Submitted:
02 June 2023
Posted:
05 June 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Background: Early rehabilitation is an important strategy for the treatment of severe diseases. The study aimed to assess the efficacy of early rehabilitation of patients with mild-to-moderate COVID-19. Methods: The retrospective single-center study with propensity score matching. Results: 180 patients (54 (44 - 62.3) yo) divided into three equal groups: 1 - physical exercises; 2 - physical exercises and chest massage in an electrostatic field; 3 - no rehabilitation. The length of stay (LOS) in the hospital in group 1 was 14 (11-15) days, group 2 - 13 (11-15) days, group 3 - 15 (13-18) days, p=0.0026. Physical exercises for patients with CT-1 improved the quality of life, assessed by the EQ-5D questionnaire, by reducing the level of anxiety and depression. The Hazard Ratio (HR) for desaturation (<93%) was 2.34 (95% Confidence Interval (CI) 1.18-4.63) for group 2, p=0.001. The HR for C-reactive protein level above 50 mg/l in patients with CT-2 was 2.33 (95% CI 1.56-3.47), p=0.0001. Conclusions: Rehabilitation programs are safe for СOVID-19-patients; reduce hospital LOS; improve the quality of life. Continuous monitoring of a patient's condition during rehabilitation is essential. ClinicalTrials.gov ID: NCT0580836
Keywords:
COVID-19
; early rehabilitation
; computed tomography
; physical exercises
; chest massage in an electrostatic field.
1. Introduction
Globally, nearly 3.3 million new cases and over 23 000 deaths were reported in the last 28 days (March, 6 to April, 2 2023), a decrease of 28% and 30%, respectively, compared to the previous 28 days (February, 6 to March, 5 2023). As of April, 2 2023, over 762 million confirmed cases and over 6.8 million deaths have been reported globally [1].
Physical exercise is an effective therapeutic strategy to mitigate the consequences of SARS-CoV-2 infection [2].
For COVID-19 patients, an integrated rehabilitative process is recommended, involving a multidisciplinary and multi-professional team providing neuromuscular, cardiac, respiratory, and swallowing interventions, and psychological support, to improve patients’ quality of life [3,4,5,6]. Unfavorable responses to exercise have influenced the wider debate on how to reintegrate physical activity and exercise while simultaneously managing symptoms during recovery from post-COVID-19 syndrome [7].
A recent cross-sectional study indicated that young individuals with mild COVID-19 with preserved lung function have long-term muscle weakness, decreased physical activity level, increased cough, and perception of dyspnea and fatigue [8]. It is necessary to formulate rehabilitation programs for these patients, to help them restore physical and respiratory function and to reduce anxiety and depression, particularly patients with comorbidities and those who live alone or in rural settings, to restore a good quality of life [9].
Several publications show the effectiveness of rehabilitation in reducing the duration of non-invasive respiratory support, reducing the risk of complications, and mortality [10,11,12,13,14]. Rehabilitation can be started in a hospital setting, even in intensive care unit (ICU) [15]. Various methods of rehabilitation have been described [6,15,16,17,18].
Adults and elderly patients surviving COVID-19 seem to improve their functional status, despite previous admission to ICU, through a short, individualized rehabilitation consisting of a 30-minute 7 days multicomponent therapeutic exercise intervention combined with resistance, endurance, and balance training [19].
There is a clear consensus that early rehabilitation is an important strategy for the treatment of polyneuropathy and myopathy in critical diseases to facilitate and improve long-term recovery. Early rehabilitation and exercise prescriptions remain to be further optimized, especially for hospitalized patients [9]. A recent retrospective observational cohort study of patients with COVID-19 showed a benefit from inpatient rehabilitation, as did their non-COVID-19 counterparts with similar rehabilitation-specific diagnoses [20].
The study aimed to assess the efficacy of early rehabilitation (physical exercises, chest massage in an electrostatic field) of patients with mild-to-moderate COVID-19 based on clinical, laboratory, and instrumental data.
2. Materials and Methods
2.1. Setting and Ethics
The retrospective single-center study with propensity score matching was conducted in clinical hospital No. 1 of the “MEDSI” group, which was a designated hospital for COVID-19 patients. The diagnosis of COVID-19 was established according to the World Health Organization interim guidance [4]. Between April 01, 2020, and June 15, 2021, 1551 consecutively admitted COVID-19 patients were screened. The study protocol conformed to the ethical guidelines of the 1975 Declaration of Helsinki. The authors followed the STROBE checklist. The study was approved by a Local Ethics Committee of I.M. Sechenov First Moscow State Medical University (Protocol #19-22, October 06, 2022). ClinicalTrials.gov ID: NCT05808361.
Inclusion Criteria:
- all patients (age 18-75 y.o.) with COVID-19 admitted to the hospital with mild or moderate COVID-19 (5-50% of lung damage according to CT-scan), hospital length of stay - 7-30 days.
Exclusion Criteria:
- less than 7 days in hospital for any reason,
- chronic decompensated diseases with extrapulmonary organ dysfunction (tumor progression, liver cirrhosis, congestive heart failure), admission to ICU,
- Patients with less than 2 chest computed tomography studies during hospitalization. Patients without signs of viral pneumonia according to computed tomography (CT-0 severity criteria). Patients with a total lesion of the lungs according to computed tomography (CT-4 severity criteria).
- Patients in whom more than 30 days have passed since the onset of the disease and before hospitalization,
- Patients who received treatment in the ICU, as well as patients who died.
2.2. Rehabilitation Programs
Rehabilitation programs include physical exercises, and chest massage in an electrostatic field, started in the first 3 days after the patient’s body temperature returned to normal.
The demographic and clinical data were collected. Laboratory data (white blood cells count, C-reactive protein), and Instrumental data (pulse oximetry, CT scan) were analyzed. Rehabilitation evaluation - Health profiles according to the EQ-5D quality of life questionnaire before and after each rehabilitation mode were analyzed.
Upon admission to the hospital, all patients signed an informed consent. All patients received basic therapy for a new coronavirus infection by the current interim guidelines of the Ministry of Health at the time of hospitalization.
The patients were divided into three groups:
Group 1: 60 patients hospitalized with a new coronavirus infection and, in addition to basic therapy, received a rehabilitation program that included physical exercises;
Group 2: 60 patients hospitalized with a new coronavirus infection and, in addition to basic therapy, received a rehabilitation program that included physical exercises, and chest massage in an electrostatic field;
Group 3: 60 patients hospitalized with a new coronavirus infection. Patients received treatment according to the temporary guideline without any rehabilitation program.
Patients within each group were divided into 2 subgroups: subgroup following the CT scan: subgroup A - CT-1; subgroup B - CT-2. Each subgroup included 30 patients (Figure 1).
The complex therapeutic exercises included exercises in the initial position of lying, sitting, and standing. In active and static motor modes under the continuous monitoring of saturation (including oxygen support, if necessary, to maintain the saturation level of more than 93%), heart rate, and respiratory rate monitoring. Breathing exercises, including respiratory muscles, elements of sound and drainage gymnastics, and diaphragmatic breathing. Aerobic exercises to increase tolerance to physical activity in a sparing motor mode.
The kinesiotherapy included exercises that improve the ventilation and drainage function of the lungs, prevent the development of atelectasis and fibrosis of the lung tissue, increase the mobility of the diaphragm, improve the functional state of the respiratory muscles, and increase the elasticity of the chest.
An important component of respiratory gymnastics was teaching diaphragmatic breathing, which contributed to enhancing of the patient’s tolerance to physical activity. The methodological basis was made up of multiple repetitions of technically simple exercises that ensured successive impact on all major muscle groups: lower and upper limbs, shoulder girdle, back, and abdominals. The exercises were aimed at training various muscle groups, combined with frequent changes in starting positions, combined with postural drainage techniques.
Physical rehabilitation of the respiratory function was carried out using methods of pulmonary rehabilitation, including inspiratory training with breathing exercises; forced expiratory maneuver with forced exhalation; method of active cyclic breathing; postural drainage. The methodology for conducting kinesiotherapy included seven basic principles:
- -
- Positioning with the active patient’s participation and teaching to regularly change the position of the body.
- -
- Verticalization taking into account the mRMI-ICU mobility index.
- -
- Dynamic physical exercises of low intensity: passive, passive-active, and active exercises for small and medium muscle groups, depending on the severity of the disease and the clinical condition of the patient. If a mobility index mRMI-ICU ≥ 6 points, in case of good tolerance of physical activity, exercises involving large muscle groups were added.
- -
- Elements of strength training.
- -
- Exercises to restore balance.
- -
- Physical exercises that increase the mobility of the chest.
- -
- Breathing exercises: an extended exhalation, localized breathing, diaphragmatic breathing; separate dynamic breathing exercises in a gentle mode at a slow pace. Lungs overdistension and fast and strong movements of the chest were avoided.
The duration of each class was 20 minutes, gymnastics was carried out 2 times a day (morning and evening) for 10 days.
Exercise termination criteria: (1) Fluctuations in body temperature > 37.2 °C; (2) respiratory symptoms and fatigue worsen and are not relieved after rest; saturation level of less than 87%; (3) investigator stops patient’s activities immediately if the following symptoms occur: tachycardia of more then 50% from initial rate, chest tightness, chest pain, breathing difficulties, shortness of breath, severe cough, dizziness, headache, blurred vision, palpitations, sweating, trouble standing, and other symptoms.
Hardware massage in an electrostatic field with a frequency of 30/60 Hz («Elgos», «Madin», Russia) of the chest area was performed to improve the drainage function of the lungs, a course of 10 procedures, daily, the duration of the procedure was 20 minutes.
2.3. Laboratory and Instrumental Examination
Instrumental examination methods included: computed tomography (LightSpeed VCT, (General Electric, USA), and Brilliance iCT Elite (Philips, Nederland). Scanning was carried out in axial projection with a slice thickness of 0.625-1 mm at mA350-400 and 120kV followed by iterative reconstruction. The percentage of lung damage was calculated using the IntelliSpace Portal V11 workstation using the COPD module by temporary guidelines [6].
Determination of the level of CRP was carried out by the method of immunoturbidimetry on analytical equipment (biochemical analyzer) manufactured by Beckman Coulter.
The assessment of the quality of life of patients was carried out based on the EQ–5D quality of life questionnaires (EuroQol Research Foundation). Patients completed this questionnaire twice, on the first day of hospitalization and the day of discharge.
2.4. Statistical Analysis
Statistical analysis was carried out using STATISTICA 13.3 (StatSoft.Inc) and BioStat (AnalystSoft Inc), Microsoft® Excel™ 2016 software, and the Power Pivot module. A method of pseudo-randomization (propensity score matching) was used. For pseudo-randomization, such confounders as levels of saturation, C-reactive protein at admission, sex and age of patients, and the presence of concomitant diseases such as respiratory failure, and diabetes mellitus were included. The normality of distribution was determined using the Shapiro-Wilk test (when the number of subjects was less than 50) or the Kolmogorov-Smirnov test (when the number of subjects was more than 50). Continuous and categorical variables were presented as median (Interquartile range, IQR), mean (95% confidence interval (CI)) or n (%), as appropriate. A comparison of quantitative characteristics of three groups Kruskal-Wallis test was performed following the Mann-Whitney U test for pairwise comparison. The χ2 tests (2×2) or Fisher’s exact test (if there were less than 10 observations) were performed to assess the significance of the differences between the characteristics according to the categorical variables. The outcomes were compared using the Kaplan-Meier survival analysis. To test for differences between two related samples the Wilcoxon W-test was used. McNemar’s test was used to compare relative indicators characterizing related populations (before and after treatment). Patient survival was analyzed using the Cox regression method. A P-value of less than 0.05 was considered statistically significant.
3. Results
3.1. Length of Stay in the Hospital
One hundred and eighty patients (54 (44 - 62.3) y, 50% male) were enrolled in the present study. The total length of stay in the hospital was 14 (12 - 16) days. The length of stay in the hospital in the first group was 14 (11-15) days, in the second - 13 (11-15) days, and in the third group - 15 (13-18) days, р=0.0026. The length of stay in the hospital according to the CT data is presented in Table 1. The length of stay in the hospital was shorter in both rehabilitation groups with CT-1 and CT-2 compared with group 3 (p=0.0637 and p=0.0026, respectively), Table 1.
The lungs injury at admission in group 1 was 25.4 (15.7-36.0)%; in group 2 - 25.2 (16.0-38.5)%; in group 3 - 26.1 (15.3-40.0)%, p>0.005; at discharge in group 1 - 19.7 (12.5-28)%, p<0.005 compared with the initial values; in the group 2 - 22.6 (14.9-32.2)%, p>0.005; in the group 3 - 24.1 (15.8-33)%, p>0.005.
3.2. Dynamics of Complaints
At admission, 278 complaints of weakness, shortness of breath, cough, and headache were recorded, by the time of discharge the number of complaints decreased to 182. The dynamics of complaints in the study groups are presented in Table 2.
3.3. Laboratory and Instrumental Data
There was no difference in the groups in the level of C-reactive protein at admission and at discharge (p=0.110 and p=0.423, respectively), Table 3.
The level of CRP above 50 mg/l (as an undesirable event) appeared on the 3rd (1-4) day of treatment and persisted for 5 (3-7) days. These data within groups and subgroups are presented in Table 4.
The hazard ratio (HR) for the onset of the CRP level above 50 mg/l in subgroups of patients with CT-2 at admission was 2.33 (95% CI 1.56-3.47), p=0.0001. The HR for the duration of the CRP level above 50 mg/l in subgroups of patients with CT-2 was 2.10 (95% CI 1.41-3.12), p=0.0001. Log-rank test for subgroups «B» by the time of onset of the CRP above 50 mg/l, p= 0.00001; for the duration of the CRP level above 50 mg/l, p=0.00017 (Figure 2a,b).
The level of leukocytes in the blood upon admission in group 1 was 5.26*10-9/l (3.78-6.57*10-9/l); in group 2 - 5.57*10-9/l (4.12-6.75*10-9/l); in group 3 - 5.18*10-9/l (3.92-6.43*10-9/l), p=0.748. At discharge in group 1, the level of leukocytes was 5.92*10-9/l (5.05-6.76*10-9/l); in the group 2 - 5.75*10-9/l (4.62-7.6*10-9/l); in group 3 - 5.92*10-9/l (4.75-7.12*10-9/l), p=0.883. Among all patients, the level of leukocytes in the blood exceeded 6.16 * 10-9/l on the 3rd (1-7th) day of hospitalization. The duration of the high level of leukocytes was 7 (2-10) days, there was no significant difference between the groups.
Saturation upon admission in group 1 was 96.3 (95.2% -97)%, in group 2 - 95.6 (93.8% -97)%, and in group 3 - 97 (95% -98)%. At discharge: in group 1 saturation was 98 (95.5-98.1)%, in group 2 - 97% (95.5%-98)%, in group 3 - 98 (96-98)%, p>0.05.
The HR for desaturation (saturation below 93%) for group 2 compared with the first group was 2.34 (95% CI 1.18-4.63), p=0.001, Figure 3.
An analysis of blood pressure at various periods of treatment showed the absence of any significant effect of rehabilitation programs (both therapeutic exercises and their complex in conjunction with the massage procedures in the electrostatic field of the chest area) and the severity of the disease.
3.4. The Quality of Life
The health profile according to the EQ-5D quality of life questionnaire at admission is presented in Table 5.
Physical exercises for patients with CT-1 (but not CT-2) significantly improved the quality of life by reducing the level of anxiety and depression, compared with patients who did not receive rehabilitation treatment or received complex rehabilitation, Table 6.
4. Discussion
This article discusses two rehabilitation programs (physical exercises alone and in combination with chest massage in an electrostatic field) and the lack of rehabilitation in patients hospitalized in an infectious hospital with mild or moderate COVID-19 pneumonia (CT-1 or CT-2).
Many studies highlighted the importance of kinesiotherapy especially in elderly patients since the decrease in motor activity that inevitably occurs with COVID-19 leads to high risks of developing sarcopenia, muscle weakness, and decompensation of chronic cardiopulmonary diseases, which in turn can lead to the development of acute respiratory distress syndrome and impaired immune response [21,22,23].
In our study 180 patients (54 (44 - 62.3) yo) were enrolled, 120 of them got rehabilitation treatment, and the outcomes were better compared to the control group of patients (without rehabilitation).
4.1. Length of Stay in the Hospital
The main findings of this study were that patients with COVID-19 pneumonia (CT-2) who completed one of the rehabilitation programs were discharged from the hospital 2 days earlier than patients without rehabilitation. There were no significant differences in the length of stay in the hospital in patients with CT-1. The same results were described in a recent study in a cohort of 76,395 adults. It was found that patients who engaged in both aerobic and muscle-strengthening activities according to the 2018 physical activity guidelines had a lower risk of SARS-CoV-2 infection, severe COVID-19, and COVID-19-related death than those who engaged in insufficient activities. The length of stay in the hospital was shortened to approximately 2 days in patients who performed both aerobics and muscle strengthening [24].
There is a direct dose-response relationship between physical activity and COVID-19 outcomes, including reduction of hospital length of stay in patients who remain physically active [25,26,27].
In the acute phase, which is mainly characterized by respiratory disorders, early respiratory rehabilitation is encouraged, to be performed at the patient’s bedside and continued in a specialized rehabilitation unit, to improve the chances of recovery [28].
According to the clinical practice recommendations, respiratory physiotherapy interventions in hospital wards or ICU may be indicated for patients who have confirmed or suspected COVID-19 and concurrently or subsequently develop exudative consolidation, mucous hypersecretion, and/or difficulty clearing secretions. Physiotherapists will have an ongoing role in providing interventions for mobilization, exercise, and rehabilitation (eg, in patients with comorbidities creating significant functional decline and/or (at risk of) ICU-acquired weakness [29].
4.2. Early and Safe Start
There are no clear indications of when to start rehabilitation. In the aforementioned articles, the initiation of any type of rehabilitation is based on an individual approach. In our study, we tried to establish the possible «therapeutic window» for the early and safe beginning of respiratory rehabilitation, massage, and mobilization exercise programs. We got the same results as other studies using different rehabilitation methods.
One of them is a retrospective review of 100 patients with COVID-19 infection admitted to a specialized rehabilitation unit, a mean delay from symptom onset to rehabilitation beginning was 20.4±10.0 days, and 26% had more than 50% pulmonary damage on computed tomographic scans. The mean length of rehabilitation stay was 9.8±5.6 days. The therapy program included overall motor strengthening with body weight exercises, elastics, and weights, with approximately 3 series of 10 repetitions for each exercise, according to the patient’s abilities. Respiratory rehabilitation exercises, including controlled diaphragmatic breathing, with work on the inspiratory and expiratory times. Aerobic work included bicycle ergometer sessions at submaximal intensity, with monitoring of vital parameters. Thus, inpatient therapy was associated with substantial functional, motor, and cardiorespiratory improvement. Nonetheless, loss of autonomy and motor weakness persisted at discharge, which occurred approximately a month after the onset of COVID-19 [30].
Another study recommended starting an exercise-based cardiac rehabilitation program in participants with mild-to-moderate symptoms of COVID-19 infection, the exercise program can be resumed gradually, following one week’s free-fever time and 48 hours without a symptom [31].
In a recent observational prospective study including patients with mild-to-moderate and stable-severe COVID-19, with a design and results similar to ours, rehabilitation was initiated (breathing exercises, range of motion exercises to maintain general and segmental mobility of the upper and lower extremities, and strengthening exercises, with the main difference in intensity and progression of treatment, depending on the individual capacity of patients) on the first day after administration, but saturation should have been above 94%. Results of this study implicate that a supervised early rehabilitation program, implemented in the treatment of patients with COVID-19 disease in the acute phasis a feasible way to significant improvement of patients’ functional outcomes [5].
It was established that muscle strength and mass assessed upon hospital admission are predictors of hospital length of stay in patients with moderate to severe COVID-19 [32].
4.2. Safety of the Rehabilitation Programs
One of the leading symptoms of a new coronavirus infection is respiratory failure. Leukopenia, high levels of CRP, and saturation below 93% are criteria for an unfavorable outcome. Leukocytosis is one of the signs of a bacterial infection. One of the criteria for discharge of a patient, in addition to stabilization of clinical and laboratory parameters, is a positive dynamics on CT scan of the lungs, or the absence of a negative dynamics. Several publications demonstrate critical values of the leukocyte level of 6.16*10-9/l, above which the prognosis of the disease worsens [33].
In our study rehabilitation programs did not lead to a negative impact on the level of leukocytes in the blood, the dynamics of CRP, the frequency of desaturation below 93%, and the level of blood pressure. A significant improvement was revealed in the form of a reduction the lung damage at discharge in patients who received physiotherapy exercises.
Yang et al. proposed a general pulmonary rehabilitation method based on the principle of 4S (simple, safe, satisfy, safe) for patients with pneumonia caused by the novel coronavirus. The Chinese Association of Rehabilitation Medicine made the first recommendation based on expert opinions, differentiating between patients with mild or critical illness and discharged patients [34]. Physical activity that promotes higher cardiorespiratory fitness may improve lung function and have anti-inflammatory effects, which may reduce the harmful effects of COVID-19 in the lungs [35].
4.3. Quality of Life
Liu concluded that a 6-week respiratory rehabilitation program significantly improves respiratory function, quality of life, and anxiety in older patients with COVID-19. Interventions included: (1) respiratory muscle training; (2) cough exercise; (3) diaphragmatic training; (4) stretching exercise; and (5) home exercise [13].
According to our results, physical exercises in combination with chest massage in an electrostatic field helped to reduce complaints of weakness. Physical exercises in patients with CT-1 (but not with CT-2) improved the quality of life, mainly by reducing the level of anxiety and depression, compared with patients who did not receive rehabilitation treatment or received complex rehabilitation. We assume that the reason for this is associated with an increase in wet cough against the background of complex rehabilitation, which led to the appearance of new complaints. The cough contributes to chest pain and increases the patient’s anxiety about these new symptoms. The data obtained are similar to existing publications on the effect of breathing exercises on the quality of life of patients [38]. It was suggested that physical activity is inversely correlated with symptoms of depression among adults and the elderly, symptoms of which develop in the vast majority of patients with COVID-19 [39].
The results of a study on the intensity of cardio-respiratory exercise in the form of walking at an intense pace are interesting, as patients who do not have cyclic training or receive training in the form of low-intensity exercise have almost twice the risk of severe and fatal COVID-19 compared to patients with regular cardio-respiratory training with a selected intensity of the exercises [40].
According to Ladlow P, et al., levels of depression are comparable among all COVID-19-exposed groups. At 5 and 12 months following COVID-19 illness greater exposure to physical training, outdoor work, routine, and team contact of service life may exert a protective effect on mental health. These may have influenced the lower values of depressive symptoms, small effect size differences in mean levels of anxiety (low to mild symptoms), and preserved the quality of life [41].
Although exercise may not directly affect SARS-CoV-2 infection, it may prevent the development of severe COVID-19, improve immune defenses, and counteract the disease’s negative impact on the immune system due to its anti-inflammatory properties, which have been shown to improve outcomes. In addition, exercise is also the most effective therapy for those with asymptomatic or mild infections, and is essential for older patients and people with chronic diseases. Therefore, maintaining a level of exercise helps to reduce the likelihood of decompensation of comorbidities in COVID-19, as well as minimizes possible complications from this disease, and should be recommended for inclusion in the standards of care for patients with COVID-19. However, one of the major obstacles to implementing early rehabilitation treatment of patients with COVID-19 is the reluctance of the rehabilitation team, due to the contagious nature of the disease [2,5].
4.4. Limitations
Several limitations of the current study warrant consideration. This is a single-center study only without mortality. The follow-up period is quite short. Spirometry was not assessed, as there was concern about the infectious risk of its use, and Pa/FiO2 measurements were not possible because patients were not ventilated. A high-risk patient or patients with comorbidities could add a confounding factor to the study.
5. Conclusions
Rehabilitation programs in the form of physical exercises along, as well as in combination with chest massage in an electrostatic field is safe for patients with a new coronavirus infection (with CT-1 or CT-2); reduce the length of stay in the hospital of patients with СT-2 at admission; helps to reduce the number of complaints of weakness during treatment; improve the quality of life by reducing levels of anxiety and depression of patients with СT-1. It is necessary to ensure constant monitoring of patients condition during rehabilitation programs, especially with lung damage of more than 25% according to CT. More future studies, such as randomized controlled trials, studies including different age range groups, and individualized approaches, need to be developed.
Author Contributions
Conceptualization, E.S.K., and N.S.S.; Methodology, D.S.M., and T.R.M.; Formal analysis, D.S.M.; Investigation, S.M.K., D.S.M., E.N.Z., E.E.A., I.V.S., and K.V.L.; Data curation, S.M.K., D.S.M., and E.S.K.; Writing—original draft preparation, S.M.K., D.S.M., and I.A.M.; Writing—review and editing, S.M.K., E.S.K., D.S.M., I.A.M., and A.I.Y.; Supervision, E.S.K., and N.S.S. All authors have read and agreed to the published version of the manuscript. Funding: This research received no external funding.
Institutional Review Board Statement
The study was conducted by the Declaration of Helsinki, and approved by a Local Ethics Committee of I.M. Sechenov First Moscow State Medical University (Protocol #19-22, October 06, 2022).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The datasets generated and analyzed during the study are available from the corresponding author upon reasonable request.
Acknowledgments
We would like to thank our rehabilitation department and laboratory staff for their excellent technical support.
Conflicts of Interest
The authors declare no conflict of interest.
References
- World Health Organization. Weekly epidemiological update on COVID-19 - 6 April 2023 Edition 137 https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19---6-april-2023.
- Filgueira, T.O.; Castoldi, A.; Santos, L.E.R.; de Amorim, G.J.; Fernandes, M.S.d.S.; Anastácio, W.d.L.D.N.; Campos, E.Z.; Santos, T.M.; Souto, F.O. The Relevance of a Physical Active Lifestyle and Physical Fitness on Immune Defense: Mitigating Disease Burden, With Focus on COVID-19 Consequences. Front. Immunol. 2021, 12, 587146. [Google Scholar] [CrossRef]
- Agostini, F.; Mangone, M.; Ruiu, P.; Paolucci, T.; Santilli, V.; Bernetti, A. Rehabilitation setting during and after Covid-19: An overview on recommendations. J. Rehabilitation Med. 2021, 53, jrm00141. [Google Scholar] [CrossRef]
- WHO Clinical management of severe acute respiratory infection when novel coronavirus (nCoV) infection is suspected. Jan 11, 2020. https://www.who.int/publications-detail/clinical-management-ofsevere-acute-respiratory-infection-when-novel-coronavirus-(ncov)-infection-is-suspected (accessed Feb 8, 2020).
- Filipović, T.; Gajić, I.; Gimigliano, F.; Backović, A.; Hrković, M.; Nikolić, D.; Filipović, A. The role of acute rehabilitation in COVID-19 patients. Eur. J. Phys. Rehabilitation Med. 2023, 59, 425–435. [Google Scholar] [CrossRef]
- Malyutin, D.; Koneva, E.; Achkasov, E.; Kostenko, A.; Tsvetkova, A.; Elfimov, M.; Eremenko, A.; Bazarov, D.; Shestakov, A.; Korchazhkina, N. Influence of therapeutic exercises and hardware massage in electrostatic field on lung damage in patients with novel coronavirus pneumonia. Vopr. Kurortol. Fizioter. i Lech. fizicheskoi kul'tury 2022, 99, 43–50. [Google Scholar] [CrossRef]
- Ladlow, P.; Barker-Davies, R.; Hill, O.; Conway, D.; O'Sullivan, O. Use of symptom-guided physical activity and exercise rehabilitation for COVID-19 and other postviral conditions. BMJ Mil. Heal. 2023, e002399. [Google Scholar] [CrossRef]
- Güneş, M.; Yana, M.; Güçlü, M.B. Physical activity levels respiratory and peripheral muscle strength and pulmonary function in young post-COVID-19 patients. Wien. Klin. Wochenschr. 2023, 135, 251–259. [Google Scholar] [CrossRef] [PubMed]
- Demeco, A.; Marotta, N.; Barletta, M.; Pino, I.; Marinaro, C.; Petraroli, A.; Moggio, L.; Ammendolia, A. Rehabilitation of patients post-COVID-19 infection: a literature review. J. Int. Med Res. 2020, 48. [Google Scholar] [CrossRef]
- Hsieh, M.; Lee, W.; Cho, H.; Wu, M.; Hu, H.; Kao, K.; Chen, N.; Tsai, Y.; Huang, C. Recovery of pulmonary functions, exercise capacity, and quality of life after pulmonary rehabilitation in survivors of ARDS due to severe influenza A (H1N1) pneumonitis. Influ. Other Respir. Viruses 2018, 12, 643–648. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.; Chen, J.; Cen, F.; Li, X.; Song, Z.; Peng, M.; Liu, X. Importance of respiratory airway management as well as psychological and rehabilitative treatments to COVID-19 patients. Am. J. Emerg. Med. 2020, 38, 1698–e1. [Google Scholar] [CrossRef]
- Lai, C.-C.; Chou, W.; Chan, K.-S.; Cheng, K.-C.; Yuan, K.-S.; Chao, C.-M.; Chen, C.-M. Early Mobilization Reduces Duration of Mechanical Ventilation and Intensive Care Unit Stay in Patients With Acute Respiratory Failure. Arch. Phys. Med. Rehabilitation 2017, 98, 931–939. [Google Scholar] [CrossRef] [PubMed]
- Liu, K.; Zhang, W.; Yang, Y.; Zhang, J.; Li, Y.; Chen, Y. Respiratory rehabilitation in elderly patients with COVID-19: A randomized controlled study. Complement. Ther. Clin. Pract. 2020, 39, 101166. [Google Scholar] [CrossRef]
- Zhu, C.; Wu, Y.; Liu, H.; Ban, Y.; Ma, X.; Zhang, Z. Early pulmonary rehabilitation for SARS-CoV-2 pneumonia: Experience from an intensive care unit outside of the Hubei province in China. Heart Lung: J. Cardiopulm. Acute Care 2020, 49, 449–450. [Google Scholar] [CrossRef] [PubMed]
- Negm, A.M.; Salopek, A.; Zaide, M.; Meng, V.J.; Prada, C.; Chang, Y.; Zanwar, P.; Santos, F.H.; Philippou, E.; Rosario, E.R.; et al. Rehabilitation Care at the Time of Coronavirus Disease-19 (COVID-19) Pandemic: A Scoping Review of Health System Recommendations. Front. Aging Neurosci. 2022, 13, 781271. [Google Scholar] [CrossRef] [PubMed]
- Sun, T.; Guo, L.; Tian, F.; Dai, T.; Xing, X.; Zhao, J.; Li, Q. Rehabilitation of patients with COVID-19. Expert Rev. Respir. Med. 2020, 14, 1249–1256. [Google Scholar] [CrossRef] [PubMed]
- Ambrose, A.F.; Kurra, A.; Tsirakidis, L.; Hunt, K.C.; Ayers, E.; Gitkind, A.; Yerra, S.; Lo, Y.; Ortiz, N.; Jamal, F.; et al. Rehabilitation and In-Hospital Mortality in COVID-19 Patients. Journals Gerontol. Ser. A 2021, 77, e148–e154. [Google Scholar] [CrossRef] [PubMed]
- Centeno-Cortez, A.K.; Díaz-Chávez, B.; Santoyo-Saavedra, D.R.; Álvarez-Méndez, P.A.; Pereda-Sámano, R.; Acosta-Torres, L.S. Respiratory physiotherapy in post-acute COVID-19 adult patients: Systematic review of literature. Revista Medica del Instituto Mexicano del Seguro Social 2022, 60, 59–66. [Google Scholar] [PubMed]
- Udina, C.; Ars, J.; Morandi, A.; Vilaró, J.; Cáceres, C.; Inzitari, M. Rehabilitation in adult post-COVID-19 patients in post-acute care with Therapeutic Exercise. J. Frailty Aging 2021, 10, 1–4. [Google Scholar] [CrossRef]
- Groah, S.L.; Pham, C.T.; Rounds, A.K.; Semel, J.J. Outcomes of patients with COVID-19 after inpatient rehabilitation. PM&R 2021, 14, 202–209. [Google Scholar] [CrossRef]
- Osterhoff, G.; Noser, J.; Held, U.; Werner, C.M.L.; Pape, H.-C.; Dietrich, M. Early Operative Versus Nonoperative Treatment of Fragility Fractures of the Pelvis: A Propensity-Matched Multicenter Study. J. Orthop. Trauma 2019, 33, e410–e415. [Google Scholar] [CrossRef]
- Wu, C.; Chen, X.; Cai, Y.; Xia, J.; Zhou, X.; Xu, S.; Huang, H.; Zhang, L.; Zhou, X.; Du, C.; et al. Risk Factors Associated With Acute Respiratory Distress Syndrome and Death in Patients With Coronavirus Disease 2019 Pneumonia in Wuhan, China. JAMA Intern. Med. 2020, 180, 934–943. [Google Scholar] [CrossRef]
- Petermann-Rocha, F.; Chen, M.; Gray, S.R.; Ho, F.K.; Pell, J.P.; Celis-Morales, C. New versus old guidelines for sarcopenia classification: What is the impact on prevalence and health outcomes? Age Ageing 2019, 49, 300–304. [Google Scholar] [CrossRef]
- Lee, S.W.; Lee, J.; Moon, S.Y.; Jin, H.Y.; Yang, J.M.; Ogino, S.; Song, M.; Hong, S.H.; Ghayda, R.A.; Kronbichler, A.; et al. Physical activity and the risk of SARS-CoV-2 infection, severe COVID-19 illness and COVID-19 related mortality in South Korea: a nationwide cohort study. Br. J. Sports Med. 2021, 56, 901–912. [Google Scholar] [CrossRef]
- Foulds, H.J.A.; Bredin, S.S.D.; Charlesworth, S.A.; Ivey, A.C.; Warburton, D.E.R. Exercise volume and intensity: a dose–response relationship with health benefits. Eur. J. Appl. Physiol. 2014, 114, 1563–1571. [Google Scholar] [CrossRef]
- Hupin, D.; Roche, F.; Gremeaux, V.; Chatard, J.C.; Oriol, M.; Gaspoz, J.M.; Barthelemy, J.C.; Edouard, P. Even a low-dose of moderate-to-vigorous physical activity reduces mortality by 22% in adults aged >/=60 years: A systematic review and meta-analysis. Br. J. Sports Med. 2015, 49, 1262–1267. [Google Scholar] [CrossRef]
- Brawner, C.A.; Ehrman, J.K.; Bole, S.; Kerrigan, D.J.; Parikh, S.S.; Lewis, B.K.; Gindi, R.M.; Keteyian, C.; Abdul-Nour, K.; Keteyian, S.J. Inverse Relationship of Maximal Exercise Capacity to Hospitalization Secondary to Coronavirus Disease 2019. Mayo Clin. Proc. 2021, 96, 32–39. [Google Scholar] [CrossRef] [PubMed]
- Brugliera, L.; Spina, A.; Castellazzi, P.; Cimino, P.; Tettamanti, A.; Houdayer, E.; Arcuri, P.; Alemanno, F.; Mortini, P.; Iannaccone, S. Rehabilitation of COVID-19 patients. J. Rehabilitation Med. 2020, 52, jrm00046. [Google Scholar] [CrossRef]
- Thomas, P.; Baldwin, C.; Bissett, B.; Boden, I.; Gosselink, R.; Granger, C.L.; Hodgson, C.; Jones, A.Y.; E Kho, M.; Moses, R.; et al. Physiotherapy management for COVID-19 in the acute hospital setting: clinical practice recommendations. J. Physiother. 2020, 66, 73–82. [Google Scholar] [CrossRef]
- Piquet, V.; Luczak, C.; Seiler, F.; Monaury, J.; Martini, A.; Ward, A.B.; Gracies, J.-M.; Motavasseli, D.; Lépine, E.; Chambard, L.; et al. Do Patients With COVID-19 Benefit from Rehabilitation? Functional Outcomes of the First 100 Patients in a COVID-19 Rehabilitation Unit. Arch. Phys. Med. Rehabilitation 2021, 102, 1067–1074. [Google Scholar] [CrossRef] [PubMed]
- Stefanakis, M.; Batalik, L.; Papathanasiou, J.; Dipla, L.; Antoniou, V.; Pepera, G. Exercise-based cardiac rehabilitation programs in the era of COVID-19: a critical review. Rev. Cardiovasc. Med. 2021, 22, 1143–1155. [Google Scholar] [CrossRef]
- Gil, S.; Filho, W.J.; Shinjo, S.K.; Ferriolli, E.; Busse, A.L.; Avelino-Silva, T.J.; Longobardi, I.; de Oliveira Júnior, G.N.; Swinton, P.; Gualano, B.; et al. Muscle strength and muscle mass as predictors of hospital length of stay in patients with moderate to severe COVID-19: A prospective observational study. J. Cachexia Sarcopenia Muscle 2021, 12, 1871–1878. [Google Scholar] [CrossRef] [PubMed]
- Zhu, B.; Feng, X.; Jiang, C.; Mi, S.; Yang, L.; Zhao, Z.; Zhang, Y.; Zhang, L. Correlation between white blood cell count at admission and mortality in COVID-19 patients: a retrospective study. BMC Infect. Dis. 2021, 21, 1–5. [Google Scholar] [CrossRef]
- Yang, F.; Liu, N.; Hu, J.Y.; Wu, L.L.; Su, G.S.; Zhong, N.S.; Zheng, Z.G. [Pulmonary rehabilitation guidelines in the principle of 4S for patients infected with 2019 novel coronavirus (2019-nCoV)]. . 2020, 43, 180–182. [Google Scholar]
- Zbinden-Foncea, H.; Francaux, M.; Deldicque, L.; Hawley, J.A. Does High Cardiorespiratory Fitness Confer Some Protection Against Proinflammatory Responses After Infection by SARS-CoV-2? Obesity 2020, 28, 1378–1381. [Google Scholar] [CrossRef]
- Maltagliati, S.; Sieber, S.; Sarrazin, P.; Cullati, S.; Chalabaev, A.; Millet, G.P.; Boisgontier, M.P.; Cheval, B. Muscle strength explains the protective effect of physical activity against COVID-19 hospitalization among adults aged 50 years and older. J. Sports Sci. 2021, 39, 2796–2803. [Google Scholar] [CrossRef]
- Halabchi, F.; Mazaheri, R.; Sabeti, K.; Yunesian, M.; Alizadeh, Z.; Ahmadinejad, Z.; Aghili, S.M.; Tavakol, Z. Regular Sports Participation as a Potential Predictor of Better Clinical Outcome in Adult Patients With COVID-19: A Large Cross-Sectional Study. J. Phys. Act. Heal. 2021, 18, 8–12. [Google Scholar] [CrossRef]
- Izzo, R.; Zincarelli, C.; Onufrio, M.; D’alessio, A.; Di Ruocco, G.; Di Minno, M.N.D.; Pisacreta, A. Early rehabilitation treatment in hospitalized patients with severe COVID-19: Effects on autonomy and quality of life. Physiother. Pr. Res. 2022, 43, 249–255. [Google Scholar] [CrossRef]
- Marques, A.; Gomez-Baya, D.; Peralta, M.; Frasquilho, D.; Santos, T.; Martins, J.; Ferrari, G.; de Matos, M.G. The Effect of Muscular Strength on Depression Symptoms in Adults: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Heal. 2020, 17, 5674. [Google Scholar] [CrossRef] [PubMed]
- Yates, T.; Razieh, C.; Zaccardi, F.; Rowlands, A.V.; Seidu, S.; Davies, M.J.; Khunti, K. Obesity, walking pace and risk of severe COVID-19 and mortality: analysis of UK Biobank. Int. J. Obes. 2021, 45, 1155–1159. [Google Scholar] [CrossRef]
- Ladlow, P.; Holdsworth, D.A.; O’sullivan, O.; Barker-Davies, R.M.; Houston, A.; Chamley, R.; Rogers-Smith, K.; Kinkaid, V.; Kedzierski, A.; Naylor, J.; et al. Exercise tolerance, fatigue, mental health, and employment status at 5 and 12 months following COVID-19 illness in a physically trained population. J. Appl. Physiol. 2023, 134, 622–637. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Flow chart. CT - computed tomography, CRP - C-reactive protein.
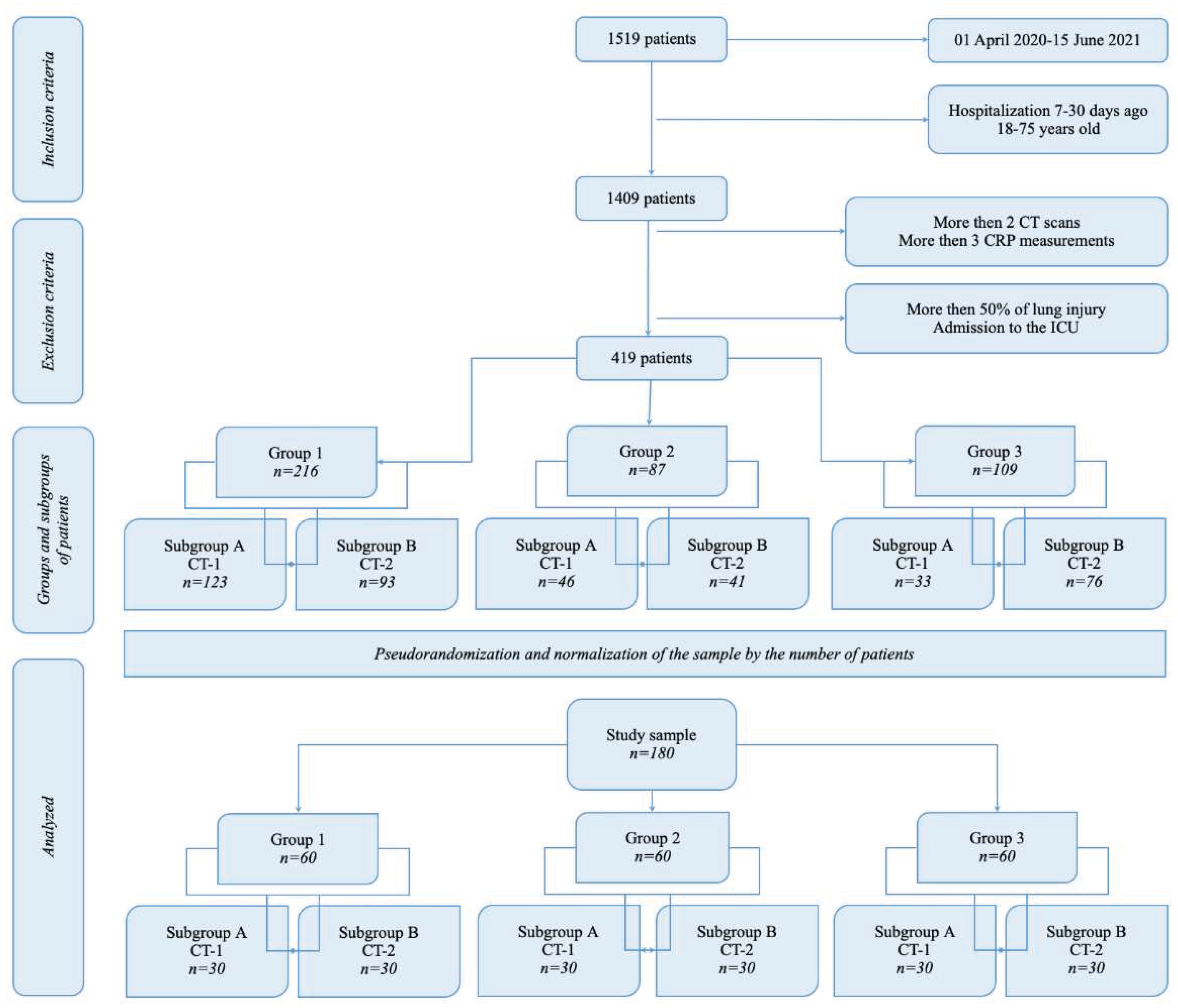
Figure 2.
Kaplan-Meier curves. Log-rank test for patients with CT-2 by the time of onset of the CRP above 50 mg/l, p= 0.00001; for the duration of the CRP level above 50 mg/l, p=0.00017: (a) Time to onset of the C-reactive protein level above 50 mg/l in study groups; (b) Duration of the C-reactive protein level above 50 mg/l in study groups: 1 - physical exercises (blue line), 2 - the combination of physical exercises and chest massage in an electrostatic field (red line), 3 - no rehabilitation (green line). + cens - censored data.
Figure 2.
Kaplan-Meier curves. Log-rank test for patients with CT-2 by the time of onset of the CRP above 50 mg/l, p= 0.00001; for the duration of the CRP level above 50 mg/l, p=0.00017: (a) Time to onset of the C-reactive protein level above 50 mg/l in study groups; (b) Duration of the C-reactive protein level above 50 mg/l in study groups: 1 - physical exercises (blue line), 2 - the combination of physical exercises and chest massage in an electrostatic field (red line), 3 - no rehabilitation (green line). + cens - censored data.
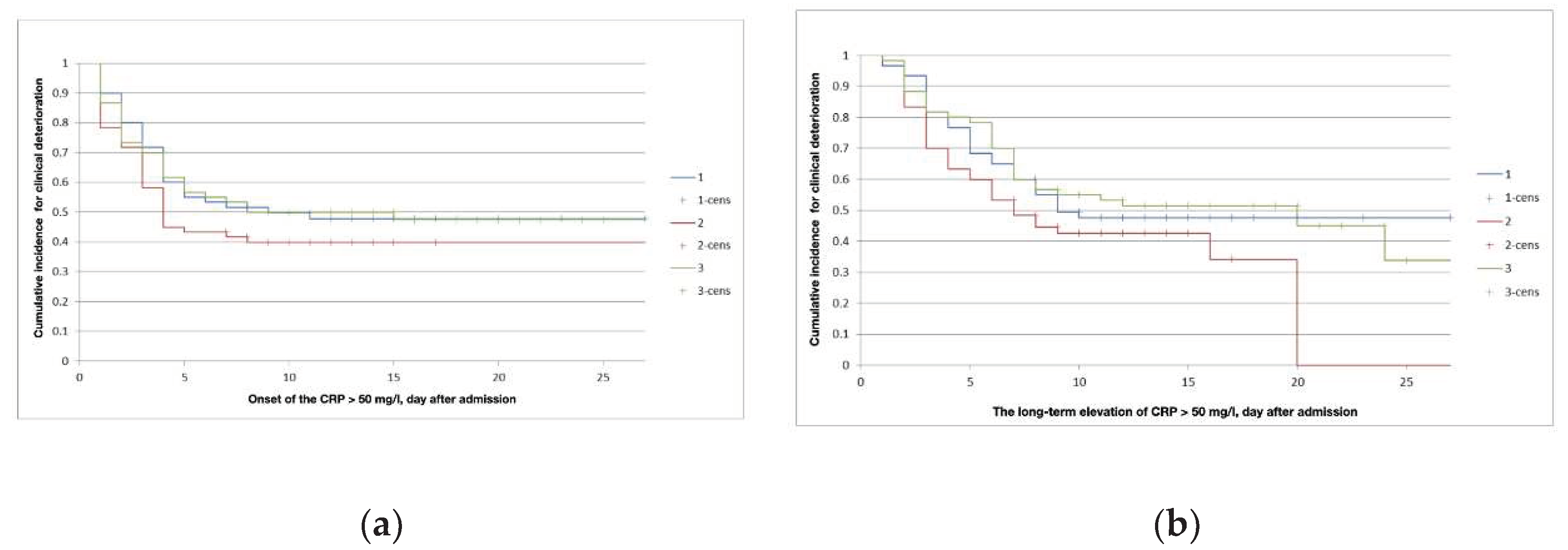
Figure 3.
The hazard ratio for desaturation (saturation below 93%) in study groups: 1 - physical exercises (blue line), 2 - the combination of physical exercises and chest massage in an electrostatic field (red line), 3 - no rehabilitation (green line). + cens - censored data. Log-rank test, p=0.001.
Figure 3.
The hazard ratio for desaturation (saturation below 93%) in study groups: 1 - physical exercises (blue line), 2 - the combination of physical exercises and chest massage in an electrostatic field (red line), 3 - no rehabilitation (green line). + cens - censored data. Log-rank test, p=0.001.
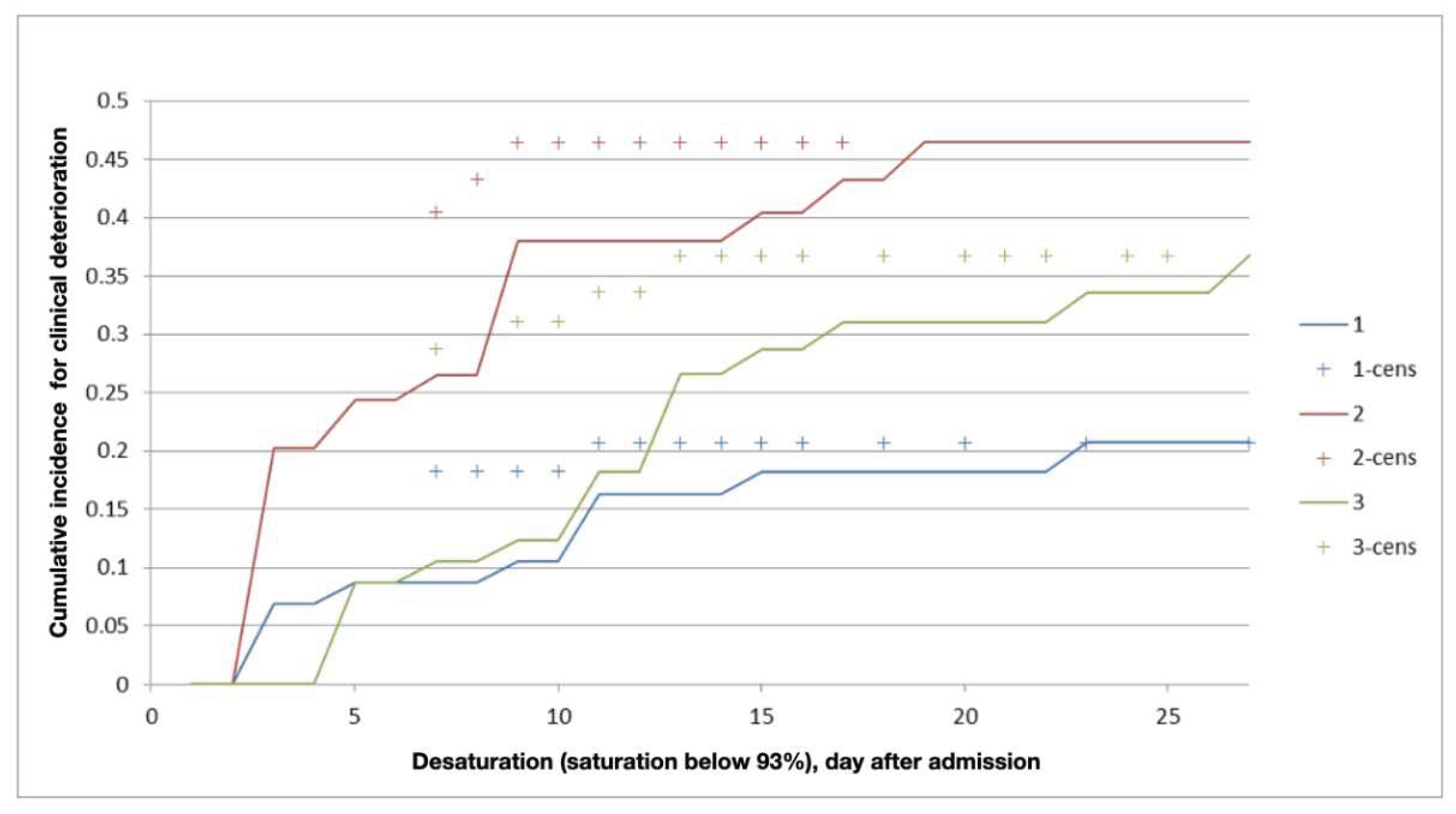

Table 1.
The length of stay in the hospital according to the CT scan (n=180).
| CT at admission | length of stay in hospital, mediana, days | Inter quartile range, days | |
|---|---|---|---|
| Group 1, n=60 | CT-1, n=30 | 13 | 11-15 |
| CТ-2, n=30 | 14 | 12-16 | |
| Group 2, n=60 | CT-1, n=30 | 12 | 9-15 |
| CТ-2, n=30 | 14 | 11-15 | |
| Group 3, n=60 | CT-1, n=30 | 14 | 12-15 |
| CТ-2, n=30 | 16 | 14-21 | |
| CT - computed tomography, CT-1 - up to 25% of lungs injury; CT-2 - 25-50% of lungs injury. | |||
Table 2.
Dynamics of complaints in the study groups.
| Complains | At admission | At discharge | p-value | |
|---|---|---|---|---|
| Group 1, n=60 | Weakness, n | 40 | 30 | 0.175 |
| headache, n | 2 | 1 | 0.0001 | |
| shortness of breath, n | 15 | 5 | 0.0001 | |
| cough, n | 18 | 3 | 0.0001 | |
| Group 2, n=60 | weakness, n | 51 | 32 | 0.013 |
| headache, n | 6 | 1 | 0.0001 | |
| shortness of breath, n | 22 | 10 | 0.0001 | |
| cough, n | 30 | 17 | 0.055 | |
| Group 3, n=60 | weakness, n | 47 | 18 | 0.458 |
| headache, n | 6 | 0 | - | |
| shortness of breath, n | 14 | 6 | 0.0001 | |
| cough, n | 27 | 9 | 0.0001 | |
| Total, n=180 | weakness, n | 138 | 80 | 0.0005 |
| headache, n | 14 | 2 | 0.0001 | |
| shortness of breath, n | 51 | 21 | 0.0001 | |
| cough, n | 75 | 29 | 0.0001 | |
Table 3.
C-reactive protein at admission and discharge.
| C-reactive protein, mg/l | Mean | CI -95% | CI +95% | |
|---|---|---|---|---|
| Group 1, n=60 | at admission | 46.03 | 33.27 | 58.80 |
| at discharge | 6.70 | 3.70 | 9.71 | |
| Group 2, n=60 | at admission | 67.71 | 50.03 | 85.38 |
| at discharge | 4.17 | 4.16 | 11.07 | |
| Group 3, n=60 | at admission | 44.69 | 32.14 | 57.24 |
| at discharge | 9.57 | 4.19 | 14.95 | |
| Total, n=180 | at admission | 52.81 | 44.44 | 61.18 |
| at discharge | 7.96 | 5.65 | 10.28 | |
Table 4.
Time intervals of C-reactive protein (CRP) above 50 mg/l during treatment.
| Group | 1 | 2 | 3 | |||
|---|---|---|---|---|---|---|
| Subgroup | A | B | A | B | A | B |
| The onset of CRP level above 50 mg/l (median, interquartile range), days | 4 (2.5-5) | 3 (2-4) | 3 (2-4) | 2 (1-4) | 3 (1-5) | 2(1.5-4) |
| Duration of CRP level above 50 mg/l (median, interquartile range), days | 4.5 (3-6) | 5 (3-8) | 3.5 (3-5.5) | 3.5(2-6.5) | 6 (3-7) | 6 (2.5-7.5) |
Table 5.
Health profile according to the EQ-5D quality of life questionnaire at admission, n=180.
| Component | Level 1 «no problem» |
Level 2 «slight problems» |
Level 3 «moderate problems» |
|---|---|---|---|
| Mobility, n (%) | 27 (15) | 96 (53) | 57 (32) |
| Self-care, n (%) | 23 (13) | 98 (54) | 59 (33) |
| Usual activities, n (%) | 11 (6) | 93 (52) | 76 (42) |
| Pain/discomfort, n (%) | 11 (6) | 98 (54.5) | 71 (39.5) |
| Anxiety/depression, n (%) | 7 (4) | 85 (47) | 88 (49) |
| p>0.05 | |||
Table 6.
Health profile according to the EQ-5D quality of life questionnaire of patients with CT-1 at discharge, n=45.
Table 6.
Health profile according to the EQ-5D quality of life questionnaire of patients with CT-1 at discharge, n=45.
| Level 1 «no problem» |
Level 2 «slight problems» |
Level 3 «moderate problems» |
Р | |
|---|---|---|---|---|
| Anxiety/depression | P-value | |||
| Group 1 A, n (%) | 23 (51) | 18 (40) | 4 (9) | 0.0098 |
| Group 2 A, n (%) | 9 (20) | 27 (60) | 9 (20) | p>0.05 |
| Group 3 A, n (%) | 10 (22) | 25 (56) | 10 (22) | p>0.05 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



