
Submitted:
17 December 2025
Posted:
18 December 2025
You are already at the latest version
Abstract
The much higher rate of premature mortality from cancer among people with mental ill-health is a major contributor to 20-year reduction in life expectancy for this population, relative to the broader population. Under-screening and delays in screening for cancers are recognised as significant issues contributing to this health inequality. This thematic review explored the common barriers to delayed cancer screening, facilitators to overcome those barriers, and the associated recommendations to improve screening rates for people with mental ill-health. A review of current literature high-lighted key themes contributing to the health disparity experienced by this population, including social determinants of health, comorbidities, and health system factors. Facilitators such as trust, support, self-care, and interventions at a health system level were also highlighted. Study quality was appraised using the MMAT v.18 and CASP tools. All studies that met the inclusion criteria, regardless of quality, were included in the review to provide a comprehensive analysis of the existing literature on this topic. Building upon this literature, further recommendations are presented on how to reduce the cancer screening inequality experienced by people with mental ill-health.
Keywords:
cancer screening
; mental ill-health
; barriers
; facilitators
; recommendations
; service users
; mental health
1. Introduction
Cancer is among the main causes of death globally, according to the World Health Organization [1]. In 2021, it was reported that globally, approximately 1.1 billion people were living with mental ill-health [2]. Despite the high prevalence of mental health conditions, significant health inequalities persist for this population, particularly regarding cancer screening. The rate of premature mortality from cancer among people with mental ill-health is approximately 16 per day compared to an expected 1.8 deaths per day in the general population [3]. This contributes to the reported 20-year reduction in life expectancy relative to the general population [3]. For breast cancer specifically, it is reported that individuals with mental ill-health are six times more likely to die prematurely from the disease than those in the general population [4].
In the existing international literature, it is well-reported that people with mental health conditions are under-screened or receive delayed cancer screening; thus, contributing to a lower life expectancy in this population compared to the general population [5,6]. Specifically, breast and lung cancer are amongst the top cancers that are the leading causes of death, and that account for higher earlier than expected death rates, for people with mental ill-health [7]. Despite the evident health inequality, solutions to delayed screening services in these mental health service populations is limited [8]. It is unclear why people with mental ill-health (hereafter referred to as ‘service users’ where applicable) receive delayed screening or are under-screened.
Addressing this health inequality is relevant to health practitioners, people with mental ill-health, and family, carers and kin providing support to them. Identifying factors that contribute to delayed cancer screening can help healthcare practitioners to improve their practices, be more proactive and conscientious in their interactions with service users who experience mental ill-health, and improve their communication with other healthcare practitioners to prevent delayed cancer screening. Similarly, identifying factors that contribute to delayed cancer screening for service users with mental ill-health can shed light on the role that support systems might play in contributing to this issue, and how they can help to address it.
The objective of this research project is to address this gap in three ways. Firstly, by identifying themes that contribute to delayed cancer screening. Secondly, by collecting recommendations and suggesting what can be done to improve cancer screening for people with mentally ill-health. Thirdly, by exploring the experiences of people with mental ill-health regarding cancer screening through applying a qualitative (interpretivist) approach.
2. Materials and Methods
The study included adults above 18 years of age who were mental health service users, residing in community settings, with contact across primary, secondary, and/or tertiary health systems. Eligible articles were peer-reviewed, published in English, and had a publication timeframe from inception or records to February 18, 2024.
We excluded studies involving adolescents, populations not in community settings (eg. Prisons or other institutions), editorials, conference papers, unpublished theses, reports, protocols, studies not reporting mental health sample data separately, and epidemiological studies not reporting service user perspectives of cancer screening. Barriers, facilitators, and recommendations were not used as inclusion criteria but were explored as outcomes later during the data extraction stage.

Table 1.
Table of inclusion and exclusion criteria.
| Element | Description | Inclusion Criteria | Exclusion Criteria |
|---|---|---|---|
| Population | Adults who are mental health service users. | -Adults above 18 years of age who were mental health service users. -Community dwelling populations. |
-Adolescents under 18 years of age. -Populations not in community settings (eg. Prisons). |
| Concept | Perspectives of mental health service users. | -Studies reporting mental health data separately. -Studies reporting service user perspectives and/or lived experiences of cancer screening. |
-Studies not reporting mental health data separately. -Studies not reporting service user perspectives and/or lived experiences of cancer screening. |
| Context | Health system and community settings. | -Community based settings with primary/secondary/ tertiary health system contact points. | -Non-community settings/institutions. |
| Type of Evidence Source | Publication type | -Peer-reviewed journal articles. | -Editorials. -Conference papers. -Unpublished theses. -Reports. -Study protocol papers. -Epidemiological studies. |
| Time Frame | Publication period. | -Inception to February 18, 2024. | -Publications outside this time frame. |
| Language | Language of the publication. | -English. | -Non-English. |
Assistance from the Flinders University research librarian was utilized in developing the search strategy. MEDLINE, (APA) PsycINFO, Scopus, and EMcare databases were searched via OVID (for MEDLINE, PsycINFO, and EMcare) and Elsevier (for Scopus) with a first search on July 2, 2023 and a final updated search on February 18, 2024. A keyword search was implemented using the following groups of terms: 1) “mental health” OR “mental illness”, 2) “miss*” OR “less likely” OR “reduced” OR “under screened” OR “influences”, and 3) “cancer screening” OR “cancer prevention” OR “cancer detection”. The terms were then combined (1 and 2 and 3) to identify relevant literature (see Supplementary File S1 for Medline search exemplar). Searches were limited to English-language, peer-reviewed journal articles.
After removing 270 duplicates from the initial 433 records in Covidence, 163 studies were screened and 41 underwent full-text review, resulting in 37 included studies that clearly met the inclusion criteria. Data extraction was piloted with a small number of included studies. The two reviewers (SL and CB) then discussed/checked parsimony of the piloted approach in capturing the content of interest in answering the research project’s aim before proceeding with extracting data across the identified included papers. The two reviewers (SL and CB) independently screened titles/abstracts and full texts, with discrepancies resolved via discussion. A descriptive summary table, generated using Microsoft Word, was tabulated for comparison amongst the eligible articles. This summary included: surname of first author/year/country, study aims/purpose, participant samples, methods/design, findings/conclusions, limitations (Supplementary File S2). The first reviewer (CB) extracted all the data; the second reviewer (SL) independently and randomly selected ~20% of the included articiples, reviewing them against the data collected by the first reviewer to ensure accuracy and consistency in approach, and then reviewed the complete collected summary data to ensure a consistent and succinct format. The reviewers worked independently and resolved any disagreements via discussion.
Outcomes of interest were barriers, facilitators, and recommendations related to cancer screening among service users. Barriers were defined as factors that prevented or delayed engagement with cancer screening; facilitators were defined as factors that prompted engagement; recommendations were defined as suggestions by articles on how to improve cancer screening uptake. The time-points when data were collected for the eligible articles were conducted heterogeneously. For instance, some studies used retrospective data collection. Similarly, the measurement methods were also done heterogeneously: for instance, some studies were cross-sectional surveys while others were cohort studies.
A deductive thematic framework using predefined outcome domains of interest (barriers, facilitators, and recommendations) as the main themes, was applied to the data. All extracted results that aligned with these outcome domains in each study were explicitly sought. No changes were made to the inclusion or definition of outcome domains, or to the importance given to them in the review. No changes were made to the processes used to select results within eligible outcome domains. Within this deductive structure, inductive subthemes were developed based on emerging patterns from the extracted data, within each of the three domains of interest. Facilitators and barriers to cancer screening uptake were considered the most important outcome domains for interpreting the review’s conclusions as they reflected the experiences of mental health service users with screening services. Experiences with screening services have the potential to influence screening rates/uptake.
Study quality was independently assessed by the two reviewers using the Mixed Methods Appraisal Tool Version 2018 (MMAT v.18) for qualitative, quantitative, and mixed methods studies, and the Critical Appraisal Skills Programme (CASP) quality rating items for systematic reviews [9]. One reviewer (CB) assessed all the studies; the second reviewer (SL) randomly screened 20% of the included studies using these quality rating tools prior to finalizing the quality rating tables. Discrepancies were resolved amongst the two reviewers via discussion.
Overall, a majority of included studies were rated as moderate to high quality (3-5 stars) on the MMAT v.18 across the different study designs (see Supplementary File S3 Tables S1-S5 for further detail). We therefore concluded that there was low risk of bias for the extracted data types.
Overall, a majority of the systemic reviews satisfied the CASP quality rating items, being scored as Yes (Y) across most or all questions. However, some uncertainty remained, particularly regarding the precision of results and applicability to local populations (see Supplementary File S3 Table S6 for further detail). Across all study types, no processes were used to obtain/confirm relevant further information from original study investigators.
We conducted a thematic analysis of findings based on Braun and Clarke’s 6-phase approach [10]. We first reviewed the 37 included studies (Phase 1: familiarization with the data) [10]. To facilitate a thorough examination of the findings, we undertook a series of steps to curate and display the data. Following the initial population of a descriptive summary table, we examined data within the articles specific to our study aims. To achieve this, a summary of findings table was generated to visually display overall findings of individual articles regarding barriers, facilitators and recommendations for addressing under-screening (Phase 2: generating initial codes) [10]. The summary of findings table included: surname of first author/year/country, aims/purpose, and findings (barriers, facilitators, and recommendations (Supplementary File S4). From the summary of findings table, inductive coding was performed to group codes into broader themes (Phase 3: searching for themes) [10]. To visually display the major themes amongst articles, we generated dedicated thematic tables (Phase 4: reviewing themes), each separately displaying barriers, facilitators and recommendations, with common themes and subthemes noted (Phase 5: defining and naming themes; see Supplementary Files S5-S7) [10]. Finally, phase 6 involved reporting and analyzing the themes in this review [10].
3. Results
Of the 37 papers identified in this review (see Figure 1), 20 were conducted in the United States of America (USA), seven in the United Kingdom (UK), 4 in Australia, 2 in Canada, and 1 each in Denmark, the Netherlands, Spain, and Sweden. Nineteen studies focused on cancer screening for women with mental illness, with the remainder involving women and men in their samples. Age of sample populations varied from 18+ years to a focus on older populations. Sample sizes also varied, influenced by the type of study designs, with the cohort studies involving many thousands in their samples. Most studies involved analysis of existing data from specific registries or large administrative datasets (n=17), with seven descriptive cross-sectional studies, five reviews, three RCTs (randomized controlled trials), three mixed methods designs, and three qualitative studies. The type of cancer screening in focus also varied across the studies (see Table 2).
The remaining studies (N=13) involved cancer screening of any type and more broadly; included some studies with specific groups including people with comorbid substance abuse disorder and mental illness [47], and military veterans [26,48].
There were three major themes involving barriers to screening: social determinants of health, mental health/comorbidities, and the health system. Each major themes then had various subthemes within them. There were nine subthemes identified within social determinants of health, six within mental health/comorbidities, and five within the health system. These are summarized below [see Supplementary File S5 for further detail].
3.1. Social Determinants of Health as a Barrier
Social determinants of health are the social and demographic conditions that effect the biological and psychological mental health of individuals’ lives [11].
3.1.1. Education
Low levels of health literacy and education were identified as major barriers for cancer screening due to individuals not fully understanding the associated risks or information health practitioners provided. Individuals with lower levels of education tend to be screened for cancers less than those with higher levels of education/health literacy [12,13,14,15,16,17]. Irwin mentioned that health care providers might not be educating patients about smoking cessation appropriately [14]. However, it appears that there’s a significant gap in the literature regarding how health practitioners explain information to people with mental health conditions.
3.1.2. Age
Various literature cited increasing age as another major barrier to cancer screening [12,16,18,19,20,21,22,23]. There seemed to be a negative association between age and cancer screening rates, particularly in cervical and breast cancer screening [16]. Older aged females were more likely to have missed Pap test and mammograms for cervical cancer and breast cancer respectfully [16]. Compared to other females in New South Wales (NSW), women 65 years old or greater with mental illness received 41% less screening rates and women 34 years or younger with mental illness received 5-10% less screening rates [23]. Variations amongst age groups might be attributable to the cohort effect [23]. However, one literature found that screening in individuals with mental health conditions was low regardless of the age group [24].
3.1.3. Low Income and Finances
Financial costs, lack of insurance, and low income were other barriers abundantly cited in the literature [13,16,17,19,20,23,25,26,27,28,29,30]. In particular, one article found this to be problematic for cervical and breast cancer screening [16]. However, another article noted that this is a barrier that many people experience, not just mental health service users [28].
3.1.4. Distance
Lack of transport to enable travel to screening facilities prevented some service users from being able to obtain cancer screening [19,20,31]. Also, the further away the screening facility is, the more difficult it can be to physically get there [16,17,23,24]. Additionally, screening participation was impeded when a screening facility was unfamiliar to the service user; especially for mamographies [32]. Unfamiliar screening facilities contributed to lack of familiarity with staff at that location and thus less trust in the facility [32].
3.1.5. Reduced Access
3.1.6. Gender and Socio-Economic Status
The gender of the health providers and service users impacted screening participation. Female health providers were preferred by female service users, particularly for cervical screening or history of sexual assault [12,34]. For colorectal cancer screening, non-adherence was greater if the service user was female compared to male [15]. Socioeconomic status was a major sub-theme identified in the literature. In all levels of socioeconomic status, women with mental illness were under screened for breast cancer [24].
3.1.7. Culture
Culture can impact screening rates in mental health service users, particularly for minority cultural groups whose primary language was different to the dominant language used by services and systems [12,13,17,22]. Tsai found that survivors of breast and prostate cancer were under screened if they were non-Hispanic other (NHO)/Hispanic as opposed to other races including non-Hispanic White (NHW) and non-Hispanic Black (NHB) [30] (pp. E714-E724). Being Aboriginal or Torres Strait Islander also resulted in less screening participation [24].
3.1.8. Never Married
Three articles found that never being married influenced cancer screening rates. There was an association amongst missing a Pap test and women who had never been married [16]. Never being married possibly results in women not having encountered preventative gynaecological services before [13]. More generally, being single was a barrier to accessing preventative cancer screening [17].
3.1.9. Reproductive History
3.2. Mental Health or Medical Comorbidities as a Barrier
3.2.1. Mental Health Condition and Severity
The more severe the mental health condition, the more this negatively impacted cancer screening participation [21,24,32]. Woodhead attributed this reduction to people with mental-ill health being less likely to seek help [32] (p. 819). Cervical cancer screening was impacted negatively by anxiety and depression [35], and depression also negatively impacted breast cancer screening [16]. Additionally, depressive symptoms might enhance the feeling of helplessness and then further deter individuals from seeking help [12]. Vigod however, found that even with more appointments to see a primary care physician, mental health service users still received less cancer screening [36] (pp. 159-168). However, increased number of hospital admissions negatively influenced screening adherence [22].
Some literature reported that having a mental health condition resulted in decreased screening for service users [18,27,37]. Furthermore, the severity of the mental health condition influenced participation in cancer screening [18], and some service users under-estimated their risk of cancer [14]. It seems like the more psychological distress the service user is experiencing, the less likely they’re screened for cancer [38]. Some literature found mixed results depending on the type of mental health diagnosis [12,22,39,40].
3.2.2. Medical (Non-Psychiatric) Comorbidities
There seems to be a negative association amongst poor physical and/or mental health and cancer screening [12,13]; generally, the poorer one’s physical or mental health, the lower the screening rate [30]. Aggarwal suggested that comorbidities have the potential to distract the health provider from cancer screening [12] (pp. 392-398).
3.2.3. Cognitive Difficulties/Impairment and Motivation
Mental health service users may experiecne cognitive diffiuclties and/or impairment that then impacts their participation in preventative care services such as cancer screening [13,14,27,33,38,41]. Mental health conditions can negatively affect individuals’ motivation and concentration which then prevents them from accessing screening services [22,30,31,32,33,38]. This can include problems with recall which prveents them from actioning referrals for screening and atending follow-up appointments.
3.2.4. Embarrassment/Stigma/Shame
Embarrassment, stigma, and shame surrounding mental health was suggested to be a common potential barrier to cancer screning [19,20,23,27,28,34,35,41], specifically for breast and cervical cancer screening [24]. This stigma resutled in reduced access to care [29]. Prejudiced attitudes of health practitoners also contributes to the barrier for mental health service users in accessing screening [43]. Interestingly, one article found that stigma was a barrier identified by both service users and mental health professionals [31]. Another article identified that embarassment was a particular barrier for obese women [13].
3.2.5. Patient Concerns About Screening (eg. Trauma, Procedures, Fear)
Fear or distrust due to past trauma experiences as part of receiving psychiatric treatment, and associated concerns with the screening process itself, were noted as key barriers to cancer screening [23,28,29,34]. Some women tended to delay/avoid breast and cervical cancers specifically if they had a history of sexual trauma [24]. Other service users reported that they were under screened because they feared receiving bad news and because of the potential for trauma [31].
Two articles noted that the nature of the screening test might be a factor that deters service users from participating in screening; specifically for cervical screening. Cervical cacner screening is an “intimate” process that service users might not feel comfortable with [23]. Some service users also delay/avoid getting cervical csreening because the process feels “impersonal” to them [17].
3.2.6. Smoking
Smoking was a barrier to cancer screening in service users with mental illness. One article attributed the decrease n screening participation to smokers already engaging in one unhealthy activity (smoking) and being more prone to participate in other unhealth behaviours [13]. People with mental ill-health have a higher chance of engaging in unhealthy activities such as smoking and being under screened for cancer [25]. More generally, Zhang found that service users who smoked were less likely to receive their cervical and breast cancer screening [16].
3.3. The Health System as a Barrier
3.3.1. Delaying Care/Prioritization
Many service users were under screened for cancer because either they or their healthcare provider delayed or placed it as a lower priority compared to other medical conditions or to their mental health conditions [15,29,34,35,41]. Specifically, breast and cervical cancer screening were delayed if service users expereinced symptoms such as anxiety or if they didn’t prioritize timely screening [16].
Lack of time is a barrier that is shared amongst mental health service users, the broader population, and health professionals [28,31]. Health professionals might not have enough time to screen individualsm whereas, service users have difficulty dedicating a block of their time to get screened [31].
3.3.2. No Primary Care Provider
Not having a primary care provider was typically associated with reduced cancer screening, but the reasons for this varied. This included simply not having one [19,20,27,35], problems with availability of primary care providers [26], or service user avoidance of the primary care setting [43]. One article found that not having a primary care provider was a mixed facilitator and barrier to cancer screening [12].
3.3.3. Siloed Health Systems
Lack of integration amongst mental health service users and physical health services was a barrier to screening participation [14,41]. System siloes included a lack of connection between cancer screening services and community mental health facilities [26], and lack of follow-up within and between services [28]. Siloes between systems were a barrier also encountered by the general population [28]. For health practitioners within these siloed systems, ambiguity or lack of role definition also resulted in under screening service users for cancer [14,22]; that is, if responsibility for cancer screening was unclear, no-one took responsibility.
Lack of communicaiton within siloed systems of care was a common barrier in the literature. Reduced communication amongst psychiatrists and primary care physicians was noted to be a barrier to cancer screening [19,20]. Similarly, lack of communication between various professionals in the health system contributed to lower screening rates; perhaps due to the uneven distribution of training for workers to develop their communciation skills [31].
The effect of lack of integration seemed to be particularly evident for breast and cervical cancer screening [24]. One article found a lack of integration to be a mixed barrier/facilitator according to the type of mental health condition, and that the integration of mental health treatment in primary care practices might explain why patients with major depressive disorder in medical homes used more preventive services compared to those with mental health conditions [39]. A lack of reminders seemed to be associated with lower levels of screening participation [19,20,28]. Mkuu noted that this barrier is expereinced by both mental health service users and the braoder population [28] (p. 252).
3.3.4. Physician Knowledge/Identification of Screening Candidates
Physicians’ lack of knowledge pertaining to mental illness and/or screening procedures served as a barrier to screening [31], as did psychiatric staffs’ lack of knowledge pertaining to cancer screening [22]. Baillargeon discovered that an incomplete health evaulation might be a barrier for receiving appropraite screening [25]. They noted that mental health service users might “drop out” prior to the health practitioner completing the cancer staging process [25].
3.3.5. Negative Attitudes and Diagnostic Overshadowing
Providers’ negative attitudes towards mental illness was perceived to be a common barrier to cancer screening [24,35]. Additionally, primary care providers that failed to acknowledge mental health complaints made by service users contributed to lower screening participation [38]. Some health professionals failed to properly identify woment hat were due for cancer screening; thus, resulting in lower participation rates [28]. Similarly, diagnostic overshadwoing, where service users’ physical symptoms were dismissed by physicians, was a common barrier cited in the literature [18,31,42].
In terms of facilitators, there were five major themes identified in this review: social determinants of health, increasing uptake in the health system, trust, support, and self-care. Each major theme then had various subthemes within them. There were six subthemes identified within increasing uptake in the health system, two within trust, three within self-care, three within social determinants of health, and two within support. These are summarized below (see Supplementary File S6 for further detail].
3.4. Social Determinants of Health as a Facilitator
Having the financial means or insurance to afford cancer screening was associated with improved screening rates [15,23,35,37]. Similarly, having the access to transport was associated with increased screening rates in service users [34]. Furthermore, having the screening process held at a familiar location led to an associated increase in screening participation amongst service users [31].
3.5. Increasing Uptake in the Health System as a Facilitator
Participation and/or cancer screening increase when staff are knowledgeable about the process and confident of their role. Additionally, the implementation of methods such as reminder phone calls, financial incentives, and targeted invitations also increase participation rates. In a similar manner, making the screening process easier for service users via more convenient testing, the use of community-based cancer navigators to aid service users, or the integration of mental and physical healthcare systems also improved screening rates and/or participation.
3.5.1. Knowledge
When staff are aware and knowledgeable about mental illness, service users are more comfortable obtaining healthcare (such as cancer screening) from them [31]. Knowledgeable staff can make the processes easier for service users by recognizing that they have a mental health condition (eg. more time needed to identify, create space for staff to ask and person to disclose).
3.5.2. Professional Role and Identity
Screening rates were facilitated by mental health professionals being conscious of their role to promote screening in service users [31].
3.5.3. Participation, Targeted Invitations, Phone Counselling
Action to implement routine systemic methods to increase participation was determined to be a facilitator in cancer screening uptake rates according to several articles. Reminders, such as phone calls, could serve as a prompt for service users [31,34,44]. Targeted invitation and phone counselling were also methods that improve the screening rates amongst service users [35]. Additionally, incentivizing service users (eg. financial incentive) was associated with higher rates of screening uptake [32,34].
3.5.4. Test Convenience
More convenient screening processes were associated with increased screening uptake, particularly for colorectal and cervical cancers. The ability to obtain a self-collected cervical cancer sample increased the convenience of the screening process [23]. In a similar manner, faecal immunochemical test (FIT) was determined to be more convenient than guaiac faecal occult blood test (gFOBT) for service users [44].
3.5.5. Community-Based Cancer Navigators
Community-based cancer navigators faciliated cancer screening by working directly with service users to help overcome barriers, link them with services, fill gaps in communicaiton, information exchange and accessibility [42].
3.5.6. Service Integration
3.6. Trust in the Service and Health Professionals as a Facilitator
Previous positive experiences with the health system, being able to choose the gender of healthcare provider, and having a regular primary care provider all positively impact engagement with cancer screening.
3.6.1. Trust and Positive Experience
When individuals with mental illness trust their primary care provider, this has the potential to lead to improved screening participation [12,38]. Previously having a positive experience with the health system and/or health professionals was a facilitator for screening uptake [31,34]. Having a good prior healthcare experience suggests that individuals would be more likely to return for follow-up care, and also future opportunities for prevention and earlier interevntion screening.
3.6.2. Healthcare Provider Gender
3.7. Presence and Nature of Support as a Facilitator
3.7.1. Support
A solid support network was associated with increased likelihood of partaking in cancer screening; whether it be support from professionals such as the primary care provider or informal social, emotional, or instrumental support such as from family or friends [12,27,34,38]. Perhaps this is because support involves encouragement to be proactive about cancer screening and address the individual’s concerns/fears, practical support to overcome barriers and obtain screening services, and role models for information and advice.
3.7.2. Presence of a Primary Care Provider and Continuity of Care
Most articles identified having a clearly designated primary care provider as a facilitator to cancer screening [27,32,38] because it likely correlated to better continuity of care [31,35,42]. However, one article identified having a primary care provider as a mixed barrier and facilitator depending on the literature [12]. Continuity of care seemed to be particularly beneficial in improving uptake for cervical cancer screening via the Pap test [17].
3.8. Positive Approach to Self-Care as a Facilitator
3.8.1. Self-Care
3.8.2. Awareness of Physical Symptoms
Being able to identify physical symptoms (eg. finding a breast lump, which prompted seeking a healthcare check) was associated with increased participation in cancer screening [31].
3.8.3. Diagnosis and Mental Health
Three articles found that having a diagnosis/mental health condition was associated with increased screening [13,24,31]. However, two articles found that the type of diagnosis/mental illness determined whether it was a barrier or facilitator to cancer screening [12,39]. Domino found that service users with less severe mental health conditions (like major depressive disorder) had lower amount of specialy mental health visits but accessed preventative services in medical homes more than service users with illnesses such as schizophrenia [39]. Aggarwal cited one literature that mentioned less breast cancer screening with psychotic disorders and another that mentioned increased breast cancer screening with substance use disorders [12].
4. Discussion
Current literature reports various barriers and facilitators to cancer screening in people with mental ill-health. Common barriers included: social determinants of health (eg. Culture, distance, access, finances), mental health/comorbidities, the health system (eg. Delayed care, siloed health systems, lack of primary care provider). Common facilitators included: social determinants of health (eg. Finances, transport, familiar location), increased uptake (eg. Knowledge, participation, targeted invitations, system integration), trust in service and health providers, presence of support, and positive approach to self-care.
There were five general recommendations in the literature on how to improve cancer screening for people with mental ill-health: improving the health system to be more responsive to the needs of people with mental ill-health, social determinants of health (particularly finances, discrimination, and education), implementing strategies to improve patient compliance/participation, further research to understand the experiences of service users, and other/miscellaneous strategies (see Table 3) [see Supplementary File S7 for further detail].
Improving the health system: Tailored interventions could increase cancer screening uptake by targeting specific groups, risk factors, or addressing specific areas of concern. There were a few suggestions in the literature on who the targeted groups might include: people with depression and anxiety might benefit from targeted programs [16]; the homeless could be targeted in an attempt to broaden the number of individuals with schizophrenia [14,42]; minority groups that may be disadvantaged [13]. Interventions that target risk factors for cancers such as lung cancer (eg. Interventions assisting with smoking cessation) were recommended [14,34,42]. Addressing risk factors of cancer has the potential to make service users more aware of their risks and thus result in increased screening rates. Similarly, interventions tailored to different age groups could be beneficial [14].
Various literature recommended addressing the apparent lack of integration amongst the physical and mental health systems. Better system integration amongst mental health service providers and primary care/physical health physicians to enhance screening rates [14,29,31,33,40,41,42,45]. Interventions, such as combining mental health services/providers with physical health services/providers and motivating service users to be more aware of their self-health, were also recommended to be implemented to increase screening uptake [18,41]. Integration of health systems could lead to more holistic care of patients; thus, resulting in more cancer screening.
The literature recommended to address barriers to access at various levels: service user level [33]; physician level (eg. The need for shared decision making in cancer screening, distinguishing which providers should advise on smoking cessation, and providers’ need for education on smoking cessation in mentally ill-health populations) could lead to improved screening rates [14]. It’s important to consider that mental illness itself can serve as a contributive risk factor in experiencing barriers to care [18]. Strategies need to be developed to consider barriers such as cognitive impairment and psychosocial factors [29]. Additionally, new strategies need to be considered for individuals with complex medication history such as co-occurring chronic medical conditions [26].
Current care models need to be revised to better suit service users and increase screening. It was recommended that new models of care be investigated, and care plans be executed [42]. Care models could involve: co-location [26,27]; referencing ideas from the Quality in the Continuum for Cancer Care framework [18].
Social determinants of health: Recommendations regarding finances, discrimination, and education could result in increased screening rates. If increased funding was advocated for by mental health nurses, service users, and organizations, then this new financial capability could work to enhance patients’ health via resources and education [33]. Assisting service users to understand insurance schemes and how to use their insurance can facilitate cancer screening [28]. Methods to make cancer screening more inclusive: addressing cultural safety [24], and racial/ethnic disparities [30], catering to different languages [13]. Furthermore, implementation of patient navigation programs was a specific recommendation made to make cancer screening more culturally accessible [30,47].
Providers and service users could benefit from further education. Educating providers on: potential biases [41]; details about the screening process [14,41]. Educating patients on: cancer risk factors and preventative measures [14,21]; cancer screening process [22]. Furthermore, education encouraging shared decision making and implementing trauma informed care would benefit service users and providers.
Improving participation: There were a few different recommendations in the literature on how to improve compliance and participation. Primary care physicians could directly ask patients about screening compliance [36]. At family physician practices, all staff members could try prompting patients to get screened [35]. Psychiatric professionals could encourage uptake of cervical cancer screening [17]. Perhaps a direct approach would allow for less ambiguity around the screening process and eligibility.
Participation could increase through changes to the screening invitation process. Literature recommended targeting patients that became lost in follow-up [42], more user-friendly methods of scheduling appointments [22], and implementing follow-up calls to patients [38]. Addressing issues in the screening invitation process can increase the number of service users that accept the invitation to be screened; thus, increasing screening rates.
A recommendation to reduce stigma around mental illness was listed in various literature but not further elaborated upon [40,43]. This rasies the issue of how stigma pertaining to mental illness could be addressed in the health system.
Communication amongst patients and health professionals (both mental health professionals and primary care providers) could be improved [38]. Health professionals could improve their communication skills with patients by having specific sessions devoted to delivering results [45]. Improve communication between oncology professionals and mental health professionals [42]. Better communication amongst health professionals and patients could result in a more integrated and patient-focused system that raises awareness to a lack of cancer screening.
Having a good support system is a recommendation made by in several literature articles. Women need to have a social support system to be prompted to participate in screening for breast cancer [38]. General practitioners and mental health professionals can work to support service users [46]. A similar recommendation was made where peer support workers could enhance the support network of service users [27]. Support can also be established so that service users feel more comfortable in being able to self-manage themselves [18]. When patients feel well-supported (eg. By peer support workers, social support networks, etc), perhaps they feel more comfortable accessing the health system and feel more at ease undergoing screening procedures.
Research: There is a vast number of recommendations in the literature for additional research to be done. Some recommendations were specific, for instance: research to investigate how to overcome barriers and whether individuals with severe mental illness have barriers that are solely relevant to them [19,20]. Other recommendations were more generic, for instance more research: into barriers and facilitators [37]; into barriers to cancer screening [35], pertaining to contributing processes related to breast cancer [40]. It’d also be beneficial to research the impact of mental illness on screening rates (example: anxiety and cervical cancer screening [16]; whether screening rates improve when depressive symptoms are treated [36]).
Future research focusing on interventions and care settings would be beneficial: use of community mental health clinic (CMHC) [14]; studies involving a variety of care settings [47]; how patient care is affected by primary care-based medical homes [39]. Future research into how individuals with comorbid mental health conditions can obtain better delivery of health services was also recommended [27]. Understanding the impact of various settings and comorbidities can enhance our knowledge of contributing factors to low screening rates amongst service users and identify areas of concern that need to be targeted.
Other/miscellaneous: It was recommended that strategies need to be implemented at individual, policy, and system levels [31,45]. Multiple literature recommended the need to create clinical guidelines and policies, suggesting that there is an obvious gap in the health system currently.
4.1. Alignment with Broader Public Health Frameworks
Overall, our findings seem to align with current policies and guidelines in various countries around the world. The Australian Cancer Plan focuses on improving participation rates in cancer screening programs, addressing social determinants of health (eg. Education, transport, socioeconomic status), addressing modifiable risk factors (eg. Smoking), and implementing targeted, culturally safe screening programs [49]. Other aspects of the Australian Cancer Plan include enhancing trust in the system, utilizing person-centered navigation models of care, integration at profession and health system levels, and reducing racism [49].
Royal Australian College of General Practitioners (RACGP) published an article that suggests how cancer screening can be improved, particularly in a general practitioner (GP) setting. It mentioned addressing time constraints, providing appropriate support, funding, and training for GPs, further research into the needs of underserviced populations, and the use of liaison oncology services to improve communication in the health system [50]. GPs have a crucial role in the continuity of care and in cancer screening; I believe this article does a decent job at highlighting the health disparity people with mental ill-health experience and serves as a good starting point for how to work towards eliminating this gap from a GP setting.
In the UK, the goals of the NHS Long Term Plan include addressing modifiable risk factors (eg. Tobacco control plan, alcohol, human papilloma virus (HPV) primary screening for cervical cancer) and implementing models of care that are based on evidence [51]. A report from Public Health England further emphasized the disparity in people with severe mental illness being under screened for cancers and being less likely to participate in cervical, breast, and bowel cancer screening [52].
In the USA, the goals of the National Cancer Plan include optimization of the workforce, increased engagement, addressing stigma regarding cancer screening processes, and implementation of National breast and cervical cancer early detection programs for those with financial difficulties [53].
In Canada, the goals of the Canadian Strategy for Cancer Control include implementing a national lung cancer screening program, implementing new models of care, having services address the needs of people who are underserviced, improving resources for remote/rural areas, integration, enhanced communication, patient navigators, encouraging smoking cessation and HPV vaccinations, further research into the barrier of minority groups, education aimed to lower the prevalence of racism, and involvement of First Nations, Inuit and Metis communities [54].
4.2. Limitations
One limitation of this review is the key-word search, time-period, and selected databases could have resulted in us missing out on relevant studies. A second limitation is that the inductive coding was subject to the author’s interpretation; thus, allowing for potential bias. A third limitation is generalizability of the results since the included studies were from various countries across the world and possibly have differing health systems.
5. Conclusions
This study investigated the common barriers and facilitators to cancer screening amongst service users and interventions to improve participation. Key barriers included social determinants of health (eg. Finances, access, distance), the presence of mental health/comorbidities, and aspects of the health system. Key facilitators included social determinants of health (eg. Transport, familiar location), interventions to increase uptake and knowledge, trust, support, and self-care.
Our findings demonstrated that barriers and facilitators are multifactorial and present across personal, professional, and systemic levels. These results emphasize the importance of implementing recommendations to assist with reducing cancer screening barriers experienced by service users. With less delayed cancer screening/underscreening, the drastically higher mortality rates for service users compared to the general population can hopefully be reduced and more equitable.
The persistent gap in cancer screening for people with mental ill-health highlights the need for further research into the experiences of mental health service users. Understanding their lived experiences may provide insights into why efforts to combat known barriers has not worked to reduce this disparity. Utilizing the lived experiences of service users, future policies and guidelines can be guided to better assist in closing this gap by addressing their needs. In addition, interventions to improve communication between health professionals and service users may make service users feel more supported, facilitating greater participation in cancer screening. Finally, working to eliminate siloed health systems can promote integrated health system that provides better patient-centered care and results in equitable cancer screening for service users.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Supplementary File S1: Table S1. Example output table from MEDLINE database search; Supplementary File S2: Table S1. Study Characteristics Summary; Supplementary File S3: Table S1. MMAT v.18 quality rating for qualitative studie, Table S2. MMAT v.18 quality rating for quantitative randomized controlled trials, Table S3. MMAT v.18 quality rating for quantitative non-randomized trials., Table S4. MMAT v.18 quality rating for quantitative descriptive studies, Table S5. MMAT v.18 quality rating for mixed methods studies., Table S6. Peer-reviewed literature - CASP quality rating of systematic reviews; Supplementary File S4: Table S1. Summary of Findings: Barriers, Facilitators, Recommendations; Supplementary File S5: Table S1. Thematic table of recommendations.; Supplementary File S6: Table S1. Thematic table of facilitators, Supplementary File S7: Table S1. Thematic table of recommendations.
Author Contributions
Conceptualization, S.L. and C.B.; methodology, S.L. and C.B.; validation, S.L., and C.B.; formal analysis, C.B. and S.L.; investigation, S.L., and C.B.; data curation, C.B. and S.L..; writing—original draft preparation, C.B.; writing—review and editing, S.L.; visualization, C.B.; supervision, S.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The original contributions presented in this study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Acknowledgments
The authors would like to acknowledge the assistance the Flinders University Librarians provided with regards to the initial keyword searches.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Abbreviations
The following abbreviations are used in this manuscript:
| MMAT | Mixed Methods Appraisal Tool |
| v.18 | Version 2018 |
| CASP | Critical Appraisal Skills Programme |
| NSW | New South Wales |
| NHO | Non-Hispanic other |
| NHW | Non-Hispanic White |
| NHB | Non-Hispanic Black |
| FIT | Faecal Immunochemical Test |
| gFOBT | Guaiac Faecal Occult Blood Test |
| USA | United States of America |
| UK | United Kingdom |
| RCT | Randomized Controlled Trials |
| CMHC | Community Mental Health Clinic |
| PCP | Primary care providers |
| RACGP | Royal Australian College of General Practitioners |
| GP | General Practitioner |
| HPV | Human papilloma virus |
References
- World Health Organization. Cancer. Fact Sheet, World Health Organization. Available online: https://www.who.int/news-room/fact-sheets/detail/cancer (accessed on 25 November 2025).
- World Health Organizatio. Mental Disorders. Fact Sheet, World Health Organization. Available online: https://www.who.int/news-room/fact-sheets/detail/mental-disorders (accessed on 25 November 2025).
- Kaine, C.; Lawn, S.; Roberts, R.; Cobb, L.; Erskine, V. Review of Physical and Mental Health Care in Australia. Lived Experience Australia Ltd., Marden, South Australia, Australia, 2022. Available online: https://www.livedexperienceaustralia.com.au/_files/ugd/07109d_c21aa5b21f1d45c687b453f0adbb725f.pdf (accessed on 25 November 2025).
- Equally Well Australia. Factsheer #8: Breast Cancer and Mental Health. Equally Well. 2025. Available online: https://equallywell.org.au/equally-well-factsheets/ (accessed on 9 December 2025).
- Colton, C.W.; Manderscheid, R.W. Congruencies in Increased Mortality Rates, Years of Potential Life Lost, and Causes of Death Among Public Mental Health Clients in Eight States. Prev. Chronic Dis. 2006, 3(2), A42. [Google Scholar]
- Roberts, R.; Johnson, C. The Potential Impact of a Public Health Approach to Improving the Physical Health of People Living with Mental Illness. Int. J. Environ. Res. Public Health. 2022, 19(18), 11746. [Google Scholar] [CrossRef]
- Roberts, R. The Physical Health of People Living With a Mental Illness: A Narrative Literature Review. Equally Well Publications and Reports. September 2019. Available online: https://www.equallywell.org.au/wp-content/uploads/2019/10/Literature-review-EquallyWell-2a.pdf (accessed on 20 June 2023).
- Kisely, S.; Siskind, D. Excess Mortality From Cancer in People With Mental Illness- Out of Sight and Out of Mind. Acta. Psychiatr. Scand. 2021, 144(4), 315–317. [Google Scholar] [CrossRef] [PubMed]
- Mixed Methods Appraisal Tool (MMAT). Criteria and User Manual (Version 2018). 1 August 2018. Available online: http://mixedmethodsappraisaltoolpublic.pbworks.com/w/file/fetch/127916259/MMAT_2018_crtieria-manual_2018-08-01_ENG.pdf (accessed on 3 April 2014).
- Braun, V.; Clarke, V. Using Thematic Analysis in Psychology. Qual. Res. Psychol. 2008, 3(2), 77–101. [Google Scholar] [CrossRef]
- World Health Organization. Social Determinants of Heealth. WHO Fact Sheets. 2025. Available online: https://www.who.int/news-room/fact-sheets/detail/social-determinants-of-health (accessed on 20 September 2025).
- Aggarwal, A.; Pandurangi, A. Disparities in Breast and Cervical Cancer Screening in Women with Mental Illness: A Systematic Literature Review. Am. J. Prev. Med. 2013, 44(4), 392–398. [Google Scholar] [CrossRef]
- Harder, E.; Juul, K.E. Factors Associated with Non-participation in Cervical Cancer Screening – A Nationwide Study of Nearly Half a Milion Women in Denmark. Prev. Med. 2018, 111, 94–100. [Google Scholar] [CrossRef]
- Irwin, K.E.; Steffens, E.B. Lung Cancer Screening Eligiblity, Risk Perceptions, and Clinician Delivery of Tobacco Cessation Among Patients with Schizophrenia. Psychiatr. Serv. 2019, 70(10), 927–934. [Google Scholar] [CrossRef]
- Siantz, E.; Wu, B. Mental Illness Is Not Associated with Adherence to Colorectal Cancer Screening: Results from the California Health Interview Survey. Dig. Dis. Sci. Serv. 2017, 62, 224–234. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Mkuu, R. Anxiety and Depressive Symptoms and Missing Breast Cancer and Cervical Screening: Results from Brazos Valley Community Health Survey. Psychol. Health Med. 2020, 25(4), 402–409. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, E.M.; Lau, M. Participation in a Swedish Cervical Cancer Screening Program Among Women with Psychiatric Diagnoses: A Population-based Cohort Study. BMC Public Health 2019, 19, 313. [Google Scholar] [CrossRef]
- Cespedes, P.; Sanchez-Martinez, V. Delay in the Diagnosis of Breast and Colorectal Cancer in People with Severe Mental Disorders. Cancer Nurs. 2020, 43(6), E356–E362. [Google Scholar] [CrossRef]
- Barley, E.A.; Borschmann, R.D. Interventions to Encourage Uptake of Cancer Screening for People with Severe Mental Illness (Review). Cochrane Database Syst. Rev.. 2013, Issue 7. Art. No., CD009641. [Google Scholar] [CrossRef]
- Barley, E.A.; Borschmann, R.D. Interventions to Encourage Uptake of Cancer Screening for People with Severe Mental Illness (Review). Cochrane Database Syst. Rev.. 2016, Issue 9. Art. No., CD009641. [Google Scholar] [CrossRef]
- Borrull-Guardeno, J.; Dominguez, A. Cervical Cancer Screening in Women with Severe Mental Disorders: An Approach to the Spanish Context. Cancer Nurs. 2019, 42(4), E31–E35. [Google Scholar] [CrossRef] [PubMed]
- Werneke, U.; Horn, O. Uptake of Screening for Breast Cancer in Patients with Mental Health Problems. J. Epidemiol. Community Health 2006, 60(7), 600–605. [Google Scholar] [CrossRef]
- Impelido, M.L.; Brewer, K. Age-specific Differences in Cervical Cancer Screening Rates in Women Using Mental Health Services in New South Wales, Australia. N. Z. J. Psychiatry 2023, 58(10), 885–891. [Google Scholar] [CrossRef]
- Lambeth, C.; Burgess, P. Breast Cancer Screening Participation in Women Using Mental Health Services in NSW, Australia: A Population Study. Soc. Psychiatry Psychiatr. Epidemiol. 2023, 59, 839–846. [Google Scholar] [CrossRef]
- Baillargeon, J.; Kuo, Y. Effect of Mental Disorders on Diagnosis, Treatment, and Survival of Older Adults with Colon Cancer. J. Am. Geriatr. Soc. 2011, 59(7), 1268–1273. [Google Scholar] [CrossRef]
- Kilbourne, A.M.; Pirraglia, P.A. Quality of General Medical Care Among Patients with Serious Mental Illness: Does Colocation of Services Matter? Psychiatr. Serv. 2011, 62(8), 922–928. [Google Scholar] [CrossRef]
- Lawrence, D.; Hancock, K.J. Cancer and Mental Illness. In Comorbidity of Mental and Physical Disorders, 1st ed.; Sartorius, N., Holt, R.I.G., Eds.; Karger: Basel, Switzerland, 2014; Volume 179, pp. 88–98. [Google Scholar] [CrossRef]
- Mkuu, R.S.; Staras, S.A. Clinicians’ Perceptions of Barriesr to Cervical Cancer Screening for Women Living With Behavioural Health Conditions: A Focus Group Study. BMC Cancer. 2022, 22(1), 252. [Google Scholar] [CrossRef]
- Murphy, K.A.; Stone, E.M. Cancer Screening Among Adults With and Without Serious Mental Illness: A Mixed Methods Study. Med. Care. 2021, 59(4), 327–333. [Google Scholar] [CrossRef]
- Tsai, M.; Bevel, M.S. Racial/Ethnic Disparity in the Relationship of Mental and Physical Health With colorectal Cancer Screening Utilization Among Breast and Prostate Cancer Survivors. JCO Oncol. Pract. 2023, 19(5), E714–E724. [Google Scholar] [CrossRef]
- Clifton, A.; Burgess, C. Influences on Uptake of Cancer Screening in Mental Health Service Users: A Qualitative Study. JCO BMC Health Serv. Res. 2016, 16(1), 257. [Google Scholar] [CrossRef]
- Woodhead, C.; Cunningham, R. Cervical and Breast Cancer Screening Uptake Among Women with Serious Mental Illness: A Data Linkage Study. BMC Cancer. 2016, 16(1), 819. [Google Scholar] [CrossRef]
- Happell, B.; Scott, D. Provision of Preventive Services for Cancer and Infectious Diseases Among Individuals With Serious Mental Illness. Psychiatr. Nurs. 2012, 26(3), 192–201. [Google Scholar] [CrossRef] [PubMed]
- Linz, S.; Jerome-D’Emilia, B. Barriers and Facilitators to Breast Cancer Screening for Women With Severe Mental Illness. J. Am. Psychiatr. Nurses Assoc. 2022, 30(3), 576–589. [Google Scholar] [CrossRef]
- Ouk, M.; Edwards, J.D. Psychiatric Morbidity and Cervical Cancer Screening: A Retrospective Population-Based Case-Cohort Study. CMAJ Open. 2020, 8(1), E134–E141. [Google Scholar] [CrossRef]
- Vigod, S.N.; Kurdyak, P.A. Depressive Symptoms As A Determinant of Breast and Cervical Cancer Screening in Women: A Populaiton-based Study in Ontario, Canada. Arch. Women’s Ment. H/ealth. 2011, 14(2), 159–168. [Google Scholar] [CrossRef] [PubMed]
- Koroukian, S.M.; Bakaki, P.M. Mental Illness and Use of Screening Mammography Among Medicaid Beneficiaries. Am. J. Prev. Med. 2012, 42(6), 606–609. [Google Scholar] [CrossRef]
- Mitchell, A.J.; Perelra, I.E.S. Breast Cancer Screning in Women with Mental Illness: Comparative Meta-Analysis of Mammography Uptake. Br. J. Psychiatry. 2014, 205(6), 428–438. [Google Scholar] [CrossRef] [PubMed]
- Domino, M.E.; Wells, R. Serving Persons with Severe Mental Illness in Primary Care-based Medical Homes. Psychiatr. Serv. 2015, 66(5), 477–483. [Google Scholar] [CrossRef]
- Sara, G.; Lambeth, C. Breast Screening Participation and Degree of Spread of Invasive Breast Cancer at Diagnosis in Mental Health Service Users, a Population Linkage Study. Cancer. 2023, 130(1), 77–85. [Google Scholar] [CrossRef]
- Ukhnaova, M.A.; Tillotson, C.J. Uptake of Preventive Services Among Patients With and Without Multimorbidity. Am. J. Prev. Med. 2020, 59(5), 621–629. [Google Scholar] [CrossRef]
- Irwin, K.E.; Henderson, D.C. Cancer Care for Individuals With Schizophrenia. Cancer. 2014, 120(3), 323–334. [Google Scholar] [CrossRef]
- Grassi, L.; McFarland, D. The Risk and the Course of Cancer Among People With Severe Mental Illness. Clin. Pract. Epidemiol. Ment. Health 2023, 19, e174501792301032. [Google Scholar] [CrossRef] [PubMed]
- Yarborough, B.J.H.; Hanson, G.C. Colorectal Cancer Screening Completion Among Individuals With and Without Mental Illnesses: A Comparison of 2 Screening Methods. Am. J. Health Promot. 2018, 32(4), 925–931. [Google Scholar] [CrossRef]
- Thomas, M.; James, M. Mammography Among Women With Severe Mental Illness: Exploring Disparities Through A Large Retrospective Cohort Study. Psychiatr. Serv. 2018, 69(1), 48–54. [Google Scholar] [CrossRef]
- Thomsen, M.K.; Jorgensen, M.D. Mental Disordres, Participation, and Tajectories in the Danish Colorectal Cancer Programme: A Population-based Cohort Study. Lancet Psychiatry. 2023, 10(7), 518–527. [Google Scholar] [CrossRef] [PubMed]
- Abuelo, C.; Ashburner, J.M. Colorectal Cancer Screening Patient Navigation for Patients with Mental Illness and/or Substance Use Disorder: Pilot Randomized Control Trial. J. Dual Diagn. 2020, 16(4), 438–446. [Google Scholar] [CrossRef] [PubMed]
- Kodl, M.M.; Powell, A.A. Mental Health, Frequency of Healthcare Visits, and Colorectal Cancer Screening. Med. Care 2010, 48(10), 934–939. [Google Scholar] [CrossRef]
- Cancer Australia. Welcome- Australian Cancer Plan. Australian Cancer Plan. Available online: https://www.australiancancerplan.gov.au/welcome (accessed on 9 December 2025).
- Tran, M.; Ee, C.; Rhee, J.; Bareham, M. General Practice, Mental Health and the Care of People with Cancer. Australian Journal of General Practice 2025, 54(10). [Google Scholar] [CrossRef] [PubMed]
- NHS England. NHS Long Term Plan Ambitions for Cancer. NHS England. Available online: https://www.england.nhs.uk/cancer/strategy/ (accessed on 9 December 2025).
- Public Health England. Severe Mental Illness (SMI): Inequalities in Cancer Screening Uptake Report. GOV.UK. Pubished 21 September 2021. Available online: https://www.gov.uk.government/publications/severe-mental-illness-inequalities-in-cancer-screening-uptake/severe-mental-illness-smi-inequalities-in-cancer-screening-uptake-report (accessed on 9 December 2025).
- National Cancer Plan. About the National Cancer Plan. NationalCancerPlan.cancer.gov. Available online: https://nationalcancerplan.cancer.gov/about (accessed on 9 December 2025).
- Canadian Partnership Against Cancer. Cancer Strategy for Cancer Control. Canadian Partnership Against Cancer. Available online: https://www.partnershipagainstcancer.ca/cancer-strategy/ (accessed on 9 December 2025).
Figure 1.
PRISMA Flow Diagram.
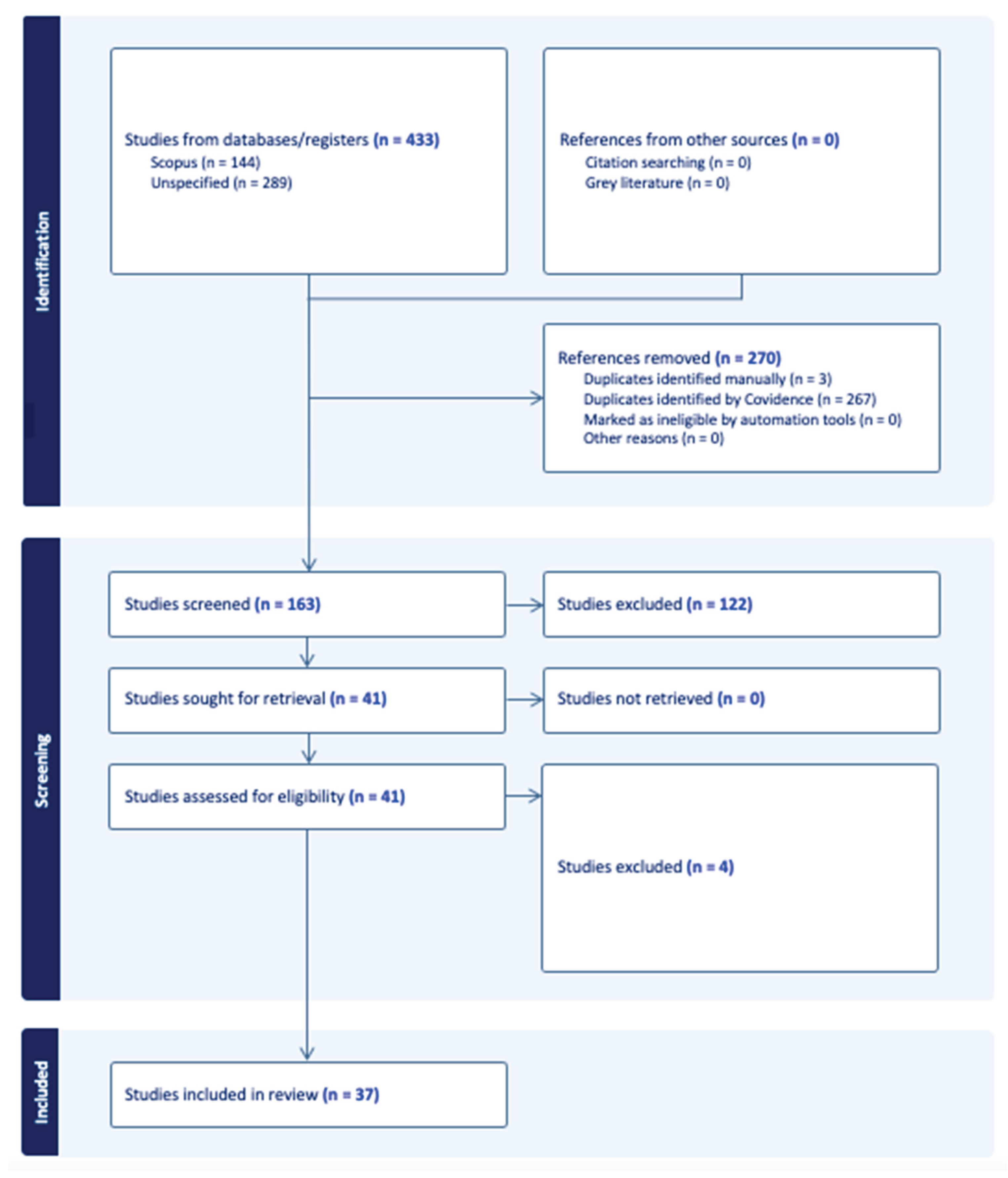
Table 2.
Type of cancer screening focused on in the literature.
| Type of Cancer Screening Focused on | Number of studies/ articles | Cited Literature |
|---|---|---|
| Breast | 8 | [22,24,34,37,38,40,45]. |
| Cervical | 6 | [13,17,21,23,28,35]. |
| Breast and cervical | 4 | [12,16,32,36]. |
| Colon | 3 | [15,25,46]. |
| Lung | 1 | [14]. |
| Breast and colon | 1 | [18]. |
| Breast and bowel | 1 | [31]. |
| Breast and prostate | 1 | [30]. |
Table 3.
Recommendations to improve cancer screening in the literature.
| Recommendation | Subthemes |
|---|---|
| Improve health system | -Tailored interventions. -Target groups, risk factors, areas of concern. -Physical and mental health system integration. -Address barriers at service user and physician levels. -Revise current care models. Consider implementing co-location of services. |
| Social determinants of health | -Increase funding. -Understand insurance schemes. -Cultural safety. Address racial/ethnic disparities. Various languages. -Patient navigation programs. -Educate providers and patients. |
| Improve participation | -Directly ask about screening. -Prompt patients. -Address issues at screening invitation process. -Reduce stigma around mental illness. -Improve communication. -Support systems. |
| Research | -Barriers and facilitators of cancer screening. -Interventions and care settings. |
| Other / miscellaneous |
-Individual, policy, and system level strategies. -Guidelines and policies. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



