Submitted:
27 June 2025
Posted:
27 June 2025
You are already at the latest version
Abstract
Surrogacy involves a surrogate carrying a baby to transfer to the intended parents after birth. This study examines how surrogacy impacts attachment patterns compared to traditional pregnancies or assisted reproductive technologies. Using PRISMA guidelines, a systematic review of databases like Scopus and PubMed identified nine relevant studies from 806 initial records, involving 1,317 participants (115 pregnant women and 118 children). Key variables included maternal-fetal attachment, depression, anxiety, and somatization in surrogates, alongside intended parents’ support and children’s exploration of their origins. Findings reveal the complexity of attachment dynamics in surrogacy, emphasizing the need for psychological support and preparation to foster secure attachments among surrogates, children, and intended parents.
Keywords:
surrogacy
; attachment
; maternal-fetal attachment
; psychological support
; systematic review
1. Introduction
Surrogacy is a controversial reproductive method often employed in cases of infertility to establish biological ties with offspring [1]. It can be categorized into traditional and gestational types. In traditional surrogacy, the gestational carrier's eggs are used, making her genetically related to the child. In gestational surrogacy, an egg donor is involved, resulting in no genetic link between the carrier and the embryo [2].
The psychological effects of surrogacy on both the gestational carrier and the child are not fully understood [3]. Research indicates that surrogates may develop less attachment to the developing embryo [4]. This emotional detachment might serve as a coping mechanism to avoid forming bonds with the embryo, thereby reducing the emotional impact of relinquishing the child [5].
Attachment theory suggests that the attachment formed during pregnancy generally transfers to the child after birth [6]. Surrogates who do not bond with the embryo may use emotional distancing or avoidance as coping strategies, potentially mitigating feelings of loss when the baby is born [5]. Observations indicate that surrogates with a commercial perspective may experience psychological detachment as preparation for emotional separation, though this may lead to long-term difficulties [7,8].
Regarding children born via surrogacy, a longitudinal study found that most do not report negative impacts on their relationships with their parents due to the lack of a genetic or gestational connection [9]. Many parents and children perceive surrogacy positively, with children expressing pride and gratitude for their mothers' roles as surrogates. However, some children have shown ambivalence, anxiety, and sadness about the experience [10].
Recent reviews suggest that gestational carriers might face long-term psychological effects, such as anxiety, depression, or feelings of insecurity [11]. The varying degrees of attachment formed during pregnancy could contribute to these psychological challenges upon relinquishing the child [12].
Considering these complexities, surrogacy presents significant ethical, legal, and psychological implications [11]. Understanding attachment dynamics between surrogate carriers and newborns is crucial [3]. As surrogacy becomes more prevalent [13], it is essential to examine its impact on emotional bonds. This study aims to analyze attachment patterns in surrogacy through a systematic review, exploring its psychological and social implications. The research question guiding this study is: How does surrogacy affect attachment patterns between children born through this method and their intended parents compared to children born through conventional pregnancies or assisted reproductive techniques [14]?
2. Materials and Methods
2.1. Procedure & Ethical Considerations
A qualitative systematic review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [15]. The protocol for this review was registered with PROSPERO (CRD42024534262).
Databases searched included Web of Science, Scopus, PubMed, and ProQuest. The search was conducted in March 2024. Boolean expressions used were as follows: (TS=(surrogacy OR surrogate motherhood OR assisted reproduction OR gestational carrier OR surrogate mother OR gestational surrogacy) AND TS=(attachment OR bonding OR bond* OR mother attachment OR child attachment)) in Web of Science; (TITLE-ABS-KEY (surrogacy OR surrogate motherhood OR assisted reproduction OR gestational carrier OR surrogate mother OR gestational surrogacy) AND TITLE-ABS-KEY (attachment OR bonding OR bond* OR mother attachment OR child attachment)) in Scopus; noft(surrogacy OR surrogate motherhood OR assisted reproduction OR gestational carrier OR surrogate mother OR gestational surrogacy) AND noft(attachment OR bonding OR bond* OR mother attachment OR child attachment) in ProQuest; and in PubMed using the [Title/Abstract] field (surrogacy OR surrogate motherhood OR assisted reproduction OR gestational carrier OR surrogate mother OR gestational surrogacy) AND (attachment OR bonding OR bond* OR mother attachment OR child attachment).
Inclusion criteria were: (a) studies evaluating factors related to attachment in surrogacy, (b) published in peer-reviewed scientific journals, (c) published in any language, and (d) published from 1959 to 2024.
Exclusion criteria included: (a) grey literature such as conference papers, (b) doctoral theses, (c) narrative reviews, (d) single-case studies, (e) articles not reporting results specific to surrogacy, (f) articles not evaluating attachment, (g) studies analyzing only the epidemiology or prevalence of surrogacy, and (h) articles not primarily focusing on surrogacy.
Retrieved articles were uploaded to HubMeta [16], an online platform for screening and data extraction in systematic reviews and meta-analyses. Duplicates were automatically removed. Two researchers (E.M.G.-A. and L.L.-T.) independently reviewed titles and abstracts to exclude studies that did not meet the inclusion criteria. Articles with discrepancies in the blind evaluations of the two researchers underwent detailed individual blind reading and re-evaluation to ensure adherence to the inclusion and exclusion criteria.
To assess inter-rater reliability, Cohen's Kappa (κ) was calculated [17]. Values between -1 and 0.40 are considered unsatisfactory, values between 0.41 and 0.75 are considered satisfactory, and values of 0.76 or greater are considered very satisfactory [18].
Databases searched included Web of Science, Scopus, PubMed, and ProQuest. The search was conducted in March 2024. Boolean expressions used were as follows: (TS=(surrogacy OR surrogate motherhood OR assisted reproduction OR gestational carrier OR surrogate mother OR gestational surrogacy) AND TS=(attachment OR bonding OR bond* OR mother attachment OR child attachment)) in Web of Science; (TITLE-ABS-KEY (surrogacy OR surrogate motherhood OR assisted reproduction OR gestational carrier OR surrogate mother OR gestational surrogacy) AND TITLE-ABS-KEY (attachment OR bonding OR bond* OR mother attachment OR child attachment)) in Scopus; noft(surrogacy OR surrogate motherhood OR assisted reproduction OR gestational carrier OR surrogate mother OR gestational surrogacy) AND noft(attachment OR bonding OR bond* OR mother attachment OR child attachment) in ProQuest; and in PubMed using the [Title/Abstract] field (surrogacy OR surrogate motherhood OR assisted reproduction OR gestational carrier OR surrogate mother OR gestational surrogacy) AND (attachment OR bonding OR bond* OR mother attachment OR child attachment).
2.2. Quality Assessment
The quality of the included studies was independently and blindly assessed by the authors (E.M.G.-A. and L.L.-T.) using an adapted version of the "Quality Assessment Tool for Quantitative Studies" developed by the Effective Public Health Practice Project [19]. This assessment was based on seven criteria: study design, selection bias, withdrawals and dropouts, confounders, data collection, data analysis, and results.
Each study was rated on 4 to 8 components based on these criteria, and an overall score was determined from these ratings. Studies were classified as "strong" if there were no "weak" ratings and at least three "moderate" ratings; "moderate" if there was one "weak" rating or fewer than three "strong" ratings; and "weak" if there were two or more "weak" ratings [20].
The total score was derived by averaging the ratings across the criteria and was categorized as weak, moderate, or strong. Scores ranged from 1 to 5, with 1 indicating low risk and high methodological quality, and 5 indicating high risk and low methodological quality [20].
2.3. Study Selection and Screening
Figure 1 illustrates the study selection process. After conducting the literature search and applying the search criteria, duplicate articles (n = 1,079) were removed, resulting in 804 articles for initial analysis. During the first selection stage, 778 studies were excluded based on title and abstract evaluation for not meeting the inclusion and exclusion criteria.
The full texts of the remaining 24 articles were then reviewed. The inter-rater reliability between the two independent evaluators (E.M.G.-A. and L.L.-T.) for screening titles and abstracts was excellent (κ = 0.89).
In the second selection phase, 15 papers were excluded: 7 for not providing the evaluated measures or variables, 7 for being theoretical articles or reviews, and 1 for being a case report. Consequently, 9 studies were selected for final analysis. The agreement between evaluators in this stage was also excellent (κ = 0.90).
3. Results
3.1. Study Characteristics.
3.1.1. Participants
Participant characteristics are summarized in Table 1. The nine selected articles included a total of 1,317 participants, comprising women, men, and children. Among the women (n = 371), 115 (8.73%) were gestational carriers [4,21,22], 122 (9.26%) were mothers who did not conceive through surrogacy [4,21,22], and 134 (10.17%) were lesbian mothers who conceived through assisted reproductive techniques, specifically donor insemination [24,26].
Among the men (n = 423), 353 (26.80%) were gay fathers who used surrogacy [20,24,25,26,27,28], and 70 (5.31%) were heterosexual fathers, with 28 through surrogacy [25] and 42 through assisted reproductive techniques, specifically gamete donation [24].
Children (n = 523) participated in the studies, comprising 39.71% of the sample. Specifically, 118 (22.56% of 523) were born through surrogacy [20,24,26,27], 67 (12.81% of 523) through donor insemination [24,26], 21 (4.01% of 523) through gamete donation [24], and the remaining 317 (60.61% of 523) were a control group of children born conventionally [26].
3.1.2. Sample Selection and Research Design
For sample selection, participants in five studies were recruited through internet forums [20,22,25,26,27] Additionally, seven studies used surrogacy contact associations [20,22,23,24,25,26,27]. Specifically, five studies involved “Rainbow Families,” the primary association of LGBTQ+ parents using assisted reproduction in Italy [20,23,24,26,27]. Four studies recruited through surrogacy agencies [4,21,22], three through same-sex parenting events [20,26,27], and six used snowball sampling [20,23,24,25,26,27].
Regarding research designs, three studies were longitudinal, with two evaluations each [20,21,27]. One study evaluated during gestation and after birth [21], while two studies evaluated years after birth [20,27]. The average evaluation period was 16 months, with a range of 13 to 18 months between evaluations.
3.1.3. Variables: Attachment Evaluation
The studies evaluated a range of dependent variables, with a focus on attachment evaluation. Five studies assessed child attachment [20,23,24,25,26] using the modified SS Questionnaire [29,30,31], the Paternal Prenatal Attachment Scale (PAAS; [32,33]), and interviews with friends and family (FFI; [34]).
Maternal-fetal attachment was evaluated in three studies [4,21,22] using the Maternal-Fetal Attachment Scale [35] and the Maternal Prenatal Attachment Scale (MAAS; [32]). Additionally, parental attachment states were measured using the Adult Attachment Interview (AAI; [36,37]) in two studies [24,27]. Parental identification of attachment figures and their willingness to act as a reference figure were also assessed [26].
3.2. Main Results
3.2.1. Attachment
Two studies [4,21] reported that surrogate gestational carriers exhibited a lower maternal-fetal bond compared to the control group. This diminished bond was characterized by reduced emotional connection, less interaction, fewer attributions of characteristics and intentions to the unborn baby, and less differentiation between the "self" and the unborn baby.
Another study [22] found that the type of surrogacy influenced the quality of maternal-fetal attachment, and the bond with the intended parents affected the number of gestational babies born. Attachment security was found to impact children’s exploration of their origins through surrogacy [20]. It did not differ by family type or surrogacy method, whether for gay fathers or lesbian mothers [26]. Additionally, attachment security was predicted by parents' willingness to act as attachment figures and their parenting behaviors [26]. Carone and colleagues [23] observed that the COVID-19 pandemic significantly affected the father-child bond in surrogacy families. Furthermore, another study found a positive relationship between the quality of co-parenting experienced by single parents in their families of origin and attachment security in their own surrogacy families [25], indicating that co-parenting influences the attachment between parents and children in surrogacy [27].
In contrast, another study by Carone and collaborators [24] found no significant differences in the distribution of attachment patterns among children born through surrogacy compared to those born through other assisted reproductive methods or from the general population.
3.2.2. Pregnancy Experience and Support
3.2.3. Psychopathology
Three studies assessed depression, anxiety, and somatization. One study found that the nationality of surrogate mothers influenced their levels of depression [22]. Lamba and colleagues [21] observed that surrogate gestational carriers exhibited higher levels of depression compared to the control group of mothers during pregnancy and after childbirth. Additionally, surrogate fathers experienced higher levels of depression during the pandemic compared to gay fathers who had children before the pandemic [23].
Regarding anxiety, one study found no significant differences between surrogate carriers and other types of mothers during pregnancy or after childbirth [21]. However, during the pandemic, another study found that surrogate fathers experienced higher levels of anxiety and increased somatization compared to those who had children before the pandemic [23].
3.2.4. Influential Variables
Age was found to affect both gestational and traditional surrogacy, as well as the number of gestational children and surrogacy for gay couples [22]. Similarly, the type of surrogacy influenced the number of gestational or traditional children born [22].
No significant differences were found between boys and girls in exploring their surrogacy origins. However, a longitudinal study showed that the interaction between disclosure and parental mind coherence at time 1 predicted greater exploration in children [27].
3.3. Quality Assessment
Table 2 presents the quality ratings assigned to the studies. The average quality score was 1.98, indicating generally moderate quality across all evaluated studies. Quality scores range from 1 to 5, with 1 representing the highest quality (lowest risk of bias) and 5 representing the lowest quality (highest risk of bias). The quality assessment was conducted by one evaluator (E.M.G.-A.).
4. Discussion
This study aims to understand how surrogacy affects attachment patterns between children born through this technique and their intended parents compared to children born through conventional pregnancies or assisted reproductive m[4,21,22ethods. The main findings indicate that maternal-fetal attachment and attachment security are influenced by various factors, including the type of surrogacy, the quality of the bond with intended parents, the parents' willingness to act as attachment figures, their parenting behaviors, the stressful experience of the COVID-19 pandemic, and the quality of co-parenting.
Firstly, surrogate gestational carriers exhibit lower maternal-fetal attachment, characterized by diminished emotional connection, reduced interaction, and fewer attributions of characteristics to the unborn baby compared to the control group [4,21,22]. This may relate to the psychological preparation required for the separation between the carrier and the baby. Stressful situations, such as those experienced during surrogacy, can lead to dissociative symptoms, which, while initially adaptive, may result in mental health issues for both the carrier and the baby [17,18]. Such dissociation might also result in a lack of guilt and engagement in risky behaviors due to emotional disconnection [17]. For babies born via surrogacy, dissociation and emotional regulation difficulties are proportional to the trauma associated with this method [18]. The type of surrogacy and the relationship with the intended parents significantly influence maternal-fetal attachment quality, emphasizing the importance of the pre-birth context in emotional relationships and subsequent outcomes [22].
Attachment security in children born via surrogacy is influenced by the willingness and behaviors of intended parents [20,26], underscoring the need for strong emotional support to foster healthy psychological development in these children.
Surrogate gestational carriers experience both positive and negative attitudes toward pregnancy and the unborn baby [4,21], reflecting potential emotional conflicts regarding surrogacy. Perceived lower social support can exacerbate these emotional tensions. Psychopathology assessments reveal that surrogate carriers experience higher levels of depression during and after pregnancy compared to non-surrogate mothers [21,22]. During the COVID-19 pandemic, surrogate fathers also exhibited higher levels of anxiety and somatization compared to other gay fathers [23]. These findings highlight the need for psychological support throughout the surrogacy process.
Two longitudinal studies [20,24] focused on children's exploration of their surrogacy origins, showing that attachment security and parental support significantly influence children's curiosity about their origins. Parental transparency and emotional coherence create a secure environment for children to explore their birth circumstances, with more supportive parents leading to greater exploration.
Although the study provides valuable insights, some limitations must be acknowledged. The limited sample sizes and the small number of researchers studying this topic may impact the generalizability of the results. Additionally, the absence of random and multicenter selection introduces potential biases, affecting external validity. The studies are not cross-cultural, and surrogacy regulations vary by country, reflecting diverse experiences. Future research could address other relevant variables for secure attachment, such as the adult attachment of surrogates [8], family structure and cohesion [9], and traumatic childhood experiences [10].
Despite these limitations, this study provides a systematic review of how surrogacy affects attachment patterns in surrogates, intended families, and children born through this method. Although limited to nine studies, the research covers a broad range of variables, offering valuable insights into this evolving practice over time and across countries.
Clinically, these results highlight the importance of incorporating psychological care into surrogacy support programs. Health professionals should be empathetically trained to understand the context and consequences of surrogacy to better support all parties involved.
5. Conclusions
Clinically, these results highlight the importance of incorporating psychological care into surrogacy support programs. Health professionals should be empathetically trained to understand the context and consequences of surrogacy to better support all parties involved.
In conclusion, this study demonstrates that factors such as the type of surrogacy, the COVID-19 pandemic, and the sexual orientation of intended families significantly influence attachment patterns between parents and children in surrogacy contexts. The findings suggest that attachment security, crucial for children's psychological development, can be affected by family dynamics and external conditions. Both surrogates and intended parents should receive psychological support and preparation to foster a stable environment that promotes secure attachment. Additionally, the results advocate for adapting policies and clinical practices to safeguard the well-being of all parties involved in surrogacy.
Author Contributions
Conceptualization, E.M.G-A and L.L-T.; writing—original draft preparation, E.M.G-A and L.L-T.; writing—review and editing, R.S-G and F.G-S; supervision, R.S-G and F.G-S project administration, L.L-T. All authors have contributed equally to the writing of the manuscript. All authors read and approved the final manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author, [L.L-T.], upon reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Taebi, M., Alavi, N. M., & Ahmadi, S. M. (2020). The experiences of surrogate mothers: A qualitative study. Nursing and Midwifery Studies, 9(2), 51–59. [CrossRef]
- Gunnarsson Payne, J., Korolczuk, E., & Mezinska, S. (2020). Surrogacy relationships: a critical interpretative review. Upsala Journal of Medical Sciences, 125(2), 183–191. [CrossRef]
- Kardasz, Z., Gerymski, R., & Parker, A. (2023). Anxiety, Attachment Styles and Life Satisfaction in the Polish LGBTQ+ Community. International Journal of Environmental Research and Public Health, 20(14), 6392. [CrossRef]
- *Fischer, S., & Gillman, I. (1991). Surrogate Motherhood: Attachment, Attitudes and Social Support. Psychiatry (New York), 54(1), 13–20. [CrossRef]
- van den Akker, O. B. A. (2017). Separation and Parenting a Surrogate Baby. Surrogate Motherhood Families, 147–168. [CrossRef]
- Rubin, R. (1984) Maternal identity and the maternal experience. New York: Springer.
- Baslington, H. (2002). The social organization of surrogacy: Relinquishing a baby and the role of payment in the psychological detachment process. Journal of Health Psychology, 7(1), 57–71. [CrossRef]
- Snyder, K. S., Luchner, A. F., & Tantleff-Dunn, S. (2023). Adverse childhood experiences and insecure attachment: The indirect effects of dissociation and emotion regulation difficulties. Psychological Trauma, Advance online publication. [CrossRef]
- Jadva, V., Jones, C., Hall, P., Imrie, S., & Golombok, S. (2023). “I know it’s not normal but it’s normal to me, and that’s all that matters”: experiences of young adults conceived through egg donation, sperm donation, and surrogacy. Human Reproduction, 38(5), 908–916. [CrossRef]
- Riddle, M.P. (2022). The psychological impact of surrogacy on the families of gestational surrogates: implications for clinical practice. Journal of Psychosomatic Obstetrics & Gynecology, 43(2), 122–127. [CrossRef]
- Dumitru, A. E., Gică, C., Iordăchescu, D. A., Panaitescu, A. M., Peltecu, G., Botezatu, R., & Gică, N. (2021). Gestational surrogacy. Medical, psychological and legal aspects. Rjlm.Ro, 29, 323–327. [CrossRef]
- Edelmann, R.J. (2004). Surrogacy: the psychological issues. Journal of Reproductive and Infant Psychology, 22(2), 123–136. [CrossRef]
- Yau, A., Friedlander, R. L., Petrini, A., Holt, M. C., White, D. E., Shin, J., Kalantry, S., & Spandorfer, S. (2021). Medical and mental health implications of gestational surrogacy. American Journal of Obstetrics and Gynecology, 225(3), 264–269. [CrossRef]
- Mamédio, C., Andrucioli de Mattos, C., & Cuce, M. (2007). The PICO strategy for the research question construction and evidence search. Revista Latino-Americana de Enfermagem, 15(3). [CrossRef]
- Page, M. J., McKenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., ... & Moher, D. (2021). The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ, 372.
- Steel, P., Fariborzi, H., & Hendijani, R. (2023). An Application of Modern Literature Review Methodology: Finding Needles in Ever-Growing Haystacks. Sage Research Methods: Business. [CrossRef]
- Orwin, R. G. (1994). Evaluating coding decisions. In H. Cooper & L. V. Hedges (Eds.), The handbook of research synthesis (pp. 139–162). Russell Sage Foundation.
- Hernández-Nieto, R. A. (2002). Contribuciones al análisis estadístico: sensibilidad estabilidad y consistencia de varios coeficientes de variabilidad relativa y el coeficiente de variación proporcional cvp el coeficiente. CreateSpace Independent Publishing Pub.
- Thomas, H. (2003). Quality assessment tool for quantitative studies. Effective Public Health Practice Project. https://www.ephpp.ca/quality-assessment-tool-for-quantitative-studies/.
- Glonti, K., Gordeev, V. S., Goryakin, Y., Reeves, A., Stuckler, D., McKee, M., & Roberts, B. (2015).A Systematic Review on Health Resilience to Economic Crises. PLOS ONE, 10(4), e0123117. [CrossRef]
- *Lamba, N., Jadva, V., Kadam, K., & Golombok, S. (2018). The psychological well-being and prenatal bonding of gestational surrogates. Human Reproduction, 33(4), 646–653. [CrossRef]
- Lorenceau, E. S., Mazzucca, L., Tisseron, S., & Pizitz, T. D. (2015). A cross-cultural study on surrogate mother’s empathy and maternal-foetal attachment. Women and Birth, 28(2), 154–159. [CrossRef]
- *Carone, N., Baiocco, R., Lingiardi, V., & Kerns, K. (2020). Child attachment security in gay father surrogacy families: Parents as safe havens and secure bases during middle childhood. Attachment and Human Development, 22(3), 269–289. [CrossRef]
- *Carone, N., Mirabella, M., Innocenzi, E., Quintigliano, M., Antoniucci, C., Manzi, D., Fortunato, A., Giovanardi, G., Speranza, A. M., & Lingiardi, V. (2023). The intergenerational transmission of attachment during middle childhood in lesbian, gay, and heterosexual parent families through assisted reproduction: The mediating role of reflective functioning. Attachment and Human Development, 1–27. [CrossRef]
- *Carone, N. (2022). Family alliance and intergenerational transmission of coparenting in gay and heterosexual single-father families through surrogacy: associations with child attachment security. International Journal of Environmental Research and Public Health, 19(13). [CrossRef]
- *Carone, N., Barone, L., Manzi, D., Baiocco, R., Lingiardi, V., & Kerns, K. (2020). Children’s exploration of their surrogacy origins in gay two-father families: longitudinal associations with child attachment security and parental scaffolding during discussions about conception. Frontiers in Psychology, 11, 512702. [CrossRef]
- *Carone, N., Manzi, D., Barone, L., Lingiardi, V., Baiocco, R., & Bos, H. M. W. (2021). Father–child bonding and mental health in gay fathers using cross-border surrogacy during the COVID-19 pandemic. BioMedicine Online, 43(4), 756–764. [CrossRef]
- *Carone, N., Manzi, D., Barone, L., Mirabella, M., Speranza, A. M., Baiocco, R., & Lingiardi, V. (2023). Disclosure and child exploration of surrogacy origins in gay father families: Fathers’ Adult Attachment Interview coherence of mind matters.of Reproductive and Infant Psychology, 42(5), 977–992. [CrossRef]
- Kerns, K., Mathews, B. L., Koehn, A. J., Williams, C. T., & Siener-Ciesla, S. (2015). Assessing both safe haven and secure base support in parent-child relationships. Attachment & Human Development, 17(4), 337–353. [CrossRef]
- Calvo, V. (2008). Aspetti di validazione della Security Scale in ambito italiano: Consistenza interna e distribuzione dei punteggi (Manoscritto non pubblicato).Università degli Studi di Padova.
- Marci, T., Lionetti, F., Moscardino, U., Pastore, M., Calvo, V., & Altoé, G.(2018). Measuring attachment security via the Security Scale: Latent structure, invariance across mothers and fathers and convergent validity. European Journal of Developmental Psychology, 15(4), 481–492. [CrossRef]
- Condon, J. T. (1993). T The assessment of antenatal emotional attachment: Development of a questionnaire instrument.British Journal of Medical Psychology, 66(2), 167–183. [CrossRef]
- Della Vedova, A. M., & Burro, R. (2017). Surveying prenatal attachment in fathers: the Italian adaptation of the Paternal Antenatal Attachment Scale (PAAS-IT). Journal of Reproductive and Infant Psychology, 35(5), 493–508. [CrossRef]
- Steele, H., & Steele, M. (2005). The construct of coherence as an indicator of attachment security in middle childhood: The Friends and Family Interview. In Attachment in Middle Childhood (pp. 137–160). Guilford Press.
- Cranley, M. S. (1981). Development of a tool for the measurement of maternal attachment during pregnancy. Nursing Research, 30, 281–284.
- George, C., Kaplan, N., & Main, M. (1985). Adult Attachment Interview protocol (Unpublished manuscript). UC Berkeley.
- Main, M., Goldwyn, R., & Hesse, E. (2002). Adult Attachment Scoring and Classification Systems (Unpublished Manual). UC Berkeley.
- Grabow, A., & Becker-Blease, K. (2023). Acquiring psychopathy and callousness traits: Examining the influence of childhood betrayal trauma and adult dissociative experiences in a community sample. Journal of Trauma & Dissociation, 24(2), 268–283. [CrossRef]
- Yárnoz, S., Alonso-Arbiol, I., Plazaola, M., María, L., & De Murieta, S. (2001). Apego en adultos y percepción de los otros. Anales de Psicología, 17(2), 159–170. [CrossRef]
- Dávila, Y. (2015). La influencia de la familia en el desarrollo del apego. Revista Anales, 57, 121–130. https://publicaciones.ucuenca.edu.ec/ojs/index.php/anales/article/view/792.
- Yılmaz, H., Arslan, C., Arslan, E., Yılmaz, H., Arslan, C., & Arslan, E. (2022). El efecto de las experiencias traumáticas en los estilos de apego. Anales de Psicología, 38(3), 489–498. [CrossRef]
Figure 1.
Flowchart for study selection.
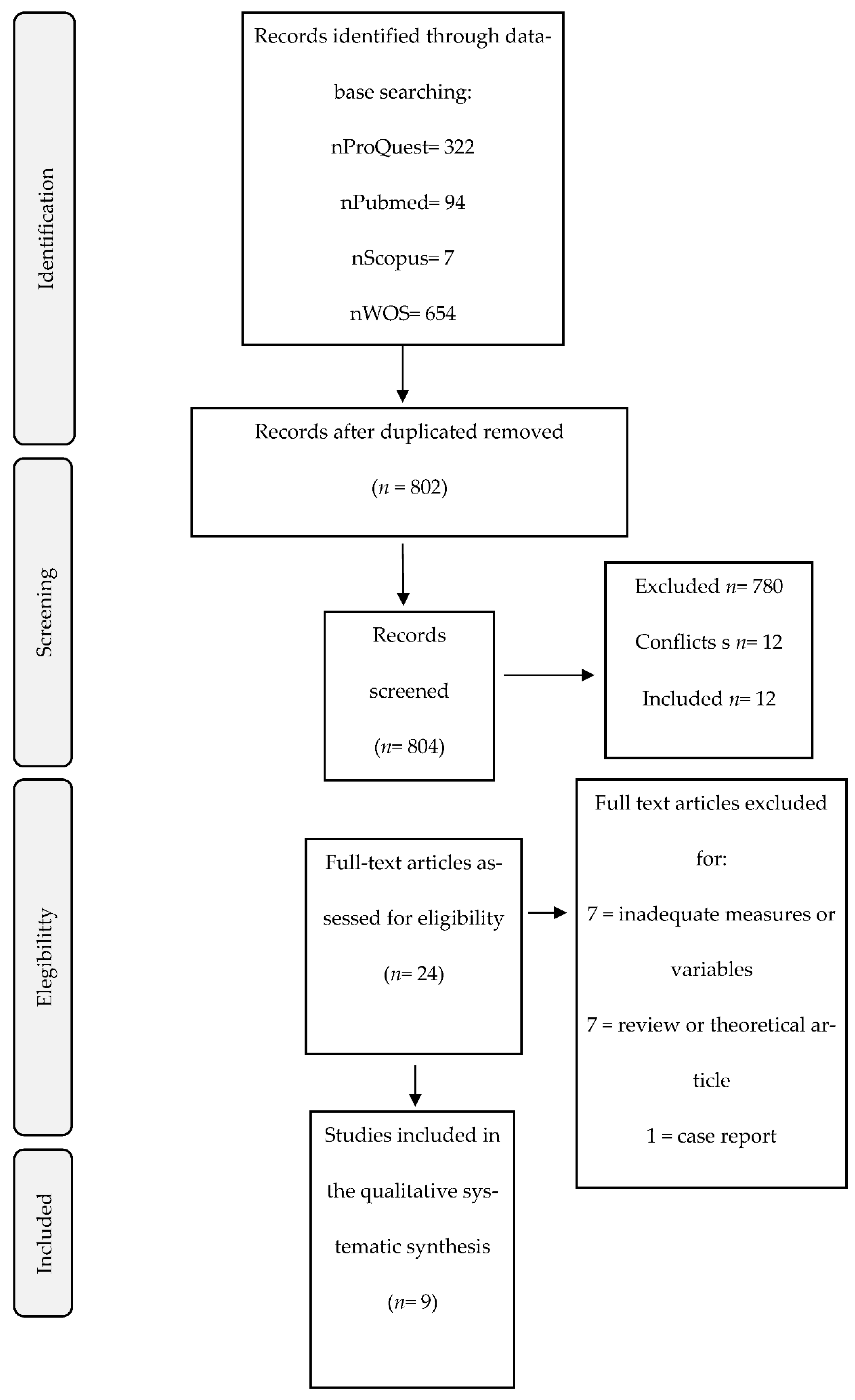

Table 1.
Main Results.
| Author and year | Country and participants | Variables | Design | Main results |
|---|---|---|---|---|
| Fischer & Gillman (1991) |
USA 42 women (21 GS; 21 pregnant but not through GS) |
- Sociodemographic and clinical variables: age, place of birth, marital status, educational level, socioeconomic status, religious affiliation, duration of pregnancy, and average number of children born. - Psychological variables: number of interpersonal resources and perceived support level, maternal-fetal attachment, maternal attitudes, self-perception, and pregnancy-related behavior. |
Observational, descriptive, cross-sectional, comparative. | Non-gestational mothers through surrogacy were more bonded to the unborn baby in: differentiation of the "self" from the fetus (t(40) = 8.14, p < .05), interaction with the baby (t(40) = 6.91, p < .05), and attribution of characteristics and intentions to the baby (t(40) = 2.07, p < .05). Surrogate mothers had more positive attitudes towards body image (t(40) = 2.07, p < .05) and attitudes towards sex (t(40) = 2.82, p < .05). They had more negative attitudes towards pregnancy and the baby (t(40) = 11.58, p < .05). |
| Lorenceau et al. (2015) | France N = 76 (44 GS; 32 mothers but not through GS) |
- Sociodemographic and clinical variables: age, nationality, age at first GS/pregnancy (comparison group), type of GS, number of children by type of GS, number of biological children, number of children by non-gestating parents' sex, desire to repeat GS experience, and previous losses before GS. - Psychological variables: empathy (personal distress, empathic concern, perspective taking, and fantasy scale), emotional state (depression and anxiety), desirability scale (social desirability), and attachment (attachment quality and attachment quantity). |
Observational, cross-sectional. | Anglo-Saxon and European surrogate mothers had lower maternal-fetal attachment (AGEST δ = 0.95) and quality (AGEST δ = 1.52), and less empathy (AGEST δ = 1.04, p < 0.05). The type of surrogacy had effects on the number of gestational or traditional children born (H(2) = 13.833, p < 0.001), as well as on the quality of maternal-fetal attachment. |
| Lamba et al. (2018) | India 119 women (50 GS; 69 pregnant but not through GS) |
- Sociodemographic variables: age, educational level, marital status, number of children, income level, religious affiliation. - Psychological variables: anxiety, depression, stress, emotional and instrumental prenatal bond, GS experiences including concealment, criticism, living situation, perceived support, satisfaction with payment, meeting the newborn, and meeting the intended parents. |
Correlational, longitudinal (T1 between 4-9 months of pregnancy; T2 between 4-6 months after birth). | Surrogate mothers had more depression before (χ²(1) = 12.9, p < 0.001) and after (χ²(1) = 6.12; p = 0.01) childbirth than non-surrogate mothers (p < 0.02), lower maternal-fetal attachment (F(1, 116) = 4.19, p = 0.04) but higher attention and care towards the unborn baby (F(1, 116) = 4.27, p = 0.04). |
| Carone, Baiocco et al. (2020) | Italy 30 children born via GS aged 7 to 13 years and their 66 same-sex parents. |
- Sociodemographic and clinical variables: age, child's sex, number of siblings, parents' ethnicity, family residence, parents' education, parents' occupation, parents' employment status, duration of the couple's relationship, child's age at t1, child's age at t2, parents' age, and annual household income. - Psychological variables: children's attachment and exploration of their surrogacy origins. |
Observational, longitudinal (T1 mean age of children was 8.3 years, T2 was 18 months later). Observational, cross-sectional, non-experimental. | The age of the children, main and interactive effects of parental support, and children's attachment security as predictors explained children's exploration of their origins, with high variance (TCD = 0.34) and low BIC (163.22). Parental scaffolding* and attachment security are interrelated (β = 0.23, p = 0.048) and affect how children explore their origins. Children with greater attachment security reported more exploration of their surrogacy origins (β = 0.30, p = 0.009), but only when there were higher levels of parental scaffolding (β = 0.20, p = 0.072). Along with the child's age factor (β = 0.02, p < 0.001), these predicted greater exploration. |
| Carone, Barone et al. (2020) | Italy 387 children (33 born via GS; 37 children born via insemination; 317 control group) and their families (66 same-sex parents; 74 lesbian parents; 634 heterosexual families). |
-Sociodemographic and clinical variables: child's sex, number of siblings, parents' ethnic background, parents' residence, parents' educational level, parents' occupation, parents' employment status, duration of the couple's relationship, marital status, genetic parenthood, child's age at the visit, parents' age, and household income. - Psychological variables: Identification of children's primary/secondary attachment figures, attachment, support seeking and affiliative proximity seeking, parenting practices and beliefs. |
Observational, cross-sectional. | The security of children's attachment did not differ by family type (gay fathers or lesbian mothers) (F(1,135) = 2.04, p = .16, ηp² = .02, d = .30). Significant associations between attachment security and positive parental control (b = 0.04, t(117) = 1.96, p = .053), parental warmth (b = 0.09, t(99) = 4.69, p < .001), parental responsiveness (b = 0.10, t(130) = 4.43, p < .001), negative parental control (b = -0.08, t(106) = -2.80, p < .01), parental rejection (b = -0.10, t(122) = -3.18, p < .01) and willingness to serve as an attachment figure (b = 0.19, t(127) = 4.97, p < .001). The willingness of parents to serve as an attachment figure and parental behaviors predicted children's attachment security better than family type (b = 0.03, t(66) = 0.74, p = .46). |
| Carone et al. (2021) | Italy 80 same-sex parents with GS children (30 during COVID-19 and 50 before). |
- Sociodemographic and clinical variables: parents' age, gender, sexual orientation, country of residence, annual household income, education and employment, number, gender, age, and conception method of the child(ren), the country where GS took or is taking place and expected birth date of the baby. - Psychological variables: parent-child bond, parents' mental health, social support, and stressful events. |
Observational, cross-sectional. | A lower father-child bond was observed during the COVID-19 pandemic (SE = 15.45, CI 2.5%-97.5% = 10.20, 73.43, p = 0.010), more depression (SE = 5.53, CI 2.5%-97.5% = 4.89, 25.66, p = 0.004), somatization (SE = 6.06, CI 2.5%-97.5% = 4.91, 30.96, p = 0.006) and anxiety (SE = 5.92, CI 2.5%-97.5% = 7.70, 31.10, p = 0.001), than previously. |
| Carone (2022) | Italy 59 single-parent families (31 same-sex and 28 heterosexuals via GS). |
- Sociodemographic and clinical variables: child's gender, number of siblings, family residence, father's ethnic background, father's educational level, father's employment status, father's marital status, non-parental caregivers involved in shared parenting, child's age, father's age, and annual household income. - Psychological variables: coparenting, child attachment. |
Observational, cross-sectional. | There are no significant differences in: co-parenting quality in families of origin between single gay fathers and single heterosexual fathers (F(1,57) = 0.257, p = 0.614, ηp² = 0.004); children's attachment security between children of single gay and heterosexual fathers (F(1,55) = 0.317, p = 0.860, ηp² = 0.001), nor between boys and girls (F(1,55) = 0.586, p = 0.447, ηp² = 0.011); family alliance by family type (Wilks’ λ(16,40) = 0.727, p = 0.536, ηp² = 0.273), nor the child's gender (Wilks’ λ(16,40) = 0.739, p = 0.590, ηp² = 0.261), nor their interaction (Wilks’ λ(16,40) = 0.784, p = 0.787, ηp² = 0.216). Significant relationship between co-parenting quality in the family of origin and children's attachment security, through conflict observed during family interactions (LTP) (estimated point = 0.561, SE = 0.269, 95% CI [0.084, 1.121], p = 0.037). No relationship between co-parenting quality in the family of origin and children's attachment security through support observed during family interactions. |
| Carone, Manzi et al. (2023) | Italy 30 children born via GS and their 60 same-sex parents. |
- Sociodemographic and clinical variables: child's gender assigned at birth, number of siblings, family residence, locations where surrogacy agreements were made, egg donors' identity status at t1, disclosure level at t1, annual household income, duration of the couple's relationship, father's ethnicity, father's education, father's occupation, father's employment status, child's age at t1, child's age at t2, and father's age. - Psychological variables: information about GS, parents' AAI mental coherence, and children's exploration of their surrogacy origins. |
Observational, longitudinal (T1 mean age of 8 years and 3 months (SD = 1.68). T2 mean age of 9 years (SD = 1.69)). | No significant differences were found between boys and girls in the exploration of their surrogacy origins (F(1,28) = 0.308, p = .583, ηp² = 0.011), nor in mind coherence between genetic parents, non-genetic parents, and parents who did not disclose their (non) genetic status (χ²(2) = 0.443, p = .801, ε² = 0.008). The interaction between disclosure and parents' mind coherence at t1 predicted greater exploration in children (β = .296, p = .013). Parents' mind coherence at t1 (β = .220, p = .065), and children's age at t2 (β = .213, p = .096), were not significant. Parents with greater coherence in their interviews (with an AAI range between 1.78 and 6.30) had children who explored their surrogacy origins more deeply. |
| Carone, Mirabella et al. (2023) | 30 lesbian mother dyads via donor insemination, 25 same-sex father dyads via GS, 21 heterosexual father dyads via gamete donation, and 76 children. | - Sociodemographic and clinical variables: child's gender assigned at birth, parents' relationship duration, child's age, number of children, parents' ethnic background, parents' educational level, employment status, parents' age, and net annual income. - Psychological variables: parents' attachment and reflective functioning. Children's attachment and verbal abilities. |
Observational, cross-sectional. | Children of lesbian mothers (β = .46, SE = .34, p = .180), gay fathers (β = -.01, SE = .36, p = .970), and heterosexual parents showed similar levels of attachment security. However, there were no differences based on the parents' gender (β = −.15, SE = .20, p = .450), sexual orientation (β = .22, SE = .26, p = .399), or their interaction (β = −.38, SE = .36, p = .289) in mind coherence. Mothers and fathers showed similar levels of reflective functioning (RF) (β = .19, SE = .17, p = .258). There were no differences in the parents' sexual orientation (β = .43, SE = .21, p = .040), with gay fathers and lesbian mothers showing higher levels of RF than heterosexual parents (main difference = 0.77, SE = 0.27, p = .027). There was a significant interaction between parents' gender and sexual orientation (β = .69, SE = .33, p = .039). There were no differences between family types in the distribution of secure and insecure attachment patterns in children according to the FFI, nor in comparisons with international and national data. There is a significant indirect effect of parents' mind coherence on children's attachment security, mediated by parents' reflective functioning. Parents with greater mind coherence achieved higher levels of RF, and higher RF levels were associated with greater children's attachment security according to the FFI. |
Note: *Parental scaffolding (the parents' efforts to accept, encourage, and emotionally support the expression of children's thoughts and feelings).
Table 2.
Quality Assessment.
| FISRT AUTOR | DESIGN | REPRESENTATIVENESS | REPRESENTATIVENESS II | CONFOUNDING FACTORS | DATA COLLECTION | DATA ANALYSIS | DATA REPORTING | OVERALL RATING |
|---|---|---|---|---|---|---|---|---|
| FISCHER | 4 | 4 | N/A | 2 | 1 | 1 | 1 | Low-moderate |
| LORENCEAO | 4 | 3 | N/A | 2 | 1 | 1 | 1 | Low-moderate |
| LAMBA | 2 | 3 | 2 | 2 | 1 | 1 | 1 | Low-moderate |
| CARONE | 2 | 3 | 2 | 2 | 1 | 1 | 1 | Low-moderate |
| CARONE | 4 | 2 | N/A | 2 | 1 | 1 | 1 | Low-moderate |
| CARONE | 4 | 3 | N/A | 2 | 1 | 1 | 2 | Low-moderate |
| CARONE | 4 | 3 | N/A | 2 | 1 | 1 | 2 | Low-moderate |
| CARONE | 2 | 3 | 2 | 2 | 1 | 1 | 2 | Low-moderate |
| CARONE | 4 | 3 | N/A | 2 | 1 | 1 | 2 | Low-moderate |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



