
Submitted:
29 June 2023
Posted:
30 June 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Introduction SARS-CoV-2 infection normally damages respiratory system but may likewise impair endocrine organs’ function. Thyroid dysfunction and hyperglycemia are common endocrine complications of SARS-CoV-2 infection. Onset of T1D and associated complications including DKA, hospitalization and death, are thought to be increased during the COVID-19 pandemic. The aim of this study is to review the available data about the incidence rate of T1D and accompanying complications since the beginning of the COVID-19 pandemic.
Methods: A systematic review was conducted using electronic databases PubMed and Google Scholar. The keywords “T1D, T1DM, Type 1 DM or Type 1 Diabetes”, “Coronavirus, SARS-CoV-2 or COVID-19” were used to search these databases. Titles and abstracts were screened for selection, and then relevant studies were reviewed in full text.
Result: we selected 21 manuscripts out of 296 identified studies. Data about the incidence rate of T1D, hospitalization and death are not consistent across countries, but DKA incidence and severity seem to be higher during the COVID-19 pandemic.
Conclusion: Our data collection demonstrated that COVID-19 may or may not increase the incidence of type 1 diabetes. Nevertheless, it is associated with higher incidence and severity of DKA in T1D patients. Antivirals are not fully protective against endocrine complications of SARS-CoV-2 infection. Combining medications that reduce SARS-CoV-2 entry into the cells and modulate the immune response to infection is an alternative practical approach to treating COVID-19.
Keywords:
ACE2
; DKA
; SARS-CoV-2
; T1D
1. Introduction
The coronavirus disease 2019 (COVID-19) pandemic, caused by the Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2), remains a prominent global health concern. SARS-CoV-2 is an RNA virus belonging to the family Coronaviridae. There are different variants with unique mutations, which mainly affect the respiratory system, but can also damage the nervous system and endocrine organs. The clinical manifestations of COVID-19 vary from asymptomatic or mild disease to acute respiratory distress syndrome (ARDS), hospitalization and death [1]. The commonly reported endocrine complications are thyroid dysfunction and hyperglycemia [2]. The connection between COVID-19 and endocrine disorders such as Diabetes Mellitus (DM) is a nuanced area of research.
DM is a metabolic disorder characterized by dysfunctional insulin signaling, compromising the ability of cells to absorb glucose, causing hyperglycemia and other debilitating complications, including micro and macro vascular complications. The two main classifications of DM, namely type 1 DM (T1D) and type 2 DM (T2D), differ in that T1D consists of defective insulin production, whereas T2DM consists of inadequate cellular response to insulin signaling [3]. COVID-19 can potentially increase the incidence rate of T1D and T2D. T1D is routinely began by pancreatic cell damage, which is immune mediated and triggered by genetic or environmental factors. Viral infection, such as e enteroviruses and respiratory viruses, are probably responsible for autoimmunity against β-cell [4,5]. Generally, COVID-19 and T2DM appear to have a bidirectional relationship, but the relationship between COVID-19 and T1D remains to be controversial and multi-faceted [6].
Diabetic ketoacidosis (DKA) is a life-threatening complication that usually occurs in patients with T1D. In T1D, the absence of insulin promotes an excess breakdown of fats as an alternative source of energy, resulting in the buildup of acidic ketones and disrupting the organ functions. During the COVID-19 pandemic, there was a notable increase in the incidence and severity of DKA in patients with T1D, suggesting a possibility that COVID-19 and DKA are causally connected [7,8,9]. However, other studies found no evidence of a physiological association between DKA and SARS-CoV-2, implying that the surge in the incidence and severity of DKA during COVID-19 is best attributed to a diminished quality of care for diabetic patients due to an overburdened healthcare system [10,11,12]. Moreover, while the severity of symptoms of T1D may have been exacerbated during the pandemic (once again, arguably due to strains on the healthcare system), the overall incidence rate of T1D may not have necessarily been impacted [13]. Therefore, the interplay between COVID-19 and T1D is rather complex.
This review aims to elucidate the intricate relationship between COVID-19 and T1D, emphasizing the different aspects of epidemiology, pathophysiology, and prognosis. By providing a comprehensive review of the impact of COVID-19 on patients with T1D, this review also identifies potential therapeutic strategies to improve their outcomes and mitigate mortality and morbidity associated with both diseases.
2. Materials and Methods
This review aims to discuss the currently available data about COVID-19 infection in type 1 diabetic patients.
Data sources and searches. According to PRISMA guidelines [14], a systematic search was conducted in PubMed database and Google Scholar for relevant studies. Search dates were between January 2020 and December 2022. The following key words were applied for search: “T1D, T1DM, Type 1 DM or Type 1 Diabetes”, “Coronavirus, SARS-CoV-2 or COVID-19”.
Study selection: Two authors (KK and NA) reviewed abstracts and third author (KA) made a cross-check. We reviewed the references of relevant reviews to include further potentially relevant article. Two authors contributed to the selection process, data extraction and data collection independently of each other. The participants, study type, outcomes and interventions were used to select the relevant studies. The selected studies were discussed to resolve disagreements and a third author participated if needed. We included (1) clinical research articles, such as cohort, cross-sectional, case-control studies and case series, (2) review articles including mini-review, systematic review and meta-analysis, (3) opinion and commentary articles, like editorial, commentary, perspective, and letter to editor, that discuss the incidence, clinical characteristics, outcomes, complications, morbidity and mortality of T1D in COVID-19 patients or vice versa. Figure 1 shows the flowchart for the systematic review.
Duplicates were eliminated after a review of all recognized articles from the initial searches. The remaining papers were read in full. The publications were summarized in terms of the author, journal, year of publication, country of origin, study design, number of participants, type of intervention, age, gender, outcomes (death, DKA, or other complications), new onset diabetes or worsening of pre-existing diabetes, and other results in general.
3. Result
A total of 296 studies were found during the initial database searches. The exclusion process resulted in 21 eligible manuscripts for further investigation [7,8,9,10,11,12,13,15,16,17,18,19,20,21,22,23,24,25,26,27,28] (Table 1).
3.1. COVID-19 and T1D incidence
The incidence of new onset T1D in children was increased in Germany [16], Hungary [29], Romania [21], Turkey [23] and USA [28] but not in Australia [8], Israel [17], Poland [13,19,20], Saudi Arabia [22] and Turkey [30] during the COVID-19 pandemic. Furthermore, there was no significant increase in new onset autoantibody-negative type 1 diabetes in children, adolescents, and young adults in Germany [10] but new onset T1D and autoantibody positivity was higher in Turkey [23] during the pandemic.
3.2. Clinical outcomes and complications of T1D patients during COVID-19
DKA, hospitalization rate, and death were studied in selected studies. DKA incidence, prevalence or severity were increased in most studies [7,8,9,11,12,13,17,18,19,20,21,22,23,26,28] during the COVID-19 pandemic. However, there was no increased in DKA incidence in autoantibody-negative type 1 diabetes in Germany [10], or in new onset T1D in Israel [17]. There was also no increase in severe DKA in Israel [17] and no increase in DKA or severity in USA [25].
4. Discussion
SARS-CoV-2 enters human cells mainly through the ACE2 receptor. There are other receptors that may mediate SARS-CoV-2 entry into human cells, including dipeptidyl peptidase 4 (DPP-4 or CD26), CD147, neuropilin-1, lectins, CD209L, and tyrosine-protein kinase receptor UFO (AXL). The host proteases, such as transmembrane protease serine 2 (TMPRSS2), furin, trypsin, elastase and cathepsin L, are also involved in the process of SARS-CoV-2 entry into cells. ACE2 on cell membrane has other responsibilities against inflammation, proliferation and fibrosis. Disintegrin and metalloproteinase domain-containing protein 17 (ADAM17) is indirectly involved in the process of SARS-CoV-2 entrance and tissue damage by shedding ACE2 from the cell membrane [31,32,33]. ACE2 expression in the GI tract and pancreas is relatively remarkable. It is also expressed in essential metabolic tissues, such as liver, kidney, adipocytes and vasculature [34]. Coronavirus can potentially target the metabolic tissues, especially the pancreas, which leads to islet cell damage [35], insulin resistance [36] and hyperglycemia (Figure 2). The current information about incidence of new onset T1D in children during the pandemic is not consistent across the countries. This could be due to differences in outcomes of treatment modalities, accessibility to effective treatment and speed of conducting a successful approach. However, COVID-19 was associated with increased incidence and severity of DKA in different countries. Furthermore, there are few case reports or case series including euglycemic DKA [37], known T1D and DKA [38], or new onset T1D with or without DKA [39,40,41,42,43,44,45,46,47] following COVID-19 infection or vaccination [48,49], which raises concern over not only a possible causal relationship between COVID-19 and T1D, but also the beneficial roles of early and practical treatment. In addition, it should be emphasized that the occurrence of new SARS-CoV-2 strains with unique mutations can potentially render resistance to the current antivirals that are routinely used, such as Paxlovid, Remdesivir and Molnupiravir [50,51].
Therefore, considering other medications with the potential capability of targeting SARS-CoV-2 receptor, reducing virus entry into the cells and alleviating inflammation may improve clinical outcomes better than antivirals. They may also assist in reducing the risk of hyperglycemia and new onset diabetes. Ursodeoxycholic acid (UDCA) reduces farnesoid X receptor (FXR) signaling, downregulates ACE2 expression in respiratory tract and diminishes susceptibility to SARS-CoV-2 infection. It was associated with reduced hospitalization, ICU admission and death of COVID-19 patients [52]. UDCA was also shown to reduce COVID-19 infectivity and severity in cirrhotic patients [53]. Antiandrogens downregulate TMPRSS2 and ACE2, which reduce SARS-CoV-2 entry into the cells [54]. They lower mortality, hospitalization rate and duration of SARS-CoV-2 infection [55]. Spironolactone, an aldosterone receptor antagonist with anti-androgenic effects, antagonizes TMPRSS2 and ADAM17, reduces virus entry into the cells, and diminishes SARS-CoV-2-mediated endothelial damage [56,57]. It has been reported that spironolactone improves the clinical scores and reduces mortality, ICU admission, intubation and end orang damage in hospitalized COVID-19 patients [57]. Metformin activates AMP-activated protein kinase (AMPK), which leads to phosphorylation of ACE2. ACE2 phosphorylation enhances ACE2 stability on cell membrane, increases Ang (angiotensin) 1-7 and endothelial nitric oxide synthase bioavailability, and therefore provides lung protection by preserving endothelial function. The phosphorylation of ACE2 may affect virus entry into the cells too. Metformin also inhibits mammalian target of rapamycin (mTOR) pathway and modulates the immune response against the infection [58,59,60]. Generally, metformin seems to be helpful by reducing SARS-CoV-2-related tissue injury. Metformin could not improve the clinical outcomes of COVID-19 patients impressively [61] but it could reduce the incidence of long COVID [62]. DPP4 inhibitors have immunomodulatory roles and possibly blunt the alternative route of virus entry through DPP4 receptors [32]. They can alleviate SARS-CoV-2 cytokine storm and injury to the organs. The use of DPP4 inhibitors in patients with SARS-CoV-2 infection was associated with improvement of glucose levels in diabetic patients and clinical improvement and reduction of inflammatory markers in diabetic and non-diabetic patients [57,63,64].
5. Conclusion
Based on the collected evidence, the effect of SARS-CoV-2 infection on the incidence of new onset T1D is controversial. However, COVID-19 increases the incidence and severity of DKA in T1D patients. Antivirals seems to be helpful but not completely protective against SARS-CoV-2-induced tissue injuries. An alternative therapeutic approach includes targeting SARS-CoV-2 receptor, blocking virus entry and alleviating inflammation, especially by combining medications with different beneficial characteristics, to tackle SARS-CoV-2 infection and associated complications. Flooring the path for future clinical trials that investigate the protective role of this alternative approach would be reasonable, as it is shown that combination of spironolactone and sitagliptin could reduce hospitalization rate and duration of disease [65].
Authors’ contributions
Kebria Kashfi and Narges Anbardar reviewed the literature and helped with writing. Kamyar Asadipooya reviewed the literature and wrote the manuscript. Artin Asadipooya helped with writing and editions.
Source of funding
There is no funding support for this project.
Data Availability
The original data of this study are listed in References. There is no other generated data for this project.
Acknowledgments
nothing
Disclosures
The authors have declared that no conflict of interest exists.
Correspondence
Kamyar Asadipooya, MD, Department of Medicine, Division of Endocrinology, Diabetes, and Metabolism, Barnstable Brown Diabetes and Obesity Center, University of Kentucky, Lexington, KY 40504, USA. Email: kas224@uky.edu
Abbreviations
ACE2, angiotensin-converting enzyme 2; ADAM17, Disintegrin and metalloproteinase domain-containing protein 17; COVID-19, coronavirus disease 2019; DKA, diabetic ketoacidosis; DPP-4, dipeptidyl peptidase-4; IRR, incidence rate ratios; IRT1D, incidence rate of type 1 diabetes; NT1D, New Onset Type 1 Diabetes; OR, Odds ratio; RR, Relative Risk; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2; TMPRSS2, transmembrane protease serine 2; T1D, Type 1 Diabetes.
References
- Rabaan, A.A.; Smajlović, S.; Tombuloglu, H.; Ćordić, S.; Hajdarević, A.; Kudić, N.; Al Mutai, A.; Turkistani, S.A.; Al-Ahmed, S.H.; Al-Zaki, N.A.; Al Marshood, M.J.; Alfaraj, A.H.; Alhumaid, S.; Al-Suhaimi, E. SARS-CoV-2 infection and multi-organ system damage: A review. Biomol Biomed. 2023, 23, 37–52. [Google Scholar] [CrossRef]
- Clarke, S.A.; Abbara, A.; Dhillo, W.S. Impact of COVID-19 on the Endocrine System: A Mini-review. Endocrinology. 2022, 163. [Google Scholar]
- Banday, M.Z.; Sameer, A.S.; Nissar, S. Pathophysiology of diabetes: An overview. Avicenna J Med. 2020, 10, 174–188. [Google Scholar]
- Kim, S.H.; Arora, I.; Hsia, D.S.; Knowler, W.C.; LeBlanc, E.; Mylonakis, E.; Pratley, R.; Pittas, A.G. New-Onset Diabetes after COVID-19. The Journal of clinical endocrinology and metabolism. 2023. [Google Scholar]
- Wang, Y.; Guo, H.; Wang, G.; Zhai, J.; Du, B. COVID-19 as a Trigger for type 1 diabetes. The Journal of clinical endocrinology and metabolism 2023. [Google Scholar]
- Muniangi-Muhitu, H.; Akalestou, E.; Salem, V.; Misra, S.; Oliver, N.S.; Rutter, G.A. Covid-19 and Diabetes: A Complex Bidirectional Relationship. Front Endocrinol (Lausanne). 2020, 11, 582936. [Google Scholar]
- Birkebaek, N.H.; Kamrath, C.; Grimsmann, J.M.; Aakesson, K.; Cherubini, V.; Dovc, K.; de Beaufort, C.; Alonso, G.T.; Gregory, J.W.; White, M.; Skrivarhaug, T.; Sumnik, Z.; Jefferies, C.; Hörtenhuber, T.; Haynes, A.; De Bock, M.; Svensson, J.; Warner, J.T.; Gani, O.; Gesuita, R.; Schiaffini, R.; Hanas, R.; Rewers, A.; Eckert, A.J.; Holl, R.W.; Cinek, O. Impact of the COVID-19 pandemic on long-term trends in the prevalence of diabetic ketoacidosis at diagnosis of paediatric type 1 diabetes: an international multicentre study based on data from 13 national diabetes registries. Lancet Diabetes Endocrinol. 2022, 10, 786–794. [Google Scholar]
- Lawrence, C.; Seckold, R.; Smart, C.; King, B.R.; Howley, P.; Feltrin, R.; Smith, T.A.; Roy, R.; Lopez, P. Increased paediatric presentations of severe diabetic ketoacidosis in an Australian tertiary centre during the COVID-19 pandemic. Diabet Med. 2021, 38, e14417. [Google Scholar]
- Li J, Wang X, Chen J, Zuo X, Zhang H, Deng A. COVID-19 infection may cause ketosis and ketoacidosis. Diabetes Obes Metab. 2020, 22, 1935–1941. [Google Scholar] [CrossRef]
- Kamrath, C.; Rosenbauer, J.; Tittel, S.R.; Warncke, K.; Hirtz, R.; Denzer, C.; Dost, A.; Neu, A.; Pacaud, D.; Holl, R.W. Frequency of Autoantibody-Negative Type 1 Diabetes in Children, Adolescents, and Young Adults During the First Wave of the COVID-19 Pandemic in Germany. Diabetes Care. 2021, 44, 1540–1546. [Google Scholar]
- Kamrath, C.; Rosenbauer, J.; Eckert, A.J.; Pappa, A.; Reschke, F.; Rohrer, T.R.; Mönkemöller, K.; Wurm, M.; Hake, K.; Raile, K.; Holl, R.W. Incidence of COVID-19 and Risk of Diabetic Ketoacidosis in New-Onset Type 1 Diabetes. Pediatrics. 2021, 148. [Google Scholar]
- Mastromauro, C.; Blasetti, A.; Primavera, M.; Ceglie, L.; Mohn, A.; Chiarelli, F.; Giannini, C. Peculiar characteristics of new-onset Type 1 Diabetes during COVID-19 pandemic. Ital J Pediatr. 2022, 48, 26. [Google Scholar]
- Zubkiewicz-Kucharska, A.; Seifert, M.; Stępkowski, M.; Noczyńska, A. Diagnosis of type 1 diabetes during the SARS-CoV-2 pandemic: Does lockdown affect the incidence and clinical status of patients? Adv Clin Exp Med. 2021, 30, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev. 2015, 4, 1. [Google Scholar]
- Cariou, B.; Hadjadj, S.; Wargny, M.; Pichelin, M.; Al-Salameh, A.; Allix, I.; Amadou, C.; Arnault, G.; Baudoux, F.; Bauduceau, B.; Borot, S.; Bourgeon-Ghittori, M.; Bourron, O.; Boutoille, D.; Cazenave-Roblot, F.; Chaumeil, C.; Cosson, E.; Coudol, S.; Darmon, P.; Disse, E.; Ducet-Boiffard, A.; Gaborit, B.; Joubert, M.; Kerlan, V.; Laviolle, B.; Marchand, L.; Meyer, L.; Potier, L.; Prevost, G.; Riveline, J.P.; Robert, R.; Saulnier, P.J.; Sultan, A.; Thébaut, J.F.; Thivolet, C.; Tramunt, B.; Vatier, C.; Roussel, R.; Gautier, J.F.; Gourdy, P. Phenotypic characteristics and prognosis of inpatients with COVID-19 and diabetes: the CORONADO study. Diabetologia. 2020, 63, 1500–1515. [Google Scholar] [PubMed]
- Kamrath, C.; Rosenbauer, J.; Eckert, A.J.; Siedler, K.; Bartelt, H.; Klose, D.; Sindichakis, M.; Herrlinger, S.; Lahn, V.; Holl, R.W. Incidence of Type 1 Diabetes in Children and Adolescents During the COVID-19 Pandemic in Germany: Results From the DPV Registry. Diabetes Care. 2022, 45, 1762–1771. [Google Scholar]
- Jacob, R.; Weiser, G.; Krupik, D.; Takagi, D.; Peled, S.; Pines, N.; Hashavya, S.; Gur-Soferman, H.; Gamsu, S.; Kaplan, O.; Maimon, M.; Oren, S.; Padeh, G.; Shavit, I. Diabetic Ketoacidosis at Emergency Department Presentation During the First Months of the SARS-CoV-2 Pandemic in Israel: A Multicenter Cross-Sectional Study. Diabetes Ther. 2021, 12, 1569–1574. [Google Scholar] [PubMed]
- Dżygało, K.; Nowaczyk, J.; Szwilling, A.; Kowalska, A. Increased frequency of severe diabetic ketoacidosis at type 1 diabetes onset among children during COVID-19 pandemic lockdown: an observational cohort study. Pediatr Endocrinol Diabetes Metab. 2020, 26, 167–175. [Google Scholar] [CrossRef]
- Ho, J.; Rosolowsky, E.; Pacaud, D.; Huang, C.; Lemay, J.A.; Brockman, N.; Rath, M.; Doulla, M. Diabetic ketoacidosis at type 1 diabetes diagnosis in children during the COVID-19 pandemic. Pediatr Diabetes. 2021, 22, 552–557. [Google Scholar]
- Pietrzak, I.; Michalak, A.; Seget, S.; Bednarska, M.; Beń-Skowronek, I.; Bossowski, A.; Chobot, A.; Dżygało, K.; Głowińska-Olszewska, B.; Górnicka, M.; Horodnicka-Józwa, A.; Jakubek-Kipa, K.; Jarosz-Chobot, P.; Marcinkiewicz, K.; Mazur, A.; Myśliwiec, M.; Nazim, J.; Niechciał, E.; Noczyńska, A.; Rusak, E.; Seifert, M.; Skotarczyk-Kowalska, E.; Skowronek, A.; Szypowska, A.; Wais, P.; Walczak, M.; Wołoszyn-Durkiewicz, A.; Wysocka-Mincewicz, M.; Zubkiewicz-Kucharska, A.; Szadkowska, A. Diabetic ketoacidosis incidence among children with new-onset type 1 diabetes in Poland and its association with COVID-19 outbreak-Two-year cross-sectional national observation by PolPeDiab Study Group. Pediatr Diabetes. 2022, 23, 944–955. [Google Scholar]
- Boboc, A.A.; Novac, C.N.; Ilie, M.T.; Ieșanu, M.I.; Galoș, F.; Bălgrădean, M.; Berghea, E.C.; Ionescu, M.D. The Impact of SARS-CoV-2 Pandemic on the New Cases of T1DM in Children. A Single-Centre Cohort Study. J Pers Med 2021, 11. [Google Scholar]
- Alaqeel, A.; Aljuraibah, F.; Alsuhaibani, M.; Huneif, M.; Alsaheel, A.; Dubayee, M.A.; Alsaedi, A.; Bakkar, A.; Alnahari, A.; Taha, A.; Alharbi, K.; Alanazi, Y.; Almadhi, S.; Khalifah, R.A. The Impact of COVID-19 Pandemic Lockdown on the Incidence of New-Onset Type 1 Diabetes and Ketoacidosis Among Saudi Children. Front Endocrinol (Lausanne). 2021, 12, 669302. [Google Scholar]
- Dilek, S.; Gürbüz, F.; Turan, İ.; Celiloğlu, C.; Yüksel, B. Changes in the presentation of newly diagnosed type 1 diabetes in children during the COVID-19 pandemic in a tertiary center in Southern Turkey. J Pediatr Endocrinol Metab. 2021, 34, 1303–1309. [Google Scholar] [PubMed]
- O'Malley, G.; Ebekozien, O.; Desimone, M.; Pinnaro, C.T.; Roberts, A.; Polsky, S.; Noor, N.; Aleppo, G.; Basina, M.; Tansey, M.; Steenkamp, D.; Vendrame, F.; Lorincz, I.; Mathias, P.; Agarwal, S.; Golden, L.; Hirsch, I.B.; Levy, C.J. COVID-19 Hospitalization in Adults with Type 1 Diabetes: Results from the T1D Exchange Multicenter Surveillance Study. The Journal of clinical endocrinology and metabolism. 2021, 106, e936–e942. [Google Scholar] [CrossRef]
- Bogale, K.T.; Urban, V.; Schaefer, E.; Bangalore Krishna, K. The Impact of COVID-19 Pandemic on Prevalence of Diabetic Ketoacidosis at Diagnosis of Type 1 Diabetes: A Single-Centre Study in Central Pennsylvania. Endocrinol Diabetes Metab. 2021, 4, e00235. [Google Scholar] [CrossRef]
- Danne, T.; Lanzinger, S.; de Bock, M.; Rhodes, E.T.; Alonso, G.T.; Barat, P.; Elhenawy, Y.; Kershaw, M.; Saboo, B.; Scharf Pinto, M.; Chobot, A.; Dovc, K. A Worldwide Perspective on COVID-19 and Diabetes Management in 22,820 Children from the SWEET Project: Diabetic Ketoacidosis Rates Increase and Glycemic Control Is Maintained. Diabetes Technol Ther. 2021, 23, 632–641. [Google Scholar]
- Mariet, A.S.; Petit, J.M.; Benzenine, E.; Quantin, C.; Bouillet, B. Incidence of new-onset type 1 diabetes during Covid-19 pandemic: A French nationwide population-based study. Diabetes Metab. 2023, 49, 101425. [Google Scholar]
- Trieu, C.; Sunil, B.; Ashraf, A.P.; Cooper, J.; Yarbrough, A.; Pinninti, S.; Boppana, S. SARS-CoV-2 infection in hospitalized children with type 1 and type 2 diabetes. J Clin Transl Endocrinol. 2021, 26, 100271. [Google Scholar]
- Herczeg, V.; Luczay, A.; Ténai, N.; Czine, G.; Tóth-Heyn, P. Anti-SARS-CoV-2 Seropositivity Among Children With Newly Diagnosed Type 1 Diabetes Mellitus: A Case-Control Study. Indian Pediatr. 2022, 59, 809–810. [Google Scholar]
- Ata, A.; Jalilova, A.; Kırkgöz, T.; Işıklar, H.; Demir, G.; Altınok, Y.A.; Özkan, B.; Zeytinlioğlu, A.; Darcan, Ş.; Özen, S.; Gökşen, D. Does COVID-19 predispose patients to type 1 diabetes mellitus? Clin Pediatr Endocrinol. 2022, 31, 33–37. [Google Scholar] [CrossRef]
- Jackson, C.B.; Farzan, M.; Chen, B.; Choe, H. Mechanisms of SARS-CoV-2 entry into cells. Nat Rev Mol Cell Biol. 2022, 23, 3–20. [Google Scholar]
- Bakhtiari, M.; Asadipooya, K. Metainflammation in COVID-19. Endocr Metab Immune Disord Drug Targets. 2022.
- Brojakowska, A.; Narula, J.; Shimony, R.; Bander, J. Clinical Implications of SARS-CoV-2 Interaction With Renin Angiotensin System: JACC Review Topic of the Week. J Am Coll Cardiol. 2020, 75, 3085–3095. [Google Scholar] [CrossRef] [PubMed]
- Hikmet, F.; Méar, L.; Edvinsson, Å.; Micke, P.; Uhlén, M.; Lindskog, C. The protein expression profile of ACE2 in human tissues. Mol Syst Biol. 2020, 16, e9610. [Google Scholar] [CrossRef]
- Liu, F.; Long, X.; Zhang, B.; Zhang, W.; Chen, X.; Zhang, Z. ACE2 Expression in Pancreas May Cause Pancreatic Damage After SARS-CoV-2 Infection. Clin Gastroenterol Hepatol. 2020, 18, 2128–2130e2122. [Google Scholar] [CrossRef]
- Govender, N.; Khaliq, O.P.; Moodley, J.; Naicker, T. Insulin resistance in COVID-19 and diabetes. Prim Care Diabetes. 2021, 15, 629–634. [Google Scholar]
- Oriot, P.; Hermans, M.P. Euglycemic diabetic ketoacidosis in a patient with type 1 diabetes and SARS-CoV-2 pneumonia: case-report and review of the literature. Acta Clin Belg. 2022, 77, 113–117. [Google Scholar] [CrossRef] [PubMed]
- Gorthi RS, Kamel G, Dhindsa S, Nayak RP. COVID-19 Presenting With Diabetic Ketoacidosis: A Case Series. AACE Clin Case Rep. 2021, 7, 6–9. [Google Scholar] [CrossRef]
- Benyakhlef, S.; Abdellaoui, W.; Tahri, A.; Rouf, S.; Latrech, H. Diabetic Ketoacidosis at Onset of Pediatric Type-1 Diabetes Triggered by Covid-19: An Original Case Report. Cureus. 2021, 13, e13958. [Google Scholar] [CrossRef]
- Nielsen-Saines, K.; Li, E.; Olivera, A.M.; Martin-Blais, R.; Bulut, Y. Case Report: Insulin-Dependent Diabetes Mellitus and Diabetic Keto-Acidosis in a Child With COVID-19. Front Pediatr. 2021, 9, 628810. [Google Scholar] [CrossRef]
- Soliman, A.T.; Al-Amri, M.; Alleethy, K.; Alaaraj, N.; Hamed, N.; De Sanctis, V. Newly-onset type 1 diabetes mellitus precipitated by COVID-19 in an 8-month-old infant. Acta Biomed. 2020, 91, ahead of print. [Google Scholar]
- Albuali, W.H.; AlGhamdi, N.A. Diabetic ketoacidosis precipitated by atypical coronavirus disease in a newly diagnosed diabetic girl. J Taibah Univ Med Sci. 2021, 16, 628–631. [Google Scholar] [CrossRef] [PubMed]
- Aly, H.H.; Fouda, E.M.; Kotby, A.A.; Magdy, S.M.; Rezk, A.R.; Nasef, M.W.A. COVID-19-Related Multisystem Inflammatory Syndrome in Children Presenting With New-Onset Type 1 Diabetes in Severe Ketoacidosis: A Case Series. Diabetes Care. 2022, 45, 983–989. [Google Scholar] [CrossRef] [PubMed]
- Parappil, P.; Ghimire, S.; Saxena, A.; Mukherjee, S.; John, B.M.; Sondhi, V.; Sengupta, P.; Acharya, S. New-onset diabetic ketoacidosis with purpura fulminans in a child with COVID-19-related multisystem inflammatory syndrome. Infect Dis (Lond). 2022, 54, 522–528. [Google Scholar] [CrossRef] [PubMed]
- Genç, S.; Evren, B.; Bozbay, A.; Aydın, E.; Genç, Ö.; Şahin, I. COULD COVID-19 TRIGGER TYPE 1 DIABETES? PRESENTATION OF COVID-19 CASE PRESENTED WITH DIABETIC KETOACIDOSIS. Acta Endocrinol (Buchar). 2021, 17, 532–536. [Google Scholar] [CrossRef]
- Halioti, A.; Kitinou, M.; Chalioti, V.M.; Chaliotis, G. SARS-CoV-2 Unmasks Type 1 Diabetes Mellitus With an Episode of Diabetic Ketoacidosis. J Med Cases. 2022, 13, 432–437. [Google Scholar] [CrossRef]
- Taşkaldıran, I.; Nar, A. A case of new-onset autoimmune type 1 diabetes mellitus following COVID-19 infection. Endocr Metab Immune Disord Drug Targets. 2023. [CrossRef]
- Ganakumar, V.; Jethwani, P.; Roy, A.; Shukla, R.; Mittal, M.; Garg, M.K. Diabetic ketoacidosis (DKA) in type 1 diabetes mellitus (T1DM) temporally related to COVID-19 vaccination. Diabetes & metabolic syndrome. 2022, 16, 102371. [Google Scholar]
- Lin, R.; Lin, Y.W.; Chen, M.H. Fulminant Type 1 Diabetes Mellitus after SARS-CoV-2 Vaccination: A Case Report. Vaccines (Basel). 2022, 10. [Google Scholar] [CrossRef]
- Edwin, H.V.; Antony, C.S. An update on COVID-19: SARS-CoV-2 variants, antiviral drugs, and vaccines. Heliyon. 2023.
- 51. von Delft A, Hall MD, Kwong AD, Purcell LA, Saikatendu KS, Schmitz U, Tallarico JA, Lee AA. Accelerating antiviral drug discovery: lessons from COVID-19. Nat Rev Drug Discov 2023, 1–19.
- Brevini, T.; Maes, M.; Webb, G.J.; John, B.V.; Fuchs, C.D.; Buescher, G.; Wang, L.; Griffiths, C.; Brown, M.L.; Scott, W.E.; 3rd Pereyra-Gerber, P.; Gelson, W.T.H.; Brown, S.; Dillon, S.; Muraro, D.; Sharp, J.; Neary, M.; Box, H.; Tatham, L.; Stewart, J.; Curley, P.; Pertinez, H.; Forrest, S.; Mlcochova, P.; Varankar, S.S.; Darvish-Damavandi, M.; Mulcahy, V.L.; Kuc, R.E.; Williams, T.L.; Heslop, J.A.; Rossetti, D.; Tysoe, O.C.; Galanakis, V.; Vila-Gonzalez, M.; Crozier, T.W.M.; Bargehr, J.; Sinha, S.; Upponi, S.S.; Fear, C.; Swift, L.; Saeb-Parsy, K.; Davies, S.E.; Wester, A.; Hagström, H.; Melum, E.; Clements, D.; Humphreys, P.; Herriott, J.; Kijak, E.; Cox, H.; Bramwell, C.; Valentijn, A.; Illingworth, C.J.R.; Dahman, B.; Bastaich, D.R.; Ferreira, R.D.; Marjot, T.; Barnes, E.; Moon, A.M.; Barritt ASt Gupta, R.K.; Baker, S.; Davenport, A.P.; Corbett, G.; Gorgoulis, V.G.; Buczacki, S.J.A.; Lee, J.H.; Matheson, N.J.; Trauner, M.; Fisher, A.J.; Gibbs, P.; Butler, A.J.; Watson, C.J.E.; Mells, G.F.; Dougan, G.; Owen, A.; Lohse, A.W.; Vallier, L.; Sampaziotis, F. FXR inhibition may protect from SARS-CoV-2 infection by reducing ACE2. Nature 2022. [Google Scholar] [CrossRef]
- John, B.V.; Bastaich, D.; Webb, G.; Brevini, T.; Moon, A.; Ferreira, R.D.; Chin, A.M.; Kaplan, D.E.; Taddei, T.H.; Serper, M.; Mahmud, N.; Deng, Y.; Chao, H.H.; Sampaziotis, F.; Dahman, B. Ursodeoxycholic acid is associated with a reduction in SARS-CoV-2 infection and reduced severity of COVID-19 in patients with cirrhosis. J Intern Med. 2023, 293, 636–647. [Google Scholar] [CrossRef] [PubMed]
- Leach, D.A.; Mohr, A.; Giotis, E.S.; Cil, E.; Isac, A.M.; Yates, L.L.; Barclay, W.S.; Zwacka, R.M.; Bevan, C.L.; Brooke, G.N. The antiandrogen enzalutamide downregulates TMPRSS2 and reduces cellular entry of SARS-CoV-2 in human lung cells. Nat Commun. 2021, 12, 4068. [Google Scholar] [CrossRef]
- Cheema, H.A.; Rehman, A.U.; Elrashedy, A.A.; Mohsin, A.; Shahid, A.; Ehsan, M.; Ayyan, M.; Ismail, H.; Almas, T. Antiandrogens for the treatment of COVID-19 patients: A meta-analysis of randomized controlled trials. J Med Virol. 2023, 95, e28740. [Google Scholar] [CrossRef]
- Fels, B.; Acharya, S.; Vahldieck, C.; Graf, T.; Käding, N.; Rupp, J.; Kusche-Vihrog, K. Mineralocorticoid receptor-antagonism prevents COVID-19-dependent glycocalyx damage. Pflugers Arch. 2022, 1–8. [Google Scholar] [CrossRef]
- Abbasi, F.; Adatorwovor, R.; Davarpanah, M.A.; Mansoori, Y.; Hajiani, M.; Azodi, F.; Sefidbakht, S.; Davoudi, S.; Rezaei, F.; Mohammadmoradi, S.; Asadipooya, K. A Randomized Trial of Sitagliptin and Spironolactone With Combination Therapy in Hospitalized Adults With COVID-19. J Endocr Soc. 2022, 6, bvac017. [Google Scholar] [CrossRef]
- Zhang, J.; Dong, J.; Martin, M.; He, M.; Gongol, B.; Marin, T.L.; Chen, L.; Shi, X.; Yin, Y.; Shang, F.; Wu, Y.; Huang, H.Y.; Zhang, J.; Zhang, Y.; Kang, J.; Moya, E.A.; Huang, H.D.; Powell, F.L.; Chen, Z.; Thistlethwaite, P.A.; Yuan, Z.Y.; Shyy, J.Y. AMP-activated Protein Kinase Phosphorylation of Angiotensin-Converting Enzyme 2 in Endothelium Mitigates Pulmonary Hypertension. Am J Respir Crit Care Med. 2018, 198, 509–520. [Google Scholar] [CrossRef]
- Sharma, S.; Ray, A.; Sadasivam, B. Metformin in COVID-19: A possible role beyond diabetes. Diabetes Res Clin Pract. 2020, 164, 108183. [Google Scholar] [CrossRef]
- Malhotra, A.; Hepokoski, M.; McCowen, K.C.; J, Y.J.S. ACE2, Metformin, and COVID-19. iScience. 2020, 23, 101425. [Google Scholar] [CrossRef]
- Bramante, C.T.; Huling, J.D.; Tignanelli, C.J.; Buse, J.B.; Liebovitz, D.M.; Nicklas, J.M.; Cohen, K.; Puskarich, M.A.; Belani, H.K.; Proper, J.L.; Siegel, L.K.; Klatt, N.R.; Odde, D.J.; Luke, D.G.; Anderson, B.; Karger, A.B.; Ingraham, N.E.; Hartman, K.M.; Rao, V.; Hagen, A.A.; Patel, B.; Fenno, S.L.; Avula, N.; Reddy, N.V.; Erickson, S.M.; Lindberg, S.; Fricton, R.; Lee, S.; Zaman, A.; Saveraid, H.G.; Tordsen, W.J.; Pullen, M.F.; Biros, M.; Sherwood, N.E.; Thompson, J.L.; Boulware, D.R.; Murray, T.A. Randomized Trial of Metformin, Ivermectin, and Fluvoxamine for Covid-19. The New England journal of medicine. 2022, 387, 599–610. [Google Scholar] [CrossRef]
- Bramante, C.T.; Buse, J.B.; Liebovitz, D.M.; Nicklas, J.M.; Puskarich, M.A.; Cohen, K.; Belani, H.K.; Anderson, B.J.; Huling, J.D.; Tignanelli, C.J.; Thompson, J.L.; Pullen, M.; Wirtz, E.L.; Siegel, L.K.; Proper, J.L.; Odde, D.J.; Klatt, N.R.; Sherwood, N.E.; Lindberg, S.M.; Karger, A.B.; Beckman, K.B.; Erickson, S.M.; Fenno, S.L.; Hartman, K.M.; Rose, M.R.; Mehta, T.; Patel, B.; Griffiths, G.; Bhat, N.S.; Murray, T.A.; Boulware, D.R. Outpatient treatment of COVID-19 and incidence of post-COVID-19 condition over 10 months (COVID-OUT): a multicentre, randomised, quadruple-blind, parallel-group, phase 3 trial. Lancet Infect Dis. 2023. [CrossRef] [PubMed]
- Nag, S.; Mandal, S.; Mukherjee, O.; Mukherjee, S.; Kundu, R. DPP-4 Inhibitors as a savior for COVID-19 patients with diabetes. Future Virol 2023. [Google Scholar] [CrossRef]
- Al-Kuraishy, H.M.; Al-Gareeb, A.I.; Qusty, N.; Alexiou, A.; Batiha, G.E. Impact of Sitagliptin on Non-diabetic Covid-19 Patients. Current molecular pharmacology. 2022, 15, 683–692. [Google Scholar] [PubMed]
- Davarpanah, M.A.; Adatorwovor, R.; Mansoori, Y.; Ramsheh, F.S.R.; Parsa, A.; Hajiani, M.; Faramarzi, H.; Kavuluru, R.; Asadipooya, K. Combination of spironolactone and sitagliptin improves clinical outcomes of outpatients with COVID-19: a prospective cohort study. J Endocrinol Invest. 2023. [CrossRef] [PubMed]
Figure 1.
Flow diagram of the screening process of literature review.
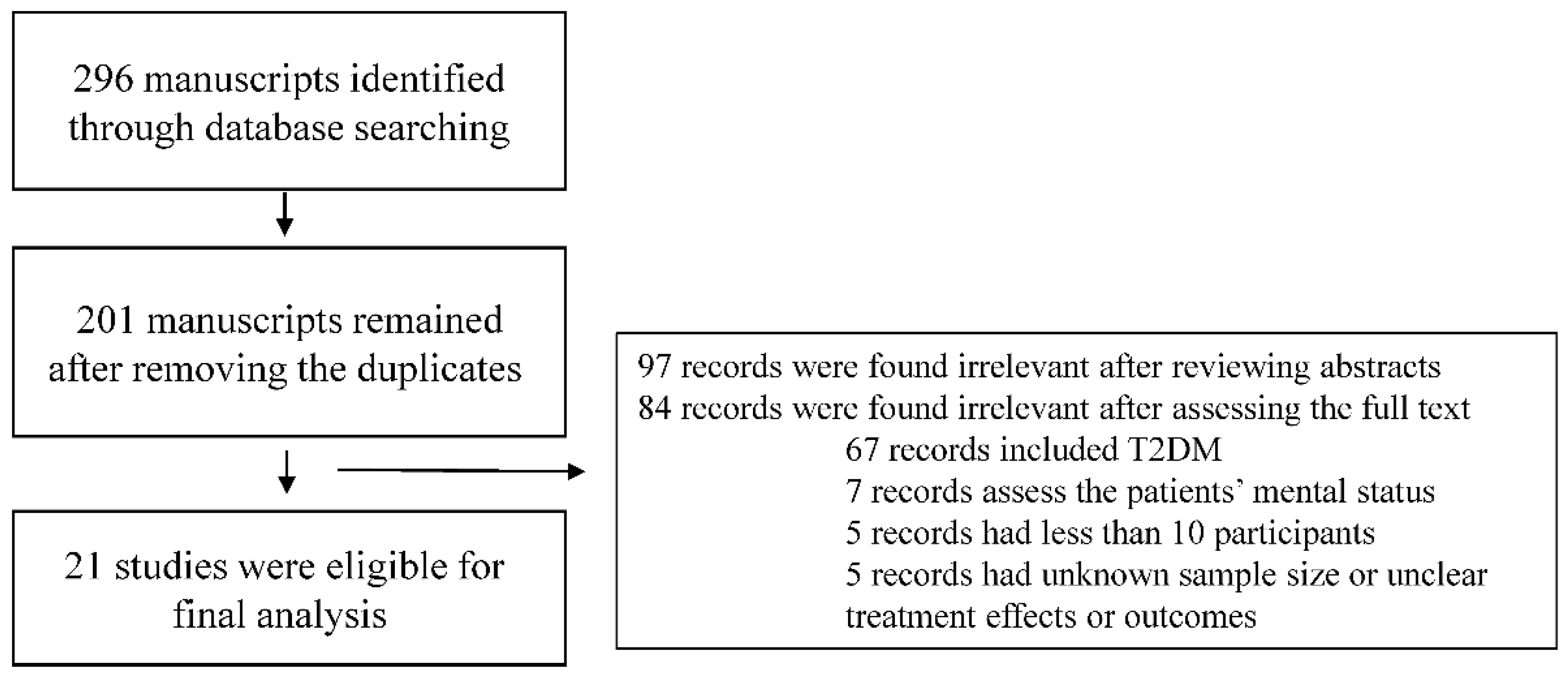
Figure 2.
Illustrating the cascade of events triggered by SARS-CoV-2 infection that reduces insulin production, increases insulin resistance and causes hyperglycemia. This in turn lead to the changes that can increase SARS-CoV-2 organ damages.
Figure 2.
Illustrating the cascade of events triggered by SARS-CoV-2 infection that reduces insulin production, increases insulin resistance and causes hyperglycemia. This in turn lead to the changes that can increase SARS-CoV-2 organ damages.
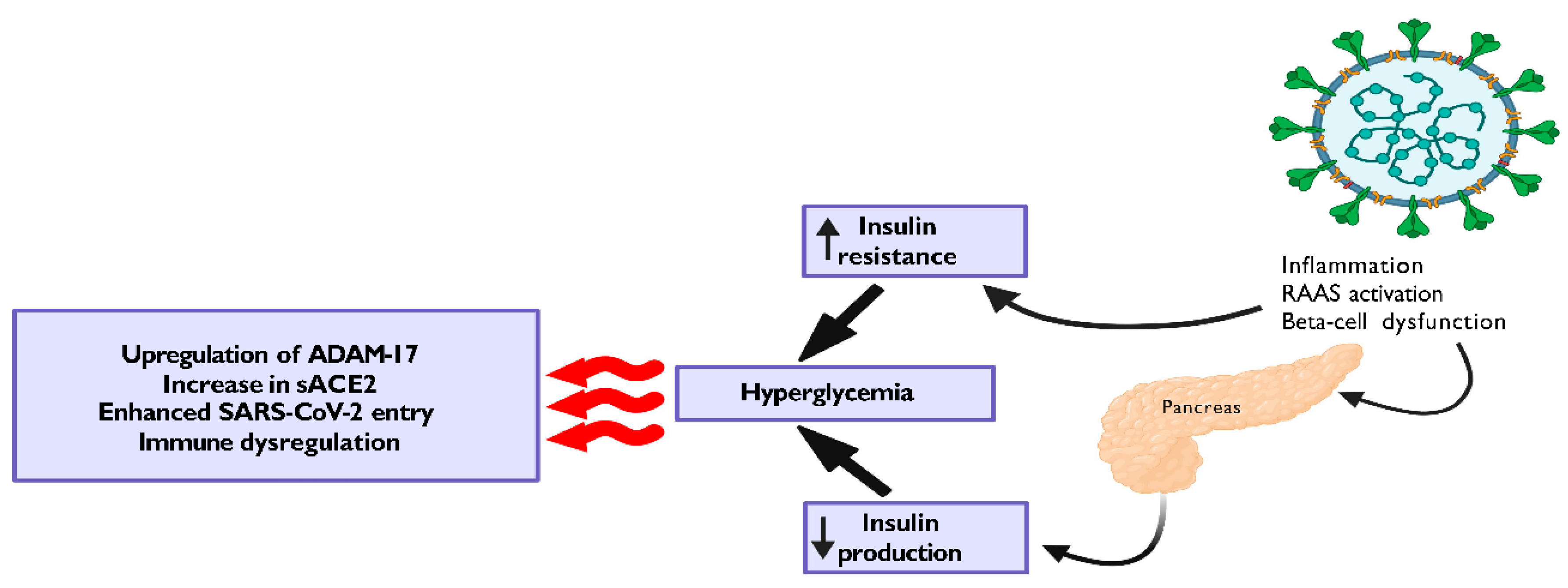

Table 1.
Outcomes and population of included studies with T1D and COVID-19 listed the countries in alphabetical order.
Table 1.
Outcomes and population of included studies with T1D and COVID-19 listed the countries in alphabetical order.
| Author, Journal, Year, Country and time of study | Study design and population | Sample size | Age | Sex (Male number and percentage) | Death, DKA or New Onset Type 1 Diabetes (NT1D) | Comments | |
| Niels H Birkebaek, Lancet Diabetes Endocrinol. 2022 Nov, Australia, Austria, Czechia, Denmark, Germany, Italy, Luxembourg, New Zealand, Norway, Slovenia, Sweden, USA [Colorado], and Wales [7] | International multicenter study, from 13 national diabetes registries, children and adolescents diagnosed with T1D (104290 children and adolescents) | 8209 in 2020 | 9.9 | 4521 (55%) | 39.4% in 2020 (DKA at T1D Diagnosis) |
There was an exacerbation of DKA prevalence in T1D patients during COVID-19 pandemic | |
| 8853 in 2021 | 9.5 | 4941 (55.8%) | 38.9% in 2021 (DKA at T1D Diagnosis) |
||||
| 87228 in 2006-2019 | 9.5 | 47066 (54%) | 27.3% (23775) DKA at T1D Diagnosis | ||||
| C. Lawrence, Diabet Med. 2021 Jan, Australia [8] | Retrospective cohort study, children <18 with the initial diagnosis of T1D | 11 (Mar-May 2020) | 8 | 27% | 73% DKA 45% severe DKA |
11 NT1D | A significant increase in the severe DKA at presentation of new-onset T1D during the COVID-19 |
| 42 (Mar-May 2015-2019) | 7.9-10.2 | 33-63% | 26% DKA 5% severe DKA |
9 (6-10) NT1D | |||
| Juyi Li, Diabetes Obes Metab. 2020 Oct, China [9] | Retrospective cohort study, hospitalized patients with COVID-19 | 658 | 57.3 | 297 (45.14%) | 64 (9.7%) death 3 (0.005%) DKA |
COVID-19 infection caused ketosis or ketoacidosis COVID-19 induced diabetic ketoacidosis in diabetic patients Ketosis increased the length of hospital stay and mortality |
|
| Cariou, et al; the CORONADO study. Diabetologia 2020, French [15] | Multicenter observational study, diabetic patients hospitalized for COVID-19 | 1317 |
69.8 | 855 (64.9%) | 10.6% death | 41 (3.1%) NT1D | No increased death in T1D No death in type 1 diabetes patients younger than 65 years |
| 1166 T2D (88.5%) |
1.00 OR for death | ||||||
| 39 T1D (3%) | 0.44 OR for death |
||||||
| Anne-Sophie Mariet, et al. Diabetes Metab. 2023 May, French [27] | Nationwide retrospective cohort study in three periods: week 2 of 2019 to week 12 of 2020, weeks 12−19 of 2020, week 19 of 2020 to week 52 of 2021 (after lockdown) | 7,995,449 |
1 - 35 | T1D hospitalizations: 6114 in 2019 6051 in2020 6593 in 2021 |
No significant increase in the hospitalizations rate for new-onset T1D during the COVID-19 pandemic in 2020 and 2021 The severity of T1D at diagnosis was not exaggerated during COVID-19 pandemic |
||
| Clemens Kamrath, Diabetes Care. 2021 Jul. Germany [10] | Multicenter cohort study, German Diabetes Registry, new onset T1D between March 1 and June 30 | 1,072 in 2020 |
10.0 | 430 (58.7%) | 6.6% (5.1-8.4) NT1D 7.2% (6.5-8.0) NT1D |
Not significant increase in new onset autoantibody-negative type 1 diabetes in children, adolescents, and young adults during the pandemic No increased susceptibility to DKA in autoantibody-negative type 1 diabetes before or during the pandemic |
|
| 8,349 (2011 – 2019) | 10.1 | 3033 (53.9%) | |||||
| Clemens Kamrath, Pediatrics. 2021 Sep. Germany [11] | Multicenter cohort from the German Diabetes Prospective Follow-up Registry | 3238 new onset T1D in 2020 | 9.8 | 1799 (55.6%) | DKA cases 1094 (33.8%) Increase in incidence of COVID-19 or death was associated with RR of DKA of 1.40 (95% confidence interval, 1.10–1.77; P = 0.006) and 1.23 (1.14–1.32; P < .001), respectively |
Significant increase in the risks of DKA and severe DKA in children with new-onset T1D during the coronavirus pandemic in Germany Ketoacidosis incidence in 2020 ranged from 22.6% in January to 43.3% in August (expected 20.1% in January to 25.3% in October) Ketoacidosis observed in 2020 in children with new-onset T1D vs expected rates (2000 to 2019) |
|
| Clemens Kamrath, Diabetes Care. 2022 Aug. Germany [16] | Multicenter Diabetes Prospective Study, German Registry, T1D incidence in children and adolescents 1/1/2020 – 6/30/2021 |
5,162 in 2020/2021 |
9.7 | (55.8 %) | 24.4% (23.6–25.2) NT1D incidence 2020/21 21.2% (20.5–21.9) NT1D expected incidence 2011 to 2019 IRR 1.15 [1.10–1.20]; P < 0.001 |
Incidence rate ratio (IRR) 1.15 (95% CI 1.10-1.20; P < 0.001) IRR in female, 1.14 (95% CI 1.07–1.21, P < 0.001) and male, 1.16 (95% CI 1.10–1.23, P < 0.001) Significant increase IRR in children aged < 6 years (IRR 1.23, 95% CI 1.13–1.33, P < 0.001) and 6–11 years (IRR 1.18, 95% CI 1.11–1.26, P < 0.001), but not in adolescents aged 12–17 years (IRR 1.06, 95% CI 0.98–1.13, P = 0.13) |
|
| 2,740 in 2018 |
9.8 | (55.0 %) | |||||
| 2,903 in 2019 |
9.7 | (54.9 %) | |||||
| Ron Jacob, Diabetes Ther. 2021 May, Israel [17] | A retrospective cross-sectional study, 11 Israeli pediatric Eds diabetes-related presentation |
150 T1D 48,176 visits (2020) |
12 | DKA in established T1D 2020 vs 2019 (59.3% vs 41.9%, P < 0.043) DKA in new onset T1D 2020 vs 2019 (53.4% vs 38.7%, p = 0.063) Not significant increase in NT1D |
Significant increase DKA rate in established T1D Non-statistically significant increase DKA rate in new onset T1D No difference in severe DKA (established T1D [15.6% vs 8.1%; P = 0.184], and newly diagnosed T1D [18.6% vs 17.5%; P = 0.858]) |
||
| 154 T1D 77,477 visits (2019) |
12 | ||||||
| Concetta Mastromauro, Ital J Pediatr. 2022 Feb, Italy [12] | Retrospective, Pediatric and Adolescent T1D Group 1/2015 – 2/2020 Group 2 3/2020 – 4/2021 |
172 new onset T1D 132 group 1 40 group 2 |
9.1 9.3 8.4 |
101 (58.7%) 81 (61.3%) 420 (50%) |
DKA (36% vs 55%, P=0.03) Severe DKA (8.4% vs 22.5%, P=0.01) |
Significant increase in DKA and severe DKA during the pandemic | |
| Katarzyna Dżygało, Pediatr Endocrinol Diabetes Metab. 2020, Poland [18] | Observational retrospective cohort study, children 0-18 years with newly diagnosed T1D | 34 group 2020 52 group 2019 (March–May) |
9.90 9.59 |
22 (64.7%) 26 (50%) |
DKA (52.94% vs 40.38%, P=0.276) Severe DKA (32.35% vs 11.54%, P=0.0262) |
DKA rate has increased by 12 percentage Severe DKA cases noted in newly diagnosed T1D children |
|
| Josephine Ho, Pediatr Diabetes. 2021 Jun, Poland [19] | Retrospective study, < 18 years old, new onset T1D during the pandemic March 17 to August 31, 2020 vs 2019 |
107 NT1D in 2020 |
9.62 |
46 (43.0%) |
No significant increase in NT1D Higher DKA (68.2% vs 45.6%; p < 0.001) and higher severe DKA (27.1% vs 13.2%; p = 0.01) in 2020 vs 2019 |
Significant increase in DKA and severe DKA in NT1D children during the COVID-19 pandemic period | |
| 114 NT1D in 2019 | 9.43 | 47 (41.2%) | |||||
| Agnieszka Zubkiewicz-Kucharska, Adv Clin Exp Med. 2021 Feb, Poland [13] | Multicenter cohort study, the T1D pediatric registry for Lower Silesia (children aged 0–18 years) Incidence rate (IR) 2000-2019 vs first four months 2020 |
0-18 |
36.67% DKA incidence 2020 vs 31.75% DKA incidence 2000-2019 (p > 0.05) T1D cases (March, April) 2020 were half of the same months in 2019 (P > 0.05) IRT1D 17.27/100,000/year in 2020 vs IRT1D 17.51/100,000/year in 2000-2019 IRT1D in 2020 (first 4 months) was significantly lower than the period 2014–2019 (P = 0.0016), but comparable to 2019 (P = 0.0808) |
Increase in IR of T1D 2000 - 2019: - 10.43/100,000/year in 2000 - 22.06/100,000/year in 2019 - 27.10/100,000/year, Peak incidence in 2017 Highest T1D incidence rate in January and February DKA incidence: - 23.65% in 2000-2004 - 34.23% in 2005-2009 - 35.59% in 2010-2014 - 36.71% in 2015-2019 The IR of T1D during the COVID-19 pandemic was comparable, although their clinical condition was worse |
|||
| 1961 in 2000 – 2019 | 0-18 | 1054 (53.72%) |
|||||
| Iwona Pietrzak, Pediatr Diabetes. 2022 Nov, Poland [20] | Multicenter cohort study, DKA incidence in T1D COVID- 19 (15/3/2020-15/3/2021) and before COVID-19 (15/2/2019-15/3/2020) | 3062 T1D 1347 (44%) DKA |
9.5 | 1632 (53.3%) | 826 (49.4%) in the 2020/2021 IR 25.90 cases/100000 1671 (54.6%) in the2020/2021 |
COVID-19 was associated with increase in the frequency of DKA and its severity | |
| 521 (37.5%) in the 2019/2020 IR 21.55 cases/100000 1391 (45.4%) in the 2019/2020 | |||||||
| Anca Andreea Boboc, J Pers Med. 2021 Jun. Romania [21] | Observational retrospective cohort study, pediatric T1D patient from Marie Curie Emergency Children’s Hospital, Bucharest. | 147 (3/2020–2/2021) |
7.59 | 243 (53%) | 65.99% DKA 13.2 NT1D/month (5/2020-2/2021) |
An increase in the incidence and severity of T1D in children during the COVID-19 pandemic 30.08% increase in new onset T1D during the pandemic 67.40% increase in DKA incidence during the pandemic |
|
| 312 (2003–2019) |
39.42% DKA 9.4 NT1D/month (5/2018-2/2019) |
||||||
| Aqeel Alaqeel, Front Endocrinol (Lausanne). 2021 Apr. Saudi Arabia [22] | Multicenter retrospective cohort study, 1–14 years admitted with new-onset T1D or DKA during the COVID-19 pandemic | 106 (March–June 2020) |
10 | 51 (48.1%) | NT1D 41 (38.7%) DKA 88 (83%) DKA frequency NT1D 23 (26%) |
DKA was higher in 2020 vs 2019 (83% vs. 73%; P=0.05; risk ratio=1.15; 95% confidence interval, 1.04–1.26) DKA frequency among new-onset T1D was higher in 2020 vs 2019 (26% vs. 13.4%; P=<0.001) |
|
| 154 (March–June 2019) |
9.7 | 69 (44.8%) | NT1D 57 (37.0%) DKA 112 (72.7%) DKA frequency NT1D 15 (13.4%) |
||||
| Semine Özdemir Dilek, J Pediatr Endocrinol Metab. 2021 Jul. Turkey [23] | Cross-sectional study, newly diagnosed with type 1 diabetes mellitus in Cukurova University hospital | 74 (2020) | 10 | 35 (47.3%) | DKA 68 (91.9%) Moderate DKA 16 (23.5%) Severe DKA 15 (22.1%) |
Increase in the number of NT1D, autoantibody positivity, rates and severity of DKA during the COVID-19 pandemic period | |
| 46 (2019) | 10.5 | 21 (45.7%) | DKA 27 (58.7%) Moderate DKA 5 (18.5%) Severe DKA 4 (14.8%) |
||||
| Grenye O’Malley, J Clin Endocrinol Metab. 2021 Jan, USA [24] | Multicenter cross-sectional, adults over the age of 19 with T1D and COVID-19 | 113 (March 1, 2020 - August 22, 2020) | 39.9 | 55 (48.7%) | Death 5 (4.4%) DKA 27 (23.8%) |
TID is associated with higher risk of morbidity and mortality in COVID-19 patients | |
| Kaleb T Bogale, Endocrinol Diabetes Metab. 2021 Feb, USA [25] | Retrospective analysis, all pediatric patients (age ≤ 18) newly diagnosed T1D (01/01/2017 - 09/14/2020) |
42 Post-COVID |
9.2 | 23 (54.8%) | DKA 20 (47.6%) Moderate or severe DKA 13 (31.0%) |
Almost similar DKA rates and severity during COVID-19 |
|
| 370 Pre-COVID | 10 | 218 (58.9%) | DKA 172 (46.5%) Moderate or severe DKA 123 (33.2%) |
||||
| Thomas Danne, Diabetes Technol Ther. 2021 Sep, USA [26] | Retrospective cohort, T1D ≤ 21 years of age, 22,820 May/June 21,820 August/September 2019 and 2020 |
12,157 (M/J2020) | 13.5 | 52% | T1D duration 4.5 At least one DKA 1.1% At least 1 severe hypo 0.3% |
A significant rise in DKA rate and mortality during COVID-19 | |
| 13,386 (A/S 2020) | 13.6 | 51.9% | T1D duration 4.6 At least one DKA 0.7% At least 1 severe hypo 0.3% |
||||
| 16,735 (M/J 2019) | 13.4 | 51.7% | T1D duration 4.5 At least one DKA 0.8% At least 1 severe hypo 0.5% |
||||
| 14,523 (A/S 2019 | 13.4 | 51.6% |
T1D duration 4.6 At least one DKA 1.0% At least 1 severe hypo 0.5% |
||||
| Connie Trieu, J Clin Transl Endocrinol. 2021 Dec, USA [28] | Hospitalized children with T1D or T2DM and SARS-CoV-2 infection between April and November 2020 | 9 NT1D + COVID |
10.5 |
2 (22%) | DKA 64.3% in 2020 DKA 56.9% in 2019 DKA 47.1% in 2018 NT1D 286 children in 2020 NT1D 246 children in 2019 NT1D 263 children in 2018 |
16.3% increased rate of NT1D in 2020 6.5% decrease of NT1D from 2018 to 2019 Increase in DKA incidence in 2020 |
|
| 12 Known T1D + COVID | 12.4 | 6 (50%) | |||||
DKA, diabetic ketoacidosis; IRR, incidence rate ratios; IRT1D, incidence rate of type 1 diabetes; NT1D, New Onset Type 1 Diabetes; OR, Odds ratio; RR, Relative Risk; T1D, Type 1 Diabetes.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



