Submitted:
30 May 2025
Posted:
04 June 2025
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
The therapeutic target of COVID-19 is focused on controlling inflammation and preventing fibrosis. Collagen-polyvinylpyrrolidone (collagen-PVP) and pirfenidone have the ability to control the cytokine storms observed in rheumatic and fibrotic disorders. Here, we explore separately their therapeutic effects on the early treatment of 26 patients with severe COVID-19, compared to 10 controls treated with dexamethasone alone. Our results showed that hospital stay, quick COVID-19 severity index (qCSI) and admission to the ICU were statistically significantly lower (P<0.02) in treated patients with collagen-PVP or pirfenidone; only collagen-PVP normalised serum glucose at discharge. Since the intracellular mechanism of action of pirfenidone is partially known, we performed a human genome microarray assay with total RNA isolated from fibroblast and monocyte cultures treated with collagen-PVP. Ingenuity Pathway Analysis showed that cell cycle, inflammation, and cell surface-extracellular matrix interactions could be regulated by collagen-PVP by downregulation of proinflammatory cytokines, while Th2 anti-inflammatory response signaling could be upregulated. Furthermore, downregulation of some of the genes involved in nitric oxide production showed a possible control for JAK, in the IFN-γ pathway, allowing the possibility of controlling inflammation through the JAK/STAT pathway, as has been observed for pirfenidone and other immunomodulators, such as ruxolitinib.
Keywords:
Collagen-polyvinylpyrrolidone
; pirfenidone
; inflammation
; SARS-CoV-2
1. Introduction
The SARS-CoV-2 pandemic that causes COVID-19 disease is life-threatening and challenges even the best health systems in the world[1,2]. Cytokine storms are considered the main cause of severity and death in patients with COVID-19, while progressive pulmonary fibrosis derived from acute respiratory distress syndrome (ARDS) has a worse prognosis, both being possible therapeutic targets[3]. The symptoms of COVID-19 are consistent with an acute inflammatory reaction and pneumonia that progresses to ARDS in a subset of patients[4]. Progressive dyspnea and hypoxia are the main reasons for hospitalization[5]; 30% of patients require admission to the intensive care unit (ICU) and 10-17% undergo intubation[4]. In laboratory studies, neutrophilia and lymphopenia were correlated with the severity of the disease[5,6]. The cytokine profile in patients with COVID-19 reveals significant increases in proinflammatory cytokines that correlate with severity[4,7]. Cytokine storm is a life-threatening immune syndrome characterised by elevated activation of immune cells and circulating proinflammatory cytokines, lymphopenia, thrombosis, and massive infiltration of mononuclear cells into multiple organs[8], and is considered the leading cause of disease severity and death in patients with COVID-19[3]. These patients have a failure of negative feedback mechanisms that prevent hyperinflammation and overproduction of inflammatory cytokines, leading to respiratory dysfunction. During SARS-CoV-2 infection, a wide variability in human responses has been observed. In mild and asymptomatic COVID-19, a slight delay in innate and adaptive immune responses has been determined, where the cause has been associated with low levels of type I and III interferons (IFNs); however, this effect is magnified in severe COVID-19. The lack of IFN allows virus replication and the prime of the immune response is delayed, although in the following phase, the levels of proinflammatory cytokines increase above the normal innate response[9]. Similarly, with low levels of IFN, epithelial cells, macrophages, and dendritic cells express high levels of proinflammatory cytokines[10] that promote the priming of the lung endothelium by cytokine receptors that activate signaling pathways related to NF-kB, MAPK, STAT3 and MyD88; therefore, endothelial cells overexpress adhesion molecules, such as selectins and adhesion proteins that facilitate leukocyte recruitment[11] that trigger cytokine storm. Specifically, during SARS-CoV-2 infection, IL-1β, IL-6, IL-8, IL-10, IL-12, IP-10, MCP-1, TNF-α and IFN-γ are elevated, although their levels vary according to the genetic characteristics of the patients and the underlying comorbidities[12]. Furthermore, in COVID-19, many of the patients who develop ARDS and survive to the acute phase of the disease, a substantial proportion die as a result of progressive pulmonary fibrosis resulting from inflammation and long-term deterioration of lung function. The pathogenesis of pulmonary fibrosis includes the deregulated release of matrix metalloproteinases during the inflammatory phase, resulting in epithelial and endothelial injury with uncontrolled fibroproliferation[13,14]. Based on experience with other diseases characterised by a cytokine storm, early intervention is essential to avoid life-threatening tissue damage. In this regard, different treatment options have been considered to limit inflammatory overactivation, such as corticosteroids, monoclonal antibodies directed against certain cytokines and/or their receptors, antiviral drugs, vaccines, oligonucleotides, peptides, and interferons[15]. Antifibrotic therapies could be valuable in preventing severe COVID-19 in patients with idiopathic pulmonary fibrosis and could play a role in the prevention of fibrosis after SARS-CoV-2 infection [16]. An option could be collagen-polyvinylpyrrolidone (collagen-PVP) with known properties to reduce pro-inflammatory cytokines and fibrosis[17,18]. Another option could be pirfenidone, an anti-inflammatory and antifibrotic drug approved for the treatment of idiopathic pulmonary fibrosis that limits inflammation and subsequent pulmonary fibrosis [19]. In this sense, due to its anti-inflammatory and antifibrotic mechanisms of action, the use of collagen-PVP and pirfenidone have been considered for this purpose.
2. Materials and Methods
2.1. Clinical Follow-Up
A prospective and longitudinal clinical trial was conducted with patients infected with SARS-CoV-2, between February 2020 and June 2021 at the General Hospital 'Dr. Nicolás San Juan', Health Institute of the State of Mexico (ISEM), Toluca, Mexico. The patient sampling method was performed for convenience in sequential order. All of them adults, hospitalized, and COVID-19 confirmed by the polymerase chain reaction (PCR) test, with total bilirubin ≤1.5 and alanine transaminase (ALT) >5 times the upper limits relative to normal values. Patients were excluded if treated with biological antirheumatic drugs, disease modifiers (DMARD) or other immunosuppressive agents; patients who required continuous therapy with systemic corticosteroids at a dose greater than 10 mg of prednisone per day or equivalent; pregnant women, nursing or intending to become pregnant during the study; patients who needed continuous treatment with strong inhibitors of CYP1A2 inhibitors (that is, Fluvoxamine, Enoxacin), calculated creatinine clearance (or estimated glomerular filtration rate) <10 ml/min or patients requiring renal replacement therapy.
For the anthropometric evaluation of each patient, the weight record and blood pressure of the participants were evaluated electronically in bed; height was measured with a conventional stadiometer and body mass index (BMI) was calculated. Body temperature, heart rate, respiratory rate, pSO2%, PCO2 and pO2 were monitored during hospitalisation of the patient. Hematic biometry, serum concentrations of glucose, uric acid, cholesterol and triacyl glycerides, blood gas, blood urea nitrogen, and creatinine were routinely performed from blood samples obtained in the fasting state according to the International Federation of Clinical Chemistry and Medical Laboratories (IFCC). Serum samples were obtained at the beginning and after 7 days of treatment and stored at -80°C for further evaluation of representative levels of Th1, Th2 and Th17 cytokines (IFN-γ, TNF-α, IL-2, -4, -10, -13 and -17) according to the manufacturer (R&D Systems, Inc. Minneapolis, MN, USA). The Kirby index, the quick COVID-19 Severity Index (qCSI), and the shock index were evaluated at admission and discharge.
Upon acceptance with the signing of informed consent, patients were sequentially assigned to one of the following treatments: pirfenidone (KitosCell tabs, CellPharma S de RL de CV. Mexico City, Mexico) 1,200mg of oral q12h or collagen-PVP (Fibroquel, Aspid SA de CV, Mexico City, Mexico) 2ml intramuscular q24 h, both for 7 days; control group was integrated by patients without pirfenidone or collagen-PVP. Furthermore, a general management protocol was always established according to clinical practice guidelines for each added disease. Briefly, all patients received 6mg of dexamethasone (intravenously) and 40 or 60mg of enoxaparin (subcutaneously, according to the patient's weight) once daily; 1g of paracetamol (intravenously) could be included when necessary.
2.2. Ethics
This trial was accepted by the Research Ethics Committee of the "Mónica Pretelini Sáenz" Maternal-Perinatal Hospital (HMPMPS) (code 2020-12-712), with current registration in the National Bioethics Commission (CONBIOETICA) and by the Research Committee of the same Hospital with registration in the Comisión Federal para la Protección contra Riesgos Sanitarios (COFEPRIS). Furthermore, the trial was registered on ClinicalTrial.gov with the ID: NCT06585319. The research was carried out under the deontological considerations recognised by the Declaration of Helsinki (Fortaleza, Brazil, 2013), and according to the level of intervention, it is considered a study with greater than minimal risk.
2.3. Human Genome Microarray Assay for In-Vitro Treated Fibroblasts and Monocytes with Collagen-PVP
The immortalized fibroblasts hTERT-BJ1 were cultured with Dulbecco's modified Eagle's Medium (Gibco, Life Technologies. NY, USA) supplemented with 10% foetal bovine serum (FBS, Gibco), 2mM L-glutamine (Gibco), 100 U/ml penicillin and 100μg/ml streptomycin (Gibco). The human monocyte cell line (THP-1) was cultured with RPMI-1640 medium (Gibco), supplemented with 10% FBS, 1mM sodium pyruvate, 0.1mM non-essential aminoacids, 0.1mM of glutamine, 100 U/ml penicillin and 100μg/ml streptomycin (Gibco). Cultures were kept at 37°C in a 5% CO2 atmosphere. Adherent THP-1 cells were serially subcultured until the appropriate cell concentration was reached to perform the experiment. Despite the experience in in vitro cell tolerance to different concentrations of collagen-PVP (1-10%)[20,21], prior to the genome microarray assay, the viability of fibroblast and monocyte cultures was evaluated by incorporation of thymidine. For collagen-PVP treatments, 2x105 cells, fibroblasts and monocytes, were seeded in 5ml of their corresponding medium in T-25 culture flasks (Corning, Glendale, AZ, USA) and kept for 24h at 37°C and 5% CO2. Cultures were incubated for 3h with FBS-free medium and then with 3% collagen-PVP prepared in the corresponding medium without FBS and incubated for 24h at 37°C and 5% CO2. The medium was removed and the flasks were washed with phosphate saline buffer. Total RNA was isolated from collagen-PVP treated and control cells using the TRIzol method (Invitrogen™. Thermo Fisher Scientific Inc. Waltham, MA, USA). RNA expression was analysed using the Genechip Human Mapping 10K v1.0 microarray developed at the Core Microarray Facility at the Instituto de Fisiología Celular, UNAM. GenArise software was used for the quantification of microarray data with a cut-off value ≥2.0 for up-regulation and ≤-2.0 for down-regulation. The target genes were analysed using DAVID Bioinformatics Resources 6.8 (NAID, NIH, Bethesda, MD, USA). For the analysis of biological function and signalling regulation, an enrichment analysis of the up- and downregulated genes was performed using the Ingenuity Pathway Analysis (IPA, Ingenuity Systems Inc., Redwood City, CA, USA). General Z-score values and raw data can be downloaded with the following GEO accession numbers GSE262736 and GSE262737. IPA generates CNs relying on a highly curated knowledge-based source (the Ingenuity Knowledge Base, IKB). IKB reports a series of experimentally observed cause-effect relationships related to transcription, expression, activation, molecular modification, binding events, and transport processes. Since these interactions have been experimentally measured, they can be associated with a definite direction of the causal effect, either activation or inhibition of the processes mentioned above at a whole genome network-wide level. Further methodological details of the CN analysis that we performed are described[22].
2.4. Statistical Analysis
From clinical and biochemical data, frequency measures (percentage) were initially obtained for categorical variables, while median values ± standard deviation (SD) for continuous variables. The stratified variables were then compared according to the type of treatment using the chi-square test (χ2) and the analysis of variance (ANOVA) for categorical variables, while the Kruskal-Wallis test was performed for continuous. The normal distribution was verified by the Shapiro-Wilk test. Significantly statistically different values were those with a P value ≤ 0.05. Stata v13.0 (StataCorp. TX, USA) was used to perform all statistical analyses.
3. Results
3.1. Treatment of Patients with COVID-19 with Collagen-PVP or Pirfenidone Improves Some of the Disease Indicators
Thirty-six patients were enroled in this work and all maintained the same base treatment (dexamethasone) during their hospitalisation period. Two groups of 15 and 11 patients received one of the two immunomodulators evaluated, collagen-PVP or pirfenidone, respectively. Since all patients were received by the hospital under severe infection conditions, 41% of them died during the trial due to complications of COVID-19 disease and no statistically significant differences were associated with the treatment group (Table 1).

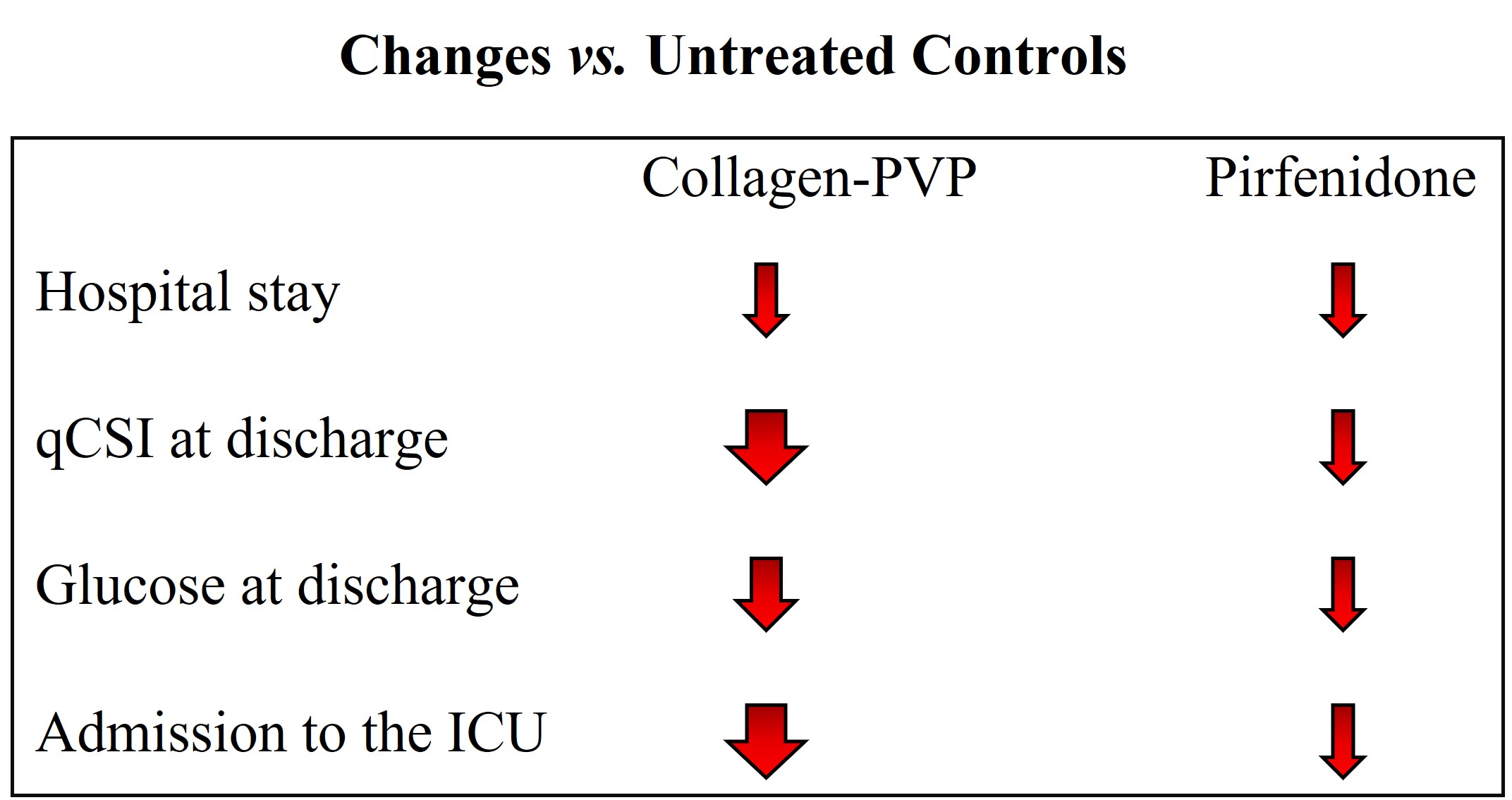
Although the reason for discharge did not show differences between the groups, the mean follow-up stay (inpatient stay) indeed exhibited statistically significant differences when patients were treated with immunomodulators; collagen-PVP and pirfenidone, 12.7 and 13.2 days, respectively, vs. 24.1 days for the control group (p=0.015, Table 2). Discharge qCSI and serum glucose indicated statistically significant differences when the 3 groups were compared (p<0.02 for both indicators, Table 2). In all cases, the values increased from collagen-PVP to controls, where no statically significant differences were observed between immunomodulator treatments. In particular, at discharge, glucose values were normal only in the group of patients treated with collagen-PVP.
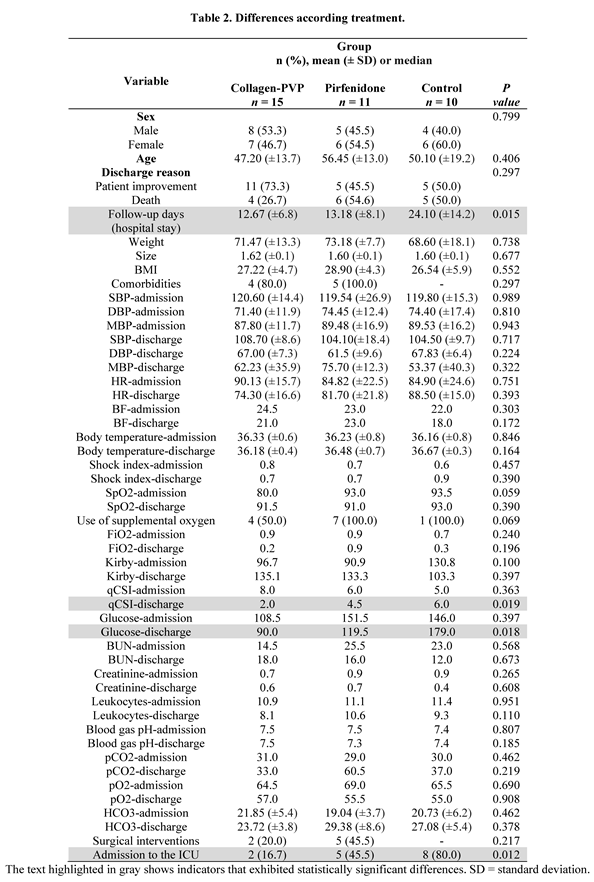
Finally, it was more common for patients in the control group to be admitted to the intensive care unit than for those treated with immunomodulators (p=0.012) and again, in the same proportion as before, the lowest number of patients was for those who underwent collagen-PVP treatment (Table 2). Regarding the evaluation of serum cytokines, their blood values were below the detection levels of the kits in the majority of patients; IFN-γ (5.7pg/ml), TNF-α (6.2pg/ml), IL-2 (7pg/ml), IL-4 (10pg/ml), IL-10 (3.9pg/ml), IL-13 (57.4pg/ml) and IL-17 (15pg/ml), in such a biochemical analysis of cytokines involved in systemic inflammation was not available.
3.2. Human Genome Microarray Assay for In-Vitro Treated Fibroblasts and Monocytes with Collagen-PVP.
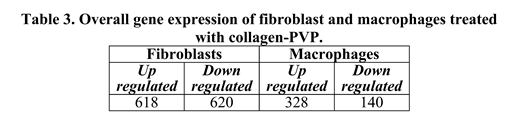
Since immunomodulators have shown a down-regulation of inflammation during COVID-19 treatment[23], including pirfenidone[24], we considered performing a presumptive analysis of gene expression after collagen-PVP treatment in stromal and immune cells. Both cell types showed interesting changes in gene expression after collagen-PVP treatment, although fibroblasts had the biggest changes (twice as up-or down-regulated as monocytes, Table 3).
In particular, monocytes treated with collagen-PVP increased the number of genes related to inflammation that involved the Th2 response and the signalling of cell extracellular matrix receptors (Table 4).
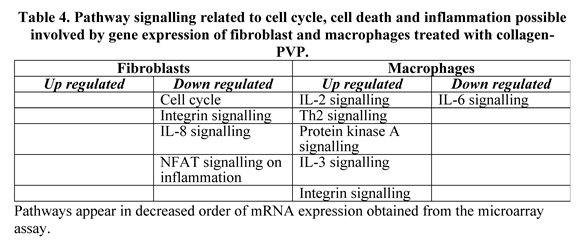
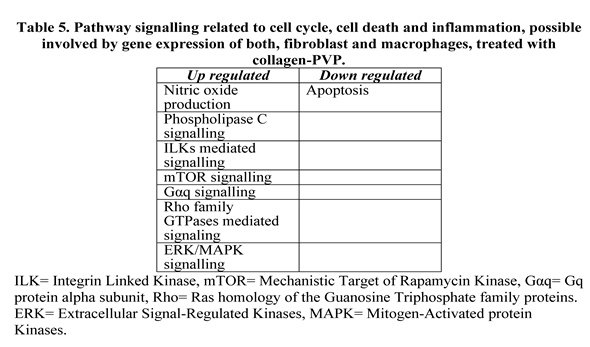
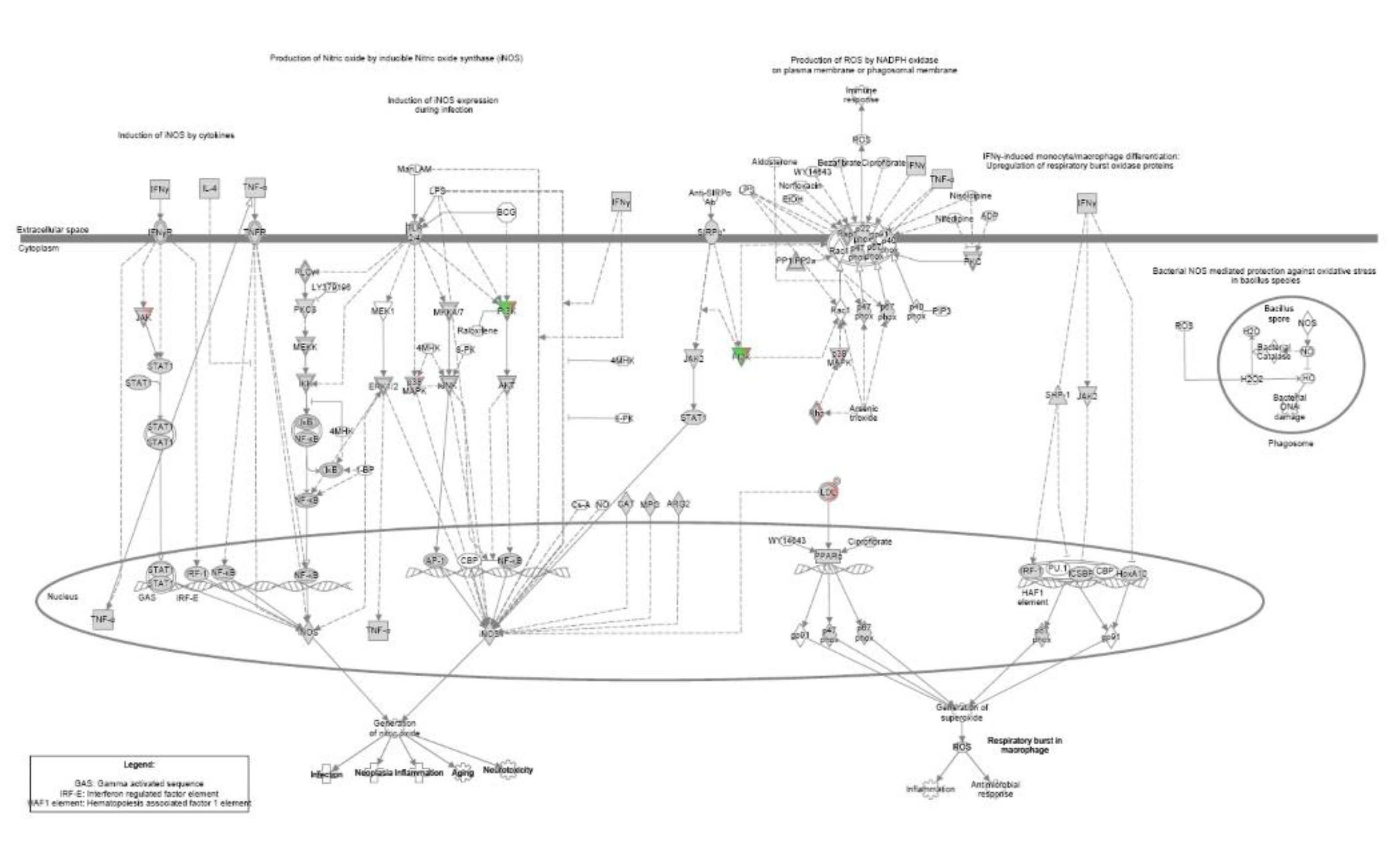
On the other hand, fibroblasts negatively regulated cell cycle, inflammation, and cell extracellular matrix receptor signalling (Figure A1 and 2 and Table 4), while monocytes decreased those related to IL-6 signalling (Figure A3 and Table 4). Furthermore, the shared signalling pathways between fibroblasts and monocytes are involved in the production of nitric oxide (Figure A4), second messenger downregulation in the signalling of the extracellular matrix receptor (Figure A2) and the cell cycle and differentiation (Table 5). Among the genes involved in the production of nitric oxide by inducible nitric oxide synthase, the IPA analysis showed a possible control for JAK, in the pathway activated by IFN-γ through its receptor, IFN-γR, letting the possibility of controlling inflammation also through the JAK/STAT pathway (Figure A4).
4. Discussion
In this work, patients with severe COVID-19 were treated with different combined strategies and the basal administration of dexamethasone. When corticosteroids have been used for the treatment of COVID-19, methylprednisolone is used primarily. Treatment with methylprednisolone reduced the risk of death (HR, 0.38; 95% CI, 0.20-0.72) among patients with ARDS, suggesting its possible intervention for the cytokine storm[25]. Although corticosteroids should not be the main focus, their administration decreased the admission rate to the intensive care unit, treated patients showed a lower need for mechanical ventilation, a shorter hospital stay, and better survival rates [26]. Desperate efforts to control the cytokine storm in patients with severe COVID-19 led to the use of specific immunomodulators, such as anakinra[27] and rilonacept[28], in order to regulate the expression of IL-1; also monoclonal antibodies against IL-6, such as tocilizumab[29] and sarilumab[30], and IFNβ-1[31]. Tocilizumab[32], alone or in combination with anakinra and immunoglobulin, or the addition of hydroxychloroquine and chloroquine, mesenchymal stem cells, and plasma from convalescent patients have shown relatively positive results because the reduction in ferritin, C-reactive protein, D-dimer, together with an improvement in vascular and respiratory signs and symptoms[33]. On the other hand, the use of remdesivir, based on its antiviral properties, and methylprednisolone as an unspecific immunomodulator, have demonstrated efficacy in the treatment of pneumonia associated with COVID-19; however, bacterial infection has been associated with this treatment, and therefore in some cases the treatment must be retired early[34]. Since there is no specific treatment for early and/or late severe COVID-19, combined strategies are still required. From corticosteroids to the most specific immunomodulator, all drugs used for COVID-19 treatment have shown different side effects, mostly related to immunosuppression, as well as kidney, liver, or heart damage[35]. In this work and others, it has been observed that patients with severe COVID-19 treated with collagen-PVP[36,37] or pirfenidone[38,39], in combination with dexamethasone, anticoagulant, and analgesic/antipyretic, showed improved pneumonia and inflammation, without the side effects derived from cytokine storm control observed with other drugs[35]. Hyperglycaemia is a secondary effect observed in several patients during or after COVID-19[40], but it was striking in this work that glucose values at the time of discharge were normal only when patients were treated with collagen-PVP, while the values observed for the pirfenidone and control groups maintained higher levels of glucose that were statistically significant compared to the collagen-PVP group. Another important variable measured during the study was the use of supplemental oxygen, although it was only close to being statistically significant different among the groups, where the sample size could have played a critical role for them. Biochemically, high levels of circulating cytokines were associated with SARS-CoV-2 infection, COVID-19 patients expressed higher levels of Th1 cytokines, but they also have Th2 immune profile cytokines, which biologically antagonise Th1 or the early proinflammatory response[41]. Despite several works that have reported serum cytokines from patients with COVID-19 in different states of disease severity, the data are ambiguous due to the high variability of the results; some reported values in units of picograms/ml[42], while others found hundreds of picograms/ml[43]. In this work, cytokine levels were undetectable in most patients, due to the sensitivity of the ELISA kits we used.
As mentioned above, pirfenidone is a drug capable of controlling inflammation[44] and pulmonary fibrosis[45]. This pharmacological property led investigators to consider its administration in patients with COVID-19[24], in such a way that pirfenidone has been considered for early and post-COVID-19 treatments. The mechanism involved in the regulation of inflammation by pirfenidone involves the regulation of proinflammatory cytokine regulation[24] and the JAK2/STAT3 pathway[46]. Our group[17] and others[47,48] have shown that collagen-PVP exhibits fibrolytic and inflammation control effects in different tissues and organs. However, intracellular mechanisms with respect to the effects of collagen-PVP have not yet been analysed, except for the decrease in integrin α2 vs. control, when human fibroblasts were cultured with 3% collagen-PVP[20]. Recently, collagen-PVP (named polymerised type I collagen) was published to downregulate STAT1 phosphorylation in type 1 macrophages, differentiated from the THP-1 monocyte cell line, where apparently the effect was driven by the binding of collagen-PVP to the leukocyte-associated immunoglobulin-like receptor 1 (LAIR1)[49]. Although these results match the IPA analysis of our work regarding JAK/STAT pathway regulation, and consequently support our hypothesis, it remains doubtful whether the target of collagen-PVP could be LAIR1, because in the experiments performed by Olivares-Martínez E. et al. a differential effect between type I collagen vs. collagen-PVP in the affinity for LAIR1 was not demonstrated[49], in such a way that if we consider that type I collagen and its degradation products are permanently available in the different organisms, and that type I collagen, as well as collagen-PVP are cleaved immediately in vitro by matrix metalloproteinase 1[20], the pharmacodynamics of collagen-PVP remains unclear.
To better understand the pathways involved in the effects of collagen-PVP on fibroblasts and monocytes, we performed a microarray assay. Our aim was to gain information, although presumptive, on whether certain pathways related to inflammation and fibrosis could be regulated similarly to observations with other drugs used in the treatment of COVID-19. Patients with mild COVID-19, who were treated with intramuscular administration of collagen-PVP, showed an improvement in the disease during the first week of treatment[37], where the effects were associated with the reduction of IP-10, IL-8, and macrophage colony stimulating factor (M-CSF)[36]. These results are consistent with our preliminary findings obtained by microarray assays performed in fibroblasts and monocyte cultures treated with 3% collagen-PVP, where some important pathways related to inflammation, apoptosis, and ECM receptor signalling were modulated. In particular, IL-6 and IL-8 signalling was negatively regulated, as well as JAK and MAPK signalling that would reduce the expression of iNOS favouring the anti-inflammatory condition[50] when stromal and immune cells were treated with collagen-PVP. Furthermore, we consider a possible upregulation of the Th2 immune response pathway could play an important role in the effects observed in patients with COVID-19 treated with collagen-PVP; and again, this hypothesis is also supported by the recently paper published by Olivares-Martínez E. et al.[49]. Despite the nice hypothetic mechanism regarding the mentioned results, it is necessary to perform concluding experiments to demonstrate specifically which of the genes involved by collagen-PVP treatment can regulate the pathways mentioned above.
5. Conclusions
This is not the first-time collagen-PVP and pirfenidone have been compared for the treatment of inflammation and fibrosis. Previously, both drugs have been shown to be able to decrease inflammation, fibrosis, and the expression of pro-inflammatory/fibrogenic cytokines[51]. Here, we have shown that collagen-PVP and pirfenidone can improve COVID-19 patient recovery similarly when administered early. Furthermore, data obtained from Ingenuity Pathway Analysis derived from microarray evaluation of fibroblast and monocyte treatment with collagen-PVP suggested a very close mechanism of action with pirfenidone, which leads to considering their combined treatment in different inflammatory and/or fibrotic conditions.
Author Contributions
Conceptualization, H. M-Z., E.K.; methodology, S. D-M., A. C-W., E.A. M.T., H.T., D. M-G., L.J. O-C., S. H-E., M.D. R-P., A.S. M-S., J. M-C., R.M.S., P. M-T.; formal analysis E. C-A., H. M-Z., E.K.; investigation, H. M-Z., E.K., E. C-A., S. D-M., A. C-W., E.A. M.T., R.M.S.; resources H. M-Z., E.K.; data curation H. M-Z., E.K., E. C-A., H.T.; writing-original draft preparation H. M-Z., E.K., A. C-W., E.A.; writing-review and editing H. M-Z., E.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Research Ethics Committee of the "Mónica Pretelini Sáenz" Maternal-Perinatal Hospital (HMPMPS) (code 2020-12-712), with current registration in the National Bioethics Commission (CONBIOETICA) and by the Research Committee of the same Hospital with registration in the Comisión Federal para la Protección contra Riesgos Sanitarios (COFEPRIS).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Trial was registered on ClinicalTrial.gov with the ID: NCT06585319. General Z-score values and raw data can be downloaded with the following GEO accession numbers GSE262736 and GSE262737.
Acknowledgments
The hTERT-BJ1 and THP-1 cell lines were kindly donated by Professors Ivan Velasco and Enrique Ortega Soto, of the Instituto de Fisiología Celular and the Instituto de Investigaciones Biomédicas, UNAM, Mexico, respectively. The authors thank Daniel Santillán Cortéz and Mario A. Tellez González for technical assistance with the ELISA analysis. Language revision was performed using Writefull AI.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| Collagen-PVP | Collagen-polyvinylpyrrolidone |
| ICU | Intensive care unit |
| qCSI | quick COVID-19 severity index |
| JAK | Janus kinase |
| STAT | signal transducers and activators of transcription |
| SD | Standard deviation |
| ILK | Integrin Linked Kinase |
| mTOR | Mechanistic Target of Rapamycin Kinase |
| Gαq | Gq protein alpha subunit |
| Rho | Ras homology of the Guanosine Triphosphate family proteins |
| ERK | Extracellular Signal-Regulated Kinases |
| MAPK | Mitogen-Activated protein Kinases |
Appendix A
Figure A1.
IL-8 signaling pathways obtained by IPA in fibroblasts modulated by in vitro treatment with collagen-PVP. The overexpression or subexpression of molecules involved in the aforementioned pathways were highlighted with green and red, respectively.
Figure A1.
IL-8 signaling pathways obtained by IPA in fibroblasts modulated by in vitro treatment with collagen-PVP. The overexpression or subexpression of molecules involved in the aforementioned pathways were highlighted with green and red, respectively.
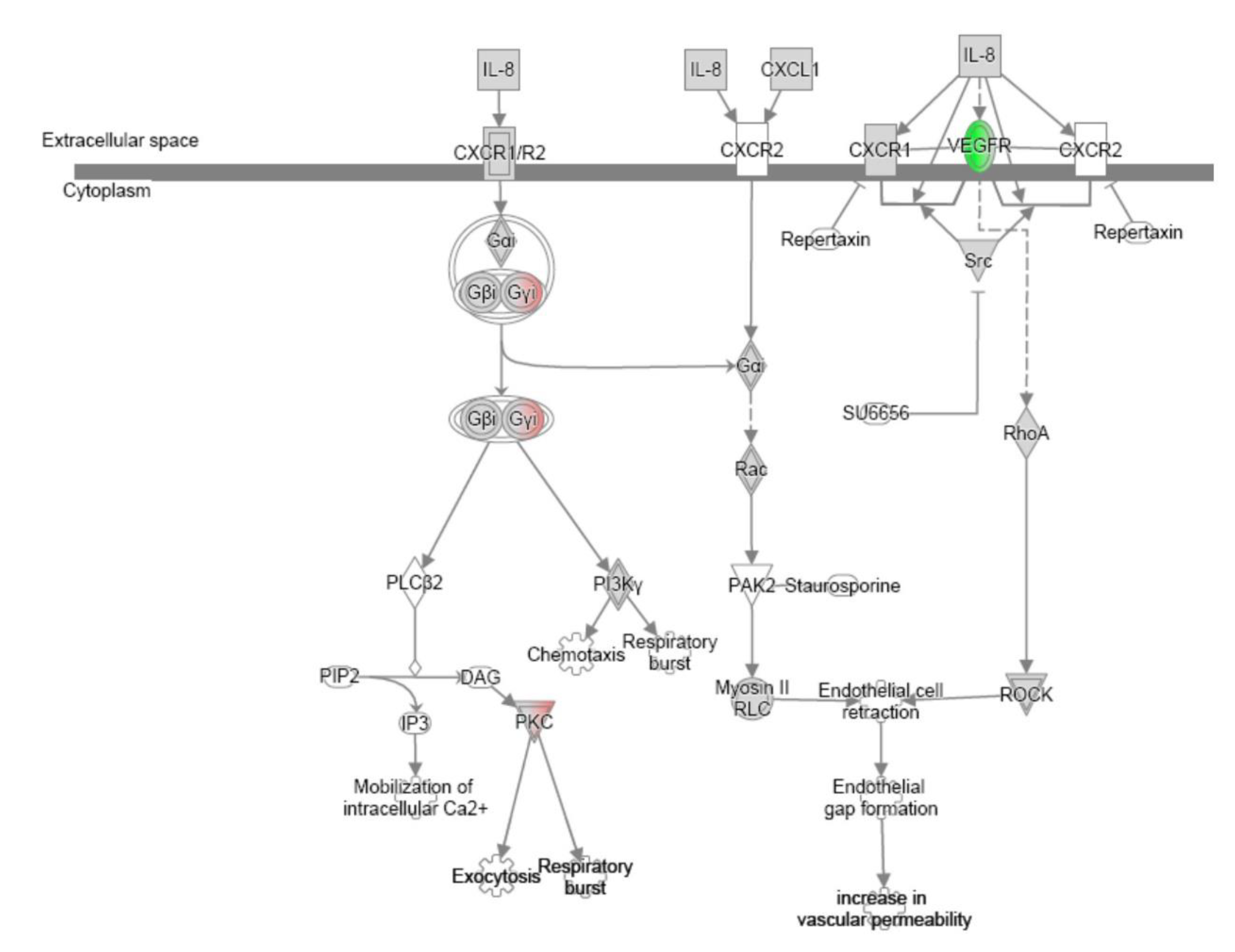
Figure A2.
Cell surface receptors-extracellular matrix signaling pathways obtained by IPA in fibroblasts and macrophages modulated by in vitro treatment with collagen-PVP. The overexpression or subexpression of molecules involved in the aforementioned pathways were highlighted with green and red, respectively.
Figure A2.
Cell surface receptors-extracellular matrix signaling pathways obtained by IPA in fibroblasts and macrophages modulated by in vitro treatment with collagen-PVP. The overexpression or subexpression of molecules involved in the aforementioned pathways were highlighted with green and red, respectively.
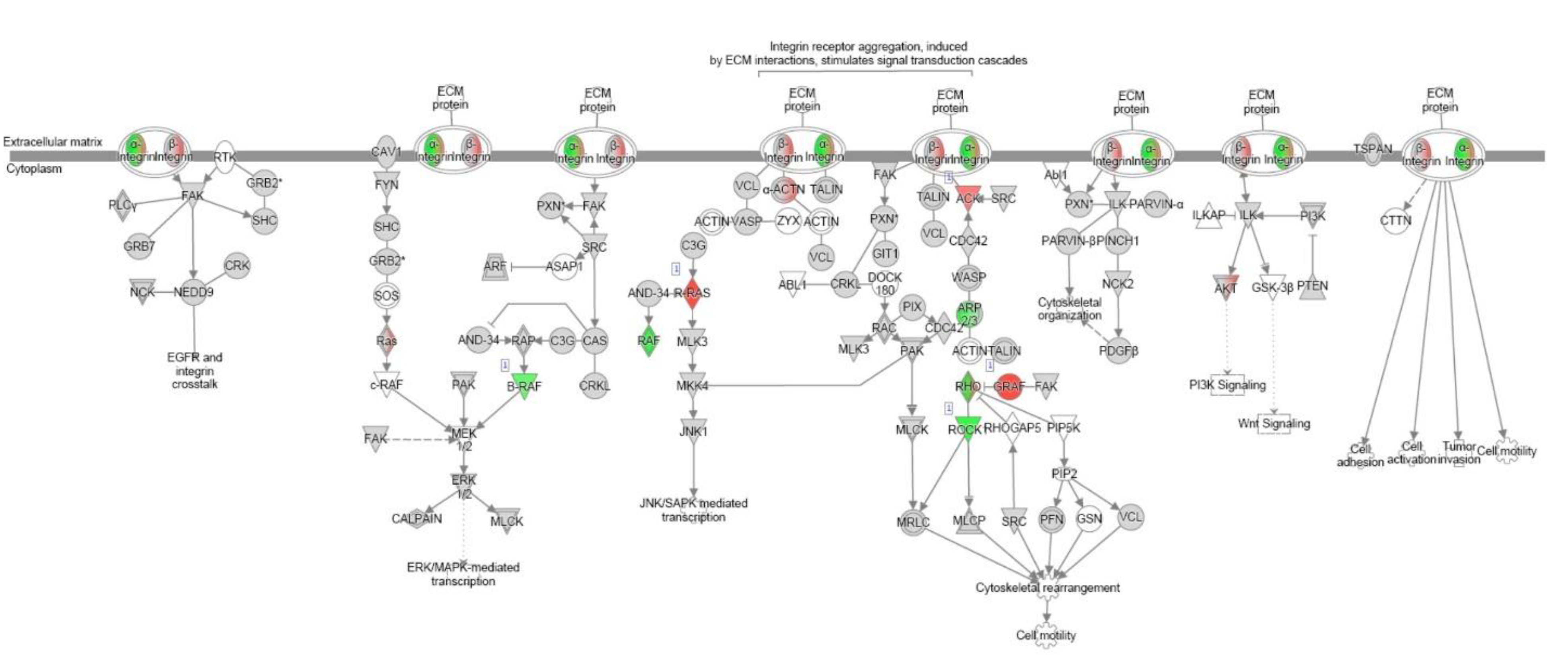
Figure A3.
IL-6 signaling pathways obtained by IPA in macrophages modulated by in vitro treatment with collagen-PVP. The overexpression or subexpression of molecules involved in the aforementioned pathways were highlighted with green and red, respectively.
Figure A3.
IL-6 signaling pathways obtained by IPA in macrophages modulated by in vitro treatment with collagen-PVP. The overexpression or subexpression of molecules involved in the aforementioned pathways were highlighted with green and red, respectively.
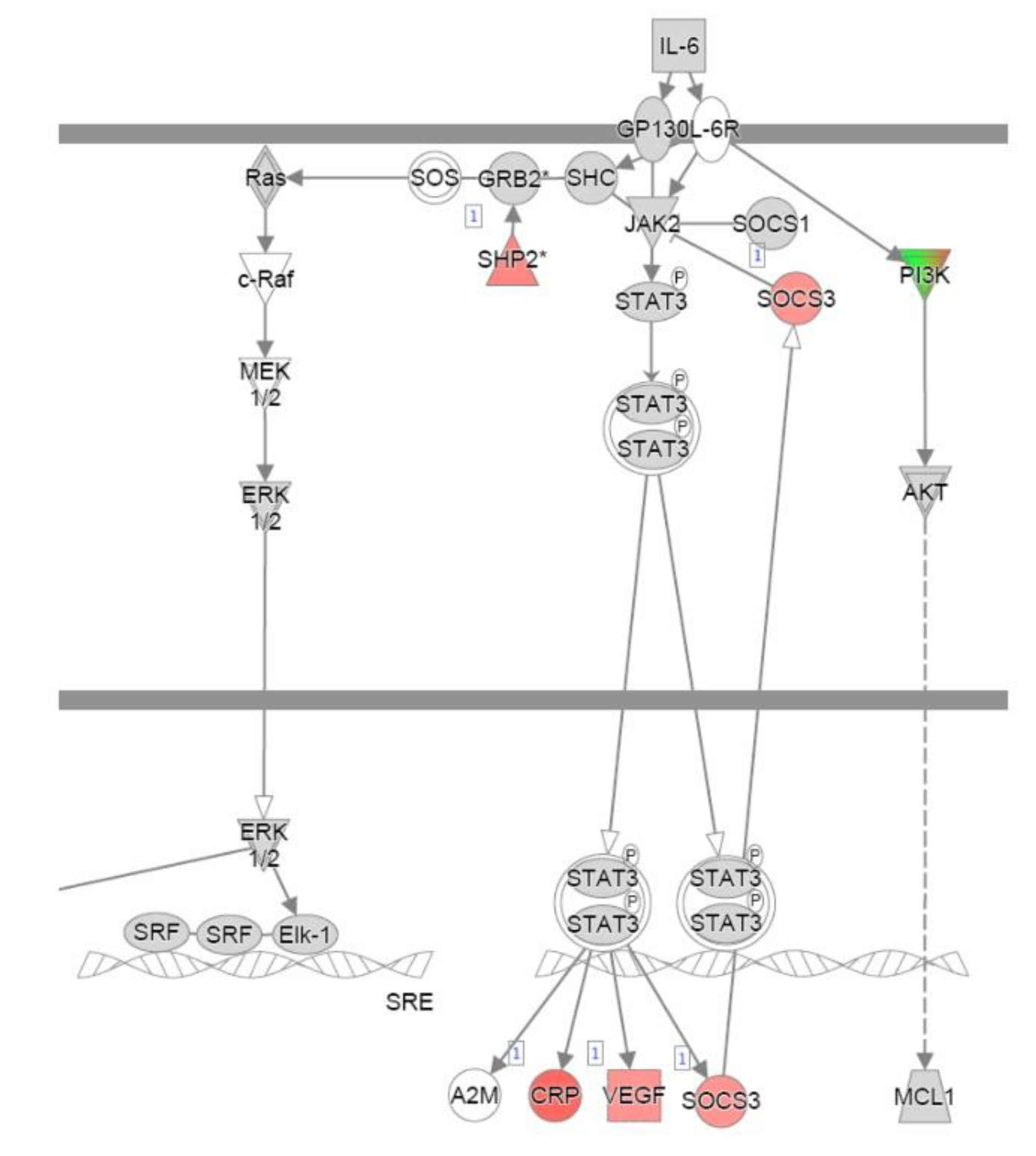
Figure A4.
Nitric oxide production signaling pathways obtained by IPA in fibroblasts and macrophages modulated by in vitro treatment with collagen-PVP. The overexpression or subexpression of molecules involved in the aforementioned pathways were highlighted with green and red, respectively.
Figure A4.
Nitric oxide production signaling pathways obtained by IPA in fibroblasts and macrophages modulated by in vitro treatment with collagen-PVP. The overexpression or subexpression of molecules involved in the aforementioned pathways were highlighted with green and red, respectively.
References
- Kinross P, Suetens C, Dias JG, Alexakis L, Wijermans A, Colzani E, et al. Rapidly increasing cumulative incidence of coronavirus disease (COVID-19) in the European Union/European Economic Area and the United Kingdom, 1 January to . Euro Surveill. 2020;25(11):2000285. 15 March. [CrossRef]
- The novel Chinese coronavirus (2019nCoV) infections: Challenges for fighting the storm. Eur J Clin Invest [Internet]. 2020 Mar [cited 2020 Mar 20];50(3). Available from: https://onlinelibrary.wiley.com/doi/abs/10.1111/eci.13209.
- Rothan HA, Byrareddy SN. The epidemiology and pathogenesis of the coronavirus disease (COVID-19) outbreak. J Autoimmun. 2020;109:102433. [CrossRef]
- Pang J, Wang MX, Ang IYH, Tan SHX, Lewis RF, Chen JI, et al. Potential Rapid Diagnostics, Vaccine and Therapeutics for 2019 Novel Coronavirus (2019-nCoV): A Systematic Review. J Clin Med. 2020;9(3):623. [CrossRef]
- Ng Y, Li Z, Chua YX, Chaw WL, Zhao Z, Er B, et al. Evaluation of the Effectiveness of Surveillance and Containment Measures for the First 100 Patients with COVID-19 in Singapore - -February 29, 2020. MMWR Morb Mortal Wkly Rep. 2020;69(11):307-311. 2 January. [CrossRef]
- Applegate WB, Ouslander JG. COVID-19 Presents High Risk to Older Persons. J Am Geriatr Soc. 2020;68(4):681. [CrossRef]
- Liang H, Acharya G. Novel corona virus disease (COVID-19) in pregnancy: What clinical recommendations to follow? Acta Obstet Gynecol Scand. 2020;99(4):439-442. [CrossRef]
- Sevillano Pires L, Andrino B, Llaneras K, Grasso D. El mapa del coronavirus: así crecen los casos día a día y país por país. 2020 Mar 19; Available from: https://elpais.com/sociedad/2020/03/16/actualidad/1584360628_538486.html.
- Sette A, Crotty S. Adaptive immunity to SARS-CoV-2 and COVID-19. Cell. 2021 Feb 18;184(4):861-880. [CrossRef]
- Ye Q, Wang B, Mao J. The pathogenesis and treatment of the `Cytokine Storm' in COVID-19. J Infect. 2020;80(6):607-613. [CrossRef]
- Flaumenhaft R, Enjyoji K, Schmaier AA. Vasculopathy in COVID-19. Blood. 2022;140(3):222-235. [CrossRef]
- Yalcin AD, Yalcin AN. Future perspective: biologic agents in patients with severe COVID-19. Immunopharmacol Immunotoxicol. 2021;43(1):1-7. [CrossRef]
- Tale S, Ghosh S, Meitei SP, Kolli M, Garbhapu AK, Pudi S. Post-COVID-19 pneumonia pulmonary fibrosis. QJM. 2020;113(11):837-838. [CrossRef]
- Vasarmidi E, Tsitoura E, Spandidos DA, Tzanakis N, Antoniou KM. Pulmonary fibrosis in the aftermath of the COVID-19 era (Review). Exp Ther Med. 2020;20(3):2557-2560. [CrossRef]
- Soy M, Keser G, Atagündüz P, Tabak F, Atagündüz I, Kayhan S. Cytokine storm in COVID-19: pathogenesis and overview of anti-inflammatory agents used in treatment. Clin Rheumatol. 2020;39(7):2085-2094. [CrossRef]
- George PM, Wells AU, Jenkins RG. Pulmonary fibrosis and COVID-19: the potential role for antifibrotic therapy. Lancet Respir Med. 2020;8(8):807-815. [CrossRef]
- Krötzsch-Gómez FE, Furuzawa-Carballeda J, Reyes-Márquez R, Quiróz-Hernández E, Díaz de León L. Cytokine expression is downregulated by collagen-polyvinylpyrrolidone in hypertrophic scars. J Invest Dermatol. 1998;111(5):828-834. [CrossRef]
- Furuzawa-Carballeda J, Krötzsch E, Barile-Fabris L, Alcalá M, Espinosa-Morales R. Subcutaneous administration of collagen-polyvinylpyrrolidone down regulates IL-1beta, TNF-alpha, TGF-beta1, ELAM-1 and VCAM-1 expression in scleroderma skin lesions. Clin Exp Dermatol. 2005;30(1):83-86. [CrossRef]
- Taniguchi H, Ebina M, Kondoh Y, Ogura T, Azuma A, Suga M, et al. Pirfenidone in idiopathic pulmonary fibrosis. Eur Respir J. 2010;35(4):821-829. [CrossRef]
- Leyva-Gómez G, Lima E, Krötzsch G, Pacheco-Marín R, Rodríguez-Fuentes N, Quintanar-Guerrero D, et al. Physicochemical and functional characterization of the collagen-polyvinylpyrrolidone copolymer. J Phys Chem B. 2014;118(31):9272-9283. [CrossRef]
- Furuzawa-Carballeda J, Rodríquez-Calderón R, Díaz de León L, Alcocer-Varela J. Mediators of inflammation are down-regulated while apoptosis is up-regulated in rheumatoid arthritis synovial tissue by polymerized collagen. Clin Exp Immunol. 2002;130(1):140-149. [CrossRef]
- Krämer A, Green J, Pollard J, Tugendreich S. Causal analysis approaches in Ingenuity Pathway Analysis. Bioinformatics. 2014;30(4):523-530. [CrossRef]
- Goker Bagca B, Biray Avci C. The potential inhibition of the JAK/STAT pathway by ruxolitinib in the treatment of COVID-19. Cytokine Growth Factor Rev. 2020;54:51-62. [CrossRef]
- Al-Kuraishy HM, Batiha GE, Faidah H, Al-Gareeb AI, Saad HM, Simal-Gandara J. Pirfenidone and post-Covid-19 pulmonary fibrosis: invoked again for realistic goals. Inflammopharmacology. 2022;30(6):2017-2026. [CrossRef]
- Wu C, Chen X, Cai Y, Xia J, Zhou X, Xu S, et al. Risk Factors Associated With Acute Respiratory Distress Syndrome and Death in Patients With Coronavirus Disease 2019 Pneumonia in Wuhan, China. JAMA Intern Med. 2020;180(7):934. [CrossRef]
- Fadel R, Morrison AR, Vahia A, Smith ZR, Chaudhry Z, Bhargava P, et al. Early Short-Course Corticosteroids in Hospitalized Patients With COVID-19. Clin Infect Dis. 2020 Nov 19;71(16):2114–20. [CrossRef]
- Mehta P, Cron RQ, Hartwell J, Manson JJ, Tattersall RS. Silencing the cytokine storm: the use of intravenous anakinra in haemophagocytic lymphohistiocytosis or macrophage activation syndrome. Lancet Rheumatol. 2020;2(6):e358–67. [CrossRef]
- Geng J, Wang F, Huang Z, Chen X, Wang Y. Perspectives on anti-IL-1 inhibitors as potential therapeutic interventions for severe COVID-19. Cytokine. 2021;143:155544. [CrossRef]
- Xu X, Han M, Li T, Sun W, Wang D, Fu B, et al. Effective treatment of severe COVID-19 patients with tocilizumab. Proc Natl Acad Sci. 2020;117(20):10970–5. [CrossRef]
- on behalf of the Gemelli-ICU Study Group, Montini L, De Pascale G, Bello G, Grieco DL, Grasselli G, et al. Compassionate use of anti-IL6 receptor antibodies in critically ill patients with acute respiratory distress syndrome due to SARS-CoV-2. Minerva Anestesiol [Internet]. 2021 Oct [cited 2021 Nov 25];87(10). Available from: https://www.minervamedica.it/index2.php?show=R02Y2021N10A1080.
- Ranieri VM, Pettilä V, Karvonen MK, Jalkanen J, Nightingale P, Brealey D, et al. Effect of Intravenous Interferon β-1a on Death and Days Free From Mechanical Ventilation Among Patients With Moderate to Severe Acute Respiratory Distress Syndrome: A Randomized Clinical Trial. JAMA. 2020;323(8):725.
- Callejas Rubio JL, Aomar Millán I, Moreno Higueras M, Muñoz Medina L, López López M, Ceballos Torres Á. Tratamiento y evolución del síndrome de tormenta de citoquinas asociados a infección por SARS-CoV-2 en pacientes octogenarios. Rev Esp Geriatría Gerontol. 2020;55(5):286–8.
- Hu B, Huang S, Yin L. The cytokine storm and COVID-19. J Med Virol. 2021;93(1):250-6.
- Gonzales-Zamora JA, Quiroz T, Vega AD. Successful treatment with Remdesivir and corticosteroids in a patient with COVID-19-associated pneumonia: A case report. Tratamiento exitoso con Remdesivir y corticoides en un paciente con neumonía asociada a COVID-19: reporte de un caso. Medwave. 2020;20(7):e7998. [CrossRef]
- Aygün İ, Kaya M, Alhajj R. Identifying side effects of commonly used drugs in the treatment of Covid 19. Sci Rep. 2020;10(1):21508. [CrossRef]
- Méndez-Flores S, Priego-Ranero Á, Azamar-Llamas D, Olvera-Prado H, Rivas-Redonda KI, Ochoa-Hein E, et al. Effect of polymerised type I collagen on hyperinflammation of adult outpatients with symptomatic COVID-19. Clin Transl Med. 2022;12(3):e763. [CrossRef]
- Carpio-Orantes LD, García-Méndez S, Sánchez-Díaz JS, Aguilar-Silva A, Contreras-Sánchez ER, Hernández SNH. Use of Fibroquel® (Polymerized type I collagen) in patients with hypoxemic inflammatory pneumonia secondary to COVID-19 in Veracruz, Mexico. J Anesth Crit Care Open Access. 2021;13(1):69‒73. [CrossRef]
- Acat M, Yildiz Gulhan P, Oner S, Turan MK. Comparison of pirfenidone and corticosteroid treatments at the COVID-19 pneumonia with the guide of artificial intelligence supported thoracic computed tomography. Int J Clin Pract. 2021;75(12):e14961. [CrossRef]
- Seifirad, S. Pirfenidone: A novel hypothetical treatment for COVID-19. Med Hypotheses. 2020;144:110005. [CrossRef]
- Rizvi AA, Kathuria A, Al Mahmeed W, Al-Rasadi K, Al-Alawi K, Banach M, et al. Post-COVID syndrome, inflammation, and diabetes. J Diabetes Complica-tions. 2022;36(11):108336. [CrossRef]
- Ye Q, Wang B, Mao J. The pathogenesis and treatment of the `Cytokine Storm' in COVID-19. J Infect. 2020;80(6):607-613. [CrossRef]
- Chen Y, Wang J, Liu C, Su L, Zhang D, Fan J, et al. IP-10 and MCP-1 as biomarkers associated with the severity of the disease of COVID-19. Mol Med. 2020;26(1):97. [CrossRef]
- Ghazavi A, Ganji A, Keshavarzian N, Rabiemajd S, Mosayebi G. Cytokine profile and disease severity in patients with COVID-19. Cytokine. 2021;137:155323. [CrossRef]
- Cao ZJ, Liu Y, Zhang Z, Yang PR, Li ZG, Song MY, et al. Pirfenidone ameliorates silica-induced lung inflammation and fibrosis in mice by inhibiting the secretion of interleukin-17A. Acta Pharmacol Sin. 2022;43(4):908-918. [CrossRef]
- Finnerty JP, Ponnuswamy A, Dutta P, Abdelaziz A, Kamil H. Efficacy of antifibrotic drugs, nintedanib and pirfenidone, in treatment of progressive pulmonary fibrosis in both idiopathic pulmonary fibrosis (IPF) and non-IPF: a systematic review and meta-analysis. BMC Pulm Med. 2021;21(1):411. [CrossRef]
- Chen Z, Zhou H, Huang X, Wang S, Ouyang X, Wang Y, et al. Pirfenidone attenuates cardiac hypertrophy against isoproterenol by inhibiting activation of the janus tyrosine kinase-2/signal transducer and activator of transcription 3 (JAK-2/STAT3) signaling pathway. Bioengineered. 2022;13(5):12772-12782. [CrossRef]
- Borja-Flores A, Macías-Hernández SI, Hernández-Molina G, Perez-Ortiz A, Reyes-Martínez E, Belzazar-Castillo de la Torre J, et al. Long-Term Effectiveness of Polymerized-Type I Collagen Intra-Articular Injections in Patients with Symptomatic Knee Osteoarthritis: Clinical and Radiographic Evaluation in a Cohort Study. Adv Orthop. 2020;2020:9398274. [CrossRef]
- Furuzawa-Carballeda J, Cabral AR, Zapata-Zuñiga M, Alcocer-Varela J. Subcutaneous administration of polymerized-type I collagen for the treatment of patients with rheumatoid arthritis. An open-label pilot trial. J Rheumatol. 2003;30(2):256-259.
- Olivares-Martínez E, Hernández-Ramírez DF, Núñez-Álvarez CA, Meza-Sánchez DE, Chapa M, Méndez-Flores S, et al. Polymerized Type I Collagen Downregulates STAT-1 Phosphorylation Through Engagement with LAIR-1 in Circulating Monocytes, Avoiding Long COVID. Int J Mol Sci. 2025;26(3):1018. [CrossRef]
- Sarode AY, Jha MK, Zutshi S, Ghosh SK, Mahor H, Sarma U, Saha B. Residue-Specific Message Encoding in CD40-Ligand. iScience. 2020 Aug 6;23(9):101441. [CrossRef]
- Olmos-Zuñiga JR, Silva-Martínez M, Jasso-Victoria R, Baltazares-Lipp M, Hernández-Jiménez C, Buendía-Roldan I, et al. Effects of Pirfenidone and Collagen-Polyvinylpyrrolidone on Macroscopic and Microscopic Changes, TGF-β1 Expression, and Collagen Deposition in an Experimental Model of Tracheal Wound Healing. Biomed Res Int. 2017;2017:6471071. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



