Submitted:
15 September 2023
Posted:
18 September 2023
You are already at the latest version
Abstract
Background: In 1962, Susser and Stein observed that the mortality rates of peptic ulcers in England and Wales increased markedly in the 1910s, maintained at a high level during the 1910s-1940s, and began to decline steadily since the early 1950s. They termed this epidemic pattern a birth-cohort phenomenon, but its mechanism has never been elucidated. Susser and Stein speculated that the occurrences of extraordinary social environmental factors roughly fit the fluctuations, but the role of environmental factors in peptic ulcers has never been identified. Objectives: This study aims to elucidate the mechanism of the birth-cohort phenomenon of peptic ulcers and identify the role of environmental factors in the disease. Methods: Starting from an etiology identified recently, this study uses the two inverse operations in calculus, differentiation, and integration, to analyze the existing data. First, a fluctuation curve in the birth-cohort phenomenon is differentiated into multiple annual mortality rates caused by individual environmental factors. Second, these annual mortality rates are integrated to reproduce the fluctuation curve in the birth-cohort phenomenon. Results: The differentiation reveals a parallel relationship between the psychological impacts of environmental factors and the mortality rates of peptic ulcers, whereas the integration reproduces a representative fluctuation curve in the birth-cohort phenomenon. The successive occurrences of multiple social environmental factors from the 1910s to 1940s maintained the increase in mortality rates, while the sustained improvements in living environments explained the steady decline of the mortality rates from the early 1950s. Conclusion: The parallel relationship suggests a causal role of environmental factors in peptic ulcers, whereas the reproduction of a representative fluctuation curve indicates that multiple environmental factors caused the birth-cohort phenomenon by Superposition Mechanism. Significantly, this study challenges the current reductionist approach used to study disease in modern medicine by demonstrating the effectiveness of an opposite methodological concept focused on integration.
Keywords:
peptic ulcers
; birth-cohort phenomenon
; Superposition Mechanism
; psychological stress
; crucial events
; environmental factors
Introduction
The birth-cohort phenomenon of peptic ulcers (including duodenal and gastric ulcers) was first reported by Susser and Stein in 1962 [1], and amended in 2002 [2]. They found that the mortality rates of gastric ulcers in England and Wales increased at the beginning of the 20th century, reached a peak, and then began to fall in the early 1950s [1,2]. They also found that the trends for duodenal ulcers were similar but followed ~5 years behind [1,2]. Susser and Stein hypothesized that each generation carried its own particular risk throughout adult life and the fluctuations in the mortality rates of peptic ulcers represented a birth-cohort phenomenon [1,2]. Subsequent analyses from Western Europe, North America, and Asia confirmed the presence of this cohort pattern [3,4,5,6]. Susser and Stein speculated that the First World War and the unemployment in the 1930s roughly fit the fluctuation in this cohort pattern [1,2], but the mechanism has never been understood.
In total 13 etiological theories have been proposed to explain the pathogenesis of peptic ulcers over the past 3 centuries [7], such as ‘No Acid, No Ulcer’ in 1910 [8] and Nerve Theory in 1913 [9]. In 1950, Alexander proposed Psychosomatic Theory [10], where multiple psychosomatic factors, such as bad habits, poor lifestyle, and unhealthy environment, were the cause of peptic ulcers [11]. Also in 1950, Selye proposed Stress Theory [12], in which psychological stress induced by social and natural events, etc. is the cause of peptic ulcers. Although each of the 4 major etiological theories was supported by numerous clinical, epidemiological, and laboratory observations, none of them has ever elucidated the birth-cohort phenomenon, along with many other characteristics and observations/phenomena of the diseases.
All the 4 major etiological theories in history were deemed to be out of date soon after the discovery of Helicobacter pylori (H. pylori) in 1982 [13]. In 1987, Marshall proposed that peptic ulcers are an infectious disease caused by the infection of H. pylori [14]. As a result, currently peptic ulcers are widely believed to be an infectious disease caused by H. pylori [15]. However, this etiology is controversial and how the bacterium leads to ulceration remains unknown [16,17,18,19,20]. The etiological theory of peptic ulcers based on H. pylori infection was designated as Theory of H. pylori [7]. Unfortunately, Theory of H. pylori cannot explain most of the 15 characteristics and 81 observations/phenomena of peptic ulcers, including 30 of the 36 observations/phenomena associated with the bacterium itself [7]. Moreover, the use of Non-steroidal Anti-inflammatory Drugs (NSAIDs) and other medications is also considered a cause of peptic ulcers, but in Theory of H. pylori, the roles of gastric acid and NSAIDs remain elusive [21,22,23]. Marshall himself could not explain the birth-cohort phenomenon of peptic ulcers [24]. Starting from Theory of H. pylori, Sonnenberg proposed a mathematical model to explain the birth-cohort phenomenon in 2006 [25]. However, this model failed to explain the temporal difference between gastric and duodenal ulcers, along with several other issues [25]. Thus, the birth-cohort phenomenon of peptic ulcers has remained an unresolved mystery for 60 years.
In recent years, numerous studies have reported that multiple environmental factors may cause peptic ulcers by inducing psychological stress. In 2013, Kanno et al observed that after the Great East Japan Earthquake in 2011, psychological stress significantly increased the incidence of peptic ulcers in H. pylori-negative and non-NSAIDs users [26]. Levenstein’s multivariable analysis in 2015 also found that life stressors, such as socioeconomic status, increased risk for peptic ulcers regardless of H. pylori infection and NSAIDs use [27]. Other studies found that peptic ulcers were caused not by H. pylori [28], but by environmental factors, such as climate [29,30], occupation [31,32], air pollution [33], regional and ethnic differences [28], industrialization [28], vacation/holidays [34], immigration [35], religion [36], smoking and alcohol abuse [37], lifestyle, and recreational habits [38]. However, the role of environmental factors in peptic ulcers remains unknown, and how they cause the birth-cohort phenomenon has never been elucidated.
To address the challenges, a recently published Complex Causal Relationship (CCR) with its accompanying methodologies [39] was applied to analyze the existing data, resulting in the birth of a new etiological theory of peptic ulcers, Theory of Nodes [40,41,42]. This theory integrated Psychosomatic Theory and Stress Theory into a new etiology, where peptic ulcers are a psychosomatic disease triggered by psychological stress [41]. Neither H. pylori nor NSAIDs are a cause of peptic ulcers but play a role secondary to gastric acid in only the late phase of peptic ulcerations [40,41,42]. This etiology addressed all the controversies and mysteries of peptic ulcers in a series of 6 articles, including all 36 observations/phenomena related to H. pylori. In the first three articles, 14 characteristics and 71 observations/phenomena of peptic ulcers were elucidated [40,41,42]. This article is the fourth one of the series, focusing on the 72nd observation/phenomenon, the birth-cohort phenomenon. Since the birth-cohort pattern is featured by the fluctuation curves, this retroactive analysis will deliberate on elucidating the mechanism of the fluctuation curves. Despite two different diseases [43,44], gastric and duodenal ulcers share similar mechanisms of the birth-cohort phenomenon. Thus herein, only the fluctuation curves of gastric ulcers are explored, and the temporal difference between gastric and duodenal ulcers will also be elucidated.
Methods
If Theory of Nodes proposed the correct cause of peptic ulcers, in light of the actual conditions in England and Wales, it should be able to reproduce the fluctuation curves in the birth-cohort phenomenon observed by Susser and Stein. Interestingly, the fluctuation curves in this phenomenon closely resemble the sides of irregular shapes, of which Isaac Newton calculated the area using calculus in the 1660s [45]. Herein, the two inverse operations in calculus, differentiation and integration, are iterated to reproduce the fluctuation curves in the birth-cohort phenomenon of peptic ulcers.
Taking clues from Newton, this study differentiates a representative fluctuation curve in the birth-cohort phenomenon 3 times. First, the fluctuation curve is differentiated into multiple total annual mortality rates, each of which is examined separately. Second, based on the etiology proposed by Theory of Nodes and combined with the local environmental conditions in England and Wales, each of the total annual mortality rates is differentiated a second time into the annual mortality rates caused by individual environmental factors in literature, which are classified into 3 categories: misdiagnosis, common events, and crucial events. Third, if there were two crucial events in a year, the annual mortality rate caused by crucial events (AMCrucial Events) is further differentiated into two annual mortality rates caused by each individual crucial event (AMCrucial event-1 and AMCrucial event-2).
Accordingly, the annual mortality rates caused by individual environmental factors are integrated 3 times to produce a fluctuation curve of the annual mortality rates. First, the annual mortality rates caused by crucial events are integrated/superposed by the formula AMCrucial Events = AMCrucial event-1 + AMCrucial event-2. Second, the total annual mortality rates of a year are further integrated/superposed by the formula AMTotal = AMMisdiagnosis + AMCommon events + AMCrucial events. The annual mortality rates calculated in these two steps are the vertical sum of the annual mortality rates by all the relevant factors; hence, this way of data integration is termed ‘Vertical Superposition’. Third, all the total annual mortality rates (AMTotal) are placed together in chronological order to produce a fluctuation curve of the annual mortality rates of peptic ulcers. The data integration in this step provides a horizontal chronological view of the total annual mortality rates and therefore, is termed ‘Horizontal Superposition’. The similarity between the produced fluctuation curve and the original fluctuation curve in the birth-cohort phenomenon will not only elucidate the mechanism of this phenomenon but also validate the etiology of peptic ulcers proposed by Theory of Nodes, as well as the methodology used in this analysis.
Results
Theory of Nodes identified that peptic ulcers are not an infectious disease caused by H. pylori; clinical observations also found that the infection of this bacterium was not essential for this disease [20,46,47]. Herein the data analyses do not consider H. pylori infection but focus on environmental factors that may induce psychological stress.
- The Classification of Exogenous and Endogenous Factors Collected from Literature
In Theory of Nodes, peptic ulcers are identified as a psychosomatic disease triggered by psychological stress [40,41,42]. Therefore, there is always a proportion of individuals who are genetically predisposed to peptic ulcers in the population, and due to past life experiences/psychosomatic factors, many individuals have developed hyperplasia and hypertrophy of gastrin and parietal cells in their stomach [41], or have formed negative life-views [40]. Thus, this proportion of individuals are “ready-to-ulcerate” individuals and may become ulcer patients if psychological stress is induced. In this case, the annual mortality rates are heavily impacted by stressors, including endogenous personality traits, and exogenous family, social, and natural environmental factors [41]. Herein all the factors in the literature that may cause an annual mortality rate of peptic ulcers, are classified/differentiated into three categories according to their respective features (Table 1).
Clinical misdiagnoses occur at a certain frequency [48,49], but were more commonly seen in the early 20th century because diagnostics were not as advanced as they are today. Misdiagnoses increased the overall mortality rate of gastric ulcers and affected statistical results. Therefore, it is regarded as the first category. The second category is termed common events, which may be caused by struggling with personality disorders [50,51] or ordinary social and natural environmental factors [52,53,54], such as climate [29,30], air pollution [33], and common life and social events [55,56,57]. Common events arise at a certain rate and cause relatively consistent mortality rates from year to year. For example, there are always a proportion of individuals facing divorce, unemployment, or conflicts with neighbours or family members, resulting in a relatively consistent mortality rate. The third category is referred to as crucial events caused by extraordinary social and natural environmental factors, which happen sporadically and last for an indeterminate amount of time, leading to an uneven mortality/morbidity rate. For example, a war [58] or an economic crisis [59,60] arises unpredictably and is resolved in a period of time. Another example is natural disasters, such as tsunamis or earthquakes [61,62], which have short duration but the effects may be felt long-term. All the 3 categories may cause their respective annual mortality rates of peptic ulcers.
- 2.
- Vertical Superposition of the Mortality Ratesof Gastric Ulcers
According to the features of the 3 categories listed in Table 1, the annual mortality rates caused by clinical misdiagnoses and common events are relatively consistent but declined very slowly due to gradually improved medical conditions, living and sociopolitical environments. In contrast, the annual mortality rates caused by crucial events fluctuate markedly: the presence of a crucial event results in a high annual mortality rate in the year, whereas the absence of a crucial event leads to a zero mortality rate.
The CCR dictates that a life phenomenon is usually the result of additive effects caused by multiple individual factors [39,41]. Therefore, a new methodological concept, Superposition Mechanism, has been derived to elucidate the mechanisms of life phenomena [39,41]. Based on this concept, the annual mortality rates (AM) caused by all the three categories are vertically superposed/integrated to calculate the total annual mortality rate of gastric ulcers by the formula AMTotal = AMMisdiagnoses + AMCommon Events + AMCrucial Events as illustrated in Figure 1, where each bar is a sum of the mortality rates on an annual basis of a hypothetical scenario. Notably, Figure 1 performs differentiation twice (studies annual mortality rates separately and classifies environmental factors into 3 categories) but integration only once (the Vertical Superposition).
- 3.
- Horizontal Superposition to Determine the Trends of Annual Mortality Rates Over Time
Once all the annual mortality rates were calculated, they were horizontally superposed to simulate the temporal trend in the mortality rates of gastric ulcers as shown in Figure 2. Alternatively, this figure can also be derived by converting the bar graph Figure 1 into a line graph to provide a chronological view of the annual mortality rates of gastric ulcers. Notably, herein Figure 2 performed the second integration that has not been completed in Figure 1 to generate the fluctuations curve caused by all the three categories in Table 1. The annual mortality rates caused by misdiagnosis and common events fluctuate slightly and therefore, the fluctuations of the total annual mortality rates are primarily due to the rise and fall of the annual mortality rates caused by crucial events (extraordinary social and natural environmental factors), whereas the slight decline after the tenth year is due to the sustained improvements in medical condition and living environment, which result in fewer misdiagnoses and psychological stress. The fluctuation curve with two noticeable peaks in Figure 2 suggests that, if peptic ulcers are considered a psychosomatic disease triggered by psychological stress [41], the occurrence and resolution of crucial events (extraordinary environmental factors) dominate the rise and fall trends of the annual mortality rates, signifying a parallel relationship between the psychological impacts of individual environmental factors and the annual mortality rates of gastric ulcers.
- 4.
- Overlapping of Fluctuation Curves Caused by a Succession of Crucial Social Events
Figure 1 and Figure 2 represent an ideal scenario. However, the reality is usually much more complicated. For instance, in the early 20th century, most European countries were affected by the First World War (1914-1918), rebuilding after the war, the unemployment caused by the economic crisis in the 1930s, and the Second World War (1939-1945), followed by another rebuilding after the War until the early 1950s. As a result, from the 1910s to 1940s, at least four crucial events occurred successively in many European countries, including England and Wales, where the data was collected by Susser and Stein for the birth-cohort phenomenon [1,2]. Similar to Figure 2, each of the 4 individual crucial events caused its own fluctuation curves, and these curves overlap as shown in Figure 3. Herein, the four curves epitomize the parallel relationship between the psychological impacts of individual environmental factors and the annual mortality rates of gastric ulcers, and they represent the third differentiation in the data analyses. Notably, since multiple crucial events occurred successively, the fall trend (decreased annual mortality rates) due to the resolution of a crucial event overlapped the rising trend (increased annual mortality rates) caused by another crucial event that followed.
- 5.
- The calculation of the Total Annual Mortality Rates Caused by all 3 Categories
In the case of a succession of 4 crucial events, the Vertical Superposition in Figure 1 was repeated to calculate the total annual mortality rates of gastric ulcers from 1905 to 1975. If there were two crucial events in a given year, the annual mortality rates they caused were superposed by the formula AMCrucial Events=AMCrucial Event-1+AMCrucial Event-2. Assume this scenario: In 1915, the mortality rate as a result of the First World War was 9%, but there were no effects from rebuilding, thus the total annual mortality rate caused by crucial events in this year was 9%. In 1920, the annual mortality rate of peptic ulcers caused by the residual effects of the First World War was 9%, and by rebuilding after the war was 9%, so the total annual mortality rate by crucial events was 9%+9%=18%. The total annual mortality rates caused by crucial events were calculated similarly for all the other years. Subsequently, the total annual mortality rate of a given year was calculated by the formula AMTotal = AMMisdiagnoses + AMCommon Events + AMCrucial Events. Then the Horizontal Superposition described in Figure 2 was iterated to generate the fluctuation curve on a five-year basis from 1905 to 1975 as shown in Figure 4. Notably, herein the annual mortality rates caused by all three categories listed in Table 1 are integrated/superposed three times in two ways (vertical and horizontal) to produce the fluctuation curve of a real scenario in England and Wales, where Susser and Stein collected the data for the birth-cohort phenomenon [1,2]. Figure 4 elucidates that after the superposition, the fall trend due to the resolution of a crucial event was counterbalanced by the rising trend caused by another crucial event that followed (as shown in Figure 3). As a result, both the fall and rise trends caused by two successive crucial events become invisible, and thus, the annual mortality rates from the 1910s to 1940s were maintained at a higher level than other decades.
However, overestimations occurred when the Vertical Superposition was applied to calculate the total annual mortality rates if there were two crucial events in a year. In 1920, 1930, and 1940, individuals might experience two crucial events and become ulcer patients but could also become patients if they experienced only one of the two events. Thus, some patients might have been counted twice, causing extremely high total annual mortality rates in 1920 (D4), 1930 (D6), and 1940 (D8) as shown in Figure 4.
- 6.
- Reproduction of the Mortality Fluctuation Curves of the Birth-Cohort Phenomena
Fortunately, Susser and Stein did not investigate the mortality rates in the years 1910, 1920, 1930, 1940, 1950, 1960, and 1970. After the data for these years were removed from the theoretical curve in Figure 4, one of the fluctuation curves in the birth-cohort phenomenon observed by Susser and Stein is reproduced as shown in Figure 5. The evolutionary process from Figure 3 to Figure 5 suggests that an integration/superposition of the annual mortality rates caused by all the three categories in Table 1 reproduced a fluctuation curve in the birth-cohort phenomenon. Conversely, a proper differentiation of the fluctuation curves in the birth-cohort phenomenon in Figure 5 restored the fluctuation curves caused by multiple individual environmental factors as illustrated in Figure 3, where the psychological impacts of individual extraordinary environmental factors are parallel with the annual mortality rates of peptic ulcers. However, after the integration/superposition, the counterbalance between two successive crucial events made the parallel relationships between the psychological impacts of individual extraordinary environmental factors and the annual mortality rates of peptic ulcers invisible (Figure 4), indicating the parallel relationships were hidden in the fluctuation curves of the birth-cohort phenomenon. As a result, Susser and Stein observed a continuous high level of annual mortality rates from the 1910s to the early 1950s. In addition, similar to the analysis in Figure 2, the relatively peaceful living and sociopolitical environments after the Second World War account for the steady decline of the annual mortality rates since the early 1950s.
Notably, the data analyses presented apply to all the age groups in the birth-cohort phenomena. In addition, the analyses can be applied to explain various parameters of peptic ulcers, such as morbidity rates, perforation rates, hospitalization rates, and disability pension rates. These parameters are all interrelated and affected by misdiagnoses, common events, and crucial events. Therefore, the fluctuation curves for all these parameters follow similar temporal trends.
- 7.
- Understanding the Details of the Birth-Cohort Phenomenon of Gastric Ulcers
Line 3 in Figure 5 suggests that if gastric ulcer is considered a psychosomatic disease triggered by psychological stress and if the concept of ‘Superposition Mechanism’ is used to analyze the existing data, the fluctuation curves in the birth-cohort phenomenon observed by Susser and Stein can be reproduced, especially the curve for the 25-34 age group who experienced the greatest effects from crucial events [1,2]. The etiology and methodology are also applicable to all the other age groups: the older the age, the more complex life experiences causing psychological stress, thereby the more susceptible to gastric ulcers. This elucidated Susser and Stein’s finding that ‘the risk of death from both gastric and duodenal ulcers can be seen to rise steadily with age’ [1,2].
Figure 5 explicitly elucidated the rise and fall in the mortality rates of gastric ulcers observed by Susser and Stein. The start of the First World War in 1914 explained the sharp rise in mortality rates of gastric ulcers in the early 20th century. The continuing trend of increase in perforated gastric ulcers until the early 1950s was maintained by a succession of multiple crucial events. The decrease in annual mortality rates in the early 1950s was due to the end of the Second World War followed by the rebuilding after the War, and the steady decline in the late 1950s was a result of sustained improvements in medical treatments, living conditions, and sociopolitical environment. The start and end of crucial events explain the slope observed from 1905 to 1915 (the First World War) and from 1945 to1955 (the Second World War and rebuilding after the war). The generation born around 1885, especially the males, were in their 20s~30s when the First World War broke out in 1914. They experienced all the crucial events from 1914 to the early 1950s in their adult life and were most probably the direct participants, executors, and/or victims. Their unfortunate experiences explained Susser and Stein’s finding that ‘for gastric ulcer in males the generation born around 1885 carried the highest risk’ [1,2]. Figure 5 also confirmed Susser and Stein’s speculation that ‘the timing of the First World War and the unemployment of the 1930s roughly fit the fluctuations and the cohorts with the highest peptic ulcer death rates’ [1,2].
- 8.
- The Mechanism of Temporal Difference between Gastric and Duodenal Ulcers
In Theory of Nodes, three factors, heredity, secondary stressors derived from crucial events, and the hyperplasia and hypertrophy of gastrin and parietal cells in the stomach induced by chronic stress [41], explain the temporal difference between gastric and duodenal ulcers observed by Susser and Stein [1,2].
The importance of heredity in peptic ulcers has been emphasized by clinical observations [63]. In Theory of Nodes, individuals susceptible to gastric and duodenal ulcers are two genetically different populations [40,41]. Thus, although the whole population experienced the same crucial events simultaneously, individuals with gastric ulcer predisposition may develop gastric ulcers, whereas individuals with duodenal ulcer predisposition may develop duodenal ulcers [42]. However, stressors for gastric ulcers, such as wars, unemployment, financial crises, catastrophes, loss of family members, and divorce, which are usually short-term and acute, may cause gastric ulcers directly right after or during crucial events [40]. In contrast, duodenal ulcers are caused by the secondary chronic stressors derived from crucial events, such as laborious work, poor work/living environments, lower social status, or strained family relations, which are usually long-term, cannot cause duodenal ulcers right away due to the chronic psychopathological process of the disease [41]. As a response to chronic stress, it takes ~5 years to induce the hyperplasia and hypertrophy of gastrin and parietal cells in the stomach [64,65], which in turn result in the hypersecretion of gastric acid and eventually, duodenal ulcers. On the other hand, unlike the easy-to-simulate acute stress that induces gastric ulcers [66,67], chronic stress that induces duodenal ulcers is difficult to duplicate in labs. As a result, all of the stress-induced ulcers in animal models were gastric ulcers [63], further supporting the temporal differences between gastric and duodenal ulcers [40].
Therefore, despite experiencing the same crucial events, some individuals developed gastric ulcers right away, causing increased mortality rates immediately, whereas some others developed duodenal ulcers ~5 years later, resulting in ‘the trends for duodenal ulcers were similar to gastric ulcers but followed approximately 5 years behind [1,2]’.
Discussion
Despite 13 etiological theories being proposed in history [7], the birth-cohort phenomenon of peptic ulcers has remained an unresolved mystery for 60 years. The application of the CCR with its accompanying methodology proposed in 2012 birthed Theory of Nodes [40,41,42], which addressed all the controversies and mysteries of peptic ulcers in a series of 6 articles, including the birth-cohort phenomenon in this fourth article [40,41,42,68,69]. Theory of Nodes attributes its success to a definite etiology of peptic ulcers, as well as an innovative methodological concept, Superposition Mechanism. Significantly, the explanation of the birth-cohort phenomenon herein identified a causal role of environmental factors in peptic ulcers.
- The Widely Believed H. pylori Infection may not be the Cause of Peptic Ulcers
Unequivocally, an etiological theory proposing the correct cause of peptic ulcers should be able to explain all the characteristics and observations/phenomena of the disease. However, Theory of H. pylori cannot face the challenges of the 15 characteristics and 81 observations/phenomena of peptic ulcers [7], indicating that H. pylori infection may not be the cause of peptic ulcers. Interestingly, herein the birth-cohort phenomenon was elucidated without considering H. pylori infection, further suggesting that this bacterium may not be the cause of peptic ulcers [17,20,70,71,72]. The data analyses elucidated that it is not H. pylori infection, but the psychological impacts induced by environmental factors that dominate the rise and fall trends of the annual mortality rates of peptic ulcers. Thus, it is not surprising that starting from H. pylori infection, neither Marshall nor Sonnenberg could explain the birth-cohort phenomenon [24,25], along with the majority of the 15 characteristics and 81 observations/phenomena of peptic ulcers.
- 2.
- The Birth-Cohort Phenomenon has Implicated a Causal Role of Environmental Factors in Peptic Ulcers
Notably, when the birth-cohort phenomenon was first observed in 1962, Susser and Stein speculated that the First World War (1914-1918) and the unemployment in the 1930s roughly fit the fluctuation curves [1,2], suggesting that this cohort pattern has implicated a causal relationship between extraordinary environmental factors/crucial events and peptic ulcers. However, modern medicine rarely attributes the cause of disease to the invisible, intangible, and incorporeal psychological stress caused by environmental factors. Instead, it gets used to attribute the cause of disease to visible, tangible, and corporeal structural abnormalities within the human body, such as gene mutations, infectious microbes, or other aberrant biological molecules. As a result, Susser and Stein’s finding was not supported by the mainstream of etiological concepts in modern medicine. In contrast, despite leading to more controversies and mysteries [16,17,18,19,20], Theory of H. pylori perfectly matched the etiological concepts of modern medicine, therefore H. pylori infection was widely believed to be the cause of peptic ulcers soon after the discovery of the bacterium in 1982 [73,74,75]. Consequently, very little progress has been made in peptic ulcer research over the past 35 years.
- 3.
- Environmental Factors Cause the Birth-Cohort Phenomenon by Superposition Mechanism
The explanation of the birth-cohort phenomenon herein supported the etiology of peptic ulcers elucidated in Theory of Nodes, where peptic ulcers are a psychosomatic disease triggered by psychological stress [41]. This etiology dictates that any factor inducing psychological stress, including various environmental factors, may cause peptic ulcers, suggesting environmental factors play a causal role in the disease. Therefore, the occurrence and resolution of crucial events (extraordinary environmental factors) dominate the rise and fall trend of the fluctuation curves of annual mortality rates. This parallel relationship reflects a causal role of extraordinary environmental factors in peptic ulcers, which was hidden in the fluctuation curves of the birth-cohort phenomenon and surfaced after 3 times of differentiations as illustrated in Figure 3. Interestingly, a parallel relationship (between the psychological impacts of ordinary environmental factors and the monthly incidence of the disease) surfaced after differentiating the fluctuation curves in the seasonal variation of peptic ulcers twice in the fifth article of the series [69]. Thus, ordinary environmental factors, such as climate, occupation, air pollution, regional and ethnic differences, industrialization, immigration, and religion, also play a causal role in peptic ulcers. In the birth-cohort phenomenon, although the ordinary social and natural environmental factors did not dominate the rise and fall trends of the fluctuation curves, the annual mortality rates they caused accounted for the steady decline in the fluctuation curves since the early 1950s. Therefore, both the birth-cohort phenomenon and seasonal variation are compelling evidence to support a causal role of environmental factors in peptic ulcers, which can be revealed by proper differentiation operations. Further, the fluctuation curves can be reproduced by integration operations, suggesting that multiple (ordinary and extraordinary) environmental factors caused the birth-cohort phenomenon of peptic ulcers via Superposition Mechanism.
It is worth mentioning that without pre-existing hyperplasia and hypertrophy of gastrin and parietal cells in the stomach and the negative life-view caused by psychosomatic factors in early life, psychological stress induced by environmental factors alone cannot cause peptic ulcers. Thus, the explanation surrounding psychological stress in this research does not conflict with the etiology proposed in Theory of Nodes, where peptic ulcers are a psychosomatic disease triggered by psychological stress.
- 4.
- A Viable Analytical Method is Indispensable to Elucidate the Birth-Cohort Phenomenon
Although Stress Theory proposed by Hans Selye in 1950 emphasized the causal roles of stressful life events in peptic ulcers [7], it has never explained the birth-cohort phenomenon over the past 60 years, indicating that a correct etiology alone is inadequate to elucidate this phenomenon. The data analyses herein highlighted the significance of a viable analytical method. Newton’s success in calculus suggests that a complete analysis should include two inverse operations, namely differentiation and integration. However, due to a reductionist approach, which attempts to explain a system in terms of its parts [76], modern medicine only differentiates/divides the human body into many small pieces and studies each piece separately, but rarely attempts to integrate the small pieces into the original whole human body, making numerous studies only half-way done. Consequently, the majority of life phenomena remain unresolved mysteries, including the birth-cohort phenomenon of peptic ulcers. In contrast, this study performed both the differentiation and integration processes as Newton did in Physics: the differentiation revealed a causal role of environmental factors in peptic ulcers, whereas the integration elucidated that multiple environmental factors cause the birth-cohort phenomenon by Superposition Mechanism, suggesting that both of the two inverse operations are indispensable methodology in life science and medical research. Further, surrounding the mechanism discovered herein, all the details of the birth-cohort phenomenon of peptic ulcers were fully understood for the first time in history. The validity showcased herein suggests that the Superposition Mechanism might be a significant complement to the current methodology in life science and medicine, and therefore, is indispensable for a full understanding of many life phenomena and diseases.
- 5.
- Limitations
A potential limitation is that there might be many crucial events between the 1910s and 1940s in England and Wales, where the birth-cohort phenomenon of peptic ulcers was observed by Susser and Stein. However, to simplify the data analyses, herein only four well-known crucial events were selected to exemplify the application of the Superposition Mechanism. The analyses suggest that, to elucidate the cohort patterns in a specific location, the greater the details of the local environmental factors are included, the more accurate the fluctuation curves that can be reproduced for a full understanding of the epidemiological observations.
Second, the key analytical method applied herein, Superposition Mechanism, is a thought process opposite to the routine reductionist approach in modern medicine. Although the application showcased herein is as easy as a simple addition, only factors with commonalities can be integrated/superposed/added up. In this study, all the mortality rates are of peptic ulcers and therefore, they can be superposed to generate fluctuation curves. Moreover, there might be many ways to superpose research data but, in this study, only the simplest two ways (vertical and horizontal) were performed for a full understanding of the birth-cohort phenomenon of peptic ulcers. All these indicate that the application of this methodological concept is not a simple mathematical addition but demands greater intelligence.
Conclusions
If peptic ulcers are considered a psychosomatic disease triggered by psychological stress and if a new methodological concept, Superposition Mechanism, is applied to analyze the existing data, the birth-cohort phenomenon of peptic ulcers can be fully elucidated. A succession of crucial events maintained the increased mortality rates from the 1910s to 1940s, and the sustained improvements in living environments caused the steady decline since the early 1950s. The chronic hyperplasia and hypertrophy of gastrin and parietal cells in the stomach caused the temporal difference between gastric and duodenal ulcers. All these suggest a causal role of environmental factors in peptic ulcers, and the birth-cohort phenomenon is compelling evidence to support that peptic ulcers are not an infectious disease caused by H. pylori infection, but a psychosomatic disease triggered by psychological stress. Significantly, a full understanding of the birth-cohort phenomenon of peptic ulcers validated a new concept, Superposition Mechanism, which may represent a significant methodological advance of life science and medicine in the 21st century.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. The online supplemental materials include 6 tables in a PDF document.
Author Contributions
SXMD is the sole author of this article, who conceived the idea, collected and analyzed data, interpreted the data analyses into the table and figures, and drafted the manuscript.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Ethical Statement
This study does not involve any animal and human and therefore, informed consents and approvals of ethics committees are not applicable.
Data Availability
The author confirms that all the data supporting this study are available within the article and/or its supplementary materials.
Declarations of Interests
The author declares that he has no conflict of interest.
References
- Susser M, Stein Z. Civilization and Peptic Ulcer. Lancet 1962;279:116–9. [CrossRef]
- Susser M, Stein Z. Civilization and peptic ulcer*. Int J Epidemiol 2002;31:13–7. [CrossRef]
- Westbrook JI, Rushworth RL. The epidemiology of peptic ulcer mortality 1953-1989: A birth cohort analysis. Int J Epidemiol 1993;22:1085–92. [CrossRef]
- Sonnenberg A, Müller H, Pace F. Birth-cohort analysis of peptic ulcer mortality in Europe. J Chronic Dis 1985;38:309–17. [CrossRef]
- Thors H, Svanes C, Thjodleifsson B. Trends in peptic ulcer morbidity and mortality in Iceland. J Clin Epidemiol 2002;55:681–6.http://www.ncbi.nlm.nih.gov/pubmed/12160916.
- Sonnenberg, A. Sonnenberg A. Occurrence of a Cohort Phenomenon in Peptic Ulcer Mortality From Switzerland. Gastroenterology 1984;86:398–401. [CrossRef]
- Dong SXM, Chang CCY, Rowe KJ. A collection of the etiological theories, characteristics, and observations/phenomena of peptic ulcers in existing data. Data Br 2018;19:1058–67. [CrossRef]
- Fatović-Ferenčić S, Banić M. No acid, no ulcer: Dragutin (Carl) Schwarz (1868-1917), the man ahead of his time. Dig Dis 2011;29:507–10. [CrossRef]
- von Bergmann, G. von Bergmann G. Ulcus duodeni und vegetatives nerve system. Berl Klin Wchnscher 1913;50:2374.
- Wolowitz, HM. Wolowitz HM. Oral involvement in peptic ulcer. J Consult Psychol 1967;31:418–9. [CrossRef]
- Kurata JH, Nogawa AN, Abbey DE, et al. A prospective study of risk for peptic ulcer disease in seventh-day adventists. Gastroenterology 1992;102:902–9. [CrossRef]
- Selye, H. Selye H. The physiology and pathology of exposure to stress. Oxford, England: : Acta 1950.
- Mégraud F, Lehours P. Helicobacter pylori detection and antimicrobial susceptibility testing. Clin Microbiol Rev 2007;20:280–322. [CrossRef]
- Marshall, BJ. Marshall BJ. Peptic Ulcer: An Infectious Disease? Hosp Pract 1987;22:87–96. [CrossRef]
- Quan C, Talley NJ. Management of peptic ulcer disease not related to Helicobacter pylori or NSAIDs. Am J Gastroenterol 2002;97:2950–61. [CrossRef]
- Ford, Alexander C.; Tally NJ. Head to Head: Does Helicobacter pylori really cause duodenal ulcers? Yes. BMJ 2009;339:b2784. [CrossRef]
- Hobsley M, Tovey FI, Bardhan KD, et al. Does Helicobacter pylori really cause duodenal ulcers? No. BMJ 2009;339:b2788. [CrossRef]
- Record CO, Rubin PC. Controversies in Management: Helicobacter pylori is not the causative agent. BMJ 1994;309:1571–2. [CrossRef]
- Kate V, Ananthakrishnan N, Tovey FI. Is Helicobacter pylori Infection the Primary Cause of Duodenal Ulceration or a Secondary Factor? A Review of the Evidence. Gastroenterol Res Pract 2013;2013:1–8. [CrossRef]
- Tovey FI, Hobsley M. Review: is Helicobacter pylori the primary cause of duodenal ulceration? J Gastroenterol Hepatol 1999;14:1053–6. [CrossRef]
- Yeomans, ND. Yeomans ND. The ulcer sleuths: The search for the cause of peptic ulcers. J Gastroenterol Hepatol 2011;26:35–41. [CrossRef]
- Musumba C, Pritchard DM, Pirmohamed M. Review article: cellular and molecular mechanisms of NSAID-induced peptic ulcers. Aliment Pharmacol Ther 2009;30:517–31. [CrossRef]
- Gisbert JP, Calvet X. Review article: Helicobacter pylori-negative duodenal ulcer disease. Aliment Pharmacol Ther 2009;30:791–815. [CrossRef]
- Marshall, B. Marshall B. Commentary: Helicobacter as the ‘environmental factor’ in Susser and Stein’s cohort theory of peptic ulcer disease. Int J Epidemiol 2002;31:21–2. [CrossRef]
- Sonnenberg, A. Sonnenberg A. Causes underlying the birth-cohort phenomenon of peptic ulcer: analysis of mortality data 1911–2000, England and Wales. Int J Epidemiol 2006;35:1090–7. [CrossRef]
- Kanno T, Iijima K, Abe Y, et al. Peptic ulcers after the Great East Japan earthquake and tsunami: possible existence of psychosocial stress ulcers in humans. J Gastroenterol 2013;48:483–90. [CrossRef]
- Levenstein S, Rosenstock S, Jacobsen RK, et al. Psychological stress increases risk for peptic ulcer, regardless of helicobacter pylori infection or use of nonsteroidal anti-inflammatory drugs. Clin Gastroenterol Hepatol 2015;13:498-506.e1. [CrossRef]
- Lam, SK. Lam SK. Differences in peptic ulcer between East and West. Baillieres Best Pract Res Clin Gastroenterol 2000;14:41–52. [CrossRef]
- Nomura T, Ohkusa T, Araki A, et al. Influence of climatic factors in the incidence of upper gastrointestinal bleeding. J Gastroenterol Hepatol 2001;16:619–23. [CrossRef]
- Liu D-Y, Gao A-N, Tang G-D, et al. Relationship between onset of peptic ulcer and meteorological factors. World J Gastroenterol 2006;12:1463. [CrossRef]
- Yuan X-G, Xie C, Chen J, et al. Seasonal changes in gastric mucosal factors associated with peptic ulcer bleeding. Exp Ther Med 2015;9:125–30. [CrossRef]
- FRIED Y, ROWLAND KM, FERRIS GR. The Physiological Measurement of Work Stress: A Critique. Pers Psychol 1984;37:583–615. [CrossRef]
- Wu M, Lu J, Yang Z, et al. Ambient air pollution and hospital visits for peptic ulcer disease in China: A three-year analysis. Environ Res 2021;196:110347. [CrossRef]
- Tom B, Brown M, Chang R. Peptic Ulcer Disease and Temperature Changes in Hawaii. J Appl Meteorol 1964;3:311–5. [CrossRef]
- Kanamori M, Shrader C-H, St. George S, et al. Influences of immigration stress and occupational exploitation on Latina seasonal workers’ substance use networks: a qualitative study. J Ethn Subst Abuse 2022;21:457–75. [CrossRef]
- Bekele A, Zemenfes D, Kassa S, et al. Patterns and Seasonal Variations of Perforated Peptic Ulcer Disease: Experience from Ethiopia. Ann African Surg 2018;14:86–91. [CrossRef]
- Yawar B, Marzouk AM, Ali H, et al. Seasonal Variation of Presentation of Perforated Peptic Ulcer Disease: An Overview of Patient Demographics, Management and Outcomes. Cureus 2021;13. [CrossRef]
- Archimandritis A, Tjivras M, Tsirantonaki M, et al. Symptomatic Peptic Ulcer (PU). J Clin Gastroenterol 1995;20:254–6. [CrossRef]
- Dong SXM, Chang CCY. Philosophical Principles of Life Science. Taipei: : Wunan Culture Enterprise 2012.
- Xin Min Dong, S. Xin Min Dong S. A Novel Psychopathological Model Explains the Pathogenesis of Gastric Ulcers. J Ment Heal Clin Psychol 2022;6:13–24. [CrossRef]
- Dong SXM. The Hyperplasia and Hypertrophy of Gastrin and Parietal Cells Induced by Chronic Stress Explain the Pathogenesis of Duodenal Ulcers. J Ment Heal Clin Psychol 2022;6:1–12. [CrossRef]
- Dong SXM. Painting a complete picture of the pathogenesis of peptic ulcers. Jounral Ment Heal Clin Psychol 2022;6:32–43. [CrossRef]
- Susser, M. Susser M. Peptic Ulcer: Rise and Fall. Christie DA, Tansey EM (eds). Wellcome Witnesses to Twentieth Century Medicine. Vol.14, 2002. London: The Wellcome Trust Centre for the History of Medicine, 2002, £10.00 ISBN: 0-85484-084-2. Int J Epidemiol 2003;32:674–5. [CrossRef]
- Damon A, Polednak AP. Constitution, genetics, and body form in peptic ulcer: A review. J Chronic Dis 1967;20:787–802. [CrossRef]
- Smith, G. Smith G. ‘Isaac Newton’ The Stanford Encyclopedia of Philosophy (Fall 2008 Edition), Edward N. Zalta (ed.). https://plato.stanford.edu/archives/fall2008/entries/newton/.
- Elitsur Y, Lawrence Z. Non-Helicobacter pylori related duodenal ulcer disease in children. Helicobacter 2001;6:239–43. [CrossRef]
- Levenstein S, Jacobsen RK, Rosenstock S, et al. Mental vulnerability, Helicobacter pylori, and incidence of hospital-diagnosed peptic ulcer over 28 years in a population-based cohort. Scand J Gastroenterol 2017;52:1–8. [CrossRef]
- Magon, P. Magon P. Abdominal epilepsy misdiagnosed as peptic ulcer pain. Indian J Pediatr 2010;77:916–916. [CrossRef]
- Kitchin DR, Lubner MG, Menias CO, et al. MDCT diagnosis of gastroduodenal ulcers: key imaging features with endoscopic correlation. Abdom Imaging 2015;40:360–84. [CrossRef]
- Mcintosh JH, Nasiry RW, Frydman M, et al. The Personality Pattern of Patients with Chronic Peptic Ulcer. Scand J Gastroenterol 1983;18:945–50. [CrossRef]
- Schuster J-P, Limosin F, Levenstein S, et al. Association Between Peptic Ulcer and Personality Disorders in a Nationally Representative US Sample. Psychosom Med 2010;72:941–6. [CrossRef]
- Ellard K, Beaurepaire J, Jones M, et al. Acute and chronic stress in duodenal ulcer disease. Gastroenterology 1990;99:1628–32. [CrossRef]
- Kennedy DP, Adolphs R. Stress and the city. Nature 2011;474:452–3. [CrossRef]
- Kurata JH, Haile BM. Epidemiology of peptic ulcer disease. Clin Gastroenterol 1984;13:289–307.http://www.ncbi.nlm.nih.gov/pubmed/6378441.
- Salleh, MR. Salleh MR. Life event, stress and illness. Malays J Med Sci 2008;15:9–18. http://www.ncbi.nlm.nih.gov/pubmed/22589633.
- Feldman M, Walker P, Green JL, et al. Life events stress and psychosocial factors in men with peptic ulcer disease: a multidimensional case-controlled study. Gastroenterology 1986;91:1370–9. [CrossRef]
- Compas, BE. Compas BE. Stress and life events during childhood and adolescence. Clin Psychol Rev 1987;7:275–302. [CrossRef]
- Riley, ID. Riley ID. Perforated peptic ulcer in war-time. Lancet 1942;243:485. [CrossRef]
- Dragstedt LR, Ragins H, Dragstedt LR, et al. Stress and Duodenal Ulcer. Ann Surg 1956;144:450–63. [CrossRef]
- Sonnenberg A, Müller H, Pace F. Birth-cohort analysis of peptic ulcer mortality in Europe. J Chronic Dis 1985;38:309–17. [CrossRef]
- Hikichi T, Sato M, Watanabe K, et al. Peptic Ulcers in Fukushima Prefecture Related to the Great East Japan Earthquake, Tsunami and Nuclear Accident. Intern Med 2018;57:915–21. [CrossRef]
- Aoyama N, Kinoshita Y, Fujimoto S, et al. Peptic Ulcers After the Hanshin-Awaji Earthquake: Increased Incidence of Bleeding Gastric Ulcers. Am J Gastroenterol 1998;93:311–6. [CrossRef]
- Glavin GB, Murison R, Overmier JB, et al. The neurobiology of stress ulcers. Brain Res Rev 1991;16:301–43. [CrossRef]
- Ganguli PC, Pearse AGE, Polak J, et al. Antral-Gastrin-Cell hyperplasia in peptic ulcer disease. Lancet 1974;303:583–6. [CrossRef]
- McGuigan JE, Harty RF, Maico DG. The role of gastrin in duodenal ulcer. Trans Am Clin Climatol Assoc 1981;92:199–207.http://www.ncbi.nlm.nih.gov/pubmed/6116307.
- Starcke K, Wiesen C, Trotzke P, et al. Effects of Acute Laboratory Stress on Executive Functions. Front Psychol 2016;7:1–8. [CrossRef]
- Brouwer A-M, Hogervorst MA. A new paradigm to induce mental stress: the Sing-a-Song Stress Test (SSST). Front Neurosci 2014;8:1–8. [CrossRef]
- Dong SXM. Novel Data Analyses Address the African Enigma and Controversies Surrounding the Roles of Helicobacter pylori in Peptic Ulcers. Preprint Published Online First: 2023. [CrossRef]
- Dong SXM. Novel data analyses explain the seasonal variations of peptic ulcers. Preprint 2023;:2023020271. [CrossRef]
- Record, CO. Record CO. Controversies in Management: Helicobacter pylori is not the causative agent. BMJ 1994;309:1571–2. [CrossRef]
- Linda R, Ransohoff DF. Is helicobacter pylori a cause of duodenal ulcer? A methodologic critique of current evidence. Am J Med 1991;91:566–72. [CrossRef]
- Zelickson MS, Bronder CM, Johnson BL, et al. Helicobacter pylori is not the predominant etiology for peptic ulcers requiring operation. Am Surg 2011;77:1054–60.http://www.ncbi.nlm.nih.gov/pubmed/21944523.
- Walsh JH, Peterson WL. The Treatment of Helicobacter pylori Infection in the Management of Peptic Ulcer Disease. N Engl J Med 1995;333:984–91. [CrossRef]
- Marshall BJ, Goodwin CS, Warren JR, et al. Prospective double-blind trial of duodenal ulcer relapse after eradication of Campylobacter pylori. Lancet (London, England) 1988;2:1437–42. [CrossRef]
- Sivri, B. Sivri B. Review Article: Trends in peptic ulcer pharmacotherapy. Fundam Clin Pharmacol 2004;18:23–31. [CrossRef]
- Gigch JP Van. Book review: Design of the modern inquiring system—i. r. descartes (1596–1650). Syst Res Behav Sci 1988;5:267–9.
Figure 1.
Vertical Superposition of the annual mortality rate of gastric ulcers. This figure represents an ideal/hypothetical scenario with all three categories. The total annual mortality rate is the sum of the annual mortality rates caused by misdiagnoses (blue), common events (green), and crucial events (light yellow) in a given year. In the first year, only misdiagnoses and common events caused the total annual mortality rate. In the second year, psychological stress due to a sudden outbreak of a war markedly increased the total annual mortality rate. The war ended in the third year, leading to a sharp decrease in the mortality rate in the fourth year. In the fifth year, the total annual mortality rate was caused only by misdiagnoses and common events again. When an economic crisis occurred in the sixth year, the total annual mortality rate increased markedly again and peaks in the seventh year. Since the economy was restored gradually in the eighth and ninth years, the annual mortality rates decreased accordingly. Due to the peaceful environment and potential medical advancement in the tenth year and afterward, the total annual mortality rates caused by misdiagnoses and common events declined gradually.
Figure 1.
Vertical Superposition of the annual mortality rate of gastric ulcers. This figure represents an ideal/hypothetical scenario with all three categories. The total annual mortality rate is the sum of the annual mortality rates caused by misdiagnoses (blue), common events (green), and crucial events (light yellow) in a given year. In the first year, only misdiagnoses and common events caused the total annual mortality rate. In the second year, psychological stress due to a sudden outbreak of a war markedly increased the total annual mortality rate. The war ended in the third year, leading to a sharp decrease in the mortality rate in the fourth year. In the fifth year, the total annual mortality rate was caused only by misdiagnoses and common events again. When an economic crisis occurred in the sixth year, the total annual mortality rate increased markedly again and peaks in the seventh year. Since the economy was restored gradually in the eighth and ninth years, the annual mortality rates decreased accordingly. Due to the peaceful environment and potential medical advancement in the tenth year and afterward, the total annual mortality rates caused by misdiagnoses and common events declined gradually.
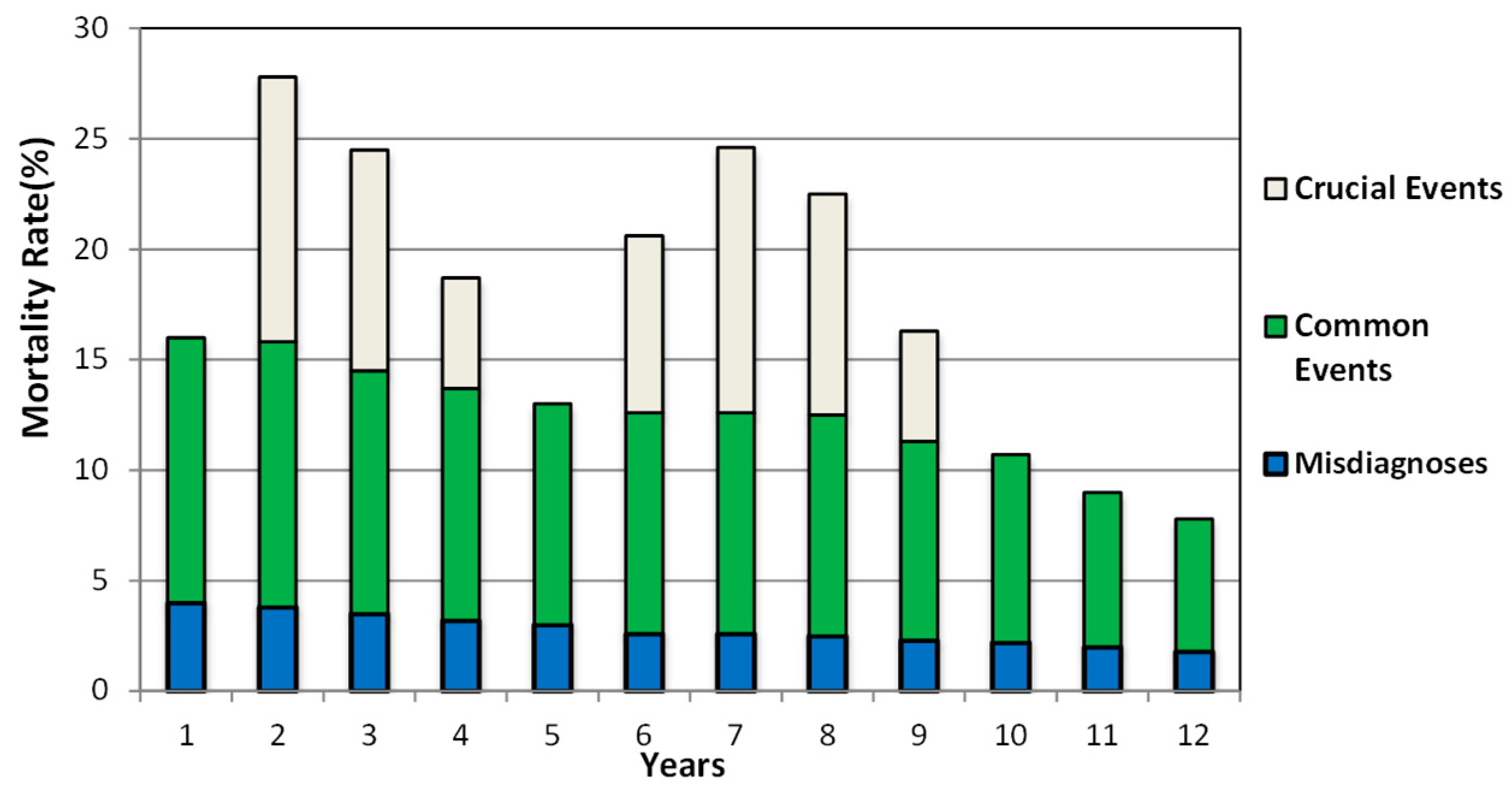
Figure 2.
Horizontal Superposition of the mortality rates of gastric ulcers. This figure illustrates the same scenario as that in Figure 1 but in the format of a line graph. Line 1 is the temporal trend of the annual mortality rates caused solely by misdiagnoses; Line 2 is the temporal trend of the sum of annual mortality rates caused by misdiagnoses and common events; Line 3 is the temporal trend of the total annual mortality rates caused by misdiagnoses, common events, and crucial events. The sharp increases in Line 3 resulted from the occurrence of two crucial events and the rapid declines indicate that the negative impacts of the two crucial events were diminishing. After the tenth year, the absence of crucial events led to the coincidence of Line 2 and Line 3, where the total annual mortality rates slightly declined due to the sustained improvements in medical conditions and living environments.
Figure 2.
Horizontal Superposition of the mortality rates of gastric ulcers. This figure illustrates the same scenario as that in Figure 1 but in the format of a line graph. Line 1 is the temporal trend of the annual mortality rates caused solely by misdiagnoses; Line 2 is the temporal trend of the sum of annual mortality rates caused by misdiagnoses and common events; Line 3 is the temporal trend of the total annual mortality rates caused by misdiagnoses, common events, and crucial events. The sharp increases in Line 3 resulted from the occurrence of two crucial events and the rapid declines indicate that the negative impacts of the two crucial events were diminishing. After the tenth year, the absence of crucial events led to the coincidence of Line 2 and Line 3, where the total annual mortality rates slightly declined due to the sustained improvements in medical conditions and living environments.
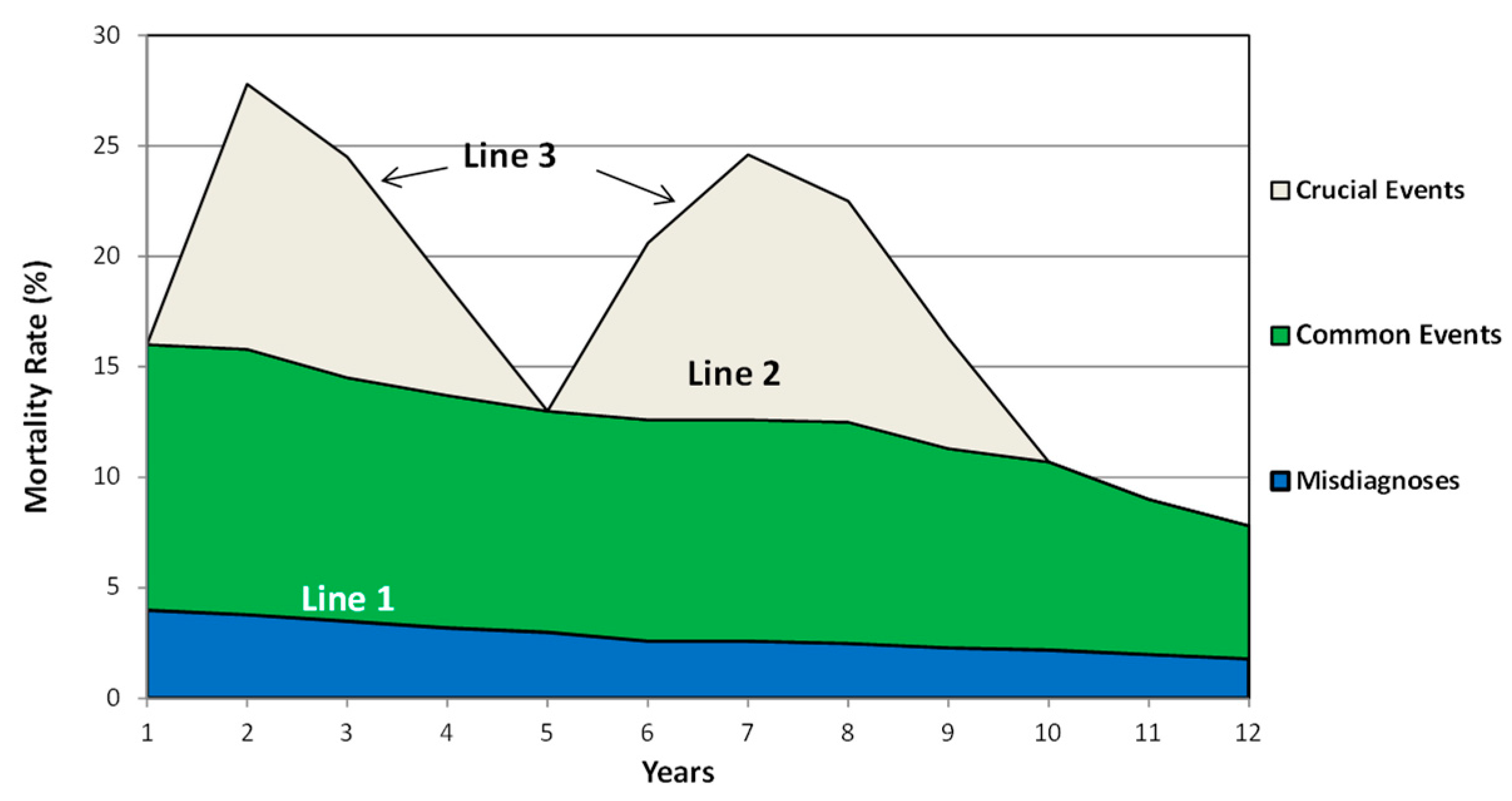
Figure 3.
Overlapping of the fluctuation curves caused by a succession of crucial events. People in England and Wales experienced at least 4 crucial events successively during the 1910s to 1940s. Line 1 and Line 2 are the temporal trends of misdiagnoses and common events as described in Figure 1. Curve D2-P1-C1-B3 is the fluctuation curve caused solely by the First World War; curve B1-C1-P2-C2-B5 is caused solely by the rebuilding after the war; curve B3-C2-P3-D8-B8 is caused solely by the economic crisis and curve B5-C3-P4-D10-D11 is caused by the Second World War and the rebuilding after the war. P1, P2, P3, and P4 are the peaks of these curves. Overlapping areas of the crucial events are B1-C1-B3-B2, B3-C2-B5-B4, and B5-C3-B7-B8-B6.
Figure 3.
Overlapping of the fluctuation curves caused by a succession of crucial events. People in England and Wales experienced at least 4 crucial events successively during the 1910s to 1940s. Line 1 and Line 2 are the temporal trends of misdiagnoses and common events as described in Figure 1. Curve D2-P1-C1-B3 is the fluctuation curve caused solely by the First World War; curve B1-C1-P2-C2-B5 is caused solely by the rebuilding after the war; curve B3-C2-P3-D8-B8 is caused solely by the economic crisis and curve B5-C3-P4-D10-D11 is caused by the Second World War and the rebuilding after the war. P1, P2, P3, and P4 are the peaks of these curves. Overlapping areas of the crucial events are B1-C1-B3-B2, B3-C2-B5-B4, and B5-C3-B7-B8-B6.
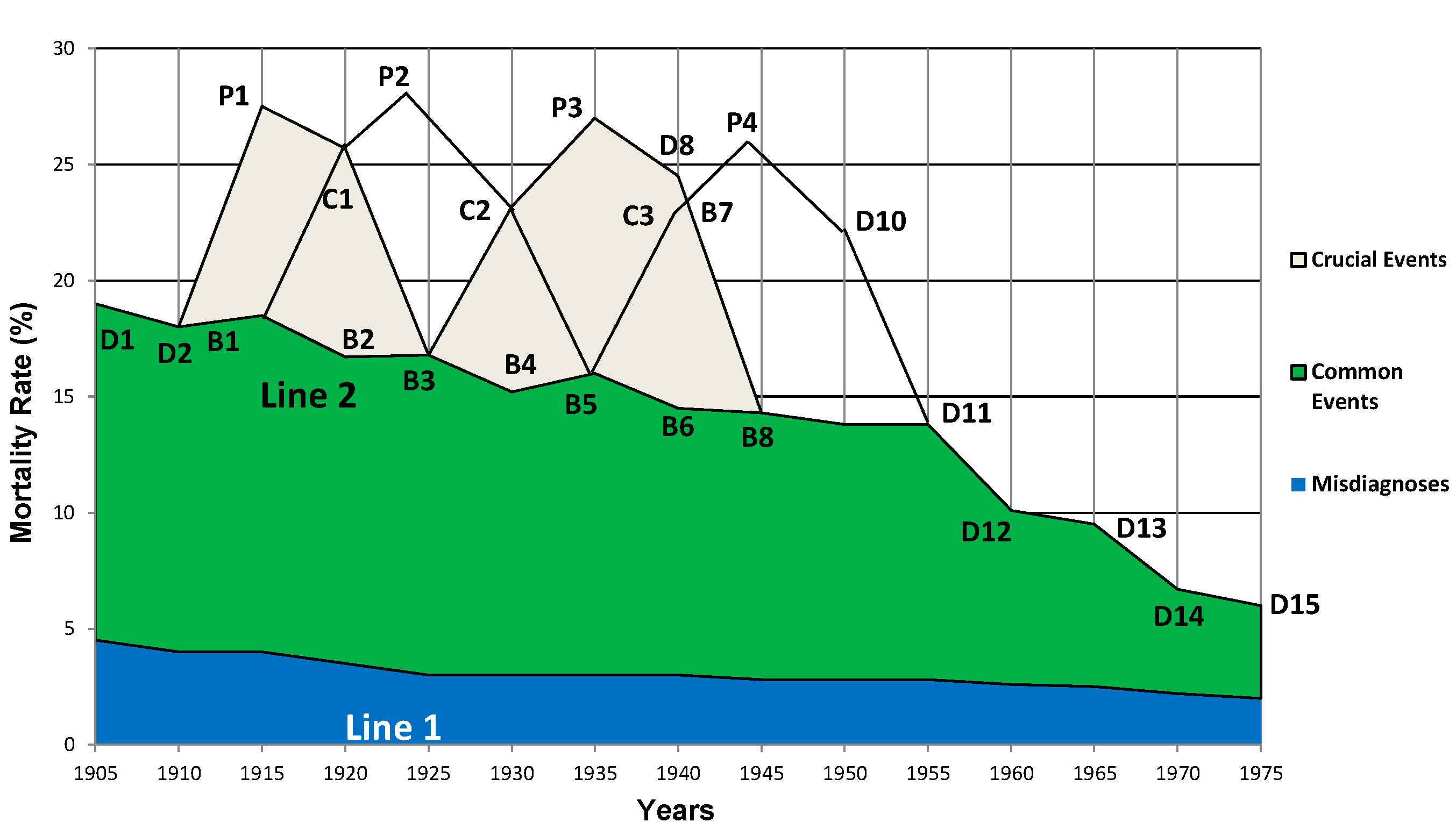
Figure 4.
Producing the fluctuation curve of a real scenario in England and Wales 1905-1975. Line 1 and Line 2 are identical to those in Figure 3. The solid line from D1 to D15 is a theoretical fluctuation curve on a five-year basis from 1905 to 1975. However, Susser and Stein’s birth-cohort study was on a ten-year basis from 1905 to 1975, of which the fluctuation curves could be produced by joining the points D1-D3-D5-D7-D9-D11-D13-D15 as illustrated by the dashed Line 3. D3 has the same value as P1 in Figure 3. Similarly, D5=P2, D7=P3, D9=P4 and points D1, D11, D13, D14 and D15 are identical to Figure 3.
Figure 4.
Producing the fluctuation curve of a real scenario in England and Wales 1905-1975. Line 1 and Line 2 are identical to those in Figure 3. The solid line from D1 to D15 is a theoretical fluctuation curve on a five-year basis from 1905 to 1975. However, Susser and Stein’s birth-cohort study was on a ten-year basis from 1905 to 1975, of which the fluctuation curves could be produced by joining the points D1-D3-D5-D7-D9-D11-D13-D15 as illustrated by the dashed Line 3. D3 has the same value as P1 in Figure 3. Similarly, D5=P2, D7=P3, D9=P4 and points D1, D11, D13, D14 and D15 are identical to Figure 3.
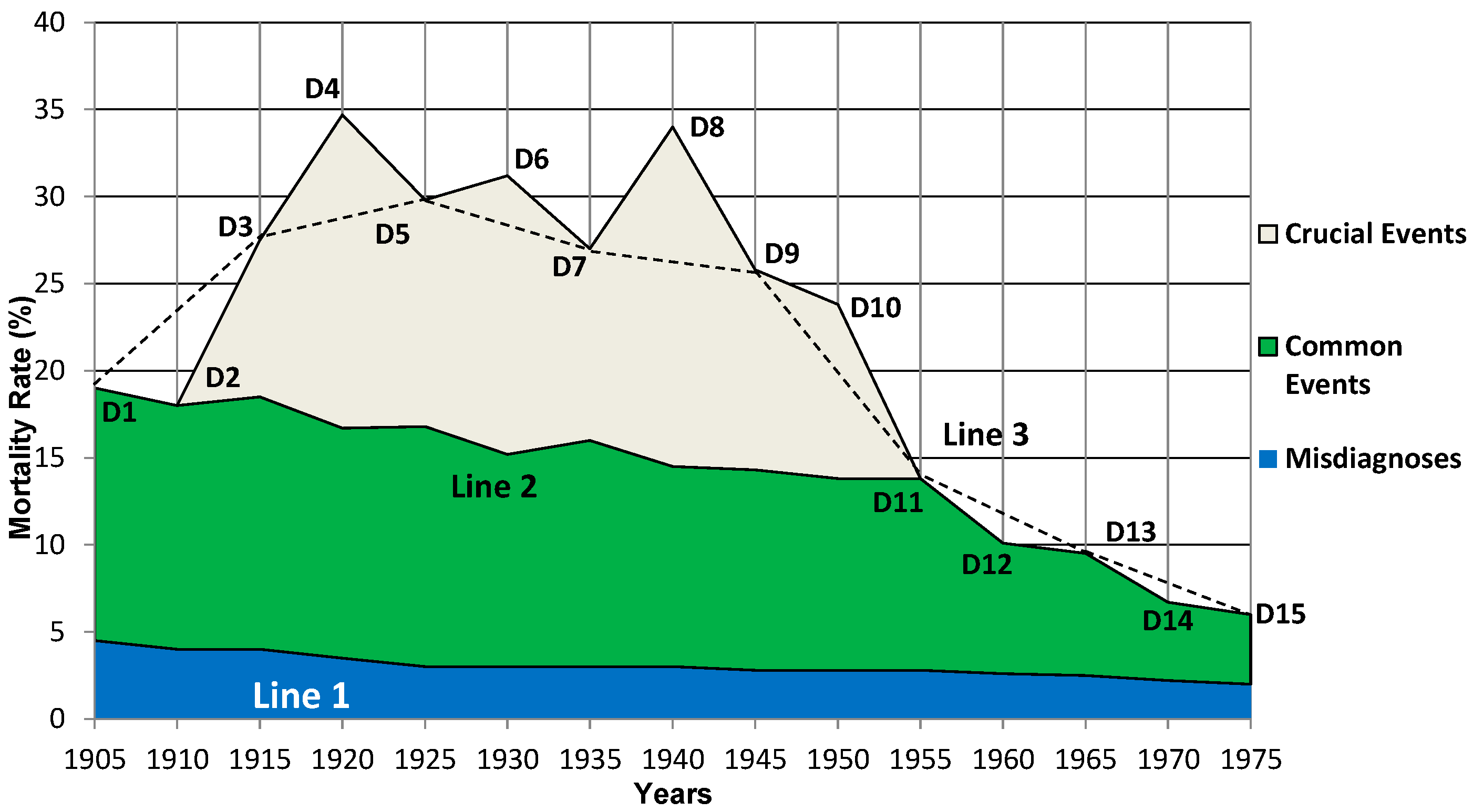
Figure 5.
Reproduction of the fluctuation curve of annual mortality rates from 1905 to 1975. In Susser and Stein’s studies, data was collected every 10 years whereas this study analyzed 5-year intervals. By removing the years not investigated in Susser and Stein’s reports (1910, 1920, 1930, 1940, 1950, 1960, 1970) in Figure 4, the dashed Line 3 presents herein reproduced a fluctuation curve in the birth-cohort phenomenon of gastric ulcers observed by Susser and Stein.
Figure 5.
Reproduction of the fluctuation curve of annual mortality rates from 1905 to 1975. In Susser and Stein’s studies, data was collected every 10 years whereas this study analyzed 5-year intervals. By removing the years not investigated in Susser and Stein’s reports (1910, 1920, 1930, 1940, 1950, 1960, 1970) in Figure 4, the dashed Line 3 presents herein reproduced a fluctuation curve in the birth-cohort phenomenon of gastric ulcers observed by Susser and Stein.
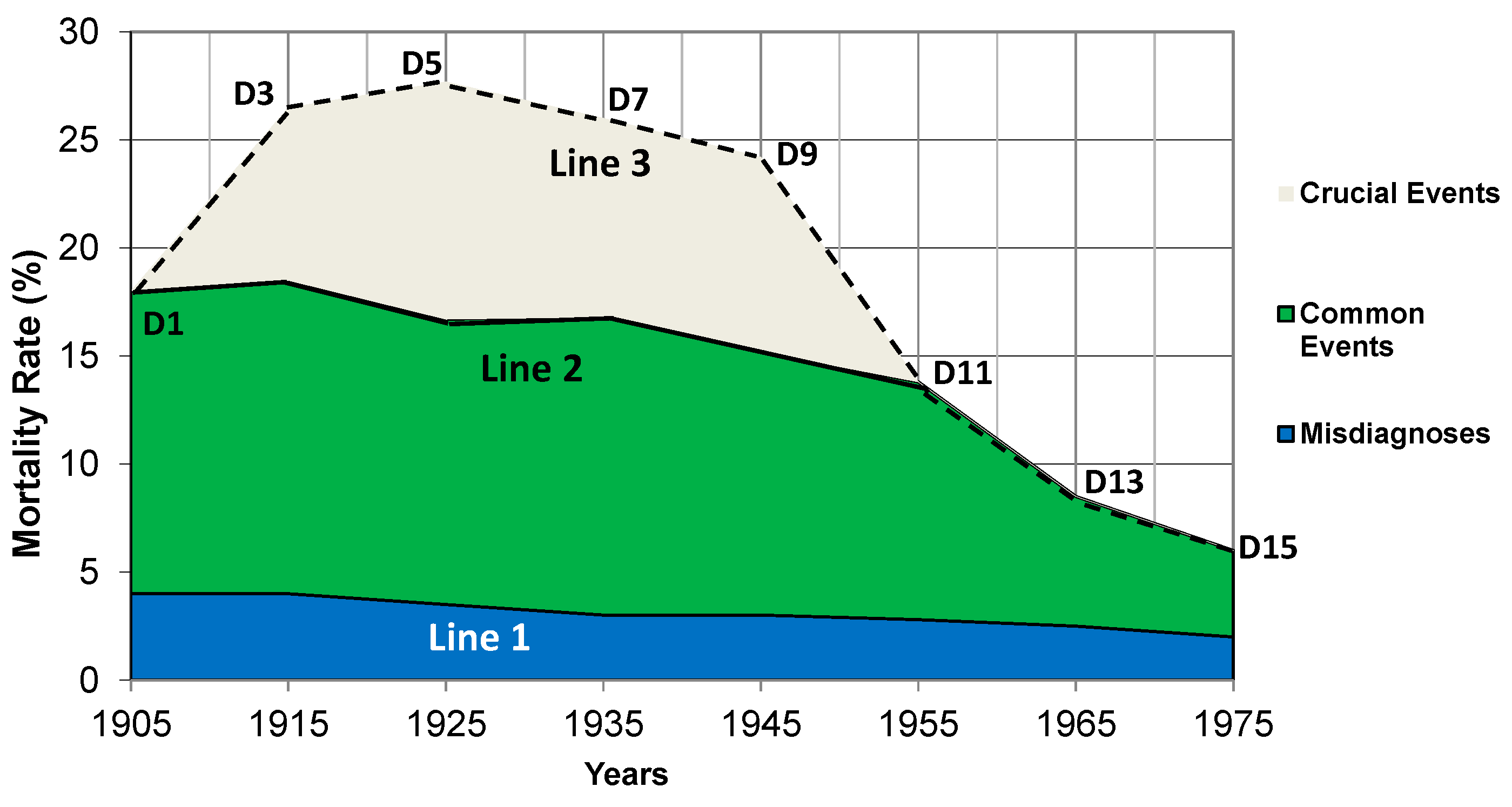

Table 1.
Classification of factors causing annual mortality rates of peptic ulcers.
| Category | Factors | Features |
|---|---|---|
| Clinical Misdiagnoses | Misdiagnoses: commonly seen in the 20th century. |
|
| Common Events |
|
|
| Crucial Events | Extraordinary environmental factors:
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



