
Submitted:
16 July 2025
Posted:
17 July 2025
You are already at the latest version
Abstract
Introduction and Hypothesis: Pregnancy-specific urinary incontinence (PS-UI) is defined as any onset of new urinary leakage during pregnancy. The study aims to analyze the prevalence and risk factors of PS-UI. We hypothesized that demographic and clinical factors, including Gestational Diabetes, may contribute to the development of PS-UI. Methods: We recruited pregnant women from the Diamater cohort study. We evaluated the maternal characteristics, demographics, anthropometrics, hyperglycemic status, and the PS-UI occurrence. A logistic regression model was performed considering the clinical variables to determine the predictive factors for PS-UI occurrence. Results: PS-UI was prevalent in 62.1% of women, 58.85% began leaking urine between 24 and 28 gestational weeks, and 51% developed PS-UI at the end of pregnancy. The pregestational BMI is a risk factor for PS-UI, and physical activity is a protective factor that halves the risk of PS-UI developing. Conclusions: The weight management and encouragement to engage in physical activity during pregnancy should be emphasized in prenatal care to reduce the risk of PS-UI. Further studies are suggested to evaluate the impact of the association due to UI later in life.
Keywords:
Pregnancy-specific urinary incontinence
; Urinary incontinence
; Pregnancy
; Prevalence
Introduction
Urinary incontinence (UI) is a prevalent condition among women worldwide that can cause physical and emotional distress, have financial consequences, and place a burden on individuals and society (1, 2). Women with UI consume significantly more medical resources and incur higher costs than those without UI, but standardized prevention and treatment may positively impact costs and outcomes (3).
Pregnancy-specific urinary incontinence (PS-UI) is UI that first appears during pregnancy (4). Although PS-UI affects up to half of pregnant women and peaks in the third trimester (5-9), there are limited studies on its epidemiology. PS-UI is a strong predictor of UI postpartum and later in life, and identifying its risk factors will help healthcare providers and pregnant women make informed decisions (2, 10, 11).
PS-UI may be mild to moderate, but UI can negatively impact health-related quality of life (8, 12). However, few pregnant women seek professional assistance for urinary leakage (12, 13). Prenatal care is an entry point into the health system and provides an opportunity to engage women and provide information about disease severity (14). Few integrated care models link antenatal care and non-communicable disease prevention (14,15) despite their effectiveness in communicable disease prevention (16). Opportunistic screening for PS-UI risk factors may be feasible during critical points in the life course (14).
Our study aims to analyze the prevalence and risk factors of PS-UI during the pregnancy span, taking into account life-course approaches to women’s health. We hypothesize that demographic and clinical factors, such as obesity, sedentarism, smoking, and gestational diabetes mellitus (GDM), may contribute to the development of PS-UI.
Method
Research Design and Subjects
The DIAMATER study is an ongoing prospective cohort study that examines the link between GDM and pelvic floor muscle dysfunction as moderators between GDM and UI throughout the lifespan (17). Following the Declaration of Helsinki, we conducted and approved the study by the Institutional Ethical Committee of the Botucatu Medical School of São Paulo State University (Protocol Number CAAE 82225617.0.0000.5411). Participants provided written informed consent, and their data were kept confidential. This report was consistent with the STROBE statement (21). This observational study screened 1450 pregnant women at the Perinatal Diabetes Research Center (PDRC) at the University Clinical Hospital of Botucatu Medical School (UNESP), Brazil, and followed them until delivery. All patients received prenatal care and gave birth at the same institution.
Eligible participants: adult (age 18-40) women in their first pregnancy and women in the second pregnancy, who had a prior planned C-section in their previous pregnancy, to avoid the previously parturition and vaginal birth impact in the pelvic floor function. All participants in the study began receiving prenatal care at the first trimester of gestation and underwent a hyperglycemia screening test at the first trimester and between 24-28 weeks of pregnancy, according to the actual recommendation screening and diagnosis (17-19).
Women with pregestational UI, known type 1 or type 2 diabetes, preterm delivery (<37 weeks of gestation), multiple pregnancies, known fetal anomaly, connective tissue diseases, and any clinical condition that may have jeopardized their health status were excluded from the study.
Data Collection
Participants were recruited until 24 weeks of gestation and invited to join the study if they met the inclusion criteria. We recruited 992 participants between 2017 and 2022. After giving their written consent, they were asked to answer a questionnaire with personal details; clinical and obstetric, historical, and anthropometric measures were taken. Participants were evaluated at two time points (TP): 24–28 weeks of gestation (1st TP) and 36–38 weeks of gestation (2nd TP).
PS-UI was defined as any onset of new urinary leakage during pregnancy (4). The participants were asked to answer “yes” or “no” as to whether they had experienced PS-UI. Participants who gave positive responses were identified as having UI, following the definition set by the International Continence Society (20). Early PS-UI was considered to be incontinence that started before 28 weeks of gestation, and Late PS-UI was that which started at the end of the third trimester, after 36 weeks of gestation.
In this cohort, the diagnostic guidelines proposed by the American Diabetes Association were used to identify patients with GDM (19) using the 75-g oral glucose tolerance test (75 g-OGTT).
Statistical Analysis
The prevalence of PS-UI was calculated by obtaining the frequencies of UI in the 1st TP, 2nd TP (without intersections), and 1st TP plus 2nd TP. With these three groups, associations with the demographic variables were made using the chi-square test.
A logistic regression model was performed considering the occurrence of UI in these three scenarios, including demographic variables as explanatory variables, to determine the participants’ risk or protective factors for UI. We used a significant 5% or the corresponding p-value in all tests and SAS for Windows, version 9.4.
Results
The study involved 992 pregnant women from the Diamater cohort (Figure 1). Thus, 616 had PS-UI, and 376 did not (non-PS-UI). Table 1 shows the demographic characteristics by PS-UI status.
Compared to those without PS-UI, women with PS-UI had a higher pregestational BMI (p=0.002) and BMI at the 1st TP (p=0.004) and 2nd TP (p=0.002). Moreover, women with PS-UI engaged in less physical activity during pregnancy (p=0.003) and presented with more chronic coughing (p=0.025).
PS-UI prevalence among the studied population was 62.1%, with 58.85% occurring between 24 and 28 weeks of gestation, as shown in Table 2. Excluding the 83 cases of early PS-UI (Figure 1), the prevalence of late PS-UI among pregnant women was 51%.
PS-UI, Pregnancy-Specific Urinary Incontinence; BMI, body mass index; OGTT, oral glucose tolerance test; TP, time point (first: 24-28 weeks of gestation; second: 36-38 weeks of gestation); Data are expressed as means ± standard deviations or absolute frequency (n) and percentage (%). The differences between the groups were compared using the Chi-square test. Significance p < 0.05. Percentages are based on the number of patients responding to each question.
Both early and late incontinence were associated with higher pregestational BMI and BMI from the time point it was assessed, as shown in Table 3. Women with early PS-UI engaged in less physical activity during pregnancy (p=0.004), while those with late PS-UI reported more chronic coughing (p=0.012) and alcohol consumption during pregnancy (p=0.047).
As demonstrated in Table 4, the logistic regression model identified pregestational BMI as a risk factor for PS-UI (OR=1.04, IC95%: 1.01; 1.07). Physical activity was identified as a protective factor, halving the risk of developing PS-UI (OR=0.5, IC95%: 0.32; 0.80). The analysis of the 1st TP also revealed that pregestational BMI was a risk factor and physical activity was a protective factor for Early PS-UI. There was no correlation between the variables and the incidence of Late PS-UI.
Discussion
PS-UI was prevalent in 62.1% of pregnant women, 58.85% began leaking urine between 24 and 28 gestational weeks, and 51% developed PS-UI at the end of pregnancy. The pregestational BMI is a risk factor for PS-UI, and physical activity is a protective factor that halves the risk of PS-UI developing.
A systematic review showed that primiparous women had a higher risk of postpartum UI following vaginal delivery compared to C-section, regardless of their continence status before childbirth. Nonetheless, the protective effect of C-section was significantly higher in nulliparous women without UI before delivery. Compared to our results, we detected a higher prevalence of PS-UI even in a sample with a previous C-section (21).
A literature review of lower urinary tract symptoms in women, with a particular emphasis on incontinence and overactive bladder, revealed that age, smoking, pregnancy, asthma, obesity, dementia, vaginal delivery, constipation, diuretic use, and certain medications were identified as risk factors for UI (22).
The pathophysiology underlying antenatal and postpartum UI remains poorly understood (23). The reduced protective effect of C-section against antenatal UI in nulliparous women with UI may be attributed to the characteristics of the women’s tissues (24). It is possible to assume that preexisting UI or pregnancy-induced UI may not be associated with perineal trauma but rather with weakened supportive tissues. Thus, it could clarify why a C-section may not prevent UI in such cases (21).
A recent study that evaluated pelvic floor outcomes at different stages of pregnancy, which included stress incontinence, anal incontinence, prolapse, and sexual dysfunction, found that at least one pelvic floor disorder symptom was experienced by 60.8% of the study cohort during pregnancy and that particular symptoms were exacerbated in the third trimester of pregnancy. The prevalence of PS-UI was lower than that presented in this study, with the participants ‘ overall rates equally distributed in the first, second, and third trimesters of pregnancy (p = 0.168). In the third trimester of pregnancy, symptoms related to urinary distress were reported to be more intense than those in the first and second trimesters of pregnancy (25).
Obesity is a well-established risk factor for UI, regardless of sex, age, and other factors (22). Hence, obesity may lead to UI in several ways. Firstly, excess weight puts additional pressure on the pelvis, bladder, and pelvic floor muscles, weakening these muscles and impairing the ability to control urination. Additionally, obesity may also increase systemic inflammation and intra-abdominal pressure, which can lead to bladder dysfunction and UI (26).
That weight loss may help improve UI in people with obesity. A study conducted by Subak et al. (2005) found that a structured weight loss program led to a significant reduction in UI episodes in overweight and obese women (27). Similarly, a meta-analysis reported that weight loss interventions were effective in reducing UI in women with obesity (28).
The exclusion of women with pregestational UI or vaginal deliveries in prior pregnancies may limit generalizability.
Conclusion
Most women had urinary incontinence at some point during their pregnancy. The onset of PS-UI was proportional among those who leaked urine between 24 and 28 gestational weeks and those who leaked at the end of pregnancy. The pregestational BMI is a risk factor for PS-UI, and physical activity is a protective factor that halves the risk of PS-UI developing. The findings suggest that weight management and encouragement to engage in physical activity during pregnancy should be incorporated into prenatal care to reduce the risk of PS-UI and, consequently, UI later in life.
Contributions
Conceptualization, Vitoria Barbosa, Sthefanie Kenickel Nunes, Patrícia Rossignoli, Bruna Catinelli, Raissa Avramidis, Adriely Bittencourt Magyori , Carlos Izaias Sartorao-Filho and Marilza Rudge; Data curation, Angélica Barbosa and Marilza Rudge; Formal analysis, Angélica Barbosa, Vitoria Barbosa, Patrícia Rossignoli, Cristiane Pedroni and Marilza Rudge; Funding acquisition, Angélica Barbosa and Marilza Rudge; Investigation, Henrique Caetano Bassin, Angélica Barbosa, Caroline Prudencio, Vitoria Barbosa, Sthefanie Kenickel Nunes, Danielle Cristina Honório França, Bruna Catinelli, Carolina Neiva Carvalho , Raissa Avramidis, Adriely Bittencourt Magyori , Carlos Izaias Sartorao-Filho and Marilza Rudge; Methodology, Henrique Caetano Bassin, Angélica Barbosa, Caroline Prudencio, Vitoria Barbosa, Cristiane Pedroni, Danielle Cristina Honório França, Bruna Catinelli, Carolina Neiva Carvalho , Raissa Avramidis, Adriely Bittencourt Magyori and Marilza Rudge; Project administration, Angélica Barbosa, Luis Sobrevia, Carlos Izaias Sartorao-Filho and Marilza Rudge; Resources, Henrique Caetano Bassin, Angélica Barbosa, Caroline Prudencio, Vitoria Barbosa, Sthefanie Kenickel Nunes, Danielle Cristina Honório França and Marilza Rudge; Software, Patrícia Rossignoli and Marilza Rudge; Supervision, Angélica Barbosa, Luis Sobrevia and Marilza Rudge; Validation, Angélica Barbosa, Caroline Prudencio, Sthefanie Kenickel Nunes, Carlos Izaias Sartorao-Filho and Marilza Rudge; Writing – original draft, Marilza Rudge; Writing – review & editing, Angélica Barbosa, Cristiane Pedroni, Carlos Izaias Sartorao-Filho and Marilza Rudge.
Funding
São Paulo Research Foundation (protocol numbers 2016/01743-5, 2019/04424-6, and 2020/09040-9) and Brazilian Federal Agency for Support and Evaluation of Graduate Education/SD - protocol number 88887.622419/2021-00. The funders had no role in study design, data collection and analysis, publication decisions, or manuscript preparation.
Conflicts of Interest
None
List of Abbreviations:
UI: urinary incontinence
PS-UI: pregnancy-specific urinary incontinence
GDM: gestational diabetes mellitus
OGTT: oral glucose tolerance test
BMI: body mass index
References
- Ali H, Ahmed A, Olivos C, Khamis K, Liu J. Mitigating urinary incontinence conditions using machine learning. BMC Med Inform Decis Mak. 2022;22(1):243. [CrossRef]
- Milsom I, Altman D, Cartwright R, et al. Epidemiology of urinary incontinence (UI) and other lower urinary tract symptoms (LUTS), pelvic organ prolapse (POP), and anal incontinence (AI). In: Abrams P, Cardozo L, Wagg A, Wein A, editors. Incontinence. 6th ed. International Continence Society; 2017. p. 4–142.
- Datar M, Pan LC, McKinney JL, Goss TF, Pulliam SJ. Healthcare resource use and cost burden of urinary incontinence to United States payers. Neurourol Urodyn. 2022;41(7):1553-1562. [CrossRef]
- Hvidman L, Foldspang A, Mommsen S, Bugge Nielsen J. Correlates of urinary incontinence in pregnancy. Int Urogynecol J Pelvic Floor Dysfunct. 2002;13(5):278-283. [CrossRef]
- Wesnes SL, Rortveit G, Bø K, Hunskaar S. Urinary incontinence during pregnancy. Obstet Gynecol. 2007;109(4):922-928. [CrossRef]
- Chang SR, Lin WA, Chang TC, Lin HH, Lee CN, Lin MI. Risk factors for stress and urge urinary incontinence during pregnancy and the first year postpartum: a prospective longitudinal study. Int Urogynecol J. 2021;32(9):2455-2464. [CrossRef]
- Zhu L, Li L, Lang JH, Xu T. Prevalence and risk factors for peri- and postpartum urinary incontinence in primiparous women in China: a prospective longitudinal study. Int Urogynecol J. 2012;23(5):563-572. [CrossRef]
- Wang X, Jin Y, Xu P, Feng S. Urinary incontinence in pregnant women and its impact on health-related quality of life. Health Qual Life Outcomes. 2022;20(1):13. [CrossRef]
- Nur Farihan M, Ng BK, Phon SE, Nor Azlin MI, Nur Azurah AG, Lim PS. Prevalence, Knowledge and Awareness of Pelvic Floor Disorder among Pregnant Women in a Tertiary Centre, Malaysia. Int J Environ Res Public Health. 2022;19(14):8314. [CrossRef]
- Hage-Fransen MAH, Wiezer M, Otto A, et al. Pregnancy- and obstetric-related risk factors for urinary incontinence, fecal incontinence, or pelvic organ prolapse later in life: A systematic review and meta-analysis. Acta Obstet Gynecol Scand. 2021;100(3):373-382. [CrossRef]
- Daly D, Clarke M, Begley C. Urinary incontinence in nulliparous women before and during pregnancy: prevalence, incidence, type, and risk factors. Int Urogynecol J. 2018;29(3):353-362. [CrossRef]
- Piculo F, Marini G, Vesentini G, et al. Pregnancy-specific urinary incontinence in women with gestational hyperglycemia worsens the occurrence and severity of urinary incontinence and quality of life over the first year postpartum. Eur J Obstet Gynecol Reprod Biol. 2020;252:336-343. [CrossRef]
- Mason L, Glenn S, Walton I, Hughes C. Women’s reluctance to seek help for stress incontinence during pregnancy and following childbirth. Midwifery. 2001;17(3):212–221. [CrossRef]
- Anyanwu L-JJC, Anyanwu OM, Yakubu AA. Missed opportunities for breast awareness information among women attending the maternal and child health services of an urban tertiary hospital in Northern Nigeria. J Cancer Res Ther. 2016;12:765–769. [CrossRef]
- Nagraj S, Kennedy SH, Norton R, et al. Cardiometabolic Risk Factors in Pregnancy and Implications for Long-Term Health: Identifying the Research Priorities for Low-Resource Settings. Front Cardiovasc Med. 2020;7:40. [CrossRef]
- Tudor Car L, Van Velthoven MH, Brusamento S, et al. Integrating prevention of mother-to-child HIV transmission programs to improve uptake: a systematic review. PLoS One. 2012;7(4):e35268. [CrossRef]
- Rudge MVC, Souza FP, Abbade JF, et al. Study protocol to investigate biomolecular muscle profile as predictors of long-term urinary incontinence in women with gestational diabetes mellitus. BMC Pregnancy Childbirth. 2020;20(1):117. Published 2020 Feb 19. [CrossRef]
- Rudge MVC, Calderon I de MP, Ramos MD, et al. Hiperglicemia materna diária diagnosticada pelo perfil glicêmico: um problema de saúde pública materno e perinatal. Rev Bras Ginecol Obstet. 2005;27(11):691-697. [CrossRef]
- International Association of Diabetes and Pregnancy Study Groups Consensus Panel, Metzger BE, Gabbe SG, et al. International association of diabetes and pregnancy study groups recommendations on the diagnosis and classification of hyperglycemia in pregnancy. Diabetes Care. 2010;33(3):676-682. [CrossRef]
- Abrams P, Cardozo L, Fall M, et al. The standardization of terminology in lower urinary tract function: report from the standardization sub-committee of the International Continence Society. Urology. 2003;61(1):37-49. [CrossRef]
- Pizzoferrato AC, Briant AR, Le Grand C, Gaichies L, Fauvet R, Fauconnier A, et al. Influence of prenatal urinary incontinence and mode of delivery in postnatal urinary incontinence: A systematic review and meta-analysis. J Gynecol Obstet Hum Reprod. 2023 Mar;52(3):102536. [CrossRef]
- Tahra A, Bayrak O, Dmochowski R. The Epidemiology and Population-Based Studies of Women with Lower Urinary Tract Symptoms: A Systematic Review. Türk Üroloji Dergisi/Turkish J Urol [Internet]. 2022 Apr 7;48(2):155–65. Available from: https://turkishjournalofurology.com/en/the-epidemiology-and-population-based-studies-of-women-with-lower-urinary-tract-symptoms-a-systematic-review-133793. [CrossRef]
- Fitzgerald, M. P., & Brensinger, C. M. What We Don’t Know About Pelvic Floor Disorders in Women. Obstetrics and GynecologyGynecology Clinics of North America. 2021; 48(4), 665-678. [CrossRef]
- Rafique S, Iqbal N, Alvi R. Risk factors for antenatal urinary incontinence in nulliparous women: A systematic review. Int J Womens Health. 2021;13:83-92.
- Baruch Y, Manodoro S, Barba M, Cola A, Re I, Frigerio M. Prevalence and Severity of Pelvic Floor Disorders during Pregnancy: Does the Trimester Make a Difference? Healthcare. 2023 Apr 11;11(8):1096. [CrossRef]
- Ferreira BL, Souza RT, Dutra LO, Moura CS. Urinary incontinence in obese women: a systematic review and meta-analysis. Int Urogynecol J. 2020 Nov;31(11):2215-2224. [CrossRef] [PubMed]
- Subak LL, Wing R, West DS, Franklin F, Vittinghoff E, Creasman JM, et al. Weight Loss to Treat Urinary Incontinence in Overweight and Obese Women. N Engl J Med. 2009 Jan 29;360(5):481–90. [CrossRef]
- Yazdany T, Jakus-Waldman S, Jeppson PC, Schimpf MO, Yurteri-Kaplan LA, Ferzandi TR, et al. American Urogynecologic Society Systematic Review: The Impact of Weight Loss Intervention on Lower Urinary Tract Symptoms and Urinary Incontinence in Overweight and Obese Women. Female Pelvic Med Reconstr Surg. 2020 Jan;26(1):16–29. [CrossRef]
Figure 1.
The Diamater cohort fluxogram.
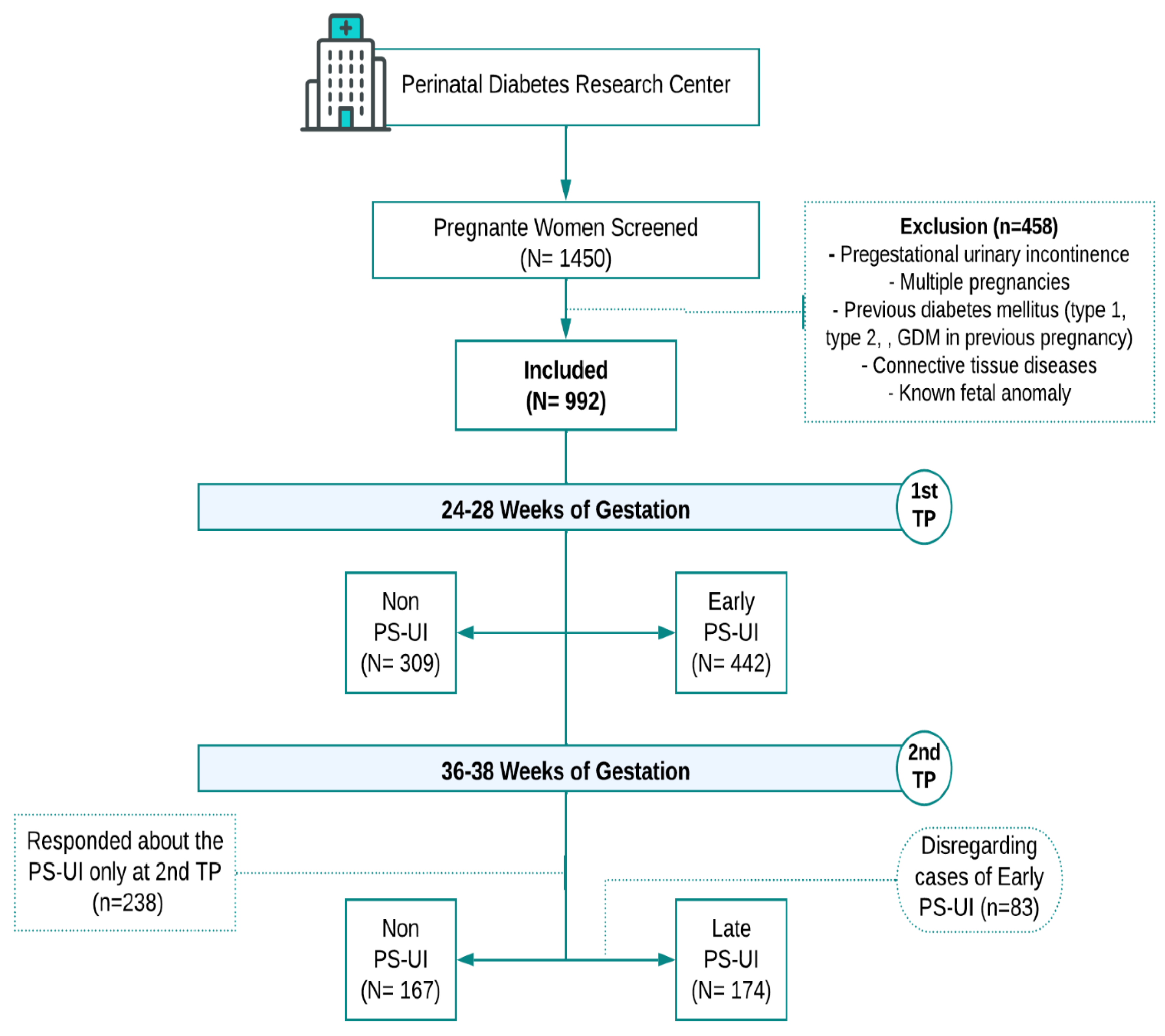

Table 1.
Characteristics of the study population.
| Variable | non PS-UI | PS-UI | p - value | ||
|---|---|---|---|---|---|
| Partnership status | Married | 311 (83.4%) | 515 (83.6%) | 0.926 | |
| Not married | 62 (16.6%) | 101 (16.4%) | |||
| Education level | basic level | 27 (7.2%) | 42 (6.9%) | 0.014 | |
| high school | 229 (61.1%) | 427 (69.7%) | |||
| college/university | 119 (31.7%) | 144 (23.5%) | |||
| Ethnicity | Caucasian | 299 (81%) | 495 (80.5%) | 0.835 | |
| Non-caucasian | 70 (19%) | 120 (19.5%) | |||
| Pregestational BMI (kg/m2) | 26.9 ± 6.25 | 28.48 ± 7.28 | 0.002 | ||
| BMI - 1st TP (kg/m2) | 29.4 ± 6.04 | 30.8 ± 6.85 | 0.004 | ||
| BMI - 2nd TP (kg/m2) | 31.6 ± 6.20 | 33.75 ± 6.51 | 0.002 | ||
| Gestational weight gain - 1st TP (kg) | 6.39 ± 5.04 | 6.08 ± 6.19 | 0.477 | ||
| Gestational weight gain - 2nd TP (kg) | 11.76 ± 7.34 | 11.36 ± 7.63 | 0.613 | ||
| Fasting blood glucose (mg/dL) | 79.48 ± 12.71 | 80.11 ± 14.44 | 0.583 | ||
| OGTT - fasting (mg/dL) | 74.82 ± 12.66 | 76.11 ± 11.06 | 0.161 | ||
| OGTT- 1 h (mg/dL) | 116.7 ± 31.27 | 119.17 ± 32.7 | 0.321 | ||
| OGTT - 2 h (mg/dL) | 105.08 ± 28.1 | 107.01± 8.88 | 0.378 | ||
| Chronic coughing | 0 | 9 (1.8%) | 0.025 | ||
| Constipation | 91 (31.5%) | 152 (28.9%) | 0.439 | ||
| Fecal incontinence | 3 (1.1%) | 6 (1.2%) | 0.887 | ||
| Previous arterial hypertension | 24 (8.3%) | 53 (10.2%) | 0.376 | ||
| Alcohol consumption | 1 (0.4%) | 9 (1.8%) | 0.091 | ||
| Smoking in pregnancy | 12 (4.3%) | 26 (5%) | 0.615 | ||
| Physical activity | 66 (23.1%) | 76 (14.7%) | 0.003 | ||
| Gestational diabetes mellitus | 81 (22%) | 154 (25.2%) | 0.242 | ||
| Pregnancy-induced hypertension | 2 (3%) | 8 (4.4%) | 0.611 | ||
| Urinary tract infection | 7 (10.8%) | 22 (12.4%) | 0.735 | ||
PS-UI, Pregnancy-Specific Urinary Incontinence; BMI, body mass index; OGTT, oral glucose tolerance test; TP, time point (1st: 24-28 weeks of gestation; 2nd: 36-38 weeks of gestation); Data are expressed as mean ± standard deviations or absolute frequency (n) and percentage (%). The differences between the groups were compared using the Chi-square test. Significance p < 0.05. Percentages are based on the number of patients responding to each question.
Table 2.
Prevalence of Pregnancy-Specific Urinary Incontinence.
| Weeks of gestation | ||||
|---|---|---|---|---|
| n | % | |||
| 24-28 weeks | ||||
| 1st TP | (1) non PS-UI | 309 | 41.15 | |
| (2) Early PS-UI | 442 | 58.85 | ||
| 36-38 weeks | ||||
| 2nd TP | (1) non PS-UI | 167 | 49.0 | |
| (2) Late PS-UI | 174 | 51.0 | ||
| 1st and 2nd TP | ||||
| (1) non-PS-UI | 376 | 37.9 | ||
| (2) PS-UI | 616 | 62.1 |
PS-UI, Pregnancy-Specific Urinary Incontinence; TP, time point (1st: 24-28 weeks of gestation; 2nd: 36-38 weeks of gestation); Data are expressed as absolute frequency (n) and percentage (%).
Table 3.
Association between Pregnancy-Specific Urinary Incontinence (PS-UI) and characteristics according to the time points.
Table 3.
Association between Pregnancy-Specific Urinary Incontinence (PS-UI) and characteristics according to the time points.
| Variable | 1st TP | 2nd TP | ||||||
|---|---|---|---|---|---|---|---|---|
| non PS-UI (n=309) | Early PS-UI (n=442) | p-value | non PS-UI (n=167) | Late PS-UI (n=174) | p-value | |||
| Partnership status | Married | 261 (84.5%) | 367 (83%) | 0.601 | 136 (82.4%) | 148 (85.1%) | 0.511 | |
| Not-married | 48 (15.5%) | 75 (17%) | 29 (17.6%) | 26 (14.9%) | ||||
| Education level | basic level | 22 (7.1%) | 27 (6.1%) | 0.007 | 11 (6.6%) | 15 (8.7%) | 0.210 | |
| high school | 191 (61.8%) | 319 (72.5%) | 93 (55.7%) | 108 (62.4%) | ||||
| college/university | 96 (31.1%) | 94 (21.4%) | 63 (5.2%) | 50 (28.9%) | ||||
| Ethnicity | Caucasian | 253 (82.4%) | 365 (82.6%) | 0.952 | 124 (76.1%) | 130 (75.1%) | 0.843 | |
| Non-caucasian | 54 (17.6%) | 77 (17.4%) | 39 (23.9%) | 43 (24.9%) | ||||
| Pregestational BMI (kg/m2) | 27.04 ± 6.28 | 28.5 ± 7.33 | 0.003 | 27.31 ± 6.42 | 29.47 ± 6.69 | 0.003 | ||
| BMI - 1st TP (kg/m2) | 29.49 ± 6.1 | 30.83 ± 6.87 | 0.005 | 29.58 ± 6.8 | 30.24 ± 6.64 | 0.637 | ||
| BMI - 2nd TP (kg/m2) | 31.23 ± 6.76 | 33.49 ± 6.33 | 0.213 | 31.67 ± 6.2 | 33.92 ± 6.64 | 0.002 | ||
| Gestational weight gain - 1st TP (kg) | 6.31 ± 5.01 | 6.09 ± 6.26 | 0.614 | 6.18 ± 7.73 | 5.85 ± 4.97 | 0.833 | ||
| Gestational weight gain - 2nd TP (kg) | 10.81 ± 5.55 | 10.62 ± 8.76 | 0.863 | 11.6 ± 8.18 | 11.81 ± 6.83 | 0.802 | ||
| Fasting blood glucose (mg/dL) | 79.86 ± 12.4 | 79.42 ± 12.23 | 0.691 | 81.63 ± 13.26 | 82.12 ± 19.37 | 0.826 | ||
| OGTT - fasting (mg/dL) | 74.58 ± 12.83 | 75.77 ± 10.58 | 0.206 | 78.46 ± 11.73 | 77.84 ± 13.2 | 0.755 | ||
| OGTT- 1 h (mg/dL) | 115.65 ± 29.98 | 118.24 ± 32.9 | 0.311 | 126.02 ± 35.13 | 123.81 ± 31.5 | 0.755 | ||
| OGTT - 2 h (mg/dL) | 105.08 ± 26.77 | 106.19 ± 28.86 | 0.615 | 112.05 ± 33.39 | 111.15 ± 28.87 | 0.862 | ||
| Chronic coughing | 0 | 1 (0.3%) | 0.426 | 0 | 8 (6.7%) | 0.012 | ||
| Constipation | 79 (31.6%) | 113 (28.7%) | 0.430 | 27 (27.8%) | 39 (29.5%) | 0.778 | ||
| Fecal incontinence | 1 (0.4%) | 3 (0.8%) | 0.568 | 2 (2.2%) | 3 (2.5%) | 0.879 | ||
| Previous arterial hypertension | 17 (6.8%) | 29 (7.3%) | 0.795 | 12 (12.4%) | 24 (19.4%) | 0.163 | ||
| Alcohol | 1 (0.4%) | 4 (1%) | 0.391 | 0 | 5 (4.2%) | 0.047 | ||
| Smoking | 8 (3.2%) | 19 (4.8%) | 0.328 | 6 (6.6%) | 7 (5.9%) | 0.832 | ||
| Physical activity | 53 (21.4%) | 51 (12.8%) | 0.004 | 22 (22.9%) | 25 (20.7%) | 0.689 | ||
| Gestational diabetes mellitus | 70 (23.0%) | 103 (23.5%) | 0.877 | 116 (70.7%) | 121 (70.3%) | 0.939 | ||
| Pregnancy-induced hypertension | 0 | 3 (4.2%) | 0.185 | 3 (3.8%) | 5 (4.6%) | 0.778 | ||
| Urinary infection | 1 (2.6%) | 7 (9.5%) | 0.184 | 9 (11.3%) | 15 (14.4%) | 0.526 | ||
PS-UI, Pregnancy-Specific Urinary Incontinence; BMI, body mass index; OGTT, oral glucose tolerance test; TP, time point (1st: 24-28 weeks of gestation; 2nd: 36-38 weeks of gestation); Data are expressed as means ± standard deviations or absolute frequency (n) and percentage (%). The differences between the groups were compared using the Chi-square test. Significance p < 0.05. P-values represent the results from the relevant statistical tests. Percentages are based on the number of patients responding to each question.
Table 4.
Model of logistic regression model of Pregnancy-Specific Urinary Incontinence (PS-UI).
| Variable | Early PS-UI (n=442) | Late PS-UI (n=442) | PS-UI (1st plus 2nd TP) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| OR* | 95% CI** | p - value | OR* | 95% CI** | p - value | OR* | 95% CI** | p - value | ||||||
| Education level | basic level | |||||||||||||
| high school | 1.28 | 0.62 ; 2.63 | 0.172 | 0.62 | 0.04 | 9.28 | 0.491 | 1.21 | 0.58 ; 2.51 | 0.304 | ||||
| college/university | 0.89 | 0.40 ; 1;96 | 0.359 | 1.20 | 0.08 ; 19.02 | 0.629 | 0.91 | 0.41 ; 2.04 | 0.493 | |||||
| Ethnicity | Caucasian | 1.22 | 0.76 ; 1.96 | 0.416 | 2.65 | 0.46 ; 15.15 | 0.274 | 1.28 | 0.88 ; 0.78 | 0.519 | ||||
| Non-caucasian | ||||||||||||||
| Age (years) | 0.99 | 0.96 ; 1.02 | 0.375 | 1.01 | 0.92 ; 1.12 | 0.805 | 0.99 | 0.96 ; 1.03 | 0.706 | |||||
| Pregestational BMI | 1.03 | 1.01 ; 1.06 | 0.014 | 1.02 | 0.93 ; 1.11 | 0.716 | 1.04 | 1.01 ; 1.07 | 0.006 | |||||
| Constipation | 1.21 | 0.84 ; 0.83 | 0.312 | 1.02 | 0.26 ; 4.03 | 0.974 | 0.78 | 0.54 ; 1.13 | 0.193 | |||||
| Fecal incontinence | 3.02 | 0.29 ; 31.82 | 0.358 | 2.81 | 0.26 ; 29.92 | 0.392 | ||||||||
| Previous arterial hypertension | 0.83 | 0.41 ; 1.70 | 0.616 | 1.4 | 0.16 ; 12.32 | 0.761 | 0.84 | 0.41 ; 1.76 | 0.652 | |||||
| Smoking | 2.08 | 0.78 ; 5.53 | 0.141 | 1.85 | 0.69 ; 4.91 | 0.220 | ||||||||
| Physical activity | 0.51 | 0.32 ; 0.80 | 0.003 | 0.72 | 0.13 ; 3.88 | 0.700 | 0.5 | 0.32 ; 0.79 | 0.003 | |||||
| Gestational diabetes mellitus | 1.10 | 1.01 ; 1.06 | 0.649 | 0.94 | 0.25 ; 3.58 | 0.928 | 1.16 | 0.75 ; 1.81 | 0.500 | |||||
PS-UI, Pregnancy-Specific Urinary Incontinence; BMI, body mass index; TP, time point (1st: 24-28 weeks of gestation; 2nd: 36-38 weeks of gestation); *Odds Ratio ; **95% Confidence Interval for Odds Ratio; Significance p < 0.05. P-values represent the results from the relevant statistical tests.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



