Submitted:
06 June 2025
Posted:
12 June 2025
You are already at the latest version
Abstract
Background: Cognitive behavioural therapy (CBT) is an evidence-based approach that has been utilised with people living with mild cognitive impairment (MCI) or dementia to improve quality of life and reduce symptomology for a range of concerns such as anxiety, depression, and sleep difficulties. Technology assisted CBT approaches can increase access to mental health support. This systematic review aims to critically synthesise the existing evidence for the barriers and facilitators to the delivery of and engagement with CBT interventions, using both technology and non-technology assisted approaches for people living with MCI or dementia. Methods: PRISMA reporting guidelines and Covidence data extraction were used to structure the review. A systematic search was conducted in multiple databases. We searched for CBT and modified CBT interventions within the last 20 years (2005-2025) targeting people living with MCI or dementia. Studies were restricted to those available in English. We included all empirical research studies that reported any information on barriers and facilitators to the delivery or engagement of CBT interventions for people living with MCI or dementia, such as randomized controlled trials (RCTs), case reports, mixed-methods, and qualitative studies. An inductive thematic analysis using an In-Vivo coding approach and content frequency calculations were used to examine the data. Results: A total of 19 studies were included and 101 factors were extracted. Factors were grouped relating to stages (access, implementation, participation, maintenance), user levels (individual, carers, providers, services, system), and constructs (attitudes, abilities, support, delivery, resources, technology). Common barriers to delivery and engagement included lack of training, lack of time, and technical difficulties with technology. Common facilitators included MCI or dementia specific adaptations to interventions and technology, and being assisted by a support person. Conclusion: The identification of barriers and application of facilitators are integral to the effective delivery of any intervention. The factors identified in this review can provide guidance for both the users and providers of CBT interventions delivered for people living with MCI or dementia. Additionally, these factors can help explain user engagement and delivery outcomes and further inform the design, development, and implementation of future psychotherapy interventions including those assisted with technology.
Keywords:
dementia/MCI
; cognitive behavioural therapy (CBT)
; technology assisted
; barriers
; facilitators
; implementation
; systematic review
1. Introduction
The World Health Organisation reported an estimation of 55 million people worldwide living with dementia, with nearly 10 million new cases each year [1]. Globally, dementia is one of the leading causes of dependency, disability, and death [1,2,3,4]. Dementia is typically diagnosed when the acquired cognitive impairment has become severe enough to compromise social and/or occupational functioning. Impairment may be in memory, intellectual ability, reasoning, social skills, and/or emotional regulation [3]. The diagnosis of mild cognitive impairment (MCI) is typically made when there is modest impairment in one or more of these domains. MCI is classified as a state intermediate between normal cognition and dementia, with essentially preserved functional abilities but representing a decline from a previously higher level [2]. Symptoms of MCI or dementia can include a wide range of physical, cognitive and emotional changes [4]. At any stage, emotional symptoms such as anxiety and depression can exacerbate physical and cognitive symptoms and contribute towards a decline in quality of life [2,4,5].
For people living with MCI or dementia, cognitive behavioural therapy (CBT) has shown evidence of efficacy in reducing the experience of both anxiety and depression, as well as improving quality of life [6,7,8,9]. CBT is a specific therapeutic modality that focusses on the interaction between thoughts, feelings, and behaviours. It utilises a collaborative approach, structured psychoeducational model, active participation, and cognitive and behavioural strategies [6,8,9,10]. However, some components of CBT may be challenging to utilise due to the individual’s level of impairment in cognitive domains such as attention, learning, memory, and executive functioning [6,8,9,10,11]. These challenges often require modifications to be made to the content, structure and techniques in order to shift the focus used in the traditional CBT approach from the cognitive components to the behavioural components of CBT. This has resulted in the emergence of modified-CBT (mCBT) and more relaxation-training based CBT approaches more suited to people living with cognitive impairment [6,7,8,9,12].
The delivery of such interventions can vary widely in terms of location and format. The use of technology in health services has been termed ‘eHealth’, often describing interventions that have been operationalised or modified for delivery through remote means [13]. eHealth interventions can take many forms, such as delivery via telehealth, or internet, and using computers or smart devices [13,14]. The benefits of eHealth include increasing access to physically isolated populations such as rural and remote communities, as well as mobility restricted individuals who may struggle to access traditional services, and specific populations such as adolescents or individuals concerned about stigma who may be reluctant to access in-person services [15,16]. Within the general population, technology-based interventions targeting psychosocial symptoms have been shown to be as equally effective as in-person interventions [16]. For individuals with MCI or dementia, assistive technologies such as telehealth have been found to be helpful in maintaining levels of independence and daily functioning [17]. However, whether technology assisted or not, there remains a significant ‘implementation gap’ with CBT interventions for people living with MCI or dementia [18,19,20,21]. This gap refers to the time between the intervention research and development, to when the intervention can be accessed and utilised by health systems or the public [18,19,20,21].
The need to reduce the gap between intervention inception to implementation has become an area of increased interest not just for researchers but for funding bodies, health systems, and the general public [19]. Despite proven efficacy, there is limited information as to how to ensure that interventions are implemented successfully outside the research context [20]. The evidence indicates that implementation requires more than just knowledge production and dissemination; it is an extensive process requiring human agency, behavioural change, culture change, and organisational change [21]. Successful implementation necessitates a focus on the mechanisms of turning new knowledge into new action; introducing solutions into a health system, understanding processes of implementation, and identifying barriers and facilitators of implementation, as well as factors that promote sustainability [18]. Thus, improving the implementation of CBT interventions for people living with MCI or dementia requires a better understanding of the specific barriers to, and facilitators for, delivery and engagement.
The aim of this systematic review is to critically appraise and synthesise the existing evidence for the barriers and facilitators in delivering CBT interventions to persons living with MCI or dementia. Here we focus on barriers and facilitators to delivery, implementation, and engagement of CBT interventions in persons living with MCI or dementia including interventions assisted with technology.
2. Methods
The systematic review protocol was published on PROSPERO, the International prospective register of systematic reviews as ‘Barriers and Facilitators to the Delivery of CBT Interventions to People Living with Dementia/MCI: Technology Assisted and Non-Technology Assisted Approaches’ (CRD42022378888; PROSPERO, 2023).
2.1. Search Strategy
A literature search following PRISMA guidelines was conducted in multiple databases, including PsycINFO, Scopus, PubMed, Web of Science, EMBASE, COCHRANE, and ProQuest. Based on the inclusion criteria, a search query was developed to include an article if the title or abstract contained at least one keyword related to MCI or dementia, and at least one keyword related to CBT. The search query and search terms for each database can be found in Appendix 1.
2.2. Study Selection
2.2.1. Inclusion and Exclusion Criteria
We included all empirical research studies within the last 20 years (2002-2022) that reported any information on barriers and facilitators to the delivery or engagement of CBT interventions for people living with MCI or dementia, such as randomized controlled trials (RCTs), case reports, mixed-methods, and qualitative studies. We excluded reviews such as umbrella, meta-analysis and systematic reviews, while hand searching the references for further studies. We excluded studies that were not available in English, as well as studies that were unavailable after requests for full texts. Protocols for future studies were also excluded.
The review included men and women over 18 years of age who had been diagnosed with MCI or dementia, dyads with carers or support persons, and CBT or modified CBT interventions targeted for delivery to people living with MCI or dementia. We included community-based delivery methods such as outpatients, community clinics, private clinics, in-home, and remote delivery. We excluded in-patient delivery methods such as hospital patients, aged care facility residents, and residential or communal facility occupants, as these environments carry their own specific barriers and facilitators.
We included studies that reported at least one clinical outcome, including psychosocial and mental health focused such as improvements in quality of life, and reductions in depression or anxiety. We also included studies reporting on physical health outcomes such as improving sleep quality and cognitive abilities. We included studies reporting opinions and experiences of intervention use from both delivery and user perspectives such as usability and satisfaction. We excluded studies that did not provide any data on barriers or facilitators to the delivery or engagement of the associated interventions.
The search results were uploaded to Covidence, a web-based software program for systematic review process management [22]. The use of Covidence allows the bulk importing and exporting of search results, the creation of tailored extraction and quality assessment templates, and the auto-filling of PRISMA flow diagrams [22,23]. Figure 1 shows a PRISMA flow diagram of the full screening process [23]. Titles and abstracts were screened against the inclusion criteria, and excluded articles were labelled with reasons for exclusion. The first and second author reviewed all titles and abstracts. A total of 5606 papers were extracted for the review. After the removal of 2497 duplicates, 3109 article titles and abstracts were screened by the first and second author. Consensus on conflicts and uncertainties about inclusion were resolved by discussion, with review by the third author available if required. Reasons for exclusions were discussed, clarified, and labelled. The same inclusion and exclusion criteria were used for reviewing the titles and abstracts in the screening phase and reviewing the full-text articles in the eligibility phase. A total of 72 full-text articles were assessed for eligibility, of which a final 14 studies met the inclusion criteria. Articles labelled as unavailable were not available in full form freely on the web. Requests for access to unavailable studies were made directly to the correspondence contacts for each study.
2.3. Data Extraction
A data extraction template (Appendix 2) was developed in Covidence for this review and piloted on three full-text papers [22]. The main data elements of interest were barriers and facilitators to delivery or implementation, and user engagement. We extracted the correspondence contact author's details, the year of publication, number of participants, participant characteristics (age, gender, diagnosis), intervention characteristics (CBT type, targeted focus), treatment details (number, frequency, duration of sessions), therapist details (number, role, training), control interventions if applicable (no intervention, care as usual, comparison intervention), completion and drop-out rates and reasons, adverse events, duration of baseline, treatment, and follow-up. We also extracted data on any technology used during the delivery or as part of engagement with the interventions (telehealth, video sessions, computerised programs, the use of devices such as mobiles and tablets, etc). The extracted data can be seen in Appendix 3.
The primary focus of this review was to analyse and identify themes in the literature data, rather than extract the outcomes of quantitative studies. Whilst there is some risk of bias, this review considered all studies that met the inclusion criteria and included a variety of methodologies including qualitative studies with no reported quantitative outcomes. Consequently, the risk of publication bias is reduced compared to an outcome meta-analysis [24]. To account for the methodological variety of studies, a quality assessment template (Appendix 4 was created in Covidence to assess study quality [22]. As per guidelines for excluding inadequately reported studies from qualitative systematic reviews, articles were assessed on four criteria and were considered to be adequately reported if a “yes” was assigned to 2 or more of these criteria: (a) was the study design explained in detail, (b) was the recruitment and selection of participants explained in detail, (c) were details of the data collection method provided, and (d) were details of the analysis method provided [25].
2.4. Data Analysis
An inductive thematic analysis was used to identify common themes among these factors [26]. Thematic analysis focuses on identifying and understanding major themes and their relationships, providing a wide-angle view and allowing the generation of new insights and concepts [27]. This is done by creating codes that represent meanings and patterns in the data [28]. Inductive thematic analysis allows codes to be derived directly from the data rather than researcher-derived interpretations [29].
An In-Vivo coding approach was used, meaning that no pre-existing coding scheme or framework was applied [30]. In-Vivo coding utilises the exact language and terminology of the reported data, which is particularly useful when examining emic perspectives (the direct perspectives of the group being studied) [31]. It should also be noted that the language choice used in the labelling of factors comes directly from the In Vivo coding approach, using language derived directly from statements made by the researchers and participants in the included studies. The authors may not have chosen certain descriptions or specific terms if a different approach was used.
We used a single coder approach, in which the first author identified and refined themes and codes throughout the analysis. This approach has been used in similar qualitative systematic reviews, as when using In-Vivo coding with no a priori codebook, a single coder approach allows for consistency of coding and interpretation of codes [24]. The first author began the analysis by systematically reviewing each included study. For each study, the following sections were analysed; abstract, results or findings, discussion, and conclusions. Individual codes were created each time a factor was described that affected the delivery of or engagement with the interventions. Factors were considered a barrier or facilitator if it was explicitly defined as a barrier or facilitator by the authors of the study, if the description in the study framed it as being a barrier or facilitator, or if the factor was reported as an implementation caution (barrier) or recommendation (facilitator). Once the codes were refined and confirmed, a further content frequency analysis was performed. Content frequency analysis creates quantitative data out of qualitative data by counting the frequency of terms or concepts [32]. This offers a more detailed perspective and enables identification of code hierarchy and priority rankings [33]. Attention must be drawn to the fact that the most frequently occurring factors are not necessarily the most important or influential factors, but rather a higher frequency indicates that more studies have measured and reported on that specific factor. It should be noted that there was a wide variation in the measures used and intervention aspects explored between the research studies included, resulting in an heterogenous data set. A spreadsheet was used to keep track of the metadata and statements (Appendix 4). This contains the raw text of the paper that includes the identified factors which formed the initial codes. Codes that referred to similar concepts were grouped together. As an understanding of the data was developed, codes were revisited and refined. Lastly, the final codes were grouped into specific themes revealed by the data (Appendix 5).
3. Results
All studies were assessed as adequately reported (Appendix 4). Eleven studies provided high level reporting on study design, recruitment and selection, data collection and analysis methods [8,10,11,34,35,36,37,38,39,40,41]. Two studies provided low level reporting on analysis methods [6,42], and one study provided low level reporting on both data collection and analysis methods [43]. No studies were excluded on quality assessment. An overview of the studies included in this review can be seen in Table 1.
Five of the studies were conducted in the United States [6,10,37,38,39], three in the United Kingdom [8,34,36], and two in Canada [11,40], with one study each being conducted in Norway [41], Japan [43], Spain [42], and the Netherlands [35]. Two of the technology assisted studies were conducted in the US [37,38], with one being conducted in the UK [36].
Eleven studies utilised semi-structured qualitative interviews to collect information on the experiences and perspectives of different participants, including the targeted individuals, carers involved, and the therapists delivering the interventions [6,8,10,34,35,36,37,39,40,41,42]. Four studies used a variety of quantitative rating scales to assess the efficacy of the interventions, as well as the usability, feasibility and acceptability from participants engaging in the interventions [6,8,10,41,42]. Three studies combined the data from their qualitative and quantitative measures with background data such as retention and completion rates, log-in records, practice logs, and time spent on practice to assist in the creation of accurate pictures of factors impacting the delivery of or engagement with the interventions [36,37,38].
Although all studies were focussed on CBT interventions for people living with MCI or dementia, some studies targeted a specific condition or experience. One study was not examining a specific intervention but rather exploring the perspectives of mental health therapists on the delivery of any types of CBT interventions for people living with MCI or dementia [34]. As such, this study was excluded from the intervention analysis. An overview of the interventions focus, delivery methods and delivery settings can be seen in Table 2. The number of intervention sessions ranged from 8-18, with the duration of sessions ranging from 30-150 minutes. All interventions were described as ‘modified CBT’, however the specific modifications made differed between each intervention. The types of modifications made were wide ranging, including focussing on different elements of CBT such as mindfulness or sleep hygiene, the types of homework set or practice exercises encouraged, and different changes to resource content and presentation to address the cognitive challenges of MCI or dementia.
A variety of resources, practice supports and technologies were used to assist the delivery of and engagement with the different interventions. The resources provided most often were specific homework tasks. The most frequent practice supports utilised to facilitate engagement with the interventions were reminder cues such as calendars, notes/signs around the house, and scheduled alarms. An overview of the resources provided, practice supports utilised, and technology types can be seen in Table 3.
3.1. Data Synthesis
Using In Vivo coding and thematic analysis, data were grouped into categories, stages, and constructs. Categories refers to the different levels of involvement with the delivery of or engagement with the interventions. The data revealed six levels: 1) the individuals with MCI or dementia, 2) the carers of the individuals with MCI or dementia, 3) the direct deliverers of the intervention, 4) the services providing access to the intervention, 5) the health system, and 6) the societal system. Stages refers to the different time periods involved in completing a therapeutic intervention. The data revealed four stages: 1) gaining access to the intervention, 2) the implementation of the intervention, 3) participating in the intervention, and 4) the maintenance of skills learned in the intervention. Constructs refers to the specific factors that were reported as barriers or facilitators to delivery to or engagement with the interventions. After several iterations of grouping and coding, ten constructs remained: 1) Personal Attitudes, 2) Carer Attitudes, 3) Referrer Attitudes, 4) Service Attitudes, 5) Societal Attitudes, 6) Abilities, 7) Resources, 8) Delivery, 9) Support, and 10) Technology. These 10 constructs contain the specific factors that were found to be barriers and facilitators to the delivery of and engagement with the interventions, found during the different stages across the different levels. A visual depiction of these can be seen in Figure 2. The definition descriptions of each construct at the different levels can be seen in Appendix 5.
A total of 101 detailed factors in the ten specific constructs were identified; 59 barriers and 42 facilitators; 10 during access stage, 18 during implementation stage, 70 during participation stage, 3 during maintenance stage; 61 on the individual level, 12 on the carer level, 15 at the deliverer level, 5 at the service provider level, 4 in the health system and 4 in the wider societal system. The content frequency for all factors was calculated. The full list of factors and their frequencies and can be seen in Appendix 6.
3.1.1. Barriers and Facilitators: Individual Level (Person with MCI / Dementia)
At the Individual level, 28 barriers and 31 facilitators were identified in the stages of Access, Participation, and Maintenance.
Access. The stigma of receiving mental health treatments and denial of the impact of the symptoms of MCI or dementia were identified as barriers.
Participation. ‘Abilities’, specifically difficulties with memory in general was the most common barrier to engaging with interventions, followed by participants being unable to engage with the intervention without the help of others. ‘Personal Attitudes’ such as lack of motivation, apathy, reluctance to engage, and reluctance to accept help were also common barriers to engagement. Identified barriers to engagement under ‘Resources,’ included when the intervention interfered with participants lives or routines, when the intervention was not easy to use, competing demands, and a general lack of time.
‘Delivery’ features and non-specific therapeutic elements, such as providing a sense of hopefulness and optimism, were identified as a facilitator to engagement. The involvement of carers in activities between sessions, such as completing homework exercises or practicing skills, and contact between sessions via telephone, email or texts, were identified as the most common ‘Support’ facilitators. Having a strong commitment to the therapy was identified as the most common facilitator under ‘Personal Attitudes’. Under ‘Resources’, the modification of terms used in therapy to match the individuals educational background and language preferences, as well as the provision of therapy information or session summaries, were the most common facilitators to engagement, followed by the use of retrieval or reminder cues, such as strategically placed signs or cards around the home and the use of calendars or alerts as prompts.
Maintenance. During the Maintenance stage, receiving follow up sessions several months after the intervention program had been completed was identified as the most common ‘Support’ facilitator for maintaining engagement.
3.1.2. Barriers and Facilitators: Carer Level
At the Carer level, 8 barriers and 4 facilitators were identified in the stages of Access, Implementation, Participation, and Maintenance.
Access. ‘Carer Attitudes’ such as lack of interest was identified as a common barrier, referring to both a lack of interest in addressing mental health concerns specifically and a lack of interest in accessing care in general. Providing information on the costs and benefits of engaging with the intervention was identified as a common ‘Resources’ facilitator.
Implementation. Lack of training was identified as an ‘Abilities’ barrier, referring to both a lack of prior education or training in assisting people living with MCI or dementia and a lack of provided training in the intervention being implemented.
Participation. Having a history of marital conflict and experiencing negative interactions with “carees” were identified barriers grouped under ‘Personal Attitudes’. The intervention requirements being or perceived as being burdensome was identified as a ‘Resources’ barrier. Finally, differing reports between dyads was identified as an ‘Abilities’ barrier, referring to Carer aptitude at accurately tracking and recording the usage of different intervention elements or the impacts of the intervention on the person with MCI or dementia.
Facilitators were identified in ‘Resources’ and ‘Support’.
Receiving training or education on dementia in general together with how to effectively communicate and coach people with MCI or dementia was identified as the most common ‘Resources’ facilitator to carer engagement, followed by receiving training or education on managing caregiver stress. Involving multiple carers in the intervention in order to reduce carer burdens such as workload, stress and to reduce conflict between carers and “carees” was identified as a ‘Support’ facilitator to carer engagement.
Maintenance. Common ‘Resources’ barriers to continuing engagement were a lack of time and competing demands.
3.1.3. Barriers and Facilitators: Deliverer Level
At the Deliverer level, 11 barriers and 3 facilitators were identified in the stages of Access, Implementation and Participation.
Access. The prioritisation of physical health was identified as a barrier to delivery, whereas clinicians having a positive attitude towards diagnoses of MCI or dementia was identified as a facilitator; both were grouped under the construct ‘Referrer Attitudes’.
Implementation. Under ‘Resources’, a general lack of time and materials, followed by high volume caseloads and service models were identified as common barriers, whereas receiving training in working with people with MCI or dementia was identified as a common facilitator. Under ‘Delivery’, the scarcity of manualised approaches that also have the flexibility to respond to a wide variety of presentations, the difficulties in making necessary adaptations to approaches to make interventions appropriate for people living with MCI or dementia, and difficulties in integrating carers in sessions were identified as common barriers. Finally, staff lacking training in working with people living with MCI or dementia and staff feeling stretched or burnt-out were common barriers under ‘Abilities’.
Participation. Using interventions with pre-made adaptations specific for people with MCI or dementia was identified as a ‘Resources’ facilitator. Difficulties managing family or dyad relationship issues, difficulties managing family or dyad dynamics, and difficulties focussing on the person with MCI or dementia during the intervention sessions were all identified as ‘Abilities’ barriers.
3.1.4. Barriers and Facilitators: Service Level
At the Service Provider level, only 5 barriers during the Implementation stage were identified. A reticence to invest in MCI or dementia due to recovery funding targets was identified as a ‘Service Attitudes’ barrier. The difficulties in coordinating staff and participant schedules were the most common barrier to implementation, followed by concerns over the potential expense of interventions, inflexible service structures, and the competing demands of other conditions and demographics were common ‘Resources’ barriers. No facilitators for service providers were discussed within the fourteen studies included. Potential facilitating factors for service providers can be extrapolated by inverting the identified barriers at this level.
3.1.5. Barriers and Facilitators: Health System Level
At the Health System level, only factors in the Implementation stage were identified. The most identified barriers to intervention implementation were under ‘Resources’, with limited resources in general followed by an under resourced healthcare system and restrictive healthcare models. The one facilitating factor identified was the growing evidence base on the benefits of mental health focussed CBT interventions for people with MCI or dementia and its influence on government policy decisions, under ‘Societal Attitudes’,
3.1.6. Barriers and Facilitators: Societal System Level
At the Societal System level, 2 barriers during the Implementation stage and 2 facilitators during the Access stage were identified under ‘Societal Attitudes’. Disability discrimination in general and specific fears of dementia were identified as barriers to accessing interventions aimed at treating mental health aspects of MCI or dementia. An increase in societal awareness about MCI or dementia specifically and mental health in general were identified as facilitators to accessing interventions.
3.2. Technology-Assisted Specific Findings
Barriers & Facilitators
In the technology-assisted interventions, 17 specific barriers were identified, only at the Individual level and only during the Participation stage. Factors were coded into the constructs ‘Abilities’, ‘Personal Attitudes’, ‘Resources’, and ‘Technology’. An overview of the factors with their technology-assisted specific frequencies can be seen in Appendix 5. . All technology-assisted interventions experienced technical difficulties with the devices, resulting in increased frustration or anxiety. Technical difficulties with the internet or server connectivity were also experienced in all interventions using the internet, as well as participant withdrawals directly due to these difficulties.
In the technology-assisted interventions, 22 specific facilitators were identified at both the Individual and Deliverer involvement levels, during the Participation stage only. Factors were coded into the constructs ‘Resources’, ‘Delivery’, and ‘Support’. At the Individual level, all technology-assisted interventions found visual aids such as videos, therapy information such as session summaries, and between session contact via emails to be facilitators of participation with the interventions. At the Deliverer level, all technology-assisted interventions found that the MCI or dementia specific adaptations made to the interventions facilitated delivery. All interventions using the internet found the ability to easily monitor participants online engagement with the interventions facilitated delivery of the intervention.
4. Discussion
The data analysis and synthesis revealed several trends in the areas of engagement and delivery, grouped by the four identified stages; access, implementation, participation and maintenance. These identified stages somewhat mirror the stages of implementation; exploration, installation, initial implementation, and full implementation, which are also grouped into similar time-based stages [21]. Grouping trends in engagement and delivery by these similar stages may provide clarity and direction for the application of findings for future interventions. Providing different areas of focus by stage may assist in prioritisation, allocation, and preparation for a variety of potential issues that may arise over time.
Analysis revealed a significant disparity in the number of identifiable factors across the different levels of involvement; individuals, carers, deliverers, service providers, health and societal systems. It became apparent that studies on complex psychosocial interventions tend to focus on the barriers and facilitators primarily at the individual and carer levels. Frequently, limited or no information is provided on the barriers and facilitators experienced at the higher organisational levels, with similar systematic reviews having also found a lack of implementation research concerning organisational and contextual factors, not limited to conditions, populations or settings [9,13,17,18,24,44,45,46,47,48,49,50]. Despite the disparity, this review synthesis was able to extract factors that could have implications across all involvement levels:
- -
- For individuals, these factors could assist in choosing interventions appropriate to their personal attitudes, abilities, and resources.
- -
- For carers, these factors could assist in choosing interventions appropriate for the person they are assisting, as well as interventions that they themselves have the time, energy, and resources for.
- -
- For referrers and providers, these factors could guide the selection of client-appropriate interventions, increase awareness of skills and techniques required for effective delivery, and provide guidance on increasing client engagement.
- -
- For mental health services, these factors could be used when selecting interventions to procure and implement into different practices and settings, as well as provide guidance on the most effective training for staff for successful implementation and delivery.
- -
- For the designers and developers of interventions, these factors can be applied to tailor interventions to the needs of the target audience, in order to increase usability, uptake, user satisfaction, and increase intervention effectivity and engagement.
- -
- For researchers, these factors can be used to understand what might be important to measure, and to develop or include specific evaluation measures in future studies.
4.1. Access Stage
The primary trend in the areas of engagement and delivery during the Access stage emerged as attitudes, with several barriers and facilitators identified at the individual, carer, deliverer, and societal system levels. At all four of these levels, attitudes towards the diagnoses and impacts of MCI or dementia, and towards mental health in general were the most common influence on accessing interventions. Negative attitudes emerged as barriers and positive attitudes emerged as facilitators. Similar trends have also emerged in previous studies and do not appear to be specific to the MCI or dementia populations, with a systematic review on user adherence with mCBT therapy for chronic health conditions finding that attitudinal factors such as motivation to be prevalent barriers to engagement with an intervention [48]. A systematic review on CBT interventions for youth anxiety also found that low client motivation affected user engagement, with high client motivation emerging as a significant facilitator [51].
The secondary trend in the areas of engagement and delivery during the Access stage emerged as resources, with concerns about limited time, means and materials being a common barrier. However, at the level of carer access, providing information on the costs and benefits of engaging with the intervention emerged as a facilitator. Similar findings have emerged in previous reviews, with the ability of services to meet cost, time and provider needs, sufficient resources and openness to change found to be facilitators for access at the service level [13,47].
At the carer and deliverer levels, the level of interest and awareness of interventions for MCI or dementia and of mental health interventions in general was also a common influence on accessing interventions. It was also found that perception of the intervention or perceived credibility were prevalent factors in participants choosing to engage with an intervention. Caregivers’ attitudes towards interventions have previously been found as a significant factor, with perceptions of burden, negative feeling towards technology, and concerns about privacy being common access barriers and perceived content credibility, relevance and usefulness being common access facilitators [13,45,48]. Positive prior experiences with mental health services and mental health technology have also been found to facilitate people’s intention to use interventions, as well as actual engagement [45].
These trends suggest that providing the cost benefit analysis information for an intervention may be a significant facilitating factor that could be applied across all levels to address both the primary and secondary trends identified during the access level. Being able to provide comprehensible, useful, and specific information for an intervention may prove to be an effective strategy to assist with the challenging task of changing the attitudes and behaviours of people at any level of involvement. Developing a good understanding of the intervention and its value among those receiving the intervention has already proved to be a significant facilitator for similar complex psychological telehealth interventions in general populations [52].
4.2. Implementation Stage
During the Implementation stage, the primary trend in the area of delivery emerged as attitudes, with several barriers and facilitators identified at the service, health, and societal system levels. Reticence to invest in interventions due to competing demands and concerns over the potential expense of interventions were the most common barriers. A growing evidence base on the benefits of mental health interventions and the resulting influence on health policy and provider decisions was identified as a facilitator. Concerns about resources and practical factors such as time and cost are one of the most prevalent barriers found in intervention implementation, not limited to the MCI or dementia population [13,45,47,48,51]. The limited capability of health insurance authorities to support innovative interventions and their preference for classically delivered care has also been described as a specific barrier at the provider and health system levels [13]. Once again, these trends suggest that providing the cost benefit analysis information for an intervention may be a facilitating factor that could be applied across all levels as a strategy to assist changing the attitudes and behaviours of people at any level of involvement during the implementation level.
The secondary trend in the areas delivery during the Implementation stage emerged as training. At the carer and deliverer level, a lack of training in the specific intervention, as well as in MCI or dementia in general, were the most common barriers. Carer’s abilities such as digital and health literacy were also found to be significant barriers in a similar review, while receiving training in specific areas such as communicating with people living with MCI or dementia and managing carer stress emerged as a facilitator in this area [13]. For deliverers, a lack of training in the specific areas of managing dyad dynamics within sessions and managing family issues were common barriers. Staff receiving intervention training was also found to be a facilitator at the deliverer level in a similar review [13]. This suggests that providing clear and relevant training in both the particular intervention and in specific areas of concern at the different levels of involvement may be a significant and effective facilitator of successful intervention delivery.
4.3. Participation Stage
During the Participation stage, the primary trends in engagement and delivery emerged as resources and abilities. At the individual level, a wide range of intervention elements tailored towards people living with MCI or dementia were identified as facilitators to engagement, often targeting common engagement barriers found at the individual level. Barriers such as memory difficulties and being unable to engage with the intervention without help were offset by facilitators such as having concrete practice plans and regular practice time, carer involvement in practices, using a variety of reminder cues, and receiving contact between intervention sessions. This does not appear to be specific to the MCI or dementia population, with reviews on chronic health and youth populations also finding participant characteristics such as abilities and health impacts to be prevalent factors impacting engagement with interventions, and clients having a certain level of cognitive functioning to be an important facilitator at the individual level [48,51].
At the carer level, barriers such as the intervention requirements being perceived as burdensome and concerns about capabilities in supporting people living with MCI or dementia were offset by facilitators such as receiving relevant training and involving multiple carers in the intervention. The type and quality of the carer or support person relationship with the person living with dementia also emerged as an influential factor, with a similar review also finding this to be important [13].
At the deliverer level, being able to access and use interventions with pre-made adaptations and inclusions tailored towards people living with MCI or dementia was a common delivery facilitator. This appears to be the counterpart to a previous review finding that when providers have to prepare materials in advance, this becomes a barrier to implementing interventions [51]. Deliverer concerns around the requirements of interventions are common and not limited to the dementia/MCI population, with multiple reviews finding high caseloads, high staff turnover and time pressure to be primary deliverer barriers [13,20,45].
The secondary trend in engagement and delivery during the Participation stage emerged as attitudes. At the individual level, a reluctance to engage and a reluctance to accept help were the most common barriers to engagement. At the carer level, having a positive relationship with the person with MCI or dementia emerged as a facilitator that appears to reduce the impact of these barriers. At the deliverer level, being able to provide optimism and hopefulness also emerged as a facilitator that appears to reduce the impact of these barriers. The influence of these facilitators was strengthened when the facilitators of receiving relevant training at the carer and deliverer levels were also present, previously mentioned above as a factor found in similar review [13].
These trends suggest that providing clear and relevant training in both the particular intervention and in the specific areas of concern at the different levels may not only be an effective facilitator of successful intervention delivery at the Implementation stage but may also be an effective facilitator for successful delivery and for successful engagement during the Participation stage as well. Maximising engagement from key stakeholders has also been to be a facilitator for similar complex psychological telehealth interventions in general populations [52]. It has been recommended that interventions strong need provider collaboration for successful implementation [13].
4.4. Maintenance Stage
As seen in the results and the synthesis, very little information on barriers and facilitators during the Maintenance stage was captured in the data. This may be due to the fact that most of the included studies were discussing research interventions, which are usually delivered over a brief period of time, often focussing on short-term effects and proving the efficacy of the intervention [53,54]. Research intervention materials are not necessarily available for participants in the long-term, and the therapeutic relationship with the therapist delivering the materials is rarely sustained [53,54]. However, many reviews have also reported a dearth of information on intervention maintenance and wider contexts such as health and social systems [9,13,17,18,24,44,45,46,47,48,49,50]. From the factors that were identified during this stage, primary trends in the area of engagement emerged as resources and support. On the individual level, continuing engagement with the intervention materials and follow up sessions to reinforce skills learned were the most common facilitators to maintaining engagement. On the carer level, a lack of time, means and materials were the most common barriers to maintaining engagement.
This suggests that including follow-up sessions as part of intervention structures, as well as providing permanent access to the intervention materials, may be effective strategies for facilitating successful delivery and maintaining successful engagement. It also suggests that interventions may need to be time efficient and low-cost or public access in order for engagement to be easily maintained amidst competing demands and limited resources.
4.5. Technology Assisted Specific Trends
4.5.1. Accessibility
The primary trend with technology assisted interventions emerged as accessibility. All technology assisted interventions in this review experienced barriers to delivery and engagement due to technical difficulties with the technology. This was also found in similar technology focussed reviews, with common barriers including accessibility issues, time-consuming processes to log in to an intervention, and difficulty navigating and finding information within an intervention [13,45,46,49]. It has also previously been reported that eHealth users stressed the importance of reducing the amount, spread and complexity of information, adding that complexity is associated with increased security risks [13,45,49]. A common barrier with intervention technology is users’ experience of technical issues, with these difficulties resulting in the exacerbation of symptoms such as anxiety, negatively impacting engagement and often resulting in participant withdrawal [13,45,48]. Providing assistance in setting up the technology, providing instructions or training in using the technology, and providing easily contactable technological support throughout the intervention emerged as common facilitators to delivery and engagement, also found in a similar review [48,49]. Further facilitators to engagement included a range of technology specific adaptations tailored towards people living with MCI or dementia, such as older adult appropriate device settings for dexterity and vision impairments. Several studies made accessibility adaptations in an attempt to address memory specific barriers to engagement such as forgetting log-in details and forgetting passwords. These adaptations included getting participants to store hardcopy log-in details near the technology device, reducing password requirements, increasing log-in time periods, or removing log in requirements altogether. However, these adaptations all reduce the security of the technology being used, particularly internet-based technologies. Data security is a major modern concern, influencing engagement and delivery at all levels of involvement. An effective balance between accessibility and security, particularly for wireless networks, may not be possible without secure, uniform standards incorporated into hardware and operating systems [55]. Previous reviews found that providing information and assurances that the digital platform was private and participants’ information could not be easily accessed by third parties was a facilitator to user engagement [45,46,49].
4.5.2. Connectivity
The secondary trend with technology assisted interventions emerged as connectivity. All internet-based technology assisted interventions in this review experienced barriers to delivery and engagement due to problems with connectivity. These problems included issues with connecting to the internet and the strength of the internet connection, which negatively impacted session delivery and participant engagement with the intervention materials. Facilitators such as providing assistance in setting up technology, providing instructions or training in using the technology, and providing easily contactable technology support throughout appear to be essential inclusions for technology assisted interventions to improve ease of delivery and to reduce participant distress and disengagement. These factors mirror those found in similar reviews, as mentioned above [13,44,45,46,48,49]. Delivery of and engagement with technology assisted interventions may also be facilitated by ensuring that intervention materials are available in an offline mode, such as a self-contained device or application, and providing intervention materials in multiple formats such as printed manuals and worksheets.
4.6. Limitations
In this systematic review, we took a wide-angle view of the barriers and facilitators that influence the delivery of and engagement with CBT interventions for people living with MCI or dementia. We did not focus on a single type of research methodology, intervention target or use of technology. In addition, there was inconsistency across the studies in measures used to assess delivery fidelity and user engagement, such as automatically recorded user data (number of logins, time spent records etc.) compared to self-reported measures (self-ratings, practice logs etc.). These variations and inconsistencies resulted in uneven information across areas of implementation and has also been found to be an issue in previous reviews [9,13,17,18,24,44,45,46,47,48,49,50]. This highlights the importance of further implementation research, as well as the use of theory-based frameworks and systematic evaluations alongside intervention implementation.
Finally, this review excluded 20 protocol papers for appropriate studies, most of which are technology assisted interventions. A future review could be conducted to include the data from the completed studies and compare with or add to the information in this review to deepen the understanding of the barriers and facilitators to delivery of and engagement with CBT interventions for people living with MCI or dementia.
7. Conclusions
There is evidence showing that CBT interventions can be effective interventions for people living with MCI or dementia, using both technology and non-technology approaches. In order for these interventions to be successful, specific factors influencing the delivery of and engagement with these interventions need to be addressed. In this systematic review, we identified 101 specific factors grouped into 10 constructs, in 5 levels of involvement across 4 time stages. By understanding the specific factors, barriers to delivery and engagement can be addressed and facilitators applied to increase intervention success. These findings can also be used as guidelines for the successful development, selection, implementation, and evaluation of future CBT interventions for people living with MCI or dementia. These findings also highlight the scarcity of practical implementation information, with organisational, contextual, and societal factors largely neglected in intervention research.
Author Contributions
The first author (Kimberley Welsh) formulated the concept of this study together with supervisors A/Prof Nadeeka Dissanayaka, and Dr Deborah Brooks. Dr Deborah Brooks is also the second reviewer of articles chosen. All co-authors critically revised drafts of the manuscript. We have no conflicts of interest to disclose. The funding source for this review is Kimberley Welsh’s PhD earmarked scholarship offered for the Medical Research Future Fund (MRFF) Dementia, Ageing and Aged Care targeted call grant. A/Prof Nadeeka Dissanayaka is supported by the NHMRC Boosting Dementia Research Leadership Fellowship. Correspondence concerning this review should be addressed to A/Prof Nadeeka Dissanayaka.
Abbreviations
| Cognitive behavioural therapy | (CBT) |
| Modified CBT | (mCBT) |
| Mild cognitive impairment | (MCI) |
| Randomized controlled trials | (RCT) |
Appendices
Multimedia Appendices
Appendix 1. Search Query and Search Terms for Databases (PDF)
Appendix 2. Data Extraction Template (PDF)
Appendix 3. Data Extraction & Quality Assessment Metadata (XLSX)
Appendix 4. Data Quality Assessment Template (PDF)
Appendix 5. Construct Definition Descriptions (PDF)
Appendix 6. Overview of Barriers and Facilitators by Theme (XLSX)
References
- World Health Organisation. Dementia. Global action plan on the public health response to dementia 2017 – 2025. Updated 2023. Accessed June 2023. https://www.who.int/news-room/fact-sheets/detail/dementia#:~:text=Key%20facts,nearly%2010%20million%20new%20cases.
- Hugo J, & Ganguli M. Dementia and cognitive impairment: epidemiology, diagnosis, and treatment. Clinics in geriatric medicine, 2014, 30(3), 421–442. [CrossRef]
- Sousa S, Teixeira L, Paul C. Assessment of Major Neurocognitive Disorders in Primary Health Care: Predictors of Individual Risk Factors. Front. Psychol., Neuropsychology, 2020, 11(1). [CrossRef]
- UNC School of Medicine. Dementia: Identifying Mild, Moderate, and Severe. Depart of Neurology, UNC School Of Medicine. 2023. Accessed June 2023. https://www.med.unc.edu/neurology/divisions/memory-and-cognitive-disorders-1/family-concerns-1/normal-aging-mild-cognitive-impairment-and-dementia/.
- Alzheimer’s Society. The progression, signs and stages of dementia. Updated January 2024, Accessed June 2023. https://www.alzheimers.org.uk/about-dementia/symptoms-and-diagnosis/how-dementia-progresses/progression-stages-dementia.
- Kraus CA, Seignourel P, Balasubramanyam V, Snow AL, Wilson NL, Kunik ME, Schulz PE, & Stanley MA. Cognitive-behavioral treatment for anxiety in patients with dementia: two case studies. Journal of psychiatric practice, 2008, 14(3), 186–192. [CrossRef]
- Paukert AL, Kraus-Schuman C, Wilson N, Snow AL, Calleo J, Kunik ME, Stanley MA. The Peaceful Mind manual: a protocol for treating anxiety in persons with dementia. Behav Modif, 2013, 37(5), 631-664. [CrossRef]
- Tay KW, Subramaniam P, & Oei TP. Cognitive behavioural therapy can be effective in treating anxiety and depression in persons with dementia: a systematic review. Psychogeriatrics, 2019. 19(3), 264-275. [CrossRef]
- Tay KW, Subramaniam P, & Oei TP. Cognitive behavioural therapy can be effective in treating anxiety and depression in persons with dementia: a systematic review. Psychogeriatrics, 2019. 19(3), 264-275. [CrossRef]
- Stanley MA, Calleo J, Bush AL, Wilson N, Snow AL, Kraus-Schuman C, Paukert AL, Petersen NJ, Brenes GA, Schulz PE, Williams SP, Kunik ME. The peaceful mind program: a pilot test of a cognitive-behavioral therapy-based intervention for anxious patients with dementia. Am J Geriatr Psychiatry. 2013. 21(7):696-708. [CrossRef]
- Ozen LJ, Dubois S, English MM, Gibbons C, Maxwell H, Lowey J, Sawula E, Bédard M. The efficacy of mindfulness-based cognitive therapy to improve depression symptoms and quality of life in individuals with memory difficulties and caregivers: A short report. Alzheimers Dement. 2022, 8(1):12252. [CrossRef]
- McClive-Reed KP, Gellis, ZD. Anxiety and related symptoms in older persons with dementia: directions for practice. J Gerontol Social Work, 2011, 54(1), 6-28. [CrossRef]
- Christie HL, Bartels SL, Boots LM, Tange HJ, Verhey FR, & de Vugt ME. A systematic review on the implementation of eHealth interventions for informal caregivers of people with dementia. Internet interventions, 2018, 13, 51-59.
- Wade VA, Karnon J, Elshaug AG, Hiller J. A systematic review of economic analyses of telehealth services using real time video communication. BMC Health Services. Research. 2010, 10(1). [CrossRef]
- Topo P. Technology Studies to Meet the Needs of People With Dementia and Their Caregivers A Literature Review. Helsinki Journal of Applied Gerontology, 2009, 28(1): 5-37. [CrossRef]
- Park MJ, Kim DJ, Lee U, Na EJ, Jeon HJ. A Literature Overview of Virtual Reality (VR) in Treatment of Psychiatric Disorders: Recent Advances and Limitations. Front Psychiatry, 2019, 10(505). [CrossRef]
- Braun A, Trivedi DP, Dickinson A, Hamilton L, Goodman C, Gage H, Manthorpe J. Managing behavioural and psychological symptoms in community dwelling older people with dementia: A systematic review of qualitative studies. Dementia. 2019, 18(7-8), 2950-2970. [CrossRef]
- Cowie J, Nicoll A, Dimova ED. The barriers and facilitators influencing the sustainability of hospital-based interventions: a systematic review. BMC Health Serv Res 2020, 588. [CrossRef]
- Glasgow RE, Lichtenstein E, Marcus AC. Why don't we see more translation of health promotion research to practice? Rethinking the efficacy-to-effectiveness transition. Am J Public Health. 2003, 93(8):1261-7. [CrossRef]
- Graham ID, Kothari A, McCutcheon C. (2018) Moving knowledge into action for more effective practice, programmes and policy: protocol for a research programme on integrated knowledge translation. Implementation Science. 13. [CrossRef]
- Titler MG. The Evidence for Evidence-Based Practice Implementation. Agency for Healthcare Research and Quality (US); 2008, Chapter 7. https://www.ncbi.nlm.nih.gov/books/NBK2659/.
- Covidence. Covidence Systematic Review Management. Melbourne, VIC. 2023. Accessed June 2023. https://www.covidence.org/.
- PRISMA. (2023). Prisma Flow Diagram. Transparent Reporting of Systematic Reviews and Meta-Analyses. Accessed June 2023.
- Lienemann BA, Unger, JB, Cruz TB, Chu K. Methods for Coding Tobacco-Related Twitter Data: A Systematic Review. Journal of Medical Internet Research, 2017, 19(3). [CrossRef]
- Carroll C, Booth A, Lloyd-Jones M. Should We Exclude Inadequately Reported Studies From Qualitative Systematic Reviews? An Evaluation of Sensitivity Analyses in Two Case Study Reviews. Qualitative Health Research Internet, 2012, 22(10), 1425-1434. [CrossRef]
- Luckman, S.(ed). Virginia Braun and Victoria Clarke, Successful qualitative research: A practical guide for beginners. Feminism & Psychology, 2016, 26(3), 387-391. [CrossRef]
- Delve HL, & Limpaecher A. How to Do Thematic Analysis. 2020. Essential Guide to Coding Qualitative Data. https://delvetool.com/blog/thematicanalysis.
- Gibbs GR. Coding part 2: Thematic coding. 2010. Accessed June 2023. http://www.youtube.com/watch?v=B_YXR9kp1_o.
- Guest G, MacQueen K, & Namey E. Applied Thematic Analysis. Thousand Oaks, CA: SAGE Publications.; 2011.
- Given L. The Sage Encyclopedia of Qualitative Research Methods. 2008. Swinburne University, Charles Sturt University, Australia: SAGE Publications. Accessed June 2023. https://repository.bbg.ac.id/bitstream/515/1/The_Sage_Encyclopedia_of_Qualitative_Research_Methods.pdf.
- Manning J. In Vivo Coding. The International Encyclopedia of Communication Research Methods. 2017. [CrossRef]
- Dicle MF, & Dicle B. Content Analysis: Frequency Distribution of Words. The Stata Journal, 2018, 18(2), 379-386. [CrossRef]
- Saldana, J. (2009). The Coding Manual for Qualitative Researchers. Thousand Oaks, California: SAGE Publications. Accessed in June 2023https://emotrab.ufba.br/wp-content/uploads/2020/09/Saldana-2013-TheCodingManualforQualitativeResearchers.pdf.
- Baker S, Brede J, Cooper R, Charlesworth G, Stott J. Barriers and facilitators to providing CBT for people living with dementia: Perceptions of psychological therapists. Clin Psychol Psychother. 2022,29(3):950-961. [CrossRef]
- Berk L, Warmenhoven F, Stiekema APM, van Oorsouw K, van Os J, de Vugt M, van Boxtel M. Mindfulness-Based Intervention for People With Dementia and Their Partners: Results of a Mixed-Methods Study. Front Aging Neurosci. 2019, 11:92. [CrossRef] [PubMed] [PubMed Central]
- Douglas S, Stott J, Spector A, Brede J, Hanratty É, Charlesworth G, Noone D, Payne J, Patel M, Aguirre E. Mindfulness-based cognitive therapy for depression in people with dementia: A qualitative study on participant, carer and facilitator experiences. Dementia (London). 2022, 21(2):457-476. [CrossRef]
- Mattos MK, Manning CA, Quigg M, Davis EM, Barnes L, Sollinger A, Eckstein M, Ritterband LM. Feasibility and Preliminary Efficacy of an Internet-Delivered Intervention for Insomnia in Individuals with Mild Cognitive Impairment. J Alzheimers Dis. 2021;84(4):1539-1550. [CrossRef]
- McPhillips MV, Li J, Petrovsky DV, Brewster GS, Ward EJ 3rd, Hodgson N, Gooneratne NS. Assisted Relaxation Therapy for Insomnia in Older Adults With Mild Cognitive Impairment: A Pilot Study. Int J Aging Hum Dev. 2023, 97(1):65-80. [CrossRef]
- Robinson CM, Paukert A, Kraus-Schuman CA, Snow AL, Kunik ME, Wilson NL, Teri L, Stanley MA. The involvement of multiple caregivers in cognitive-behavior therapy for anxiety in persons with dementia. Aging & Mental Health, 2011 15:3, 291-298. [CrossRef]
- Staubo H, Misvaer N, Tonga JB, Kvigne K, Ulstein I. People with dementia may benefit from adapted cognitive behavioural therapy. Sykepleien Forskning 2017, 12(63874). [CrossRef]
- Tonga JB, Karlsoeen BB, Arnevik EA, Werheid K, Korsnes MS, Ulstein ID. Challenges With Manual-Based Multimodal Psychotherapy for People With Alzheimer's Disease: A Case Study. Am J Alzheimers Dis Other Demen. 2016 (4):311-7. [CrossRef]
- García-Alberca JM. Cognitive-behavioral treatment for depressed patients with Alzheimer’s disease. An open trial. Archives of Gerontology and Geriatrics, 2021, 71:1-8. [CrossRef]
- Kashimura M, Nomura T, Ishiwata A, Kitamura S, and Tateno A. Cognitive Behavioral Therapy for Improving Mood in an Older Adult with Mild Cognitive Impairment: A Case Report. J Nippon Med Sch, 2019,86(6). [CrossRef]
- Bauernschmidt D, Wittmann J, Hirt J, Meyer G, Bieber A. The Implementation Success of Technology-Based Counseling in Dementia Care: Scoping Review. JMIR Aging. 2024,7:515-44. [CrossRef]
- Borghouts J, Eikey E, Mark G, De Leon C, Schueller SM, Schneider M, Stadnick N, Zheng K, Mukamel D, Sorkin DH. Barriers to and Facilitators of User Engagement With Digital Mental Health Interventions: Systematic Review. J Med Internet Res. 2021, 23(3):24387. [CrossRef] [PubMed] [PubMed Central]
- Fleming T, Bavin L, Lucassen M, Stasiak K, Hopkins S, & Merry S. Beyond the Trial: Systematic Review of Real-WorldUptake and Engagement With Digital Self-Help Interventions for Depression, Low Mood, or Anxiety. Journal of Medical Internet Research, 2018, 20(6), 199. [CrossRef]
- Groot Kormelinck CM, Janus SIM, Smalbrugge M, Gerritsen DL, Zuidema SU. Systematic review on barriers and facilitators of complex interventions for residents with dementia in long-term care. Int Psychogeriatr. 2021 Sep;33(9):873-889. [CrossRef]
- Marks E, Moghaddam N, De Boos D, Malins, S. A systematic review of the barriers and facilitators to adherence to mindfulness-based cognitive therapy for those with chronic conditions. British Journal of Health Psychology, 2022, 28(2):338-365. [CrossRef]
- Ng MM, Firth J, Minen, M., & Torous, J. (2019). User Engagement in Mental Health Apps: A Review of Measurement, Reporting, and Validity. Psychiatric Services, 70(7), 538-544. [CrossRef]
- Orgeta V, Qazi A, Spector A, Orrell M. Psychological treatments for depression and anxiety in dementia and mild cognitive impairment: systematic review and meta-analysis. Br J Psychiatry, 2015 207(4), 293-298. [CrossRef]
- Ringle VA, Read KL, Edmunds JM, Brodman DM, Kendall PC, Barg F, Beidas RS. Barriers to and Facilitators in the Implementation of Cognitive-Behavioral Therapy for Youth Anxiety in the Community. Psychiatr Serv. 2015, 66(9):938-45. [CrossRef]
- Faija CL, Connell J, Gellatly J, Rushton K, Lovell K, Brooks H, Armitage C, Bower P, & Bee P. Enhancing the quality of psychological interventions delivered by telephone in mental health services: increasing the likelihood of successful implementation using a theory of change. BMC Psychiatry, 2023, 23(1):405. [CrossRef]
- Gitlin LN. Introducing a new intervention: an overview of research phases and common challenges. American Journal of Occupational Therapy, 2013, 67(2):177-84. [CrossRef]
- Marchand E, Stice E, Rohde P, Becker CB. Moving from efficacy to effectiveness trials in prevention research. Behav Res Ther, 2011, 49(1):32-41. [CrossRef]
- XaCroix C. Security vs Access. Classroom, EdTech. Updated 2006. Accessed June 2023. https://edtechmagazine.com/k12/article/2006/10/security-vs-acces.
Figure 1.
PRISMA Flow Diagram of Screening Process.
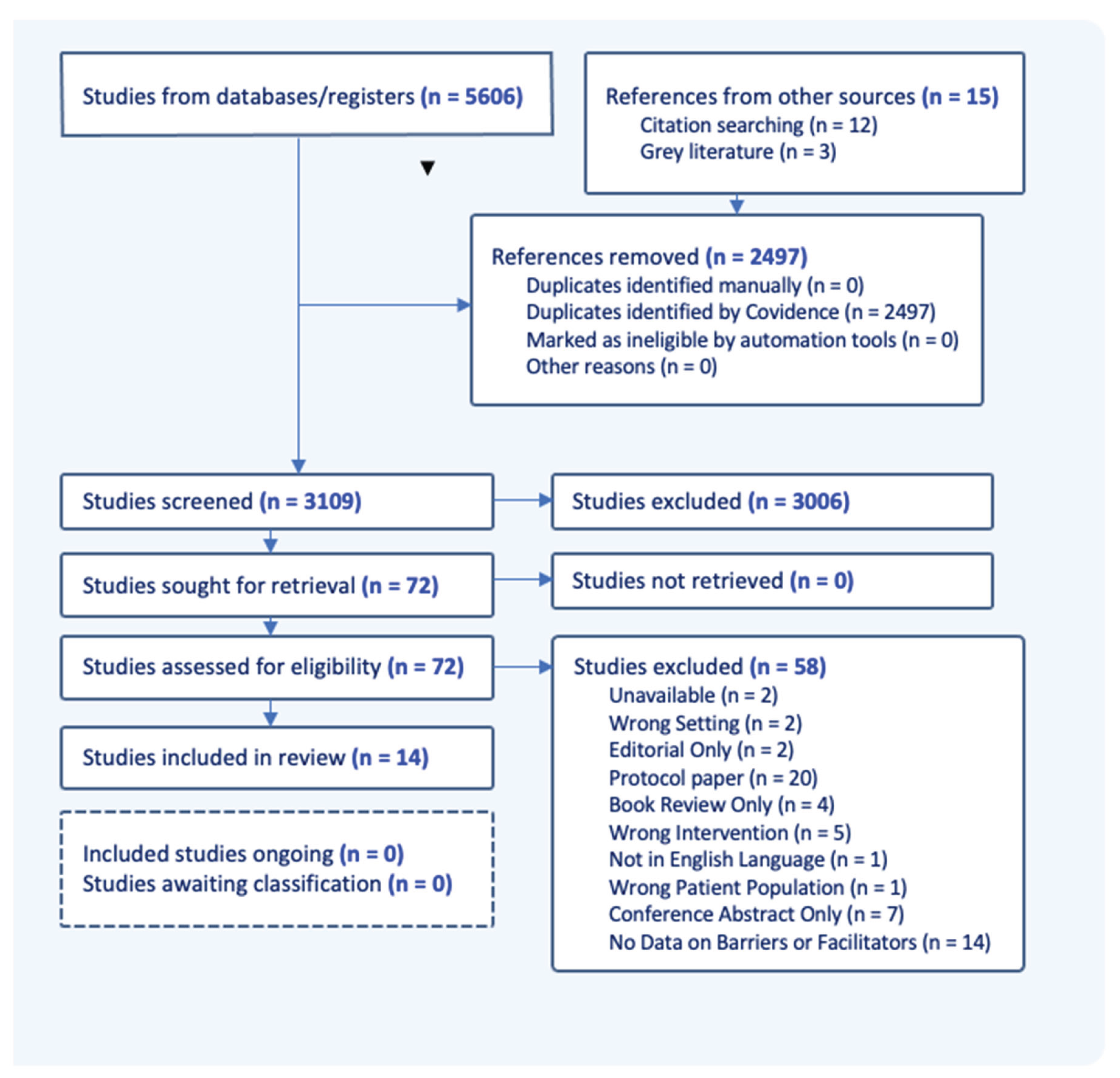
Figure 2.
Theme Grouping Overview.
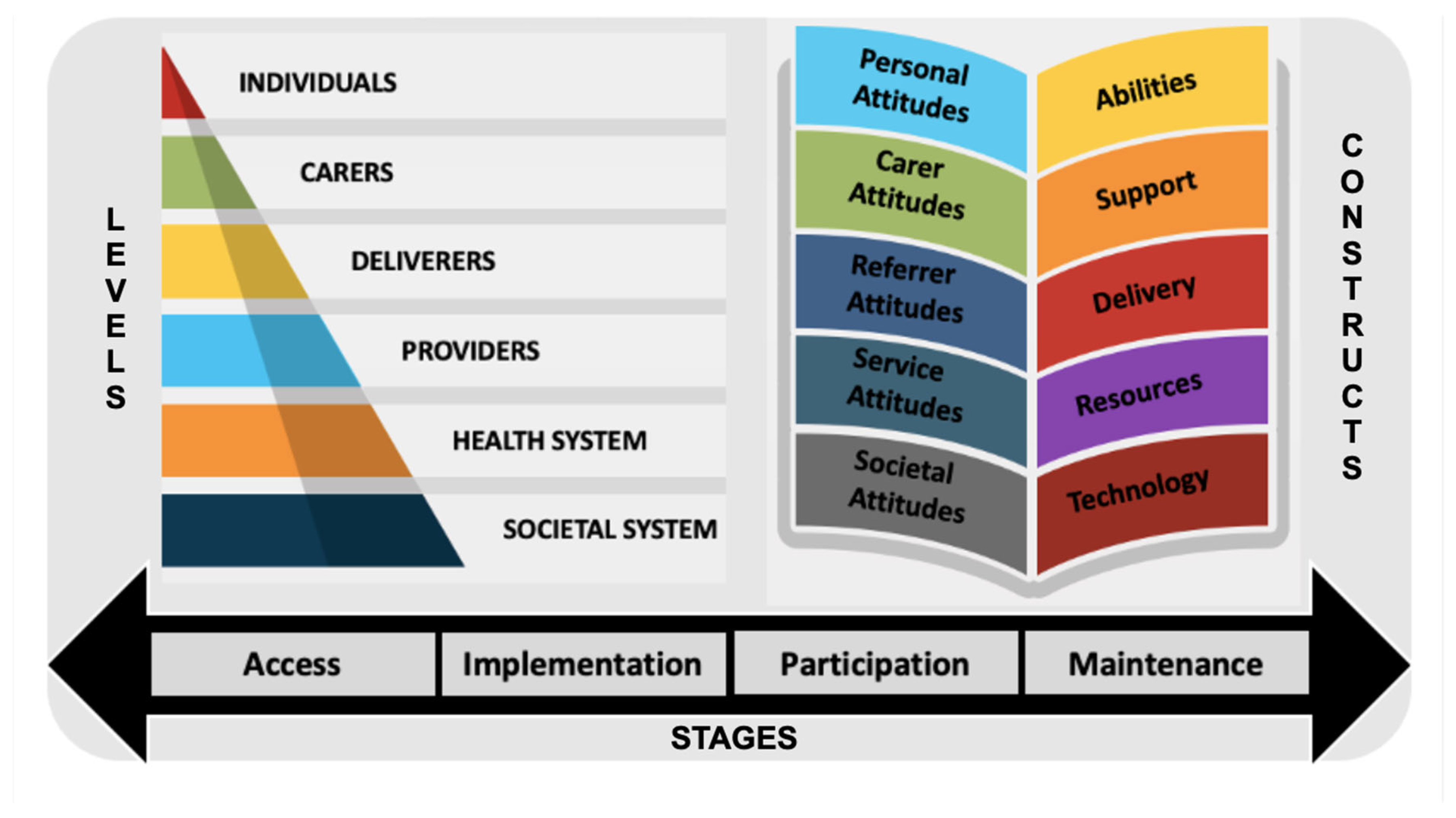

Table 1.
Study Characteristics Overview.
| Study Design | Values, n (%) | Tech Type | Values, n (%) | Participants | Values, n (%) |
| RCT* | 6 (42.8) | Non-Tech | 5 (35.7) | Dyad | 9 (64.3) |
| NR ExpTrial** | 2 (14.3) | Tech | 3 (28.6) | Individual | 4 (28.6) |
| Mixed Methods | 1 (7.1) | Both*** | 6 (35.7) | Therapists | 1 (7.1) |
| Case Report | 3 (21.4) | ||||
| Qual Research | 2 (14.3) |
*Randomised Controlled Trial. **Non-Randomised Experimental Trial. ***The category both refers to interventions that were primarily non-technology assisted but may have included only minor use of one type of technology to facilitate the delivery of or engagement with the intervention, such as a reminder emails, texts or phone calls prior to each session. Interventions that utilised more than one type of technology or, used one type of technology in more than way to facilitate the delivery of or engagement with the intervention, such as making reminder calls and providing audio or video recordings to support home practice, were labelled as technology assisted.
Table 2.
Intervention Focus, Delivery Methods and Delivery Settings.
| Focus | Values, n (%) | Method | Values, n (%) | Setting | Values, n (%) |
| Anxiety | 5 (35.7) | In Person Only | 5 (35.7) | At Home Only | 3 (21.4) |
| Depression | 3 (21.4) | IP and Phone | 6 (42.8) | Community | 9 (35.7) |
| Insomnia | 2 (14.3) | Internet-Based | 2 (14.3) | Hospital Clinic | 1 (7.1) |
| Increase in QoL | 3 (21.4) |
Table 3.
Intervention Resources Provided, Practice Supports and Technology Types.
| Resources | Values, n (%) | Practice Supports | Values, n (%) | Technology Types | Values, n (%) |
| HW Tasks | 13 (100) | Reminder Cues | 6 (46.2) | Telephone | 5 (38.5) |
| Worksheets | 4 (30.8) | Reminder Calls | 5 (38.5) | Non-Wireless* | 3 (23.1) |
| Workbook | 2 (15.4) | Audio Recording | 4 (30.8) | WirelessInternet** | 3 (23.1) |
| Video Recording | 1 (7.7) | - Smart Devices | 1 (7.7) | ||
| - Web Portal | 1 (7.7) | ||||
| - Application | 1 (7.7) |
* Non-wireless internet devices are referring to devices that do not need to be connected to the internet in order to complete the therapeutic task, such as personal computers using a USB or music players using a CD. ** Wireless internet devices refer to devices such as laptops, smartphones, and tablets, which use wireless internet to access applications, webpages and web portals to complete the therapeutic task.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



