
Submitted:
05 August 2025
Posted:
05 August 2025
You are already at the latest version
Abstract
Co-sleeping has been practiced throughout human evolution and refers to mother and child sleeping in the same bed.In recent decades, some Western cultures have proposed avoiding co-sleeping due to the risk of sudden death in infants under 4 months of age. This could contradict the custom of mothers sleeping with their breastfed babies, a practice that fosters maternal-child bonding with a better response from the mother to the child's needs for shelter, affection, and nourishment, allowing for nighttime breastfeeding on demand. This study aims to contribute to the recognition of the relationship between nighttime breastfeeding and the nutritional status of infants and to determine whether it provides protection against malnutrition or obesity in children in this age group.
Keywords:
breastfeeding
; night feeding
; co-sleeping
; obesity
; malnutrition
Introduction
Childhood is a critical period of life in which optimal nutritional habits are established to achieve adequate growth and avoid diet-related diseases [1]. Adequate nutrition during infancy and early childhood is essential to ensure that children reach their full potential in growth, health and neurodevelopment. Poor nutrition increases the risk of disease and is directly or indirectly responsible for one-third of the estimated 9.5 million deaths that occurred in children under 5 years of age in 2006. Inappropriate nutrition can lead to childhood obesity, which is a growing problem in many countries [2].
An infant is a child who primarily feeds on milk. The infant period can be divided into:
- Infant: from one month of age to one year of age.
-
Older infant: from the first year of life to two years of age. The infant has an accelerated growth rate that gradually decreases towards the second year of life when the growth rate stabilizes [3] The recommendations of the WHO and UNICEF for optimal infant nutrition, as established in the Global Strategy are:
- Exclusive breastfeeding during the first 6 months of life
-
Start adequate and safe complementary feeding from 6 months of age, maintaining breastfeeding until two years of age or more [2].The Spanish Academy of Pediatrics (AEP) reminds us of the periods of child feeding as defined by the Nutrition Committee of the American Academy of Pediatrics:Breastfeeding period: comprises the first 6 months of life, during which the child's diet should be exclusively breast milk or, failing that, infant formula. Breast milk protein is of optimal quality and is the reference standard [4]. Breastfeeding should begin early, in the first hours after birth, avoiding bottle feeding. This promotes mother-child contact and provides the first stimulus for milk secretion.It is well established that breastfeeding decreases the risk of death in childhood and protects the child against infections, necrotizing enterocolitis, obesity, type 2 diabetes, leukemia and promotes neurodevelopment [5]
| BENEFITS OF BREASTFEEDING | |
| FOR THE CHILD | FOR THE MOTHER |
| Decrease in infectious gastrointestinal and respiratory diseases | Decreased postpartum bleeding |
| Protection against allergic diseases such as asthma, rhinitis and atopy | Decreased menstrual bleeding and lactational amenorrhea |
| Protection against obesity, hypertension, dyslipidemia, and type 2 diabetes mellitus during adulthood | Decreased risk of high blood pressure, obesity, type 2 diabetes, and dyslipidemia |
| Decreased risk of developing leukemia during childhood | Longer intergenic period |
| Reducing the risk of developing necrotizing enterocolitis in newborns | Faster recovery of pre-pregnancy weight |
| Reduction in the risk of inflammatory bowel diseases and gluten allergies | Decreased risk of breast and ovarian cancer |
| Better neurodevelopment and better IQ score | |
| Lower risk of attention deficit, autism spectrum disorder, and behavioral disorders | |
|
Emotional affective relationship that favors the child's psychological development and mother reinforces her maternal behavior | |
Adapted from Chilean Journal of Pediatrics 2017.
Transitional period: It is part of the second half of life, up to the first year of life. During this period, dietary diversification begins with the gradual introduction of complementary feeding and the introduction of foods other than breast milk or formula.It is beneficial for children to continue exclusive breastfeeding after six months, until the second year while receiving adequate and safe complementary feeding [6].
To start complementary feeding, the physical and system maturation of the baby should be taken into account to consider whether he or she is able to start with foods other than milk [7]. The number of recommended feedings is also subject to a variety of factors. It is suggested to start with one meal a day and progress to two between 6 and 8 months, then between 9 and 11 months three meals are recommended and between 11 and 23 months increase to four meals [4,8]. The volume of milk should complete a total of 400 to 500 ml/day, if this volume is not reached, another dairy product should be added during the day to contribute to covering calcium requirements [9].
Modified adult period: It covers the preschool and school age up to 7-8 years of age. During this period, the child gradually adopts a diet that is more similar to that of adults, and gradually a diet that provides 30% of the total energy in the form of fat, and of this a third in the form of saturated fat, instead of the 50% of saturated fat found in breast milk [1].
Co-Sleeping and Night Feeding
Throughout the centuries, generations and human evolution, it has been a constant that children share a bed with their parents (known as co-sleeping), especially with their mothers. When children sleep with their mothers, they adapt to maternal rhythms and achieve mutual self-regulation [10]. Reference has been made to a greater maternal-child emotional bond in the practice of co-sleeping, which is common in many societies and is often associated with maintaining nighttime breastfeeding. Offering breastfeeding at night increases prolactin levels, which allows for the maintenance of adequate breast milk production. It has also been found that mothers with greater motivation for breastfeeding tend to co-sleep with their babies, and those who co-sleep with their children consistently have a longer breastfeeding duration [11]
Generally, newborns experience constant feeding periods, even during the night. Around the second or third month of life, children spend more time sleeping at night, requiring fewer milk feeds during these hours. However, some infants, for emotional and social reasons, receive nighttime feedings, primarily breastfeeding. This in turn can lead to sleep disorders with awakenings conditioned by feeding, even when it is not necessary [12].
Some authors have found an association between short sleep duration in early life and the development of childhood obesity. In the cohort followed by Halal et al., it was found that 5.3% and 8% of children at 4 years of age had developed obesity and overweight respectively [13]. In a different sense, the study carried out by Olsen et al [14] showed that those children who shared their bed with their parents more frequently had a 3 times lower risk of being overweight.
Many cultures and societies continue to practice co-sleeping today; for example, in Norway, the incidence is 60% in the first year of life.
Materials and Methods
Study Data and Sample
A non-theoretical sample was taken consisting of a group of eighty-eight (88) infants aged between 4 and 12 months who attended an outpatient consultation in a private pediatric office consecutively for one month.
Inclusion Criteria
The study included infants who had reached 4 months of age up to 12 months and 29 days of age, who had been full-term newborns (between 37 and 41 weeks 6 days of gestation), healthy, with weight and height within normal ranges for gestational age, had not been hospitalized in the neonatal period and did not suffer from any chronic or acute disease at the time of the study.
Exclusion Criteria
Infants with a history of being born preterm, postterm, or with any neonatal pathology, a history of low birth weight (<2500 g), or large-for-gestational-age (>4000 g) at term were excluded. Those with any acute or chronic pathology at the time of the study were also excluded.
Procedures
A questionnaire containing 24 questions divided into three parts was applied.
Part One: Patient identification data (ID number, initials of first and last names), patient's date of birth and age.
Part two: nighttime feeding, type of feedings received during the night, frequency of nighttime feedings, type of feedings received during the daytime.
Part three: Anthropometric measurements and extrapolation to WHO growth charts and curves for weight-for-age, length-for-age, weight-for-height, body mass index (BMI)-for-age, and head circumference-for-age.
Weight was measured on a properly calibrated digital baby scale, length was measured with an infantometer, and head circumference was measured with a generic tape measure. The calculation of BMI, standard deviation for weight, length, weight/length (w/l), head circumference (pc), and BMI was performed using the Anthro application, and classification was made based on the WHO growth curves and charts.
Method
A database was designed in Excel, imported, and analyzed using Epiinfo 7.1, yielding simple frequency analysis and bivariate analysis. The results are presented in statistical tables, graphs, and measures of central tendency, standard deviation, and intervals.
Information Collection or Processing: Ethical Aspects
The aspects established in Resolution 008430 of 1993 of the Republic of Colombia were taken into account, especially regarding informed consent, confidentiality of the data provided, and exclusivity of the study for scientific purposes.
Results and Discussion
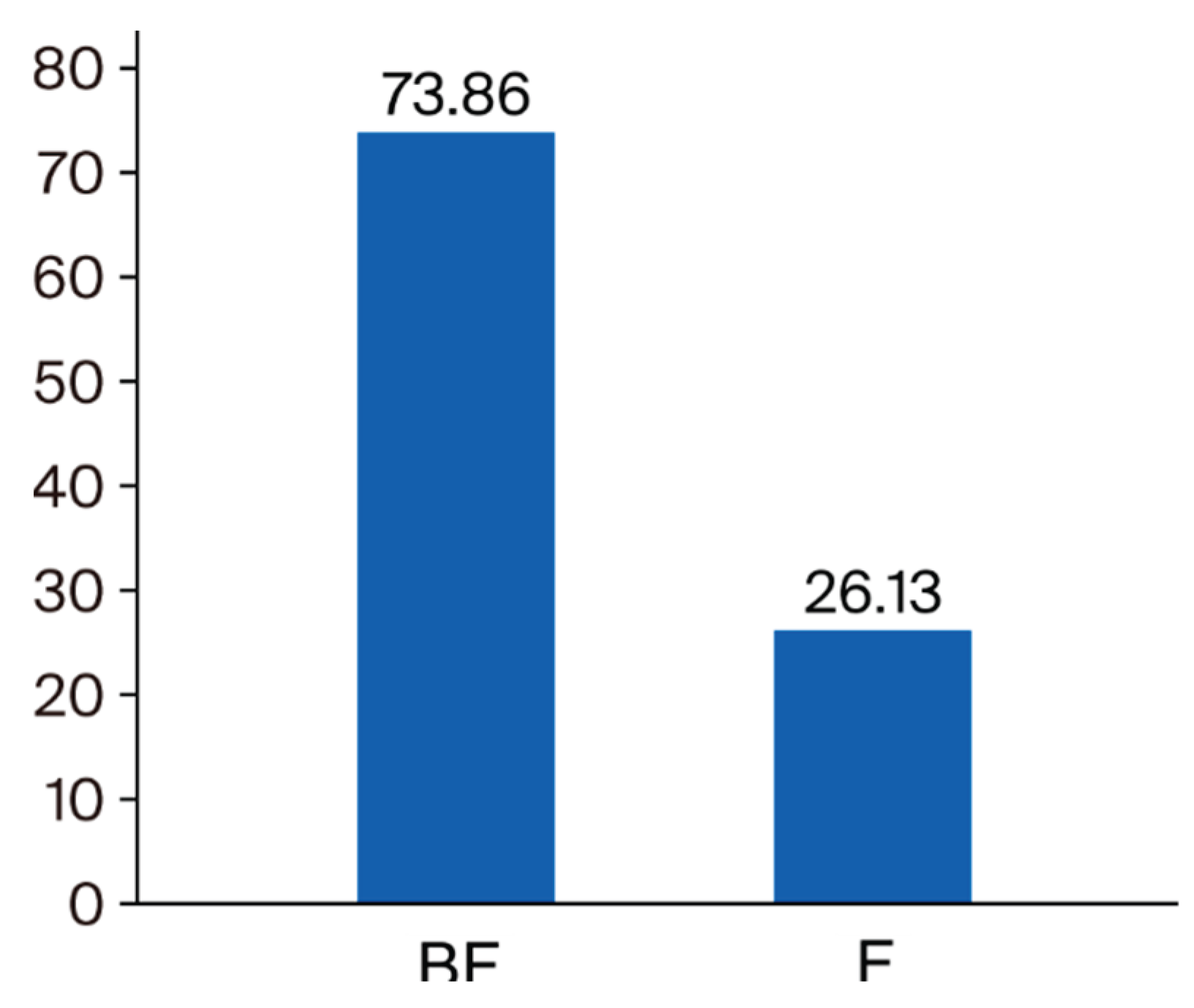
Information was obtained from 88 infants, of which 73.86% (65 children) were male and 26.13% female, aged between 4 and 12 months.
| AGE MONTHS | Percentage |
| 4 | 21.05% |
| 5 | 15.79% |
| 6 | 5.26% |
| 7 | 21.05% |
| 8 | 15.79% |
| 9 | 10.53% |
| 10 | 5.26% |
| 11 | 5.26% |
| Total | 100.00% |
Board1. Percentage of the population studied according to age
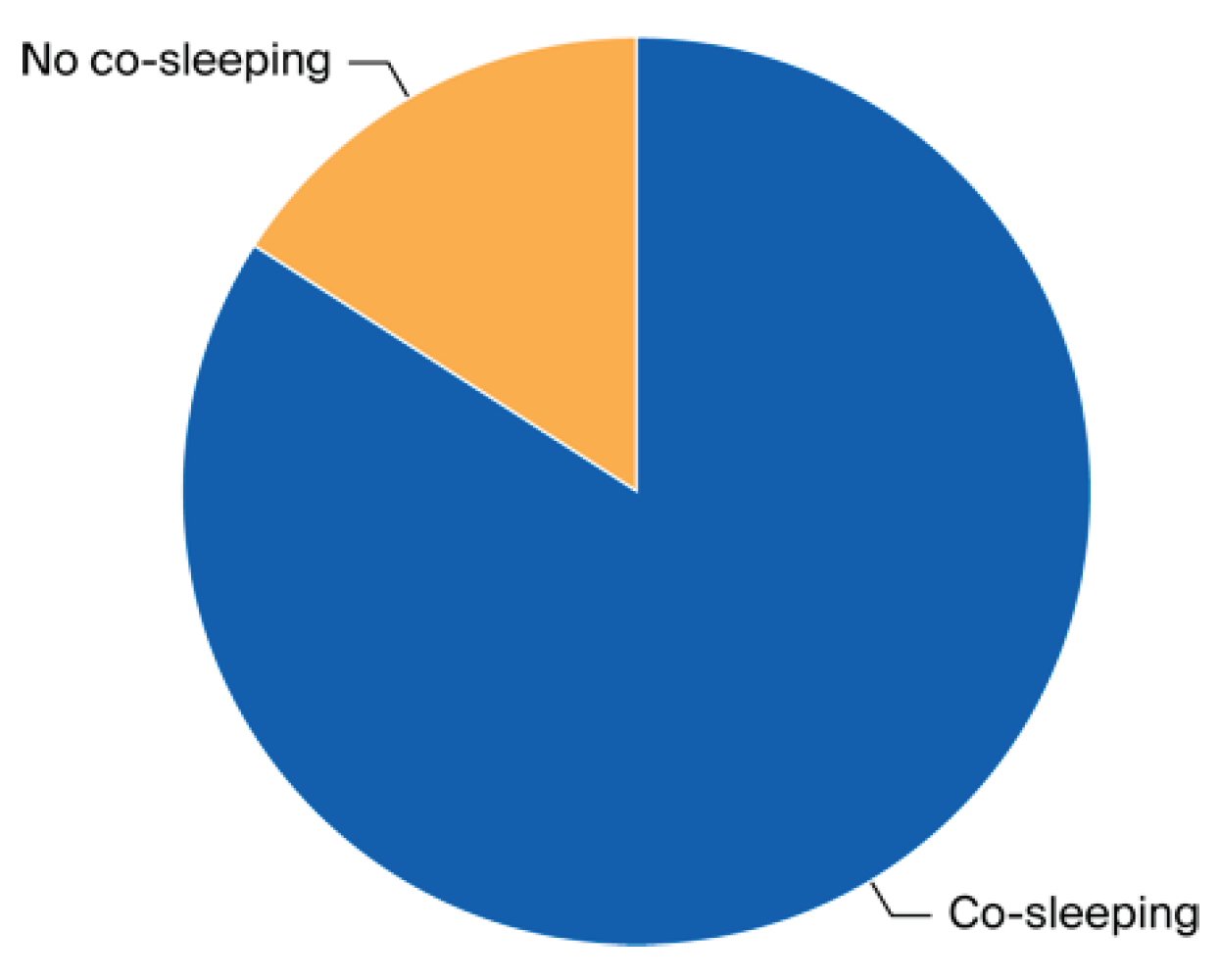
It was also found that most of the children, 74 of them (84%), shared a bed-sharing relationship with their parents and all received nighttime breastfeeding: 65 of them received only breast milk (73.86%) and 23 of them received only formula milk (26.13%). None received any other type of nighttime feeding.
Graph 1.
Co-sleeping practice.
Graph 2.
Type of night feeding.
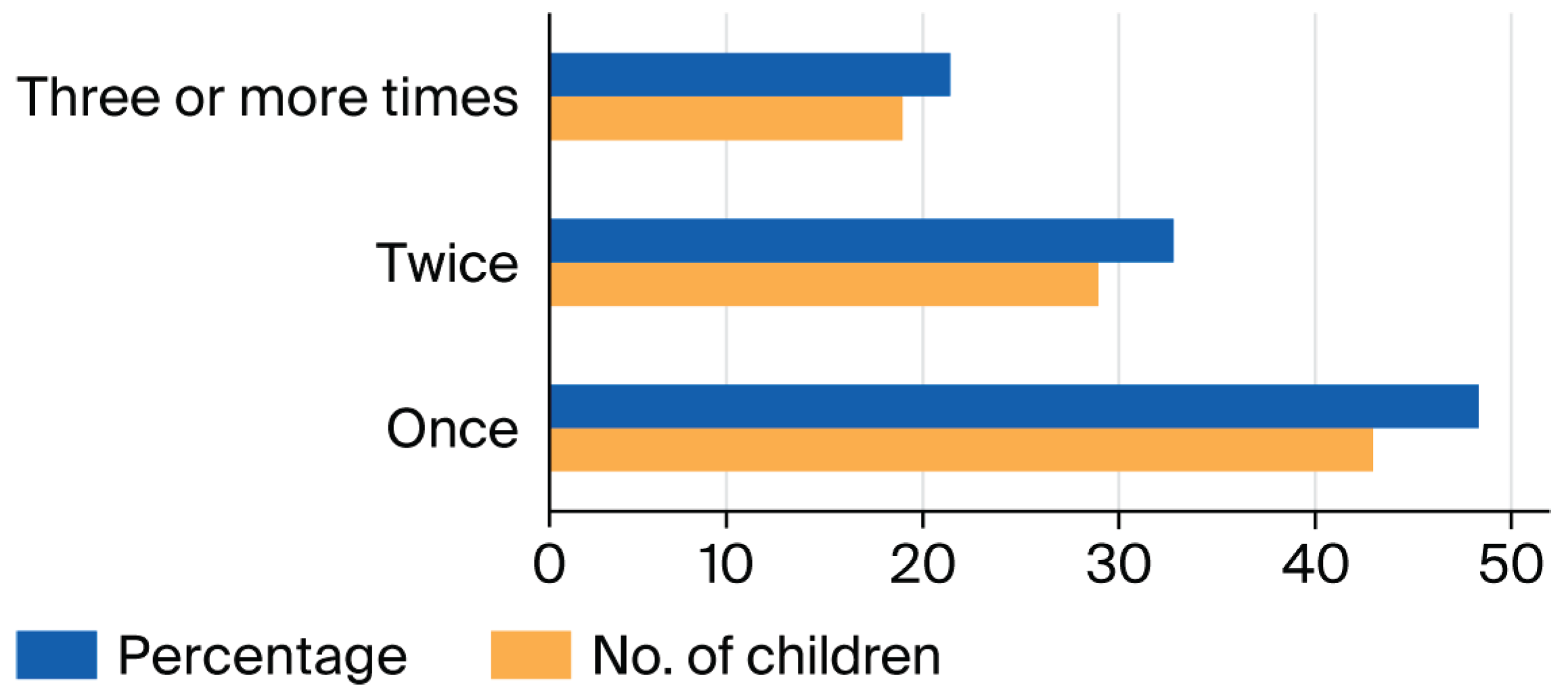
The frequency of awakenings to feed was most often once per night, followed by two awakenings and less frequently 3 or more times.
Graph 3.
Frequency of waking up to eat.
| Age in months | n | % |
| 4 | 14 | 15.9 |
| 5 | 14 | 15.9 |
| 6 | 9 | 10.2 |
| 7 | 14 | 15.9 |
| 8 | 14 | 15.9 |
| 9 | 9 | 10.2 |
| 10 | 5 | 5.7 |
| 11 | 4 | 4.5 |
| 12 | 5 | 5.7 |
| Total | 88 | 100.00 |
Board2. Nighttime feeding frequency by age
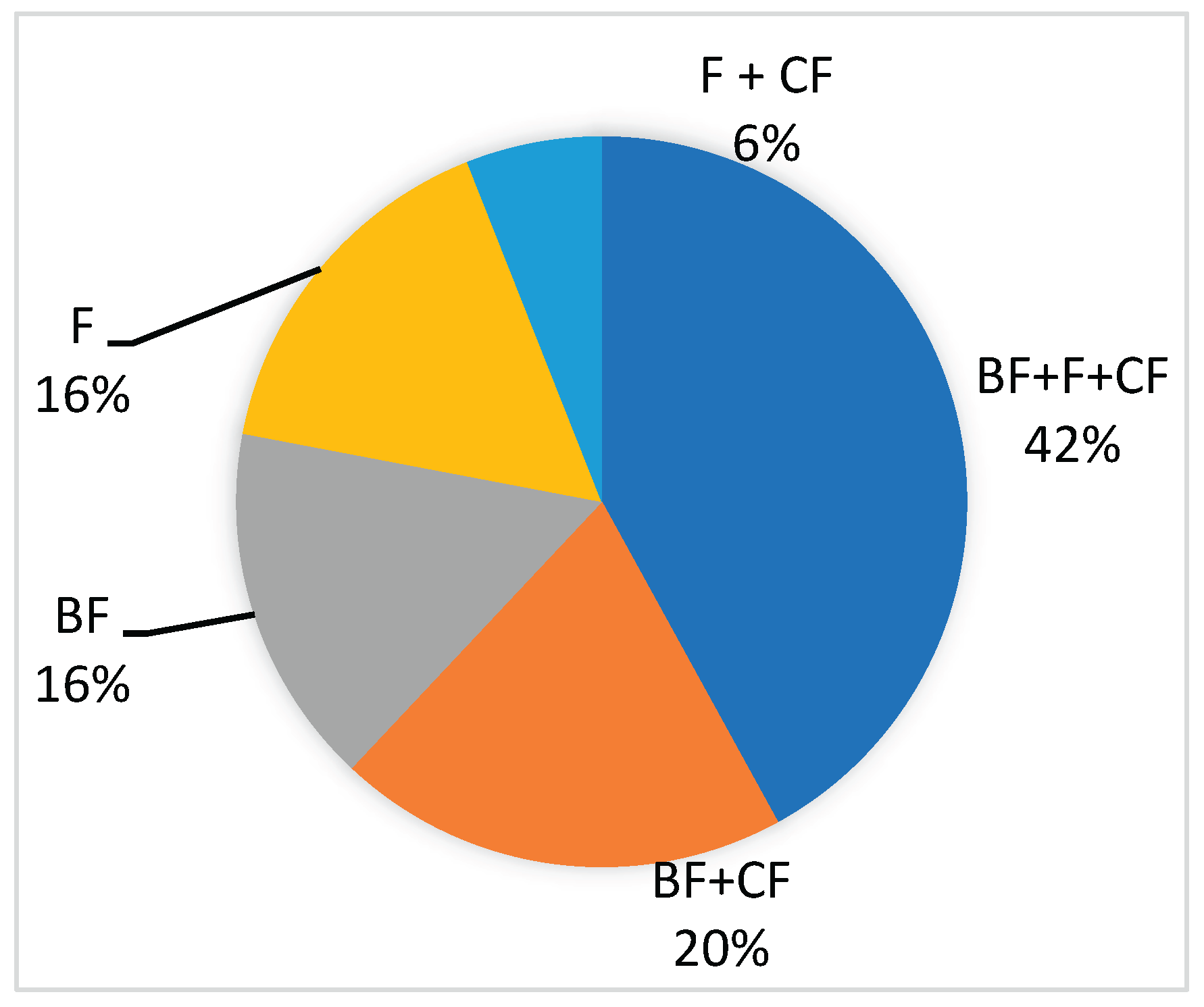
Regarding daytime feeding, the majority (42%) of children received breastfeeding (BF) + formula (F) + complementary feeding (CF). Twenty percent received breastfeeding + complementary feeding. Sixteen percent received exclusive breast, another 16% exclusive formula, and only 6% consumed formula + complementary feeding.
Graph 4.
Daytime feeding type.
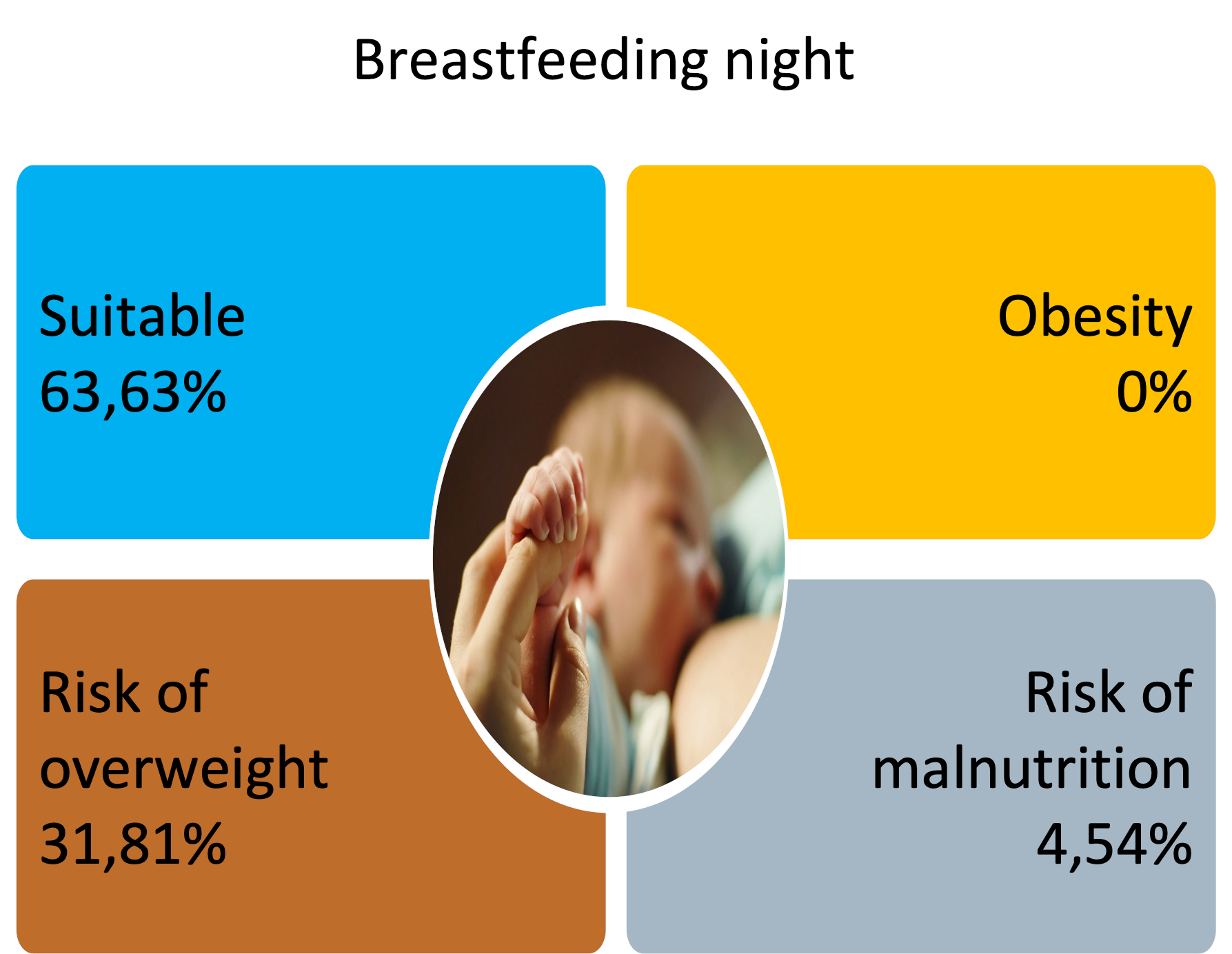
Regarding anthropometric indices, when weight-for-age (W/A) was assessed, the majority (56 children) were within the appropriate range, but none were underweight. Regarding length-for-age (L/A), 79 children were adequately tall (89.77%), and nine of them were at risk of short stature, with standard deviations between -1 and -2.
The P/L indicator showed greater variability in its results, which are shown in the following table, but none of them with obesity.
| CLASSIFICATION | Frequency | Percentage |
| SUITABLE | 56 | 63.63% |
| RISK OF MALNUTRITION | 4 | 4.54% |
| RISK OF OVERWEIGHT | 28 | 31.81% |
| Total | 88 | 100.00% |
Board3Nutritional classification of children
After reviewing the results of this sample of children under one year of age who were co-sleeping and receiving nighttime feedings, the vast majority of which were breast milk or formula, but no other type of food. However, despite the continued nighttime breastfeeding in children who also received complementary feedings during the day, none of them were found to be obese. Approximately one-third were at risk of being overweight, and four were at risk of malnutrition, the causes of which warranted further study.
Anthropometric indicators related to weight, height, weight/weight, and BMI in most children were within normal ranges without compromising their nutritional status.
It is of great importance to consider that breastfeeding, primarily breast milk, offers many biological, immunological, nutritional, and even emotional benefits to babies. It is well known that breastfeeding provides children with probiotics, which are very important in preventing various pathologies, including chronic and inflammatory conditions such as obesity. This protective effect may also be evident in infants who receive additional breast milk at night.
Some studies, such as the one conducted in Singapore, showed that children who were fed at night had a greater increase in BMI between 12 and 24 months of age, so their recommendation was to inform parents so that changes could be adopted to reduce the risk of childhood obesity [15].
Among the difficulties encountered in children who co-sleep and are night-fed are difficulty falling asleep, more night-time awakenings, and disturbed parental sleep. In the cohort studied in France, it was found that those children who were breastfed after 6 months of age had all of the above-mentioned conditions [16]. The greater number of night awakenings in children who are fed at night is more frequent in those who are breastfed compared to those who receive milk formula, although the differences may be minimal [17].
There are some references that relate night wakings with weight gain in infants, and some studies even show that preschool and school children with more night wakings and fewer hours of sleep at night have a higher risk of developing childhood obesity [18,19]. The study conducted by O'Shea et al., showed that when caregivers reduced adaptive feeding during the night according to the child's age, the BMI remained stable, thus contributing to reducing the increase in this nutritional indicator and the risk of developing obesity later. [20].
Knowing that Hispanic children are at greater risk for obesity and also that they sleep less as infants, Gray et al. conducted a study with mothers and their infants. They found that there are various social and economic reasons for co-sleeping, and mothers acknowledge that breastfeeding at night helps their children calm down and helps them and their partners sleep better [21].
Conclusions
The present study shows that nighttime feeding continues to be practiced among infants, especially with less consumption of breast milk and formula. Although previous publications report an increase in body mass in preschoolers and schoolchildren who receive nighttime feeding, the study of infants who receive nighttime feeding and those who receive nighttime feeding did not find an increase in this indicator. This may suggest that breastfeeding, especially breast milk, may be protective against obesity at this age.
However, further studies and larger samples are needed to more consistently determine the effect of nighttime feeding on children's nutritional status, even in those who receive nighttime foods other than breast milk and formula.
References
- Folgoso, CC, Martinón-Torres, N., & Martínez, BM (2021). Nutrition during the first 1,000 days of life. Diagnostic and therapeutic protocols in pediatric gastroenterology, hepatology, and nutrition. https://www.aeped.es/sites/default/files/documentos/protocolos_seghnp-aep_2023.pdf#page=445.
- World Health Organization. (2009). Indicators for assessing infant and young child feeding practices: conclusions of the consensus meeting held on 6–8 November 2007 in Washington, DC, USA. In Indicators for assessing infant and young child feeding practices: conclusions of the consensus meeting held on 6–8 November 2007 in Washington, DC, USA. https://pesquisa.bvsalud.org/portal/resource/pt/who-44156.
- American Academy of Pediatrics Committee on Nutrition. Feeding the child. In: Kleinman RE, Greer FR, eds. Pediatric Nutrition. 7th ed. Ed Grove Village, IL:American Academy of Pediatrics; 2014: 143.
- Argentine Pediatric Society. Nutrition Committee. Nutritional Guide for Healthy Children from 0 to 2 Years. 2001. https://pediatria.ucoz.es/_ld/0/14_Alimentacion-So.pdf.
- Brahm P, Valdés V. Benefits of breastfeeding and risks of not breastfeeding. Rev chil Pediatr. 2017;88(1):7-14. [CrossRef]
- Rojas M, C. Breastfeeding. In: Leal Quevedo, Ed. The Efficient Pediatrician. 7th ed. 2013.
- Daza W, Dadán S. Complementary feeding in the first year of life. Precop SCP. CCAP, 8; 4: 18-27.
- Feeding from 6 to 24 months. Health information and education: Preventive advice. Child Health Program. AEPap. 2009.
- Chilean Ministry of Health. Nutritional Guidelines for Children Under 2 Years of Age. Nutritional Guidelines for Adolescents. Department of Nutrition and Life Cycle, Division of Disease Prevention and Control. 2005. https://www.enfermeriaaps.com/portal/wp-content/uploads/2016/01/Guide-to-feeding-of-children-under-2-years-Guide-to-feeding-until-adolescent-minsal-chile-2015.pdf.
- Landa R, L., et al. (2012). Co-sleeping promotes breastfeeding and does not increase the risk of sudden infant death: Sleeping with parents. Pediatría Atención Primaria, 14(53), 53-60. https://scielo.isciii.es/pdf/pap/v14n53/revision1.pdf.
- Ball, H.L., Howel, D., Bryant, A., Best, E., Russell, C., & Ward-Platt, M. (2016). Bed-sharing by breastfeeding mothers: who bed-shares and what is the relationship with breastfeeding duration?. Acta paediatrica, 105(6), 628-634. [CrossRef]
- Madar, A.A., Kurniasari, A., Marjerrison, N. et al. Breastfeeding and Sleeping Patterns Among 6–12-Month-Old Infants in Norway. Matern Child Health J 28, 496–505 (2024). [CrossRef]
- Halal, CS, Matijasevich, A., Howe, LD, Santos, IS, Barros, FC, & Nunes, ML (2016). Short sleep duration in the first years of life and obesity/overweight at age 4 years: a birth cohort study. The Journal of pediatrics, 168, 99-103. [CrossRef]
- Olsen, NJ, Rohde, JF, Händel, MN, Stougaard, M., Mortensen, EL, & Heitmann, BL (2018). Joining Parents' Bed at Night and Overweight among 2-to 6-Year-Old Children-Results from the 'Healthy Start'Randomized Intervention. Obesity facts, 11(5),372-380. [CrossRef]
- Seng, C.T., et al. (2016). Predominantly nighttime feeding and weight outcomes in infants. The American journal of clinical nutrition, 104(2), 380-388). [CrossRef]
- Messayke, S., Davisse-Paturet, C., Nicklaus, S., Dufourg, MN, Charles, MA, de Lauzon-Guillain, B., & Plancoulaine, S. (2021). Infant feeding practices and sleep at 1 year of age in the nationwide ELFE cohort. Maternal & child nutrition, 17(1), e13072. [CrossRef]
- Ongprasert, K., Chawachat, J., Kiratipaisarl, W. et al (2025). Breast milk feeding practices and frequencies among complementary-fed children: a cross-sectional study in Northern Thailand. Int Breastfeed J 20, 28. [CrossRef]
- Roy, M., Haszard, JJ, Savage, JS, Yolton, K., et al. (2020). Bedtime, body mass index and obesity risk in preschool-aged children. Pediatric Obesity, 15(9), e12650-e12650. [CrossRef]
- Bedtime in preschool-aged children and risk for adolescent obesity. J Pediatr. 2016;09(176):17–22. [CrossRef]
- O'Shea, KJ, Ferguson, MC, Esposito, L. et al. The impact of reducing the frequency of night feeding on infant BMI. Pediatr Res 91, 254–260 (2022). [CrossRef]
- Gray, MJ, Vazquez, CE & Agnihotri, O. “Struggle at night – He doesn't let me sleep sometimes”: a qualitative analysis of sleeping habits and routines of Hispanic toddlers at risk for obesity. BMC Pediatr 22, 413 (2022). [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



