
Submitted:
14 July 2023
Posted:
14 July 2023
You are already at the latest version
Abstract
It is estimated that about 50% of geriatric rehabilitation patients suffer from sarcopenia. Thereby, malnutrition is frequently associated with sarcopenia and dietary intake is the main modifiable risk factor. During hospitalization, older adults are recommended to consume more dietary protein than the current recommended dietary allowance of 0.8 g/kg body weight per day to optimize the recovery of muscular strength and physical function. This prospective study examined the effect of a short-term protein supplementation with protein-enriched foods and drinks on hand-grip strength, nutritional status and physical function in older patients at risk of malnutrition during a three week inpatient orthopedic rehabilitation stay. The Mini Nutritional Assessment (MNA) was used to assess malnutrition. Patients with a MNA score ≤ 23.5 points were randomly assigned to an intervention group (goal: to consume 1.2–1.5 g protein/kg body weight per day) or a control group (standard care). Both groups carried out the same rehabilitation program. Physical recovery parameters were determined at admission and discharge. There was a trend for participants in the intervention group to consume more protein than the control group (P = 0.058): 95.3 (SD 13.2) g/day as compared to 77.2 (SD 24.2) g/day, which corresponds to a mean protein intake of 1.6 (SD 0.3) g/kg/day vs. 1.3 (SD 0.5) g/kg/day. Dietary protein supplementation increased body weight by an average of 0.9 (SD 1.1) kg and fat mass by an average of 0.9 (SD 1.2) kg as compared with baseline (P = 0.039 and P = 0.050, respectively). There was no significant change in hand-grip strength, body composition and physical function. In conclusion, a short-term intervention with protein-enriched foods and drinks enabled older patients at risk of malnutrition to increase their protein intake to levels that are higher than their required intake. In these older individuals with appropriate protein intake, dietary protein supplementation did not result in a greater improvement in physical recovery outcomes during short-term inpatient rehabilitation. The intervention improved dietary protein intake, but further research (e.g., a full-scale randomized controlled trial with sufficient power) is required to determine the effects on physical function outcomes.
Keywords:
aging
; dietary protein
; hand-grip strength
; physical function
; rehabilitation
; sarcopenia
1. Introduction
One of the many threats to an independent lifestyle is the age-related loss of muscle mass and strength, which is referred to as sarcopenia. Sarcopenia can lead to functional impairments and mobility limitations which are related to other geriatric syndromes, such as a propensity to experience falls and immobility [1]. Another important health risk in old age that is often poorly recognized and underdiagnosed is malnutrition. Malnutrition is frequently associated with sarcopenia and poorer chances of functional recovery [2,3]. Both conditions are highly prevalent in geriatric rehabilitation inpatients [4]; thus, they are important to address in the quest to prevent physical dependence in old age. Therefore, it is essential to diagnose and treat malnutrition during inpatient rehabilitation.
Initiating early treatments to maintain proper muscle mass and function is crucial to ensuring optimal patient outcomes across the healthcare continuum [5]. Interventions to support physical function and recovery in geriatric rehabilitation patients include resistance training and nutrition, because both have been shown to improve muscular strength, body composition, and functional performance in older adults [6,7,8]. The currently recommended dietary allowance (RDA) for protein, 0.8 grams protein per kilogram of body weight per day, might not be adequate for maintaining muscle health in old age. For this reason, experts have proposed to increase dietary protein recommendations for older age groups to 1.0 to 1.2 g/kg body weight per day, and an even higher protein intake (1.2 to 1.5 g/kg body weight/day) is advised for those who are exercising or for older people during hospitalization or rehabilitation [9].
The majority of hospital inpatients fail to meet even their minimum estimated energy and protein requirements [10,11,12]. The aim of this pilot study was to evaluate the feasibility (including recruitment, intervention uptake, completion of post-intervention assessment, and completeness of outcome data collection) and the preliminary efficacy of a short-term protein supplementation on physical recovery in older patients at risk of malnutrition during a three-week inpatient orthopedic rehabilitation stay.
2. Material and Methods
2.1. Study Design and Participants
This study was designed as a single-center, randomized, controlled, open-label, parallel-group intervention pilot study with pre- and post-intervention assessments. The goal was to include 20 malnourished older patients who had been admitted to a three-week inpatient orthopedic rehabilitation at the Rehabilitation Center Kitzbuehel in Austria. All patients who were 65 years and older and were at risk of malnutrition were screened for study eligibility. Subjects were excluded if they had a food allergy or intolerance that restricted them from receiving the protein-rich menu or the protein-enriched intervention products, suffered from chronic renal insufficiency (stages 3 or 4), cognitive impairment, or had any other relevant medical history that prevented their participation in the intervention or could affect the study outcome. Eligible patients were asked to participate in the study within the first two days of their rehabilitation stay and signed a written informed consent after receiving detailed explanation of the study and its potential risks. The Medical Ethics Research Committee of Innsbruck Medical University gave their approval for this study.
2.2. Diagnosis of Malnutrition
The nutrition status of all participants was assessed at admission using the Mini Nutrition Assessment Short Form (MNA-SF) questionnaire [13]. If the participant’s score was 11 or less, indicating a “malnutrition risk”, a trained dietitian continued to ask the remaining questions to obtain additional information about factors that could impact their nutritional status. A score between 17 to 23.5 points indicated that the participant was “at risk of malnutrition”, and a score of less than 17 points, that they were “malnourished”.
2.3. Nutritional Intervention
Eligible participants were randomly assigned to an intervention group (n = 10) or a control group (n = 10) in a 1:1 ratio by using the Randomizer for Clinical Trials tool developed at the Medical University of Graz (http://www.randomizer.at/). During the rehabilitation stay, patients in both groups were free to choose different menus. Members of the intervention group received additionally protein-enriched foods (goal: to consume 1.2 to 1.5 g/kg body weight/day) and a protein-enriched drink (providing 150 kcal and 10 g protein per serving, taken twice daily as a between-meal snack). To reach this goal, an individual nutritional plan was developed by a trained dietitian for each patient. The control group received the standard energy and protein-rich hospital menu that was developed for patients aged 65 years and older admitted to this rehabilitation center.
2.4. Rehabilitation Program
In Austria, an insured person who needs post-acute care or conservative treatments is eligible to receive medical rehabilitation care. The orthopedic rehabilitation program (WHO phase 2) lasts 21 days and comprises a variety of services, including exercise therapy (muscle-strengthening exercises for the hip, thigh, and the upper arm and shoulder muscles on three non-consecutive days of the week, 30 minutes per session), electrotherapy, lymphatic drainage, massage, and hydrotherapy. Patients receive an average of two to three hours of treatment daily or 1800 therapy minutes in total during the three-week program [14].
2.5. Outcomes and Data Collection
Data on participant recruitment rate, intervention uptake, and completeness of outcome data collection were recorded for feasibility outcome reporting. Nutritional intake was measured on day four and subsequently in weeks two and three of the rehabilitation stay using a detailed three-day dietary protocol. A checklist of specific food and beverages was used to verify the reported intake, and a visual guide to portion sizes was used to estimate the portion sizes. The verified food records were entered into the food calculation program Necta (Evoca Group, Pinkafeld, Austria) to assess energy and protein intake according to the German Nutrient Database (BLS, Federal Research Centre for Nutrition and Food, Karlsruhe, Germany). In addition, analytical values compiled from food-producing firms were used to estimate the protein content of foods. Average energy and protein intakes were calculated for each patient during the rehabilitation stay. To estimate the patients’ nutritional needs, energy requirements were calculated based on the resting energy expenditure using the Harris and Benedict equation [15] and were multiplied by a factor of 1.4 to estimate the minimal energy requirements [16].
Maximum hand-grip strength (kg) was determined at admission and one day before discharge using a SAEHAN hand dynamometer (Saehan Corporation, South Korea); the highest of the three measurements was reported for the dominant hand. The assessment of hand-grip strength has been assigned considerable clinical value, and this strength is considered as a key characteristic of sarcopenia, with low hand-grip strength (< 27 kg for men and < 16 kg for women) representing the first defining characteristic [17].
Measures of nutritional status included the MNA score at admission, prealbumin level (mg/dL), and the anthropometric and body composition parameters. The body weight, rounded up to the nearest 0.1 kg, was measured on a calibrated weighing chair without shoes or heavy clothing (KERN MCC 250K100M, Stuttgart-Balingen, Germany). The standing height, rounded up to the nearest 0.1 cm, was measured without footwear. The body mass index (BMI) was calculated by dividing the body weight by the height squared (kg/m2). Prior to and at the end of the intervention, all patients were tested for fat-free mass (kg), body cell mass (kg) and fat mass (kg) by using the bioelectrical impedance analysis (BIA) method (BIACORPUS RX4004M, MEDI CAL HealthCare GmbH, Karlsruhe, Germany). Furthermore, the BIA phase angle (PhA°) was determined as an index of the ratio between extracellular and intracellular water, body cell mass, and cellular integrity. A low PhA (cut-off point values from 4.05 to 5.05°) has been shown to be associated with sarcopenia and malnutrition and to be a predictive factor for hospitalization, falls, and frailty [18,19]. A body composition assessment was carried out by trained dietitians according to standard operating procedures.
Each patient’s functional status was assessed with the Health Assessment Questionnaire (HAQ) [20]. The HAQ comprises 20 questions and has been widely validated. The score ranges from 0 (no functional limitations) to 3 (serious function limitations); a score below 0.5 is considered normal, whereas a score above 1.5 indicates severe disability.
2.6. Sample Size
For the chosen 2x2 design, eight participants in the intervention group are required to ensure a large interaction (time x group) effect with α = 0.05 (one-sided) (1 – β = 0.80, assuming an average correlation of the measurement series of r = 0.5; rANOVA). For the within-factor (time) with two measurements (pre-post), fourteen participants in the intervention group are necessary for a large intervention effect (dependent t-test). In this pilot (phase 0) randomized controlled trial, a sample size of twenty patients was considered to evaluate feasibility and limited efficacy testing in preparation for a larger/full-scale trial [21].
2.7. Statistical Analysis
Descriptive statistics were used to describe baseline characteristics and are presented as means and standard deviation (SD). A per-protocol analysis was performed with SPSS (IBM SPSS Statistics version 27, IBM Corp, Armonk, NY, USA). Differences between the two groups at admission (t1) were examined with independent-samples t-test and χ2 test. Changes during rehabilitation from t1 to discharge (t2) were examined using dependent t-test and repeated-measures analyses of variance (rANOVA). To examine changes in variables between the intervention and control group during rehabilitation, the grouping variable was added to the rANOVA. Due to the small sample size and the exploratory nature of this pilot study, inferential statistics were performed to estimate the effects of the intervention (i.e., limited efficacy testing), and the statistical calculations performed are ultimately descriptive. When interpreting the observed effects, the empirical results from the literature were taken into consideration. P-values, therefore, express the replicability of the obtained results in the population under study. A P-value of less than 0.10 (two-sided test) was considered to indicate a trend towards statistical significance to reduce the beta risk.
3. Results
Baseline characteristics are presented in Table 1. Figure 1 shows the flow chart of subjects with reasons for exclusion. Out of the 327 subjects assessed for eligibility, 163 subjects were not at risk of malnutrition. Regarding the 83 subjects assessed as being at risk of malnutrition, the physician did not refer patients to a dietitian for additional nutritional assessments and interventions. For another 54 subjects, the full MNA score indicated a good nutritional status. Of the 27 patients approached for recruitment, 20 agreed and seven declined, yielding a recruitment rate of 74%. In total, twenty participants were randomized to either an intervention group (n = 10) or a control group (n = 10). The participant retention rate was 100% in terms of participants who were randomized to an intervention, attended study visits, and completed measures. At admission, all patients were at risk of malnutrition (MNA score: 21.1 (SD 1.9) points), with no significant differences noted between groups (P = 0.575). During rehabilitation, the intervention group consumed more protein than the control group (P = 0.058): 95.3 (SD 13.2) g/day as compared with 77.2 (SD 24.2) g/day, which corresponds to a mean protein intake of 1.6 (SD 0.3) g/kg per day vs. 1.3 (SD 0.5) g/kg per day. Moreover, the intervention group reached a higher energy intake than the control group (P = 0.021): 2180 (SD 385) kcal/day as compared with 1746 (SD 381) kcal/day.
Figure 2 shows the average protein distribution across the self-selected main meals as a percent of the total provided amount of protein. Breakfast, lunch, and dinner provided 37%, 38%, and 25% protein by a whole food normal diet (Figure 2A) and 38%, 30%, and 32% protein by a whole food plant-based diet, respectively (Figure 2B).
Physical recovery outcomes are shown in Table 2. Body weight improved by an average of 0.9 (SD 1.1) kg in the intervention group (P = 0.039), but was not different between groups (P = 0.762; time x group: P = 0.487). The fat mass increased in participants given higher amounts of protein (P = 0.050), but did not change in the control group (P = 0.923; time x group: P = 0.110). A trend towards an increase in serum prealbumin was observed in the intervention group, ranging from a mean of 21.1 (SD 8.1) mg/dL at admission to 23.6 (SD 8.9) mg/dL at discharge (P = 0.070), whereas the serum prealbumin levels remained unchanged in the control group (P = 0.634; time x group: P = 0.092). In both groups, the hand-grip strength, fat-free mass, body cell mass, and physical function (HAQ) score did not change over time.
4. Discussion
The European Society for Clinical Nutrition and Metabolism (ESPEN) guidelines on clinical nutrition and hydration in geriatrics recommend that a positive malnutrition screening should be followed by a systematic assessment, individual nutritional intervention, monitoring, and the corresponding adjustment of interventions [22]. Because most physicians are not trained to complete a comprehensive nutritional assessment, a critical function of the physician is working with dietitians and other health professionals (e.g., nurses and physical therapists) to implement nutrition care processes. In the present pilot study, almost 50% of the at-risk patients were not referred to a dietitian for further treatment. On the other hand, the retention rate (proportion of participants with valid dietary intake and physical recovery outcome data at follow-up) was found to be 100%. This highlights the importance of providing adequate clinical nutrition training for all healthcare professionals including physicians as a first step, as this enables them to provide timely and adequate nutritional support during rehabilitation stays for patients at risk of malnutrition. The next step would be to draw up a nutritional care plan using a multidisciplinary approach to ensure that older adults are assessed and treated accordingly to improve patients’ nutritional condition.
Protein-enriched foods and drinks were successfully implemented in the menu of older adults during inpatient rehabilitation. Although dietary protein supplementation increased the protein intake to levels that are higher than their required intake, the intervention did not result in a greater improvement in physical recovery outcomes. Time effects were identified for nutritional status (body weight and fat mass), and a trend toward statistical significance for prealbumin was observed. Overall, the average values for some outcomes increased in the intervention group, but few of these reached statistical significance and can be described as trends at best. This may be for two reasons: the high protein intake in the control group of 1.3 g/kg per day and the short follow-up time. These two explanations could also be associated with the fact that merely increasing protein might not be sufficient unless skeletal muscle mass is also built up, an especially relevant aspect for patients at risk of malnutrition [23,24]. Similarly, the results of a recent meta-analysis of randomized clinical trials demonstrated that, although nutritional therapy increased the daily energetic and protein intake, nutritional support had few effects on functional outcomes in malnourished medical inpatients. These results, however, may be attributed to the relatively short duration of the nutritional support [25]. Because we did not want to act against the standard advice to consume a protein-rich diet, the rather high protein intake seen in the control group is probably due to the fact that the rehabilitation center offers protein- and energy-rich menus to older patients during rehabilitation. However, even the recommended high protein intake of 1.2 to 1.5 g/kg per day may be too low for functionally limited older patients to successfully recover muscular strength and physical function, especially those with chronic diseases [26].
Furthermore, the nature of the training stimulus using physiotherapy exercises may have been too low in intensity to stimulate a robust increase in muscle protein synthesis rates. Indeed, the training component per se is of primary importance in improving muscle mass and strength, as well as functional capacity, because a substantial proportion of the older population benefits from a resistance-type exercise training intervention [27]. However, the level of responsiveness to resistance training is strongly affected by the duration of the exercise intervention, with more positive responses observed after more prolonged exercise training [28].
In the present pilot study, older patients at risk of malnutrition exhibited a higher probability of sarcopenia, reaching a prevalence of 45%. This was indicated by their maximum hand-grip strength, which was compared with the cut-off point values for weak hand-grip strength obtained from a healthy, non-frail older population [29]. In a recent systematic review of data from a total of 34,955 participants older than 60 years, the prevalence of sarcopenia was approximately 10% in community-dwelling individuals, 24% in hospitalized individuals, and 51% and 31% for men and women, respectively, in nursing homes [30]. Thus, a significant proportion of older persons suffer from sarcopenia (i.e., a major proportion in clinical and nursing home settings), even in healthy populations. Sarcopenia is associated with adverse health outcomes such as falls, fractures, functional impairments, and mobility limitations, accompanied by an elevated risk for hospitalization, morbidity, and mortality [31].
Conversely, being at nutritional risk is significantly associated odds of suffering from sarcopenia that are two- to three-times higher than normal, resulting in the invention of a new term: “sarcopenia malnutrition syndrome” [32]. The simultaneous presence of malnutrition has been shown to reinforce the loss of muscle mass, muscle strength, and function, which has severe implications for physical performance in older people in both the community and hospital settings [33,34,35]. An analysis of prevalence data for malnutrition and nutritional risk in older adults across different healthcare settings using MNA showed a wide range of malnutrition, ranging from 3% in the community setting to approximately 30% in rehabilitation and sub-acute care settings [36]. Additionally, nutritional status can be assessed by measuring BIA-derived PhA as a proxy for water distribution and body cell mass and, from a practical standpoint, as an index of overall muscle quality [17]. PhA decreases with malnutrition and is directly related to sarcopenia [18]. However, a low PhA mainly indicates an increased risk of malnutrition and does not reveal the underlying cause. It is safe to say, however, that PhA increases when resistance training is practiced and decreases when detraining or inflammation occur [19]. We studied PhA in older rehabilitation patients and found low PhA levels (mean values from 3.83 ± 0.80°), observing no change over time; this may be due to the relatively short follow-up times accompanied by unchanged lean body mass. Low PhA has been linked to dysmobility syndrome (osteoporosis, low lean mass, falls in the preceding year, low grip strength, high fat mass, and poor timed up and go performance) [37], an increased risk of falls, and incident disability in older adults [38,39].
The purpose of this pilot study was to assess the short-term effectiveness of an individualized nutrition intervention in older patients at risk of malnutrition during inpatient rehabilitation. A major strength of this trial is the randomized controlled study design, the inclusion of old and very old subjects, and the use of an objective and standardized test to assess muscle strength and function. However, several limitations must be considered when interpreting the data. Due to the low sample size (lack of power), as only 20 total participants were included in the analysis, this pilot study only provides an indication of its possible effects, but a larger sample (trial) is needed to evaluate the effect of the intervention definitively. Based on our findings, with an observed power of 0.75 for the within-factor (time; η2 = 0.79) and 0.24 for the interaction effect (time x group; η2 = 0.21), a sample size of at least 50 participants for the intervention group (and potentially 50 participants for the control group) would be needed to conduct a larger/full-scale, adequately powered trial (1 - β = 0.95 with α = 0.05) in this rehabilitation setting. Another limitation is the short follow-up time of three weeks. Future interventions will include a post-rehabilitation follow-up to increase the power of the findings. The use of HAQ in estimating physical function was chosen to assess physical pain, function, and health in general, but the patients’ social fitness and well-being may be underrecognized. Nevertheless, the HAQ is one of the most widely used comprehensive, validated, patient-oriented outcome assessment instruments for the evaluation of functional limitations in activities of daily living. A major critical drawback of the study was the rather high protein intake observed in the control group, as they could freely choose what and how much to consume; ideally, strict guidelines regarding what and when to eat should have been given. Finally, the participants’ food habits and lifestyle behaviors before rehabilitation as well as the exercise type or intensity were not assessed. Although information extracted from discussions with physiotherapy staff were not quantified, this seems to indicate that most older patients performed low-intensity exercise. While low-intensity physical activity has significant health benefits, moderate- to high-intensity resistance training is recommended to increase muscle mass, strength, and function in older adults [40]. Because of practical constraints, it was not possible to blind our participants or the study assessors for the intervention allocation, which could have influenced our results.
5. Conclusions
The current pilot study provides insights into the implementation and outcomes of a randomized controlled trial using individualized nutrition support in this unique rehabilitation setting. Our findings show that a short-term intervention with protein-enriched foods and drinks enabled older patients at risk of malnutrition to increase their protein intake to levels that are higher than their required intake. In these older adults with appropriate protein intakes, dietary protein supplementation did not result in a greater improvement in physical recovery outcomes during short-term inpatient rehabilitation. This might be explained by a low difference in total protein intake between groups of 0.3 g/kg body weight per day. Although this intervention shows promise in older patients at risk of malnutrition, further research (e.g., a full-scale randomized controlled trial with sufficient power) is required to determine the effects on physical function outcomes. Moreover, the observed high prevalence of sarcopenia among geriatric rehabilitation patients highlights the need for enhanced rehabilitation programs that target early screening of malnutrition and sarcopenia in a multidisciplinary approach to ensure that older adults are assessed and treated accordingly.
Author Contributions
Conceptualization, M.J.F., B.S., V.G; Methodology, M.J.F., B.S., V.G; Data Curation, I.J., P.R., V.G; Writing – Original Draft Preparation, B.S.; Writing – Review & Editing, B.S., V.G., H.N., W.B., M.J.F.; Supervision, M.J.F.; Project Administration, V.G.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
All procedures performed in studies involving human participants were in accordance with the ethical standards of the Medical Ethics Research Committee of Innsbruck Medical University (AN2016-0132 363/4.20) and with the 1964 Helsinki declaration and its later amendments.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available upon request from the corresponding author.
Acknowledgments
The authors thank the dietitians Barbara Brandtner, Petra Eberharter, Sara Ragazzini, and the therapist Katrin Gollner, who took part in the assessment process. We thank Dr. Sara Crockett for proofreading the manuscript.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Cruz-Jentoft AJ, Sayer AA. Sarcopenia. Lancet 2019, 393, 2636–2646.
- Beaudart C, Sanchez-Rodriguez D, Locquet M, Reginster JY, Lengelé L, Bruyère O. Malnutrition as a strong predictor of the onset of sarcopenia. Nutrients 2019, 11, 2883. [Google Scholar]
- Landi F, Calvani R, Ortolani E, Salini S, Martone AM, Santoro L, Santoliquido A, Sisto A, Picca A, Marzetti E. The association between sarcopenia and functional outcomes among older patients with hip fracture undergoing in-hospital rehabilitation. Osteoporos Int 2017, 28, 1569–1576. [Google Scholar]
- Verstraeten LMG, van Wijngaarden JP, Pacifico J, Reijnierse EM, Meskers CGM, Maier AB. Association between malnutrition and stages of sarcopenia in geriatric rehabilitation inpatients: RESORT. Clin Nutr 2021, 40, 4090–4096. [Google Scholar] [CrossRef] [PubMed]
- Prado CM, Purcell SA, Alish C, Pereira SL, Deutz NE, Heyland DK, Goodpaster BH, Tappenden KA, Heymsfield SB. Implications of low muscle mass across the continuum of care: A narrative review. Ann Med 2018, 50, 675–693. [Google Scholar]
- Ramadi A, Ezeugwu VE, Weber S, Funabashi M, Lima CA, Perracini MR, Beaupre LA. Progressive Resistance Training Program Characteristics in Rehabilitation Programs Following Hip Fracture: A Meta-Analysis and Meta-Regression. Geriatr Orthop Surg Rehabil 2022, 13, 21514593221090799. [Google Scholar]
- Rondanelli M, Cereda E, Klersy C, Faliva MA, Peroni G, Nichetti M, Gasparri C, Iannello G, Spadaccini D, Infantino V, Caccialanza R, Perna S. Improving rehabilitation in sarcopenia: a randomized-controlled trial utilizing a muscle-targeted food for special medical purposes. J Cachexia Sarcopenia Muscle 2020, 11, 1535–1547. [Google Scholar] [CrossRef] [PubMed]
- van Wijngaarden JP, Wojzischke J, van den Berg C, Cetinyurek-Yavuz A, Diekmann R, Luiking YC, Bauer JM. Effects of Nutritional Interventions on Nutritional and Functional Outcomes in Geriatric Rehabilitation Patients: A Systematic Review and Meta-Analysis. J Am Med Dir Assoc 2020, 21, 1207–1215. [Google Scholar]
- Bauer J, Biolo G, Cederholm T, Cesari M, Cruz-Jentoft AJ, Morley JE, Phillips S, Sieber C, Stehle P, Teta D, Visvanathan R, Volpi E, Boirie Y. Evidence-based recommendations for optimal dietary protein intake in older people: a position paper from the PROT-AGE Study Group. J Am Med Dir Assoc 2013, 14, 542–559. [Google Scholar] [CrossRef] [PubMed]
- Groenendijk I, Kramer CS, den Boeft LM, Hobbelen HSM, van der Putten GJ, de Groot LCPGM. Hip Fracture Patients in Geriatric Rehabilitation Show Poor Nutritional Status, Dietary Intake and Muscle Health. Nutrients 2020, 12, 2528. [Google Scholar]
- Weijzen MEG, Kouw IWK, Geerlings P, Verdijk LB, van Loon LJC. During Hospitalization, Older Patients at Risk for Malnutrition Consume <0.65 Grams of Protein per Kilogram Body Weight per Day. Nutr Clin Pract 2020, 35, 655–663. [Google Scholar]
- Hermanky M, Korninger C, Fuchs D, Strasser B. Effects of a protein optimized diet combined with moderate resistance training on the postoperative course in older patients with hip fracture. Aktuel Ernahrungsmed 2017, 42, 180–187. [Google Scholar]
- Kaiser MJ, Bauer JM, Ramsch C, Uter W, Guigoz Y, Cederholm T, Thomas DR, Anthony P, Charlton KE, Maggio M, Tsai AC, Grathwohl D, Vellas B, Sieber CC; MNA-International Group. Validation of the Mini Nutritional Assessment short-form (MNA-SF): a practical tool for identification of nutritional status. J Nutr Health Aging 2009, 13, 782–788. [Google Scholar]
- Grote V, Unger A, Böttcher E, Muntean M, Puff H, Marktl W, Mur E, Kullich W, Holasek S, Hofmann P, Lackner HK, Goswami N, Moser M. General and Disease-Specific Health Indicator Changes Associated with Inpatient Rehabilitation. J Am Med Dir Assoc 2020, 21, 2017.e10–2017.e27. [Google Scholar]
- Roza AM, Shizgal HM. The Harris Benedict equation reevaluated: resting energy requirements and the body cell mass. Am J Clin Nutr 1984, 40, 168–182. [Google Scholar] [CrossRef] [PubMed]
- Volkert D, Beck AM, Cederholm T, Cruz-Jentoft A, Goisser S, Hooper L, Kiesswetter E, Maggio M, Raynaud-Simon A, Sieber CC, Sobotka L, van Asselt D, Wirth R, Bischoff SC. ESPEN guideline on clinical nutrition and hydration in geriatrics. Clin Nutr 2019, 38, 10–47. [Google Scholar]
- Cruz-Jentoft AJ, Bahat G, Bauer J, Boirie Y, Bruyère O, Cederholm T, Cooper C, Landi F, Rolland Y, Sayer AA, Schneider SM, Sieber CC, Topinkova E, Vandewoude M, Visser M, Zamboni M; Writing Group for the European Working Group on Sarcopenia in Older People 2 (EWGSOP2), and the Extended Group for EWGSOP2. Sarcopenia: Revised European Consensus on Definition and Diagnosis. Age Ageing 2018, 48, 16–31.
- Di Vincenzo O, Marra M, Di Gregorio A, Pasanisi F, Scalfi L. Bioelectrical impedance analysis (BIA)-derived phase angle in sarcopenia: A systematic review. Clin Nutr 2021, 40, 3052–3061. [Google Scholar] [CrossRef] [PubMed]
- Norman K, Herpich C, Müller-Werdan U. Role of phase angle in older adults with focus on the geriatric syndromes sarcopenia and frailty. Rev Endocr Metab Disord 2022, 1–9.
- Bruce B, Fries JF. The Stanford Health Assessment Questionnaire: dimensions and practical applications. Health Qual Life Outcomes 2003, 1, 20. [Google Scholar] [CrossRef] [PubMed]
- Hertzog MA. Considerations in determining sample size for pilot studies. Res Nurs Health 2008, 31, 180–191. [CrossRef] [PubMed]
- Volkert D, Beck AM, Cederholm T, Cruz-Jentoft A, Goisser S, Hooper L, Kiesswetter E, Maggio M, Raynaud-Simon A, Sieber CC, Sobotka L, van Asselt D, Wirth R, Bischoff SC. ESPEN guideline on clinical nutrition and hydration in geriatrics. Clin Nutr 2019, 38, 10–47. [Google Scholar]
- Deutz NEP, Ashurst I, Ballesteros MD, Bear DE, Cruz-Jentoft AJ, Genton L, Landi F, Laviano A, Norman K, Prado CM. The underappreciated role of low muscle mass in the management of malnutrition. J Am Med Dir Assoc 2019, 20, 22–27. [Google Scholar] [CrossRef] [PubMed]
- Liao CD, Chen HC, Huang SW, Liou TH. The role of muscle mass gain following protein supplementation plus exercise therapy in older adults with sarcopenia and frailty risks: A systematic review and meta-regression analysis of randomized trials. Nutrients 2019, 11, 1713. [Google Scholar] [CrossRef] [PubMed]
- Gomes F, Baumgartner A, Bounoure L, Bally M, Deutz NE, Greenwald JL, Stanga Z, Mueller B, Schuetz P. Association of Nutritional Support With Clinical Outcomes Among Medical Inpatients Who Are Malnourished or at Nutritional Risk: An Updated Systematic Review and Meta-analysis. JAMA Netw Open 2019, 2, e1915138. [Google Scholar]
- Bhasin S, Apovian CM, Travison TG, Pencina K, Moore LL, Huang G, Campbell WW, Li Z, Howland AS, Chen R, Knapp PE, Singer MR, Shah M, Secinaro K, Eder RV, Hally K, Schram H, Bearup R, Beleva YM, McCarthy AC, Woodbury E, McKinnon J, Fleck G, Storer TW, Basaria S. Effect of Protein Intake on Lean Body Mass in Functionally Limited Older Men: A Randomized Clinical Trial. JAMA Intern Med 2018, 178, 530–541. [Google Scholar]
- Tieland M, Dirks ML, van der Zwaluw N, Verdijk LB, van de Rest O, de Groot LC, van Loon L. Protein supplementation increases muscle mass gain during prolonged resistance-type exercise training in frail elderly people: a randomized, double-blind, placebo-controlled trial. J Am Med Dir Assoc 2012, 13, 713–9. [Google Scholar]
- Churchward-Venne TA, Tieland M, Verdijk LB, Leenders M, Dirks ML, de Groot LC, van Loon LJ. There Are No Nonresponders to Resistance-Type Exercise Training in Older Men and Women. J Am Med Dir Assoc 2015, 16, 400–411. [Google Scholar]
- Dodds RM, Syddall HE, Cooper R, Benzeval M, Deary IJ, Dennison EM, Der G, Gale CR, Inskip HM, Jagger C, Kirkwood TB, Lawlor DA, Robinson SM, Starr JM, Steptoe A, Tilling K, Kuh D, Cooper C, Sayer AA. Grip strength across the life course: normative data from twelve British studies. PLoS One 2014, 9, e113637. [Google Scholar]
- Papadopoulou SK, Tsintavis P, Potsaki P, Papandreou D. Differences in the Prevalence of Sarcopenia in Community-Dwelling, Nursing Home and Hospitalized Individuals. A Systematic Review and Meta-Analysis. J Nutr Health Aging 2020, 24, 83–90. [Google Scholar]
- Bianchi L, Ferrucci L, Cherubini A, Maggio M, Bandinelli S, Savino E, Brombo G, Zuliani G, Guralnik JM, Landi F, Volpato S. The Predictive Value of the EWGSOP Definition of Sarcopenia: Results from the InCHIANTI Study. J Gerontol A Biol Sci Med Sci 2016, 71, 259–64. [Google Scholar] [CrossRef] [PubMed]
- Tan VMH, Pang BWJ, Lau LK, Jabbar KA, Seah WT, Chen KK, Ng TP, Wee SL. Malnutrition and Sarcopenia in Community-Dwelling Adults in Singapore: Yishun Health Study. J Nutr Health Aging 2021, 25, 374–381. [Google Scholar]
- Lengelé L, Bruyère O, Beaudart C, Reginster JY, Locquet M. Impact of Malnutrition Status on Muscle Parameter Changes over a 5-Year Follow-Up of Community-Dwelling Older Adults from the SarcoPhAge Cohort. Nutrients 2021, 13, 407. [Google Scholar]
- Pourhassan M, Rommersbach N, Lueg G, Klimek C, Schnatmann M, Liermann D, Janssen G, Wirth R. The Impact of Malnutrition on Acute Muscle Wasting in Frail Older Hospitalized Patients. Nutrients 2020, 12, 1387. [Google Scholar] [CrossRef] [PubMed]
- Rossi AP, Zanandrea V, Zoico E, Zanardo M, Caliari C, Confente S, Gabriele S, Mazzali G, Fantin F, Zamboni M. Inflammation and nutritional status as predictors of physical performance and strength loss during hospitalization. Eur J Clin Nutr 2016, 70, 1439–1442. [Google Scholar] [CrossRef] [PubMed]
- Cereda E, Pedrolli C, Klersy C, Bonardi C, Quarleri L, Cappello S, Turri A, Rondanelli M, Caccialanza R. Nutritional status in older persons according to healthcare setting: A systematic review and meta-analysis of prevalence data using MNA. Clin Nutr 2016, 35, 1282–1290. [Google Scholar]
- Jung YW, Hong N, Kim CO, Kim HC, Youm Y, Choi J-, Rhee Y. The diagnostic value of phase angle, an integrative bioelectrical marker, for identifying individuals with dysmobility syndrome: the Korean Urban-Rural Elderly study. Osteoporos Int 2021, 32, 939–949. [Google Scholar]
- Uemura K, Yamada M, Okamoto H. Association of bioimpedance phase angle and prospective falls in older adults. Geriatr Gerontol Int 2019, 19, 503–507. [Google Scholar]
- Uemura K, Doi T, Tsutsumimoto K, Nakakubo S, Kim MJ, Kurita S, Ishii H, Shimada H. Predictivity of bioimpedance phase angle for incident disability in older adults. J Cachexia Sarcopenia Muscle 2020, 11, 46–54. [Google Scholar]
- Mertz KH, Reitelseder S, Bechshoeft R, Bulow J, Højfeldt G, Jensen M, Schacht SR, Lind MV, Rasmussen MA, Mikkelsen UR, Tetens I, Engelsen SB, Nielsen DS, Jespersen AP, Holm L. The effect of daily protein supplementation, with or without resistance training for 1 year, on muscle size, strength, and function in healthy older adults: A randomized controlled trial. Am J Clin Nutr 2021, 113, 790–800. [Google Scholar]
Figure 1.
Flow diagram of participant enrollment.
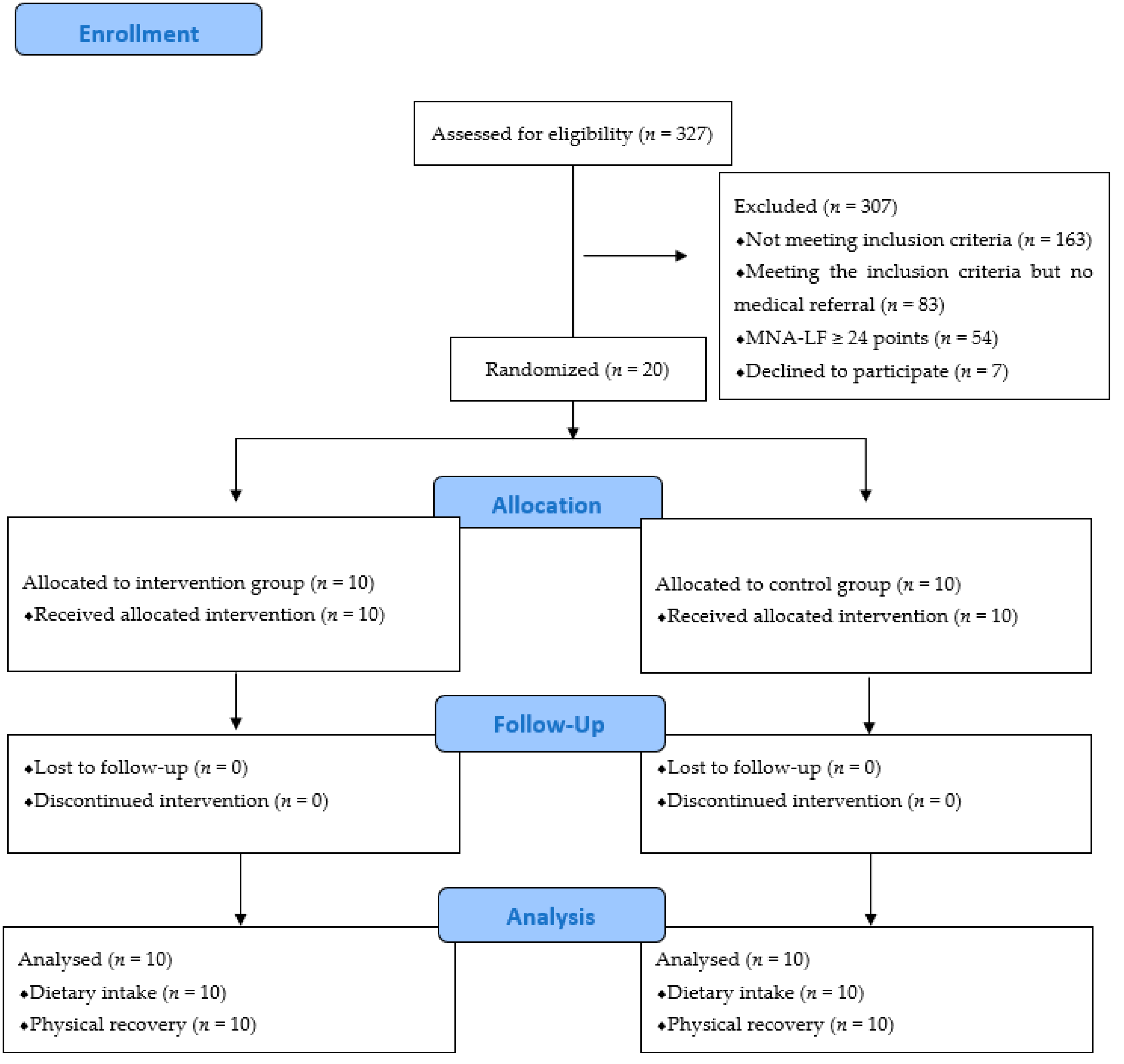
Figure 2.
Average protein distribution across self-selected main meals (expressed as a percentage of the total amount of protein provided) in 20 older patients during rehabilitation.
Figure 2.
Average protein distribution across self-selected main meals (expressed as a percentage of the total amount of protein provided) in 20 older patients during rehabilitation.
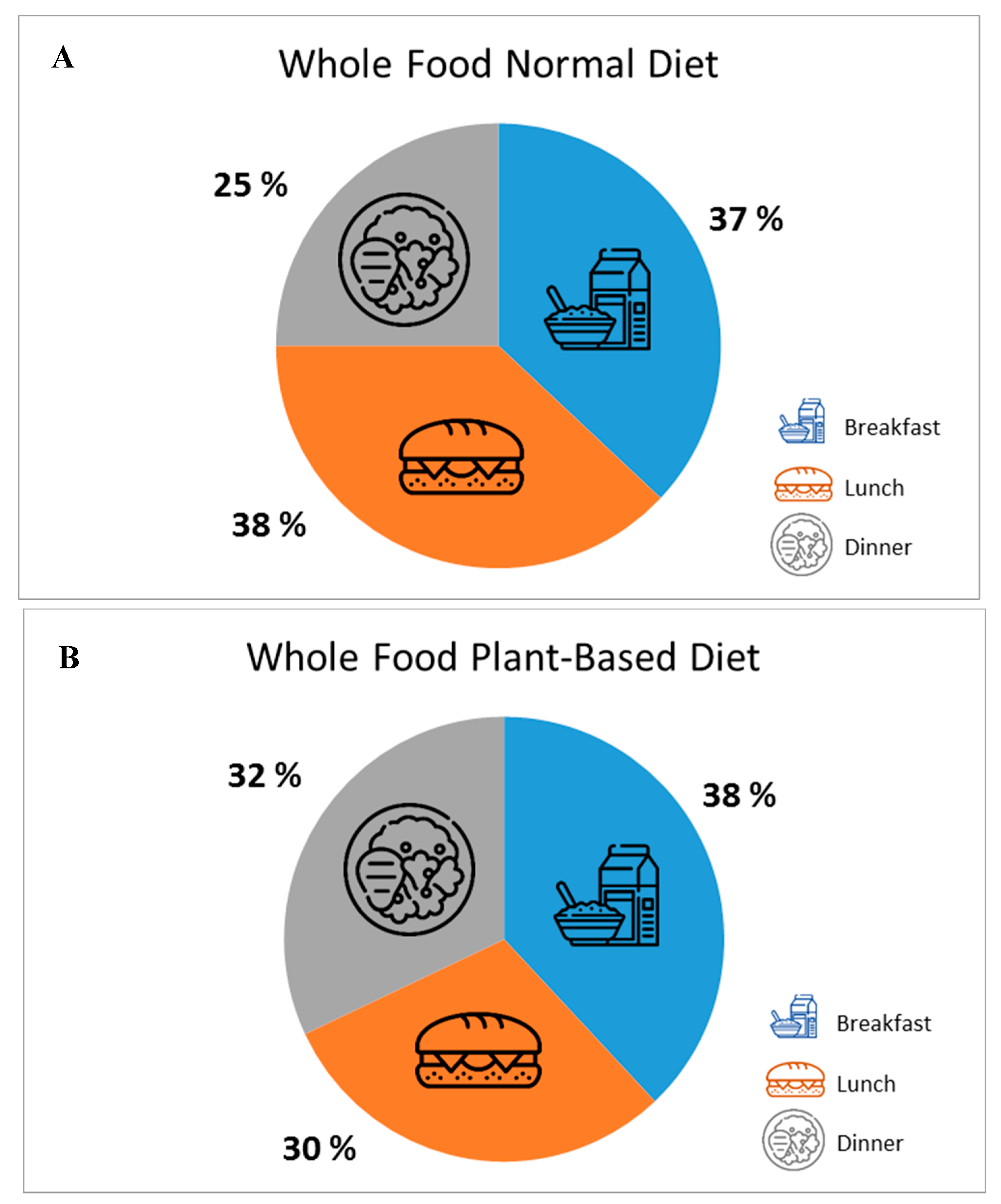

Table 1.
Patients’ characteristics.
| Intervention (n = 10) | Control (n = 10) | P | |
|---|---|---|---|
| Age (years) | 75.0 ± 6.5 | 74.2 ± 6.8 | 0.792 |
| Sex (male/female) | 1/9 | 2/8 | 0.531 |
| Height (cm) | 163.0 ± 8.3 | 162.6 ± 6.8 | 0.907 |
| Body weight (kg) | 60.4 ± 6.9 | 62.2 ± 15.0 | 0.735 |
| BMI (kg/m2) | 22.9 ± 4.0 | 23.5 ± 5.9 | 0.792 |
| RMR (kcal/d) | 1198 ± 99 | 1232 ± 174 | 0.604 |
| MNA (score) | 21.4 ± 2.4 | 20.9 ± 1.3 | 0.575 |
| Mobility aids (yes/no) | 4/6 | 4/6 | 1.000 |
| Medical diagnosis for admission (n) Arthrosis Diseases of the musculoskeletal system Lower limb injuries |
1 2 7 |
1 1 8 |
0.819 |
Values are means ± standard deviation (SD); numbers and percentages; MNA, Mini Nutritional Assessment; Resting metabolic rate (RMR) was calculated based upon gender, body weight, height and age, using the adjusted Harris and Benedict equation [14]: Male: (88.4 + 13.4 x weight in kilograms) + (4.8 x height in centimeters) – (5.68 x age). Female: (447.6 + 9.25 x weight in kilograms) + (3.10 x height in centimeters) – (4.33 x age).
Table 2.
Physical-recovery outcomes at admission (t1) and discharge (t2) in the intervention and control group.
Table 2.
Physical-recovery outcomes at admission (t1) and discharge (t2) in the intervention and control group.
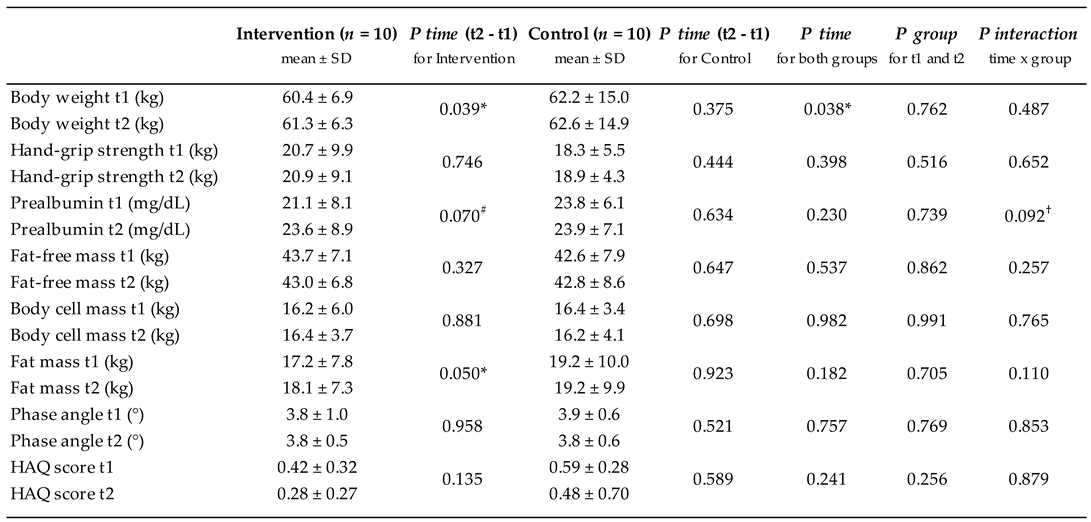
Values are means ± standard deviation (SD); numbers and percentages. HAQ, Health Assessment Questionnaire. *Significant time effect (P < 0.05) compared with admission within a group; #Trend toward significant time effect (P < 0.10) as compared with admission within a group. †Trend toward significant intervention effect or interaction of intervention and time effect (P < 0.10).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



