Submitted:
09 June 2025
Posted:
10 June 2025
You are already at the latest version
Abstract
Introduction: Low medication adherence and low hypertension control are a public health challenge, particularly in low- and middle-income countries (LMICs). System healthcare and patient-related barriers hinder the successful management of hypertension. This study aimed to identify the perceptions of barriers and facilitators for managing hypertension among health system stakeholders in Santander, Colombia. Material and methods: We conducted a qualitative, phenomenological, and interpretative study, comprising five focus groups to explore the barriers and facilitators for managing people with hypertension. Each focus group was formed with stakeholders from territorial entities, healthcare insurers, or healthcare providers. Meetings were held between December 2022 and February 2023. The sessions were recorded and transcribed using NVivo Transcription and analyzed using NVivo version 1.6.1. Results: Seven categories of barriers and facilitators were identified: strategies, resources, access, risk assessment, cross-sector collaboration, articulation, and stewardship. Of those strategies, articulation and stewardship emerged as the main barriers, as revealed through axial coding and cluster analysis, which highlighted deficiencies in stewardship practices, a lack of clear objectives, and misalignment with public policy frameworks. Conclusion: Multisectoral actions extending beyond healthcare providers and aimed at improving coordination and intersectoral collaboration are essential for enhancing hypertension control in LMICs, such as Colombia. Addressing social determinants and strengthening primary healthcare through community-based strategies are critical, making stewardship and improved access key priorities.
Keywords:
cardiovascular risk
; hypertension
; barriers
; facilitators
; community-based health programs
; qualitative study
Introduction
Globally, nearly one-third of adults are affected by hypertension, with the highest burden observed in low- and middle-income countries (LMICs) [1]. Despite advancements in pharmacological treatments and health services, less than 20% of individuals with hypertension achieve adequate control, likely due to barriers at the system, provider, and individual levels [2]. A systematic review of 28 studies identified key barriers to hypertension control, including limited time and attention from providers, ineffective interventions, and inadequate provider skills and attitudes [3]. More recently, an analysis of the HEARTS initiative for hypertension and cardiovascular risk management, which assessed 22 countries in the Americas, revealed significant barriers to accessing essential and optimal medications [4]. Conversely, several facilitators have been identified that support the implementation of relevant, consensus-driven, and sustainable interventions, such as family support, motivation, and the incorporation of lifestyle modifications [3]. In Colombia, cardiovascular risk management programs are part of a national and multisectoral strategy involving several stakeholders with clearly defined responsibilities. The healthcare system consists of three primary stakeholders: (i) the government, represented by national, departmental, and municipal health authorities or territorial entities, which supervise the accountability of healthcare insurers; (ii) the healthcare insurers, or Plan Benefit Administrators (EAPBs), responsible for ensuring population access to care; and (iii) the healthcare providers, or Provider Institutions (IPSs), directly responsible for delivering care. Despite the efforts of each of these stakeholders, hypertension and cardiovascular risk control rates remain suboptimal [5]. Most existing data on barriers and facilitators to hypertension management come from high-income countries, where socioeconomic and health system contexts differ substantially [3]. Thus, there is a need to better understand the organizational, structural, and social determinants that affect hypertension control in LMICs like Colombia. Qualitative research offers valuable insights into the motivations, behaviors, and sociocultural contexts in which health phenomena occur, facilitating the identification of programs, strategies, or approaches that are most effective. This study aimed to determine the perceptions of barriers and facilitators for managing hypertension among health system stakeholders in Santander, Colombia.
Materials and Methods
Study Type and Population
As part of the “Implementation, Integration, and Institutionalization of a Community-Based Care Program to Reduce Cardiovascular Risk in Santander” (RE-HOPE) implementation study, we conducted a qualitative, phenomenological study within an interpretive paradigm [6]. The RE-HOPE project aims to implement a community-based care strategy to improve hypertension control across several municipalities in Santander, Colombia. For this qualitative analysis, we included healthcare providers from public and private institutions with expertise in service regulation, access, administration, and health insurance management. Participants were recruited from 11 public healthcare centers in Bucaramanga, Santander. This report follows the Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines [7].
Sample Selection
A typical case sampling approach was used to ensure a heterogeneous and representative group [8]. Focus groups were formed based on the following inclusion criteria: physicians, nurses, or nursing assistants with at least two years of experience and formal employment in one of the following institutions: municipal or departmental health secretariats, healthcare insurers, or healthcare provider institutions. In line with standard recommendations, each focus group aimed to include between 6 and 10 participants to ensure optimal engagement [8].
Instruments and Data Collection Process
Eligible professionals were contacted by telephone and invited to voluntarily participate in the study. Upon agreement and provision of informed consent, focus group sessions were scheduled between December 2022 and February 2023. The consent process included authorization for the recording and use of audio, photographs, and videos. Sessions were conducted in quiet, distraction-free environments at the participants' workplaces to ensure fluid conversation and high-quality audio recordings. Research staff received training in standardized focus group facilitation and moderation techniques [8]. Each session was moderated by a member of the research team, while a second team member served as an observer. The moderator used a semi-structured interview guide and a predefined script, while the observer ensured adherence to protocol, documented nonverbal cues, and supported the overall process. Both team members facilitated active participation, ensuring that all attendees had the opportunity to express their views. Interviews were conducted in Spanish and later translated into English.
Processing and Analysis
Verbatim and automated transcriptions were generated using the NVivo Transcription system (NVivo software, version 1.6.1). Methodological rigor was ensured by applying Lincoln and Guba’s criteria for qualitative research (Table 1), which safeguarded against the influence of participants’ preexisting perceptions on the interpretation of their responses [9]. To preserve credibility and confidentiality, each recording was anonymized and assigned a unique code. The participants validated the findings during follow-up meetings. To ensure auditability, all textual reports were reviewed by both the session moderator and the observer, followed by a third independent review conducted by another member of the research team. The accuracy of the transcriptions was thoroughly verified. Exhaustiveness was achieved by applying the data saturation criterion. Lastly, transferability was enhanced by tailoring context-specific questions to each participant’s lived experience. The qualitative analysis followed a multi-stage approach. A member of the research team who was not involved in the focus groups reviewed the transcripts and interpreted participants’ perceptions of barriers and facilitators to hypertension control. Based on participants’ experiences and perspectives, open coding was applied to develop initial thematic categories. Subsequently, an interpretive analysis was performed using axial coding to connect categories and organize narratives and accounts. Cluster analysis was then conducted to identify relationships within the textual data that could further enrich the understanding of perceived barriers and facilitators. In the final stage, confirmability was ensured through an independent review by a researcher not involved in data collection. As part of the audit trail, all qualitative analysis codes were archived in a Mendeley Data repository. The data collection protocol was approved by the Bioethics Committee of the Universidad de Santander (Act No. 018, dated August 29, 2022). The study was funded by Colombia’s General System of Royalties BPIN code: 2020000100447
Results
A total of 25 representatives from the three main stakeholder groups—territorial entities, healthcare insurers, and healthcare providers—participated in the study. An average response rate of 89% was achieved across five focus groups. Each session lasted between 19 and 57 minutes, and participants attended only one focus group. Most participants were women (84%), and more than one-third (80%) of the focus groups were conducted with individuals from territorial entities and healthcare insurers (Table 2). During the open coding phase (descriptive analysis), seven key categories or codes were identified: strategies, resources, access, risk assessment, intersectoral collaboration, articulation, and leadership. These categories were derived from interpreting the transcripts within the broader context of public health practice in Colombia [10]. Definitions for each code are shown in Supplemental Table 1.
The distribution of topics or codes by stakeholder is presented in Table 3. Notably, the healthcare insurers did not reference codes such as access, intersectoral collaboration, or stewardship; the latter was exclusively mentioned by stakeholders from territorial entities. These participants also emphasized the importance of risk measurement, followed by intersectoral collaboration. In contrast, healthcare providers did not refer to risk measurement or stewardship. Their narratives predominantly focused on access, followed by intersectoral collaboration, and less frequently mentioned articulation or resources.
Findings by Category (Interpretative Analysis)
“Strategies” was the most frequently mentioned category in both the testimonies and the coding process. Stakeholders from insurance companies and territorial entities described different actions and plans aimed at identifying and following up with individuals at high risk for cardiovascular disease. These included efforts in health education and information dissemination to encourage engagement with healthcare providers. Community-based initiatives were also highlighted as key tools for raising public awareness. Several participants shared successful experiences involving the implementation and monitoring of strategies in collaboration with national and international organizations, which contributed to capacity building and strengthened intersectoral coordination within the department.
“In previous years, information and education strategies have been developed so that people become involved with institutions. The department (government) generates some activities so that in X municipality they work with the community and that information reaches them.” Woman, 41 years old, territorial entities.
“There were community groups, they had educators or physical activity facilitators [...] So we started and worked on the experience at the departmental level, Santander en Movimiento worked for about four, six years… for more than 10 years we worked first on Carmen and then Santander en Movimiento.” Woman, 57 years old, territorial entities.
Stakeholders involved in population-level cardiovascular risk management recognized fragmentation across primary, secondary, and tertiary care levels. This fragmentation is characterized by difficulties in transferring information about high-risk populations, underscoring the need for improved coordination and more integrated approaches. The negative impact of these barriers is exacerbated not only by the lack of community-based interventions but also by the failure of existing efforts to align with the objectives of the Collective Intervention Plans (PIC) implemented in the territories. Participants emphasized the crucial role of community leaders in implementing effective health strategies. They underlined the importance of enhancing information flow between entities, particularly from healthcare insurers to health providers. This concern was reflected in the focus group discussions as follows:
“That is where the identification of the risk of these patients begins. The commitment was for 2023, when it was over, to be able to have and deliver this very important information that the insurers must consolidate or make a collective intervention plan that is effective for the population.” Woman, 39 years old, EAPB.
“The EPS door-to-door service seems very good to me, because they tell us how many there are or send them, and of course, we are percipient and we attend to them, it is difficult for us to go and get them, the most we can do is call, and many times it is lost, but the insurer's door-to-door service, I think is important, and it seems to me the most effective because people get motivated to bring the elderly, when they are visited, give them a piece of paper with the appointment, to guide them.” Woman, 50 years old, IPS.
“It would be necessary for community leaders to provide support through a loudspeaker, for the leader to make a loudspeaker in the health brigades.” Woman, 26 years old, IPS.
Health providers and territorial entities stakeholders referred to the importance of implementing more effective strategies to reduce cardiovascular risk, particularly in individuals who resume healthy lifestyles and habits, combined with community-based actions, as shown below:
“Above all, promoting healthy lifestyles, that is the most important thing, encouraging exercise, proper nutritional habits.” Woman, 36 years old, IPS.
“In this case, it would be necessary for community leaders to provide support through a public address system, for the leader to make public address systems in the health brigades.” Woman, 31 years old, IPS.
Within the “resources” category, stakeholders from insurance companies highlighted their responsibility for managing resources at the individual level, which poses barriers due to the need for effective optimization and allocation across diverse territories. In contrast, resources at the population level are managed by territorial entities. Territorial entities support health promotion activities, risk control, and demand generation. Persistent resource shortages constitute a major barrier to inter-institutional collaboration. This often results in misalignments, as some stakeholders focus on individualized care while others prioritize collective interventions—each shaped by the imperative to respond to population health needs.
“There is something super important that plays a role and is called the optimization of the UPC (Per Capitation Payment Unit – “Unidad de Pago por Capitación”) is how much the ministry gives me to be able to execute the risk of the entire population, so with that UPC, I must optimize it. It is not that it is worth more to me, I will do it for you, it is that there is no more money from the ministry and here we all must adapt to that resource that there is.” Woman, 39 years old, EAPB.
“… well, all the activities that are in the collective intervention plan have been developing and taking advantage of that, to do these complementarities in its municipalities that do not have sufficient resources, then let's say that it comes in there to attend and support this search, the early diagnosis of people with cardiovascular risk.” Woman, 41 years old, territorial entities.
“It is necessary to assign personnel to these activities, because we within the health personnel, have assigned some responsibilities, which demand time, and the responsibilities are very high for us to be taking charge of that.” Woman, 41 years old, Nurse, IPS.
“Articulation” was the third most frequently discussed category across the focus groups. Its importance was widely acknowledged; yet, participants also emphasized its fragility among territorial entities, healthcare insurers, and both public and private healthcare providers at primary and secondary levels. Weak articulation among stakeholders was identified as a central barrier affecting the delivery of comprehensive care within cardiovascular risk management programs:
“Yes, there must be comprehensiveness and there must be an articulation between providers. Who makes that articulation? The insurer through contracts, because we do not hire providers, we hire comprehensive routes. If then, within that exercise it is very complicated to work, join the public and private network… so, it is quite complicated to unite them” Woman, 39 years old, EAPB.
“It is necessary to synchronize with the EAPB, because the patient is recruited, but then they do not give the appointment, the patient gets tired, that internal medicine package is almost always lost, … it is necessary to manage with the EAPB, because the internists do not manage the health centers. We do the laboratories, we give them the medicines, but the specialists are not reached by the patient, they are lost.” Woman, 36 years old, Nurse, IPS.
Several successful experiences of coordination between territorial entities, healthcare insurers, and healthcare providers, as well as between insurers and providers, were described. These cases demonstrated the potential to facilitate interaction, dialogue, and feedback across primary and complementary care services through professionals or analysts specifically assigned to the program. The importance of information documented in clinical records was reaffirmed, particularly regarding indicators used to monitor risk management (precursor conditions) and program adherence. These data serve as valuable inputs for evidence-based decision-making, including the development of comprehensive care pathways and strategies to reduce service fragmentation.
“As far as the plan for collective interventions and the provision of services is concerned, let's say, several activities have been articulated with the municipal entity and with the providers in the territory, citing the insurers.” Woman, 41 years old, territorial entities.
“So, what is the advantage we have with this actor in our model? And it is that they permanently articulate with the primary provider and here within the EAPB there is a professional for these municipalities in charge of cardiovascular risk. So, let's say that it allows for this articulation between the three, between the three EAPB stakeholders, primary and complementary, then it allows this route to flow more. Yes, and the results, well, we are really seeing them. So, we provide training at the first level from that complementary component and this, I think, is one of the greatest, as well as successful experiences that we have currently regarding this cohort.” Woman, 39 years old, EAPB.
“Yes, there are the analysts, for example, who are with the IMAP (information system), so there is also a professional in charge there and there are the analysts, who are in charge of doing those follow-ups, whether they gave you the medicine or not, and they notify us of those developments and we, well, as we are the ones who ultimately hire the provider.” Woman, 36 years old, EAPB.
“Access” to services was conceptualized as the actual potential for entry into and utilization of essential healthcare services, based on insightful interpretations offered by institutional stakeholders. Overall, the narratives highlighted access barriers related to sociodemographic characteristics, limitations in social support networks, and logistical challenges faced by service providers, particularly in the distribution of medications for cardiovascular risk management.
“… those who come from rural areas or dispersed rural areas are even worse. The difficulties there are many and what would be needed because there are many… many adjustments, because even if the individual plan includes promotion and maintenance within the route, everything that has to be done for a person and the complementary interventions, it does fall short, the resources are few for the dispersion that exists here, it is complex” Woman, 41 years old, territorial entities.
“Age, the population is almost always or most commonly elderly, most people at risk (cardiovascular risk program) do not have a support network, and the level of education is very low, so they do not even know what they are taking, age is important, the support network, education, is what affects the most among other things.” Woman, 52 years old, Physician, IPS.
“When they go to the pharmacy, they ask for medicine and there is no medicine, so they have to go back to the doctor, and he changes the medicine, if there is, if not, they have to wait, so that he calls the EAPB pharmacy to deliver it, even the user gets lost because of this.” Woman, 26 years old, Nursing Assistant, IPS.
“Cross-sector collaboration” emerged as a critical category requiring coordinated efforts across the health system to effectively overcome key barriers and ensure the delivery of comprehensive care and services. Participants identified several challenges, including a lack of alignment among stakeholders, the absence of governance frameworks for resource management and allocation, and limited institutional capacity to coordinate and implement the diverse actions necessary to achieve integrated and effective care.
“There are challenges that involve these other areas, the challenge of articulation with other sectors such as infrastructure, sports, and education; In other words, if there is a big challenge, it is the issue of achieving articulation between all sectors to achieve a goal. Specifically, for example, the CERS (Healthy Cities, Environments and Ruralities – “Ciudades, Entornos y Ruralidades Saludables”) strategy that comes from the Ministry that includes infrastructure of sports sites that are not the responsibility of the Ministry of Health, which makes it more difficult to achieve this articulation” Woman, 57 years old, territorial entities.
“But we are falling short, there are things, because there are many actions from different fronts that must be worked on, from industry, from education, from everywhere.” Woman, 41 years old, territorial entities.
“We need to improve a lot to reduce these cardiovascular risks, but it does not only depend on us, but on other people and other circumstances, things outside of us, but there are many needs and things to improve.” Woman, 31 years old, Nurse, IPS.
In the “risk measurement” category, the role of data flow and information exchange among system stakeholders was highlighted as essential for planning both individual and population-level activities. Participants emphasized the importance of validating and enriching this information during the collection and analysis processes. Testimonies from representatives of territorial entities and healthcare insurers underscored the value placed on strengthening information systems to support continuous monitoring and evaluation of cardiovascular risk management at both individual and collective levels.
“Within the cardiovascular risk database, all the interventions that are established within the route are contemplated, such as taking laboratory tests in its control, according to the stratification that the user has, all the diagnostic aids and all the consultations, whether by general medicine, specialized medicine and paramedics, nutrition, psychology. So, this information is captured within the database, which also allows us to see how this evolution occurs.” Woman, 39 years old, EAPB.
“…the indicators: I think that the most successful thing that one can show are the indicators.” Woman, 39 years old, territorial entities.
In contrast, some successful experiences were highlighted, including previous projects conducted in Santander that enabled the evaluation, analysis, and validation of cardiovascular risk measurement among key population stakeholders. For territorial entities, resuming such initiatives was deemed pertinent and potentially feasible through joint efforts and sustained implementation. However, healthcare providers did not offer specific insights or narratives related to this category.
“The STEPWise 1 and 2 study, those studies were successful and if you notice, those studies are the result of all the work that was done over those years,… so it is a successful experience that Santander had, which has suddenly been abandoned a little, but I know that with collective interventions and giving it, let’s say, support to the dimension (dimension 2 of Public Health) it can be rescued again, that we do not need to suddenly invest so much, but rather help the municipality to organize what it has at home” Woman, 57 years old, territorial entities.
“Stewardship” was a category that emerged exclusively among stakeholders from territorial entities. Several barriers to effective state governance need to be addressed to foster collaboration and coordination in the implementation of public policies. While participants acknowledged the adequacy and clarity of existing legislation, regulations, and government strategies, they also emphasized a lack of personnel with the capacity to advocate for intersectoral agreements, monitor the organization of strategic plans, and manage cardiovascular risk and related interventions within the framework of the current Comprehensive Health Care Routes (RIAS).
“And the other thing is that there is also a barrier at the state level” Woman, 57 years old, territorial entities.
“People are needed, people with clear policies, there are many policies. There are many strategies, there are many, but get your teeth into it, sit down as a territorial entity and say let's work on this” Woman, 57 years old, territorial entities.
“This must be a government policy, so that it is not the same” Woman, 41 years old, territorial entities.
Findings from the Cluster Analysis
The dendrogram derived from the cluster analysis (Figure 1) illustrates the set of emerging subcategories of patterns identified within some of the pre-established categories or codes. This analysis was conducted based on the similarity of words in the responses to questions posed by representatives of institutional stakeholders. The word “access” was always closely related to “cross-sector collaboration”, and, in turn, this was closely related to “strategies” and “articulation”. For access and cross-sector collaboration, subtopics such as difficulties, challenges, purposes, need for improvement, and effort in articulation were found; while, for articulation and strategies, difficulties and obstacles remained, along with the implementation barriers. In the confirmability analysis, some interrelations between subcategories of interest were identified, observing that barriers in access and the need for improvement were more closely related to the health insurance. The relationship between the three types of stakeholders became evident from the subcategories of Implementation barriers and Purposes (Supplemental Figure 1).
Discussion
In Colombia, the management of cardiovascular risk represents a complex challenge involving multiple institutional stakeholders within the healthcare system, including territorial entities, health insurers, and healthcare providers. This study identified the primary barriers to effective cardiovascular risk management as the lack of robust strategies, limited resources, and inadequate inter-institutional coordination. Conversely, key facilitators included improved access to services, enhanced information flow, and strengthened stewardship, encompassing governance and leadership capacities. An interesting finding was the identification of categories that were strongly emphasized by some participants but entirely unaddressed by others—differences that appeared to be directly associated with the institutional roles of the entities they represented. For instance, stakeholders from healthcare insurers did not mention access, while those from healthcare providers did not address risk measurement; likewise, stewardship was exclusively discussed by representatives of the territorial entities.
Generalizing the determinants of effective and contextually relevant management might be challenging. For instance, a study assessing the implementation of health system guidelines in LMICs showed that barriers and facilitators differ significantly depending on the type of institution and its specific functions within the system [11]. Additionally, accessibility and risk assessment are critical components for strengthening the resilience of health systems. In the present study, the codes regarding access by healthcare insurers and risk assessment by healthcare providers may indicate a disconnect between institutional public health policies and operational priorities [12]. Similarly, the concept of health system resilience highlights the importance of strong governance and stewardship, as well as the active involvement of territorial entities in implementing health policies, which may explain why this category was mentioned exclusively by representatives from these institutions. Nevertheless, while stewardship is central to the mandate of territorial entities, its effective implementation also requires the collaboration and alignment of all stakeholders to ensure that such policies are not only adopted but also operationalized in accordance with each stakeholder’s institutional scope and capacity.
Several studies have examined the impact of information flow on the effectiveness of interventions in LMICs, and it has been reported that there is a significant need to improve articulation and equity in access to digital health information [3, 13]. The perceived barriers centered on the fragmentation between stakeholders, a lack of fluidity and relevance of information for decision-making, and the absence of clear purposes or goals aimed at achieving health objectives. For instance, in Latin American countries, it has been noted that fragmentation poses a significant challenge to scaling up effective secondary prevention strategies [14]. Ensuring that community-based strategies transcend the discourse of public policies towards their implementation is essential. The perceptions of providers regarding the characteristics of interventions to be implemented, as well as those of the recipients, are often overlooked. In this regard, the translation of evidence into practice influences the characteristics perceived by providers, impacting the efficiency of an implementation strategy [12]. Additionally, education strategies should be continued during the implementation of an intervention, given the demonstrated decline in knowledge retention among providers over time. Indeed, health literacy should involve both health professionals and non-medical personnel. The HOPE-4 study, conducted in 1371 hypertensive patients from Colombia and Malaysia, demonstrated that implementing a comprehensive care model led by trained non-medical health personnel, in conjunction with the continuous administration of appropriate pharmacological treatment and psychosocial support, increased pharmacological adherence in the intervention group and significantly reduced cardiovascular risk compared to standard care[15].
The lack of continuity appears to be associated with other key categories, including cross-sector collaboration, articulation, and stewardship. In this context, the importance of resources and effective stewardship in shaping public policy is particularly salient in low-resource settings [16]. Therefore, it is crucial to evaluate implementation outcomes, including acceptability, fidelity, feasibility, scalability, and sustainability, particularly in community-based strategies. However, evidence on the most appropriate tools to promote and support multisectoral actions remains limited. In LMICs, multisectoral approaches are often hindered by institutional weaknesses and fragmentation, including within the health sector itself, which undermines the coordination needed to address the structural drivers and social norms that impact vulnerable populations [17]. Addressing these multisectoral challenges requires robust governance and leadership; however, our findings reveal that leadership is frequently confined to territorial entities, with less-defined roles for other institutions and stakeholders. This was evidenced by the absence of references to governance responsibilities among health insurers and providers, as well as the prevailing perception that multisectoral coordination lies outside the health sector’s purview. Leadership must be collaborative and distributed across stakeholders, including non-health sectors such as education, sports, and culture, and institutional governance must be strengthened. Tackling social disparities requires directly addressing social determinants and aligning institutional mandates through coordinated, cross-sectoral efforts [17, 18].
Limitations
The projected participation rate was not obtained; however, saturation of the categories was achieved with the representatives who participated. The geographical delimitation of the study, only in one Colombian department, and some actors coming mainly from urban areas, do not necessarily representative of all the health subsystems of Colombia and highlights the importance of considering contextual factors that allow for a deeper understanding of the interaction dynamics and power relations specific to each specific environment.
Conclusions
Multisectoral actions are crucial for achieving optimal control of cardiovascular risk. They are essential for achieving robust and sustainable health systems, particularly in LMICs where social disparities are high. Multisectoral actions require leadership that facilitates collaboration and articulation among health system actors. Despite evidence addressing governance and leadership barriers in managing specific health conditions or diseases, a notable gap remains in explicit research on conceptual frameworks and mechanisms related to stewardship from public health, administrative, or allied health fields. Critical components, such as cross-sector collaboration and stewardship, have not been recognized as fundamental elements, either as barriers or facilitators, in the effective management of cardiovascular risk. Studies should promote learning communities and evidence-based practices to strengthen multisectoral actions. Future research should explore conflicts of interest, organizational cultures, leadership mechanisms, and goal setting, while also assessing the transferability of results across institutions.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
P.L-J., J.O. conceived and initiated the RE-HOPE study, supervised its conduct, and reviewed and commented on the draft. A.C., D.M-B. administrated and supervised the project, resources, and software. J.P.L-L., Y.G-C. wrote the analysis plan and drafted the manuscript. C.T.,C.G.,M.L-C. assisted with interpreting the data and drafting the manuscript.
Funding
This study was developed within the Re-HOPE Project (Implementación, integración e institucionalización de un programa de atención basado en comunidad para disminuir el riesgo de enfermedad cardiovascular en Santander. BPIN code: 2020000100447). Funded by the Ministry of Science and Technology through Colombia’s General Royalties System.
Institutional Review Board Statement
The data collection protocol was approved by the Bioethics Committee of the Universidad de Santander (Act No. 018, dated August 29, 2022).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the stud
Data Availability Statement
Individual-level data will not be shared because RE-HOPE is an ongoing study. Requests for aggregated data will be considered on a case-by-case basis upon receipt of a reasonable request.
Conflicts of Interest
All authors declare that they have no conflicts of interest.
References
- Miranda JJ, Barrientos-Gutierrez T, Corvalan C, Hyder AA, Lazo-Porras M, Oni T, et al. Understanding the rise of cardiometabolic diseases in low- and middle-income countries. Nat Med. 2019, 25, 1667–79. [Google Scholar] [CrossRef] [PubMed]
- Joseph P, Lanas F, Roth G, Lopez-Jaramillo P, Lonn E, Miller V, et al. Cardiovascular disease in the Americas: the epidemiology of cardiovascular disease and its risk factors. Lancet Reg Health Am. 2025, 42, 100960. [Google Scholar]
- Wandell PE, de Waard AM, Holzmann MJ, Gornitzki C, Lionis C, de Wit N, et al. Barriers and facilitators among health professionals in primary care to prevention of cardiometabolic diseases: A systematic review. Fam Pract. 2018, 35, 383–98. [Google Scholar] [CrossRef] [PubMed]
- Souza KM, Giron N, Vallini J, Hallar K, Ordunez P, Rosende A, et al. Barriers to access to antihypertensive medicines: insights from the HEARTS initiative in latin American and Caribbean region. J Pharm Policy Pract. 2024, 17, 2379045. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Jaramillo P, Lopez-Lopez JP, Otero J, Alarcon-Ariza N, Mogollon-Zehr M, Camacho PA, et al. May Measurement Month 2019: an analysis of blood pressure screening results from Colombia. Eur Heart J Suppl. 2021, 23 (Suppl B), B46–B8. [Google Scholar] [CrossRef] [PubMed]
- Fade, S. Using interpretative phenomenological analysis for public health nutrition and dietetic research: a practical guide. Proc Nutr Soc. 2004, 63, 647–53. [Google Scholar] [CrossRef] [PubMed]
- Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007, 19, 349–57. [Google Scholar] [CrossRef] [PubMed]
- Smith J, Firth J. Qualitative data analysis: the framework approach. Nurse Res. 2011, 18, 52–62. [Google Scholar] [CrossRef] [PubMed]
- E.G. LYSG. Naturalistic Inquiry. Beverly Hills: Sage, 1985.
- Legido-Quigley H, Camacho Lopez PA, Balabanova D, Perel P, Lopez-Jaramillo P, Nieuwlaat R, et al. Patients' knowledge, attitudes, behaviour and health care experiences on the prevention, detection, management and control of hypertension in Colombia: a qualitative study. PLoS One. 2015, 10, e0122112. [Google Scholar]
- Breneol S, Curran JA, Marten R, Minocha K, Johnson C, Wong H, et al. Strategies to adapt and implement health system guidelines and recommendations: a scoping review. Health Res Policy Syst. 2022, 20, 64. [Google Scholar] [CrossRef] [PubMed]
- Bishai D, Saleh BM, Huda M, Aly EM, Hafiz M, Ardalan A, et al. Practical strategies to achieve resilient health systems: results from a scoping review. BMC Health Serv Res. 2024, 24, 297. [Google Scholar]
- Gibson DG, Tamrat T, Mehl G. The State of Digital Interventions for Demand Generation in Low- and Middle-Income Countries: Considerations, Emerging Approaches, and Research Gaps. Glob Health Sci Pract. 2018, 6 (Suppl 1), S49–S60. [Google Scholar] [CrossRef] [PubMed]
- Avezum A, Perel P, Oliveira GBF, Lopez-Jaramillo P, Restrepo G, Loustalot F, et al. Challenges and Opportunities to Scale Up Cardiovascular Disease Secondary Prevention in Latin America and the Caribbean. Glob Heart. 2018, 13, 83–91. [Google Scholar] [CrossRef] [PubMed]
- Schwalm JD, McCready T, Lopez-Jaramillo P, Yusoff K, Attaran A, Lamelas P, et al. A community-based comprehensive intervention to reduce cardiovascular risk in hypertension (HOPE 4): a cluster-randomised controlled trial. Lancet. 2019, 394, 1231–42. [Google Scholar] [CrossRef] [PubMed]
- Bovet P, Chiolero A, Paccaud F, Banatvala N. Screening for cardiovascular disease risk and subsequent management in low and middle income countries: challenges and opportunities. Public Health Rev 2015, 36, 13. [CrossRef] [PubMed]
- Rasanathan K, Atkins V, Mwansambo C, Soucat A, Bennett S. Governing multisectoral action for health in low-income and middle-income countries: an agenda for the way forward. BMJ Glob Health. 2018, 3 (Suppl 4), e000890. [Google Scholar]
- Bennett S, Glandon D, Rasanathan K. Governing multisectoral action for health in low-income and middle-income countries: unpacking the problem and rising to the challenge. BMJ Glob Health. 2018, 3 (Suppl 4), e000880. [Google Scholar]
Figure 1.
Dendrogram of the emerging subcategories derived from the cluster analysis by word similarity.
Figure 1.
Dendrogram of the emerging subcategories derived from the cluster analysis by word similarity.
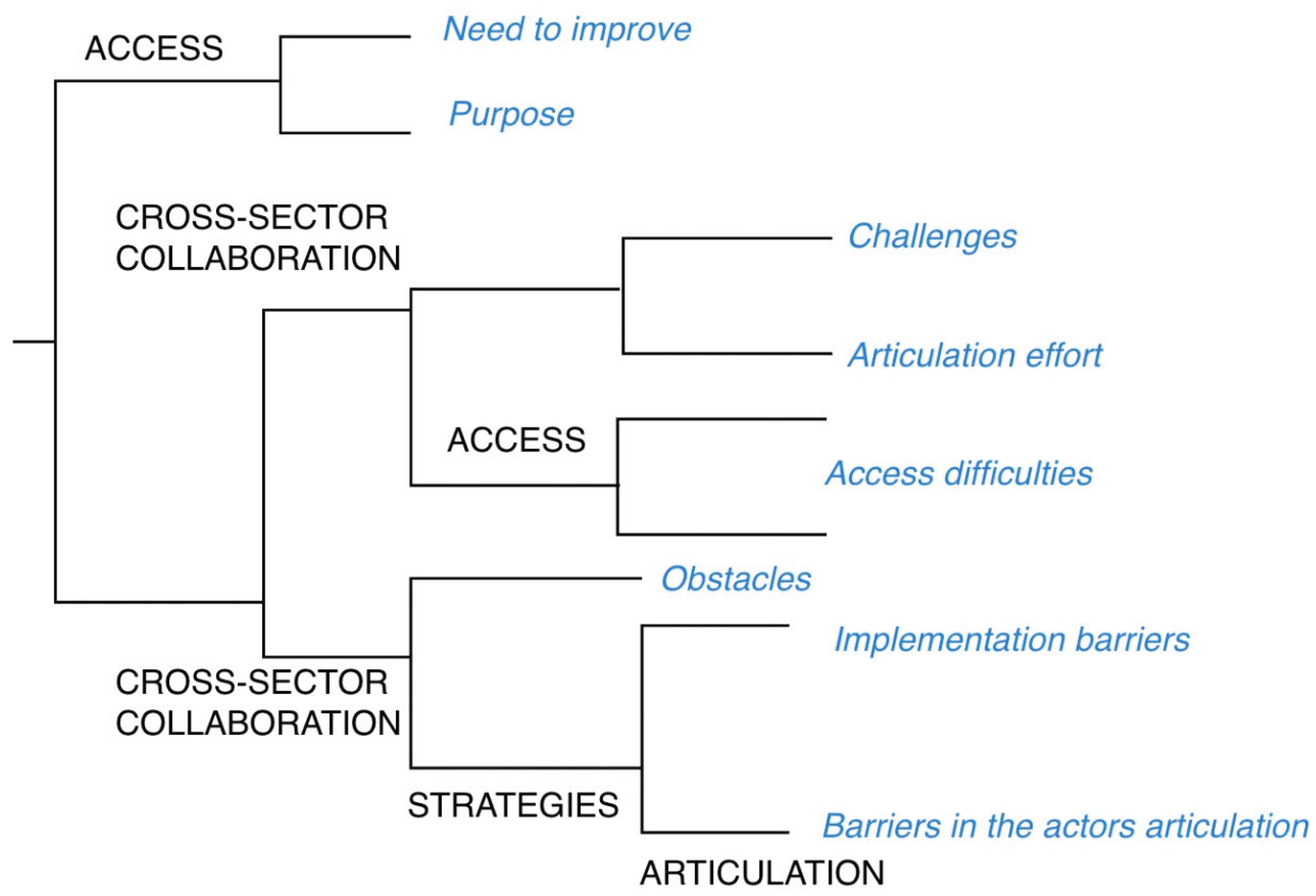

Table 1.
Question examples from the scripts provided to the focus group, categorized by stakeholder.
Table 1.
Question examples from the scripts provided to the focus group, categorized by stakeholder.
| Stakeholder | Questions |
| Territorial entities | -According to your experience, what are the reasons that guarantee the management of cardiovascular risk? -How is access to the cardiovascular risk management program regulated? -How can the cardiovascular risk management be improved in Santander? |
| Health Benefit Plan Management Companies/Healthcare insurers | -We would like to know in which way the activities between the entities and the community are articulated. -Describe how you manage the cardiovascular risk of your affiliates. |
| Healthcare provider institutions | -Describe the follow up done to the participants the cardiovascular risk programs. -What do you think could be the actions or community strategies to recruit and monitor patients? -In your opinion, what actions can be implemented to improve the cardiovascular risk program in your institution? |
Table 2.
Focus group participants.
| Stakeholder | Number of focus groups | Sex | Background | |
| Male | Female | |||
| Territorial entities | 2 | 2 | 12 | Professional with specialty |
| Health Benefit Plan Management Companies/Healthcare insurers | 2 | 2 | 3 | Specialized professionals. |
| Healthcare provider institutions | 1 | 0 | 6 | Doctors, nurses and nursing assistants. |
Table 3.
Distribution of codes or references identified by stakeholders in the focus groups.
| Category | Proportion of codes by stakeholder | ||
| EAPB (%) | ET (%) | IPS (%) | |
| Access (n= 14) | 0 | 21 | 79 |
| Articulation (n= 17) | 71 | 18 | 11 |
| Strategies (n= 26) | 54 | 27 | 19 |
| Intersectorality (n= 6) | 0 | 50 | 50 |
| Risk Measurement(n= 6) | 34 | 66 | 0 |
| Stewardship (n= 3) | 0 | 100 | 0 |
| Resources (n= 20) | 55 | 30 | 15 |
| EAPB: Health Benefit Plan Management Companies. IPS – Health-service Provider Institutions. ET: Territorial Entities | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



