Submitted:
16 June 2023
Posted:
16 June 2023
You are already at the latest version
Abstract
Hypertension and arterial stiffness are the main factors contributing to cardiovascular disease. L-citrulline, a nitric oxide precursor, has been proposed as a blood pressure-lowering intervention. This study aimed to investigate the impact of L-citrulline on central and peripheral blood pressure, arterial stiffness, and muscle oxygenation at rest and during an isometric knee extension exercise protocol. Twelve older males received 6 g of L-citrulline or a placebo for six days using a double-blind crossover design. Blood hemodynamics parameters (i.e., arterial and brachial systolic and diastolic blood pressure, mean arterial pressure, pulse pressure, heart rate), arterial stiffness (i.e., augmented pressure, augmentation index, forward, backward wave pressure and carotid-femoral pulse wave velocity) and muscle oxygenation [i.e., oxyhemoglobin (Δ[O2Hb]) and deoxyhemoglobin (Δ[HHb]), total hemoglobin concentration (Δ[tHb]) and tissue saturation index (TSI%)], were measured at baseline, post-supplementation and during isometric exercise. No significant effects of L-citrulline supplementation were observed at rest or during exercise on blood pressure, arterial stiffness, and muscle blood flow. Both central and peripheral blood pressure were increased during the exercise, which is consistent with isometric contractions. The results of the present study question the efficacy of short-term L-citrulline in decreasing blood pressure at rest or attenuating blood pressure increases during isometric exercise.
Keywords:
nitric oxide
; dietary supplements
; endothelium function
; hypertension
; cardiovascular disease
; blood flow
1. Introduction
Cardiovascular disease is the number one cause of morbidity and mortality worldwide [1]. Several mechanisms have been identified as contributors to cardiovascular disease, including hypertension [2], endothelial dysfunction [3], and arterial stiffness [4]. Elevated blood pressure appears to trigger arterial stiffness, whereas increased arterial stiffness is associated with blood pressure progression [2,3,4], indicating a vicious cycle that contributes to an elevated risk of developing cardiovascular disease. Indeed, hypertension and arterial stiffness have been proposed as independent risk factors for cardiovascular conditions in the general population [5,6], further highlighting their clinical relevance.
Nitric oxide is a critical signaling molecule and a potent vasodilator that regulates vascular endothelial function [7,8]. In addition, nitric oxide is essential to skeletal muscle function [9] by improving oxygen supply and metabolism [10] and redox status [11]. In the human body, nitric oxide is mainly generated through two main pathways: i) endothelial nitric oxide synthases, which utilize oxygen and L-arginine to synthesize nitric oxide and L-citrulline, and ii) the nitrate-nitrite-nitric oxide reduction pathway, which is stimulated during low oxygen availability or hypoxia [12]. Nitric oxide regulates vascular function by activating the soluble guanylate cyclase pathway in the vascular smooth muscle cells [17], resulting in smooth muscle relaxation, vascular wall expansion, and improved blood flow [7,8].
Considering the pivotal role of nitric oxide in cardiovascular function and blood flow [7], supplementation with nitric oxide precursors like L-citrulline and L-arginine has been widely used to enhance nitric oxide bioavailability [13,14]. While L-arginine supplementation seemed to be the first option in this direction, L-arginine is highly degraded in the liver [15] and impairs nitric oxide synthesis [16]. Moreover, high levels of L-arginine may stimulate the enzyme arginase, leading to increased L-arginine catabolism [17]. In contrast, L-citrulline, a byproduct of nitric oxide synthesis via L-arginine oxidation, is efficiently recycled to L-arginine in the kidneys through the enzymes arginosuccinate synthase and arginosuccinate lyase, facilitating nitric oxide bioavailability [18]. Interestingly, oral supplementation of L-citrulline remains largely intact in the intestine and liver and is directly transported to the kidneys [19], resulting in higher plasma levels of L-arginine than direct supplementation with L-arginine [20]. Therefore, L-citrulline has been proposed as a potential non-pharmacological agent to enhance nitric oxide bioavailability, promoting cardiovascular health [21,22]. It's worth mentioning that pharmacokinetic studies have shown that short-term L-citrulline supplementation is safe and well tolerated [20].
L-citrulline has shown promising results as a blood pressure-lowering nutritional intervention, as it has been reported to reduce resting blood pressure [23,24,25,26]. These positive effects might be attributed to increased vasodilation as a result of higher plasma L-arginine concentrations and enhanced nitric oxide bioavailability [21,22]. Furthermore, a recent meta-analysis [27] has demonstrated a more significant effect of L-citrulline supplementation on non-resting but transient arterial pressure changes induced by exercise or cold exposure. This evidence is noteworthy as arterial pressure elevation during exercise is often not controlled by antihypertensive medication, and it has been identified as an independent risk factor for cardiovascular events and mortality [28]. Exercise-induced increases in blood pressure can be caused by sympathetic and muscle metaboreflex-mediated vasoconstriction, an attempt of the body to increase blood flow to the working muscles [29]. However, the heterogeneity of the relevant studies (e.g., different supplementation doses, duration, and population under investigation) limits the ability to draw definitive conclusions regarding the effects of L-citrulline supplementation, and further research is required.
Even though several studies have examined the effect of oral L-citrulline supplementation on blood pressure and arterial stiffness, evidence has been limited to resting conditions or following cold pressure exposure. The present study investigated the impact of a six-day L-citrulline supplementation on aortic and brachial blood pressure, arterial stiffness, and muscle blood flow at rest and after an acute isometric resistance exercise protocol in older adults. Acute isometric knee extensors exercise was used to attenuate hemodynamics inducing significant increases in blood pressure [29]. We hypothesized that L-citrulline supplementation would have beneficial effects on blood pressure and arterial stiffness at rest. Additionally, during exercise, we expect that L-citrulline supplementation would attenuate the anticipated increases in blood pressure and enhance blood flow to the working muscles.
2. Materials and Methods
2.1. Participants
Twelve healthy older males were recruited to participate in this study. Table 1 presents participant anthropometrics. Participants were informed of the purpose of the study and methods used, providing written consent. The participants were included in this study if they were healthy and had no history of musculoskeletal injury in the legs during the previous six months. They were instructed to refrain from vigorous physical activity for 48 hours before the testing sessions. They were prohibited from drinking alcohol or caffeine within the last 24 hours. Volunteers were non-smokers and received no medication or nutritional supplements in the previous three months before their participation in the study. Researchers trained and motivated the participants to record their food intake for two days before the first session of the isometric exercise protocol. Participants were instructed to use that record and follow the same food intake before the second exercise session. Also, Participants were asked to maintain their usual lifestyle, including diet and physical activity, throughout the study.
2.2. Anthropometry
Prior to each trial, body mass was measured to the nearest 0.1 kg using an analogue balance scale (Seca 710, Hamburg, Germany), and height was recorded to the nearest 1 cm using a stadiometer (Seca 208, Hamburg, Germany). Using the seven skinfolds method and the Siri equation, the body-fat percentage was evaluated using a Harpenden Skinfold Caliper (John Bull, St. Albans, United Kingdom).
2.3. Experimental Design
This study was a randomized, double-masked, counterbalanced crossover placebo-controlled design. The experimental setup is shown in Figure 1. We provided a complete familiarization of the testing procedure before the data collection. Participants' anthropometric characteristics and maximum voluntary isometric contraction (MVIC) of their right knee extensor muscles were measured on the first visit.
On the second visit, participants visited the laboratory to perform the first session of isometric exercise. Before the exercise session, baseline measurements were performed, including hemodynamic parameters, aortic pulse wave analysis, arterial stiffness, and muscle blood flow. Then, using a double-masked method, participants were randomly assigned to receive 6 g (3 g every 12 h) of L-citrulline (Now, L-citrulline Pure Powder, Bloomingdale, IL) or a placebo (maltodextrin) daily for six days, starting from the next day after the visit (first treatment period). L-citrulline or placebo were in liquid form in identical bottles. After completing the six days of supplementation, participants returned to the laboratory, and the same outcome measures were recorded. Testing sessions were performed within 12 to 14 hours after the participants consumed the last dose of L-citrulline or placebo the night before to avoid the acute effects of the supplementation [20].
Then the participants underwent a two-week wash-out period to avoid any potential carryover effects, after which the second 'treatment' period started (placebo or L-citrulline) and followed the same procedures and measurements.
2.4. Blood Hemodynamics
After ten minutes of rest in the seated position in a quiet room with the temperature set at 24 °C, blood hemodynamics were measured in duplicates using the SphygmoCor Xcel device (AtCor Medical, Sydney, Australia). Outcome measures included aortic and brachial systolic blood pressure (SBP), diastolic blood pressure (DBP), mean arterial pressure (MAP), in addition to aortic pulse pressure (PP), and heart rate (HR). Hemodynamic parameters were measured at baseline, before supplementation, post-supplementation, and during the second minute of the isometric knee extension exercise. All measurements took place in the morning between 08:00-10:00.
2.5. Arterial Pressure Waveform Analysis and Pulse Wave Velocity
Sphygmocor Xcel was used to analyze arterial pressure waveform. Briefly, with the participants seated, a conventional cuff oscillometer was tailored to the right arm centered over the brachial artery. The inflation began automatically through the device's software for evaluating brachial systolic and diastolic pressure. Then the cuff deflated and inflated again below diastolic pressure to get a volumetric displacement signal representing the peripheral vascular waveform [30]. The parameters used in the study for the waveform analysis were augmented pressure (AP), augmentation index (AIx), forward (Pf), and backward (Pb) wave pressure. Similarly, these parameters were measured at baseline before supplementation, post-supplementation, and during the second minute of the isometric exercise of the knee extensors muscles.
Carotid-femoral pulse wave velocity (cfPWV) was measured using the same equipment and method [30] to assess arterial stiffness. The examiner fitted a femoral cuff to the upper side of the right thigh, and simultaneously a tonometry was placed over the participant's right carotid artery. The cfPWV was calculated as the transit time between the femoral and carotid pulse. Velocity measurement was calculated as the pulse wave difference in transit time between the upper side of the femoral cuff and the carotid artery, divided by the distance. The distance between the upper side of the femoral cuff and the carotid was measured with a validated measuring tape by subtracting the distance from the carotid to the suprasternal notch. cfPWV was measured pre and post-supplementation.
2.6. Muscle Oxygenation and Blood Flow
Near-infrared spectroscopy (NIRS) was used to non-invasive evaluate vastus lateralis oxygenation and blood flow at baseline pre-supplementation, post-supplementation, during isometric exercise, and after three minutes of recovery (PortaMon, Artinis Medical Systems, Elst, Netherlands). The measurement was conducted as previously described [31]. During exercise, muscle oxygenation and blood flow were recorded at the end of the first and second minutes. The device continuously recorded regional tissue oxygenation; thus, the data from the last 30 seconds (i.e., 30 to 60 seconds for the first minute and 90 to 120 seconds for the second minute) were averaged and used for subsequent analysis. The outcome measures obtained were oxyhemoglobin (Δ[O2Hb]) and deoxyhemoglobin (Δ[HHb]), which represents the dynamic balance between muscle oxygen delivery and extraction in the evaluated muscle. Total hemoglobin concentration (Δ[tHb]) was calculated as the sum of O2Hb and HHb, representing changes in microvascular blood flow. The tissue saturation index (TSI%) was also measured, reflecting muscle oxygenation and saturation balance.
2.7. Isometric Knee Extensors Exercise
During the participant's first visit, their MVIC of the right leg knee extensor muscles was measured using an electronic dynamometer (K-Link, Kinvent, Montpelier, France) which is a dynamometer used in the evaluation and rehabilitation of muscle strength that provides real-time feedback [32].
Participants were seated on an adjustable chair with their legs dangling and their knees bent to 90o. A strap attached to a solid bar was connected to the device and fitted around the participants' right ankle. Participants were then asked to push forward (straighten their knee) as hard as possible for five seconds without moving their trunks. Three trials were recorded, and the data was stored using the KFORCE APP (Kinvent, Montpelier, France). The average of the two closest values was calculated as the MVIC.
After assessing knee extensor MVIC, the researchers conducted the isometric exercise protocol based on each participant's MVIC. The exercise protocol consisted of two minutes of isometric exercise of the right knee extensor muscles at 30 % of their MVIC. The setup was the same as the one used during the evaluation of MVIC. Visual feedback was provided to the participants through a tablet screen during the exercise to ensure the desired force was achieved. After the end of the test, participants remained seated for three minutes for recovery.
2.8. Statistical Analysis
Data are presented as means and standard deviations (SD). Normal data distribution was tested and confirmed using the Shapiro-Wilk test for all dependent variables. A two-way repeated-measures ANOVA test ((group (L-citrulline vs. placebo) × time (baseline, post supplementation, and post isometric exercise)) was performed for aortic and brachial SBP, DBP, MAP, HR, AP, AIx, Pf, Pb, and cfPWV. A second two-way repeated-measures ANOVA test was performed for Δ[O2Hb], Δ[HHb], Δ[tHb], and TSI% ((group (L-citrulline vs. placebo) × time (baseline, post-supplementation, at the end of the first and the second minute of exercise and three minutes post-exercise during recovery)). If a significant interaction was found, pairwise comparisons were performed using the Sidak test. Statistical significance was accepted, a priori, at p < 0.05. Data were analyzed using the SPSS 25 statistical package (SPSS Inc., Chicago. IL).
3. Results
3.1. Blood Hemodynamics
No statistically significant condition by time interaction or main effect of condition was found for aortic or brachial SBP, DBP, MAP, and HR. However, a significant main effect of time was found for all parameters (Table 2). Specifically, both conditions exhibited similar increases during isometric exercise compared to post-supplementation for aortic SBP (L-citrulline condition: +20.8 mmHg; 95% CI [5.1, 36.4], and placebo condition: +21.3 mmHg; 95% CI [5.6, 37.0] and for aortic DBP (L-citrulline condition: +14.4 mmHg; 95% CI [4.4, 24.3] and placebo condition: +13.4 mmHg; 95% CI [3.4, 23.3]. Similar increases for both conditions were also found for brachial SBP and DBP (L-citrulline condition: +20.0 mmHg; 95% CI [5.6, 34.3] and placebo condition: +23.9 mmHg; 95% CI [9.5 38.2] and (L-citrulline condition: +12.5 mmHg; 95% CI [−0.2, 25.0], and placebo condition: +13.1 mmHg; 95% CI [0.6, 25.7]) respectively. For MAP, similar increases were observed for both conditions (L-citrulline condition: +17.0 mmHg; 95% CI [7.2, 26.3], and placebo condition: 16.6 mmHg; 95% CI [7.2, 26.3]). For HR, a significant main effect of time was found with similar increases in both conditions (L-citrulline condition: +14.4 bpm; 95% CI [8.5, 20.3], and placebo condition: 12.7 mmHg; 95% CI [6.8, 18.6]). No significant main effect of time, condition, or condition-by-time interaction was found for aortic PP. The percentage changes in blood hemodynamic parameters during exercise compared to the pre-exercise values are presented in Figure 2.
3.2. Arterial Pressure Waveform Analysis and Pulse Wave Velocity
No statistically significant main effect of time, condition, or condition-by-time interaction was found for AP, AIx, Pf, Pb, and cfPWV (Table 3).
3.3. Muscle Oxygenation and Blood Flow
Regarding muscle oxygenation and blood flow indices, neither a main effect of condition nor a condition by time interaction was found in Δ[O2Hb] (p = 0.845 and p = 0.517, respectively), Δ[HHb] (p = 0.710 and p = 0.127, respectively), Δ[tHb] (p = 0.888 and p = 0.891, respectively), and TSI% (p = 0.408 and p = 0.644, respectively) between L-citrulline and the placebo measured in vastus lateralis muscle (Figure 3A–D). However, a significant main effect of time was found for Δ[O2Hb] (p < 0.001), Δ[HHb] (p < 0.001), Δ[tHb] (p = 0.002), and TSI% (p < 0.001). More specifically, isometric exercise induced a decrease in Δ[O2Hb] during the first and the second minute in both the L-citrulline (at first minute: −3.9 μΜ; 95% CI [−6.2, −1.6,] and at the second minute: −3.8 μΜ; 95% CI [−4.9, -0.01]) and placebo conditions (at first minute: −2.9 μΜ; 95% CI [−5.2, −0.6,] and at the second minute: −2.4 μΜ; 95% CI [−4.9, 0.02]). For Δ[HHb], increases were observed during exercise in both conditions. For L-citrulline (at first minute: +6.2 μΜ; 95% CI [3.5, 9,] and at the second minute: +6.3 μΜ; 95% CI [4.1, 8.6]) and for placebo (at first minute: +4.4 μΜ; 95% CI [1.7, 7.2] and at the second minute: +4.3 μΜ; 95% CI [2.1, 6.6]). Relative changes during exercise compared to the pre-exercise values were observed in both conditions for THb in the L-citruline condition (at first minute: +2.3 μΜ; 95% CI [−0.9, 5.5] and at the second minute: +2.5 μΜ; 95% CI [−1.0, 6.0]) and for placebo (at first minute: +1.5 μΜ; 95% CI [−1.7, 4.7] and at the second minute: +1.9 μΜ; 95% CI [−1.6, 5.4]). Furthermore, decreases for TSI during exercise in both conditions were for L-citrulline (at first minute: −7.6 μΜ; 95% CI [−12.9, −2.3,] and at the second minute: −7.5 μΜ; 95% CI [−11.7, −3.2]) and for placebo (at first minute: −8.1 μΜ; 95% CI [−13.4, −2.8] and at the second minute: −7.1 μΜ; 95% CI [−11.3, −2.9]) compared to the pre-exercise values.
4. Discussion
The primary aim of this study was to examine the effect of L-citrulline supplementation for six days on central and peripheral blood pressure at rest and during blood pressure attenuations induced by isometric exercise in healthy older males. Additionally, arterial stiffness parameters were assessed at rest and during exercise, as well as muscle oxygenation and blood flow indices in vastus lateralis using near-infrared spectroscopy. In contrast to our hypothesis, our findings indicated that six days of oral L-citrulline supplementation did not affect resting or non-resting aortic or brachial BP, nor on arterial stiffness and muscle oxygenation and blood flow in older individuals.
In the present study, older individuals were specifically recruited due to the higher prevalence of increased blood pressure [33,34], endothelial dysfunction [35], reduced muscle blood flow [36], and impaired nitric oxide synthesis [37] in this age group. Therefore, the supplementation with L-citrulline was targeted, as it has been suggested to have favorable effects on blood pressure [26], endothelial dysfunction [23], and muscle blood flow [38]. The isometric exercise was chosen as a physiological stimulus to induce blood pressure elevation and investigate whether a non-pharmacological intervention (i.e., L-citrulline) can attenuate the increases in blood pressure during this activity. It's worth mentioning that low-intensity isometric muscle contractions are highly involved in everyday activities, such as grocery shopping, claiming stairs, gardening, etc. Thus, any blood pressure attenuation from L-citrulline supplementation at rest or during exercise would have significant clinical application.
4.1. L-Citrulline and Blood Pressure
Increased blood pressure is considered a significant risk factor for cardiovascular disease progression, and interventions leading to lowering blood pressure are considered an effective strategy to avoid adverse effects on cardiovascular health. More specifically, it has been suggested that non-pharmacological nutritional factors, such as L-citrulline, could positively impact vascular health [22]. As a nitric oxide precursor, L-citrulline supplementation increases nitric oxide synthesis and bioavailability [31,39,40]. Nitric oxide plays a crucial role in regulating vascular endothelial function and blood pressure by relaxing the smooth muscle cells and expanding the vascular wall [7,8]. A recent meta-analysis reported decreases in blood pressure after L-citrulline supplementation [27], supporting the potential of this intervention. However, it is essential to note that while the existing evidence is encouraging [22,41], the number of investigations is limited. Further studies are required to confirm the potential of L-citrulline supplementation in reducing blood pressure and promoting cardiovascular health.
The present study found that a six-day supplementation does not affect resting or non-resting blood pressure (aortic or brachial). These findings are consistent with similar studies that have investigated the effects of L-citrulline supplementation on resting blood pressure in young and older adults using the same dosage, ranging from seven days to four weeks, and found no effect of L-citrulline on resting blood pressure [39,42,43,44]. However, contrasting results have been reported in other studies. For example, it has been reported that a four-week supplementation of 10 g of L-citrulline significantly lowered resting diastolic aortic blood pressure and MAP in hypertensive postmenopausal women [23]. Additionally, favorable effects on arterial systolic blood pressure in young males have been reported [24], and brachial and aortic systolic and diastolic blood pressure in postmenopausal obese women [25,26] after 4 and 8 weeks of L-citrulline supplementation. It is worth noting that three out of the four studies that reported decreases in blood pressure recruited hypertensive postmenopausal obese individuals [23,25,26]. In the present study, older yet healthy individuals were recruited, as their blood pressure values are considered pre-hypertensive and without clinical cardiovascular diseases that would justify pharmacological prescription. Thus, the participants' clinical condition in these studies [23,25,26], might have influenced the response to L-citrulline supplementation, as obesity and menopause are associated with hypertension progression and development [45]. Furthermore, the duration of the supplementation was more prolonged in these studies, ranging from four to eight weeks, which could have influenced the effectiveness of the intervention [46]. Nevertheless, it would be interesting for future studies to compare the impact of short-term versus more extended supplementation protocols on individuals with normal and high blood pressure levels.
Besides resting blood pressure, this study was the first to assess the effect of short-term use of L-citrulline supplementation on exercise-induced blood pressure increases, specifically during acute isometric knee extensor exercise. We have shown that two minutes of isometric knee extensor exercise at 30% of pre-determined maximum strength is adequate to elevate both peripheral and central blood pressure significantly but without any attenuation following L-citrulline supplementation. To the best of our knowledge, only one study has assessed the impact of L-citrulline on exercise-induced blood pressure increase, using isometric handgrip exercise as a stimulus [42]. In that study, the authors reported lower aortic and brachial SBP and lower aortic DBP during exercise in the group that received 6 g of L-citrulline for two weeks. Thus, a more extended supplementation may be required to attenuate blood hemodynamic increases during isometric exercise [46]. Furthermore, participants in that study were obese, which might enhance the blood-lowering effects of L-citrulline, as decreases have also been observed in obese individuals at rest [23,25,26]. Obesity is a chronic medical condition that negatively affecting vascular health [47]. Considering the observations above, it is likely that L-citrulline supplementation may present a more significant effect on blood pressure in subjects with prior endothelial dysfunction, such as obesity.
Given that exercise-induced blood pressure augmentation has been proposed as a better predictor of the development of cardiovascular disease in middle-aged individuals [48], we emphasize the need for future studies assessing the efficiency of supplements on hemodynamics to not only focus on resting conditions but also evaluate transient changes in response to exercise.
4.2. L-Citrulline and Arterial Stiffness
In addition to blood pressure improvements, L-citrulline also appears to favor arterial stiffness, assessed through measurements such as pulse wave velocity or aortic pulse wave reflection and augmentation index at rest or following a combined cold pressure test with isometric exercise [24,38,39,42,44]. However, in this study, in contrast to our hypothesis, six days of oral L-citrulline supplementation did not improve arterial stiffness in older men, as indicated by measurements of cf-PWV, aortic pulse wave reflection, and AIx. These observations contrast previous research that reported reduced resting PWV and AIx following one [39] and two weeks [24,42] of L-citrulline supplementation. However, other studies failed to observe any resting PWV and AIx changes within the same time frame [38,44], which somehow questions the effect of L-citrulline supplementation on arterial stiffness. Notably, the only investigation showing improvements in resting PWV after one week of L-citrulline supplementation recruited middle-aged males with PWV values >14 m/s [39], which is the cutoff value for risk prediction of developing cardiovascular disease [49]. Our study's baseline values for cf-PWV were 7.5 m/s. This evidence suggests that individuals at a higher risk for cardiovascular disease development experience more pronounced hemodynamic changes following L-citrulline supplementation than healthy individuals [50].
Furthermore, we assessed the effect of L-citrulline supplementation on aortic pulse wave reflection and augmentation index (AIx) in response to isometric exercise as a physiological stimulus of hemodynamic disturbances. Previous studies have reported varying results regarding the impact of L-citrulline on AIx at rest. Still, some have shown improvements in response to specific physiological stimuli, such as the cold pressor test [42] or concurrent cold pressor test with isometric handgrip exercise [24] following short-term use of L-citrulline. Only one study evaluated AIx during isometric exercise alone after supplementation following two weeks of 6 g of L-citrulline [42], reporting a reduction of AIx. Therefore, further studies are needed to clarify the time-course effects of L-citrulline on hemodynamic responses to exercise. Assessing the impact of supplements, drugs, and other interventions in response to isometric exercise increases the clinical relevance of the studies. These responses may better reflect the real-world situations where cardiac events can be triggered in asymptomatic older individuals during everyday activities.
4.3. L-Citrulline, Muscle Oxygenation, and Blood Flow
In the present study, near-infrared spectroscopy was utilized to assess local muscle oxygenation and blood flow on the vastus lateralis muscle following L-citrulline supplementation. Near-infrared spectroscopy is a reliable method for detecting hemoglobin in smaller vessels and provides insights into regional oxygen metabolism and blood flow [51]. The vastus lateralis muscle was chosen as this muscle is highly active during isometric knee extensor activity [52]. However, no significant changes were found in vastus lateralis oxygenation and blood flow at rest, during and after isometric exercise following L-citrulline supplementation, compared to the placebo group. These results were obtained despite the isometric exercise protocol causing significant changes in all outcome measures.
Our group has observed similar findings of no change in sternocleidomastoid muscle oxygenation and blood flow after acute and short-term L-citrulline supplementation, increasing nitric oxide bioavailability [31,40]. Similarly, Kim et al. [53] reported that acute supplementation with 3 g of L-citrulline increased nitric oxide levels but failed to improve blood flow in healthy young and older adults with heart failure. On the contrary, Bailey et al. [54], with a seven-day supplementation period and 6 g of L-citrulline per day in young males, observed favorable changes in the VO2 kinetics of the vastus lateralis. Furthermore, Gonzales et al. [38] reported increases in femoral blood flow in older males after supplementing with the seven g of L-citrulline for 14 days, while no changes were observed in older females.
4.4. Limitations
The major limitation of the present study was the lack of any measurement of nitric oxide production, which could have provided us with valuable mechanistic insights into nitric oxide metabolism. We suggest future nutritional interventions incorporating nitric oxide measurements in various compartments, such as plasma and muscle, when evaluating the effects of dietary interventions with nitric oxide precursors like L-citrulline. Additionally, it is crucial to recognize that blood pressure regulation and the development of cardiovascular diseases can vary between males and females throughout [55,56]. Even though such sex differences in vascular health may ease after menopause [57], recruiting males only in our investigation limits our findings' generalizability to females. Future research should aim to include both male and female participants to understand better potential sex differences in the effects of L-citrulline supplementation on blood pressure and cardiovascular health.
4.5. Conclusion
Our results did not find evidence to support any blood-lowering effect of 6 g L-citrulline supplementation for six days or any favorable impact on arterial stiffness and muscle blood flow in older males at rest or during isometric exercise that cause significant elevations in blood pressure. Although it has been suggested that L-citrulline may reduce blood pressure [22,27,41], we believe that more research is necessary to support this potential role, as the number of studies is limited, and the findings are inconsistent. Most studies reporting decreases in blood pressure after L-citrulline supplementation were observed during disturbed hemodynamics (e.g., during the cold pressor test with or without concurrent exercise), whereas findings for resting central and peripheral blood pressure remained controversial. Therefore, relying solely on L-citrulline for blood pressure management while delaying any medical treatment (i.e., medication) or lifestyle changes (i.e., exercise, balanced diet, weight loss) might be risky for health.
It remains of particular interest to select older yet healthy persons in this study who could benefit from L-citrulline supplementation, as it is generally characterized by endothelial dysfunction and pre-hypertension but not yet developed clinical cardiovascular diseases to justify pharmacological prescription.
Author Contributions
Conceptualization, AAT and AT; methodology, AT, FC, and GMP; formal nalysis, AT, and SC; investigation, GMP, and FC; writing—original draft preparation, AT., GMP, and FC; writing—review and editing, AAT and SC; supervision, A.A.Τ; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was granted approval by the Cyprus National Bioethics Committee (ΕΕΒΚ/ΕΠ/2022/59) and was conducted in accordance with the Declaration of Helsinki.
Informed Consent Statement
Informed consent was obtained from all participants involved in the study.
Data Availability Statement
Data from the current study are available from the corresponding author upon reasonable request.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.Z.; Benjamin, E.J.; Benziger, C.P.; et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990-2019: Update From the GBD 2019 Study. J Am Coll Cardiol 2020, 76, 2982–3021. [Google Scholar] [CrossRef]
- Kaess, B.M.; Rong, J.; Larson, M.G.; Hamburg, N.M.; Vita, J.A.; Levy, D.; Benjamin, E.J.; Vasan, R.S.; Mitchell, G.F. Aortic stiffness, blood pressure progression, and incident hypertension. JAMA 2012, 308, 875–881. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, G.F. Arterial stiffness and hypertension: chicken or egg? Hypertension 2014, 64, 210–214. [Google Scholar] [CrossRef]
- Safar, M.E.; Asmar, R.; Benetos, A.; Blacher, J.; Boutouyrie, P.; Lacolley, P.; Laurent, S.; London, G.; Pannier, B.; Protogerou, A.; et al. Interaction Between Hypertension and Arterial Stiffness. Hypertension 2018, 72, 796–805. [Google Scholar] [CrossRef]
- Mancia, G.; Bombelli, M.; Facchetti, R.; Madotto, F.; Corrao, G.; Trevano, F.Q.; Grassi, G.; Sega, R. Long-term prognostic value of blood pressure variability in the general population: results of the Pressioni Arteriose Monitorate e Loro Associazioni Study. Hypertension 2007, 49, 1265–1270. [Google Scholar] [CrossRef]
- Willum-Hansen, T.; Staessen, J.A.; Torp-Pedersen, C.; Rasmussen, S.; Thijs, L.; Ibsen, H.; Jeppesen, J. Prognostic value of aortic pulse wave velocity as index of arterial stiffness in the general population. Circulation 2006, 113, 664–670. [Google Scholar] [CrossRef]
- Lundberg, J.O.; Weitzberg, E. Nitric oxide signaling in health and disease. Cell 2022, 185, 2853–2878. [Google Scholar] [CrossRef] [PubMed]
- Tousoulis, D.; Kampoli, A.M.; Tentolouris, C.; Papageorgiou, N.; Stefanadis, C. The role of nitric oxide on endothelial function. Curr Vasc Pharmacol 2012, 10, 4–18. [Google Scholar] [CrossRef] [PubMed]
- Stamler, J.S.; Meissner, G. Physiology of nitric oxide in skeletal muscle. Physiol Rev 2001, 81, 209–237. [Google Scholar] [CrossRef]
- Chatzinikolaou, P.N.; Margaritelis, N.V.; Chatzinikolaou, A.N.; Paschalis, V.; Theodorou, A.A.; Vrabas, I.S.; Kyparos, A.; Nikolaidis, M.G. Oxygen Transport. A Redox O2dyssey. In Oxidative Eustress in Exercise Physiology, Cobley, J.N., Davison, G.W., Eds.; CRC Press: Boca Raton, 2022. [Google Scholar]
- Margaritelis, N.V.; Paschalis, V.; Theodorou, A.A.; Kyparos, A.; Nikolaidis, M.G. Antioxidants in Personalized Nutrition and Exercise. Adv Nutr 2018, 9, 813–823. [Google Scholar] [CrossRef]
- Tejero, J.; Shiva, S.; Gladwin, M.T. Sources of Vascular Nitric Oxide and Reactive Oxygen Species and Their Regulation. Physiol Rev 2019, 99, 311–379. [Google Scholar] [CrossRef] [PubMed]
- Bescos, R.; Sureda, A.; Tur, J.A.; Pons, A. The effect of nitric-oxide-related supplements on human performance. Sports Med 2012, 42, 99–117. [Google Scholar] [CrossRef] [PubMed]
- Kerksick, C.M.; Wilborn, C.D.; Roberts, M.D.; Smith-Ryan, A.; Kleiner, S.M.; Jager, R.; Collins, R.; Cooke, M.; Davis, J.N.; Galvan, E.; et al. ISSN exercise & sports nutrition review update: research & recommendations. J Int Soc Sports Nutr 2018, 15, 38. [Google Scholar] [CrossRef]
- van de Poll, M.C.; Siroen, M.P.; van Leeuwen, P.A.; Soeters, P.B.; Melis, G.C.; Boelens, P.G.; Deutz, N.E.; Dejong, C.H. Interorgan amino acid exchange in humans: consequences for arginine and citrulline metabolism. Am J Clin Nutr 2007, 85, 167–172. [Google Scholar] [CrossRef] [PubMed]
- Schwedhelm, E.; Maas, R.; Freese, R.; Jung, D.; Lukacs, Z.; Jambrecina, A.; Spickler, W.; Schulze, F.; Boger, R.H. Pharmacokinetic and pharmacodynamic properties of oral L-citrulline and L-arginine: impact on nitric oxide metabolism. Br J Clin Pharmacol 2008, 65, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Morris, S.M., Jr. Enzymes of arginine metabolism. J Nutr 2004, 134, 2743S–2747S. [Google Scholar] [CrossRef] [PubMed]
- Curis, E.; Nicolis, I.; Moinard, C.; Osowska, S.; Zerrouk, N.; Benazeth, S.; Cynober, L. Almost all about citrulline in mammals. Amino Acids 2005, 29, 177–205. [Google Scholar] [CrossRef] [PubMed]
- Windmueller, H.G.; Spaeth, A.E. Source and fate of circulating citrulline. Am J Physiol 1981, 241, E473–E480. [Google Scholar] [CrossRef]
- Moinard, C.; Maccario, J.; Walrand, S.; Lasserre, V.; Marc, J.; Boirie, Y.; Cynober, L. Arginine behaviour after arginine or citrulline administration in older subjects. Br J Nutr 2016, 115, 399–404. [Google Scholar] [CrossRef]
- Aguayo, E.; Martínez-Sánchez, A.; Fernández-Lobato, B.; Alacid, F. L-Citrulline: A Non-Essential Amino Acid with Important Roles in Human Health. Applied Sciences 2021, 11, 3293. [Google Scholar] [CrossRef]
- Allerton, T.D.; Proctor, D.N.; Stephens, J.M.; Dugas, T.R.; Spielmann, G.; Irving, B.A. l-Citrulline Supplementation: Impact on Cardiometabolic Health. Nutrients 2018, 10. [Google Scholar] [CrossRef] [PubMed]
- Maharaj, A.; Fischer, S.M.; Dillon, K.N.; Kang, Y.; Martinez, M.A.; Figueroa, A. Effects of L-Citrulline Supplementation on Endothelial Function and Blood Pressure in Hypertensive Postmenopausal Women. Nutrients 2022, 14. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Gonzalez, M.A.; Koutnik, A.P.; Ramirez, K.; Wong, A.; Figueroa, A. The effects of short term L-citrulline supplementation on wave reflection responses to cold exposure with concurrent isometric exercise. Am J Hypertens 2013, 26, 518–526. [Google Scholar] [CrossRef] [PubMed]
- Wong, A.; Alvarez-Alvarado, S.; Jaime, S.J.; Kinsey, A.W.; Spicer, M.T.; Madzima, T.A.; Figueroa, A. Combined whole-body vibration training and l-citrulline supplementation improves pressure wave reflection in obese postmenopausal women. Appl Physiol Nutr Metab 2016, 41, 292–297. [Google Scholar] [CrossRef] [PubMed]
- Wong, A.; Chernykh, O.; Figueroa, A. Chronic l-citrulline supplementation improves cardiac sympathovagal balance in obese postmenopausal women: A preliminary report. Auton Neurosci 2016, 198, 50–53. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.H.; Li, X.L.; Zhang, W.G.; Figueroa, A.; Chen, L.H.; Qin, L.Q. Effect of oral L-citrulline on brachial and aortic blood pressure defined by resting status: evidence from randomized controlled trials. Nutr Metab (Lond) 2019, 16, 89. [Google Scholar] [CrossRef]
- Chant, B.; Bakali, M.; Hinton, T.; Burchell, A.E.; Nightingale, A.K.; Paton, J.F.R.; Hart, E.C. Antihypertensive Treatment Fails to Control Blood Pressure During Exercise. Hypertension 2018, 72, 102–109. [Google Scholar] [CrossRef]
- Fisher, J.P.; Young, C.N.; Fadel, P.J. Autonomic adjustments to exercise in humans. Compr Physiol 2015, 5, 475–512. [Google Scholar] [CrossRef]
- Butlin, M.; Qasem, A. Large Artery Stiffness Assessment Using SphygmoCor Technology. Pulse (Basel) 2017, 4, 180–192. [Google Scholar] [CrossRef] [PubMed]
- Theodorou, A.A.; Zinelis, P.T.; Malliou, V.J.; Chatzinikolaou, P.N.; Margaritelis, N.V.; Mandalidis, D.; Geladas, N.D.; Paschalis, V. Acute L-Citrulline Supplementation Increases Nitric Oxide Bioavailability but Not Inspiratory Muscle Oxygenation and Respiratory Performance. Nutrients 2021, 13. [Google Scholar] [CrossRef] [PubMed]
- Andrews, A.W.; Thomas, M.W.; Bohannon, R.W. Normative values for isometric muscle force measurements obtained with hand-held dynamometers. Phys Ther 1996, 76, 248–259. [Google Scholar] [CrossRef]
- Chrysant, S.G.; Chrysant, G.S. The age-related hemodynamic changes of blood pressure and their impact on the incidence of cardiovascular disease and stroke: new evidence. J Clin Hypertens (Greenwich) 2014, 16, 87–90. [Google Scholar] [CrossRef]
- Pinto, E. Blood pressure and ageing. Postgrad Med J 2007, 83, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Ungvari, Z.; Tarantini, S.; Kiss, T.; Wren, J.D.; Giles, C.B.; Griffin, C.T.; Murfee, W.L.; Pacher, P.; Csiszar, A. Endothelial dysfunction and angiogenesis impairment in the ageing vasculature. Nat Rev Cardiol 2018, 15, 555–565. [Google Scholar] [CrossRef] [PubMed]
- Lawrenson, L.; Poole, J.G.; Kim, J.; Brown, C.; Patel, P.; Richardson, R.S. Vascular and metabolic response to isolated small muscle mass exercise: effect of age. Am J Physiol Heart Circ Physiol 2003, 285, H1023–H1031. [Google Scholar] [CrossRef]
- Torregrossa, A.C.; Aranke, M.; Bryan, N.S. Nitric oxide and geriatrics: Implications in diagnostics and treatment of the elderly. J Geriatr Cardiol 2011, 8, 230–242. [Google Scholar] [CrossRef]
- Gonzales, J.U.; Raymond, A.; Ashley, J.; Kim, Y. Does l-citrulline supplementation improve exercise blood flow in older adults? Exp Physiol 2017, 102, 1661–1671. [Google Scholar] [CrossRef] [PubMed]
- Ochiai, M.; Hayashi, T.; Morita, M.; Ina, K.; Maeda, M.; Watanabe, F.; Morishita, K. Short-term effects of L-citrulline supplementation on arterial stiffness in middle-aged men. Int J Cardiol 2012, 155, 257–261. [Google Scholar] [CrossRef]
- Theodorou, A.A.; Chatzinikolaou, P.N.; Margaritelis, N.V.; Christodoulou, F.; Tsatalas, T.; Paschalis, V. Short-Term L-Citrulline Supplementation Does Not Affect Inspiratory Muscle Oxygenation and Respiratory Performance in Older Adults. Nutrients 2023, 15. [Google Scholar] [CrossRef] [PubMed]
- Khalaf, D.; Kruger, M.; Wehland, M.; Infanger, M.; Grimm, D. The Effects of Oral l-Arginine and l-Citrulline Supplementation on Blood Pressure. Nutrients 2019, 11. [Google Scholar] [CrossRef]
- Figueroa, A.; Alvarez-Alvarado, S.; Jaime, S.J.; Kalfon, R. l-Citrulline supplementation attenuates blood pressure, wave reflection and arterial stiffness responses to metaboreflex and cold stress in overweight men. Br J Nutr 2016, 116, 279–285. [Google Scholar] [CrossRef]
- Figueroa, A.; Trivino, J.A.; Sanchez-Gonzalez, M.A.; Vicil, F. Oral L-citrulline supplementation attenuates blood pressure response to cold pressor test in young men. Am J Hypertens 2010, 23, 12–16. [Google Scholar] [CrossRef]
- Jaime, S.J.; Nagel, J.; Maharaj, A.; Fischer, S.M.; Schwab, E.; Martinson, C.; Radtke, K.; Mikat, R.P.; Figueroa, A. L-Citrulline supplementation attenuates aortic pulse pressure and wave reflection responses to cold stress in older adults. Exp Gerontol 2022, 159, 111685. [Google Scholar] [CrossRef]
- Morimoto, S.; Ichihara, A. Late age at menopause positively associated with obesity-mediated hypertension. Hypertens Res 2023. [Google Scholar] [CrossRef]
- Smeets, E.; Mensink, R.P.; Joris, P.J. Effects of L-citrulline supplementation and watermelon consumption on longer-term and postprandial vascular function and cardiometabolic risk markers: A meta-analysis of randomized controlled trials in adults. Br J Nutr 2021, 128, 1–34. [Google Scholar] [CrossRef]
- Rhee, E.J. The Influence of Obesity and Metabolic Health on Vascular Health. Endocrinol Metab (Seoul) 2022, 37, 1–8. [Google Scholar] [CrossRef]
- Lewis, G.D.; Gona, P.; Larson, M.G.; Plehn, J.F.; Benjamin, E.J.; O'Donnell, C.J.; Levy, D.; Vasan, R.S.; Wang, T.J. Exercise blood pressure and the risk of incident cardiovascular disease (from the Framingham Heart Study). Am J Cardiol 2008, 101, 1614–1620. [Google Scholar] [CrossRef]
- Yamashina, A.; Tomiyama, H.; Arai, T.; Hirose, K.; Koji, Y.; Hirayama, Y.; Yamamoto, Y.; Hori, S. Brachial-ankle pulse wave velocity as a marker of atherosclerotic vascular damage and cardiovascular risk. Hypertens Res 2003, 26, 615–622. [Google Scholar] [CrossRef] [PubMed]
- Figueroa, A.; Wong, A.; Jaime, S.J.; Gonzales, J.U. Influence of L-citrulline and watermelon supplementation on vascular function and exercise performance. Curr Opin Clin Nutr Metab Care 2017, 20, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Jones, S.; Chiesa, S.T.; Chaturvedi, N.; Hughes, A.D. Recent developments in near-infrared spectroscopy (NIRS) for the assessment of local skeletal muscle microvascular function and capacity to utilise oxygen. Artery Res 2016, 16, 25–33. [Google Scholar] [CrossRef] [PubMed]
- Pincivero, D.M.; Gandhi, V.; Timmons, M.K.; Coelho, A.J. Quadriceps femoris electromyogram during concentric, isometric and eccentric phases of fatiguing dynamic knee extensions. J Biomech 2006, 39, 246–254. [Google Scholar] [CrossRef] [PubMed]
- Kim, I.Y.; Schutzler, S.E.; Schrader, A.; Spencer, H.J.; Azhar, G.; Deutz, N.E.; Wolfe, R.R. Acute ingestion of citrulline stimulates nitric oxide synthesis but does not increase blood flow in healthy young and older adults with heart failure. Am J Physiol Endocrinol Metab 2015, 309, E915–E924. [Google Scholar] [CrossRef] [PubMed]
- Bailey, S.J.; Blackwell, J.R.; Lord, T.; Vanhatalo, A.; Winyard, P.G.; Jones, A.M. l-Citrulline supplementation improves O2 uptake kinetics and high-intensity exercise performance in humans. J Appl Physiol (1985) 2015, 119, 385–395. [Google Scholar] [CrossRef] [PubMed]
- Connelly, P.J.; Currie, G.; Delles, C. Sex Differences in the Prevalence, Outcomes and Management of Hypertension. Curr Hypertens Rep 2022, 24, 185–192. [Google Scholar] [CrossRef]
- Reckelhoff, J.F. Mechanisms of sex and gender differences in hypertension. J Hum Hypertens 2023. [Google Scholar] [CrossRef]
- Stanhewicz, A.E.; Wenner, M.M.; Stachenfeld, N.S. Sex differences in endothelial function important to vascular health and overall cardiovascular disease risk across the lifespan. Am J Physiol Heart Circ Physiol 2018, 315, H1569–H1588. [Google Scholar] [CrossRef]
Figure 1.
Experimental design. Arrows indicate the data collection time points (i.e., baseline, post-supplementation, and during isometric exercise. Exer, isometric exercise protocol.
Figure 1.
Experimental design. Arrows indicate the data collection time points (i.e., baseline, post-supplementation, and during isometric exercise. Exer, isometric exercise protocol.
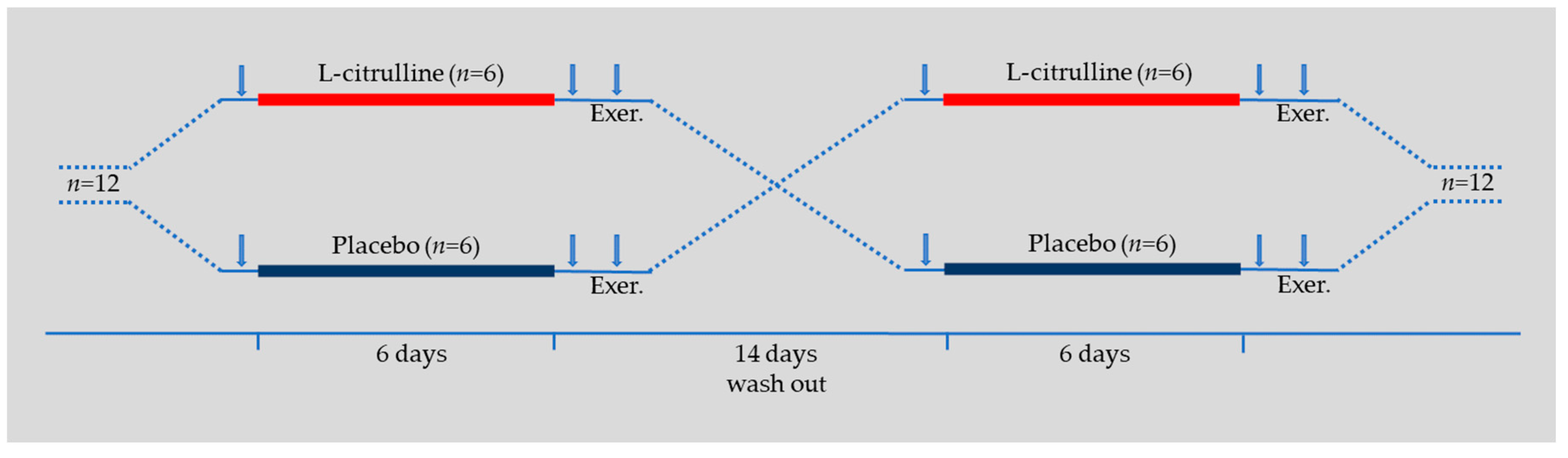
Figure 2.
Blood hemodynamic percent changes during isometric exercise protocol compared to pre-exercise values (mean ± SD).
Figure 2.
Blood hemodynamic percent changes during isometric exercise protocol compared to pre-exercise values (mean ± SD).
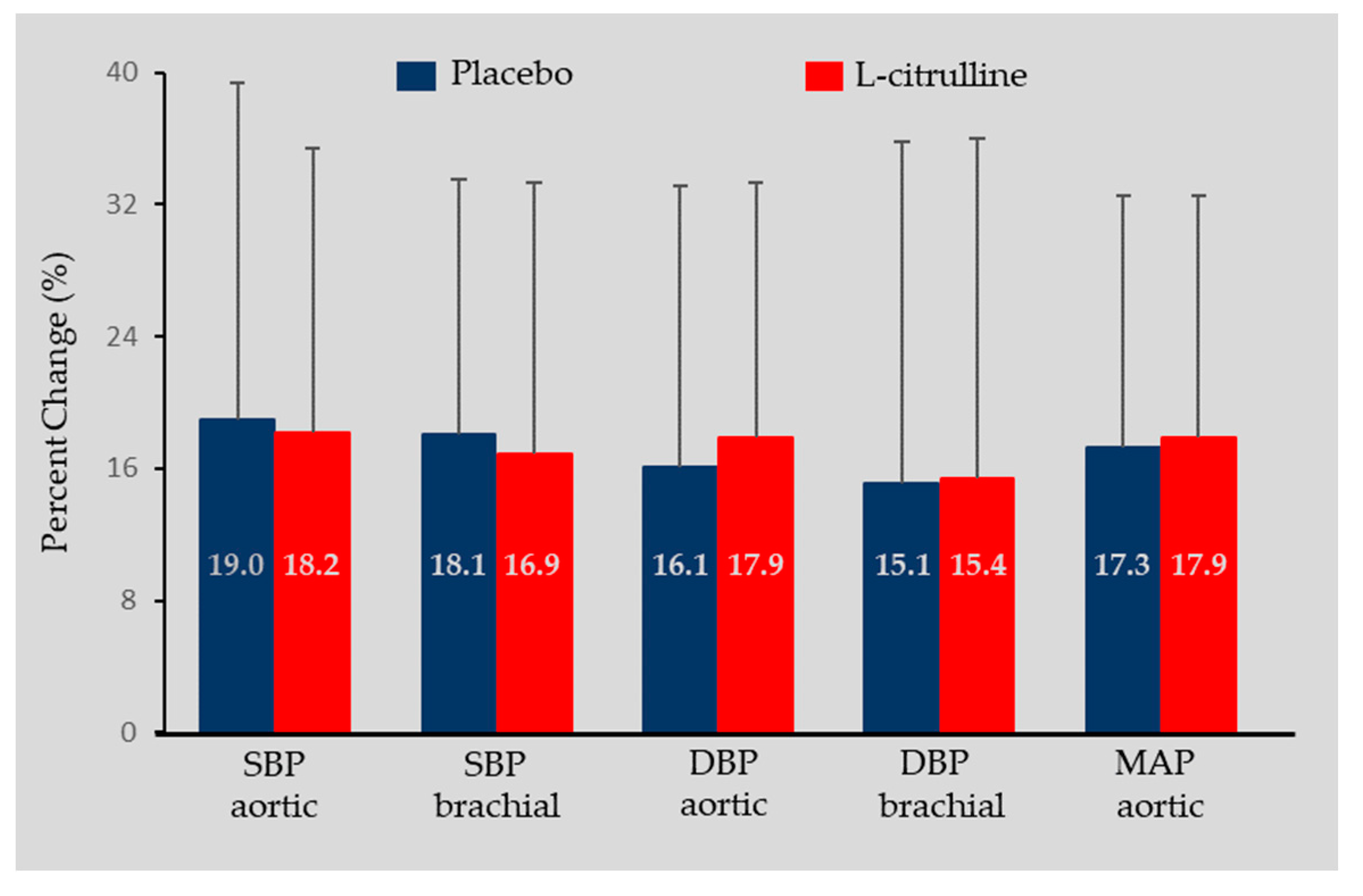
Figure 3.
Vastus lateralis muscle oxyhemoglobin (O2Hb) (A), deoxyhemoglobin (HHb) (B), total hemoglobin (tHb) (C), and tissue saturation index at baseline, after six days of L-citrulline supplementation (red circles) and placebo (blue circles), 60 and 120 seconds during and post isometric exercise protocol.
Figure 3.
Vastus lateralis muscle oxyhemoglobin (O2Hb) (A), deoxyhemoglobin (HHb) (B), total hemoglobin (tHb) (C), and tissue saturation index at baseline, after six days of L-citrulline supplementation (red circles) and placebo (blue circles), 60 and 120 seconds during and post isometric exercise protocol.
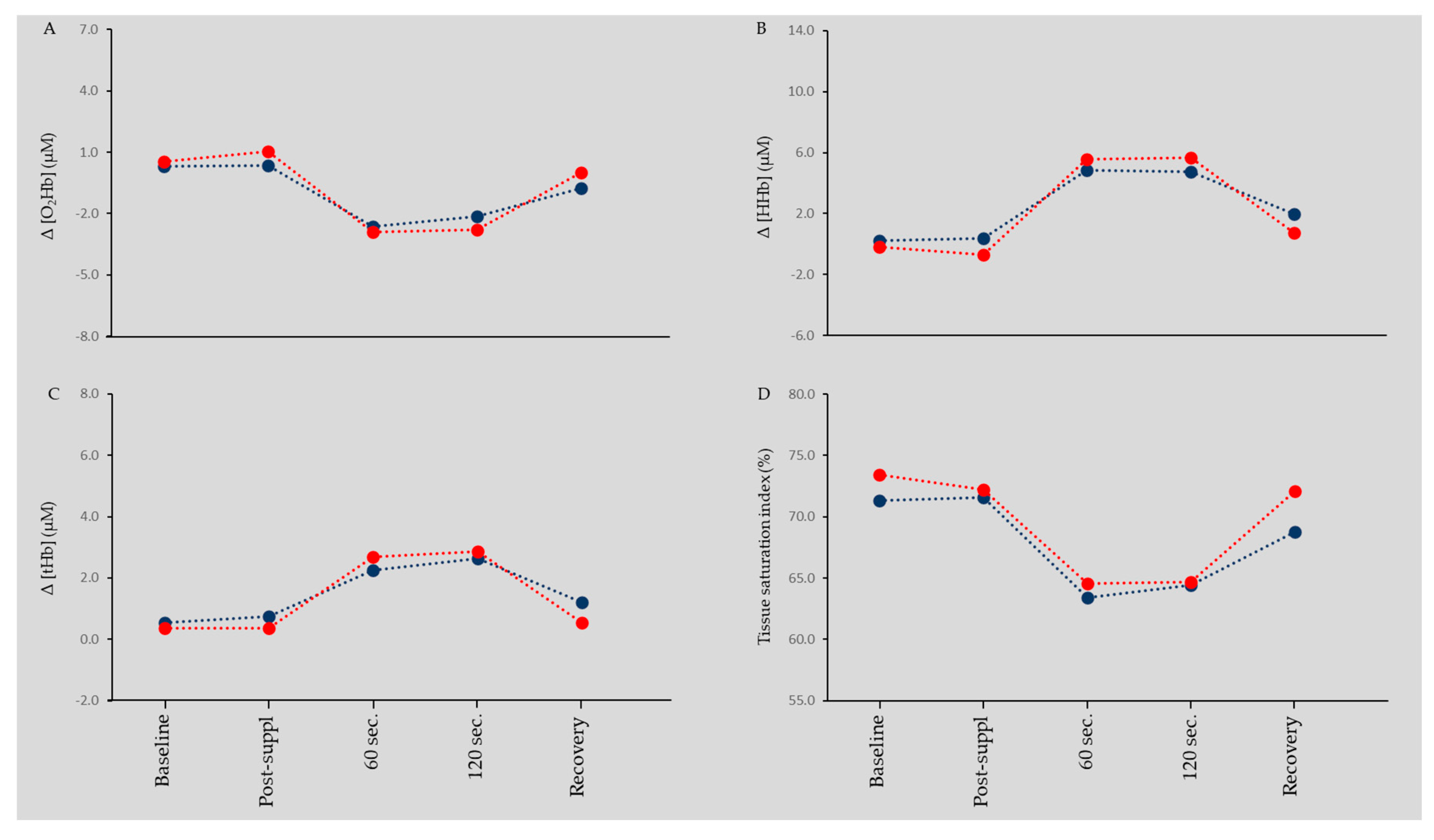

Table 1.
Participants’ anthropometric characteristics (mean ± S.D.).
| n = 12 | |||
|---|---|---|---|
| Age (yr) | 64.3 | ± | 5.1 |
| Height (cm) | 173.9 | ± | 4.2 |
| Weight (kg) | 78.4 | ± | 6.9 |
| BMI (Kg/m2) | 26.0 | ± | 2.7 |
| Body fat (%) | 26.8 | ± | 2.6 |
| Waist circumference (cm) | 100 | ± | 5.6 |
| Hip circumference (cm) | 105.8 | ± | 6.8 |
| Waist-to-hip ratio | 0.95 | ± | 0.02 |
Table 2.
Aortic and brachial blood hemodynamics at baseline, post supplementation, and during the isometric exercise protocol (mean ± SD).
Table 2.
Aortic and brachial blood hemodynamics at baseline, post supplementation, and during the isometric exercise protocol (mean ± SD).
| Interactions and Main Effects | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | Post Suppl. | Dur. Exercise | C×T | C | T | |||||||
| Heart Rate (bpm) | ||||||||||||
| Placebo | 64.1 | ± | 6.3 | 64.0 | ± | 7.9 | 76.8 | ± | 11.5 | p=0.631 | p=0.963 | p<0.001 |
| L-Citrulline | 63.5 | ± | 5.9 | 63.7 | ± | 6.1 | 78.1 | ± | 9.0 | |||
| Aortic SBP (mmHg) | ||||||||||||
| Placebo | 121.9 | ± | 13.3 | 121.2 | ± | 12.7 | 142.5 | ± | 17.4 | p=0.899 | p=0.822 | p<0.001 |
| L-Citrulline | 120.0 | ± | 11.5 | 121.1 | ± | 11.3 | 141.8 | ± | 14.4 | |||
| Brachial SBP (mmHg) | ||||||||||||
| Placebo | 130.8 | ± | 13.2 | 129.4 | ± | 12.6 | 152.5 | ± | 21.6 | p=0.553 | p=0.788 | p<0.001 |
| L-Citrulline | 131.5 | ± | 12.6 | 130.1 | ± | 14.5 | 151.8 | ± | 23.8 | |||
| Aortic DBP (mmHg) | ||||||||||||
| Placebo | 83.3 | ± | 6.1 | 84.1 | ± | 6.5 | 97.5 | ± | 14.8 | p=0.919 | p=0.608 | p<0.001 |
| L-Citrulline | 82.1 | ± | 5.9 | 81.9 | ± | 7.2 | 96.3 | ± | 9.0 | |||
| Brachial DBP (mmHg) | ||||||||||||
| Placebo | 83.4 | ± | 6.0 | 84.2 | ± | 7.9 | 97.3 | ± | 21.5 | p=0.808 | p=0.652 | p<0.001 |
| L-Citrulline | 82.8 | ± | 7.6 | 82.1 | ± | 6.5 | 94.6 | ± | 17.1 | |||
| Aortic MAP (mmHg) | ||||||||||||
| Placebo | 99.2 | ± | 8.0 | 99.4 | ± | 8.2 | 116.0 | ± | 13.0 | p=0.962 | p=0.660 | p<0.001 |
| L-Citrulline | 97.7 | ± | 6.6 | 98.1 | ± | 7.2 | 115.1 | ± | 12.6 | |||
| Aortic PP (mmHg) | ||||||||||||
| Placebo | 38.6 | ± | 11.4 | 37.1 | ± | 10.7 | 45.01 | ± | 18.7 | p=0.856 | p=0.876 | p=0.071 |
| L-Citrulline | 37.9 | ± | 11.5 | 39.2 | ± | 11.4 | 45.5 | ± | 12.0 | |||
SBP, systolic blood pressure; mmHg, DBP, diastolic blood pressure; MAP, mean arterial pressure; PP, pulse pressure; bpm, beats per minute; mmHg, millimeter of mercury; C×T, two-way interaction between condition and time; C, main effect of condition; T, main effect of time.
Table 3.
Pulse wave analysis and arterial stiffness at baseline, post supplementation, and during the isometric exercise protocol (mean ± SD).
Table 3.
Pulse wave analysis and arterial stiffness at baseline, post supplementation, and during the isometric exercise protocol (mean ± SD).
| Interactions and Main Effects | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | Post Suppl. | Dur. Exercise | C×T | C | T | |||||||
| Augmented pressure (mmHg) | ||||||||||||
| Placebo | 10.8 | ± | 4.4 | 11.0 | ± | 4.4 | 11.3 | ± | 5.7 | p=0.537 | p=0.730 | p=0.286 |
| L-Citrulline | 11.1 | ± | 4.4 | 11.2 | ± | 4.0 | 12.8. | ± | 6.8 | |||
| Augmentation Index (%) | ||||||||||||
| Placebo | 31.9 | ± | 20.3 | 32.9 | ± | 19.4 | 37.2 | ± | 16.2 | p=0.729 | p=0.965 | p=0.796 |
| L-Citrulline | 35.7 | ± | 17.5 | 31.6 | ± | 14.6 | 33.5 | ± | 17.6 | |||
| Forward Wave Pressure (mmHg) | ||||||||||||
| Placebo | 43.3 | ± | 5.6 | 31.9 | ± | 5.1 | 32.7 | ± | 4.8 | p=0.896 | p=0.816 | p=0.503 |
| L-Citrulline | 31.5 | ± | 4.5 | 31.6 | ± | 5.6 | 32.4 | ± | 6.1 | |||
| Backward Wave Pressure (mmHg) | ||||||||||||
| Placebo | 17.2 | ± | 4.0 | 17.5 | ± | 4.2 | 17.8 | ± | 4.4 | p=0.769 | p=0.659 | p=0.631 |
| L-Citrulline | 16.8 | ± | 5.3 | 16.5 | ± | 3.2 | 17.0 | ± | 4.2 | |||
| c-f Pulse Wave Velocity (m/s) | ||||||||||||
| Placebo | 7.3 | ± | 1.7 | 7.1 | ± | 1.4 | p=0.251 | p=0.251 | p=0.666 | |||
| L-Citrulline | 7.7 | ± | 1.8 | 7.7 | ± | 1.8 | ||||||
c-f, carotid-femoral; mmHg, millimeter of mercury; m/s, meters pes second; C×T, two-way interaction between condition and time; C, main effect of condition; T, main effect of time.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



