
Submitted:
20 February 2023
Posted:
27 February 2023
You are already at the latest version
Abstract
The survival rate of extracorporeal life support (ECLS) remains overall at 60 %. Research and development is slow, partly due to the lack of sophisticated experimental models. This publication introduces a dedicated rodent oxygenator (“RatOx”) and shows preliminary in vitro classification tests. The RatOx has an adaptable fiber module size for various rodent models. Gas transfer performance over the fiber module for different blood flows and fiber module sizes were tested according to DIN EN ISO 7199.At the maximum possible amount of effective fiber surface and a blood flow of 100 ml/min, the oxygenator performance has been tested to a maximum of 6.27 ml O2/min and 8.2 ml CO2/min, respectively. The priming volume for this the largest fiber module is 5.4 ml, while the smallest possible configuration with a single fiber mat layer has 1.1 ml of priming volume. The novel RatOx ECLS system has been evaluated in-vitro to comply to a high degree with all predefined functionality criteria for rodent sized animal models. We intend for the RatOx to become a standard testing platform for scientific studies on ECLS therapy and technology.
Keywords:
ECLS
; ECMO
; animal model
; rodent
; rat
; mouse
; hamster
; CPB
; in-vivo
; oxygenator
1. Introduction
Patients suffering from critical cardiac and/or respiratory dysfunction of any cause can be bridged to treatment or recovery using an extracorporeal circulation that can comprise of an artificial heart, lungs and a heat source. So-called extracorporeal life support (ECLS) is a high-mortality procedure and considered a last-resort measure [1]. Technology, knowledge about and experience in the handling of ECLS is evolving quickly, which is why an increasing number of indications are being treated with ECLS and more patients are considered eligible after weighing risks against potential benefits. The overall increase in ECLS deployments can be seen in the numbers regularly published by the Extracorporeal Life Support Organization (ELSO); these numbers reflect global ECLS deployment from centers registered with the ELSO. Irrespective of the various medical indications, more than 176,000 patients received ECLS between 1990 and today. After a first leap in deployments following the H1N1-pandemic 2008/09, ECLS was also an important therapy during the COVID-19 pandemic [2]. This increases the relevance of ECLS as a therapy and signifies the demand for expedited ECLS research models, especially as ECLS still suffers from many complications. [3]
Research and development on ECLS technology and therapy has been ongoing since its introduction in the 1970’s. Nonetheless, the survival rate keeps relatively stable at only 60 % [3,4]. No major breakthroughs since the introduction of hybrid dense polymethylpentene-membranes (PMP) have been introduced. Manifold knowledge gaps and hence innovation barriers exist in the context of ECLS [5], listed here from three perspectives: 1) Clinical research: ECLS is a relatively low volume therapy. In 2017 through 2021, only 85,318 cases have been recorded by ELSO, including a plausible sudden increase by COVID-19 patients [3]; this means smaller patient cohorts for any clinical study and a non-economic cost-benefit ratio for research in the field. The patient population is also highly heterogenic and the underlying causes for a patient to require ECLS are also manifold. Hence, forming patient collectives with similar baseline characteristics is often unfeasible. (Multiple) blinding is practically impossible due to immediate unblinding. ECLS is a high-risk, last-resort therapeutic measure; patient selection for the merit of a study is ethically difficult. As only critical patients with primary pathologies are treated with ECLS, the actual cause of death despite or due to ECLS therapy is often difficult to isolate. 2) Modelling: ECLS is a very problematic therapy regarding hemocompatibility and blood damage. Extremely large artificial surfaces in the extracorporeal systems are coupled with non-physiologic flow fields, which have not yet been decrypted in depth. Testing this hemocompatibility mostly requires animal trials. Normally, porcine models are used for preclinical testing [6]. These trials are cumbersome, expensive, ethically difficult, and require extensive planning. Current in-vitro test methods are not sufficiently conclusive. Further, many complications of ECLS occur days or weeks after therapy initiation. This implies that modeling of the processes leading to any given complication is often difficult or not feasible. 3) Technology: Different commercially available ECLS oxygenator designs show different inflammatory and hemocompatibility-related behavior for similar therapeutic applications [7,8] with limited knowledge on causes, pathways, extent, and impact. Further, an aggravating circumstance for impeded research on the key component of the technology, the gas exchanging hollow fiber membranes, is the unbalanced market for these fibers; the technology leader (Membrana GmbH, 3M, Wuppertal, Germany) has a de facto monopoly and the small market offers low incentives for innovation.
In order to overcome the obstacles listed above and to study both therapy and technology, researchers have started using rodent models in their ECLS studies, as listed in Table 1. Cardiopulmonary-bypass (CPB) models are not included in this table. Although ECLS originates from CPB and shares several features, the application period is in the range of hours for CPB and days to weeks in ECLS to name the primary distinguishing characteristic. Other differences may include the induction of cardioplegia and hypothermia on the clinical side and the deployment of open reservoirs and roller pump (vs. closed reservoirs and centrifugal pumps) in ECLS. For rodent models in CPB research, Ballaux et al. [9], Berner et al. [10], Samarska et al. [11], Jungwirth, de Lange [12], and Umei [13] provide excellent overviews of according publications.
However, most of the identified ECLS animal-models seem to use the same or similar miniaturized membrane oxygenators originally intended for CPB research. These devices are not optimal for longer experimental durations. The most distinguishing feature of chronically employed oxygenators is choice of the implemented fibers. Almost all identified small animal oxygenators use microporous polypropylene fibers (PP). These fibers are not stable after a few hours of use, mainly due to plasma leaking through the fibers, but also due to fouling and condensation on the gas side of the membranes. Hence, (sub-)chronic small animal models are currently not possible, while many of the complications of ECLS are occurring only after days or weeks after therapy initiation. This implies that modeling of the processes leading to any given complication is often difficult or not feasible. Historically, ECLS therapy gained importance in human care when PP was substituted as the membrane polymer by the hybrid polymethylpentene (PMP) membrane with solid outer phase for solution-diffusion mass transfer (see Evseev et al. for details [14]). The same principle is also applicable for in-vivo experiments. Note that it should be technically possible to implement other fibers at least in the self-manufactured models without redesigning.
Apart from the materials, the blood rheology within any oxygenator plays an important role in the initiation and propagation of hemostasis, thrombosis, hemolysis and inflammatory response. In contrast to CPB, almost half of all fatal complications in ECLS originate from therapy-induced coagulation or bleeding disorders [15]. Shear rates, low-flow and stagnation zones and washout properties of the oxygenator are defined by the flow path design. Most of the identified rodent-sized oxygenators are kept simple with an axial flow path along axially aligned hollow fibers, similar to common hemodialyzers but with the blood flow on the outer fiber surface. None of the designs is a scaled down version of the more sophisticated ECLS units with optimized flow paths that are currently on the market. This may also explain why all of the previously publications focus rather on the clinical aspects of their study and less on the oxygenator technology. Only one of the oxygenator performances has been evaluated in-vitro (see Fujii et al. (2021) in Table 1 [16], referencing original work by Yamada et al. [17]), as is standard for full-size devices in clinical use, standardized in the DIN EN ISO 7199 [18].
All studies stated in the table are either preliminary or proof-of-concept efforts. The short experimental durations may reflect the lack of long-term stability of the oxygenators. Design details are not consistently available: Two of the oxygenators are still commercially available (“Membrane oxygenator for small animal experiments”, Xi'an Xijing Medical Appliance Co., Ltd, Xi’an, Shaanxi, China [19] and “Gas Exchange Oxygenator, Miniature”, Living Systems Instrumentation, Catamount Research and Development, Inc., St. Albans, Vermont, USA [20]). For three other oxygenators, no information on their commercial availability could be obtained (in Table 1, see “SAMO”, used by Fichter et al., Warenits et al., Magnet et al. and Edinger et al. 2020 and 2021, as well as “Micro-1”, used by Chang et al., Cho et al., Fujii et al. 2020, Edinger et al. 2020 and 2022). One oxygenator is a miniaturized hemodializer (see Vu et al. in Table 1). The remaining devices are presented as in-house fabrications without details on the design and manufacturing process.

Table 1.
Identified rodent sized ECLS models with details on test setup and oxygenator specifications. ECC: Extracorporeal circuit; ECPR: Extracorporeal cardiopulmonary resuscitation; CPB: Cardiopulmonary bypass; VV-ECMO: Veno-venous extracorporeal membrane oxygenation; VA-ECMO: Veno-arterial ECMO; ECCO2R: Extracorporeal carbon dioxide removal; AV-cannulation: Arterio-venous ECMO.
Table 1.
Identified rodent sized ECLS models with details on test setup and oxygenator specifications. ECC: Extracorporeal circuit; ECPR: Extracorporeal cardiopulmonary resuscitation; CPB: Cardiopulmonary bypass; VV-ECMO: Veno-venous extracorporeal membrane oxygenation; VA-ECMO: Veno-arterial ECMO; ECCO2R: Extracorporeal carbon dioxide removal; AV-cannulation: Arterio-venous ECMO.
| Authors | Year | Animal model | ECLS support mode | Oxygenator design and membrane type | Priming volume | Effective membrane surface area | Flow during experiment | Duration of experiment | Tested DIN EN ISO 7199 | Ref. |
|---|---|---|---|---|---|---|---|---|---|---|
| Ali et al. | 2014 | Sprague-Dawley rat | ECPR | Undisclosed design/vendor. Images show axial intraluminar flow oxygenator. Silicone membrane. | 8ml | Undisclosed | 5-6ml/min. Note: Flow was recorded at targeted ECPR-induced arterial pressure of 25-30mmHg. | 7.3±2.8min ECPR + 30 min weaning | Undisclosed | [21] |
| Fichter et al. | 2016 | Fischer-344-rat | Extracorporeal organ perfusion | Oxygenator named "Small Animal Micro Oxygenator” (SAMO). 3-layer of stacked membrane mats of undisclosed size (5-10cm edge length, approximated from published image). Polypropylene membranes. | 10ml for the entire ECC | Undisclosed | 2ml/min to perfuse isolated free flap | 8h | Undisclosed | [22] |
|
Warenits et al. |
2016 | Sprague–Dawley rat | ECPR | "SAMO"-oxygenator, please refer to Fichter et al. in this table. Membrane type undisclosed in this publication; group has worked with the same device with polypropylene fibers (see Magnet et al. and Fichter et al. in this table). | Undisclosed | Undisclosed | 100ml/kg/min | 10min + 43- 83 min weaning |
Undisclosed | [23] |
|
Wiegmann et al. |
2016 | In vitro | N/A | In-house design. Single-fiber-mat design. Not for actual ECLS therapy, but for experimental endothelialization of hollow fiber surfaces (oxygenator-like flow chamber). Membranes heparin/albumin-coated polymethylpentene fibers with experimental endothelialization. | 4.275ml | 18.75cm² fiber mat area which translates to 40cm² effective membrane surface area | 15, 30, 60, 90ml/min | 96h | Undisclosed | [24] |
| Magnet et al. | 2017 | Sprague–Dawley rat | ECPR, typical CBP features | "SAMO"-oxygenator, please refer to Fichter et al. in this table. Polypropylene membrane. | Undisclosed, 15ml for the entire ECC | Undisclosed | 100ml/kg/min with rats between 460 and 510g. | Max. 10 min + 30min weaning | Undisclosed | [25] |
| Chang et al. | 2017 | Wistar–Kyoto rat | ECPR | "Micro-1"-Rat oxygenator (Dongguan Kewei Medical Instrument Co., Ltd., Guangdong, China). Current commercial availability unclear. Axial flow oxygenator, with unknown intra- and extraluminar phases. Membrane type undisclosed in this publication; a different group also listed in this table has worked presumably with the same device by the same vendor with polypropylene fibers (Cho2021). | Undisclosed, 19-20 ml for the entire ECC | Undisclosed in this publication; Cho et al., also listed in this table, have worked likely with the same device by the same vendor with 500cm². | Undisclosed | 30min | Undisclosed | [26] |
| Madrahimov et al. | 2018 | C57BL/6 mouse | VV-ECMO | CPB-oxygenator, in-house design, axial intraluminar flow. Polypropylene membrane. Further information in other publications of Madrahimov et al. [27,28] | Undisclosed, <0.3ml in referenced [27] |
Undisclosed, 50 fibers of 80 mm each of undisclosed outer diameter | 1.5-5ml/min | 2h ECC + 5min weaning | Undisclosed | [29] |
|
Natanov et al. |
2019 | C57BL/6 mouse | VV-ECMO | CPB-oxygenator, in-house design, axial intraluminar flow. Polypropylene membrane. Please refer to Madrahimov et al. in this table for further information. | Undisclosed, 500µl for the entire ECC | Undisclosed, 50 fibers of 80 mm each of undisclosed outer diameter | Undisclosed, 3-5ml/min in [29] | 4h | Undisclosed | [30] |
| Vu et al. | 2019 | Sprague–Dawley rat | ECCO2R/ Dialysis | “M10” miniaturized dialyzer (Gambro, Lakewood, USA). Only previously described by the group in May et al. [31] and by Goldstein et al. [32]. Axial intraluminar flow oxygenator for neonates. Membrane so-called "AN69" hydrophilic hollow fiber made of s a copolymer of acrylonitrile and sodium methallyl sulfonate. See Thomas et al. [33] for details. | Undisclosed, but the device was designed for infants of 2-15kg. | 420cm² | 1ml/min | Undisclosed | Undisclosed | [34] |
|
Wollborn et al. |
2019 | Sprague–Dawley rat | VA-ECMO vs. ECPR | “OX” miniature gas exchange oxygenator, Living Systems Instrumentation, St. Albans City, Vermont, USA. Not further described in the study. Product description by the vendor shows an axial extraluminar flow oxygenator and a polypropylene membrane [20]. | Undisclosed, 6ml for entire ECC. Product sheet by the vendor: 1.6ml |
Undisclosed. Supplier: 115cm² [20] |
10-18ml/min, to reach target mean arterial pressure of 65 mmHg | 2.5h + undisclosed weaning | Undisclosed | [35] |
| Fujii et al. | 2020 | Sprague–Dawley rat | VA-ECMO | “Micro-1” (Senko Medical Instrument Mfg. Co., Ltd, Tokyo, Japan). Image shows an axial flow oxygenator, apparently with intraluminar flow. The oxygenator seems shorter but larger in diameter than other axial flow oxygenators in this table. The oxygenator could not be identified on the vendor’s product lists. Membrane type undisclosed. | Undisclosed, 8ml for entire ECC | Undisclosed | 70ml/kg/min | 2h | Undisclosed | [36] |
|
Edinger et al. |
2020 | Lewis rat | VA-ECMO | The “Micro-1” (please refer to Chang et al. in this table) was tested against the “SAMO” (please refer to Fichter et al. in this table) without further device specifications. Both membrane types undisclosed, both polypropylene in other publications with the same devices (Magnet et al and Cho et al. in this table) | SAMO: 7ml Micro-1: 3.5ml |
SAMO: 500cm² Micro-1: Published with 50cm² in potentially erroneous contrast to Cho et al. who published 500cm². |
90ml/kg/min | 2h | Undisclosed, gas transfer evaluated in CPB-study [37]. | [38] |
|
Wilbs et al. |
2020 | New Zealand white rabbit | VV-ECMO | In-house design with 40 stacked fiber mat layers. Despite incorporating genuine hollow fibers, the oxygenator was built non-functional regarding gas-transfer. It can be considered a simplified mock-oxygenator for hemocompatibility testing.. Polymethylpentene membrane. This fiber arrangement and fiber bundle design is similar to the RatOx-oxygenator. The stacked fiber mat layers have a cross-sectional flow area that is half of the RatOx. In consequence, the oxygenator requires twice as many fiber mat layers for the same effective surface area with potentially higher pressure drop. | Undisclosed | 263cm2. | 45ml/min | 4h | Undisclosed | [39] |
| Li et al. | 2021 | Sprague-Dawley rat | VV-ECMO | CPB-oxygenator, axial extraluminar flow. Produced by Xi'an Xijing Medical Appliance Co. Limited, Xi'An, China. The membrane type is undisclosed in the publication but following an inquiry at the supplier, polypropylene fibers are used. | 3ml | 200cm² | 80–90ml/kg/min | 3.5h | Undisclosed. | [40] |
| Cho et al. | 2021 | Sprague-Dawley rat | VA-ECMO vs. VV-ECMO | "Micro-1"-oxygenator; please refer to Chang et al. in this table. Polypropylene membrane. | 3.5ml | 500cm² | 50ml/min | 2h | Undisclosed | [41] |
| Fujii et al. | 2021 | Sprague-Dawley rat | VV-ECMO | Axial, extraluminar flow oxygenator. Note that in this publication, the figure suggests an intraluminal flow, while the original publication by Yamada et al. clearly states an extraluminar flow. This original publication covers two further slightly larger oxygenator variants. They also state that polypropylene fibers are used. [17] | Undisclosed, 8ml for entire ECC. Yamada et al. state a priming volume of 3ml [17]. | Undisclosed. Yamada et al.: 236cm² [17] |
50-60ml/kg/min | 2h | Yes, in Yamada et al. [17] | [16] |
| Umei et al. | 2021 | Sprague-Dawley rat | Mock-ECLS, pump-supported AV-cannulation | 3D-printed flow cell designed to simulate the local geometry, blood flow patterns and surface area to blood volume ratio of a commercially available oxygenator hollow fiber bundle. Unable to transfer gas. The membrane type is non-functional, clear acrylate resin (PR-48, Colorado Polymer Solutions, Boulder, CO). | 0.3ml for the oxygenator, 2.5ml for the entire ECC | 15cm² | 1.9ml/min | 8 h | Undisclosed | [13] |
|
Edinger et al. |
2021 | Lewis rat | VA-ECMO | "SAMO"-oxygenator; please refer to Chang et al 2017 in this table. Polypropylene membrane. | Undisclosed, 11ml for the entire ECC |
Undisclosed, 500cm² in publication of Edinger et al. (2020) in this table | 90ml/min | 2h | Undisclosed | [42] |
|
Govender et al. |
2022 | Syrian golden hamster | VA-ECMO | ECC-setup without oxygenator. | Not applicable | Not applicable | 15% of CO | 1.5h ECC | Not applicable | [43] |
| Greite et al. | 2022 | C57BL/6 mouse | VV-ECMO | Redesigned from [28]; CPB-oxygenator, in-house-design, axial intraluminar flow. Polypropylene membrane. | 200µl | Undisclosed, 50 fibers of 80mm each of undisclosed outer diameter | Undisclosed, 2.34-6.5ml/min in [28] | 2h ECC + 2h weaning | Undisclosed | [44] |
| Huang et al. | 2022 | Sprague-Dawley rat | VV-ECMO | See details from Li et al. in this table. | See details from Li et al. in this table. | See details from Li et al. in this table. | See details from Li et al. in this table. | 3h | Undisclosed | [45] |
| Zhang et al. | 2022 | Sprague-Dawley rat | VV-ECMO | See details from Li et al. in this table. | See details from Li et al. in this table | See details from Li et al. in this table | 80–90ml/kg/min | 2h | Undisclosed | [46] |
|
Edinger et al. |
2022 | Lewis rat | VA-ECMO | "Micro-1 "-oxygenator; please refer to Chang et al. 2017 in this table. Polypropylene membrane | 9ml | Undisclosed, 500cm² in publication by Cho et al. in this table | 90ml/min | 2h | Undisclosed | [47] |
|
Kharnaf et al. |
2022 | C57BL/6 mouse | VA-ECMO | “OX” miniature gas exchange oxygenator; please refer to Wollborn et al. in this table. | 1.6ml oxygenator priming (NaCl, Hetastarch,), 2 ml in remaining ECC (blood from two donor mice) | 115cm² (supplementary Materials) | 3–5ml/min | 1h | Undisclosed | [48] |
|
Alabdullh et al. |
2022 | In vitro | N/A | In-house design. Single-fiber-mat design. Not for actual ECLS therapy, but for experimental endothelialization of hollow fiber surfaces (oxygenator-like flow chamber). The oxygenator design is an advancement of the previously published device by Wiegmann et al. in this table. Heparin/albumin-coated polymethylpentene fibers with endothelialization. | 4ml | 19cm² | Static | 6h and 24h | Undisclosed | [49] |
In order to overcome the technical limitations of current rodent oxygenators stated above, we developed the so-called “RatOx”, which is specifically designed to be used individualized for a variety of rodent models. Additionally, some further design features were integrated for improved versatility, usability and for allowing studies with focus on the oxygenator technology in addition to clinical research.
The oxygenator offers several degrees of freedom on sizing and hollow fiber properties. Its design is scaled down from state of the art human care oxygenators. The novel oxygenator is scalable for different rodents. It can be produced with a minimal amount of hollow fibers for experiments such as the cellularization/endothelialization of surfaces [24,49]; or it can be produced for maximum efficacy as in full support scenarios of larger rodents. Care was taken, to design an oxygenator that many groups can use and potentially even manufacture themselves. We intend to have the RatOx oxygenator used as a standard testing platform, both in vitro and in vivo. This allows cross-model and cross-institutional data pooling and analyses.
In this publication, we describe the novel rodent-dedicated oxygenator and preliminary results of in-vitro classification experiments for the most relevant performance parameters i.e. gas transfer and priming volume. To assess the transferability of the system into other institutes, we compare our initial results with the ones obtained by an independent laboratory who performed an additional test series with a different set of equipment but the same oxygenator design and methods.
Materials and Methods
Oxygenator design:
Based on the identified existing devices for rodent ECLS models and their applicability restrictions, we deducted and synthesized requirements for a novel system with the aim to overcome as many limitations as possible. We further defined requirements that exceed these limitations. A summary of all design targets can be found in Table 2.
The requirements on sizing and dimensions were deducted from the physiology of laboratory animals in sized between mice and guinea pigs. The respective values were amalgamated from various sources in the literature, including the studies listed in Table 1. All identified values are listed in Table 3 below. Because the majority of studies in Table 1 worked with Sprague-Dawley rats, a full-support ECLS-scenario for a young rat was defined as intended upper functionality boundary.
In-vitro proof-of-concept:
Further, in-vitro experiments to evaluate the performance of the RatOx oxygenator were conducted. We adapted the test setups from our established protocols for human full size oxygenators [62,63,64]. The latter are in accordance with the DIN EN ISO 7199 [18], which is part of the regulatory process for commercialized ECLS oxygenators.
All experiments were conducted with fully heparinized (15.000 IU/l, Ratiopharm, Ulm, Germany) fresh porcine whole blood from a local slaughterhouse, treated immediately with 1.6 ml/l gentamicin (Ratiopharm, Ulm, Germany), 1.8 ml/l 50 % Glucose (B.Braun, Melsungen, Germany) and 100 ml/l 0.9 % NaCl (B.Braun, Melsungen, Germany). The hemoglobin concentration was kept at 12 +/- 1 mg/dl blood, the temperature at 37 +/- 1 °C, and the Base Excess at 0 +/- 5 mmol/l using 8.4 % hydrogencarbonate (B.Braun, Melsungen, Germany). The test loop comprised a blood pump, the to-be-tested oxygenators, a heat exchanger, ports for sampling prior and after to the oxygenators, and sensors for pressures, flows, and temperature. For the gas transfer tests, a second circulation was used to obtain physiologic venous blood gas levels before each oxygenator, as defined in ISO 7199 (SO2 = 65 +/- 5 %, pCO2 = 45 +/- 5 mmHg) [18]. Both circulations were connected to form a cross circuit using a self-built spillover hard-shell reservoir from which the test loop draws conditioned blood. The adherence of venous values in the conditioned blood was closely monitored. We recorded values for oxygen transfer, carbon dioxide elimination and pressure loss on the blood side for different numbers of fiber mats and different blood flows. For blood gases, an ABL Flex 825 (Radiometer GmbH, Willich, Germany) was used. To calculate oxygen and carbon dioxide transfer (VO2 and VCO2), we used the absolute gas concentration values for physically dissolved and hemoglobin-bound oxygen as well as physically dissolved and chemically bound carbon dioxide (ctO2 and ctCO2). Gas transfer values are calculated with venous and arterial samples drawn immediately before and after the oxygenators. Differently sized oxygenators (29, 42, and 55 fiber membrane layers) were tested over a range of blood flows through the oxygenator. The tested blood flows were 60, 80, 90, and 100 ml/min. The according sweep gas flow was at a ratio of s21 (gas flow/blood flow) with pure oxygen. To test whether the oxygenator shows a linear correlation for higher flows, we also tested 500 ml/min for the 42 layer RatOx.
One additional test series was performed at an external cooperating institute the Engineering Organ Support Technologies group at the University of Twente, the Netherlands. The Engineering Organ Support technologies group applied the same RatOx design and manufacturing process for their in-vitro blood tests as the one used by the University Hospital RWTH Aachen, with individual alterations to them permitted. The aim of this knowledge transfer within the present study was to evaluate the feasibility of cross-institutional RatOx-utilization. Apart from technical information, nothing else was provided, including parts, manufacturing tools, or materials. The University of Twente implemented and customized according manufacturing modalities to their individual conditions. Specifically, they altered the potting process for the fiber bundle thereby expediting the potting process and building fiber bundles with 56 fiber mat layers, above the originally intended maximum of 55 layers. Further, they used Elastosil 625 silicone (Mc Technics, Visé, Belgium), which has more rigid mechanical properties than the Elastosil 620 used in University Hospital Aachen. Most other manufacturing process modalities are similar and can be requested from our research groups. This way, ten identical fiber bundles were produced. Because the fibers are the most influencing factor of the oxygenator, the same uncoated PMP fibers were implemented (Membrana GmbH, 3M, Wuppertal, Germany). Apart from the oxygenator, the University of Twente implemented a test circuit also based on the DIN EN ISO 7199 [18]. In difference to the test procedure in Aachen, the blood-gas-analyzer was an i-STAT Alinity POC (Abbott, Illinois, USA), the heat exchanger heated the blood in the conditioning loop and not proximal to the test section, and the tested blood flows were 60, 100, 140 and 180 ml/min with a constant sweep gas flow of 500 ml/min. During these experiments, oxygen and carbon dioxide transfer rates were recorded.
Last, we tested several manufactured RatOx-devices using water for their priming volume in order to confirm the analytically derived Equation 1 (Results section below). We defined the inner volume of the RatOx to be the entity of extraluminar fluid within all blood-leading parts and between the entry and exit ports where the circuitry (blood tubes) are connected.
3. Results
Oxygenator design:
The RatOx oxygenator is a scaled-down version of a stacked-design oxygenator with round potting. The basic design therefore reflects the state-of-the-art [65] and is, for example, comparable with the Hemovent-oxygenator for adult patients [66]. Figure 1 shows an image of a fully assembled RatOx oxygenator produced in our laboratory. Figure 2 depicts its assembled components, cut at the middle plane, rested on a rig: the cylindrical housing (dark transparent grey) holds the fiber bundle (white/blue) that is compressed by two disc-shaped lids (red), which also host the in- and outlet Luer connectors for standard ¼” tubing. The compression force is provided by a large hand-operated screw (green) that moves relatively to the housing caps (yellow). The fiber bundle, which is adaptable in size by changing the number of fiber mat layers, is further depicted in Figure 3 in a medium sized version with 29 layers.
The dimensioning of the RatOx oxygenator was based on the physiology of rats and related rodents (Table 3). The effective gas transfer was estimated based on available gas transfer data in the literature (e.g. Evseev et al. [14]). The size of the oxygenator can be varied by the number of fiber mat layers, according to the intended experimental model. It is further possible to select fiber module sizes for individual animals based on their body weight in a heterogenic distributed animal cohort. The RatOx oxygenator allows any number of fiber mats between 1 and 55, depending on the demand of the ECLS or animal model; for example, using standard polymethylpentene (PMP) fibers (Membrana GmbH, 3M, Wuppertal, Germany) with an outer diameter of 380 µm and a fiber spacing of 200 µm results in an effective gas exchange surface between 10.6 cm² and 580 cm² (linear correlation). Within the present study, all further calculations and tests were conducted with these PMP fibers. The fiber mats are normally intermittently rotated by 90°, though technically any angle between fiber mats could be applied. Gas and blood side of the hollow fibers are separated by a potting process using colored silicone (Elastosil RT 620, Wacker Chemie AG, Munich, Germany); as well, the gas inlet and outlet is separated by this potting. Figure 3 shows a single fiber module with 29 fiber mat layers. After the round potting, the flow path through the fiber bundle has a diameter of 25 mm, while the height is dependent on the number of fiber mats.
The priming volume of an empty RatOx was derived from CAD-drawings to be 1.0 ml; every fiber mat layer adding 0.075 ml of priming volume (Equation 1). The priming volume is calculated from the top edge of the upper connector, to the bottom edge of the lower connector, i.e. all fluid compartments within the red and blue/white parts of the RatOx depicted in Figure 2.
This priming volume affects the clinically relevant hemodilution, described by Equation 2 below.
For hollow fibers, any commercially available fiber type can be implemented, as long as the fibers are knitted to fiber mats. Mostly, oxygenator fibers are made of PMP for long-term applications, or microporous polypropylene (PP) for short-term applications [14]. These fibers can be obtained as single layer fiber mat spools (Membrana GmbH, 3M, Wuppertal, Germany). Alternatively, commercially available oxygenators can be cut open and fibers can be scavenged. This way, the post-production alterations to the fiber mats by the oxygenator manufacturer, like anti-thrombotic coatings [14,67,68], can be transferred to the rodent model. For laboratories developing and studying their own fibers, surface alterations, or coatings, all fibers can be integrated as long as they are knitted to fiber mats [67,69,70,71].
For cost efficacy, the fiber bundle is the only component designed as a disposable. For air-free priming and detecting leakages, transparent polymethylmethacrylat (PMMA) for the housing was selected. Components with direct blood contact further need to be hemocompatible, which is why we used PMMA or polycarbonate (PC). All reusable parts need to be sterilizable. We chose polyoxymethylene (POM) as a material for components without blood contact and without the need for transparency (screw and outer caps). To reduce cost and to be able to analyze the fiber bundle post-experiment (see Figure 4), the RatOx housing can be disassembled non-destructively. All parts of the oxygenator can be manufactured with a 3-axis machining center without the need for other complex equipment.
In-vitro proof-of-concept:
The priming volume calculated by Equation 1 was tested for random fabricated fiber modules and the function (Equation 1) could be confirmed for every device. For that, we defined the inner volume of a RatOx to begin with the outer rim of the Luer connector on the blood leading parts and to stop on the outer rim of the opposite connector. In Figure 2, this means the extraluminar space with all red and white components.
Further, the gas transfer efficacy was experimentally evaluated. Figure 5 shows the results. Depicted are oxygen transfer (circles, positive values) and carbon dioxide transfer (triangles, negative values) for four different oxygenator blood flows and three different fiber mat layer numbers (29, 42, 55 layers). Blood flows of 60, 80, 90, 100 ml/min were evaluated. The zoomed-out graph shows the same results with an additional operating point of 500 ml/min for a 42-layer RatOx.
Using the same example as above, for a 55-layer module (n=1) and 100 ml/min blood flow, the gas transfer of the RatOx oxygenator is approximately 5.53 ml/min for oxygen and -5.50 ml/min for carbon dioxide, respectively. The same 55-layer RatOx at a blood flow of 60 ml/min yielded in average 3.88 ml/min oxygen transfer and -3.76 ml/min carbon dioxide transfer. 29-layer RatOx (n=4) showed values of 3.65 ± 0.28 ml/min oxygen transfer, -2.52 ± 1.05 ml/min carbon dioxide transfer (both at 100 ml/min) and 2.85 ± 0.32 ml/min oxygen transfer, -3.05 ± 0.39 ml/min carbon dioxide transfer (both at 60 ml/min), respectively.
The additional test in a second, independent laboratory showed the following results, depicted in Figure 6, augmented with the comparable experiments in the original institute (extracted from Figure 5):
For increasing blood flows, the oxygenators perform in an almost linear correlation regarding oxygen and carbon dioxide transfer rates. The mean oxygen transfer rate for 60 ml/min is 4.30 ml/min (standard deviation ± 0.41 ml/min), for 100 ml/min 6.27 ml/min (standard deviation ± 0.98 ml/min), for 140 ml/min 8.83 ml/min (standard deviation ± 1.77 ml/min) and for 180 ml/min 9.33 ml/min (standard deviation ± 0.73 ml/min). The comparable values from Aachen for 60 ml/min and 100 ml/min are 3.88 ml/min and 5.53 ml/min, respectively. The mean carbon dioxide transfer rate for 60 ml/min is -4.87 ml/min (standard deviation ± 1.10 ml/min), for 100 ml/min -8.20 ml/min (standard deviation ± 1.97 ml/min), for 140 ml/min -8.64 ml/min (standard deviation ± 3.50 ml/min) and for 180 ml/min -10.28 ml/min (standard deviation ± 3.37 ml/min). The comparable values from Aachen for 60 ml/min and 100 ml/min are -3.76 ml/min and -5.50 ml/min, respectively. All values are further listed in Table 4.
4. Discussion
Overall, based on the results above, the RatOx oxygenator is functioning as expected. All values were within the intended range or exceeding it. In the following, the results are discussed in more detail, reflecting on the predefined design requirements in Table 2 and the experiment results.
State of the art design: The oxygenator design is directly comparable to recently marketed devices like the oxygenators by Nautilus (MC3, Dexter, USA) and Hemovent (Hemovent, Aachen, Germany, recently acquired by Shanghai MicroPort Medical Group Co., Ltd.). [65,66] Interchangeable fiber type: Every type of hollow fiber with any surface modification can be implemented with minor restrictions to the freedom of choice, e.g. the requirement that the fibers are woven to mats. Variable gas exchange surface: The RatOx comes in 55 different sizes with a minimum of 10 cm² and a maximum of 580 cm² for standard PMP fibers by Membrana (Membrana GmbH, 3M, Wuppertal, Germany). The University of Twente has shown that, with an altered fiber bundle potting process, even larger stacks with more than 55 layers are possible. Low priming volume: For larger rodents, like rats, the priming volume <6 ml translates into hemodilutions below 25 %, which meets the predefined requirements. For smaller animals, such as mice, the minimum static priming volume of 1 ml can easily cause hemodilution around 50 %, which is clinically more difficult to handle, depending on the experimental setup. Low pressure loss: Unfortunately, we lack continuous data regarding the pressure drop over the RatOx oxygenator and cannot comment on the results. Hemocompatibility: As well, we did not yet reach the stage to conduct hemocompatibility tests and can therefore not comment. However, care was taken to only use materials in blood contact known to be hemocompatible. In addition, the flow path design was adapted from optimized full-sized ECLS devices and we do not expect hemocompatibility issues. Transparent housing: It is possible to directly detect entrapped gas bubbles in the blood flow between the edges of the fiber bundle and the cylindrical casing. It is also possible to detect undesired leaks due to defective fibers and seals. Reusable housing and removable fiber bundle: apart from the fiber bundle, all components of the RatOx-oxygenator are designed for repeated use. The fiber bundle can easily be explanted post-experiment for further analyses, as was shown in Figure 4.
Effective gas transfer: For a given operating point of 100 ml/min blood flow, the oxygen transfer was measured to be 5.53 mlO2/min. This is only around 70 % of the intended full support of a 280 g rat (Table 3) with 55 layers and 100 ml/min blood flow. The results from Twente suggest a 10 % higher gas transfer performance. The mean gas transfer rates at the given 100 ml/min blood for n=10 56-layer oxygenators showed values of 6.27 ml/min. The determined demand of 7.90 ml/min as a design requirement specification was based on a single publication (Bedford et al. from 1979 [50]) for awake, resting rats. The actual oxygen demand may be higher or lower, especially when the rat is differently treated, for example with sedation or hypothermia. Apart from the full-support ECLS-mode, partial support therapies definitely work with the introduced system. This is why and how even larger animals, e.g. rabbits, can be used with the RatOx system. Wilbs et al. [39], also listed in Table 1, gave an according example, where they treat New Zealand White Rabbits with a systemic anticoagulant, monitoring the hemocompatibility of a non-functional ECLS unit.
We also tested two 42-layer oxygenators with an operating point far out of the relevant range for rodents. Generally, the oxygen uptake for a given batch of blood increases with a slower blood flow through the oxygenator as there is more time for the mass transport. This correlation is not valid for very low blood flows as the oxygen saturation reaches its limit before the blood has passed the later hollow fiber layers. A graph of arterial oxygen saturation over blood flow would start with a plateau at almost 100 %. It would then show a characteristic salient point at a certain blood flow from where the curve decreases linearly. To test the oxygenator for this expected linear correlation for higher blood flows, we added the operating point of 500 ml/min blood on the experiment day where we tested with the 42-layer oxygenator. This is far away from the normal cardiac output of rodents and thus out of the range of operating points that can be run in an in-vivo experiment; but the functional limit of the oxygenator for in-vitro-testing may be much higher. We are aiming to show that any required gas transfer efficacy up to an operating point of 500 ml/min can be reached.
Reproducibility, cross-lab usability and manufacturability: The experiment series in Twente University was conducted to see potentials and limitations to the transfer of laboratory-grade test oxygenators between institutions. Despite major obstacles of the technology transfer, like local conditions, and equipment, the obtained test results offer the opportunity to be discussed. The technology transfer was, at a minimum, sufficiently successful to conduct standardized experiments according to DIN EN ISO 7199, despite a comprehensive manufacturing process. Both the oxygen and the carbon dioxide transfer results of the devices from Twente showed a higher efficacy. In the case of the oxygen transfer, the differences were minor; the results from Aachen lie within the range of the standard deviation from Twente. For the carbon dioxide transfer, the same is only true for the lower operating point of 60 ml/min blood flow, but the tendency for a larger discrepancy is visible for higher flows. Since we only tested a single device in Aachen for a proof-of-concept, a statistical evaluation would be inconclusive. Yet, the potential differences between test results from Aachen and Twente are plausible:
First, the standardized test methodology in DIN EN ISO 7199 offers room for individual adjustments and adaptions. The blood handling, blood age, transport modalities after blood donation, process of blood collection, etc. may differ. Second, the experiment conduction itself may differ, as, for example, in the duration between sample collection and blood gas measurement, the test circuit setup, or the priming process. In this case, the heat exchanger was situated at two different locations with unmonitored effect on the gas uptake/elimination in the test devices. This is also a particularity of the RatOx-system, as it does not contain heat-exchanger-fibers as conventional oxygenators do. Third, the sweep gas flow rate was set to be at a gas/blood flow ratio 4:1 in Aachen, but kept constant over all operating points in Twente. While we know from the clinical experience with ECLS that the oxygen uptake is mainly dependent on the blood flow, the carbon dioxide elimination is mainly dependent on the sweep gas flow rate, or gas/blood flow ratio [72]. In our results, the carbon dioxide transfer efficacies do indeed diverge stronger than for oxygen.
Apart from the test circuit, the device itself may also cause differences in the results. The University of Twente has implemented adaptions and improvements to the manufacturing process that may have a (positive) influence on the gas transfer efficacy. For example, Twente used a more rigid silicone, which may have resulted in an improved fiber patency following the cutting process to reopen the fibers after potting, or as a counterforce to the compression after the device assembly. Also, one additional fiber mat was included in the devices of Twente, increasing the functional gas transfer surface area by ~2 %; on the other hand, the average flow path cross section area was 1 mm smaller, effectively reducing the functional gas transfer surface area of the fiber bundle by 4 %. Both effects should neutralize each other partly.
5. Conclusions and outlook
This publication introduces the design of a novel dedicated rodent oxygenator. We conducted preliminary experiments to prove our concept. Overall, we conclude that the RatOx oxygenator is a potential new tool for advanced small animal in-vivo testing as well as expedited in-vitro testing of artificial lung support.
The RatOx oxygenator is designed to be a highly versatile, reproducible oxygenator that aims to become a standard tool in ECLS research and development. The defined requirements reflect this target. Our preliminary laboratory results are promising to allow for various different experimental setups, both in vivo and in vitro. The oxygenator is extremely versatile, as the fibers can be selected with minimal restrictions. Figure 5, Figure 6, Equation 1 and Equation 2 can be used to estimate the required fiber mat layer number for any animal model design, based on the required gas transfer performance demand and/or the maximum tolerable hemodilution. Physiologic values for relevant animals are listed in Table 3. Further, fibers can be altered through modifications and coatings. The adaptable size of the oxygenator allows for different models, e.g. different rodents, different ELCS support types, or even low-surface-area endothelialization. At the same time, the oxygenator is very similar in design to full-scale, commercially available oxygenators, allowing for direct comparisons.
We conclude that the RatOx oxygenator may enable research and development in much earlier technological phases, with higher throughput. This opens path for radical novel experimental setups and models, enhancing the scientific output for ECLS and, in the long run, for therapeutic outcome for patients suffering from severe sicknesses.
Beside in-vivo studies on rodents, a highly scaled down ECLS system also allows for increased-throughput in-vitro testing. The small priming volume means that several test circuits can be used in parallel and that human blood donations suffice for experiments. This allows parameter studies on, e.g. design features, material properties, hemocompatibility and more.
As an ECLS system can be used to bridge cardiorespiratory failure, it can be used to keep an entire organism perfused, effectively limiting necrotic and apoptotic processes and allowing for a near-physiological metabolism. With a rodent-sized ECLS system, euthanized animals can be used for studies requiring any form of metabolism, yet without keeping the animal alive. This way, animal trials can be reduced with positive ethical and economic implications.
We are now targeting to establish the RatOx in further in-vitro setups, e.g. hemocompatibility testing, and in different animal models. The major limitation of the presented experimental methods are the low number of repetitions, as we presented preliminary results. Further, we did not continuously measure the pressure drops, which is part of the standardized classification protocol. Our future aim is, on one hand, to provide comprehensive in-vitro and in-silico classification experiments and, on the other hand, to collect RatOx-specific technical data from collaborating institutes from their experiments with the RatOx-system.
To complement the system, we are further developing the remaining components of an ECMO circuit in rodent size (pump, reservoir, heat exchanger) to the same specifications.
We hope for many groups to adapt the RatOx platform to establish a database of results, enabling cross-laboratory and broader, collaborative research. The results from our experiment series in Twente are very promising in showing that a transfer of the technology to other institutions is feasible. Potentially, these very promising results are difficult to repeat for institutions with less experience and equipment for medical device manufacturing compared to the University of Twente; this problem can be overcome to a major degree by not only supplying technological information between laboratories, but actual equipment. As many groups have already used different other oxygenators, the handling of the circuit apart from the manufacturing process is well established across many laboratories. This is especially true if groups working primarily on CPB research are included as well.
Funding
This research received no external funding.
Data Availability Statement
Please contact the authors for data and designs of the RatOx oxygenator.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Tramm, R.; Ilic, D.; Davies, A.R.; Pellegrino, V.A.; Romero, L.; Hodgson, C. Extracorporeal membrane oxygenation for critically ill adults. Cochrane Database Syst. Rev. 2015, 1, CD010381. [Google Scholar] [CrossRef] [PubMed]
- Gannon, W.D.; Trindade, A.J.; Stokes, J.W.; Casey, J.D.; Benson, C.; Patel, Y.J.; Pugh, M.E.; Semler, M.W.; Bacchetta, M.; Rice, T.W. Extracorporeal Membrane Oxygenation Selection by Multidisciplinary Consensus: The ECMO Council. ASAIO J. 2023, 69, 167–173. [Google Scholar] [CrossRef] [PubMed]
- Extracorporeal Life Support Organization. ECLS registry report, international summary 2022. Available online: https://www.elso.org/registry/internationalsummaryandreports/internationalsummary.aspx (accessed on 20 March 2023).
- Bartlett, R.H. ECMO: The next ten years. The Egyptian Journal of Critical Care Medicine 2016, 4, 7–10. [Google Scholar] [CrossRef]
- Lescouflair, T.; Figura, R.; Tran, A.; Kilic, A. Adult veno-arterial extracorporeal life support. J. Thorac. Dis. 2018, 10, S1811–S1818. [Google Scholar] [CrossRef] [PubMed]
- Millar, J.E.; Bartnikowski, N.; Bahr, V. von; Malfertheiner, M.V.; Obonyo, N.G.; Belliato, M.; Suen, J.Y.; Combes, A.; McAuley, D.F.; Lorusso, R.; et al. Extracorporeal membrane oxygenation (ECMO) and the acute respiratory distress syndrome (ARDS): a systematic review of pre-clinical models. Intensive Care Med. Exp. 2019, 7, 18. [Google Scholar] [CrossRef] [PubMed]
- Yildirim, F.; Amanvermez Senarslan, D.; Yersel, S.; Bayram, B.; Taneli, F.; Tetik, O. Systemic inflammatory response during cardiopulmonary bypass: Axial flow versus radial flow oxygenators. Int. J. Artif. Organs 2022, 45, 278–283. [Google Scholar] [CrossRef]
- Rungatscher, A.; Tessari, M.; Stranieri, C.; Solani, E.; Linardi, D.; Milani, E.; Montresor, A.; Merigo, F.; Salvetti, B.; Menon, T.; et al. Oxygenator Is the Main Responsible for Leukocyte Activation in Experimental Model of Extracorporeal Circulation: A Cautionary Tale. Mediators Inflamm. 2015, 2015, 484979. [Google Scholar] [CrossRef]
- Ballaux, P.K.; Gourlay, T.; Ratnatunga, C.P.; Taylor, K.M. A literature review of cardiopulmonary bypass models for rats. Perfusion 1999, 14, 411–417. [Google Scholar] [CrossRef]
- Berner, M.; Clément, D.; Stadelmann, M.; Kistler, M.; Boone, Y.; Carrel, T.P.; Tevaearai, H.T.; Longnus, S.L. Development of an ultra mini-oxygenator for use in low-volume, buffer-perfused preparations. Int. J. Artif. Organs 2012, 35, 308–315. [Google Scholar] [CrossRef]
- Samarska, I.V.; Henning, R.H.; Buikema, H.; Bouma, H.R.; Houwertjes, M.C.; Mungroop, H.; Struys, M.M.R.F.; Absalom, A.R.; Epema, A.H. Troubleshooting the rat model of cardiopulmonary bypass: effects of avoiding blood transfusion on long-term survival, inflammation and organ damage. J. Pharmacol. Toxicol. Methods 2013, 67, 82–90. [Google Scholar] [CrossRef]
- Jungwirth, B.; Lange, F. de. Animal models of cardiopulmonary bypass: development, applications, and impact. Semin. Cardiothorac. Vasc. Anesth. 2010, 14, 136–140. [Google Scholar] [CrossRef]
- Umei, N.; Lai, A.; Miller, J.; Shin, S.; Roberts, K.; Ai Qatarneh, S.; Ichiba, S.; Sakamoto, A.; Cook, K.E. Establishment and evaluation of a rat model of extracorporeal membrane oxygenation (ECMO) thrombosis using a 3D-printed mock-oxygenator. J. Transl. Med. 2021, 19, 179. [Google Scholar] [CrossRef] [PubMed]
- Evseev, A.K.; Zhuravel, S.V.; Alentiev, A.Y.; Goroncharovskaya, I.V.; Petrikov, S.S. Membranes in Extracorporeal Blood Oxygenation Technology. Membr. Membr. Technol. 2019, 1, 201–211. [Google Scholar] [CrossRef]
- Olson, S.R.; Murphree, C.R.; Zonies, D.; Meyer, A.D.; Mccarty, O.J.T.; Deloughery, T.G.; Shatzel, J.J. Thrombosis and Bleeding in Extracorporeal Membrane Oxygenation (ECMO) Without Anticoagulation: A Systematic Review. ASAIO J. 2021, 67, 290–296. [Google Scholar] [CrossRef]
- Fujii, Y.; Sumikura, H.; Nagahama, D. Establishment of a novel miniature veno-venous extracorporeal membrane oxygenation model in the rat. Artif. Organs 2021, 45, 63–67. [Google Scholar] [CrossRef] [PubMed]
- Yamada, T.; Sumikura, H.; Fujii, Y.; Arafune, T.; Ohgoe, Y.; Yaguchi, T.; Homma, A. Fundamental Examination of an Extracapillary Blood Flow Type Oxygenator for Extracorporeal Circulation Model of a Rat. Journal of Life Support Engineering 2018, 30, 96–104. [Google Scholar] [CrossRef]
- DIN EN ISO 7199:2020-10: Kardiovaskuläre Implantate und künstliche Organe - Blut-Gas-Austauscher (Oxygenatoren), 2020-10; Beuth Verlag GmbH: Berlin, 11.040.40. Available online: https://www.beuth.de/de/norm/din-en-iso-7199/317329787.
- XiJing Medical. Xi'an xijing medical appliance co.,ltd of product catalogue 2022.10 - Membrane oxygenator for animal experiments. Available online: https://www.alibaba.com/product-detail/Membrane-oxygenator-for-animal-experiments_62468042966.html?spm=a2700.shop_index.74.6.3c5e1627VqckuQ (accessed on 29 January 2023).
- Living Systems Instruments. Gas Exchange Oxygenator, Miniature. Available online: https://livingsys.com/product/miniature-gas-exchange-oxygenator/ (accessed on 29 January 2023).
- Ali, A.A.; Downey, P.; Singh, G.; Qi, W.; George, I.; Takayama, H.; Kirtane, A.; Krishnan, P.; Zalewski, A.; Freed, D.; et al. Rat model of veno-arterial extracorporeal membrane oxygenation. J. Transl. Med. 2014, 12, 37. [Google Scholar] [CrossRef] [PubMed]
- Fichter, A.M.; Ritschl, L.M.; Borgmann, A.; Humbs, M.; Luppa, P.B.; Wolff, K.-D.; Mücke, T. Development of an Extracorporeal Perfusion Device for Small Animal Free Flaps. PLoS One 2016, 11, e0147755. [Google Scholar] [CrossRef]
- Warenits, A.-M.; Sterz, F.; Schober, A.; Ettl, F.; Magnet, I.A.M.; Högler, S.; Teubenbacher, U.; Grassmann, D.; Wagner, M.; Janata, A.; et al. Reduction of Serious Adverse Events Demanding Study Exclusion in Model Development: Extracorporeal Life Support Resuscitation of Ventricular Fibrillation Cardiac Arrest in Rats. Shock 2016, 46, 704–712. [Google Scholar] [CrossRef]
- Wiegmann, B.; Seggern, H. von; Höffler, K.; Korossis, S.; Dipresa, D.; Pflaum, M.; Schmeckebier, S.; Seume, J.; Haverich, A. Developing a biohybrid lung - sufficient endothelialization of poly-4-methly-1-pentene gas exchange hollow-fiber membranes. J. Mech. Behav. Biomed. Mater. 2016, 60, 301–311. [Google Scholar] [CrossRef]
- Magnet, I.A.M.; Ettl, F.; Schober, A.; Warenits, A.-M.; Grassmann, D.; Wagner, M.; Schriefl, C.; Clodi, C.; Teubenbacher, U.; Högler, S.; et al. Extracorporeal Life Support Increases Survival After Prolonged Ventricular Fibrillation Cardiac Arrest in the Rat. Shock 2017, 48, 674–680. [Google Scholar] [CrossRef]
- Chang, R.-W.; Luo, C.-M.; Yu, H.-Y.; Chen, Y.-S.; Wang, C.-H. Investigation of the pathophysiology of cardiopulmonary bypass using rodent extracorporeal life support model. BMC Cardiovasc. Disord. 2017, 17, 123. [Google Scholar] [CrossRef] [PubMed]
- Madrahimov, N.; Natanov, R.; Boyle, E.C.; Goecke, T.; Knöfel, A.-K.; Irkha, V.; Solovieva, A.; Höffler, K.; Maus, U.; Kühn, C.; et al. Cardiopulmonary Bypass in a Mouse Model: A Novel Approach. J. Vis. Exp. 2017. [Google Scholar] [CrossRef]
- Madrahimov, N.; Boyle, E.C.; Gueler, F.; Goecke, T.; Knöfel, A.-K.; Irkha, V.; Maegel, L.; Höffler, K.; Natanov, R.; Ismail, I.; et al. Novel mouse model of cardiopulmonary bypass. Eur. J. Cardiothorac. Surg. 2018, 53, 186–193. [Google Scholar] [CrossRef]
- Madrahimov, N.; Khalikov, A.; Boyle, E.C.; Natanov, R.; Knoefel, A.-K.; Siemeni, T.; Hoeffler, K.; Haverich, A.; Maus, U.; Kuehn, C. Veno-Venous Extracorporeal Membrane Oxygenation in a Mouse. J. Vis. Exp. 2018. [Google Scholar] [CrossRef] [PubMed]
- Natanov, R.; Khalikov, A.; Gueler, F.; Maus, U.; Boyle, E.C.; Haverich, A.; Kühn, C.; Madrahimov, N. Four hours of veno-venous extracorporeal membrane oxygenation using bi-caval cannulation affects kidney function and induces moderate lung damage in a mouse model. Intensive Care Med. Exp. 2019, 7, 72. [Google Scholar] [CrossRef] [PubMed]
- May, A.G.; Sen, A.; Cove, M.E.; Kellum, J.A.; Federspiel, W.J. Extracorporeal CO2 removal by hemodialysis: in vitro model and feasibility. Intensive Care Med. Exp. 2017, 5, 20. [Google Scholar] [CrossRef]
- Goldstein, S.L.; Hackbarth, R.; Bunchman, T.E.; Blowey, D.; and Brophy, P.D. Evaluation of the PRISMA M10® Circuit in Critically Ill Infants with Acute Kidney Injury: A Report from the Prospective Pediatric CRRT Registry Group. [CrossRef]
- Thomas, M.; Moriyama, K.; Ledebo, I. AN69: Evolution of the world's first high permeability membrane. Contrib. Nephrol. 2011, 173, 119–129. [Google Scholar] [CrossRef]
- Vu, L.H.; Kellum, J.A.; Federspiel, W.J.; Cove, M.E. Carbon dioxide removal using low bicarbonate dialysis in rodents. Perfusion 2019, 34, 578–583. [Google Scholar] [CrossRef]
- Wollborn, J.; Siemering, S.; Steiger, C.; Buerkle, H.; Goebel, U.; Schick, M.A. Phosphodiesterase-4 inhibition reduces ECLS-induced vascular permeability and improves microcirculation in a rodent model of extracorporeal resuscitation. Am. J. Physiol. Heart Circ. Physiol. 2019, 316, H751–H761. [Google Scholar] [CrossRef]
- Fujii, Y.; Tatsumi, E.; Nakamura, F.; Oite, T. PaO2 greater than 300 mmHg promotes an inflammatory response during extracorporeal circulation in a rat extracorporeal membrane oxygenation model. J. Thorac. Dis. 2020, 12, 749–757. [Google Scholar] [CrossRef] [PubMed]
- Dong, G.-H.; Xu, B.; Wang, C.-T.; Qian, J.-J.; Liu, H.; Huang, G.; Jing, H. A rat model of cardiopulmonary bypass with excellent survival. J. Surg. Res. 2005, 123, 171–175. [Google Scholar] [CrossRef] [PubMed]
- Edinger, F.; Schneck, E.; Schulte, C.; Gehron, J.; Mueller, S.; Sander, M.; Koch, C. Comparison of the effect of membrane sizes and fibre arrangements of two membrane oxygenators on the inflammatory response, oxygenation and decarboxylation in a rat model of extracorporeal membrane oxygenation. BMC Cardiovasc. Disord. 2020, 20, 294. [Google Scholar] [CrossRef]
- Wilbs, J.; Kong, X.-D.; Middendorp, S.J.; Prince, R.; Cooke, A.; Demarest, C.T.; Abdelhafez, M.M.; Roberts, K.; Umei, N.; Gonschorek, P.; et al. Cyclic peptide FXII inhibitor provides safe anticoagulation in a thrombosis model and in artificial lungs. Nat. Commun. 2020, 11, 3890. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Huang, J.; Zhang, R.; Wang, S.; Cheng, X.; Zhang, P.; Zhai, K.; Wang, W.; Liu, D.; Gao, B. Establishment of a venovenous extracorporeal membrane oxygenation in a rat model of acute respiratory distress syndrome. Perfusion 2021, 38, 85–91. [Google Scholar] [CrossRef]
- Cho, H.-J.; Kayumov, M.; Kim, D.; Lee, K.; Onyekachi, F.O.; Jeung, K.-W.; Kim, Y.; Suen, J.Y.; Fraser, J.F.; Jeong, I.-S. Acute Immune Response in Venoarterial and Venovenous Extracorporeal Membrane Oxygenation Models of Rats. ASAIO J. 2021, 67, 546–553. [Google Scholar] [CrossRef] [PubMed]
- Edinger, F.; Schmitt, C.; Koch, C.; McIntosh, J.M.; Janciauskiene, S.; Markmann, M.; Sander, M.; Padberg, W.; Grau, V. Application of alpha1-antitrypsin in a rat model of veno-arterial extracorporeal membrane oxygenation. Sci. Rep. 2021, 11, 15849. [Google Scholar] [CrossRef] [PubMed]
- Govender, K.; Cabrales, P. Extracorporeal circulation impairs microcirculation perfusion and organ function. J. Appl. Physiol. (1985) 2022, 132, 794–810. [Google Scholar] [CrossRef] [PubMed]
- Greite, R.; Störmer, J.; Gueler, F.; Khalikov, R.; Haverich, A.; Kühn, C.; Madrahimov, N.; Natanov, R. Different Acute Kidney Injury Patterns after Renal Ischemia Reperfusion Injury and Extracorporeal Membrane Oxygenation in Mice. Int. J. Mol. Sci. 2022, 23. [Google Scholar] [CrossRef]
- Huang, J.; Zhang, R.; Zhai, K.; Li, J.; Yao, M.; Wei, S.; Cheng, X.; Yang, J.; Gao, B.; Wu, X.; et al. Venovenous extracorporeal membrane oxygenation promotes alveolar epithelial recovery by activating Hippo/YAP signaling after lung injury. J. Heart Lung Transplant. 2022, 41, 1391–1400. [Google Scholar] [CrossRef]
- Zhang, R.; Zhai, K.; Huang, J.; Wei, S.; Yang, J.; Zhang, Y.; Wu, X.; Li, Y.; Gao, B. Sevoflurane alleviates lung injury and inflammatory response compared with propofol in a rat model of VV ECMO. Perfusion 2022, 2676591221131217. [Google Scholar] [CrossRef] [PubMed]
- Edinger, F.; Schneck, E.; Schulte, C.; Schmidt, G.; Gehron, J.; Sander, M.; Koch, C. Impact of the inspiratory oxygen fraction on the cardiac output during jugulo-femoral venoarterial extracorporeal membrane oxygenation in the rat. BMC Cardiovasc. Disord. 2022, 22, 174. [Google Scholar] [CrossRef] [PubMed]
- Kharnaf, M.; Hogue, S.; Wilkes, Z.; Reagor, J.A.; Leino, D.G.; Gourley, B.; Rosenfeldt, L.; Ma, Q.; Devarajan, P.; Palumbo, J.S.; et al. A Murine Model of Veno-Arterial Extracorporeal Membrane Oxygenation. ASAIO J. 2022, 68, e243–e250. [Google Scholar] [CrossRef] [PubMed]
- Alabdullh, H.A.; Pflaum, M.; Mälzer, M.; Kipp, M.; Naghilouy-Hidaji, H.; Adam, D.; Kühn, C.; Natanov, R.; Niehaus, A.; Haverich, A.; et al. Biohybrid lung Development: Towards Complete Endothelialization of an Assembled Extracorporeal Membrane Oxygenator. Bioengineering (Basel) 2023, 10. [Google Scholar] [CrossRef] [PubMed]
- Bedford, T.G.; Tipton, C.M.; Wilson, N.C.; Oppliger, R.A.; Gisolfi, C.V. Maximum oxygen consumption of rats and its changes with various experimental procedures.
- Brands, M.W.; Lee, W.F.; Keen, H.L.; Alonso-Galicia, M.; Zappe, D.H.; Hall, J.E. Cardiac output and renal function during insulin hypertension in Sprague-Dawley rats.
- Probst, R.J.; Lim, J.M.; Bird, D.N.; Pole, G.L.; Sato, A.K.; Claybaugh, J.R. Gender Differences in the Blood Volume of Conscious Sprague-Dawley Rats. Journal of the American Association for Laboratory Animal Science 2006, 45, 49–52. [Google Scholar] [PubMed]
- Fox, J.G. Laboratory Animal Medicine, 3rd ed.; Elsevier Science & Technology: San Diego, 2015; ISBN 9780124095274. [Google Scholar]
- The laboratory rabbit, guinea pig, hamster, and other rodents; Suckow, M.A.; Stevens, K.A.; Wilson, R.P., Eds., 1st ed.; Elsevier: London, 2012, ISBN 978-0-12-380920-9.
- Barbee, R.W.; Perry, B.D.; Re, R.N.; Murgo, J.P. Microsphere and dilution techniques for the determination of blood flows and volumes in conscious mice. American Journal of Physiology 1992, 263, 728–633. [Google Scholar] [CrossRef]
- Morrison, P.R. Oxygen consumption in several small wild mammals. J. Cell. Comp. Physiol. 1948, 31, 69–96. [Google Scholar] [CrossRef]
- Quesenberry, K.E.; Carpenter, J.W. Ferrets, Rabbits, and Rodents; Elsevier (Saunders): Philadelphia, 2012; ISBN 9781416066217. [Google Scholar]
- Cabrales, P.; Acero, C.; Intaglietta, M.; Tsai, A.G. Measurement of the cardiac output in small animals by thermodilution. Microvasc. Res. 2003, 66, 77–82. [Google Scholar] [CrossRef]
- Altman, P.L.; Dittmer, D.S. Biological Handbooks: Respiration and circulation, 1971, ISBN 9780913822050.
- Ross, B.; McIntosh, M.; Rodaros, D.; Hébert, T.E.; Rohlicek, C.V. Systemic arterial pressure at maturity in rats following chronic hypoxia in early life. Am. J. Hypertens. 2010, 23, 1228–1233. [Google Scholar] [CrossRef] [PubMed]
- Drożdż, D.; A. Gorecki. Oxygen Consumption and Heat Production in Chinchillas. Acta Theriologica 1987, 81–86.
- Hesselmann, F.; Scherenberg, N.; Bongartz, P.; Djeljadini, S.; Wessling, M.; Cornelissen, C.; Schmitz-Rode, T.; Steinseifer, U.; Jansen, S.V.; Arens, J. Structure-dependent gas transfer performance of 3D-membranes for artificial membrane lungs. Journal of Membrane Science 2021, 634, 119371. [Google Scholar] [CrossRef]
- Kaesler, A.; Rosen, M.; Schlanstein, P.C.; Wagner, G.; Groß-Hardt, S.; Schmitz-Rode, T.; Steinseifer, U.; Arens, J. How Computational Modeling can Help to Predict Gas Transfer in Artificial Lungs Early in the Design Process. ASAIO J. 2020, 66, 683–690. [Google Scholar] [CrossRef] [PubMed]
- Arens, J.; Schraven, L.; Kaesler, A.; Flege, C.; Schmitz-Rode, T.; Rossaint, R.; Steinseifer, U.; Kopp, R. Development and evaluation of a variable, miniaturized oxygenator for various test methods. Artif. Organs 2022. [Google Scholar] [CrossRef] [PubMed]
- Hesselmann, F.; Focke, J.M.; Schlanstein, P.C.; Steuer, N.B.; Kaesler, A.; Reinartz, S.D.; Schmitz-Rode, T.; Steinseifer, U.; Jansen, S.V.; Arens, J. Introducing 3D-potting: a novel production process for artificial membrane lungs with superior blood flow design. Bio-des. Manuf. 2022, 5, 141–152. [Google Scholar] [CrossRef]
- Karagiannidis, C.; Joost, T.; Strassmann, S.; Weber-Carstens, S.; Combes, A.; Windisch, W.; Brodie, D. Safety and Efficacy of a Novel Pneumatically Driven Extracorporeal Membrane Oxygenation Device. Ann. Thorac. Surg. 2020, 109, 1684–1691. [Google Scholar] [CrossRef]
- He, T.; He, J.; Wang, Z.; Cui, Z. Modification strategies to improve the membrane hemocompatibility in extracorporeal membrane oxygenator (ECMO). Adv. Compos. Hybrid Mater. 2021, 4, 847–864. [Google Scholar] [CrossRef]
- Maul, T.M.; Massicotte, M.P.; Wearden, P.D. ECMO Biocompatibility: Surface Coatings, Anticoagulation, and Coagulation Monitoring. In Extracorporeal Membrane Oxygenation: Advances in Therapy; Firstenberg, M.S., Ed.; InTech, 2016, ISBN 978-953-51-2552-5.
- Alentiev, A.Y.; Bogdanova, Y.G.; v. d. Dolzhikova; Belov, N.A.; Nikiforov, R.Y.; Alentiev, D.A.; Karpov, G.O.; Bermeshev, M.V.; Borovkova, N.V.; Evseev, A.K.; et al. The Evaluation of the Hemocompatibility of Polymer Membrane Materials for Blood Oxygenation. Membr. Membr. Technol. 2020, 2, 368–382. [CrossRef]
- Park, A.; Song, Y.; Yi, E.; Duy Nguyen, B.T.; Han, D.; Sohn, E.; Park, Y.; Jung, J.; Lee, Y.M.; Cho, Y.H.; et al. Blood Oxygenation Using Fluoropolymer-Based Artificial Lung Membranes. ACS Biomater. Sci. Eng. 2020, 6, 6424–6434. [Google Scholar] [CrossRef] [PubMed]
- Ontaneda, A.; Annich, G.M. Novel Surfaces in Extracorporeal Membrane Oxygenation Circuits. Front. Med. (Lausanne) 2018, 5, 321. [Google Scholar] [CrossRef]
- Gajkowski, E.F.; Herrera, G.; Hatton, L.; Velia Antonini, M.; Vercaemst, L.; Cooley, E. ELSO Guidelines for Adult and Pediatric Extracorporeal Membrane Oxygenation Circuits. ASAIO J. 2022, 68, 133–152. [Google Scholar] [CrossRef]
Figure 1.
Fully assembled, maximum size RatOx before an in-vitro experiment. Blue-white: silicone potted fiber bundle (55 layers).
Figure 1.
Fully assembled, maximum size RatOx before an in-vitro experiment. Blue-white: silicone potted fiber bundle (55 layers).
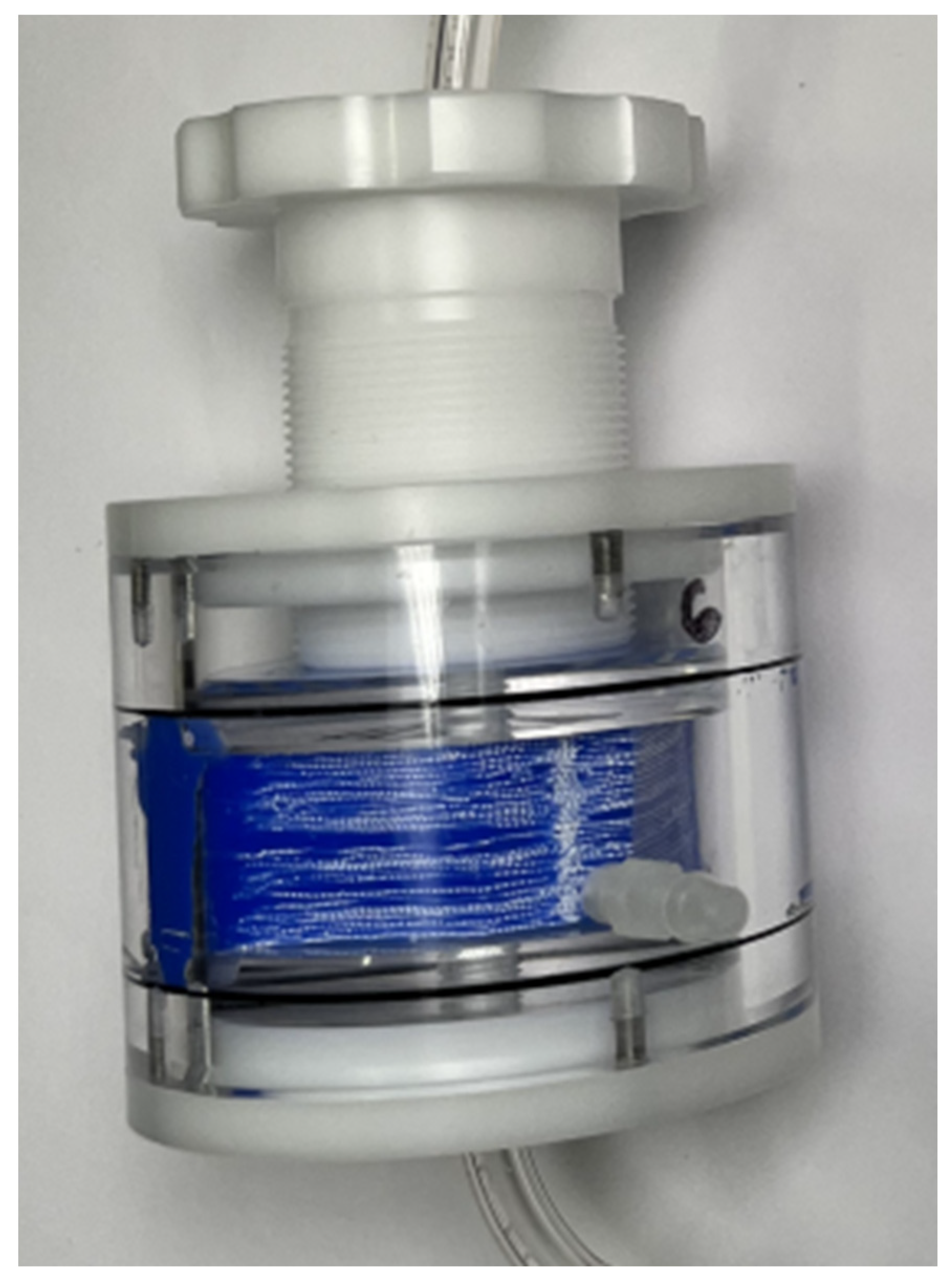
Figure 2.
CAD sketch of a RatOx oxygenator on a pedestal. White: Size-variable fiber mat; blue: potting silicone around the fiber mat, forming a fiber bundle; red: top and bottom cap with connector for circuit tubing; dark grey: cylindrically shaped, transparent housing; yellow: outer caps; green: screw to fasten all components with varying fiber module heights.
Figure 2.
CAD sketch of a RatOx oxygenator on a pedestal. White: Size-variable fiber mat; blue: potting silicone around the fiber mat, forming a fiber bundle; red: top and bottom cap with connector for circuit tubing; dark grey: cylindrically shaped, transparent housing; yellow: outer caps; green: screw to fasten all components with varying fiber module heights.
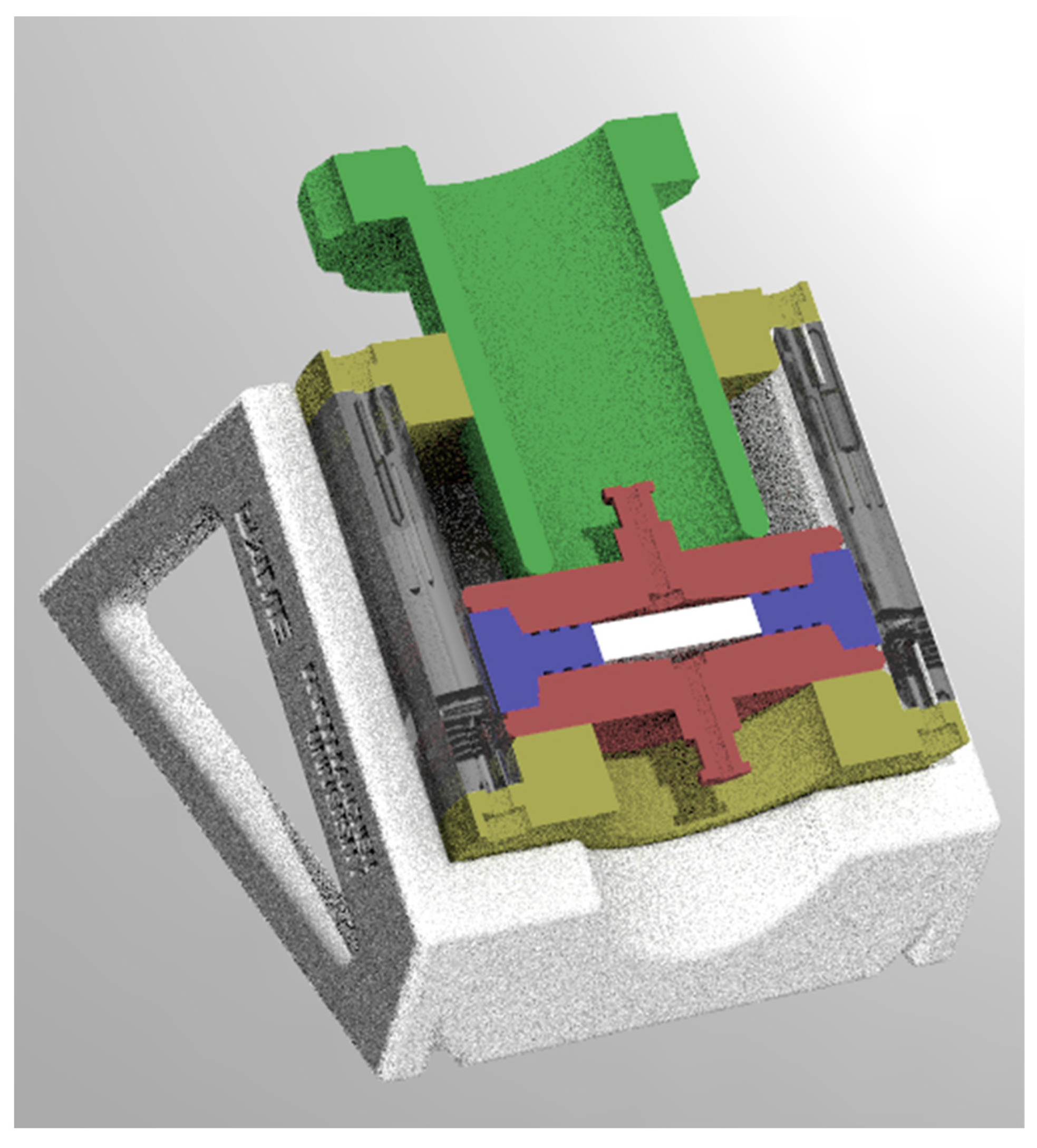
Figure 3.
Photograph of a medium-size, silicone potted fiber module (29 layers), re-opened fibers, before assembly.
Figure 3.
Photograph of a medium-size, silicone potted fiber module (29 layers), re-opened fibers, before assembly.
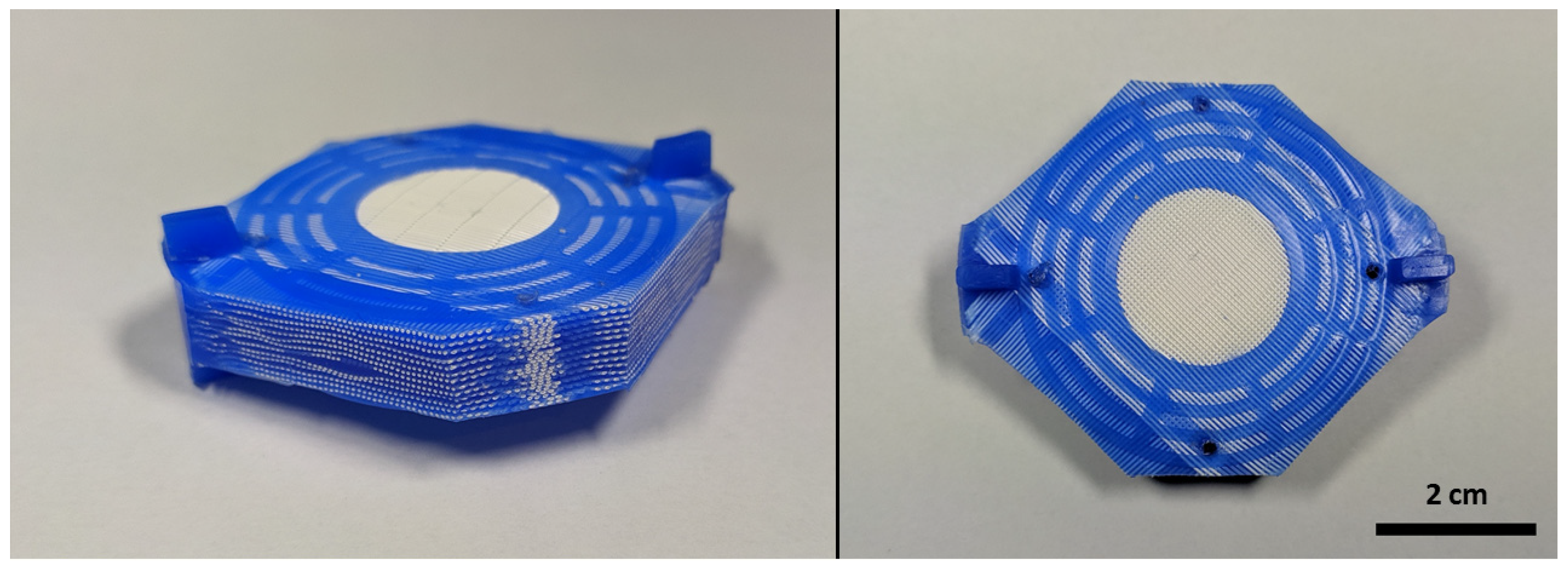
Figure 4.
– Examples of fiber modules explanted post experiment for visual inspection. (a, b): Fiber bundle where layer by layer is cut away for visual inspection. (c): 55 layer fiber module with uncoated PMP fiber mats from a disassembled RatOx oxygenator after an experiment with low-anticoagulated, fresh, whole, porcine blood. The module was cut in a middle plane. (d): An identical module with blood from the same donor in the same experiment, but with high anticoagulation dosis.
Figure 4.
– Examples of fiber modules explanted post experiment for visual inspection. (a, b): Fiber bundle where layer by layer is cut away for visual inspection. (c): 55 layer fiber module with uncoated PMP fiber mats from a disassembled RatOx oxygenator after an experiment with low-anticoagulated, fresh, whole, porcine blood. The module was cut in a middle plane. (d): An identical module with blood from the same donor in the same experiment, but with high anticoagulation dosis.
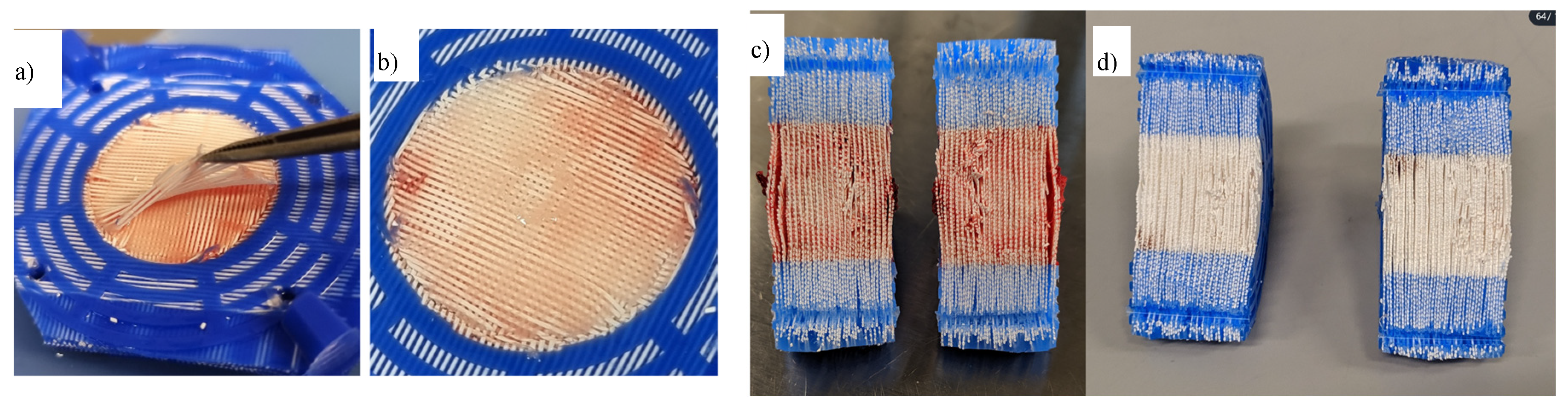
Figure 5.
Gas transfer efficacy over blood flow for three different fiber mat layer numbers. The zoomed-out graph on the right further shows two measured values for 500 ml/min blood flow to show that a linear extrapolation of the values measured in the lower flow regimes is approximately valid. Blue squares: 29 fiber mat layers, beige circles: 42 fiber mat layers, red stars: 55 fiber mat layers. Solid lines: Oxygen transfer performance, broken line: carbon dioxide transfer performance.
Figure 5.
Gas transfer efficacy over blood flow for three different fiber mat layer numbers. The zoomed-out graph on the right further shows two measured values for 500 ml/min blood flow to show that a linear extrapolation of the values measured in the lower flow regimes is approximately valid. Blue squares: 29 fiber mat layers, beige circles: 42 fiber mat layers, red stars: 55 fiber mat layers. Solid lines: Oxygen transfer performance, broken line: carbon dioxide transfer performance.
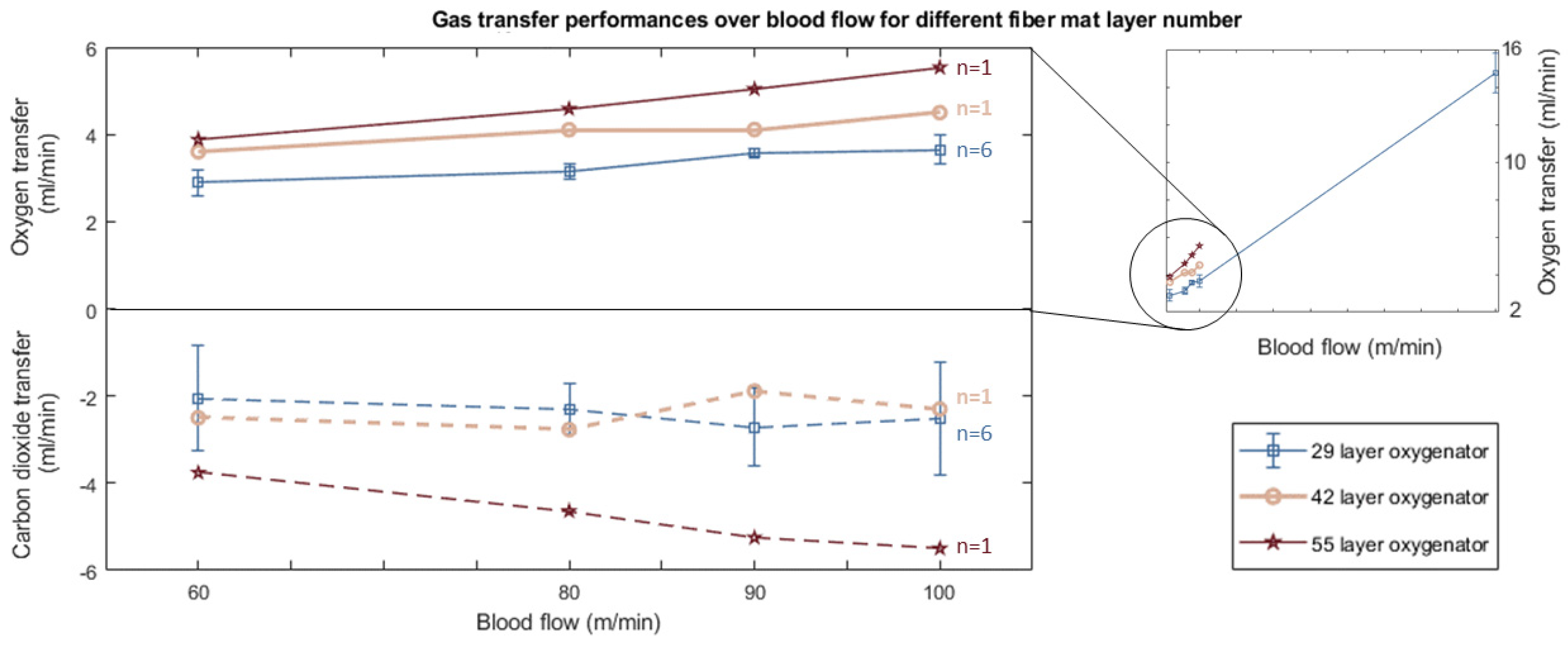
Figure 6.
Oxygen and Carbon dioxide transfer rates over blood flow. Blue: n=10 experiments with 56 fiber layer oxygenators manufactured and tested in Twente University. Red stars: Similar experiments with a single 55 layer mat oxygenator, manufactured and tested in University Hospital Aachen (identical data also shown in Figure 5). Solid lines: Oxygen transfer performance, broken line: carbon dioxide transfer performance.
Figure 6.
Oxygen and Carbon dioxide transfer rates over blood flow. Blue: n=10 experiments with 56 fiber layer oxygenators manufactured and tested in Twente University. Red stars: Similar experiments with a single 55 layer mat oxygenator, manufactured and tested in University Hospital Aachen (identical data also shown in Figure 5). Solid lines: Oxygen transfer performance, broken line: carbon dioxide transfer performance.
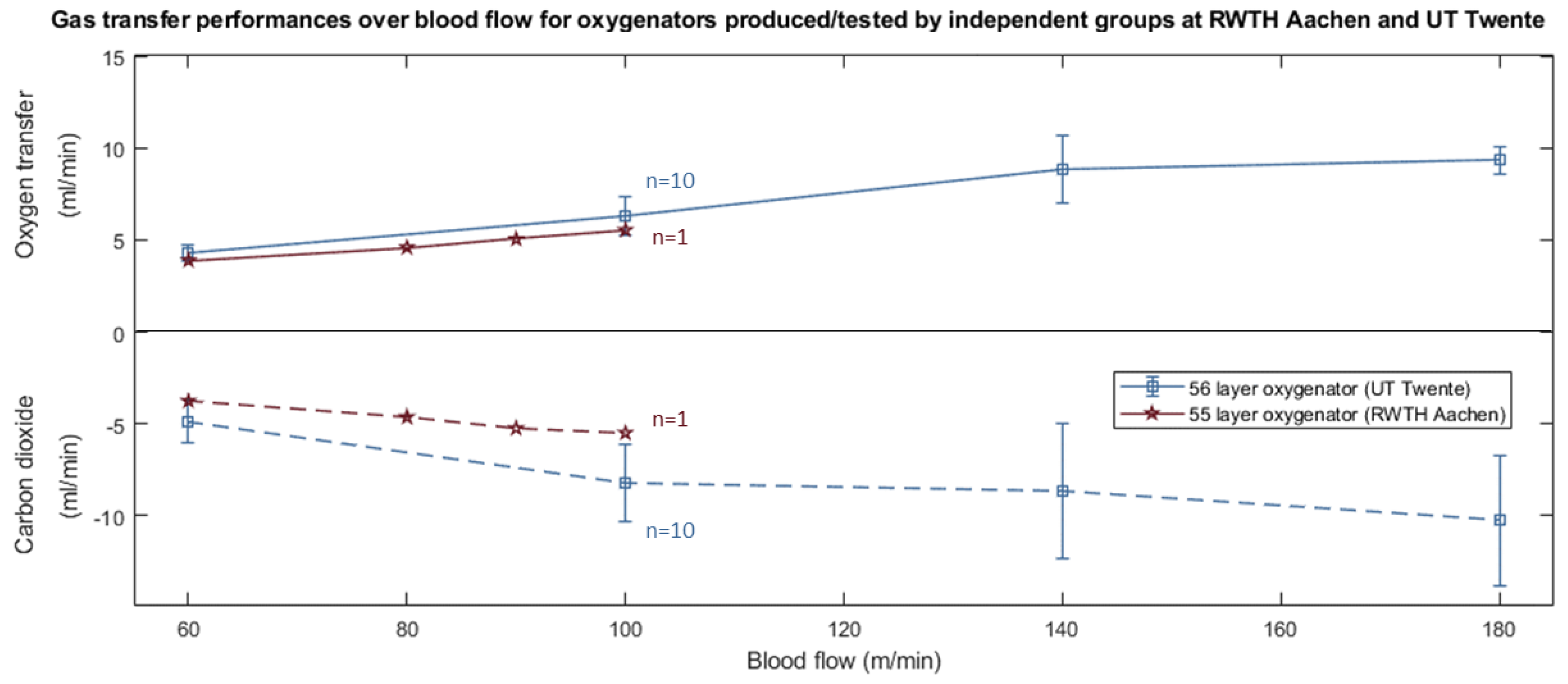
Table 2.
Requirement specifications and design targets.
| Requirement | Design target |
|---|---|
| State of the art design | The oxygenator is built using state-of-the-art design principles. The basic functions are scaled-down from commercially available oxygenators. |
| Interchangeable fiber type | All available and similar hollow fiber membrane types can be used. |
| Effective gas transfer | Based on a rodent body weight of 280 g and a (resting) O2 demand of 0.028 mlO2 per gram body weight per minute (Sprague-Dawley rats, both parameters published by Bedfort et al. already in 1979 [50]), the maximum oxygen transfer capacity of the rodent oxygenator should be at a minimum of 7.9 mlO2/min. This is valid at a blood flow value similar to the physiologic cardiac output (121 ml/min, for a 350 g Sprague-Dawley rat, published by Brands et al. [51] translates to approximately 100 ml/min for a 280 g rat, assuming validity of a linear interpolation). |
| Variable gas exchange surface | The oxygenator design allows for using differently large fiber modules for different animal models and ECLS modalities. The surface size is between 10 cm² for experimental incubation with scarce endothelial cells (25 % of the surface area seeded in a specifically designed incubator by Wiegmann et al. [24]) and sufficient gas transfer exchange area to allow the targeted 7.9 mlO2/min of transfer. |
| Low priming volume | Static priming volume is as low as possible to keep hemodilution low. The gas exchange surface is adjustable to keep the variable priming volume low (see above). The blood volume of a 280 g Sprague-Dawley rat can be estimated to be 20,44 ml [52]. Depending on the model, a hemodilution of 20-30 % can be tolerated, which translates to approximately 5-9 ml maximum priming volume. |
| Low pressure loss | To avoid the need of large pumps and to allow for arteriovenous ECLS cannulation, the pressure differential due to flow resistance over the oxygenator does not exceed 25 % of the average mean arterial pressure of the animal, analog to full sized oxygenators in humans. In the Sprague-Dawley rat, this means a tolerable pressure drop of 25 mmHg. |
| Hemocompatibility | Blood leading components of the oxygenator do not cause avoidable hemocompatibility issues and undesired influences for hemocompatibility testing. |
| Transparent housing | The oxygenator is designed to allow spotting of air bubbles and plasma leakage, using transparent materials where necessary. |
| Reusable housing and removable fiber bundle | To decrease economic burden and to increase availability, the oxygenator design allows non-destructive disassembly, e.g. without adhesives. All blood-leading materials are made from sterilizable materials. The (disposable) fiber bundle can be explanted and mechanically opened for visual inspection (e.g. immunofluorescence, microscopy). |
| Reproducibility, cross-lab usability and manufacturability | The oxygenator manufacturing and assembly process is simple and yields highly reproducible oxygenators. Fabrication and deployment of the oxygenator does not require any special equipment. The manufacturing process uses low-tech equipment so that other laboratories and working groups can produce test objects on their own. If other working groups do not possess sufficient equipment or resources, the oxygenator can be produced by collaborating institutions. This allows the reproduction of results as well as cross-study data interpretation, despite the large influence the oxygenator unit has on physiologic systems like hemostasis/thrombosis or inflammatory response [8]. |
Table 3.
Small animals potentially relevant for ECLS modelling with the RatOx oxygenator. The values listed in this table were amalgamated both from published studies using the respective animal model (mostly for ECLS and/or CPB) as well as reference tables from textbook to fill missing data. The data does not differentiate regarding animal sex, age, maturity status, pathology, feeding status, and, in some correspondingly denoted cases, strain. For further reading, excellent overviews of each animal are published by Fox et al. [53] and Suckow et al. [54]. Hgb: hemoglobin; Hct: hematocrit.
Table 3.
Small animals potentially relevant for ECLS modelling with the RatOx oxygenator. The values listed in this table were amalgamated both from published studies using the respective animal model (mostly for ECLS and/or CPB) as well as reference tables from textbook to fill missing data. The data does not differentiate regarding animal sex, age, maturity status, pathology, feeding status, and, in some correspondingly denoted cases, strain. For further reading, excellent overviews of each animal are published by Fox et al. [53] and Suckow et al. [54]. Hgb: hemoglobin; Hct: hematocrit.
| Rodent | Bodyweight (g) |
Blood volume (ml/kg) |
Hgb (g/dl) |
Hct (%) |
Gas demand O2 (l/kg/h) |
Heart rate (min-1) |
Mean art. pressure (mmHg) |
Cardiac index (ml/min/kg) |
Ref. | Comment |
|---|---|---|---|---|---|---|---|---|---|---|
| Mouse (C3H/HeJ,C57BL/6) | 30±5 | 80±4 | 14±2 (a) | 45±7(a) | 3.5±1.5(b) | 652±25 | 92±3 | 591±49 | [28,29,30,54,55,56] |
(a) Deer Mouse (b) Approximation for 6 mouse species based on data from [56]. |
| Gerbil | 89±43 | 73±12 | 14±4 | 44±8 | N/A | 430±170 | 89±11 | N/A | [54,57] | |
| Golden Syrian Hamster | 100±40 | 73±7 (c) | 15±5(d) | 45±15(d) | 2.2±0.9 (e) | 390±110 | 113±12 | 197.0±19 | [43,54,58,59] |
(c) listed in [57] without specified hamster strain (d) listed in [54] without specified hamster strain (e) Gas demand decreasing distinctly with age (11-70 days) |
| Sprague Dawley rat | 410±190 | 58±2 | 15±2(f) | 50±3(g) | 1.7±0.1(h) | 378±64 | 105±20 | 345±20(i) | [23,40,50,52,54,55,60] |
(f) Values for rat strains Kangaroo rat and Cotton rat, in [54] (g) Values for rat strains Kangaroo rat, listed in [54] (h) calculated from values of 280 g bodyweight animals (i) calculated from values of 350 g bodyweight animals |
| Chinchilla | 500±100 | 57±24(j) | 12±3 | 43±12 | 0.7±0.1 | 125±25 | N/A | N/A | [54,57,61] | (j) Estimate from absolute values listed in [54] |
| Guinea Pig | 950±250 | 80±13 | 14±3 | 40±10 | 0.8±0.04 | 395±75 | 67±3 | 270±30 | [53,54,57] |
Table 4.
Oxygen and Carbon dioxide transfer rates over blood flow for n=1 experiments with 55 layer oxygenators conducted in University Hospital Aachen and n=10 experiments with 56 fiber layer oxygenators conducted in Twente University.
Table 4.
Oxygen and Carbon dioxide transfer rates over blood flow for n=1 experiments with 55 layer oxygenators conducted in University Hospital Aachen and n=10 experiments with 56 fiber layer oxygenators conducted in Twente University.
| Blood flow (ml/min) |
Aachen (55 layers) |
Twente (56 layers) |
|||
|---|---|---|---|---|---|
| Oxygen transfer (ml/min) |
Carbon dioxide transfer (ml/min) |
Oxygen transfer (ml/min) |
Carbon dioxide transfer (ml/min) |
||
| 60 | 3.88 | -3.76 | 4.30±0.41 | -4.97±1.10 | |
| 80 | 4.59 | -4.64 | N/A | N/A | |
| 90 | 5.04 | -5.25 | N/A | N/A | |
| 100 | 5.53 | -5.50 | 6.27±0.98 | -8.20±1.97 | |
| 140 | N/A | N/A | 8.83±1.77 | -8.64±3.50 | |
| 180 | N/A | N/A | 9.33±0.73 | -10.28±3.37 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



