Submitted:
17 June 2023
Posted:
19 June 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Public Health Officers' (PHO) experiences in reaction to the COVID-19 pandemic can be based on whether the PHO is passive or active. Therefore, the study’s objectives are to identify the types of experiences and analyse the predictors of proactive practical experiences in solving COVID-19 among PHOs in the upper southern region of Thailand. Methods: An explanatory mixed-methods approach was used to collect data, through questionnaires and online in-depth interviews. The study was conducted from August 4, 2020, to August 3, 2021. Results: The results included 60 PHOs from 60 PCUs in 6 provinces, with 41 (68.3%) females and an average age of 35.57 years (SD = 11.61). The PHOs’ knowledge, understanding, and participation experience aspects were mostly proactive rather than passive. Factors that significantly predicted proactive practical experiences included sex (ORadj = 1.52, 95% CI = 1.04–2.21), age (ORadj = 1.69, 95% CI = 1.16-2.48), married status (ORadj = 1.69, 95% CI = 1.16-2.48), education level (ORadj = 1.50, 95% CI = 1.02–2.20), and position for work (ORadj = 1.69, 95% CI = 1.16-2.48). Conclusions: PHOs’ knowledge, understanding, opinion, and participation experiences were significant predictors of practical experience. Primary health care systems should promote proactive experiences in all four aspects to increase proactive practical experiences.
Keywords:
public health officer
; COVID-19 solution
; proactive oractice
; mixed methods approach
; experience
; primary care unit
; Thailand
1. Introduction
The pandemic of COVID-19 has been a significant concern for healthcare providers worldwide, including Thailand. The Thai healthcare system seeks to rapidly identify and isolate infected patients, provide necessary care, and conduct contact tracing to prevent further transmission [1,2]. In addition, emphasis has been placed on efforts to prevent hospital infections and encourage people to take preventative measures, such as practising hand hygiene, wearing face masks, and getting tested for symptoms. Different provinces have implemented context-specific preventive measures while adhering to national guidelines [3,4]. Due to the work of the public health officer (PHO), the number of COVID-19 cases in Thailand dropped from a high of 188 recorded in a day (March 22, 2020) to a low of 15 on April 22, 2020 [5]. This shows how important the PHO’s job is.
During the pandemic in Thailand, the work of the PHO was important to the COVID-19 solution in the primary care unit (PCU). The Public Health Office (PHO), which is in charge of screening infected people, assessing risks, investigating diseases, putting in place measures for preventing and controlling infections, spreading information about risks, and making people more aware of the problem, is seen as the first line of defence against the problem. They were following and keeping an eye on the rules set out by the Ministry of Public Health to stop COVID-19. Making sure people refrain from going out, stay away from crowds, keep social distance, work from home, and wear masks when they leave the house. People returning from high-risk locations, both from abroad and from Bangkok and other provinces, were subjected to a 14-day quarantine at home, as well as efforts to prevent the virus from being imported from overseas [6,7].
Following the activities associated with the PHO’s duty mentioned above, this represents their COVID-19 experience. Roth and Jornet [8] define experience as the integration of a person’s knowledge, understanding, opinions, participation, and skills acquired through their learning process in response to events they have encountered at a particular time. This experience can be classified as either passive or active [9]. Passive experience involves gaining knowledge and understanding from reading, hearing, and visualising information from various media, whereas active experience involves the ability to define, plan, or present real-world actions. Therefore, PHO’s experiences in their PCU in reaction to the COVID-19 pandemic can be broken down into five categories: knowledge, understanding, opinion, participation, and practise. These categories are based on whether the PHO was passive or active. Activities like getting orders from the district public health office, listening to the COVID-19 situation report, watching announcements from different media, using incidence and prevalence rates on COVID-19, campaigning to educate and promote disease prevention measures, telling people about COVID-19 outbreaks in the community, making pamphlets to give out to people, putting up posters in the community, screening communities for COVID-19, investigating the disease, and reporting to the district public health office were all considered proactive [1,6,7]. However, government rules to address COVID-19 are an example of a passive experience [10].
In the past, there was no research pertaining to this level of experience and related factors among PHOs in Thailand. This research is distinguished by a model of experience evaluation that emphasises both quantitative and qualitative aspects. By employing an explanatory mixed methods study, this research aims to evaluate the level of experience and analyse the factor associated to proactive practical experience in addressing the COVID-19 pandemic among PHOs in PCUs from the six provinces in Thailand’s upper southern area. The findings will help the primary health care system adjust the determine measures, operational guidelines, and recommendations for resolving future outbreaks.
2. Materials and Methods
The research used an explanatory mixed-methods design, with the first part being a quantitative survey using questionnaires and the second part being qualitative research using the phenomenological study approach through in-depth interviews. The data were collected from public health officials who had experience solving COVID-19 problems among public health officers in the upper southern region of Thailand using purposive sampling. The study was conducted after obtaining approval from the Human Research Ethics Committee of Walailak University (No. WUEC-20-218-01), from August 4, 2020, to August 3, 2021.
2.1. Quantitative methods
2.1.1. Population and sample
In the upper southern region of Thailand, there are 302 primary care units distributed across 23 districts in seven provinces. The sample size of PHOs was determined using the G*Power 3.1 calculus program (http://www.gpower.hhu.de/en.html. 3.11.61) [11], with a test family of “exact” and a statistical test of “bivariate normal model,” with a significance level (α) of 0.05 and a power of 0.95. The program suggested a sample size of 60 PHOs. Stratified sampling was performed at the province and district levels, based on the sample size, followed by simple random sampling to select one PHO from each PCU using a purposive technique (Figure 1).
2.1.2. Instruments of quantitative approach
The study employed a quantitative design using questionnaires that demonstrated content validity (CVI = 0.96) and reliability (Cronbach’s alpha = 0.83). The questionnaire was developed from a literature review and had six sections. Apart from participant characteristics, knowledge, understanding, opinion, participation, and practical experience were measured using a Likert scale with five levels.
The study classified experiences into proactive and passive experiences based on Bloom’s cut-off point of 90% [12]. Proactive experience were determined by a percentage of correct answers of more than or equal to 90% (≥ 9 points), while passive experience were determined by a percentage lower than 90% (< 9 points).
2.1.3. Data analysis of quantitative
Representative characteristics of 60 participants were analysed for frequency, percentage, mean, and standard deviation. The types of experiences were analysed using a frequency percentage analysis of scores for each aspect of the experience. The factors associated with the practical experiences in solving COVID-19 problems among public health officers were analysed by univariate and multivariate statistics at the 95% confidence interval (95% CI) at a P-value significance <0.05 value.
2.2. Qualitative methods
2.2.1. Study design and participation
An in-depth interview was conducted as part of a phenomenological study to explore how individuals experience certain phenomena in their close environment and derive meaning from them. It is crucial to remember that each person’s phenomenology is distinct dependent on their experiences [13]. Therefore, the experiences of public health officers involved with COVID-19 solutions may differ and require a tailored approach.
2.2.2. Participant as the key informant
A total of eight public health officers from six provinces in the upper southern area of Thailand qualified for the in-depth interview. The study utilised purposive sampling techniques, including inclusion criteria such as public health officers actively involved in district roles and willing to participate in the interview. Exclusion criteria were applied, and any public health officer who felt uncomfortable during the interview was allowed to discontinue.
2.2.3. Guide of questionnaire for in-depth interview
Three experts validated the unstructured questionnaires used in the interviews, and their results showed a content validity index (CVI) value of 0.97. Due to the nature of the public health officers’ roles and responsibilities in preventing and controlling COVID-19 in their districts, the study divided the guide of open-ended questions into six main questions. These included: 1) What do you know about COVID-19 and your thinking about it? 2) Can you share your experiences regarding COVID-19 in your area of responsibility? 3) How have you addressed the COVID-19 situation in the areas you are responsible for? 4) Can you explain how you report on COVID-19 solutions? 5) What has been the response of the community you serve to COVID-19 solution? and 6) What are the problems, obstacles, and suggestions for solving the COVID-19 problem that you have encountered?
2.2.4. Data collection of in-depth interview
The research team informed the participants about the objectives of the study, obtained oral consent, and facilitated the public health officers’ views and experiences on COVID-19 solutions. Due to the pandemic situation, the researchers conducted interviews through telephone, line application, and face-to-face, depending on the participants’ availability. The telephone was used to establish a relationship with the participants, and interviews lasted between 30-45 minutes. If the data was unsaturated, the researchers set the next interview time according to the participants’ condition. For face-to-face interviews, the researchers followed COVID-19 prevention guidelines. The researchers used unstructured questionnaires for the interview and recorded the sound and tone of the public health officers’ responses.
2.2.5. Data analysis of qualitative approach
Various data analysis methods have been utilised in phenomenology research. In this study, thematic analysis was employed, with the five steps outlined by Braun and Clarke [14-16]. In each interview, the researcher interviewed the participants, analysed their responses within 24 hours, and made note of unclear points to be revisited with the same or next participant.
2.2.6. Trustworthiness
At the end of the qualitative data analysis, the researcher presented the results of the theme to the same eight public health officers so they could thematically review the interpretation of their response and validate it. This technique is the most important one to establish a study’s credibility [17].
3. Results
3.1. Characteristics information in quantitative method
The results from the self-administered questionnaire about personal data of district public health officers were 60 public health officers (60 primary care units (PCUs)), who were distributed in six provinces of the upper southern region of Thailand. The characteristics showed almost 41 (68.3%) females, an average age of more than or equal to 27 years, 40 (66.7%) (mean = 35.57; SD = 11.61 and range 22–59), a higher education of bachelor’s degree 48 (86.7%), and a public health scholar position 38 (63.3%). Half (30 (50.0%)) of the PHO have been in their current service position for < or ≥ 6 years (mean = 12.32, SD = 12.02, and range 1-38 years), and there are 11 (35.0%) COVID-19 patient cases in the district (Table 1).
Among the PHOs surveyed, the top 4 COVID-19 solution activities (Figure 2) with a score higher than 90% were as follows: 1) screening for COVID-19 in the community and conducting disease investigations (100.0%); 2) conducting campaigns to educate and promote disease prevention measures (95.0%); 3) communicating news of COVID-19 outbreaks in the community (93.2%); and 4) receiving orders from the district public health office (91.7%). Additionally, the following activities were also frequently performed: viewing announcements from various media, collecting information and submitting reports to the district public health office, creating pamphlets and posters for distribution in the community, using incidence and prevalence rates for COVID-19 as a reference, and improving environmental sanitation to prevent the spread of COVID-19 with a score below 90%.
3.2. Level of PHO’s Experience to solve COVID-19 in upper southern region, Thailand
Out of the 60 public health officers surveyed, 34 (56.7%) had categorised experiences that were at a proactive level, while 26 (43.3%) had experiences that were at a passive level. In terms of the specific experience aspects, their experiences in knowledge, understanding, and participation were almost exclusively at a proactive level, with frequencies (percentages) of 48 (80.0%), 38 (63.3%), and 32 (53.3%), respectively. However, their experiences of opinion were predominantly at a passive level, with a frequency (percentage) of 37 (61.7%). Furthermore, the experiences of practicality were equally distributed between proactive and passive levels, with frequencies (percentages) of 30 (50%) and 30 (50.0%), respectively (Figure 3).
3.3. Predictor of the proactive practical experiences to solve COVID-19 among PHOs in upper southern region, Thailand.
A study conducted among public health officers revealed that various factors were associated with having proactive practical experiences in addressing COVID-19 (Table 2). Male officers were found to have 1.52 times greater odds of having practical experiences compared to female officers (ORadj = 1.52, 95% CI = 1.04–2.21), and officers under the age of 27 had 1.69 times greater odds of having practical experiences compared to those who were 27 or older (ORadj = 1.69, 95% CI = 1.16–2.48). Single, divorced, or separated officers had 1.69 times greater odds of having practical experiences compared to married officers (ORadj = 1.69, 95% CI = 1.16-2.48), and officers with a bachelor’s degree had 1.50 times greater odds of having practical experiences compared to those with a master’s degree (ORadj = 1.50, 95% CI = 1.02-2.20). Public health practitioners had 1.69 times greater odds of having proactive practical experiences compared to public health scholars (ORadj = 1.69, 95% CI = 1.26–2.48). Additionally, PHOs with proactive knowledge, understanding, opinion, and participation experiences had significantly greater odds of having proactive practical experiences in solving COVID-19.
3.4. The theme of PHOs’ experiences in solving COVID-19 from a qualitative study
The eight public health officers from the upper southern region of Thailand who volunteered to participate comprised 4 females and 4 males, 2 of whom were single and 6 were married. In terms of education, 5 held bachelor’s degrees and 3 held master’s degrees. The age range of the participants was from 24 to 60 years old, with a mean age of 41.13 years (SD = 11.44). The participants had a range of experience in public health service, with the duration of service ranging from 1 to 40 years and a mean of 15.75 years (SD = 13.13). The number of patients under their care varied from 0 to 65, with a mean of 10 (SD = 22.60). The study identified 12 sub-themes from the questions asked related to the experiences of these public health officers in dealing with COVID-19. These are presented in Table 3.
4. Discussion
At the time of this investigation, there were eleven COVID-19 patient cases in the district. Meanwhile, as of July 17, 2020, 744 COVID-19 cases had been confirmed throughout southern Thailand [18,19], which was attributed to individuals from a cluster of COVID-19 patients in Iran and Malaysia travelling to the southern provinces of Thailand, Nakhon Si Thammarat and Surat Thani, in March 2020, and potentially exposed to a number of people. Between January 19 and 25, 2022, the highest rates of new COVID-19 cases were still identified in the southern tourist hotspots of Phuket and Phangnga [2]. However, Thailand’s primary health care (PHC) infrastructure played a significant role in preventing the spread of the COVID-19 virus. Today, the PHC has a highly developed network that connects to each sub-district via health promoting hospitals (HPH) and then to the household level via a network of village health volunteers (VHV) [20,21].
Among the COVID-19 solution activities mentioned, more than 90% of the PHOs in this survey believe that screening for COVID-19, education campaigns, sharing outbreak news, and adherence to district order are the most effective. In support, Ogboghodo et al. [22] stated that screening at the crucial interface and other facility ports of entry is a must for the quick identification and isolation of infected patients during outbreaks of highly infectious diseases such as the COVID-19 pandemic. Similarly, Grey et al. [23] mentioned that health and hygiene initiatives, encouraging individuals to change their behaviours, and reinforcing consistent messages are successful ways of lowering infection rates. It is crucial that communities recognise the virus as a health danger and follow the public health office’s orders for preventive actions to combat it. There will be widespread and terrible effects if people are unwilling to do this.
In the southern part of Thailand, almost all of the PHOs’ experiences with COVID-19 in terms of knowledge, understanding, and participation were at a proactive level. According to Geertshuis et al. [24], individuals with high proactive behaviour actively seek out and take advantage of many chances, show initiative, take action, and endure until their goals are met. They are driven and committed to making a difference in the lives of those around them. Health workers should be proactive agents of change whose knowledge protects populations from viral pandemics. Knowledge of health workers is crucial for efficient infection protection and control (IPC). Geberemariyam et al. [25] and Assefa et al. [26] found that a lack of knowledge of infection protection and control guidelines, as well as a lack of awareness of preventive indications during daily patient care and the potential risks of microorganism transmission to patients, are obstacles to solution activities. This will result in delayed diagnosis of new cases, infection dissemination, and inadequate infection control practises. Therefore, PHOs must be well-informed about the pathogen and disease in order to wage an effective war against the virus [27].
In addition, Cheng et al., [28] recognise the critical relevance of infection control readiness in the healthcare system based on their previous experiences with new respiratory illnesses. Subramaniam et al. [29] also said that the fact that workers do not take part in activities to find solutions is a big reason why people do not follow the rules. In this study, a lot of PHOs took part in solution activities by attending COVID-19-related network meetings, where they talked about ways to teach the public about COVID-19 and get the general public involved in bringing attention to COVID-19 guidelines. Likewise, health workers were proven to be effective in emergency management during the Ebola outbreak in Guinea, Sierra Leone, and Liberia by quickly identifying cases, as well as in pandemic preparedness by effectively communicating in a culturally relevant manner, educating and mobilising communities, contributing to surveillance systems, and bridging gaps in health service provision.
However, the majority of their experiences with opinion were passive. More than half of PHOs believe the disease to be terrifying since it cannot be controlled or prevented, it can result in death, and it poses a risk to their line of work. This is in line with what Ioannou et al. [30] found, that a large number of healthcare workers (HCWs) are also afraid of getting the virus and passing it to their families. This is a very important finding because anxiety and fear of getting COVID-19 may affect the quality of care given and may make health officers less willing to take part in solution activities. Contrary to this, Olateju et al. [31] found that despite participants’ awareness of the increased risk of COVID-19 exposure due to their role, they were still willing to work because they believed that exposure to diseases was an integral part of their job as healthcare workers. Again, a significant proportion of PHOs in this study are uncertain as to whether or not everyone should participate in COVID-19 prevention. Infection control should not be viewed as the responsibility of a select few individuals; rather, it is the result of a collective effort by all health care professionals [32] and the society as a whole.
Furthermore, the experiences of practicality were equally distributed between proactive and passive levels. Many are proactive in conducting on-site inspections to ensure compliance with COVID-19 guidelines, and reporting data to the district public health department, while some are passive in investigating diseases with people at risk of contracting COVID-19, and setting the plan to prevent and control COVID-19. In an optimal setting, health professionals should serve as health promoters. Putting a lot of effort into encouraging behaviour change by serving as role models, defining goals, and forming effective partnerships with stakeholders. By engaging in these activities, they help to strengthen connections between society and the healthcare system and reduce compliance dropouts [33].
The findings of this study conducted among public health officers revealed that gender, age, marital status, education level, and work position were associated with having proactive practical experiences in addressing COVID-19. For instance, male officers were found to have 1.52 times greater odds of having practical experience compared to female officers. This may be because most of the PHOs that were studied were female and many of them were married. Women reported being more likely than males to spend more time caring for children and likely handle the home obligations during the pandemic, which may reduce their practical experience [34]. In contrast, the majority of participants in a study by Regenold et al. [35] reported that their gender had no impact on their experiences as healthcare workers during COVID-19. Furthermore, compared to PHOs who were 27 or older, PHOs under 27 had 1.69 times the likelihood of having practical experience. Murman [36] claims that there are detectable declines in cognitive function associated with ageing. The most notable shifts are the decreases in cognitive functions including processing speed, working memory, and executive cognitive function that are necessary for making quick, well-considered decisions. Although, expertise gained throughout a lifetime is retained well into old age.
We also discovered that single, divorced, or separated PHOs were 1.69 times more likely to have practical experience than married officers. This is consistent with the findings of the Regenold et al. [35] study, in which a lot of health care employees claimed that mothers and fathers are put in an especially difficult situation when balancing work and home obligations. As previously stated, Mele et al. [34] found that healthcare workers who identified as female and had dependents under the age of ten experienced the highest levels of anxiety during the pandemic. The married PHOs’ household obligations and fear about infecting their family with COVID-19 may have limited their practical experience.
Accordingly, the eight PHOs interviewed to discuss the topic expressed their feelings. Many perceived COVID-19 to be a severe outbreak due to the lack of a specific treatment and its rapid spread. One PHO attributed the rapid spread of the infection in the southern district of Thailand to the reunification of international travelers with their families without screening. Amzat et al. [37] from Nigeria, also affirmed that the majority of those who entered the country did not adhere to the Nigerian Centre for Disease Control’s (NCDC) 14-day self-isolation recommendation. To effectively disseminate information about COVID-19, a line or Facebook network group is utilised to broadcast messages, posters and pamphlets are created and disseminated throughout the community, and public health officers and village health volunteers are involved in correcting practises. As one of the PHOs stated, it is essential to increase community understanding in order to effectively prevent COVID-19. Those who misunderstood the prevention guidelines and did not comprehend quarantine procedures will benefit greatly from this. Some people may mistake the symptoms of COVID-19 for the common cold, particularly if their immune system is powerful enough to mask the virus. The virus’ incubation period can last for several days, and asymptomatic individuals can still be carriers. However, laboratory tests are required to accurately detect the virus, as symptoms may be absent, making prevention challenging [38].
5. Conclusions
The findings of this study shows that proactive experience of the PHOs has significant influence on COVID-19 prevention and control. Through doing and personal experience, knowledge leads to a much deeper comprehension of a concept; therefore, understanding about the infection can help PHOs become more practical. This call for leadership to provide infection prevention and control training and education as required.
Author Contributions
Conceptualization, C.S.; methodology, S.S., and C.S.; formal analysis, C.S. C.K. and F.A.; investigation, K.S. and N.N.; resources, C.S.; data curation, Sh.S., and C.K.; writing—original draft preparation, C.S., F.A, and Sh.S.; writing—review and editing, S.S., C.S., and F.A., visualization, S.S.; supervision, C.S.; project administration, C.S.; funding acquisition, C.S., All authors have read and agreed to the published version of the manuscript.
Funding
The project was supported by the Excellent Centre for Dengue and Community Public Health (EC for DACH), School of Public Health, Walailak University.
Institutional Review Board Statement
In this research, research ethics were considered by the Human Research Ethics Committee of Walailak University, No. WUEC-20-218-01, given from August 4, 2020, to August 3, 2021. Participants could refuse and/or leave this research at any time. The data in the evaluation forms was kept confidential without specifying the participants’ names in the document.
Informed Consent Statement
Before the collecting data, informed consent was obtained from all subjects involved in the study; verbal consent was taken from each of the participants, and their names and identities were kept anonymous.
Data Availability Statement
All datasets are available upon request to the corresponding authors.
Acknowledgments
We gratefully thank the 60 public health officers in the 7 provinces of upper regional Thailand. Excellent Centre for Dengue and Community Public Health: EC for DACH, School of Public Health, Walailak University, and all respondents who cooperated well in this study.
Conflicts of Interest
The authors declare no conflict of interest and received both written and verbal information before they agreed to participate in the study. The funders had no role in the design of the study, in the collection, analysis, or interpretation of data, in the writing of the manuscript, or in the decision to publish the results.
References
- Thai Ministry of Public Health. Strategic Plan: Covid-19 Strategy: Managing the new wave of the Covid-19 Epidemic Ministry of Public Health, January 2021. Available online: https://ddc.moph.go.th/viralpneumonia/eng/file/main/en_Thailand%20Covid-19%20plan_MOPH_2021.pdf (accessed on 9 June 2023).
- World Health Organisation. COVID-19 Situation, Thailand; 2022. Available online: https://cdn.who.int/media/docs/default-source/searo/thailand/2022_01_26_tha-sitrep-220-covid-19.pdf?sfvrsn=bf4f76d6_3 (accessed on 28 May 2023).
- Tuangratananon, T.; Julchoo, S.; Phaiyarom, M.; Panichkriangkrai, W; Pudpong, N.; Patcharanarumol, W. et al. Healthcare providers’ perspectives on integrating NCDs into primary healthcare in Thailand: a mixed method study. Health Res. Policy Sys. 2021, 19, 139. [CrossRef] [PubMed]
- Thaprawat, P.; Greene, M.T.; Saint, S.; Kasatpibal, N.; Fowler, K.E.; Apisarnthanarak, A. Status of hospital infection prevention practices in Thailand in the era of COVID-19: Results from a national survey. Am J. Infect. Control. 2022, 50, 975–980. [Google Scholar] [CrossRef]
- Siree, O. Praise of the Thai medical team!! Hundred days to fight “COVID”, the number of patients continues to decline. The Bangkok Insight. 2020. Available online: https://www.thebangkokinsight.com/340658/ (accessed on 4 June 2023).
- Pipattanachat, V. Role of Health Professions Career by the Community Health Professions Act, B.E. 2556 (2013). Pub. Health & Health Laws J, 2016; 1. [Google Scholar]
- Thai Ministry of Public Health. Guidelines for surveillance and investigation of the novel coronavirus disease 2019. DDC EOC; 2020. Retrieved June 09, 2023 from. Available online: https://ddc.moph.go.th/viralpneumonia/file/g_km/handout004_26022020.pdf.
- Roth, W.M.; Jornet, A. Towards a theory of experience. Science Education. 2014, 98, 106–126. [Google Scholar] [CrossRef]
- Libertus, K.; Needham, A. Teach to reach: The effects of active vs. passive reaching experiences on action and perception. Vision Res. 2010, 50, 2750–2757. [Google Scholar] [CrossRef] [PubMed]
- Dwyer, D. Experiences of registered nurses as managers and leaders in residential aged care facilities: a systematic review. Int J. Evid. Based Healthc. 2011, 9, 388–402. [Google Scholar] [CrossRef]
- Cohen, J. Statistical power analysis for the behavioral sciences. Lawrence Erlbaum Associates, 1988.
- Harvey, K.; Horton, L. Bloom’s Human Characteristics and School Learning. The Phi Delta Kappan 1977, 59, 189–193. [Google Scholar]
- Laverty, S.M. Hermerneutic phenomenology and phenomenology: a comparison of historical and methodological considerations. Int. J. Qual. Methods 2003, 2, 21–35. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Thematic analysis. In Cooper H. (Ed.), Research designs. Amarican Psychological Association, 2012, 2.
- Suwanbamrung, C.; Kaewsawat, S. Public Health Students’ Reflection regarding the First Case of Coronavirus Disease 2019 in a University, Southern Thailand. J. Health Care and Res. 2020, 1, 1,182–192. [Google Scholar]
- Flick, U.; Lardorff, E.V.; Steinke, I. A companion to qualitative research. SAGE Publications. 2004. [Google Scholar]
- Rerkswattavorn, C.; Chanprasertpinyo, W. Knowledge, Attitudes, and Practices Toward the Coronavirus Disease 2019 (COVID-19) Pandemic in a Population Under Community-Wide Containment Measures in Southern Thailand. Infect. Drug Resist. 2022, 15, 6391–6403. [Google Scholar] [CrossRef] [PubMed]
- Kaewchandee, C.; Hnuthong, U.; Thinkan, S.; Rahman, S.; Sangpoom, S.; Suwanbamrung, C. The experiences of district public health officers during the COVID-19 crisis and its management in the upper southern region of Thailand: A mixed methods approach. Heliyon 2023, 9, e12558. [Google Scholar] [CrossRef]
- Triukose, S.; Nitinawarat, S.; Satian, P.; Somboonsavatdee, A.; Chotikarn, P.; Thammasanya, T.; Wanlapakorn, N.; Sudhinaraset, N.; Boonyamalik, P.; Kakhong, B.; Poovorawan, Y. Effects of public health interventions on the epidemiological spread during the first wave of the COVID-19 outbreak in Thailand. PLoS ONE 2021, 16, e0246274. [Google Scholar] [CrossRef] [PubMed]
- Sangpoom, S.; Adesina, F.; Saetang, J.; Thammachot, N.; Jeenmuang, K.; Suwanbamrung, C. Health workers’ capability, opportunity, motivation, and behavior to prevent and control COVID-19 in a high-risk district in Thailand. Rocz Panstw Zakl Hig. 2023, 74, 71–81. [Google Scholar] [PubMed]
- Ogboghodo, E.O.; Osaigbovo, I.I.; Obaseki, D.E.; Iduitua, M.T.N.; Asamah, D. , Oduware, E. et al. Implementation of a COVID-19 screening tool in a southern Nigerian tertiary health facility. PLOS Glob. Public Health. 2022, 2, e0000578. [Google Scholar]
- Gray, D.J.; Kurscheid, J.; Mationg, M.L.; Williams, G.M.; Gordon, C.; Kelly, M. et al. Health-education to prevent COVID-19 in schoolchildren: a call to action. Infect. Dis. Poverty 2020, 9, 81. [Google Scholar] [CrossRef]
- Geertshuis, S.; Jung, M.; Cooper-Thomas, H. Preparing Students for Higher Education: The Role of Proactivity. Int. J. Learn High Educ. 2014, 26, 157–169. [Google Scholar]
- Geberemariyam, B.S.; Donka, G.M.; Wordofa, B. Assessment of knowledge and practices of healthcare workers towards infection prevention and associated factors in healthcare facilities of West Arsi District, Southeast Ethiopia: a facility-based cross-sectional study. Arch. Public Health 2018, 76, 1–11. [Google Scholar]
- Assefa, J.; Diress, G.; Adane, S. Infection prevention knowledge, practice, and its associated factors among healthcare providers in primary healthcare unit of Wogdie District, Northeast Ethiopia, 2019: a cross-sectional study. Antimicrob. Resist. Infect. Control 2020, 9, 1–9. [Google Scholar] [CrossRef]
- Almohammed, O.A.; Aldwihi, L.A.; Alragas, A.M.; Almoteer, A.I.; Gopalakrishnan, S.; Alqahtani, N.M. Knowledge, Attitude, and Practices Associated With COVID-19 Among Healthcare Workers in Hospitals: A Cross-Sectional Study in Saudi Arabia. Front Public Health 2021, 9, 643053. [Google Scholar] [CrossRef]
- Cheng, V.C.C.; Wong, S.C.; To, K.K.W.; Ho, P.L.; Yuen, K.Y. Preparedness and proactive infection control measures against the emerging novel coronavirus in China. J. Hosp. Infect. 2020, 104, 254–255. [Google Scholar] [CrossRef] [PubMed]
- Subramaniam, C.; Shamsudin, F.M.; Zin, M.L.; Ramalu, S.S.; Hassan, Z. The influence of safety management practices on safety behavior: A study among manufacturing SMES in Malaysia. Int. J. Sup. Chain Mgt. 2016, 5, 148–160. [Google Scholar]
- Ioannou, P.; Karakonstantis, S.; Mathioudaki, A.; Sourris, A.; Papakosta, V.; Panagopoulos, P. et al. Knowledge and Perceptions about COVID-19 among Health Care Workers: Evidence from COVID-19 Hospitals during the Second Pandemic Wave. Trop. Med. Int. Health 2021, 6, 136. [Google Scholar] [CrossRef]
- Olateju, Z.; Olufunlayo, T.; MacArthur, C.; Leung, C.; Taylor, B. Community health workers experiences and perceptions of working during the COVID-19 pandemic in Lagos, Nigeria—A qualitative study. PLOS ONE 2022, 17, e0265092. [Google Scholar] [CrossRef] [PubMed]
- Shah, Z.; Singh, V.; Supehia, S.; Mohan, L.; Gupta, P.K.; Sharma, M.; Sharma, S. Expectations of healthcare personnel from infection prevention and control services for preparedness of healthcare organisation in view of COVID-19 pandemic. Med. J. Armed Forces India 2021, 77 (Suppl 2), S459–S465. [Google Scholar] [CrossRef]
- Rashid, J.; Taiwo, O.O.; Barraza-Roppe, B.; Lemus, M. Using Community Health Workers to Prevent Infectious Diseases in Women. Emerg. Infect. Dis. 2004; 10, e11. [Google Scholar]
- Mele, B.S.; Holroyd-Leduc, J.M.; Harasym, P.; Dumanski, S.M.; Fiest, K.; Graham, I.D. et al. Healthcare workers’ perception of gender and work roles during the COVID-19 pandemic: a mixed-methods study. BMJ Open 2021, 11, e056434. [Google Scholar] [CrossRef]
- Regenold, N.; Vindrola-Padros, C. Gender Matters: A Gender Analysis of Healthcare Workers’ Experiences during the First COVID-19 Pandemic Peak in England. Soc. Sci. 2021, 10, 43. [Google Scholar] [CrossRef]
- Murman, D.L. The Impact of Age on Cognition. Seminars in hearing 2015, 36, 111–121. [Google Scholar] [CrossRef]
- Amzat, J.; Aminu, K.; Kolo, V.I.; Akinyele, A.A.; Ogundairo, J.A.; Danjibo, M.C. Coronavirus outbreak in Nigeria: Burden and socio-medical response during the first 100 days. Int. J. Infect. Dis. 2020, 98, 218–224. [Google Scholar] [CrossRef]
- Ganyani, T.; Kremer, C.; Chen, D.; Torneri, A.; Faes, C.; Wallinga, J.; Hens, N. Estimating the generation interval for coronavirus disease (COVID-19) based on symptom onset data, March 2020. Euro Surveill. 2020, 25, 2000257. [Google Scholar] [CrossRef]
Figure 1.
Mapping 60 PCUs in 6 provinces, upper southern region, Thailand.
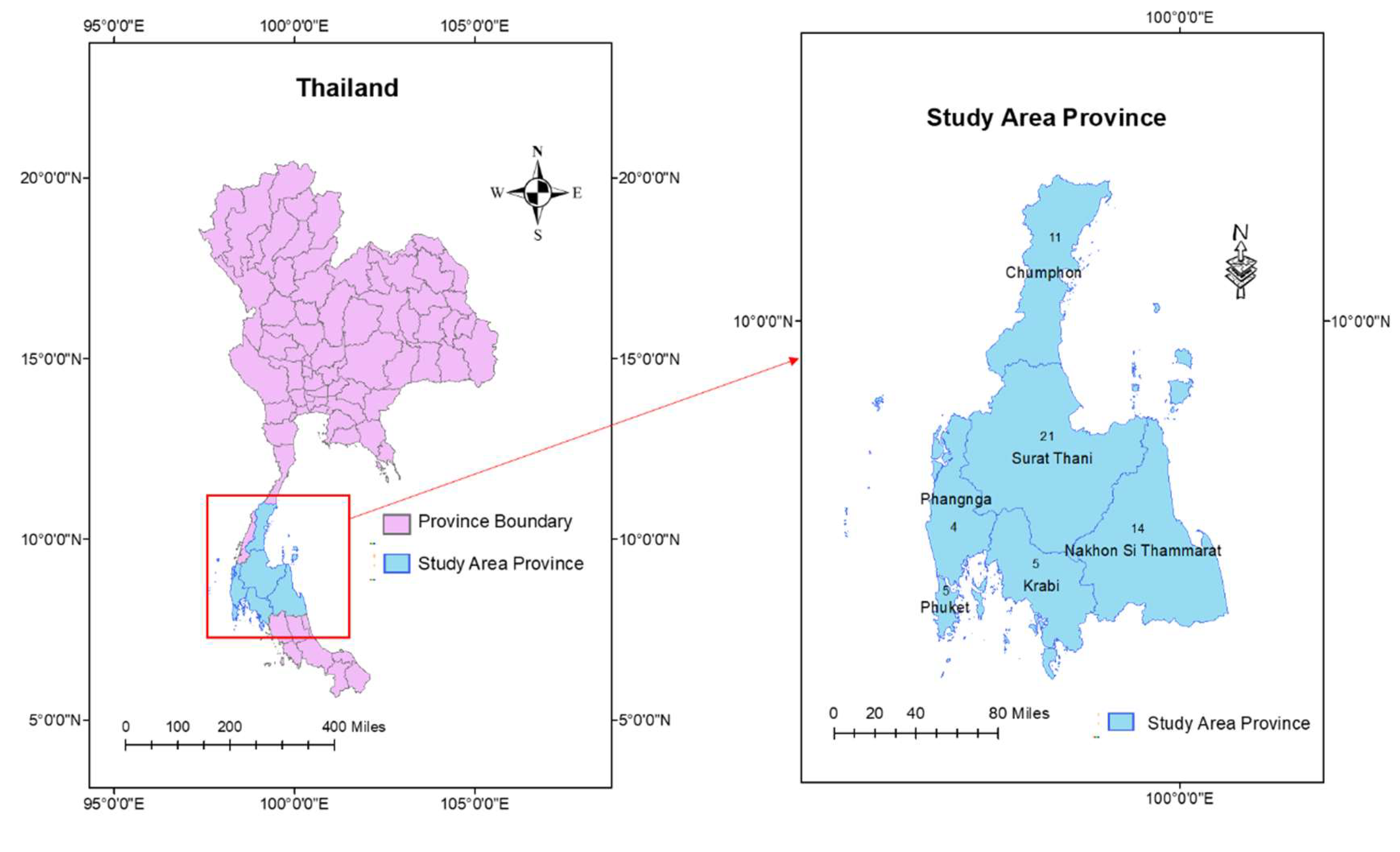
Figure 2.
PHO’s activities to solve COVID-19 in upper southern region, Thailand.
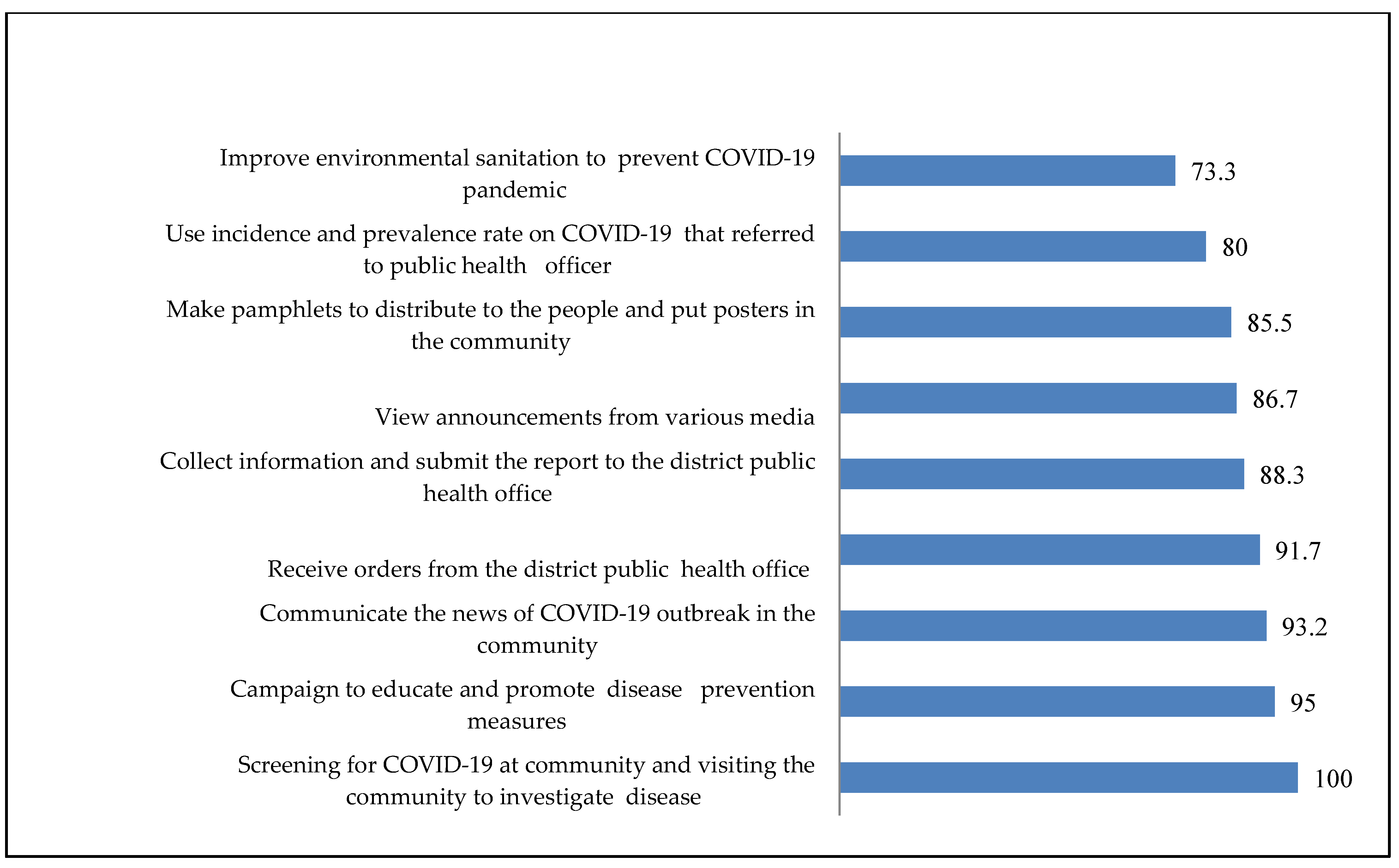
Figure 3.
PHO’s experience to solve COVID-19 in upper southern region, Thailand.


Table 1.
Characterize information of the 60 PHOs from 60 PCUs.
| Personal data | n (%) |
|---|---|
| Sex | |
| Male | 19 (31.7) |
| Female | 41 (68.3) |
| Age (Year old ) (S.D.) = 35.57 (11.61), Min = 22, Max = 59 | |
| < 27 | 20 (33.3) |
| ≥ 27 | 40 (66.7) |
| Marital status | |
| Single/divorced/separated | 29 (48.3) |
| Married | 31 (51.7) |
| Education level | |
| Bachelor’s degree | 48 (86.7) |
| Master’s degree | 12 (13.3) |
| Public health position | |
| Public Health Scholar | 38 (63.3) |
| Public Health Practitioner | 22 (36.7) |
|
Length of time worked in the current position (S.D.) = 12.32 (12.02), Min = 1, Max = 38 | |
| ≤ 6 year old | 30 (50.0) |
| > 6 year old | 30 (50.0) |
| COVID-19 patients in the area | |
| No | 49 (75.0) |
| Yes | 11 (25.0) |
Table 2.
Predictor of proactive practical experiences to solve COVID-19 among PHOs in the upper southern region of Thailand.
Table 2.
Predictor of proactive practical experiences to solve COVID-19 among PHOs in the upper southern region of Thailand.
| Factors | Proactive practical experiences (n=30) | ORa | ORbadj | 95%CI | p-value |
|---|---|---|---|---|---|
| Sex | |||||
| Male | 9 | 0.86 | 1.52 | 1.04-2.21 | 0.029* |
| Female | 21 | 1.00 | |||
| Age (years old) | |||||
| <27 | 11 | 1.35 | 1.69 | 1.16-2.48 | 0.006* |
| ≥27 | 19 | 1.00 | |||
| Marital status | |||||
| Single/divorced/separated | 12 | 0.51 | 1.69 | 1.16-2.48 | 0.006* |
| Married | 18 | 1.00 | |||
| Education level | |||||
| Bachelor’s degree | 24 | 1.00 | 1.50 | 1.02-2.20 | 0.040* |
| Master’s degree | 6 | 1.00 | |||
| Position for work | |||||
| Public Health Practitioner | 23 | 3.28 | 1.69 | 1.16-2.48 | 0.006* |
| Public Health Scholar | 7 | 1.00 | |||
| Length of time worked in the current position | |||||
| > 6 year old | 17 | 1.71 | 0.93 | 0.60-1.46 | 0.829 |
| ≤ 6 year old | 13 | 1.00 | |||
| Presence of COVID-19 patients in the area | |||||
| No have | 25 | 1.25 | 1.24 | 0.84-1.82 | 0.301 |
| Have | 5 | 1.00 | |||
| Knowledge experience | |||||
| Proactive | 24 | 1.00 | 1.65 | 1.13-2.40 | 0.008* |
| Passive | 6 | 1.00 | |||
| Understanding experience | |||||
| Proactive | 23 | 3.76 | 1.47 | 1.01-2.14 | 0.045* |
| Passive | 7 | 1.00 | |||
| Opinion experience | |||||
| Proactive | 7 | 1.22 | 1.48 | 1.01-2.21 | 0.046* |
| Passive | 23 | 1.00 | |||
| Participationexperience | |||||
| Proactive | 24 | 11.00 | 1.58 | 1.08-2.31 | <0.017* |
| Passive | 6 | 1.00 | |||
* p-value < 0.05, Goodness of fit = 0.636, Adjusted for Education level and Position for work; aUnivariate analysis, Chi-Square test, bMultivariate analysis, Multiple logistic regression
Table 3.
Sub-theme, meaning, and responses from the 8 PHOs’ experiences in upper Souhern region, Thailand.
Table 3.
Sub-theme, meaning, and responses from the 8 PHOs’ experiences in upper Souhern region, Thailand.
| Sub-themes | Meaning | Responses |
|---|---|---|
| Perceptions about the pandemic and awareness of COVID-19. | Significant impact on the world.
|
It was a pretty serious outbreak because there was no specific cure and it happened so quickly. In the infected area, there is a spread of COVID-19 infection among those who returned from travel and reunited with people at home (PHO1). |
| COVID-19’s knowledge leads to standard practice and guidelines. | Educating people on preventive measures and control strategies:
|
It began with forming a team with a network to create a Facebook and video on the online application to publicise and educate people in various places, such as mosques, schools, government service facilities, and hotels. Distributing leaflets, and pasting posters in the community as an education program. This highlights the beginning of the program’s implementation process (PHO5). Preventing and controlling COVID-19 in quarantine areas, promoting mask-wearing, and social distancing in the public” (PHO1). |
| A careful understanding of COVID-19 solutions is necessary | People must comprehend the public health officer’s methods for preventing COVID-19.
|
During the first phase of the pandemic, people misunderstood the prevention guidelines and did not understand quarantine procedures. They entered the village without notifying their public health officer and bypassed checkpoints set up by primary care units, entering the community through natural channels. It is crucial to enhance people’s understanding in the community to effectively prevent COVID-19” (PHO6). |
| Recognizing the nature and severity of COVID-19 | Understanding the symptoms associated with the virus:
|
As previously mentioned, “COVID-19 is a severe disease that can cause damage to the lungs and lead to death. Although death may not occur, individuals may still experience lasting symptoms that affect their daily lives. Therefore, if an infection does occur, it must be taken care of to prevent potential complications (PHO4). |
| COVID-19 impacts lifestyle and quality of life | Individuals returning from high-risk areas must be quarantined and separated from their families. Not visiting others while sick |
It has an impact on the way of life of people in the area, with long-term effects on the economy, society, and the livelihoods of people in all areas (PHO5). |
|
Respond to and trust public health officials to solve COVID-19 |
To trust and cooperate with public health officials to combat COVID-19. | A successful process involves participation from all sectors. When a disease outbreak occurs, everyone tends to rely solely on public health officials to handle it. However, with the prevalence of COVID-19, all sectors must contribute to prevention and control efforts to improve outcomes. If public health officials are the only ones responsible, controlling the disease becomes challenging. Making everyone a stakeholder in preventing and controlling the disease is crucial (PHO 5). |
| Establishment of a collaborative network of stakeholders to address the COVID-19 pandemic. | The cooperation between various stakeholders, such as government agencies, private organizations, and the local community, to tackle the challenges posed by COVID-19. | The network of communities begins at the district level, including the district public health office, sub-district health center, village head, and village health volunteer, all of whom participate in the collaborative effort. Coordination with the network of communities involves writing letters to request support and assistance to fill any remaining gaps (PHO 7). |
| Stakeholders’ contribution to spreading awareness and monitoring COVID-19 treatment |
|
If companies provide alcohol, it can be distributed to schools, community organizations for funeral use, and placed in various locations in the community. It can also serve as a model for villagers. Knowledge is shared by transmitting it to over 130 community organizations, and each responsible community organization will then pass on the knowledge about COVID-19 prevention (PHO2). |
| COVID-19 screening and referral checkpoints. | Establishing checkpoints in various locations, such as schools, hotels, temples, mosques, and village extraction points. | If someone in quarantine has a suspected disease, we screen them and send them to the district hospital for investigation. For the common people in the community, there were checkpoints at the screening points in the village. This indicates the importance of taking proactive measures to prevent the spread of COVID-19 in the community (PHO3). I have been involved in every aspect of combating COVID-19, from setting up screening and referral checkpoints in schools, hotels, temples, and mosques to working together to prevent the spread of the disease, providing knowledge, monitoring and taking care of high-risk groups in isolation for 14 days, and searching for infected patients (PHO6). |
| Collaboration and sharing opinions to improve solutions | The process of working together and gathering ideas from different communities to find solutions to problems. | We work with network leaders, the local administration organization head, and the district public health office to ensure adequate supplies. The local administration organization will provide support for food, and the primary care unit of the public health office will continue to provide COVID-19-related knowledge to the community (PHO8). |
| Conducting community examinations, follow-ups, and reporting | The process of implementing an operational plan to monitor and track individuals who may have been exposed to COVID-19 in the community. | The operational plan creates group lines for each group in the community and brings people at risk into the group line to report symptoms for 14 days. If there is no confirmed case, that person will be immediately removed from the group line (PHO1). |
| Today’s practical prevention and control lead to future solutions | Proactive plan | At first, there is a passive plan, but when there is a COVID-19 patient, the plan changes to a proactive plan, such as the meeting of the district committee every week to adjust the plan, setting up additional checkpoints to screen employees. For the second round, there are meetings with all stakeholders, such as the local government and the police department, to solve the problem (PHO5). |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



