
Submitted:
14 July 2023
Posted:
17 July 2023
You are already at the latest version
Abstract
Background: Wilms' tumor (or nephroblastoma) is a malignant and solid neoplasm that derives from the primitive renal bud. It represents the most frequent primary tumor of the urogenital tract in childhood, and treatment consists of surgery and chemo-radiotherapy. However, concerning the quality of life, the new therapeutic frontier is exploring other safer and potentially more effective options, such as minimally invasive surgery and biological drugs. Method: Literature (Pubmed) from January 2013 to March 2023 was reviewed. Results: One hundred five articles were included in the review. Conclusion: In addition to the therapeutic strategies already identified, such as classic surgery and pharmacological therapies, recent studies focus attention on the new frontiers of minimally invasive surgery, such as diagnostics using biomarkers and immunotherapy, which could represent a new therapeutic option and possibly less risky than in the past, contributing in fact to the current knowledge of the scientific panorama in terms of "tumor microenvironment" and systemic implications deriving from oncological disease.
Keywords:
wilms
; nephroblastoma
; pediatric urogenital cancer
1. Introduction
1.1. General, and epidemiological profiles
Wilms' tumor (or nephroblastoma) is a solid malignant neoplasm that derives from the primitive renal bud. Wilms' tumor represents the most frequent primary renal form of the urogenital tract in childhood [1] and can be unilateral (in 90-95%), bilateral or multicentric (in forms related to genetic factors), with both synchronous and metachronous presentation [2]. The prevalence of this tumor ranges between 2% and 6% among all childhood neoplasms [3], with an estimated worldwide prevalence of around 1:10,000 [4], based on three characteristics that influence its epidemiological trend: a) age (this tumor mainly affects children under the age of 15 with an average age at diagnosis between 2 and 5 years, and in general as many as 75% of cases occur before the age of 5); b) genders (it is more frequent among females than males); c) country of origin (it has a higher incidence in individuals of African origin, while it has a much lower incidence among Asians, with Europeans being in an intermediate position. [5,6,7]
1.2. Pathology
From a macroscopic point of view, the tumor appears as a mass with well-defined margins, single or more rarely multiple, of a soft consistency; when cut, it appears grayish in colour and homogeneous in appearance, although cysts, areas of necrosis or bleeding may be found inside. On the other hand, microscopic examination can reveal various aspects, which recall the various stages of the embryological development of the kidney. The most common picture consists of three cell types (epithelial, stromal, and blastoma) in various percentages. Each of these cell types can be present in different stages of differentiation: for example, epithelial cells can differentiate into tubular or glomerular cells, while stromal cells can remain undifferentiated or take on a fibrotic, myxoid or even skeletal muscle cell appearance. [8]
Figure 1.
Wilms tumor. The image and description are from the AFIP Atlas of Tumor Pathology, according to entry #407018 in Pathology Education Instructional Resource. The Armed Forces Institute of Pathology Electronic Fascicles (CD-ROM Version of the Atlas of Tumor Pathology) contains U.S. Government work which may be used without restriction.
Figure 1.
Wilms tumor. The image and description are from the AFIP Atlas of Tumor Pathology, according to entry #407018 in Pathology Education Instructional Resource. The Armed Forces Institute of Pathology Electronic Fascicles (CD-ROM Version of the Atlas of Tumor Pathology) contains U.S. Government work which may be used without restriction.
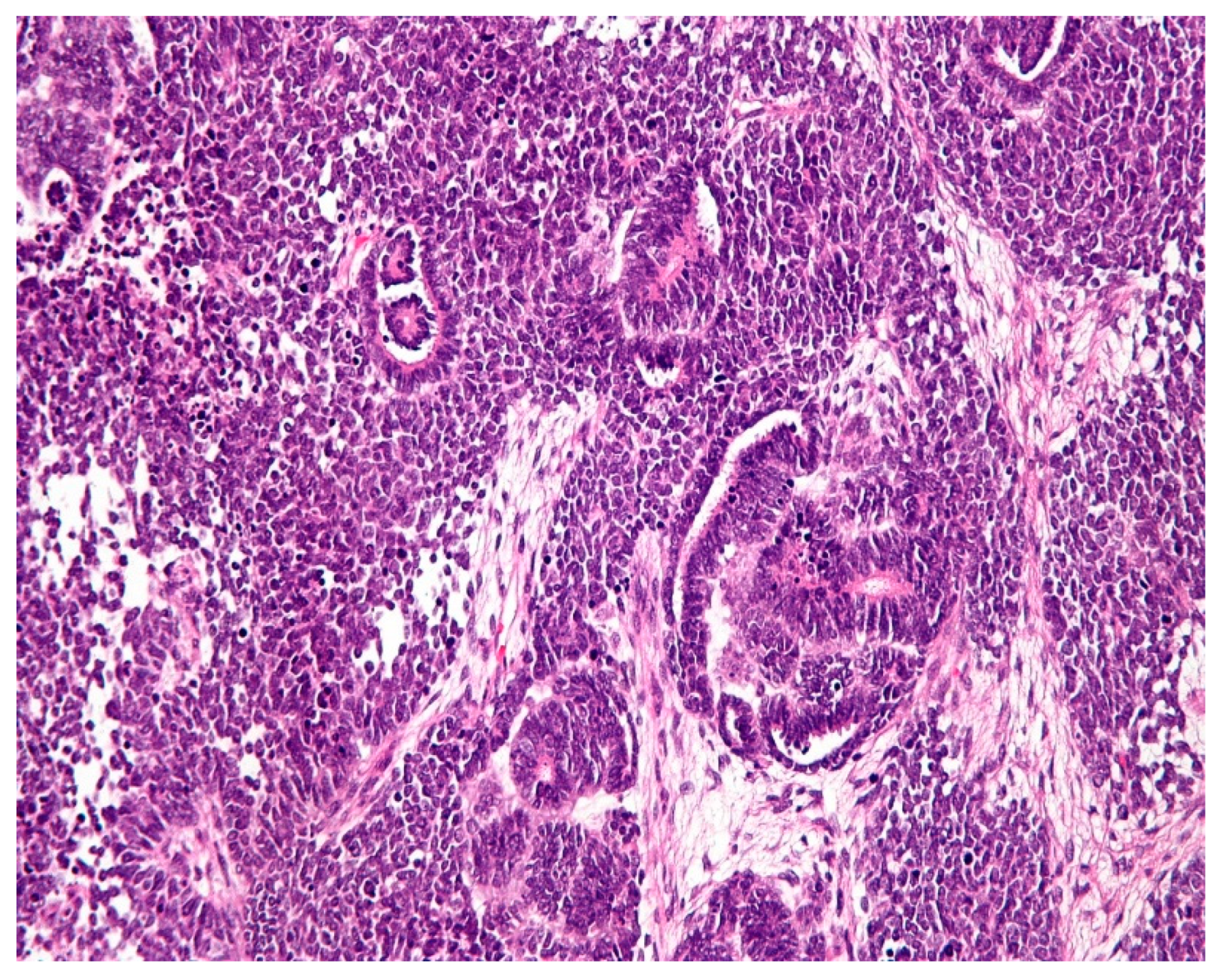
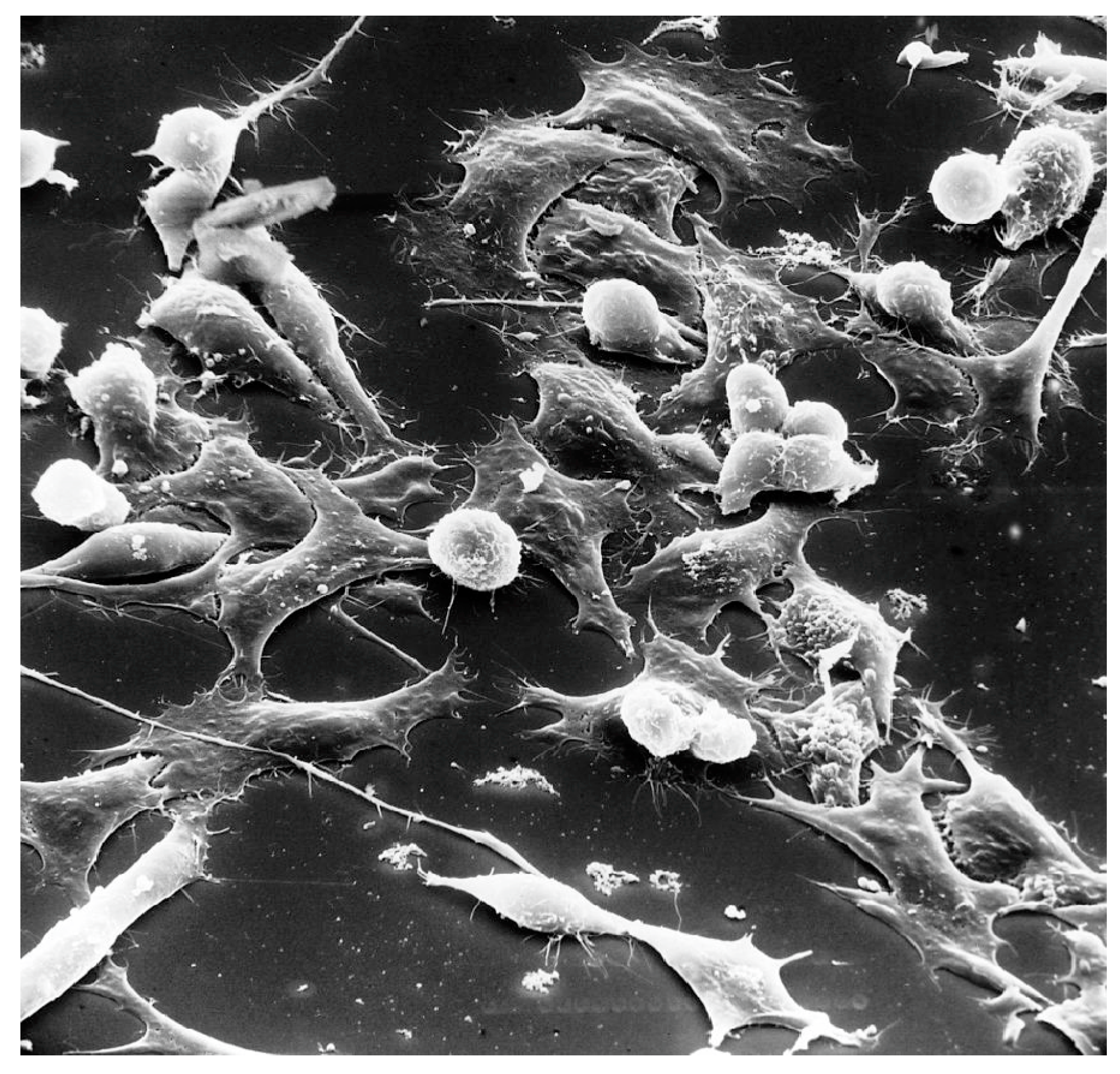
Figure 2.
Wilms tumor. Scanning electron micrograph of a Wilms' tumor, which is a human tumor that like typical tumors when attaches to a surface is round. After it has been attached it spreads out. The magnification is x130. This image is in the public domain and can be freely reused. Source: https://visualsonline. cancer.gov/details.cfm?imageid=1763.
Figure 2.
Wilms tumor. Scanning electron micrograph of a Wilms' tumor, which is a human tumor that like typical tumors when attaches to a surface is round. After it has been attached it spreads out. The magnification is x130. This image is in the public domain and can be freely reused. Source: https://visualsonline. cancer.gov/details.cfm?imageid=1763.
1.3. Clinical profiles
Unlike renal cell carcinoma, which is often asymptomatic, Wilms' tumor often manifests itself in the form of a palpable abdominal mass, with a smooth surface and the presence of abdominal pain. Systemic symptoms consist of fever, weight loss, and fatigue, and less frequently also hematuria (due to internal bleeding) and hypertension (as a result of renin production by tumor cells or activation of the renin-angiotensin-aldosterone axis due to reduced blood supply to the kidney when the tumor compresses the renal artery) can be present. Five stages of the disease are generally identified, and defined based on the extent of the tumor and its eventual distant spread: a) Stage I (tumor completely surgically removed, without infiltration of the renal capsule or involvement of the vessels, integrity of the tumor mass and absence of tumor cells at the margin of resection); b) Stage II (tumor completely surgically removed, resection margins free from neoplastic cells or presence of infiltration of perirenal fat or blood vessels); c) Stage III (incomplete surgical excision of the tumour, spread to abdominal or pelvic lymph nodes or peritoneum, preoperative chemotherapy, and previous tumor biopsy, rupture of the tumor mass during surgery or piecemeal surgical excision; d) Stage IV (spread to extra-abdominal lymph nodes or distant metastases); e) Stage V (bilateral tumor, with each tumor in turn staged from I to IV). [9,10] Wilms' tumor is often associated with other malformations or congenital defects of the urogenital system or other systems. It presents in Beckwith-Wiedemann syndrome, a genetic pathology usually caused by an imprinting defect or uniparental paternal disomy for the 11p15 region, with an incidence of 1:15,000 births [11] or WAGR syndrome that is characterized by mental retardation, aniridia, and genital anomalies [12] or Denys-Drash syndrome in which male pseudohermaphroditism is observed due to a defect in the development of the gonads and renal insufficiency [13].
1.4. Aim
A review was conducted to determine the state of the art on this neoplasm and the implications derived from the discoveries regarding genetic predisposition and alternative therapies to classic surgery and chemo-radiotherapy.
2. Materials and method
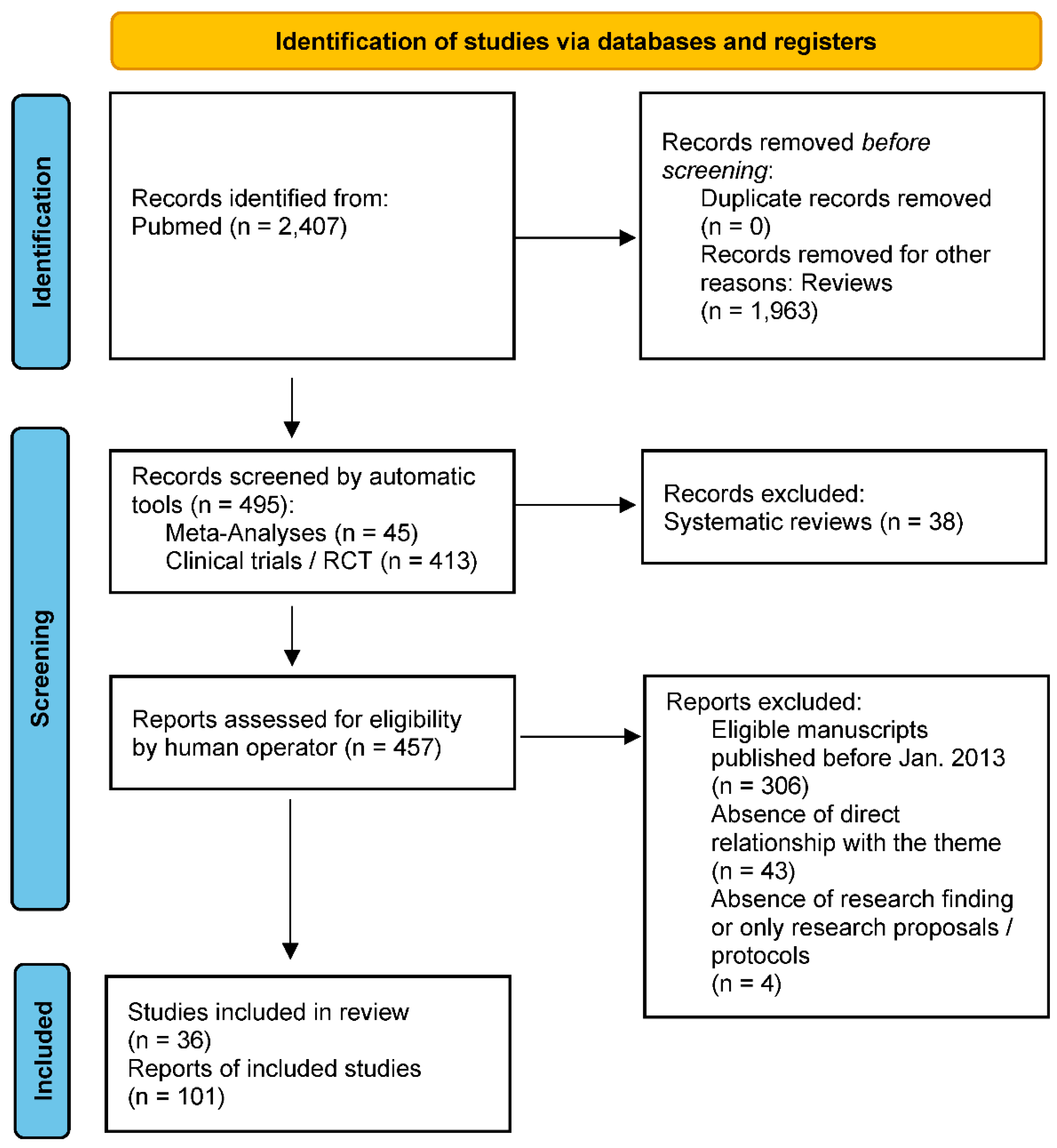
The authors searched PubMed, from January 2013 to March 2023, for meta-analyses, clinical trials and randomized controlled trials using the binomial “Wilms OR Nephroblastoma”, selecting 458 eligibility results. To have a greater and complete overview of the topic, ultimately selecting a total of 65 studies, still adding 36 more reviews to be able to argue the elaborated content (to more easily contextualize definitions and clinical-diagnostic profiles), for an overall total of 101 results. Simple reviews, opinion contributions, or publications in popular volumes were excluded because they were not relevant or redundant for this work. The search was not limited to English-language papers.
Figure 3.
PRISMA flow diagram template for systematic reviews. Matthew J Page et al. BMJ 2021;372:bmj.n71.
Figure 3.
PRISMA flow diagram template for systematic reviews. Matthew J Page et al. BMJ 2021;372:bmj.n71.
3. Results
3.1. Etiology
Most scientific literature agrees that Wilms' tumor develops as a result of a genetic mutation. The implicated gene is called WT1 (from "Wilms Tumor") and is a tumor suppressor. The WT1 gene has been located on the short arm of chromosome 11 at position 11p13 and encodes a protein involved in the early stages of embryological development of the kidney (nephroblast differentiation). This gene is expressed only for a short period in embryogenesis, increasing during gestation reaching a peak at birth, to then decreasing significantly in the first 15 days after delivery (this regulation of gene expression is selective for the kidney). [14] If mutated in both alleles, this gene causes tumor onset. In hereditary forms, the mutation on one of the alleles is inherited from one parent, while the mutation on the other allele is acquired later, while in sporadic (non-hereditary) forms both mutations are acquired. [15] Some gene mutations, on the other hand, lead to the production of a non-functioning protein, thus determining a lack of control of cellular differentiation; however, when present in germ cells, these mutations cause severe developmental abnormalities of the kidneys and abnormalities of sexual differentiation, demonstrating the essential role of WT1 in the normal development of the urogenital tract. Other mutations are implicated in Wilm’s tumor, such as the inactivation of the WTX gene located on the short arm of chromosome 11 at position 11p15, deletion of WT2, and loss of heterozygosity of 16q and 1p [16,17,18], as well as the TP53 mutation is associated with a worse prognosis [19], while HMGA2 gene polymorphisms might weakly influence Wilms tumor predisposition, under certain circumstances [20]. Exposure to pesticides (such as organophosphates), vitamin deficiency of folic acid during pregnancy, and maternal consumption of cigarettes, and alcohol are finally related to this pathology. [21,22]
3.2. Diagnosis
Wilms’ tumor should always be suspected in the presence of a palpable abdominal mass in childhood, and abdominal ultrasonography is the simplest, noninvasive diagnostic method that can aid in the differential diagnosis of hydronephrosis or other benign lesions of the kidney. On ultrasound, Wilm’s tumor has the characteristics of a solid and inhomogeneous mass, in the context of which hypoechoic areas may be highlighted as the expression of intratumor necrosis. [23] On the other hand, contrast-enhanced computed tomography is more accurate and has the advantage of precisely defining the intra-abdominal extension of the tumor (for example, the invasion of lymph nodes or the presence of thrombi in the renal vein or the vena cava). Magnetic resonance imaging defines the invasion of the great vessels much better than ultrasound [24] or computed tomography [25] or Positron Emission Tomography [26], although the latter is rarely used in U.S. medical practice. The use of biomarkers [27], including the prognostic biomarker circulating tumor DNA, seems promising but needs more insight into their use and validity [28,29,30].
3.3. Therapy
Treatments are modulated according to clinical and anatomopathological variables, as well as according to national protocols specific to each national health system. Generally, the initial treatment of unilateral Wilms' tumor is primary surgical resection (with an approach that can be either anticipated or delayed based precisely on each patient's histologic and clinical outcomes) followed by adjuvant chemotherapy. A select group of younger patients with small tumors can be cured with surgery alone. The type of chemotherapy drug and the duration of therapy depend on the tumor histology and stage. Chemotherapy regimens depend on the risk group but usually consist of actinomycin D (dactinomycin) and vincristine, with or without doxorubicin, or adriamycin. For more aggressive tumors, intensive multi-agent chemotherapy regimens are used. Children with very large unresectable tumors or bilateral tumors are candidates for chemotherapy followed by reevaluation and resection at a later time. Radiotherapy is given to children who have the disease at a higher stage (stage III, and in the presence of distant metastases, usually of the lungs, which do not regress readily with chemotherapy). In most cases, radical nephrectomy is practised, i.e. the surgical removal of the affected kidney, associated with the resection of the regional and para-aortic lymph nodes ipsilateral to the neoplasm; in bilateral tumors or patients with specific syndromes predisposing to the onset of nephroblastoma, partial nephrectomy is to be preferred whenever feasible [31,32,33,34,35]; when possible, especially in the case of bilaterality, preference should be given to even partial preservation of the renal structure, unless clinical conditions permit and the balance with the renal function to be preserved is compatible with possible tumor recurrence [36,37]. There emerges an improvement in clinical picture and renal parenchyma over historical outcomes in children with the bilateral form if the treatment approach includes standardized three-drug preoperative chemotherapy, surgical resection within 12 weeks of diagnosis and response, and postoperative therapy based on the histologic picture [38]; still, although investigational, one study showed that concomitant administration of WT1-immunotherapy and standard neoadjuvant therapy was well tolerated and induced WT1-specific antibodies in patients undergoing aromatase inhibitors in the neoadjuvant phase, however, in patients undergoing neoadjuvant chemotherapy or trastuzumab-chemotherapy combination, the humoral response was impaired or attenuated, probably due to the co-administration of corticosteroids and/or the chemotherapeutics themselves [39]. One study finally showed that radiofrequency with cryoablation was also effective for this tumor type [40]. However, immunotherapy and cryotherapy are not yet generally approved therapies by scientific communities such as the Children's Oncology Group and the Renal Tumour Study Group of the International Society of Paediatric Oncology (SIOP-RTSG), due to the few studies still in the literature. [41]
3.4. Prognosis
It is primarily linked to the histological aspect of the neoplasm, where the presence of anaplastic (undifferentiated) cells suggests a more unfavourable prognosis. The prognosis of Wilms' tumor also depends on the stage at diagnosis and the patient's age (as older age is associated with a worse prognosis). Cure rates for low-stage (kidney-localized) disease range from 85 to 95%; and even children with more advanced diseases have a good prognosis: cure rates range from 60% (unfavourable histology) to 90% (favourable histology). However, the tumor can sometimes recur, generally within two years of diagnosis, although healing is also possible in children with relapsing cancer. The outcome after recurrence is better in children who present with a low-stage disease, whose tumors tend to recur in a site that has not been irradiated, who relapse more than one year after onset, and who initially receive less intensive treatment. [42] Thus, the issue of tumor recurrence, especially in the hypothesis of bilaterality, is a negative index that warrants more careful and prolonged monitoring over time. [43]
3.5. Nutritional implications
Diagnosis of Wilms' tumor implies a modification of the patient's nutritional plan, based on the symptoms and severity of the disease, such as to make a generalization impossible as each patient is a unique universe that requires a careful analysis of all factors involved, starting from age and subjective anamnesis, following him in all stages of the disease process. A synergistic relationship will thus be established with any other therapies that may be prescribed, to promote the necessary functional integration, which could lead to a specific diet or a supplementary regimen of minerals and vitamins, including prebiotic and probiotic therapies capable of promoting eubiosis of the organism which finds itself having to face cycles of decompensating pharmacological therapy. [44,45]
3.6. Psychological implications
As in all forms of oncology, the "cancer" event also necessarily impacts the psychological profile of the patient affected by the disease, just as it impacts the personal and relational life of his or her family members, considering also the average age of the patient (of child range). Having to deal with the issue of death is always complicated, and for this reason, the family network must be supported at all stages of the disease, to ensure those minimum tools necessary to compensate for the distress caused by the disease. In the case of Wilms' tumor, the final prognosis is good in most cases, especially if diagnosed in the early stages of the disease, and thus there is a greater chance of helping the patient and his or her family to overcome this complicated phase; however, the therapist must be prepared to deal with the possible distress that is grafted onto one or more personality frameworks of the people involved, perhaps already dysfunctional or decompensated by other pathologies, including mental pathologies, in psychophysical comorbidity. One needs only think of neurotic pictures, characterized by anxious, phobic, somatic, obsessive, or humoral (whether depressive or manic) outbursts, all the way to personality disorders. In more complex cases, irrespective of one's personality framework, the "cancer" event itself can trigger both acute distress (in its mildest forms) and adjustment disorder (following the diagnosis and processing process), all the way up to true post-traumatic stress, especially if the diagnosis is more unfavourable or not adequately managed by the clinical and family network. Therefore, the need to support the patient and family, from the earliest stages of the illness, is central to the healing process (including through cycles of psychotherapy and parental training techniques), also and especially in the future perspective, and unfortunately, both in medical practice and in the literature such profiles are often underestimated or relegated to mere services offered on par with organizational refreshments, effectively distorting the valuable clinical intervention on the cognitive and psychological sphere of the actors involved in the clinical stage. [46,47,48,49,50,51,52,53,54]
4. Discussion
The literature of the past decade, in addition to confirming pathology and clinical knowledge, has focused on etiologic research of genetic biomarkers, as well as minimally invasive surgery and new biologic therapies. Indeed, numerous biomarkers of Wilms' tumor have been confirmed and variations in prevalence have been highlighted, but most of these studies were based on small (and therefore unrepresentative) samples; in particular, they showed that the limited prevalence of currently known genetic alterations in Wilms' tumors indicates that significant factors of initiation and progression remain to be discovered, thus a marked emphasis on ethnicity as one source of heterogeneity. [29] The literature is equally rich in contributions on the topic of classical surgery and drug therapies (including chemo-radiotherapy);, as science progressed, much attention was paid to those qualitative profiles of the patient's life that were necessarily bent to the therapist's desire to promote healing. In patients with Wilms' tumor, the high cure rate (>90%) achieved with the combination of surgery (including minimally invasive techniques [55,56] and ablation) and radio-chemotherapy was often at the expense of high early and/or late toxicity, as well as treatment-resistant entities, such as diffuse anaplastic tumors or recurrent disease (also comorbidities), which still pose unresolved or difficult to solve clinical problems due to the lack of specific research, if not studies still in the experimental phase [39,40,57,58,59,60,61] or with specific protocols that nevertheless use nevertheless small [62] or even insufficient population samples [63,64], also by virtue of specific vaccinations for Wilms' tumor peptide 1 involved in other oncological diseases (e.g. glioblastoma, pancreatic adenocarcinoma, promyelocytic leukemia, acute myeloid leukemia, certain types of head-neck cancer, malignant glioma, lung carcinoma, ovarian and uterine carcinoma, and melanoma) [65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93] and myelodysplastic syndrome [94,95]. The effects of preoperative chemotherapy, however, appear promising [96], distinguishing between the three different tumor lineages (in fact, stromal and epithelial features have been shown to correlate with more favourable histology, whereas blastemal features are more unfavourable as late-stage tumors shift precisely toward the renal blastemal archetype) [97,98]. Finally, attention to psychological, nutritional, and athletic profiles [99,100] also becomes crucial in facilitating the patient's healing process, while also paying attention to aspects often considered secondary to intestinal eubiosis [101] and general systemic eubiosis.
5. Conclusions
Minimally invasive surgery, as well as diagnostics using biomarkers and combined therapies, could represent a new and possibly less risky therapeutic option than in the past, effectively contributing to the current knowledge of the scientific landscape in terms of "tumor microenvironment" and the resulting systemic implications from oncological disease. The research, in this regard, is still incomplete and immature, and therefore requires further study and specific studies with significantly larger and more representative population samples, although these profiles nevertheless appear promising, especially because of the new single and combination therapies. On the other hand, there appears to be insufficient attention to therapeutic profiles aimed at restoring the eubiosis and psychological well-being of the patient and his or her family members, profiles that are almost always underestimated and in the background among the possible therapies suggested by health professionals.
Funding
This work received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgements
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Spreafico, F.; Bellani, F.F. Wilms' tumor: past, present and (possibly) future. Expert Rev Anticancer Ther 2006, 6, 249–258. [Google Scholar] [CrossRef] [PubMed]
- Welter, N.; Brzezinski, J.; Treece, A.; Chintagumpala, M.; Young, M.D.; Perotti, D.; Kieran, K.; Jongmans, M.C.J.; Murphy, A.J. The pathophysiology of bilateral and multifocal Wilms tumors: What we can learn from the study of predisposition syndromes. Pediatr. Blood Cancer 2022, 70, e29984. [Google Scholar] [CrossRef] [PubMed]
- Vujanic, G.M.; Parsons, L.N.; D’Hooghe, E.; Treece, A.L.; Collini, P.; Perlman, E.J. Pathology of Wilms' tumour in International Society of Paediatric Oncology (SIOP) and Children's oncology group (COG) renal tumour studies: Similarities and differences. Histopathology 2022, 80, 1026–1037. [Google Scholar] [CrossRef] [PubMed]
- García-Perdomo, H.A.; González-Arboleda, A.A.; Fernandez, N. Genitourinary Tract Tumors in Children: An Update. Curr. Pediatr. Rev. 2022. [Google Scholar] [CrossRef]
- Ekenze, S.O.; Okafor, O.C.; Obasi, A.A.; Okafor, D.C.; Nnabugwu, I.I. Wilms tumor in Africa: A systematic review of management challenges and outcome in two decades (2000-2019). Pediatr. Blood Cancer 2020, 67, e28695. [Google Scholar] [CrossRef] [PubMed]
- Ortiz, M.V.; Koenig, C.; Armstrong, A.E.; Brok, J.; de Camargo, B.; Mavinkurve-Groothuis, A.M.C. Advances in the clinical management of high-risk Wilms tumors. Pediatr Blood Cancer 2023, 70, e30153. [Google Scholar] [CrossRef]
- Libes, J.; Hol, J.; Vallance, K.L.; van Tinteren, H.; Benedetti, D.J.; Ramirez Villar, G.L. Pediatric renal tumor epidemiology: Global perspectives, progress, and challenges. Pediatr Blood Cancer 2023, 70, e30006. [Google Scholar] [CrossRef]
- Mohd, A.B.; A Ghannam, R.; Mohd, O.B.; Elayan, R.; Albakri, K.; Huneiti, N.; Daraghmeh, F.; Al-Khatatbeh, E.; Al-Thnaibat, M. Etiologies, Gross Appearance, Histopathological Patterns, Prognosis, and Best Treatments for Subtypes of Renal Carcinoma: An Educational Review. Cureus 2022, 14, e32338. [Google Scholar] [CrossRef]
- Takahashi, R.; Asanuma, H.; Mizuno, R.; Oya, M. Current clinical perspective of urological oncology in the adolescent and young adult generation. Int. J. Clin. Oncol. 2022, 28, 28–40. [Google Scholar] [CrossRef]
- Perrotta, G. Port-Site Metastasis (PSM): Definition, clinical contexts and possible preventive actions to reduce risk. J Surg Surgical Res 2021, 7, 088–092. [Google Scholar] [CrossRef]
- Quarello, P.; Carli, D.; Biasoni, D.; Nappo, S.G.; Morosi, C.; Cotti, R.; Garelli, E.; Zucchetti, G.; Spadea, M.; Tirtei, E.; et al. Implications of an Underlying Beckwith–Wiedemann Syndrome for Wilms Tumor Treatment Strategies. Cancers 2023, 15, 1292. [Google Scholar] [CrossRef]
- Craver, R.; Stark, M.; Moss, S.; Long, S.; Prasad, P.; Roth, C.C. WAGR, Sex Reversal, Bilateral Gonadoblastomas, and Intralobar Nephrogenic Rests: Uncertainties of Pre-Biopsy Chemotherapy in a High Risk Syndrome for Nephroblastoma. Fetal Pediatr. Pathol. 2022, 42, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Bhutani, N.; Kajal, P.; Sharma, U. Many faces of Wilms Tumor: Recent advances and future directions. Ann. Med. Surg. 2021, 64, 102202. [Google Scholar] [CrossRef] [PubMed]
- Grant, C.N.; Rhee, D.; Tracy, E.T.; Aldrink, J.H.; Baertschiger, R.M.; Lautz, T.B.; Glick, R.D.; Rodeberg, D.A.; Ehrlich, P.F.; Christison-Lagay, E. Pediatric solid tumors and associated cancer predisposition syndromes: Workup, management, and surveillance. A summary from the APSA Cancer Committee. J. Pediatr. Surg. 2021, 57, 430–442. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.; Xiong, Q.-W.; Wang, J.-H.; Peng, W.-X. Roles of lncRNAs in childhood cancer: Current landscape and future perspectives. Front. Oncol. 2023, 13, 1060107. [Google Scholar] [CrossRef]
- Hont, A.B.; Dumont, B.; Sutton, K.S.; Anderson, J.; Kentsis, A.; Drost, J.; Hong, A.L.; Verschuur, A. The tumor microenvironment and immune targeting therapy in pediatric renal tumors. Pediatr. Blood Cancer 2022, 70, e30110. [Google Scholar] [CrossRef]
- Bánki, T.; Drost, J.; Heuvel-Eibrink, M.M.v.D.; Mavinkurve-Groothuis, A.M.C.; de Krijger, R.R. Somatic, Genetic and Epigenetic Changes in Nephrogenic Rests and Their Role in the Transformation to Wilms Tumors, a Systematic Review. Cancers 2023, 15, 1363. [Google Scholar] [CrossRef]
- Bu, Q.; He, H.; Fan, D.; Lyu, J.; Pan, Z.; You, H. Association between loss of heterozygosity of chromosome 16q and survival in Wilms’ tumor: A meta-analysis. Pathol. - Res. Pr. 2018, 214, 1772–1777. [Google Scholar] [CrossRef]
- Lizhi, L.; Rongdong, H.; Shaohua, H.; Yingquan, K.; Huihuang, X.; Shan, L.; Kunbin, T.; Di, X. Association Between TP53 Mutation and Prognosis in Wilms Tumor: A Meta-Analysis. Fetal Pediatr. Pathol. 2020, 40, 653–662. [Google Scholar] [CrossRef]
- Cheng, J.; Zhuo, Z.; Yang, L.; Zhao, P.; Zhang, J.; Zhou, H.; He, J.; Li, P. HMGA2 gene polymorphisms and Wilms tumor susceptibility in Chinese children: a four-center case-control study. Biotechnol. Appl. Biochem. 2019, 67, 939–945. [Google Scholar] [CrossRef]
- Khan, A.; Feulefack, J.; Sergi, C. Exposure to pesticides and pediatric Wilms’ tumor. A meta-analysis on pre-conception and pregnancy parental exposure with an IARC/WHO commentary. Hum. Exp. Toxicol. 2022, 41. [Google Scholar] [CrossRef] [PubMed]
- Doganis, D.; Katsimpris, A.; Panagopoulou, P.; Bouka, P.; Bouka, E.; Moschovi, M.; Polychronopoulou, S.; Papakonstantinou, E.; Tragiannidis, A.; Katzilakis, N.; et al. Maternal lifestyle characteristics and Wilms tumor risk in the offspring: A systematic review and meta-analysis. Cancer Epidemiology 2020, 67, 101769. [Google Scholar] [CrossRef]
- Welter, N.; Furtwangler, R.; Schneider, G.; Graf, N.; Schenk, J-P. Tumor predisposition syndromes and nephroblastoma: early diagnosis with imaging. Radiologie (Heidelb) 2022, 62, 1033–1042. [Google Scholar] [CrossRef]
- Jedrzejewski, G.; Wozniak, M.M.; Pawelec, A.; Matera, A.; Kunach, M.; Madej, T.; Wieczorek, A.P.; Nowakowska, K. Ultrasound screening for neoplasms in children up to 6 years old. Medicine 2016, 95, e5124. [Google Scholar] [CrossRef] [PubMed]
- van der Beek, J.N.; Artunduaga, M.; Schenk, J.; Eklund, M.J.; Smith, E.A.; Lederman, H.M.; Warwick, A.B.; Littooij, A.S.; Khanna, G. Similarities and controversies in imaging of pediatric renal tumors: A SIOP-RTSG and COG collaboration. Pediatr. Blood Cancer 2022, 70, e30080. [Google Scholar] [CrossRef] [PubMed]
- Uslu, L.; Donig, J.; Link, M.; Rosenberg, J.; Quon, A.; Daldrup-Link, H.E. Value of 18F-FDG PET and PET/CT for Evaluation of Pediatric Malignancies. J. Nucl. Med. 2015, 56, 274–286. [Google Scholar] [CrossRef] [PubMed]
- Madanat-Harjuoja, L.M.; Renfro, L.A.; Klega, K.; Tornwall, B.; Thorner, A.R.; Nag, A. Circulating Tumor DNA as a Biomarker in Patients With Stage III and IV Wilms Tumor: Analysis From a Children's Oncology Group Trial, AREN0533. J Clin Oncol 2022, 40, 3047–3056. [Google Scholar] [CrossRef]
- Walz, A.L.; Maschietto, M.; Crompton, B.; Evageliou, N.; Dix, D.; Tytgat, G.; Gessler, M.; Gisselsson, D.; Daw, N.C.; Wegert, J. Tumor biology, biomarkers, and liquid biopsy in pediatric renal tumors. Pediatr. Blood Cancer 2023, 70, e30130. [Google Scholar] [CrossRef]
- Deng, C.; Dai, R.; Li, X.; Liu, F. Genetic variation frequencies in Wilms' tumor: A meta-analysis and systematic review. Cancer Sci. 2016, 107, 690–699. [Google Scholar] [CrossRef]
- Chagtai, T.; Zill, C.; Dainese, L.; Wegert, J.; Savola, S.; Popov, S. Gain of 1q As a Prognostic Biomarker in Wilms Tumors (WTs) Treated With Preoperative Chemotherapy in the International Society of Paediatric Oncology (SIOP) WT 2001 Trial: A SIOP Renal Tumours Biology Consortium Study. J Clin Oncol 2016, 34, 3195–203. [Google Scholar] [CrossRef]
- National Cancer Institute (NIH). Wilms Tumor and Other Childhood Kidney Tumors Treatment (PDQ®)–Patient Version. Available online: https://www.cancer.gov/types/kidney/patient/wilms-treatment-pdq#section/_29.
- Palmisani, F.; Kovar, H.; Kager, L.; Amann, G.; Metzelder, M.; Bergmann, M. Systematic review of the immunological landscape of Wilms tumors. Mol. Ther. - Oncolytics 2021, 22, 454–467. [Google Scholar] [CrossRef]
- Abdelhafeez, A.H.; Reljic, T.; Kumar, A.; Banu, T.; Cox, S.; Davidoff, A.M.; Elgendy, A.; Ghandour, K.; Gerstle, J.T.; Karpelowsky, J.; et al. Evidence-based surgical guidelines for treating children with Wilms tumor in low-resource settings. Pediatr. Blood Cancer 2022, 69, e29906. [Google Scholar] [CrossRef]
- Sforza, S.; Palmieri, V.E.; Raspollini, M.R.; Roviello, G.; Mantovani, A.; Basso, U.; Affinita, M.C.; D'Angelo, A.; Antonuzzo, L.; Carini, M.; et al. Robotic approach with neoadjuvant chemotherapy in adult Wilms’ tumor: A feasibility study report and a systematic review of the literature. Asian J. Urol. 2023, 10, 128–136. [Google Scholar] [CrossRef]
- Malek, M.M.; Behr, C.A.; Aldrink, J.H.; Dasgupta, R.; Heaton, T.E.; Gehred, A.; Lautz, T.B.; Baertschiger, R.M.; Christison-Lagay, E.R.; Tracy, E.T.; et al. Minimally invasive surgery for pediatric renal tumors: A systematic review by the APSA Cancer Committee. J. Pediatr. Surg. 2020, 55, 2251–2259. [Google Scholar] [CrossRef] [PubMed]
- Han, Q.; Li, K.; Dong, K.; Xiao, X.; Yao, W.; Liu, G. Clinical features, treatment, and outcomes of bilateral Wilms' tumor: A systematic review and meta-analysis. J. Pediatr. Surg. 2018, 53, 2465–2469. [Google Scholar] [CrossRef]
- Charlton, J.; Irtan, S.; Bergeron, C.; Pritchard-Jones, K. Bilateral Wilms tumour: a review of clinical and molecular features. Expert Rev. Mol. Med. 2017, 19, e8. [Google Scholar] [CrossRef] [PubMed]
- Ehrlich, P.; Chi, Y.Y.; Chintagumpala, M.M.; Hoffer, F.A.; Perlman, E.J.; Kalapurakal, J.A. Results of the First Prospective Multi-institutional Treatment Study in Children With Bilateral Wilms Tumor (AREN0534): A Report From the Children's Oncology Group. Ann Surg 2017, 266, 470–478. [Google Scholar] [CrossRef]
- Higgins, M.; Curigliano, G.; Dieras, V.; Kuemmel, S.; Kunz, G.; Fasching, P.A.; Campone, M.; Bachelot, T.; Krivorotko, P.; Chan, S.; et al. Safety and immunogenicity of neoadjuvant treatment using WT1-immunotherapeutic in combination with standard therapy in patients with WT1-positive Stage II/III breast cancer: a randomized Phase I study. Breast Cancer Res. Treat. 2017, 162, 479–488. [Google Scholar] [CrossRef] [PubMed]
- Gómez, F.M.; Patel, P.A.; Stuart, S.; Roebuck, D.J. Systematic review of ablation techniques for the treatment of malignant or aggressive benign lesions in children. Pediatr. Radiol. 2014, 44, 1281–1289. [Google Scholar] [CrossRef]
- van den Heuvel-Eibrink, M.M.; Hol, J.A.; Pritchard-Jones, K.; van Tinteren, H.; Furtwängler, R.; Verschuur, A.C.; Vujanic, G.M.; Leuschner, I.; Brok, J.; Rübe, C.; et al. Rationale for the treatment of Wilms tumour in the UMBRELLA SIOP–RTSG 2016 protocol. Nat. Rev. Urol. 2017, 14, 743–752. [Google Scholar] [CrossRef]
- Pater, L.; Melchior, P.; Rube, C.; Cooper, B.T.; McAleer, M.F.; Kalapurakal, J.A.; Paulino, A.C. Wilms tumor. Pediatr Blood Cancer 2021, 68, e28257. [Google Scholar] [CrossRef] [PubMed]
- Malogolowkin, M.; Spreafico, F.; Dome, J.S.; van Tinteren, H.; Pritchard-Jones, K.; van den Heuvel-Eibrink, M.; Bergeron, C.; de Kraker, J.; Graf, N. ; On behalf of the COG Renal Tumors Committee and the SIOP Renal Tumor Study Group Incidence and outcomes of patients with late recurrence of Wilms' tumor. Pediatr. Blood Cancer 2013, 60, 1612–1615. [Google Scholar] [CrossRef] [PubMed]
- Perrotta, G. The acceptance in the elaboration of mourning in oncological diseases: definition, theoretical models, and practical applications. Needs analysis and subjective oncological reality. Biomed J Sci & Tech Res 2019, 21, 2019. [Google Scholar] [CrossRef]
- Geets, E.; Meuwissen, M.; Van Hul, W. Clinical, molecular genetics and therapeutic aspects of syndromic obesity. Clin. Genet. 2018, 95, 23–40. [Google Scholar] [CrossRef] [PubMed]
- Wu, H-Y. Wilms' tumor management. Curr Opin Urol 2005, 15, 273–276. [Google Scholar] [CrossRef]
- Liu, E.K.; Suson, K.D. Syndromic Wilms tumor: a review of predisposing conditions, surveillance and treatment. Transl. Androl. Urol. 2020, 9, 2370–2381. [Google Scholar] [CrossRef]
- Perrotta, G. Anxiety disorders: definitions, contexts, neural correlates and strategic therapy. J Neur Neurosci 2019, 6, 046. [Google Scholar]
- Perrotta, G. Post-traumatic stress disorder: Definition, contexts, neural correlations and cognitive-behavioural therapy. J Pub Health Catalog 2019, 2, 40–7. [Google Scholar]
- Perrotta, G. Depressive disorders: Defi nitions, contexts, differential diagnosis, neural correlates and clinical strategies. Arch. Depression Anxiety 2019, 5, 009–033. [Google Scholar] [CrossRef]
- Perrotta, G. Obsessive-Compulsive Disorder: definition, contexts, neural correlates and clinical strategies. J. Neurol. 2019, 2019, 8–16. [Google Scholar]
- Perrotta, G. Bipolar disorder: definition, differential diagnosis, clinical contexts and therapeutic approaches. Neurosci. Neurol. Surg. 2019, 5, 01–06. [Google Scholar] [CrossRef]
- Perrotta, G. Psychological trauma: definition, clinical contexts, neural correlations and therapeutic approaches. Curr Res Psychiatry Brain Disord 2020, CRPBD-100006. [Google Scholar]
- Perrotta, G. The reality plan and the subjective construction of one's perception: the strategic theoretical model among sensations, perceptions, defence mechanisms, needs, personal constructs, beliefs system, social influences and systematic errors. J Clin. Res. Rep. 2019, 1. [Google Scholar] [CrossRef]
- Bouty, A.; Blanc, T.; Leclair, M.D.; Lavrand, F.; Faure, A.; Binet, A.; Rod, J.; O'Brien, M.; Sarnacki, S.; Nightingale, M.; et al. Minimally invasive surgery for unilateral Wilms tumors: Multicenter retrospective analysis of 50 transperitoneal laparoscopic total nephrectomies. Pediatr. Blood Cancer 2020, 67, e28212. [Google Scholar] [CrossRef] [PubMed]
- Gavens, E.; Arul, G.S.; Pachl, M. A single centre matched pair series comparing minimally invasive and open surgery for the resection of pediatric renal tumours. Surg. Oncol. 2020, 35, 498–503. [Google Scholar] [CrossRef]
- Dix, D.B.; Seibel, N.L.; Chi, Y.-Y.; Khanna, G.; Gratias, E.; Anderson, J.R.; Mullen, E.A.; Geller, J.I.; Kalapurakal, J.A.; Paulino, A.C.; et al. Treatment of Stage IV Favorable Histology Wilms Tumor With Lung Metastases: A Report From the Children’s Oncology Group AREN0533 Study. J. Clin. Oncol. 2018, 36, 1564–1570. [Google Scholar] [CrossRef]
- Irtan, S.; Messahel, B.; Moroz, V.; Taylor, R.E.; Grundy, R.; Kelsey, A.; Vujanic, G.; Pritchard-Jones, K. Outcomes of non-anaplastic stage III and ‘inoperable’ Wilms tumour treated in the UKW3 trial. Radiother. Oncol. 2019, 131, 1–7. [Google Scholar] [CrossRef]
- Vujanic, G.M.; D’Hooghe, E.; Popov, S.D.; Sebire, N.J.; Kelsey, A. The effect of preoperative chemotherapy on histological subtyping and staging of Wilms tumors: The United Kingdom Children's Cancer Study Group (UKCCSG) Wilms tumor trial 3 (UKW3) experience. Pediatr Blood Cancer 2019, 66, e27549. [Google Scholar] [CrossRef]
- Joannon, P.; Becker, A.; Kabalan, P.; Concha, E.; Beresi, V.; Salgado, C.; Martínez, P.; Olate, P.; Arriagada, M.; Espinoza, F.; et al. Results of Therapy for Wilms Tumor and Other Malignant Kidney Tumors: A Report From the Chilean Pediatric National Cancer Program (PINDA). J. Pediatr. Hematol. 2016, 38, 372–377. [Google Scholar] [CrossRef]
- Weigel, B.; Malempati, S.; Reid, J.M.; Voss, S.D.; Cho, S.Y.; Chen, H.X. Phase 2 trial of cixutumumab in children, adolescents, and young adults with refractory solid tumors: a report from the Children's Oncology Group. Pediatr Blood Cancer 2014, 61, 452–6. [Google Scholar] [CrossRef]
- Hol, J.A.; Heuvel-Eibrink, M.M.V.D.; Graf, N.; Pritchard-Jones, K.; Brok, J.; Van Tinteren, H.; Howell, L.; Verschuur, A.; Bergeron, C.; Kager, L.; et al. Irinotecan for relapsed Wilms tumor in pediatric patients: SIOP experience and review of the literature-A report from the SIOP Renal Tumor Study Group. Pediatr. Blood Cancer 2017, 65, e26849. [Google Scholar] [CrossRef]
- Kim, A.; Widemann, B.C.; Krailo, M.; Jayaprakash, N.; Fox, E.; Weigel, B. Phase 2 trial of sorafenib in children and young adults with refractory solid tumors: A report from the Children's Oncology Group. Pediatr Blood Cancer 2015, 62, 1562–6. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, N.; Tsuboi, A.; Kagawa, N.; Chiba, Y.; Izumoto, S.; Kinoshita, M.; Kijima, N.; Oka, Y.; Morimoto, S.; Nakajima, H.; et al. Wilms tumor 1 peptide vaccination combined with temozolomide against newly diagnosed glioblastoma: safety and impact on immunological response. Cancer Immunol. Immunother. 2015, 64, 707–716. [Google Scholar] [CrossRef] [PubMed]
- Koido, S.; Homma, S.; Okamoto, M.; Takakura, K.; Mori, M.; Yoshizaki, S. Treatment with chemotherapy and dendritic cells pulsed with multiple Wilms' tumor 1 (WT1)-specific MHC class I/II-restricted epitopes for pancreatic cancer. Clin Cancer Res 2014, 20, 4228–39. [Google Scholar] [CrossRef]
- Mitrovic, M.; Kostic, T.; Virijevic, M.; Karan-Djurasevic, T.; Vukovic, N.S.; Pavlovic, S.; Tosic, N. The influence of Wilms' tumor 1 gene expression level on prognosis and risk stratification of acute promyelocytic leukemia patients. Int. J. Lab. Hematol. 2019, 42, 82–87. [Google Scholar] [CrossRef] [PubMed]
- Jacobsohn, D.A.; Loken, M.R.; Fei, M.; Adams, A.; Brodersen, L.E.; Logan, B.R.; Ahn, K.W.; Shaw, B.E.; Kletzel, M.; Olszewski, M.; et al. Outcomes of Measurable Residual Disease in Pediatric Acute Myeloid Leukemia before and after Hematopoietic Stem Cell Transplant: Validation of Difference from Normal Flow Cytometry with Chimerism Studies and Wilms Tumor 1 Gene Expression. Biol. Blood Marrow Transplant. 2018, 24, 2040–2046. [Google Scholar] [CrossRef]
- Shibasaki, Y.; Seki, Y.; Tanaka, T.; Miyakoshi, S.; Fuse, K.; Kozakai, T.; Kobayashi, H.; Ushiki, T.; Abe, T.; Yano, T.; et al. The association of level of reduction of Wilms’ tumor gene 1 mRNA transcript in bone marrow and outcome in acute myeloid leukemia patients. Leuk. Res. 2015, 39, 667–671. [Google Scholar] [CrossRef]
- Ogasawara, M.; Miyashita, M.; Yamagishi, Y.; Ota, S. Phase I/II Pilot Study of Wilms' Tumor 1 Peptide-Pulsed Dendritic Cell Vaccination Combined With Conventional Chemotherapy in Patients With Head and Neck Cancer. Ther. Apher. Dial. 2019, 23, 279–288. [Google Scholar] [CrossRef]
- Kreutmair, S.; Pfeifer, D.; Waterhouse, M.; Takács, F.; Graessel, L.; Döhner, K.; Duyster, J.; Illert, A.L.; Frey, A.-V.; Schmitt, M.; et al. First-in-human study of WT1 recombinant protein vaccination in elderly patients with AML in remission: a single-center experience. Cancer Immunol. Immunother. 2022, 71, 2913–2928. [Google Scholar] [CrossRef]
- Sakai, K.; Shimodaira, S.; Maejima, S.; Udagawa, N.; Sano, K.; Higuchi, Y.; Koya, T.; Ochiai, T.; Koide, M.; Uehara, S.; et al. Dendritic cell–based immunotherapy targeting Wilms’ tumor 1 in patients with recurrent malignant glioma. J. Neurosurg. 2015, 123, 989–997. [Google Scholar] [CrossRef]
- Long, J.; Fang, S.; Dai, Q.; Liu, X.; Zhu, W.; Wang, S. The Wilms Tumor-1 (WT1) rs16754 polymorphism is a prognostic factor in acute myeloid leukemia (AML): a meta-analysis. Oncotarget 2016, 7, 32079–87. [Google Scholar] [CrossRef] [PubMed]
- Nishida, S.; Koido, S.; Takeda, Y.; Homma, S.; Komita, H.; Takahara, A.; Morita, S.; Ito, T.; Morimoto, S.; Hara, K.; et al. Wilms Tumor Gene (WT1) Peptide–based Cancer Vaccine Combined With Gemcitabine for Patients With Advanced Pancreatic Cancer. J. Immunother. 2014, 37, 105–114. [Google Scholar] [CrossRef] [PubMed]
- Saito, S.; Yanagisawa, R.; Yoshikawa, K.; Higuchi, Y.; Koya, T.; Yoshizawa, K.; Tanaka, M.; Sakashita, K.; Kobayashi, T.; Kurata, T.; et al. Safety and tolerability of allogeneic dendritic cell vaccination with induction of Wilms tumor 1–specific T cells in a pediatric donor and pediatric patient with relapsed leukemia: a case report and review of the literature. Cytotherapy 2014, 17, 330–335. [Google Scholar] [CrossRef] [PubMed]
- Tsuboi, A.; Hashimoto, N.; Fujiki, F.; Morimoto, S.; Kagawa, N.; Nakajima, H.; Hosen, N.; Nishida, S.; Nakata, J.; Morita, S.; et al. A phase I clinical study of a cocktail vaccine of Wilms’ tumor 1 (WT1) HLA class I and II peptides for recurrent malignant glioma. Cancer Immunol. Immunother. 2018, 68, 331–340. [Google Scholar] [CrossRef] [PubMed]
- Takagi, M.; Ogawa, C.; Iehara, T.; Aoki-Nogami, Y.; Ishibashi, E.; Imai, M.; Kimura, T.; Nagata, M.; Yasuhara, M.; Masutani, M.; et al. First phase 1 clinical study of olaparib in pediatric patients with refractory solid tumors. Cancer 2022, 128, 2949–2957. [Google Scholar] [CrossRef]
- Hirabayashi, K.; Yanagisawa, R.; Saito, S.; Higuchi, Y.; Koya, T.; Sano, K.; Koido, S.; Okamoto, M.; Sugiyama, H.; Nakazawa, Y.; et al. Feasibility and Immune Response of WT1 Peptide Vaccination in Combination with OK-432 for Paediatric Solid Tumors. Anticancer. Res. 2018, 38, 2227–2234. [Google Scholar] [CrossRef]
- Yanagisawa, R.; Koizumi, T.; Koya, T.; Sano, K.; Koido, S.; Nagai, K.; Kobayashi, M.; Okamoto, M.; Sugiyama, H.; Shimodaira, S. WT1-pulsed Dendritic Cell Vaccine Combined with Chemotherapy for Resected Pancreatic Cancer in a Phase I Study. Anticancer. Res. 2018, 38, 2217–2225. [Google Scholar] [CrossRef]
- Zhang, W.; Lu, X.; Cui, P.; Piao, C.; Xiao, M.; Liu, X.; Wang, Y.; Wu, X.; Liu, J.; Yang, L. Phase I/II clinical trial of a Wilms’ tumor 1-targeted dendritic cell vaccination-based immunotherapy in patients with advanced cancer. Cancer Immunol. Immunother. 2018, 68, 121–130. [Google Scholar] [CrossRef]
- Mayanagi, S.; Kitago, M.; Sakurai, T.; Matsuda, T.; Fujita, T.; Higuchi, H.; Taguchi, J.; Takeuchi, H.; Itano, O.; Aiura, K.; et al. Phase I pilot study of Wilms tumor gene 1 peptide-pulsed dendritic cell vaccination combined with gemcitabine in pancreatic cancer. Cancer Sci. 2015, 106, 397–406. [Google Scholar] [CrossRef]
- Brayer, J.; Lancet, J.E.; Powers, J.; List, A.; Balducci, L.; Komrokji, R.; Pinilla-Ibarz, J. WT1 vaccination in AML and MDS: A pilot trial with synthetic analog peptides. Am. J. Hematol. 2015, 90, 602–607. [Google Scholar] [CrossRef]
- Ota, S.; Miyashita, M.; Yamagishi, Y.; Ogasawara, M. Baseline immunity predicts prognosis of pancreatic cancer patients treated with WT1 and/or MUC1 peptide-loaded dendritic cell vaccination and a standard chemotherapy. Hum. Vaccines Immunother. 2021, 17, 5563–5572. [Google Scholar] [CrossRef]
- Ito, Z.; Kan, S.; Bito, T.; Horiuchi, S.; Akasu, T.; Yoshida, S.; Kajihara, M.; Hokari, A.; Saruta, M.; Yoshida, N.; et al. Predicted Markers of Overall Survival in Pancreatic Cancer Patients Receiving Dendritic Cell Vaccinations Targeting WT1. Oncology 2019, 97, 135–148. [Google Scholar] [CrossRef]
- Kyi, C.; Doubrovina, E.; Zhou, Q.; Kravetz, S.; Iasonos, A.; Aghajanian, C.; Sabbatini, P.; Spriggs, D.; O'Reilly, R.J.; E O’cearbhaill, R. Phase I dose escalation safety and feasibility study of autologous WT1-sensitized T cells for the treatment of patients with recurrent ovarian cancer. J. Immunother. Cancer 2021, 9, e002752. [Google Scholar] [CrossRef]
- Fukuda, K.; Funakoshi, T.; Sakurai, T.; Nakamura, Y.; Mori, M.; Tanese, K.; Tanikawa, A.; Taguchi, J.; Fujita, T.; Okamoto, M.; et al. Peptide-pulsed dendritic cell vaccine in combination with carboplatin and paclitaxel chemotherapy for stage IV melanoma. Melanoma Res. 2017, 27, 326–334. [Google Scholar] [CrossRef] [PubMed]
- Green, D.M.; Lange, J.M.; Qu, A.; Peterson, S.M.; Kalapurakal, J.A.; Stokes, D.C.; Grigoriev, Y.A.; Takashima, J.R.; Norkool, P.; Friedman, D.L.; et al. Pulmonary disease after treatment for wilms tumor: A report from the national wilms tumor long-term follow-up study. Pediatr. Blood Cancer 2013, 60, 1721–1726. [Google Scholar] [CrossRef] [PubMed]
- Maslak, P.G.; Dao, T.; Bernal, Y.; Chanel, S.M.; Zhang, R.; Frattini, M.; Rosenblat, T.; Jurcic, J.G.; Brentjens, R.J.; Arcila, M.E.; et al. Phase 2 trial of a multivalent WT1 peptide vaccine (galinpepimut-S) in acute myeloid leukemia. Blood Adv. 2018, 2, 224–234. [Google Scholar] [CrossRef]
- Coosemans, A.; Vanderstraeten, A.; Tuyaerts, S.; Verschuere, T.; Moerman, P.; Berneman, Z.; Vergote, I.; Amant, F.; Van Gool, S.W. Wilms' Tumor Gene 1 (WT1)--loaded dendritic cell immunotherapy in patients with uterine tumors: a phase I/II clinical trial. Anticancer Res. 2013, 33. [Google Scholar]
- Nishida, S.; Ishikawa, T.; Egawa, S.; Koido, S.; Yanagimoto, H.; Ishii, J.; Kanno, Y.; Kokura, S.; Yasuda, H.; Oba, M.S.; et al. Combination Gemcitabine and WT1 Peptide Vaccination Improves Progression-Free Survival in Advanced Pancreatic Ductal Adenocarcinoma: A Phase II Randomized Study. Cancer Immunol. Res. 2018, 6, 320–331. [Google Scholar] [CrossRef]
- Oji, Y.; Hashimoto, N.; Tsuboi, A.; Murakami, Y.; Iwai, M.; Kagawa, N.; Chiba, Y.; Izumoto, S.; Elisseeva, O.; Ichinohasama, R.; et al. Association of WT1 IgG antibody against WT1 peptide with prolonged survival in glioblastoma multiforme patients vaccinated with WT1 peptide. Int. J. Cancer 2016, 139, 1391–1401. [Google Scholar] [CrossRef]
- Nakata, J.; Nakae, Y.; Kawakami, M.; Morimoto, S.; Motooka, D.; Hosen, N.; Fujiki, F.; Nakajima, H.; Hasegawa, K.; Nishida, S.; et al. Wilms tumour 1 peptide vaccine as a cure-oriented post-chemotherapy strategy for patients with acute myeloid leukaemia at high risk of relapse. Br. J. Haematol. 2017, 182, 287–290. [Google Scholar] [CrossRef] [PubMed]
- Uttenthal, B.; Martinez-Davila, I.; Ivey, A.; Craddock, C.; Chen, F.; Virchis, A.; Kottaridis, P.; Grimwade, D.; Khwaja, A.; Stauss, H.; et al. Wilms’ Tumour 1 (WT1) peptide vaccination in patients with acute myeloid leukaemia induces short-livedWT1-specific immune responses. Br. J. Haematol. 2013, 164, 366–375. [Google Scholar] [CrossRef] [PubMed]
- Lu, J.; Gu, Y.; Li, Q.; Zhong, H.; Wang, X.; Zheng, Z. Wilms' tumor 1 (WT1) as a prognosis factor in gynecological cancers: A meta-analysis. Medicine (Baltimore) 2018, 97, e11485. [Google Scholar] [CrossRef] [PubMed]
- Ueda, Y.; Ogura, M.; Miyakoshi, S.; Suzuki, T.; Heike, Y.; Tagashira, S. Phase 1/2 study of the WT1 peptide cancer vaccine WT4869 in patients with myelodysplastic syndrome. Cancer Sci 2017, 108, 2445–2453. [Google Scholar] [CrossRef] [PubMed]
- Israyelyan, A.; Goldstein, L.; Tsai, W.; Aquino, L.; Forman, S.J.; Nakamura, R.; Diamond, D.J. Real-time assessment of relapse risk based on the WT1 marker in acute leukemia and myelodysplastic syndrome patients after hematopoietic cell transplantation. Bone Marrow Transplant. 2014, 50, 26–33. [Google Scholar] [CrossRef]
- Liu, G.; Zhang, Y.; Fu, K.; Hu, J.; Zhao, Z.; Fu, W.; Liu, G.-C. Meta-analysis of the effect of preoperative chemotherapy on Wilms' tumor. J. B.U.ON. : Off. J. Balk. Union Oncol. 2018, 23, 211–217. [Google Scholar]
- Koshinaga, T.; Takimoto, T.; Okita, H.; Tanaka, Y.; Inoue, E.; Oue, T. Blastemal predominant type Wilms tumor in Japan: Japan Children's Cancer Group. Pediatr Int 2019, 61, 351–357. [Google Scholar] [CrossRef]
- Trink, A.; Kanter, I.; Pode-Shakked, N.; Urbach, A.; Dekel, B.; Kalisky, T. Geometry of Gene Expression Space of Wilms' Tumors From Human Patients. Neoplasia 2018, 20, 871–881. [Google Scholar] [CrossRef]
- Hartman, A.; Pluijm, S.M.; Wijnen, M.; Neggers, S.J.; Clemens, E.; Pieters, R.; Heuvel-Eibrink, M.M.v.D. Health-related fitness in very long-term survivors of childhood cancer: A cross-sectional study. Pediatr. Blood Cancer 2017, 65, e26907. [Google Scholar] [CrossRef]
- Yin, Y.; Cao, H.; Zou, H. Influence of psychological nursing intervention in the recovery of children with Wilms' tumor. Minerva Pediatr. 2019, 71, 545–547. [Google Scholar] [CrossRef] [PubMed]
- Perrotta, G. The intestinal microbiota: Towards a multifactorial integrative model. Eubiosis and dysbiosis in morbid physical and psychological conditions. Arch Clin Gastroenterol 2021, 7, 024–035. [Google Scholar]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



