-3.490) | 0.947 | 0.481(0.187-1.238) | 0.481 | 0.264 (0.095-0.730) | 0.010 |
| Age (yrs) | 1.009 (0.963-1.057) | 0.705 | 1.002 (0.963-1.042) | 0.926 | 1.041 (1.003-1.081) | 0.034 |
| Residence | 0.976 (0.209-3.283) | 0.969 | 0.347 (0.134-0.901) | 0.030 | 0.938 (0.374-2.353) | 0.891 |
| Employment status | 1.227 (0.314-4.799) | 0.768 | 1.171 (0.403-3.405) | 0.772 | 1.246 (0.479-3.242) | 0.652 |
| Education | 0.722 (0.134-3.879) | 0.704 | 0.455 (0.111-1.863) | 0.273 | 0.462 (0.107-1.984) | 0.299 |
| Tobacco use | 0.600 (0.150-2.404) | 0.471 | 1.192 (0.425-3.343) | 0.738 | 0.558 (0.213-1.457) | 0.233 |
| Comorbidities | 2.327 (0.672-8.060) | 0.183 | 3.062 (1.057-8.874) | 0.039 | 2.357 (0.875-6.351) | 0.090 |
| Disease duration (years) | 1.027 (0.967-1.092) | 0.385 | 0.997 (0.944-1.053) | 0.907 | 0.973 (0.925-1.023) | 0.286 |
| Physician visits (per year) | 0.904 (0.759-1.077) | 0.260 | 1.006 (0.889-1.137) | 0.929 | 1.007 (0.899-1.127) | 0.910 |
| Tender joint count | 0.974 (0.892-1.062) | 0.549 | 0.974 (0.907-1.046) | 0.464 | 0.996 (0.936-1.061) | 0.913 |
| Swollen joint count | 1.001 (0.841-1.191) | 0.992 | 1.007 (0.871-1.163) | 0.930 | 1.039 (0.908-1.189) | 0.579 |
| SE (mm/h) | 1.009 (0.995-1.023) | 0.226 | 1.005 (0.992-1.017) | 0.473 | 1.008 (0.996-1.020) | 0.186 |
| CRP (mg/l) | 1.001 (0.978-1.024) | 0.947 | 0.992 (0.971-1.014) | 0.498 | 1.005 (0.987-1.023) | 0.587 |
| IL-6 (pg/ml) | 0.982 (0.948-1.018) | 0.327 | 1.003 (0.986-1.021) | 0.727 | 0.997 (0.981-1.013) | 0.711 |
| Dosage MTX (mg) | 0.881 (0.783-0.992) | 0.036 | 0.952 (0.864-1.048) | 0.314 | 0.981 (0.889-1.071) | 0.673 |
| Concomitant steroids | 0.273 (0.078-0.956) | 0.042 | 0.306 (0.094-0.998) | 0.050 | 0.157 (0.033-0.746) | 0.020 |
| Dosage of steroids (mg) | 1.019 (0.829-1.252) | 0.857 | 1.067 (0.905-1.258) | 0.440 | 0.995 (0.859-1.154) | 0.951 |
| sDMARDs | 1.303 (0.470-3.615) | 0.611 | 2.267 (0.980-5.244) | 0.056 | 1.886 (0.866-4.107) | 0.110 |
| bDMARDs | 0.677 (0.205-2.231) | 0.521 | 1.062 (0.424-2.662) | 0.898 | 1.143 (0.493-2.649) | 0.756 |
| Side effects of MTX | 2.182 (0.782-6.085) | 0.136 | 1.519 (0.624-3.696) | 0.357 | 1.797 (0.770-4.193) | 0.175 |
| CDAI | 0.997 (0.957-1.039) | 0.893 | 0.994 (0.960-1.029) | 0.729 | 1.016 (0.983-1.049) | 0.344 |
| DAS 28-ESR | 1.047 (0.781-1.404) | 0.759 | 0.980 (0.768-1.250) | 0.869 | 1.058 (0.846-1.323) | 0.624 |
| VAS | 0.999 (0.976-1.022) | 0.942 | 1.006 (0.986-1.025) | 0.574 | 1.011 (0.993-1.029) | 0.246 |
| HAQ | 0.920 (0.315-2.690) | 0.879 | 1.038 (0.434-2.482) | 0.934 | 1.179 (0.524-2.654) | 0.691 |
| HADS depression | 1.137 (0.986-1.311) | 0.077 | 1.142 (1.010-1.293) | 0.035 | 1.068 (0.956-1.193) | 0.245 |
| HADS anxiety | 1.126 (0.988-1.283) | 0.076 | 1.017 (0.909-1.137) | 0.773 | 0.934 (0.842-1.038) | 0.204 |
Table 4.
Multivariate logistic regression analysis: predictors of non-adherence measured by the MARS-5.
Table 4.
Multivariate logistic regression analysis: predictors of non-adherence measured by the MARS-5.
| Predictor | OR (95%CI) | p |
| HADS depression | 1.131 (0.994-1.286) | 0.061 |
| Concomitant use of steroids | 0.281 (0.078-0.999) | 0.050 |
| Comorbidities | 0.805 (0.538-1.206) | 0.293 |
‡ The given values represent the standardized regression coefficient β.
Table 5.
Multivariate logistic regression analysis: predictors of non-adherence measured by the CQR.
Table 5.
Multivariate logistic regression analysis: predictors of non-adherence measured by the CQR.
| Predictor | OR (95%CI) | p |
| Gender | 0.256 (0.088-0.742) | 0.012 |
| Age | 1.038 (0.996-1.082) | 0.075 |
| Concomitant use of steroids | 0.196 (0.039-0.992) | 0.049 |
‡ The given values represent the standardized regression coefficient β.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



