
Submitted:
25 March 2023
Posted:
27 March 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Abstract: The overuse of antibiotic prophylaxis during the COVID-19 pandemic would have led to the devel-opment of antibiotic-resistant bacterial strains, thereby increasing the epidemiological burden of antimicrobi-al resistance. The aim of this study was to determine the prevalence and antibiotic resistance pattern of bacte-ria isolated in 02 referral health facilities in Yaoundé before and during the COVID-19 pandemic era. We conducted a retrospective study over a period of 03 years (from 1 January 2019 to 31 December 2021) in the bacteriology units of the Central and General Hospitals of Yaoundé, Cameroon. The review of the services' registers was done to record bacterial isolates (Streptococcus, Staphylococcus, Neisseria meningitidis and Entero-bacteriaceae) as well as their susceptibility to selected, specific and highly potent antibiotics: Cefixime, Azythromycin and Erythromycin. The relationship between each group of resistant bacteria and the antibiotic of interest was determined by simple linear regression; the comparison of the prevalences of before (2019) and during 2 consecutive years of the COVID-19 pandemic onset (2020 and 2021) was done by the Chi2 test of in-dependence. In all, 426 bacterial strains were included. It appeared that the highest number of bacteria iso-lates and lowest rate of bacterial resistance were recorded during the pre-COVID 2019 period in 2019 (160 isolates vs. 58.8% resistance rate). Conversely, lower bacteria stains but greater resistance burden were rec-orded during the pandemic era (2020 and 2021) with the lowest bacteria amount and peak of bacteria re-sistance registered in 2020, the year of COVID-19 onset (120 isolates vs. 70% resistance in 2020 and 146 iso-lates vs.58.9% resistance in 2021). In contrast to almost all others groups of bacteria where the resistance burden was quite constant over years, the Enterobacteriaceae exhibited greater resistance rate during the pandemic period [60%(48/80) in 2019 to 86.9%(60/69) in 2020 and 64.5%(61/95) in 2021)]. Concerning antibiotics, unlike Erythromycin, Azythromycin related resitance increased during the pandemic period and the resistance to Cefixim tends to decrease the year of the pandemic onset (2020) and re-increase one year therafter. A significant association was found between resistant Enterobacteriaceae strains and Cefixime (R= 0.7; P-value= 0.0001) and also, between resistant Staphylococcus strains and Erythromycin (R= 0.8; P-value= 0.0001). It could be that the more frequent use of these antibiotics has increased resistance rate especially in Enterobacteriaceae. Anticromicrobial resistance should be closely monitor during and after COVID pandemic era.
Keywords:
resistant bacteria
; COVID-19 pandemic era
; antibiotics
1. Introduction
From the late 1940s to the 1970s, many antibiotic molecules of natural or synthetic origin were discovered. The dazzling success of the first anti-infective treatments caused the problem of infectious diseases to be considered somewhat hastily as definitively settled. However, the enthusiasm quickly waned with the appearance of the first bacterial resistance to antibiotics [1]. With each new antibiotic introduced into therapy, the bacteria have been able to adapt and resist more or less quickly [2]. Today, bacteria are resistant to all potentially active antibiotics, although antibiotic resistance can be natural or acquired [3]. Natural resistance is expressed by all strains of a species and its genetic support is a mobile genetic element while acquired resistance is present only in certain strains within a given species. This resistance may be due to mutations affecting genes present on the chromosome or to the acquisition of foreign genes [3]. These genes can come from the chromosome of different species or be conveyed by mobile genetic elements that can be transferred from one bacterium to another, we speak of horizontal transmission because it occurs outside of any mechanism of reproduction. This transfer allows rapid diffusion of resistance genes and can sometimes take place between very distant bacteria on the phylogenetic level, or even between Gram-negative bacteria and Gram-positive bacteria [4]. According to epidemiological data, the appearance and increase of bacterial resistance concerns many countries, with variations depending on the type of microorganism and depending on the country. They concern bacterial species with an important role in community infectious diseases [4].
In February 2017, the World Health Organization (WHO) published its first list of priority pathogens resistant to antibiotics, thus requiring the research and development of new molecules [5]. The list in question enumerates the 12 families of bacteria most threatening to human health. This work by WHO is part of its efforts to combat growing antimicrobial resistance around the world [5]. It is a new tool to ensure that research and development meets urgent public health needs. The most critical group includes multi-drug resistant (BMR) bacteria that pose a particular threat in hospitals, or for patients whose care requires the use of devices such as respirators or blood catheters [5]. It includes Acinetobacter producing a carbapenemase, Pseudomonas producing a carbapenemase and various enterobacteriaceae resistant to carbapenems and beta-lactams [5]. They can cause severe, often fatal infections, such as blood infections and pneumonia. The second and third groups on the list (the high and medium priority categories) include other increasingly resistant bacteria causing more common illnesses such as gonorrhea or salmonella food poisoning. In more detail we find in Priority 2 (high): Enterococcus faecium (resistance to vancomycin); Staphylococcus aureus (methicylline resistance, intermediate or complete vancomycin resistance); Helicobacter pylori (resistance to clarithromycin); Campylobacter spp (resistance to fluoroquinolones); Salmonellae (resistance to fluoroquinolones); Neisseria gonorrhoeae, (cephalosporin resistance, fluoroquinolone resistance) [5]. In priority 3 (medium): Streptococcus pneumoniae (insensitive to penicillin); Haemophilus influenzae (ampicillin resistance); Shigella spp. (resistant to fluoroquinolones). These multi-resistant bacteria (BMR) are isolated either during the diagnosis of pathological samples or during screening, which identifies patients colonized by BMR and reduces the frequency of their isolation [5]. The problem is that most of the bacteria that have become resistant or multi-resistant are human commensal bacteria, benefiting from the selection pressure of antibiotics whose frequency of use is high and regular [4]. This dissemination of multi-resistant bacteria concerns bacterial species having an important role in community infectiology such as Streptococcus pneumoniae and in nosocomial infectiology like Staphylococcus aureus, Enterobacteriaceae, Acinetobacter baumanii and Pseudomonas aeruginosa. Bacteria are talked to be multi-resistant to antibiotics (BMR) when, due to the accumulation of acquired resistance to more than 03 families of antibiotics, they are no longer sensitive to more than a small number of antibiotics that can be used therapeutically [4]. The high frequency, the pathogenic potential and the commensal nature expose BMRs to the risk of their dissemination outside the hospital. The clonal and easily transferable nature of the mobile genetic element allows these BMRs to transfer several resistance factors to other bacteria, which will be expressed in this new bacterial host. This is called "co-resistance". BMRs pose a major therapeutic problem in terms of management and prognosis, and therefore in general public health [6].
The COVID-19 pandemic has considerably modified the medical activities within the health structures as well as the behavior of the populations, with regard to the use of probabilistic antibiotic therapy on a recurrent basis [7]. Faced with the epidemic peak of respiratory distress and the adoption of prophylaxis against opportunistic COVID-19 infections, the use of certain antibiotics, in particular Cefixime and Azythromycin, have increased considerably to the point of arriving at a situation of shortage of supply [7]. Antibiotic consumption increased by 19% compared to the previous year over the period March-April 2019 (768 against 644 DDD/1000 DHD) [7]. The most prescribed antibiotics and the most important in consumption during the onset of the pandemic were: Amoxicillin (+7%), Cefixime (+30%), Imipenem (+66%), Azythromycin and Erythromycin (+138% each) [7]. During the occurrence of this pandemic, prescriptions or numerous, prolonged self-medications with an increasingly broad spectrum of antibiotics, even the use of last-line molecules for rescue were significantly increased [7]. Antibiotic prophylaxis administered to palliate opportunistic bacterial infections in patients with suspected COVID-19 infection probably influenced the selection pressure of commensal bacteria in this pandemic context[7]. It therefore sounds really interesting to investigate the resistance of bacteria to antibiotics after the COVID-19 pandemics era. The aim of this study was to determine the prevalence and antibiotic resistance pattern of bacteria isolated in 02 referral health facilities in Yaounde before and during the COVID-19 pandemic era.
2. Results
2.1 Age and sex of the study population
From 2019 to 2021, 426 strains were isolated from patients attending the bacteriology unit (a single bacterial strain per patient) of 02 referral hospitals for COVID-19 including 160 in 2019, 120in 2020 and 146 in 2021.
Among those 426 bacterial strains, we recorded 67 females vs. 93 males in 2019; 51 females vs. 69 males in 2020 and finally 66 females vs. 80 males in 2021. The age range ]25-50]years was predominant during the 3 years (53.1% in 2019, 43,3% in 2020 and 49,3% in 2021) and the mean age of the study population was 54.8±18.9years in 2019, 40.3±15.5 in 2020 and 38±14.6 in 2021. The most common sample was the pus, with 61.9%.
Table I. Age and sex of the study population.

| n | % | |||
| Pre-COVID19 (2019) N=160 |
Sex | Male | 93 | 38.4 |
| female | 67 | 36.4 | ||
| Age | ]0-25] | 30 | 18.7 | |
| ]25-50] | 85 | 53.1 | ||
| 50> | 45 | 28.1 | ||
|
During COVID-19 (2020) N=120 |
Sex | Male | 69 | 28.5 |
| female | 51 | 27.7 | ||
| Age | ]0-25] | 31 | 25.8 | |
| ]25-50] | 52 | 43.3 | ||
| 50> | 37 | 30.8 | ||
|
During COVID-19 (2021) N=146 |
Sex | Male | 80 | 33 |
| female | 66 | 35.9 | ||
| Age | ]0-25] | 37 | 25.3 | |
| ]25-50] | 72 | 49.3 | ||
| 50> | 37 | 25.3 |
2.2. Bacteria profile of the study population
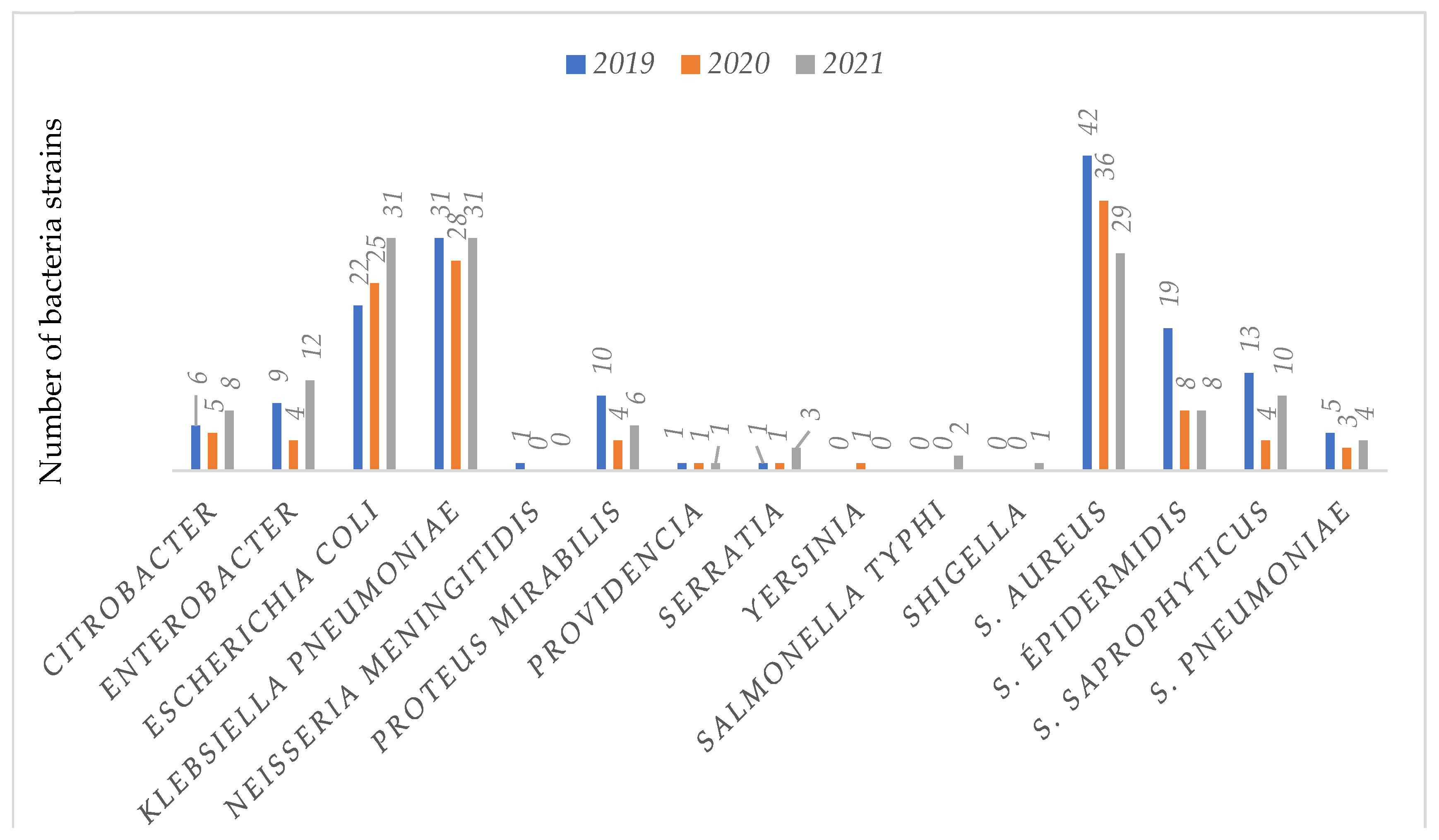
From the Figure 2, we notice that 51.4% (219/426) of bacteria isolates were Enterobacteriaceae; 45% (192/426) of Staphylococcus strains; 3%(13/426) of Streptococcus strains and 0.3%(2/426) of Neisseria meningitidis.
Figure 1.
Number per bacterial species over the 03 years.
2.3. Number of bacteria isolate and their corresponding resistance rate over years
The horizontal bar chart and curves below (Figure 2) show the numbers of bacterial strains and their resistance rate over years.
From these graph (Figure 2), it tends to appear that in 2019, corresponding to the pre-COVID-19 period, the highest number of bacteria isolates and lowest rate of bacterial resitance were recorded (160 isolates vs. 58.8% resistance rate). However, we noticed in contrast lower bacteria isolated during COVID-19 pandemic era but greater resistance burden with the lowest bacteria amount and peak of bacteria resistance registered in 2020, the year of COVID-19 onset (120 isolates vs. 70% resistance in 2020 and 146 isolates vs.58.9% resistance in 2021)
2.4. Resistance pattern of bacterial strains isolated in 2019, 2020 and 2021.
2.4.1. Resistance rate by group of bacteria
The graph below represents the resistance rate by group of bacteria over time
Figure 3 showed that unlike almost all others groups of bacteria where the resistance burden was quite constant over years, the Enterobacteriaceae exhibited greater resistance rate during the pandemic period [60%(48/80) in 2019 vs 86.9%(60/69) in 2020 and 64.2%(61/95) in 2021)]. Furthermore, no resitance to antibiotics has been noted concerning Neisseria meningetidis in 2020 and 2021 [100%(1/1) in 2019 vs 0% of strain in 2020 and 2021)].
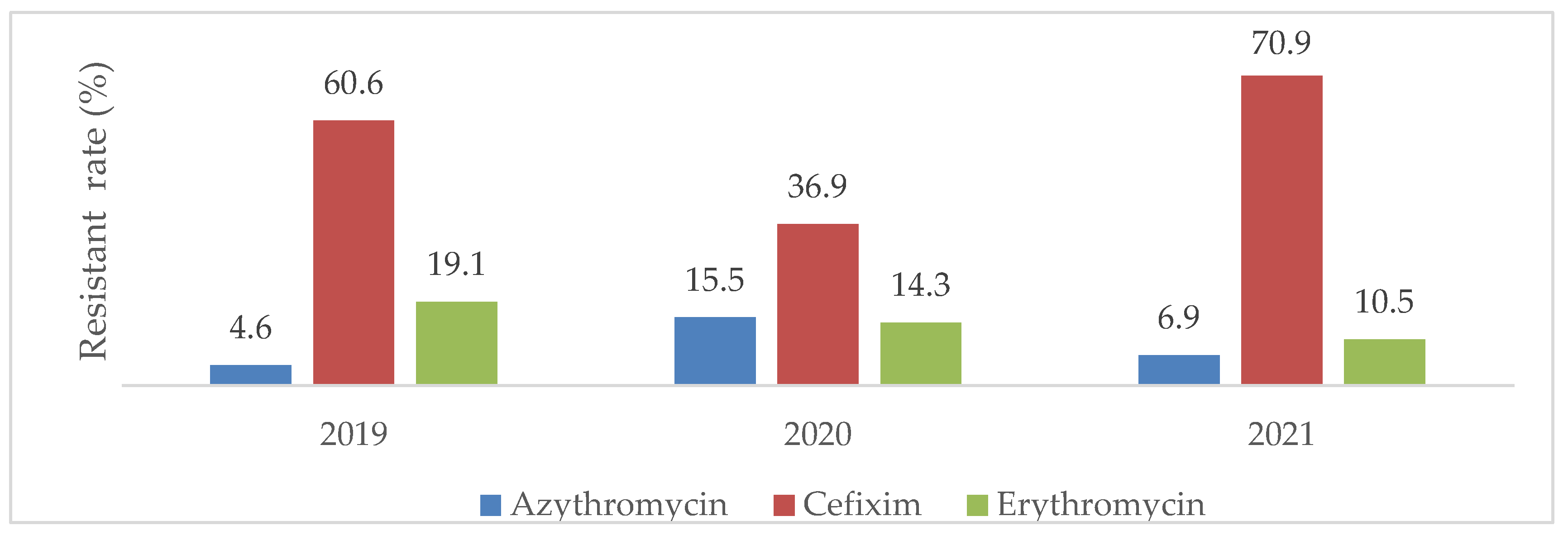
2.4.2. Global resistance rate of bacteria according to the antibiotics of interest.
Cefixime, Azythromycin, Erythromycin were antibiotics of interest for the bacterial strains involved in this study. The Figure 4 shows the global distribution of bacterial resistance to these antibiotics.
This graph highlights that overall bacterial resistance rate to Azythromycin increased during the pandemic period with the highest rate of resistance recorded in 2020 (4.6% resistance rate in 2019, 15.5% in 2020 and 6.9% in 2021) over time. The resistance to Cefixim tends to decrease the year of the pandemic onset (2020) and re-increase one year therafter (60.6% resistance rate in 2019, 36.9% in 2020 and 70.9% in 2021) and concerning Erythromycin, its resistance rate was slightly decreasing over time (19.1% resistance rate in 2019, 14.3% in 2020 and 10.5% in 2021).
2.4.3. Global Resistant rate according to year of isolation
The table below reflects the rate of bacterial resistance with regard to year of isolation (Table II)
Table II. Global resistant rate according to year of isolation.
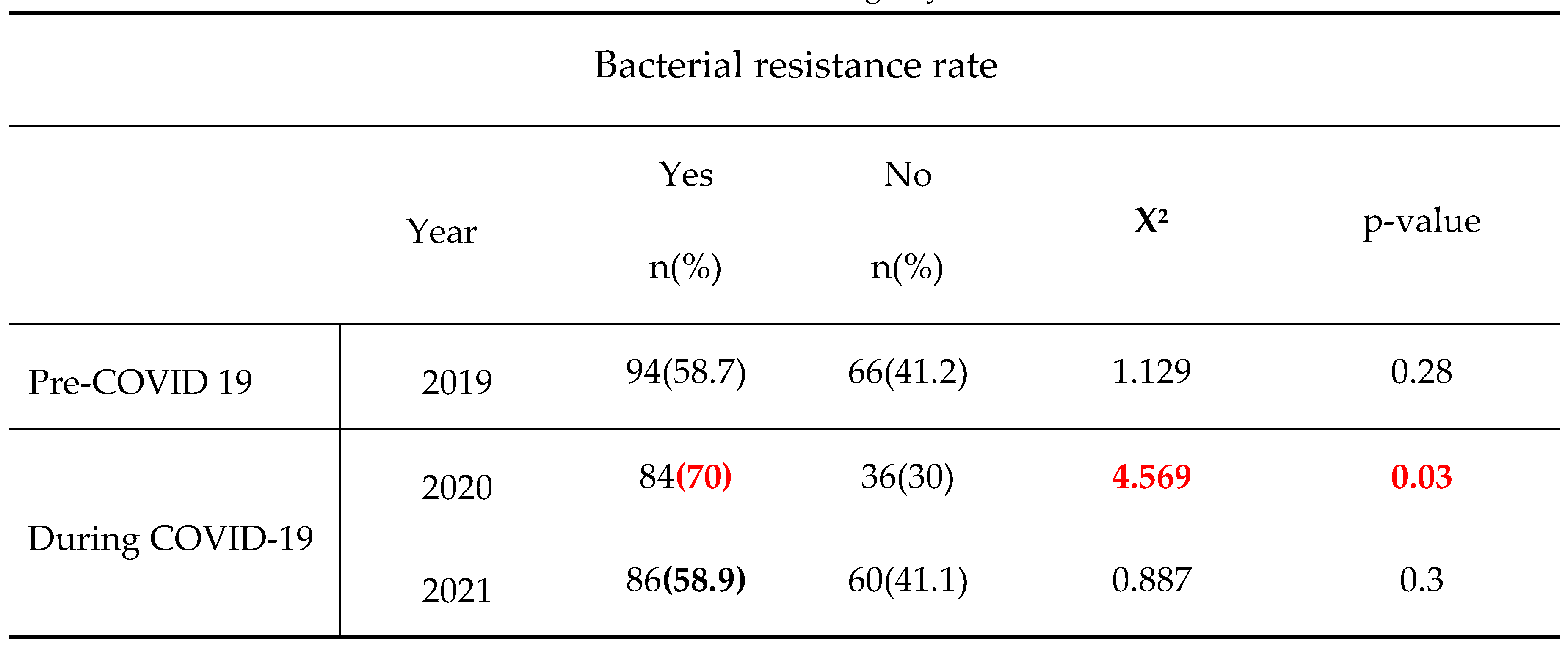
From that table, the overall bacterial resistance rate globally increased in 2020 and 2021 with the highest rate of resistance recorded in 2020, the year of COVID onset (p=0.03).
2.4.4. Sex and bacteria resistant rate
The table below reflects the rate of bacterial resistance according to gender (Table III)
Table III. Bacteria resistant rate according to gender.
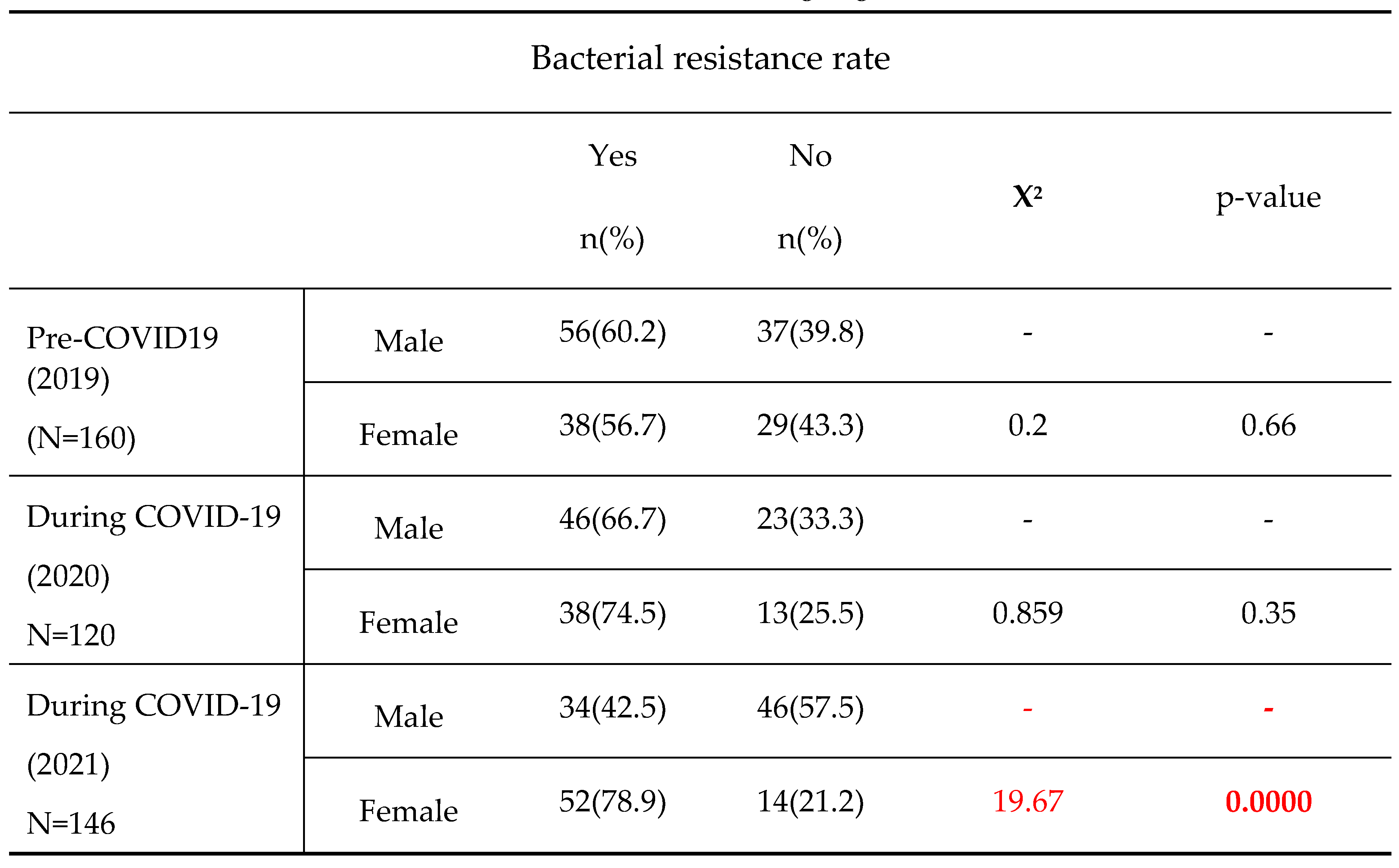
The table reveals an increase bacterial resistance rate in female subjects over years [56.7 in 2019, 74.5% in 2020 and 78.9% in 2021] with a significantly higher bacteria resistance rate in female than males in 2021 (78.9%vs.42.5%, p=0.0000)
2.4.5. Age and global resistance rate
In comparison to subjects aged ]0-25] with decreasing resistance rate over time, the subjects aged ]25-50]and >50 more likely exhibited relatively high resistant bacteria with the peak of resistance recorded in 2020, the year of COVID-19 onset. However, the observed differences were not statistically significant
Table I V. Resistant bacterial strain according to age.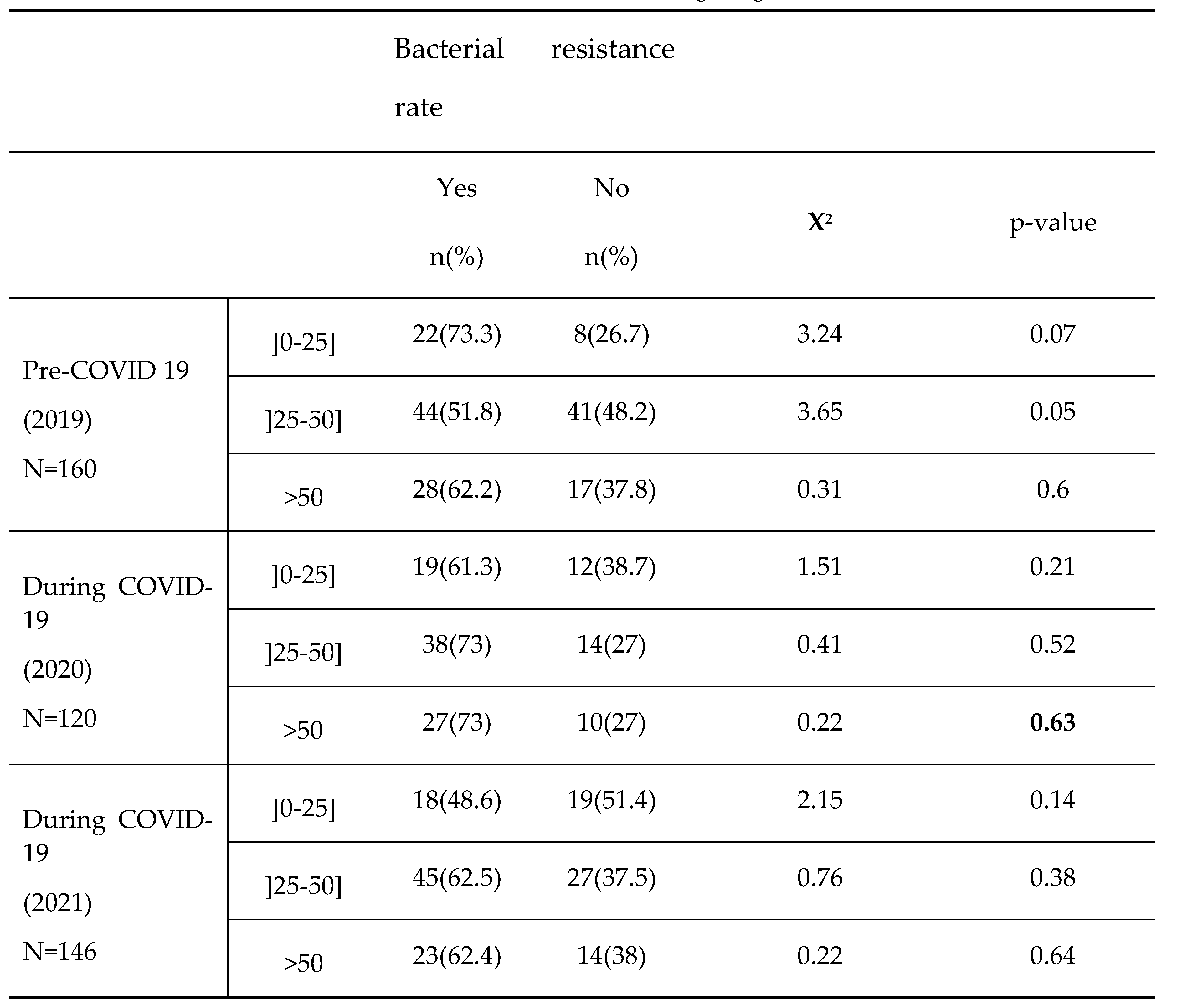
2.5. Repartition of bacterial resistant strains according to selected antibiotics before (2019) and during COVID-19 pandemic (2020 and 2021).
The Table V below highlights relationships between each group of resistant bacteria and the selected antibiotic.
Table V. Relationship between each group of resistant bacteria and the antibiotic best indicated to destroy it.
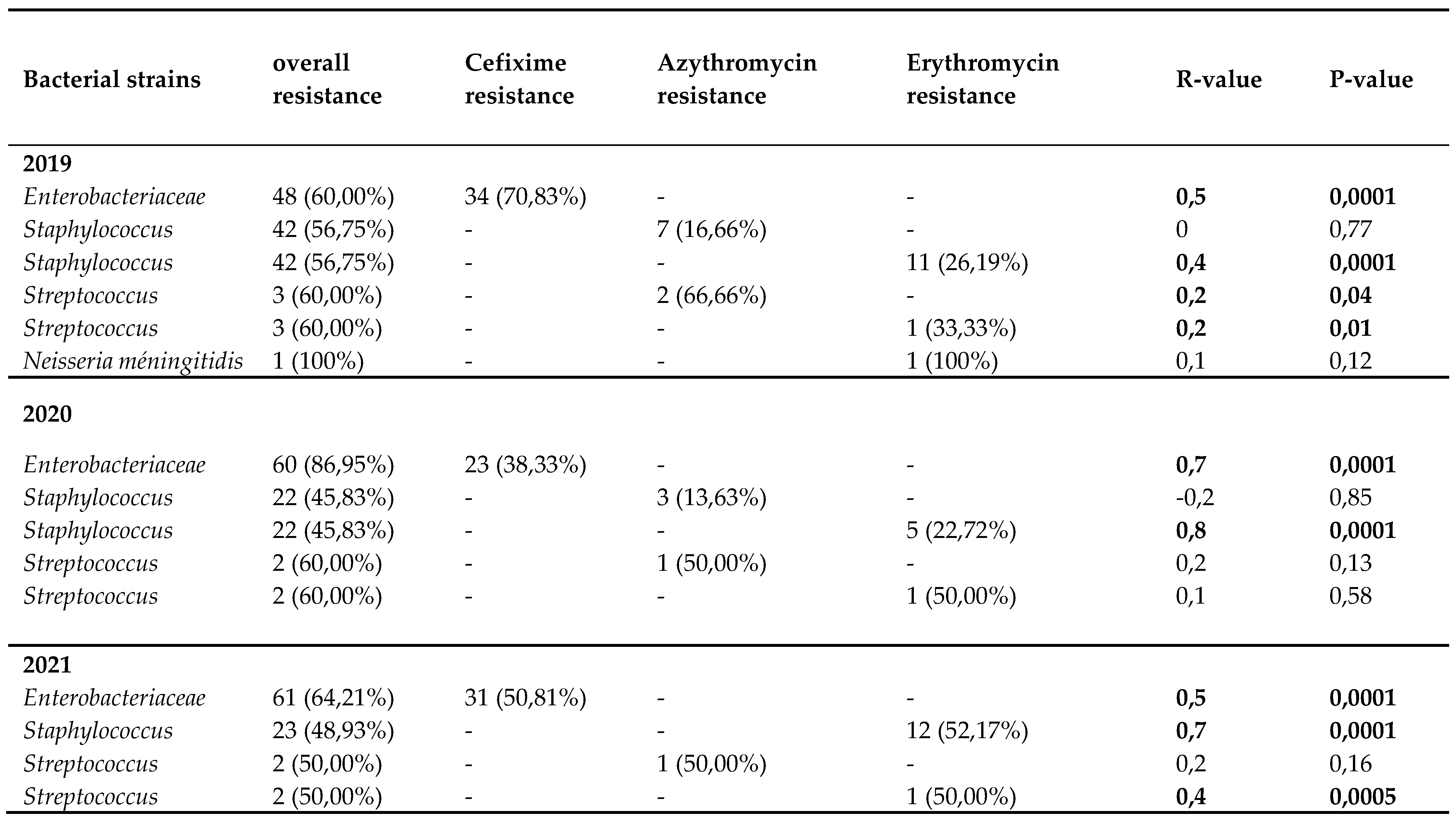
This table reveals that taken individually, resistance of each bacteria isolate to its selected antibiotic tends to slightly decrease the year of the COVI-19 pandemic onset(2020) and then either re-increase or stay constant one year thereafter (2021). We can thus note significantly strong relationships between the bacterial strains that became resistant and some specific antibiotics used over the 3 years, notably, Cefixime and resistant Enterobacteriaceae strain [ (R=0,5; P= 0.0001 in 2019); (R=0.7 ; P=0.0001 in 2020); (R=0.5; P=0.0001 in 2021)]; then between Erythromycin and resistant Staphylococcus[(R=0,4 ; P=0.0001 in 2019); (R=0.8 ; P=0.0001 in 2020); (R=0.7; P=0.0001 in 2021)] and Streptococcus strains [ (R=0,0.2 ; P=0.01 in 2019); (R=0.4; P=0.0005in 2021)]; Similarly, Streptococcus strains that have become resistant are linked to the use of Azythromycin just in 2019(R=0.2; P-value= 0.04).
3. Discussion
In order to determine the prevalence and antibiotic resistance pattern of bacteria isolated in 02 referral health facilities in Yaounde before and during the COVID-19 pandemic era, a retrospective study was conducted in 02 referral health facilities in Yaounde, Cameroon. For that purpose, data were collected from each hospital databases (registries, laboratory books) before (2019) and during the pandemic (2020 and 2021), then, analyzed thereafter.
In all, 426 strains were isolated from patients attending the bacteriology unit (a single bacterial strain per patient) of the 02 referral hospitals for COVID-19 as follow: 37.5% (160/426) in 2019, 28.2% (120/426) in 2020 and 37.27% (146/426) in 2021. These results coincide to those of Chih-Cheng and al in patients of Veterans General Hospital of Taiwan who had also found a decreasing number of Streptococcus pneumonia, Staphylococcus aureus, Enterococcus spp, Escherichia coli and Klebsiella pneumonia from 2019 to 2020 [7]. The high number of strains isolated in the pre-CoVID19 period (2019) constrasting with the lowest amount in the year of COVID onset (in 2020) is logical and could rely on the wide and systematic implementation of COVID-19 barriers measures including hygienic measures, wearing of face mask, social distancing that lead to rapid and overall decline of respiratory tract infections as well as feco-oral transmitted diseases [8] In fact, giving similar routes of transmission, all barriers measures applicable for COVID-19 have the advantage to also block others infections [9] Furthermore, the occurrence of the COVID-19 pandemic led to an overconsumption of antibiotics as well as self-medication, which in turn destroyed the lot of potential pathogenic and commensal bacterial populations [8].
Concerning the bacterial profile, 51.4% (219/426) of the included bacteria isolates were Enterobacteriaceae, 45% (192/426) Staphylococcus strains, 3% (13/426) Streptococcus strains and 0.3% (2/426) of Neisseria meningitides with relatively high rate of resistance over time. Chih-Cheng also found Enterobacteriaceae as the most isolated bacteria 30.8% (49/159) in patients at Veterans General Hospital of Taiwan between 2019 and 2020[8]. Others previous studies worldwide have also reported the predominance of Enterobacteriaceae in clinical samples [11,13,15]. In fact, Enterobacteriaceae are the most incriminated commensal germs in opportunistic infections in general [11,15]. In this study, the main isolated species among Enterobacteriaceae were Klebsiella pneumoniae 41.1% (90/219), E. coli 35.6% (78/219), Enterobacter 11.4% (25/219) and proteus mirabilis 9.13% (20/219), similar trends has been already observed in previous studies [11,15]. In fact, the rapid emergence of bacteria especially resistant bacteria is occurring worldwide, endangering the efficacy of antibiotics, which have transformed medicine and saved millions of lives [16,17,18,19]
In this study, bacterial resistance tends to increase in female’s subjects over years. Moreover, In comparison to subjects aged ]0-25] with decreasing resistance rate over time, the subjects aged ]25-50] and >50 more likely exhibited relatively higher resistance with the peak of resistance recorded in 2020, the year of COVID-19 onset, even though the observed differences were not statistically significant. Previous studies already reported a high prevalence of bacterial resistant strain either with ages [14] and or in female’s subjects [1]. This disproportionate burden of antimicrobial resistance (AMR) on women is due to both demand and supply-side factors. Some demand-side factors which increase women’s vulnerability to AMR are biological factors, women’s nature and type of employment, excessive home-based care work, and limited access to healthcare [20](WHO, 2018). On the supply-side, gender differences in antibiotic prescription by doctors due to lack of training and gender-bias increase women’s antibiotic usage (AMU) [21,22]. In fact, Women are 27% more likely to receive an antibiotic prescription in their lifetime compared to men [23]. Furthermore, the high rate of antimicrobial resistance in subject aged >25 years during the COVID-19 pandemic in this study is not surprising. This aged range corresponds to the most active part of the Cameroonian population who is believed to have taken the highest amount of medications including antibiotics to protect against COVID-19 at work as the pandemic evolved in 2020.
This study also showed that in 2019, corresponding to the pre-COVID-19 period, the highest number of bacteria isolates and lowest rate of bacterial resitance were recorded (160 isolates vs. 58.8% resistance rate). However, we noticed in contrast lower bacteria isolated during COVID-19 pandemic era but greater resistance burden with the lowest bacteria amount and peak of bacteria resistance registered in 2020, the year of COVID-19 onset (120 isolates vs. 70% resistance in 2020 and 146 isolates vs.58.9% resistance in 2021). Multiple studies reported an unexpected high incidence of infections due to methicillin-resistant S. aureus, carbapenem-resistant A. baumannii, carbapenem-resistant Enterobacteriaceae among COVID-19 patients admitted to the intensive care unit [9,15]. Moreover, a metanalysis Of 1331 articles of Ruwandi shows that during the first 18 months of the pandemic, AMR prevalence was high in COVID-19 patients and varied by hospital and geography although there was substantial heterogeneity [10]. According to ruwandi et al, the increase in the prevalence of resistant strains in 2020 could be straightly related to the peak of antibiotic consumption during the COVID-19 pandemic onset, ranging up to 74.7 % from 2019 to 2020 for antibiotics such as Fosfomycin [10]; that generally increased the selection pressure and evolvement of resistance mechanism [10].
In constrat to almost all others groups of bacteria where the resistance burden was quite constant over years, Enterobacteriaceae exhibited greater resistance rate during the pandemic period [60%(48/80) in 2019 vs 86.9%(60/69) in 2020 and 64.2%(61/95) in 2021)]. Furthermore, no resitance to antibiotics has been noted concerning Neisseria meningetidis in 2020 and 2021 [100%(1/1) in 2019 vs 0% of strain in 2020 and 2021)]. A similar study on the impact of SARS-CoV-2 epidemic on antimicrobial resistance shows that, the Gram-negative bacteria were isolated from 78% of patients with predominant Enterobactericaea resistant strains including carbapenemases producers such as K. pneumoniae (92.6%) and A. baumannii (72.8%)[11]. This result is not different from that of Sanofi, which estimates that 30% of Klebsiella pneumoniae strains show resistance to 3rd generation cephalosporins in France, in 2020 [12]. Unlike Neisseria meningetidis, Enterobacteriaceae are widely distributed and have a large host range [24], they can cross-infect and spread between medical staff and patients, and also their genetic materials (such as plasmids or transposons) can be obtained from the outside world, leading to horizontal transmission of drug-resistant genes, which further leads to the wide spread of drug-resistant bacteria [25,26].
The resistance of each bacteria isolate to its selected antibiotic tends to slightly decrease the year of the COVI-19 pandemic onset (2020) before re-increasing or staying constant one year thereafter (2021). A significant association was found between resistant Enterobacteriaceae strains and Cefixime (R= 0.7; P-value= 0.0001) and also, between resistant Staphylococcus strains and Erythromycin (R= 0.8; P-value= 0.0001). Chih-Cheng et al reported in 2020 Taiwan a rapid increase in multidrug-resistant organisms (MDROs), including extended-spectrum β-lactamase (ESBL)-producing Klebsiella pneumoniae, carbapenem-resistant New Delhi metallo-β-lactamase (NDM)-producing Enterobacterales, Acinetobacter baumannii, methicillin-resistant Staphylococcus aureus (MRSA) [7]. Besides, several recent reports have described an increase in multidrug-resistant organisms (MDROs) during the COVID-19 pandemic [27,28,29,30]. The cause of this high resistance is multifactorial and is particularly related to high rates of antimicrobial agent utilization in COVID-19 patients with a relatively low rate of co- or secondary infections [31]. This clearly confirms that anticromicrobial resistance should be continuously closely-monitor during and after COVID pandemic era.
4. Materials and Methods
4.1. Study duration and location
A retrospective cross-sectional and analytical study was conducted at the Central Hospital and the General Hospital of Yaounde from September 2021 to July 2022. Data from registries were collected over a period of 3years from 1 January 2019 to 31 December 2021.
4.2. Sampling method and Sampling population
Our study focused on bacteria Streptococcus, Staphylococcus, Haemophilus influenzae, Neisseria meningitidis and Enterobacteriaceae resistant or not to Cefixime, Azythromycin and Erythromycin; isolated from samples of patients consulting the bacteriology laboratories of the Central and General hospitals of Yaoundé from January 2019 to December 2021, archived in the annual registers where the data is organized by week and month with all the information on the pre-analytical information, analytical and post-analytical. We carried out a census on the basis of already existing data. All the bacteria Streptococcus, Staphylococcus, Haemophilus influenzae, Neisseria meningitidis and Enterobacteriaceae resistant to Cefixime and to Azythromycin and Erythromycin recorded in the results registers of the bacteriology department were sampled. Indeed, the recording of the results in the registers that we questioned was done according to a fairly rigorous protocol, by providing information on the patient sampled, the type of sample taken, the dates of sampling and analysis, the techniques analysis used, the germs identified, the results of the antibiogram for each germ isolated. We therefore extracted the data day after day by questioning the registers to obtain the information that should allow us to meet our objectives.
4.3. Statistical analysis
Data were collected using Kobotolbox software, entered into a Microsoft Excel 2016 database (version 15.13.3) and analyzed using StatView software (version 5.0.0.0) and the simple linear regression statistical test a was used to show the relationships between the antibiotics of interest tested and the resistant bacterial strains isolated and the Chi-Square of independence to compare the carriage prevalences of resistant bacterial strains from 2019 and 2021 to that of the year of the onset of the pandemic to COVID19.
Data such as age, sex, location of patients whose samples were subjected to bacteriological analyzes were presented as a percentage. Also the distribution of the frequency of isolated bacteria, the genus to which they belong, the antibiotics to which the bacteria were resistant were presented in strip diagram and tables. The resistance profile of the strains as well as their relationship with the antibiotics of interest were presented in tables and the resistant strain and antibiotic relationships were established via simple linear regression. We have made an annual presentation of the overall prevalence of carriage of selected resistant bacteria, spread over each of the 03 years, on a vertical band and curve diagram. Statistical comparisons of the variation in the prevalence of the carriage of resistant bacterial strains in 2019 and 2021 with that of the year of the onset of the COVID19 pandemic (2020), were made by the Chi-Square test and presented in tables.
5. Conclusions
It could be that the more frequent use of these antibiotics has increased the resistance rate of bacteria especially Enterobacteriaceae. Thus, Anticromicrobial resistance should be closely monitor during and after COVID pandemic era.
Author Contributions
Conceptualization, Cecile Ingrid Djuikoue, Willy Yamdeu Djonkouh, Rodrigue Kamga Wouambo and Benjamin D. Pokam; Data curation, Cecile Ingrid Djuikoue, Willy Yamdeu Djonkouh, Cavin Epie Bekolo, Paule Dana Djouela Djoulako and Gilder Tonfack Temgoua; Formal analysis, Willy Yamdeu Djonkouh, Cavin Epie Bekolo, Rodrigue Kamga Wouambo and Paule Dana Djouela Djoulako; Investigation, Willy Yamdeu Djonkouh, Rodrigue Kamga Wouambo and Gilder Tonfack Temgoua; Methodology, Cecile Ingrid Djuikoue, Paule Dana Djouela Djoulako and Benjamin D. Pokam; Project administration, Cecile Ingrid Djuikoue, Cavin Epie Bekolo, Benjamin D. Pokam, Nicolas Antoine-Moussiaux and Teke R. Apalata; Resources, Raspail Carrel Founou, Gilder Tonfack Temgoua, Nicolas Antoine-Moussiaux and Teke R. Apalata; Software, Willy Yamdeu Djonkouh, Paule Dana Djouela Djoulako and Gilder Tonfack Temgoua; Supervision, Raspail Carrel Founou and Teke R. Apalata; Validation, Paule Dana Djouela Djoulako and Teke R. Apalata; Visualization, Cecile Ingrid Djuikoue, Willy Yamdeu Djonkouh, Rodrigue Kamga Wouambo, Raspail Carrel Founou and Benjamin D. Pokam; Writing – original draft, Cecile Ingrid Djuikoue, Willy Yamdeu Djonkouh, Rodrigue Kamga Wouambo and Paule Dana Djouela Djoulako; Writing – review & editing, Cecile Ingrid Djuikoue, Willy Yamdeu Djonkouh, Cavin Epie Bekolo, Rodrigue Kamga Wouambo, Raspail Carrel Founou, Paule Dana Djouela Djoulako, Gilder Tonfack Temgoua, Benjamin D. Pokam, Nicolas Antoine-Moussiaux and Teke R. Apalata.
Funding
This research did not receive any specific grant from funding agencies
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by An ethical clearance was obtained on the basis of the evaluation and validation of the research protocol by the Centre Regional Commitee (CE N°02229/CRERSHC/2022), the Institutional Committee for Research on Human Health of the Yaounde General Hospital (Ref N°22322/HGY/DG/DPM/APM-TR), the ethic committee of the Yaounde Central Hospital (N°2022/121/AR/MINSANTE/SG/DHCY/UAF).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the
study. Written informed consent has been obtained from the patient(s) to publish this paper.
Data Availability Statement
All data are available upon request.
Acknowledgments
We gratefully thank all participants to this research.
Conflicts of Interest
The authors declare that the research was conducted in the absence of anycommercial or financial relationships that could be construed as a potential conflict of interest.
References
- Courvalin, P. Courvalin P., Leclerq R. et al.Evolution of bacterial resistance to antibiotics.:. Med Sci 1997, 13, 925 6. [Google Scholar]
- Ploy M.-C, Gassama A., Chainier D., Denis F. Integrons as a genetic carrier of antibiotic resistance, ELSEVIER, 2005; Volume 20, pp. 343–352. [CrossRef]
- Roy PH et al. Dissemination of antibiotic resistance: genetic engineering at work in bacteria. Med Sci 1997, 13(927- 33).
- Benmehidi M et al, Situation épidémiologique des bactéries multi-résistantes (BMR) aux antibiotiques en réanimation médicale au CHU de Batna, thèse de doctorat en Sciences Biomédicales option microbiologie. November 2014; 19–20.
- WHO. Publication of the list of bacteria against which new antibiotics are urgently needed. Press release, GENEVA. 27 February 2017. [Google Scholar]
- Benmehidi, M., et al. Epidemiological situation of multi-resistant bacteria (BMR) to antibiotics in Medical Intensive Care at the University Hospital of Batna. University Hadj Lakhdar of Batna Faculty of Medicine of Batna Department of Medicine, defense THESIS For the obtention of the Degree of Doctor in Medical Sciences Option Microbiology, Algeria, 20 November 2014.
- Chih-Cheng L., Shey-Ying C., Wen-Chien K., Po-Ren H. Increased antimicrobial resistance during the COVID-19 pandemic. Department of Internal Medicine, Kaohsiung Veterans General Hospital, Tainan Branch, Tainan, Taiwan, Taipei, 2020; 57, 4, 106324. [CrossRef]
- Segala, F.V.; Bavaro, D.F.; Di Gennaro, F.; Salvati, F.; Marotta, C.; Saracino, A.; Murri, R.; Fantoni, M. Impact of SARS-CoV-2 Epidemic on Antimicrobial Resistance: A Literature Review. Viruses 2021, 13, 2110. [Google Scholar] [CrossRef]
- Junot, H., Meloni C., Bleibtreu A., Robert A. Impact of the COVID-19 pandemic on hospital antibiotic consumption, a single-center study of a metropolitan ESR. Medicine and Infectious Diseases Supplement, 20. 2020, 50(6), S94. [CrossRef]
- Ruwandi Kariyawasam, M., Danielle Julien A., Dana C. Antimicrobial resistance (AMR) in COVID-19 patients: a systematic review and meta-analysis (November 2019–June 2021). Departments of Production Animal Health and Community Health Sciences,, One Health at UCalgary, University of Calgary, Drive NW, Calgary T2N 4N1, Canada 3330 Hospital. Antimicrobial Resistance & Infection Control 2022, 11, 45.
- Shey-Ying, C., Wen-Chien K., Po-Ren H et al. Increased antimicrobial resistance during the COVID-19 pandemic. Department of Internal Medicine, National Taiwan University Hospital, Tainan Branch, Tainan, Taiwan. University College of Medicine, Taipei, 21. hsporen@ntu.edu.tw. 20 April.
- Sanofi. Fiche INVS, Klebsiella pneumoniae. Sanofi-Aventis France, 7000035453-12/2021; Antibio-Responsible.fr.
- Bradley J, Miranda So, Sumit Raybardhan, et al. Antibiotic prescribing in patients with COVID-19: Rapid review and meta-analysis. Public Health Ontario, ON, Canada, University of Toronto. Clinical Microbiology and Infection, 2021; 27, 520–531. [CrossRef]
- Gesu, G.P. Gesu G.P., Marchetti F. Increasing Resistance According to Patient’s Age and Sex in Escherichia coli Isolated from Urine in Italy. Journal of Chemotherapy 2019, 2, 161–165. [Google Scholar] [CrossRef]
- Djuikoue, C.I. Djuikoue, C.I., Djoulako, P.D.D., Wouambo, R.K., Tomi, C.N., Kiyang, C.P., Tchitchoua, M.C., Nyatchoutou, V.M., Messeu, B.K., Tagne, H.K., Nana, C.D.S., Benhamed, N., Kamga, H.G. and Poka, B.D.T. Phenotypic Characterization of Carbapenemase-Producing Enterobacteriaceae Strains in a Referral Teaching Hospital in Yaoundé, Cameroon. Open Journal of Medical Microbiology 2023, 13, 52–67. [Google Scholar] [CrossRef]
- Golkar Z, Bagazra O, Pace DG. Bacteriophage therapy: a potential solution for the antibiotic resistance crisis. J Infect Dev Ctries. 2014, 8, 136–136. 13.
- Gould IM, Bal AM. New antibiotic agents in the pipeline and how they can overcome microbial resistance. Virulence 2013, 4, 185–191. [CrossRef] [PubMed]
- Wright GD. Something new: revisiting natural products in antibiotic drug discovery. Can J Microbiol. 2014, 60, 147–154. [CrossRef]
- Sengupta S, Chattopadhyay MK, Grossart HP. The multifaceted roles of antibiotics and antibiotic resistance in nature. Front Microbiol. 2013, 4, 47.
- WHO. Tackling antimicrobial resistance (AMR) together. Working paper 5.0: Enhancing the focus on gender and equity. Geneva: World Health Organization. 2018. Available online: https://apps.who.int/iris/bitstream/handle/10665/336977/WHO-WSI-AMR-2018.3-eng.
- Bertakis, K. D. The influence of gender on the doctor–patient interaction. Patient Education and Counseling. 2009, 76, 356–360. [CrossRef] [PubMed]
- Eggermont, D., Smit, M. A. M., Kwestroo, G. A., Verheij, R. A., Hek, K., & Kunst, A. E. (2018). The influence of gender concordance between general practitioner and patient on antibiotic prescribing for sore throat symptoms: A retrospective study. BMC Family Practice 2018, 19, 175. [CrossRef]
- Schröder, W. Schröder, W., Sommer, H., Gladstone, B. P., Foschi, F., Hellman, J., Evengard, B., & Tacconelli, E. (2016). Gender differences in antibiotic prescribing in the community: A systematic review and meta-analysis. Journal of Antimicrobial Chemotherapy 2016, 71, 1800–1806. [Google Scholar] [CrossRef] [PubMed]
- Fang Rong, Yuanyuan Sun, Xiao Li, Chenhao Zhang, "Drug Resistance Mechanism of Enterobacteriaceae with Decreased Antibiotic Sensitivity", Applied Bionics and Biomechanics. 2022, 2022, 8285437. [CrossRef]
- P. Storey, M. Dollin, N. Rayess et al., “The effect of prophylactic topical antibiotics on bacterial resistance patterns in Endophthalmitis following intravitreal injection,”. Graefes Archive for Clinical and Experimental Ophthalmology 2016, 254, 254–254.
- S. Lin, J. J. Koh, T. T. Aung et al., “Symmetrically substituted Xanthone Amphiphiles combat gram-positive bacterial resistance with enhanced membrane selectivity,”. Journal of Medicinal Chemistry 2017, 60, 1362–1378. [CrossRef]
- E. Farfour, M. Lecuru, L. Dortet, M.L. Guen, C. Cerf, F. Karnycheff, et al. Carbapenemase-producing Enterobacterales outbreak: another dark side of COVID-19. Am J Infect Control 2020, 48, 1533–1536. [CrossRef]
- B. Tiri, E. Sensi, V. Marsiliani, M. Cantarini, G. Priante, C. Vernelli, et al. Antimicrobial stewardship program, COVID-19, and infection control: spread of carbapenem-resistant Klebsiella pneumoniae colonization in ICU COVID-19 patients. J Clin Med 2020, 9, E2744. [CrossRef]
- Li, J. Wang, Y. Yang, P. Cai, J. Cao, X. Cai, et al. Etiology and antimicrobial resistance of secondary bacterial infections in patients hospitalized with COVID-19 in Wuhan, China: a retrospective analysis. Antimicrob Resist Infect Control 2020, 9, 153. [CrossRef]
- E. Sharifipour, S. Shams, M. Esmkhani, J. Khodadadi, R. Fotouhi-Ardakani, A. Koohpaei, et al. Evaluation of bacterial co-infections of the respiratory tract in COVID-19 patients admitted to ICUBMC Infect Dis. 2020, 20, 646.
- T.M. Rawson, L.S.P. Moore, N. Zhu, N. Ranganathan, K. Skolimowska, M. Gilchrist, et al. Bacterial and fungal coinfection in individuals with coronavirus: a rapid review to support COVID-19 antimicrobial prescribing. Clin Infect Dis 2020, 71, 2459.
Figure 2.
Overall numbers of bacteria isolate and their corresponding resistance rate.
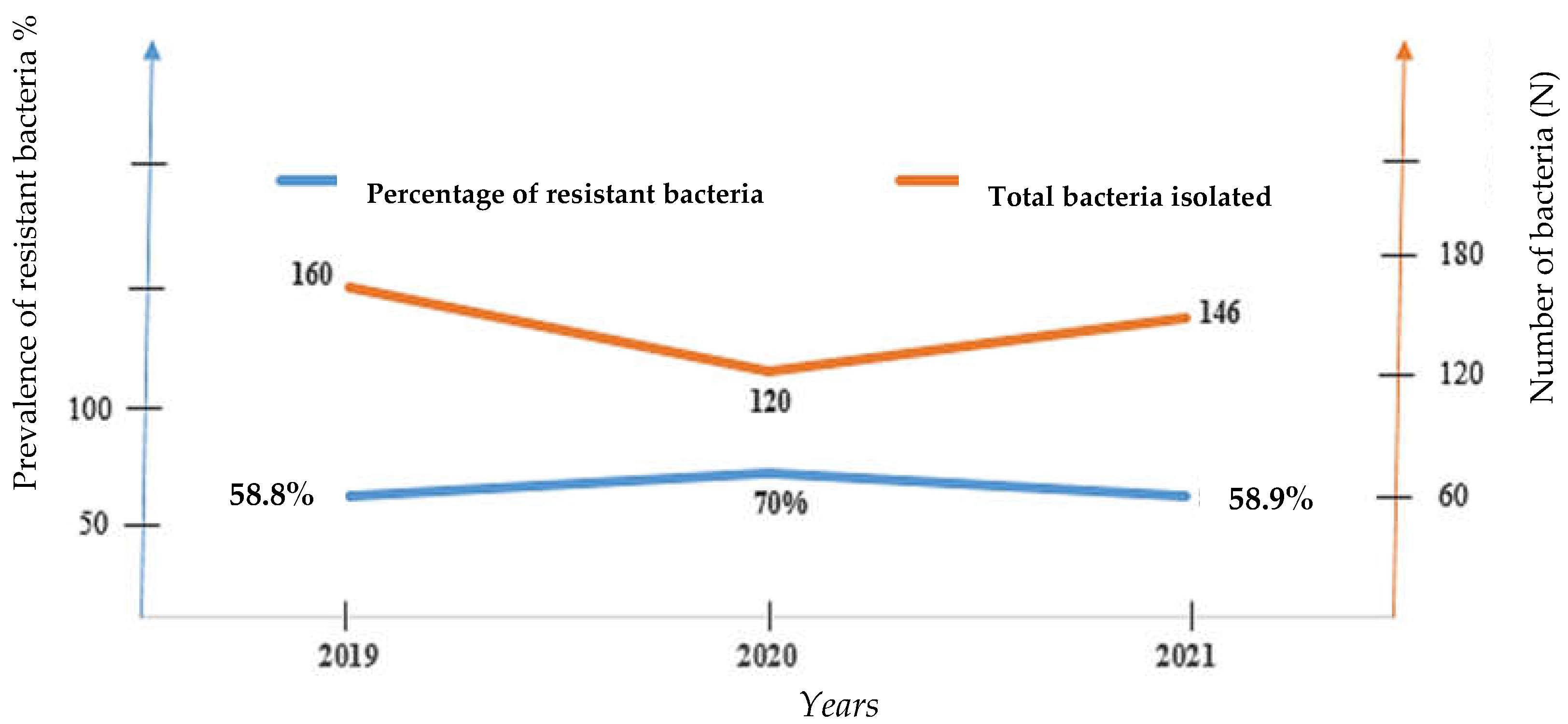
Figure 3.
Resistance rate by group of bacteria in 2019, 2020 and 2021.
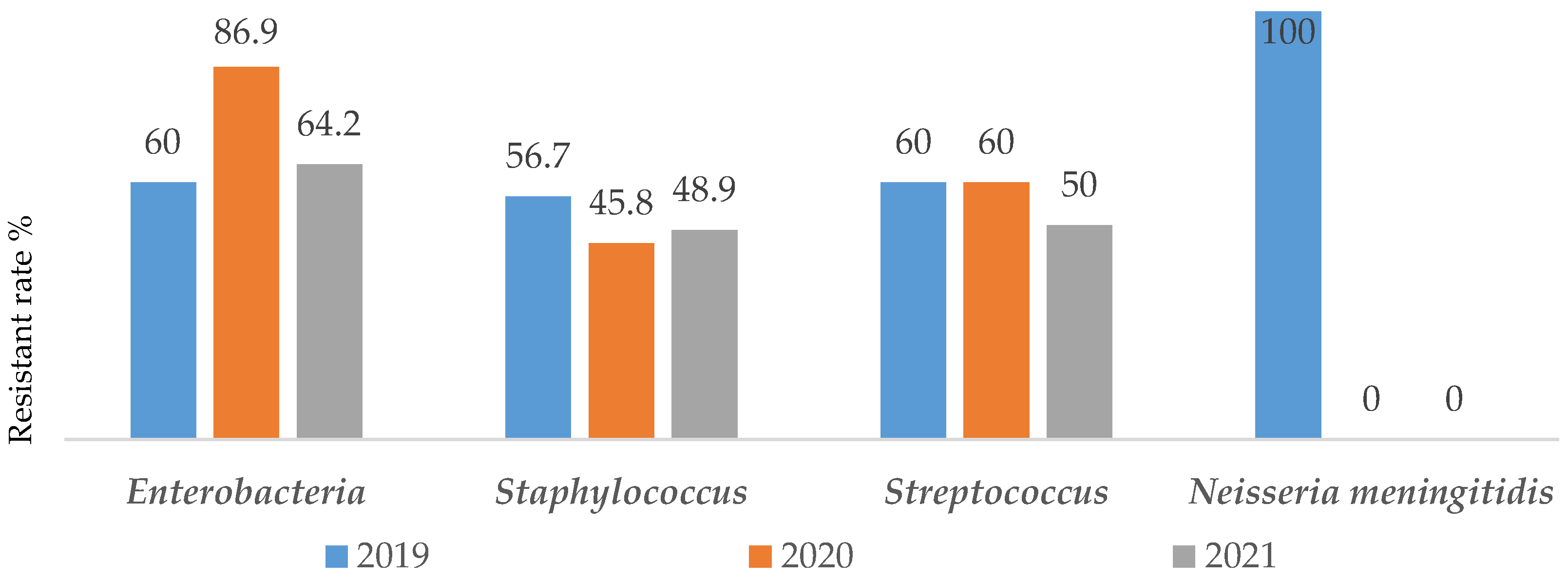
Figure 4.
Global Resistance rate to antibiotics over time.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



