
Submitted:
17 April 2025
Posted:
18 April 2025
You are already at the latest version
Abstract
Background/Objectives: Mental disorders and diabetes-related distress (DRD) are under-addressed aspects of person-centered diabetes care. This study examines the burden of depression, anxiety, and DRD among adults with type 1 or 1.5 (T1D/T1.5D), type 2 (T2D), and gestational diabetes (GD), and explores their experiences and barriers in receiving mental health services. Methods: This study uses quantitative data from the 2023/24 Diabetes, Distress, and Disparities (3D) Study, which consists of 573 adults with diabetes (51.3% with T1D/T1.5D, 43.5% with T2D, and 4.4% with current/past GD). Mental health assessments included the Patient Health Questionnaire-9 (depression), Generalized Anxiety Disorder-7 (anxiety), and Problem Areas in Diabetes-11 (DRD). Logistic regression was used to examine the prevalence of mental health concerns and behavioral service use. Results: Overall, 14.5% had clinically-significant depression, 8.0% had anxiety, and 23.6% had elevated DRD. Symptoms of depression, anxiety, and DRD had a positive, non-linear relationship with poor glycemic control. Approximately 30% of those with clinically-significant emotional health concerns did not receive any behavioral health services in the past 12 months. Black adults were less likely to receive behavioral health treatment than non-Hispanic Whites (Odds ratio=0.24, 95% CI: 0.07- 0.77). Common reasons for not receiving behavioral health services included not knowing where to go, cost, and lack of accessible providers. Conclusions: Gaps in addressing emotional health needs of people with diabetes persist. Healthcare systems need to integrate addressing psychosocial factors as part of person-centered diabetes care.
Keywords:
diabetes
; depression
; anxiety
; diabetes-related distress
; mental health services
1. Introduction
Psychosocial aspects of diabetes (e.g., mental disorders, emotional distress, stress) are an important, yet under-addressed, feature of living with diabetes [1]. It is established that people with diabetes (PWD) have approximately twice the prevalence of anxiety and depression disorders relative to people who do not have diabetes (~20% vs. 10%) [2,3]. For many years, it was assumed that this comorbidity largely arose due to the “depression-genic” nature of being diagnosed with diabetes. However, over the past 25 years a large body of longitudinal research now indicates that the relationship between diabetes and poor mental health is bi-directional, reflecting both common biological (i.e., hypercortisolism, inflammation) and behavioral (i.e., disrupted sleep, poor diet, alcohol and tobacco use) mediating pathways [4,5].
In considering how diabetes relates to poor mental health over the lifespan, it is critical to note that this bi-directional relationship also varies by diabetes type. Type 2 diabetes (T2D) typically does not onset until the mid-late 50s or early 60s, and as a result depression and anxiety (which have highest incidence in adolescence and early adulthood) are more often predictors, rather than consequences, of a new T2D diagnosis [4,6]. In contrast, depression and anxiety are often concurrent with, or sequelae of, a diagnosis of type 1 (T1D) [7,8]. While less well studied, perinatal depression and anxiety can also accompany a diagnosis of gestational diabetes (GD) [9,10]. Finally, regardless of diabetes type, depression and anxiety are both predictors and correlates of poor glycemic control and diabetes-related complications [11].
In addition to depression and anxiety, between 30-50% of PWD experience diabetes-related distress (DRD), which reflects the emotional burden of daily self-management required of this chronic condition [12,13]. While DRD often co-occurs with depression and anxiety, leaders in the field argue that it is a distinct psychosocial construct [14,15]. The distinction between DRD and disorders such as depression and anxiety is warranted, in part, due to the different approaches typically used to manage these emotional states. While clinical trials have demonstrated that psychotherapy is as effective as pharmacotherapy for treating most depression and anxiety disorders, in the US and in many other developed economies these conditions are typically solely treated with medications [16]. This reality reflects both an overstretched behavioral health workforce and insurance policies which make pharmacotherapy a far more affordable treatment option for most patients. In contrast, the interventions for DRD are largely non-pharmacologic and draw on foundational concepts in cognitive behavioral therapy and even mindfulness practices to help PWD manage their concerns about diabetes and develop self-efficacy around self-care behaviors [17,18,19].
Regardless of whether mental health concerns occur before, after, or alongside a diagnosis of diabetes, these symptoms and conditions have important implications for “person-centered” diabetes care, i.e., care that centers a PWD’s goals, needs, and values regarding their health [20]. The importance and relevance of psychosocial factors to person-centered diabetes care were first enumerated by the Diabetes Attitudes, Wishes and Needs (DAWN) Studies. These multi-national studies surveyed thousands of adults with T1D and T2D, as well as healthcare providers, and provided some of the most comprehensive assessments of the impact of diabetes on people’s lives [21,22]. DAWN illustrated that PWD reported that their disease negatively impacted multiple domains of their lives, including their overall physical health (62%), relationship with family/friends (20%), and emotional well-being (46%) [13]. Despite this broad impact, DAWN found that less than one-third said that their healthcare provider had asked about their emotional health or how diabetes affects their lives in the past 12 months; in contrast, nearly 75% said their healthcare team had measured their blood sugar during this same period. Follow-up studies of DAWN have shown that less than 20% of PWD that had clinically-significant depression and/or DRD received any psychological care [23]. This illustrates the substantial gap between the psychosocial aspects of diabetes care that PWD need versus the actions and structures of the healthcare systems they navigate [24].
Since the completion of the DAWN studies in 2012, the American Diabetes Association (ADA) has made two major efforts to address the concerns raised by these studies. The first was a position statement in 2016 which argued that addressing psychological well-being was essential to the delivery of “patient”-centered care, calling for collaborative, integrated psychosocial care to be provided to “all people with diabetes” (scored as an “A” recommendation), and that providers should screen for DRD, depression, anxiety, and related behaviors multiple times over the course of the condition (scored as a “B” recommendation) [1]. In 2020, the ADA released its Behavioral Health Toolkit, which provided both decision-guidance and standardized tools (e.g., Patient Health Questionnaire for depression) for healthcare providers to implement these recommendations [25]. In short, over the past decade there has been increasing attention to psychosocial care needs of PWD by both researchers and professional organizations, and therefore it is reasonable to assess whether the gaps in care identified by DAWN have begun to shrink.
In addition, the advent of diabetes management technology (e.g., continuous glucose monitors) and related mobile technology devices (e.g., monitors for actigraphy, sleep, mood) mean that PWD potentially have access to a wide array of digital data on their overall health, and their diabetes management specifically, in a manner that was not true when the DAWN studies were fielded. However, such devices remain cost-prohibitive for many people, and even among those who have access it is an open question as to whether and how this technology ecosystem can support (or even impair) the emotional components of diabetes management [26,27]. Moreover, while technology has become increasingly integrated into diabetes care, mental health care remains largely a “brick and mortar” business that is plagued by understaffing, long wait times, and a lack of culturally-appropriate providers, which means that under-detection and under-treatment of mental health conditions for PWD may persist despite efforts by the ADA for reform [28].
Building on this large body of research on psychosocial aspects of diabetes, the goals of this paper are threefold: First, to describe the burden of clinically-relevant depression, anxiety and DRD among a diverse sample of adults with T1D, T2D and GD. Second, to examine the experiences of mental health service utilization among these individuals seen at a large US-based medical center. Finally, to characterize the barriers experienced by adults with diabetes when they seek mental health services. By mapping the mental health care needs among this PWD, this project can help identify actionable gaps that health systems can address in order to provide more person-centered diabetes care.
2. Materials and Methods
Participants come from the Diabetes, Distress and Disparities (3D) Study of Self-Management and Mental Health, which was fielded over an 18-month period in 2023-2024. The primary objective of the 3D Study is to quantify and characterize the psychosocial care needs of adults with T1D, latent autoimmune diabetes in adulthood (LADA or T1.5D), T2D, and current or past gestational diabetes. The overarching goal of this project is to partner with various stakeholders to implement evidence-based strategies to address identified gaps in person-centered diabetes care in the Michigan Medicine healthcare system and beyond.
The 3D Study employed a two-part sequential mixed methods design: Part 1 consisted of a 30–40-minute quantitative web survey (in Qualtrics) that assessed a range of topics relevant to self-management including diabetes-related distress, depression, anxiety, diabetes-related stigma, technology use, social support, and social determinants of health. Part 1 consists of 573 PWD (5% overall response rate). Details of the data collection and fieldwork procedures are described elsewhere [29]. Briefly, persons aged 18+ with a current diagnosis or history of diabetes seen at Michigan Medicine in the prior two years were identified by ICD-9/10 codes: 249, 250, 775.1, E08, E09, E10, E11, E13, O24, and P70.2. People with T1D and GD were over-sampled to increase their representation, given the relatively low prevalence of these forms of diabetes relative to T2D. Individuals were invited via email to participate in the survey by an intermediate Michigan Medicine Electronic Health Record (EHR) broker to protect confidentiality. Participants who completed the Part 1 survey and indicated their willingness to be contacted about future research were eligible for Part 2 of the study, which consisted of a 60-minute one-on-one semi-structured interview to probe more complex topics such as patient-provider relationships, priorities in care, and self-efficacy (n=40 also completed Part 2). This analysis only uses data from Part 1 of the 3D Study.
The 3D Study was approved by the IRB at the University of Michigan (HUM00223735) and all participants provided written informed consent. The 3D Study materials and data collection protocols are publicly-available at the Open Science Framework (https://osf.io/yfz6b/).
Depression. Current depressive symptoms were assessed using the Patient Health Questionnaire (PHQ-9), a brief instrument for assessing clinically-relevant depression in primary care settings [30]. The PHQ-9 assesses the frequency of nine symptoms drawn from the Diagnostic and Statistical Manual of Mental Disorders (DSM) criteria for Major Depression (i.e., dysphoria, anhedonia, sleep disturbances, appetite disturbances, cognitive challenges, fatigue, psychomotor changes, feeling of worthlessness, and suicidal ideation) each assessed on a 4-point scale ranging from Not at all to Nearly every day, referring to the past 2 weeks. A final item, which asks about how much difficulty the person has experienced due to these symptoms, is not used in the scoring. Only participants with complete data on all nine symptoms were included in the analysis (n=77 due to missing data on one or more symptoms). Scores were summed (range: 0 to 27) and dichotomized, with values ≥15 indicating moderately severe or more depression.
Anxiety. Current anxiety symptoms were assessed using the Generalized Anxiety Disorder-7 (GAD), a brief screening instrument for assessing clinically-relevant anxiety in primary care settings [31]. It consists of seven items drawn from DSM criteria for anxiety disorders (i.e., feeling nervous, uncontrollable worry, general nervousness, being unable to relax, feeling restless, being irritable, and feeling fearful about the future) each assessed on a 4-point scale ranging from Not at all to Nearly every day, referring to the past 2 weeks. A final item, which asks about how much difficulty the person has experienced due to these symptoms, is not used in the scoring. Only participants with complete data on all seven symptoms were included in the analysis (n=58 due to missing data on one or more symptoms). Scores were summed (range: 0 to 21) and dichotomized, with values ≥15 indicating severe anxiety.
Diabetes-related distress. Current DRD was assessed using the Problem Areas in Diabetes (PAID-11), a brief instrument for assessing emotional aspects of living with diabetes [32]. It asks “how much of a current problem” various experiences, feelings, and beliefs related to diabetes are for the person (i.e., 11 items including feeling scared (depressed) about diabetes, uncertainty about emotions, worrying about low blood sugar, concerns about food, worrying about complications, feeling anxiety and/or guilt about self-management, feeling overwhelmed, mental energy needed to manage diabetes, coping with complications, and feeling “burned out”). Each item is assessed on a five-point scale ranging from Not a problem to Serious problem. Only participants with complete data on all 11 items were included in the analysis (n=52 due to missing data on one or more symptoms). Scores were summed (range: 0 to 44) and dichotomized, with values > 18 indicating clinically-relevant (elevated) DRD.
Mental health services use. Receipt of mental, behavioral, and/or substance use treatment in the past 12 months was assessed by a series of questions. Participants were asked if they had received any “professional counseling, medication, or treatment” for emotions, mental health, or behavior. A second question asked specifically about use of any prescription medications for treating a “mental or emotional condition”. These two items were combined into a single dichotomous variable for analysis, indicating any vs. no mental health services received in the past 12 months.
Barriers to mental health services. To assess barriers to receipt of mental health care, participants were asked if there was “any time [in the past 12 months] when you needed mental health treatment or counseling for yourself but didn’t get it?” and those who responded affirmatively were asked why they were unable to get the treatment they needed. Response options were not mutually-exclusive and included: cost, concern that treatment would cause others to have a negative opinion of them, concern that treatment would have a negative impact on their job, lack of or inadequate insurance coverage, concerns about confidentiality, concerns that they would be forced to undergo inpatient or medication treatment, unable to find a provider, or some other reason.
Diabetes characteristics. Diabetes type and hemoglobin A1c (HbA1c) were assessed by self-report. Individuals who reported a history of multiple types of diabetes were re-coded as having a single “primary” type based on which was more persistent (e.g., individuals who reported both T2D and gestational diabetes were coded as having T2D). Individuals who reported having both T1D and T2D were coded as having T1.5, as this diagnosis is often made after mis-diagnosis of T2D. HbA1c is an indicator of glycemic control over the past 30-90 days, with values <7% indicating adequate control. Participants were asked to report their most recent HbA1c (%) value; individuals who reported a range (e.g., “usually between 5.6 to 5.9%”), rather than a single value, were assigned the highest value they provided.
All covariates were assessed by self-report. Demographic characteristics included age (in years), gender (man, woman, gender non-conforming), race/ethnicity (Native American/Alaskan Native, Asian, Black/African American, Latino, White, more than one race, and prefer not to say, which was re-coded for analysis as White, Black/African American, and all others), highest level of education obtained (recoded for analysis as high school or less, associate’s degree/certificate program, bachelor’s degree, and advanced degree), household income (re-coded for analysis as <$50,000, $50,000 to <$100,000, $100,000 to <$150,000 and $150,000 or more).
While this is primarily a descriptive analysis, we have three overarching hypotheses: 1) Depression, anxiety, and DRD (and their co-occurrence) will be more prevalent among PWD compared to similarly-age general population samples, 2) Even though participants were drawn from a major academic medical center, the majority of those with clinically-significant depression, anxiety, and DRD will not have received any mental health services, and 3) Reflecting disparities in healthcare access, factors such as age, gender, race/ethnicity, and socioeconomic status will be associated with barriers to mental health service use even after accounting for clinical need as indicated by depression, anxiety, and DRD symptoms.
Initially, sample characteristics as a function of mental health conditions (depression and anxiety) were quantified using descriptive statistics. Graphs were used to illustrate the prevalence of clinically-significant depression, anxiety, and DRD by diabetes type and HbA1c, calculated from multivariable logistic regression models that adjusted for demographic characteristics. Next, descriptive statistics and logistic regression was used to explore predictors of mental health service use among those with clinically-significant depression, anxiety, and DRD. Finally, graphs were used to illustrate the most common reasons cited for not receiving mental health care. Due to small cells, people with T1.5 were combined with those with T1D, and for most analyses there were insufficient numbers of those with GD to estimate regression models.
While this is primarily a descriptive analysis, when making comparisons we use a threshold of p<0.05 to evaluate statistically significant differences and all p-values refer to two-tailed tests.
3. Results
The Phase 1 sample of the 3D Study consists of 573 adults with diabetes, approximately half with T1D/T1.5D (n=294, 51.3%) or T2D (n=249, 43.5%); 25 had current or past history of GD (4.3%) and n=5 did not know their diabetes type. This sample had a mean age of 53.3 years (SD: 17.3, range: 19 – 92) and 54% were women. Scores on the PHQ-9 (7.7, SD: 6.3), GAD-7 (5.3, SD: 5.5), and PAID-11 (11.8, SD: 10.0) indicate that, on average, participants in the 3D Study reported mild to moderate emotional distress across the three scales.
3.1. Burden of Clinically-Relevant Depression, Anxiety and DRD
Overall, 14.5% had clinically-significant depression, 8.0% had clinically-significant anxiety, and 23.6% had elevated DRD. For comparison, a 2025 study from the National Health and Nutrition Examination Survey (NHANES), which also used the PHQ-9 but applied a lower scoring threshold of >9 (vs. our threshold of >14) symptoms, reported the prevalence of depression among US adults was 12.4% [33]. Also, in 2019, the National Health Interview Survey (NHIS), which also used the GAD-7 and applied the same threshold as the 3D Study, reported that only 2.8% of US adults had clinically-significant anxiety [34]. As expected, depression, anxiety, and DRD were highly correlated (r2 ranged from 0.645 to 0.797), and 39% of those with clinically-significant depression also had clinically-significant anxiety. As shown by Table 1, having comorbid depression/anxiety was associated with higher HbA1c (7.93% vs. 6.96% for those with neither condition), and approximately 70% of people with elevated depression, anxiety, or both received some form of behavior or mental health treatment in the past 12 months as compared to 30% who had neither depression nor anxiety.
As shown by the panels of Figure 1, adults with T1D/T1.5D had higher prevalence of clinically-significant depression, anxiety, and DRD than those with T2D. Other factors that were significantly associated with poor mental health included younger age, being a woman, and lower household income; race and educational attainment were not significantly correlated with clinically-significant depression, anxiety or DRD. While not shown in the figure due to small cells, people with current or past GD had relatively low unadjusted prevalence of depression (4.0%), anxiety (4.0%) and DRD (12.0%) indicating that this population may not have the same mental health concerns as other PWD.
As shown by the panels of Figure 2, there was a non-linear relationship between HbA1c and poor mental health. For HbA1c values <7.5% there was no correlation between these measures, but for values HbA1c>7.5%, increasing levels of HbA1c were positively associated with probability of clinically-significant depression, anxiety, and DRD.
3.3. Mental Health Services Use and Barriers to Psychosocial Care Among PWD
Overall, 42.6% had received any form of mental/behavioral health services in the prior 12 months. Unsurprisingly, a greater proportion of people with elevated scores of depression (77.1%), anxiety (76.1%), or DRD (63.0%) received any mental health care in the past year compared to people who had none of these (34.7%). As shown by Table 2, among those with clinically-elevated depression, anxiety and/or DRD (n=153), significant predictors of receiving mental health care in the past year were gender and race/ethnicity. Women were more than twice as likely as men to report mental health treatment in the past 12 months whereas Black/African American respondents had 76% lower odds of receiving treatment. While not shown in the regression table, 66.7% people with GD who had any clinically-significant emotional health concern received any mental health treatment in the past year. Finally, as shown by Figure 3, the most prevalent barriers to mental health treatment were related to access and availability. Almost half of persons who reported barriers to mental health treatment indicated that at least one barrier was not captured in the list provided in the study question. The primary factor that was associated with reporting >1 reason for being unable to access treatment when needed was lower income (54.1% of people with household incomes <$50,000 reported >1 reason vs. only 2.7% of those with incomes >$150,000).
4. Discussion
This cross-sectional study of adults with diabetes aimed to describe the “emotional side of diabetes” and use of behavioral health services in this population, in order to understand the extent to which recent efforts by the ADA and related organizations have begun to close gaps in “person-centered” diabetes care [35]. The findings from this study are threefold: First, depression, anxiety, and DRD are highly prevalent in this population, and are more common among persons with T1D/T1.5D compared to those with T2D. Overall, 38.6% of people with T1/1.5D, 23.5% of people with T2D, and 13.6% with GD had at least one mental health concern. Second, approximately 30% of people with clinically-significant depression or anxiety had not accessed any behavioral health services in the past year. While this is notably higher than previous studies of mental health service use among PWD [23], there were still notable disparities in access to care. Specifically, Black PWD were significantly less likely to have received needed behavioral health care. The primary reasons for not accessing behavioral health services were that they didn’t know where to go for services, cost, or a lack of providers in the area or insurance network. Finally, these emotional aspects of diabetes have implications for the management of this condition as indicated by glycemic control. Symptoms of depression, anxiety, and DRD had a non-linear relationship with HbA1c, such that for those with HbA1c values >7.5% as emotional symptoms increased so did A1c values. Collectively, these findings emphasize that substantial gaps remain in effectively addressing emotional aspects of diabetes, and point to the importance of integrative approaches to diabetes care.
Building on the foundational work and insights of the DAWN studies, which highlighted the psychosocial care needs and gaps in person-centered care globally, our study provides a more current view of these challenges within a U.S. context. Our data also offer a nuanced look at how emotional symptoms (i.e., anxiety, depression, DRD) are linked to glycemic outcomes, adding depth to prior DAWN findings by showing a non-linear relationship between HbA1c and emotional distress. By oversampling individuals with T1D/T1.5D, who comprised a smaller proportion of DAWN2 participants (e.g., 80 with T1D vs 420 with T2D per country), we were able to identify important subgroup differences in emotional burden and service use. Despite increased attention to the emotional side of diabetes over the past decade, our findings underscore persistent barriers to accessing behavioral health care.
It is important to recognize that barriers to psychosocial care do not have to be absolute (e.g., zero behavioral health providers in the area) in order to significantly impact the lives of PWD. Standard models of diabetes care tend to distinguish between “disease” and “life”, and this divide creates tensions that have direct implications for the emotional side of this condition [36]. Empirical research has shown that this divide impairs problem-solving even around “disease” topics like medication adherence [37]. Fortunately, decades of empirical health services research has provided compelling evidence that person-centered collaborative care models (CCM, e.g., models of care in which a team of health professionals with differing expertise, roles, and responsibilities) generate clinically-significant improvements in both glycemic control (measured by HbA1c) and depressive symptoms for adults with comorbid depression and diabetes [38]. These models of care are also cost-effective [39,40,41]. However, implementation of these models remains low [42], with factors such as financing and staffing needs cited as major barriers to adoption of person-centered care models [43,44].
Regardless of whether psychosocial support directly improves clinical diabetes indicators (e.g., glycemic control) [45,46,47], it is established is that such interventions are effective for reducing symptoms of anxiety, depression, DRD and improving quality of life for PWD [45,48,49]. This is an end worthy of pursuit in and of itself for PWD and their families [1]. Given the behavioral health workforce shortage, it is essential that healthcare systems explore creative means of achieving this goal, including employing Community Health Workers (CHW) or connecting with local organizations (e.g., YMCA, church health ministries, etc.) to implement diabetes peer support programs. Such programs are clinically- and cost-effective means of bridging the gap between “disease” and “life” for PWD in a manner that can be more adaptable to the needs of disadvantaged groups that have a higher burden of diabetes, particularly T2D (e.g., lower income, racial/ethnic minorities, rural areas) [50,51,52,53,54,55,56,57]. It remains to be seen whether technology, which has become such a core part of self-management for PWD (e.g., insulin pump, CGMs, apps, etc.) [58], can also help support the emotional aspects of this condition [59,60]. Future analyses of the 3D Study data can explore this possibility.
Findings should be interpreted in light of study limitations. This is a cross-sectional, descriptive study, and thus we are unable to test hypotheses of causal relationships. While the PHQ-9, GAD-7 and PAID-11 are widely used screening instruments for depression, anxiety, and DRD, respectively, they are not as sensitive as clinical diagnostic assessments. While the 3D Study was designed to recruit people with T1D, T2D and GD, limited sample size of the latter group precluded some analyses. Finally, due to policies protecting patient confidentiality, we are unable to assess the degree to which those who agreed to participate in the 3D Study differed from those who were invited but did not respond. Strengths include sample diversity (e.g., in terms of diabetes type, age, gender, and race/ethnicity) and the inclusion of multiple indicators of emotional health. Finally, the study team consulted with multiple patient advisory boards in the development of the survey, which helps ensure the study reflects the priorities of the people who live with this condition [61]..
5. Conclusions
While CCM and related models are a clinically- and cost-effective embodiment of person-centered diabetes care, they are not cost-free [62]. Indeed, no intervention, no matter how minor, that a healthcare system delivers is “free,” and the only ways systems can reduce costs (in an absolute sense) is by reducing demand for services - or by limiting the services they provide - from their patients. The comorbidity of diabetes with depression and anxiety requires a different type of algebra for understanding the costs of action - and of inaction - than what is typically employed by providers, systems, and payers. Even if addressing mental health concerns of PWD (whether through medications or psychotherapy) does not directly impact diabetes clinical outcomes (e.g., HbA1c), this should not discount the benefit to the individual and their family of effectively addressing their emotional needs [63]. Currently, gaps in addressing psychosocial aspects of diabetes care increases the (emotional) costs of living with diabetes [1,64], which has substantial impacts on individuals’ quality of life, ability to work, financial stability, and overall health [65,66]. Healthcare systems should consider that when they do not provide person-centered diabetes care, they are likely generating costs for PWD, i.e., the very people they seek to serve.
Author Contributions
B. Mezuk: Conceptualization, Writing - Original draft, Writing - Review & editing, Funding acquisition. K.M. Mannor: Writing – Original draft, Methodology, Visualization, Formal analysis, Writing - Reviewing & editing. R. Hebert: Data curation, Writing - Review & editing. L. Kouassi: Data curation, Writing - Review & editing. E. Spring: Investigation, Writing - Review & editing. B. Flores: Investigation. A. Rodríguez-Putnam: Supervision, Project administration, Writing - Review & editing.
Funding
The 3D study is supported by the Caswell Diabetes Institute at the University of Michigan. B. Mezuk is also supported by NIMH (R25MH136652).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of the University of Michigan (HUM00223735), approved on 20 March 2023.
Informed Consent Statement
This study is approved by the Institutional Review Board at the University of Michigan (HUM00223735) and all participants provided written informed consent.
Data Availability Statement
The 3D Study materials are publicly-available at https://osf.io/yfz6b/.
Acknowledgments
The authors would like to thank Ms. Caitlan DeVries for her support in coordinating the 3D study, and the participants in the 3D study for sharing their experiences. Without their involvement this study would not have been possible.
Conflicts of Interest
The authors have no conflicts of interest to report.
References
- Young-Hyman, D.; De Groot, M.; Hill-Briggs, F.; Gonzalez, J.S.; Hood, K.; Peyrot, M. Psychosocial Care for People With Diabetes: A Position Statement of the American Diabetes Association. Diabetes Care 2016, 39, 2126–2140. [Google Scholar] [CrossRef] [PubMed]
- Holt, R.I.G.; de Groot, M.; Golden, S.H. Diabetes and Depression. Curr. Diab. Rep. 2014, 14, 491. [Google Scholar] [CrossRef] [PubMed]
- Holt, R.I.G.; de Groot, M.; Lucki, I.; Hunter, C.M.; Sartorius, N.; Golden, S.H. NIDDK International Conference Report on Diabetes and Depression: Current Understanding and Future Directions. Diabetes Care 2014, 37, 2067–2077. [Google Scholar] [CrossRef] [PubMed]
- Mezuk, B.; Eaton, W.W.; Albrecht, S.; Golden, S.H. Depression and Type 2 Diabetes Over the Lifespan: A Meta-Analysis. Diabetes Care 2008, 31, 2383–2390. [Google Scholar] [CrossRef]
- Bergmans, R.S.; Rapp, A.; Kelly, K.M.; Weiss, D.; Mezuk, B. Understanding the Relationship between Type 2 Diabetes and Depression: Lessons from Genetically Informative Study Designs. Diabet. Med. 2021, 38, e14399. [Google Scholar] [CrossRef]
- Golden, S.H.; Lazo, M.; Carnethon, M.; Bertoni, A.G.; Schreiner, P.J.; Diez Roux, A.V.; Lee, H.B.; Lyketsos, C. Examining a Bidirectional Association Between Depressive Symptoms and Diabetes. JAMA 2008, 299, 2751–2759. [Google Scholar] [CrossRef]
- van Duinkerken, E.; Snoek, F.J.; De Wit, M. The Cognitive and Psychological Effects of Living with Type 1 Diabetes: A Narrative Review. Diabet. Med. 2020, 37, 555–563. [Google Scholar] [CrossRef]
- Fisher, L.; Polonsky, W.H.; Hessler, D.M.; Masharani, U.; Blumer, I.; Peters, A.L.; Strycker, L.A.; Bowyer, V. Understanding the Sources of Diabetes Distress in Adults with Type 1 Diabetes. J. Diabetes Complications 2015, 29, 572–577. [Google Scholar] [CrossRef]
- Zhang, C.; Jing, L.; Wang, J. Does Depression Increase the Risk of Gestational Diabetes Mellitus? A Systematic Review and Meta-Analysis. Pak. J. Med. Sci. 2022, 39. [Google Scholar] [CrossRef]
- Wilson, C.A.; Newham, J.; Rankin, J.; Ismail, K.; Simonoff, E.; Reynolds, R.M.; Stoll, N.; Howard, L.M. Systematic Review and Meta-Analysis of Risk of Gestational Diabetes in Women with Preconception Mental Disorders. J. Psychiatr. Res. 2022, 149, 293–306. [Google Scholar] [CrossRef]
- Wojujutari Ajele, K.; Sunday Idemudia, E. The Role of Depression and Diabetes Distress in Glycemic Control: A Meta-Analysis. Diabetes Res. Clin. Pract. 2025, 221, 112014. [Google Scholar] [CrossRef]
- Perrin, N.E.; Davies, M.J.; Robertson, N.; Snoek, F.J.; Khunti, K. The Prevalence of Diabetes-specific Emotional Distress in People with Type 2 Diabetes: A Systematic Review and Meta-analysis. Diabet. Med. 2017, 34, 1508–1520. [Google Scholar] [CrossRef] [PubMed]
- Nicolucci, A.; Kovacs Burns, K.; Holt, R.I.G.; Comaschi, M.; Hermanns, N.; Ishii, H.; Kokoszka, A.; Pouwer, F.; Skovlund, S.E.; Stuckey, H.; et al. Diabetes Attitudes, Wishes and Needs Second Study (DAWN2TM): Cross-national Benchmarking of Diabetes-related Psychosocial Outcomes for People with Diabetes. Diabet. Med. 2013, 30, 767–777. [Google Scholar] [CrossRef] [PubMed]
- Snoek, F.J.; Bremmer, M.A.; Hermanns, N. Constructs of Depression and Distress in Diabetes: Time for an Appraisal. Lancet Diabetes Endocrinol. 2025, 3, 450–460. [Google Scholar] [CrossRef]
- Fisher, L.; Skaff, M.M.; Mullan, J.T.; Arean, P.; Mohr, D.; Masharani, U.; Glasgow, R.; Laurencin, G. Clinical Depression Versus Distress Among Patients With Type 2 Diabetes. Diabetes Care 2007, 30, 542–548. [Google Scholar] [CrossRef]
- Olfson, M.; Marcus, S.C. National Patterns in Antidepressant Medication Treatment. Arch. Gen. Psychiatry 2009, 66, 848. [Google Scholar] [CrossRef]
- Fernández-Rodríguez, R.; Zhao, L.; Bizzozero-Peroni, B.; Martínez-Vizcaíno, V.; Mesas, A.E.; Wittert, G.; Heilbronn, L.K. Are E-Health Interventions Effective in Reducing Diabetes-Related Distress and Depression in Patients with Type 2 Diabetes? A Systematic Review with Meta-Analysis. Telemed. J. E-Health Off. J. Am. Telemed. Assoc. 2024, 30, 919–939. [Google Scholar] [CrossRef]
- Jenkinson, E.; Knoop, I.; Hudson, J.L.; Moss-Morris, R.; Hackett, R.A. The Effectiveness of Cognitive Behavioural Therapy and Third-Wave Cognitive Behavioural Interventions on Diabetes-Related Distress: A Systematic Review and Meta-Analysis. Diabet. Med. J. Br. Diabet. Assoc. 2022, 39, e14948. [Google Scholar] [CrossRef]
- Ni, Y.-X.; Ma, L.; Li, J.-P. Effects of Mindfulness-Based Intervention on Glycemic Control and Psychological Outcomes in People with Diabetes: A Systematic Review and Meta-Analysis. J. Diabetes Investig. 2021, 12, 1092–1103. [Google Scholar] [CrossRef]
- Weinger, K.; De Groot, M.; Cefalu, W.T. Psychosocial Research and Care in Diabetes: Altering Lives by Understanding Attitudes. Diabetes Care 2016, 39, 2122–2125. [Google Scholar] [CrossRef]
- Peyrot, M.; Rubin, R.R.; Lauritzen, T.; Snoek, F.J.; Matthews, D.R.; Skovlund, S.E. Psychosocial Problems and Barriers to Improved Diabetes Management: Results of the Cross-National Diabetes Attitudes, Wishes and Needs (DAWN) Study. Diabet. Med. 2005, 22, 1379–1385. [Google Scholar] [CrossRef] [PubMed]
- Peyrot, M.; Burns, K.K.; Davies, M.; Forbes, A.; Hermanns, N.; Holt, R.; Kalra, S.; Nicolucci, A.; Pouwer, F.; Wens, J.; et al. Diabetes Attitudes Wishes and Needs 2 (DAWN2): A Multinational, Multi-Stakeholder Study of Psychosocial Issues in Diabetes and Person-Centred Diabetes Care. Diabetes Res. Clin. Pract. 2013, 99, 174–184. [Google Scholar] [CrossRef]
- Snoek, F.J.; Kersch, N.Y.A.; Eldrup, E.; Harman-Boehm, I.; Hermanns, N.; Kokoszka, A.; Matthews, D.R.; McGuire, B.E.; Pibernik-Okanović, M.; Singer, J.; et al. Monitoring of Individual Needs in Diabetes (MIND)-2: Follow-up Data from the Cross-National Diabetes Attitudes, Wishes, and Needs (DAWN) MIND Study. Diabetes Care 2012, 35, 2128–2132. [Google Scholar] [CrossRef]
- Hermanns, N.; Caputo, S.; Dzida, G.; Khunti, K.; Meneghini, L.F.; Snoek, F. Screening, Evaluation and Management of Depression in People with Diabetes in Primary Care. Prim. Care Diabetes 2013, 7, 1–10. [Google Scholar] [CrossRef]
- Behavioral Health Toolkit Available online: https://professional.diabetes.org/professional-development/behavioral-mental-health/behavioral-health-toolkit.
- Fagherazzi, G. Technologies Will Not Make Diabetes Disappear: How to Integrate the Concept of Diabetes Distress into Care. Diabetes Epidemiol. Manag. 2023, 11, 100140. [Google Scholar] [CrossRef]
- Vieira, P.; Kobayasi, R.; Pereira, F.; Zaia, I.M.; Sasaki, S.U. Impact of Technology Use in Type 2 Diabetes Distress: A Systematic Review. World J. Diabetes 2020, 11, 459–467. [Google Scholar] [CrossRef]
- Health Care Workforce: Key Issues, Challenges, and the Path Forward; Office of the Assistant Secretary for Planning and Evaluation, U.S. Department of Health and Human Services, 2024.
- Caitlan DeVries; Briana Mezuk; Alana Ewen; Alejandro Rodríguez-Putnam Diabetes Mental Health Initiative: The 3-D Study of Self-Management and Mental Health: Diabetes, Distress, and Disparities Available online: https://osf.io/yfz6b/.
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W. The PHQ-9: Validity of a Brief Depression Severity Measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Löwe, B. A Brief Measure for Assessing Generalized Anxiety Disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092. [Google Scholar] [CrossRef]
- Stanulewicz, N.; Mansell, P.; Cooke, D.; Hopkins, D.; Speight, J.; Blake, H. PAID-11: A Brief Measure of Diabetes Distress Validated in Adults with Type 1 Diabetes. Diabetes Res. Clin. Pract. 2019, 149, 27–38. [Google Scholar] [CrossRef]
- Jiang, Y.; Deng, W.; Zhao, M. Influence of the COVID-19 Pandemic on the Prevalence of Depression in U. S. Adults: Evidence from NHANES. Sci. Rep. 2025, 15, 3107. [Google Scholar] [CrossRef]
- Terlizzi, E.; Zablotsky, B. Symptoms of Anxiety and Depression Among Adults: United States, 2019 and 2022; National Health Statistics Reports; National Center for Health Statistics (U.S.): Hyattsville, MD, 2024. [Google Scholar]
- Polonsky, W.H.; Fisher, L.; Hessler, D.; Desai, U.; King, S.B.; Perez-Nieves, M. Toward a More Comprehensive Understanding of the Emotional Side of Type 2 Diabetes: A Re-Envisioning of the Assessment of Diabetes Distress. J. Diabetes Complications 2021, 36, 108103. [Google Scholar] [CrossRef] [PubMed]
- Zoffmann, V.; Kirkevold, M. Life Versus Disease in Difficult Diabetes Care: Conflicting Perspectives Disempower Patients and Professionals in Problem Solving. Qual. Health Res. 2005, 15, 750–765. [Google Scholar] [CrossRef] [PubMed]
- Ratanawongsa, N.; Karter, A.J.; Parker, M.M.; Lyles, C.R.; Heisler, M.; Moffet, H.H.; Adler, N.; Warton, E.M.; Schillinger, D. Communication and Medication Adherence: The Diabetes Study of Northern California. JAMA Intern. Med. 2013, 173, 210–218. [Google Scholar] [CrossRef] [PubMed]
- Cooper, Z.W.; O’Shields, J.; Ali, M.K.; Chwastiak, L.; Johnson, L.C.M. Effects of Integrated Care Approaches to Address Co-Occurring Depression and Diabetes: A Systematic Review and Meta-Analysis. Diabetes Care 2024, 47, 2291–2304. [Google Scholar] [CrossRef]
- Von Korff, M.; Katon, W.; Bush, T.; Lin, E.H.B.; Simon, G.; Saunders, K.; Ludman, E.; Walker, E.; Unutzer, J. Treatment Costs, Cost Offset, and Cost-Effectiveness of Collaborative Management of Depression: Psychosom. Med. 1998, 60, 143–149. [Google Scholar] [CrossRef]
- Simon, G.E.; Katon, W.J.; VonKorff, M.; Unützer, J.; Lin, E.H.B.; Walker, E.A.; Bush, T.; Rutter, C.; Ludman, E. Cost-Effectiveness of a Collaborative Care Program for Primary Care Patients With Persistent Depression. Am. J. Psychiatry 2001, 158, 1638–1644. [Google Scholar] [CrossRef]
- Katon, W.; Russo, J.; Lin, E.H.B.; Schmittdiel, J.; Ciechanowski, P.; Ludman, E.; Peterson, D.; Young, B.; Von Korff, M. Cost-Effectiveness of a Multicondition Collaborative Care Intervention: A Randomized Controlled Trial. Arch. Gen. Psychiatry 2012, 69, 506–514. [Google Scholar] [CrossRef]
- Davy, C.; Bleasel, J.; Liu, H.; Tchan, M.; Ponniah, S.; Brown, A. Factors Influencing the Implementation of Chronic Care Models: A Systematic Literature Review. BMC Fam. Pract. 2015, 16, 102. [Google Scholar] [CrossRef]
- Leidner, C.; Vennedey, V.; Hillen, H.; Ansmann, L.; Stock, S.; Kuntz, L.; Pfaff, H.; Hower, K.I. Implementation of Patient-Centred Care: Which System-Level Determinants Matter from a Decision Maker’s Perspective? Results from a Qualitative Interview Study across Various Health and Social Care Organisations. BMJ Open 2021, 11, e050054. [Google Scholar] [CrossRef]
- Vennedey, V.; Hower, K.I.; Hillen, H.; Ansmann, L.; Kuntz, L.; Stock, S. Patients’ Perspectives of Facilitators and Barriers to Patient-Centred Care: Insights from Qualitative Patient Interviews. BMJ Open 2020, 10, e033449. [Google Scholar] [CrossRef]
- Uchendu, C.; Blake, H. Effectiveness of Cognitive–Behavioural Therapy on Glycaemic Control and Psychological Outcomes in Adults with Diabetes Mellitus: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Diabet. Med. 2016, 34, 328–339. [Google Scholar] [CrossRef]
- Winkley, K.; Ismail, K.; Landau, S.; Eisler, I. Psychological Interventions to Improve Glycaemic Control in Patients with Type 1 Diabetes: Systematic Review and Meta-Analysis of Randomised Controlled Trials. BMJ 2006, 333, 65. [Google Scholar] [CrossRef]
- Winkley, K.; Upsher, R.; Stahl, D.; Pollard, D.; Kasera, A.; Brennan, A.; Heller, S.; Ismail, K. Psychological Interventions to Improve Self-Management of Type 1 and Type 2 Diabetes: A Systematic Review. Health Technol. Assess. 2020, 24, 1–232. [Google Scholar] [CrossRef]
- Zu, W.; Zhang, S.; Du, L.; Huang, X.; Nie, W.; Wang, L. The Effectiveness of Psychological Interventions on Diabetes Distress and Glycemic Level in Adults with Type 2 Diabetes: A Systematic Review and Meta-Analysis. BMC Psychiatry 2024, 24, 660. [Google Scholar] [CrossRef]
- Baumeister, H.; Hutter, N.; Bengel, J. Psychological and Pharmacological Interventions for Depression in Patients with Diabetes Mellitus and Depression. Cochrane Database Syst. Rev. 2012. [CrossRef]
- Azmiardi, A.; Murti, B.; Febrinasari, R.P.; Tamtomo, D.G. The Effect of Peer Support in Diabetes Self-Management Education on Glycemic Control in Patients with Type 2 Diabetes: A Systematic Review and Meta-Analysis. Epidemiol. Health 2021, 43, e2021090. [Google Scholar] [CrossRef]
- Heisler, M. Overview of Peer Support Models to Improve Diabetes Self-Management and Clinical Outcomes. Diabetes Spectr. 2007, 20, 214–221. [Google Scholar] [CrossRef]
- Hermanns, N.; Ehrmann, D.; Finke-Groene, K.; Kulzer, B. Trends in Diabetes Self-Management Education: Where Are We Coming from and Where Are We Going? A Narrative Review. Diabet. Med. J. Br. Diabet. Assoc. 2020, 37, 436–447. [Google Scholar] [CrossRef]
- Deverts, D.J.; Zupa, M.F.; Kieffer, E.C.; Gonzalez, S.; Guajardo, C.; Valbuena, F.; Piatt, G.A.; Yabes, J.G.; Lalama, C.; Heisler, M.; et al. Patient and Family Engagement in Culturally-Tailored Diabetes Self-Management Education in a Hispanic Community. Patient Educ. Couns. 2025, 134, 108669. [Google Scholar] [CrossRef]
- Rosland, A.-M.; Piette, J.D.; Trivedi, R.; Lee, A.; Stoll, S.; Youk, A.O.; Obrosky, D.S.; Deverts, D.; Kerr, E.A.; Heisler, M. Effectiveness of a Health Coaching Intervention for Patient-Family Dyads to Improve Outcomes Among Adults With Diabetes: A Randomized Clinical Trial. JAMA Netw. Open 2022, 5, e2237960. [Google Scholar] [CrossRef]
- Saint, K.; Heisler, M. Experiences of Participants Who Then Become Coaches in a Peer Coach Diabetes Self-Management Program: Lessons for Future Programs. Chronic Illn. 2021, 19, 265–275. [Google Scholar] [CrossRef]
- Verma, I.; Gopaldasani, V.; Jain, V.; Chauhan, S.; Chawla, R.; Verma, P.K.; Hosseinzadeh, H. The Impact of Peer Coach-Led Type 2 Diabetes Mellitus Interventions on Glycaemic Control and Self-Management Outcomes: A Systematic Review and Meta-Analysis. Prim. Care Diabetes 2022, 16, 719–735. [Google Scholar] [CrossRef]
- Fleming, J.; Nguyen, K.; Winston, J.; Allen, J.O.; Smith, J.; Thornton, W.; Mejia Ruiz, M.J.; Mezuk, B. Promoting Sustained Diabetes Management: Identifying Challenges and Opportunities in Developing an Alumni Peer Support Component of the YMCA Diabetes Control Program. Patient Educ. Couns. 2022, 105, 1322–1328. [Google Scholar] [CrossRef]
- Atac, O.; Heier, K.R.; Moga, D.; Fowlkes, J.; Sohn, M.-W.; Kruse-Diehr, A.J.; Waters, T.M.; Lacy, M.E. Demographic Variation in Continuous Glucose Monitoring Utilisation among Patients with Type 1 Diabetes from a US Regional Academic Medical Centre: A Retrospective Cohort Study, 2018-2021. BMJ Open 2025, 15, e088785. [Google Scholar] [CrossRef]
- Kostiuk, M.; Moore, S.L.; Kramer, E.S.; Gilens, J.F.; Sarwal, A.; Saxon, D.; Thomas, J.F.; Oser, T.K. Assessment and Intervention for Diabetes Distress in Primary Care Using Clinical and Technological Interventions: Protocol for a Single-Arm Pilot Trial. JMIR Res. Protoc. 2025, 14, e62916. [Google Scholar] [CrossRef]
- Roth, M.; Bodenhofer, J.; Fischill-Neudeck, M.; Roth, C.; Domhardt, M.; Emsenhuber, G.; Grabner, B.; Oostingh, G.J.; Schuster, A. Comparison of the Efficacy of Type 2 Diabetes Group Training Courses With and Without the Integration of mHealth Support in a Controlled Trial Setting: Results of a Comparative Pilot Study. Diabetes Spectr. 2024, 38, 58–67. [Google Scholar] [CrossRef]
- Advisors Available online: https://diabetes.med.umich.edu/about/advisors#patient-family-advisory-council-pfac.
- Person-Centered Care Available online:. Available online: https://www.cms.gov/priorities/innovation/key-concepts/person-centered-care (accessed on 24 March 2025).
- van der Feltz-Cornelis, C.M.; Nuyen, J.; Stoop, C.; Chan, J.; Jacobson, A.M.; Katon, W.; Snoek, F.; Sartorius, N. Effect of Interventions for Major Depressive Disorder and Significant Depressive Symptoms in Patients with Diabetes Mellitus: A Systematic Review and Meta-Analysis. Gen. Hosp. Psychiatry 2010, 32, 380–395. [Google Scholar] [CrossRef]
- Fisher, E.B.; Chan, J.C.N.; Nan, H.; Sartorius, N.; Oldenburg, B. Co-Occurrence of Diabetes and Depression: Conceptual Considerations for an Emerging Global Health Challenge. J. Affect. Disord. 2012, 142, S56–S66. [Google Scholar] [CrossRef]
- Greenberg, P.E.; Fournier, A.-A.; Sisitsky, T.; Simes, M.; Berman, R.; Koenigsberg, S.H.; Kessler, R.C. The Economic Burden of Adults with Major Depressive Disorder in the United States (2010 and 2018). PharmacoEconomics 2021, 39, 653–665. [Google Scholar] [CrossRef]
- Kavelaars, R.; Ward, H. ; Mackie, deMauri S. ; Modi, K.M.; Mohandas, A. The Burden of Anxiety among a Nationally Representative US Adult Population. J. Affect. Disord. 2023, 336, 81–91. [Google Scholar] [CrossRef]
Figure 1.
Prevalence values for adults with diabetes adjusted for age, gender, race/ethnicity, income, and education for clinically-significant (a) Depression; (b) Anxiety; (c) Diabetes-related distress.
Figure 1.
Prevalence values for adults with diabetes adjusted for age, gender, race/ethnicity, income, and education for clinically-significant (a) Depression; (b) Anxiety; (c) Diabetes-related distress.
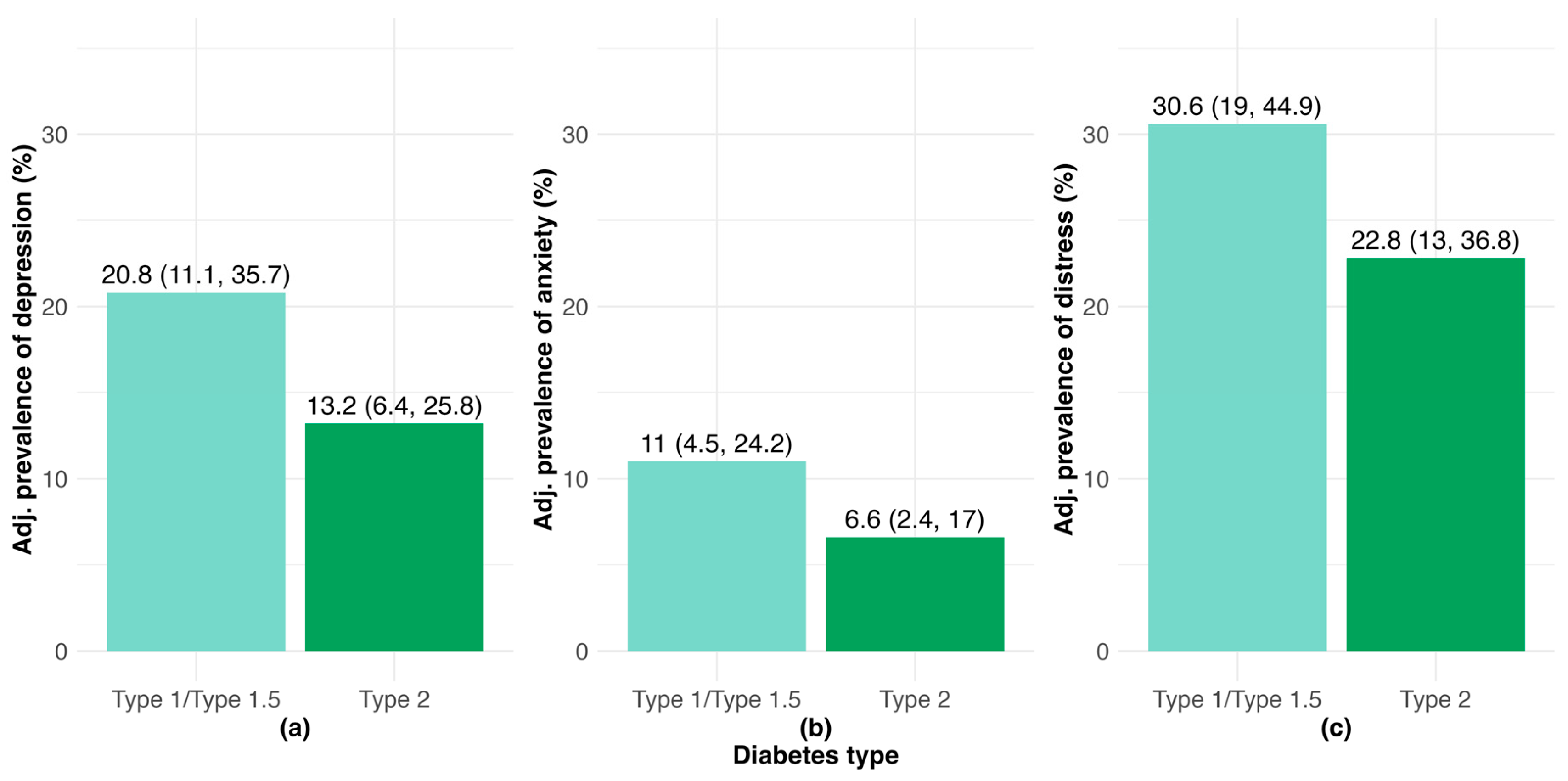
Figure 2.
Prevalence values by HbA1c values for adults with diabetes adjusted for age, gender, race/ethnicity, income, and education for clinically-significant: (a) Depression; (b) Anxiety; (c) Diabetes-related distress.
Figure 2.
Prevalence values by HbA1c values for adults with diabetes adjusted for age, gender, race/ethnicity, income, and education for clinically-significant: (a) Depression; (b) Anxiety; (c) Diabetes-related distress.
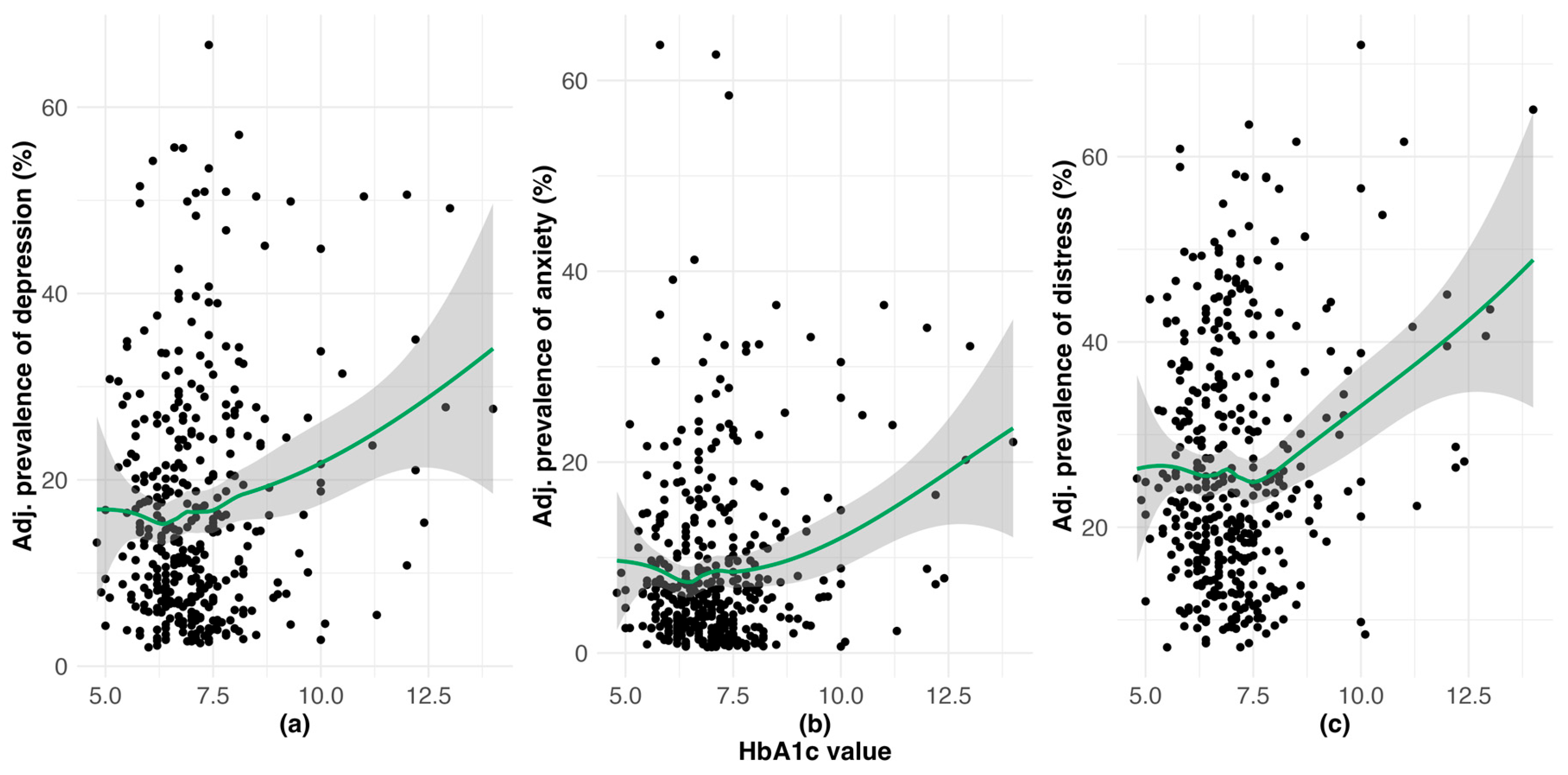
Figure 3.
Reasons for why PWD could not access mental health services when needed (responses are not mutually-exclusive, n=133).
Figure 3.
Reasons for why PWD could not access mental health services when needed (responses are not mutually-exclusive, n=133).
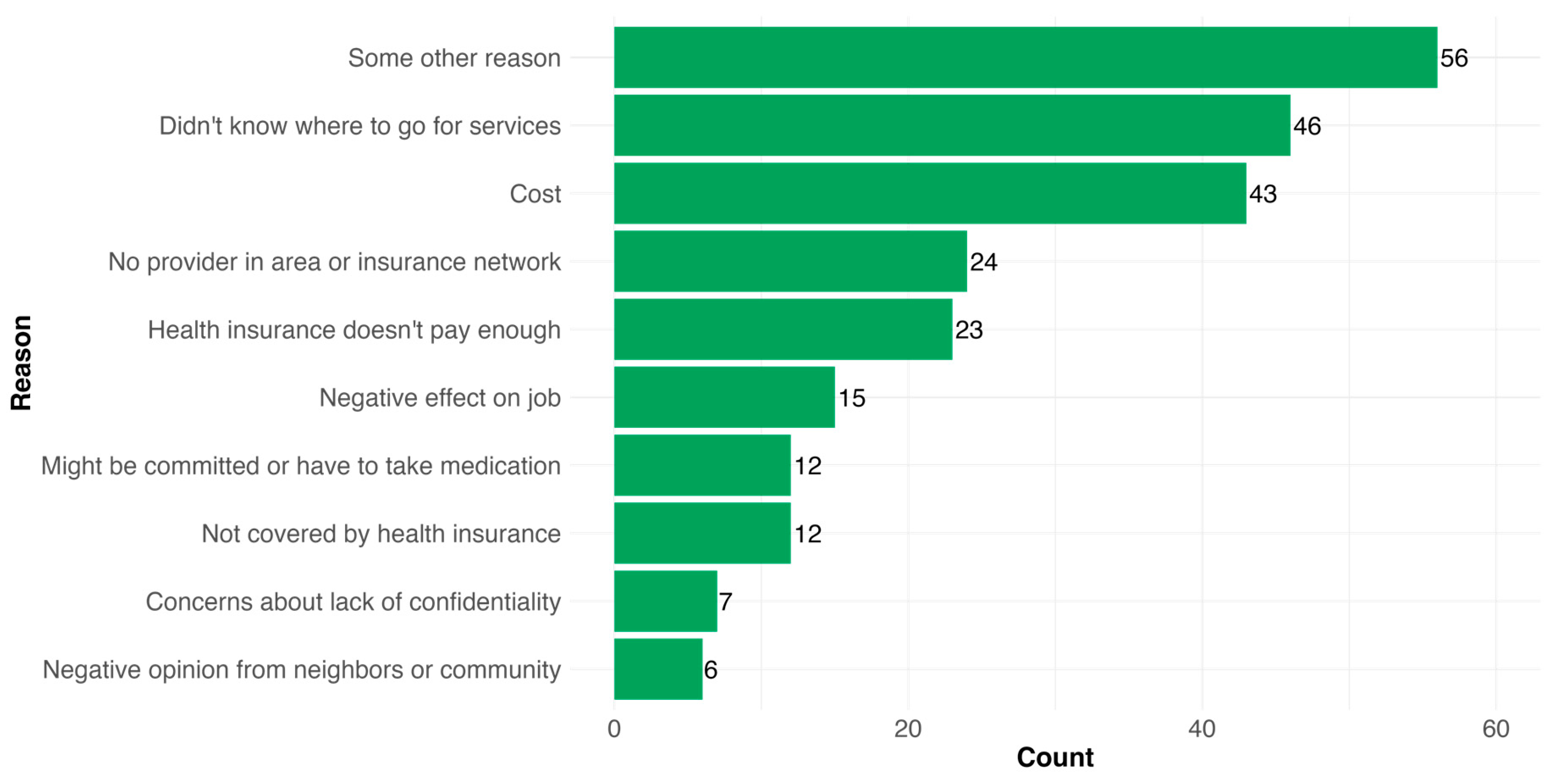

Table 1.
Characteristics of 3D Study phase 1 participants by anxiety and depression status.
| Anxiety only (N=13) |
Depression and anxiety (N=33) |
Depression only (N=50) |
Neither (N=433) |
|
|---|---|---|---|---|
| PHQ-9 score | ||||
| Mean (SD) | 9.25 (4.43) | 20.1 (2.69) | 17.8 (2.52) | 5.43 (4.12) |
| Missing | 9 (69.2%) | 0 (0%) | 0 (0%) | 24 (5.5%) |
| PAID-11 score | ||||
| Mean (SD) | 22.6 (10.8) | 25.6 (10.1) | 21.1 (9.24) | 9.33 (8.16) |
| Missing | 0 (0%) | 0 (0%) | 1 (2.0%) | 9 (2.1%) |
| GAD-7 score | ||||
| Mean (SD) | 18.0 (2.00) | 17.7 (2.05) | 9.54 (3.28) | 3.46 (3.56) |
| Missing | 0 (0%) | 0 (0%) | 4 (8.0%) | 10 (2.3%) |
| Diabetes type | ||||
| Type 1/Type 1.5 | 8 (61.5%) | 17 (51.5%) | 31 (62.0%) | 216 (49.9%) |
| Type 2 | 5 (38.5%) | 15 (45.5%) | 18 (36.0%) | 192 (44.3%) |
| Gestational (past or current) | 0 (0%) | 1 (3.0%) | 0 (0%) | 21 (4.8%) |
| Diabetes - Type Unknown | 0 (0%) | 0 (0%) | 1 (2.0%) | 4 (0.9%) |
| Latest HbA1c value | ||||
| Mean (SD) | 7.59 (1.36) | 7.93 (1.72) | 7.40 (1.69) | 6.96 (1.27) |
| Missing | 1 (7.7%) | 9 (27.3%) | 3 (6.0%) | 57 (13.2%) |
| Current age | ||||
| Mean (SD) | 46.8 (15.8) | 41.0 (13.5) | 49.2 (14.5) | 55.9 (17.0) |
| Gender | ||||
| Man | 3 (23.1%) | 5 (15.2%) | 12 (24.0%) | 170 (39.3%) |
| Woman | 8 (61.5%) | 26 (78.8%) | 34 (68.0%) | 239 (55.2%) |
| Gender non-conforming | 0 (0%) | 2 (6.1%) | 0 (0%) | 2 (0.5%) |
| Missing | 2 (15.4%) | 0 (0%) | 4 (8.0%) | 22 (5.1%) |
| Race/ethnicity | ||||
| Native American or Alaskan Native | 0 (0%) | 1 (3.0%) | 0 (0%) | 3 (0.7%) |
| Asian | 0 (0%) | 0 (0%) | 0 (0%) | 15 (3.5%) |
| Black or African American | 1 (7.7%) | 3 (9.1%) | 3 (6.0%) | 41 (9.5%) |
| Latino | 0 (0%) | 1 (3.0%) | 0 (0%) | 8 (1.8%) |
| White | 8 (61.5%) | 26 (78.8%) | 41 (82.0%) | 326 (75.3%) |
| Prefer not to Disclose | 4 (30.8%) | 0 (0%) | 5 (10.0%) | 32 (7.4%) |
| More than one race | 0 (0%) | 2 (6.1%) | 1 (2.0%) | 8 (1.8%) |
| Highest grade of school | ||||
| High school diploma or below | 2 (15.4%) | 9 (27.3%) | 9 (18.0%) | 80 (18.5%) |
| Associate’s degree or certificate program | 5 (38.5%) | 8 (24.2%) | 11 (22.0%) | 63 (14.5%) |
| Bachelor’s degree | 3 (23.1%) | 7 (21.2%) | 17 (34.0%) | 131 (30.3%) |
| Advanced degree | 3 (23.1%) | 9 (27.3%) | 13 (26.0%) | 159 (36.7%) |
| Annual household income | ||||
| Less than $50,000 | 7 (53.8%) | 18 (54.5%) | 24 (48.0%) | 113 (26.1%) |
| $50,000-$99,999 | 3 (23.1%) | 5 (15.2%) | 12 (24.0%) | 150 (34.6%) |
| $100,000-$149,999 | 2 (15.4%) | 5 (15.2%) | 7 (14.0%) | 73 (16.9%) |
| $150,000 or more | 1 (7.7%) | 5 (15.2%) | 7 (14.0%) | 87 (20.1%) |
| Missing | 0 (0%) | 0 (0%) | 0 (0%) | 10 (2.3%) |
| Behavioral or mental health treatment in past 12 months | ||||
| Yes | 9 (69.2%) | 24 (72.7%) | 35 (70.0%) | 132 (30.5%) |
| No | 4 (30.8%) | 9 (27.3%) | 15 (30.0%) | 289 (66.7%) |
| Missing | 0 (0%) | 0 (0%) | 0 (0%) | 12 (2.8%) |
| Take prescription medication for mental/emotional condition in the past 12 months | ||||
| Yes | 7 (53.8%) | 25 (75.8%) | 34 (68.0%) | 126 (29.1%) |
| No | 6 (46.2%) | 7 (21.2%) | 15 (30.0%) | 294 (67.9%) |
| Missing | 0 (0%) | 1 (3.0%) | 1 (2.0%) | 13 (3.0%) |
| Any mental health treatment or prescription medication use for mental health condition in last 12 months | ||||
| Yes | 9 (69.2%) | 26 (78.8%) | 38 (76.0%) | 165 (38.1%) |
| No | 4 (30.8%) | 7 (21.2%) | 12 (24.0%) | 266 (61.4%) |
| Missing | 0 (0%) | 0 (0%) | 0 (0%) | 2 (0.5%) |
n = 44 had missing PHQ-9 and GAD-7 score. Depression: PHQ-9 ≥15 (Severe or moderately severe). Anxiety: GAD-7 ≥15 (Severe).
Table 2.
Predictors of receiving any mental health treatment in the prior 12 months among adults with diabetes and clinically significant depression, anxiety or DRD (n = 153).
Table 2.
Predictors of receiving any mental health treatment in the prior 12 months among adults with diabetes and clinically significant depression, anxiety or DRD (n = 153).
| Characteristic | N | OR | 95% CI | p-value |
|---|---|---|---|---|
| (Intercept) | 153 | 1.80 | 0.29, 11.7 | 0.5 |
| Diabetes type | 153 | |||
| Type 2 | — | — | ||
| Type 1/Type 1.5 | 1.24 | 0.53, 2.90 | 0.6 | |
| Current age | 153 | 1.00 | 0.97, 1.03 | >0.9 |
| Annual household income | 153 | |||
| Less than $50,000 | — | — | ||
| $50,000-$99,999 | 0.57 | 0.23, 1.39 | 0.2 | |
| $100,000-$149,999 | 0.40 | 0.14, 1.17 | 0.10 | |
| $150,000 or more | 1.02 | 0.30, 3.87 | >0.9 | |
| Gender | 153 | |||
| Man | — | — | ||
| Woman | 2.43 | 1.11, 5.40 | 0.027 | |
| Highest grade of school | 153 | |||
| High school diploma or below | — | — | ||
| Associate’s degree or certificate program | 0.61 | 0.20, 1.79 | 0.4 | |
| Bachelor’s degree | 0.73 | 0.26, 2.03 | 0.6 | |
| Advanced degree | 1.09 | 0.36, 3.26 | 0.9 | |
| Race/ethnicity | 153 | |||
| White | — | — | ||
| Black or African American | 0.24 | 0.07, 0.77 | 0.018 | |
| Another race | 1.28 | 0.37, 5.19 | 0.7 |
Abbreviations: CI = Confidence Interval, OR = Odds Ratio.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



