Submitted:
06 June 2025
Posted:
09 June 2025
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Post-COVID dysautonomia has emerged as a prominent and debilitating manifestation of Long COVID, characterized by a wide spectrum of autonomic dysfunctions including postural orthostatic tachycardia syndrome (POTS), orthostatic hypotension, and gastrointestinal dysmotility. Despite growing recognition, the pathophysiological underpinnings, clinical presentation, and optimal management of this condition remain incompletely understood.This narrative review aims to synthesize current evidence on the mechanisms, clinical features, diagnostic approaches, and emerging therapeutic strategies for dysautonomia following SARS-CoV-2 infection, while highlighting knowledge gaps and future research directions.A comprehensive literature review was conducted using PubMed, Scopus, and Google Scholar to identify peer-reviewed studies, reviews, and case series relevant to post-COVID autonomic dysfunction. Articles published between 2020 and 2025 were included, with emphasis on mechanistic insights, clinical case definitions, and management outcomes.Multiple pathophysiological mechanisms are implicated, including autoimmune activation, persistent neuroinflammation, vagal nerve injury, endothelial dysfunction, and residual viral reservoirs. Clinically, patients may present with multisystemic symptoms that overlap with myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS). Diagnostic workup includes autonomic function testing, tilt-table testing, and biomarker evaluation. Emerging treatment modalities range from beta-blockers and volume expansion to neuromodulation and immunotherapy, though evidence remains limited and heterogeneous.Post-COVID dysautonomia represents a complex, multifactorial condition with significant implications for patient quality of life. Improved diagnostic criteria, mechanistic biomarkers, and randomized controlled trials are urgently needed to guide management and therapeutic development. Interdisciplinary collaboration will be critical in addressing the growing burden of autonomic dysfunction in the post-pandemic era.
Keywords:
long COVID
; post-acute sequelae of SARS-CoV-2 infection (PASC)
; dysautonomia
; postural orthostatic tachycardia syndrome (POTS)
; autonomic nervous system
Introduction
The global burden of COVID-19 has extended beyond acute infection, giving rise to a constellation of persistent symptoms now termed “Long COVID” or Post-Acute Sequelae of SARS-CoV-2 Infection (PASC). Among the most debilitating and underrecognized manifestations is dysautonomia, particularly presenting in a postural orthostatic tachycardia syndrome (POTS)-like fashion. While initially described in case reports, the incidence and clinical relevance of post-COVID autonomic dysfunction have become increasingly apparent. An estimated 30% of Long COVID patients report symptoms suggestive of autonomic imbalance, yet pathophysiologic mechanisms remain poorly defined and treatment strategies unstandardized. This narrative review synthesizes current evidence on post-COVID dysautonomia, focusing on proposed mechanisms, clinical phenotypes, diagnostic approaches, and therapeutic strategies.
Normal Autonomic Physiology
The autonomic nervous system (ANS) regulates involuntary bodily functions, including heart rate, blood pressure, digestion, and thermoregulation. It is divided into the sympathetic (“fight or flight”) and parasympathetic (“rest and digest”) branches. Key regulatory elements include:
- Baroreflex arc: regulates blood pressure via mechanoreceptor-mediated control of heart rate and vascular tone.
- Vagal nerve: modulates parasympathetic output to the heart and GI tract.
- Sympathetic chain: mediates norepinephrine-driven vasoconstriction and cardiac output.
ANS homeostasis maintains blood flow and metabolic function during positional changes or physical exertion. Disruption of this delicate balance results in orthostatic intolerance, tachycardia, and systemic symptoms seen in dysautonomia.
Proposed Mechanisms in Post-COVID Dysautonomia
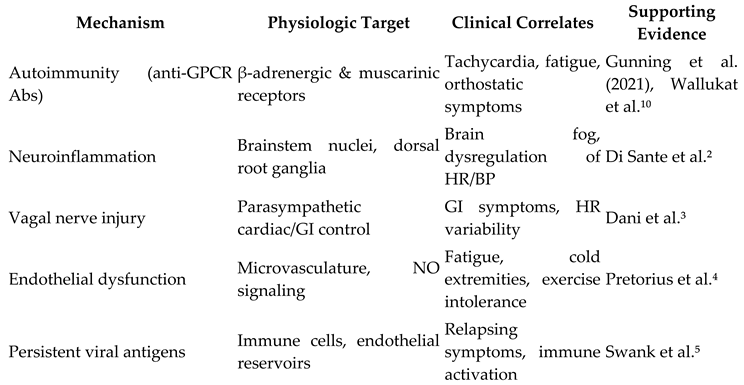
Multiple overlapping hypotheses have emerged to explain the onset of dysautonomia after SARS-CoV-2 infection:
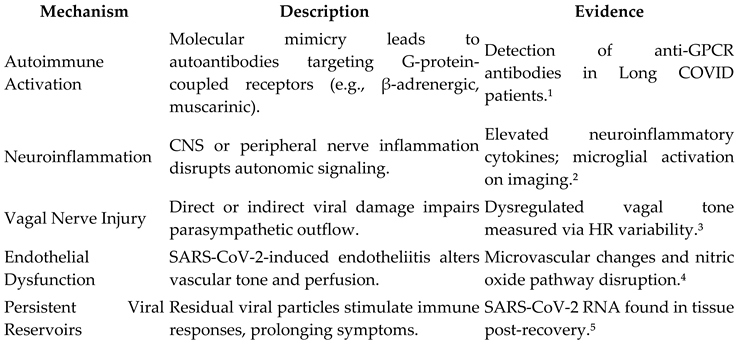
The combination of these mechanisms likely leads to a maladaptive autonomic state resembling chronic fatigue syndrome (CFS/ME) or classical POTS.
Clinical Manifestations
Patients with post-COVID dysautonomia report a spectrum of symptoms that vary in severity and duration:
- Orthostatic Intolerance: lightheadedness, palpitations, dizziness upon standing
- Tachycardia: sustained HR increase ≥30 bpm within 10 minutes of standing (POTS criteria)
- Fatigue and Malaise: often disabling and worsened by exertion (post-exertional malaise)
- Cognitive Impairment (“Brain Fog”): difficulty concentrating, memory lapses
- Gastrointestinal Symptoms: nausea, bloating, delayed gastric emptying
- Temperature Dysregulation: hot flashes, cold extremities
- Sleep Disturbance: insomnia, non-restorative sleep
These symptoms often fluctuate, mimicking autoimmune or post-viral syndromes, and disproportionately affect young females, echoing pre-pandemic POTS demographics.
Diagnostic Approaches
There is no single test for post-COVID dysautonomia. Diagnosis relies on a combination of clinical history and physiologic testing:
- 10-minute standing test: HR and BP measured supine and standing; HR increase ≥30 bpm with minimal BP drop supports POTS.
- Tilt-table testing: standard for diagnosing orthostatic intolerance and neurocardiogenic syncope.
- Heart rate variability analysis: evaluates vagal tone and autonomic balance.
- QSART (Quantitative Sudomotor Axon Reflex Test): assesses sympathetic sweat gland function.
- Serologic markers: under investigation (e.g., anti-GPCR antibodies).
Importantly, differential diagnoses (e.g., anemia, deconditioning, adrenal insufficiency) must be excluded.
Therapeutic Strategies
Management of post-COVID dysautonomia remains empirical and multi-pronged, focusing on symptom relief, autonomic retraining, and functional recovery.
Nonpharmacologic Approaches
- Hydration and Salt Loading: 2–4L fluid/day and up to 10g salt intake improves blood volume.
- Compression Garments: reduce venous pooling.
- Exercise Rehabilitation: starting with horizontal exercise (recumbent bike, rowing) and gradual progression.
Pharmacologic Options
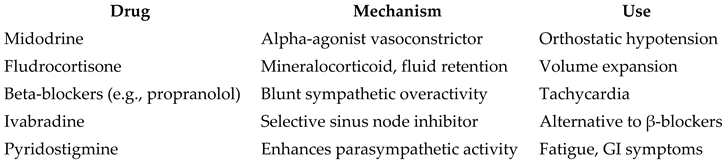
Management should be individualized, ideally with input from cardiology, neurology, and rehabilitation medicine.
Controversies and Knowledge Gaps
Key areas of uncertainty remain:
- Autoimmunity vs central sensitization: Are symptoms immune-mediated or centrally driven?
- Lack of biomarkers: Limits diagnostic specificity and treatment targeting.
- Overlap with ME/CFS: Shared symptomology raises questions about shared pathophysiology.
- Sex Disparities: Why are young women disproportionately affected?
- Heterogeneity: No single phenotype or treatment protocol fits all patients.
Future Research Directions
To advance care and understanding, research should focus on:
- Longitudinal cohort studies to map symptom trajectory and resolution.
- Biomarker discovery (e.g., cytokines, antibodies, HR variability).
- Immunophenotyping to clarify autoimmune contributions.
- Clinical trials of pharmacologic and rehabilitation interventions.
- Neuroimaging to visualize brainstem and autonomic centers.
Integration of omics, wearable technology, and machine learning may enhance phenotyping and predictive modeling.
Conclusion
Dysautonomia has emerged as a prevalent and disabling component of Long COVID, marked by orthostatic intolerance, autonomic imbalance, and impaired quality of life. While multiple pathophysiologic theories exist, none fully account for the heterogeneity seen clinically. Diagnosis remains largely clinical, and treatment requires a multidisciplinary, individualized approach. With mounting evidence and increasing awareness, focused research efforts are urgently needed to refine diagnostic criteria, identify biomarkers, and develop targeted therapies to address this complex and evolving post-viral syndrome.
Author Contributions
I, Brendan Jones, conceptualized the review, conducted the literature search, synthesized the findings, and wrote the manuscript.
Funding
No external funding was received for this work.
Conflict of Interest
The author declares no conflicts of interest.
Use of AI Tools
This manuscript was prepared with the assistance of AI language models to enhance clarity, grammar, and structure. All intellectual content, critical analysis, and interpretation of data remain the sole responsibility of the author.
References
- Gunning WT, Kvale H, Kramer PM, Karabin BL, Grubb BP. Postural orthostatic tachycardia syndrome following COVID-19. Heart Rhythm. 2021;18(9):1760-1765. [CrossRef]
- Di Sante G, Buonsenso D, Rose CD, et al. Immune profile of children with post-acute sequelae of SARS-CoV-2 infection (Long COVID). Cell Death Dis. 2021;12(10):1-9. [CrossRef]
- Dani M, Dirksen A, Taraborrelli P, et al. Autonomic dysfunction in 'long COVID': rationale, physiology and management strategies. Clin Med (Lond). 2021;21(1):e63-e67. [CrossRef]
- Pretorius E, Vlok M, Venter C, et al. Persistent clotting protein pathology in Long COVID/Post-Acute Sequelae of COVID-19 (PASC) is accompanied by increased levels of antiplasmin. Cardiovasc Diabetol. 2021;20(1):172. [CrossRef]
- Swank Z, Senussi Y, Manickas-Hill Z, Yu XG, Li JZ. Persistent circulating SARS-CoV-2 spike is associated with post-acute COVID-19 sequelae. Clin Infect Dis. 2023;76(1):e487-e490. [CrossRef]
- Wallukat G, Hohberger B, Wenzel K, et al. Functional autoantibodies against G-protein coupled receptors in patients with persistent Long-COVID-19 symptoms. J Transl Autoimmun. 2021;4:100100. [CrossRef]
- Blitshteyn S, Whitelaw S. Postural orthostatic tachycardia syndrome (POTS) and other autonomic disorders after COVID-19 infection: a case series of 20 patients. Immunol Res. 2021;69(2):205-211. [CrossRef]
- Raj SR, Guzman JC, Harvey P, et al. Canadian Cardiovascular Society Position Statement on Postural Orthostatic Tachycardia Syndrome (POTS) and Related Disorders of Chronic Orthostatic Intolerance. Can J Cardiol. 2020;36(3):357-372. [CrossRef]
- Miglis MG, Prieto T, Shaik R, Muppidi S. A case report of postural tachycardia syndrome after COVID-19. Clin Auton Res. 2020;30(5):449-451. [CrossRef]
- Wallukat G, Schimke I. Agonistic autoantibodies directed against G-protein–coupled receptors and their relationship to cardiovascular diseases. Front Biosci (Elite Ed). 2014;6:264-278. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



