
Submitted:
03 June 2025
Posted:
03 June 2025
You are already at the latest version
Abstract
Background and Clinical Significance: Spontaneous renal hematoma, also known as Wunderlich Syndrome (WS) is a rare disease, characterized by the acute onset of spontaneous renal hemorrhage into the subcapsular, perirenal, and/or pararenal spaces, without a history of prior trauma. It can be a life-threatening condition due to hemorrhagic shock, consequently, prompt diagnosis and therapeutic approach are essential for favorable outcomes. Treatment ranges from conservative management to surgical intervention. The most common etiologies are neoplasms, vascular diseases but it can be also observed in patients undergoing hemodialysis, especially those with acquired cystic kidney disease or renal cell carcinoma. However, patients with CKD, on particular those on dialysis, have a paradoxical hemostatic potential with increased rates of bleeding, so WS may occur even without the so-called common risk factors. The multifactorial pathogenesis in these patients includes specific coagulation abnormalities and the impaired architectonics of the renal tissue, as well as the use of antithrombotic agents. Case Presentation: We present a case report of a 62-year-old male on chronic dialysis who developed a sudden right-sided lumbar pain and hematuria during dialysis without evidence of prior trauma. Imaging revealed a large subcapsular hematoma of the right kidney. Despite conservative treatment, his condition worsened and the hematoma enlarged, requiring emergency nephrectomy. Pathology confirmed extensive hemorrhage in a nephrosclerotic kidney. Postoperatively, his condition gradually improved. Conclusions: This case highlights the importance of considering WS in hemodialysis patients, and should be included in differential diagnosis of acute abdominal pain.
Keywords:
Wunderlich syndrome
; spontaneous renal hematoma
; hemodialysis
1. Introduction and Clinical Significance
Wunderlich Syndrome (WS) is a rare clinical syndrome characterized by the acute onset of spontaneous renal hemorrhage into the subcapsular, perirenal, and/or pararenal spaces, without a history of prior trauma [1]. The most common etiologies are renal neoplasms and vascular disease, while rarer causes of WS include renal infections, cystic disease, coagulation disorders [1]. Spontaneous renal hematoma (SRH) may also occur in patients with chronic kidney disease (CKD), especially those who undergo hemodialysis treatment. In patients with end-stage renal disease (ESRD), it is most usually associated with acquired cystic kidney disease (ACKD) or renal cell carcinoma (RCC). Additionally, antithrombotic agents used for hemodialysis (HD) and CKD- related hemostasis abnormalities probably act as contributing factors [2].
Clinical significance: We present a case of a 62-year-old male with ESRD on chronic hemodialysis who developed Wunderlich syndrome without traditionally recognisable risk factors.
2. Case Presentation
A 62-year-old male with a history of moderate arterial hypertension and no other comorbidities (including kidney diseases) up to 2019, when severe azotemia was detected while abdominal ultrasonography revealed bilateral nephrosclerosis. Since then he has been undergoing regular hemodialysis treatment via arteriovenous fistula /AVF/. His systemic outpatient therapy consisted of antihypertensive therapy - amlodipine 10 mg q.d., bisoprolol 5mg q.d., as well as dialysis related therapy that includes acetylsalicylic acid 100 mg q.d.,, erythtropoietin supplementation and administration of low- molecular- weight heparin while on dialysis procedures.
During a regular dialysis session, he complained of severe pain in the right lumbar region and hematuria. Detailedly obtained medical history revealed that the patient experienced similar symptoms the previous evening while engaging in routine daily activities. He denied any preceding trauma. On physical examination he presented afebrile, with pale, sweaty skin and arterial hypotension (BP 90/60 mmHg). Bedside abdominal ultrasound demonstrated subcapsular free fluid of the right kidney. Emergency contrast-enhanced computed tomography (CT) confirmed a massive subcapsular hematoma of the right kidney (size 10.8 × 8.6 cm) (Figure 1), infiltrating the retroperitoneal fat tissue. The patient was admitted to the Urology clinic.
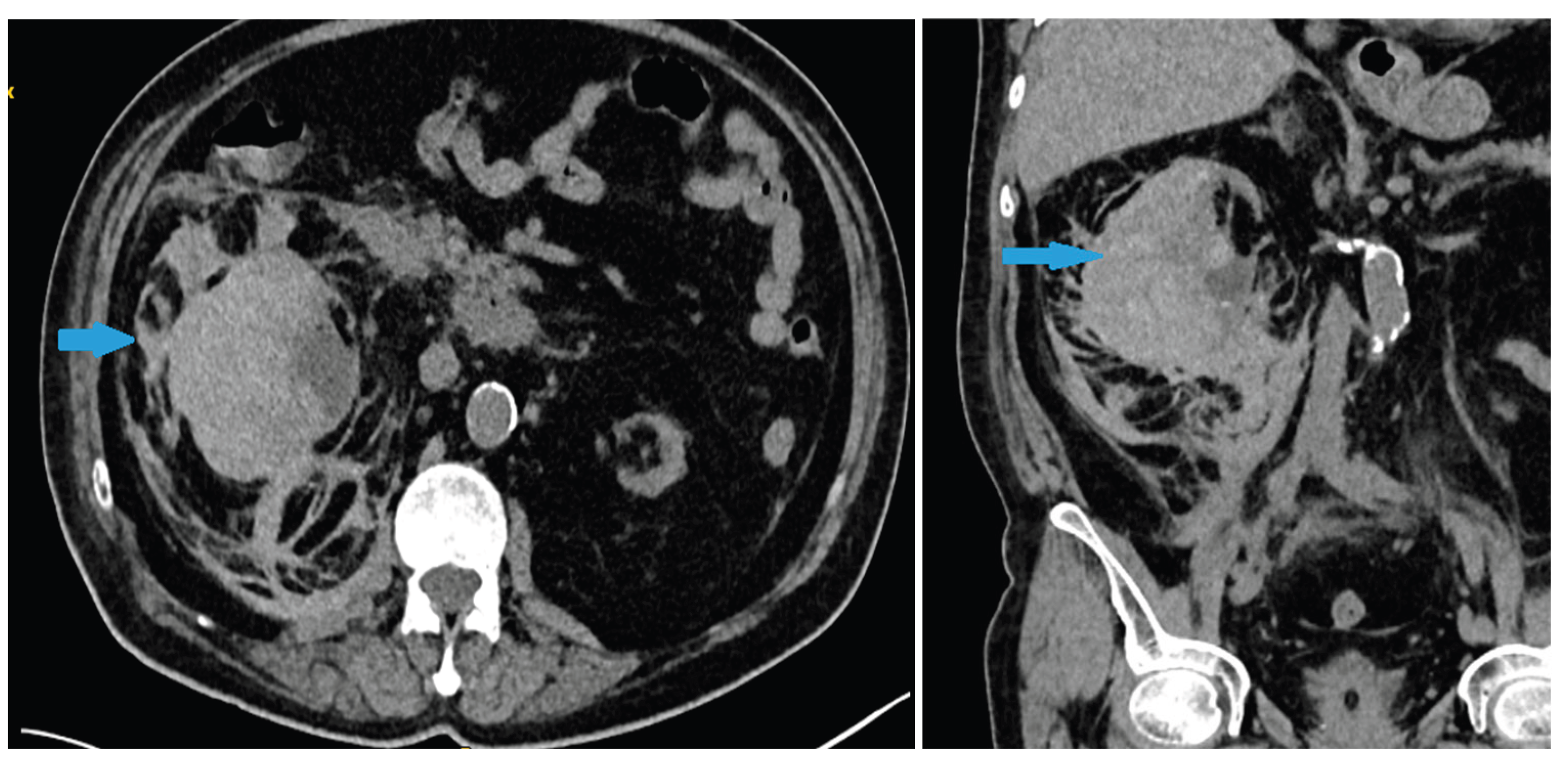
Laboratory tests revealed a decrease in hemoglobin levels to 78 g/L (a drop of 40 g/L compared to previous results few weeks prior) with normal coagulation tests, without thrombocytopenia, other laboratory results were also unremarkable with the exception of azotemia. Conservative therapy with blood transfusions, antibiotics, hemostatic agents, and analgesics was initiated. On the second day of hospitalization, laboratory results indicated worsening of the anaemia and a follow-up abdominal CT showed an increase in hematoma size and the presence of a retroperitoneal blood collection (Figure 2a,b ). An emergency open surgery was performed. Intraoperatively a transverse lesion was identified in the middle part of the right kidney. The right kidney was removed, and the whole specimen was sent for pathological examination. The histology findings confirmed nephrosclerotic kidney with extensive subcapsular parenchymal hemorrhages and marked chronic tubulointerstitial nephritis. In the following days, the patient continued his treatment with blood transfusions, leading to improvement and normalization of hematologic parameters.
3. Discussion
Renal hematomas are relatively rarе but clinically significant conditions. The primary causes of renal hematomas are categorized as traumatic, spontaneous and iatrogenic. A retrospective review from 2011 to 2021, reported the distribution as follows: traumatic (21%), spontaneous (32%), and iatrogenic (47%) [3]. Spontaneous renal hematoma, also known as Wunderlich Syndrome, was first described by Bonet in 1679 and later by Wunderlich [1]. A meta-analysis of SRH cases from 1985 to 1999 identified 165 cases, while a recent systematic review identified an additional 102 cases [4].
In general, renal neoplasms - most commonly benign angiomyolipomas and renal cell carcinoma (RCC), account for 60–65% of cases, while vascular diseases (such as vasculitis, renal artery aneurysms, arteriovenous malformations, and renal vein thrombosis) represent the second most common cause, comprising 20–30% of cases [1]. Rare causes of WS include renal infections, cystic diseases, nephrolithiasis, pregnancy, coagulation disorders, and anticoagulation therapy [1].
CKD and especially ESRD are a recognizable, but rare causes for Wunderlich syndrome [5]. CKD is associated with a 1.5-fold increased bleeding risk compared to patients with normal kidney function [6]. Increased bleeding is thought to be driven principally by platelet dysfunction, with additional contributions from alterations in the coagulation cascade with deranged von Willebrand factor and platelet interactions, increased nitric oxide and impaired fibrinolysis, as well as the sequelae of anemia [7]. The prevalence of abnormal bleeding time is higher as eGFR declines. [8] Moreover, clinically relevant bleeding in CKD patients has been reported in 24–50% of patients on HD, with a >2-fold increased prevalence compared to non–dialysis-dependent CKD patients [7]. The frequency of SRH is reported to be higher with HD than with peritoneal dialysis [9]. The incidence of WS in dialysis is 1-3% with male predominance (74.5%) [9].
In individuals with ESRD (particularly on hemodialysis), acquired cystic kidney disease (ACKD) and cyst rupture are the leading causes of WS. Studies show that 74% of patients on hemodialysis for over four years develop ACKD. 80% of RCC cases are linked to ACKD [10]. However, in our patient, neither pathologic examination nor imaging studies showed evidence of ACKD or RCC.
Chronic inflammation and oxidative stress associated with ESRD weaken renal tissues and vasculature, making the kidney more susceptible to spontaneous bleeding [11]. Probably, the observed transverse renal lesion is highly attributable to compromised renal and parenchymal integrity and vascular fragility.
Anticoagulation use, regardless of its indications seems to be a factor for SRH [9]. Heparinization during dialysis can possibly explain the occurrence of SRH during or shortly after hemodialysis sessions [2,9]. However, our patient’s symptoms began a day before dialysis—two days after his last session—indicating no circulating heparin. Although antiplatelet agents have also been reported in some cases, they are less frequent cause for SPH [9].Moreover, vascular access seems to be an additional reason for increased risk of bleeding, where it has been established that dialysis catheters are linked to coagulation changes and higher bleeding risk, but our patient uses an AV fistula as a vascular access [12].
In conclusion, we postulate that CKD and dialysis by themselves are a sufficient cause for the occurrence of Wunderlich syndrome due to the above- mentioned specific coagulation abnormalities and the impaired architectonics of the renal tissue, with antithrombotic medications acting as an additional contributing factor.
Clinically, patients may present with isolated flank pain (67%), hematuria (40%), hypovolemic shock (27%), and Lenk's triad (about 20%) [1]. SRH should be strongly suspected in every patient with ESRD (particularly on hemodialysis) presenting with more or less severe abdominal or flank pain, hypotension, and a sudden onset drop of hemoglobin [2]. Laboratory findings include anemia and hematuria. Meta-analysis results indicate that CT is 100% sensitive for detecting retroperitoneal hemorrhage and is superior to ultrasound for identifying underlying renal pathology. Thus, CT remains the imaging modality of choice, allowing precise measurement and monitoring of hematomas [13]. When a CT scan does not identify underlying cause, angiography may be needed [14]. It is particularly useful when the CT findings are inconclusive and further investigation is required to identify the cause of the hematoma.
Initial reports suggested radical or modified nephrectomy for all cases. However, based on recent case series, conservative management may be a reasonable approach [10]. Conservative treatment may prevent unnecessary nephrectomy in patients with benign disease and stable condition, additionally, such an approach is recommended when diagnostic studies fail to show significant pathology [13]. Selective arterial embolization is another method for controlling active bleeding, particularly in hemodynamically unstable patients [10]. Indications for surgical management include progressive anemia, a palpable retroperitoneal hematoma, and symptoms of peritoneal irritation, as well as suspicion of malignancy [13]. Initially, our patient was managed conservatively given his stable condition. However, his condition deteriorated with ongoing bleeding and hematoma enlargement. Considering the risks of the procedure and the lack of benefit in preserving the kidney, the patient underwent a right nephrectomy. Despite the life-threatening nature of WS, the patient achieved full recovery due to expeditious diagnosis and therapeutic management.
4. Conclusions
WS continue to be a clinical and therapeutic dilemma. The presented case underscores the importance of physicians to maintain high vigilance for spontaneous renal hemorrhage despite the rarity of this condition. Patients receiving dialysis therapy constitute a distinct high-risk group due to the number of risk factors associated with the dialysis itself. Early surgical intervention proved lifesaving in this instance, though it highlights the challenges of managing catastrophic bleeding complications in this fragile population.
Author Contributions
E.A. collected clinical information, drafted the manuscript, and was responsible for the critical revision of the manuscript for important intellectual content. N.D. , M.V. and E.V. supported the data collection and helped draft the manuscript. All authors participated in revising the draft manuscript and approving the final manuscript.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki. Ethical approval is not required for this study in accordance with local or national guidelines.
Informed Consent Statement
Written informed consent has been obtained from the patient to publish this paper.
Data Availability Statement
All data generated or analyzed during this study are included in this article and its online supplementary material. Further inquiries can be directed to the corresponding author.
Conflicts of Interest
The authors have no conflicts of interest to declare.
References
- Shah, J.N.; Gandhi, D.; Prasad, S.R.; Sandhu, P.K.; Banker, H.; Molina, R.; Khan, M.S.; Garg, T.; Katabathina, V.S. Wunderlich Syndrome: Comprehensive Review of Diagnosis and Management. Radiographics 2023, 43, 1–15. [Google Scholar] [CrossRef]
- Tonolini, M.; Ierardi, A.M.; Carrafiello, G. Letter to the Editor: Spontaneous Renal Haemorrhage in End-Stage Renal Disease. Insights Imaging 2015, 6, 693–695. [Google Scholar] [CrossRef] [PubMed]
- Lynch, E.; Gaines, J.; James, J.; Aro, T.; Hoenig, D.; Okeke, Z.; et al. Informing an Approach to the Subcapsular Renal Hematoma (SRH): A Ten-Year Review of the Natural History and Progression of SRH. J. Urol. 2023, 209 (Suppl. 4), e111. [Google Scholar] [CrossRef]
- Paudel, S.; Steinberg, P.; Denker, B.; et al. Spontaneous Renal Hemorrhage: Case Report and Review of the Literature. Res. Sq. 2022, Preprint. [Google Scholar] [CrossRef]
- Marquez, M.M.A.; Lim, A.S.; Guiritan, A.T.R. Wunderlich Syndrome in a Patient with ESKD Diagnosed with COVID-19: A Case Report: TH-PO1150. J. Am. Soc. Nephrol. 2024, 35. [Google Scholar] [CrossRef]
- Ocak, G.; Rookmaaker, M.B.; Algra, A.; de Borst, G.J.; Doevendans, P.A.; Kappelle, L.J.; Verhaar, M.C.; Visseren, F.L.; van der Graaf, Y.; Grobbee, D.E.; et al. Chronic Kidney Disease and Bleeding Risk in Patients at High Cardiovascular Risk: A Cohort Study. J. Thromb. Haemost. 2018, 16, 65–73. [Google Scholar] [CrossRef] [PubMed]
- Nunns, G.R.; Moore, E.E.; Chapman, M.P.; Moore, H.B.; Stettler, G.R.; Peltz, E.; Burlew, C.C.; Silliman, C.C.; Banerjee, A.; Sauaia, A. The Hypercoagulability Paradox of Chronic Kidney Disease: The Role of Fibrinogen. Am. J. Surg. 2017, 214, 1215–1218. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.Y.; Oak, C.Y.; Kim, M.J.; Kim, C.S.; Choi, J.S.; Bae, E.H.; et al. Prevalence and Associations for Abnormal Bleeding Times in Patients with Renal Insufficiency. Platelets 2013, 24, 213–218. [Google Scholar] [CrossRef] [PubMed]
- Malek-Marín, T.; Arenas, D.; Gil, T.; Moledous, A.; Okubo, M.; Arenas, J.J.; Morales, A.; Cotilla, E. Spontaneous Retroperitoneal Hemorrhage in Dialysis: A Presentation of 5 Cases and Review of the Literature. Clin. Nephrol. 2010, 74, 229–244. [Google Scholar] [CrossRef] [PubMed]
- Kawahara, T.; Kawahara, K.; Ito, H.; Yamaguchi, S.; Mitsuhashi, H.; Makiyama, K.; Uemura, H.; Sakai, M.; Kubota, Y. Spontaneous Renal Hemorrhage in Hemodialysis Patients. Case Rep. Nephrol. Urol. 2011, 1, 1–6. [Google Scholar] [CrossRef] [PubMed]
- El Abidi, H.; Ibrahimi, A.; El Aboudi, A.; Mikou, M.A.; Boualaoui, I.; Labbi, Z.; El Aoufir, O.; Fikri, M.; El Sayegh, H.; Nouini, Y. Management of Spontaneous Subscapular Renal Hemorrhage: A Multidisciplinary and Hybrid Approach to Wunderlich Syndrome. Radiol. Case Rep. 2025, 20, 3106–3110. [Google Scholar] [CrossRef] [PubMed]
- Fouda, D.; Lionel, F.; Elimby, E.; Dongmo, N.; Bitoungui, A.; Te, V.; Ngouadjeu. Evaluation of Bleeding Risk by Hemostatic Parameters in Hemodialysis at the Douala General Hospital. Open J. Nephrol. 2023, 13, 31–38. [Google Scholar] [CrossRef]
- Kim, J.-K.; Ha, S.; Lee, J.W. Bilateral Spontaneous Perirenal Haemorrhage in a Patient on Haemodialysis. NDT Plus. 2009, 2, 412–414. [Google Scholar] [CrossRef]
- Baishya, R.K.; Dhawan, D.R.; Sabnis, R.B.; Desai, M.R. Spontaneous Subcapsular Renal Hematoma: A Case Report and Review of Literature. Urol. Ann. 2011, 3, 44–46. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
The blue arrow indicates massive subcapsular hematoma of the right kidney (size 10.8 × 8.6 cm) /.
Figure 1.
The blue arrow indicates massive subcapsular hematoma of the right kidney (size 10.8 × 8.6 cm) /.
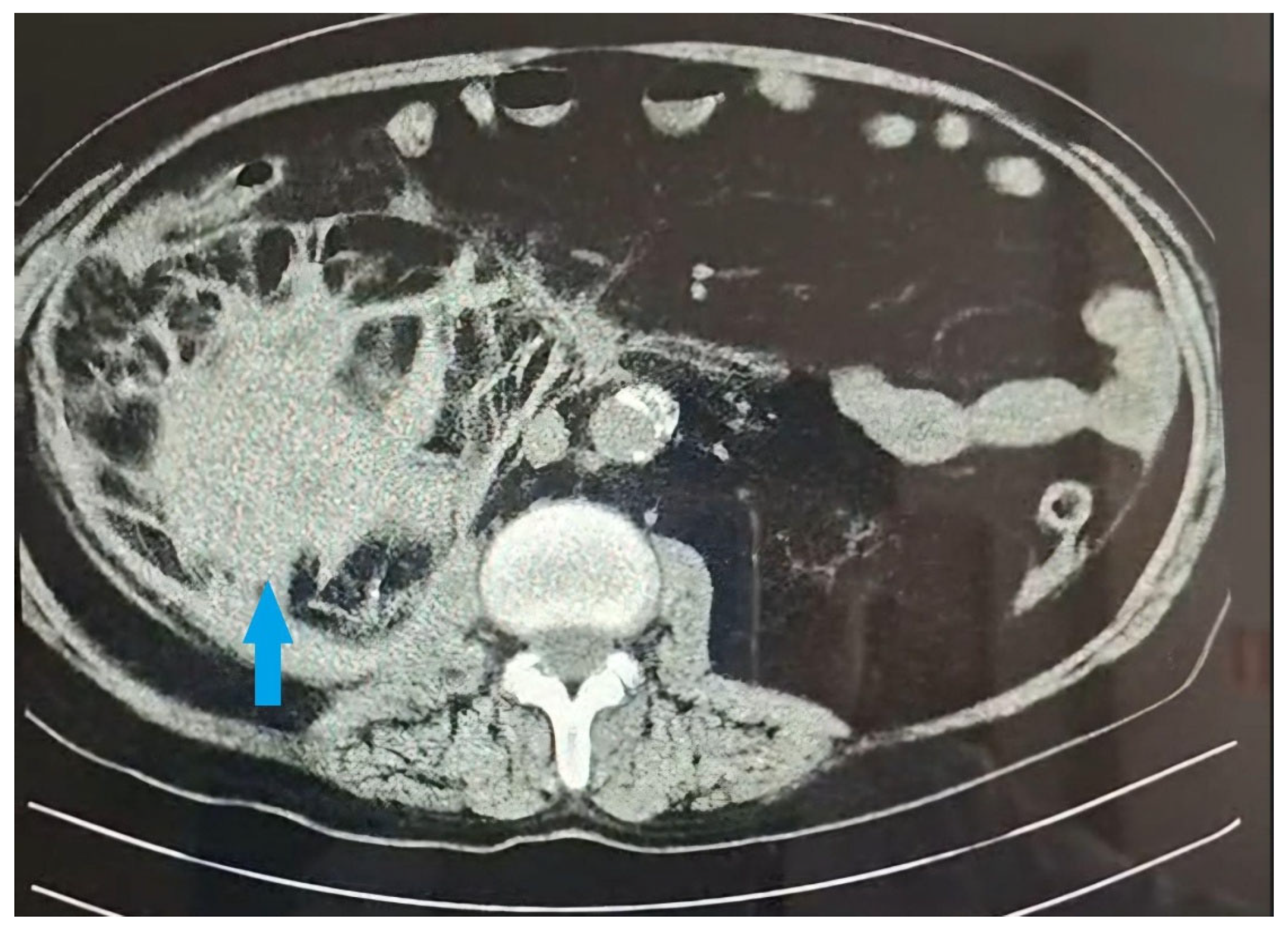
Figure 2.
a,b The blue arrows indicates CT scan on second day- showed an increase in hematoma size 12.37x6.23cm and the presence of a retroperitoneal blood collection.
Figure 2.
a,b The blue arrows indicates CT scan on second day- showed an increase in hematoma size 12.37x6.23cm and the presence of a retroperitoneal blood collection.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



