
Submitted:
19 March 2025
Posted:
20 March 2025
You are already at the latest version
Abstract
Individuals diagnosed with substance use disorders (SUD) exhibit notable deficits in executive function (EFs). In the context of substance abuse, the pro-inflammatory cytokine interleukin-6 (IL-6) appears to contribute to these cognitive impairments significantly. Background/Objectives: However, the specific neuropsychological parameters most affected by executive dysfunction remain poorly understood. Methods: In this study, sixteen patients diagnosed with SUD in the withdrawal phase were compared to twenty age-matched control subjects to ascertain which aspects of EFs were most adversely impacted. Plasma levels of IL-6 were quantified using enzyme-linked immunosorbent assay (ELISA). Data were analyzed using the Confidence Interval-Based Estimation of Relevance (CIBER) model to determine the most sensitive executive performance indicators. Results: Findings from the CIBER analysis revealed that the Wisconsin Card Sorting Test yielded the most pronounced cognitive discrepancies between males with and without SUD diagnoses. Elevated levels of IL-6 and associated executive dysfunction were observed to persist in males with SUD throughout the withdrawal phase. Conclusions: Notably, cognitive flexibility emerged as the most sensitive parameter indicative of executive dysfunction, suggesting its potential utility in tailoring clinical interventions for SUD patients during this critical recovery period.
Keywords:
CIBER
; executive dysfunction
; biomarker
; polydrug consumers
; addiction
1. Introduction
The Diagnostic and Statistical Manual of Mental Disorders, Fifth Version (DSM-5) [1], defines substance use disorders (SUD) as cycles of consumption and relapses leading to pervasive substance abuse [2,3]. This cycle encompasses three distinct phases: the binge/intoxication phase, the withdrawal/negative affect phase, and the preoccupation/anticipation (craving) phase [4]. Individuals diagnosed with SUD commonly exhibit profound neuropsychological deficits, specifically in executive functions (EFs) [5]. EFs are critical cognitive processes facilitating independent, goal-oriented, self-directed, and adaptive behavior [6,7]. Miyake et al. conceptualize EFs as comprising three core components: working memory, inhibition, and cognitive flexibility [8]. In patients with SUD, dysfunctions in these executive domains partially account for maladaptive consumption behaviors. They are linked to poor treatment adherence, high dropout rates [9], diminished motivation for change [10], and limited self-awareness [11], which are associated with higher rates of relapses that hinder rehabilitation [12].
A potential mechanism underlying executive dysfunctions in drug consumers is the inflammatory response mediated by activated microglia cells [13,14]. Reactive microglia secrete pro-inflammatory cytokines such as interleukin- 1 (IL-1), IL-6, and tumor necrosis factor-alpha (TNF-α) [15,16] These pro-inflammatory cytokines can interact with monoaminergic terminals [17], potentially resulting in reduced activation of the ventral striatum and impaired cortico-striatal connectivity [18]. In patients with SUD, elevated levels of IL-6 are correlated with reduced connectivity within the cortico-striatal-limbic regions [19], which supports the hypothesis that neuroinflammation contributes to hypoactivity in dopaminergic pathways and, consequently, executive function impairments through diminished activity in the frontal lobes [20,21,22].
Plasma levels of IL-6 positively correlate with increases in adrenocorticotropic hormone (ACTH), a key stress response regulator [23,24]. This relationship suggests a close association between stress and IL-6 levels [23]. Notably, the interaction between stress and IL-6 appears to be influenced by sex differences. Under physiological conditions, adult women exhibit elevated IL-6 levels in response to stressors compared to their male counterparts [25]. In females with a history of amphetamine addiction, increased ACTH levels, potentially driven by estrogenic modulation, coincide with elevated IL-6 levels and corresponding impairments in cognitive flexibility [26,27]. Interestingly, research suggests that females may engage more rapidly in drug-seeking behaviors and cravings [28]. In contrast, males tend to experience more frequent issues related to substance intoxication and exhibit poorer rehabilitation outcomes [29]. Therefore, it is crucial to investigate whether males with SUD also show alterations in IL-6 levels and to explore the implications of these fluctuations on executive function performance during periods of abstinence.
The Confidence Interval-Based Estimation of Relevance (CIBER) is an innovative statistical framework introduced by Crutzen et al. [30] that facilitates the transformation of raw data into a visual representation, enabling the comparison of correlation coefficients, means, and confidence intervals. In this visualization, data are depicted as diamond shapes, which assist in evaluating effect sizes within meta-analyses employing univariate distributions [31]. In the present study, we applied this model to generate a comprehensive map illustrating multiple statistical comparisons among cognitive parameters encompassing working memory, inhibition, and cognitive flexibility performance in polydrug male consumers who have maintained 5.5 months of abstinence.
2. Materials and Methods
2.1. Participants and Recruitment
A cross-sectional, non-experimental observational study was conducted. Thirty-six male voluntary participants with an average age of 24 years were included and distributed in two groups. The first group consisted of 16 patients with SUD diagnosis who received a recent intervention scheme with a multimodal treatment for drug abuse disorders in the foundation “México Me Necesita” (Guadalajara City, México). The second group was assembled with 20 healthy subjects paired by age, education, and no story of drug consumption. The inclusion and exclusion criteria of SUD participants were based on individual case records. Inclusion criteria were: 1) male patients (18-45 years old) with a previous diagnosis of SUD and who voluntarily want to receive a resident scheme of rehabilitation in the foundation “México Me Necesita” and 2) At least 12 years of schooling. Exclusion criteria were: 1) a previous history of neurosurgical procedures, previous clinical history for head trauma, psychiatric disorders, and any visual condition that was not corrected by glasses, and voluntary withdrawal from the study. In the control group, we applied a clinical interview to identify past or present problematic drug behavior. The subjects in this group reported a social consumption of alcohol, such as a couple of cups of wine or beer cans at parties, tobacco (one or two cigars per week), and denied consumption of any other licit or illicit drug. They also denied the presence of problems in their social, familiar, and academic/workplace environments related to alcohol or smoke consumption. In this group, we request to halt any consumption of alcohol or tobacco for at least one week before neuropsychological evaluation and blood testing. All the participants were informed about the specific aims or purposes of the study and were asked to voluntarily fill out and sign a consent letter. This protocol and its procedures were approved and supervised by the Ethical Committee (207/2021) of the Instituto Jaliscience de Salud Mental (SALME), Mexico, following the federal regulations and guidelines stipulated in the Mexican Official Norm (NOM-028-SSA2-1999 and NOM-012-SSA3-2012) and conducted following Declaration of Helsinki.
2.2. IL-6 Determination
To determine the levels of IL-6, peripheral blood of all participants was obtained between 8:00 and 9:00 a.m. Plasma was then obtained by centrifugation and stored at -80 C until analysis. IL-6 plasma levels were determined with the kit Enzyme Immunoassay for IL-6 (Abcam, ab46042), following the step-by-step protocol provided by the manufacturer. All samples were analyzed by duplicate. Optical density was determined with a Multiskan FC model plate reader (Thermo Scientific Cat. 51119100) at 450nm. The concentrations of each enzyme were expressed in pg/ml, and final concentrations were obtained by interpolation with the standard curve.
2.3. Neuropsychological Evaluation
The neuropsychological assessment was performed with the PsyToolkit stimulator [32] visualized in a Chrome browser version 90.0.4430.212. To identify changes in Working memory (WM) tasks, the N-Back paradigm was set at level 2 of difficulty, and a variant with 15 letters from “A” to “T” was used in a total of 50 random trials on a black background screen. To confirm that the participant adequately understood the task, we employed two phases, one of the 1-Back and 2-Back training trials and the actual test, which starts directly in the 2-Back difficulty. The stimuli were presented at a rate of 250 milliseconds with a 500-millisecond response limit. Feedback was provided through two colored strips above and below each stimulus: green for the correct answers and red for the wrong ones. In addition, the direct and inverse.
We used the classical rules and settings of the Go/No-Go paradigm to evaluate inhibitory control and attention. The participant must emit a response according to the stimulus presented; the green color indicates that they must press the button, while the red color indicates that they must not press it. Stimuli were displayed at a rate of 500 milliseconds with a maximum response delay of 2000 milliseconds. Two errors were quantified: pressing the button when a red “No-Go” stimulus appears, which indicates a failure to inhibit the response (commission error), and not pressing the button when a green “Go” stimulus appears, which indicates a failure to execute the required response (omission error).
Finally, we applied the Wisconsin Card Sorting Test (WCST) to identify cognitive flexibility. The participants had to sort cards under three possible options: shape, number, or color. A card that can be grouped with the three possibilities was presented every 250 milliseconds; the subject had 5000 milliseconds to match it with the possible options; if there was an error in the answer, auditory feedback with the word “no” was provided. The elements considered during the evaluation are perseverative and non-perseverative errors, correct answers, and response times.
2.4. Data Analysis
We used the Mann-Whitney U test to verify the effectiveness of the matching process for the sociodemographic data of age and schooling. The analysis did not find significant differences in age (U = 108.5, δ = 0.48, p = 0.15) and schooling (U = 186.5, δ = 0.27, p = 0.29) between the groups, which supports that both groups were properly matched. We also calculated the effect size for our findings, providing context for the observed differences, which helped to establish the practical significance of our results alongside p-values. To ensure a robust experimental design for detecting group differences, we established the statistical power for bidirectional independent samples: β = 0.80 and α = 0.05, with group sizes of n1 = 16 and n2 = 20. This configuration resulted in a minimum effect size (Cohen’s d) of 0.96 (r = 0.43) for Type-II error and 0.70 (r = 0.33) for Type-I error. The Shapiro-Wilk test was employed to assess the sample distribution, which indicated a non-parametric distribution. Hence, the U Mann-Whitney was calculated to determine differences between groups. We apply the Spearman correlation to identify the association between IL-6 levels and cognitive parameters. The CIBER method generates a visual map with two panels. In the left panel, the diamonds represent the 99.99% confidence interval (CI) for each cognitive parameter, and the diamonds’ color represents the groups. In the right panel, the diamonds represent the mean of each cognitive item, and the more intense the color of the diamond, the greater the meaning of each item (strength association), whereas the less intense the color of the diamond, the lower the item’s relevance. Thus, the redder the diamond, the stronger the negative association, whereas the greener the diamond, the stronger the positive association. The lines in the right panel are graduated according to the standard deviation (SD) from -2 to +2 with 95% CIs. The quantitative analysis was expressed as 95% CIs (Low|Up).
3. Results
3.1. The plasma Levels of IL-6 Are Increased in Polydrug Male Consumers During Abstinence
The participants in the SUD group were polydrug consumers of methamphetamines, tobacco, and alcohol. In this group, 31.58% also had a consumption of cannabinoids, 10.53% inhalants, and 5.26% benzodiazepines (Table 1), with a range of abstinence time between 100 – 324 days. We quantified the plasmatic IL-6 and found that the SUD group had high levels of this cytokine, 13.16 pg/ml (IQR= 12.07 – 14; n = 16 subjects) when compared to the control group 10.04 pg/ml (IQR= 8.64-14.10; n= 20 subjects) and these differences were statistically significant (U = 93, p = 0.033) (Figure 1).
3.2. Executive Dysfunction Persists in Polydrug Males During Abstinence
We observed a worsening EFs’ performance in the SUD group (Table 2). In the evaluation of working memory performance with the NBra cognitive parameter, the SUD group had the worst performance (80.00 correct answers, IQR = 74.67 - 88.00; n= 16) in comparison to the control group (88.66 correct answers, IQR= 82.33 - 92.00; n= 20. U = 86, p= 0.019). The SUD group also shows more reaction times (NBrt= 25.96, IQR= 24.17-26.66; n= 16 subjects) vs the control group (NBrt=25.00, IQR= 22.36-25.59; n= 20 subjects. U = 94, p= 0.037). This evidence indicates that SUD patients present poor working memory performance and require more time to monitor and update the information.
In the Go/No-Go task, we measured the inhibitory capacity through the results of the correct answers in the Go condition and found that the SUD group present a poor inhibitory capacity (Gora= 100, IQR = 97.50 – 100; n = 16 subjects) when compared to the control group who present a median of 100 in this score (IQR = 100 - 100; n = 20 subjects. U = 110, p = 0.009). Regarding the reaction time, the SUD group responded quicker (GOrt = 37.56, IQR = 36.50 - 44.03; n = 16 subjects) than the control subjects (GOrt = 43.91, IQR= 38.39 - 48.13; n = 20 subjects. U = 88, p= 0.023), whereas commission in the No-Go condition, the control group obtained higher correct answers (NoGora = 100, IQR= 97.50 – 100; n = 20 subjects) as compared to the SUD group (NoGora = 90.00, IQR= 80.00 - 90.00; n = 16 subjects. U = 58.5, p = 0.001). Furthermore, the reaction time in the SUD group was longer (NoGort=18.27, IQR = 16.49 -18.31; n = 16 subjects) than in controls (NoGort = 20, IQR = 19.59 - 20.00; n = 20 subjects. U = 60, p = 0.001). Altogether, these results indicate that the ability to inhibit responses and verify the type of response is significantly deficient in the SUD group.
We assessed cognitive flexibility with the WCST task and found that the SUD group had a significantly worse performance in correct answers (WCSTra = 65.83, IQR= 47.08-73.75; n= 16 subjects) as compared to the control group (WCSTra = 81.67, IQR = 78.33 - 83.33; n = subjects. U = 35, p= 0.001). We do not find significant differences in reaction times between the SUD (WCSTrt= 20.59, IQR= 15.36 - 24.60; n= 16 subjects) and the control group (WCSTrt= 15.82, IQR= 13.65 - 17.96; n= 20 subjects. U = 0.101, p= 0.063). In perseverative errors, we found statistical significance (U = 53.5, p = 0.010) between the SUD (WCSTpe = 20.00, IQR = 15.00 - 27.08; n = 16 subjects) and control group (WCSTpe= 11.67, IQR = 10-15; n = 20 subjects), which mean that SUD group had more significant difficulties in changing its responses when faced with different forms of classifications. In contrast, the non-perseverative errors of SUD subjects (WCSTnpe = 10.00, IQR= 6.25-19.17; n = 16 subjects) were also higher than in controls (WCSTnpe = 6.67, IQR= 5.00 - 8.75; n = 20 subjects), but these differences were in the limit of statistical significance (U = 99, p= 0.053). Altogether, these data indicate that individuals with SUD have significantly impaired cognitive flexibility compared to controls, shown by fewer correct answers and more perseverative errors in the WCST. While reaction times did not differ significantly, higher perseverative errors indicate difficulty adapting to new rules. Increases in non-perseverative errors also suggest broader cognitive flexibility challenges.
3.3. Correlations Between Cognitive Task Performance and Reaction Time
To identify the strength of the association between correct answers and reaction time across all cognitive tasks, we conducted a correlation analysis via the Spearman test (Table 3) and found a moderate negative association between NBra and NBrt (Spearman’s rho of -0.538, p=0.001). This indicates that participants who perform more efficiently in terms of correct responses also tend to have faster reaction times. This pattern may imply that the ability to maintain information actively in working memory is related to faster processing of that information.
In the Go/No-Go task, a significant moderate positive correlation was found between Gora and NoGora (Spearman’s rho = 0.476, p = 0.003), which suggests that participants who perform well in the “go” section also tend to perform well in the “no-go” section. This could reflect that good performance in one executive function (such as controlled impulsivity in the “go” section) is associated with adequate inhibitory control in the other (inhibiting responses in the “no-go” section). The association between the parameters Gora and Gort indicates a low relationship (Spearman’s rho = 0.151, p = 0.38), which suggests that accuracy and speed in this task may be functioning relatively independently. Specifically, a participant may be accurate in their responses but take more time to do so, or they may respond quickly but make more errors, suggesting that response control and speed are not strongly linked or reflect different cognitive processing strategies. The analysis of Gora and NoGort results in a moderate positive relationship between these two variables (Spearman’s rho = 0.515, p = 0.001), which could suggest an interaction between response control and the speed of inhibition. Specifically, participants who are more accurate in the “go” section seem to take more time to inhibit their responses in the “no-go” section.
In the Wisconsin Card Sorting Test, several strong negative correlations were identified. WCSTra correlated negatively with WCSTrt, showing a moderate correlation (Spearman’s rho = -0.564, p = 0.001). This indicates that those with faster reaction times tend to perform better on the task, reflecting greater cognitive efficiency and quicker mental flexibility, which are traits of individuals with stronger executive functions. The high correlation between WCSTra and WCSTpe (Spearman’s rho = -0.790, p = 0.001) strongly suggests that participants who respond correctly on the test make fewer perseverative errors. Since perseverative errors are a key measure of cognitive flexibility, a higher number of correct responses is linked to a better ability to shift strategies or adapt to new rules without relying on previously incorrect rules. This relationship implies that those with stronger executive control and greater cognitive flexibility (fewer perseverative errors) are more effective in the task. Regarding the association between WCSTra and WCSTnpe (Spearman’s rho = -0.760, p = 0.001), the data suggests that participants who provide correct answers also make fewer non-perseverative errors. These results strongly indicate that those performing better on the task are also more proficient at adapting to rule changes without making errors related to the incorrect application of new strategies.
There was also a significant positive and moderate correlation between WCSTrt and WCSTpe (Spearman’s rho = 0.536, p = 0.001), suggesting that slower response times may be linked to difficulties in adapting to new rules or cognitive flexibility. Alternatively, longer reaction times might indicate doubt when shifting strategies, leading to persistent incorrect responses or an inability to adapt appropriately to rule changes. Regarding the relationship between WCSTrt and WCSTnpe (Spearman’s rho = 0.533, p = 0.001), it reflects that individuals who have longer reaction times tend to make more non-perseverative errors. These data suggest a difficulty in applying new rules, possibly due to slower decision-making or an inability to inhibit incorrect responses.
3.4. Plasma IL-6 Levels Correlate to Working Memory Performance in Adult Males
To identify if IL-6 levels are associated with working memory, inhibition, and cognitive flexibility performance. In the analysis of all groups, the plasmatic IL-6 levels present a negative correlation with the number of correct answers (NBra: r = - 0.397; p = 0.017) and a positive correlation with reaction time (NBrt: r = 0.347; p = 0.038) in the N-Back test whereas in the Go/No-Go task, the cytokine levels show a negative correlation with the number of correct answers in the Go condition (r = - 0.321; p = 0.05). The other cognitive parameters evaluated did not show statistical differences (Table 2). When we compared the association between IL-6 levels with FE performance per group, we found that in the control group, the plasma IL-6 levels only presented a positive correlation with the reaction time in the N-Back test (NBrt: r = 0.572; p=0.008), whereas, in the SUD group, the plasmatic IL-6 levels did not show statistical significance, except by a limitrophe statistical significance in the number of perseverative errors (WCSTpe: r = 0.472; p = 0.065).
3.5. Inhibition and Cognitive Flexibility Are the Most Sensitive Cognitive Parameters That Differentiate EFs’ Performance Between the Groups
We applied the CIBER method to obtain a map and analyze the distance and data distribution of different cognitive parameters that comprise working memory, inhibition, and cognitive flexibility performance. In the left panel, we described the cognitive parameters as follows. For working memory, NBack correct answer (NBra) and NBack reaction time (NBrt). For inhibition, Go-no-go correct answer Go (Gora), Go-no-go right answer no-go (NoGora), Go-no-go reaction time Go (Gort), Go-no-go reaction time no-go (NoGort). For cognitive flexibility, WCST correct answer (WCSTra), WCST reaction time (WCSTrt), WCST perseverative error (WCSTpe), and WCST non-perseverative error (WCSTnpe) (Figure 2).
Visually, the left panel represents the distance in performance of each cognitive parameter according to the group. In this panel, diamond shapes represent the 99.99% CI, and diamond colors indicate the group. The quantitative analysis was carried out by identifying the CI (Low|Up) and the overlap index to obtain mean differences between groups of each cognitive parameter. For working memory, NBra 6.37 (1.47|11.26), NBrt 1.33 (0.06|2.60). For inhibition, Gora 0.78 (0.24|1.32), NoGora 11.75 (4.48|19.02), Gort 6.01 (.92|11.08), and NoGort: 2.01 (0.75|3.26). For cognitive flexibility, WCSTra of 19.41 (11.26|27.6), WCSTrt 5.15 (1.3|9), WCSTpe 8.3 (3.51|13.06), and WCSTpe 8.3 (1.43|15.3). According to the analysis of the data in the left panel, we can observe that NoGora for inhibition, WCSTra and WCSTpe for cognitive flexibility are the most sensitive parameters for identifying cognitive impairment in SUD patients during the withdrawal phase. This sensitivity suggests these measures could be particularly effective in neuropsychological assessments and interventions for these individuals (Figure 2).
The analysis in the right panel (Figure 2) shows the delta (δ) values representing the mean differences between SUD and control groups across cognitive parameters, with associated 95% confidence intervals (95% CI). In this right panel, the lines are graduated according to 95% CIs from -2 to +2 and indicate the direction of the association of each cognitive parameter. Therefore, the redder and greener the diamond, the stronger the directionality of the association, whereas the grayer (duller) the diamond, the weaker the association. Thus, NoGora (δ = 1.101 (0.3463|1.8337), WCSTra (δ= 1.623 (0.7759|2.4428), and WCSTpe (δ = 0.822 (0.106|1.5196) were the cognitive parameters with higher distance data distribution. Our data indicated that NBra δ = 0.886 (0.1621|1.5911) and NBrt a δ = 0.716 (0.0128|1.4033) suggested moderate differences in working memory performance, indicating that individuals in the SUD group typically perform worse than controls. In the evaluation of inhibition, we obtained the following data Gora δ=0.983 (0.2453|1.6992), NoGora δ = 1.101 (0.3463|1.8337); Gort δ = 0.805 (0.0912|1.5009) and NoGort δ = 1.089 (0.3359|1.8197). These findings indicate significant differences in inhibition performance, especially in the “no-go” task, which reflects challenges in impulse control of SUD individuals. When analyzing cognitive flexibility, we found a marked impact on this ability in the SUD group when compared to controls, WCSTra δ= 1.623 (0.7759|2.4428) and WCSTrt a δ= 0.914 (0.1857|1.6216), which was confirmed with WCSTpe a δ = 1.184(0.4158|1.9282) and WCSTpe a δ = 0.822 (0.106|1.5196) parameters. Altogether, this evidence indicates that the number of right answers in the No Go condition for inhibition response and the number of correct answers plus perseverative errors in the Wisconsin test for flexibility may be potential cognitive targets to be addressed in neuropsychological treatments in SUD patients and monitoring their therapeutic progress. Hence, scientific evidence suggests that cognitive parameters could function as a prediction of relapse in addictions [33,34], a deep statistical analysis would be necessary to evaluate the impact of cognition in drug recovery.
4. Discussion
In the present study, we report that polydrug consumers show a persistent increase in IL-6 plasma levels and deficits in working memory, inhibition, and cognitive flexibility performance during the withdrawal phase. Interestingly, IL-6 levels have a negative correlation with the number of correct answers and a positive correlation in the reaction time in the N-Back test for working memory. The CIBER analysis indicated that the inhibition response (correct answers in the No Go condition) and cognitive flexibility (correct answers and perseverative errors) are the most sensitive parameters to assess cognitive performance between the groups. Whereas the majority of intercorrelations between reaction time and right answers in all the tasks show a moderate to strong association.
The presence of higher levels of interleukins has been demonstrated in drug addiction [35]. In a recent meta-analysis by Wei (2020), they report elevated IL-6 levels as one of the highest proinflammatory cytokines in SUD patients with current abuse of alcohol, cocaine, opioids, nicotine, marijuana, and ketamine. This increase has been related to overstimulation of the HPA axis [36] followed by an increase of glucocorticoids [37]. Recently, it has been proposed that in addictive behavior exists biological and cultural intersex differences [38] that may affect the development, maintenance, and treatment response [39]. At the biological level, these sex differences are related to changes in hypothalamic-pituitary-adrenal (HPA) axis activity and mesolimbic sensitivity to dopamine [40]. Specifically, females present a decrease in the expression of D3 receptors in the nucleus accumbens [41] and higher levels of two biomarkers of stress, cortisol, and ACTH [23,42], when compared to males. Interestingly, there is co-stimulation between the increase of ACTH and IL-6 levels [23], which suggests that a stressor stimulus can increase the hyperactivity of HPA and maintain higher IL-6. Although, the availability of D2 receptors in the orbitofrontal cortex has also been involved in IL-6 dysregulation [43]. In female drug abusers, high levels of Il-6 tend to persist for three months after drug consumption cessation [27]. In our study, we found that IL-6 can remain increased for at least 5.5 months during the abstinence stage
In a recent meta-analysis, it has been reported that the normal range of IL-6 plasma levels in healthy individuals is 0 pg/ml to a maximum of 43.5 pg/ml, with a typical average range between 0.13 and 30.46 pg/ml [44]. In our study, we observed that the expression levels in the SUD group are higher compared to the control group, yet they fall within the range reported by this meta-analysis. Luo et al. (2021) also found values similar to ours, specifically higher IL-6 levels in amphetamine users compared to their controls, which also fall within the same range reported by this meta-analysis [45]. Although our data fall within the normal range, the elevated levels of IL-6 in individuals with SUD highlight the necessity for clinical awareness and further research to define their potential implications in clinical management.
IL-6 is considered one of the pivotal inflammation markers related to executive functions such as working memory [46]. Recently, the CIBER analysis was proposed as an innovative statistic model focused on identifying the social and cognitive determinants [47]. It also evaluates intention and self-efficacy to assist interventions in pregnant adolescents [48], as well as beliefs and behaviors of health providers [49], obesity [50], and more. However, in recent years, this model has also been proposed as an effective tool to identify cognitive performance in pathophysiological conditions such as alcoholism [51]. Our results indicate that the performance in inhibition and cognitive flexibility showed the highest score difference among all the executive functions evaluated, suggesting that they could be pivotal targets for designing neuropsychological rehabilitation programs during abstinence treatments in polydrug consumers. Identifying the cognitive parameters that need improvement in neuropsychological treatments is quite relevant because EFs’ performance is a strong predictor of treatment adherence during abstinence [52].
Cognitive flexibility is a process that regulates goal-directed behavior and is part of the mental set-shifting ability [53]. WCST is a reliable test to evaluate set-shifting. Hence, this test has been proposed as a cognitive indicator of frontal dysfunction. Specifically, a high number of perseverative errors (an error that occurs when a subject organizes or classifies a card according to a pre-established rule and not according to the current one) has been associated with lateral or dorsomedial prefrontal lesions [54]. In subjects with remitted smoking addiction, brain lesions in the insula, dorsal cingulated cortex, and dorsolateral prefrontal cortex have been reported, and a similar pattern of lesions has been suggested with other drug addictions [55]. Colzato et al. [56] report that the recreational use of stimulant drugs such as cocaine plus alcohol could be associated with increases in perseverative errors via dysfunction of DA2 receptors because of pint-size ischemic strokes [57]. In this paper, our analyses with the CIBER model identify perseverative errors as the most sensitive cognitive parameter, which may facilitate neuropsychological diagnosis and rehabilitation plans in these patients.
Cognitive flexibility requires the coordination and interaction between updating (working memory) and inhibition responses [53]. In this regard, the Go/No-Go test is one of the primary assays used to investigate inhibition responses [58], which evaluates the ability to respond to stimuli (go condition) while discriminating and stopping other stimuli (no-go condition) [59]. The score in the no-go condition indicates commissions, a type of error based on premature responses related to impulsivity [57]. In drug abusers, it has been suggested that failures in inhibition response underlie the impulsivity behavior that favors consumption [60]. According to the CIBER analysis, the number of correct answers in the no-go condition (commissions) and perseverative errors is a very relevant cognitive parameter to be evaluated during the withdrawal phase of drug addiction. This information will help clinicians design neuropsychological programs that improve inhibition response since cognitive function has been reported as a predictive parameter of relapse in some kinds of drugs (33,34).
In our study, we found that a worse performance in executive function persisted for at least 5.5 months during the abstinence stage. Depending on the type of drug abuse, the abstinence period is associated with sustained cognitive impairments. For example, a lack of recovery in cognitive functioning following the cessation of benzodiazepine has also been reported [61], while Loeber et al. showed that patients with alcohol abuse who underwent 3 months of withdrawal display poorer performance in executive function [62] that persists beyond 6 months [63] compared to healthy controls. In methamphetamine abusers, partial improvement has been reported over the course of 6 months [64].
Our data indicates that the average age of the SUD group does not differ significantly from the control group, with all participants falling within their 20s to 30s age. Age is a significant demographic variable that affects cognitive performance, as it has been reported that reaction time increases by 2 to 6 milliseconds per decade [65]. In this regard, a previous study suggested that the most significant differences in reaction times mediated by age are observed in groups with a considerable age gap between individuals, approximately 30 years [66]. In our study, all the subjects are in the same age range (20s to 30s), so we consider that the differences reported in the present study are not due to variations in age between the groups. Regarding the N-Back task, a meta-analysis by Yaple et al. which indicates that differences in reaction times are more pronounced in age groups between 23.57 and 38.13 years [67]. Since our study group is within this age range, we believe that age should not significantly impact our results on this task. Similarly, in the Go-No-Go test, our age group suggests that age effects on reaction times are less noticeable. These findings support the assertion that the observed performance differences are not due to significant age variations between the groups.
While our study offers significant insights, it is essential to acknowledge certain limitations. The relatively small sample size for group comparisons might have influenced the depth of the analysis. Although the CIBER model is an approach aimed at reducing data uncertainty, it should be evaluated alongside other clinical factors, such as medical history and individual responses to treatments. Future research could enhance the robustness of network analyses by expanding the SUD sample size, facilitating progress from theoretical to causal network interpretations. Additionally, prospective studies should focus on longitudinally monitoring SUD patients to explore potential correlations between relapse frequency and duration, interleukin-6 (IL-6) levels, and executive function performance. These approaches will further enrich our understanding of their long-term effects.
5. Conclusions
During the abstinence phase, polydrug users demonstrate marked deficits in working memory, inhibition, and cognitive flexibility, coupled with elevated plasma IL-6 levels. These neurocognitive impairments were evidenced by diminished correct responses in the Go/No-Go test and increased perseverative errors, suggesting that these may serve as cognitive biomarkers for diagnosing or monitoring the therapeutic progress in these patients. Targeting these deficits could guide the development of neuropsychological interventions such as self-impulse control training, tasks for adapting to new circumstances, strategies for skill development, and problem-solving and decision-making skills aimed at rehabilitating executive dysfunction in males with SUD during withdrawal, thereby enhancing treatment efficacy and reducing relapse risk.
Author Contributions
Conceptualization, Gonzalez-Castañeda Rocio E. and Galvez-Contreras Alma; methodology, Guzmán-González Jesua; software, Guzmán-González Jesua; validation, Gonzalez-Perez Oscar, Gonzalez-Castañeda Rocio E. and Galvez-Contreras Alma; investigation, Gonzalez-Castañeda Rocio E. and Guzmán-González Jesua; resources, Gonzalez-Perez Oscar, Perez-Alcaraz Iris S; data curation, Guzmán-González Jesua; writing—original draft preparation, Gonzalez-Castañeda Rocio E. and Guzmán-González Jesua; writing—review and editing, Gonzalez-Perez Oscar, Gonzalez-Castañeda Rocio E. and Galvez-Contreras Alma; visualization, Galvez-Contreras Alma; methodology, Guzmán-González Jesua; supervision, Jimenez-Navarro Israel I.; All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by Consejo Nacional de Humanidades, Ciencias y Tecnologías (CONAHCYT) with the scholarship number (2019-000002-01NACF-03040) to JIGG, (1085872) to ISPA, and the grant CF-2023-G893.
Institutional Review Board Statement
This protocol and its procedures were approved and supervised by the Ethical Committee (207/2021) of the Instituto Jaliscience de Salud Mental (SALME), Mexico, following the federal regulations and guidelines stipulated in the Mexican Official Norm (NOM-028-SSA2-1999 and NOM-012-SSA3-2012) and conducted following Declaration of Helsinki.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data is unavailable due to clinical privacy, but it can be requested from the authors of the article.
Acknowledgments
Thanks to Fundación México Me Necesita.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- American Psychological Association. Clinical Psychology. 2020.
- Fillmore MT. Drug Abuse as a Problem of Impaired Control: Current Approaches and Findings. Behav Cogn Neurosci Rev [Internet]. 2003 Sep 18;2(3):179–97. Available from: http://journals.sagepub.com/doi/10.1177/1534582303257007. [CrossRef]
- Volkow ND, Wang G-J, Fowler JS, Logan J, Gatley SJ, Hitzemann R, et al. Decreased striatal dopaminergic responsiveness in detoxified cocaine-dependent subjects. Nature [Internet]. 1997 Apr;386(6627):830–3. Available from: http://www.nature.com/articles/386830a0.
- Koob GF, Volkow ND. Neurocircuitry of Addiction. Neuropsychopharmacology [Internet]. 2010 Jan 26;35(1):217–38. Available from: https://www.nature.com/articles/npp2009110.
- Casey BJ, Jones RM. Neurobiology of the Adolescent Brain and Behavior: Implications for Substance Use Disorders. J Am Acad Child Adolesc Psychiatry [Internet]. 2010 Dec;49(12):1189–201. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0890856710006702.
- Lezak MD, Howieson D, Bigler E, Tranel D. Neuropsychological Assessment. 5th ed. New York: Oxford University Press Inc; 2012.
- Gilbert SJ, Burgess PW. Executive function. Curr Biol [Internet]. 2008 Feb;18(3):R110–4. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0960982207023676.
- Miyake A, Friedman NP, Emerson MJ, Witzki AH, Howerter A, Wager TD. The Unity and Diversity of Executive Functions and Their Contributions to Complex “Frontal Lobe” Tasks: A Latent Variable Analysis. Cogn Psychol. 2000 Aug;41(1):49–100.
- Aharonovich E, Nunes E, Hasin D. Cognitive impairment, retention and abstinence among cocaine abusers in cognitive-behavioral treatment. Drug Alcohol Depend [Internet]. 2003 Aug 20;71(2):207–11. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0376871603000929.
- Blume AW, Alan Marlatt G. The Role of Executive Cognitive Functions in Changing Substance Use: What We Know and What We Need to Know. Ann Behav Med [Internet]. 2009 Apr 28;37(2):117–25. Available from: https://academic.oup.com/abm/article/37/2/117-125/4565848.
- Horner MD, Harvey RT, Denier CA. Self-report and objective measures of cognitive deficit in patients entering substance abuse treatment. Psychiatry Res [Internet]. 1999 May;86(2):155–61. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0165178199000311.
- Aharonovich E, Hasin DS, Brooks AC, Liu X, Bisaga A, Nunes E V. Cognitive deficits predict low treatment retention in cocaine dependent patients. Drug Alcohol Depend [Internet]. 2006 Feb;81(3):313–22. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0376871605002516.
- Loftis JM, Choi D, Hoffman W, Huckans MS. Methamphetamine causes persistent immune dysregulation: a cross-species, translational report. Neurotox Res [Internet]. 2011 Jul;20(1):59–68. Available from: http://www.ncbi.nlm.nih.gov/pubmed/20953917.
- Wisor JP, Schmidt MA, Clegern WC. Cerebral microglia mediate sleep/wake and neuroinflammatory effects of methamphetamine. Brain Behav Immun [Internet]. 2011 May;25(4):767–76. Available from: http://www.ncbi.nlm.nih.gov/pubmed/21333736.
- Hanisch U-K. Microglia as a source and target of cytokines. Glia [Internet]. 2002 Nov;40(2):140–55. Available from: https://onlinelibrary.wiley.com/doi/10.1002/glia.10161. [CrossRef]
- Kreutzberg GW. Microglia: a sensor for pathological events in the CNS. Trends Neurosci [Internet]. 1996 Aug;19(8):312–8. Available from: https://linkinghub.elsevier.com/retrieve/pii/0166223696100497.
- Sekine Y, Iyo M, Ouchi Y, Matsunaga T, Tsukada H, Okada H, et al. Methamphetamine-Related Psychiatric Symptoms and Reduced Brain Dopamine Transporters Studied With PET. Am J Psychiatry [Internet]. 2001 Aug;158(8):1206–14. Available from: http://psychiatryonline.org/doi/abs/10.1176/appi.ajp.158.8.1206. [CrossRef]
- Felger JC, Li Z, Haroon E, Woolwine BJ, Jung MY, Hu X, et al. Inflammation is associated with decreased functional connectivity within corticostriatal reward circuitry in depression. Mol Psychiatry [Internet]. 2016 Oct 10;21(10):1358–65. Available from: http://www.nature.com/articles/mp2015168.
- Kohno M, Loftis JM, Huckans M, Dennis LE, McCready H, Hoffman WF. The relationship between interleukin-6 and functional connectivity in methamphetamine users. Neurosci Lett [Internet]. 2018 Jun;677:49–54. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0304394018303008.
- Dean AC, Kohno M, Morales AM, Ghahremani DG, London ED. Denial in methamphetamine users: Associations with cognition and functional connectivity in brain. Drug Alcohol Depend [Internet]. 2015 Jun 1;151:84–91. Available from: http://www.ncbi.nlm.nih.gov/pubmed/25840750.
- Dean AC, Kohno M, Hellemann G, London ED. Childhood maltreatment and amygdala connectivity in methamphetamine dependence: a pilot study. Brain Behav [Internet]. 2014;4(6):867–76. Available from: http://www.ncbi.nlm.nih.gov/pubmed/25365801.
- Kohno M, Morales AM, Ghahremani DG, Hellemann G, London ED. Risky decision making, prefrontal cortex, and mesocorticolimbic functional connectivity in methamphetamine dependence. JAMA psychiatry [Internet]. 2014 Jul 1;71(7):812–20. Available from: http://www.ncbi.nlm.nih.gov/pubmed/24850532.
- Jankord R, Turk JR, Schadt JC, Casati J, Ganjam VK, Price EM, et al. Sex Difference in Link between Interleukin-6 and Stress. Endocrinology [Internet]. 2007 Aug 1;148(8):3758–64. Available from: https://academic.oup.com/endo/article/148/8/3758/2502096.
- Anthenelli RM, Heffner JL, Blom TJ, Daniel BE, McKenna BS, Wand GS. Sex differences in the ACTH and cortisol response to pharmacological probes are stressor-specific and occur regardless of alcohol dependence history. Psychoneuroendocrinology [Internet]. 2018 Aug;94:72–82. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0306453017316384.
- Lockwood KG, Marsland AL, Cohen S, Gianaros PJ. Sex differences in the association between stressor-evoked interleukin-6 reactivity and C-reactive protein. Brain Behav Immun [Internet]. 2016 Nov;58:173–80. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0889159116301957.
- Carroll ME, Anker JJ. Sex differences and ovarian hormones in animal models of drug dependence. Horm Behav [Internet]. 2010 Jun;58(1):44–56. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0018506X09002219.
- Levandowski ML, Hess ARB, Grassi-Oliveira R, de Almeida RMM. Plasma interleukin-6 and executive function in crack cocaine-dependent women. Neurosci Lett [Internet]. 2016 Aug;628:85–90. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0304394016304323.
- Illenberger JM, Mactutus CF, Booze RM, Harrod SB. Testing environment shape differentially modulates baseline and nicotine-induced changes in behavior: Sex differences, hypoactivity, and behavioral sensitization. Pharmacol Biochem Behav [Internet]. 2018 Feb;165:14–24. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0091305717305270.
- Fattore L, Marti M, Mostallino R, Castelli MP. Sex and Gender Differences in the Effects of Novel Psychoactive Substances. Brain Sci [Internet]. 2020 Sep 3;10(9):606. Available from: https://www.mdpi.com/2076-3425/10/9/606.
- Peters G-JY, Crutzen R. Establishing determinant relevance using CIBER: an introduction and tutorial [Internet]. 2018. Available from: https://osf.io/5wjy4.
- Crutzen R, Ygram-Peters GJ, Noijen J. Using confidence interval-based estimation of relevance to select social-cognitive determinants for behavior change interventions. 2017;
- Stoet G. PsyToolkit: A software package for programming psychological experiments using Linux. Behav Res Methods. 2010 Nov;42(4):1096–104.
- Valentine G, Sofuoglu M. Cognitive Effects of Nicotine: Recent Progress. Curr Neuropharmacol [Internet]. 2018 May 1;16(4):403–14. Available from: http://www.eurekaselect.com/156791/article.
- Ashare RL, Schmidt HD. Optimizing treatments for nicotine dependence by increasing cognitive performance during withdrawal. Expert Opin Drug Discov [Internet]. 2014 Jun;9(6):579–94. Available from: http://www.ncbi.nlm.nih.gov/pubmed/24707983.
- Wei Z, Chen L, Zhang J, Cheng Y. Aberrations in peripheral inflammatory cytokine levels in substance use disorders: a meta-analysis of 74 studies. Addiction [Internet]. 2020 Dec 18;115(12):2257–67. Available from: https://onlinelibrary.wiley.com/doi/10.1111/add.15160. [CrossRef]
- Kubera M, Filip M, Budziszewska B, Basta-Kaim A, Wydra K, Leskiewicz M, et al. Immunosuppression Induced by a Conditioned Stimulus Associated With Cocaine Self-Administration. J Pharmacol Sci [Internet]. 2008;107(4):361–9. Available from: http://www.jstage.jst.go.jp/article/jphs/107/4/107_FP0072106/_article.
- Elenkov IJ. Glucocorticoids and the Th1/Th2 Balance. Ann N Y Acad Sci [Internet]. 2004 Jun;1024(1):138–46. Available from: http://doi.wiley.com/10.1196/annals.1321.010. [CrossRef]
- Harrod SB, Booze RM, Welch M, Browning CE, Mactutus CF. Acute and repeated intravenous cocaine-induced locomotor activity is altered as a function of sex and gonadectomy. Pharmacol Biochem Behav [Internet]. 2005 Sep;82(1):170–81. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0091305705002777.
- Becker JB, McClellan ML, Reed BG. Sex differences, gender and addiction. J Neurosci Res [Internet]. 2017 Jan 2;95(1–2):136–47. Available from: https://onlinelibrary.wiley.com/doi/10.1002/jnr.23963. [CrossRef]
- Fox HC, Sinha R. Sex Differences in Drug-Related Stress-System Changes. Harv Rev Psychiatry [Internet]. 2009 Apr;17(2):103–19. Available from: https://journals.lww.com/00023727-200904000-00004.
- Harrod SB, Mactutus CF, Bennett K, Hasselrot U, Wu G, Welch M, et al. Sex differences and repeated intravenous nicotine: behavioral sensitization and dopamine receptors. Pharmacol Biochem Behav [Internet]. 2004 Jul;78(3):581–92. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0091305704001546.
- Jacobskind JS, Rosinger ZJ, Zuloaga DG. Hypothalamic-pituitary-adrenal axis responsiveness to methamphetamine is modulated by gonadectomy in males. Brain Res [Internet]. 2017 Dec;1677:74–85. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0006899317304171.
- Volkow ND, Chang L, Wang G-J, Fowler JS, Ding Y-S, Sedler M, et al. Low Level of Brain Dopamine D 2 Receptors in Methamphetamine Abusers: Association With Metabolism in the Orbitofrontal Cortex. Am J Psychiatry [Internet]. 2001 Dec;158(12):2015–21. Available from: http://psychiatryonline.org/doi/abs/10.1176/appi.ajp.158.12.2015. [CrossRef]
- Said EA, Al-Reesi I, Al-Shizawi N, Jaju S, Al-Balushi MS, Koh CY, et al. Defining IL-6 levels in healthy individuals: A meta-analysis. J Med Virol [Internet]. 2021 Jun 22;93(6):3915–24. Available from: https://onlinelibrary.wiley.com/doi/10.1002/jmv.26654. [CrossRef]
- Luo Y, He H, Ou Y, Zhou Y, Fan N. Elevated serum levels of TNF-α, IL-6, and IL-18 in chronic methamphetamine users. Hum Psychopharmacol Clin Exp [Internet]. 2022 Jan 25;37(1). Available from: https://onlinelibrary.wiley.com/doi/10.1002/hup.2810. [CrossRef]
- Trevizol AP, Brietzke E, Grigolon RB, Subramaniapillai M, McIntyre RS, Mansur RB. Peripheral interleukin-6 levels and working memory in non-obese adults: A post-hoc analysis from the CALERIE study. Nutrition [Internet]. 2019 Feb;58:18–22. Available from: http://www.ncbi.nlm.nih.gov/pubmed/30273821.
- Vervoort L, Naets T, De Guchtenaere A, Tanghe A, Braet C. Using confidence interval-based estimation of relevance to explore bottom-up and top-down determinants of problematic eating behavior in children and adolescents with obesity from a dual pathway perspective. Appetite [Internet]. 2020 Jul 1;150:104676. Available from: http://www.ncbi.nlm.nih.gov/pubmed/32198094.
- Sewpaul R, Crutzen R, Reddy P. Psychosocial determinants of the intention and self-efficacy to attend antenatal appointments among pregnant adolescents and young women in Cape Town, South Africa: a cross-sectional study. BMC Public Health [Internet]. 2022 Sep 23;22(1):1809. Available from: http://www.ncbi.nlm.nih.gov/pubmed/36151528.
- Srisurapanont M, Lamyai W, Pono K, Indrakamhaeng D, Saengsin A, Songhong N, et al. Cognitive impairment in methamphetamine users with recent psychosis: A cross-sectional study in Thailand. Drug Alcohol Depend [Internet]. 2020 May;210:107961. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0376871620301265.
- Lugones-Sanchez C, Crutzen R, Recio-Rodriguez JI, Garcia-Ortiz L. Establishing the relevance of psychological determinants regarding physical activity in people with overweight and obesity. Int J Clin Health Psychol [Internet]. 2021;21(3):100250. Available from: http://www.ncbi.nlm.nih.gov/pubmed/33995540.
- Crutzen R, Peters G-JY. A lean method for selecting determinants when developing behavior change interventions. Heal Psychol Behav Med [Internet]. 2023 Dec 31;11(1). Available from: https://www.tandfonline.com/doi/full/10.1080/21642850.2023.2167719. [CrossRef]
- Charlton RA, Lamar M, Zhang A, Ren X, Ajilore O, Pandey GN, et al. Associations between pro-inflammatory cytokines, learning, and memory in late-life depression and healthy aging. Int J Geriatr Psychiatry [Internet]. 2018 Jan;33(1):104–12. Available from: https://onlinelibrary.wiley.com/doi/10.1002/gps.4686.
- Uddin LQ. Cognitive and behavioural flexibility: neural mechanisms and clinical considerations. Nat Rev Neurosci [Internet]. 2021 Mar 3;22(3):167–79. Available from: https://www.nature.com/articles/s41583-021-00428-w.
- Teubner-Rhodes S, Vaden KI, Dubno JR, Eckert MA. Cognitive persistence: Development and validation of a novel measure from the Wisconsin Card Sorting Test. Neuropsychologia [Internet]. 2017 Jul;102:95–108. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0028393217302014.
- Joutsa J, Moussawi K, Siddiqi SH, Abdolahi A, Drew W, Cohen AL, et al. Brain lesions disrupting addiction map to a common human brain circuit. Nat Med [Internet]. 2022 Jun 13;28(6):1249–55. Available from: https://www.nature.com/articles/s41591-022-01834-y.
- Colzato LS, Huizinga M, Hommel B. Recreational cocaine polydrug use impairs cognitive flexibility but not working memory. Psychopharmacology (Berl) [Internet]. 2009 Dec 2;207(2):225–34. Available from: http://link.springer.com/10.1007/s00213-009-1650-0.
- Morein-Zamir S, Robbins TW. Fronto-striatal circuits in response-inhibition: Relevance to addiction. Brain Res [Internet]. 2015 Dec;1628:117–29. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0006899314011998.
- Sjoberg EA, Cole GG. Sex Differences on the Go/No-Go Test of Inhibition. Arch Sex Behav [Internet]. 2018 Feb 12;47(2):537–42. Available from: http://link.springer.com/10.1007/s10508-017-1010-9.
- Young ME, Sutherland SC, McCoy AW. Optimal go/no-go ratios to maximize false alarms. Behav Res Methods [Internet]. 2018 Jun 29;50(3):1020–9. Available from: http://link.springer.com/10.3758/s13428-017-0923-5.
- Bari A, Robbins TW. Inhibition and impulsivity: Behavioral and neural basis of response control. Prog Neurobiol [Internet]. 2013 Sep;108:44–79. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0301008213000543.
- Barker MJ, Greenwood KM, Jackson M, Crowe SF. Cognitive Effects of Long-Term Benzodiazepine Use. CNS Drugs [Internet]. 2004;18(1):37–48. Available from: http://link.springer.com/10.2165/00023210-200418010-00004.
- Loeber S, Duka T, Welzel Marquez H, Nakovics H, Heinz A, Mann K, et al. Effects of Repeated Withdrawal from Alcohol on Recovery of Cognitive Impairment under Abstinence and Rate of Relapse. Alcohol Alcohol [Internet]. 2010 Nov 1;45(6):541–7. Available from: https://academic.oup.com/alcalc/article-lookup/doi/10.1093/alcalc/agq065.
- Munro CA, Saxton J, Butters MA. The neuropsychological consequences of abstinence among older alcoholics: a cross-sectional study. Alcohol Clin Exp Res [Internet]. 2000 Oct;24(10):1510–6. Available from: http://www.ncbi.nlm.nih.gov/pubmed/11045859.
- Proebstl L, Krause D, Kamp F, Hager L, Manz K, Schacht-Jablonowsky M, et al. Methamphetamine withdrawal and the restoration of cognitive functions – a study over a course of 6 months abstinence. Psychiatry Res [Internet]. 2019 Nov;281:112599. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0165178119314933.
- Hardwick RM, Forrence AD, Costello MG, Zackowski K, Haith AM. Age-related increases in reaction time result from slower preparation, not delayed initiation. J Neurophysiol [Internet]. 2022 Sep 1;128(3):582–92. Available from: https://journals.physiology.org/doi/10.1152/jn.00072.2022. [CrossRef]
- Cheng C-H, Tsai H-Y, Cheng H-N. The effect of age on N2 and P3 components: A meta-analysis of Go/Nogo tasks. Brain Cogn [Internet]. 2019 Oct;135:103574. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0278262618303737.
- Yaple ZA, Stevens WD, Arsalidou M. Meta-analyses of the n-back working memory task: fMRI evidence of age-related changes in prefrontal cortex involvement across the adult lifespan. Neuroimage [Internet]. 2019 Aug;196:16–31. Available from: https://linkinghub.elsevier.com/retrieve/pii/S1053811919302812.
Figure 1.
Peripheric IL-6 levels between groups. Boxplot of the peripheral levels of IL-6 and their differences between the groups (rbr = 0.42), the red dot symbolizes the median of the groups, which was for the SUD group 13.2 (12.07 - 14) and 10 (8.64 - 14.10) for the control group.
Figure 1.
Peripheric IL-6 levels between groups. Boxplot of the peripheral levels of IL-6 and their differences between the groups (rbr = 0.42), the red dot symbolizes the median of the groups, which was for the SUD group 13.2 (12.07 - 14) and 10 (8.64 - 14.10) for the control group.
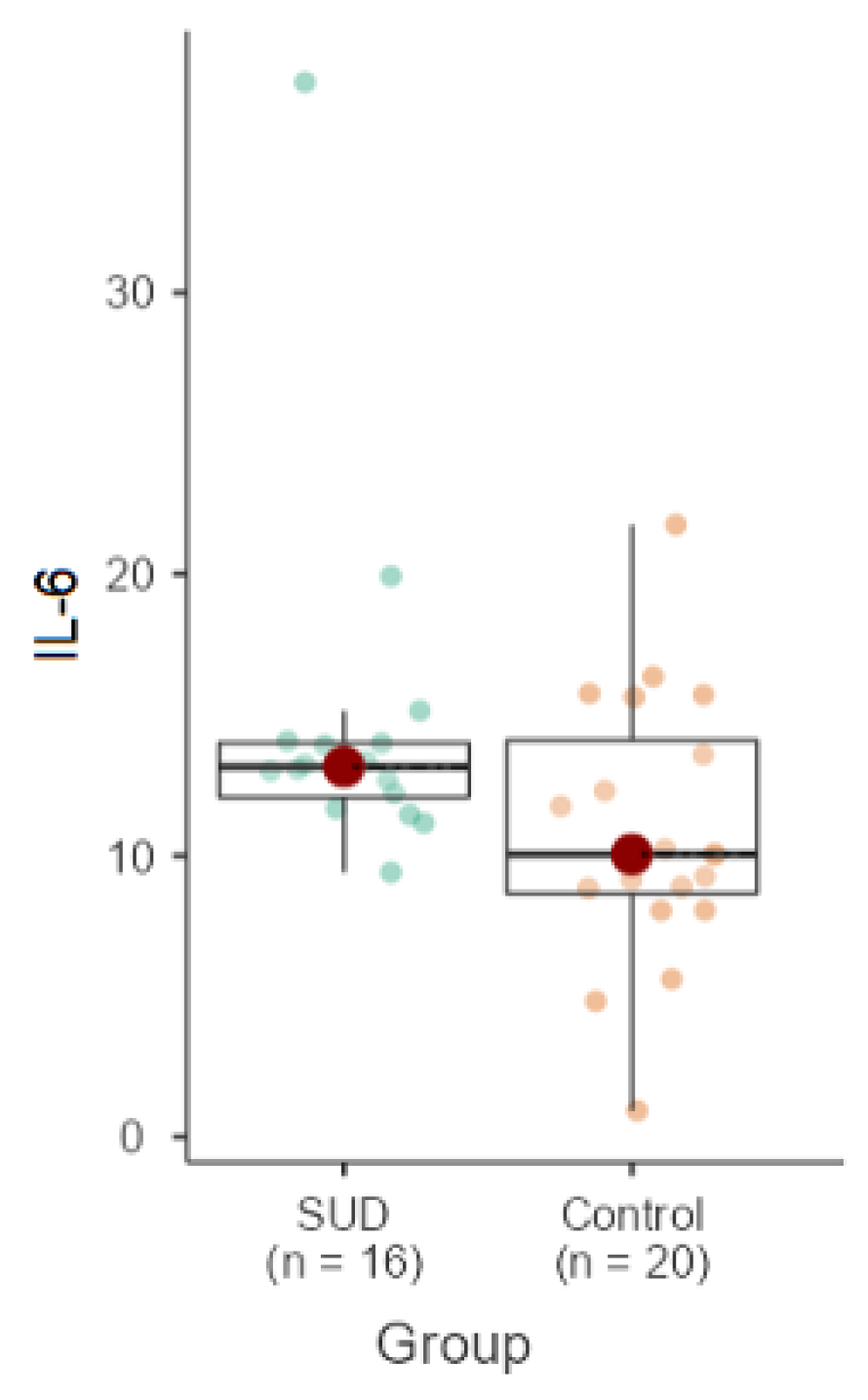
Figure 2.
CIBER plot of EF performance visualizing means and differences between control and SUD groups. The fill color of the diamonds indicates the group: SUD (aquamarine) and control (purple). Each dot indicates the score of each subject and the distance between diamonds represents the difference of distribution data. In the right panel, the diamond colors indicate the direction and strength of the differences. The color indicates the association of the answers: a green-colored diamond suggests positive associations and a red-colored diamond has negative associations. The more intense the color the stronger the associations.
Figure 2.
CIBER plot of EF performance visualizing means and differences between control and SUD groups. The fill color of the diamonds indicates the group: SUD (aquamarine) and control (purple). Each dot indicates the score of each subject and the distance between diamonds represents the difference of distribution data. In the right panel, the diamond colors indicate the direction and strength of the differences. The color indicates the association of the answers: a green-colored diamond suggests positive associations and a red-colored diamond has negative associations. The more intense the color the stronger the associations.
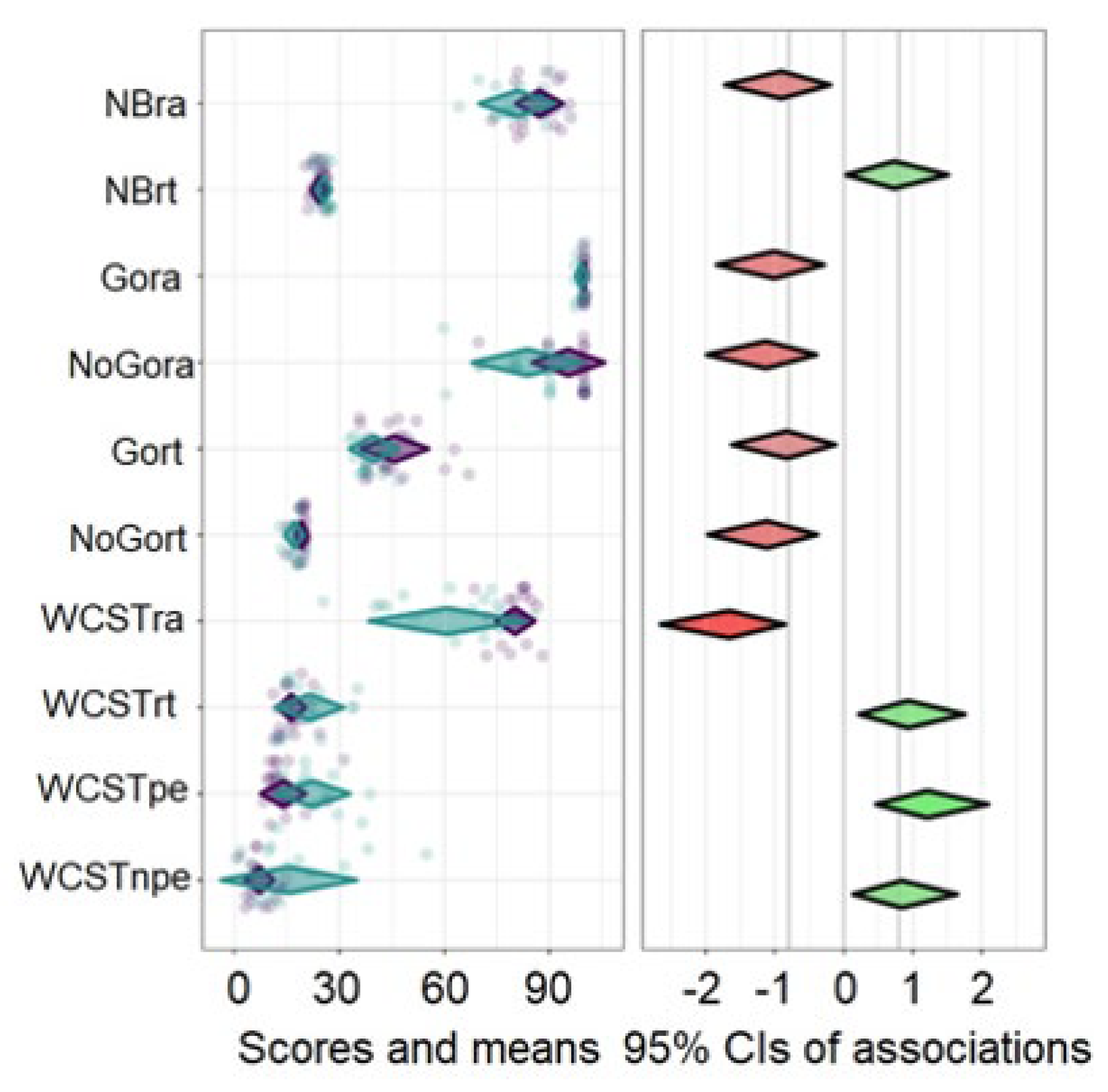

Table 1.
Sociodemographic characteristics of the SUD group and control.
| Control Med(IQR) |
SUD Med (IQR) |
Statistical test | |
|---|---|---|---|
| Age | 21.0 (2.0) | 24.5 (7.75) | U = 108.5, δ = 0.48, p = 0.15 |
| Year of schooling | 12.0 (0.0) | 12.0 (0.0) | U = 186.5, δ = 0.27, p = 0.29 |
| Days with abstinence | 171 (59.8) | ||
| f (%) | |||
| Consumption type | |||
| Alcohol | 16 (100%) | ||
| Tobacco | 16 (100%) | ||
| Inhalants | 2 (10.53%) | ||
| Cannabinoids | 6 (31.58%) | ||
| Benzodiazepines | 1 (5.26%) | ||
| Methamphetamines | 16 (100%) | ||
| Sociodemographic data are expressed as the median (Med) and interquartile rank (IQR), and frequency (f) of. Statistical analysis: Mann-Whitney U test. | |||
Table 2.
Performance of the SUD and control groups in the neuropsychological test.
| Test | Control Med (IQR) |
SUD Med (IQR) |
U | p |
|---|---|---|---|---|
| NBack right answer | 88.66 (82.33-92.00) | 80 (74.67-88.00) | 86 | 0.019* |
| NBack reaction time | 25.00(22.36-25.59) | 25.96(24.17-26.66) | 94 | 0.037* |
| Go-no-go right answer Go | 100 (100-100) | 100 ((97.50-100) | 110 | 0.009** |
| Go-no-go right answer no-go | 100 (97.50-100) | 90 (80.00-90.00) | 58.5 | 0.001* |
| Go-no-go reaction time Go | 43.91 (38.39-48.13) | 37-56 (36.50-44.03) | 88 | 0.023* |
| Go-no-go reaction time no-go | 20.00 (19.59-20.00) | 18.27(16.49-18.31) | 60 | 0.001*** |
| WCST right answer | 81.66 (78.33-83.33) | 65.83 (47.08-73.75) | 35 | 0.001*** |
| WCST reaction time | 15.82 (13.65-17.96) | 20.59 (15.36-24) | 101 | 0.063 |
| WCST perseverative errors | 11.66 (10-15) | 20 ((15.00-27.08) | 53.5 | 0.001*** |
| WCST non-perseverative errors | 6.66 (5.00-8.75) | 10 (6.25-19.17) | 99 | 0.053 |
| Data are expressed as the median (M) and the interquartile rank (IQR). WSCT = Wisconsin sort card test; NB = N-Back test. Statistical differences were established with the Mann-Whitney U test (P < 0.05). | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



