Submitted:
01 March 2023
Posted:
02 March 2023
You are already at the latest version
Abstract
Abstract: Sand-cement bound screed floor layers are at risk for work-related low back pain, lumbosacral radicular syndrome and knee osteoarthritis given their working technique of level-ling screed with their trunk bended and mainly supported by their hands and knees. To reduce the exposure of the physical demands of bending of the trunk and kneeling, a manually moved screed levelling machine was developed for floor layers in the Netherlands. The aim of this pa-per is to estimate the potential health gain of the manually moved screed levelling machine on the risk of low back pain (LBP), lumbosacral radicular syndrome (LRS) and knee osteoarthritis (KOA) compared to the traditional working technique. The potential health gain was assessed using the epidemiological population estimates of the Population Attributable Fraction (PAF) and the Potential Impact Fraction (PIF) combined with work-related risk estimates for these three disorders from systematic reviews. The percentage of workers exceeding these risk esti-mates was based on worksite observations among in total 28 floor layers. For LBP, 16/18 work-ers were at risk using the traditional working technique with PAF=38%, and for the manually moved screed levelling machine this was 6/10 with PIF=13%. For LRS, these data were 16/18 with PAF=55% and 14/18 with PIF=18% and for KOA, 8/10 with PAF=35% and 2/10 with PIF=26%. A manually moved screed levelling machine might have a significant impact on the prevention of LBP, LRS and KOA among floor layers in the Netherlands and a health impact assessment is a feasible approach to assess health gains in an efficient way.
Keywords:
low back pain
; osteoarthritis
; knee
; prevalence
; workplace
; exposure
; musculoskeletal diseases
; risk factors
; prevention
; construction industry
1. Introduction
Worldwide the construction industry is characterized by a high prevalence of musculoskeletal complaints [1]. This review of Umer et al. showed that in the construction industry, musculoskeletal complaints with the highest one-year prevalence concern the low back with 51%, followed by the knee with 37%, and in third place is the shoulder with 32% [1]. The prevalences of the other body regions are 30% for the wrist, 24% for the neck and ankle/foot, 20% for the elbow and upper back, and 15% for the hip/thigh [1]. These prevalences of low back and knee complaints are also high when looking at clinically assessed diagnoses of musculoskeletal diseases and disorders among construction workers. Dale et al. reported annual prevalences of claims for acute musculoskeletal injuries (ICD10:S00-T14) and chronic musculoskeletal disorders (ICD10:M.x [x = any number] over the period of January 2015 to June 2018 [2]. The percentage for the back/torso was 30% and runners-up were both the lower and upper extremity with 15%, respectively. Similar results are reported by Van der Molen et al. in their study on incidence rates of occupational diseases in the Dutch construction sector for 2010–2014 [3]. These incidence rates were based on a dynamic prospective cohort of occupational physicians reporting to the Netherlands Center for Occupational Diseases. An occupational disease is defined as a clinically assessed diagnosis that is predominantly caused by work-related factors according to the reporting occupational physician [3]. The annual incidence of low back pain (ICD-10 code M545) was the highest with 750 per 100,000 construction workers. For osteoarthritis including the knee (ICD-10 codes M159, M169, M179, M189, M199 and excluding the spine) this was 688 per 100,000 construction workers. Not only self-reported complaints of the low back and knee, physician-diagnosed (occupational) diseases or disorders of the low back and knee, but also surgically treated musculoskeletal diseases and disorders regarding the low back and knee appear high among construction workers, like lumbar disc herniation [4,5] and hip and knee osteoarthritis [6]. Construction workers with these musculoskeletal diseases or disorders are at increased risk of sick leave [7] and paid labor force exit due to work disability [8]. An occupation within the construction industry where workers run an increased risk of low back pain, lumbosacral radicular syndrome and knee osteoarthritis are sand-cement bound screed floor layers [9-11]
To get insight in the efficacy of a preventive measures to reduce the number of floor layers with such a disease or disorder, insight in the proportional reduction of the number of these diseases or disorders is needed if floor layers are not or less exposed to the physical demands of this type of work [12,13]. In recent years, several systematic reviews have assessed to what extent physical demands at work contributed to these multifactorial musculoskeletal diseases and disorders, like low back pain [14], lumbosacral radiculopathy syndrome [15] and knee osteoarthritis [16]. Insight in the attributable fraction does not only provide insight in the number of work-related diseases or disorders that potentially might be prevented, but can also be used to estimate the potential health benefit of a specific preventive measure. Especially lumbosacral radicular syndrome and knee osteoarthritis have a long latency period before symptom onset. Therefore, a controlled prevention study to assess the incidence these musculoskeletal diseases is not only time consuming but probably requires a great number of participants to secure enough new cases and statistical power.
An alternative might be to perform a health impact assessment. The World Health Organisation [17] defines a health impact assessment as ‘… a practical approach used to judge the potential health effects of a policy, program or project on a population, particularly on vulnerable or disadvantaged groups. Recommendations are produced for decision-makers and stakeholders, with the aim of maximizing the proposal’s positive health effects and minimizing its negative health effects.’
In the Netherlands, the Dutch Labor Inspectorate wanted to reduce the exposure to bending of the trunk and kneeling among sand-cement bound screed floor layers and thereby reduce the risk of low back pain, lumbosacral radicular syndrome and knee osteoarthritis by stimulating the use of a manually moved screed levelling machine (Figure 1). Compared to the traditional working technique (Figure 1a), the work can be performed in a more upright standing and walking position (Figure 1b). This recommendation of the Dutch Labor Inspectorate was based on two studies of Visser et al. [11, 18]. The first study [11] assessed the physical work demands of the traditional working technique of sand-cement bound screed floor layers and of anhydrite-bound screed floor layer [11]. The second study [18] assessed the physical work demands only among sand–cement bound screed floor layers using two electrical screed levelling machines namely a manually moved screed levelling machine (Figure 1b) and a self-propelled machine.. Based on these two studies, Visser et al [11, 18] concluded that the manually moved screed levelling machine may help to reduce the high physical work demands on floor layers while working with the traditional working technique. However, the studies by Visser et al [11,18] did not answer the question how much the health benefit is for floor layers regarding the reduction of the risk on low back pain, lumbosacral radicular syndrome and knee osteoarthritis. To overcome this research gap, this paper aims to assess what the potential health benefit is for low back pain, lumbosacral radicular syndrome and knee osteoarthritis using a health impact assessment. Given that the exposure to bending of the trunk and kneeling among sand-cement bound screed floor layers using the manually moved screed levelling machine is lower than using the traditional working technique, we hypothesize that the manually moved screed levelling machine results in a reduction of the risk of low back pain, lumbosacral radicular syndrome and knee osteoarthritis. However, the real world potential effects size has to be established yet.
In summary, therefore the research question is: How much health gain can be expected by working with the manually moved screed levelling machine compared to the traditional working technique in preventing low back pain, lumbosacral radicular syndrome and knee osteoarthritis among sand-cement bound screed floor layers in the Netherlands?
2. Materials and Methods
2.1. Design and population
To answer the research question we calculated the Population Attributable Fraction and the Potential Impact Fraction. To do so, we used the data from the studies by Visser et al. [11,18] that described the exposure to the physical work demands of bending of the trunk and kneeling. These two papers described in total four working techniques. The first paper described workplace assessments among sand–cement-bound screed floor and among anhydrite-bound screed floor layers [11]. The sand–cement-bound screed floor layers used the traditional working technique (Figure 1a) and these data were used in the present study. The second paper described similar workplace assessments, but this time among sand–cement bound screed floor layers using two electrical screed levelling machines namely a manually moved screed levelling machine (Figure 1b) and a self-propelled machine. In this paper we only used the data of the manually moved screed levelling machine. This manually moved screed weighs about 24 kg and is 2 meters wide (Figure 1B). The manually moved screed levelling machine can be pushed, pulled, lifted or carried in the desired direction during the levelling of the screed floor.
The exposure to the physical work demands of bending of the trunk and kneeling using the traditional working technique and the manually moved screed levelling machine was assessed by means of real time observation of in total 28 male floor layers during regular working days: 18 floor layers while working with the traditional working technique and 10 floor layers while working with the manually moved screed levelling machine [11,18]. The mean and standard deviation of age, body height, body weight and seniority of these 28 screed floor layer were 41 (11) years, 181 (8) cm, 86 (12) kg and 16 (12) years, respectively.
In addition, to assess the number of screed floor layers at risk for low back pain, lumbosacral radicular syndrome, and knee osteoarthritis, the exposure limits for bending of the trunk and kneeling as reported in the systematic reviews with meta-analysis of Lötters et al., Kuijer et al. and Verbeek et al. were used [14-16]. These exposure limits are defined in the following paragraph 2.2.
2.2. Population Attributable Fraction
To answer the research question, first the population attributable fractions (PAF) was calculated using the formula 1 [19,20]:
- PAF = P*(OR-1)/[1+P(OR-1),
with P the prevalence of workers at risk for a low back pain, lumbosacral radicular syndrome or knee osteoarthritis and being exposed to the work-related risk factor at stake. For low back pain and lumbosacral radicular syndrome, the risk factor at stake is working 30 minutes or more per workday with the trunk bent more than 40° [14, 15]. For osteoarthritis of the knee, the risk factor at stake is kneeling 60 minutes or more per workday [16]. In this paper we used the odds ratio (OR) instead of the relative risk given that the prevalence of these diseases or disorders is relatively low [21].
Thereby, the PAF shows what percentage of low back pain, lumbosacral radicular syndrome and knee osteoarthritis can be attributed to the physical work-demands in the work of sand-cement bound screed floor layers based on the traditional working technique.
To calculate the PAF, for low back pain and lumbosacral radicular syndrome, as said the exposure limit was defined at working 30 minutes per day with the trunk bent more than 40°. The corresponding ORs are derived from the systematic reviews with meta-analysis of Lötters et al. and Kuijer et al. [14,15]. For low back pain the OR=1.7 (95% Confidence Interval (95%CI) 1.4-2.0) [14 Table 2 in that paper, 22] and for lumbosacral radicular syndrome the OR=2.4 (95%CI 1.7-3.6) [15, Figure 2 in that paper],. For knee osteoarthritis, as said this was kneeling 60 minutes per workday with the corresponding OR=1.7 (95%CI 1.4-2.1) [16,Figure 1 in that paper]. These exposure limits were also based on the reporting guidelines of the Netherland Center for Occupational Diseases [23].
The percentage of workers exceeding these exposure limits was based on worksite observations among 18 floor layers for the traditional working technique. The observations are described in detail in the papers by Visser et al. [11,18]. In short, the work demands - the duration of bending of the trunk more than 40° and the time kneeling - were real-time observed by in total three observers using Task Recording and Analysis on Computer system at the workplace [24]. Each floor layer was observed by one observer. The observer was trained in real-time observations with the help of video fragments of floor layers using the traditional working technique and working with the manually moved screed levelling machine. The intra-observer reliability for the main tasks and work demands was sufficient and the intra-class coefficient ranged from 0.7 to 1.0. This interclass coefficient was considered adequate for workplace observations [11,18].
2.3. Potential Impact Fraction
Based on the PAF, the potential impact fraction (PIF) is estimated as the proportional reduction in incidence due to a reduction in the exposure to physical work demands [25]. The PIF is calculated using formula 2 [26]:
- 2.
- PIF = (P-P’)(IDR-1)/P(IDR-1)+1),
with P the prevalence of workers at risk while working without an ergonomic intervention, P’ the prevalence of workers at risk when working with an ergonomic intervention and IDR the Incidence Density Ratio, which in the present study is replaced with the OR.
The percentage of workers exceeding these exposure limits while working with the manually moved screed levelling machine was based on worksite observations among 10 floor layers working with the manually moved screed levelling machine. The observations are described in detail in the papers by Visser et al. and a summary is given above in paragraph 2.1 [11,18].
3. Results
3.1. Population Attributable Fraction
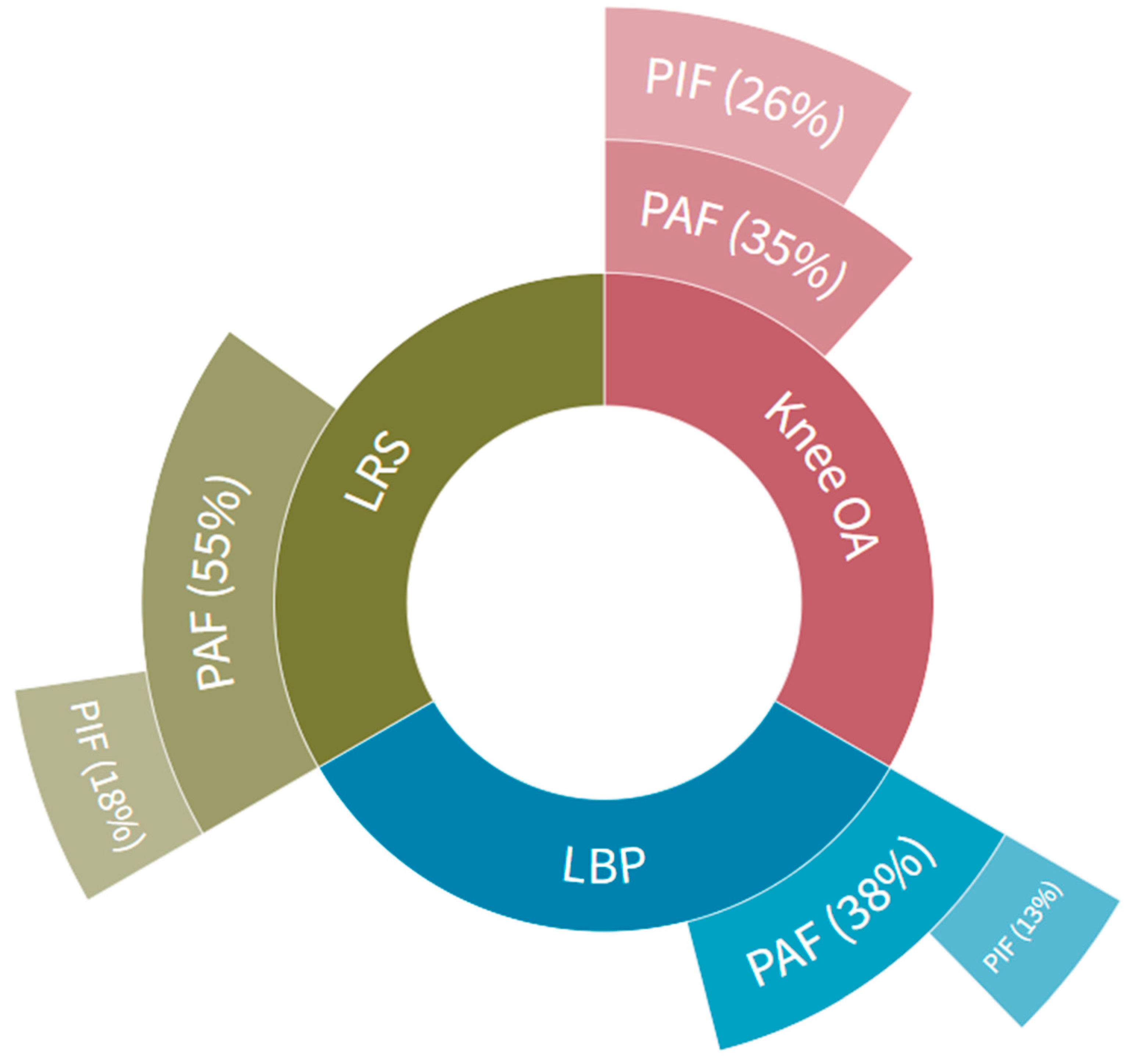
The mean time working with the trunk bent more than 40° was 98 minutes per worker per working day using the traditional working technique of sand-cement bound screed floor layers [11] (Table 3) and 16/18 workers were at risk for both low back pain and lumbosacral radicular syndrome. For knee osteoarthritis, these data were 97 minutes per working day and 14/18 workers [11] (Table 3). This means that the maximum preventable work-related fraction based on the PAF for low back pain is 38%, for lumbosacral radicular syndrome is 55% and for knee osteoarthritis is 35% (Figure 2).
3.2. Potential Impact Fraction
The mean time working with the trunk bent more than 40° was 37 minutes per worker per working day using the manually moved screed levelling machine [18] and 6/10 workers were at risk for both low back pain and for lumbosacral radicular syndrome. For knee osteoarthritis, these data were 2/10 workers and 37 minutes per worker per working day [18] (Table 1). This means that the maximum preventable work-related fraction based on the PIF for low back pain is 13%, for lumbosacral radicular syndrome is 18% and for knee osteoarthritis is 26% (Figure 2). When comparing the percentages of the PIF with the PAF, this means that the manually moved screed levelling machine seems most effective for the work-related prevention of knee osteoarthritis (26/35, 74%), next for lumbosacral radicular syndrome (18/35, 51%) and least for low back pain (13/38, 34%).
4. Discussion
The main finding of this study is that working with a manually moved screed levelling machine might result in a reduction of low back pain, lumbosacral radicular syndrome and knee osteoarthritis among floor layers in the Netherlands compared to the traditional working technique. In addition, since nine out of ten floor layers found the manually moved screed levelling machine applicable in practice [18], the Dutch Labor Inspectorate advices to use the traditional working technique only in areas smaller than 30 m2 given the size and weight of the manually moved screed levelling machine to avoid unnecessary lifting and carrying. Moreover, this study shows what the added value might be of a health impact assessment as a practical and efficient approach to estimate the potential health benefits for three prevalent work-related musculoskeletal disorders based on the use of an ergonomic measure at a worksite without having to perform a prospective intervention study with a large group of workers and a follow-up of several years.
4.1. Comparison with other studies and prospects
Regarding the estimated efficacy of a manually moved screed levelling machine we have to make the following caveat. For the manually moved screed levelling machine, the estimated reduction per worker per working day is about 1 hour for bending of the trunk en 1 hour for the time kneeling given that one floor layer operates the machine [18]. However, floor layers often work in teams of a total of three workers: one works with the manually moved screed levelling machine, another floor layer as the hodman distributing the sand–cement mixture on the floor, and a third-floor layer setting out the height of the floor by manually levelling the floor around the walls. In practice, workers might rotate during or between days. Therefore, the manually moved screed levelling machine might change the work demands of all three workers and might have a smaller effect than estimated in the present study. However, especially given the large effect on the exposure reduction of kneeling, this reduction might be sufficient to reduce the risk of knee osteoarthritis for all three floor layers. This expectation is in line with the findings of the studies of Jensen and Friche on knee complaints [27-29]. Working more often in an upright working posture reduced the number of floor layers reporting knee pain already after 3 months (28% vs. 6%) [27]. After two years, floor layers who used the new upright working technique less often, had a doubled risk of reporting having complaints daily or for more than 30 days during the previous 12 months (OR 2.46, 95% CI 1.03 to 5.83) or reporting locking of the knees (OR 2.89, 95% CI 1.11 to 7.5)[28,29]. Moreover, a reduction in moderate-to-severe knee pain was greatest if floor layers started to use the new working methods before they developed the knee complaints (OR 2.7 95%CI 1.02-7.26) [28,29]. These studies and the present study are also good examples that change in the so-called ‘individual working practice’ by using assistive devices also contribute to a reduction in work-related musculoskeletal knee disorders [30,31]. This is important for knee osteoarthritis, given the worldwide strong increase of this disabling disease especially among workers and the relatively little attention that is given to prevention of the work-related risk factors [32-34] and remains important for the highly prevalent work-related low back pain [35].
We liked to compare the efficacy of the manually moved screed levelling machine on the reduction of the risk of musculoskeletal disorders with other ergonomic interventions that have been implemented and assessed in the workplace. Unfortunately, we were not able to find any other ergonomic studies on the prevention of musculoskeletal disorders that used a health impact assessment or PIF to assess the efficacy. Regarding the use of health impact assessments in ergonomic studies, we found no other studies in PubMed on January 19th 2023. We retrieved 926 results using “Health Impact Assessment” as Mesh term in the PubMed database. This search was combined with “Ergonomics” as Mesh term, including 60.624 results. This combined search with AND only resulted in two papers: one paper described potential health effects based on telework in response to the spread of COVID-19 and the other study assessed activities of daily living in older and healthy adults [36,37]. So none of these two studies reported on a potential health benefit for musculoskeletal disorders due to an ergonomic intervention. To be more certain, we also performed a search in PubMed using PIF. We retrieved 71 results using ‘Potential Impact Fraction’[Text Word] on February 27th 2023. Again, none of the studies reported on a potential health benefit for musculoskeletal disorders due to an ergonomic intervention. Most studies addressed the impact of a risk factor or intervention on cancer [44, 45]. Examples are obesity, smoking, alcohol consumption, fruit and vegetable intake and physical activity. Other preventable diseases often studied were diabetes and cardiovascular diseases. This emphasizes the merits of the use of a health impact assessment in the field of ergonomic intervention studies to prevent work-related musculoskeletal disorders, as is done in the present study. Given the numerous studies performed on physical exposure assessments in ergonomics to prevent these work-related musculoskeletal disorders [30], we suggest that researchers and practitioners more often consider including a simple health impact assessment to estimate the potential health benefit in terms of a musculoskeletal disease or disorder of a preventive ergonomic measure.
4.2. Strengths and limitations
A strength of the present paper is that a health impact assessment as performed in the present study might be a relatively simple tool to bridge the gap between ergonomic prevention studies on exposure reduction and epidemiological studies on potential health benefits. By using a health impact assessment, additional insight is given in the extent an actual reduction of exposure might mean in terms of a specific work-related or occupational disease or disorder. Also for other musculoskeletal diseases or disorders than the three described in the present study, reviews are available to set clinically relevant exposure limits. Examples are carpal tunnel syndrome [38], lateral epicondylitis [39], subacromial pain syndrome [40] and hip osteoarthritis [41]. Another strength is the actual measurement of exposures at the worksite to assess the proportion of workers exceeding these health related exposure limits [11,18].
A limitation is that we perform no follow up study to validate whether workers using the manually moved screed levelling machine more often, are indeed less susceptible to low back pain, lumbosacral radicular syndrome and knee osteoarthritis in the upcoming years like for instance Jensen and Friche did with a two-year follow up [28,29]. Even given the latency period for lumbosacral radicular syndrome and knee osteoarthritis to become symptomatic, this might be manageable using a worker specific occupational health surveillance program in the Dutch construction industry [42]. An example that such a study is feasible was the evaluation whether an informational campaign resulted in an increased use of ergonomic measures and subsequently resulted in less self-reported musculoskeletal complaints over a five year time period [43]. Thereby questionnaire data of the occupational health surveillance were retrieved twice from a large cohort of about 1000 Dutch carpenters and pavers, once in 2000 and once in 2005. Another limitation might be that the observation time for working with the manually moved screed levelling machine in the study of Visser et al. [18] were extrapolated to an entire working day to compare them with the results of Visser et al. [11]. Since the mean time working bending of the trunk was 37 minutes and around the exposure limit of 30 minutes, the prevalence of workers at risk might be different if these observations were performed during a full working day, like in the study of Visser et al. [11]. Probably the time bending is mainly dependent of the type of floors: it can be expected that the prevalence of workers at risk is lower while working in larger open spaces when the manually moved screed levelling machine can be used, and will be higher when working in narrow corridors given that the size of the manually moved screed levelling machine is too big for these latter circumstances and therefore workers will use the traditional working technique.
5. Conclusions
Based on a health impact assessment and calculating the potential impact fraction using workplace observations regarding exposure of physical work demands, we showed that a manually moved screed levelling machine might have a significant impact on the prevention of low back pain, lumbosacral radicular syndrome and knee osteoarthritis among floor layers in the Netherlands compared to the traditional working technique based on a health impact assessment. The estimated percentage reduction of the preventable work-related fraction varies between 74% for knee osteoarthritis and 34% for low back pain. Moreover, this paper shows that a health impact assessment is relatively simple approach to estimate health benefits in ergonomic prevention studies on the prevention of musculoskeletal diseases and disorders.
Author Contributions
“Conceptualization, P.K., S.V. and H.F.M.; methodology, P.K., S.V. and H.F.M.; validation, P.K., S.V. and H.F.M; data curation and software, S.V.; investigation, P.K. and S.V.; formal analysis, P.K. and S.V.; writing—original draft preparation, P.K..; writing—review and editing, S.V. and H.F.M.; visualization, S.V..; supervision, P.K.; All authors have read and agreed to the published version of the manuscript.”
Funding
“This research received no external funding.”
Institutional Review Board Statement
“Not applicable.”
Informed Consent Statement
“Not applicable.’’
Data Availability Statement
“Not applicable.”
Conflicts of Interest
“The authors declare no conflict of interest.”
References
- Umer, W.; Antwi-Afari, M.F.; Li, H.; Szeto, G.P.Y.; Wong, A.Y.L. The prevalence of musculoskeletal symptoms in the construction industry: a systematic review and meta-analysis. Int Arch Occup Environ Health. 2018, 91(2), 125–144. [Google Scholar] [CrossRef] [PubMed]
- Dale, A.M.; Buckner-Petty, S.; Evanoff, B.A.; Gage, B.F. Predictors of long-term opioid use and opioid use disorder among construction workers: Analysis of claims data. Am J Ind Med. 2021, 64(1), 48–57. [Google Scholar] [CrossRef] [PubMed]
- van der Molen, H.F.; de Vries, S.C.; Stocks, S.J.; Warning, J.; Frings-Dresen, M.H. Incidence rates of occupational diseases in the Dutch construction sector, 2010-2014. Occup Environ Med. 2016, 73(5), 350–2. [Google Scholar] [CrossRef]
- Wahlström, J.; Burström, L.; Nilsson, T.; Järvholm, B. Risk factors for hospitalization due to lumbar disc disease. Spine (Phila Pa 1976), 1334. [Google Scholar] [CrossRef]
- Wahlström, J.; Burström, L.; Johnson, P.W.; Nilsson, T.; Järvholm, B. Exposure to whole-body vibration and hospitalization due to lumbar disc herniation. Int Arch Occup Environ Health. 2018, 91(6), 689–694. [Google Scholar] [CrossRef] [PubMed]
- Järvholm, B.; From, C.; Lewold, S.; Malchau, H.; Vingård, E. Incidence of surgically treated osteoarthritis in the hip and knee in male construction workers. Occup Environ Med. 2008, 65(4), 275–8. [Google Scholar] [CrossRef] [PubMed]
- Bosman, L.C.; Dijkstra, L.; Joling, C.I.; Heymans, M.W. Twisk, J.W.; Roelen, C.A. Prediction models to identify workers at risk of sick leave due to low-back pain in the Dutch construction industry. Scand J Work Environ Health. [CrossRef]
- Järvholm, B.; Stattin, M.; Robroek, S.J.; Janlert, U.; Karlsson, B.; Burdorf, A. Heavy work and disability pension - a long term follow-up of Swedish construction workers. Scand J Work Environ Health. 2014, 40(4), 335–42. [Google Scholar] [CrossRef] [PubMed]
- Burdorf, A.; Windhorst, J.; van der Beek, A.J.; van der Molen, H.F.; Swuste, P.H.J.J. The effects of mechanised equipment on physical load among road workers and floor layers in the construction industry. Int. J. Ind. Ergon. [CrossRef]
- McGaha, J.; Miller, K.; Descatha, A.; Welch, L.; Buchholz, B.; Evanoff, B.; Dale, A.M. Exploring physical exposures and identifying high-risk work tasks within the floor layer trade. Appl. Ergon. 2014, 45(4), 857–864. [Google Scholar] [CrossRef] [PubMed]
- Visser, S.; van der Molen, H.F.; Kuijer, P.P.F.M.; van Holland, B.J.; Frings-Dresen, M.H.W. Evaluation of two working methods for screed floor layers on musculoskeletal complaints, work demands and workload. 2013, Ergonomics, 56(1), 69-78. [CrossRef]
- van der Beek, A.J.; Dennerlein, J.T.; Huysmans, M.A.; Mathiassen, S.E.; Burdorf, A.; van Mechelen, W.; van Dieën, J.H.; Frings-Dresen, M.H.; Holtermann, A.; Janwantanakul, P.; van der Molen, H.F.; Rempel, D.; Straker, L.; Walker-Bone, K.; Coenen, P. A research framework for the development and implementation of interventions preventing work-related musculoskeletal disorders. Scand J Work Environ Health. 2017, 43(6), 526–539. [Google Scholar] [CrossRef]
- Tamminga, S.J.; Kuijer, P.P.F.M.; Badarin, K.; Alfonso, J.H.; Amaro, J.; Curti, S.; Canu, I.G.; Mattioli, S.; Mehlum, I.S.; Rempel, D.; Roquelaure, Y.; Visser, S.; van der Molen, H.F. Towards harmonisation of case definitions for eight work-related musculoskeletal disorders - an international multi-disciplinary Delphi study. BMC Musculoskelet Disord. 2021, 22(1), 1018. [Google Scholar] [CrossRef]
- Lötters, F.; Burdorf, A.; Kuiper, J.; Miedema, H. Model for the work-relatedness of low-back pain. Scand J Work Environ Health. 2003, 29(6), 431–40. [Google Scholar] [CrossRef]
- Kuijer, P.P.F.M.; Verbeek, J.H.; Seidler, A.; Ellegast, R.; Hulshof, C.T.J.; Frings-Dresen, M.H.W.; van der Molen, H.F. Work-relatedness of lumbosacral radiculopathy syndrome: Review and dose-response meta-analysis. Neurology. 2018, 91(12), 558–564. [Google Scholar] [CrossRef] [PubMed]
- Verbeek, J.; Mischke, C.; Robinson, R.; Ijaz, S.; Kuijer, P.; Kievit, A.; Ojajärvi, A.; Neuvonen, K. Occupational Exposure to Knee Loading and the Risk of Osteoarthritis of the Knee: A Systematic Review and a Dose-Response Meta-Analysis. Saf Health Work. 2017, 8(2), 130–142. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation Health impact assessment Available online:. Available online: https://www.who.int/health-topics/health-impact-assessment#tab=tab_1 (accessed on January 5th 2022).
- Visser, S.; van der Molen, H.F.; Kuijer, P.P.; Sluiter, J.K.; Frings-Dresen, M.H. Stand up: comparison of two electrical screed levelling machines to reduce the work demands for the knees and low back among floor layers. Ergonomics. 2016, 59(9), 1224–31. [Google Scholar] [CrossRef] [PubMed]
- Poole, C. A history of the population attributable fraction and related measures. Ann Epidemiol. 2015, 25(3), 147–54. [Google Scholar] [CrossRef] [PubMed]
- van der Molen, H.F.; Hulshof, C.T.; Kuijer, P.P.F.M. How to improve the assessment of the impact of occupational diseases at a national level? The Netherlands as an example. Occup Environ Med. 2019, 76(1), 30–32. [Google Scholar] [CrossRef] [PubMed]
- Davies, H.T.; Crombie, I.K.; Tavakoli, M. When can odds ratios mislead? BMJ. 1998, 316(7136), 989–91. [Google Scholar] [CrossRef] [PubMed]
- Kuiper, J.I.; Burdorf, A.; Frings-Dresen, M.H.; Kuijer, P.P.; Spreeuwers, D.; Lötters, F.J.; Miedema, H.S. Assessing the work-relatedness of nonspecific low-back pain. Scand J Work Environ Health. 2005, 31(3), 237–43. [Google Scholar] [CrossRef] [PubMed]
- Musculoskeletal disorders (In Dutch: Aandoeningen aan bewegingsapparaat) Available online:. Available online: https://www.beroepsziekten.nl/registratierichtlijnen/aandoeningen-bewegingsapparaat (accessed on January 20th 2022).
- Frings-Dresen, M.H.W.; Kuijer, P.P.F.M. The TRAC-system: An observation method for analysing work demands at the workplace. Saf. Sci. [CrossRef]
- Burdorf, A.; Koppelaar, E.; Evanoff, B. Assessment of the impact of lifting device use on low back pain and musculoskeletal injury claims among nurses. Occup Environ Med. 2013, 70(7), 491–7. [Google Scholar] [CrossRef] [PubMed]
- Morgenstern, H.; Bursic, E.S. A method for using epidemiologic data to estimate the potential impact of an intervention on the health status of a target population. J Community Health 1982, 7, 292–309. [Google Scholar] [CrossRef] [PubMed]
- Jensen, L.K.; Friche, C. Effects of training to implement new tools and working methods to reduce knee load in floor layers. Appl Ergon. 2007, 38(5), 655–65. [Google Scholar] [CrossRef]
- Jensen, L.K.; Friche, C. Effects of training to implement new working methods to reduce knee strain in floor layers. A two-year follow-up. Occup Environ Med. [CrossRef]
- Jensen, L.K.; Friche, C. Implementation of new working methods in the floor-laying trade: Long-term effects on knee load and knee complaints. Am J Ind Med. 2010, 53(6), 615–27. [Google Scholar] [CrossRef] [PubMed]
- Wijdeven, B.; Visser, B.; Daams, J.; Kuijer, P.P.F.M. A first step towards a framework for interventions for Individual Working Practice to prevent work-related musculoskeletal disorders: a scoping review. BMC Musculoskelet Disord., accepted.
- van der Molen, H.F.; Sluiter, J.K.; Hulshof, C.T.; Vink, P.; van Duivenbooden, C.; Frings-Dresen, M.H. Conceptual framework for the implementation of interventions in the construction industry. Scand J Work Environ Health. /: Suppl 2:96-103. https.
- d’Errico, A.; Fontana, D.; Sebastiani, G.; Ardito, C. Risk of symptomatic osteoarthritis associated with exposure to ergonomic factors at work in a nationwide Italian survey. Int Arch Occup Environ Health. 2023, 96(1), 143–154. [Google Scholar] [CrossRef] [PubMed]
- Hardenberg, M.; Speklé, E.M.; Coenen, P.; Brus, I.M.; Kuijer, P.P.F.M. The economic burden of knee and hip osteoarthritis: absenteeism and costs in the Dutch workforce. BMC Musculoskelet Disord. 2022, 23(1), 364. [Google Scholar] [CrossRef] [PubMed]
- Kuijer, P.P.F.M.; Burdorf, A. Prevention at work needed to curb the worldwide strong increase in knee replacement surgery for working-age osteoarthritis patients. Scand J Work Environ Health. 2020, 46(5), 457–460. [Google Scholar] [CrossRef] [PubMed]
- Punnett, L.; Prüss-Utün, A.; Nelson, D.I.; Fingerhut, M.A.; Leigh, J.; Tak, S.; Phillips, S. Estimating the global burden of low back pain attributable to combined occupational exposures. Am J Ind Med. 2005, 48(6), 459–69. [Google Scholar] [CrossRef] [PubMed]
- Nagata, T.; Ito, D.; Nagata, M.; Fujimoto, A.; Ito, R.; Odagami, K.; Kajiki, S.; Uehara, M.; Oyama, I. ; Dohi. S.; Fujino, Y., Ed.; Mori, K. Anticipated health effects and proposed countermeasures following the immediate introduction of telework in response to the spread of COVID-19: The findings of a rapid health impact assessment in Japan. J Occup Health. 2021, 63(1), e12198. [Google Scholar] [CrossRef]
- Sreedevi, U.; Alaparthi, G.K.; Krishnan, S.; Chakravarthy Bairapareddy, K.; Anand, R.; Acharya, V. Normative Values for Londrina ADL Protocol in Healthy Individuals in Age Group of 40-60 Years among Indian Population: A Cross-Sectional Study. Can Respir J. 2020, 8612928. [Google Scholar] [CrossRef] [PubMed]
- Hassan, A.; Beumer, A.; Kuijer, P.P.F.M.; van der Molen, H.F. Work-relatedness of carpal tunnel syndrome: Systematic review including meta-analysis and GRADE. Health Sci Rep. 2022, 5(6), e888. [Google Scholar] [CrossRef]
- Bretschneider, S.F.; Los, F.S.; Eygendaal, D.; Kuijer, P.P.F.M.; van der Molen, H.F. Work-relatedness of lateral epicondylitis: Systematic review including meta-analysis and GRADE work-relatedness of lateral epicondylitis. Am J Ind Med. 2022, 65(1), 41–50. [Google Scholar] [CrossRef] [PubMed]
- van der Molen, H.F.; Foresti, C.; Daams, J.G.; Frings-Dresen, M.H.W.; Kuijer, P.P.F.M. Work-related risk factors for specific shoulder disorders: a systematic review and meta-analysis. Occup Environ Med. 2017, 74(10), 745–755. [Google Scholar] [CrossRef]
- Seidler, A.; Lüben, L.; Hegewald, J.; Bolm-Audorff, U.; Bergmann, A.; Liebers, F.; Ramdohr, C.; Romero Starke, K.; Freiberg, A.; Unverzagt, S. Dose-response relationship between cumulative physical workload and osteoarthritis of the hip - a meta-analysis applying an external reference population for exposure assignment. BMC Musculoskelet Disord. 2018, 19(1), 182. [Google Scholar] [CrossRef]
- Boschman, J.S.; van der Molen, H.F.; van Duivenbooden, C.; Sluiter, J.K.; Frings-Dresen, M.H. A trial of a job-specific workers’ health surveillance program for construction workers: study protocol. BMC Public Health. 2011, 11, 743. [Google Scholar] [CrossRef] [PubMed]
- van der Molen, H.F.; Sluiter, J.K.; Frings-Dresen, M.H. The use of ergonomic measures and musculoskeletal complaints among carpenters and pavers in a 4.5-year follow-up study. Ergonomics. [CrossRef]
- Rezende, L.F.M.; Malhão, T.A.; da Silva Barbosa, R.; Schilithz, A.O.C.; da Silva, R.C.F.; Moreira, L.G.M.; Machado, P.A.N.; Arguelhes, B.P.; Melo, M.E.L.D. The future costs of cancer attributable to excess body weight in Brazil, 2030-2040. BMC Public Health. 2022, 22(1), 1236. [Google Scholar] [CrossRef] [PubMed]
- Gredner, T.; Niedermaier, T.; Steindorf, K.; Brenner, H.; Mons, U. Impact of reducing excess body weight and physical inactivity on cancer incidence in Germany from 2020 to 2050-a simulation model. Eur J Cancer. [CrossRef]
Figure 1.
A sand-cement bound screed floor layer working (a) using the traditional working technique and (b) using the manually moved screed levelling machine.
Figure 1.
A sand-cement bound screed floor layer working (a) using the traditional working technique and (b) using the manually moved screed levelling machine.

Figure 2.
The maximum preventable work-related fraction (%) for low back pain (LBP), for lumbosacral radicular syndrome (LRS) and for knee osteoarthritis (Knee OA) based on the Population Attributable Fraction (PAF) while working with the traditional working technique and the potential impact fraction (PIF, also in %) while working with the manually moved screed levelling machine.
Figure 2.
The maximum preventable work-related fraction (%) for low back pain (LBP), for lumbosacral radicular syndrome (LRS) and for knee osteoarthritis (Knee OA) based on the Population Attributable Fraction (PAF) while working with the traditional working technique and the potential impact fraction (PIF, also in %) while working with the manually moved screed levelling machine.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



