Submitted:
20 June 2023
Posted:
21 June 2023
You are already at the latest version
Abstract
Lymphedema is a chronic and debilitating disease that affects up to 250 million patients worldwide. Recent advances in understanding its pathophysiology, along with improved diagnosis and microsurgical techniques, have enhanced our ability to cope with the challenging task of treating this disease. This review provides an overview of the disease from a surgeon's point of view, including existing imaging modalities used for preoperative assessment, as well as surgical procedures used in its treatment. Advantages and drawbacks of various existing modalities used for pre or intraoperative assessment of lymphatic vessels are discussed. Lymphedema treatment has shifted from palliative debulking procedures (liposuction and direct excision) to those aimed at restoring lymphatic flow and countering the pathophysiology of the disease (lymphaticovenous anastomosis and vascularized lymph node transfer). A combination of both approaches can result in a synergistic benefit for patients and are discussed in this review. Despite recent advances, some controversies persist, and further studies are needed to better define surgical treatment algorithms.
Keywords:
Lymphedema
; Preoperative assessment
; Surgical treatment
; Liposuction
; Direct excision
; LVA
; VLNT
1. Introduction
Lymphedema is characterized by an abnormal accumulation of protein-rich fluid within the interstitium, resulting in swelling of the affected area. It can manifest as primary, when results from a structural or developmental defect in lymphatic system, or secondary, due to iatrogenic causes. Most cases of lymphedema in developed countries are secondary, resulting from damage to the lymphatic system induced by cancer or cancer treatment [1,2]. The diagnosis of lymphedema is primarily clinical and may be confirmed by imaging studies. Nonsurgical treatment remains the cornerstone of early-stage management, with the aim of increasing interstitial pressure and decreasing capillary filtration [3]. However, this approach does not address the underlying lymphatic dysfunction or pathophysiology of disease progression. In cases where nonsurgical management is no longer effective, surgical options are considered, including debulking and physiologic procedures. As our ability to understand the pathogenesis of the disease has increased, along with advances in microsurgical techniques, new physiologic procedures have been developed, with the goal of restoring lymphatic function and flow within the affected area. These include lymphaticovenous anastomosis and vascularized lymph node transfers. When the disease continues to progress, irreversible damage to the tissue occurs, including extensive fibrosis and accumulation of adipose tissue, a condition which can only be managed by debulking procedures. The goal of those procedures is to reduce limb volume, improve patient's symptoms and discomfort, but without the ability to restore lymphatic flow. Although these procedures have shown significant benefits for lymphedema patients, there is a lack of clear guidelines and reproducibility of studies [2,3,4,5,6]. This review provides an overview of the disease from a surgeon's point of view, including existing imaging modalities used for preoperative assessment, as well as surgical procedures used in the treatment of Lymphedema.
2. Imaging for diagnosis
Clinical evaluation is the primary method of diagnosing lymphedema, and during the physical exam it is important to exclude other conditions that can cause limb swelling like congestive heart failure, renal failure, malignancy, thyroid disease and more. Lymphatic imaging studies, such as lymphoscintigraphy and indocyanine green lymphography, can assist in the accurate differential diagnosis of lymphedema, disease staging and with choosing the appropriate treatment modality.
2.1. Lymphoscintigraphy
Lymphoscintigraphy (LSG) gives a general overview of the lymphatic function and has been considered the gold standard for confirming lymphedema diagnosis [7]. This technique involves injecting a technetium-labeled colloid subdermally in the distal limb, followed by nuclear scanning to assess the lymphatic system. In patients with lymphedema, colloid transport through the lymphatics to the nodal basin is often compromised, resulting in delayed uptake and fluid leakage into the subcutaneous tissue [8]. Although LSG is helpful in evaluating central lymphatic system abnormalities and the extent of the disease, it has several limitations, including poor anatomic/spatial resolution, inability to assess interstitial tissues and accompanying vasculature of the lymphatic system, radiation exposure, and lengthy examination times [1,2,7] (Figure 1).
2.2. Indocyanine green lymphography
Indocyanine green lymphography (ICG-L) is currently the preferred diagnostic imaging technique for the lymphatic system among surgeons [8]. It has higher sensitivity and specificity for diagnosing lymphedema compared to lymphoscintigraphy [7]. It is also used for the selection of surgical treatment modality and to give guidance to conservative treatment by manual lymphatic drainage. An intradermal injection of an ICG tracer in the distal limb is followed by visualization of the lymphatic vessels under a near-infrared camera. It is a minimally invasive, simple, and highly accurate method for assessing lymphatic system status [9]. It enables the evaluation of the functional status of superficial lymphatic vessels, determine their location, collateral lymphatic circulation, and dermal backflow [2,9,10]. A staging system correlating disease severity with pattern of dermal backflow on ICG-L has been developed by developed by Yamamoto et al. [11]. A linear pattern is considered as normal, while splash, stardust, and diffuse patterns represent abnormalities with increasing levels of deterioration in lymphatic function (Figure 2). In severe cases of dermal backflow, lymphatic flow beneath it is masked and cannot be detected by ICG-L. Other limitations include an inability to visualize lymphatic vessels deeper than 1.5-2.0 cm from the skin surface and an inability to assess interstitial tissues, the venous system, or lymph nodes (except during surgery)[1,7,8,10]. Furthermore, the evaluation is operator-dependent, such as ultrasound.
3. Imaging for treatment
After establishing the diagnosis of lymphedema, the next step will be choosing the appropriate treatment option, and the possibility of performing a lymphaticovenous anastomosis (LVA) becomes an important aspect of surgical decision making. Functional lymphatic vessels and nearby receiving veins are important requirements for LVA, and therefore, preoperative imaging plays a significant role in substantiating the treatment choice. An ideal imaging study should evaluate the anatomy and function of lymph nodes and lymphatic vessels, show their course in three dimensions, and display the venous network that will function as an anastomotic acceptor site [12]. In addition to being a diagnostic tool, indocyanine green lymphography (ICG-L) is also part of the preoperative evaluation for lymphatic surgery. Other helpful imaging modalities include magnetic resonance lymphangiography (MRL), single-photon emission computed tomography/computed tomography (SPECT/CT), ultra high-frequency ultrasound (UHF-US), and photoacoustic (PA) imaging (Table 1).
3.1. Indocyanine green lymphography
As discussed before, can serve as a valuable tool in the outpatient setting for diagnosis and guiding treatment decisions. During LVA surgery, ICG-L facilitates the localization of lymphatic vessels, distinguish between normal and abnormal drainage pathways, and optimizes LVA surgical efficacy by assessing anastomosis patency. These benefits make ICG-L a valuable intraoperative tool for surgeons performing LVA procedures [11].
3.2. Magnetic resonance lymphangiography (MRL)
Magnetic resonance lymphangiography (MRL) is typically performed by injecting a gadolinium-based contrast agent intradermally in the interdigital web spaces. There is also a possibility to perform MRL without the injection of contrast agent, but no information is obtained about the functional status of lymphatics and veins and it has a lesser spatial resolution when compared to contrast-enhanced MRL[12]. Contrast-enhanced MRL produces high-resolution images of the lymphatic channels, including number, size, depth, trajectory, and regions of dermal backflow [9]. In fact, MRL has a higher sensitivity to detect lymphatic vessel abnormalities than other imaging modalities such as lymphoscintigraphy (LSG), indocyanine green lymphangiography (ICG-L), and Ultrasound Doppler [9]. As opposed to ICG-L, MRL provides a three-dimensional image of the entire extremity and provides information about the quantity and quality of both the superficial and deep lymphatic systems. It also allows to visualize the lymph node basin, venous system, and quality of the interstitial fluid [1,2]. This capacity to identify and map functional lymphatic channels preoperatively makes MRL useful in determining suitable targets for performing lymphovenous anastomosis (LVA) (Figure 3). Studies [9,13] found that concordant use of MRL and ICG-L in identifying functional lymphatic vessels correlates with a higher probability of successful LVA. Additionally, MRL can evaluate the composition of a lymphedematous limb, aiding in the determination of appropriate surgical treatment. Patients with normal subcutaneous tissues or fluid-dominant edema may benefit from microsurgical reconstruction, while adipose-dominant edema is usually treated with liposuction and fibrosclerotic-dominant edema with direct excision [1]. A study performed by Dayan et. al[14] found that even patients within the same International Society of Lymphology class may have different percentages of fat and fluid, which can impact treatment choice and demands an appropriate preoperative assessment. However, MRL is an expensive tool compared to ICG-L, may produce images with venous enhancement due to venous uptake of contrast agent, is time-consuming, difficult for patients with claustrophobia, and might be impossible for patients with non-compatible implants [15].
3.3. Single-photon emission computed tomography/computed tomography (SPECT/CT)
SPECT/CT is a hybrid imaging modality that combines planar imaging of SPECT with CT. This technique provides anatomical localization of radio-activated lymph nodes and functional and three-dimensional information about the lymphatic system [16,17]. SPECT/CT can differentiate between lymphatic vessels and veins, and between tracer uptake in lymph nodes and lymphoceles. It is also capable of identifying dermal backflow from lymphatic vessel leakage and locating appropriate lymphatic vessels for LVA [18,19]. However, SPECT/CT has some drawbacks including high cost and exposure to radiation, as well as low resolution for localizing lymphatic channels [17].
3.4. Ultra high-frequency ultrasound (UHF-US)
Ultra high frequency ultrasound (UHF-US) with a frequency range of 48-70 MHz provides improved resolution compared to conventional ultrasound (15-24 MHz). It enables accurate, real-time visualization of lymphatic vessels, even those with diameters smaller than 0.3 mm, and allows to distinguish them from the subcutaneous veins or the nerves [20]. Lymphatic vessels are differentiated based on their shape, echogenic texture, color, doppler collapsibility, convergence, and location [21]. UHF-US can also classify lymphatic vessels into two types: type I (less obstructed lymphatic channels, including normal and ectasis types) and type II (more obstructed lymphatic channels, including contraction and sclerosis types). Differentiating between these types is important for selecting suitable lymphatic vessels for LVA intraoperatively. Over time, the damaged lymphatic vessels become sclerotic and lose their ability to drain lymph fluid effectively, therefore, anastomosing lymphatic vessels type I have a significant advantage in LVA surgery [22]. UHF-US limitations include operator-dependency and limited distance reach, as it can obtain images only up to 10mm from the skin. To detect lymphatic vessels deeper than 10mm, a transducer with a frequency of 48 MHz (max image depth:23.5mm) is recommended [20].
3.5. Photoacoustic (PA) or optoacoustic imaging
Photoacoustic imaging is a novel technique that utilizes the photoacoustic effect to visualize the lymphatic and vascular systems in three dimensions with high resolution. This imaging modality, known as PA lymphangiography, involves the absorption of a specific wavelength of light by chromophores such as melanin, hemoglobin, or ICG, leading to thermoelastic expansion and the production of acoustic waves that are detected by an ultrasound transducer [23,24]. Unlike ICG-L, which also relies on ICG to identify lymphatic vessels, PA imaging can accurately differentiate between veins and lymphatic vessels, asses the three-dimensional relationship between them and is less influenced by dermal backflow [23]. Consequently, using PA imaging intraoperatively enables rapid identification of optimal sites for LVA and assessment of anastomosis patency. In fact, PA imaging fulfills many of the criteria for an ideal imaging modality for surgical planning. However, it is still a developing technology and handheld PA imaging devices are limited to a depth of 1cm. Additionally, accurately adjusting position of the PA lymphangiography figures and the patient’s limb for clinical application remains challenging [23,24]. Despite these challenges, PA lymphangiography shows great promise as a valuable tool in lymphatic surgery.
4. Surgical treatment
In cases where conservative management fails to improve lymphedema, surgical intervention may be considered. The surgical options can be classified as debulking or physiologic procedures. The former is typically performed in the later stages of the disease when there has been a transition from fluid-dominated edema to adipose or fibrosclerotic-dominated edema. Commonly used debulking procedures include suction-assisted lipectomy and direct excision, both focused on reducing the volume of the limb rather than restoring lymphatic flow. Physiologic treatment involves microsurgery techniques and focuses on restore lymphatic flow and function. A treatment algorithm for patients with symptoms of lymphedema is provided (Figure S1).
4.1. Debulking procedures
4.1.1. Suction-assisted lipectomy (SAL)
Suction-assisted lipectomy (SAL) is a minimally invasive surgical procedure that removes fibrotic subcutaneous adipose tissue using suction cannulas. This technique involves small skin incisions, and power-assisted devices may be used to aid in the removal of fibrous soft tissue. The procedure is performed circumferentially from distal to proximal and in a longitudinal direction to minimize damage to the remaining lymphatics, although some damage is inevitable. The goal of SAL is to remove the maximal amount of adipose tissue, and the incisions are left open to drain externally. Intraoperatively, custom compression garments are applied, and lifelong use of compression garments is required to prevent recurrence [25,26]. Several studies have confirmed the long-term reduction of volume, improvement in quality of life, and decrease in infection rates with SAL [26,27,28]. In selected patients, SAL may be performed in conjunction with physiologic surgery to reduce dependence on compression garments and to improve outcomes [26]. However, SAL is not effective for patients with end-stage fibrosclerotic lymphedema, and direct excision is required in those cases.
4.1.2. Direct excision
In cases of advanced fibrosclerotic lymphedema, direct excision of the diseased interstitial tissues may be necessary, with or without skin resection. The Charles procedure involves removing subcutaneous tissues and skin circumferentially, followed by skin grafts applied over the muscle fascia. Modified versions of this procedure incorporate negative pressure wound therapy and delayed skin grafting to improve graft take and wound recovery [13]. Alternatively, the modified Homan's procedure [26] enables primary skin closure, after performing the excision in a staged manner. These procedures are indicated for patients with irreversible fibrosclerotic lymphedema and significant symptoms, such as recurrent infections, impaired mobility, ulcerations, and malignancies. Although direct excision surgery provides consistent results with improvement in well-being and function [29], it is associated with significant morbidity, scarring, risk of graft loss, skin flap necrosis, lymphedema distal to the excised area, and sensory loss [1]. Additionally, patients may still need to use compression garments after surgery, and in cases where lymphedema recurs in the extremity, amputations may be necessary.
4.2. Physiologic procedures
Advancements in the treatment of lymphedema have been achieved through the implementation of microsurgery, which allows for targeted treatment of the underlying cause of the disease. Physiological procedures have been developed to restore the lymphatic flow, with the two main techniques being lymphaticovenular anastomosis (LVA) and vascularized lymph node transfer (VLNT).
4.2.1. LVA
The goal of lymphaticovenular anastomosis (LVA) is to restore lymphatic circulation by connecting functional lymphatic channels to subdermal venules of similar size, creating peripheral shunts within the lymphedematous limb. This allows unidirectional flow from the congested high-pressure lymphatic system to the lower-pressure venous system [30]. To achieve successful long-term LVA, certain principles must be followed. Candidates for LVA must have functional or at least draining lymphatic vessels and a venule in proximity without reflux. As dynamic venous stenosis may contribute to lymphedema, some authors recommend screening for venous compression or reflux as part of the perioperative evaluation, to evaluate the utility of scar fibrosis release, angioplasty, or venous stenting in the treatment of venous insufficiency [31,32]. A meticulous surgical technique is critical for a successful long-term LVA [26]. At selected cutaneous sites, two-centimeter skin incisions are made, and lymphatic channels and venules are carefully dissected under a microscope using super-microsurgery instruments. Nylon sutures of 11-0 or 12-0 are used for the anastomosis, and the anastomotic technique is selected depending on the relative calibers of the vessels found. Veins and lymphatics can mainly be anastomosed in the end-to-side, end-to-end, side-to-side, and side-to-end arrangements. The most efficient bypass is considered by some authors to be side-to-end, as it allows for bidirectional lymph flow into a recipient vein while preserving the native lymph flow of the vessels and preventing damage to existing vessels [6]. However, there is no established consensus regarding the best technique to use or the number of anastomoses to perform [33,34]. After performing the anastomosis, its patency can be tested with ICG-L or patent blue dye (Figure 4). LVA is more effective in patients with early stages of lymphedema, although there can be a synergistic benefit when performed synchronously with vascularized lymph node transplantation in advanced-stage lymphedema. In fact, lymphedema treatment is a highly individualized process, and its effectiveness is consistently enhanced in combined approaches [30]. The eligibility of the LVA procedure is mainly determined by the presence of healthy, functional lymphatic vessels rather than the stage of lymphedema [32,35]. LVA can also be helpful in the treatment of lymphorrhea as demonstrated by some studies [36,37]. The complications of LVA are minimal, with rates reported at 5.9% [30]. LVA offers significant advantages for the patient, being a minimally invasive procedure that can be done as an outpatient procedure under local or general anesthesia with a short recovery time and minimal postoperative restrictions [32] (Figure 5).
4.2.2. VLNT
In later stages of lymphedema, when lymphatic channels are obliterated, alternative surgical interventions have been proposed, including vascularized lymph node transfer (VLNT). VLNT is a microsurgical technique that involves the transplantation of a vascularized lymph node and the surrounding tissue into the affected limb, anastomosing it to the arterial and venous systems in the recipient site. Typically, VLNT is performed for patients with moderate to advanced lymphedema, with damaged lymphatic vessels or decreased lymph node function. The precise physiological mechanisms behind the effects of VLNT on lymphedema are not yet fully understood. However, two primary hypotheses have been put forward to explain these effects. The first hypothesis proposes that VLNT induces lymphangiogenesis, which establishes connections between the lymph nodes and the recipient site's lymphatic vessels. The second hypothesis suggests that the transferred lymph nodes function as a "pump" by absorbing interstitial fluid and transporting it into the systemic circulation via the intrinsic lymphovenous shunt within the nodes [38]. The proposed mechanisms provide evidence for the efficacy of both proximal anatomical (orthotopic) and distal non-anatomical (heterotopic) placement of lymph node flaps. Indeed, there is ongoing debate regarding the ideal location of the recipient site [33]. Typical locations for VLNT include the axilla, elbow, wrist, groin, knee and ankle. In selected patients, planned for postmastectomy breast reconstruction and suitable for autologous reconstruction, a chimeric flap of deep inferior epigastric artery perforator (DIEP) flap and groin vascularized lymph node flap placed in the axilla may be suggested as an optimal solution for breast reconstruction and lymphedema. Since upper extremity lymphedema often occurs after previous surgery with or without radiation to the axilla, scar tissue in the area and around the axillary vein may need to be released to provide a healthy bed for lymphangiogenesis. Similar to the axilla, the groin region may also need extensive removal or dissection of scar tissue from past surgeries and radiotherapy [32]. In such situations, orthotopic placement of VLNT is likely more reasonable as it can address both objectives. However, research suggests that the selection of recipient sites does not have a significant impact on the outcomes, and hence, the choice is typically based on the availability of recipient vessels and surgeon preference. Although multiple studies have shown encouraging results of vascularized lymph node transfer (VLNT) in improving symptoms and quality of life in patients with lymphedema, patients are still required to use compression garments after the surgery [39]. There are several potential donor sites for VLNT, including the groin, lateral thoracic, supraclavicular, submental, omental, and jejunal mesenteric node flaps (Table 2). Among these options, the most commonly used is the groin flap [40]. Its surgical anatomy and safety of harvesting has been clearly described [41]. Although VLNT has shown promising results in treating lymphedema, mild to severe secondary iatrogenic lymphedema at the donor site has been reported in some cases [1,25,40,42]. Even in the absence of clinical lymphedema of the donor site, lymphatic function alterations are seen, thus caution should be taken [43,44]. However, according to the literature, symptomatic iatrogenic donor site lymphedema is a rare complication [25,33]. To minimize this risk, reverse lymphatic mapping has been suggested as a mandatory test, involving the injection of ICG or patent blue dye in the distal part of the limbs and the avoidance of marked draining nodes during flap harvesting [45]. Other complications, such as seroma, lymphocele, infection, and delayed wound closure, have also been observed. Compared to LVA, VLNT requires a longer hospital stay and surgical time [25].
4.2.2.1. Groin lymph node flap
The vascularized groin lymph node flap was the first to be described and remains the most commonly used donor site for VLNT [46]. This flap is based on the superficial circumflex iliac vessels and is favored due to well-described anatomic studies, well-concealed scar, and feasibility to be combined with breast reconstruction [47,48]. The major complication associated with its harvest is the possibility of causing iatrogenic secondary lymphedema. To minimize this risk, the flap harvest should be limited to the area between the superficial inferior epigastric vein and the superficial circumflex iliac vein. Additionally, it is recommended to avoid harvesting lymphatic tissue caudal to the groin crease, deep to the deep fascia, and medial to a circle of 2cm diameter area centered half across the inguinal ligament [41] Reverse lymphatic mapping can be used intraoperatively, further reducing the risk of iatrogenic lymphedema, by identifying lymph nodes that preferentially drain the extremity related to the donor site. Limitations of the flap include a short pedicle length and small arterial caliber [26].
4.2.2.2. Lateral thoracic lymph node flap
The lateral thoracic lymph node flap is usually based on the lateral thoracic vessels and can also be harvested based on branches of the axillary artery or the thoracodorsal artery in cases where the artery is absent [49,50]. Since it includes axillary level I lymph nodes, it may not be suitable after an axillary dissection. The complication rate of this flap has been described as the highest among the five most frequently used lymph node donor sites [51]. Therefore, it is imperative to use reverse lymphatic mapping and avoid dissection over the drainage of the upper extremity, cephalad to the second intercostal brachial nerve, and medial to the lateral border of the pectoralis minor [52]. However, the flap presents some advantages that make it an attractive alternative to other VLNT donor sites, such as consistent anatomy, inconspicuous donor site scar, and long pedicle length [49]. It can be placed on orthotopic or heterotopic position due to its versatility in flap design [26] and it include abundant lymph nodes. An anatomical study revealed an average of 13.06 ± 3.42 lymph nodes within the flap [51], but it is unknown if all 13 lymph nodes can be safely harvested since the study did not use reverse lymphatic mapping.
4.2.2.3. Supraclavicular lymph node flap
The supraclavicular lymph node flap is based on the supraclavicular branch of the transverse cervical vessels and encompasses cervical level Vb lymph nodes. The lymph nodes drain lymph fluid mainly from the breast, lung, esophagus, and oral cavity [53,54]. Although there is a risk of injuring the supraclavicular nerves during flap harvest, the risk of iatrogenic lymphedema is significantly lower compared to groin or lateral thoracic flaps. Only one case of secondary lymphedema following supraclavicular lymph node flap harvest has been reported in the literature so far [49]. Harvesting from the right side is usually preferred to avoid thoracic duct injury, even though it contains fewer lymph nodes than the left side [26]. Other advantages of the flap are its reliability, pliability and a well-hidden scar that can be easily concealed by clothing [26,49,54].
4.2.2.4. Submental lymph node flap
The submental lymph node flap is based on the submental artery, a branch of the facial artery. The flap can include submental (Ia) and submandibular (Ib) lymph nodes [26]. On average, the flap contains 3-5 lymph nodes and has a consistent anatomy [49,55,56,57]. M H Cheng’s group [58] suggested that the outcome of lymphedema surgery is dependent on the number of lymph nodes present in the flap, hence some authors recommend preoperative neck imaging to identify the side with the greatest number of lymph nodes and their position [55,56]. There are no cases in the literature of iatrogenic lymphedema with submental lymph node flap. Another advantage of the flap is its small volume, making it suitable for heterotopic placement. The disadvantages of the flap include a short pedicle length, a visible scar, and the possibility of injuring the marginal mandibular nerve during harvest [26,49,55].
4.2.2.5. Omental lymph node flap
The omental lymph node flap can be utilized as either a pedicled or free flap. Complications such as iatrogenic hernia, small-bowel obstruction, and donor site infection have been reported with the pedicled flap technique, which has limited its widespread use, and therefore its transfer is mostly carried out by microsurgery [49,59]. While the entire omentum can be harvested, it is typically limited to perivascular tissue and lymph nodes surrounding the gastroepiploic vascular arcade, using the right or left gastroepiploic vessels while sparing the rest [49,59]. Due to its high lymph node density and versatility in flap size, bilateral or dual-level transfer on both sides of the pedicle is feasible [26,49,59,60]. The flap is highly reliable, and unlike other VLNTs, its anatomy also permits a consistent efferent lymphatic vessel to be used for LVA [61]. There is no risk of donor site lymphedema. The main complications are related to abdominal surgery, and previous abdominal operations, intraabdominal adhesions, and scarring may restrict its use. The use of laparoscopic techniques including robotic surgery, to harvest the flap, reduces donor site morbidity while also allowing for minimal scarring that can be concealed under the patient's clothing [26,49,59,61].
4.2.2.6. Jejunal mesenteric lymph node flaps
The use of the jejunal mesenteric lymph node flap as a pedicled flap was abandoned due to its associated complications, like the omental lymph node flap. As a free flap, it can be harvested from the periphery of the mesentery to incorporate a vascular arcade adjacent to the jejunum or from closer to the root of the mesentery, with each approach having some limitations. The former approach may be associated with ischemic bowel complications, while the latter may require a flow-through design to augment venous outflow. As an intra-abdominal procedure, harvesting the flap can lead to hernias and obstructions [49,59,62]. Nonetheless, the flap provides a reliable lymph node cluster with no risk of donor site lymphedema. It can be harvested through a mini-laparotomy, abdominoplasty, or laparoscopic incisions, allowing for a well-concealed scar [26,49,59].
4.3. Preventive lymphatic surgery (LYMPHA approach) [63]
In recent times, there has been a growing interest in preventive lymphatic surgery as a potential approach to reduce the risk of lymphedema resulting from cancer surgery. This surgical approach involves immediate lymphatic reconstruction at the time of node dissection. However, studies have yielded conflicting results, and its effectiveness remains controversial. A systematic review and meta-analysis conducted by Ciudad et al. [64] revealed that patients treated with prophylactic LVA (lymphaticovenular anastomosis) had a pooled lymphedema rate that was significantly lower than that reported in the literature: 5.15% for axillary lymph nodes and 6.66% for ilio-inguinal nodes. Nevertheless, high-quality studies are necessary to establish clear recommendations regarding the use of preventive lymphatic surgery.
5. Discussion
Lymphedema is a chronic and debilitating disease that affects millions of patients worldwide [3]. Recent advances in understanding its pathophysiology, along with improved diagnosis and microsurgical techniques, have enhanced our ability to cope with the challenging task of treating this disease. This review aims to summarize lymphedema management from a surgeon’s point of view, although it is crucial to note that complex decongestive therapy is the primary treatment, and surgical procedures are only considered when conservative treatments are no longer effective.
There are several surgical procedures available for the surgeon, that will vary depending on lymphedema’s stage. In general, microsurgical reconstruction is effective for fluid-dominant edema, suction-assisted lipectomy for adipose-dominant edema, and direct excision for fibrosclerotic-dominant edema [1]. However, surgical treatment is highly individualized and should be tailored according to the progression of the disease, optimally combined to achieve a better outcome. Thus, imaging examinations are of paramount importance when planning the treatment. We discussed the advantages and drawbacks of various existing modalities used for pre or intraoperative assessment of lymphatic vessels. Lymphoscintigraphy is a highly sensitive and specific study to diagnose but not quantify lymphedema [30]. ICG-L is currently the essential diagnostic imaging technique, since it provides real-time evaluation of the superficial lymphatic vessels, dermal back flow patterns, and the presence and location of functional lymphatic channels. Its downside is the absence of in-depth information and inability to assess interstitial tissue or venous system, limitations that can have implications on surgical decision-making and led to the use of MRL [2]. The high financial cost of the MRL is outweighed by its ability to provide information regarding the quality of the interstitial fluid and 3D high-resolution presence of functional lymphatics and veins in the vicinity to perform an LVA. However, it is less practical for routine implementation due to logistical issues as opposed to portable UHF-US [21]. On the other hand, the implementation of UHF-US is not straightforward because of the demanding learning curve and the limited in-depth information it can provide. The optimal imaging modality for surgical planning should have the ability to assess in real-time the interstitial tissues, the anatomy and functionality of lymph nodes and lymphatic vessels, demonstrate their course in three dimensions, and demonstrate the venous network that will serve as an acceptor site for anastomosis. PA imaging is a promising tool that fulfills many of these criteria, however its use is limited due to being a developing technology, not yet adapted for widespread clinical practice [23,24].
Once the patient has been evaluated, the treatment plan for lymphedema should be determined. While the focus of lymphedema treatment has shifted from palliative debulking procedures to those aimed at restoring lymphatic flow and countering the pathophysiology of the disease, debulking procedures still play a role in surgical management. This is because there are currently no physiologic methods available to reverse the adipose hypertrophy and fibrotic edema that occur in later stages of the disease. Modifications in the Charles procedure have resulted in improved patient outcomes and reduced morbidity in cases of advanced fibrosclerotic lymphedema. Furthermore, the use of suction-assisted lipectomy has broadened the range of excisional surgery, providing benefits to patients with less severe lymphedema[65]. In selected patients, it can also be performed as an adjunctive procedure to physiologic surgeries, reducing reliance on compression garments and enhancing outcome. However, the optimal timing for each procedure remains uncertain [26,66]. Physiologic treatments are mainly divided into LVA and VLNT procedures. Due to the lack of standardized protocols, there is currently insufficient evidence supporting the effectiveness of either procedure. While there is no consensus on which procedure is more effective, both have demonstrated the ability to decrease the severity of lymphedema [66]. In the case of LVA, the average reduction in volume varies from 2.4 to 69%, while for VLNT it ranges from 7.1 to 74.5% [3]. In order to perform LVA, it is necessary for patients to have patent or ideally functional superficial lymphatic vessels and a venule nearby that can be used for anastomosis. Several studies have demonstrated that LVA is more effective in patients with early stages of lymphedema, but a synergistic effect may exist when performed simultaneously with VLNT in advanced-stage lymphedema [30,66]. The complications of LVA are minimal with rates reported at 5.9%, and the surgery can be performed as an outpatient procedure [30,32]. VLNT can be performed irrespective of the presence of healthy superficial lymphatic vessels, however, the rate of complications associated with it is 30.1% [30]. Several potential donor sites can be considered for the procedure, with the groin lymph nodes being the most commonly utilized site, mainly due to the well-hidden scar and the feasibility of combining it with free abdominal tissue transfer for breast reconstruction [53]. Donor site lymphedema is one of the most concerning complications associated with VLNT. As a preventive measure, a reverse lymphatic mapping is advised for groin lymph nodes and lateral thoracic lymph nodes transfers to avoid damaging the limb draining nodes in the region. Submental, omental and jejunal mesenteric lymph node flaps are not associated with iatrogenic lymphedema. However, in the case of submental flaps, there is a risk of injuring the marginal mandibular nerve and producing an unsightly scar. Intra-abdominal lymph nodes flaps are associated with risks relating to abdominal surgery, and it is advisable to perform the surgery in collaboration with a general surgeon. The supraclavicular lymph node flap presents a low risk of iatrogenic lymphedema, but there is a potential risk of injury to vital structures in the neck region. The optimal recipient site location remains also a subject of debate [33]. In cases where it is necessary to release a scar resulting from prior regional lymphadenectomy and/or radiation, it is recommended to choose a proximal location. However, some surgeons argue that lymph nodes absorb interstitial fluid and pump it into the venous circulation through intrinsic LVA and therefore suggest using a distal location to achieve this effect from the most gravity-dependent position. The combination of physiologic procedures with debulking techniques has the potential to enhance functional outcomes and quality of life in patients. Nonetheless, postoperative compression garments or physiotherapy are still recommended to maintain or further reduce limb volume [13,25].
6. Conclusion
This article is an overview of the diagnosis and treatment of lymphedema, emphasizing the importance of making informed clinical decisions based on a wide variety of imaging techniques available. Currently, ICG-L is considered the essential diagnostic tool due to the combination of real-time information and ease of use. While PA imaging is a promising technique, further evidence is required to validate its utility in surgical planning. The evolution of lymphedema surgery from debulking to physiologic procedures has been proven effective, and a combination of both approaches can result in a synergistic benefit for patients. The surgical procedures should be performed by experienced surgeons to reduce the risks associated with them. Despite recent advances, some controversies persist, and further studies are needed to better define surgical treatment algorithms.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Funding
This research received no external funding.
Informed Consent Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Zeltzer AA, Anzarut A, Hamdi M. A Review of Lymphedema for the Hand and Upper-Extremity Surgeon. J Hand Surg Am 2018, 43, 1016–1025. [Google Scholar] [CrossRef] [PubMed]
- Zeltzer AA, Brussaard C, Koning M, et al. MR lymphography in patients with upper limb lymphedema: The GPS for feasibility and surgical planning for lympho-venous bypass. J Surg Oncol 2018, 118, 407–415. [Google Scholar] [CrossRef]
- Will PA, Wan Z, Seide SE, et al. Supermicrosurgical treatment for lymphedema: a systematic review and network meta-analysis protocol. Syst Rev 2022, 11, 18. [Google Scholar] [CrossRef]
- Winters H, Tielemans HJP, Paulus V, Hummelink S, Slater NJ, Ulrich DJO. A systematic review and meta-analysis of vascularized lymph node transfer for breast cancer-related lymphedema. J Vasc Surg Venous Lymphat Disord 2022, 10, 786–795.e1. [Google Scholar] [CrossRef] [PubMed]
- Beederman M, Garza RM, Agarwal S, Chang DW. Outcomes for Physiologic Microsurgical Treatment of Secondary Lymphedema Involving the Extremity. Ann Surg 2022, 276, e255–e263. [Google Scholar] [CrossRef]
- Verhey EM, Kandi LA, Lee YS, et al. Outcomes of Lymphovenous Anastomosis for Lower Extremity Lymphedema: A Systematic Review. Plast Reconstr Surg Glob Open 2022, 10, e4529. [Google Scholar] [CrossRef]
- Knackstedt R, Chen WF. Current Concepts in Surgical Management of Lymphedema. Phys Med Rehabil Clin N Am 2022, 33, 885–899. [Google Scholar] [CrossRef]
- Beederman M, Chang DW. Advances in surgical treatment of lymphedema. Arch Plast Surg 2021, 48, 670–677. [Google Scholar] [CrossRef]
- Pons G, Clavero JA, Alomar X, Rodríguez-Bauza E, Tom LK, Masia J. Preoperative planning of lymphaticovenous anastomosis: The use of magnetic resonance lymphangiography as a complement to indocyanine green lymphography. J Plast Reconstr Aesthet Surg 2019, 72, 884–891. [Google Scholar] [CrossRef]
- Chang EI, Chu CK, Chang EI. Advancements in imaging technology for microvascular free tissue transfer. J Surg Oncol 2018, 118, 729–735. [Google Scholar] [CrossRef]
- Akita S, Unno N, Maegawa J, et al. A phase III, multicenter, single-arm study to assess the utility of indocyanine green fluorescent lymphography in the treatment of secondary lymphedema. J Vasc Surg Venous Lymphat Disord 2022, 10, 728–737.e3. [Google Scholar] [CrossRef] [PubMed]
- Guerrini S, Gentili F, Mazzei FG, Gennaro P, Volterrani L, Mazzei MA. Magnetic resonance lymphangiography: with or without contrast? Diagn Interv Radiol 2020, 26, 587–595. [Google Scholar] [CrossRef] [PubMed]
- Park KE, Allam O, Chandler L, et al. Surgical management of lymphedema: a review of current literature. Gland Surg 2020, 9, 503–511. [Google Scholar] [CrossRef] [PubMed]
- Dayan JH, Wiser I, Verma R, et al. Regional Patterns of Fluid and Fat Accumulation in Patients with Lower Extremity Lymphedema Using Magnetic Resonance Angiography. Plast Reconstr Surg 2020, 145, 555–563. [Google Scholar] [CrossRef]
- Forte AJ, Boczar D, Huayllani MT, et al. Use of magnetic resonance imaging lymphangiography for preoperative planning in lymphedema surgery: A systematic review. Microsurgery 2021, 41, 384–390. [Google Scholar] [CrossRef]
- Gentileschi S, Albanese R, Pino V, et al. SPECT/CT and fusion ultrasound to target the efferent groin lymph node for lymphatic surgery. Microsurgery 2019, 39, 605–612. [Google Scholar] [CrossRef]
- Du X, Liu C. Application of imaging in lymphedema surgical therapies. Gland Surg 2020, 9, 582–588. [Google Scholar] [CrossRef]
- Iimura T, Fukushima Y, Kumita S, Ogawa R, Hyakusoku H. Estimating Lymphodynamic Conditions and Lymphovenous Anastomosis Efficacy Using (99m)Tc-phytate Lymphoscintigraphy with SPECT-CT in Patients with Lower-limb Lymphedema. Plast Reconstr Surg Glob Open 2015, 3, e404. [Google Scholar] [CrossRef]
- Weiss M, Baumeister RG, Frick A, Wallmichrath J, Bartenstein P, Rominger A. Primary lymphedema of the lower limb: the clinical utility of single photon emission computed tomography/CT. Korean J Radiol 2015, 16, 188–195. [Google Scholar] [CrossRef]
- Hayashi A, Giacalone G, Yamamoto T, et al. Ultra High-frequency Ultrasonographic Imaging with 70 MHz Scanner for Visualization of the Lymphatic Vessels. Plast Reconstr Surg Glob Open 2019, 7, e2086. [Google Scholar] [CrossRef]
- van Heumen S, Riksen JJM, Bramer WM, van Soest G, Vasilic D. Imaging of the Lymphatic Vessels for Surgical Planning: A Systematic Review. Ann Surg Oncol 2023, 30, 462–479. [Google Scholar] [CrossRef] [PubMed]
- Bianchi A, Visconti G, Hayashi A, Santoro A, Longo V, Salgarello M. Ultra-High frequency ultrasound imaging of lymphatic channels correlates with their histological features: A step forward in lymphatic surgery. J Plast Reconstr Aesthet Surg 2020, 73, 1622–1629. [Google Scholar] [CrossRef] [PubMed]
- Suzuki Y, Kajita H, Watanabe S, et al. Application of Photoacoustic Imaging for Lymphedema Treatment. J Reconstr Microsurg 2022, 38, 254–262. [Google Scholar] [CrossRef] [PubMed]
- Suzuki Y, Kajita H, Watanabe S, et al. Surgical Applications of Lymphatic Vessel Visualization Using Photoacoustic Imaging and Augmented Reality. J Clin Med 2021, 11, 194. [Google Scholar] [CrossRef] [PubMed]
- Gallagher K, Marulanda K, Gray S. Surgical Intervention for Lymphedema. Surg Oncol Clin N Am 2018, 27, 195–215. [Google Scholar] [CrossRef]
- Schaverien MV, Coroneos CJ. Surgical Treatment of Lymphedema. Plast Reconstr Surg 2019, 144, 738–758. [Google Scholar] [CrossRef]
- Greene AK, Maclellan RA. Operative Treatment of Lymphedema Using Suction-Assisted Lipectomy. Ann Plast Surg 2016, 77, 337–340. [Google Scholar] [CrossRef]
- Greene AK, Maclellan R. Management of Lymphedema with Suction-Assisted Lipectomy. Plastic and Reconstructive Surgery 2014, 134, 36. [Google Scholar] [CrossRef]
- Van der Walt JC, Perks TJ, Zeeman BJ, Bruce-Chwatt AJ, Graewe FR. Modified Charles procedure using negative pressure dressings for primary lymphedema: a functional assessment. Ann Plast Surg 2009, 62, 669–675. [Google Scholar] [CrossRef]
- Carl HM, Walia G, Bello R, et al. Systematic Review of the Surgical Treatment of Extremity Lymphedema. J Reconstr Microsurg 2017, 33, 412–425. [Google Scholar] [CrossRef]
- Gupta R, Mathijs E, Hart J, Bates J, Powers J, Chaiyasate K. May-Thurner Syndrome and Lymphedema Reconstruction. Plast Reconstr Surg Glob Open 2022, 10, e4377. [Google Scholar] [CrossRef] [PubMed]
- Chang DW, Masia J, Garza R, 3rd, Skoracki R, Neligan PC. Lymphedema: Surgical and Medical Therapy. Plast Reconstr Surg 2016, 138, 209s–218s. [Google Scholar] [CrossRef] [PubMed]
- Hanson SE, Chang EI, Schaverien MV, Chu C, Selber JC, Hanasono MM. Controversies in Surgical Management of Lymphedema. Plast Reconstr Surg Glob Open 2020, 8, e2671. [Google Scholar] [CrossRef] [PubMed]
- Scaglioni MF, Fontein DBY, Arvanitakis M, Giovanoli P. Systematic review of lymphovenous anastomosis (LVA) for the treatment of lymphedema. Microsurgery 2017, 37, 947–953. [Google Scholar] [CrossRef]
- de Sire A, Losco L, Lippi L, et al. Surgical Treatment and Rehabilitation Strategies for Upper and Lower Extremity Lymphedema: A Comprehensive Review. Medicina (Kaunas) 2022, 58, 954. [Google Scholar] [CrossRef]
- Martins de Carvalho F, Almeida A, Silva Á, Marques M. Treatment of Lymphorrhea Associated with an Amputation Stump with Lymphaticovenular Anastomosis. Acta Med Port 2022, 35, 384–387. [Google Scholar] [CrossRef]
- Yang JC-S, Yen Y-H, Wu S-C, Lin W-C, Chiang M-H, Hsieh C-H. Supermicrosurgical Lymphaticovenous Anastomosis as an Alternative Treatment Option for Patients with Lymphorrhea. Plastic and Reconstructive Surgery 2019, 144, 1214–1224. [Google Scholar] [CrossRef]
- Cheng MH, Huang JJ, Wu CW, et al. The mechanism of vascularized lymph node transfer for lymphedema: natural lymphaticovenous drainage. Plast Reconstr Surg 2014, 133, 192e–198e. [Google Scholar] [CrossRef]
- De Brucker B, Zeltzer A, Seidenstuecker K, Hendrickx B, Adriaenssens N, Hamdi M. Breast Cancer-Related Lymphedema: Quality of Life after Lymph Node Transfer. Plast Reconstr Surg 2016, 137, 1673–1680. [Google Scholar] [CrossRef]
- Scaglioni MF, Arvanitakis M, Chen YC, Giovanoli P, Chia-Shen Yang J, Chang EI. Comprehensive review of vascularized lymph node transfers for lymphedema: Outcomes and complications. Microsurgery 2018, 38, 222–229. [Google Scholar] [CrossRef]
- Zeltzer AA, Anzarut A, Braeckmans D, et al. The vascularized groin lymph node flap (VGLN): Anatomical study and flap planning using multi-detector CT scanner. The golden triangle for flap harvesting. J Surg Oncol 2017, 116, 378–383. [Google Scholar] [CrossRef]
- Vignes S, Blanchard M, Yannoutsos A, Arrault M. Complications of autologous lymph-node transplantation for limb lymphoedema. Eur J Vasc Endovasc Surg 2013, 45, 516–520. [Google Scholar] [CrossRef]
- Sulo E, Hartiala P, Viitanen T, Mäki M, Seppänen M, Saarikko A. Risk of donor-site lymphatic vessel dysfunction after microvascular lymph node transfer. J Plast Reconstr Aesthet Surg 2015, 68, 551–558. [Google Scholar] [CrossRef]
- Viitanen TP, Mäki MT, Seppänen MP, Suominen EA, Saaristo AM. Donor-site lymphatic function after microvascular lymph node transfer. Plast Reconstr Surg 2012, 130, 1246–1253. [Google Scholar] [CrossRef]
- Dayan JH, Dayan E, Smith ML. Reverse lymphatic mapping: a new technique for maximizing safety in vascularized lymph node transfer. Plast Reconstr Surg 2015, 135, 277–285. [Google Scholar] [CrossRef]
- Becker C, Assouad J, Riquet M, Hidden G. Postmastectomy lymphedema: long-term results following microsurgical lymph node transplantation. Ann Surg 2006, 243, 313–315. [Google Scholar] [CrossRef] [PubMed]
- Chang EI, Masià J, Smith ML. Combining Autologous Breast Reconstruction and Vascularized Lymph Node Transfer. Semin Plast Surg 2018, 32, 36–41. [Google Scholar] [CrossRef] [PubMed]
- Chang, E.I. Optimizing Treatment of Breast Cancer Related Lymphedema Using Combined DIEP Flap and Lymphedema Surgery. Arch Plast Surg 2022, 49, 150–157. [Google Scholar] [CrossRef]
- Schaverien MV, Badash I, Patel KM, Selber JC, Cheng MH. Vascularized Lymph Node Transfer for Lymphedema. Semin Plast Surg 2018, 32, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Barreiro GC, Baptista RR, Kasai KE, et al. Lymph fasciocutaneous lateral thoracic artery flap: anatomical study and clinical use. J Reconstr Microsurg 2014, 30, 389–396. [Google Scholar] [CrossRef]
- Tinhofer IE, Meng S, Steinbacher J, et al. The surgical anatomy of the vascularized lateral thoracic artery lymph node flap-A cadaver study. J Surg Oncol 2017, 116, 1062–1068. [Google Scholar] [CrossRef] [PubMed]
- Coroneos CJ, Asaad M, Wong FC, et al. Outcomes and technical modifications of vascularized lymph node transplantation from the lateral thoracic region for treatment of lymphedema. J Surg Oncol 2022, 125, 603–614. [Google Scholar] [CrossRef] [PubMed]
- Visconti G, Bianchi A, Salgarello M, et al. Lymphatic Tissue Transfer: Ultrasound-Guided Description and Preoperative Planning of Vascularised Lymph Nodes, Lymphatic Units, and Lymphatic Vessels Transfers. J Pers Med 2022, 12. [Google Scholar] [CrossRef]
- Maldonado AA, Chen R, Chang DW. The use of supraclavicular free flap with vascularized lymph node transfer for treatment of lymphedema: A prospective study of 100 consecutive cases. J Surg Oncol 2017, 115, 68–71. [Google Scholar] [CrossRef]
- Mazerolle P, Meresse T, Gangloff D, Kolsi K, Dupret-Bories A. Vascularized lymph node transfer with submental free flap. Eur Ann Otorhinolaryngol Head Neck Dis 2020, 137, 73–77. [Google Scholar] [CrossRef] [PubMed]
- Paulus VAA, Winters H, Hummelink S, Schulten S, Ulrich DJO, Vasilic D. Submental flap for vascularized lymph node transfer; a CTA-based study on lymph node distribution. J Surg Oncol 2020, 122, 1226–1231. [Google Scholar] [CrossRef]
- Tzou CH, Meng S, Ines T, et al. Surgical anatomy of the vascularized submental lymph node flap: Anatomic study of correlation of submental artery perforators and quantity of submental lymph node. J Surg Oncol 2017, 115, 54–59. [Google Scholar] [CrossRef]
- Gustafsson J, Chu SY, Chan WH, Cheng MH. Correlation between Quantity of Transferred Lymph Nodes and Outcome in Vascularized Submental Lymph Node Flap Transfer for Lower Limb Lymphedema. Plast Reconstr Surg 2018, 142, 1056–1063. [Google Scholar] [CrossRef]
- Danforth R, Skoracki R. Intra-abdominal donors for vascularized lymph node transfer: an update and review. Plastic and Aesthetic Research 2021, 8, 48. [Google Scholar] [CrossRef]
- Kenworthy EO, Nelson JA, Verma R, Mbabuike J, Mehrara BJ, Dayan JH. Double vascularized omentum lymphatic transplant (VOLT) for the treatment of lymphedema. J Surg Oncol 2018, 117, 1413–1419. [Google Scholar] [CrossRef]
- Nguyen AT, Suami H, Hanasono MM, Womack VA, Wong FC, Chang EI. Long-term outcomes of the minimally invasive free vascularized omental lymphatic flap for the treatment of lymphedema. J Surg Oncol 2017, 115, 84–89. [Google Scholar] [CrossRef] [PubMed]
- Kraft CT, Eiferman D, Jordan S, Skoracki RJ. Complications after vascularized jejunal mesenteric lymph node transfer: A 3-year experience. Microsurgery 2019, 39, 497–501. [Google Scholar] [CrossRef] [PubMed]
- Boccardo F, Casabona F, De Cian F, et al. Lymphedema microsurgical preventive healing approach: a new technique for primary prevention of arm lymphedema after mastectomy. Ann Surg Oncol 2009, 16, 703–708. [Google Scholar] [CrossRef]
- Ciudad P, Escandón JM, Bustos VP, Manrique OJ, Kaciulyte J. Primary Prevention of Cancer-Related Lymphedema Using Preventive Lymphatic Surgery: Systematic Review and Meta-analysis. Indian J Plast Surg 2022, 55, 18–25. [Google Scholar] [CrossRef] [PubMed]
- Viviano SL, Neligan PC. Updates on Excisional Procedures for Lymphedema. Adv Wound Care (New Rochelle) 2022, 11, 419–427. [Google Scholar] [CrossRef]
- Chang DW, Dayan J, Greene AK, et al. Surgical Treatment of Lymphedema: A Systematic Review and Meta-Analysis of Controlled Trials. Results of a Consensus Conference. Plast Reconstr Surg 2021, 147, 975–993. [Google Scholar] [CrossRef]
Figure 1.
Lymphoscintigraphy of the upper limb. It depicts severe left lymphedema.
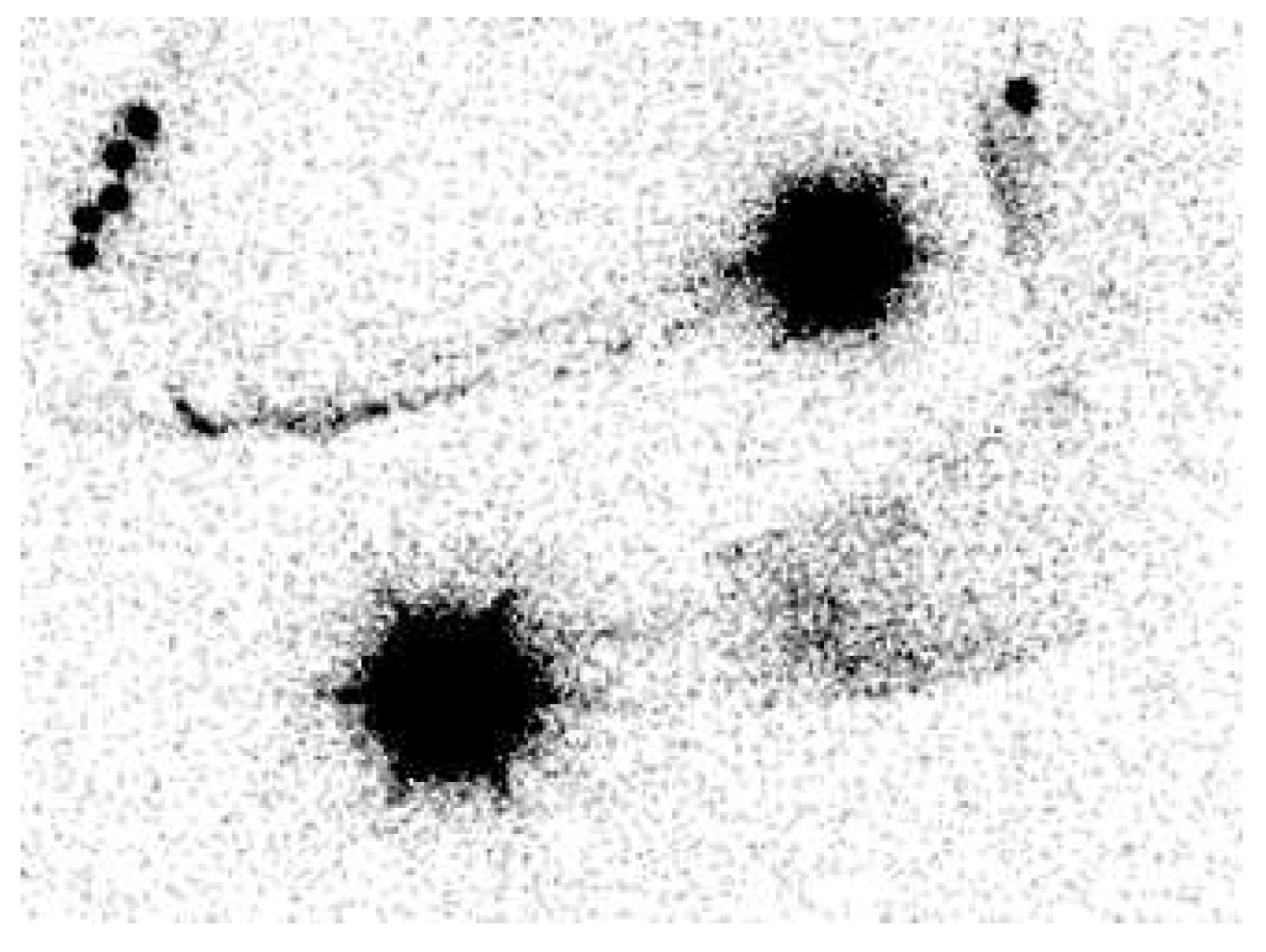
Figure 2.
Linear pattern demonstrated by ICG lymphography.

Figure 3.
Figure 3. Magnetic resonance lymphangiography provides anatomic delineation and 3D reconstruction images of lymphatics and adjacent veins. Long arrows=lymphatic channels, short arrows=vein, circle=crossing of both (=possible place of incision).
Figure 3.
Figure 3. Magnetic resonance lymphangiography provides anatomic delineation and 3D reconstruction images of lymphatics and adjacent veins. Long arrows=lymphatic channels, short arrows=vein, circle=crossing of both (=possible place of incision).
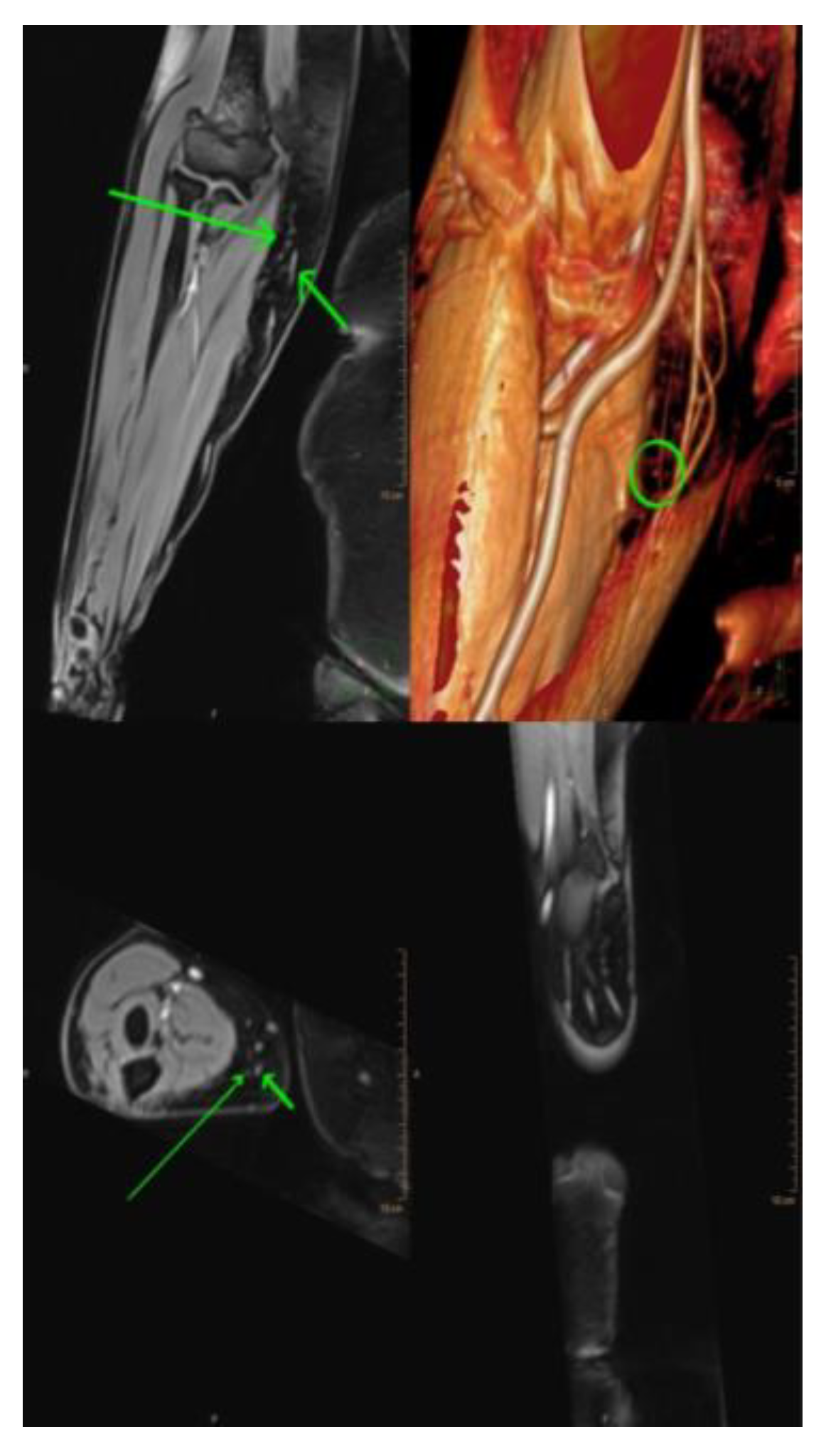
Figure 4.
LVA was performed successfully in an end-to-end fashion. The patent blue on the subdermal venule shows the patency of LVA.
Figure 4.
LVA was performed successfully in an end-to-end fashion. The patent blue on the subdermal venule shows the patency of LVA.
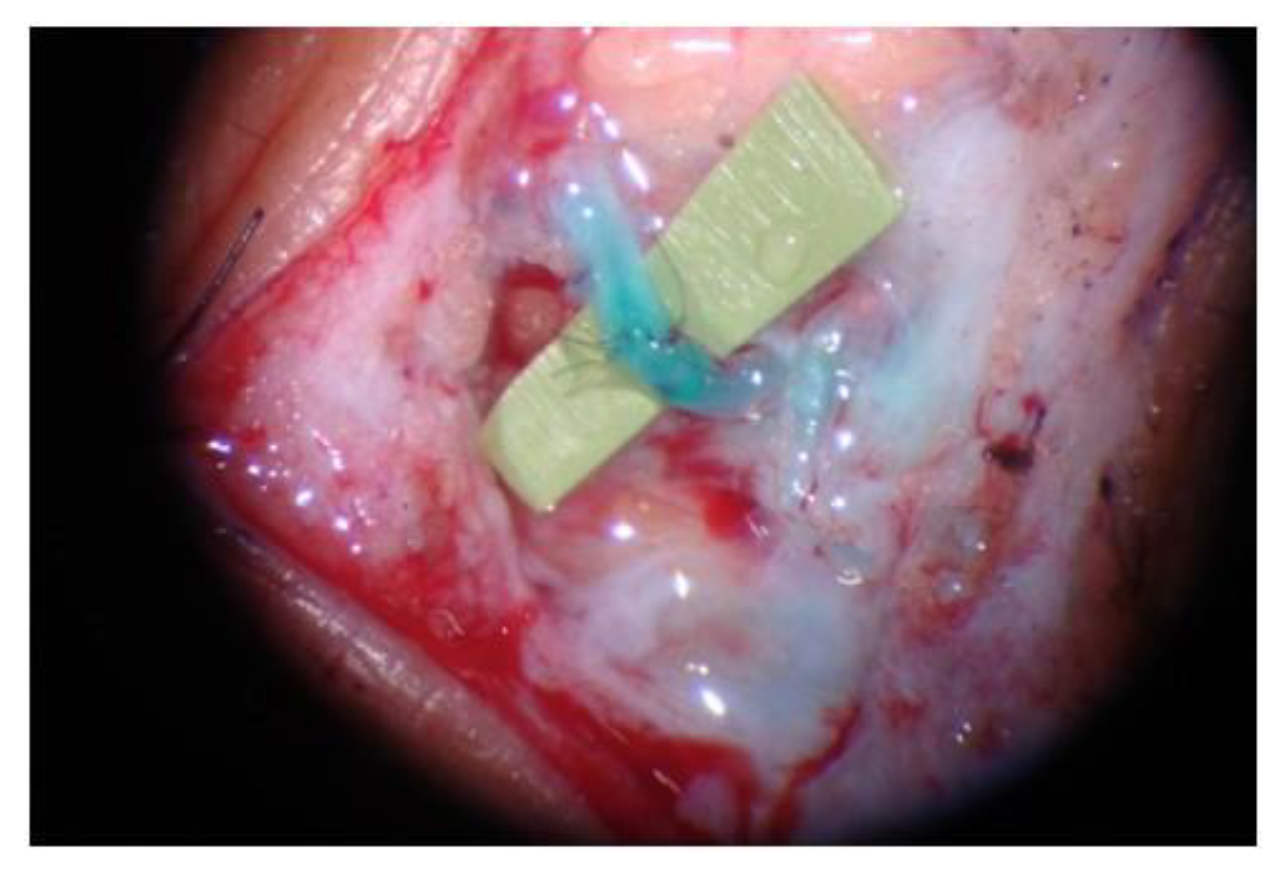
Figure 5.
(a) Patient with right upper extremity lymphedema stage 1; (b) Patient treated with 3 LVA. It was achieved a reduction in interlimb volume from 34% to 12%.
Figure 5.
(a) Patient with right upper extremity lymphedema stage 1; (b) Patient treated with 3 LVA. It was achieved a reduction in interlimb volume from 34% to 12%.
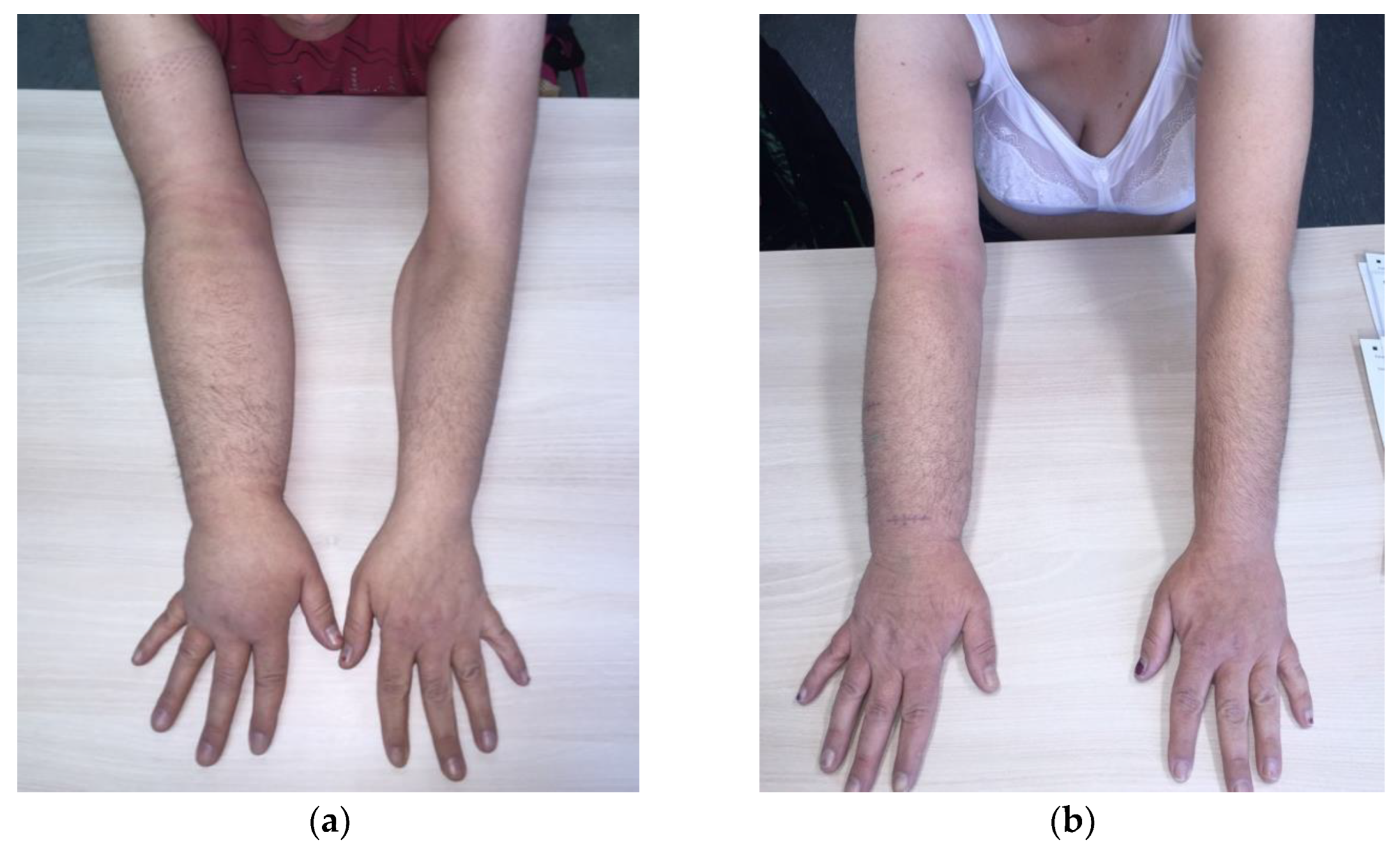

Table 1.
Overview of the imaging modalities and their advantages and limitations on evaluating the lymphatic system.
Table 1.
Overview of the imaging modalities and their advantages and limitations on evaluating the lymphatic system.
| Imaging modalities | Advantages | Limitations |
|---|---|---|
| LSG |
|
|
| ICG-L |
|
|
| MRL |
|
|
| SPECT/CT |
|
|
| UHF-US |
|
|
| PA imaging |
|
|
Table 2.
Characteristics of the vascularized lymph node flap options.
| VLNT | Advantages | Limitations |
|---|---|---|
| Groin flap |
|
|
| Lateral thoracic flap |
|
|
| Supraclavicular flap |
|
|
| Submental flap |
|
|
| Omental flap |
|
|
| Jejunal flap |
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



