Submitted:
28 May 2025
Posted:
29 May 2025
You are already at the latest version
Abstract
Background/Objectives: The optimal duration of antibiotic therapy, a cornerstone of PJI treatment, remains a topic of considerable debate, with current recommendations often based on limited evidence and expert consensus. Emerging evidence suggests that shorter antibiotic courses may be as effective as prolonged therapies in select cases, provided thorough surgical debridement is performed and biofilm-active agents are used.
We aimed to synthesize available data on antibiotic therapy duration based on the surgical technique, along with recall of definitions, diagnosis criteria and classification. Future perspectives on PJI diagnosis have been also presented.
Methods: Following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA), databases were searched using predefined medical subject headings (MeSH) and PUBMED. Randomized controlled trials (RCTs), observational studies, and expert guidelines have been synthetized.
Results: A total of 2305 articles involving observational studies and randomized controlled trials were reviewed. We summarized the results of studies that have compared shorter antibiotic courses to prolonged therapies according to the surgical procedure. Forty five studies were analyzed. Definitions and classification of PJI were mentioned for a better analysis. Future perspectives were also noted.
Conclusions: This review highlights the limited data available for evaluating antibiotic duration in the setting of PJI. The most studies found that a shorter antibiotic duration was non-inferior to a longer duration in selected cases but evidence-based guidelines to harmonize practices and improve outcomes for PJI patients are needed.
Keywords:
PJI
; BJI
; treatment
; antibiotic duration
; DAIR
; surgery
; one-step exchange
; two-step exchange
; arthroplasty
1. Introduction
Prosthetic joint infections (PJI) represent a severe and complex complication in orthopedic surgery, significantly impacting patient morbidity and healthcare systems with 15-year incidences of 1.5–2% and a 5-year mortality exceeding 20% [1]. In 2017, the incidence of hip and knee PJI in the United States was 2.1% and 2.3%, respectively, with comparable rates observed in Korea [1]. In France, PJIs account for approximately 4% of all osteo-articular infections [2]. By 2030, hospital costs related to hip and knee PJI in the United States are projected to reach $1.85 billion annually [1].
PJI are foreign-body associated infections that often necessitate a surgical approach, typically involving the removal of the foreign body and extended antibiotic treatment duration [2]. Standard surgical procedures include the removal of the arthroplasty, usually followed by the implantation of a new prosthetic device in a one- or two-stage exchange procedure [3]. A more conservative surgical approach that involves debridement, antibiotics, and retention of the implant (DAIR) is proposed for selected patients with acute PJI. It can offer a reasonable chance of success in managing the infection [3]. According to the IDSA guidelines of 2013, the treatment duration of PJI ranges from 3 to 6 months [4]. These extended durations were recommended due to biofilm-embedded bacteria. Recently, there were trends to shorten antibiotic length. In 2018, the International Meeting on Musculoskeletal Infections recommended to reduce the antibiotic duration for PJI managed with DAIR to 6 weeks [5,6].
Our primary objective in this narrative review is to evaluate the effectiveness of the total duration of antimicrobial therapy in treating PJI according to the surgical approach.
2. Methods
2.1. Literature Search Strategy
We carried out this systematic review out following the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) [7]. An extensive search was conducted over four medical electronic databases (PubMed, Embase Science Direct, and Cochrane Library) from the 1st of January 1998 to the 1st of April 2025.
To optimize our search strategy, we integrated these key words: ‘antibiotic duration’, ‘antibiotic lengh’, ‘short duration antibiotic’, ‘short course antibiotic’, ‘prolonged antibiotic’, ‘prosthetic joint infection’, ‘periprosthetic joint infection’, ‘bone and joint infection’, ‘arthroplasty infection, ’surgery’, ‘DAIR’, ‘one-step exchange’, ‘two-step exchange’ and ‘biofilm’.
2.2. Selection Criteria
Abstracts were screened; studies and clinical trials evaluating the impact of antibiotic duration on clinical outcomes were selected. We also reviewed additional references cited within these articles to identify relevant earlier studies. Exclusion criteria included case reports, conference presentations, studies focused on antibiotic prophylaxis, chronic suppressive therapy, microbiological and radiological diagnosis. Fungal or mycobacterial PJI were either excluded as well as articles written in languages other than English, French. Osteoarticular infections without a hardware implant were not retained for analysis.
2.3. Data Extraction and Criteria Appraisal
We gathered the data from article texts, abstracts, tables, and figures. For data extraction we followed the Population, Intervention, Comparison, Outcome (PICO) structure and included information such as the title, author name, year of publication, study structure, sample size, patient characteristics, antibiotics (molecules and their duration, routes of administration), surgery intervention, outcomes, and conclusions.
3. Results
A total of n = 2305 studies were initially identified from the databases based on the redefined inclusion and exclusion criteria. After removing articles that met the exclusion criteria, n = 45 articles were ultimately selected for inclusion in our systematic review. The study selection and screening process is illustrated in the PRISMA [7] flow diagram (Figure 1).
For our narrative review, we will begin with a brief overview of the definitions and classifications of PJI to provide a clearer understanding of the treatment strategies.
4. Definitions and Classifications
4.1. Defining Prosthetic Joint Infections and Clinical Presentation
Accurate diagnosis of PJI is a challenging issue and requires a combination of clinical signs, microbiological evidence, and imaging findings.
In 2011, the diagnosis of PJI was established through standards suggested by The Musculoskeletal Infectious Society (MSIS) that underwent un update by the International Consensus Meeting on PJI [8,9]. Two years later in 2013, the Infectious Diseases Society of America (IDSA) published definitions of PJI with a slight distinction [4]. In a more recent publication with evidence-based data, the MSIS and the International Consensus Meeting (ICM) have developed in 2018 a more updated version [5]. These criteria and definitions are outlined in Table 1.
4.2. Classification of Prosthetic Joint Infections
Management of PJIs is a challenge and various classification systems have been introduced, which consider variables such as onset of symptoms, pathogenesis and clinical manifestations.
Classifications for PJI were established to predict the most appropriate treatment strategy according to physiopathology of infection.
Mainly, classifications are based on the time of symptom onset: early (within three months post-surgery), delayed (3–12 months post-surgery), or late (beyond 12 months). Early infections are often caused by virulent organisms such as Staphylococcus aureus, whereas delayed and late infections frequently involve less aggressive pathogens like coagulase-negative staphylococci [3,10] (Table 2).
These physiopathology classifications are important for well-designed clinical trials and set the rationale for prolonged treatment, based on the difficulty of treating biofilm-embedded bacteria and surgical treatment or conservative strategy like DAIR (debridement, antibiotics and implant retention).
Coventry proposed a classification of PJI. He devided infections into three stages according to the onset timing: Stage I (acute), within the first three months; Stage II, more than three months post-surgery intervention; and Stage III, two years after the initial infection [10,11]. Tsukayama et al. [12] classified infections into four categories: 1) Positive intraoperative cultures; 2) Early postoperative infection occurring within four weeks; 3) Late chronic infection (beyond four weeks); 4) Acute hematogenous infection.
Theses classifications help to determining the optimal surgical technique, the appropriate duration of antibiotic therapy, and the prognosis of PJI, limiting the development of evidence-based approaches and accurate prognostic assessments [13].
To address this gap, the PJI-TNM classification was introduced by Alt et al. in 2020 [4]. One of the most widely used and successful classification systems in medicine is the TNM classification for malignant tumors in oncology that was developed by Pierre Denoix in the late 1940s and early 1950s [14]. Beyond treatment planning, the TNM system provides valuable prognostic information and enables clinical and scientific comparisons of treatment outcomes. These principles are also relevant for PJI. The commonly stated phrase “treat the infection like a tumor” highlights similarities between PJIs and malignancies, particularly the necessity for surgical resection of affected tissue, the optimal choice of antibiotics and their duration. This system applies the principles of the well-established oncological TNM classification to better reflect the severity and complexity of PJIs. The three key factors defining PJIs were mapped to the TNM framework:
- T (Tissue & Implant) – Condition of the infected implant and periarticular soft tissues.
- N (Non-human Cell) – The causative microorganism.
- M (Morbidity of the Patient) – The host’s overall health and comorbidities.
Each category is further subdivided by a number (0–3) and a letter (a–c) to distinguish between various situations. A lowercase "r" is placed in front of the TNM classification in case of recurrent infection in the same joint.
5. Prosthetic Joint Infection Surgery Options
A collaborative approach involving orthopedic surgeons, infectious disease specialists, and patients is essential in managing PJI. Treatment typically combines surgical intervention with antibiotic therapy. Surgery is a major pillar in the management of PJI. Surgical treatment options include DAIR, one-stage or two-stage exchange, resection arthroplasty, arthrodesis, and amputation [3,13,15]. Among these, the surgical treatment of reference is removal of the arthroplasty [2].
DAIR consist of debridement, antibiotics and implant retention. Debridement involves the removal of infected, devitalized bone and soft tissue, hematomas, fibrous membranes and sinus tracts. It should be undertaken to reduce the bioburden of the pathogens and to improve the efficiency of the patient’s immune system [16].
In one-stage revision, within the same surgical intervention, a new prothesis is implanted after removing all the foreign material and full debridement. Antibiotics is administered for two to three weeks prior to the prosthesis exchange if the pathogen is identified before the surgery intervention and the patient had no signs of sepsis [3]. By contrast, the two-stage exchange procedure includes a delayed reimplantation of a new prothesis. Resection arthroplasty allows for the definitive removal of the prosthesis, along with debridement, without reimplantation thereafter [3]. In certain cases, surgery options are not possible and conservative treatment is recommended with long term suppressive antibiotics [2].
For the radical surgery approaches (DAIR or prosthesis removal) long-term antibiotics are prescribed for certain duration that could be extended due to the challenge of treating biofilm-associated bacteria. However, treatment duration is not well established and it is in most of cases empirical [2]. It differs based on the surgical approach and the underlying cause of the infection.
Antibiotic selection is a multifactorial decision, influenced by the identified pathogen, its antibiotic susceptibility profile, its capacity to form a biofilm, the severity of the infection, and host-related factors [17].
Here we will discuss the duration of antibiotics based on the surgical procedure performed.
6. Antibiotic Duration of PJI According to the Surgery Options
Orthopedic infectious disease specialists collaborate with surgeons and microbiologists to determine antibiotic regimens. They are based on the patient's overall health status, clinical context, detected microorganism, its susceptibility and the surgery procedure [18]. Empirical antibiotics are given usually 72 to 144 hours before microbiology data are available. The therapy duration is measured from the surgery date to the discontinuation date [18]. The type of microorganism might also influence treatment duration. Generally, treatment lasts 6 to 12 according to surgical management [17].
6.1. Prosthetic Joint Infection Treated with DAIR
6.1.1. The Recommended Duration of Antibiotics
The optimal length of antibiotic therapy after PJI surgery remains debated, depending on the chosen medical–surgical strategy (implant retention versus removal) and the practices of individual treatment teams [17].
Treatment begins during the first-stage procedure. The approach should be individualized based on the infecting organism and patient factors. Intravenous administration is often recommended for the first week, followed by oral therapy if an appropriate agent is available and the organism's sensitivity allows [16,19].
6.1.2. Comparative Studies to Shorten the Antibiotic Duration for PJI
Numerous studies have been undertaken to evaluate the reduction of antibiotic treatment duration from six months to three months, and in some cases to six weeks, depending on the type of surgical procedure. The main findings of these key studies are summarized in Table 5.
Twelve Weeks Versus Eight Weeks
Puhto et al. have conducted a study in which they aimed to evaluate the effect of shortening antibiotic treatment duration in PJI managed with DAIR [26]. In 2006, the standard antibiotic regimen was reduced from 6 to 3 months for total knee arthroplasty (TKA), and from 3 to 2 months for total hip arthroplasty (THA) in their hospital [26]. They conducted a retrospective review of all DAIR-treated TKA and THA PJIs between February 2001 and August 2009. Of 132 patients, 86 (65%) completed the full antibiotic course and were included in the analysis. Among them, 32 (37%) had THA and 54 (63%) had TKA. Treatment success was observed in 34 patients (89.5%) in the longer-duration group and in 42 patients (87.5%) in the shorter-duration group (p = 0.78). These results suggest that, when antibiotic therapy is completed as planned, shorter treatment duration 3 months for TKA and 2 months for THA is as effective as longer courses [26].
In a more recent study, Tornero et al. have prospectively collected and retrospectively reviewed from 1999 to 2013 143 cases of PJI managed with DAIR with minimum follow-up of 2 years. The failure rate after a median duration of oral antibiotic treatment of 69 days (IQR 45–95 days) was 11.8%. They have concluded that the only factor associated with failure was the oral antibiotic selection, not the duration of treatment. Thus, duration of 8 weeks seems to be a good alternative to prolonged regimens [25].
A Spanish team, have published in 2013 a retrospective, multicenter, observational study of cases of PJI by S. aureus that were managed with DAIR (2003–2010). The success rate was 55%. There were no differences in relapse that were observed between patients regardless of treatment duration, which ranged from 60 to more than 90 days [27].
The same team has conducted a more recent randomized clinical trial in 2016 comparing short versus long duration of levofloxacin plus rifampicin for acute staphylococcal PJI managed with DAIR [28]. Sixty three patients were included. The primary endpoint of the study was the cure rate with a median follow-up duration of 540 days. In the intention-to-treat analysis, cure rates were 58% in the long-schedule group and 73% in the short-schedule group (difference: 15.7%, 95% CI: 39.2% to 7.8%). Among the 44 patients (70%) included in the per-protocol analysis, cure rates were 95.0% for the long schedule and 91.7% for the short schedule (difference: 3.3%, 95% CI: 11.7% to 18.3%). Thus, they suggest that an 8-week course of levofloxacin and rifampicin may be non-inferior to longer standard regimens for acute staphylococcal PJI managed with DAIR [28].
Considering these studies, in 2024, the American Academy of Orthopaedic Surgeons have published that there is no difference in outcomes between antibiotic protocols lasting 8 weeks versus those lasting 3 to 6 months [2].
Twelve Weeks Versus Six Weeks
In 2010, Bernard et al. included in their study 144 PJI cases, consisting of 62 hip arthroplasties, 62 knee arthroplasties, and 20 hip hemiarthroplasties, with a follow-up period ranging from 26 to 65 months. Surgical interventions comprised 60 DAIR, 10 one-stage prosthesis exchanges, 57 two-stage exchanges, and 17 Girdlestone procedures or knee arthrodeses. Antibiotic therapy lasted 6 weeks in 70 episodes (49%) and 12 weeks in 74 episodes. Overall, cure was achieved in 115 cases (80%). Only two patients failed in the short-term group (90% cure rate) [30].
In 2017, Chaussade et al. in the same French team have included in a multicenter retrospective study 87 episodes of PJI with debridement performed within 3 weeks of symptom onset [31]. Sixty patients (69%) sustained remission after a mean follow-up of 52.1 months. In a multivariate analysis no statistical difference was demonstrated difference between hip and knee cases (73.3% vs. 59.3%, 95% confidence interval (CI), 0.20–1.38), or between patients receiving 6 weeks versus 12 weeks of antibiotic treatment (70.5% vs. 67.4%, 95% CI 0.27–2.10, p = 0.60). Therefore, as conclusion there were no difference in long-term remission between patients treated with DAIR who received either 6 or 12 weeks of antibiotic therapy [31]. Further prospective randomized trials were recommended [31].
Thus, Bernard in 2021 published DATIPO, a large French open-label, randomized, non-inferiority trial comparing 6 weeks versus 12 weeks of antibiotic therapy for patients with PJI, with 205 patients in each group [32]. The study did not confirm the non-inferiority of 6-week therapy, as 18% of patients in the 6-week group experienced persistent infection, compared to 9% in the 12-week group. Subgroup analyses highlighted significant differences based on the surgical approach: for patients managed with DAIR, the 6-week regimen resulted in notably worse outcomes than the 12-week regimen (30.7% vs. 14.5%, respectively). No significant difference was observed for patients who underwent one-stage exchange (4% vs. 2.8%). However, for patients receiving a two-stage exchange, those treated with 6 weeks of antibiotics had more adverse outcomes (15% vs. 4.9%) [32].
Table 5 provides an overview of these studies.
6.2. PJI Treated with Single-Step Exchange Procedure
Single-stage revision surgery has recently experienced interest as a treatment strategy for PJI [33]. The success of a one-stage exchange arthroplasty depends heavily on careful patient selection, precise surgical technique, and coordinated perioperative management by a multidisciplinary team. Similar to the two-stage exchange, the effectiveness of this approach is closely tied to the thoroughness of debridement and the extent to which the microbial load is reduced [16].
Rowan et al. have published a review in 2018 assessing evidence that single-step exchange for PJI has an increased interest since the last 5 years [34]. The reinfection rates (RR) were of 7.6% (95% CI 3.4–13.1) and 8.8% (95% CI 7.2–10.6) for single-stage and two-stage revisions respectively [33]. Thus, they advocate for recommanding of single-stage revision in cases of significant bone loss and atypical PJI, such as fungal infections [34].
In our review of PJI managed by single-step exchange procedure, the reported RRs for this technique range from 5% to 25% [35,36,37,38,39,40,41,42,43], which are comparable to those observed with two-stage revisions (9% to 20%) [44]. For instance, a study involving 28 patients who underwent single-stage revision for chronic knee arthroplasty infections reported no reinfections at a three-year follow-up [35]. Similarly, another study examining 50 knee revisions with an average follow-up of 10.5 years found a reinfection rate of only 2% [45]. However, Buchholz et al. reported a reinfection rate of 23% when using single-stage revision. It was explained that the patients were managed without systemic antibiotics [46]. Similarly, Ammon and Stockley observed a 14% recurrence rate (8 out of 57 cases) following staged revision procedures performed without systemic antibiotic therapy in patients who required impaction allografting as part of their reconstruction [47,48].
According to IDSA guidelines published in 2013, current recommendations suggest that one-stage exchange should be followed by 4 to 6 weeks of pathogen-specific antimicrobial therapy, based on limited but existing evidence, with an additional 3 months of oral suppressive therapy [4].
The Endo-Klinik in Germany has reported using a shorter course 10 to 14 days of antibiotics post–one-stage exchange except in cases involving streptococcal infections [48]. Over their 35 years of experience, they have claimed success rates ranging from 75% to 90% [49].
Studies that tried to shorten antibiotic duration for PJI managed by single-step exchange are mentioned in table 6.
Table 6. Summary of Studies on Antibiotic Treatment Duration for Prosthetic Joint Infections managed by single-step exchange
6.3. PJI treated With Two-Step Exchange Procedure
A review of some former studies, highlights significant variability in treatment protocols, ranging from no antibiotic use at all [46,47] to extended intravenous courses lasting up to 9 weeks, often followed by oral therapy for varying durations [35,54,55]. According to the IDSA guidelines published in 2013, the typical duration of systemic antibiotics for PJI managed with a two-stage exchange procedure ranges from 4 to 6 weeks [4]. However, some studies suggest that this duration could be significantly reduced. Hoed-Reddick et al. achieved an 89% success rate in eradicating infection during staged revision for infected total knee arthroplasty, using only 24 hours of intravenous cefuroxime in a cohort of 53 patients [56].
The same team reported on a cohort of 114 patients who underwent two-stage revision procedures utilizing antibiotic-impregnated cement beads and only 24 hours of intravenous antibiotic prophylaxis [57]. With a minimum follow-up of two years, they achieved a success rate of 87.7%. These results suggest that radical debridement combined with local antibiotic delivery via cement beads may offer comparable efficacy to that of prolonged systemic antibiotic regimens [57].
While conceptually similar to the study of McKenna et al. [58], there were several important differences. The protocol of Hoad-Reddick employed vancomycin alone within biconcave cement beads, whereas Mc Kenna et al used a combination of tobramycin and vancomycin embedded in a contoured cement spacer. They believe that the spacer not only helps preserve soft tissue tension but also improves interim joint function and patient mobility, potentially contributing to a shorter hospital stay. Furthermore, their approach included a 5-day course of intravenous antibiotics, intended to eliminate residual bacteria dislodged during surgery, missed during debridement, or located in areas beyond the reach of the cement spacer [57,58].
The two-stage protocol, involving prosthesis removal and the placement of an antibiotic-loaded cement spacer, is considered the gold standard for managing late PJI in Europe and North America [59]. The most commonly used local antibiotics include vancomycin and aminoglycosides, primarily gentamicin, although tobramycin is also employed [2].
In 2019, a Swiss open-label randomized controlled trial involving 123 patients with bone and joint infections treated with hardware removal, a 4-week antibiotic regimen was shown to be non-inferior to a 6-week course. The study included 39 cases of PJI treated with a two-stage exchange [60]. Notably, only two patients (5%) received local antibiotic treatment with tobramycin. After a median follow-up of 2.2 years, no significant difference was observed between the groups, with microbiological cure rates of 98% in the 4-week group and 94% in the 6-week group [60].
6.4. PJI Treated with Total Removal Without Implantation
6.4.1. Permanent Resection Arthroplasty
Permanent resection arthroplasty is a definitive surgery intervention in PJI. It consists in a total remove of all components along with soft-tissue and bone debridement without re-implantation of new prothesis. Excision arthroplasty may be a suitable option for low-demand patients whose primary functional requirement is comfortable sitting, as this is often more easily attained compared to outcomes following knee arthrodesis [3,16,61].
As a salvage procedure, infection can be eradicated in 50% to 89% of patients [62,63]. Wasielewski et al. have managed seventy-six consecutive infected total knee arthroplasties in 74 patients. Intravenous antibiotics were administered perioperatively for a minimum duration of 3 weeks and up to 3 months. Eighty two percent of patients (41/50) received intravenous antibiotic therapy for approximately 6 weeks (±6 days). Subsequent oral antibiotics were not prescribed in all cases. Their duration varied, ranging from no oral treatment to indefinite antibiotic suppressive antibiotherapy. The cure rate was 94% [63].
Table 7 provides a synthesis of studies examining the duration of antibiotic therapy in cases of PJI managed through implant removal.
This procedure was the traditional treatment of PJI. It is suitable for young, active patients in whom reconstructive alternatives have failed, particularly those presenting with osteoarticular infection, chronic pain, leg-length discrepancy, or rotational malalignment with success rates for infection control and fusion range from 88% to 94% and 75% to 88%, respectively [71,72,73].
Antibiotic duration is controversial for arthrodesis. Kutscha-Lissberg et al. have treated their patients with parenteral antibiotics, according to the resistance of germs. It was initiated just before the operation for at least 10 days and was continued up to 6 weeks orally [72].
6.4.3. Amputation
Above-knee amputation is considered an absolute last resort in the management of PJI following total knee arthroplasty, and is rarely indicated [16]. It may be the only viable treatment in cases of life-threatening systemic sepsis which can be managed with aggressive open debridement, continuous lavage, and the use of suction drains. When bone loss is so severe that arthrodesis is no longer feasible, amputation may be the only remaining option [16]. According to IDSA guidelines published in 2013, antibiotic therapy following amputation, generally only needs to be continued for 24 to 48 hours provided that all infected tissue has been completely removed and there is no evidence of ongoing infection elsewhere in the body, such as bacteremia or a deep-seated abscess [4].
These all studies tried to reduce the antibiotic duration for PJI, but they are faced to failure rate in some cases due to the difficulty in targeting biofilm-associated bacteria.
6.5. Discussion
In the past, we used to treat people for PJI for at least 3 months much longer than the 4 to 6 weeks normally recommended for bone and joint infections without orthopedic hardware [74]. The duration is essentially due to the difficulty in eradicating bacteria within biofilms [75].
In France, Bernard et al. undertook a multi-center, randomized controlled trial (DATIPO), in which they enrolled 410 patients suffering from hip or knee PJI. Participants were randomized to receive either 6 weeks or 12 weeks of antibiotic therapy, following surgical source control [32]. The primary outcome was infection persistence or recurrence within two years following cessation of antibiotic therapy, reported in 18.1% of the 6-week group vs. 9.4% of the 12-week group. The risk difference confidence interval precluded non-inferiority for the shorter course. Sub-group analysis revealed that inferior outcomes were accentuated in patients treated with DAIR, with an absolute risk difference of 16.2%. However, no significant differences in outcomes between 6- and 12-week regimens were observed in patients managed with one- or two-stage revision. These observations demonstrate the importance of retained infected hardware, as vital to determine the prognosis of treatment of PJI [32].
In a multicenter randomized controlled trial conducted in Spain, Lora-Tamayo and collaborators evaluated an 8-week antibiotic duration compared with 3- and 6-month length regimens in the treatment of staphylococcal PJI of the hip or knee treated with DAIR [28]. The intention-to-treat analysis showed non-inferiority of clinical cure, but the trial was conducted using fluoroquinolone–rifampicin treatment groups, and excluded patients with poor initial prognosis or high risk of early treatment failure [28].
Single-stage revision surgery has gained increasing popularity in the management of PJI. Studies on single-stage revision have reported promising results, with reinfection rates ranging from 5% to 25% [35,36,37,38,39,40,41,42,43], which are comparable to those seen with two-stage revision procedures (9% to 20%) [44].
The randomized controlled trial conducted by Benkabouche et al. found no significant difference in recurrence rates between 4- and 6-week antibiotic courses following the removal of orthopedic hardware [60].
In summary of these studies, the overall evidence suggests that antibiotic duration may be safely reduced to 6 weeks in selected patient groups particularly those with acute PJI at low risk of failure following DAIR, and those with chronic infections managed through revision surgery. The results of the SOLARIO trial are awaited [76]. It is a multicenter, open-label, randomized controlled non-inferiority study designed to compare short versus long systemic antibiotic therapy in conjunction with local antibiotic treatment for orthopedic infections. Participants will be randomized 1:1 to receive either a short course (≤ 7 days) or a standard long course (≥ 4 weeks) of systemic antibiotics. The primary endpoint is treatment failure within 12 months post-surgery, evaluated by an independent, blinded Endpoint Committee. A non-inferiority margin of 10% will be applied in both per-protocol and intention-to-treat analyses. One potential limitation of this study is that it encompasses all bone and joint infections, which may reduce the specificity of the findings for particular subgroups, such as PJI [76].
As mentioned earlier, the duration of antibiotics was prolonged due to biofilm-embedded bacteria. The switch to oral therapy is now possible and it has gained interest after the British randomized controlled trial OVIVA conducted in 2019 [19]. This study involved 1,054 patients with BJI. Participants were randomized to either switch to oral therapy within 7 days after surgery or continue with a full 6-week course of intravenous antibiotics, followed by additional oral therapy if necessary. Among the randomized patients, 61% had infections related to a foreign body, including prosthetic joints. The surgery procedures included DAIR, implant removal, or one- or two-stage exchange procedures [19]. The results showed that early oral treatment, administered to approximately 90% of patients in the oral therapy arm, was non-inferior to the prolonged intravenous antibiotic regimen in terms of treatment failure. This trial supports the early transition to oral antibiotics for complex orthopedic implant-related infections, provided that adequate surgical debridement is performed and an oral antibiotic with antibiofilm properties and sufficient bioavailability is available [19].
7. The Role of Biofilms in PJI Treatment
The formation of biofilms on implanted devices plays a crucial role in the onset and persistence of infections [15].
Biofilm formation is a key factor complicating PJI management, as bacteria within biofilms exhibit significant resistance to both antibiotics and host immune responses [1,77]. The biofilm protects the bacteria via its matrix against antibiotics or immune cell attacks. This matrix is a polarized and contains proteins, polysaccharides, nucleic acids and lipids [78]. To penetrate biofilm, antibiotics should have proteins as a target and an extended duration is required. For more antibiotic efficiency, it is valuable to measure the biofilm matrix, biomass and viability [78].
Anti-biofilm molecules usually combine various compounds inhibiting the biofilm formation. They are mainly isolated from natural sources, or can be synthetic compounds. Chelating agents and antibiotics have also been found to possess anti-biofilm activity [78].
Studies have highlighted the importance of combining surgical debridement with biofilm-active antibiotics, such as rifampin in combination with a fluoroquinolone, to improve treatment outcomes [79,80].
Despite these strategies, the persistence of biofilm-related infections underscores the need for novel therapeutic approaches and further research into biofilm-targeted treatments [81].
Recently a phase 1 clinical study analyzing TRL1068, a native human monoclonal antibody that destabilize bacterial biofilms yielded promising results [81]. This is the first in-human research. It has the advantage of a broad-spectrum activity against both Gram-positive and Gram-negative species in PJI [81].
8. Future Perspectives
In recent years, artificial intelligence (AI) has become very popular in medical imaging, and convolutional neural networks have been widely used for their excellent performance, high accuracy, and short response time.
The diagnosis of PJI is challenging and costly. A missed or delayed diagnosis can have a tremendous impact on patients and put high financial strain on our healthcare budget. Advancements in artificial intelligence, molecular diagnostics and pathogen-specific treatments offer promising avenues for improving PJI management.
The BIOFIRE® Joint Infection Panel is a diagnostic test that utilizes multiplex PCR technology to identify microorganisms in synovial fluid samples from patients suspected of having septic arthritis in native joints or PJI with high sensitivity and specificity [82]. It allows a rapid microbiological diagnosis which could reduce empirical antibiotic treatment. Moreover, it improves bacterial identification especially in case with previous antibiotic treatment.
Next-generation sequencing (NGS) is being increasingly adopted for the diagnosis of PJI; however, its clinical value remains inadequately defined [83]. Shotgun metagenomic sequencing (sNGS) has shown promise in identifying pathogens in sonicate fluid that are missed by conventional culture methods. Despite its diagnostic potential, sNGS remains technically demanding and expensive. In this context, Hong et al. conducted a study in which 16S ribosomal RNA (rRNA) gene-based targeted metagenomic sequencing (tNGS) was evaluated alongside sNGS for microbial detection and identification in sonicate fluid samples from patients with failed total THA and TKA. 16S rRNA gene-based tNGS represents a promising diagnostic approach for identifying pathogens in sonicate fluid from failed total hip and knee arthroplasties, particularly in culture-negative PJI cases. Its performance characteristics are comparable to those of sNGS [83].
The integration of AI and machine learning (ML) into clinical decision-making could further sharpen PJI management by analyzing patient-specific factors and predicting optimal treatment strategies.
Machine learning is a subset of artificial intelligence that can mimic human thought processes and, in some cases, even surpass human capabilities. Developing an ML model typically involves dividing large datasets and their outcomes into training and test sets, which are then fed into a computer system. The system analyzes the data to identify patterns and creates an algorithm based on these associations. It generates an algorithm that can then be applied to make predictions or decisions on new, previously unseen data [84].
In a systematic review conducted by Chong et al. numerous parameters were discussed: prediction, diagnosis, treatment and prognosis [84]. The prediction of the early preoperative risk of PJI may help for a better optimization of surgery decisions. Machine learning may assist in the diagnosis of PJI in a manner distinct from the 2018 International Consensus Meeting (ICM) and the 2021 European Bone and Joint Infection Society (EBJIS) definitions, as they rely on neutrophil count and the positive high-power field number. In contrast, the ML model may bypass these parameters, as the diagnosis is not exclusively based on neutrophil count, but also incorporates several other infection indicators, such as tissue edema, capillary hyperplasia, and neutrophil infiltration and proliferation [5,84,85]. With regard to antibiotic prescription, as ML can generate infection predictions in a short time frame, it allows the early prescription of antibiotics [84]. Several ML models exhibit microbiological capabilities, including the identification of antibiotic susceptibility in pathogens associated with clinical failure, particularly non-culturable PJI pathogens, which are implicated in 5%–42% of PJI cases [84].
To improve treatment outcomes, it is essential to make an early and accurate decision regarding the appropriate therapeutic approach and to optimize the patient’s condition preoperatively. ML may assist in identifying patients who require such optimization to ensure a better prognosis [84,86].
Recently a novel ML-derived PJI “in-time” diagnostic system constructed by Chen et al. have demonstrated significantly improved diagnostic potency for surgical decision-making compared with the commonly used criteria [86]. The sensitivity and precision of this model were significantly higher than those observed in the ICM 2018 in their development cohort (90.6% vs. 76.1%, p = 0.032; 94.5% vs. 86.7%, p = 0.020) and in the internal validation cohort (84.2% vs. 78.6%; 94.6% vs. 81.8%) [86].
9. Conclusions
This review underscores the complexity and variability of antibiotic therapy duration in PJI management, highlighting the need for a more standardized and evidence-based approach. While current practices often rely on prolonged courses, emerging data suggest that shorter durations may be effective in select cases, reducing the risks associated with extended antibiotic use. Future research should focus on multicenter trials, advanced diagnostics, and innovative therapeutic strategies to address the persistent challenges in PJI treatment. By leveraging technological advancements and fostering collaboration, the orthopedic and infectious disease communities can improve outcomes for patients with this challenging condition.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Patel, R. Periprosthetic Joint Infection. N Engl J Med 2023, 388, 251–262. [Google Scholar] [CrossRef] [PubMed]
- Jaime Lora-Tamayo, Mikel Mancheno-Losa , María Ángeles Meléndez-Carmona , Pilar Hernández-Jiménez , Natividad Benito and Oscar Murillo. Appropriate Duration of Antimicrobial Treatment for Prosthetic Joint Infections: A Narrative Review. Antibiotics 2024, 13(4), 293. [CrossRef]
- Zimmerli, W.; Trampuz, A.; Ochsner, P.E. Prosthetic-Joint Infections. New England Journal of Medicine 2004, 351, 1645–1654. [Google Scholar] [CrossRef] [PubMed]
- Osmon, D.R.; Berbari, E.F.; Berendt, A.R.; Lew, D.; Zimmerli, W.; Steckelberg, J.M.; Rao, N.; Hanssen, A.; Wilson, W.R. Diagnosis and Management of Prosthetic Joint Infection: Clinical Practice Guidelines by the Infectious Diseases Society of America (IDSA). Clinical Infectious Diseases 2013, 56, e1–e25. [Google Scholar] [CrossRef] [PubMed]
- Parvizi J, Tan TL, Goswami K, et al. The 2018 definition of periprosthetic hip and knee infection: an evidence-based and validated criteria. J Arthroplasty. 2018, 33, 1309–1314. [Google Scholar] [CrossRef]
- Argenson, J.N.; Arndt, M.; Babis, G.; Battenberg, A.; Budhiparama, N.; Catani, F.; Chen, F.; de Beaubien, B.; Ebied, A.; Esposito, S.; et al. Hip and Knee Section, Treatment, Debridement and Retention of Implant: Proceedings of International Consensus on Orthopedic Infections. J. Arthroplast. 2019, 34, S399–S419. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, 1–27. [Google Scholar] [CrossRef]
- Parvizi, J.; Zmistowski, B.; Berbari, E.F.; Bauer, T.W.; Springer, B.D.; Della Valle, C.J.; Garvin, K.L.; Mont, M.A.; Wongworawat, M.D.; Zalavras, C.G. New Definition for Periprosthetic Joint Infection: From the Workgroup of the Musculoskeletal Infection Society. Clinical Orthopaedics & Related Research 2011, 469, 2992–2994. [Google Scholar] [CrossRef]
- Parvizi, J.; Gehrke, T. Definition of Periprosthetic Joint Infection. The Journal of Arthroplasty 2014, 29, 1331. [Google Scholar] [CrossRef]
- Gomez-Urena, E.O.; Tande, A.J.; Osmon, D.R.; Berbari, E.F. Diagnosis of Prosthetic Joint Infection. Infectious Disease Clinics of North America 2017, 31, 219–235. [Google Scholar] [CrossRef]
- Coventry, M.B. Treatment of Infections Occurring in Total Hip Surgery. Orthop Clin North Am 1975, 6, 991–1003. [Google Scholar] [CrossRef]
- Tsukayama, D.T.; Estrada, R.; Gustilo, R.B. Infection after Total Hip Arthroplasty. A Study of the Treatment of One Hundred and Six Infections*: The Journal of Bone & Joint Surgery 1996, 78, 512–523. [Google Scholar] [CrossRef]
- Andre Lunz, Burkhard Lehner, Moritz N. Voss, Kevin Knappe, Sebastian Jaeger, Moritz M. Innmann, Tobias Renkawitz and Georg W. Omlor. Impact and Modification of the New PJI-TNM Classification for Periprosthetic Joint Infections. J. Clin. Med. 2023, 12, 1262. [Google Scholar] [CrossRef]
- Arne Kienzle, Sandy Walter, Paul Kohli, Clemens Gwinner, Sebastian Hardt, Michael Muller, Carsten Perka, Stefanie Donner. Assessing the TNM Classification for Periprosthetic Joint Infections of the Knee: Predictive Validity for Functional and Subjective Outcomes. J. Pers. Med. 2025, 15, 24. [Google Scholar] [CrossRef]
- Rabih, O. Darouiche, Treatment of Infections Associated with Surgical Implants. N Engl J Med 2004, 350, 1422–9. [Google Scholar]
- T. Gehrke, P. Alijanipour, J. Parvizi. The management of an infected total knee arthroplasty. Bone Joint J 2015, 97-B, 20–9.
- Ryan Miller, Carlos A. Higuera, Janet Wu, Pharm, Alison Klika, Maja Babic, Nicolas S. Piuzzi. Periprosthetic Joint Infection A Review of Antibiotic Treatment. JBJS REVIEWS 2020, 8, e19.00224. [Google Scholar] [CrossRef]
- Don Bambino Geno Tai, Elie F. Berbari, Gina A. Suh, Brian D. Lahr, Matthew P. Abdel, and Aaron J Tande. Truth in DAIR: Duration of Therapy and the Use of Quinolone/Rifampin-Based Regimens After Debridement and Implant Retention for Periprosthetic Joint Infections. Open Forum Infect Dis. 2022 Jul 25;9, ofac363. [CrossRef]
- Li HK, Rombach I, Zambellas R, et al. Oral versus intravenous antibiotics for bone and joint infection. N Engl J Med. 2019, 380, 425–36. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Berdal J, Skramm I, Mowinckel P, Gulbrandsen P, Bjørnholt JV. Useof rifampicin and ciprofloxacin combination therapy after surgical debridement in the treatment of early manifestation prosthetic joint infections. Clin Microbiol Infect 2005, 11, 843–845. [Google Scholar] [CrossRef]
- Soriano A, Garcıa S, Bori G et al. Treatment of acute post-surgical infection of joint arthroplasty. Clin Microbiol Infect 2006, 12, 930–933. [Google Scholar] [CrossRef]
- Martinez-Pastor JC, Munoz-Mahamud E, Vilchez F et al. Outcome of acute prosthetic joint infections due to gram-negative bacilli treated with open debridement and retention of the prosthesis. Antimicrob Agents Chemother 2009, 53, 4772–4777. [Google Scholar] [CrossRef]
- Cobo J, Miguel LGS, Euba G et al. Early prosthetic joint infection: outcomes with debridement and implant retention followed by antibiotic therapy. Clin Microbiol Infect 2010, 17, 1632–1637. [Google Scholar]
- Vilchez F, Martı´nez-Pastor JC, Garcıa-Ramiro S et al. Outcome and predictors of treatment failure in early post-surgical prosthetic joint infections due to Staphylococcus aureus treated with debridement. Clin Microbiol Infect 2011, 17, 439–444. [Google Scholar] [CrossRef] [PubMed]
- Tornero, E.; Morata, L.; Martínez-Pastor, J.C.; Angulo, S.; Combalia, A.; Bori, G.; García-Ramiro, S.; Bosch, J.; Mensa, J.; Soriano, A. Importance of selection and duration of antibiotic regimen in prosthetic joint infections treated with debridement and implant retention. J. Antimicrob. Chemother. 2016, 71, 1395–1401. [Google Scholar] [CrossRef] [PubMed]
- A.-P. Puhto, T. A.-P. Puhto, T. Puhto and H. Syrjala. Short-course antibiotics for prosthetic joint infections treated with prosthesis retention.
- Lora-Tamayo, J.; Murillo, O.; Iribarren, J.A.; Soriano, A.; Sánchez-Somolinos, M.; Baraia-Etxaburu, J.M.; Rico, A.; Palomino, J.; Rodríguez-Pardo, D.; Horcajada, J.P.; et al. A large multicenter study of methicillin-susceptible and methicillin-resistant staphylococcus aureus prosthetic joint infections managed with implant retention. Clin. Infect. Dis. 2013, 56, 182–194. [Google Scholar] [CrossRef] [PubMed]
- Lora-Tamayo, J.; Euba, G.; Cobo, J.; Horcajada, J.P.; Soriano, A.; Sandoval, E.; Pigrau, C.; Benito, N.; Falgueras, L.; Palomino, J.; et al. Short- versus long-duration levofloxacin plus rifampicin for acute staphylococcal prosthetic joint infection managed with implant retention: A randomised clinical trial. Int. J. Antimicrob. Agents 2016, 48, 310–316. [Google Scholar] [CrossRef]
- American Academy of Orthopaedic Surgeons. Systematic Literature Review on the Management of Surgical Site Infections. Report No.: 9 June 2018. Available online: https://www.aaos.org/globalassets/quality-and-practice-resources/surgical-siteinfections/ssi-sr_8-29-19.pdf (accessed on 15 March 2024).
- Bernard, L.; Legout, L.; Zürcher-Pfund, L.; Stern, R.; Rohner, P.; Peter, R.; Assal, M.; Lew, D.; Hoffmeyer, P.; Six, I.U. Six weeks of antibiotic treatment is sufficient following surgery for septic arthroplasty. J. Infect. 2010, 61, 125–132. [Google Scholar] [CrossRef]
- Chaussade, H.; Uçkay, I.; Vuagnat, A.; Druon, J.; Gras, G.; Rosset, P.; Lipsky, B.A.; Bernard, L. Antibiotic therapy duration for prosthetic joint infections treated by Debridement and Implant Retention (DAIR): Similar long-term remission for 6 weeks as compared to 12 weeks. Int. J. Infect. Dis. 2017, 63, 37–42. [Google Scholar] [CrossRef]
- Bernard, L.; Arvieux, C.; Brunschweiler, B.; Touchais, S.; Ansart, S.; Bru, J.-P.; Oziol, E.; Boeri, C.; Gras, G.; Druon, J.; et al. Antibiotic Therapy for 6 or 12 Weeks for Prosthetic Joint Infection. N. Engl. J. Med. 2021, 384, 1991–2001. [Google Scholar] [CrossRef]
- Khaled, M. Yaghmour, Emanuele Chisari and Wasim S. Khan. Single-Stage Revision Surgery in Infected Total Knee Arthroplasty: A PRISMA Systematic Review. J. Clin. Med. 2019, 8, 174. [Google Scholar] [CrossRef]
- Rowan, F.E.; Donaldson, M.J.; Pietrzak, J.R.; Haddad, F.S. The Role of One-Stage Exchange for Prosthetic Joint Infection. Curr. Rev. Musculoskelet. Med. 2018, 11, 370–379. [Google Scholar] [CrossRef]
- Haddad, F.S.; Sukeik, M.; Alazzawi, S. Is Single-stage Revision According to a Strict Protocol Effective in Treatment of Chronic Knee Arthroplasty Infections? Clin. Orthop. Relat. Res. 2015, 473, 8–14. [Google Scholar]
- Castellani, L.; Daneman, N.; Mubareka, S.; Jenkinson, R. Factors Associated with Choice and Success of OneVersus Two-Stage Revision Arthroplasty for Infected Hip and Knee Prostheses. HSS J. 2017, 13, 224–231. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Ni, M.; Li, X.X.; Zhang, Q.; Li, X.X.; Chen, J. Two-stage revisions for culture-negative infected total knee arthroplasties: A five-year outcome in comparison with one-stage and two-stage revisions for culture-positive cases. J. Orthop. Sci. 2017, 22, 306–312. [Google Scholar] [CrossRef] [PubMed]
- Jenny, J.Y.; Barbe, B.; Gaudias, J.; Boeri, C.; Argenson, J.N. High infection control rate and function after routine one-stage exchange for chronically infected TKA. Clin. Orthop. Relat. Res. 2013, 471, 238–243. [Google Scholar] [CrossRef] [PubMed]
- Cochran, A.R.; Ong, K.L.; Lau, E.; Mont, M.A.; Malkani, A.L. Risk of Reinfection After Treatment of Infected Total Knee Arthroplasty. J. Arthroplast. 2016, 31, 156–161. [Google Scholar] [CrossRef]
- Massin, P.; Delory, T.; Lhotellier, L.; Pasquier, G.; Roche, O.; Cazenave, A.; Estellat, C.; Jenny, J.Y. Infection recurrence factors in one- and two-stage total knee prosthesis exchanges. Knee Surg. Sport Traumatol. Arthrosc. 2016, 24, 3131–3139. [Google Scholar] [CrossRef]
- Singer, J.; Merz, A.; Frommelt, L.; Fink, B. High rate of infection control with one-stage revision of septic knee prostheses excluding MRSA and MRSE. Clin. Orthop. Relat. Res. 2012, 470, 1461–1471. [Google Scholar] [CrossRef]
- Shanmugasundaram, S.; Ricciardi, B.F.; Briggs, T.W.R.; Sussmann, P.S.; Bostrom, M.P. Evaluation and Management of Periprosthetic Joint Infection-an International, Multicenter Study. HSS J. 2014, 10, 36–44. [Google Scholar] [CrossRef]
- Jenny, J.Y.; Barbe, B.; Cazenave, A.; Roche, O.; Massin, P. Patient selection does not improve the success rate of infected TKA one stage exchange. Knee 2016, 23, 1012–1015. [Google Scholar] [CrossRef]
- Setor, K. Kunutsor*, Michael R. Whitehouse, Ashley W. Blom, Andrew D. Beswick, INFORM Team. Patient-Related Risk Factors for Periprosthetic Joint Infection after Total Joint Arthroplasty: A Systematic Review and Meta-Analysis. PLOS ONE |. [CrossRef]
- Tibrewal, S.; Malagelada, F.; Jeyaseelan, L.; Posch, F.; Scott, G. Single-stage revision for the infected total knee replacement: Results from a single centre. Bone Jt. J. 2014, 96, 759–764. [Google Scholar] [CrossRef]
- Buchholz HW, Elson RA, Engelbrecht E, Lodenkamper H, Rottger J, Siegel A. Management of deep infection of total hip replacement. J Bone Joint Surg Br 1981, 63-B, 342–353.
- Ammon P, Stockley I. Allograft bone in two-stage revision of the hip for infection. Is it safe? J Bone Joint Surg Br 2004, 86, 962–965. [Google Scholar]
- Stockley I, Mockford BJ, Hoad-Reddick A, Norman P. The use of two-stage exchange arthroplasty with depot antibiotics in the absence of long-term antibiotic therapy in infected total hip replacement. J Bone Joint Surg Br 2008, 90, 145–148. [Google Scholar]
- Kendoff D, Gehrke T. Surgical management of periprosthetic joint infection: one-stage exchange. J Knee Surg. 2014, 27, 273–278. [Google Scholar] [CrossRef] [PubMed]
- Whiteside, L.A.; Peppers, M.; Nayfeh, T.A.; Roy, M.E. Methicillin-resistant Staphylococcus aureus in TKA treated with revision and direct intra-articular antibiotic infusion. Clin. Orthop. Relat. Res. 2011, 469, 26–33. [Google Scholar] [CrossRef] [PubMed]
- Baker, P.; Petheram, T.G.; Kurtz, S.; Konttinen, Y.T.; Gregg, P.; Deehan, D. Patient reported outcome measures after revision of the infected TKR: Comparison of single versus two-stage revision. Knee Surg. Sport Traumatol. Arthrosc. 2013, 21, 2713–2720. [Google Scholar] [CrossRef]
- de Paula Leite Cury, R.; Cinagawa, E.H.T.; Camargo, O.P.A.; Honda, E.K.; Klautau, G.B.; Salles, M.J.C. Treatment of infection after total knee arthroplasty. Acta Ortopédica Bras. 2015, 23, 239–243. [Google Scholar] [CrossRef]
- Zahar, A.; Kendoff, D.O.; Klatte, T.O.; Gehrke, T.A. Can Good Infection Control Be Obtained in One-stage Exchange of the Infected TKA to a Rotating Hinge Design? 10–year Results. Clin. Orthop. Relat. Res. 2016, 474, 81–87. [Google Scholar] [CrossRef]
- Raut VV, Siney PD, Wroblewski BM. One-stage revision of infected total hip replacements with discharging sinuses. J Bone Joint Surg Br 1994, 76, 721–724. [Google Scholar]
- Buttaro MA, Pusso R, Piccaluga F. Vancomycin-supplemented impacted bone allografts in infected hip arthroplasty. Two-stage revision results. J Bone Joint Surg Br 2005, 87, 314–319. [Google Scholar]
- Hoad-Reddick DA, Evans CR, Norman P, Stockley I. Is there a role for extended antibiotic therapy in a two-stage revision of the infected knee arthroplasty? J Bone Joint Surg Br 2005, 87, 171–174. [Google Scholar]
- Stockley I, Mockford BJ, Hoad-Reddick A, Norman P. The use of two-stage exchange arthroplasty with depot antibiotics in the absence of long-term antibiotic therapy in infected total hip replacement. J Bone Joint Surg Br 2008, 90, 145–148.
- Paul, B. McKenna · Keiran O’Shea · Eric L. Masterson.Two-stage revision of infected hip arthroplasty using a shortened post-operative course of antibiotics. Arch Orthop Trauma Surg 2009, 129, 489–494. [Google Scholar] [CrossRef]
- Anagnostakos, K. Therapeutic use of antibiotic-loaded bone cement in the treatment of hip and knee joint infections. J Bone Joint Infect. 2017, 2, 29–37. [Google Scholar] [CrossRef] [PubMed]
- Benkabouche, M.; Racloz, G.; Spechbach, H.; Lipsky, B.A.; Gaspoz, J.M.; Uçkay, I. Four versus six weeks of antibiotic therapy for osteoarticular infections after implant removal: A randomized trial. J. Antimicrob. Chemother. 2019, 74, 2394–2399. [Google Scholar] [CrossRef] [PubMed]
- Ilker Uçkay, Kheeldass Jugun, Axel Gamulin, Joe Wagener, Pierre Hoffmeyer, Daniel Lew. Chronic Osteomyelitis. Curr Infect Dis Rep 2012, 14, 566–575. [Google Scholar] [CrossRef]
- Falahee MH, Matthews LS, Kaufer H. Resection arthroplasty as a salvage procedure for a knee with infection after a total arthroplasty. J Bone Joint Surg [Am] 1987, 69-A, 1013–1021.
- Wasielewski RC, Barden RM, Rosenberg AG. Results of different surgical procedures on total knee arthroplasty infections. J Arthroplasty 1996, 11, 931–93. [Google Scholar] [CrossRef]
- Taggart, T.; Kerry, R.M.; Norman, P.; Stockley, I. The use of vancomycin-impregnated cement beads in the management of infection of prosthetic joints. J. Bone Jt. Surg. Br. 2002, 84, 70–72. [Google Scholar] [CrossRef]
- Hart, W.J.; Jones, R.S. Two-stage revision of infected total knee replacements using articulating cement spacers and short-term antibiotic therapy. J. Bone Jt. Surg. Ser. B 2006, 88, 1011–1015. [Google Scholar] [CrossRef]
- Whittaker, J.P.; Warren, R.E.; Jones, R.S.; Gregson, P.A. Is prolonged systemic antibiotic treatment essential in two-stage revision hip replacement for chronic Gram-positive infection? J. Bone Jt. Surg. Ser. B 2009, 91, 44–51. [Google Scholar] [CrossRef]
- Mittal, Y.; Fehring, T.K.; Hanssen, A.; Marculescu, C.; Odum, S.M.; Osmon, D. Two-stage reimplantation for periprosthetic knee infection involving resistant organisms. J. Bone Jt. Surg. 2007, 89, 1227–1231. [Google Scholar] [CrossRef]
- Hsieh, P.H.; Huang, K.C.; Lee, P.C.; Lee, M.S. Two-stage revision of infected hip arthroplasty using an antibiotic-loaded spacer: Retrospective comparison between short-term and prolonged antibiotic therapy. J. Antimicrob. Chemother. 2009, 64, 392–397. [Google Scholar] [CrossRef]
- El Helou, O.C.; Berbari, E.F.; Lahr, B.D.; Marculescu, C.E.; Razonable, R.R.; Steckelberg, J.M.; Hanssen, A.D.; Osmon, D.R. Management of prosthetic joint infection treated with two-stage exchange: The impact of antimicrobial therapy duration. Curr. Orthop. Pract. 2011, 22, 333–338. [Google Scholar] [CrossRef]
- Ma, H.H.; Chou, T.F.A.; Tsai, S.W.; Chen, C.F.; Wu, P.K.; Chen, C.M.; Wu, P.-K.; Chen, C.-M.; Chen, W.-M. Is short-course systemic antibiotic therapy using an antibiotic-loaded cement spacer safe after resection for infected total knee arthroplasty? A comparative study. J. Formos. Med. Assoc. 2020, 119, 1070–1079. [Google Scholar] [CrossRef] [PubMed]
- Mabry TM, Jacofsky DJ, Haidukewych GJ, et al. Comparison of intramedullary nailing and external fixation knee arthrodesis for the infected knee replacement. Clin Orthop Relat Res 2007, 464, 11–15. [Google Scholar] [CrossRef] [PubMed]
- Kutscha-Lissberg F, Hebler U, Esenwein SA, et al. Fusion of the septic knee with external hybrid fixator. Knee Surg Sports Traumatol Arthrosc 2006, 14, 968–974. [Google Scholar] [CrossRef]
- Spina M, Gualdrini G, Fosco M, et al. Knee arthrodesis with the Ilizarov external fixator as treatment for septic failure of knee arthroplasty. J Orthop Traumatol 2010, 11, 81–88. [Google Scholar] [CrossRef]
- Benjamin Le Vavasseur, Valérie Zeller. Antibiotic Therapy for Prosthetic Joint Infections: An Overview. Antibiotics 2022, 11, 486. [Google Scholar] [CrossRef]
- Wouter Rottier, Jessica Seidelman and Marjan Wouthuyzen-Bakker. Antimicrobial treatment of patients with a periprosthetic joint infection: basic principles. l. Arthroplasty 2023, 5, 10. [Google Scholar] [CrossRef]
- Maria Dudareva, Michelle Kümin, Werner Vach, Klaus Kaier, Jamie Ferguson, Martin McNally and Matthew Scarborough. Short or Long Antibiotic Regimes in Orthopaedics (SOLARIO): a randomised controlled open-label non-inferiority trial of duration of systemic antibiotics in adults with orthopaedic infection treated operatively with local antibiotic therapy. Trials 2019, 20, 693. [Google Scholar] [CrossRef]
- Costerton, J.W.; Stewart, P.S.; Greenberg, E.P. Bacterial Biofilms: A Common Cause of Persistent Infections. Science 1999, 284, 1318–1322. [Google Scholar] [CrossRef]
- Roy, R.; Tiwari, M.; Donelli, G.; Tiwari, V. Strategies for Combating Bacterial Biofilms: A Focus on Anti-Biofilm Agents and Their Mechanisms of Action. Virulence 2018, 9, 522–554. [Google Scholar] [CrossRef]
- Widmer, A.F.; Gaechter, A.; Ochsner, P.E.; Zimmerli, W. Antimicrobial Treatment of Orthopedic Implant-Related Infections with Rifampin Combinations. Clinical Infectious Diseases 1992, 14, 1251–1253. [Google Scholar] [CrossRef] [PubMed]
- Drancourt, M.; Stein, A.; Argenson, J.N.; Zannier, A.; Curvale, G.; Raoult, D. Oral Rifampin plus Ofloxacin for Treatment of Staphylococcus-Infected Orthopedic Implants. Antimicrob Agents Chemother 1993, 37, 1214–1218. [Google Scholar] [CrossRef] [PubMed]
- Conway, J.; Delanois, R.E.; Mont, M.A.; Stavrakis, A.; McPherson, E.; Stolarski, E.; Incavo, S.; Oakes, D.; Salvagno, R.; Adams, J.S.; et al. Phase 1 Study of the Pharmacokinetics and Clinical Proof-of-Concept Activity of a Biofilm-Disrupting Human Monoclonal Antibody in Patients with Chronic Prosthetic Joint Infection of the Knee or Hip. Antimicrob Agents Chemother 2024, 68, e00655–24. [Google Scholar] [CrossRef] [PubMed]
- Stéphanie, Pascual; et al. Potential value of a rapid syndromic multiplex PCR for the diagnosis of native and prosthetic joint infections: a real-world evidence study. J. Bone Joint Infect. 2024, 9, 87–97. [Google Scholar] [CrossRef]
- Hyo-Lim Hong. Targeted Versus Shotgun Metagenomic Sequencing-based Detection of Microorganisms in Sonicate Fluid for Periprosthetic Joint Infection Diagnosis. e1456 CID 2023:76 (1 February).
- Yuk Yee Chong, Ping Keung Chan1, Vincent Wai Kwan Chan, Amy Cheung, Michelle Hilda Luk, Man Hong Cheung, Henry Fu1 and Kwong Yuen Chiu. Application of machine learning in the prevention of periprosthetic joint infection following total knee arthroplasty: a systematic review. Arthroplasty 2023, 5, 38. [Google Scholar] [CrossRef]
- McNally M, Sousa R, Wouthuyzen-Bakker M, Chen AF, Soriano A, Vogely HC, et al. The EBJIS defnition of periprosthetic joint infection. Bone Joint J. 2021, 103-B, 18–25.
- Chen, W.; Hu, X.; Gu, C.; Zhang, Z.; Zheng, L.; Pan, B.; Wu, X.; Sun, W.; Sheng, P. A machine learning-based model for “In-time” prediction of periprosthetic joint infection. DIGITAL HEALTH Volume 10: 1–15 : sagepub.com/journals-permissions. https://doi.org/10.1177/20552076241253531 journals.sagepub.com/home/dhj. [CrossRef]
Figure 1.
PRISMA Flow Diagram of PJI Systematic Review.
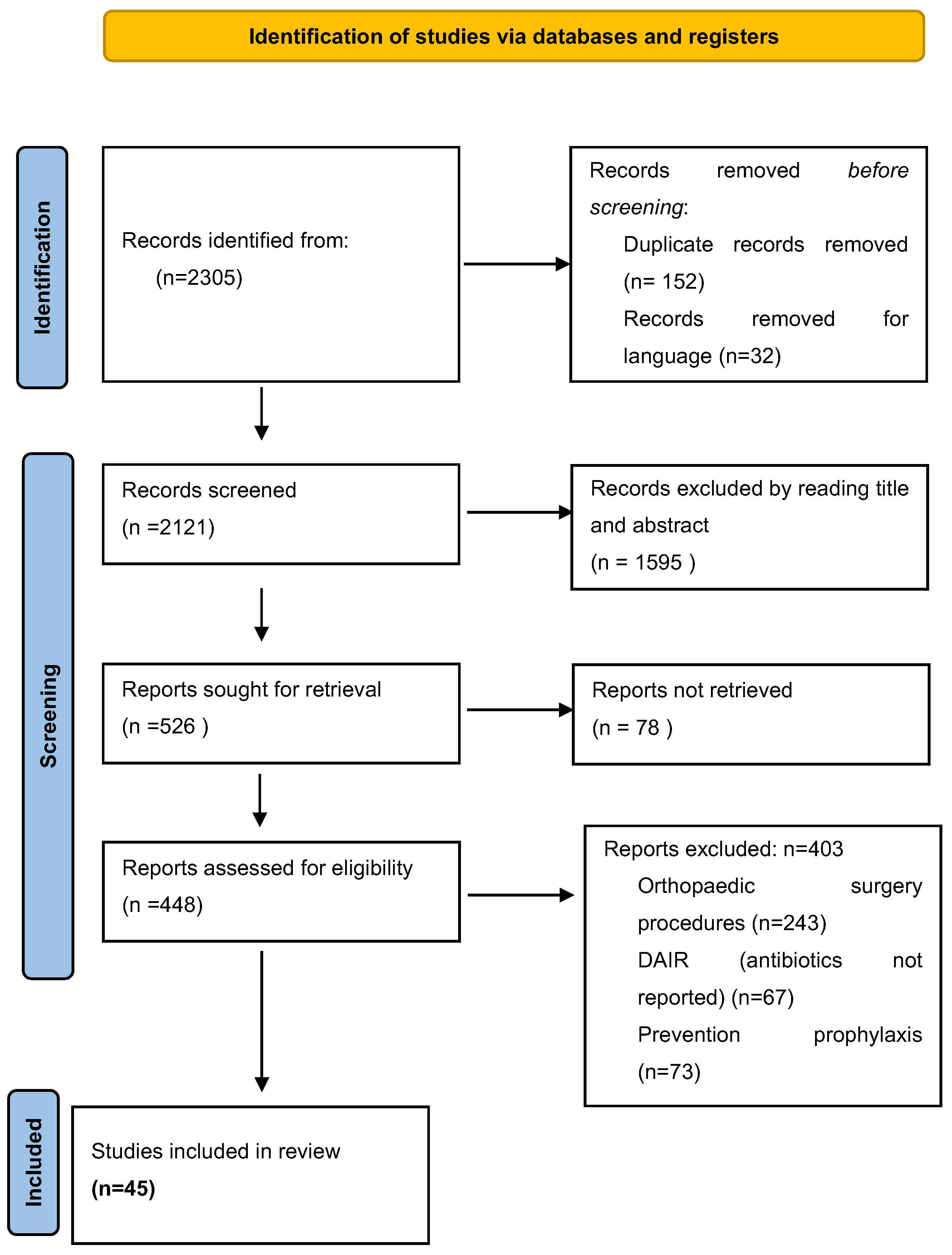

Table 1.
Proposed definitions of prosthetic joint infections.
| Musculoskeletal Infection Society (MSIS) 2011 [8] |
International Consensus Meeting 2013 [9] |
IDSA 2013 [4] | Musculoskeletal Infection Society (MSIS) 2018 [5] |
|---|---|---|---|
| Infected if at least one major criteria is present: - Two positive periprosthetic cultures with phenotypically identical organisms - A sinus tract communicating with the joint - Presence of purulence in the affected joint - Positive histologic analysis of periprosthetic tissue - A single positive culture |
Infected if at least one major criteria is present: - Two positive periprosthetic cultures with phenotypically identical organisms - A sinus tract communicating with the joint |
Infected if one of the following criteria is present: - Sinus tract communicating with prosthesis - Presence of purulence - Acute inflammation on histopathologic evaluation of periprosthetic tissue - Two or more positive cultures with the same organism (intra-operatively and/or pre-operatively) - Single positive culture with virulent organism |
Infected if at least one major criteria is present: - Two positive cultures of the same organism - Sinus tract with evidence of communication to the joint or visualization of the prosthesis |
| Infected if at least four out of six minor criteria exist: - Elevated CRP and ESR - Elevated synovial fluid PMN% |
Infected if three out of five minor criteria exist: - Elevated CRP and ESR - Elevated synovial fluid WBC count or ++ change on leukocyte esterase test strip -Elevated synovial fluid PMN% -Positive histologic analysis of periprosthetic tissue -A single positive culture |
Infected if preoperative diagnosis score ≥ 6 / Possibly infected if preoperative diagnosis score between 2 and 5: - Elevated CRP or D-Dimer (Serum): 2 - Elevated ESR (Serum): 1 - Elevated synovial WBC count or LE (Synovial): 3 - Positive alpha-defensin (Synovial): 3 - Elevated synovial PMN (%): 2 - Elevated synovial CRP: 1 Infected if intraoperative diagnosis score ≥ 6 / Possibly infected if intraoperative diagnosis score between 4 and 5: - Positive histology: 3 - Positive purulence: 3 - Single positive culture: 2 |
Abbreviations: CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; WBC: white blood cells, PMN%, polymorphonuclear neutrophils percentage. Proceed with caution in: adverse local tissue reaction, crystal deposition disease, slow growing organisms. ; LE, leukocyte esterase; . a For patients with inconclusive minor criteria, operative criteria can also be used to fulfill definition for PJI. b Consider further molecular diagnostics such as next-generation sequencing.
Table 2.
Classification and clinical presentation of prosthetic joint infections.
| Type of Infection |
Time of presentation | Mechanism of infection | Clinical Presentation | Organisms | |
|---|---|---|---|---|---|
| Early | < 3 months | Intraoperative contamination |
Acute | Acute Sudden onset erythema, edema, warmth, and tenderness |
Virulent bacteria (i.e., Staphylococcus aureus) |
| Delayed | 3-12 months | Intraoperative contamination |
Chronic | Joint pain and stiffness |
Low virulent bacteria (coagulase-negative staphylococci) |
| Late | >12 months | Hematogenous Seeding Intraoperative contamination |
Acute Chronic |
Sudden-onset erythema, edema, tenderness and warmth, Joint pain, sinus tract |
Virulent bacteria (i.e., S.aureus) Low virulent bacteria (i.e., Propionibacterium acnes) |
Table 3.
The original PJI-TNM classification as introduced by Alt et al. in 2020 [14].
Table 3.
The original PJI-TNM classification as introduced by Alt et al. in 2020 [14].
| T/N/M | Classification | Subclassification | Descriptive |
|---|---|---|---|
| T: Tissue and Implant Conditions | T0 T1 T2 |
a b a b a b |
Stable standard implant without important soft tissue defect Stable revision implant without important soft tissue defect Loosened standard implant without important soft tissue defect Loosened revision implant without important soft tissue defect Severe soft tissue defect with standard implant Severe soft tissue defect with revision implant |
| N: Non-human Cells (Bacteria and Fungi) | NO N1 N2 |
a b a b a b c |
No mature biofilm formation (former: acute), directly postoperatively No mature biofilm formation (former: acute), late hematogenous Mature biofilm formation (former: chronic) without ‘difficult to treat bacteria’ Mature biofilm formation (former: chronic) with culture-negative infection Mature biofilm formation (former: chronic) with ‘difficult to treat bacteria’ Mature biofilm formation (former: chronic) with polymicrobial infection Mature biofilm formation (former: chronic) with fungi |
| M: Morbidity of the Patient | M0 M1 M2 M3 |
a b c |
Not or only mildly compromised (Charlson Comorbidity Index: 0–1) Moderately compromised patient (Charlson Comorbidity Index: 2–3) Severely compromised patient (Charlson Comorbidity Index: 4–5) Patient refuses surgical treatment Patient does not benefit from surgical treatment Patient does not survive surgical treatment |
T – Tissue and implant conditions. For this item: standard implants (‘a’) versus revision implants (‘b’); N – Non-human cells (bacteria and/or fungi), M – Morbidity of the patient, r: recurrent infection.
Table 4.
Summary of Non-Comparative Studies on Antibiotic Treatment Duration in Prosthetic Joint Infections Managed with DAIR.
Table 4.
Summary of Non-Comparative Studies on Antibiotic Treatment Duration in Prosthetic Joint Infections Managed with DAIR.
| Author Year Reference | Study design | Patients N | Bacteria Major strains isolated | Antibiotics | Antibiotic duration (mean) | Follow-up (mean) Months | Success treatment rate (%) |
|---|---|---|---|---|---|---|---|
| Berdal et al. 2005 [20] | Prospective | 29 | Staphylococcus aureus | Rifampicin plus Cirpofloxacin | 3 Months | 22.5 | 83 |
| Soriano et al. 2006 [21] | Prospective | 39 | Gram positive Cocci | Levofloxacin plus Rifampicin | 2.7 +/-1 Months | 24 | 76.6 |
| Martínez-Pastor et al. 2009 [22] | Prospective | 47 | Enterobacteriaceae family | Bata-lactam for IVFluoroquinolones for oral | Intraveinous 14 days Oral 2.6 months |
15.4 | 74.5 |
| Cobo et al. 2010 [23] | Prospective | 117 | Gram negative strains Gram positive cocci |
Not reported | 2.5 Months | 25 | 57.3 |
| Vilchez et al. 2011 [24] | Prospective | 53 | Staphylococcus aureus | IV: 11 ± 7 days and oral 88 ± 46 days |
24 | 75.5 | |
| Tornero et al. 2015 [25] | Prospective | 143 | Gram negative strains Gram positive cocci |
Fluoroquinolones Rifampicin in combination |
IV: 8 days Oral 69 days |
48 | 88.2 |
Table 5.
Summary of Studies on Antibiotic Treatment Duration for Prosthetic Joint Infections managed by DAIR.
Table 5.
Summary of Studies on Antibiotic Treatment Duration for Prosthetic Joint Infections managed by DAIR.
| Author Year (Reference) | Study design | Bacteria (Major Strains Isolated) | Antibiotics (Major prescribed) | Antibiotic duration | Patients in each arm | Outcome & Conclusion |
|---|---|---|---|---|---|---|
| Bernard et al. 2010 [30] |
Prospective observational, non-randomized monocentric |
Staphylococci (66%) |
Rifampicin (n=58, always in combination and only for staphylococcal infections), Ciprofloxacin (n=42), vancomycin (n=40), and amoxicillin/clavulanic acid (n=25). |
6 weeks vs 12 weeks |
144 episodes -6 weeks: 70 episodes (70/144, 49%) -12 weeks: 74 episodes(74/144, 51%) |
Overall cure in 115 episodes (80%) -6 weeks: 90% cure vs. -12 weeks: 55% Failure 29 (20%) antibiotic therapy might be able to be limited to a 6-week course Randomized trials are needed |
|
Puhto et al., 2012 [26] |
Retrospective observational, pre-post-design monocentric |
Staphylococcus aureus (42%) |
Rifampicin and fluoroquinolones for GP strains |
2-3 months vs 3-6 months |
ITT: long n= 60 Short n= 72 PP: long n=38 Short n=48 |
Non-inferiority of short treatments. Cure rates: ITT—Long 57%, Short 58% (p = 0.85) PP—Long 89%, Short 87% (p = 0.78) Short antibiotic treatment seems to be a good alternative for patients treated with DAIR prospective randomized controlled trials are urgently needed |
|
Lora-Tamayo. et al., 2013 [27] |
Retrospective observational, multicenter |
Staphylococcus aureus |
(>75% rifampin-based combinations) |
<61 days 61–90 days >90 days |
231 patients n=52 n=52 n=127 |
Cure rate: <61 days—75% 60–90 days—77% >90 days—77% (p = 0.434) |
|
Lora-Tamayo. et al., 2016 [28] |
Randomized, open clinical trial, multicenter |
Staphylococci |
Levofloxacin and Rifampicin |
8 weeks vs 3–6 months 3 months for hip prostheses and 6 months for knee prostheses |
N= 63 ITT: long n= 33 Short n= 30 PP: long n=20 Short n=24 |
Non-inferiority. Cure rates: ITT—Long 58%, Short 73% (Δ = −15.7 95% CI −39.2% to +7.8%) PP—Long 95%, Short 92% (Δ = +3.3% 95% CI −11.7%to +18.3%) 8 weeks of L+R could be non-inferior to longer standard treatments for acute staphylococcal PJI managed with DAIR |
| Chaussade et al. 2017 [31] | Retrospective observational, multicenter |
Staphylococci (40%) |
Rifampin-based combinations for GP and fluoroquinolones |
6 weeks vs. 12 weeks |
N= 87 -6 weeks n=44 -12 weeks n=43 |
Cure rates: 67.4% in the long treatment group 70.5% in the short treatment group (aOR 0.76, 95%CI 0.27–2.10) Prospective randomized trials are required |
|
Bernard et al. 2021 DATIPO [32] |
Randomized, open clinical trial, multicenter |
Staphylococcus aureus (30-40%) |
Rifampin-based combinations and fluoroquinolones |
6 weeks vs. 12 weeks |
N= 151 -6 weeks n=75 -12 weeks n=76 |
Failure rate for 6 weeks: 30.7% Failure rate for 12 weeks: 14.5% Difference: 16.2% (95% CI: 2.9% to 29.5%) Non inferiority was not shown |
DAIR—debridement, antibiotics, and implant retention. GP: Gram-positive microorganisms. ITT: intention-to-treat analysis. PP: per-protocol analysis. 95% CI: 95% confidence interval.
Table 6.
Summary of Studies on Antibiotic Treatment Duration for Prosthetic Joint Infections managed by single-step exchange.
Table 6.
Summary of Studies on Antibiotic Treatment Duration for Prosthetic Joint Infections managed by single-step exchange.
| Author (year, reference) | Patients N | Study design | Antibiotics (major prescribed) | Antibiotic duration | Local antibiotics or suppressive | Follow-up (mean) Years | Outcome | Conclusion |
|---|---|---|---|---|---|---|---|---|
| Whiteside et al. (2011) [50] | 18 | Retrospective Cohort | Not reported | Intravenous 2-4 weeks |
Local Vancomycin : intraaticular |
5.1 |
RR = 5.5% FO: Mean KSS was 78 ± 8 at 1year, 83 ± 9 at 2 years, 84 ± 8 at 5years, 85 ± 10 at 6 years, and 84 at 8 years |
A single-stage revision total TKA for MRSA infection, managed with six weeks of intra-articular vancomycin administration, effectively controlled the infection |
|
Singer at al. (2012) [41] |
57 | Retrospective | Rifampicin fluoro-quinolones Combination : 50.8% |
Overall duration : 6 weeks -2 weeks IV after surgery – 4 weeks : oral antibiotics |
Local Gentamicin | 3 | RR = 15% FO: KSS after surgery was 72 points (range, 20–98 points), the Knee Society function score was 71 points (range, 10–100 points), and the Oxford–12 knee score was 27 points (range, 13–44 points). |
One-stage revision of knee PJI leads to a high rate of infection control of 95% and reasonable patient function when the pathogen is identifiable and when MRSA and MRSE infections are excluded. Recurrence is about 15% in hinged prothesis |
| Jenny et al. (2013) [38] | 47 | Observational Cohort Prospective | -IV : vancomycin, teicoplanin -Oral Rifampicin Levofloaxcin |
-IV : 3.5 (1–16 weeks), -Oral : 12 (3–16 weeks) |
Suppressive ATB : not reported | 3 | RR = 12% FO: The median preoperative KSS function score was 42 points. 56% of the patients had a KSS of >150 points postoperatively | Single-stage exchange may offer a viable alternative for managing chronically infected TKA, providing a more convenient approach for patients by avoiding the risks associated with two separate surgeries and hospitalizations, while also reducing overall healthcare costs. |
| Baker et al (2013) [51] | 33 | Prospective | Not reported | Not reported | Not reported | 0.5 (7 months) |
RR = 21% FO: The mean pre– and post–operative OKS were 15 (95% CI, 13–18) and 25 (95% CI, 21–29), respectively, giving a mean improvement of 10 (95% CI, 5–14) | No difference between single-stage and two-stage revision of the infected knee replacement |
| Shanmugasundaram et al. (2014) [42] | 5 | Retrospective | Not reported | Not reported | Antibiotic spacers | 2 | RR = 17.2% FO: Not reported | In hip prosthetic joint infections (PJI), the initial success rate was 60% for one-stage exchange and 70% for two-stage exchange. For knee PJI, success rates were higher—80% for one-stage exchange and 75% for two-stage exchange. Future advances in microbiological diagnosis are needed |
| Tibrewal et al. (2014) [45] | 50 | Prospective | Not reported | -IV : 2 weeks -Oral : 3 months |
Antibiotic-impregnated cement | 10 | RR = 2% FO: the mean OKS increased by a factor of 2.4 from 14.5 (6 to 25) pre–operatively to 34.5 (26 to 38) one year after surgery. This represents a mean absolute improvement of 20.0 points (95% CI: 17.8 to 22.2, p < 0.001). | Single-stage revision may achieve clinical outcomes comparable to those of two-stage revision. Additionally, the single-stage approach is associated with reduced healthcare costs, lower patient morbidity, and decreased overall inconvenience. |
| Cury Rde P et al. (2015) [52] | 6 | Retrospective | Not reported | -IV : 2-4 weeks -Oral : 6 months |
Suppressive : 4 patients | 3 | RR = 16.7% FO: WOMAC score 49.5 (47–55) |
The DAIR, one-stage revision and two-stage revision success rates were 75%, 83.3%, and 100%, respectively |
| Haddad et al. (2015) [35] | 28 | Retrospective | Not reported | -6 Weeks (IV and/or Oral) | antibiotic-loaded cement Gentamicin Vancomycin | 2 | RR = 0% FO: KSS was higher in the single–stage group than in the two–stage group (mean, 88; range, 38–97 versus 76; range, 29–93; p < 0.001) Preoperative mean KSS was 32 in the single–stage group (range, 18–65) |
Single-stage approach can be an alternative to the two-stage procedure in carefully selected patients with chronically infected TKA. Prospective trials are needed. |
| Zahar et al. (2016) [53] | 46 | Retrospective | Not reported | 14.2 ( 10–17 days) | Antibiotic-loaded cement Gentamicin ClindamycinVancomycin |
10 | RR = 7% FO: HSS score improved significantly from a mean preoperative value of 35 (±24.2 SD; range, 13–99) to an average of 69.6 (±22.5 SD; range, 22–100) |
The overall infection control rate was of 93% and good clinical results Further research into one-stage exchange techniques for PJI in TKA are needed |
| Cochran et al. (2016) [39] | 3069 | Retrospective Observational Database | Not reported | Not reported | Not reported | 6 | RR = 24.6% at 1 year and 38.25% at 6 years FO: Not reported |
Two-stage reimplantation, despite 19% recurrence, had the highest success rateover single-stage and DAIR. |
| Jenny et al. (2016) [43] | Intervention group = 54, Control group = 77, | Retrospective case-control | Not reported | 3 months | Not reported | 2 | RR = Intervention group: 15% Control group: 22% FO: KSS over 160 points (80%). No significant difference between the two groups | When a single-stage exchange is performed, patient selection does not appear to influence the outcome. |
| Massin et al. (2016) [40] | 108 | Retrospective | Not reported | Not reported | Not reported | 2 | RR = 24% FO: IKS 88.6 ± 9.4 |
One-stage procedures are preferable in women, because they offer greater comfort without increasing the risk of recurrence. Routine one-stage procedures may be a reasonable option in the treatment of infected TKR |
| Li et al. (2017) [37] | 22 | Retrospective | Vnacomycin | 4-6 weeks | Not reported | 5 | RR = 9.1% FO: Not reported |
No significant difference between single–stage and two–stage revision in terms of satisfaction rates, and overall infection control rates. |
| Castellani et al. (2017) [36] | 14 | Retrospective | Not reported | Not reported | Not reported | 1 | RR = 7.2% FO: Not reported |
Superiority of one- versus two-stage revision and the value of antibiotic-free periods prior to definitive revision remain unclear. Large prospective studies or randomized controlled trials are needed |
RR: reinfection rate, FO: functional outcome, HSS: Hospital for Special Surgery knee score, IKS: International Knee Society Score, KSS: Knee Society Score, OKS: Oxford Knee Score, WOMAC: Western Ontario and McMaster Universities Osteoarthritis Index, TKR : total knee replacement, TKA : total knee arthroplasty, DAIR : debridement, antibiotics and implant retention, MRSA Methicillin-resistant Staphylococcus aureus, MRSE Methicillin-resistant Staphylococcus epidermidis .
Table 7.
Summary of Studies on Antibiotic Treatment Duration for Prosthetic Joint Infections managed by implant removal.
Table 7.
Summary of Studies on Antibiotic Treatment Duration for Prosthetic Joint Infections managed by implant removal.
| Author year Reference | Study design | Patients/ Prothesis site | Bacteria (major strains isolated) | Systemic antibiotics |
Systemic antibiotics duration (days) |
Local antibiotics | Mean follow up (Months) |
Outcome Additional Intra operative positive Persistence/Relapse debridement cultures at reimplantation |
|---|---|---|---|---|---|---|---|---|
|
Taggart et al., 2003 [64] |
Prospective observational, single-center, non-comparative |
33/Hip & Knee | 93% Gram-positives 71% staphylococci |
Not reported | 5 | Vancomycin | 67 | 0% 9% 3% |
|
Hoad-Reddick et al., 2005 [56] |
Prospective observational, single-center, non-comparative |
52/knee |
63% staphylococci |
None Cefuroxime as prophylaxis |
1 |
Various | 56 | 12% 16% 9% |
|
Hart & Jones, 2006 [65] |
Prospective observational, single-center, non-comparative |
48/knee | 96% Gram-positives 76% staphylococci |
Vancomycin | 14 | Vancomycin+ gentamicin | 49 | 13% 23% 13% |
|
Stockley et al., 2008 [57] |
Prospective observational, single-center, non-comparative |
114/hip |
61% staphylococci |
NoneCephalosporin as prophylaxis | 1 | Various | 74 | 4% 16% 12% |
|
Whittaker et al., 2009 [66] |
Prospective observational, single-center, non-comparative |
44/Hip | All Gram-positives 72% staphylococci |
Vancomycin | 14 | Vancomycin+ gentamicin | 49 | 7% 2% 7% |
|
McKenna et al., 2009 [58] |
Retrospective, observational, single-center, non-comparative |
31/Hip | All Gram-positives 77% staphylococci |
Vancomycin | 5 | Various | 35 | 0% 0% 0% |
|
Mittal et al., 2007 [67] |
Retrospective, observational, multicenter, comparative |
37/knee | Methicillin-resistant staphylococci |
Not reported | ≥6 weeks IV vs. <6 weeks IV |
Various | 51 | - 0% Short: 2/15 (13%) Long: 2/22: (9%) (p = 0.07) |
|
Hsieh et al., 2009 [68] |
Retrospective, observational, single-center, comparative |
99/knee | 67% Gram-positives 53% staphylococci |
A first-generation cephalosporin and gentamicin | 4–6 weeks vs. 7 days |
Various | 43 | Long 2/46 (4%) - Long: 2/46 (4%) Short 1/53 (2%) Short: 3/53 (6%) |
|
El Helou et al., 2011 [69] |
Retrospective, observational, single-center, comparative, propensity score-adjusted |
208/hip and knee | Mainly Gram-positives. 62% staphylococci |
Not reported |
4 weeks +/-7 d vs. 6 weeks +/-7 d |
Vancomycin +/- Tobramycin |
60 | - Short: 6.1% Short: 16% Long: 8.7% Long: 27% |
|
Benkabouche et al., 2019 [60] |
Single-center, open, randomized clinical trial |
39 /Hip & Knee | Various | Vancomycin IV Fluoroquinolones Oral |
6 weeks (39-45 days) Vs 4 weeks (27–30 days) |
Only 2 cases (5%); tobramycin |
26 | No significant difference was observed in the PJI group |
|
Ma et al, 2020 [70] |
Retrospective, observational, single-center, comparative |
64/knee |
69% staphylococci |
Not reported | 4–6 weeks vs.≤7 days | Vancomycin (} aminoglycosides) |
75 | Need for salvage antimicrobials or surgery Long: 11/43 (26%); Short: 3/21 (14%) |
|
Bernard et al., 2021 [32] |
Multicenter, open, randomized clinical trial |
81/Hip & knee | 40% S. aureus | Rifampicin Fluoroquinolones |
6 weeks vs. 12 weeks |
Not reported | ≥24 | Failure: 6 w: 6/40 (15%); 12 w: 2/41 (5%) (p > 0.05) Difference: 10.1% (95%CI −0.9–22.2), longer antibiotic duration is recommended |
RR: reinfection rate, FO: functional outcome, HSS: Hospital for Special Surgery knee score, IKS: International Knee Society Score, KSS: Knee Society Score, OKS: Oxford Knee Score, WOMAC: Western Ontario and McMaster Universities Osteoarthritis Index, TKR : total knee replacement, TKA : total knee arthroplasty, DAIR : debridement, antibiotics and implant retention, MRSA Methicillin-resistant Staphylococcus aureus, MRSE Methicillin-resistant Staphylococcus epidermidis 6.4.2. Arthrodesis.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



