
Submitted:
21 May 2025
Posted:
22 May 2025
You are already at the latest version
Abstract
Background
Immunisation is an effective intervention for controlling more than 20 life-threatening infectious diseases, reducing both morbidity and mortality. One major vaccination-related achievement was the worldwide eradication of smallpox; the world was declared free of smallpox by the World Health Assembly on 8 May 1980. A second major vaccination-related success has been a reduction in wild poliovirus cases by 99.9% since 1988, from more than 350,000 incident cases that year to 30 in 2022.
Objectives
To assess the effects of interventions aimed at increasing vaccination uptake among adults.
Search methods
A search was conducted in CENTRAL, Embase Ovid, Medline Ovid, PubMed, Web of Science, and Global Index Medicus databases for primary studies, in August 2021, and updated in November 2024.
Selection criteria
Randomised trials, irrespective of their publication status and language of publication, were eligible for inclusion in this review.
Data collection and analysis
Two review authors independently screened records, assessed full-text articles to identify potentially eligible studies, extracted data, and evaluated risk of bias, resolving differences by consensus. For each included study, we calculated risk ratios (RR) with 95% confidence intervals (CI). We pooled study results using random-effects meta-analyses and used GRADE to assess the certainty of the evidence.
Main results
Thirty-five randomised controlled trials met the inclusion criteria and were included in the review, the majority of which were conducted in the United States of America (U.S.A.). The interventions were aimed at improving vaccination uptake among adults aged 18 years and above who were eligible for vaccination. Most of the studies assessed uptake of influenza vaccine (18 studies), with the rest investigating a variety of vaccines, including hepatitis A virus, coronavirus disease of 2019 (COVID-19), hepatitis B virus, pneumococcal, tetanus, diphtheria, and pertussis (Tdap), herpes zoster (the acronym would be either: herpes zoster vaccine (HZV) or recombinant zoster vaccine (RZV) or live shingles zoster vaccine (ZVL) ), and human papillomavirus (HPV) vaccines (18 studies). Our results indicate that letter reminders were slightly effective in increasing influenza vaccination uptake compared to the control (RR: 1.75, 95% CI: 0.97, 1.16; 6 studies; 161,495 participants; low-certainty evidence). There were increased levels of influenza vaccination uptake among participants who received education interventions compared to those who were in the control group (RR: 1.88, 95% CI: 0.61, 5.76; 3 studies, 1,318 participants; low-certainty evidence). Tracking and outreach interventions also increased the influenza vaccination uptake (RR:1.87, 95% CI: 0.78, 4.46; 2 studies, 33,752 participants; low-certainty evidence).
Conclusion
Letter reminders and education directed at recipients are effective in increasing vaccination uptake compared to the controls.
Keywords:
Adult Vaccination
; Vaccination Uptake
; Effective Interventions
1. Introduction
Worldwide, vaccine preventable diseases (VPDs) cause millions of deaths each year [1]. Vaccination is the act of introducing a vaccine into the body to produce immunity to a specific disease, and immunisation is the process by which a person becomes protected against a disease through vaccination [2]. Immunisation is often used interchangeably with vaccination or inoculation. Immunisation is a evidence-based tool for controlling more than 20 life-threatening infectious diseases, reducing both morbidity and mortality [3]. One major vaccination-related achievement was the worldwide eradication of smallpox; the world was declared free of smallpox by the World Health Assembly on 8 May 1980 [1]. A second major vaccination-related success has been a reduction in wild poliovirus cases by 99.9% since 1988, from more than 350,000 incident cases that year to 175 in 2019 [4], [5].
Of the three serotypes of wild poliovirus, type 2 was certified as eradicated in 2015 and type 3 was certified as eradicated in 2018. Five of six World Health Organization (WHO) regions have been certified as being free of wild poliovirus; the exception is the Eastern Mediterranean Region, with polio being endemic in Afghanistan and Pakistan [6]. The WHO estimates that vaccination prevents between four million and five million deaths annually [3]. Additionally, the Vaccine Impact Modelling Consortium, representing 16 independent research groups, conducted modelling to estimate the effect of vaccination programmes on disability-adjusted life years and deaths for 10 pathogens among 98 low- and middle-income countries [7]. Between 2000 and 2030, vaccinations are estimated to avert 69 million deaths among these countries [7]. In the United States (U.S.), an estimated 7.5 million influenza cases, 105,000 hospitalisations, 3.69 million medical visits, and 6,300 deaths were averted because of influenza vaccination during the 2019 to 2020 influenza season [8].
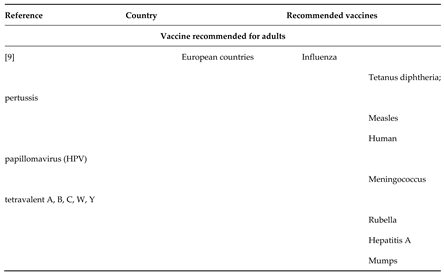
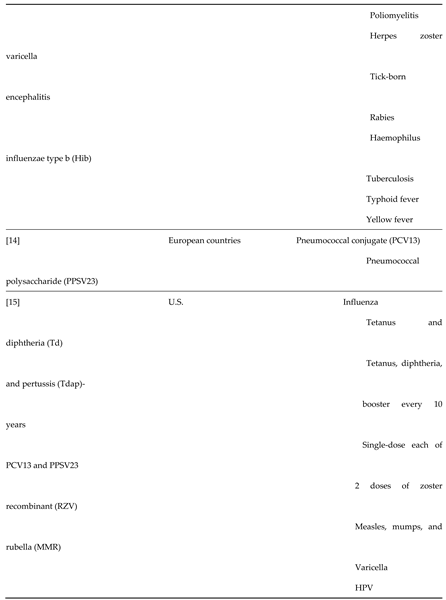
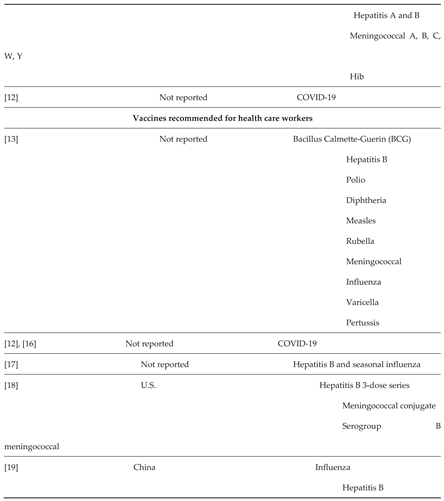
1.1. Recommended Vaccines
Vaccines received by adults vary widely by country with respect to the number and types of vaccination, target populations, and whether they are recommended or required [8]–[10]. The requirements also vary by age, comorbidity, vaccination history, and other factors [10], [11]. We have summarised the recommended vaccines for adults and health care workers (HCW) Table 1). In many countries or circumstances, health care workers (HCWs) are the target populations for receiving vaccinations because they may have an increased risk of being exposed to life-threatening infections if involved in direct patient care [12], [13]. There is paucity of data on adult vaccination recommendations in low- and middle-income countries.
Table 1.
1.2. Vaccination Uptake Among Adults
Although vaccination provides tremendous health benefits to populations, vaccination uptake among adults is suboptimal, globally, leaving many adults without protection against vaccine preventable diseases [11], [20]. For example, influenza vaccination uptake among adults is generally low and varies by county. Among U.S. adults, 46.1% received influenza vaccination during the 2017 to 2018 influenza season [11]. This is similar to the median influenza vaccination coverage of 47.1% among adults aged 55 years and older in the European Union (EU) and European Economic Area (EEA) Member States during 2016 to 2017 [20]. However, influenza vaccination uptake ranged from 2% to 72.8% among the 22 reporting EU and EEA member states; all falling short of the 75% EU target [20].
In one medical claims-based study of more than 500,000 members of a private health insurance plan in South Africa, only 5% of the population received the influenza vaccine in 2015 [21]. In one cross-sectional study conducted in Beijing, China during May and June 2015, self-reported influenza vaccination levels were 16.0% among respondents aged less than 60 years and 48.7% among those aged 60 years and older [22]. The uptake of other types of adult vaccinations is also generally low. For example, results from the 2018 U.S. National Health Interview Survey demonstrated that adult vaccination uptake was low in all age groups for a composite measure, which included influenza, pneumococcal, herpes zoster, and tetanus and diphtheria (Td) or tetanus, diphtheria, and pertussis (Tdap) vaccines [11]. During 2018, an estimated 13.5% of US adults, aged 19 years and older, had received all age-appropriate vaccines included in the composite measure [11].
During 2018, pneumococcal vaccination uptake was 23.3% for at least one dose and 7.5% for at least two doses among U.S. adults at increased risk. Similarly, a telephone interview conducted with more than 4,000 adults aged 65 years and older, among nine European countries revealed that only 18% of these respondents had received a pneumonia vaccination [23]. An estimated 24.1% of U.S. adults aged 50 years and older had received the herpes zoster vaccine; and 58.9% to 64.5% of adults had received a tetanus toxoid vaccination during the previous 10 years, with slight variations between age groups [11]. As of January 2021, only 22% of U.S. young adults had completed the human papillomavirus (HPV) vaccination series [24]. Uptake among women was similar by age group (i.e. 42.0% for women aged 19 to 21 years and 41.4% for women aged 22 to 26 years) [25].
For hepatitis B vaccination, uptake of two or three doses among adults was 24.6% for adults aged 19 years or older, 32.0% among adults aged 19 to 49 years, and 16.5% among adults aged 50 years or older [25]. Wide disparities in COVID-19 vaccination uptake exist between countries [26]. By 16 July 2021, 3.6 billion doses of COVID-19 vaccines were administered worldwide, with 30 million doses administered each day. However, there was wide variation in access to and uptake between world regions; with more than 25% of the world population having received at least one dose of a COVID-19 vaccine, but only 1% of people in low-income countries had received at least one dose [27]. There is also wide variation among high-income countries, with more than 60% of adults in the U.S., Canada, UK, Israel, and other Western countries having received at least one dose as of 16 July 2021. This is different from vaccination coverage in low-income countries, i.e., 30% in Morocco, 26% in Colombia, 23% in India, 22% in Russia, 7% in South Africa, and less than 1% in most countries in sub-Saharan Africa [27]. The consequence of suboptimal uptake of vaccination is a high burden of morbidity and mortality from vaccine preventable diseases.
1.3. Description of the Intervention
Interventions suggested to improve vaccination uptake include those that target recipients of vaccination services, providers of vaccination services, and health systems [28]–[33]. In addition, interventions may focus on structural, broader systems or policy changes, or both [34], [35]. Patient- or person-focused interventions include: educating people to prompt providers to check their vaccination cards, reminding recipients to receive vaccines; health education programmes, communication strategies such as presumptive communication approaches, use of science and anecdotes, motivational interviewing, and application of the Health Belief Model (an example of one theory that is used to structure messages and interventions aimed at increasing the uptake of vaccinations); direct advertising and promotional campaigns from pharmaceutical companies, health insurance companies, and health systems; and incentives [29], [31], [36].
Provider-focused interventions include training, supporting supervision or educational outreach visits, provider reminders or clinical decision support tools, audit and feedback, academic detailing, provider incentives, standing vaccination orders, and use of a vaccination champion in a clinical practice [28], [36]–[38]. Systems-level interventions include changing practices at health care clinics, adopting population health strategies, use of electronic health records, systematic screening of vaccination histories of people admitted to hospitals, bringing vaccination services closer to consultation rooms, providing vaccination in non-traditional sites, such as inpatient units, emergency departments, businesses, other community-based settings, and during home visits, and expanding clinic hours to accommodate patient schedules [28], [31], [36]. Broader systems or policy-level interventions include vaccination mandates for employment, school, or college matriculation, or a combination of these; use of vaccination registries; providing free vaccinations or reducing out-of-pocket costs for patients; and health insurance coverage of vaccinations [34].
1.4. How the Intervention Might Work
The interventions might work through addressing barriers to access and increasing demand for vaccinations [39]–[41]. The factors that have been reported to be associated with low vaccination uptake among adults may be classified at the patient-, provider-, health system-, or policy-level [34], [42]. Patient- or person-level barriers include lack of access, lack of health insurance coverage, affordability, concerns about safety and adverse effects, lack of awareness or knowledge, health literacy, belief that healthy people do not need vaccinations, not trusting pharmaceutical companies, forgetting vaccination appointments, not getting a clear recommendation from the health care provider, not having routine visits with primary health care providers, and fear of needles [34], [42], [43].
Provider-level barriers to vaccination include forgetting to offer them, costs to the practice, concerns about reimbursement and costs to patients, storage challenges, knowledge, attitudes, beliefs about safety and efficacy, time constraints, lack of confidence or discomfort with discussing vaccines, not being up to date with own vaccinations, and lack of institutional trust [44], [45]. Health system barriers to vaccination include insufficient infrastructure to deliver adult vaccinations, such as insufficient funding, challenges with supply chain or distribution processes, and lack of population management systems, lack of provider reminder systems, clinical decision support tools, and patient reminder or recall systems [29], [34], [43], [46]. Policy-related barriers to vaccination delivery include lack of vaccination mandates as well as policies that limit vaccinations to specific adult populations in some countries [42]. The recipient-, provider-, health system-, and policy-level interventions aim to increase uptake of adult vaccinations by addressing respective barriers to vaccinations.
1.5. Why It Is Important to Do This Review
Adult vaccination is important because adults are a vulnerable population to infectious diseases due to their compromised immune system as they grow older. Older adults are at increased risk of poor outcomes from infectious diseases due to their ageing immune systems [47]. Additionally, the changes in chemokine localisation and the structure of lymph nodes affect the function of the immune system in older people [48], [49]. There are also new and emerging infections, such as Ebola and COVID-19, for which both younger and older adults are primary vaccination targets. That is why the WHO, U.S. Centers for Disease Control and Prevention, European Centre for Disease Prevention and Control, and other agencies recommend adults to receive vaccinations.
While adults should receive vaccinations, the uptake of vaccines among this group remains low or falls short of achieving vaccination targets. Low vaccination uptake among adults may be attributed to patient-, provider-, health system-, or policy-level barriers [34]. Successful strategies to improve rates of uptake of vaccination among adults will result in reductions in morbidity, mortality, and health care costs [50]. Therefore, more widespread interventions are needed to address existing barriers and enhance vaccination uptake among adults Table 1: [28]–[32], [51], [52]
1.6. Objectives
To assess the effects of interventions aimed at increasing vaccination uptake among adults.
2. Methods
2.1. Criteria for Considering Studies for This Review
2.1.1. Types of Studies
We included randomised controlled trials (RCTs), irrespective of their publication status and language of publication.
2.1.2. Types of Participants
Eligible participants included adults, as defined by study authors, eligible for vaccines approved for use in the country of the study. The eligible adults included carers of older adults and any type of HCWs targeted for vaccinations. We included studies where a subset of participants were adults and when outcomes were specifically reported for the applicable strata.
2.1.3. Types of Interventions
We assessed interventions aimed at improving uptake of routine vaccines, including vaccines for special conditions or special indications, among adults. Eligible interventions included those that targeted recipients of vaccination, providers of vaccination services, and health systems, including policy changes.
2.2. Recipient-Oriented Interventions.
- Interventions to inform or educate adults about vaccination.
- Advertising and promotional campaigns for adult vaccination.
- Recipient reminders [29].
- Recipient incentives.
- Communication strategies: presumptive communication approach; gain-framed versus loss-framed communication; use of science and anecdotes; motivational interviewing; health coaching; clinicians providing a strong recommendation to the adult; and other communication tactics to facilitate decision-making.
- Tailored interventions (e.g. the Medicare Annual Wellness Visit in the U.S., which aims to establish a five- to 10-year personalised prevention plan, including needed vaccinations).
2.3. Interventions Targeting Providers of Adult Vaccination Service
- Education or training of vaccinators.
- Audit and feedback for vaccinators or clinical practices.
- Provider reminders.
- Clinical decision support tools.
- Academic detailing.
- Supportive supervision of, or educational outreach visits to, vaccinators.
- Pay-for-performance.
- Provider incentives.
- Standing vaccination orders.
- Use of vaccination champions.
- Quality improvement processes.
2.4. Interventions Directed at the Broader Health System
- Reliable cold chain system.
- Vaccine stock management.
- Expanded services (e.g. extended hours for vaccination services).
- Increased vaccination budget.
- Integration of vaccinations with other services.
- Provision of vaccinations in non-traditional settings: inpatient units, emergency departments,
- workplaces, home visits, community, churches.
- Use of vaccination registries and other electronic health records.
- Public information programmes.
- Provision of transport for vaccination.
- Vaccine mandates (e.g. for employment, school, university matriculation).
- Provision of free vaccinations or reductions in out-of-pocket costs.
- Offer health insurance coverage of vaccinations.
2.5. Multi-Component Interventions
- 1.
- Those that included more than one type of tactic for increasing coverage.
2.6. Exclusion
We excluded trials assessing interventions for improving uptake of travel vaccines as these vaccines are often mandatory for travellers. We also excluded studies where a subset of participants met the study criteria, if outcomes were not reported for the applicable strata.
2.7. Comparison
We included trials comparing these interventions with no intervention or usual care.
2.8. Types of Outcome Measures
This study included primary and secondary outcomes listed below.
2.8.1. Primary Outcomes
Vaccination uptake, defined as the proportion of adults who have received the recommended dose(s) of the vaccine studied.
2.8.2. Secondary Outcomes
Proportion of people who are 'up-to-date' with needed vaccinations, as defined by the authors.
Other vaccination uptake indicators, as defined by the authors.
2.9. Search methods for Identification of Studies
2.9.1. Electronic Searches
The search strategies were designed by an Information Specialist in consultation with the review authors. We searched the Cochrane Database of Systematic Reviews (CDSR) and Epistemonikos (www.epistemonikos.org/) for related systematic reviews.
We searched the following databases for primary studies, from inception to the date of search. Cochrane Central Register of Controlled Trials (CENTRAL; latest issue), in the Cochrane Library
- Medline Ovid
- Embase Ovid
- PubMed
- Web of Science
- Conference Proceedings Citation Index – Science
- Global Index Medicus.
We used keywords and controlled vocabulary terms in the search strategies and applied no limits on language. We used a modified version of the Cochrane Highly Sensitive Search Strategy to identify randomised trials [53]. See published protocol for the MEDLINE search strategy, which we adapted for other databases [54].
2.9.2. Searching Other Resources
Trial registries
We searched the following trial registries.
- WHO ICTRP (International Clinical Trials Registry Platform; www.who.int/ictrp).
- US National Institutes of Health Ongoing Trials Register ClinicalTrials.gov (www.clinicaltrials.gov).
2.10. Grey Literature
We conducted a search of two grey literature databases to identify studies not indexed in the databases listed above.
- OpenGrey (www.opengrey.eu).
- Grey Literature Report (New York Academy of Medicine; www.greylit.org).
2.11. Other Resources
We also reviewed reference lists of all included studies and relevant systematic reviews for additional potentially eligible primary studies. We contacted authors of included studies to clarify reported published information and to seek unpublished results. We contacted researchers with expertise in adult vaccination. We also conducted cited reference searches for all included studies in Science Citation Index (Web of Science, Clarivate). We provided appendices for all strategies used.
2.12. Data Collection and Analysis
2.12.1. Selection of Studies
We downloaded all titles and abstracts retrieved by electronic searching to EndNote and remove duplicates. Two review authors (AJ and TM or LM and MS) independently screened titles and abstracts for inclusion. We retrieved the full-text study reports or publications; and two review authors (AJ and TM or LM and MS) independently screened the full-text, identified studies for inclusion, and identified and recorded reasons for exclusion of the ineligible studies. We resolved any disagreements through discussion and consulted other review authors (CSW, DN and JJV) when consensus was not reached. We listed studies that initially appeared to meet the inclusion criteria but added the studies to the 'Characteristics of excluded studies' table if criteria were not met (Table S1). We recorded the selection process in sufficient detail to complete a PRISMA flow diagram [55].
2.12.2. Data Extraction and Management
We used the Effective Practice and Organisation of Care (EPOC) standard data collection form and adapted it for study characteristics and outcome data [56]. We piloted the form on at least one study in the review. Two review authors (AJ and TM or LM and MS) independently extracted the following study characteristics from the included studies and entered the data into Review Manager Web (Review Manager Web 2019).
- Methods: study design, number of study centres and location, study setting, withdrawals, date of study, and follow-up.
- Participants: number, mean age, age range, sex, inclusion criteria, exclusion criteria, and other relevant characteristics.
- Interventions: intervention components, and comparisons.
- Outcomes: main and other outcomes specified and collected, and time points reported.
- Notes: funding for trial, notable conflicts of interest of trial authors, and ethical approval.
Two review authors (AJ and TM or LM and MS) independently extracted outcome data from included studies. We resolved disagreements by consensus. If any of them persisted we would have involved other review authors (CSW, DN and JJV) to arbitrate.
2.12.3. Assessment of Risk of Bias in Included Studies
Two review authors (AJ and TM or LM and MS) independently assessed risk of bias for the included studies using the criteria outlined in the Cochrane Handbook for Systematic Reviews of Interventions Section 8.5 [57], and the guidance from the EPOC group [58]. We resolved any disagreements by discussion or by involving other review authors (CSW, DN and JJV). We assessed the risk of bias according to the following domains.
- Random sequence generation.
- Allocation concealment.
- Blinding of participants and personnel.
- Blinding of outcome assessment.
- Incomplete outcome data.
- Selective outcome reporting.
- Baseline outcomes measurement.
- Baseline characteristics.
- Other bias
We judged each potential source of bias as high, low, or unclear. We briefly provided reasons from the studies for our judgement in the risk of bias. We summarised the risk of bias judgements across different studies for each of the domains listed. An overall risk of bias assessment (high, low, or unclear) was assigned to each of the included studies using the approach suggested in Chapter 8 of the Cochrane Handbook for Systematic Reviews of Interventions [57]. We considered studies with low risk of bias for all key domains or where it seems unlikely for bias to have seriously altered the results, to have a low risk of bias. We considered studies where risk of bias in at least one domain was unclear or judged to have some risk of bias that could plausibly raise doubts about the conclusions, to have an unclear risk of bias. We considered studies with a high risk of bias in at least one domain or judged to have serious bias that decreases the certainty of the conclusions, to have a high risk of bias.
2.12.4. Measures of Treatment Effect
We estimated the effect of the intervention using the risk ratio as all our outcomes will be dichotomous data, together with the appropriate associated 95% confidence interval [57].
2.12.5. Unit of Analysis Issues
While in our published protocol we reported that we would include cluster RCTs, we excluded them in this review because of the challenges experienced during adjusting for clustering and maintaining methodological consistency. We only included individual RCTs in our meta-analysis, to preserve internal validity and comparability across included studies. Due to this, we did not conduct unit of analysis in our review.
2.12.6. Dealing with Missing Data
We did not contact investigators as we did not observe any missing outcome data from the included studies.
2.12.7. Assessment of Heterogeneity
We found sufficient number of studies, where we judged participants, interventions, comparisons, and outcomes sufficiently similar, and therefore conducted meta-analysis [59] . We used the I² statistic to measure heterogeneity among the trials in each analysis. We assessed low heterogeneity as an I2 statistic between 0% and 50%, moderate heterogeneity as I2 from 51% to 75%, and high heterogeneity as I2 above 75% [57].
2.12.8. Assessment of Reporting Biases
We did not examine possible publication biases because studies in our subgroup analysis were less than 10.
2.12.9. Data Synthesis
We undertook meta-analyses only if the interventions, participants, and vaccines were similar enough for pooling to make sense [59]. A common way that trialists indicate when they have skewed data is by reporting medians and interquartile ranges, however, we did not encounter this. Where multiple trial arms are reported in a single trial, we included only the relevant arms.
2.12.10. Summary of Findings and GRADE
Two review authors (AJ and LM or AJ and AH) independently assessed the certainty of the evidence (high, moderate, low, and very low) using the five GRADE considerations, risk of bias, consistency of effect, imprecision, indirectness, and publication bias [60]. We used methods and recommendations described in Section 8.5 and Chapter 12 of the Cochrane Handbook for Systematic Reviews of interventions [57], and the EPOC worksheets [61], and we used GRADEpro software (GRADEpro GDT). We resolved disagreements on certainty ratings by discussion and provided justification for decisions to down-grade or upgrade the ratings using footnotes in the table and made comments to aid readers' understanding of the review where necessary. We used plain language statements to report these findings in the review [61]. We summarised the findings in summary of findings tables for the main intervention comparisons and included uptake of adult vaccines. We also included our primary (i.e. vaccination uptake) comparing them with no intervention or usual care. We did not address any equity issues such as cost, and socioeconomic and geographic status by evaluating the reported results from the included studies to inform future designs of interventions aimed at improving adult vaccination uptake.
2.12.11. Subgroup Analysis and Investigation of Heterogeneity
We identified substantial heterogeneity and explored it by prespecified subgroup analysis. We defined subgroups based on the type of vaccines, interventions, and controls. Concerning studies [62], [63] with multiple intervention groups, we included independent comparisons and divided controls among the different comparison groups, to avoid the double counting of participants [64].
2.12.12. Sensitivity Analysis
We did not perform sensitivity analyses defined a priori to assess the robustness of our conclusions and explore its impact on effect sizes. This would have involved the following.
- Restricting the analysis to published studies.
- Restricting the analysis to studies with a low risk of bias.
- Imputing missing data.
2.12.13. Stakeholder Consultation and Involvement
We did not involve patients and stakeholders in the design of this review. However, the findings of the review will be shared with stakeholders, including policy makers, researchers, and other consumers.
2.12.14. Summary of Findings and Assessment of the Certainty of the Evidence
We used the summary of findings tables to present the key information from the review, providing the certainty of evidence, the effect of the interventions, and a summary of the available evidence for all important outcomes. Two review authors (AJ and LM or AJ and AH) independently assessed the certainty of the evidence (high, moderate, low, and very low) using the five GRADE considerations (risk of bias, consistency of effect, imprecision, indirectness, and publication bias) [60]. We used methods and recommendations described in Section 8.5 and Chapter 12 of the Cochrane Handbook for Systematic Reviews of interventions (Higgins 2019) [57], and the EPOC worksheets [61], and we used GRADEpro software (GRADEpro GDT). We resolved disagreements on certainty ratings by discussion and provided justification for decisions to downgrade or upgrade the ratings using footnotes in the summary of findings tables and make comments to aid readers' understanding of the review where necessary.
We used plain language statements to report these findings in the review [61]. The summary of findings tables includes our primary outcome (i.e. vaccination uptake) comparing them with no intervention or usual care.
2.13. Statistical Analysis
All statistical analyses were conducted using R (version 12.1). We used the meta package to perform meta-analyses of binary outcomes, calculating risk ratios (RRs) and 95% confidence intervals (CIs) using the Mantel–Haenszel method for pooling and the DerSimonian–Laird estimator to account for random effects. The dataset was first stratified by predefined analysis groups, and each subgroup was analysed separately. For each analysis, we used the metabin() function to synthesize data on intervention and control events and total sample sizes, grouped by study and further stratified by subgroup where applicable. Forest plots were generated for each analysis using the meta and grid packages, with customized formatting for clarity and consistent visual presentation.
3. Results
3.1. Description of Studies
3.1.1. Results of the Search
Our literature search yielded 12,754 records from electronic databases and other sources. Twenty duplicates were identified and excluded from the records. Therefore, we screened 12,734 studies, of which 12,082 were ineligible for inclusion in our review. The full texts of the remaining 652 potentially eligible studies were assessed, and 617 were excluded, with reasons for exclusion provided in the Characteristics of excluded studies table (Table S1). Thirty-five studies met the inclusion criteria and were included in the review. The search process and selection of studies is presented in Figure S1.
3.1.2. Included Studies
Study design and setting
The 35 included studies (Table S2) were randomised controlled trials with individuals as the unit of randomisation. A majority of the included studies were conducted in the U.S. [62], [63], [73]–[82], [65], [83]–[86], [66]–[72] Others were carried out in Australia [87]–[90] Belgium [91], Switzerland [92], Hong Kong [93], Denmark [94], England and Hawaii [95], [96].
Participants
All the included studies investigated the effects of interventions in vaccination uptake among adults aged 18 years and above who were eligible for vaccination. Most of the included studies further described the type of adults investigated as those who were at high risk of influenza complications [65], underwent a health check between the end of 2016 influenza epidemic and beginning of the next influenza vaccination campaign [92], active patients of participating primary care centers [67], were deficient in either the influenza, Tdap, and or pneumococcal vaccines [68], with chronic disease, had vaccine indications, and had not been previously vaccinated [69], had never had Hepatitis B testing [70], patients admitted to the medical service during the study period [72], either hepatitis C virus (HCV) negative, of unknown HCV status, or, if HCV positive, with no prior medical care or diagnostic evaluation for HCV [74], did not have herpes zoster vaccine [78], who were voluntarily initiating the first HPV vaccine dose [80], front-line health care workers [63], [85], [94], [95], had a first trimester obstetric visit during the study period (Stockwell 2014) [82], individuals who were missing pneumococcal and herpes zoster (HZV) vaccinations, young adults 18–64 years without diabetes, older adults ≥ 65 years without diabetes, adults ≥18 years with diabetes [62].
Interventions and comparisons
A summary and detailed description of the interventions and comparisons used in the included studies are presented in the Characteristics of included studies table. The interventions are stipulated as recipient and provider-oriented interventions.
Recipient-oriented interventions
Six studies investigated recipient-oriented interventions comprised of reminder interventions, namely, mailed letters [62], [65], [81], [85], [94], [96], mailed postcards [65], [87], [92] phone call reminders [68], [70], [83] message reminders [66], [73], [79], [82] Eight studies assessed education strategies [65], [69], [97], [71], [74], [77], [78], [84], [90], [91], [93] tracking and portal outreach where HCWs tracked the medical records of patients using electronic databases [66], [67] and 2, assessed promotional campaigns which were done through conspicuous messaging using an app [73], [76], provider reminders [67], [95], letter [63]), raffle plus letter [63], ruffle [63] and financial incentives [88], [89] These were all compared to standard care.
Provider-oriented interventions
Provider-oriented interventions also consisted of 2 studies that evaluated letter reminders [67], [95], while 1 assessed education using a letter and incentive strategies using a raffle [63]. All were compared to standard care.
Outcomes
Majority of the included studies reported data on our primary outcome, i.e., vaccination uptake. In total, 18 studies evaluated the effects of various recipient and provider interventions on influenza vaccination uptake [62], [63], [85]–[87], [92]–[96], [65]–[68], [73], [76], [77], [82]. Some of the studies also investigated the effects of the interventions on uptake of other vaccines, i.e., COVID-19, hepatitis A virus (HAV), hepatitis B virus (HBV), pneumococcal, tetanus, Tdap, HZV, and HPV [65], [68], [84], [88]–[91], [96], [69], [70], [74], [77]–[79], [81], [83]. The pre-determined secondary outcomes, proportion of people who are 'up-to-date' with needed vaccinations, and other vaccination indicators, were not reported in the included studies.
Excluded studies
Our reasons for excluding some of the studies from this review are briefly specified in the Characteristics of Excluded Studies table (Table S1). The predominant reasons for exclusion were irrelevant study designs, e.g., cluster RCTs, reviews, or ongoing clinical. Other reasons were unrelated comparison groups where some of the studies compared two interventions without a control group. Some assessed the effects of interventions on outcomes that were not related to our review question [66]
Risk of bias in included studies
Allocation Random sequence generation had a low risk of bias in 19 studies [62], [67], [86]–[89], [92], [93], [95], [97], [68], [69], [73], [74], [77]–[79], [83], unclear risk in 12 studies [63], [65], [91], [96], [66], [72], [75], [76], [80]–[82], [85] and high risk in 4 studies [70], [71], [84], [94] Allocation concealment had a low risk of bias in 10 studies [62], [67], [77]–[79], [86], [88]–[90], [97], unclear risk in 19 studies [63], [65], [82], [83], [85], [87], [91]–[93], [95], [96], [66], [68], [73]–[76], [80], [81] and high risk in 5 studies [69]–[71], [84], [94]
Blinding
Regarding blinding of participants and personnel, there was low risk of bias in 10 studies [62], [67], [97], [68], [69], [75], [77], [79], [86], [88], [93], unclear risk in 19 studies [63], [65], [85], [87], [89]–[92], [94], [96], [73], [76], [78], [80]–[84] and high risk in 5 studies [66], [70], [71], [74], [95]. Blinding of outcome assessment had low risk of bias in 11 studies [62], [63], [91], [67]–[69], [79], [80], [86]–[88], unclear risk in 18 studies [65], [73], [85], [92]–[96], [75]–[78], [81]–[84] and high risk in 3 studies [66], [70], [74]
Incomplete outcome data
There was low risk of bias in 27 studies [66], [67], [79], [80], [82]–[89], [68], [90]–[92], [94], [95], [97], [69]–[71], [74]–[76], [78], unclear risk in 3 studies [62,63,93] and high risk in 5 studies [65], [73], [77,81,96] under incomplete outcome data.
Selective reporting
Twenty-three studies were rated as having low risk of bias [62,67,78]–[80], [82,83,85]–[68,89,90]–[97], [69]–[71], [73], [74,76,77], 4 studies with unclear risk of bias [63], [75,81,84], and 2 with high risk of bias [65], [66].
Other potential sources of bias
Twenty-three studies had no evidence of other sources of bias [62], [63], [81,82,85], [86,88,90], [92,93,95], [66,96,97], [68,71,98], [73,74,78]–[80] while 6 had unclear risk [69], [75]–[77], [84]) and 6, a high risk [65,67,70], [83,91,94]. Other types of potential risk of bias included recall bias by the participants based on the telephone survey, funder and conflicts of interest statement not mentioned, providers may have been less likely to check the patient’s vaccination record because they assumed that the absence of a reminder indicated prior vaccination, some of the patients in the control group knew of persons who had received an invitation for free influenza vaccination, and missing data.
3.2. Effects of Interventions
3.2.1. Recipient-Oriented Interventions
Overall Reminders Versus Control or Standard Care
Patients receiving reminder interventions were more likely to have received the influenza vaccine compared to those who were in the control group (RR: 1.28, 95% CI: 0.85, 1.93). Similarly, patients in the intervention group were more likely to have received other vaccinations, namely, HBV, pneumococcal, and herpes zoster vaccines (RR: 1.46, 95% CI: 1.05, 2.03) compared to those in the control.
Different Types of Reminders on Vaccination Uptake
We assessed the effects of different types of reminders on vaccination uptake; and our results indicate that letter reminders were quite effective in increasing influenza vaccination uptake compared to the control (RR: 1.75, 95% CI: 0.97, 3.17). There was a slight effect on influenza vaccination for participants who received postcard (RR: 1.11, 95% CI: 1.05, 1.16), phone call (RR: 1.19, 95% CI: 1.12, 1.26) and message reminders (RR: 1.00. 95% CI: 0.89, 1.14). For participants who received reminders, there was an increase in uptake of HBV, pneumococcal, and herpes zoster vaccines, in letter reminders (RR: 1.68, 95% CI: 1.04, 2.70) compared to phone call reminders (RR: 1.32, 95% CI: 0.88, 1.98), Figure S2.
Education Versus Control or Standard Care
There was an increase in influenza vaccination uptake among participants who received the education interventions compared to those who were in the control group (RR: 1.88, 95% CI: 0.61, 5.76). Compared to the control group, participants in the intervention were also more likely to receive other vaccinations, i.e., HAV, HBV, pneumococcal, Tdap, and herpes zoster vaccines (RR: 4.30, 95% CI: 2.96, 6.25), Figure S3.
Tracking and Outreach Versus Control or Standard Care
There was an increased likelihood of influenza vaccination uptake among participants in the tracking and outreach group relative to participants in the control group (RR: 1.87, 95% CI: 0.78, 4.46), Figure S2.
Promotional Campaigns vs Control or Standard Care
Promotional campaigns showed minimal differences in influenza vaccination uptake among participants in the promotional campaign group and standard care (RR: 1.07, 95% CI: 1.02, 1.13, Figure S2).
Financial Incentives
The associations between financial incentives and Hepatitis B vaccination completion (RR: 1.31, 95% CI: 1.07, 1.59) and COVID-19 (second dose) vaccination uptake (RR: 1.22, 95% CI: 0.85, 1.74) were relatively small, but important, Figure S4.
3.2.2. Provider-Oriented Interventions
Letter Reminders Versus Control or Standard Care
In the primary care centres, providers in the letter reminder group had an increased influenza vaccination uptake compared to those in the control group (RR: 1.76, 95% CI: 0.65, 4.75), Figure S2.
4. Discussion
4.1. Summary of Main Results
The current systematic review reports findings on the effectiveness of recipient-oriented interventions, i.e., reminders (letter, postcard, phone call and message reminders), education strategies, financial incentives, tracking and outreach, and promotional campaigns in increasing vaccination uptake and completion. This review also reports on the effectiveness of provider-oriented interventions (letter reminders and education strategies) in increasing vaccination uptake among eligible patients. We found that letter reminders directed at recipients of vaccination had the strongest association with increased influenza vaccination uptake, with smaller effect sizes among persons who received postcards and phone calls, and no difference among persons who received message reminders. Furthermore, letter reminders were associated with increased uptake of other vaccinations, namely, HBV, pneumococcal and HZV, compared to phone call reminders. Overall, patient reminder interventions were shown to be effective in increasing vaccination uptake among adults.
The patients who received educational interventions had increased uptake of influenza, HAV, HBV, pneumococcal, Tdap, and HZV vaccination. Similarly, tracking and outreach interventions were associated with increased vaccination uptake, while there were minimal differences in vaccination rates between study groups in the promotional campaign intervention studies. Financial incentives were shown to have relatively small associations with the completion of Hepatitis B and uptake of COVID-19 vaccinations. Interventions, namely, letter reminders and educational interventions, were also directed at providers of vaccination to increase uptake among recipients. This study found that patients of providers who received letter reminders had increased influenza vaccination uptake.
4.2. Overall Completeness and Applicability of Evidence
The present systematic review has included studies reporting on recipient and provider-oriented interventions aimed at increasing vaccination uptake of vaccines recommended by WHO and the CDC for adults aged 18 years and above, in all country settings. This review identified and included 35 studies, most of which were conducted in high-income countries (HICs). Although there are barriers and facilitators of vaccination uptake among eligible adults, interventions may help in increasing uptake. One such barrier is the issue of vaccine hesitancy, which is defined as a "delay in acceptance, or refusal, of vaccines despite the availability of vaccine services" [99]). The factors that influence vaccine hesitancy may range from contextual (lack of communication), individual and group (low perceived risk of infection), and vaccine or vaccination specific issues (no invitation from providers, supply chain issues) [100]). Despite these barriers, our review has shown that some of the interventions aimed at recipients and providers may effectively increase vaccination uptake among adults.
The most effective recipient-oriented interventions were educational strategies reported by [77], followed by mailed letter reminders reported by [62], [94], and [96], which increased uptake of influenza; and phone call reminders by [70] which were associated with increased uptake of HBV vaccination. The study by [77] enrolled pregnant women, of which 57% in the intervention group received the influenza vaccination, compared to 36% in the usual care group. A quarter of the enrolled participants were classified as vaccine hesitant, which could explain why some women did not get vaccinated. Previous research has reported that vaccine hesitancy, resulting in not obtaining vaccination, is commonly due to lack of information, fear of vaccine side effects, and the belief that infection provides a greater immunity than the vaccine itself [42]. It is therefore possible that the vaccine-hesitant women who did not receive the influenza vaccination were not fully informed about the influenza vaccination concerning its effectiveness and side effects. It is worthy to note that most of these studies were conducted in HICs, which could imply that the interventions may not be suitable for low-and-middle-income countries (LMICs).
“Certainty of the evidence” or “Quality of the evidence”? Sometimes Cochrane editors don’t want authors to use the word “quality” to describe evidence.
4.3. Quality of the Evidence
We included 35 RCTs in this review, of which 25 had a high risk of bias, 3 had an unclear risk of bias, and 7 had a low risk of bias. The domains that predominantly contributed to the high and unclear risk of bias are selective reporting, random sequence generation (i.e., lack of non-concealment of allocation), and lack of blinding of participants. Although the certainty of the evidence for the interventions was generally low (Table S4), the results of the present study suggest that the currently available evidence demonstrates that the interventions are likely to be effective.
4.4. Potential Biases in the Review Process
We minimised bias in the process of conducting and reporting this review, as per the standard Cochrane guidelines [57]. However, this review has potential limitations, one of which involves language bias where all the included studies were published in English meaning that we may have missed results were studies were published in other languages.
4.5. Agreements and Disagreements with Other Studies or Reviews
To the best of our knowledge, few published systematic reviews have been conducted to assess the effectiveness of interventions aimed at increasing vaccination uptake among adults. We have identified only three published systematic reviews. One, published in 2022, assessed the effectiveness of interventions to improve vaccination uptake among adults [101]. The second, focused on interventions aimed at increasing influenza vaccination among older adults, specifically those 60 years and older. Jacobson Vann 2018 studied the effects of patient reminder and recall interventions on vaccination rates, reporting results for adults separately from children and adolescents [29]. Like our study, Thomas 2018 and Jacobson Vann 2018 also evaluated the effectiveness of patient reminder or recall interventions, namely, letters, postcards, or phone calls, compared to a control in [29], [84]. Unlike the present study, which observed high risk of bias in majority of the included studies, the studies included in the systematic review were classified as having moderate risk of bias [84].
Jacobson Vann 2018 also reported results for text messages, autodialer, and patient reminders combined with provider reminders [29]. In the current review and those conducted by Thomas 2018 and Jacobson Vann 2018, these interventions were shown to be associated with increased influenza vaccination rates. Of the 75 included studies in Jacobson Vann 2018, 24 focused on adult influenza and eight focused on other adult vaccinations [29]. All risk ratios for studies included in the meta-analyses, except one, demonstrated positive effects, ranging from 0.95 (95% CI, 0.49 - 1.84) to 3.11 (95% CI, 1.16 - 8.36) (Jacobson Vann 2018) [29]. Thomas 2018 also assessed education interventions, that is, face-to-face three-minute presentations by medical students, and client-based education where nurses or pharmacists provided education to participants on influenza vaccination compared to no intervention. The study reported that having medical students and nurses deliver education sessions to participants was associated with increased influenza vaccination [84]. Similarly, our study reported that one-on-one verbal education sessions and educating participants by disseminating information through handing out pamphlets and social media were associated with increased influenza vaccination rates.
Both the present study and the one by Thomas 2018 also investigated patient outreach, i.e., home visits and tracking were associated with increased influenza vaccination rates [84]. Furthermore, these two studies also targeted providers using reminder and education interventions. Both studies reported that letter reminders targeted at providers slightly increased influenza vaccination. Moreover, these two reviews showed that education strategies, namely, educational reminders, academic detailing, and peer comparisons, were associated with increased influenza vaccination. While the review by Batteux 2022 showed that interventions, specifically monetary incentives, and communication strategies, such as through a delivery video, presentation, reminders, and messaging, were associated with increased COVID-19 vaccination [101]. Although our study did not include any study that investigated COVID-19 uptake, both the present study and the one by Thomas 2018 showed effectiveness of interventions in increasing vaccination uptake.
5. Authors' Conclusions
5.1. Implications for Practice
Our review reports that recipient-oriented interventions, namely, letter reminders, education sessions, and tracking and outreach, generally had the highest associations with increased vaccination uptake. Postcards and phone interventions had small positive associations with vaccination uptake; and message reminders were not associated with vaccination uptake. Letter reminders directed at providers also seem to have been associated with improved vaccination uptake among adults. Although some of these interventions may have slightly improved vaccination uptake, our study reported low certainty evidence for the interventions. This suggests that when implementing such interventions, implementation scientists, clinicians, public health agencies, and health systems need to monitor and evaluate how effective the interventions are.
5.2. Implications for Research
Based on the findings from this systematic review, evidence on the effects of interventions aimed at improving vaccination uptake among adults is insufficient as there are only 35 studies our review has reported on. All these studies are from high income countries (HICs), suggesting that the results may not be generalisable to low-and middle-income countries (LMICs).
To understand the effects of these interventions and apply them across different settings, research needs to be conducted in LMICs as well. Furthermore, future studies in both HICs and LMICs should also investigate and report on the cost effectiveness of implementing the interventions to increase vaccination uptake among adults. In addition, this review reported low-certainty evidence on the effects of recipient-oriented and provider-oriented interventions; thus, there is a need for future research to address this and expand on other interventions that can be used to improve vaccination uptake among adults.
Acknowledgments
We acknowledge the help of the EPOC with designing the search strategy. The authors would also like to acknowledge the South African Medical Research Council for affording us with the space and resources to conduct this review.
References
- S. Vanderslott, “How is the world doing in its fight against vaccine preventable diseases?,” ourworldindata.org/vaccine-preventable-diseases.
- M. J. Chachou, F. K. M. J. Chachou, F. K. Mukinda, V. Motaze, and C. S. Wiysonge, “Electronic and postal reminders for improving immunisation coverage in children: protocol for a systematic review and meta-analysis,” BMJ Open, vol. 5, no. 10, p. e008310. [CrossRef]
- “World Health Organization. Global immunization coverage 2019,” www.who.int/news-room/facts-in-pictures/detail/immunization.
- W. H. Organization, “Poliomyelitis Eradication Report by the Director‐General. 74th World Health Assembly. A74/19. 21 April 2021,” apps.who.int/gb/ebwha/pdf_files/WHA74/A74_19‐en.pdf.
- C. S. Wiysonge, “How ending polio in Africa has had positive spinoffs for public health. The Conversation. 3 November 2020,” theconversation.com/africa.
- K. Ramanathan et al., “Since January 2020 Elsevier has created a COVID‐19 resource centre with free information in English and Mandarin on the novel coronavirus COVID‐ research that is available on the COVID‐19 resource centre ‐ including this for unrestricted research re‐use a,” no. January, pp. 19–21, 2020.
- X. Li et al., “Estimating the health impact of vaccination against ten pathogens in 98 low‐income and middle‐income countries from 2000 to 2030: a modelling study,” Lancet, vol. 397, no. 10272, pp. 398–408.
- E. I. Illnesses and M. Visits, “Estimated Influenza‐Related Illnesses , Medical Visits , Hospitalizations , and Deaths in the United States — 2019 – 2020 Influenza Season – Estimates represent data as of October 2021,” no. October, pp. 1–6, 2021.
- D. C. Cassimos, E. Effraimidou, S. Medic, T. Konstantinidis, M. Theodoridou, and H. C. Maltezou, “Vaccination programs for adults in Europe, 2019,” Vaccines, vol. 8, no. 1, p. 34. [CrossRef]
- W. H. Organization, “Table 1: summary of WHO position papers – recommendations for routine immunization; updated September 2020,” www.who.int/immunization/policy/Immunization_routine_table1.pdf.
- P. J. Lu, M. C. Hung, A. Srivastav, L. A. Grohskopf, M. Kobayashi, and A. M. Harris, “Surveillance of vaccination coverage among adult populations – United States, 2018,” MMWR Morbidity and Mortality Weekly Report. Surveillance Summaries, vol. 70, no. 3, pp. 1–26, 2021.
- Christie, J. T. Brooks, L. A. Hicks, E. K. Sauber-Schatz, J. S. Yoder, and M. A. Honein, “Guidance for Implementing COVID-19 Prevention Strategies in the Context of Varying Community Transmission Levels and Vaccination Coverage,” MMWR. Morbidity and Mortality Weekly Report, vol. 70, no. 30, pp. 1044–1047, 2021. [CrossRef]
- W. H. Organization, “Table 4: summary of WHO position papers – immunization of health care workers; updated September 2020,” www.who.int/immunization/policy/Immunization_routine_table4.pdf. 20 September.
- C. Bonnave, D. Mertens, W. Peetermans, K. Cobbaert, B. Ghesquiere, and M. Deschodt, “Adult vaccination for pneumococcal disease: a comparison of the national guidelines in Europe,” European Journal of Clinical Microbiology & Infectious Diseases, vol. 38, no. 4, pp. 785–791. [CrossRef]
- U. S. C. for D. C. and Prevention, “Recommended adult immunization schedule for ages 19 years or older. United States, 2021; updated 11 February 2021,” www.cdc.gov/vaccines/schedules/downloads/adult/adult-combined-schedule.pdf.
- S. Cooper, H. van Rooyen, and C. S. Wiysonge, “COVID-19 vaccine hesitancy in South Africa: how can we maximize uptake of COVID-19 vaccines?,” Expert Review of Vaccines, vol. July, pp. 1–13. [CrossRef]
- H. C. Maltezou et al., “Vaccination of healthcare personnel in Europe: update to current policies,” Vaccine, vol. 37, no. 52, pp. 7576–7584, 2019. [CrossRef]
- et al; C. for D. C. and P. (CDC), “Immunization of Health-Care Workers: Recommendations of the Advisory Committee on Immunization Practices (ACIP) and the Hospital Infection Control Practices Advisory Committee (HICPAC).” 1997.
- L. Wang, X. L. Wang, X. Zhang, and G. Chen, “Vaccination of Chinese health-care workers calls for more attention,” Human Vaccines & Immunotherapeutics, vol. 16, no. 7, pp. 1498–1501. [CrossRef]
- E. C. for D. P. and Control, “Seasonal influenza vaccination and antiviral use in EU/EEA member states – overview of vaccine recommendations for 2017–2018 and vaccination coverage rates for 2015–2016 and 2016–2017 influenza seasons. Stockholm. ECDC. November 2018,” www.ecdc.europa.eu/sites/default/files/documents/seasonal-influenza-antiviral-use-2018.pdf.
- G. Solanki, M. G. Solanki, M. Cornell, and R. Lalloo, “Uptake and cost of influenza vaccines in a private health insured South African population.,” Southern African journal of infectious diseases, vol. 33, no. 5, 2018. [CrossRef]
- S. Wu, J. Su, P. Yang, H. Zhang, H. Li, and Y. Chu, “Factors associated with the uptake of seasonal influenza vaccination in older and younger adults: a large, population-based survey in Beijing, China,” BMJ Open, vol. 7, no. 9, p. e017459, 2018.
- PneuV 2017, “Adult pneumonia vaccination understanding in Europe: 65 years and over. 17,” www.ipsos.com/sites/default/files/ct/publication/documents/2017-10/ipsos-healthcare-pneu-vue-65s-and-over-report_0.pdf. 2017. 20 July.
- B. A. Glenn, N. J. B. A. Glenn, N. J. Nonzee, L. Tieu, B. Pedone, B. O. Cowgill, and R. Bastani, “Human papillomavirus (HPV) vaccination in the transition between adolescence and adulthood,” Vaccine, vol. 39, no. 25, pp. 3435–3444, 2021. [CrossRef]
- W. W. Williams et al., “Vaccination coverage among adults, excluding influenza vaccination – United States, 2013,” MMWR Morbidity and Mortality Weekly Report, vol. 64, no. 4, pp. 95–102, 2015.
- D. Ndwandwe and C. S. Wiysonge, “COVID-19 vaccines,” Current Opinion in Immunology, vol. 71, pp. 97–104, 2021.
- H. Ritchie, E. Ortiz-Ospina, D. Beltekian, E. Mathieu, J. Hasell, and B. Macdonald, “Coronavirus pandemic (COVID-19),” ourworldindata.org/covid-vaccinations. 2021.
- L. H. Abdullahi, B. M. Kagina, V. N. Ndze, G. D. Hussey, and C. S. Wiysonge, “Improving vaccination uptake among adolescents,” Cochrane Database of Systematic Reviews, vol. 2020, no. 1, 2020. https://doi.org/10.1002/14651858.CD011895.pub2 LK - http://resolver.lib.washington.edu/resserv?sid=EMBASE&issn=1469493X&id=10.1002%2F14651858.CD011895.pub2&atitle=Improving+vaccination+uptake+among+adolescents&stitle=Cochrane+Database+Syst.+Rev.&title=Cochrane+Database+of+Systematic+Reviews&volume=2020&issue=1&spage=&epage=&aulast=Abdullahi&aufirst=Leila+H&auinit=L.H.&aufull=Abdullahi+L.H.&coden=&isbn=&pages=-&date=2020&auinit1=L&auinitm=H.
- J. C. Jacobson Vann, R. M. Jacobson, T. Coyne-Beasley, J. K. Asafu-Adjei, and P. G. Szilagyi, “Patient reminder and recall interventions to improve immunization rates,” Cochrane Database of Systematic Reviews, no. 1, 2018. [CrossRef]
- J. Kaufman et al., “Face to face interventions for informing or educating parents about early childhood vaccination,” Cochrane Database of Systematic Reviews, no. 5, 2018. [CrossRef]
- Oyo-Ita; et al. , “Interventions for improving coverage of childhood immunisation in low- and middle-income countries (Review),” The Cochrane database of systematic reviews, no. 7, p. CD008145, 2016. [CrossRef]
- Saeterdal, S. Lewin, A. Austvoll-Dahlgren, C. Glenton, and S. Munabi-Babigumira, “Interventions aimed at communities to inform and/or educate about early childhood vaccination,” Cochrane Database of Systematic Reviews, no. 11, 2014. [CrossRef]
- S. Wiysonge, T. Young, T. Kredo, M. McCaul, and J. Volmink, “Interventions for improving childhood vaccination coverage in low- and middle-income countries,” South African Medical Journal, vol. 105, no. 11, pp. 892–893, 2015. [CrossRef]
- K. B. Cartmell et al., “Barriers, facilitators, and potential strategies for increasing HPV vaccination: A statewide assessment to inform action,” Papillomavirus Research, vol. 5, pp. 21–31, 2018. [CrossRef]
- C. P. S. T. Force, “Increasing appropriate vaccination: reducing client out-of-pocket costs for vaccinations. Task Force finding and rationale statement,” www.thecommunityguide.org/findings/vaccination-programs-reducing-client-out-pocket-costs.
- E. J. Mavundza, C. J. Iwu‐Jaja, A. B. Wiyeh, B. Gausi, L. H. Abdullahi, and G. Halle‐Ekane, “A systematic review of interventions to improve HPV vaccination coverage,” Vaccines, vol. 9, no. 7, p. 687. [CrossRef]
- K. McKeirnan, K. Colorafi, Z. Sun, K. Daratha, D. Potyk, and J. McCarthy, “Improving pneumococcal vaccination rates among older adults through academic detailing: medicine, nursing and pharmacy partnership,” Vaccines, vol. 9, no. 4, p. 317.
- Oyo-Ita, C. S. Wiysonge, C. Oringanje, C. E. Nwachukwu, O. Oduwole, and M. M. Meremikwu, “Interventions for improving coverage of childhood immunisation in low- and middle-income countries,” Cochrane Database of Systematic Reviews, no. 7. [CrossRef]
- J. Iwu, N. Ngcobo, A. Jaca, A. Wiyeh, E. Pienaar, and U. Chikte, “A systematic review of vaccine availability at the national, district, and health facility level in the WHO African Region,” Expert Review of Vaccines, vol. 19, no. 7, pp. 639–651.
- S. Tankwanchi, B. Bowman, M. Garrison, H. Larson, and C. S. Wiysonge, “Vaccine hesitancy in migrant communities: a rapid review of latest evidence,” Current Opinion in Immunology, vol. 71, pp. 62–68. [CrossRef]
- S. Wiysonge, P. W. Mahasha, D. E. Ndwandwe, N. Ngcobo, K. Grimmer, and J. Dizon, “Contextualised strategies to increase childhood and adolescent vaccination coverage in South Africa: a mixed-methods study,” BMJ Open, vol. 10, no. 6, p. e028476.
- E. Alici et al., “Facilitators and barriers to adult vaccination in South East Asia and Latin America,” Available from epoc.cochrane.org/epoc-specific-resources-review-authors, vol. 74, no. 1, pp. 398–408, 2017. [CrossRef]
- R. Johnson, K. L. Nichol, and K. Lipczynski, “Barriers to adult immunization,” American Journal of Medicine, vol. 12, no. 7 Suppl 2, pp. S28-35, 2008.
- J. Neufeind, C. Betsch, K. B. Habersaat, M. Eckardt, P. Schmid, and O. Wichmann, “Barriers and drivers to adult vaccination among family physicians – insights for tailoring the immunization program in Germany,” Vaccine, vol. 38, no. 27, pp. 4252–4262. [CrossRef]
- M. McNamara, P. O. Buck, S. Yan, L. R. Friedland, K. Lerch, and A. Murphy, “Is patient insurance type related to physician recommendation, administration and referral for adult vaccination? A survey of US physicians,” Human Vaccines & Immunotherapeutics, vol. 15, no. 9, pp. 2217–2226, 2019. [CrossRef]
- B. M. Davis and D. Black, “Facilitators and barriers to adult vaccination in South East Asia and Latin America,” Value in Health, vol. 20, no. 9, p. PA934. [CrossRef]
- C. M. Weyand and J. J. Goronzy, “Aging of the immune system. Mechanisms and therapeutic targets,” Annals of the American Thoracic Society, vol. 13, no. Suppl 5, pp. S422-8.
- R. Masters, A. Hall, J. M. Bartley, S. R. Keilich, E. C. Lorenzo, and E. R. Jellison, “Assessment of lymph node stromal cells as an underlying factor in age-related immune impairment,” Journals of Gerontology. Series A, Biological Sciences and Medical Sciences, vol. 74, no. 11, pp. 1734–1743, 2019. [CrossRef]
- H. L. Thompson, M. J. Smithey, C. D. Surh, and J. Nikolich-Žugich, “Functional and homeostatic impact of age-related changes in lymph node stroma,” Frontiers in Immunology, vol. 8, p. 706, 2017. [CrossRef]
- L. Tan, “Adult vaccination: now is the time to realize an unfulfilled potential,” Human Vaccines & Immunotherapeutics, vol. 11, no. 9, pp. 2158–2166, 2015. [CrossRef]
- S. Cooper, B. M. Schmidt, E. Z. Sambala, A. Swartz, C. J. Colvin, and N. Leon, “Factors that influence parents’ and informal caregivers’ acceptance of routine childhood vaccination: a qualitative evidence synthesis,” Cochrane Database of Systematic Reviews, no. 2. [CrossRef]
- S. Cooper et al., “Factors that influence acceptance of human papillomavirus (HPV) vaccination for adolescents: A qualitative evidence synthesis,” Cochrane Database of Systematic Reviews, vol. 2019, no. 9, 2019. https://doi.org/10.1002/14651858.CD013430 LK - http://resolver.lib.washington.edu/resserv?sid=EMBASE&issn=1469493X&id=10.1002%2F14651858.CD013430&atitle=Factors+that+influence+acceptance+of+human+papillomavirus+%28HPV%29+vaccination+for+adolescents%3A+A+qualitative+evidence+synthesis&stitle=Cochrane+Database+Syst.+Rev.&title=Cochrane+Database+of+Systematic+Reviews&volume=2019&issue=9&spage=&epage=&aulast=Cooper&aufirst=Sara&auinit=S.&aufull=Cooper+S.&coden=&isbn=&pages=-&date=2019&auinit1=S&auinitm=.
- C. Lefebvre, J. C. Lefebvre, J. Glanville, S. Briscoe, A. Littlewood, C. Marshall, and M. M-I, “Chapter 4: Searching for and selecting studies. In: Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 6.0 (updated 19). Cochrane, 2019,” Available from training.cochrane.org/handbook/archive/v6. 20 July.
- Jaca, M. Sishuba, J. C. Jacobson Vann, C. S. Wiysonge, and D. Ndwandwe, “Interventions to improve vaccination uptake among adults,” Cochrane Database of Systematic Reviews, vol. 2021, no. 11, 2021. [CrossRef]
- A. Liberati, D. G. Altman, J. Tetzlaff, C. Mulrow, P. C. Gotzsche, and J. P. Ioannidis, “The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration,” PLoS Medicine, vol. 6, no. 7, p. e1000100, 2009.
- C. E. P. and O. of Care, “Data collection form. EPOC resources for review authors, 2017,” Available from epoc.cochrane.org/epoc-specific-resources-review-authors.
- J. P. Higgins et al., “Cochrane Handbook for Systematic Reviews of Interventions Version 6.0 (updated July 2019). Cochrane, 2019,” Available from training.cochrane.org/handbook/archive/v6. 2019.
- E. P. and O. of Care, “Suggested risk of bias criteria for EPOC reviews. EPOC resources for review authors, 2017,” Available from epoc.cochrane.org/epoc-specific-resources-review-authors.
- M. Borenstein, L. V Hedges, J. P. Higgins, and H. R. Rothstein, “When does it make sense to perform a meta-analysis?,” in Introduction to Meta-Analysis, Chichester (UK): John Wiley & Sons, Ltd.
- G. H. Guyatt, “GRADE : an emerging consensus on rating quality of evidence and strength of recommendations,” vol. 336, no. April, 2008. [CrossRef]
- C. E. P. and O. of Care, “EPOC worksheets for preparing a ‘Summary of findings’ table using GRADE. EPOC resources for review authors, 2017,” Available from epoc.cochrane.org/epoc-specific-resources-review-authors.
- P. G. Szilagyi et al., “Effect of Personalized Messages Sent by a Health System’sPatient Portal on Influenza Vaccination Rates:a Randomized Clinical Trial.,” J Gen Intern Med, vol. x, no. x, p. x NS-Szilagyi 2021, 2021. [CrossRef]
- S. Doratotaj, M. L. Macknin, and and S. Worley, “A novel approach to improve influenzavaccination rates among health careprofessionals: A prospectiverandomized controlled trial.,” Am J Infect Control, vol. 36, pp. 301-3 NS-Doratotj 2008, 2008.
- Cochrane Handbok, “Cochrane Handbook,” pp. 25–26, 2024, [Online]. Available: https://training.cochrane.org/handbook/PDF/v6.4.
- M. Baker, B. McCaarthy, V. F. Gurley, and M. U. Yood, “Influenza immunization in a managed care organization.,” J Gen Intern Med, vol. 1998, no. 13, pp. 469-475 NS-Baker 1998, 1998. [CrossRef]
- S. L. Cutrona et al., “Improving Rates of Outpatient Influenza Vaccination Through EHRPortal Messages and Interactive Automated Calls: A RandomizedControlled Trial,” J Gen Intern Med, vol. 33, no. 5, pp. 659–67 NS-Cultrona 2018, 2018. [CrossRef]
- S. G. Humiston et al., “Increasing Inner-City Adult InfluenzaVaccination Rates: A RandomizedControlled Trial.,” Public Health Reports, vol. 126, no. 2, pp. 39-47 NS-Humiston 2011, 2011.
- L. P. Hurley et al., “RCT of Centralized Vaccine Reminder/Recall for Adults,” Am J Prev Med, vol. 55, no. 2, pp. 231–239 NS-Hurley 2018, 2018. [CrossRef]
- T. A. Jacobson, D. M. Thomas, F. J. Morton, G. Offutt, J. Shevlin, and S. Ray, “Use of a low-literacy patient education tool to enhance pneumococcal vaccination rates.,” JAMA, vol. 282, pp. 646-650 NS-Jacobson 1999, 1999. [CrossRef]
- H.-S. Juon, C. Strong, F. Kim, E. Park, and S. Lee, “Lay HealthWorker Intervention ImprovedCompliance with Hepatitis B Vaccination inAsian Americans: Randomized ControlledTrial.,” PLOS ONE, vol. xx, no. x, pp. 1-14 NS-Juon 2016, 2016. [CrossRef]
- S. E. Kim, B. J. Turner, J. Steinberg, L. Solano, E. Hoffman, and S. Saluja, “Partners in vaccination: A community-based intervention to promote COVID-19 vaccination among low-income homebound and disabled adults,” Disability and Health Journal, vol. 17, no. 3, p. 101589, 2024. [CrossRef]
- R. S. Klein and N. Adachi, “Pneumococcal Vaccine in the Hospital Improved Use and Implications for High-Risk Patients.,” Arch Intern Med, vol. 143, pp. 1878-1881 NS-Klein 1983, 1983.
- W.-N. Lee et al., “Large-scale influenza vaccination promotion on a mobile app platform: Arandomized controlled trial.,” Vaccine, vol. xxxx, no. xxx, pp. 1-7 NS-Lee 2020, 2020. [CrossRef]
- C. L. Masson et al., “A Randomized Trial of a Hepatitis Care CoordinationModel in Methadone Maintenance Treatment.,” American Journal of Public Health, vol. 103, no. 10, pp. 81-88 NS-Masson 2013, 2013. [CrossRef]
- W. P. Moran, K. Nelson, J. L. Wofford, and R. Velez, “Computer-generated Mailed Remindersfor Influenza Immunization:A Clinical Trial.,” J Gen Intern Med, vol. 7, no. 5, pp. 535-537 NS-Moran 1992, 1992.
- K. Nehme, M. Delphia, E. M. Cha, M. Thomas, and and D. Lakey, “Promoting Influenza Vaccination Amongan ACA Health Plan Subscriber Population:A Randomized Trial.,” American Journal of Health Promotion, vol. 33, no. 6, pp. 916-920 NS-Nehme 2019, 2019. [CrossRef]
- S. T. O’Leary, K. J. Narwaney, N. M. Wagner, C. R. Kraus, S. B. Omer, and J. M. Glanz, “Efficacy of a Web-Based Intervention to IncreaseUptake of Maternal Vaccines: An RCT.,” Am J Prev Med, vol. 57, no. 4, p. e125−e133 NS-O’Leary 2019, 2019. [CrossRef]
- S. H. Otsuka, N. H. Tayal, K. Porter, P. J. Embi, and and S. J. Beatty, “Improving Herpes Zoster Vaccination Rates Through Use of aClinical Pharmacist and a Personal Health Record,” Am J Med., vol. 126, no. 9, pp. 832.e1–832.e6 NS-Otsuka 2013, 2013. [CrossRef]
- A. Reddy et al., “Behaviorally Informed Text Message Nudges to Schedule COVID-19 Vaccinations: A Randomized Controlled Trial,” Journal of General Internal Medicine, no. 012345 6789, 2024. [CrossRef]
- R. Richman, L. Maddy, E. Torres, and and E. J. Goldberg, “A randomized intervention study to evaluate whether electronic messaging canincrease human papillomavirus vaccine completion and knowledge amongcollege students.,” Journal of American College Health, vol. 64, no. 4, pp. 269-78 NS-Richman 2016, 2016. [CrossRef]
- M. J. Siebers and and V. B. Hun, “Increasing the Pneumococcal Vaccination Rate of Elderly Patients in a General Internal Medicine Clinic.,” Journal of the American Geriatrics Society, vol. 33, no. 3, pp. 175-178 NS-Siebers 1985, 1985.
- M. S. Stockwell et al., “Influenza Vaccine Text Message Reminders for Urban,Low-Income Pregnant Women: A Randomized Controlled Trial.,” American Journal of Public Health, vol. 104, no. S1, pp. 7-12 NS-Stockwell 2014, 2014. [CrossRef]
- S. Stolpe and and N. K. Choudhry, “Effect of Automated Immunization Registry-BasedTelephonic Interventions on Adult Vaccination Rates inCommunity Pharmacies: A Randomized Controlled Trial,” J Manag Care Spec Pharm., vol. 25, no. 9, pp. 989-94 NS-Stolpe 2019, 2019. [CrossRef]
- M. Thomas et al., “Patient education strategies to improve pneumococcal vaccination rates: randomized trial. TT - Journal of Investigational medicine,” J Investig Med, vol. 51, no. 3, pp. 141-148 NS-Thomas 2003, 2003.
- E. Ueberroth, H. R. Labonte, and and M. R. Wallace, “Impact of Patient Portal Messaging Reminderswith Self-Scheduling Option on Influenza Vaccination Rates:a Prospective, Randomized Trial.,” J Gen Intern Med, vol. x, no. x, p. x NS-Ueberroth 2021, 2021. [CrossRef]
- D. Yokum1, J. C. Lauffenburger2, and R. G. and N. K. Choudhr, “Letters designed with behavioural science increase influenza vaccination in Medicare beneficiaries.,” Nature Human Behaviour, vol. 2, no. 10, pp. 743–749 NS-Yokum 2018, 2018.
- M. P. and J. Ward, “Postcard reminders from GPs for influenza vaccine: Are they more effective than an ad hoc approach?,” Journal of Public Health, vol. 22, no. 2, pp. 254-256 NS-Puech 1998, 1998.
- L. K. Mccosker, R. S. Ware, H. Seale, D. Hooshmand, R. O. Leary, and M. J. Downes, “The effect of a financial incentive on COVID-19 vaccination uptake, and predictors of uptake, in people experiencing homelessness : A randomized controlled trial,” Vaccine, vol. 42, no. 10, pp. 2578–2584, 2024. [CrossRef]
- L. Topp et al., “A randomised controlled trial of financial incentives to increase hepatitis B vaccination completion among people who inject drugs in Australia,” Preventive Medicine, vol. 57, no. 4, pp. 297–303, 2013. [CrossRef]
- Q. Ju, H. Xiao, H. Peng, and Y. Gan, “How to Improve People’s Intentions Regarding COVID‐19 Vaccination in China: A Randomized Controlled Trial,” International Journal of Behavioral Medicine, no. 0123456789, 2024, doi: 10.1007/s12529‐024‐10258‐6. [CrossRef]
- S. Coenen et al., “Effects of Education and Information on Vaccination Behavior inPatients with Inflammatory Bowel Disease.,” Inflamm Bowel Dis, vol. 23, pp. 318-324 NS-Coenen 2016, 2016.
- M. Currat and C. L.-B. and G. Zanetti, “Promotion of the influenza vaccination tohospital staff during pre-employmenthealth check: a prospective, randomised,controlled trial.,” Journal of Occupational Medicine and Toxicology, vol. 15, pp. 34 NS-Currat 2020, 2020.
- K. C. Leung et al., “Impact of patient education on influenza vaccine uptake among community-dwelling elderly: a randomized controlled trial.,” Health Education Research, vol. 32, no. 5, pp. 455-464 NS-Leung 2017, 2017.
- Jør. Nexøe and J. K. & T. Rønne, “Impact of postal invitations and user fee oninfluenza vaccination rates among the elderly: Arandomized controlled trial in general practice,” Scand J Prim Health Care, vol. 15, pp. 109-112 NS-Nexeo 1997, 1997.
- K. A. Schmidtke et al., “Randomised controlled trial of atheory-basedintervention to promptfront-linestaff to take up theseasonal influenza vaccine.,” BMJ Qual Saf, vol. 29, pp. 189–197 NS-Schmidtke 2020, 2020.
- S. M. D. Terrell-Perica, P. V Effler, P. M. Houck, L. Lee, and G. H. Crosthwaite, “The Effect of a Combined Influenza/PneumococcalImmunization Reminder Letter.,” Am J Prev Med, vol. 21, no. 4, pp. 256-260 NS-Terrell-Perica 2001, 2001.
- P. L. Hu, E. Y. L. Koh, J. S. H. Tay, V. X.-B. Chan, S. S. M. Goh, and S. Z. Wang, “Assessing the impact of educational methods on influenza vaccine uptake and patient knowledge and attitudes: a randomised controlled trial.,” Singapore Medical Journal, vol. 64, no. 2, pp. 98-104 NS-Pei-Lin 2021, 2023.
- L. Topp et al., “A randomised controlled trial of financial incentives to increase hepatitis B vaccination completion among people who inject drugs in Australia,” Prev Med, vol. 57, no. 4, pp. 297-303 NS-Topp 2013.
- S. (Cindy) S. and V. Dubey, “Addressing vaccine hesitancy Clinical guidance for primary care physicians working with parents.,” Can Fam Physician, vol. 65, no. 3, pp. 175–181, 2019.
- A. Fuller; et al. , “Barriers and facilitators to vaccination uptake against COVID-19, influenza, andpneumococcal pneumonia inimmunosuppressed adults with immune mediated inflammatory diseases: A qualitative interview study during the COVID-19pandemic.,” PLOS ONE, vol. xx, no. xx, pp. 1–14, 2022.
- E. Batteux, F. Mills, L. F. Jones, and C. S. and DaleWeston, “The Effectiveness of Interventions for Increasing COVID-19Vaccine Uptake: A Systematic Review.,” Vaccines, vol. 10, no. 3, p. 386, 2022.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



