
Submitted:
16 May 2023
Posted:
16 May 2023
You are already at the latest version
Abstract
Background: Children with anorectal malformation (ARM) require long-term follow-up, especially for fecal continence and main predictors of longer-term success are the type of ARM, associated anomalies and sacral integrity. Three-Dimensional High Resolution Anorectal Manometry (3D-HRAM) provides an image of the pressure profile of anal sphincter complex. Aim of study was to evaluate the anal sphincter function in ARM patients with 3D HRAM correlating this analysis to clinical outcome and to associated malformations.
Methods: Forty ARM patients, were submitted to 3D HRAM: manometric, anatomical and clinical score were correlated to response to bowel management (BM).
Results: A positive correlation between all scores and type of ARM was found: in high ARM and in patients with spinal anomalies (regardless to ARM type) lower scores were reported and even after BM they do not achieve good continence.
Conclusions: 3D-HRAM provides information on the functional anatomy of the sphincter complex. Our study shows good correlation between the manometric results and clinical outcome, confirming spinal malformations and ARM type as most important prognostic risk factors for poor outcome. Specific sphincteric defects can be explored with manometry, allowing for tailored bowel management strategies.
Keywords:
anorectal malformations
; high resolution anorectal manometry
; fecal incontinence
; bowel management
1. Introduction
Anorectal malformations (ARMs), occurring in 1:4000/5000 neonates, involve the last tract of the gastrointestinal tube and relative structures, such as the perineal body and urogenital organs. These types of malformations fall on a wide spectrum, from simpler to more complex defects such as cloaca; therefore, functional outcomes range from good - in the simplest cases - to poor in the rarest and most complex situations. From early life, ARM children require a diagnostic pathway that identifies the exact type of malformation (along with comorbidities) and therefore the correct treatment and management path [1,2,3,4,5,6,7,8]. In recent years, pediatric surgeons have gradually focused more and more on long-term follow-up, especially for fecal continence: even when surgical interventions restore near-normal anatomy of both the genitourinary and the gastrointestinal systems, fecal continence remains dependent on complex interactions between pelvic anatomy (both innate and surgically reconstructed) and the central nervous system. This can make postsurgical management very complicated: despite adequate surgical repair, 60-70% of ARM patients will still experience severe constipation and/or fecal incontinence persisting into adulthood for many of these patients (23% to 40%), which has a very significant impact on the quality of life [9,10,11,12,13,14,15,16,17,18]. Furthermore, between 50 and 80% of ARM patients suffer from at least one additional congenital malformation (genitourinary, cardiac, skeletal, or spinal). As a consequence, lifelong multidisciplinary follow-up can be required to optimize outcome and manage complications timely. Patients with associated anomalies of the spinal cord, sacrum or GU system, for instance, tend to experience an overall poorer outcome and quality of life. [19,20,21,22,23,24,25,26,27].
The main predictors of longer-term success in fecal continence in ARM patients are the type of anorectal malformation; the presence of spinal anomalies; and the sacral integrity. These parameters can be used to determine the patient's potential for bowel control and thus their bowel management regime, such as oral medications or enema/TAI (transanal irrigation). [28,29,30,31,32,33].Functional assessment of the anorectum has been performed recently with High Resolution Manometry (HRM), establishing normal values in pediatric age too. [34]. Standard manometric studies in children with ARM suggest that anorectal pressure profiles are indicators of abnormal sphincter function and therefore predictors of fecal incontinence (FI) after surgical correction. [35]. As the structural integrity and function of pelvic floor muscles plays a critical role in establishing and maintaining continence, Three-Dimensional High Resolution Anorectal Manometry (3D-HRAM) can provide an image of the pressure profile of the whole anal sphincter complex, thus allowing to evaluate each individual muscle’s contributions to intra-anal pressure characteristics; this has been evaluated in ARM patients as well, but only a few studies have addressed the findings on advanced anorectal manometry in relation to the long-term functional outcome [36]. The goal of our study was to evaluate the anal sphincter function in ARM patients with high-resolution anorectal manometry and 3D reconstruction, correlating the advanced and multiplanar pressure analysis to clinical outcome and bowel management needs; as a secondary target, we evaluated how the presence of associated malformations (urological and spinal, namely) can affect the prognosis.
2. Materials and Methods
Patients
A prospective analysis was conducted in our center from 2020 to 2022. Forty patients up to 17 years of age, operated on for anorectal malformations, were included in the study. All patients included in this study underwent perineal surgery with both Posterior Sagittal Anorectoplasty (PSARP) or anterior approach; we excluded patients who underwent laparoscopic surgery. We classified ARM types based on the Krickenbeck International Classification according to the type of fistula and on the basis of Wingspread classification into high, intermediate or low based on the level of rectum in relation to the levator ani muscle on an invertogram. [37,38].
Associated anomalies - above all urological and spinal - were assessed in all patients. Namely, for spinal anomalies the sacral ratio was evaluated [27,31].; other intestinal or extraintestinal anomalies were also recorded. All patients had fecal incontinence evaluated with colonic enema and rectal ultrasound, in order to identify a megarectum in patients with retentive fecal incontinence compared to those with primary fecal incontinence, as previously described [39].
Patients with pseudo- incontinence are patients with potential for bowel control, but who soil due to fecal impactions or because the stools move too quickly; patients with true incontinence, on the other hand, lack the ability to have a voluntary bowel movement, have poor pelvic sphincters and may have poor innervation of the rectum and sphincters in case of spinal associated anomalies.
We defined an anatomic score (reported in Table 1) for all patients, based on the anatomical perineal data: the closer to normal the patient’s perineal anatomy, the higher the score on a scale from 0 to 10.
As for clinical outcome, we calculated the Rintala Bowel Function Score in all patients, based on seven questions, each with a possible score from 0 to 3 (except for the frequency of defecation, going from 0 to 2). We considered a total score of 18 or more as an indicator of normal bowel continence. [40]. This score was evaluated before and after introduction of bowel management (BM) with enema or TAI. The response to BM was defined as poor, sufficient or excellent considering the difference in Rintala score after at least 3 months of treatment with TAI; we used our previously reported TAI protocol [41].
Manometric Procedure
All patients underwent anorectal manometry with 3D sphincter reconstruction, as described in our previous paper [41]. The study was performed with ManoScan® Anorectal High-Resolution Manometry (3D HRAM 360/3D, Medtronic, Dublin, Ireland). Data acquisition, display, and analyses were performed with the ManoView Software.
All patients received an enema the night prior to the procedure.
The 3D HRAM probe is a solid-state rigid tube, with 256 sensors distributed in 16 circumferences spaced along 16 axial levels. The probe has a central lumen for inflation and a luer lock at one end, through which a non-latex balloon is attached; the probe is marked to identify the anterior or posterior axis and the orientation was maintained accurately throughout, to avoid any rotation; with the patient in the left lateral position, after lubrication, the probe was gently inserted into the anal canal and slowly advanced until the upper and lower borders of the high-pressure zone were identified. The posterior marking on the probe was used by the investigator throughout the study to maintain proper orientation of the probe in relation to ventral and dorsal aspects of the anal canal. Once the probe in place, a resting period of at least 90 seconds was allowed until the patients were conformable and relaxed.
During a conventional 2-dimensional (2D) high-resolution manometry, the manometry probe allows a standard visualization of the anal canal as a high-pressure zone (HPZ) at rest (anal resting pressure, ARP) and during squeeze (anal squeeze pressure, ASP), measuring its length. The high-pressure zone was identified and thirty seconds of resting pressures were obtained. The patients were then instructed to squeeze (maximum voluntary contraction), thus determining their ability to squeeze and recording the squeeze pressure characteristics (force in mmHg, reported as total pressure post increment, and its duration above or below 10 sec). In order to evaluate the recto-anal inhibitory reflex (RAIR), the balloon was then rapidly inflated and deflated with a series of volumes, and a full dose-response curve was obtained. After identifying the HPZ and measuring rest and squeeze pressures, the corresponding 3D HDARM topographic pressure view was used to obtain longitudinal and radial pressure measurements of the anal canal, both at rest and during squeeze maneuver, in order to evaluate the dynamics of the anal channel.
With 2D and 3D HRAM, we evaluated the following parameters:
- Mean resting anal pressure;
- Maximum voluntary contraction during squeeze maneuver (vs. resting pressure);
- Sphincteric asymmetry (difference between resting and squeeze pressure above 20% between four cardinal anal segments, evaluated with 3D analysis);
- RAIR/rectal sensibility (recto-anal inhibitory reflex / first sensation and urge sensation)
- Presence of abdominal-perineal dyssynergia
- General aspects of pressure cylindric image
On the basis of the overall manometric results we have devised a manometric score, as shown in Table 2.
Correlations between the type of ARM, presence of associated anomalies, anatomical, clinical and manometric scores were calculated; the manometric score in different types of ARM has also been correlated to BM response.
Statistical Analysis
Statistical analysis of quantitative and qualitative data, including descriptive statistics, was performed for all items. The Shapiro–Wilk test was used to evaluate the normality of the distribution of the quantitative data. Continuous data were expressed as mean ± standard deviation (SD), unless otherwise specified. Frequency analysis was performed using the Pearson’s chi-square test and Fisher exact test, as needed. The univariate analysis of variance (ANOVA) was performed to compare the mean differences in continuous variables between the different patient groups or different patient subgroups, and post hoc analysis with the Tukey test was used to determine whether there were pairwise intragroup differences. Moreover, a multinomial regression analysis was performed to evaluate the relationship between BM response and HRM and EO data.
Data were analyzed by IBM SPSS Software 24 version (IBM Corp., Armonk, NY, USA). All p-values were two-sided and p<0.05 was considered statistically significant.
3. Results
Demographic data, types of ARM and anatomical scores are reported in Table 3.
Among male patients, 3 had recto-vescical fistula, 5 had recto-urethral prostatic fistula, 4 had recto-urethral bulbar fistula and 10 had perineal fistula; among female patients, 1 had cloaca with short channel, 5 had recto-vestibular fistula, 6 had perineal fistula and 1 had rectal atresia without fistula.
According to the Wingspread classification 19 pts had a high ARM, whereas 21 had a low ARM; 10 male pts also had urinary malformations (4 vescical ureteral reflux - VUR, 1 renal agenesis, 2 vescical diverticula, 1 posterior urethral valve and 2 hypospadias); 4 female pts had VUR, whereas 2 had vaginal malformation (vaginal atresia and septate uterus). Sacral and spinal malformation were reported in 11 pts (8 males and 3 females), namely tethered cord (3 pts), sacral cleft (3 pts), sacral agenesis (1 pt), hemisacrum (1 pt) and presacral mass (3 pts). In all patients with sacral anomalies the sacral ratio (SR) was less than 0.5. Colostomy was performed in 19 patients (13 males and 6 females), whereas surgery was performed in a single stage in all the others.
Correlations between type of ARM, associated anomalies, anatomical, manometric and clinical (pre and post BM) score are reported in Table 4.
A positive correlation between anatomical score and type of ARM was found: in patients with high ARM a lower anatomical score was reported if compared with low ARM (p <0.005 ); patients with high ARM also have lower values of Rintala and manometric scores, and even after BM they do not achieve continence score values associated with good continence, thus needing daily BM to remain clean. In patients with low ARM, the Rintala score pre-BM was better, as well as the manometric score; in these patients, the response to BM was excellent, with high values of the continence score. Regardless of ARM type, patients with spinal anomalies also showed lower values in anatomical, clinical and manometric scores and had a poor response to BM; an intermediate behavior was found in patients with urological malformations.
No correlation was found between the scores and the presence of other anomalies such as esophageal atresia, cardiac malformation or limb anomalies.
Correlation between manometric score and response to BM in all patients, considering the type of ARM and associated anomalies, are reported in Table 5.
We founded a correlation between manometric score and response to BM: in patients with a manometric score higher than 5, the response to BM was excellent, with a good continence as follow in Figure 1 A,B.
Values of anal pressure, divided in the four quadrants, are reported in Table 6. All patients with ARM have values that are significantly lower than references in literature for pediatric patients without ARM; patients with spinal anomalies, regardless of type of ARM, showed even lower pressure values compared with other ARM patients that do not have a spinal anomaly
Table 6. A: Description of manometric parameters for all 4 sphincter quadrants on 3D reconstruction, in all patients and according the type of ARM and associated anomalies. Pts: patients; ARM: anorectal malformation, BM: bowel management, HRM: high resolution manometry; malf: malformation; ARP: anal resting pressure; ASP: anal squeeze pressure; ant: anterior; post: posterior; SD: standard deviation.
| Type of ARM |
Mean ARP mmHg Mean (SD) |
Ant ARP Mean (SD) |
Post ARP Mean (SD) |
Right ARP Mean (SD) |
Left ARP Mean (SD) |
Mean ASP Mean (SD) |
Ant ASP Mean (SD) |
Post ASP Mean (SD) |
Right ASP Mean (SD) |
Left ASP Mean (SD) |
| Total pts | 35.6 (13.1) | 32.9 (13.6) |
37.2 (13.4) | 33.6 (12.7) | 33.6 (13.7) | 78.9 (31.5) | 74.1 (30.5) | 84.1 (34.3) | 75.8 (32.1) | 53.1 (20.7) |
| High ARM | 26.0 (9.6) | 23.3 (9.7) |
27.4 (10.3) | 24.8 (9.7) | 24.2 (10.5) | 55.4 (19.7) | 51.2 (19.9) | 58.2 (21.2) | 51.4 (21.1) | 53.1 (20.7) |
| Low ARM | 44.3 (9.4) | 41.8 (10.2) |
46.1 (8.9) |
41.6 (9.6) | 42.2 (10.2) |
100.1 (24.1) | 94.9 (22.6) | 107.4 (26.2) | 97.9 (23.1) | 98.9 (24.1) |
| ARM with urological malf | 26.9 (8.9) | 23.9 (8.7) | 28.2 (10.2) | 25.0 (8.7) | 25.1 (9.2) |
59.9 (26.3) | 55.1 (26.2) | 63.3 (27.5) | 56.0 (27.7) | 57.7 (27.8) |
| ARM with spinal malf | 20.1 (5.0) | 17.3 (5.3) | 21.3 (6.1) |
19.1 (5.7) | 18.6 (7.1) |
42.6 (12.1) | 38.4 (12.2) | 44.6 (13.6) | 38.6 (14.7) | 40.0 (14.3) |
| p | < 0.005 | < 0.005 | < 0.005 | < 0.005 | < 0.005 | < 0.005 | < 0.005 | < 0.005 | < 0.005 | < 0.005 |
Table 6. B: Description of manometric parameters after 3D reconstruction in all and according the type of ARM and associated anomalies. Pts: patients; ARM: anorectal malformation, BM: bowel management, HRM: high resolution manometry; malf: malformation; SD: standard deviation; HPZ: high pressure zone; RAIR: recto anal inhibitory reflex.
| Type of ARM |
Lenght HPZ cm Mean (SD) |
Asimmetry > 20% (n/%) |
Duration of contraction < 10 sec (n/%) |
Dyssynergy (n/%) |
RAIR present (n/%) |
| Total pts | 1.9(0.6) | 11/40 | 13/40 | 19/40 | 11/40 |
| High ARM | 1.6(0.5) | 9/19 | 12/19 | 11/19 | 9/19 |
| Low ARM | 2.2(0.5) | 2/21 | 1/21 | 8/21 | 20/21 |
| ARM with urological malf | 1.7(0.48) | 7/16 | 10/16 | 11/16 | 8/16 |
| ARM with spinal malf | 1.4(0.5) | 9/11 | 10/11 | 6/11 | 1/11 |
| p |
In the Figure 2 A and B the anal channel pressure profile was showed with differences between patients with high and low ARM respectively: in the first case (A) the colorimetric image of anal sphincter showed a very low pressure both at rest, during squeeze with an altered comprehensive aspect of cylinder.
4. Discussion
Anorectal malformations (ARM) are anomalies that cannot be corrected by surgery only. Even for patients with excellent surgical outcomes, defecation issues can remain a lifetime experience. Some patients may be indistinguishable from normal subjects, other may present severe functional alterations [1,2,3,4,5,6,7,8]. An important aspect is related to the presence of associated anomalies, affecting up to 60–70% of ARM patients (30% of all patients have cardiac defects, >50% have urological abnormalities, 5–10% have esophageal/duodenal atresia). These associated anomalies deeply affect the prognosis and can also complicate surgery. [8,9,10,11,12,13,14,15,16,17,18].
Fecal continence depends on three main factors: sensation within the rectum, good colonic motility, and good sphincter control [42]: patients with ARM have varying degrees of underdevelopment of the muscle complex [43]. Patients with ARMs are born without an anal canal: therefore, sensation does not exist and it seems that the patient can perceive only distention of the rectum (proprioception): the most important clinical implication of this, is that liquid stool or soft fecal material may not be felt by the patient as it does not distend the rectum.
According to Levitt and Peña, the outcome of surgical patients can be based on the anatomical classification of the ARM and the presence of sacral and/or associated spinal cord anomalies. [4,17,18]. The authors described the morphological and functional factors responsible for constipation (megarectum, megasigmoid, and denervation) and fecal incontinence (defect of development of anal sphincters, rectal sensation, and bowel motility) and proposed an individualized bowel management program that must be started early for patients with the worst prognosis in order to keep the patient clean and stooling regularly and to improve their quality of life: the goal of a BM program is to find a laxative or enema regimen that reliably empties the colon, allows the patient to achieve social continence, and resume daily activities. [15,44]. There is a need for assessment tools to standardize clinical outcomes in patients with ARM: these tools can be either laboratory methods such as anorectal manometry or clinical scoring systems identifying a correlation between them, in order to use these as prognostic outcomes with a practical implication.
Constipation is the most frequent morbidity encountered after the surgical repair of an ARM and is most common in patients having preserved rectosigmoid after pull-down surgery for ARMs: it occurs due to mechanical or functional reasons and its inadequate treatment can result in mega rectum/mega rectosigmoid leading to fecal impaction and overflow incontinence [17,18]. Failure to recognize or adequately treat this associated hypomotility in ARM patients can lead to significant morbidity, which we believe is largely preventable. Children treated for low ARM usually have a good bowel control, but still may suffer from temporary episodes of fecal incontinence, especially when they experience diarrhea. Some 25% of all ARM children suffer from true fecal incontinence, and those are the patients who will need a constant and tailored bowel management program to keep clean: they have a hypoplastic anal sphincter, correlated to severity of ARM, and unfortunately in some cases this can be worsened by surgery if there is no correct centering of the neoanus within the muscle complex, or if there is damage to the rectum innervation during its mobilization. [11,16,17,18].
Reports of associated urological anomalies in ARM patients widely vary with reports from 18% to 85%:most series with active screening protocols report a prevalence of around 50% across all ARM types. There are 4 main factors that influence long term urological health: the presence of intrinsic kidney or bladder anomalies at birth, the presence of sacral dysgenesis, the effect of the operative intervention to correct the ARM and the effect of spinal cord tethering causing bladder dysfunction which may change over time. A normal renal and urinary tract assessment at birth does not preclude the development of potentially serious long-term complications, which may remain clinically silent until there is severe chronic kidney disease. [22,23,45].
Evaluation of the sacrum in patients with ARM is important because of the well-established association between sacral hypodevelopment or dysmorphism and poor functional outcome after anorectal reconstruction. In addition to the sacral bony abnormalities, evaluation of spinal dysraphism should include abnormalities of the spinal cord itself because so-called spinal cord tethering is associated with various orthopedic, urologic, and gastrointestinal problems. The presence of severe sacral abnormalities is associated with hypoplastic sphincters. If more than two sacral vertebrae are missing, or if the patient has other major sacral deformities, such as hemivertebrae and vertebral fusions, the functional outcome is worse than in patients with normal sacrum or lesser degree of sacral maldevelopment: a sacral ratio less of 0.6 was related to poor outcome. The prevalence of spinal dysraphism in patients with ARMs is about 35 %, and clinically significant spinal cord tethering requiring detethering surgery is about 20 %: more complex types of anorectal defects were associated with a higher prevalence of spinal dysraphism. [24,25,26,27,28,29,30,31]. Regarding the functional assessment of continence with anorectal conventional manometric, data obtained at rest and after voluntary muscular contraction and information related to rectal sensation and after eliciting the RAIR, can give a good picture of sphincter activity. The resting pressure depends on the constant state of contraction if the IAS at rest (85%) and partially on the EAS (15%), whereas the squeezing pressure is generated by the voluntary contraction of the EAS. A positive RAIR indicates good activity of the IAS, whereas its absence correlates well to a deficiency or scarring of the sphincter. [35,36,37,38,39,40,41,42,43,44,45,46]. Manometric studies in children with ARM have demonstrated that low intra-anal pressures at rest-squeeze, and the absence of the recto-anal inhibitory reflex (RAIR) are associated with poor clinical outcomes and incontinence. Many patients with ARM lack the recto-anal inhibitory reflex probably as a consequence of corrective surgery or the inborn atresia of the anal canal: an absence of RAIR is proposed to contribute to the development of constipation as it increases anal resting pressure [46,47,48,49,50]. These manometric data was well correlated with morphological studies using endoanal ultrasound [51,52,53] and magnetic resonance (MRI) [54,55,56,57,58].: Caldaro et al underlined how the integrity of the IAS and an adequate anal resting pressure (ARP) of 30 mm Hg were necessary to assure a good continence. [53]. In our previous study we demonstrated a good correlation between manometry and magnetic resonance correlating this to the response to biofeedback and BM. [59]. However, traditional water-perfused and 2D high-resolution manometric testing do not allow for full characterization of the anal canal and its individual muscle contributions: it does not provide specific information about individual components of anorectal pressure and function and so it can’t predict an exact prognosis. Recently, 3D high-definition anorectal manometry (3D HRAM) has been evolved for a detailed assessment of pressure distributions in the anal canal: it has 256 sensors distributed circumferentially providing a topographic and three-dimensional (3D) pressure representation of the anal canal. [36]. Well correlating with MRI and ultrasound, 3D HRAM has been used in adults to evaluate anatomic structures and delineate the individual muscle contributions of the puborectalis (PR) muscle, internal anal sphincter (IAS), and the external anal sphincter (EAS) to intra-anal pressure characteristics. [60,61,62]. In patients with ARM a radial and longitudinal asymmetry across the anal canal and sphincter defects have been demonstrated and these data could be correlated to the severity of fecal incontinence. Elevated distal canal pressures on anorectal manometry are a primary contribution of the EAS: inadequate placement of the anal opening to the center of the EAS muscle complex affects continence and disruption, defects, and scarring of the EAS muscle complex have been associated with low intra-anal pressures and clinically correlated with FI. During the dynamic process from rest to squeeze the ability to generate the squeeze was significantly different between controls and ARM patients, indicating a decline in the ability to voluntarily recruit the EAS muscles and generate appropriate squeeze effort and this has been associated with altered fecal continence [50,63,64,65]. The PR muscle plays a key role in maintenance of continence by preservation of the anorectal angle at rest and by contraction and narrowing of the anorectal angle during squeeze. Abnormalities of the PR muscle complex disrupt its ability to modulate the anorectal angle and, therefore, compromise continence: these data have been shown in children with anorectal malformations with poor clinical outcomes and associated FI. [66]. High-resolution manometry also enables a precise diagnosis of the type of dyssynergia: ARM-patients with constipation have a dyssynergic pattern type 1 in 90% of cases and type IV in the last cases. [67,68]. There is a great variation in literature as for functional results after repair of anorectal malformations. This is due to the fact that there is no generally agreed method to assess the bowel function of patients with anorectal malformations. In the study of Ambartsumyan et al, manometric properties obtained with 3D HRAM at rest were not associated with reported predictor of fecal continence. [66] In our analysis, we confirmed the results of previous studies conducted with traditional manometry: ARM patients showed anomalies of sphincter as lower pressure values, in particular the posterior quadrant pressures are diminished at rest and squeeze in the high ARM group vs low and an altered topographic 3D view was showed, RAIR was absent in high ARM especially in cases with associated spinal anomalies. Radial and longitudinal aspect of the anal channel was different in high and low ARM. Differently from previous 3D HRAM study, we found a strong correlation between manometric results and clinical outcome, with specific regard to the type of ARM and presence of urological and spinal anomalies. In order to simplify the comparison and correlation with clinical continence score, we created an anatomic and a manometric score taking into account the status of perineum post-surgery and the main parameters evaluated during manometry. Manometric results correlated well to clinical and anatomical scores; our study demonstrates that patients with high ARM and spinal anomalies show lower values of the manometric score, and that is correlated to a poor response to BM. Such correlations enhance the value of manometry, especially 3D HRAM, as a study tool in patients with ARM, in order to provide prognostic data that correlates with the degree of continence and quality of life perspectives: based on manometric data, we can predict how the patient will respond to BM, and so we can tailor the BM with TAI and BFB treatment in order to ensure the maximum level of cleanliness. We propose a biofeedback program to collaborative patients with disruptions of the IAS to develop the strength of the sphincter: biofeedback exercises improve patients' control of the appropriate group of muscles for continence and can also increase the compliance of children with the other bowel management treatments [59]. In patients with high ARMs and severe defects of the IAS, biofeedback therapy was performed to reinforce voluntary sphincter function because adequate anal continence could not be achieved when IAS was absent.
We can also confirm that the presence of associated anomalies such as urological or spinal negatively affects the prognosis of ARM patients. In these cases, it is mandatory to start tailored BM programs as soon as possible. The main limit of our study is that we evaluated only ARM patients with fecal incontinence, and therefore we are missing a control group made up of patients with or without ARM but normally continent. We decided to refer to the manometric values in literature, as they are confirmed and standardized in several studies. Additionally, we did not correlate the manometric data with topographic pressure view to a pure morphological study, such as endoanal ultrasound or MRI. We chose not to include patients treated with laparoscopic approach in this study as it is our intent to focus on those in future study: we strongly think that laparoscopically assisted anorectal pull-through (LAARP) for high-type ARMs can reduce the amount of posterior dissection of the sphincter mechanism, required for the accurate placement of the neorectum into the muscle complex, and should therefore result in lesser disturbance of the muscle innervation, in better sphincter symmetry, and lesser irregularity and perirectal fibrosis compared to PSARP [69,70].
5. Conclusions
3D-HRAM can provide information on the functional anatomy of the sphincter complex after reconstruction in patients affected by ARM. The clinical significance of this method has yet to be fully proven, but, in our opinion, our study shows good correlation between the manometric results and clinical outcome, additionally confirming spinal malformations and ARM type as most important prognostic risk factors for poor outcome. Individual patient and specific sphincteric defects can be explored with manometry, thus allowing for tailored bowel management strategies. [71].
Author Contributions
Conceptualization: A.M. Caruso and M.R. Di Pace. Methodology: D. Bommarito,. Girgenti, A Glenda.Software: U. Calabrese, A. Figuccia. Validation: M. Milazzo, M.R Di Pace. Formal analysis: A. Casuccio. Investigation: F. Baldanza, F. Grasso, E. Giglione. Resources: A.M. Caruso. Data curation: A.M. Caruso and M.R. Di Pace. Writing—original draft preparation: A.M. Caruso. Writing—review and editing: M.R. Di Pace. Visualization: V. Girgenti, D. Bommarito. Supervision: M. R Di Pace M. Milazzo. Project administration: A.M. Caruso and M.R. Di Pace All authors have read and agreed to the published version of the manuscript
Funding
not applicable.
Institutional Review Board Statement
All subjects gave their informed consent for inclusion before they participated in the study. The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Ethics Committee of Palermo, the code of ethic approval is CIP 001 TAI-pediatric- Rev 0 (19 feb 2020)
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study
Acknowledgments
The authors thank Andrea Mandalà for his contribution in the image’s creation
Conflicts of Interest
The authors have no financial conflicts of interest to declare
References
- King SK, Krois W, Lacher M, et al. Optimal management of the newborn with an anorectal malformation and evaluation of their continence potential. Semin Pediatr Surg. 2020 Dec;29(6):150996. [CrossRef]
- Masi P, Miele E, Staiano A. Pediatric anorectal disorders. Gastroenterol Clin North Am. 2008 Sep;37(3):709-30, x. [CrossRef]
- Rintala RJ, Pakarinen MP. Imperforate anus: long- and short-term outcome. Semin Pediatr Surg. 2008 May;17(2):79-89. [CrossRef]
- Bischoff A, Levitt MA, Peña A. Update on the management of anorectal malformations. Pediatr Surg Int. 2013 Sep;29(9):899-904. [CrossRef]
- Arnoldi R, Macchini F, Gentilino V, et al. Anorectal malformations with good prognosis: variables affecting the functional outcome. J Pediatr Surg. 2014 Aug;49(8):1232-6. [CrossRef]
- Pelizzo G, Canonica CPM, Destro F, et al. Anorectal Malformations: Ideal Surgery Timing to Reduce Incontinence and Optimize QoL. Children (Basel). 2023 Feb 18;10(2):404. [CrossRef]
- Upadhyaya VD, Bharti LK, Mishra A, et al. Constipation after surgery for anorectal malformations: Unrecognised problem until it is a problem. Afr J Paediatr Surg. 2021 Jan-Mar;18(1):67-71. [CrossRef]
- AbouZeid AA, Bayoumi MM, Abo El-Ela MM. Anorectal anomalies in the female: Highlights on surgical management. J Pediatr Surg. 2021 Sep;56(9):1570-1575. [CrossRef]
- Baxter KJ, Garza JM, Rollins MD, et al. Multi-institutional review of bowel management strategies in children with anorectal malformations. J Pediatr Surg. 2020 Dec;55(12):2752-2757. [CrossRef]
- Style CC, Hsu DM, Verla MA, et al. Development of a multidisciplinary colorectal and pelvic health program: Program implementation and clinical impact. J Pediatr Surg. 2020 Nov;55(11):2397-2402. [CrossRef]
- Nash O, Zobell S, Worst K. Bowel management for the treatment of fecal incontinence and constipation in patients with anorectal malformations. Seminars in Pediatric Surgery. 2020. [CrossRef]
- Tofft L, Klasson S, Salö M, et al. Patient-reported physical and psychosocial significance of abdominal scarring in anorectal malformations. J Pediatr Surg. 2022 Oct;57(10):348-353. [CrossRef]
- Van der Steeg HJJ, Van Rooij IALM, Iacobelli BD, et al. Bowel function and associated risk factors at preschool and early childhood age in children with anorectal malformation type rectovestibular fistula: An ARM-Net consortium study. J Pediatr Surg. 2022 Sep;57(9):89-96. [CrossRef]
- Chang PC, Duh YC, Fu YW, et al. How much do we know about constipation after surgery for anorectal malformation? Pediatr Neonatol. 2020 Feb;61(1):58-62. [CrossRef]
- Bischoff A, Levitt MA, Peña A. Bowel management for the treatment of pediatric fecal incontinence. Pediatr Surg Int. 2009 Dec;25(12):1027-42. [CrossRef]
- Levitt M, Peña A. Update on pediatric faecal incontinence. Eur J Pediatr Surg. 2009 Feb;19(1):1-9. [CrossRef]
- Levitt MA, Kant A, Peña A. The morbidity of constipation in patients with anorectal malformations. J Pediatr Surg. 2010 Jun;45(6):1228-33. [CrossRef]
- Levitt MA, Peña A. Pediatric fecal incontinence: a surgeon's perspective. Pediatr Rev. 2010 Mar;31(3):91-101. [CrossRef]
- Oh C, Youn JK, Han JW, et al. Analysis of Associated Anomalies in Anorectal Malformation: Major and Minor Anomalies. J Korean Med Sci. 2020 Apr 13;35(14):e98. [CrossRef]
- De Beaufort CMC, Van den Akker ACM, Kuijper CF, et al. The importance of screening for additional anomalies in patients with anorectal malformations: A retrospective cohort study. J Pediatr Surg. 2022 Nov 25:S0022-3468(22)00740-0. [CrossRef]
- Kruger P, Teague WJ, Khanal R, et al. Screening for associated anomalies in anorectal malformations: the need for a standardized approach. ANZ J Surg. 2019 Oct;89(10):1250-1252. [CrossRef]
- Skerritt C, DaJusta DG, Fuchs ME, et al. Long-term urologic and gynecologic follow-up and the importance of collaboration for patients with anorectal malformations. Semin Pediatr Surg. 2020 Dec;29(6):150987. [CrossRef]
- Duci M, Midrio P, Castagnetti M, et al. Urinary Tract Anomalies in Patients With Anorectal Malformations: The Role of Screening and Clinical Follow-Up. Urology. 2020 Sep;143:216-220. [CrossRef]
- Levitt MA, Patel M, Rodriguez G,et al. The tethered spinal cord in patients with anorectal malformations. J Pediatr Surg. 1997 Mar;32(3):462-8. [CrossRef]
- Kim SM, Chang HK, Lee MJ, Shim KW, Oh JT, Kim DS, et al. Spinal dysraphism with anorectal malformation: lumbosacral magnetic resonance imaging evaluation of 120 patients. J Pediatr Surg 2010;45:769e76. [CrossRef]
- Kyrklund K, Pakarinen MP, Taskinen S, et al. Spinal cord anomalies in patients with anorectal malformations without severe sacral abnormalities or meningomyelocele: outcomes after expectant, conservative management. J Neurosurg Spine. 2016 Dec;25(6):782-789. [CrossRef]
- Marı´a Fanjul, I. Samuk, P. Bagolan et al. Tethered cord in patients affected by anorectal malformations: a survey from the ARM-Net Consortium. Pediatr Surg Int (2017) 33:849–854. [CrossRef]
- Fernandez-Portilla E, Moreno-Acosta L, Dominguez-Muñoz A, et al. Functional outcome after cord detethering in fecally incontinent patients with anorectal malformations. Pediatr Surg Int. 2021 Apr;37(4):419-424. [CrossRef]
- Esposito G, Totonelli G, Morini F, et al. Predictive value of spinal bone anomalies for spinal cord abnormalities in patients with anorectal malformations. J Pediatr Surg. 2021 Oct;56(10):1803-1810. [CrossRef]
- Ahmad H, Halleran DR, Vardanyan J,et al. Functional fecal and urinary outcomes after sacrococcygeal mass resection in pediatric patients. J Pediatr Surg. 2021 Jun;56(6):1142-1147. [CrossRef]
- Chen Z, Zheng L, Zhang M, Zhang J, Kong R, Chen Y, Liang Z, Levitt MA, Wei CH, Wang Y. Sacral Curvature in Addition to Sacral Ratio to Assess Sacral Development and the Association With the Type of Anorectal Malformations. Front Pediatr. 2021 Oct 1;9:732524. https://doi.org/10.3389/fped.2021.732524. Erratum in: Front Pediatr. 2022 May 06;10:922448. PMID: 34660489; PMCID: PMC8519007.
- Bjoersum-Meyer T, Kaalby L, Lund L, et al. Long-term Functional Urinary and Sexual Outcomes in Patients with Anorectal Malformations-A Systematic Review. Eur Urol Open Sci. 2021 Feb 3;25:29-38. [CrossRef]
- Senel E, Demirbag S, Tiryaki T, et al. Postoperative anorectal manometric evaluation of patients with anorectal malformation. Pediatr Int. 2007 Apr;49(2):210-4. [CrossRef]
- Banasiuk M, Banaszkiewicz A, Dziekiewicz M, et al. Values From Three-dimensional High-resolution Anorectal Manometry Analysis of Children Without Lower Gastrointestinal Symptoms. Clin Gastroenterol Hepatol. 2016 Jul;14(7):993-1000.e3. [CrossRef]
- Bjørsum-Meyer T, Christensen P, Jakobsen MS, et al. Correlation of anorectal manometry measures to severity of fecal incontinence in patients with anorectal malformations - a cross-sectional study. Sci Rep. 2020 Apr 7;10(1):6016. [CrossRef]
- Ambartsumyan L, Rodriguez L, Morera C, et al. Longitudinal and radial characteristics of intra-anal pressures in children using 3D high-definition anorectal manometry: new observations. Am J Gastroenterol. 2013 Dec;108(12):1918-28. [CrossRef]
- Holschneider, A.; Hutson, J.; Peña, A.; Beket, E.; Chatterjee, S.; Coran, A.; Davies, M.; Georgeson, K.; Grosfeld, J.; Gupta, D.; et al. Preliminary report on the International Conference for the Development of Standards for the Treatment of Anorectal Malformations. J. Pediatr. Surg. 2005, 40, 1521–1526. [Google Scholar] [CrossRef] [PubMed]
- Levitt, M.A.; Pena, A. Imperforate Anus and Cloacal Malformations. In Aschcraft’s Pediatric Surgery, 6th ed.; Holcomb, G.W., III, Murphy, J.P., St Peter, S.D., Eds.; Elsevier Inc.: Amsterdam, The Netherlands, 2014. [Google Scholar]
- Di Pace MR, Catalano P, Caruso AM et al. Is rectal disimpact always necessary in children with chronic constipation? Evaluation with pelvic ultrasound. Pediatr Surg Int 2010; 26:601–606. [CrossRef]
- Rintala R., J. , Lindahl H et al. Is normal bowel function possible after repair of intermediate and high anorectal malformations ?. Journal of Pediatric Surgery 1995; vol. 30 (3): 491–49. [CrossRef]
- Caruso AM, Milazzo MPM, Bommarito D et al. Advanced management protocol of Transanal Irrigation in order to improve the outcome of pediatric patients with fecal incontinence Children 2021; dec11: 8(12):1174. [CrossRef]
- Roupakias S, Sinopidis X. Pelvic Floor Muscles Contribution in Surgical Outcome of Children with High-type Anorectal Malformations. Prague Med Rep. 2021;122(3):191-200. [CrossRef]
- Feil P, Krois W, Weber M, et al. Low muscle volume of the anal sphincter complex: A novel prognostic factor in children with anorectal malformations? J Pediatr Surg. 2022 Aug;57(8):1467-1472. [CrossRef]
- Lim IIP, Cushing CC, Jenkins T, et al. Prospective quality of life outcomes in pediatric fecal incontinence following bowel management. J Pediatr Surg. 2021 Aug;56(8):1459-1464. https://doi.org/10.1016/j.jpedsurg.2021.04.025. [CrossRef]
- Deng C. Re: role of urodynamics in male patients of high-anorectal malformations: a prospective study. Pediatr Surg Int. 2021 Aug;37(8):1149-1150. [CrossRef]
- Mert M, Sayan A, Köylüoğlu G. Comparing the fecal continence scores of patients with anorectal malformation with anorectal manometric findings. Pediatr Surg Int. 2021 Aug;37(8):1013-1019. [CrossRef]
- Kumar S, Al Ramadan S, Gupta V, et al. Use of anorectal manometry for evaluation of postoperative results of patients with anorectal malformation: a study from Kuwait. J Pediatr Surg. 2010 Sep;45(9):1843-8. [CrossRef]
- Kyrklund K, Pakarinen MP, Rintala RJ. Manometric findings in relation to functional outcomes in different types of anorectal malformations. J Pediatr Surg. 2017 Apr;52(4):563-568. [CrossRef]
- Keshtgar AS, Athanasakos E, Clayden GS, et al. Evaluation of outcome of anorectal anomaly in childhood: the role of anorectal manometry and endosonography. Pediatr Surg Int. 2008 Aug;24(8):885-92. [CrossRef]
- Bhat NA, Grover VP, Bhatnagar V. Manometric evaluation of postoperative patients with anorectal anomalies. Indian J Gastroenterol. 2004 Nov-Dec;23(6):206-8.
- Emblem R, Mørkrid L, Bjørnland K. Anal endosonography is useful for postoperative assessment of anorectal malformations. J Pediatr Surg. 2007 Sep;42(9):1549-54. [CrossRef]
- Wang Z, Hu L, Jin X, et al. Evaluation of postoperative anal functions using endoanal ultrasonography and anorectal manometry in children with congenital anorectal malformations. J Pediatr Surg. 2016 Mar;51(3):416-20. [CrossRef]
- Caldaro T, Romeo E, De Angelis P, et al. Three-dimensional endoanal ultrasound and anorectal manometry in children with anorectal malformations: new discoveries. J Pediatr Surg. 2012 May;47(5):956-63. [CrossRef]
- Desai SN, Choudhury H, Joshi P, et al. Magnetic resonance imaging evaluation after anorectal pull-through surgery for anorectal malformations: a comprehensive review. Pol J Radiol. 2018 Jul 11;83:e348-e352. [CrossRef]
- Bjørsum-Meyer T, Christensen P, Baatrup G, et al. Magnetic resonance imaging of the anal sphincter and spine in patients with anorectal malformations after posterior sagittal anorectoplasty: a late follow-up cross-sectional study. Pediatr Surg Int. 2021 Jan;37(1):85-91. [CrossRef]
- Husberg B, Rosenborg M, Frenckner B. Magnetic resonance imaging of anal sphincters after reconstruction of high or intermediate anorectal anomalies with posterior sagittal anorectoplasty and fistula-preserving technique. J Pediatr Surg. 1997 Oct;32(10):1436-42. [CrossRef]
- Fukuya T, Honda H, Kubota M, et al. Postoperative MRI evaluation of anorectal malformations with clinical correlation. Pediatr Radiol. 1993;23(8):583-6. [CrossRef]
- Morandi A, Borzani I, Macchini F, et al. Correlation between magnetic resonance imaging findings after posterior sagittal anorectoplasty for anorectal malformations and the clinical outcome: Preliminary report. J Pediatr Surg. 2016 Nov;51(11):1859-1863. [CrossRef]
- Caruso AM, Catalano P, Li Voti G, et al. Prognostic evaluation of biofeedback response in patients treated for anorectal malformation. J Pediatr Surg. 2015 Oct;50(10):1648-52. [CrossRef]
- Cheeney G, Remes-Troche JM, Attaluri A, Rao SS. Investigation of anal motor characteristics of the sensorimotor response (SMR) using 3-D anorectal pressure topography. Am J Physiol Gastrointest Liver Physiol. 2011;300(2):G236-G240.
- Liu, J. et al. Functional correlates of anal canal anatomy: puborectalis muscle and anal canal pressure. Am. J. Gastroenterol. 101, 1092–7 (2006).
- Li, Y. , Yang, X., Xu, C., Zhang, Y. & Zhang, X. Normal values and pressure morphology for three-dimensional high-resolution anorectal manometry of asymptomatic adults: a study in 110 subjects. Int. J. Colorectal Dis. 28, 1161–68 (2013).
- Padda BS, Jung SA, Pretorius D, Nager CW, Den-Boer D, Mittal RK. Effects of pelvic floor muscle contraction on anal canal pressure. Am J Physiol Gastrointest Liver Physiol. 2007;292(2):G565-G571.
- Raizada V, Mittal RK. Pelvic floor anatomy and applied physiology. Gastroenterol Clin North Am. 2008;37(3):493-509, vii.
- Liu J, Guaderrama N, Nager CW, Pretorius DH, Master S, Mittal RK. Functional correlates of anal canal anatomy: puborectalis muscle and anal canal pressure. Am J Gastroenterol. 2006;101(5):1092-1097.
- Ambartsumyan L, Shaffer M, Carlin K, et al. Comparison of longitudinal and radial characteristics of intra-anal pressures using 3D high-definition anorectal manometry between children with anoretal malformations and functional constipation. Neurogastroenterol Motil. 2021 Feb;33(2):e13971. [CrossRef]
- Makosiej R, Makosiej A, Bossowski A, et al. Dyssynergic Defecation and Anal Sphincter Disorders in Children in High-Resolution Anorectal Manometry Investigation. J Pediatr Gastroenterol Nutr. 2020 Oct;71(4):484-490. [CrossRef]
- Bjørsum-Meyer T, Christensen P, Baatrup G, et al. Dyssynergic patterns of defecation in constipated adolescents and young adults with anorectal malformations. Sci Rep. 2020 Nov 12;10(1):19673. [CrossRef]
- Gupta CR, Bhoy T, Mohta A, et al. Comparison of clinical outcome and anal manometry following laparoscopic-assisted anorectoplasty and posterior sagittal anorectoplasty in patients with high and intermediate anorectal malformation: A randomised controlled trial. Afr J Paediatr Surg. 2022 Jul-Sep;19(3):160-163. [CrossRef]
- Pathak M, Saxena AK. Postoperative "complications" following laparoscopic-assisted anorectoplasty: A systematic review. Pediatr Surg Int. 2020 Nov;36(11):1299-1307. [CrossRef]
- K.J. Baxter, J.M. K.J. Baxter, J.M. Garza, M.D. Rollins, et al., Multi-institutional review of bowel management strategies in children with anorectal malformations, Journal of Pediatric Surgery (2020), doi.org/10.1016/j.jpedsurg.2020.04.023on Day Month Year).
Figure 1.
(A) Correlation between EO score and response to Bowel management. (0: Poor; 1: discrete; 2: excellent). EO: extern anatomic objective score. (B) Correlation between HRM score and response to Bowel management. (0: Poor; 1: discrete; 2: excellent).
Figure 1.
(A) Correlation between EO score and response to Bowel management. (0: Poor; 1: discrete; 2: excellent). EO: extern anatomic objective score. (B) Correlation between HRM score and response to Bowel management. (0: Poor; 1: discrete; 2: excellent).
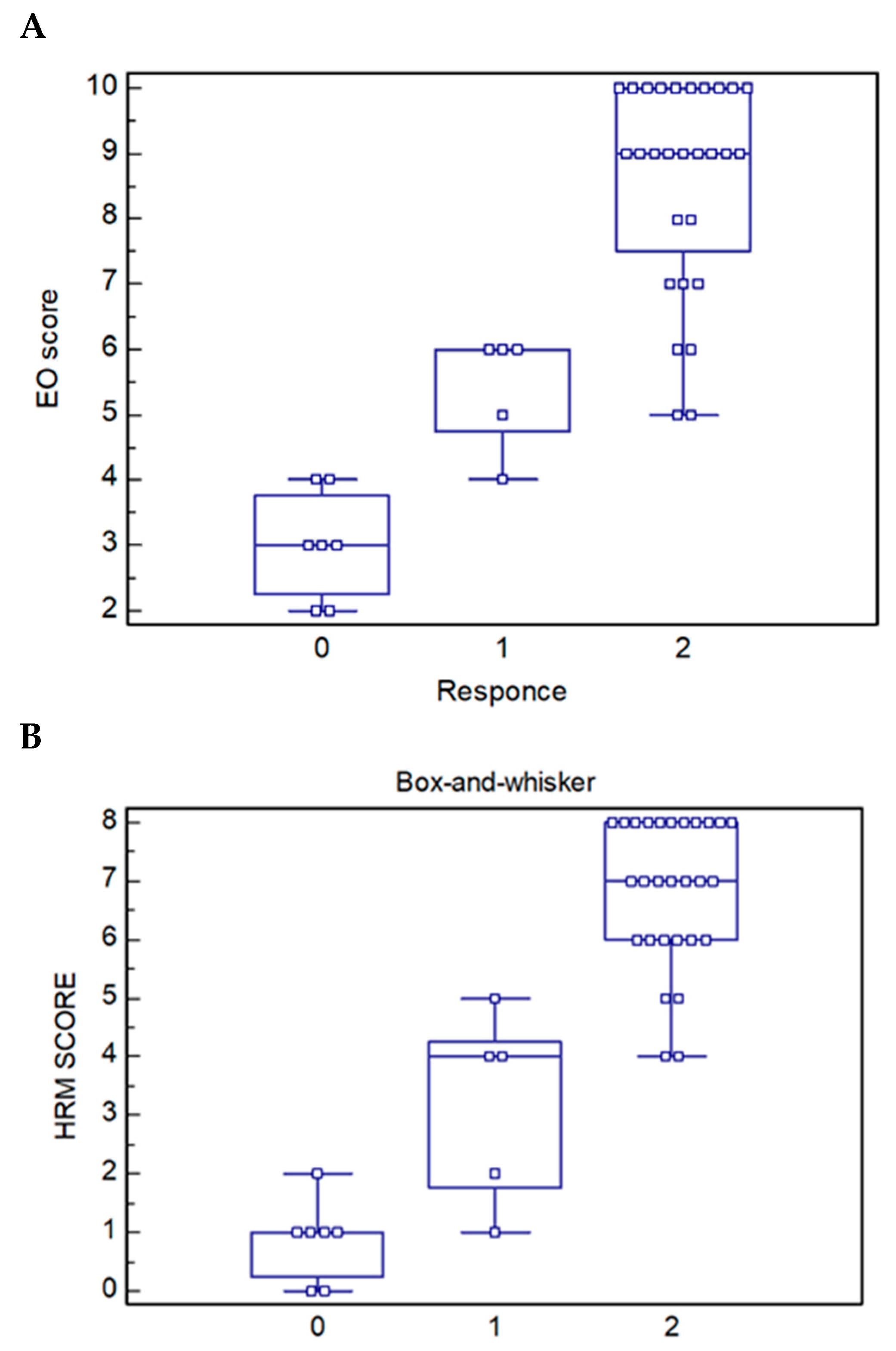
Figure 2.
Caption. 3D High Resolution Anorectal manometry (3d HRAM) in patients without (A) and with (B) sphincter anomalies. The image shows the 3D reconstruction of the anal canal at rest and after squeeze (images below). A: patient with low Anorectal Malformation: sphincter with good pressure values and symmetry; the pressure increment after squeeze is good for amplitude and symmetry. B: patient with high Anorectal Malformation: severe anal hypotonus and asymmetry with lower pressure in anterior, right and left segments at rest; during squeeze the pressure is higher but not present in all segments.
Figure 2.
Caption. 3D High Resolution Anorectal manometry (3d HRAM) in patients without (A) and with (B) sphincter anomalies. The image shows the 3D reconstruction of the anal canal at rest and after squeeze (images below). A: patient with low Anorectal Malformation: sphincter with good pressure values and symmetry; the pressure increment after squeeze is good for amplitude and symmetry. B: patient with high Anorectal Malformation: severe anal hypotonus and asymmetry with lower pressure in anterior, right and left segments at rest; during squeeze the pressure is higher but not present in all segments.
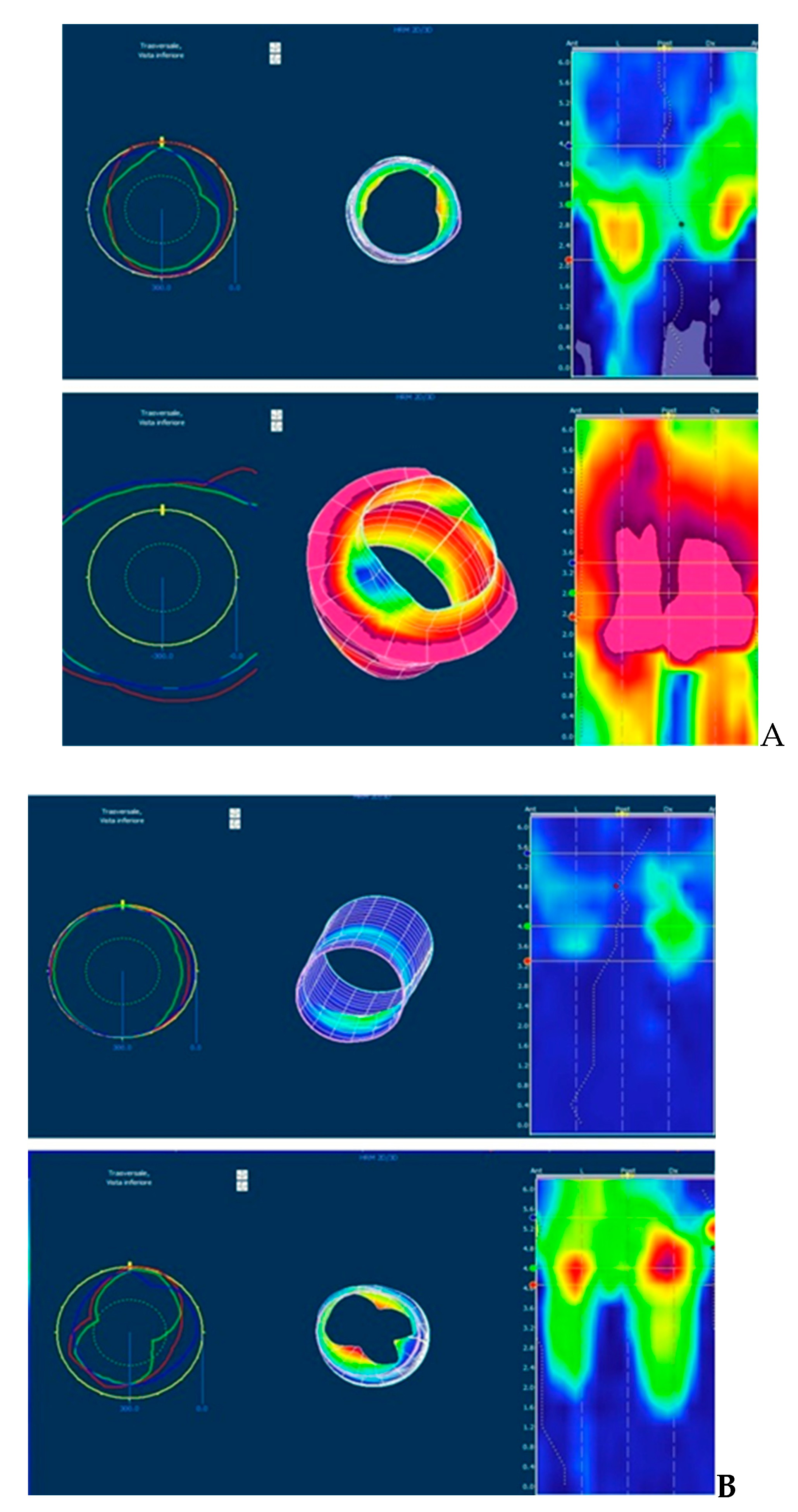

Table 1.
Anatomic perineal score after surgery: score 0 and score 1 were associated with a bad and good perineal aspect respectively.
Table 1.
Anatomic perineal score after surgery: score 0 and score 1 were associated with a bad and good perineal aspect respectively.
| Anatomic parameter | Score 0 | Score 1 |
| Perineal and buttock trophism | poor | good |
| Anal folds | ipoplasic | normal |
| Scrotum/fornix- anus distance | normal | short or long |
| Lateral deviation of neoanus | present | absent |
| Mucosal anal prolaps | present | absent |
| Perineal scar | good | ugly |
| Perianal lesions | present | absent |
| Sacral anomalies | present | absent |
| Intergluteal line | dysmorphic | normal |
| Dyscromic or fluff presacral | Present | absent |
Table 2.
High Resolution manometric score: score 0 and score 1 were associated with a bad and good sphincter function respectively. HRM: High Resolution Manometry; HPZ: high pressure zone; ARP: anal resting pressure; ASP: anal squeeze pressure (reported as increment of ARP); MVC: maximal voluntary contraction; sec: seconds; RAIR: recto anal inhibitory reflex.
Table 2.
High Resolution manometric score: score 0 and score 1 were associated with a bad and good sphincter function respectively. HRM: High Resolution Manometry; HPZ: high pressure zone; ARP: anal resting pressure; ASP: anal squeeze pressure (reported as increment of ARP); MVC: maximal voluntary contraction; sec: seconds; RAIR: recto anal inhibitory reflex.
| HRM parameter | Score 0 | Score 1 |
| Lenght of HPZ (cm) | < 1.5 |
|
| ARP (mmHg) | < 50 | >50 |
| Sphincter asimmetry (%) |
|
< 20% |
| ASP ( mmHg) | < 40 |
|
| Duration of MVC (sec) | < 10 |
|
| Dyssinergic evacuation | yes | absent |
| Rectal sensitivity/RAIR | Altered/absent | Normal/present |
| 3D spatial image | Uneven cylinder | Uniform cylinder |
Table 3.
Demographic parameters of patients with ARM. Pts: patients; M: males; F: females; ARM : anorectal malformation; tot: total.
Table 3.
Demographic parameters of patients with ARM. Pts: patients; M: males; F: females; ARM : anorectal malformation; tot: total.
| Variable | High ARM | Low ARM | Tot | P | |
| sex | M | 12 | 15 | 27 | 0.738 |
| F | 7 | 6 | 13 | ||
| tot | 19 | 21 | 40 | ||
| Age (years) | 8.8 ± 2.8 | 8.1± 3.1 | 0.47 | ||
| Spinal malformation | 9 | 2 | 11 | 0.012 | |
| Urological malformation | 13 | 3 | 16 | < 0.05 | |
| Other associated anomalies | 3 | 2 | 5 | 0.65 | |
| Colostomy | 13 | 0 | 13 | < 0.05 | |
Table 4.
Description of anatomical, Rintala continence (pre and post bowel management) and manometric scores according the type of ARM and associated anomalies Pts: patients; ARM: anorectal malformation, BM: bowel management, HRM: high resolution manometry.
Table 4.
Description of anatomical, Rintala continence (pre and post bowel management) and manometric scores according the type of ARM and associated anomalies Pts: patients; ARM: anorectal malformation, BM: bowel management, HRM: high resolution manometry.
| High ARM | Low ARM |
ARM with Uro Vs ARM without Uro |
ARM with spinal Vs ARM without spinal |
p | |
| Parameter | |||||
| Anatomical score (mean) | 5.05±2.0 | 9.1± 1.1 | 5.5 ± 2.4 8.3 ± 2.1 p .00 |
3.8 ± 1.4 8.4 ± 1.6 p .00 |
<0.05 |
| Pre BM Rintala score | 5.7 ± 4.8 | 15.9± 2.6 | 14. 4 ± 5.3 6.6 ± 5.2 p .00 |
3.1 ± 3.2 14.0 ± 4.3 p .00 |
<0.05 |
| HRM score | 3.3 ± 2.4 | 7.1 ± 1.2 | 3.7 ± 2.5 6.3 ± 2.2 p .001 |
1.8 ± 1.5 6.6± 1.5 p .00 |
<0.05 |
| Post BM Rintala score | 12.3 ± 5.1 | 19.1± 1.8 | 13 .1 ± 5.1 17.7 ± 4.1 p .003 |
8.9 ± 3.1 18.5 ± 2.3 p .00 |
<0.05 |
| p | <0.05 | <0.05 | <0.05 | <0.05 |
Table 5.
Correlation between HRM score and response to Bowel Management according type of ARM and associated urological and spinal anomalies. Pts: patients; ARM: anorectal malformation, BM: bowel management, HRM: high resolution manometry; SD : standard deviation.
Table 5.
Correlation between HRM score and response to Bowel Management according type of ARM and associated urological and spinal anomalies. Pts: patients; ARM: anorectal malformation, BM: bowel management, HRM: high resolution manometry; SD : standard deviation.
| Type of ARM |
HRM score Mean (SD) |
Response to BM | p | ||
| poor | sufficient | excellent | |||
| High ARM | 19 PTS 3.32 (2.4) |
7 PTS 0.86(0.69) |
3 PTS 2.67(2.08) |
9 PTS 5.44(1.01) |
<0.0005 |
| Low ARM | 21 PTS 7.14(1.23) |
0 PTS | 2 4.0(0.0) |
19 PTS 7.47(0.70) |
<0.0005 |
| ARM with urological malformation | 16 PTS 3.75(2.59) |
5 PTS 0.60(0.55) |
3 PTS 3.67(1.52) |
8 PTS 5.75(1.39) |
<0.0005 |
| ARM with spinal malformation | 11 PTS 1.82(1.53) |
7 PTS 0.86(0.69) |
3 PTS 3.33(1.15) |
1 PTS 4.0(0.0) |
0.003 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



