
Submitted:
10 April 2023
Posted:
11 April 2023
You are already at the latest version
Abstract
Abstract: Five patients with standard medical treatment-resistant symptoms of skin lesions, ear infections, allergic rhinitis, nasal congestion, asthma, heartburn, and failure to thrive were success- fully treated with an integrative medicine assessment and integrative medicine treatment approach. The integrative medicine assessment method of autonomic response testing enabled the identifica- tion of nickel sensitivity as a common element in these patients. It guided the use of the integrative medicine therapies of low dose immunotherapy, gamma linoleic acid supplementation, chelation, dietary nickel restriction, and removal of nickel containing dental and cosmetic appliances. A chart review of 151 patients indicated a strong association of nickel and the simultaneous presence of skin lesions.
Keywords:
allergies
; nickel
; eczema
; atopy
; asthma
; otitis media
Introduction
Nickel and other metal allergies are problematic internationally[1-5]. In the United States, there has seen an increase in the number of nickel allergy cases appearing in the peer reviewed literature. It is estimated that 15-20% of the Western population is allergic to at least one metal[1].
The most common form of allergic reaction to nickel is allergic contact dermatitis (ACD)[6,7]. However, nickel allergy can manifest without direct contact to the skin. Included in these non-skin contact manifestations are asthma, allergic rhinitis, eczema, hand dermatitis, gastrointestinal, and neurological symptoms. These non-skin contact manifestations have been referred to as systemic contact dermatitis (SCD)[6,8]. SCD caused by nickel is Systemic Nickel Allergy Syndrome (SNAS) which we consider a major factor in atopy. Sources of nickel exposure include dental materials, dietary intake, and jewelry[2,7-15]. In a case series of 20 patients with allergic rhinitis, 11 of whom also had asthma, Brera reported improvement in nasal and bronchial symptoms with a low nickel diet[16]. Pigatto described the removal of nickel dental sources which resulted in resolution of SCD within 12 months[15]. Atsushi reported a case of successful resolution of eczema of the palm of the hand after removing dental crowns and replacing them with crowns composed of material non-allergenic to the patient[17].
Here we extend our previous single case study of refractory SNAS related to a dental crown containing nickel which was approached with the integrative medicine assessment method of autonomic response testing (ART) and integrative medicine treatments[18]. We describe four additional refractory cases and a chart review of 151 patients who were seen at the Chung Institute of Integrative Medicine (CIIM) in Moorestown, NJ. The chart review focused on the association of nickel sensitivity and the simultaneous presence of skin lesions. Most patients at CIIM have failed standard medical care and many have failed other integrative medical care. Mothers of the four underage patients in the case series gave informed consent. Informed consent was given by the fifth case subject who is now eighteen.
Integrative Medicine Assessment and Treatment Methods
The following are descriptions of the integrative medicine assessment method and the most pertinent integrative medicine treatments discussed in this article.
Autonomic Response Testing (ART)
ART is one of the versions of applied kinesiology. Applied kinesiology was originated by George Goodheart, Jr., DC[19]. Other versions of applied kinesiology have been developed with the conviction that the newer versions are more accurate. A number of integrative medicine practitioners use some version of applied kinesiology to identify disease factors and possible therapeutic agents. Applied kinesiology expands on manual muscle testing assessment by introducing a stimulus such as a food, toxin, allergen, etc. The two assessments are compared, determining whether the response to the stimulus yielded strengthening, weakening, or no change in muscle function. This change in muscle function is used as a predictive assessment of positive, negative, or neutral responses to the stimulus, respectively.
The herein discussed version named ART was developed by Dietrich Klinghardt MD, PhD and Louisa Williams DC, ND. Dr. Klinghardt provides training programs on ART throughout the year[20-22]. It is noted that different versions of applied kinesiology may give conflicting results. Thus far, there is only one peer reviewed evaluation of ART. We published a pilot study (14 patients) on the validity of ART for predicting the results of an Immunoglobulin E blood test for allergy identification[23]. Our results were positive sensitivity, specificity, positive predictive value, negative predictive value, overall accuracy, phi coefficient, and Cohen’s kappa were all in the anticipated direction. All the preceding measures were of useful or strong strength.
ART therapeutics draws on all available therapeutics including those from Chinese medicine, Ayurvedic medicine, homeopathy, osteopathic medicine, allopathic medicine, chiropractic medicine, dentistry, etc. ART helps to guide the choice of interventions. This guidance has resulted in positive clinical outcomes in patients who have failed standard medical therapy. The crux of ART is the assessment procedure, which is twofold. ART informs the identification of contributing factors to the ailment and the choice of intervention.
ART has been extremely helpful at the CIIM for helping patients who have failed standard medical assessment and treatment[24-28].
Low Dose Immunotherapy (LDI)
Low Dose Immunotherapy (LDI) uses extreme dilutions, similar to homeopathic dilutions of antigens, that cause the allergic response in order to help desensitize the immune system. Low Dose Immunotherapy (LDI), developed by Ty Vincent[29,30], evolved from Low Dose Antigen Immunotherapy (LDA) developed by William Schrader M.D. [31,32] and is based on enzyme potentiated desensitization (EPD) which was developed by McEwan[31]. LDI treatments can be delivered to a patient sublingually to build immune tolerance to antigens. It is believed extreme low doses of a given antigens will stimulate the production of T regulator cells which are responsible for suppressing “allergic” reactions which can often progress to pathologic autoimmunity[30]. Dr. Vincent has expanded this concept to include mixtures for chemicals and environmental irritants as well as pathogens thought to play a pivotal role in the development of autoimmunity. We have found LDI especially useful in our practice for airborne allergens and food sensitivities as well as skin lesions, nickel sensitivity, and almost any other inflammatory trigger. Our practice has modified the described methods by tailoring the base concentrations of the immune mixtures to the individual patient. This is accomplished by using ART to test different dilutions resulting in the administration of greater dilutions and more frequent dosing intervals. We have experienced excellent results using these modifications and rarely observe exacerbations of patient symptoms which is a stronger possibility when the more concentrated base mixtures are used.
Low Nickel Diet
Perez et.al. described the resolution of eczema with elimination of high nickel containing foods.[33] We are finding most individuals with ATOPY not only have contact sensitivity but have sensitivity to ingesting nickel from foods with high nickel content, nickel from water stored in stainless steel bottles, and metal dental appliances. Our clinical experience is in concordance with Perez et. al. who reported successful treatment of eczema with a low nickel diet. In addition, the dietary effects extend to other atopic symptoms such as chronic nasopharyngeal and airway inflammation. When nickel containing foods are ingested, we believe it can greatly increase the inflammation in not only the skin but in the mucosal lining of the upper and lower respiratory tract; eye mucosal membrane; and the gut.
Nickel is found in a large quantity of foods making a low nickel diet challenging. We instruct our patients to avoid all foods known for high nickel content. This includes tea, coffee, cocoa, chocolate, soybeans, oatmeal, nuts, almonds, fresh and dried legumes. Most animal products have lower nickel content except for some fish (tuna, salmon, mackerel, herring) which should be avoided. Green leafy vegetables should be used sparingly but most other vegetables can be consumed. We encourage avoiding canned food items and the use of stainless steel for cooking acidic foods as the metal may increase the nickel content of food[34].
Supplementation with gamma linolenic acid (GLA)
Little is communicated about omega-6’s because most American diets contain plenty of omega-6’s in the form of linoleic acid. The average person is able to convert this fatty acid in the body into another important fatty acid called gamma linolenic acid using the delta-6-desaturase enzyme. Atopic individuals are thought to have either a deficiency or an ineffective delta-6-desaturase enzyme. Gamma linolenic acid (GLA) is eventually converted to Prostaglandin E-1 (PGE-1) which is an important anti-inflammatory messenger molecule. Reduced PGE-1 results in greater inflammation in the respiratory lining, skin, and nerves[35].
Supplementing with GLA can bypass this enzymatic defect in conversion or GLA deficiency. GLA then can be converted into PGE-1[35].
GLA can be found in three supplements: borage seed oil, evening primrose oil, and black currant seed oil. Our patients use either borage seed oil or evening primrose oil.
EDTA
The oral chelating agent, LipoPhos® EDTA manufactured by Allergy Research Group, 2300 North Loop Road, Alameda CA is used to reduce the nickel burden. EDTA (ethylenediaminetetraacetic acid) is a synthetic amino acid used to remove heavy metals from the body. It is usually given via intravenous infusion. The phospholipid blend LipoPhos® EDTA is orally administered without gastrointestinal symptoms. [36].
Case Reports
Case 1: 13-year-old female eighth grader with severe refractory eczema. The patient’s eczema was first noticed at age 3 and was managed with topical over-the-counter creams. A flare up the summer before coming to our practice lead to painful, raw, open skin. The itching and pain was severe enough to interfere with sleep. Treatment was sought at urgent care, allergist, dermatologist, and an eczema team at Children’s Hospital of Philadelphia which included an allergist, dermatologist, and hematologist. Treatments included hydrocortisone cream, methylprednisolone, clobetasole ointment, cetirizine cream. Symptoms worsened over the course of treatment. She began having chills, difficulty regulating body temperature, and fatigue. She developed hair loss on her scalp and eyebrows. The patient was unable to attend school the two months prior to our clinic visit due to the severity of symptoms.
The patient was seen at our clinic 16 times over the course of 1 year. She was assessed with autonomic response testing (ART). The ART assessment informed us of the contributing factors to the eczema and their remedies. ART indicated the following contributing factors: nickel, strep A and aluminum. Her treatments included: a low-nickel diet; acupuncture; ionic foot baths; LipoPhos® EDTA; modified Low Dose Immunotherapy (LDI) for nickel, skin, staph/strep combination, general foods, and microbiome; Cilantro; vitamin D3 5000 IU daily; vitamin K2 125 mcg daily; and GLA in the form of Borage oil (240 mg) two capsules daily.
By one month after the initial visit, there was improvement in the rash, sleep and itch symptoms. The patient was able to resume some social activities, comfortably wear clothes and exercise. Six months after the initial visit (10 visits total), she started high school in person. By the 16th visit, her skin was >95% better without use of steroid creams. Her mother noted more social activities and normal functioning.
She had no recurrence for four years, until she had her belly button pierced with a nickel containing piece of jewelry. Her systemic eczema symptoms quickly developed and became severe. Follow up treatment was similar to our original approach along with removal of the metal belly ring. The eczema rash and itch resolved in a three-month period and did not require medication. Since then, the patient reports minor recurrences when she ingests high nickel containing foods.

Case 2: The patient presented in our office at 2 years of age with chronic runny nose and 8 ear infections within a period of 6 months. He was treated with antibiotics for each of the ear infections. These provided only temporary relief. The symptoms returned within 5 days after the last dose of antibiotics.
ART testing revealed sensitivity to nickel and deficiency of GLA. The patient’s mother was given careful instructions on a low nickel diet and borage oil supplementation. Four weeks after the initial visit, the patient’s ears were 100% improved and allergy symptoms were 90% improved with some mild, sporadic nasal congestion. The patient returned to the office for follow up three years after the initial visit for allergy symptoms which were first noticed after one and a half asymptomatic years. At that time, the patient’s mother reported patient had no ear infections after initial visit. At follow up, ART testing revealed an issue with airborne allergies, nickel and the measles, mumps and rubella vaccination (MMR). He was treated with a modified LDI for airborne allergens and MMR; LipoPhos® EDTA; cilantro and Nogier low level laser auricular therapy. The allergy symptoms were 90% improved after that single visit. The patient is now seen in the office annually for checkup and management of mild seasonal allergies. He has had no recurrence of ear infections.
Case 3: Eight-year-old girl presented at our clinic with history of asthma, allergic rhinitis, eczema, and history of multiple ear infections[18]. The eczema rash at times was raw, bleeding, and with extreme itching. The asthma symptoms began approximately four years before the patient presented at our clinic. Her history included ear infections needing tube placement in ears four times and a metal dental cap that preceded asthma symptoms by 4-5 months.
Previous medical care included an allergist, ENT specialist, dentist, and homeopath. Previous treatments included oral steroids, an inhaler, topical steroid creams, homeopathic drops, and tube placement in ears on four occasions.
She was seen at our clinic four times in her first year as a patient. ART was used at each visit and revealed the following issues: nickel, dental cap, parasites, and airborne allergies. Treatments included Nogier low level laser auricular therapy, albendazole, tinidazole, GLA in the form of borage oil, and vitamin D with K2. The patient’s mother was carefully instructed on a low nickel diet. The metal dental cap (which contained a small amount of nickel) was removed after the first visit. This resulted in a cessation of wheezing and eczema within three weeks.
The patient had infrequent follow-ups for minor conditions over the next three years. She then returned after an exercise induced asthma flare. ART was used at each visit and revealed issues with airborne allergies and nickel. She was treated with modified LDI for airborne allergies, LipoPhos® EDTA, GLA in the form of borage oil, and body acupuncture. She has had infrequent follow-up visits over the past four years for minor complaints and has had no asthma recurrence over the past four years.
Case 4: Nine-week-old boy who developed reflux, constipation and irritability at 2-3 weeks of age. He stopped eating and lost weight. His pediatrician diagnosed him with a milk protein allergy. The pediatrician treated him with famotidine and a formula change to the amino acid formula Elecare™ with no relief of symptoms.
ART testing was performed at each visit and indicated an abnormal response to the following: nickel, cow’s milk, baby formula Similac® Alimentum, yeast and aluminum. The patient was treated with modified LDI for baby formula. His reflux, constipation and irritability symptoms improved 75% after first visit and 100% after three visits (two and a half months from first visit). He returned for follow up three and a half years after the initial visit with nasal congestion. ART testing indicated an abnormal response to nickel, and airborne allergies. He was treated with modified LDI for airborne allergens, Nogier low level laser auricular therapy, vitamin D, and LipoPhos® EDTA. Allergy symptoms improved after treatment. Patient visits office annually for treatment of mild allergy symptoms
Case 5: Thirteen-year-old boy with a two-year history of dry, scaly rash on his face and chronic heartburn. Previous medical care included primary care physician, orthodontist for braces, dermatologist, and allergist. The patient had allergy testing. Prior treatments included citirizine, clocortolone and crisaborole.
ART testing, performed at each visit, indicated issues with nickel, dental braces, H. Pylori, and GLA. Treatments included GLA, LipoPhos® EDTA, low nickel diet, body acupuncture and modified LDI for nickel and H. Pylori. Heartburn was 100% improved after his initial visit, the rash was 75% improved with braces in place. When the braces were removed, the rash and itch temporarily worsened. The rash was 100% improved 14 months after the initial visit, two months after braces were removed.
Clinical Practice Survey of association of nickel sensitivity with presence of skin lesions
We examined all records in our recently installed electronic records system for patients who were ART tested for nickel and the simultaneous presence of a skin lesion (excluding contact dermatitis) on the same day. We then populated a 2X2 table with nickel test results and skin lesion presence. The total number of patients was 151. The proportion of nickel positive patients who had skin lesions was 36 percent while the proportion of nickel negative patients was 0.8 percent. The difference was statistically significant (p< 0.0001). See Figure 1.
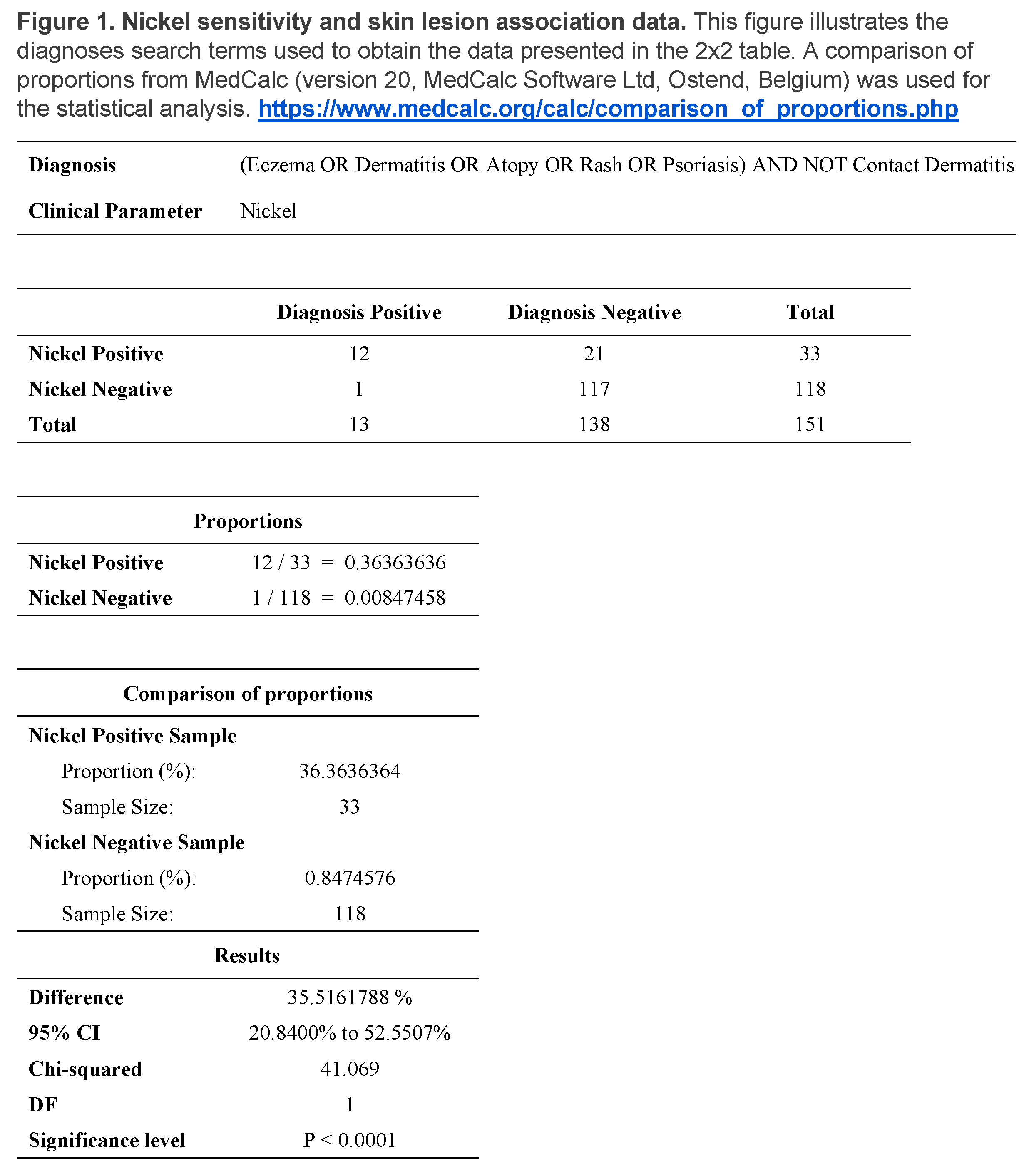
These results support our clinical observations of nickel often being a contributing factor to the presence of skin lesions other than direct contact dermatitis and are in line with other studies showing a relationship of nickel to skin lesions[3-5].
Discussion
Five patients with standard medical treatment-resistant symptoms of skin lesions, ear infections, allergic rhinitis, nasal congestion, asthma, heartburn, and failure to thrive were successfully treated with an integrative medicine assessment and integrative medicine treatment approach. ART allowed the identification of nickel sensitivity and guided the use of the integrative medicine therapies of LDI, GLA, chelation, dietary nickel restriction, and removal of nickel containing dental and cosmetic appliances. Nickel was a factor in those instances of recurrent symptoms after original symptom resolution. The most dramatic example was Case 1 in which a belly button piercing of a nickel containing piece of jewelry resulted in recurrence of systemic eczema. A chart review of 151 patients indicated a strong association of nickel and the simultaneous presence of skin lesions.
We feel that SNAS was the underlying factor in our patients’ chronic treatment-resistant illnesses. Since many of our patients had atopic symptoms, we also feel SNAS along with genetics underlies atopy.
This report is a retrospective case series report and chart review survey thus occupying a place at the bottom of the evidence hierarchy. The patients received multiple forms of treatment. Thus, multiple confounders are present. It is not possible to state with certainty which treatment component had the biggest effect. Future rigorous research is required to determine the dominant factor, factors or combination of factors regarding disease manifestation and treatment. The purpose of this report is to stimulate: 1. consideration of nickel as a possible factor in chronic disease and 2. further evaluation of ART and the integrative medical treatments: LDI, GLA, chelation, dietary nickel restriction, and removal of nickel containing materials from the body in the management of nickel related chronic medical conditions. We welcome collaboration with others.
Conclusion
The integrative medicine assessment method of ART and the integrative treatment methods of LDI, GLA supplementation, chelation, dietary nickel restriction, and removal of nickel containing materials from the body in nickel related chronic disease deserve attention from the research community.
Author Contributions
Conceptualization, M.K.C. & P.J.L.; methodology, P.J.L. & T.C.; formal analysis, P.J.L. & T.C.; writing—original draft preparation, P.J.L.& B. B.; writing—review and editing, M.K.C., B.B., T.C. and P.J.L.; supervision, M.K.C. & P.J.L. All authors have read and agreed to the published version of the manuscript.
Funding
The Won Sook Chung Foundation of Moorestown, NJ organized and supported this project.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Informed consents were obtained for all subjects involved in the case series.
Data Availability Statement
Data sets generated can be requested from the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Schmidt, M.; Goebeler, M. Immunology of metal allergies. J Dtsch Dermatol Ges 2015, 13, 653–660. [Google Scholar] [CrossRef]
- Jacob, S.E.; Goldenberg, A.; Pelletier, J.L.; Fonacier, L.S.; Usatine, R.; Silverberg, N. Nickel Allergy and Our Children's Health: A Review of Indexed Cases and a View of Future Prevention. Pediatric dermatology 2015, 32, 779–785. [Google Scholar] [CrossRef]
- Mukovozov, I.M.; Kashetsky, N.; de Gannes, G. Prevalence of Contact Allergy to Nickel: A Retrospective Chart Review. Dermatitis 2022, 33, 355–361. [Google Scholar] [CrossRef]
- Cattani, C.A.S.; Oppermann, K.; Perazzoli, S.; Guarda, N.H.; Baréa, P.; Bonamigo, R.R. Sensitizing agents found in children and adolescents with recalcitrant atopic dermatitis: a cross-sectional study with a pediatric battery. Anais brasileiros de dermatología 2022, 97, 307–314. [Google Scholar] [CrossRef]
- Mahlberg, S.; Scarberry, K.B.; Nedorost, S. Association Between Dyshidrotic Dermatitis and Metal Allergy: An Evaluation of 1,613 Patch Tests. Dermatitis 2022, 33, e37. [Google Scholar] [CrossRef]
- Yoshihisa, Y.; Shimizu, T. Metal Allergy and Systemic Contact Dermatitis: An Overview. Dermatology research and practice 2012, 2012, 749561–749565. [Google Scholar] [CrossRef]
- Hsu, J.W.; Matiz, C.; Jacob, S.E. Nickel Allergy: Localized, Id, and Systemic Manifestations in Children: Nickel Allergy Manifestations. Pediatric dermatology 2011, 28, 276–280. [Google Scholar] [CrossRef]
- Zirwas, M.J.; Molenda, M.A. Dietary nickel as a cause of systemic contact dermatitis. J Clin Aesthet Dermatol 2009, 2, 39–43. [Google Scholar]
- Hosoki, M.; Bando, E.; Asaoka, K.; Takeuchi, H.; Nishigawa, K. Assessment of allergic hypersensitivity to dental materials. Bio-medical materials and engineering 2009, 19, 53–61. [Google Scholar] [CrossRef]
- Jensen, C.S.; Menné, T.; Duus Johansen, J. Systemic contact dermatitis after oral exposure to nickel: a review with a modified meta-analysis. Contact dermatitis 2006, 54, 79–86. [Google Scholar] [CrossRef]
- Hadasik, K.; Bergler-Czop, B.; Miziołek, B.; Salwowska, N.; Skrzypek-Salamon, A. Pruritus ani and perianal eczema as a manifestation of systemic contact dermatitis. Postȩpy dermatologii i alergologii 2017, 34, 174–176. [Google Scholar] [CrossRef]
- Alanko, K.; Kanerva, L.; Jolanki, R.; Kannas, L.; Estlander, T. Oral mucosal diseases investigated by patch testing with a dental screening series. Contact dermatitis 1996, 34, 263–267. [Google Scholar] [CrossRef]
- Muris, J.; Feilzer, A. Micro analysis of metals in dental restorations as part of a diagnostic approach in metal allergies. Neuro endocrinology letters 2007, 27 Suppl 1, 49–52. [Google Scholar]
- Forsell, M.; Marcusson, J.A.; Carlmark, B.; Johansson, O. Analysis of the metal content of in vivo-fixed dental alloys by means of a simple office procedure. Swed Dent J 1997, 21, 161–168. [Google Scholar]
- Pigatto, P.D.; Brambilla, L.; Ferrucci, S.; Zerboni, R.; Somalvico, F.; Guzzi, G. Systemic allergic contact dermatitis associated with allergy to intraoral metals. Dermatol Online J 2014, 20. [Google Scholar] [CrossRef]
- Brera, S.; Nicolini, A. Respiratory manifestations due to nickel. Acta Otorhinolaryngol Ital 2005, 25, 113–115. [Google Scholar]
- Altsushi, M. [A case report of a metal allergy patient whose prosthesis was identified allergenic by non-destructive metal element analysis and a dermatological patch test]. Nihon Hotetsu Shika Gakkai Zasshi 2006, 50, 276–279. [Google Scholar] [CrossRef]
- Chung, M.; Richmond, J.; LaRiccia, P. Successful Integrative Medicine Assessment and Treatment of Chronic Allergic Rhinitis, Asthma and Eczema Related to a Metal Dental Crown: Case Report. Chronicity 2019, 11, 11–16. [Google Scholar]
- Walther, D. Applied Kineseology, Synopsis 2nd Edition, 2nd ed.; Triad of Health Pulishing: Shawnee Mission, KS 66202, 2016. [Google Scholar]
- Klinghardt, D.; Williams, L. Autonomic Response Testing (workshop manual). self-Published: Woodinville, WA, 1996.
- Healing, K.I.-t.H.o. https://klinghardtinstitute.com/. Available online: (accessed on 3/30/23).
- Klinghardt, D; with editing Derksen, A. Klinghardt D; with editing Derksen, A. ART I Autonomic Response Testing (Workshop Manual). 2009.
- Frandsen, A.; McClure, M.; Chung, M.K.; Lariccia, P.J. Autonomic response testing compared with immunoglobulin e allergy panel test results: Preliminary report. Alternative therapies in health and medicine 2018, 24, 10–14. [Google Scholar]
- Couture, D.C.; Chung, M.K.; Shinnick, P.; Curzon, J.; McClure, M.J.; Lariccia, P.J. Integrative Medicine Approach to Pediatric Obsessive-Compulsive Disorder and Anxiety: a Case Report. Global advances in health and medicine 2016, 5, 117–121. [Google Scholar] [CrossRef]
- Brobyn, T.L., P. J. Successful Treatment of Chronic Edema, Recurrent Cellulitis and Leg Pain using Autonomic Response Testing Assessment: Case Report. Journal of the Science of Healing Outcomes 2017, 9, 10. [Google Scholar]
- Chung, M.K.; LaRiccia, P.J. Successful Integrative Medicine Assessment and Treatment of Chronic Pain Associated With Breast Surgery: A Report of 3 Cases. Holist Nurs Pract 2017, 31, 21–29. [Google Scholar] [CrossRef]
- Brobyn, T.L.; Chung, M.K. Clinical Roundup: Selected Treatment Options for Mood Disorders—Part 2 The use of autonomic response testing and the 5 phases paradigm to identify unresolved feelings in patients with mood disorders. Alternative and Complementary Therapies 2015, 21, 182–188. [Google Scholar] [CrossRef]
- Chung, M.; LaRiccia, P. How Do You Deactivate Painful Scars in Your Practice? Medical acupuncture 2016, 28, 162–167. [Google Scholar] [CrossRef]
- Vincent, T. Low Dose Immunotherapy (LDI) for Autoimmune Diseases and Chronic Inflammatory Disorders (providers manual). 2018.
- Global Immunotherapy LLC. Available online: https://globalimmunotherapy.com/ (accessed on 3/30/23).
- Shrader, W.A. Low dose allergen immunotherapy (LDA): the allergy treatment of the future - here now. Townsend letter 2012, 46. [Google Scholar]
- Santa Fe Center for Allergy and Environmental Medicine. Available online: http://drshrader.com/ (accessed on 3/30/23).
- Da Mata Perez, L.; Franca, A.T.; Zimmerman, J.R. Systemic nickel allergy syndrome. The World Allergy Organization journal 2015, 8, A89–A89. [Google Scholar] [CrossRef]
- Sharma, A. Low nickel diet in dermatology. Indian journal of dermatology 2013, 58, 240–240. [Google Scholar] [CrossRef]
- Horrobin, D.F. Fatty acid metabolism in health and disease: the role of Δ-6-desaturase. The American journal of clinical nutrition 1993, 57, 732S–737S. [Google Scholar] [CrossRef]
- Allergy Research Group. Available online: https://www.allergyresearchgroup.com/content/97.pdf (accessed on 2/28/23).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



