
Submitted:
02 June 2023
Posted:
06 June 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Background: The novel coronavirus (COVID-19) infection is primarily transmitted through respiratory droplets from an infected person and contact with tainted surfaces or items. Social distancing became the primary measure of preventing the spread of COVID-19, with the principal aim being to reduce the probability of contact with an already infected person. Social distancing can be distressing, as it is against the community's way of life. Saudi Arabia imposed a curfew and suspended all religious, entertainment, sporting, and mass congregations. The daily updates on COVID-19 infection and mortality are upsetting and further, aggravate depression and anxiety. With this background, this study was planned with the following objectives. To determine the sociodemographic profile of the study participants, to find the prevalence of psychological morbidity, and to measure the association between the sociodemographic details, COVID-19 associated factors, and psychological effects among Abha citizens during the COVID-19 pandemic. Methodology: A descriptive cross-sectional community-based study was conducted in the Abha city population from August 2021 to July 22. This study followed snowball sampling, the data was collected using an online Google form the link was shared in WhatsApp groups and through emails to contacts, asking friends to share it with their friends, until reaching the adequate sample size the responses were accepted. Results: A total of 530 participated, and their age ranged from 19 -70 years. Many of the participants (34.5%, n=183) belonged to 36-45 years old. Most of the responders were 69.8% married and Females (69.2%, n=367). Half of the participants had been quarantined (49.6%), and 51.5% were scared from fear of COVID-19. 64.8% of the participants had depression; 14.2%, 20.8%, 13.6%, and 16.2% had mild, moderate, severe, and extremely severe depression, respectively. Around 58.2% of participants suffered from anxiety; 5.8% experienced mild anxiety, 21.7% moderate anxiety, and 30.7% severe anxiety. The proportion of stress among the participants was 45.0%; 10.8% had mild stress, 9.4% had moderate stress, and 24.5% had severe to extremely severe stress. Conclusions: COVID-19 poses mental health problems among individuals and communities. There is a need to find the more susceptible individuals for mental health issues or other psychological disorders. Mental health and psychological problems can be resolved with health education, counseling, and appropriate interventions to curb the negative health impacts of COVID-19.
Keywords:
COVID-19
; Mental Health problems
; DASS-21 scale
; Depression
; Anxiety
Introduction
The novel coronavirus (COVID-19) infection is primarily transmitted through respiratory droplets from an infected person and contact with tainted surfaces or items. (Centres for Disease Control and Prevention, 2021) [1]. The disease quickly spread worldwide due to the increased rate of international travel. Saudi Arabia reported the first case of COVID-19 on March 2, 2020. Since then, the rate of infection has continued to increase gradually. Six months after its initial case, Saudi Arabia reported 841,469 COVID-19 cases (Worldo Meter) [2]. The rate of transmission and the associated mortality rate led to the adoption of strict measures to curb the transmission, such as partial and total movement limitations, prohibiting significant events and unnecessary congregations, and wearing face masks in public (Alshammari et al., 2020) [3]..
Social distancing became the primary measure of preventing the spread of COVID-19, with the principal aim being to reduce the probability of contact with an already infected person. Social distancing can be distressing, as it is against the community's way of life. Saudi Arabia suspended all religious, entertainment, sporting, and mass congregations. Attending schools, mosques, and all other non-essential gatherings were suspended, and a curfew was imposed (Aldarhami et al., 2020).[4] Family and social gatherings are common around the country, which stopped due to lockdowns that create a lot of stress among the people living in Saudi Arabia.
Stress is the specific relationship between a person and the environment through which environmental demands exceed personal adaptive capacity, leading to either psychological or biological changes and predisposing one to infections (Li et al., 2020) [5]. The absence of treatment, the uncertainty surrounding the disease's prognosis, and the containment measures implemented to curb the spread of the virus pose psychological threats to all members of the population (Hazarika et al., 2021) [6]. Participants worried less about dying or even having the disease themselves (Barzilay et al., 2020) [7]. The public worried more about a family member contracting the disease and even unknowingly infecting others (Barzilay et al., 2020) [7]. The illness's financial burden and hospitalization were COVID-19 concerns leading to anxiety, stress, and depression, and this pattern is consistent across all ages and genders.
Additionally, having a family member infected or having a young member working outside the home resulted in elevated levels of anxiety and stress (Mazza et al., 2020) [8]. A depressed person has a lower chance of achieving life goals and a high probability of attempting suicide. Natural disasters, and disease outbreaks, can increase the prevalence of depression and its long-term impacts on the population. The daily updates on COVID-19 infection and mortality are upsetting and further, aggravate depression and anxiety. With this background, this study was planned with the following objectives.
Objectives
- To determine the sociodemographic profile of the study participants
- To find the prevalence of psychological morbidity among Abha citizens during the COVID-19 pandemic.
- To measure the association between the sociodemographic details, associated factors of Covid-19, and psychological effects among the Abha community.
Methodology
Study Design and Setting
A descriptive, cross-sectional community-based study was conducted in the Abha city population from August 2021 to July 22.
Sampling Technique and sample size
A non-probability snowball sampling technique used in a restricted environment. The minimum sample size was calculated by using a sample size calculator. Regarding the prevalence of psychological morbidity during COVID-19, the previous study reported 44.9% reported minimal psychological impact. The minimum sample was determined to be 511.[9] The data collection was performed and accomplished in the Abha community. A sample of 683 participants participated, from whom 153 were eliminated for having lived in the city for less than six months or having been out of the city during the study.
Methods
After performing an intensive literature review, receiving expert consultation, and examining content validity, the survey tool was selected. Previous studies have used surveys to measure psychological morbidity, a reliable and valid measure for assessing mental health status, and an Arabic survey designed by Ali and Amira (2017) was adopted.[10] The study tool was piloted to determine the instrument's reliability, and a calculated reliability coefficient (Cronbach's α) of 0.87 was observed. The data were collected using an online Google form. This study followed the snowball sampling technique and shared the Google form link with WhatsApp groups and through emails to contacts, asking friends to share it with their friends. Before beginning to fill out the Google form, this study's objectives and goals were explained in the local language and English also. After assuring them about the data confidentiality and anonymous data shared only for research purposes, digital consent was provided, and they accepted the privacy policy for the protection of personal data before completing the survey. No personal data that can recognize the individuals was collected and the data were analyzed in coded form only.
Residents who had lived in the city for less than six months and those outside the city during the study were excluded. It was assumed that individuals with less than six months of residency were only conversant with the city's post-COVID-19 life, making their responses subject to influence from experiences in other regions.
Residents younger than 18 years of age were also excluded from the study due to the mixed evidence concerning the applicability of DASS-21 to children and adolescents (Shaw et al., 2016).[11] Additionally, individuals younger than 18 are minors, and involving them in a study would require consent from their guardians.
Data Collection Tool and Technique
The DASS-21 is a self-reported questionnaire that includes 21 items, seven items for each depression, anxiety, and stress subscale. The questionnaire was divided into three sections: the first section concerned sociodemographic variables, such as age, gender, residence, education, participants' level of income, and nationality; the second section covered COVID-19 and its associated factors; and the third section assessed psychological influence by utilizing the Arabic version of the DASS-21 effectively discriminated against depression, anxiety, and stress. Participants were asked to score every item on a scale of 0–3 (with 0 meaning it did not apply to them at all—NEVER, one meaning it applied to them only to some degree—SOMETIMES, two meaning it applied to them to a considerable degree or a good part of the time—OFTEN, and three meaning it applied to them very much—ALMOST ALWAYS). The sum scores were reached by adding the scores for each (sub)scale and multiplying by 2.
Data Analysis
Google Forms was used to collect data, and the data were imported, coded, and analyzed using IBM SPSS Statistics for Windows, version 25. The questionnaires were assessed for completeness before advancing to the next section. Descriptive analysis depended on frequency, and distribution percentage was performed for all variables. Various instruments, including graphs, means, and standard deviations, were applied through descriptive analysis for the psychological impact category. Multivariate binary logistic regression was used to assess the significant factors' relationship between sociodemographic and psychological impact (depression, anxiety, and stress) levels and to define COVID-19's associated factors and psychological impacts among the Abha community. Statistical significance was measured using a p-value, and a score less than 0.05 was considered statistically significant.
The sum score for the longer version of the DASS-21 scale ranges between 0 and 120. Under each specific subscale, the range is between 0 and 42. However, the cut-off scores for the shorter version of the DASS-21 are 60 and 21, respectively. This study's cut-off scores were derived from Lovibond and Lovibond (1995). After multiplying each subscale by 2, the results were categorized as follows: depression—normal (0−9), mild (10−13), moderate (14−20), severe (21–27), and extremely severe (≥28); anxiety—normal (0−7), mild (8−9), moderate (10−14), severe (15–19) and extremely severe (≥20); and stress—normal (0−14), mild (15−18), moderate (19−25), severe (26–33) and highly severe (≥34). Summed scores of 10 and above indicated depression, eight and above marked anxiety, and 15 and above labeled it as stress.
Results
A total of 530 participants completed the survey tool. The participants' age ranged from 19 -70 years. Many of the participants (34.5%, n=183) belonged to 36-45 years old. Most of the responders (69.2%, n=367) were Females. Majority of respondents 69.8% were married, and 77.9% had a graduate level of education. More than half (60.8%, n=322) are employed in different sectors, while only 18.9% (n=100) worked in the healthcare sector. Over a third of the study participants (35.8%) had monthly incomes exceeding 10,000 SR.

Table 1.
Distribution of sociodemographic factors and Covid-19 and its associated factors among people living in Abha, Saudi Arabia.
Table 1.
Distribution of sociodemographic factors and Covid-19 and its associated factors among people living in Abha, Saudi Arabia.
| Personal data | N | % | |
| Age | 19-25 26-35 36-45 46-55 56-65 >65 |
102 134 183 77 26 8 |
19.2% 25.3% 34.5% 14.5% 4.9% 1.5% |
| Gender | Male Female |
163 367 |
30.8% 69.2% |
| Nationality | Saudi Non-Saudi |
519 11 |
97.9% 2.1% |
| Marital status | Married Single Divorced/widow |
370 134 26 |
69.8% 25.3% 4.9% |
| Education | Less than secondary Secondary University/more |
17 100 413 |
3.2% 18.9% 77.9% |
| Level of income | <5000 5000-10000 10000-20000 >20000 |
179 138 190 23 |
33.8% 26.0% 35.8% 4.3% |
| Employment | Yes No |
322 208 |
60.8% 39.2% |
| Are you a healthcare practitioner? |
Yes No |
100 430 |
18.9% 81.1% |
Half of the participants had been quarantined (49.6%), and 51.5% were scared from fear of COVID-19. Additionally, about 52.1% had been infected with COVID-19, and 51.5% and 47.4% had relatives/acquaintances who were infected or died with COVID-19, respectively. Finally, 44.5% of the participants had received psychological support (Table 2).
Table 3 and Figure 1 shows that the psychological health status of the Abha community was affected to varying degrees. 64.8% of the participants had depression; 14.2%, 20.8%, 13.6%, and 16.2% had mild, moderate, severe, and extremely severe depression, respectively. Around 58.2% of participants suffered from anxiety; 5.8% experienced mild anxiety, 21.7% moderate anxiety, and 30.7% severe anxiety. The proportion of stress among the participants was 45.0%; 10.8% had mild stress, 9.4% had moderate stress, and 24.5% had severe to extremely severe stress. Based on the score ranges from the DASS manual, the mean scores of depression, anxiety, and stress for all participants were found in the mild range for stress (15.47 +/- 12.31) and in the moderate range for depression (14.84 +/- 10.64) and anxiety (11.33 +/- 10.26).
Table 4 shows the distribution of depression, anxiety, and stress among the survey participants. The most-reported depressive item was feeling downhearted and blue (73.0%), followed by lack of motivation (69.4%) and inability to become enthusiastic about anything (68.1%). The most reported anxiety factors were awareness of mouth dryness (56.0%), followed by feeling scared without any good reason (53.8%), and concerns about panic and making a fool of oneself (50.8%). Additionally, the most reported stress items were using a lot of nervous energy (66.4%) and getting agitated (67.0%), followed by difficulty winding down (65.3%) and being rather touchy (64.9%).
Table 5 shows the binary logistic regression-adjusted ORs (95% CIs) and p-values for different demographical factors and their relation to depression, anxiety, and stress. Participants who were 19–25 (OR=2.01 [CI=1.00–4.04; p=0.049]) and 36–45 (OR=2.20 [CI=0.90–5.37; p=0.045]) years old were two times more likely to have depression. Additionally, the odds of having depression were three times more likely among single participants (OR=2.76 [CI=1.00–7.59; p=0.050]), while married participants were two times more likely to have anxiety (OR=1.98 [CI=1.09–3.60; p=0.025]) and stress (OR=2.16 [CI=1.21–3.83; p=0.009]), respectively. Furthermore, earning less than 5000 SR was a significant predictor of depression (OR=0.57 [CI=0.33–1.00; p=0.050]) and stress (OR=0.59 [CI=0.34–1.00; p=0.050]), respectively. Other sociodemographic variables, including gender, education level, employment, and nationality, were not associated with the DASS subscale scores.
Table 6 shows multivariable-adjusted ORs (95% CIs) for factors associated with the psychological status of the Abha community. Healthcare practitioners were approximately two times more likely to have depression, and participants who had a relative or acquaintance who died of COVID-19 had higher odds of having depression, but this trend was not seen in their stress (OR=1.89 [CI=1.18–2.92; p=0.007]) or anxiety (OR=0.65 [CI=0.45–0.95; p=0.026]) levels, respectively. Furthermore, fearing exposure to COVID-19 was a significant predictor for anxiety (OR=1.46 (CI=1.02–2.09; p=0.039]). Finally, no significant differences were found in stress in any of the variables selected.
Discussion
This study was conducted to assess the psychological impacts of COVID-19 on the Abha community. Psychological factors, such as depression, anxiety, and stress, were recorded using a non-probability sampling technique. Sociodemographic variables, such as age, gender, education level, income level, and nationality, were considered when recording the response. Among the 530 participants, 64.8% recorded symptoms of depression, while 58.2% and 45.0% recorded anxiety and stress symptoms, respectively. Similar trends were observed in some of the other studies conducted to assess the impact of COVID-19. In one of the studies conducted in Egypt, high percentages of depression, anxiety, and stress were recorded among students, with 70.5% experiencing depression, 53.6% anxiety, and 47.8% stress. The high anxiety among the students was attributed to the time spent following COVID-19 updates (Ghazawy et al., 2021) [12].
Some recent studies conducted to assess the impacts of COVID-19 supported the fact that younger individuals are more likely to suffer from depression. In the current study, the 19–25 and 36–45 age groups reported significant associations with depression. A published study from China confirmed that the young adult group (18–30) suffered from mental health issues (Qiu et al., 2020) [13]. A study published in Spain demonstrated a similar finding of high depression and stress in young adults 18–33 years old (Jiménez et al., 2020) [14]. A study on Iranian people showed a significant association between anxiety and age. The 21–40 age group showed higher anxiety than others, which contradicted the present study's findings, where there was a non-significant association between anxiety and age group (Moghanibashi-Mansourieh, 2020) [15].
Individuals 18–22 years old are most likely to suffer from mental illness and depression, and about 75% of mental illnesses start during this stage (Downs et al., 2018) [16]. The reason for higher depression in this age group may be that people 19–25 years old are mostly students or just starting their careers and tend to have more significant mental problems than the general population (Mortier et al., 2018) [17]. Academic pressure and worry about the future are common concerns for people in this age bracket who are under constant pressure to perform in the educational field, encounter accommodation problems, and must adjust to a new social life and manage life stage transitions (Acharya et al., 2018; Heckman et al., 2014) [19,20].
Contrary to the current study's findings, some studies have reported lower percentages of depression, anxiety, and stress. A study in Ethiopia found a lower prevalence of psychological impacts, reporting 30.8% for depression, 26.3% for anxiety, and 24.4% for stress (Shifra et al., 2021(.[21] A study from India also found the prevalence of depression, anxiety, and stress to be 34.7%, 32%, and 35.5%, respectively (Hazarika et al., 2021) [6]. A study that investigated COVID-19's immediate psychological impact and associated factors during the initial stages of the pandemic in China recorded the prevalence of severe depression and stress at 16.5% and 8.1%, respectively (Wang et al., 2020) [22]. Similarly, a study in Iran recorded the prevalence of severe anxiety at 19.1%, a significant difference from our study's findings (Moghanibashi-Mansourieh, 2020) [15].
In the current study, moderate to severe symptoms of depression, anxiety, and stress were shown by 34.4%, 31.3%, and 23% of the study participants, respectively. These higher response rates can be attributed to the participants' increased awareness of mental health, anxiety, and depression. Previous studies were performed in the early stages of the pandemic when there were few COVID-19 cases in Saudi Arabia; hence, a lower prevalence was observed. However, our study's findings were consistent with another study conducted in Al-Qassim, Saudi Arabia, which reported moderate to severe psychological impacts of COVID-19 (Alkhamees et al., 2020) [23].
This study depicts the non-significant association between factors such as nationality and education level with physiological factors (i.e., depression, anxiety, and stress), and the odds of having depression were three times more likely among single participants. A recently published study conducted in India found the same result (Hazarika et al., 2021) [6]. In the present study, married participants were two times more likely to have anxiety and stress. Similar findings were reported in another study, in which 37% of the married residents had anxiety. In contrast, only 22.7% of the single population had it. The reason for high anxiety in married people may be the sense of responsibility for their families; they worry about the health of their family members, which ignites anxiety (Fu et al., 2020) [24]. Our study shows a non-significant association between the male gender and dependable variables, e.g., depression, anxiety, and stress. The analysis showed that males were less likely to suffer the psychological impact of a pandemic. This finding agrees with the results from Wang et al. (2021) [25], which indicated that being a Spanish male was not a predictor for having psychological impacts of COVID-19, according to the DASS-21.
Another study from Pakistan investigated the impact of COVID-19 on the community. The findings were consistent with our results and showed that males had better stress-coping mechanisms and faced fewer psychological issues (Salman et al., 2020) [26]. A gender gap exists for the prevalence of anxiety, depression, and other psychological or mental health issues. While one study from China revealed that there are no statistically significant differences in gender (Huang & Zhao, 2021) [27], a non-significant gender association with anxiety was reported in another study conducted in China (Ahmed et al., 2020) [28].
In the current study, participants with lower incomes were more likely to suffer from depression and stress than high-income participants, as economic pressure significantly impacts mental health and tends to amplify the psychological conditions during the COVID-19 pandemic. These findings were consistent with the reported results of a previous study in Al-Qassim (Alkhamees et al., 2020) [23].
The present study found no significant association between education level and psychological factors, whereas some previous studies reported contradicting findings. A recent publication in Iran said that a higher education level contributes to a higher anxiety level, and the study attributed the result to the knowledge of the respondents (Moghanibashi-Mansourieh, 2020) [15]. The more a person knows about a potential hazard, the more likely the person is to become anxious. Another study conducted among Italians showed that lower education levels and unemployment were associated with higher depression levels (Mazza et al., 2020) [6]. A different study reported that COVID-19-related stress was related to low education. Another study in Shenzhen said there was no significant association between education level and psychological distress (Cai et al., 2020), which supports the findings of our current study [29].
In our study, healthcare practitioners were approximately two times more likely to have depression, and similar results have been reported in other studies. Liu et al. (2020)[30] performed a survey of medical staff members and found higher rates of depression (50.4%) and anxiety (44.6%) than in the public. Ho et al. (2020) [31] reported that healthcare professionals, particularly those working in the COVID-19 isolation wards and involved in COVID-19 patient care, are more likely to suffer from psychological conditions due to the constant fear of being infected with COVID-19. In line with current findings, a cross-sectional study based on a web-based survey predicted a higher likelihood of health professionals suffering mental distortion due to the constant change of being infected due to pandemics (Huang & Zhao, 2020) [27]. In contrast to the present research, some recent studies have reported a lower psychological impact of COVID-19 on healthcare professionals. People working in sectors other than healthcare were found to have more psychological disturbances. A meta-analysis of studies conducted to monitor the impacts of COVID-19 among healthcare workers reported that depression was 5.1% and 25.5% lower in healthcare workers than in the general public. These studies attributed the lower psychological impact on healthcare workers to their knowledge of the disease and their coping abilities to counter the threat much better than the general public (Arafa et al., 2021) [32].
The present study found that participants who had relatives or acquaintances die of COVID-19 had greater odds of having depression but not stress or anxiety. This finding is consistent with Gallagher et al. (2020) [33], who identified that having a relative or acquaintance die of COVID-19 was a potential risk factor for psychological impacts and depression. Contrary to the current study, which found no significant association between close infection and depression, a study reported a higher percentage of depression among individuals who had relatives, friends, or family members become infected with COVID-19 (Moghanibashi-Mansourieh, 2020) [15]. An infected family member or close relative aggravates distress and worry, which affects emotions. Thus, this signifies a strong association between all psychological symptoms and infection in close relatives or family members (Cai et al., 2020) [29].
A study conducted to explore the factors affecting healthcare workers' psychological conditions reported that infected colleagues and family members resulted in increased psychological distress. These findings were commonly observed in areas more severely affected by COVID-19 (Dai et al., 2020) [34].
Furthermore, in the present study, fearing exposure to COVID-19 was a significant predictor for anxiety, and Mahbub et al. (2021) reported similar findings among poor urban women in Dhaka, where 51.2% said COVID-19 was the most feared factor and 50.2% feared losing loved ones, which triggered psychological distress among them. Another study reiterated the fact that fear of COVID-19 triggers anxiety among people. COVID-19 also made people anxious about their future careers (Mohammad et al., 2021) [35].
Limitations
Comparing our results with other studies conducted in European countries or China may present vast differences based on the socio-demographic and cultural perspectives between populations of different communities. The survey was performed via online channels, which may contribute to non-response bias; however, the survey lasted for more than two weeks to increase responses. The results from this study might be subjected to selection bias and information bias (Pannucci et al., 2010) [36]. Since the information was collected via remote social channels and online surveys, the information given can be reliable and effective only up to a specific limit (Lefever et al., 2007) [37]. Since the study is cross-sectional, the course and timing of psychological events cannot be accurately defined; hence, a longitudinal study design could provide information about long-term psychological impacts. However, regardless of its limitations, the study represents COVID-19's impact on the people of Abha. Additionally, the study establishes a foundation for future researchers regarding the factors influencing mental health and the ways to help minimize their impact.
Conclusion
The virulence of this virus has not only raised public health concerns but has also caused various other mental and psychological disorders. According to this study, COVID-19 poses mental health problems among individuals and communities. There is a need to find the more susceptible individuals for mental health issues or other psychological disorders. Mental health and psychological problems can be resolved with health education, counseling, and appropriate interventions to curb the negative health impacts of COVID-19.
Authors Contributions
"R.C.'s conception of the study, designing the study, the data acquisition, initial drafting of the article, Approved the final version H. A Conception of the study, designing the study, and initial drafting of the article, resource finding, Approved the final version, and agreed to be accountable. N.K.T. Concept design, Data collection, the initial drafting of the article, Supervision, resource finding, Approved the final version. H.R.G. Data initial analysis, drafting of the article, revision, Software, Validation, Approved the final version. M.P. Drafting of the article, revision, plagiarism correction, English grammar, Approved the final version B.R.N.: manuscript revised, data analysis, L.K.V.R. The final revision of the Manuscript, plagiarism correction, and the final editing before submitting it. "All authors read and approved the final manuscript." All authors have read and agreed to the published version of the manuscript.
Ethical Considerations
The Directorate of Health Affairs-Assir region, Regional Committee for Research Ethics (H-06-B-091) approved bearing the ethical approval number REC-NO: REC-01-07-2021 dated 01-07-2021.
Acknowledgments
We want to thank all the participants and those who helped to circulate this survey during the data collection process.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Center for Disease Control and Prevention. Coronavirus disease 2019 (COVID-19). Last Updated Apr. 5, 2021. Available from https://www.cdc.gov/coronavirus/2019-ncov/more/science-and-research/surface-transmission.html.
- Awwad F, Mohamoud M, Abonazel M. Estimating COVID-19 cases in Makkah region of Saudi Arabia: Space-time ARIMA modeling. PLOS ONE. 2021;16(4): e0250149. [CrossRef]
- Alshammari T, Altebainawi A, Alenzi K. Importance of early precautionary actions in avoiding the spread of COVID-19: Saudi Arabia as an example. Saudi Pharmaceutical Journal.2020;28:898-902. [CrossRef]
- Aldarhami A, Bazaid A, Althomali O, Binsaleh N. Public perceptions and commitment to social distancing “staying-at-home” during COVID-19 pandemic: A national survey in Saudi Arabia. International Journal of General Medicine, 2020;13: 677-686. [CrossRef]
- Li X, Wu H, Meng F, Li L, Wang Y, Zhou M. Relations of COVID-19-Related Stressors and Social Support with Chinese College Students' Psychological Response During the COVID-19 Pandemic. Front Psychiatry. 2020;11:551315. [CrossRef]
- Hazarika M, Das S, Bhandari SS, Sharma P. The psychological impact of the COVID-19 pandemic and associated risk factors during the initial stage among the general population in India. Open J Psychiatry Allied Sci. 2021;12(1):31-35. [CrossRef]
- Barzilay R, Moore TM, Greenberg DM, et al. Resilience, COVID-19-related stress, anxiety, and depression during the pandemic in a large population enriched for healthcare providers. Transl Psychiatry 2020:10:291. [CrossRef]
- Mazza C, Ricci E, Biondi S, Colasanti M, Ferracuti S, Napoli C, Roma P. A Nationwide Survey of Psychological Distress among Italian People during the COVID-19 Pandemic: Immediate Psychological Responses and Associated Factors. International Journal of Environmental Research and Public Health. 2020; 17(9):3165. [CrossRef]
- Rafique N, Al Tufaif F, Alhammali W, Alalwan R, Aljaroudi A, AlFaraj F, Latif R, Ibrahim Al-Asoom L, Alsunni AA, Al Ghamdi KS, Salem AM, Yar T. The Psychological Impact of COVID-19 on Residents of Saudi Arabia. Psychol Res Behav Manag. 2022; 15:1221-1234. [CrossRef]
- Ali, A., Ahmed, A., Sharaf, A., Kawakami, N., Abdeldayem, S., & Green, J. (2017). The Arabic version of the Depression Anxiety Stress Scale-21: Cumulative scaling and discriminant-validation testing. Asian Journal of Psychiatry, 30, 56-58. [CrossRef]
- Shaw T, Campbell M, Runions K, Zubrick S. Properties of the DASS-21 in an Australian community adolescent population. Journal of Clinical Psychology 2016;73(7): 879-892. [CrossRef]
- Ghazawy ER, Ewis AA, Mahfouz EM, Khalil DM, Arafa A, Mohammed Z, Mohammed EF, Hassan EE, Abdel Hamid S, Ewis SA, Mohammed AES. Psychological impacts of the COVID-19 pandemic on university students in Egypt. Health Promot Int. 2021 Aug 30;36(4):1116-1125. [CrossRef]
- Qiu J, Shen B, Zhao M, Wang Z, Xie B, Xu Y. A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: implications and policy recommendations. Gen Psychiatr. 2020;33(2): e100213. Erratum in: Gen Psychiatr. 2020 Apr 27;33(2): e100213corr1.. [CrossRef]
- Jiménez Ó, Sánchez-Sánchez LC, García-Montes JM. Psychological Impact of COVID-19 Confinement and Its Relationship with Meditation. International Journal of Environmental Research and Public Health. 2020;17(18):6642. [CrossRef]
- Moghanibashi-Mansourieh A. Assessing the anxiety level of the Iranian general population during the COVID-19 outbreak. Asian J Psychiatr. 2020;51:102076. [CrossRef]
- Downs N, Galles E, Skehan B, Lipson SK. Be True to Our Schools-Models of Care in College Mental Health. Curr Psychiatry Rep. 2018;20(9):72. [CrossRef]
- Mortier P, Auerbach RP, Alonso J, Bantjes J, Benjet C, Cuijpers P. WHO WMH-ICS Collaborators. Suicidal Thoughts and Behaviors Among First-Year College Students: Results From the WMH-ICS Project. J Am Acad Child Adolesc Psychiatry. 2018;57(4):263-273.e1. [CrossRef]
- Martínez-Líbano J, Yeomans MM, Oyanedel JC. Psychometric Properties of the Emotional Exhaustion Scale (ECE) in Chilean Higher Education Students. Eur J Investig Health Psychol Educ. 2022;12(1):50-60. [CrossRef]
- Acharya L, Jin L, Collins W. College life is stressful today–Emerging stressors and depressive symptoms in college students. Journal of American college health. 2018;66(7):655-664. doi:10.1080/07448481.2018.1451869.
- Heckman S, Lim H, Montalto C. Factors related to financial stress among college students. Journal of Financial Therapy. 2014;5(1):19–39. [CrossRef]
- Shifera N, Mesafint G, Sayih A, Yilak G, Molla A, Yosef T, Matiyas R. The Psychological Impacts During the Initial Phase of the COVID-19 Outbreak, and its Associated Factors Among Pastoral Community in West Omo Zone, South-West Ethiopia, 2020: A Community-Based Study. Psychol Res Behav Manag. 2021;14:835-846. [CrossRef]
- Wang C, Pan R, Wan X, Tan Y, Xu L, Ho CS, Ho RC. Immediate Psychological Responses and Associated Factors during the Initial Stage of the 2019 Coronavirus Disease (COVID-19) Epidemic among the General Population in China. International Journal of Environmental Research and Public Health. 2020; 17(5):1729. [CrossRef]
- Alkhamees AA, Alrashed SA, Alzunaydi AA, Almohimeed AS, Aljohani MS. The psychological impact of COVID-19 pandemic on the general population of Saudi Arabia. Compr Psychiatry. 2020;102:152192. [CrossRef]
- Fu W, Wang C, Zou L., et al. Psychological health, sleep quality, and coping styles to stress facing COVID-19 in Wuhan, China. Transl Psychiatry 2020;10:225. [CrossRef]
- Wang C, López-Núñez M, Pan R, Wan X, Tan Y, Xu L, Choo F, Ho R, Ho C, Aparicio García M The Impact of the COVID-19 Pandemic on Physical and Mental Health in China and Spain: Cross-sectional Study. JMIR Form Res 2021;5(5):e27818 URL: https://formative.jmir.org/2021/5/e27818. [CrossRef]
- Salman M, Asif N, Mustafa ZU, Khan TM, Shehzadi N, Tahir H, Raza MH, Khan MT, Hussain K, Khan YH, Butt MH, Mallhi TH. Psychological Impairment and Coping Strategies During the COVID-19 Pandemic Among Students in Pakistan: A Cross-Sectional Analysis. Disaster Med Public Health Prep. 2022;16(3):920-926. [CrossRef]
- Yeen Huang, Ning Zhao. Mental health burden for the public affected by the COVID-19 outbreak in China: Who will be the high-risk group? Psychology, Health & Medicine. 2021;26:23-34. [CrossRef]
- Ahmed MZ, Ahmed O, Aibao Z, Hanbin S, Siyu L, Ahmad A. Epidemic of COVID-19 in China and associated Psychological Problems. Asian J Psychiatr. 2020;51:102092. [CrossRef]
- Cai X, Hu X, Ekumi IO, Wang J, An Y, Li Z, Yuan B. Psychological Distress and Its Correlates Among COVID-19 Survivors During Early Convalescence Across Age Groups. Am J Geriatr Psychiatry. 2020;28(10):1030-1039. [CrossRef]
- Liu CY, Yang YZ, Zhang XM, Xu X, Dou QL, Zhang WW, Cheng ASK. The prevalence and influencing factors in anxiety in medical workers fighting COVID-19 in China: a cross-sectional survey. Epidemiol Infect. 2020;20:148:e98. [CrossRef]
- Ho CS, Chee CY, Ho RC. Mental Health Strategies to Combat the Psychological Impact of Coronavirus Disease 2019 (COVID-19) Beyond Paranoia and Panic. Ann Acad Med Singap. 2020;49(3):155-160. PMID: 32200399.
- Arafa A, Mohamed A, Saleh L, Senosy S. Psychological Impacts of the COVID-19 Pandemic on the Public in Egypt. Community Ment Health J. 2021;57(1):64-69. [CrossRef]
- Gallagher MW, Zvolensky MJ, Long LJ, Rogers AH, Garey L. The Impact of Covid-19 Experiences and Associated Stress on Anxiety, Depression, and Functional Impairment in American Adults. Cognit Ther Res. 2020;44(6):1043-1051. [CrossRef]
- Dai Y, Hu G, Xiong H, Qiu H, Yuan X, Yuan X. Psychological impact of the coronavirus disease 2019 (COVID-19) outbreak on healthcare workers in China. medRxiv preprint 2020. [CrossRef]
- Mohammad Mahbub Alam Talukder, Md. Tuhin Mia, Nashir Uddin Shaikh, Nasreen Sultana Chowdhury, Md. Ismael, Morshed Alam, Mohammad Ala Uddin. Effects of COVID-19 Pandemic on Depressive Symptoms among Poor Urban Women: A Study in Dhaka City of Bangladesh. Research in Psychology and Behavioral Sciences. 2021;9: 9-16. [CrossRef]
- Pannucci, Christopher J, Wilkins, Edwin G MD. Identifying and Avoiding Bias in Research. Plastic and Reconstructive Surgery 2010;126(2):619-625. |. [CrossRef]
- Lefever S, Dal M, Matthíasdóttir Á. Online data collection in academic research: Advantages and limitations. British Journal of Educational Technology, 2007;38(4): 574-582. [CrossRef]
Figure 1.
Distribution of psychological health parameters as per the DASS 21 scale.
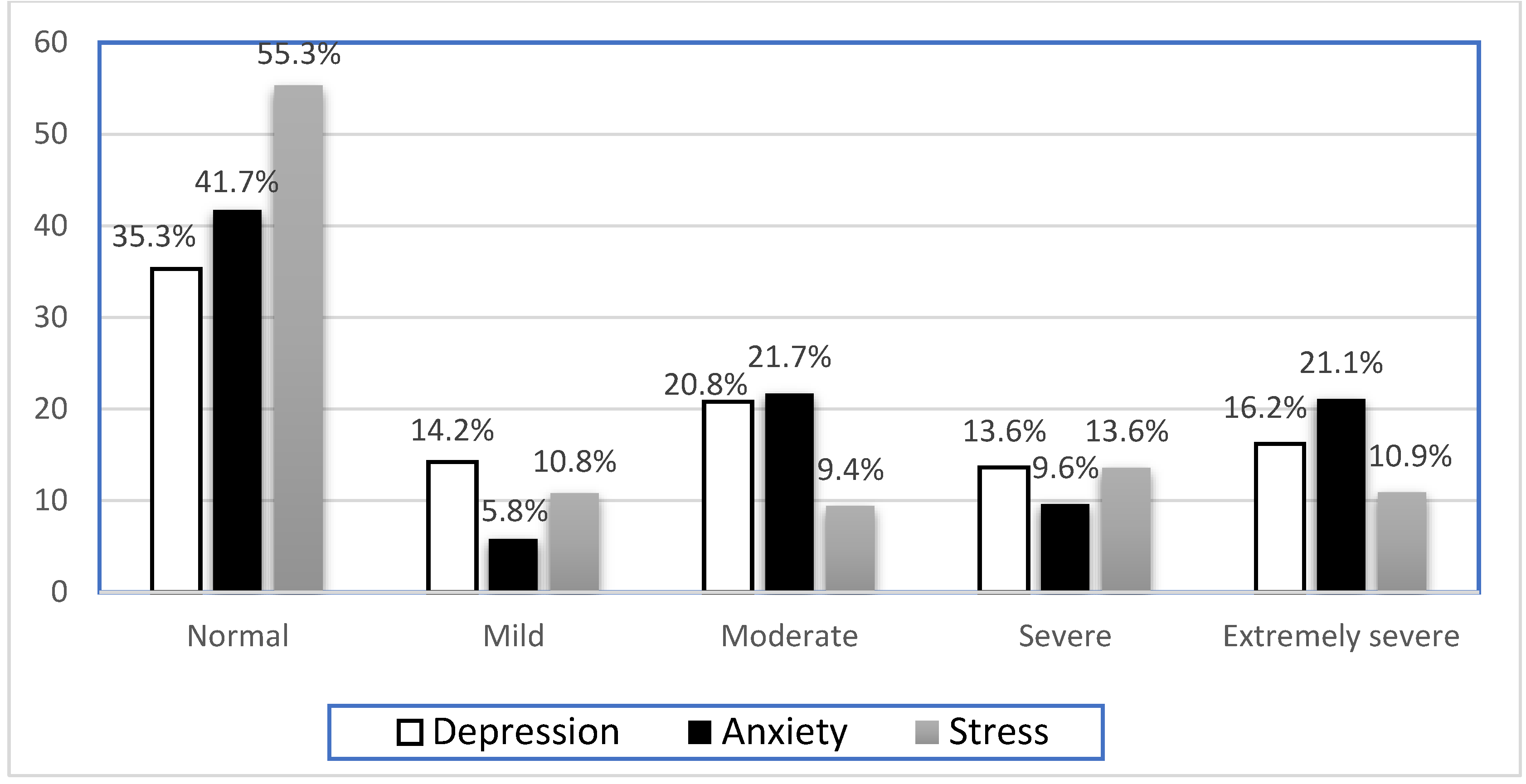
Table 2.
Distribution of study participants based on COVID-19 status.
| COVID-19 Infection | Status | Number | Percentage |
| Have you ever been infected with Covid-19? | Yes No |
276 254 |
52.1% 47.9% |
| Relative or acquaintance infected with COVID-19 | Yes No |
273 257 |
51.5% 48.5% |
| A relative or acquaintance died of COVID-19 | Yes No |
251 279 |
47.4% 52.6% |
| Have you been quarantined? | Yes No |
263 267 |
49.6% 50.4% |
| Have you received psychological support? |
Yes No |
236 294 |
44.5% 55.5% |
| Fearing exposure to COVID-19? | Yes No |
273 257 |
51.5% 48.5% |
Table 3.
Distribution of the study population based on the prevalence of depression, anxiety, and stress.
Table 3.
Distribution of the study population based on the prevalence of depression, anxiety, and stress.
| Depression | Anxiety | Stress | ||||
| No | % | No | % | No | % | |
| Normal | 187 | 35.30% | 221 | 41.7 | 293 | 55.3 |
| Mild | 75 | 14.2 | 31 | 5.8 | 57 | 10.8 |
| Moderate | 110 | 20.8 | 115 | 21.7 | 50 | 9.4 |
| Severe | 72 | 13.6 | 51 | 9.6 | 72 | 13.6 |
| Extremely severe | 86 | 16.2 | 112 | 21.1 | 58 | 10.9 |
| Mean depression score (mean ± SD) | 14.84 ± 10.64 | - | 11.33 ± 10.26 | - | 15.47 ± 12.31 | - |
Table 4.
Distribution of study sample based on DASS-21 scores:.
| Domain | Item | Did not apply to me at all. Never No % |
Applied to me to some degree or some of the time. Sometimes No % |
Applied to me to a considerable degree or a good part of the time. Often No % |
Applied to me very much most of the time. Almost Always No % |
| Depression | I could not seem to experience any positive feelings at all | 178 33.6% | 201 37.9% | 108 20.4% | 43 8.1% |
| I found it difficult to work up the initiative to do things | 162 30.6% | 190 35.8% | 126 23.8% | 52 9.8% | |
| I felt that I had nothing to look forward to | 225 42.5% | 160 30.2% | 104 19.6% | 41 7.7% | |
| I felt downhearted and blue | 143 27.0% | 158 29.8% | 117 22.1% | 112 21.1% | |
| I was unable to become enthusiastic about anything | 166 31.3% | 145 27.4% | 114 21.5% | 102 19.2% | |
| I felt I wasn’t worth much as a person | 316 59.6% | 104 19.6% | 74 14.0% | 36 6.8% | |
| I felt that life was meaningless | 251 47.4% | 110 20.8% | 90 17.0% | 79 14.9% | |
| Anxiety | I was aware of the dryness of my mouth. | 226 42.6% | 165 31.1% | 83 15.7% | 56 10.6% |
| I experienced breathing difficulty | 296 55.8% | 123 23.2% | 68 12.8% | 43 8.1% | |
| I experienced trembling | 306 57.7% | 124 23.4% | 59 11.1% | 41 7.7% | |
| I was worried about situations in which I might panic and make a fool of myself. | 261 49.2% | 135 25.5% | 80 15.1% | 54 10.2% | |
| I felt I was close to panic | 300 56.6% | 127 24.0% | 58 10.9% | 45 8.5% | |
| I was aware of the action of my heart in the absence of physical exertion. | 266 50.2% | 145 27.4% | 65 12.3% | 54 10.2% | |
| I felt scared without any good reason. | 245 46.2% | 148 27.9% | 81 15.3% | 56 10.6% | |
| Stress | I found it hard to wind down | 184 34.7% | 184 34.7% | 98 18.5% | 64 12.1% |
| I tended to over-react to situations | 222 41.9% | 164 30.9% | 91 17.2% | 53 10.0% | |
| I felt that I was using a lot of nervous energy | 178 33.6% | 163 30.8% | 96 18.1% | 93 17.5% | |
| I found myself getting agitated | 175 33.0% | 160 30.2% | 117 22.1% | 78 14.7% | |
| I found it difficult to relax | 189 35.7% | 160 30.3% | 87 16.4% | 94 17.7% | |
| I was intolerant of anything that kept me from getting on with what I was doing. | 204 38.5 | 172 32.5% | 85 16.0% | 69 13.0% | |
| I felt that I was rather touchy | 186 35.1% | 169 31.9% | 99 18.7% | 76 14.3% |
Table 5.
Binary logistic regression for sociodemographic factors and their association with the psychological impact of COVID-19.
Table 5.
Binary logistic regression for sociodemographic factors and their association with the psychological impact of COVID-19.
| Dependent variables and significantly associated variables | Adjusted OR (95% CI) | P-value |
| Dependent variable: Depression** | ||
| Age group 19-25 years |
2.01 (1.00 – 4.04) |
0.049* |
| 26-35 years 36-45 years 46-55 years 55-65 years |
1.79 (0.83 – 3.88) 2.20 (0.90 – 5.37) 1.56 (0.50 – 4.87) 0.23 (0.00 – 0.00) |
0.139 0.045* 0.334 0.999 |
| Sex (Male) | 0.97 (0.64 - 1.49) | 0.898 |
| Nationality (Saudi) | 0.22 (0.03 - 1.91) | 0.171 |
| Marital status Married Single |
1.89 (0.81 – 4.44) 2.76 (1.00 – 7.59) |
0.143 0.050* |
| Level of education Less than secondary Secondary |
0.542 (0.17 – 1.71) 0.934 (0.55-1.58) |
0.295 0.799 |
| Level of income <5000 5000-10000 10000-20000 |
0.57 (0.33 – 1.00) 0.76 (0.42 – 1.35) 0.89 (0.33 -2.41) |
0.050* 0.346 0.820 |
| Do you work (yes) | 0.62 (0.37 – 1.04) | 0.068 |
| Dependent variable: Anxiety** | ||
| Age 19-25 years |
1.33 (0.67 – 2.62) |
0.411 |
| 26-35 years 36-45 years 46-55 years 56-65 years Sex (Male) |
0.72 (0.34 – 1.53) 1.31 (0.55 – 3.09) 1.34 (0.44 – 4.10) 2.76 (0.44 – 17.2) 0.67 (0.44 – 1.02) |
0.397 0.542 0.605 0.277 0.064 |
| Nationality (Saudi) | 0.64 (0.15 -2.74) | 0.555 |
| Marital status Married Single |
1.98 (1.09 – 3.60) 1.04 (0.44 – 2.46) |
0.025* 0.926 |
| Level of education Less than secondary Secondary |
1.39 (0.45 – 4.36) 1.32 (0.79 – 2.20) |
0.570 0.293 |
| Level of income <5000 5000-10000 10000-20000 |
1.64 (0.64 -4.17) 1.03 (0.41 – 2.60) 1.15 (0.46 – 2.89) |
0.302 0.949 0.761 |
| Do you work? | 1.32 (0.80 – 2.20) | 0.280 |
| Dependent variable: Stress** | ||
| Age 19-25 years |
1.72 (0.89 – 3.32) |
0.106 |
| 26-35 years 36-45 years 46-55 years 56-65 years Sex (Male) |
1.14 (0.54 – 2.42) 1.50 (0.64 – 3.54) 1.47 (0.49 – 4.42) 1.55 (0.30 – 7.97) 0.90 (0.59 – 1.35) |
0.725 0.350 0.492 0.600 0.594 |
| Nationality (Saudi) | 0.67 (0.18 – 2.48) | 0.553 |
| Marital status Married Single |
2.16 (1.21 – 3.83) 0.89 (0.38 – 2.09) |
0.009* 0.797 |
| Level of education Less than secondary Secondary |
1.60 (0.53 – 4.79) 1.13 (0.68 – 1.87) |
0.403 0.634 |
| Level of income <5000 5000-10000 10000-20000 |
0.59 (0.34 – 1.00) 0.85 (0.48 – 1.48) 1.19 (0.48 – 2.99) |
0.050* 0.556 0.706 |
| Do you work? | 1.13 (0.69 – 1.85) | 0.635 |
Table 6.
Binary logistic regression for associated factors of COVID-19 and their psychological impacts among the Abha community:.
Table 6.
Binary logistic regression for associated factors of COVID-19 and their psychological impacts among the Abha community:.
| Dependent variables and significantly associated variables | Adjusted OR (95% CI) | P-value |
| Dependent variable: Depression** | ||
| Healthcare practitioner (Yes) |
1.89 (1.18 – 2.92) | 0.007 |
| Have you ever been infected with COVID-19? (Yes) |
1.34 (0.92 – 1.95) | 0.125 |
| Relative or acquaintance died of COVID-19 (Yes) |
0.65 (0.45 – 0.95) | 0.026* |
| Have you been quarantined? (Yes) | 1.31 (0.91 – 1.90) | 0.153 |
| Have you received psychological support (Yes) |
1.16 (0.78 – 1.71) |
0.472 |
| Fearing exposure to COVID-19 (Yes) | 1.26 (0.86 – 1.83) | 0.234 |
| Dependent variable: Anxiety** | ||
| Healthcare practitioner (Yes) | 1.27 (0.81 – 1.98) | 0.293 |
| Have you ever been infected with COVID-19 (Yes) | 1.01 (0.70 – 1.44) | 0.956 |
| Relative or acquaintance died of COVID-19 (Yes) |
0.81 (0.56 – 1.16) |
0.249 |
| Have you been quarantined? (Yes) | 0.97 (0.68 – 1.38) | 0.873 |
| Have you received psychological support (Yes) |
0.90 (0.62 – 1.31) |
0.577 |
| Fearing exposure to COVID-19? (Yes) | 1.46 (1.02 – 2.09) | 0.039* |
| Dependent variable: Stress** | ||
| Healthcare practitioner (Yes) | 0.92 (0.59 – 1.43) | 0.697 |
| Have you ever been infected with COVID-19 (Yes) |
0.78 (0.55 – 1.11) |
0.171 |
| Relative or acquaintance died of COVID-19 (Yes) |
1.03 (0.72 – 1.47) |
0.875 |
| Have you been quarantined? (Yes) | 0.84 (0.59 – 1.19) | 0.331 |
| Have you received psychological support (yes) | 0.93 (0.64 – 1.35) | 0.697 |
| Fearing exposure to COVID-19 (Yes) | 0.75 (0.52 – 1.07) | 0.107 |
| OR – Odds ratio CI’s – Confidence interval Bolded OR & CI’s: p-value ≤0.05. **– depression >9, Anxiety >7 and stress >14 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



