
Submitted:
30 May 2023
Posted:
01 June 2023
You are already at the latest version
Abstract
In the pathogenesis of endometriosis, the differences between the eutopic and ectopic endometrium as well as between the eutopic endometrium with and without endometriosis are repeatedly pointed out. Various mechanisms have been suggested to explain these changes among them epithelial-mesenchymal transition (EMT). Recently, we suggested based on immunohistochemical data that most of the changes occur after and not before implantation of endometrial cells into ectopic locations. Furthermore, the subtle changes between eutopic endometrium with and without endometriosis and maintenance of epithelial cell-to cell contacts only suggest a partial EMT. In this study, we have re-analyzed the mRNA expression array data of eutopic and ectopic endometrium with respect to expression changes and EMT. Especially, we found that the similarity between eutopic endometrium with and without endometriosis is extremely high (~99.1%). In contrast, eutopic endometrium compared to ectopic endometrium only shows an overall similarity of ~95.3%. Analysis of some EMT-associated genes revealed small differences in the mRNA expression levels of some members of the claudin family. The array data suggest that the changes in eutopic endometrium at the beginning of the disease are quite subtle and that the majority of differences occur after implantation into ectopic locations.
Keywords:
endometrium
; endometriosis
; epithelial-mesenchymal transition
; EMT
; claudins
; keratins
Introduction
The histological appearance of endometrial glands and stroma sometimes with hemosiderin-laden macrophages outside the uterine cavity is still the definition of endometriosis used by pathologists worldwide [1]. In contrast to epithelial endometriosis which is quite rare, a large study of pelvic endometriosis showed a higher percentage (44.9%) of cases (123/274) as stromal endometriosis [2]. Additionally, we have recently provided strong indications that stromal endometriosis is also common (~53%) in catamenial pneumothorax if caused by ectopic endometrial lesions [3]. In many cases endometriosis causes pain and/or infertility [4].
Histological definition of endometriosis was recently described as outdated and that it no longer reflects the true scope and manifestations of the disease [5]. Furthermore, Taylor et al. [5] emphasized that the clinical presentation is varied, that the presence of pelvic lesions is heterogeneous, and that the manifestations of the disease outside the female reproductive tract remain poorly understood. They concluded that endometriosis is a systemic disease rather than a disease predominantly affecting the pelvis [5]. Although this criticism is justified in many points, we really lack an understanding of how the sometimes very small ectopic lesions might cause the systemic disease in many patients. We suggest including the uterus in this consideration, because suppression of menstrual bleeding with contraceptives and hysterectomies with or without laparoscopy cured endometrial pain in the majority of cases with low reoperations rates [6,7,8,9].
Although the Sampson hypothesis of retrograde menstruation [10] provides a reasonable model for ectopic endometrial tissue [11], it is still unclear why only 0.7-8.6% of women in the general population develop endometriosis [12]. Thus, several additional hypotheses such as inflammation, oxidative stress, disturbance of the peritoneal barrier and genetic/epigenetic changes have been put forward to explain this discrepancy [13,14,15].
Previous studies have suggested that the eutopic endometrium with and without endometriosis is different [16,17], assuming that initiation of endometriosis might start in the endometrium. One of the mechanisms which have been suggested to play a role is epithelial-mesenchymal transition (EMT). EMT is involved in wound healing, fibrosis, tissue regeneration, inflammation and cancer metastasis [18,19,20] and was classified into: (1) type I EMT during embryonic development, (2) type II EMT during wound healing and tissue regeneration, and (3) type III EMT associated with cancer [19]. The gradual remodelling of the epithelial cell architecture is a multi-stage process, characterized by the first EMT hallmark: the loss of epithelial markers resulting in disruption of cell-cell contacts, remodelling of the cytoskeleton and loss of apical-basal polarity. This is then followed by the second hallmark of EMT namely the acquisition of mesenchymal markers [18,19,20,21,22]. The cellular changes often result in a mesenchymal phenotype with spindle-like cell shape, increased cell migration, invasion and cell survival (resistance to anoikis) [22,23]. Despite these significant changes only a small set of transcription factors (TFs) or master regulators of EMT are involved. These include the Snail family proteins Snail1 (Snail), Snail2 (Slug), Zinc finger E-box binding (Zeb) homeobox family proteins Zeb1 and Zeb2, and TWIST family proteins Twist1 and Twist2 [24].
The first evidence of EMT in endometriosis in vivo was described for pelvic endometriosis by immunohistochemistry with EMT markers such as cytokeratin, E/N-Cadherin, Vimentin, and S100A4 [25]. After attachment to the peritoneum the reverse process called mesenchymal-epithelial transition (MET) was postulated to occur for peritoneal and deep infiltrating endometriosis [25]. Similarly, a decreased expression of cytokeratin in ectopic compared to eutopic endometrium was found [26,27], however, we demonstrated a stable expression of keratin 18, 19 and mucin-1 in eutopic and ectopic epithelial cells without any loss of the epithelial phenotype [28]. It needs to be emphasized again that ectopic endometriotic lesions still consist of epithelial glands surrounded by stromal cells without an apparent mesenchymal phenotype of the epithelial cells [1,28].
In this study we re-analyzed mRNA/cDNA arrays to take a closer look at the key differences between endometrium with and without endometriosis and between the eutopic and ectopic endometrium. In this review, particular attention was paid to possible mRNA expression changes of EMT-associated genes.
2. Materials and methods
For this systematic review we followed the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) guidelines [29].
2.1. Search strategy and eligibility criteria
We performed a systematic search using PubMed from 1990 up to 1. April 2023. PubMed was searched for “endometriosis” in conjunction with “array”, “mRNA expression”, and “cDNA library”. All human studies reporting original data concerning mRNA expression/cDNA/array and eutopic/ectopic endometrium/endometriosis as well as related studies in all languages were included in this review. Studies were excluded if they were not published in established peer reviewed journals.
2.2. Study Selection
Results from the initial searches were collated, and duplicates deleted. Title andabstract screening were completed independently by two authors (MAR and LK). Full texts were retrieved and reviewed independently by MAR and LK and each study evaluated for inclusion using the pre-determined eligibility criteria. Any disagreements were resolved via discussion among the authors, and consensus achieved. Additional studies were identified through forward and backward chaining of the included studies.
2.3. Data Extraction and Synthesis
Data was extracted independently by MAR and LK. We looked for the keywords: E/N-cadherin, Snail1, Slug (also known as Snail2), Twist, claudin(s), occludin, integrin(s), keratin(s), and transforming growth factor-betas (TGF-βs). Data included, but were not limited to title, author, journal, year of publication, population studied, phase of the menstrual cycle, results and outcomes. Results were synthesized in a thematic manner. The authors independently identified recurring genes in the final list of included studies. This final list of genes was discussed until consensus reached by the authors. A meta-analysis was not possible in this review due to the heterogeneity of methodology and results obtained in the papers included in the study.
Results
A total of 14 studies were included in the analysis (Figure 1), 5 comparing eutopic endometrium with and without endometriosis (Table 1). The comparison resulted in a total of 1,195 of 129,937 (0.92%) genes or samples with altered mRNA expression (Table 1). A slight regulation of claudin-3, claudin-6, claudin-10 and claudin-14 ranging from 0.59 up to 2.3 was described in only 2 of 5 manuscripts (Table 2) [30,32]. Additionally, TGF-β3 expression was also found to be increased in eutopic endometrium of endometriosis patients compared to eutopic endometrium without endometriosis (Table 2) [30,32]. Not any of the other EMT-associated genes was found in more than one study to be regulated.
In 9 studies comparison of the eutopic endometrium with the ectopic endometrium showed a high percentage (4.74%, 15,234/321,149) of genes/samples with an altered mRNA expression (Table 3). In total, the altered expression of genes/samples in the ectopic endometrium compared to the eutopic endometrium (4.74%) is ~5x higher compared to the eutopic endometrium with and without endometriosis (0.92%, Table 1 and Table 3).
The comparison of eutopic with ectopic endometrium revealed increased expression of claudin-1, -5, -6, -9, -11, -15, -17, and -22 (Table 4). Remarkably, claudin-11 showed the highest scores of increased ectopic gene expression ranging from 54.5 up to 100 (Table 4). Claudin-2, -3, -4, -7, -10, and -22 demonstrated a slight to modest decreased expression in ectopic endometrium compared to eutopic endometrium (Table 4). Furthermore, TGF-β3 expression was also increased in ectopic endometrium compared to eutopic endometrium (Table 4).
Discussion
In this study, the comparison of the eutopic endometrium with and without endometriosis revealed only a slight difference (0.92%) in mRNA expression. Accordingly, there were very few changes in the EMT-associated genes. Only some claudins (N=3) and TGF-β3 were abnormally expressed, whereas expression of the other EMT-associated genes were not mentioned in more than one study. In contrast, comparison of eutopic endometrium with ectopic endometrium showed a clearly higher number (4.74%) of impaired gene expression. Similarly, more claudins (N=15) and TGF-β3 were abnormally expressed, while EMT-regulating transcription factors such ZEB1, and Snail1/2 (Slug), were not described in more than one study. Of note, mRNA expression of claudin-11 was often strongly increased in ectopic endometrium compared to eutopic endometrium. Overall, it was noticeable that ovarian endometriosis was examined very frequently, but peritoneal and deep infiltrating endometriosis only very rarely. No study has up to date examined the proportion of stroma and epithelium in the eutopic and ectopic endometrium, which is possible using markers such as CD10 and keratins. Only one study using cell picking, revealed no differences in gene expression between eutopic and ectopic endometrium [38].
Our observation that there are only very few differences in eutopic endometrium with and without endometriosis is supported by a recently published meta-analysis, which did not show a single differently expressed gene in the mid-secretory phase [46]. Remarkably two other studies about miRNAs [47] and methylation patterns [48] also reported similar results. Methylation pattern revealed only 1 of 42.990 probes (0.002%) to be different between eutopic endometrium with and without endometriosis, while 12378 methylation patterns (28.8%) were dissimilar between eutopic and ectopic endometrium [47]. Similarly, the microRNA differences between eutopic endometrium with and without endometriosis was comparatively low with 15/1105 (=1.36%) but noticeably more frequent between eutopic and ectopic endometrium 156/1105 (=14.1%) [48]. These studies are consistent with our results that changes in eutopic endometrium with and without endometriosis are minimal, and that the differences between eutopic and ectopic endometrium are clearly larger.
Although a recent bioinformatic analysis of three microarray datasets emphasized the importance of EMT in the development of endometriosis due to down-regulation of E-cadherin (CDH1) [49], another study ruled out EMT in the endometrium, because only the endometrial epithelial cells but not the stromal cells showed DNA alterations/mutations [50]. As demonstrated in our previous review on EMT, the main problem with many studies on EMT is that mostly only acquisition of mesenchymal markers and not the loss of epithelial markers, in particular the cell-to-cell contacts, have been examined [51]. Thus, loss of cell-to-cell contacts, the first hallmark of EMT, does not occur in eutopic endometrium with and without endometriosis as well as in ectopic endometrium, and the epithelial phenotype of the cells is still clearly preserved [1,28]. The small increase in mesenchymal gene expression of endometrial epithelial cells does not allow the assumption of a cell transition to mesenchymal cells, but at most the conclusion of a partial EMT without the loss of the epithelial cell characteristics [51].
Gene expression between eutopic and ectopic endometrium showed about ~5 times more differences (4.74%) compared to that of eutopic endometrium with and without endometriosis (0.92%). We can thus conclude with a high degree of certainty that most of the differences in gene expression did not occur before but after implantation of the endometrial cells. This conclusion supports our hypothesis of a partial EMT without loss of the epithelial phenotype, which we had put forward from immunohistochemical analysis of EMT-associated proteins of the eutopic and ectopic endometrium [51]. Although we cannot completely rule out that circulating endometrial cells (CECs) may have been altered by EMT prior to implantation, there has been no study to date showing alterations of CECs by EMT. Remarkably, endometrial tissue fragments from endometriosis and control patients did not differ in their implantation potential on chorionic allantois membranes (CAMs) in vitro. The authors suggested that implantation is possibly determined by external factors regulating influences on the endometrial implants [52]. Similarly, Nap et al. [53] showed that the integrity of endometrial tissue architecture determined the success of implantation of human endometrium into CAM ectopic locations in vitro.
Our analysis of EMT-associated genes showed altered expression patterns only for claudin-3, -6, -10, and -14 and TGF-β3 in eutopic endometrium with and without endometriosis while comparison between eutopic and ectopic endometrium revealed aberrant gene expression of 11 claudins (claudin-1 up to claudin-11), and claudin-15, -17, and -22. The highest increase in expression was reported for claudin-11 [40,42,45]. In contrast to two reports that described an impaired expression of claudin-3 in endometriosis [54,55], we recently found an unchanged protein localization in the eutopic endometrium with and without endometriosis and also in the ectopic endometrium [56] which might be due to different fixation protocols used. Similarly, we found a high abundance (~98%) of claudin-10 in nearly all endometrial and endometriotic glands, but no differences in the claudin-10 positive endometrial glands between cases with and without endometriosis [57]. A significantly higher expression of claudin-10 was detected in the ectopic endometrium of deep infiltrating and ovarian endometriosis [57]. Interestingly, a shift in claudin-10 from a predominant apical localization in the eutopic endometrium to a more pronounced basal/cytoplasmic localization in the ectopic endometria of all three endometriotic entities (ovarian, peritoneal, deep infiltrating) was observed. Of note, despite the impaired endometriotic localization of claudin-10, the epithelial phenotype was retained in all glands [57].
A decreased expression of Claudin-7 was observed in ectopic compared to eutopic endometrium in the array studies [42,45] as well as with immunohistochemistry [54]. Claudin-7 was identified primarily at the basolateral junctions of the glandular epithelial cells in eutopic endometrium as well as in the ectopic lesions in nearly all glands and cysts [58]. Quantification of claudin-7 localization showed a slight increase in peritoneal and deep infiltrating endometriosis compared to eutopic endometrium [58].
In three array studies a strong increase in claudin-11 mRNA expression in ectopic compared to eutopic endometrium was described [40,42,45], however, without any supporting protein data. In contrast, we observed only a moderately decreased abundance of claudin-11 in ovarian endometriosis compared to eutopic endometrium [58]. Claudin-11 was localized mainly in the apicolateral junctions in nearly all glandular epithelial cells of the eutopic endometrium. Interestingly, deregulation of claudin-11 localization to basal or basolateral localization in ovarian, peritoneal, and deep infiltrating endometriosis was observed. Silencing of claudin-11 decreased invasiveness of endometriotic epithelial 12Z cells significantly in endometriotic epithelial 49Z cells [58]. None of the other claudins have been analyzed in more depth to date.
Beyond the three isoforms of the TGF-βs, TGF-β1-3, expression of TGF-β3 mRNA was increased in eutopic endometrium with endometriosis compared to those without endometriosis [30,32]. Similarly, TGF-β3 gene expression was also higher in ectopic compared to eutopic endometrium [39,42]. TGF-β1 showed the highest expression compared to TGF-β2 and TGF-β3 in the human endometrium [59]. TGF-β3 was increased at menstruation remaining high during the proliferative phase and was preferentially expressed in the stroma. In contrast, TGF-β1 was increased in the peritoneal fluid (PF) of women with endometriosis compared to those without the disease, while TGF-β3 was not altered [60]. However, higher PF and serum levels of TGF-β1, -β2, and –β3 were observed in women with endometriosis compared to controls [61].
Strength and limitations
This is the first study evaluating the similarities and differences in gene expression between eutopic endometria with and without endometriosis with special emphasis on EMT-associated genes. One limitation lies in the fact that the total number of samples is higher than the real number of genes. However, the analysis was less about absolutes and more about relative values.
Conclusions
Results of this study clearly show very little differences in gene expression between eutopic endometrium with and without endometriosis. In contrast, the differences between eutopic and ectopic endometrium are much larger. We suggest that the main changes happen after and not before implantation. Remarkably, there were also few differences in expression of EMT-associated genes with complete absence of the master genes. It can therefore be assumed that there is at most only a partial EMT, with no loss of the epithelial phenotype, and that EMT plays only a minor if not negligible role in the initiation of endometriosis.
Author Contributions
Collection of manuscripts and writing (M.A.R, L.K.), suggestions and proofreading (E.O.M, C.O.A, F.Z, I.M.-H.), writing and proofreading (E.M., R.M., C.O.A.O., M.A.R.) and whole concept, literature search, writing, and proofreading (L.K.). All authors have read and agreed to the published version of the manuscript. Declaration of Conflicting Interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The research received no external funding.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Clement, P.B. The pathology of endometriosis: a survey of the many faces of a common disease emphasizing diagnostic pitfalls and unusual and newly appreciated aspects. Adv. Anat. Pathol. 2007, 14, 241–260.
- Boyle, D.P.; McCluggage, W.G. Peritoneal stromal endometriosis: a detailed morphological analysis of a large series of cases of a common and under-recognised form of endometriosis. J. Clin. Pathol. 2009, 62, 530–533. [CrossRef]
- Mecha, E.; Makunja, R.; Maoga, J.B.; Mwaura, A.N.; Riaz, M.A.; Omwandho, C.O.A.; Meinhold-Heerlein, I.; Konrad, L. The Importance of Stromal Endometriosis in Thoracic Endometriosis. Cells 2021, 10, 180. [CrossRef]
- Taylor, H.S.; Adamson, G.D.; Diamond, M.P.; Goldstein, S.R.; Horne, A.W.; Missmer, S.A.; Snabes, M.C.; Surrey, E.; Taylor, R.N. An evidence-based approach to assessing surgical versus clinical diagnosis of symptomatic endometriosis. Int. J. Gynecol. Obstet. 2018, 142, 131–142. [CrossRef]
- Taylor, H.S.; Kotlyar, A.M.; A Flores, V. Endometriosis is a chronic systemic disease: clinical challenges and novel innovations. Lancet 2021, 397, 839–852. [CrossRef]
- Rizk, B.; Fischer, A.; Lotfy, H.; Turki, R.; Zahed, H.; Malik, R.; Holliday, C.; Glass, A.; Fishel, H.; Soliman, M.; et al. Recurrence of endometriosis after hysterectomy. Facts Views Vis. Obgyn. 2014, 6, 219–227.
- Sandström, A.; Bixo, M.; Johansson, M.; Bäckström, T.; Turkmen, S. Effect of hysterectomy on pain in women with endometriosis: a population-based registry study. BJOG: Int. J. Obstet. Gynaecol. 2020, 127, 1628–1635. [CrossRef]
- Bougie, O.; McClintock, C.; Pudwell, J.; Brogly, S.B.; Velez, M.P. Long-term follow-up of endometriosis surgery in Ontario: a population-based cohort study. Am. J. Obstet. Gynecol. 2021, 225, 270.e1–270.e19. [CrossRef]
- Long, A.J.; Kaur, P.; Lukey, A.; Allaire, C.; Kwon, J.S.; Talhouk, A.; Yong, P.J.; Hanley, G.E. Reoperation and pain-related outcomes after hysterectomy for endometriosis by oophorectomy status. Am. J. Obstet. Gynecol. 2023, 228, 57.e1–57.e18. [CrossRef]
- Sampson, J.A. Peritoneal endometriosis due to the menstrual dissemination of endometrial tissue into the peritoneal cavity. Am. J. Obstet. Gynecol. 1927, 14, 422–469. [CrossRef]
- Yovich, J.L.; Rowlands, P.K.; Lingham, S.; Sillender, M.; Srinivasan, S. Pathogenesis of endometriosis: Look no further than John Sampson. Reprod. Biomed. Online 2020, 40, 7–11. [CrossRef]
- Ghiasi, M.; Kulkarni, M.T.; Missmer, S.A. Is endometriosis more common and more severe than it was 30 years ago? J. Minim. Invasive Gynecol. 2020, 27, 452-461.
- Young, V.J.; Brown, J.K.; Saunders, P.T.; Horne, A.W. The role of the peritoneum in the pathogenesis of endometriosis. Hum. Reprod. Updat. 2013, 19, 558–569. [CrossRef]
- Koninckx, P.R.; Ussia, A.; Adamyan, L.; Wattiez, A.; Gomel, V.; Martin, D.C. Pathogenesis of endometriosis: the genetic/epigenetic theory. Fertil. Steril. 2019, 111, 327–340. [CrossRef]
- Samimi, M.; Pourhanifeh, M.H.; Mehdizadehkashi, A.; Eftekar, T.; Asemi, Z. The role of inflammation, oxidative stress, angiogenesis, and apoptosis in the pathophysiology of endometriosis: Basis science and new insights based on gene expression. J. Cell. Physiol. 2018, 234, 19384-19392.
- Liu, H.; Lang, J.H. Is abnormal eutopic endometrium the cause of endometriosis? The role of the eutopic endometrium in pathogenesis of endometriosis. Med. Sci. Monit. 2011, 17, RA92-99.
- Benagiano, G.; Brosens, I.; Habiba, M. Structural and molecular features of the endomyometrium in endometriosis and adenomyosis. Hum. Reprod. Updat. 2014, 20, 386–402. [CrossRef]
- Jolly, M.K.; Ware, K.E. Gilja, S.; Somarelli, J.A.; Levine, H. EMT and MET: necessary or permissive for metastasis? Mol. Oncol. 2017, 11, 755-769.
- Kalluri, R.; Weinberg, R.A. The basics of epithelial-mesenchymal transition. J. Clin. Investig. 2009, 119, 1420–1428. [CrossRef]
- Dongre, A.; Weinberg, R.A. New insights into the mechanisms of epithelial-mesenchymal transition and implications for cancer. Nat. Rev. Mol. Cell Biol. 2019, 20, 69–84. [CrossRef]
- Pei, D.; Shu, X.; Gassama-Diagne, A.; Thiery, J.P. Mesenchymal–epithelial transition in development and reprogramming. Nature 2019, 21, 44–53. [CrossRef]
- Diepenbruck, M.; Christofori, G. Epithelial-mesenchymal transition (EMT) and metastasis: yes, no, maybe? Curr. Opin. Cell Biol. 2016, 43, 7-13.
- Savagner, P. Epithelial-mesenchymal transitions: from cell plasticity to concept elasticity. Curr. Top. Dev. Biol. 2015, 112, 273-300.
- Debnath, P.; Huirem, R.S.; Dutta, P.; Palchaudhuri, S. Epithelial–mesenchymal transition and its transcription factors. Biosci. Rep. 2022, 42, BSR20211754. [CrossRef]
- Matsuzaki, S.; Darcha, C. Epithelial to mesenchymal transition-like and mesenchymal to epithelial transition-like processes might be involved in the pathogenesis of pelvic endometriosis†. Hum. Reprod. 2012, 27, 712–721. [CrossRef]
- Nisolle, M.; Casanas-Roux, F.; Donnez, J. Coexpression of cytokeratin and vimentin in eutopic endometrium and endometriosis throughout the menstrual cycle: evaluation by a computerized method. Fertil. Steril. 1995, 64, 69–75. [CrossRef]
- Song, I.O.; Hong, S.R.; Huh, Y.; Yoo, K.J.; Koong, M.K.; Jun, J.Y.; Kang, I.S. Expression of Vimentin and Cytokeratin in Eutopic and Ectopic Endometrium of Women with Adenomyosis and Ovarian Endometrioma. Am. J. Reprod. Immunol. 1998, 40, 26–31. [CrossRef]
- Konrad, L.; Gronbach, J.; Horné; F.; Mecha, E.O.; Berkes, E.; Frank, M.; Gattenlöhner, S.; Omwandho, C.O.; Oehmke, F.; Tinneberg, H.R. Similar characteristics of endometrial and endometriotic epithelial cells. Reprod. Sci. 2019, 26, 49-59.
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. PLOS Med. 2021, 18, e1003583.
- Kao, L.C.; Germeyer, A.; Tulac, S.; Lobo, S.; Yang, J.P.; Taylor, R.N.; Osteen, K.; Lessey, B.A.; Giudice, L.C. Expression Profiling of Endometrium from Women with Endometriosis Reveals Candidate Genes for Disease-Based Implantation Failure and Infertility. Endocrinology 2003, 144, 2870–2881. [CrossRef]
- Absenger, Y.; Hess-Stumpp, H.; Kreft, B.; Krätzschmar, J.; Haendler, B.; Schütze, N.; Regidor, P.; Winterhager, E. Cyr61, a deregulated gene in endometriosis. Mol. Hum. Reprod. 2004, 10, 399–407. [CrossRef]
- Burney, R.O.; Talbi, S.; Hamilton, A.E.; Vo, K.C.; Nyegaard, M.; Nezhat, C.R.; Lessey, B.A.; Giudice, L.C. Gene expression analysis of endometrium reveals progesterone resistance and candidate susceptibility genes in women with endometriosis. Endocrinology 2007, 148, 3814–3826. [CrossRef]
- Sherwin, J.; Sharkey, A.; Mihalyi, A.; Simsa, P.; Catalano, R.; D’Hooghe, T. Global gene analysis of late secretory phase, eutopic endometrium does not provide the basis for a minimally invasive test of endometriosis. Hum. Reprod. 2008, 23, 1063–1068. [CrossRef]
- Fassbender, A.; Verbeeck, N.; Börnigen, D.; Kyama, C.; Bokor, A.; Vodolazkaia, A.; Peeraer, K.; Tomassetti, C.; Meuleman, C.; Gevaert, O.; et al. Combined mRNA microarray and proteomic analysis of eutopic endometrium of women with and without endometriosis. Hum. Reprod. 2012, 27, 2020–2029. [CrossRef]
- Eyster, K.M.; Boles, A.L.; Brannian, J.D.; Hansen, K.A. DNA microarray analysis of gene expression markers of endometriosis. Fertil. Steril. 2002, 77, 38–42. [CrossRef]
- Arimoto, T.; Katagiri, T.; Oda, K.; Tsunoda, T.; Yasugi, T.; Osuga, Y.; Yoshikawa, H.; Nishii, O.; Yano, T.; Taketani, Y.; et al. Genome-wide cDNA microarray analysis of gene-expression profiles involved in ovarian endometriosis. Int. J. Oncol. 2003, 22, 551–560.
- Matsuzaki, S.; Canis, M.; Vaurs-Barrière, C.; Boespflug-Tanguy, O.; Dastugue, B.; Mage, G. DNA microarray analysis of gene expression in eutopic from patients with deep endometriosis using laser capture microdissection. Fertil. Steril. 2005, 84Suppl. 2, 1180–1190. [CrossRef]
- Wu, Y.; Kajdacsy-Balla, A.; Strawn, E.; Basir, Z.; Halverson, G.; Jailwala, P.; Wang, Y.; Wang, X.; Ghosh, S.; Guo, S.-W. Transcriptional Characterizations of Differences between Eutopic and Ectopic Endometrium. Endocrinology 2006, 147, 232–246. [CrossRef]
- Mettler, L.; Salmassi, A.; Schollmeyer, T.; Schmutzler, A.G.; Püngel, F.; Jonat, W. Comparison of c-DNA microarray analysis of gene expression between eutopic endometrium and ectopic endometrium (endometriosis). J. Assist. Reprod. Genet. 2007, 24, 249–258. [CrossRef]
- Eyster, K.M.; Klinkova, O.; Kennedy, V.; Hansen, K.A. Whole genome deoxyribonucleic acid microarry analysis of gene expression in ectopic versus eutopic endometrium. Fertil. Steril. 2007, 88, 1505-1533.
- Zafrakas, M.; Tarlatzis, B.C.; Streichert, T.; Pournaropoulos, F.; Wölfle, U.; Smeets, S.J.; Wittek, B.; Grimbizis, G.; Brakenhoff, R.H.; Pantel, K.; et al. Genome-wide microarray gene expression, array-CGH analysis, and telomerase activity in advanced ovarian endometriosis: a high degree of differentiation rather than malignant potential.. Int. J. Mol. Med. 2008, 21, 335–344. [CrossRef]
- Borghese, B.; Mondon, F.; Noël, J.-C.; Fayt, I.; Mignot, T.-M.; Vaiman, D.; Chapron, C. Gene Expression Profile for Ectopic Versus Eutopic Endometrium Provides New Insights into Endometriosis Oncogenic Potential. Mol. Endocrinol. 2008, 22, 2557–2562. [CrossRef]
- Khan, M.A.; Sengupta, J.; Mittal, S.; Ghosh, D. Genome-wide expressions in autologous eutopic and ectopic endometrium of fertile women with endometriosis. Reprod. Biol. Endocrinol. 2012, 10, 84. [CrossRef]
- Monsivais, D.; Bray, J.D.; Su, E.; Pavone, M.E.; Dyson, M.T.; Navarro, A.; Kakinuma, T.; Bulun, S.E. Activated glucocorticoid and eicosanoid pathways in endometriosis. Fertil. Steril. 2012, 98, 117–125. [CrossRef]
- Sohler, F.; Sommer, A.; Wachter, D.L.; Agaimy, A.; Fischer, O.M.; Renner, S.P.; Burghaus, S.; Fasching, P.A.; Beckmann, M.W.; Fuhrmann, U.; et al. Tissue Remodeling and Nonendometrium-Like Menstrual Cycling Are Hallmarks of Peritoneal Endometriosis Lesions. Reprod. Sci. 2012, 20, 85–102. [CrossRef]
- Vargas, E.; García-Moreno, E.; Aghajanova, L.; Salumets, A.; A Horcajadas, J.; Esteban, F.J.; Altmäe, S. The mid-secretory endometrial transcriptomic landscape in endometriosis: a meta-analysis. Hum. Reprod. Open 2022, 2022, hoac016. [CrossRef]
- Wang, L.; Zhao, J.; Li, Y.; Wang, Z.; Kang, S. Genome-wide analysis of DNA methylation in endometriosis using Illumina Human Methylation 450 K BeadChips. Mol. Reprod. Dev. 2019, 86, 491–501. [CrossRef]
- Braza-Boïls, A.; Marí-Alexandre, J.; Gilabert, J.; Sánchez-Izquierdo, D.; España, F.; Estellés, A.; Gilabert-Estellés, J. MicroRNA expression profile in endometriosis: its relation to angiogenesis and fibrinolytic factors. Hum. Reprod. 2014, 29, 978–988. [CrossRef]
- Chen, M.; Zhou, Y.; Xu, H.; Hill, C.; Ewing, R.M.; He, D.; Zhang, X.; Wang, Y. Bioinformatic analysis reveals the importance of epithelial-mesenchymal transition in the development of endometriosis. Sci. Rep. 2020, 10, 8442. [CrossRef]
- Suda, K.; Nakaoka, H.; Yoshihara, K.; Ishiguro, T.; Adachi, S.; Kase, H.; Motoyama, T.; Inoue, I.; Enomoto, T. Different mutation profiles between epithelium and stroma in endometriosis and normal endometrium. Hum. Reprod. 2019, 34, 1899–1905. [CrossRef]
- Konrad, L.; Dietze, R.; Riaz, M.A.; Scheiner-Bobis, G.; Behnke, J.; Horné, F.; Hoerscher, A.; Reising, C.; Meinhold-Heerlein, I. Epithelial-Mesenchymal transition in endometriosis – When does it happen? J. Clin. Med. 2020, 9, E1915.
- Gescher, D.M.; Siggelkow, W.; Meyhoefer-Malik, A.; Malik, E. A priori implantation potential does not differ in eutopic endometrium of patients with and without endometriosis. Arch. Gynecol. Obstet. 2005, 272, 117–123. [CrossRef]
- Nap, A.W.; Groothuis, P.G.; Demir, A.Y.; Maas, J.W.; Dunselman, G.A.; de Goeij, A.F.; Evers, J.L. Tissue integrity is essential for ectopic implantation of human endometrium in the chicken chorioallantoic membrane. Hum. Reprod. 2003, 18, 30–34. [CrossRef]
- Gaetje, R.; Holtrich, U.; Engels, K.; Kissler, S.; Rody, A.; Karn, T.; Kaufmann, M. Differential expression of claudins in human endometrium and endometriosis. Gynecol. Endocrinol. 2008, 24, 442–449. [CrossRef]
- Pan, X.-Y.; Li, X.; Weng, Z.-P.; Wang, B. Altered expression of claudin-3 and claudin-4 in ectopic endometrium of women with endometriosis. Fertil. Steril. 2009, 91, 1692–1699. [CrossRef]
- Hoerscher, A.; Horné, F.; Dietze, R.; Berkes, E.; Oehmke, F.; Tinneberg, H.-R.; Meinhold-Heerlein, I.; Konrad, L. Localization of claudin-2 and claudin-3 in eutopic and ectopic endometrium is highly similar. Arch. Gynecol. Obstet. 2020, 301, 1003–1011. [CrossRef]
- Loeffelmann, A.C.; Hoerscher, A.; Riaz, M.A.; Zeppernick, F.; Meinhold-Heerlein, I.; Konrad, L. Claudin-10 Expression Is Increased in Endometriosis and Adenomyosis and Mislocalized in Ectopic Endometriosis. Diagnostics 2022, 12, 2848. [CrossRef]
- Horné, F.; Dietze, R.; Berkes, E.; Oehmke, F.; Tinneberg, H.-R.; Meinhold-Heerlein, I.; Konrad, L. Impaired Localization of Claudin-11 in Endometriotic Epithelial Cells Compared to Endometrial Cells. Reprod. Sci. 2019, 26, 1181–1192. [CrossRef]
- Chevronnay, H.P.G.; Cornet, P.B.; Delvaux, D.; Lemoine, P.; Courtoy, P.J.; Henriet, P.; Marbaix, E. Opposite Regulation of Transforming Growth Factors-β2 and -β3 Expression in the Human Endometrium. Endocrinology 2008, 149, 1015–1025. [CrossRef]
- Young, V.J.; Brown, J.K.; Saunders, P.T.K.; Duncan, W.C.; Horne, A.W. The Peritoneum Is Both a Source and Target of TGF-β in Women with Endometriosis. PLOS ONE 2014, 9, e106773. [CrossRef]
- Sikora, J.; Smycz-Kubańska, M.; Mielczarek-Palacz, A.; Bednarek, I.; Kondera-Anasz, Z. The involvement of multifunctional TGF-β and related cytokines in pathogenesis of endometriosis. Immunol. Lett. 2018, 201, 31–37. [CrossRef]
Figure 1.
PRISMA flowchart of literature search and data selection. This systematic retrospective review is based upon literature research conducted in PubMed. The main focus was on mRNA/cDNA array analysis, EMT and endometriosis in the eutopic and ectopic endometrium. These reports were carefully read and data extracted.
Figure 1.
PRISMA flowchart of literature search and data selection. This systematic retrospective review is based upon literature research conducted in PubMed. The main focus was on mRNA/cDNA array analysis, EMT and endometriosis in the eutopic and ectopic endometrium. These reports were carefully read and data extracted.
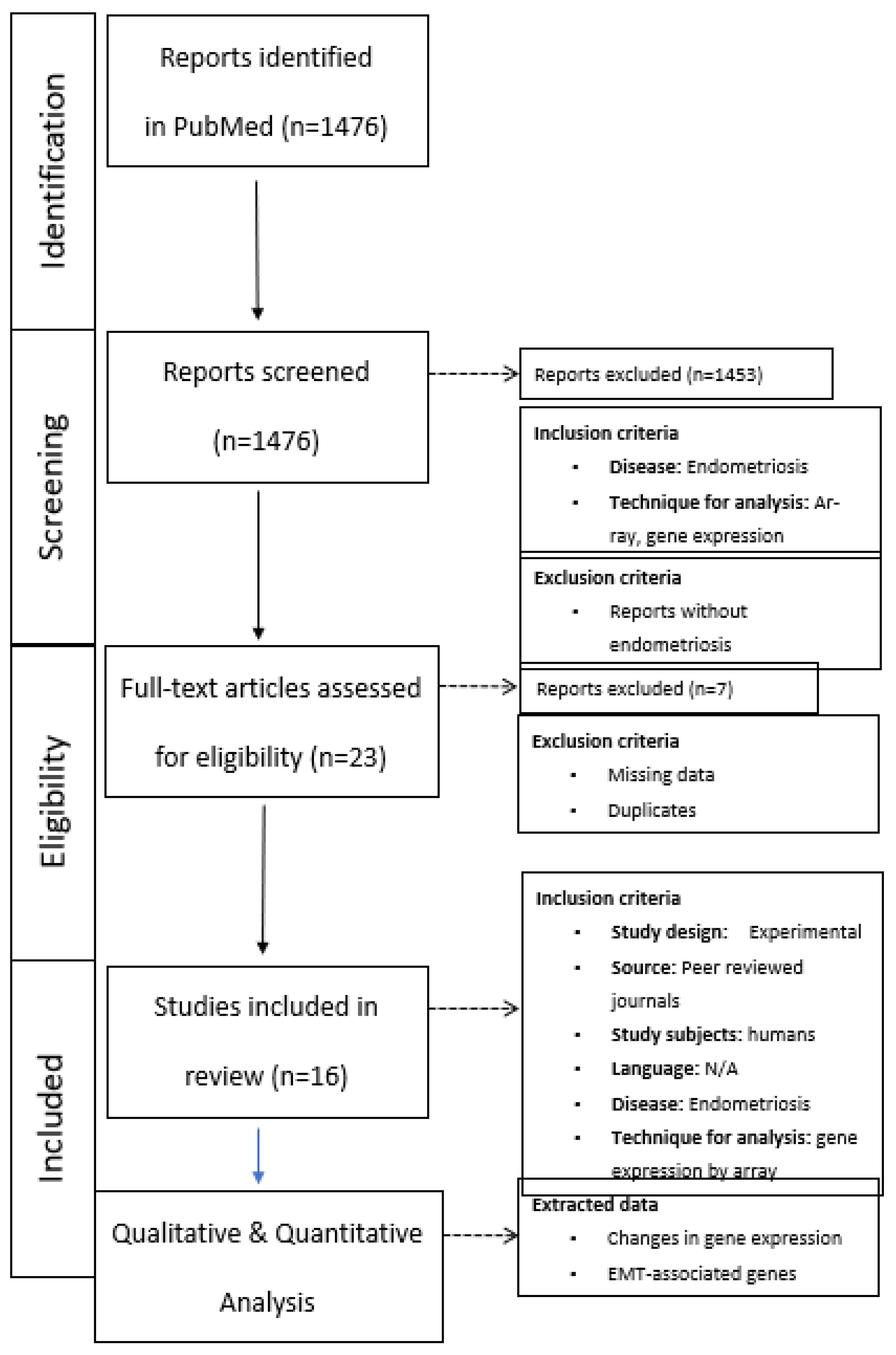

Table 1.
Genome-wide analysis of eutopic endometrium with and without endometriosis.
| Endometrium healthy | Endometrium with endometriosis |
Endometriotic lesions, all | OMA | PE | DIE | References |
| N=7 | N=8, 206/12.686 (1.6%) | n.d. | n.d. | n.d. | n.d. | 30 |
| N=41 | N=43, 95/12.651 (0.8%) | N=19 lesions, not spec. | Not spec. | Not spec. | Not spec. | 31 |
| N=16 | N=21, 885/54.600 (1.62%) | n.d. | n.d. | n.d. | n.d. | 32 |
| N=6 | N=10, 9/22.000 (0.04%) | n.d. | n.d. | n.d. | n.d. | 33 |
| N=18 | N=31 0/28.000 (0%) |
n.d. | n.d. | n.d. | n.d. | 34 |
| Sum | 1.195/129.937 (0.92%) |
Altered mRNA expression is shown as total values and as % in brackets. OMA, endometrioma; PE, peritoneal endometriosis; DIE, deep infiltrating endometriosis; n.d., not done; not spec., not specified.
Table 2.
Up- or down-regulation of EMT-associated genes in eutopic endometrium without vs with endometriosis.
Table 2.
Up- or down-regulation of EMT-associated genes in eutopic endometrium without vs with endometriosis.
| Genes | Up-regulation | Down-regulation | References |
| Claudin-3 | - | 0.59 | 32 |
| Claudin-6 | 1.54 | - | 32 |
| Claudin-10 | 2.3 | - | 30 |
| Claudin-14 | - | 0.65 | 32 |
| TGF-β3 | 100 3.14 |
- - |
30 32 |
Table 3.
Genome-wide analysis of eutopic and ectopic endometrium.
| Endometrium healthy | Endometrium with endometriosis |
Endometriotic lesions, all | OMA | PE | DIE | References |
| n.d. | N=3 | N=3 (paired) 8/4,133 (0.2%) |
N=3 | n.d. | n.d. | 35 |
| n.d. | N=23 | N=23 (paired) 1,413/23,040 (6.1%) |
N=23 | n.d. | n.d. | 36 |
| n.d. | N=12 | N=12 (paired) 0/1,176 (0%) |
n.d. | n.d | N=12 | 37 |
| n.d. | N=12 | N=25 (paired) 904/9,600 (4684*) (9.4%/19.3%*) |
N=6 | N=5 | N=1 | 38 |
| N=5 (not used for the array) | N=5 | N=5 (paired) 13/1,176 (940*) (1.1%/1.38*) |
N=5 | n.d. | n.d. | 39 |
| n.d. | N=10 | N=10 (paired) 1,146/53,000 (2.16%) |
yes | yes | Not. spec | 40 |
| n.d. | N=4 | N=4 (paired) 36/44,928 (0.08%) |
N=4 | n.d. | n.d. | 41 |
| n.d. | N=6 | N=6 (paired) 5,600/53,000 (10.6%) |
N=6 | n.d. | n.d. | 42 |
| n.d. | N=18 | N=18 (paired) 847/29,421 (2.88%) |
N=18 | n.d. | n.d. | 43 |
| n.d. | N=6 | N=6 (paired) 1,366/47,000 (2.9%) |
N=6 | n.d. | n.d. | 44 |
| n.d. | N=17 | N=18 (paired) 3,901/54,675 (7.1%) |
n.d. | N=18 | n.d. | 45 |
| Sum | 15,234/321,149 (314,821*) (4.74%/4.84%*) |
*In two studies numbers of mRNA changes per gene were included. Calculation change per gene only slightly increases the rates of change by 0.1% (4.74% vs. 4.84%). OMA, endometrioma; PE, peritoneal endometriosis; DIE, deep infiltrating endometriosis; n.d., not done; not spec., not specified.
Table 4.
Up- or down-regulation of EMT-associated genes in eutopic endometrium compared to ectopic endometrium.
Table 4.
Up- or down-regulation of EMT-associated genes in eutopic endometrium compared to ectopic endometrium.
| Genes | Up-regulation | Down-regulation | References |
| Claudin-1 | 6.64 0.87-2.85 |
- - |
45 43 |
| Claudin-2 | - | 0.45-0.55 | 43 |
| Claudin-3 | - - - |
0.14 0.06 0.58 |
45 43 35 |
| Claudin-4 | - - |
0.11 0.1 |
45 43 |
| Claudin-5 | 4,31 7.46 |
- - |
45 43 |
| Claudin-6 | 1.05 | - | 43 |
| Claudin-7 | - - |
0.19 0.12 |
45 43 |
| Claudin-8 | - | 0.28 | 43 |
| Claudin-9 | 2.16 | - | 43 |
| Claudin-10 | - | 0.17 | 43 |
| Claudin-11 | 54.05 69.3 100 |
- - - |
45 43 40 |
| Claudin-15 | 1.31-2.07 | - | 43 |
| Claudin-17 | 1.25 | - | 43 |
| Claudin-22 | - | 0.17 | 43 |
| TGF-β3 | 4.86 0.9-1.7 |
- - |
43 39 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



